Caring for children with cerebral malaria: insights … PROOF Please cite this article in press as:...
5
UNCORRECTED PROOF TRSTMH 1058 1—5 Please cite this article in press as: Taylor TE. Caring for children with cerebral malaria: insights gleaned from 20 years on a research ward in Malawi. Trans R Soc Trop Med Hyg (2008), doi:10.1016/j.trstmh.2008.10.049 ARTICLE IN PRESS +Model TRSTMH 1058 1—5 Transactions of the Royal Society of Tropical Medicine and Hygiene (2008) xxx, xxx—xxx 1 available at www.sciencedirect.com journal homepage: www.elsevierhealth.com/journals/trst Caring for children with cerebral malaria: insights gleaned from 20 years on a research ward in Malawi 2 3 Terrie E. Taylor ∗ 4 College of Osteopathic Medicine, Department of Internal Medicine, Michigan State University, B309-B West Fee Hall, E. Lansing, MI 48824, USA 5 6 Received 3 October 2008; accepted 27 October 2008 7 KEYWORDS Cerebral malaria; Clinical management; Blantyre Coma Score; Malarial retinopathy; Paediatric; Africa Summary Clinicians treating patients with severe malaria in endemic areas confront a variety of challenges inherent to resource-poor settings, but it is possible to provide excellent care. The basic requirements, in addition to a thorough clinical examination of the patient, include assess- ing parasitaemia; determining anaemia (via haematocrit or haemoglobin); estimating blood glucose and lactate concentrations; establishing and maintaining i.v. access; measuring oxy- gen saturation and providing supplemental oxygen when necessary; grouping, cross-matching and transfusing blood. This paper provides practical information on determining the Blantyre Coma Score, collecting cerebrospinal fluid and measuring the opening pressure, and adminis- tering controlled volumes of i.v. fluids. Included is a narrative protocol describing the approach to patients with cerebral malaria used on the research ward at the Queen Elizabeth Central Hospital in Blantyre, Malawi. 8 9 10 11 12 13 14 15 16 17 18 © 2008 Published by Elsevier Ltd on behalf of Royal Society of Tropical Medicine and Hygiene. 19 1. Introduction 20 Clinicians treating patients with severe malaria in endemic 21 areas confront a variety of challenges inherent to 22 resource-poor settings: laboratory capacities are limited, so 23 assessment of electrolytes, liver function and renal function 24 is rare; clinical supplies (cannulas, i.v. tubing, burettes) may 25 not always be in stock; and staffing levels are often low. 26 Nevertheless, it is possible to provide excellent care. The 27 discussion that follows provides practical information for 28 clinicians in malaria-endemic areas who are caring for chil- 29 ∗ Tel.: +1 517 353 8975; fax: +1 517 432 1062. E-mail address: [email protected] dren with cerebral malaria. It does not include a discussion 30 of specific antimalarial drug treatment protocols. 31 2. Guide to techniques 32 2.1. Determining depth of coma 33 The Blantyre Coma Score 1 is derived from the Glasgow Coma 34 Score and was developed because several key indicators on 35 the Glasgow Coma Score, e.g. eye opening in response to 36 pain and verbal responses to pain, were inappropriate in 37 the context of paediatric malaria. 38 The Blantyre Coma Score is one of the best clinical indi- 39 cators of the severity of cerebral malaria in children; fully 40 conscious children would score 5, while children who do 41 0035-9203/$ — see front matter © 2008 Published by Elsevier Ltd on behalf of Royal Society of Tropical Medicine and Hygiene. doi:10.1016/j.trstmh.2008.10.049
-
Upload
nguyenkien -
Category
Documents
-
view
218 -
download
1
Transcript of Caring for children with cerebral malaria: insights … PROOF Please cite this article in press as:...

1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
D P
RO
OF
ARTICLE IN PRESS+ModelTRSTMH 1058 1—5
Transactions of the Royal Society of Tropical Medicine and Hygiene (2008) xxx, xxx—xxx
avai lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ierhea l th .com/ journa ls / t rs t
Caring for children with cerebral malaria: insightsgleaned from 20 years on a research ward in Malawi
Terrie E. Taylor ∗
College of Osteopathic Medicine, Department of Internal Medicine, Michigan State University, B309-B West Fee Hall,E. Lansing, MI 48824, USA
Received 3 October 2008; accepted 27 October 2008
KEYWORDSCerebral malaria;Clinical management;Blantyre Coma Score;Malarial retinopathy;Paediatric;
Summary Clinicians treating patients with severe malaria in endemic areas confront a varietyof challenges inherent to resource-poor settings, but it is possible to provide excellent care. Thebasic requirements, in addition to a thorough clinical examination of the patient, include assess-ing parasitaemia; determining anaemia (via haematocrit or haemoglobin); estimating bloodglucose and lactate concentrations; establishing and maintaining i.v. access; measuring oxy-gen saturation and providing supplemental oxygen when necessary; grouping, cross-matching
TEAfrica and transfusing blood. This paper provides practical information on determining the BlantyreComa Score, collecting cerebrospinal fluid and measuring the opening pressure, and adminis-tering controlled volumes of i.v. fluids. Included is a narrative protocol describing the approachto patients with cerebral malaria used on the research ward at the Queen Elizabeth CentralHospital in Blantyre, Malawi.
r Ltd
d 30
o 31
2 32
2 33
RR
EC© 2008 Published by Elsevie
1. Introduction
Clinicians treating patients with severe malaria in endemicareas confront a variety of challenges inherent toresource-poor settings: laboratory capacities are limited, soassessment of electrolytes, liver function and renal functionis rare; clinical supplies (cannulas, i.v. tubing, burettes) may
UN
CO
Please cite this article in press as: Taylor TE. Caring for childrea research ward in Malawi. Trans R Soc Trop Med Hyg (2008), d
not always be in stock; and staffing levels are often low.Nevertheless, it is possible to provide excellent care. Thediscussion that follows provides practical information forclinicians in malaria-endemic areas who are caring for chil-
∗ Tel.: +1 517 353 8975; fax: +1 517 432 1062.E-mail address: [email protected]
T 34
S 35
t 36
pt
cc
0035-9203/$ — see front matter © 2008 Published by Elsevier Ltd on behadoi:10.1016/j.trstmh.2008.10.049
on behalf of Royal Society of Tropical Medicine and Hygiene.
ren with cerebral malaria. It does not include a discussionf specific antimalarial drug treatment protocols.
. Guide to techniques
.1. Determining depth of coma
he Blantyre Coma Score1 is derived from the Glasgow Comacore and was developed because several key indicators onhe Glasgow Coma Score, e.g. eye opening in response to
TRSTMH 1058 1—5n with cerebral malaria: insights gleaned from 20 years onoi:10.1016/j.trstmh.2008.10.049
ain and verbal responses to pain, were inappropriate in 37
he context of paediatric malaria. 38
The Blantyre Coma Score is one of the best clinical indi- 39
ators of the severity of cerebral malaria in children; fully 40
onscious children would score 5, while children who do 41
lf of Royal Society of Tropical Medicine and Hygiene.

INT
2
n42
i43
44
b45
t46
147
(48
249
T50
o51
e52
053
s54
t55
256
i57
258
I59
p60
a61
a62
i63
264
T65
t66
a67
s 68
l 69
v 70
p 71
t 72
a 73
74
C 75
m 76
s 77
c 78
2 79
B 80
a 81
c 82
83
m 84
i 85
a 86
b 87
c 88
t 89
Ftntita
ARTICLE+ModelRSTMH 1058 1—5
ot respond at all to painful stimuli score 0. Mortality ratesncrease significantly when the score is 2 or less.1
The Blantyre Coma Score can be assessed quickly at theedside, is reproducible2 and requires no equipment or elec-ricity. There are three elements: motor (possible scores 0,, 2), verbal (possible scores 0, 1, 2), and eye movementspossible scores 0, 1).
.1.1. Blantyre Coma Score: motor responsehe first step is to apply firm pressure to a fingernail bed andbserve the response. If there is no response or if the patientxtends his/her arm, the score for the motor response is. If the patient withdraws, pressure is then applied to theternum or the supraorbital ridge. If the patient can localizehe painful stimulus by actually moving it away s/he scores; if s/he can only withdraw, the score for the motor elements 1.
.1.2. Blantyre Coma Score: verbal responset is important to listen to the verbal response while applyingainful stimuli. No response at all is scored as 0. A moan orn abnormal cry receives a score of 1, and a normal cry orppropriate speech (in children who are old enough to talk)s scored as 2.
UN
CO
RR
EC
TED
Please cite this article in press as: Taylor TE. Caring for childrea research ward in Malawi. Trans R Soc Trop Med Hyg (2008), d
.1.3. Blantyre Coma Score: eye movementshis can only be assessed in patients who are alert enougho open their eyes. Shine a bright light into the eyes or usevisual threat to determine whether or not the patient can
iatnd
igure 1 Measuring the opening pressure using a ‘flexible manoechnique is the connector that links the No. 1 (1.5′′, 21-gauge) neeeedle (A). The connector has a membrane on one end to receiveo screw onto the No. 1 needle. First the needle is placed in the sps established the Luer lock is attached to the needle, the distal enubing is held vertically. When the CSF level equilibrates and fluctuand recorded (C).
OO
F
PRESST.E. Taylor
ee. If s/he is able to close his/her eyes to avoid a brightight, or to blink in response to threat, then provide a movingisual target, e.g. the face of the examiner, to see if theatient is able to follow a moving object. Patients who canrack a moving object receive a score of 1; those who cannotre scored as 0.
The most common pitfall in determining the Blantyreoma Score is applying insufficient pressure; the recom-ended approach is to apply slowly increasing pressure,
topping when the patient responds or when the examineran apply no more pressure.
.2. Performing a lumbar puncture
acterial meningitis can masquerade as cerebral malaria,nd the only way to exclude meningitis is to examine theerebrospinal fluid (CSF).
Many clinical sites in sub-Saharan Africa use a simplifiedethod for lumbar punctures (LP) (Figure 1). The patient
s placed in the left or right lateral recumbent position,nd the interspace between L3 and L4 is identified (directlyeneath the iliac crest). The skin is cleaned thoroughly withotton swabs soaked in alcohol, and the sheath surroundinghe spinal cord is pierced by a 21 gauge, 1.5′′ needle. A flex-
PR
TRSTMH 1058 1—5n with cerebral malaria: insights gleaned from 20 years onoi:10.1016/j.trstmh.2008.10.049
ble manometer can be used to measure opening pressure, 90
nd then the CSF can be collected either from the manome- 91
er itself (lowered) or directly from the needle. Once the 92
eedle is removed the puncture site can be covered with a 93
ressing.
meter’, i.e. a scalp vein needle. The critical element in thisdle inserted into the spinal canal with the scalp vein/butterflythe scalp vein/butterfly needle and a Luer lock on the other,inal canal (B). Once the free flow of cerebrospinal fluid (CSF)d of the scalp vein/butterfly needle is uncapped and the longtes with respiration its height is measured with a tape measure

ED
OO
F
ARTICLE IN PRESS+ModelTRSTMH 1058 1—5
Children with cerebral malaria 3
Figure 2 Controlling the infusion rate of i.v. fluids can be accomplished without an infusion pump by intercalating a ‘drip chamber’,or burette, between the 1 l bag of i.v. fluids and the i.v. tubing which connects to the i.v. catheter in the patient (A). The calculated
andf can
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
p 124
m 125
b 126
l 127
p 128
t 129
t 130
s 131
3 132
p 133
O 134
c 135
r 136
g 137
o 138
l 139
m 140
f 141
142
i 143
t 144
B 145
p 146
n 147
NCOR
RE
CT
volume of fluids (generally 2 h worth) is placed in the chamberand, to assist the staff, the time at the halfway point (B). Stafrate. This approach can also be used for blood transfusions.
2.3. Examining the optic fundi
The standard clinical case definition of cerebral malaria (seebelow) is incorrect about 25% of the time according to anautopsy-based study.3 The most reliable clinical indicator ofthe cerebral sequestration of parasitized erythrocytes (thehistological hallmark of cerebral malaria) is the presenceof one or more elements of malarial retinopathy:4 white-centred haemorrhages, vessel changes and whitening.
Malarial retinopathy is best appreciated in eyes thathave been fully dilated with mydriatics, and examinedwith a direct ophthalmoscope (which provides magnifica-tion) and an indirect ophthalmoscope (which provides athree-dimensional perspective as well as a wider field ofview). These examinations are routine for trained ophthal-mologists, but non-ophthalmologist clinicians can learn torecognize these features too, and the technique has provenuseful in identifying patients with true cerebral malaria.
2.4. Administering intravenous fluids andmedications
Patients with severe malaria generally require i.v. fluid sup-port until they are able to swallow reliably. Most hospitalsin malaria-endemic areas do not have infusion pumps andmost have only 1 l bags of i.v. fluids available. It is possi-ble to work out the number of drops/minute that would be
U
Please cite this article in press as: Taylor TE. Caring for childrea research ward in Malawi. Trans R Soc Trop Med Hyg (2008), d
required to deliver the desired amount of fluid each hourfrom a 1 l bag, but it is nearly impossible to monitor fluiddelivery as there are no volume indicators on a 1 l bag of i.v.fluid, and there is a real risk of delivering too much fluid toa patient.
m
sra
PRtape is affixed to the side noting the start time, the end time
tell, at a glance, if the fluids are infusing at the appropriate
The research ward at the Queen Elizabeth Central Hos-ital in Blantyre, Malawi has developed a simple method ofonitoring i.v. fluid administration involving intercalating aurette, or ‘drip chamber’, between the patient and the 1bag. A known amount of i.v. fluid (generally 2 h worth) islaced in the chamber, the chamber is labelled with tape,he drip rate is set, and then any member of the clinicaleam can tell, at a glance, if the infusion is proceeding ascheduled (Figure 2).
. The Blantyre approach to managingaediatric patients with cerebral malaria
n admission, patients should be examined for alternativeauses of fever and coma. Note temperature, pulse rate andhythm, respiratory rate and rhythm, blood pressure, oxy-en saturation, Blantyre Coma Score, capillary refill, degreef pallor, pupillary response to light, blood glucose, bloodactate, haemoglobin/haematocrit and parasitaemia. Instilydriatics and examine the optic fundi when both eyes are
ully dilated.Intravenous access should be established immediately
n patients who are hypoglycaemic. Administer 50% dex-rose (1 ml/kg) and recheck the blood glucose after 15 min.oluses of 50% dextrose (1 ml/kg) are repeated until theatient is normoglycaemic. If more than two doses areeeded, consider increasing the glucose concentration in the
TRSTMH 1058 1—5n with cerebral malaria: insights gleaned from 20 years onoi:10.1016/j.trstmh.2008.10.049
aintenance i.v. fluids. 148
If the patient is convulsing on admission, attention 149
hould be focused on stopping the convulsions. This may 150
equire the use of antipyretics and i.v. glucose as well as 151
nticonvulsants. 152
UN
CO
RR
EC
TED
PR
OO
F
TRSTMH 1058 1—5Please cite this article in press as: Taylor TE. Caring for children with cerebral malaria: insights gleaned from 20 years ona research ward in Malawi. Trans R Soc Trop Med Hyg (2008), doi:10.1016/j.trstmh.2008.10.049
ARTICLE IN PRESS+ModelTRSTMH 1058 1—5
4 T.E. Taylor
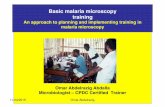
Figure 3 This flowchart contains most of the information needed to monitor the clinical progress of children with cerebral malaria.Medications, i.v. fluids and blood transfusions are recorded on a separate sheet on the research ward at the Queen Elizabeth CentralHospital in Blantyre, Malawi.

ED
IN
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
m 200
m 201
S 202
s 203
a 204
A 205
e 206
o 207
t 208
T 209
t 210
t 211
F 212
a 213
a 214
o 215
C 216
E 217
c 218
t 219
a 220
t 221
R 222
223
224
225
226
227
228
229
230
231
232
233
234
235
ECT
ARTICLE+ModelTRSTMH 1058 1—5
Children with cerebral malaria
If there are no clinical contraindications to a LP, oneshould be performed to exclude concomitant meningitis. Ifthere is evidence of papilloedema on ocular fundus exami-nation or if the patient is too unstable for an LP, presumptivetreatment for meningitis should be started.
At this point it should be possible to determine if thepatient meets the standard clinical case definition of cere-bral malaria: Blantyre Coma Score of 2 or less, Plasmodiumfalciparum parasitaemia of any density and no other obvi-ous cause of coma (hypoglycaemia, meningitis or a post-ictalstate).5
Oxygen saturation <90% is rare in patients with severemalaria but, when present, patients should be treated withexogenous oxygen; this is generally most affordable whenprovided by an oxygen concentrator via a nasal cannula.Hypoxemia should raise the suspicion of a concomitant lowerrespiratory tract infection.
Blood should be collected for grouping and cross-matching as soon as possible in patients with severe malarialanaemia who require transfusion, and the blood for transfu-sion should be administered as soon as it is available.
Intravenous fluids and antimalarial treatment shouldcommence as soon as possible, accompanied by regular clin-ical observations.
Consideration should be given to the use of broad-spectrum antibiotics in patients with severe anaemia,particularly if they manifest any signs or symptoms of sep-sis (hypotension, cool extremities, delayed capillary refill orhyperlactataemia).6
Two-hourly clinical assessments of vital signs and theBlantyre Coma Score permit the early detection of commoncomplications. If the coma score decreases after the startof treatment, investigations should focus on the possibilityof fits, hypoglycaemia or worsening anaemia.
While patients are unconscious, six-hourly assessments ofparasitaemia, haemoglobin/haematocrit, glucose and lac-tate allow for rapid recognition of potential complications,and can be coordinated with subsequent doses of antimalar-ial drugs.
The use of a one-page flow chart containing all the vitalinformation may help to simplify management decisions(Figure 3).
UN
CO
RR
Please cite this article in press as: Taylor TE. Caring for childrea research ward in Malawi. Trans R Soc Trop Med Hyg (2008), d
On the research ward in Blantyre nurses make the two-hourly observations and administer medications. Cliniciansmake ward rounds twice each day and a clinician is avail-able at all times to re-assess children if/when their clinicalcondition changes.
PR
OO
F
PRESS5
Using this approach the overall mortality rate for childreneeting the standard clinical case definition of cerebralalaria is 17.8%. For children admitted with a Blantyre Coma
core of 2 it is 10.4%, for those with a coma score on admis-ion of 1 it is 16.7%, and for of those with a coma score ondmission of 0 it is 34.2% (unpublished observations).
cknowledgements: TET wrote the entire paper based onxperiences shared with Malcolm E. Molyneux and manyther clinicians over 20 years on the research ward athe Queen Elizabeth Central Hospital in Blantyre, Malawi.hanks go to Nathaniel Duke for the photographs used inhis paper, and the loyal nurses of the research ward forheir kind, thoughtful care of our patients over the years.
unding: Support for the malaria research work that gener-ted these insights was supported by The Wellcome Trust, UKnd the US National Institutes of Health through a numberf different grants between 1986 and 2008.
onflicts of interest: None declared.
thical approval: The institutional review boards/ethicsommittees at the University of Malawi College of Medicine,he University of Liverpool, and Michigan State Universitypproved the studies that provided the infrastructure forhese suggestions.
eferences
1. Molyneux ME, Taylor TE, Wirima JJ, Borgstein A. Clinical featuresand prognostic indicators in paediatric cerebral malaria. A studyof 131 comatose Malawian children. Q J Med 1989;265:441—59.
2. Newton CR, Chokwe T, Schellenberg JA, Winstanley PA, ForsterD, Peshu N, et al. Coma scales for children with severe falci-parum malaria. Trans R Soc Trop Med Hyg 1997;91:161—5.
3. Taylor T, Fu W, Carr R, Whitten R, Muller J, Fosiko N, et al. Dif-ferentiating the pathologies of cerebral malaria by postmortemparasite counts. Nat Med 2004;10:143—5.
4. Beare NA, Taylor TE, Harding SP, Lewallen S, Molyneux ME. Malar-ial retinopathy: a newly established diagnostic sign in severemalaria. Am J Trop Med Hyg 2006;75:790—7.
5. WHO. Guidelines for the treatment of malaria 2006. Geneva:
TRSTMH 1058 1—5n with cerebral malaria: insights gleaned from 20 years onoi:10.1016/j.trstmh.2008.10.049
World Health Organization; 2006. 236
6. Bronzan RN, Taylor TE, Mwenechanya J, Tembo M, Kayira K, 237
Bwanaisa L, et al. Bacteremia in Malawian children with severe 238
malaria: prevalence, etiology, HIV coinfection, and outcome. 239
J Infect Dis 2007;195:895—904. 240
















![Cerebral Malaria [Dr. Usman Sp. S]](https://static.fdocuments.us/doc/165x107/577d1d971a28ab4e1e8c97e2/cerebral-malaria-dr-usman-sp-s.jpg)