Carpal Tunnel Syndrome
25
Carpal Tunnel Syndrome By: Amin Yousefelahi Rafsanjan Medical School
-
Upload
ayousefelahi -
Category
Health & Medicine
-
view
150 -
download
2
Transcript of Carpal Tunnel Syndrome

Carpal Tunnel
SyndromeBy: Amin
Yousefelahi Rafsanjan Medical School

CTS Definition

Carpal Tunnel Anatomy
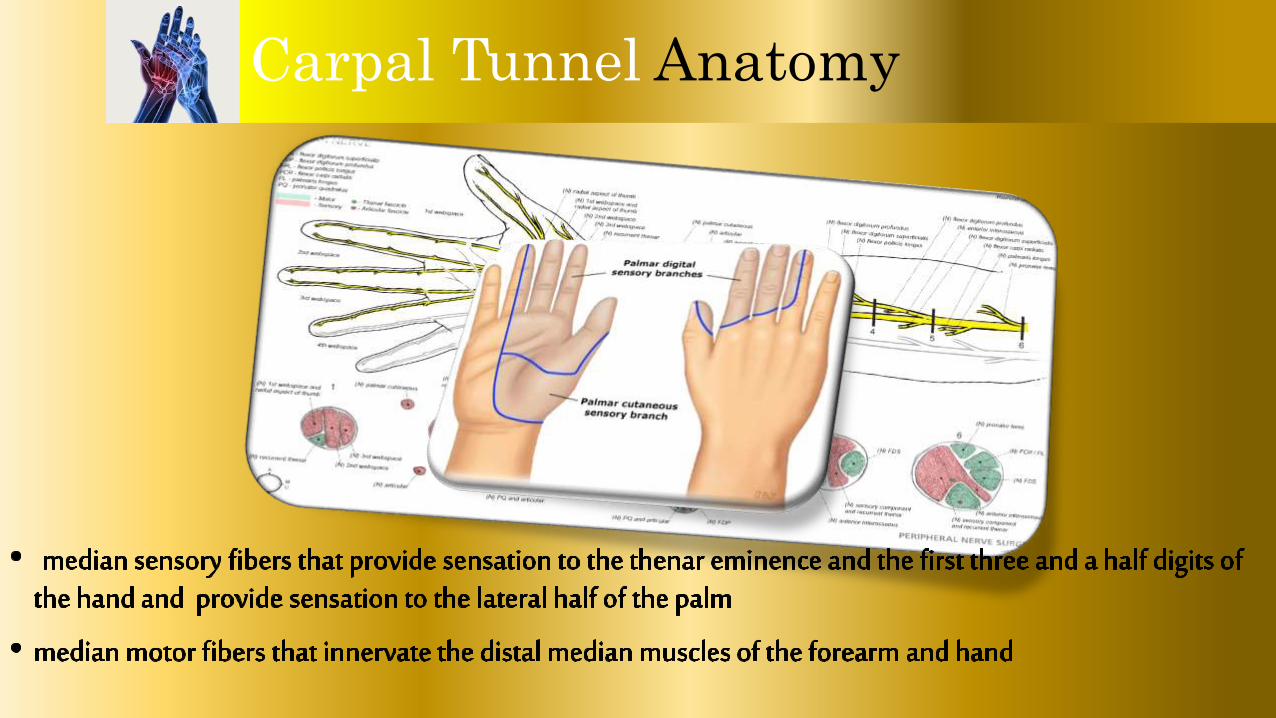
Carpal Tunnel Anatomy

CTS Epidemiology
Carpal tunnel syndrome is a common disorder. The estimated prevalence of CTS in the general population is 1 to 5 percent. CTS is more frequent in women (female to male ratio for CTS prevalence was approximately 3 to 1). The prevalence of CTS appears to be highest in obese women, and lowest in thin and normal-sized men. The frequency of CTS may be higher in the industrial setting than in the general population, as illustrated by prevalence estimates of 5 to 15 percent in the workplace.

Gout
Hypothyroidism
Diabetes
RA
Wrist Sprain
Pregnancy

CTS Etiology

CTS Etiology

CTS Pathophysiology

CTS Pathophysiology

CTS CLINICAL FEATURES
• The hallmark is pain or paresthesia (numbness and tingling) in a distribution median nerve, with involvement of the first three digits and the radial half of the fourth digit.
• The symptoms are typically worse at night and characteristically awaken patients from sleep.
• Bilateral CTS is common. • The symptoms of CTS have a wide range of variability.
• The pain and paresthesia may be localized to the wrist• involve the entire hand • radiate proximally to as high as the shoulder.
CTS CLINICAL FEATURES
• CTS symptoms are often provoked by activities that involve flexing or extending the wrist or raising the arms.
• In more severe CTS, motor involvement leads to complaints of weakness or clumsiness when using the hands. Clinical signs may include weakness of thumb abduction and opposition, and atrophy of the thenareminence.


CTS Diagnosis
• CTS is a clinical diagnosis that is suspected when the characteristic symptoms and signs are present. The most important of these are nocturnal pain or paresthesia in the distribution of the median nerve.
• Provocative maneuvers 1) Phalen maneuver: the patient fully flexes the palms at the
wrist with the elbow in full flextion to provide extra pressure on the median nerve. Alternatively, the backs of the hands are placed against each other to provide hyperflexion of the wrist.
1) sensitivity of 68 percent and specificity of 73


CTS Diagnosis
• The Tinel test: involves firm percussion performed over the course of the median nerve just proximal to or on top of the carpal tunnel.• A positive Tinel sign may be less sensitive (50 percent)
than the Phalen sign, but has similar specificity (77 percent)
• The manual carpal compression test: is performed by applying pressure over the transverse carpal ligament, and it is deemed positive if paresthesia occur within 30 seconds of applying pressure. • sensitivity and specificity is 64 and 83 percent



CTS Diagnosis
• The hand elevation test: involves raising the hands above head for one minute. The test is positive if it reproduces the symptoms of CTS. • The sensitivity and specificity appear to be similar to or
slightly better than those reported for Tinel and Phalenmaneuvers.


CTS Diagnosis
• Electromyography• Nerve conduction studies (NCS) and
electromyography (EMG) are useful to support the diagnosis of CTS and to rule out other abnormalities. The electrodiagnosis of CTS rests upon the demonstration of impaired median nerve conduction across the carpal tunnel in the context of normal conduction elsewhere. EMG is used to exclude other conditions such as polyneuropathy, plexopathy, and radiculopathy.

CTS Diagnosis
• Imaging studies: are not routinely employed in the
evaluation for possible CTS• Ultrasonography: have shown that patients with CTS have
significantly increased cross-sectional area of the median nerve • cutoffs of 8.5 to 10 mm 2 • The sensitivities ranged from 65 to 97 percent
specificities ranged from 73 to 98 percent.• MRI can detect abnormalities of the median nerve, flexor
tendons, vascular structures, and transverse carpal ligament in the region of the carpal tunnel.
CTS Treatment
• For patients with mild to moderate symptomatic CTS,• we recommend nocturnal wrist splinting as
preferred initial medical therapy because it is effective for short-term symptom relief. It is also safe and well-tolerated
• glucocorticoid injection(s), oral glucocorticoids• NSAIDs• Yoga & particular exercise • Ultrasound therapy

CTS Treatment
• For patients with moderate to severe CTS that is refractory to conservative measures • we suggest surgical decompression• Surgery appears to be more effective than splinting
or glucocorticoid injection for sustained CTS symptom relief