Caring for Persons with Diabetes Developed by: American Optometric Association Health Promotions...
82
Caring for Persons with Diabetes Developed by: American Optometric Association Health Promotions Committee
-
Upload
donna-tate -
Category
Documents
-
view
214 -
download
0
Transcript of Caring for Persons with Diabetes Developed by: American Optometric Association Health Promotions...

Caring for Persons with Diabetes Caring for Persons with Diabetes
Developed by:
American Optometric Association
Health Promotions Committee
Epidemiology of DiabetesEpidemiology of Diabetes
26 million Americans have diabetes– 90% have type 2 diabetes
79 million more Americans are at high risk for developing diabetes within ten years
1.8 million new cases diagnosed each year
Diabetes care accounts for 1 of every 6 health care dollars spent in the US

Epidemiology of Diabetes
The incidence of Type 2 diabetes in Americans < 20 years of age has grown 1100% since 1970
It is the fastest growing sub-population of diabetes by far
Diabetes is the 6th leading cause of death in the US
The leading cause of blindness in those < 74 yo
The leading cause of kidney failure
The leading cause of non-traumatic amputation

Diabetes MythsDiabetes Myths
Diabetes is caused by eating too much sugar
Not taking medications to control diabetes means the disease is less serious
Having type 2 diabetes is ‘better’ than having type 1 diabetes
Type 2 diabetes is not hereditary

A Look at the Numbers…A Look at the Numbers…

Diabetes Affects 28.5 Million AmericansDiabetes Affects 28.5 Million Americans
Of those:– 18.8 million diagnosed– 7 million not yet diagnosed– 215,000 are under 20 and mostly have
type I diabetes

Diabetes is…Diabetes is…
The LEADING cause of– Kidney failure– Non-traumatic lower limb amputations– New cases of blindness in adults
A MAJOR cause of – Heart disease– Stroke
The 7th leading cause of death in USA

Diabetes: A DefinitionDiabetes: A Definition
Failure of the pancreas to produce sufficient amounts of the hormone insulin
- or - Resistance of the body’s cells to the action of insulin

InsulinInsulin
Insulin allows cells throughout the body to absorb sugar (glucose) from the bloodstream
The source of glucose is mostly from carbohydrates in the foods we eat, but it can also be made by breaking down glucose stored in our muscles and liver
Insulin & Glucose are necessary for the brain, heart & kidneys to function

When Insulin isn’t Helping Glucose into the Cells…When Insulin isn’t Helping Glucose into the Cells…
Hyperglycemia occurs (blood sugar levels go up)
This causes damage to body tissues, especially blood vessels
This then leads to eye disease, kidney disease, nerve disease and heart disease
Diabetes-related eye disease predicts these other diseases

Diabetes Mellitus - ClassificationDiabetes Mellitus - Classification
Insulin Dependent (IDDM) Non-Insulin Dependent (NIDDM) Gestational (GDM)

Insulin-Dependent Diabetes Mellitus (IDDM)Insulin-Dependent Diabetes Mellitus (IDDM)
Results from destruction of islet cells in the pancreas More common in persons under 20 years of age Etiology both genetic and environmental Patients acutely symptomatic at the time of onset (“the polys”)

Non-Insulin Dependent Diabetes Mellitus (NIDDM)Non-Insulin Dependent Diabetes Mellitus (NIDDM)
Resistance of body tissues to the action of insulin:– Insulin resistance– Beta-cell failure
Usually occurs after age 40 Gradual onset of symptoms (half are unaware) Occurring more frequently in children Risk factors:
– Overweight & sedentary– Family history of diabetes– Ethnic origin

Gestational Diabetes Mellitus (GDM)Gestational Diabetes Mellitus (GDM)
Glucose intolerance of variable severity with onset or first recognition during pregnancy (2nd & 3rd trimester)
Complicates between 1% and 4% of pregnancies Limited to the term of the pregnancy Fetal outcome - Macrosomia GDM Moms are 50% more likely to develop NIDDM later Offspring are more likely to develop NIDDM during their lifetime

What Are the Symptoms?What Are the Symptoms?
All type 1 patients have symptoms
Many type 2 patients have few or no symptoms until serious complications develop
(e.g. a heart attack)
Symptoms of HypoglycemiaSymptoms of Hypoglycemia
Shaking Weakness
Sweating Fatigue
Fast heart beat Head Ache
Dizziness Irritable
Anxious
Hunger
Impaired vision

Symptoms of severe low blood sugarSymptoms of severe low blood sugar
Seizure
Loss of consciousness (coma)
Stroke
Death

Treatment of HypoglycemiaTreatment of Hypoglycemia
15 to 20 grams of carbohydrate that puts glucose into your bloodstream in about 5 minute will raise your blood sugar about 30 milligrams per deciliter (mg/dL) in about 15 to 20 minutes
Check your blood sugar level again 15 minutes Have person drink ½ glass of juice or regular soft drink,or 1 glass of milk
If symptoms don’t stop, call internist
Then eat a light snack (1/2 peanut butter or meat sandwich and ½ glass of milk)
Always have a rapid-acting carbohydrate in the office

Symptoms of HyperglycemiaSymptoms of Hyperglycemia
Extreme thirst Blurred vision
Frequent urination
Dry skin
Healing difficulties
Hunger
Drowsiness

Treatment of HyperglycemiaTreatment of Hyperglycemia
Have patient test blood sugar You can often lower your blood glucose level by exercising.
However, if your blood glucose is above 240 mg/dl, check your urine for ketones.
If you have ketones, do not exercise Exercising when ketones are present may make your blood
glucose level go even higher. Drink more water Change medication/ eating habits If >200mg/dl for several tests, for two days, or if extremely
elevated:
Call internist

Treatment Modes Treatment Modes
Pen injectors
Inhaled Insulin (currently off the market)
Insulin pumps
CGMs
Net based education
New medications
Insulin used more than in past

Non-Retinal Eye ComplicationsNon-Retinal Eye Complications
CORNEA - One of two clear tissues in the body
LENS - The other clear tissue– It is a very complex process to keep these tissues clear

Refractive errorRefractive error
In poorly controlled diabetes very high levels of glucose can cause the lens metabolism to shunt down a sorbital pathway
Sorbital buildup in the lens creates an osmotic swelling of the lens with resulting in refractive changes

Poor Pupil ResponsePoor Pupil Response
Before DilatingDrops
30 minutes AfterDilating Drops

Non-Retinal Eye ComplicationsNon-Retinal Eye Complications
IRIS - Colored part of eye - rubeosis irides - new vessel growth that can cause serious glaucoma complications and is usually associated with PDR– Typically is associated with advanced diabetic retinopathy;
not easy to identify
GLAUCOMA - Twice as likely in persons with diabetes and more likely to cause vision loss

Non-Retinal Eye ComplicationsNon-Retinal Eye Complications
OPTIC NERVE - Can sometimes swell (optic neuritis) - generally found in younger persons with diabetes and can lead to permanent vision loss
CRANIAL NEUROPATHIES - Ptosis (lid droop) and proptosis (eye bulge); occasional reversible diplopia; Bell’s Palsy
Eyelids - Skin related problems
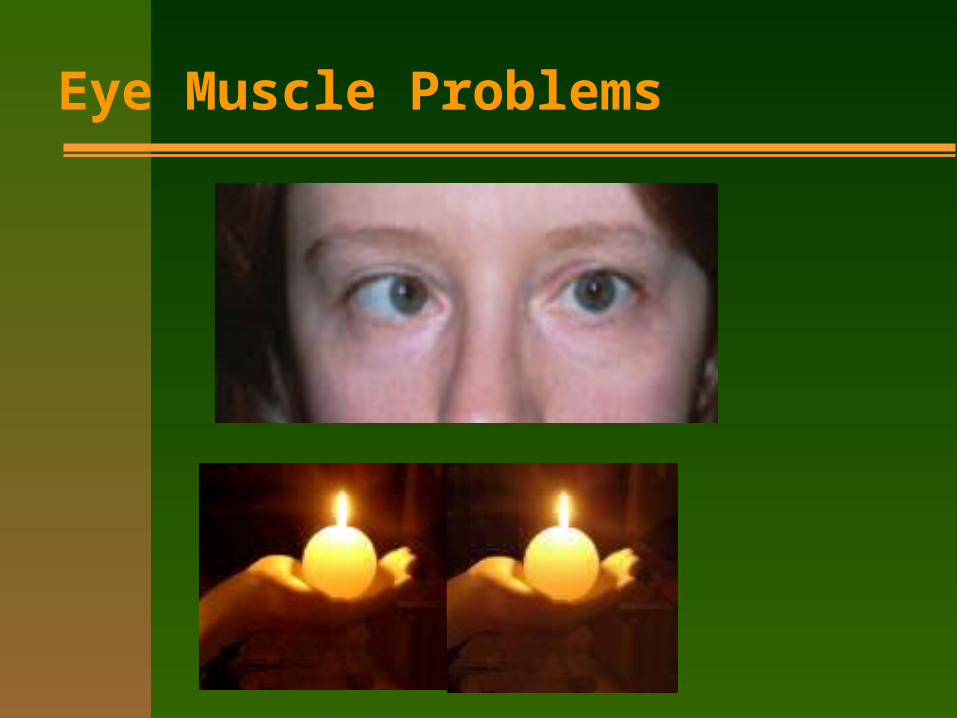
Eye Muscle Problems

Retinal Eye ComplicationsRetinal Eye Complications
BDR - Background Diabetic Retinopathy– Microaneurysms, leakage of intravascular fluid,
intraretinal hemorrhage, retinal ischemia
PPDR - Pre Proliferative Diabetic Retinopathy PDR - Proliferative Retinopathy
– New Vessel Growth
Remember – the retina is a very thin tissue

Mild NPDRMild NPDR
Standard Photo 1

Moderate NPDRModerate NPDR
Standard Photo 2A

Severe NPDRSevere NPDR
Standard Photo 2B

Very Severe NPDRVery Severe NPDR
Standard Photo 5

Proliferative Diabetic Retinopathy (PDR)Proliferative Diabetic Retinopathy (PDR)
Neovascularization of the Disc (NVD) Neovascularization Elsewhere (NVE) Pre-retinal Hemorrhage (PRH) Vitreous Hemorrhage (VH)

Non-High Risk Proliferative Diabetic RetinopathyNon-High Risk Proliferative Diabetic Retinopathy
Standard Photo 10A Standard Photo 6B

High Risk Proliferative Diabetic RetinopathyHigh Risk Proliferative Diabetic Retinopathy
Standard Photo 10C Standard Photo 7 Standard Photo 10 Standard photo 13

Laser Photocoagulation TreatmentLaser Photocoagulation Treatment

InjectionsInjections
Triamcinolone acetonide
Lucentis and Avastin

Diabetic Macular Edema(DME)Diabetic Macular Edema(DME)
The collection of intraretinal fluid in the macular area Disrupts retinal structure With or without lipid exudate or cystoid changes Focal or diffuse Can occur at any stage of retinopathy Only treated when it becomes “clinically significant” Follow-up every 3 to 4 months by a retinal specialist

Clinically Significant Macular Edema (CSME)Clinically Significant Macular Edema (CSME)
Patients referred for treatment immediately. CSME responsible for nearly HALF of all vision loss in diabetes!

Diabetic RetinopathyDiabetic Retinopathy
The most significant ocular complication of diabetes The leading cause of blindness - ages 20-74 All complications of diabetes have a slow progression
in the beginning– leads to patient non-compliance

Type I DiabetesType I Diabetes
Past thinking: Usually free of retinopathy for first ten years after diagnosis
Present Thinking: 20% have retinopathy at one year; 67% have retinopathy at five years
95% have retinopathy after 15 years or more

Type II DiabetesType II Diabetes
May have retinopathy at diagnosis
30% have retinopathy within 5 years
80% have retinopathy within 15 years

Severity of Diabetic RetinopathySeverity of Diabetic Retinopathy
Depends on– Disease Duration - always ask how long– High Blood Pressure - very serious– High Glycosolated Hemoglobin– Smoking = major risk
Example:– Patient A.J. (HTN, A1c = 10, smoker): diabetes
less than 20 years; vision: 20/800– Patient D.D. (good control of all risk factors):
diabetes greater than 25 years, vision: 20/15

Optometric Management of Persons with DiabetesOptometric Management of Persons with Diabetes
Frequency of Exams– After Diagnosis: Every Year Dilated Pupil Exam
(Should be pre-scheduled)– After First Diagnosis of Diabetic Eye Changes:
Every year or six months– At Pre-Proliferative Stage
Should be referred to retinal specialist Less than 50% of persons with diabetes get dilated
eye exams yearly– You must preschedule!!

Treatment OptionsTreatment Options
PREVENTION - 75% of all diabetic retinopathy could be eliminated with proper control of the disease– Medication - Drs. do adequate job– Exercise - Drs. do poor job– Diet - Drs. do poor job
One of the greatest causes of death and disability in the USA is overeating and a diet heavy in fats, meats, and sugars

Treatment OptionsTreatment Options
Argon Laser Photocoagulation Pan Retinal Photocoagulation
– Laser kills peripheral retinal tissue– feedback to brain says - “this is dead tissue, no
need to grow vessels here” Victrectomy
– Remove bloody scarred vitreous and replace with saline
– Injections
Laser PhotocoagulationLaser Photocoagulation
Reduces visual loss by 50% Goals:
– Prevent further neovascularization– Reduce risk of vitreous hemorrhage and/or reduce
traction retinal detachment Side Effects (lessened now with injections)
– Constriction of peripheral vision– Decreased night vision– Loss of acuity

Treatment OptionsTreatment Options
Early Diagnosis is the Key– ALWAYS preschedule your patients with diabetes
for annual (and other) visits Education/Motivation is Essential
– 1-800-DIABETES/diabetes.org– Diet Consult– Exercise Consult– Diabetes Education Classes now covered by
major medical and Medicare

Why Does Diabetes Kill So Many Americans?Why Does Diabetes Kill So Many Americans?
Doctors do not seem to understand the disease
Patients do not seem to understand the disease
The public does not seem to understand the disease
Not many people care– primarily affects older people, or under/un-insured

Obesity by the numbersObesity by the numbers
Complications from obesity kill more Americans than smoking – and smoking kills 1000 Americans per day!!!!
Strokes, hypertension, cardiovascular disease, and diabetes can all cause blindness, as well as other disabilities and death


Supersized SuicideSupersized Suicide
The food industry produces 3800 calories per day for every person in the USA; up from 3300 from the 70s.
Adult females need 2200; adult males 2500 The food industry spends 10 billion dollars
yearly in direct advertising and another 20 billion in indirect advertising (school scoreboards etc.)
Two words: Free Refills!! (and what ever happened to a ten ounce bottle of soda?)
Supersized SuicideSupersized Suicide
The campaign for fruits and vegetables spends about 2 million per year on public education
The food industry pushes processed foods (potatoes are cheap; potato chips are not)
Portion sizes have increased dramatically

Kids in the line of fireKids in the line of fire
70% of obese children will become obese adults
Most breakfast cereals and kid drinks should be labeled as candy – Froot Loops has no fruit and no fiber
Soda Pop parties; food as a reward; candy and bake sale fundraisers; terrible cafeteria food; less exercise, more video games, and more computer time

A paradigm shift needs to occurA paradigm shift needs to occur
Insurance will pay for special shoes, medical procedures (such as amputation), however, dietary counseling needs to be covered as well.
Nutrition training is important for doctors, additionally it is important to discuss weight even when the patient’s ‘vital signs’ seem OK
Obesity is not a cosmetic issue, it is a medical issue

Research on obesity is obsceneResearch on obesity is obscene
NIH = 226 million for obesity research
NIH = 2 billion for cardiovascular research
If we cured the obesity, we wouldn’t have near the cardiovascular disease!

Are we just overeating?Are we just overeating?
We are exercising less Our jobs require less manual labor We have larger portions shoved at us We have advertising bombarding us We are eating out more For easing stress, if we don’t do drugs, we do
food Even as adults, food is a reward

Is this just a USA thing?Is this just a USA thing?
Well, no, but look at this……….

Great Marketing TricksGreat Marketing Tricks
Millions of dollars are spent encouraging us to eat more highly processed foods

What can WE do??What can WE do??
Share portions Special order Take home boxes or just leave it on the plate Don’t be blinded by the advertising Eat less processed foods Reduce meats, fats, and high sugar foods Forget about special ‘no protein, all protein, no white
food, blah, blah, blah diets and simply change your eating behavior
Exercise more
Self Monitoring of Blood GlucoseSelf Monitoring of Blood Glucose
One Touch Ping and Animas Pump

SMBGSMBG
Self-monitoring of blood glucose
All patients should perform SMBG– Fasting and after meals (ideally, but rarely done,
and if so usually on Type I persons)– 50% of people with diabetes do NO SMBG
Normal blood glucose is between 70-110– Up to 150 after a meal– Less than 90 in the morning after fasting

Continuous Glucose MonitorsContinuous Glucose Monitors
Inserted under the skin Replaced generally weekly Shows trends Still must be calibrated with finger sticks
twice daily Alarm settings can signal a call to action Some will “talk” to an insulin pump but not
make automatic changes
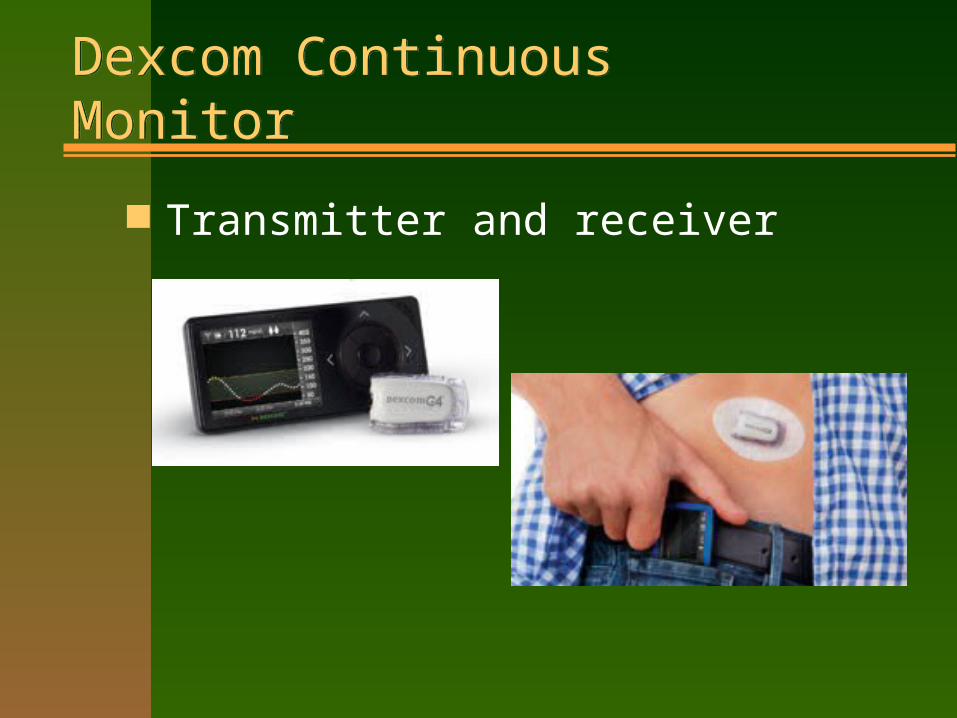
Dexcom Continuous MonitorDexcom Continuous Monitor
Transmitter and receiver
What Does Diabetes Research Tell Us?What Does Diabetes Research Tell Us?
Keeping blood pressure levels below 130/80 lowers the risk of all diabetes complications
Getting an annual dilated eye exam cuts the risk of going blind from diabetes by up to 95% by allowing for early detection of eye complications

Hemoglobin A1c (HbA1c)Hemoglobin A1c (HbA1c)
HbA1c measures the AVERAGE blood sugar level over the preceding 3 months
HbA1c predicts those people most likely to go blind and/or die from diabetes
“Normal” HbA1c is around 5%
The average patient with diabetes has an HbA1c of 8.5%
For most people with diabetes, the HbA1c goal is <6.5%– Exceptions are kids and those with established CVD
What Does Diabetes Research Tell Us?What Does Diabetes Research Tell Us?
Keeping blood sugar levels as close to normal as possible lowers the risk of all diabetes complications– Diet (especially portion control)– Exercise (lowers blood sugar & improves
insulin resistance)– Medication
Patients & Doctors need to know their numbers and what they mean…

Preventing DiabetesPreventing Diabetes
Walking 30 minutes each day, five days each week, reduces the risk of developing diabetes by up to 60%
Sleeping 7-8 hours and eating more vegetables also lowers diabetes risk
If you don’t get diabetes, you can’t go blind, lose a foot, or die from diabetes!

Who Should Educate?Who Should Educate?
Each and every health care provider, including para-optomteric staff
The best way to change unhealthy behaviors is by building a relationship with your patient
If the patient hears the same plan from every provider, they are more likely to follow through on proper care

Practical Tips for Health Care TeamPractical Tips for Health Care Team
Tell the doctor you’re interested in helping provide excellent diabetes care
Learn all you can about diabetes
Make sure you’ve got orange juice or sugared soda set aside for patients
Develop a plan to measure blood pressure & ask about HbA1c for every patient with diabetes

Practical Tips for Health Care TeamPractical Tips for Health Care Team
Ask about SMBG
Ask about physical activity
Ask about common diabetes medicines– Insulin and/or pills for blood sugar– Blood pressure & cholesterol medicines– Aspirin therapy

Practical Tips for Health Care TeamPractical Tips for Health Care Team
Ask who treats their diabetes & how often they’re seen
Ask if they would like more information on diabetes and preventing complications
Help the doctor to make sure that every patient with diabetes is dilated annually
Remember that diabetes is not who they are, but a condition they have

What the DCCT Told UsWhat the DCCT Told Us
Prevention IS the cure– 76% less retinopathy– 54% less kidney disease– 60% less neuropathy– 50% less amputations
These results are over ten years old and doctors and patients still do not understand

Key PointsKey Points
Diabetes is a serious disease Diabetes has become an epidemic Treating diabetes complications like eye disease and
heart disease is a LOT more expensive than preventing those complications
Eye doctors and their assistants are on the ‘front line’ in the battle against diabetes, and can make a real difference

Optometric Role in Managing Patients with DiabetesOptometric Role in Managing Patients with Diabetes
Take a good case history to find the undiagnosed (6 million)– Episodes of blurred vision?– Polys – Increased thirst, hunger, urination, – FFFF – Fat, Forty, Female, Family History
Low Vision Training– provide low vision care for the partially sighted
Pre-schedule all persons with diabetes Refer to diabetes specialists
– Internists– Dieticians– Diabetes educators

Low vision examsLow vision exams
Low Vision exams
-evaluate functional vision and
-assesses individual needs (especially
important for those with vision loss due
to diabetes)

LCD video magnification LCD video magnification
Sharper image than TV Up to 50X magnification Takes up less space Around 2200.00 Enables patient to read or
look at pictures And write checks and
letters

Lighted magnifiers reduce glare and provide contrast
Lighted magnifiers reduce glare and provide contrast

Spectacle mounted telescopes can improve distance vision dramaticallySpectacle mounted telescopes can improve distance vision dramatically

State Department of RehabilitationState Department of Rehabilitation
Can Give a Workshop on Services They Provide
Can Be A Great Referral Service for Low Vision Patients

Summary:Summary:
Very Serious Disease Early Detection Essential Education Essential Good Control = Less Complications Intervention/Treatments = Less Blindness Low Vision Services May Help to
Rehabilitate Patients Who Have Lost Vision

THANK YOU!THANK YOU!
For More Info:
American Optometric Association: aoa.org
American Diabetes Association: diabetes.org
National Institutes of Health: ndep.nih.gov


















