CARROTS THEN STICKS Medicare and Medicaid Incentive Payments and Penalties for Physicians Part One...
61
CARROTS THEN STICKS Medicare and Medicaid Incentive Payments and Penalties for Physicians Part One of Two Part Series Presented by: POWERS PYLES SUTTER & VERVILLE, PC January 18, 2011 1501 M Street, NW Seventh Floor Washington, DC 20005 Phone: (202) 466-6550 Fax: (202) 785-1756 www.ppsv.com Presenters: Rebecca Burke [email protected] Barbara Straub Williams [email protected] Diane Millman [email protected]
-
Upload
damian-harrison -
Category
Documents
-
view
219 -
download
2
Transcript of CARROTS THEN STICKS Medicare and Medicaid Incentive Payments and Penalties for Physicians Part One...

CARROTS THEN STICKSMedicare and Medicaid Incentive Payments
and Penalties for PhysiciansPart One of Two Part Series
Presented by:
POWERS PYLES SUTTER & VERVILLE, PCJanuary 18, 2011
1501 M Street, NWSeventh FloorWashington, DC 20005Phone: (202) 466-6550Fax: (202) 785-1756www.ppsv.com
Presenters:
Rebecca [email protected]
Barbara Straub [email protected]
Diane Millman [email protected]
Disclaimer
This presentation is for informational purposes only and does not provide legal services or advice. Use of this information does not create an attorney-client relationship. You should not act, or refrain from acting, on the basis of information contained herein without seeking additional legal counsel regarding your own situation.
The firm does not necessarily endorse, and is not responsible for, any third-party content that may be accessed through links or otherwise.
If we can assist you or answer any questions you might have, please call us in Washington, DC at 202.466.6550, or send us an email.
© Copyright 2011, Powers Pyles Sutter & Verville PC, Washington, DC, USA.

3
Overview■ Powerpoints will address:
1) Primary Care and Surgery Bonuses
2) Medicare and Medicaid HITECH EHR incentives and penalties
3) Medicare E-prescribing incentives and penalties
4) Medicare PQRS incentive and penalties

Primary Care Bonus
Beginning January 1, 2011 for 5 years – 10 Percent Medicare payment bonus for “primary care services.”
Must be furnished by “primary care practitioner” which is defined as: a physician nurse practitioner clinical nurse specialist physician assistant
4

Primary Care Bonus
With primary specialty designation of: Family medicine Internal Medicine Geriatrics Pediatrics Or NPP/PA/CNS designation
5

Primary Care Bonus – 60% Test
60% of Medicare physician fee schedule allowed charges must be attributable to “primary care services.”
Primary Care Services are: Outpatient office visits Nursing facility visits including discharge day management
and annual assessment Domiciliary visits Physician supervision of patients in domiciliary home Home visits
Annual Wellness Visits and the Initial Preventive Physical Exam do not qualify as “primary care services.”
6

Primary Care Bonus – Calculation
“Allowed charges” for denominator of 60 percent calculation to exclude laboratory, DME, or drugs.
CMS has also removed from the denominator of the calculation hospital and emergency department visits.
7

Primary Care Bonus - Calculation
CMS will look at claims data for two years prior to bonus to determine eligibility.
Thus, eligibility for bonus in 2011 will be based on 2009 claims.
Exception for new primary care practitioners: For physicians newly enrolling, CMS will determine eligibility based on prior year.
Example: if physician enrolls anytime in 2010, 2010 claims will be looked at.
8

Primary Care Bonus Disbursement
CMS will calculate bonus eligibility based on practitioner’s NPI.
No need to register or apply. NP or PA cannot qualify if services are billed
“incident to” the physician. CMS intends to pay the bonus in a lump sum on a
quarterly basis. For newly enrolled physicians bonus will probably not
be disbursed until 3rd quarter of the year but payment will be for the full year.
9

Challenging CMS Bonus Calculation There is no judicial or administrative review However, CMS will review calculation errors
brought to their attention.
10

Impact on HPSA Bonus
The Primary Care Bonus is on top of any bonus a physician may receive for practicing in a health professional shortage area.
Therefore, physicians can be eligible for both bonuses.
11

General Surgery Bonus
+10% bonus for general surgeons working in health professional shortage areas: 2011 - 2015. Applies to major procedures (10- and 90-day global payments)
Bonus is on top of existing HPSA bonus.
12

General Surgery Bonus
Payment will be made quarterly Medicare contractors will identify qualifying
physicians and pay the bonus – no need to apply. CMS website to determine if you are in an area
that qualifies for a bonus:
https://www.cms.gov/HPSAPSAPhysicianBonuses/01_Overview.asp#TopOfPage

Physician Value-Based Payment Modifier
Secretary to establish physician payment modifier to provide for differential payment based on quality of care compared to cost
Quality to be evaluated based on quality measures including those related to outcomes
Measures shall be risk adjusted and payment differential established by HHS regulation
Beginning in 2015, payment modifier for quality shall apply to subset of physicians
Beginning in 2017, it shall apply to all physicians
14

CMS Implementation Strategy – Development of Episode Grouper An “episode grouper” is software that organizes
claims data into clinically coherent episodes of care across different providers
It includes all contacts with the health care system for a specific health problem between a start and end point.
15

CMS Implementation Strategy – Episode Grouper CMS intends to implement the physician payment
modifier through an episode grouper. The costs will be risk-adjusted Episodes will be attributed to providers The grouper will allow CMS to compare costs of
care for similar patients across physicians
16

Timetable for Implementation of Payment Modifier Prototype episode grouper by January 1, 2012
limited to small number of conditions Expand and refine prototype grouper for limited
use in 2015 Use for all physicians in 2017
17

COMPARISON OVERVIEW – EHR, eRx and PQRS Medicare EHR Medicaid EHR Medicare eRx PQRS
Eligible Professional
MD, DO, Dentist, Podiatrist, Optometrist or Chiropractor, EXCEPT hospital-based
Physician, Dentist, Midwife, NP and some PAs, EXCEPT hospital-based.
MD, DO, Dentist, Oral Surgeon, Podiatrist, Optometrist, Chiropractor, PA, NP, Nurse Sp., Social Worker, Psychologist, Dietician, Nutritionist, Audiologist, PT, OT, ST.
Same as eRx
Patient Volume Requirement
None 30% Medicaid; 20% for Peds; special rules if practice in FQHC or RHC
At least 10% of allowed charges in designated codes
No, but must have sufficient Medicare patients to meet reporting thresholds.
General Requirements for Incentive Payment
Meaningful use, including clinical data reporting
Meaningful use, clinical data reporting (BUT in 1st year can buy, implement or upgrade).
25 e-prescriptions in designated codes
For Individual Measures:Claims: At least 3 measures for 50% of eligible patientsRegistry and EHR: At least 3 measures for 80% of eligible patients. For Group Measures: See Table 74 in final PFS Rule (11/29/10 Fed Reg)
Group Practice EPs can assign payment to group
No specific provision Yes, if participating in PQRS. Yes, apply before 1/31/11 for 2011.
Payment $24,000 - $44,000 (+ 10% if HPSA)
$63,750 2011 and 2012 – 1% add-on2013 – 0.5% add-on
2011 – 1% add-on2012-2014 – 0.5% add-onAdditional 0.5% add-on for MOC participation
Incentive Start 1/1/11 1/1/11 2009 2007
Penalties (only apply if qualify for incentive)
2015 - 1% decrease2016 - 2% decrease2017 - 3% decrease2018 - 3-5% decrease
None 2012 - 1% decrease2013 - 1.5% decrease2014 and after - 2% decrease
2015 – 1.5% decrease2016 and after – 2% decrease
18
Overview - EHR, eRx and PQRS
Can an EP receive Medicare EHR, Medicaid EHR, eRx and PQRS incentives? Cannot receive both Medicare and Medicaid EHR incentive Cannot receive both Medicare EHR and eRx incentives Group that participates in eRx must participate PQRS So, “combo” choices are:
Medicare EHR and PQRS Medicaid EHR, eRx and/or PQRS eRx and/or PQRS
19

Medicare EHR Incentives
Medicare and Medicaid EHR Program Resources :
CMS Website on EHR Incentives: http://www.cms.gov/EHRIncentivePrograms/
42 CFR Part 495 Federal Register – July 28, 2010 – pp. 44314-588
20

Medicare EHR Incentives
Medicare Eligibility and Criteria Starting 2011, incentive payments are available for “eligible
professionals” (or “EPs”) that are “meaningful users” of “certified EHR technology.”
For Medicare, an EP is defined as a physician, dentist, podiatrist, optometrist or chiropractor.
EP cannot be hospital-based. A hospital-based EP is one who provides 90% or more in his or her covered professional services in an inpatient or ER dept. (Place of service codes 21 and 23). 90% test based on number of services, not amount of charges or payment.
21

Medicare EHR Incentives
Medicare Payments Incentive payment is 75% of allowed charges, subject to cap.
Note: Highest payments if start using EHR in 2011 or 2012. Based on claims submitted by end of February for prior year. Single, annual payment once criteria met. If in a Health Professional Shortage Area, payments are increased by 10%. Payment based on SSI/TIN number.
2011 2012 2013 2014 2015 2016 TOTAL
Start Use in 2011 18,000 12,000 8,000 4,000 2,000 0 44,000
Start Use in 2012 18,000 12,000 8,000 4,000 2,000 44,000
Start Use in 2013 15,000 12,000 8,000 4,000 39,000
Start Use in 2014 12,000 8,000 4,000 24,000
Start Use in 2015 0 0 0
22

Medicare EHR Penalties
Penalties begin in 2015 for professionals who are not meaningful users. Reduction to Medicare Fee Schedule: FY 2015 – 1% FY 2016 – 2% FY 2017 – and subsequent years – 3% For 2018 and subsequent years – may be up to 5%
If hospital-based EP, penalties do not apply. Hardship exceptions.
Case-by-case basis. Ex: no internet access in area. Annual determination. No more than 5 years. CMS will issue guidance later.
23
Medicare EHR Incentives
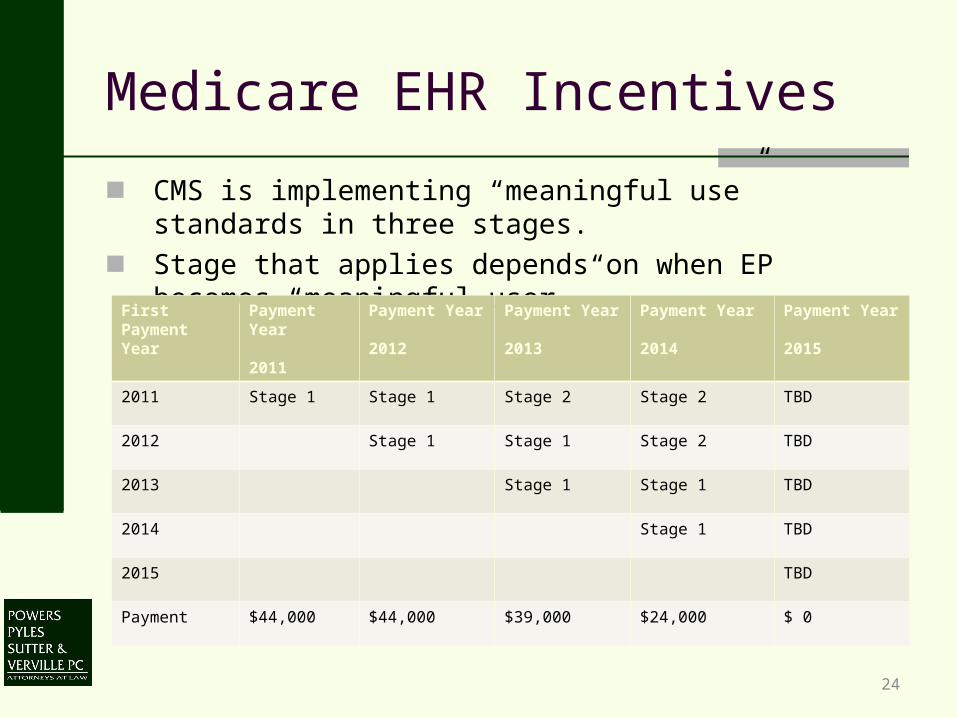
■ CMS is implementing “meaningful use” standards in three stages.
■ Stage that applies depends on when EP becomes “meaningful user.”
First Payment Year
Payment Year
2011
Payment Year
2012
Payment Year
2013
Payment Year
2014
Payment Year
2015
2011 Stage 1 Stage 1 Stage 2 Stage 2 TBD
2012 Stage 1 Stage 1 Stage 2 TBD
2013 Stage 1 Stage 1 TBD
2014 Stage 1 TBD
2015 TBD
Payment $44,000 $44,000 $39,000 $24,000 $ 0
24

Medicare EHR Incentives
Two types of Stage 1 measures: 1) Core measures 15; and 2) Menu measures select 5 from list of 10. Exclusions apply to some measures and reduce total # of required
measures. Example: EPs must use computerized provider order entry (CPOE) for at least one prescription for 30% of all unique patients with a prescription. (Note: CPOE – computer assistance to enter
medical order, but not transmit order.) Exclusion: Any EP who writes fewer than 100 prescriptions during the reporting period.
Some measures only counted as to patients whose records are maintained through EHR.
List of measures on CMS website.
25
Medicare EHR Incentives
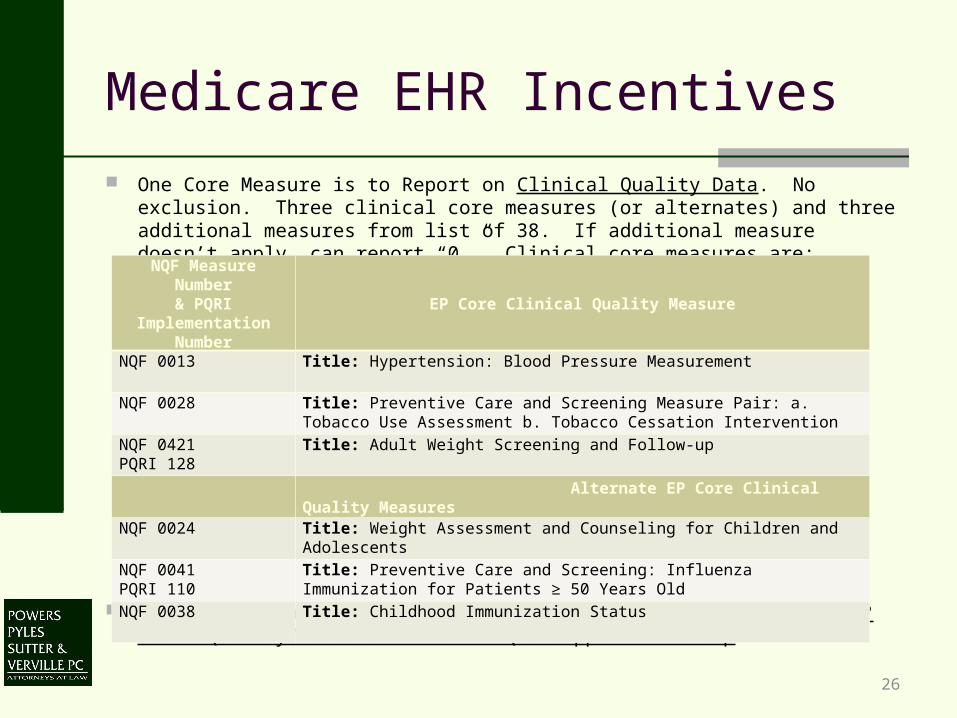
One Core Measure is to Report on Clinical Quality Data. No exclusion. Three clinical core measures (or alternates) and three additional measures from list of 38. If additional measure doesn’t apply, can report “0.” Clinical core measures are:
Additional measures at: http://www.cms.gov/apps/ama/license.asp?file=/QualityMeasures/Downloads/QMEPSupplemental.zip
NQF Measure Number& PQRI
Implementation Number
EP Core Clinical Quality Measure
NQF 0013 Title: Hypertension: Blood Pressure Measurement
NQF 0028 Title: Preventive Care and Screening Measure Pair: a. Tobacco Use Assessment b. Tobacco Cessation Intervention
NQF 0421PQRI 128
Title: Adult Weight Screening and Follow-up
Alternate EP Core Clinical Quality Measures
NQF 0024 Title: Weight Assessment and Counseling for Children and Adolescents
NQF 0041PQRI 110
Title: Preventive Care and Screening: Influenza Immunization for Patients ≥ 50 Years Old
NQF 0038 Title: Childhood Immunization Status
26

Medicare EHR Incentives
Demonstrating meaningful use: For 2011, report meaningful use through attestation statement,
including clinical quality measures. For 2012, CMS plans electronic reporting.
Reporting period for meaningful use: For first year that EP reports – reporting period is any
continuous 90-day period, which allows EPs to begin as late as October 1.
Subsequent years – reporting period is entire year.
27

Medicare EHR Incentives
If EP practices at more than one location: EP must have 50% more of his/her patient visits at location(s) with
EHR; and Meaningful use measures apply only to locations with EHR.
Note that payments are made based on individual’s SSI or TIN number, but if EP practices in a group, the EPs may reassign incentive payments. Assignment not required, even if other Medicare payments are reassigned. If EP reassigns, must assign entire amount to only one employer or entity.
28

Medicare EHR Incentives
How to Register? Registration opened January 3. CMS expects attestations and
payments to begin May 2011.
Compliance Reviews CMS plans to conduct selected compliance reviews to validate
eligibility.
EPs must maintain evidence of eligibility for 6 years.
Posting CMS will post online EPs who are meaningful users.
29
Medicare EHR Incentives
What is Certified EHR technology?
EPs must use technology that is certified.
EPs can check whether technology is certified on the CMS website. Link: http://onc-chpl.force.com/ehrcert
30

Medicare EHR Incentives – Appeals
No administrative or judicial review of:
Methods or standards for payment incentives and penalties;
Methods or standards for determining meaningful user and hardship exception; or
Methods or standards for determining eligible professionals.
31

Medicaid EHR Incentives
Medicaid Eligibility and Criteria Eligible Professionals:
Physician Dentist Certified nurse-midwife Nurse Practitioner Physician Assistants if practicing in a RHC or FQHC led by a Physician
Assistant. Not hospital-based (same definition as for Medicare). Patient Volume > 30% Medicaid; but Pediatricians > 20% Medicaid.
OR Same professionals who practice in FQHC or RHC and patient volume >
30% “Needy Individuals.” Needy Individuals includes Medicaid, SCHIP, uncompensated care or sliding scale care based on ability to pay. CMS may adjust uncompensated care to account for bad debt.
32

Medicaid EHR Incentives
To get first year Medicaid payment, EP doesn’t have to show “meaningful use;” have option to show adopted, implemented or upgraded EHR. Purchase of EHR is sufficient.
For subsequent payments, must demonstrate meaningful use. States are permitted to modify some of the Medicare meaningful use criteria.
Registration currently available in some states (Alaska, Iowa, Kentucky, Louisiana, Oklahoma, Michigan, Mississippi, N. Carolina, S. Carolina, Tennessee and
Texas). Other states will roll out registration later in year.
33

Medicaid Incentives
Calendar Year
2011 2012 2013 2014 2015 2016
2011 $21,250 ---------- ---------- --------- ----------- ------------
2012 $8,500 $21,250 ---------- --------- ----------- ------------
2013 $8,500 $8,500 $21,250 ---------- ---------- ----------
2014 $8,500 $8,500 $8,500 $21,250 ---------- ----------
2015 $8,500 $8,500 $8,500 $8,500 $21,250 ----------
2016 $8,500 $8,500 $8,500 $8,500 $8,500 $21,250
2017 ---------- $8,500 $8,500 $8,500 $8,500 $8,500
2018 ---------- ---------- $8,500 $8,500 $8,500 $8,500
2019 ---------- ---------- ---------- $8,500 $8,500 $8,500
2020 ---------- ---------- ---------- ---------- $8,500 $8,500
2021 ---------- ---------- ---------- ---------- ---------- $8,500
TOTAL $63,750 $63,750 $63,750 $63,750 $63,750 $63,750
Medicaid Incentive Payments for EPs who begin adoption in
■ States can spread the Medicaid payments over 3 to 6 years.■ Pediatricians qualifying under 20% Medicaid criteria get 2/3 of above.
34

Medicaid Incentives
No Medicaid penalties. If EP practices in more than one state, must pick one state
annually for Medicaid payment. Review process for disputes (unlike Medicare).
35

E-prescribing “eRx” Incentive Payment
eRx Incentive Payment – Resources CMS website: http://www.cms.gov/ERxIncentive/ 42 CFR § 412.92 Federal Register – Nov. 29, 2010 – p. 73551-66.
36

eRx Incentive Payment
Eligible Professionals: Physicians (MD, DO, Dentist, Oral Surgeon, Podiatrist, Optometrist, Chiropractor) Physical and Occupational Therapists Qualified Speech-Language Pathologists Nurse practitioners Physician Assistants Clinical Nurse Specialists Certified Registered Nurse Anesthetists (and anesthesiologist assistants) Certified Nurse Midwives Clinical Social Workers Clinical Psychologists Registered Dieticians Nutrition Professionals Qualified Audiologists
37

eRx Incentive Payment
Two requirements:
At least 10% or more of EP’s allowed charges must be in these codes:
90801; 90802; 90804; 90805; 90806; 90807; 90808; 90809; 90862; 92002; 92004; 92012; 92014; 96150; 96151; 96152; 99201; 99202; 99203; 99204; 99205; 99211; 99212; 99213; 99214; 99215; G0101; G0108; G0109; 99304; 99305; 99306; 99307; 99308; 99309; 99310; 99315; 99316; 99324; 99325; 99326; 99327; 99328; 99334; 99335; 99336; 99337; 99341; 99342; 99343; 99344; 99345; 99347; 99348; 99349; and 99350.
Must report 25 e-prescribing events in one or more of these codes. Report by using G8553 on claim. G8553 code means that at least one prescription in connection with the visit was e-prescribed. Faxed prescriptions do not count. If pharmacy can’t receive the prescription electronically, still counts.
38

eRx Incentive Payment
General description of codes: 90801, 90802, 90804 - 90809, 90862 – Psych 92002, 92004, 92012, 92014 – Eye 96150, 96151, 96152 – Behavioral Assessment 99201 – 99205 – New Patient E/M 99211 – 99215 – Established Patient E/M G0101, G0108, G0109 – Screening and Diabetic Training 99304 – 99310 – SNF/NF Visits 99315, 99316 – SNF/NF Discharge Services 99324 – 99328, 99334 – 99337 – E/M in ALF, Group Home, etc.
99341 – 99345, 99347 – 99350 – E/M in Patient Home
39

eRx Incentive Payment
eRx incentive is percentage of all Medicare fee schedule charges (not including drugs) based on EP’s TIN/NPI. 2011, 2012 – 1% 2013 – 0.5%
EPs have until February 28, 2012 to submit CY 2011 claims to show they qualify. (If qualified for CY 2010, have until February 28, 2011).
40

eRx Incentive Payment
May report through:
Claims submissions.
Qualified Registry – (Some registries qualify for both PQRS and eRx). Check CMS website for list of registries. Currently 2010 list available: http://www.cms.gov/PQRI/Downloads/Qualified_Registries_Phase4_eRxPQRI_06282010_FINAL.pdf
Qualified EHR – Check CMS website for list. http://www.cms.gov/PQRI/Downloads/QualifiedEHRVendorsforthe2011PhysicianQualityReportingandeRx121310.pdf
41

eRx Incentive Payment – Group Practices Group practices with 200 or > EPs (“GPRO I”) are eligible for
incentives if:1) at least 2,500 electronic prescriptions.
2) participate in PQRS.
Group practices with < 200 EPs (“GPRO II”) are eligible if:1) at least 75-1,875 electronic prescriptions (varies based on the group’s
size)
2) participate in PQRS
Group has to self-nominate by 1/31/11 to participate in PQRS
42
eRx Incentive Payment
Must use “qualified” electronic prescribing system, which incorporates e-prescribing standards under Medicare Part D CMS will not identify qualified systems, but has requirements:
(a) Generate a complete active medication list incorporating electronic data from pharmacies and PBMs using NCPDP SCRIPT 8.1.
(b) Select medications, print prescriptions, conduct alerts and electronically transmit prescriptions using NCPDP SCRIPT 8.1.
(c) Provide information related to lower cost, therapeutically appropriate alternatives using NCPDP Formulary + Benefits 1.0. (not required for 2011 if (d) met).
(d) Provide information on formulary or tiered formulary medications, patient eligibility, and authorization requirements received electronically from the patient’s drug plan (if available) using one of 3 standards.
43

eRx – Penalties
2012 – 1% reduction 2013 – 1.5% reduction 2014 – 2% reduction Individual EPs must :
report at least 10 electronic prescriptions to avoid penalty for 2012. Reporting period 1/1/11 – 6/30/11 (processed by 7/31);
report at least 25 electronic prescriptions to avoid penalty for 2013. Reporting period 1/1/11 – 12/31/11.
Groups must meet 2011 criteria for incentive payment between 1/11/11-6/30/11 (processed by 7/31) to avoid penalty
Must report through claims to avoid penalty (no registry or EHR)
44
eRx – Penalties
Penalty Exceptions: Individual EPs
EP who is not a physician, NP or PA as of June 30, 2011 EP who does not have 100 cases in applicable codes EP who does not meet 10% code floor to be eligible for incentive Hardship Exception:
Hardship Exception Codes: Use G8642 (practice in rural area without high speed internet access) or G8643 (practice in area without available pharmacies for e-prescribing).
Groups Third and fourth exceptions above also apply to groups
45

EHR and eRx: Integration & Penalties
If an EP gets an EHR incentive in 2011 and 2012, can still get eRx 2012 penalty E-prescribing measures are different E-prescribing system requirements are different
If an EP gets an eRx incentive in 2011 and 2012, can still get eRx penalty Reporting periods for incentive and penalty are different For individual EPs (not groups) reporting requirements are
different.
Significant opposition to using 1/1/11 – 6/30/11 as reporting period for 2012 eRx penalty & lack of coordination with EHR e-prescribing measures.
46

PQRS: Physician Quality Review System PQRI established by 2006 Tax Relief and Health Care Act
(TRHCA) (P.L. 109-432).
PQRI further modified as a result of the Medicare, Medicaid, and SCHIP Extension Act of 2007 (MMSEA) (Pub. L. 110-275) and the Medicare Improvements for Patients and Providers Act of 2008 (MIPPA) (Pub. L. 110-275).
In 2011, the program name was changed to Physician Quality
Reporting System (Physician Quality Reporting).
47

Background - PQRS
Individual eligible professionals do not need to sign-up or pre-register in order to participate in claims reporting but may need to register for use of registry, group practice reporting.
The PQRS requirements and measure specifications may be different from the PQRI requirements and measure specifications for a prior year.
Eligible professionals are responsible for ensuring that they are using the PQRS measurements for the correct program year.
48

2011 PQRS Requirements
1% Incentive Payment Reporting Mechanisms for Individual Eligible Professionals
Claims Qualified Registry Qualified EHR
Reporting Periods for Individual Eligible Professionals 12 months - Jan. 1, 2011 - Dec. 31, 2011 6 months - Jul. 1, 2011 - Dec. 31, 2011 (claims and registry-based
reporting only)
Individual eligible professionals may report individual Physician Quality Reporting System measures or measures groups
49
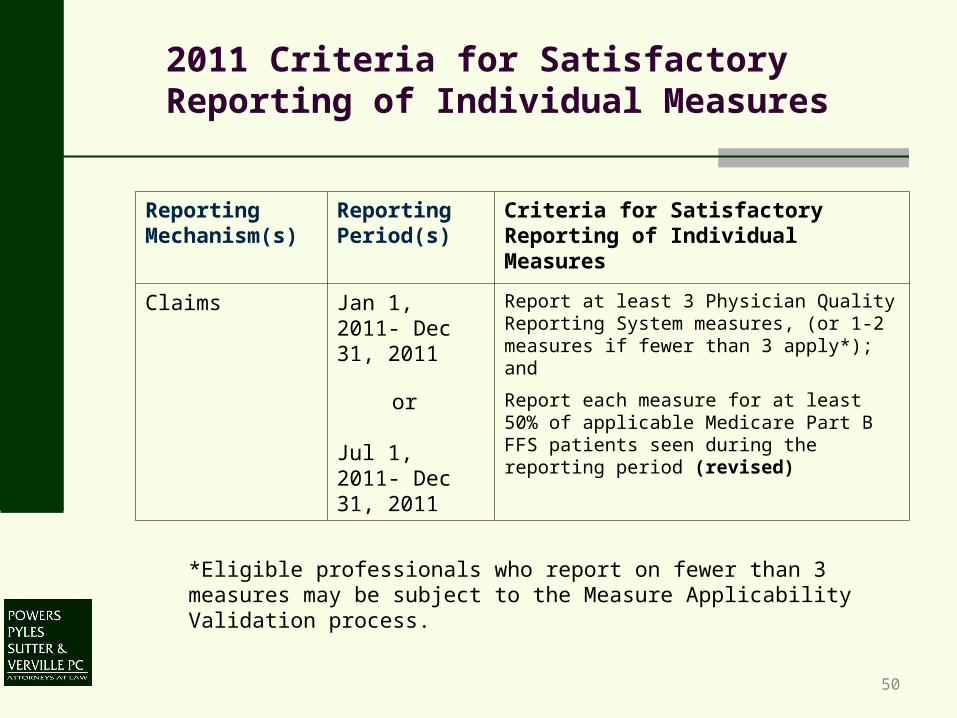
2011 Criteria for Satisfactory Reporting of Individual Measures
*Eligible professionals who report on fewer than 3 measures may be subject to the Measure Applicability Validation process.
50
Reporting Mechanism(s)
Reporting Period(s)
Criteria for Satisfactory Reporting of Individual Measures
Claims Jan 1, 2011- Dec 31, 2011
Report at least 3 Physician Quality Reporting System measures, (or 1-2 measures if fewer than 3 apply*); and
or
Jul 1, 2011- Dec 31, 2011
Report each measure for at least 50% of applicable Medicare Part B FFS patients seen during the reporting period (revised)

2011 Criteria for Satisfactory Reporting Individual Measures (cont)
*Measures with a 0% performance rate will not be counted (new) 51
Reporting Mechanism(s)
Reporting Period(s)
Criteria for Satisfactory Reporting of Individual Measures
Registry Jan 1, 2011 - Dec 31, 2011
Report at least 3 Physician Quality Reporting System measures*; and
or Jul 1, 2011- Dec 31, 2011
Report each measure for at least 80% of applicable Medicare Part B FFS patients seen during the reporting period
EHR Jan 1, 2011- Dec 31, 2011
Report at least 3 Physician Quality Reporting System EHR measures*; and
Report each measure for at least 80% of applicable Medicare Part B FFS patients seen during the reporting period

PQRS Group practice reporting mechanisms
GPRO I—for self-nominated groups of 200 or more.
GPRO II– Pilot for approx. 500 self-nominated groups with less than
200 eligible professionals
Reporting Mechanism - claims (or, if the only measures
groups that apply to the practice are the registry-only
measures groups, registry)
Reporting Period- Jan 1, 2011- Dec 31, 2011
52

MOC Incentive Program
Beginning in 2011, additional incentive of 0.5% is available by meeting Maintenance of Certification requirements:
To earn MOC incentive, professional must: Submit PQRS data for a 12-month reporting period
AND More frequently than is required to qualify for or maintain
board certification: Participate in a Maintenance of Certification Program
and Successfully complete a qualified Maintenance of
Certification Program practice assessment.
53
Informal Review Process
54
The Affordable Care Act requires CMS to establish an informal process for eligible professionals to seek a review of the determination that an eligible professional did not satisfactorily submit data on Physician Quality Reporting System measures.
Requests for an informal review must be emailed to the QualityNet Help Desk at [email protected] within 90 days of the release of the professional’s 2011 feedback report.
A written response will be provided within 60 days of receiving the original request.

Public Reporting
MIPPA requires CMS to post on a website the names of eligible professionals and group practices who have satisfactorily reported under the Physician Quality Reporting System
This information, for 2011, will be posted on the Physician Compare Website (the Affordable Care Act requires CMS to develop this website by January 1, 2011) after the 2011 incentive payments are made in 2012.
55

Other ACA Provisions
Physician Quality Reporting System incentives through 2014
1% for 2011
0.5% for 2012- 2014
Physician Quality Reporting System negative payment adjustment
beginning 2015
1.5%downward payment adjustment for 2015
2% downward payment adjustment for 2016 and each subsequent
year
Develop plan to integrate reporting under the Physician Quality Reporting
System and reporting under EHR Incentive Program by 1/1/2012
Timely feedback
56

2010 PQRS Submission Deadlines
January 2, 2011 - January 31, 2011 – Test submission period for registries and eligible professionals utilizing the EHR-based reporting mechanism for the 2010 Physician Quality Reporting System and/or eRx Incentive Program
February 1, 2011 - March 31, 2011 – Data submission period for registries, GPROs and eligible professionals utilizing the EHR-based reporting mechanism for the 2010 Physician Quality Reporting System and/or eRx Incentive Program
February 28, 2011 – Date by which 2010 claims must be processed to be included in 2010 Physician Quality Reporting System and eRx Incentive Program analyses
57

PQRS Submission Deadlines
January 31, 2011 – Registry self-nomination deadline for the 2011 PQRS and eRx Incentive Program
January 31, 2011 – EHR vendor self-nomination deadline for the 2012 PQRS and eRx Incentive Program
January 31, 2011 – GPRO I and II self-nomination deadline for the 2011 PQRS and e-Rx Incentive Program
January 31, 2011 – MOC self-nomination deadline for the 2011 PQRS.
58

Powers Pyles Sutter & Verville PCContact Information
Rebecca Burke, Of Counsel
Powers Pyles Sutter & Verville PC
1501 M Street, NW
7th Floor
Washington, DC 20005
Phone: 202.872.6751
Fax: 202.785.1756
Email: [email protected]
59

Powers Pyles Sutter & Verville PCContact Information
Barbara Straub Williams, Principal
Powers Pyles Sutter & Verville PC
1501 M Street, NW
7th Floor
Washington, DC 20005
Phone: 202.872.6733
Fax: 202.785.1756
Email: [email protected]
60
Powers Pyles Sutter & Verville PCContact Information
Diane Millman, Principal
Powers Pyles Sutter & Verville PC
1501 M Street, NW
7th Floor
Washington, DC 20005
Phone: 202.872.6725
Fax: 202.785.1756
Email: [email protected]
61