
Caring Connection
28
CONNECTION CARING ST. JOSEPH’S A Publication of St. Joseph’s Hospital Health Center | Spring 2009 | Vol. 6, No. 1 IN THIS ISSUE: Second Chances
-
Upload
st-josephs-hospital-health-center -
Category
Documents
-
view
225 -
download
1
description
A publication from St. Joseph's Hospital Health Center.
Transcript of Caring Connection
ConneCtionCaringS t . J o S e p h ’ S
A Publication of St. Joseph’s Hospital Health Center | Spring 2009 | Vol. 6, No. 1
IN THIS ISSUE:
Second Chances

2 Caring ConneCtion l St. JoSeph’S hoSpital health Center l Spring 2009 l www.sjhsyr.org
“the charity of the good knows no creed and is confined to no one place.” these words of Mother Marianne Cope,
one of the first administrators of St. Joseph’s hospital, are as relevant to us today as they were more than a century ago.
as St. Joseph’s celebrates its 140th year, i am reminded of the spirit in which the hospital was founded by five Franciscan sisters who, in 1869, courageously estab-lished Syracuse’s first hospital—St. Joseph’s —to care for those who suffered from the common malarial and typhoid fevers of the day as well as the sick poor.
as we reflect on those pioneering sisters and all those who have followed—as well as
the many, many lay people who have cared for our community as members of St. Joseph’s—i am often awed by those on whose shoulders we now stand. We have a great responsibility.
a hospital changes during its lifetime—often growing in size and services, adapting to technology, and responding to and leading change in the broader society. St. Joseph’s has grown from 15 patient beds in 1869 to a network of health care services in 2009 that include a 431-bed hospital, outpatient services (such as family medicine and mental health), specialty services (such as hemodialysis and wound care), home care and a college of nursing. throughout all of the milestones that we have shared with our community (you will find many of these in the timeline on page 15), we have not wavered in our commitment to provide a higher level of health care compassionately to all those who seek our help.
as much as we revere our history, we are compelled to prepare for the future. one way is by examining our core—our mission and our values. over the past eight months, literally more than a thou-sand St. Joseph’s employees, physicians, members of our Council of advisors and Board of trustees, as well as our sponsors, the Sisters of St. Francis, provided input into the development of a restatement of St. Joseph’s mission statement and values that reflect who we are
today and that will guide us for years to come. as Sister rose ann renna, vice president for mission services, explained: our mission is what we do and our values are how and why we do it. although our previous mission statement and guiding values served us well for 20 years, it was St. Joseph’s intent to create a new statement that could be recalled easily and would feel inclusive to our diverse community. in addition, this mission statement needed to reflect St. Joseph’s guiding beliefs. i wholeheartedly believe that we have done that. Simply stated:
“We are passionate healers dedicated to honoring the Sacred in our sisters and brothers.”
providing guidance in how to live this mission are our core values:“In the spirit of good Stewardship, we heal by practicing: Compassion through our kindness, concern and genuine caring; Reverence in honoring the dignity of the human spirit; Excellence by expecting the best of ourselves and others; Integrity by being and speaking the truth.” i’d like to thank all of those who participated in the development
of our mission statement and values. their insight was invaluable to this extraordinarily important process.
St. Joseph’s is also readying itself for the kick off this fall of phase ii of our facility master plan. having completed phase i, which resulted in an expanded lobby/conference center, Medical office Centre, 800-space parking garage and skybridge, this phase will provide the physical space and configuration necessary to meet the demands of providing health care in the 21st century. i hope you will read more about our plans in the article that appears on page 3.
as we celebrate the 140th anniversary of admitting St. Joseph’s first patient, i join our entire network family in thanking you for entrusting St. Joseph’s to care for you and your loved ones. You have our pledge that we will do our very best to honor that sacred trust.
theodore pasinskipresident
a h i g h e r l e v e l o F C a r e
our MissionWe are passionate healers dedicated
to honoring the Sacred in our sisters and
brothers.
our Core valuesIn the spirit of good Stewardship,
we heal by practicing: Compassion
through our kindness, concern and
genuine caring; Reverence in
honoring the dignity of the human
spirit; Excellence by expecting the
best of ourselves and others; Integrity
by being and speaking the truth.
ContentsUp-to-Date 3
Conscientious Care and a Family’s Love Return Critically Ill Judge to the Bench 4
Pulmonary Rehabilitation Helps Couple Enjoy Life—Afloat or Ashore 6
New Hip Resurfacing Procedure Has Him Back on his Feet and Skis 8
Love and ‘Round-the-Clock Attention Bring Little Giovanna Home 10
Thanks to Robotic Surgery, Quality of Life Remains 12
Skill, Teamwork and New Technology Combine to Create a ‘Miracle Patient’ 14
St. Joseph’s Hospital Health Center—Celebrating 140 Years 15
Our Foundation Report 22
Front Cover:When Dryden Town Justice Joseph Valentinelli dismissed charges against a hospice worker who had been making a business call on his cell phone while driving, he could not have foreseen that the former defendant would be on the ambulance crew that kept him alive during a tension-filled rush to St. Joseph’s emergency department. Article on page 4.
Theodore Pasinski

www.sjhsyr.org l Spring 2009 l St. JoSeph’S hoSpital health Center l Caring ConneCtion 3
uP lTo lDATe
Gearing Up for Phase II
W ith phase I of St. Joseph’s Hospital Health Center’s facility master plan completed—resulting in an expanded lobby/
conference center, Medical office Centre, 800-space parking garage and skybridge—the hospital is gearing up for phase II.
expected to kick off this fall after New York state review, phase II will be divided into two parts: A and B. After completion, St. Joseph’s will be better equipped to provide health care well into the 21st century.
With an expected completion date of 2011, phase IIA includes:l an expanded emergency department that will allow
St. Joseph’s to care for more patients and reduce ambulance diversions
l increased space to meet the needs of patients using emergency psychiatric services
l relocation and expansion of nutritional services to improve efficiency and support a new “room service” model
l a state-of-the-art primary data center
Following the completion of phase IIA, phase IIB is expected to begin in 2011 and be completed in 2013. Phase IIB includes a:
l 104,000-square-foot patient tower that will house 110 new private patient rooms that are 35 percent larger than current semi-private rooms
l 73,000-square-foot surgical suite with 14 operating rooms that are 50 percent larger than existing operating rooms and that will support hybrid technology that allows more flexibility during clinical procedures
Phase II of St. Joseph’s facility master plan will provide both short-term and long-term benefits to the community. It will:
l improve patient care and staff workflowl create approximately 200 new health care jobsl employ nearly 600 construction workers, many of whom will
be unionl engage local architects, engineers and vendorsl generate between $1 million and $2 million in additional local
revenue (e.g., meals, room and board)
l be designed in concert with the Metropolitan Development Association of Syracuse and Central New York
l be environmentally sustainable/renewable, pursuing LeeD “silver” certification
l improve the streetscape along the Connective Corridor as well as improve street and site lighting, thereby enhancing safety
l upgrade city underground water and storm water infrastruc-ture, which will benefit surrounding neighborhoods
l cost more than $200 million (including $500,000 in permit fees to the city of Syracuse)
St. Joseph’s Is ‘Baby-Friendly’
St. Joseph’s Hospital Health Center is a “Baby-Friendly” hospi-tal, according to the World Health organization Baby-Friendly
Hospital Initiative (BFHI). It is the only Central New York hospital to receive the designation and one of only 77 in the country. New York state has just two other hospitals with the distinction.
The BFHI is a global program sponsored by the World Health organization (WHo) and the united Nations Children’s Fund (uNICeF) to encourage and recognize hospitals and birthing centers that offer an optimal level of care for lactation. The BFHI assists hospitals in giving breastfeeding mothers the information, confidence and skills needed to successfully initiate and continue breastfeeding their babies, and gives special recognition to hospitals that have done so.
According to the Centers for Disease Control and Prevention, what occurs in the hospital or birth center plays a crucial role in establishing breastfeeding and helping mothers to continue breast-feeding after leaving the birth facility.
Through the BFHI, St. Joseph’s promotes, protects and supports breastfeeding, following 10 steps outlined by uNICeF/WHo. A full list of the steps may be found at www.babyfriendlyusa.org.
St. Joseph’s has six lactation consultants—the highest number of any Syracuse hospital—and they are available seven days a week. In addition, the hospital supports its own employees who are breast-feeding their babies after returning to work. A private pumping room is available for employees to use.
uP-To-DATe continued on page 28
Looking from the northeast toward N. Townsend Street, the lower elevation in this architectural rendering illustrates St. Joseph’s emergency services building, which will contain the emergency department, emergency psychiatric services, an observation unit, café, sterile services and the data center. Adjoining the emergency services building, the taller structure is the north building, which will house a surgical suite with 14 operating rooms, critical care floor with 38 private patient rooms, and two medical-surgical floors with 72 private patient rooms.
A new mother breastfeeds her infant with the guidance of Patricia Aiken, RN, a St. Joseph’s lactation consultant.

a h i g h e r l e v e l o F C a r e
thirty-seven years as a high school earth science teacher; 14 years as an elected justice in the town of Dryden; a husband to his wife, Mary, for 50 years; the father of three; devoted grandfather to garrison and
Colin—maybe Joseph valentinelli just needed a rest. if that was it, then he got more than he bargained
for the morning of oct. 20, 2008. although valentinelli is a bear of man at a muscled
6' 5", he smiles easily and displays a subtle, yet quick, sense of humor around his family and friends. Wearing an argyle sweater, he gives the impression of being loving and a bit “cuddly”—more teddy bear than grizzly. Draped in his black judicial robes and peering down from his bench, however, Judge valentinelli must be able to strike mild terror into a defendant’s heart. But, to those who saw him that october morning, the thought never would have crossed their minds. the mitral valve between his heart’s left atrium and left ventricle had given way, essentially reversing the flow
of blood through his heart. he could hardly breathe. his heart stopped the first time in the ambulance outside his Dryden home. paramedics resuscitated him. he was stabilized in Cortland, given an echocar-diogram that isolated the valve problem, and then rushed to St. Joseph’s hospital heath Center.
the ambulance ride was just the beginning of what would be a 45-day-long struggle for Judge valentinelli, the team of nurses and specialists who managed his treatment, and the close family that supported him, the doctors, nurses and each other.
“When he arrived we were waiting for him in the operating room,” says g. randall green, MD, who was a surgeon on call that morning. “he arrested again at St. Joseph’s. he was barely alive, just clinging to life.”
although the original echocardiogram appeared to show a problem with valentinelli’s mitral value, surgeons couldn’t begin treating it without knowing the condition of his coronary arteries. as Dr. green says, he and the surgical team “couldn’t just jump in” without knowing whether he also had coronary artery disease.
“We literally stood there as Dr. Simons (alan Simons, MD) performed the angiogram,” Dr. green recalls. “his coronary arteries were fine. he wasn’t having a heart attack. So, it was back to the operating room.”
a high-resolution transesophageal echocardiogram (tee) confirmed the original diagnosis. it was, Dr. green says, as if much of the blood flowing through his patient’s heart in its regular sequence suddenly started flowing the wrong way.
“he went from being an active, healthy guy moving around and doing everything one minute, to being in congestive heart failure and close to death the next.”
over the next four hours, Dr. green and his team of physician assistants and nurses replaced valentinelli’s non-functioning mitral valve with an artificial biopros-thetic valve. the cardiac surgery team has performed hundreds of such procedures at St. Joseph’s. in many ways, Dr. green says, the valve replacement was the easiest part of valentinelli’s care. When the surgery ended and their patient was taken off the heart-lung machine that had circulated oxygenated blood for him, the replacement valve worked as intended.
“Dr. green came up to me after the surgery and said the operation was a success,” Mrs. valentinelli remem-bers, “but he said we had a long way to go.”
Dr. green’s prediction was confirmed when valen-tinelli didn’t wake up—not in a few hours, not in a day, not in a week.
“When a day goes by, i think to myself this isn’t good,” Dr. green says. “after several days, you really start to wonder.”
private thoughts are one thing, but Dr. green says the entire team caring for valentinelli and his family maintained an optimistic approach, continuing, he says, “to fight.” part of the concern was the fact that no one really knew what had happened to valentinelli before he woke up in pain and having trouble breathing. he
Conscientious Care and a Family’s Love Return Critically Ill Judge to the Bench
“He needs me as much as I need him,” says Valentinelli’s grandson, Colin Wood, of his grandfather. “We’re good friends.” Wood says he is considering a career in critical care nursing after witness-ing firsthand the dedi cation, caring and work ethic of the nurs-es who cared for his “Papa” at St. Joseph’s.
4 Caring ConneCtion l St. JoSeph’S hoSpital health Center l Spring 2009 l www.sjhsyr.org

www.sjhsyr.org l Spring 2009 l St. JoSeph’S hoSpital health Center l Caring ConneCtion 5
may have been, as physicians say, “poorly perfused” (lacking blood flow and oxygen) for hours creating the possibility of brain damage.
For days, valentinelli didn’t stir. he wasn’t on any pain medication or sedatives, so drugs weren’t causing his non-responsiveness. By now a large medical team was looking after valentinelli. Salil gupta, MD, a nephrologist, worked to maintain his kidney function that can be compromised in such situations. neurolo-gists were consulted about possible brain damage. St. Joseph’s intensivists (physicians with advanced training in treating the most seriously ill) worked closely with Drs. green and gupta, nurses and physi-cian assistants. a ventilator helped valentinelli breathe easier. a feeding tube kept him nourished.
“it’s never a single person who succeeds,” Dr. green says. “it’s the whole system that does it. the big guy (Mr. valentinelli) also had an incredibly supportive family. We all propped each other up.
“his family was so confident, so optimistic that it was almost viral—contagious. When they walked into a room everyone felt this man was going to make it, get back home and go to work. i think they made a real difference in his outcome.”
interviews with Mrs. valentinelli and their two daughters, terri Wood and lisa valentinelli confirmed Dr. green’s observation. each spent hours with valen-tinelli talking about sports, the price of gasoline, happenings in Dryden, and the approaching elections, even though he didn’t respond.
“they started calling me ‘Crying lisa,’” valentinelli’s younger daughter says. “that was my job—to hold Dad’s hand, talk and cry in that order. We knew that Dad was in bad shape, but the people here never led us to believe that it was as bad as it was.
“Sometimes i’d call at two or three in the morning to check on how he was, and never was i made to feel that i was bothering them. that was a huge thing for us.”
Mrs. valentinelli, who had survived a life- threatening illness two years ago, cheered everyone who heard her talking to her non-responsive husband. She talked to him as if he were conscious and fully alert: “look here, you silly creep, you’re not going to die on me now. i’ve got too many things for you to do around the house!”
then valentinelli’s son, paul, called daily from his home in Baltimore, as well. the intensive care unit staff grew to rely on the cupcakes and cookies that flowed from the valentinelli’s kitchens, just as the family came to rely on the “chicken drummers” from St. Joseph’s cafeteria. the daughters treated the staff one night to a feast from Dinosaur Bar-b-que, saying their father had paid for it. “Well, he’d better wake up,” a nurse said. “You’re spending all his money.”
and then, not too many days later, Joseph valenti-nelli moved his finger.
at first, the movements were so gradual and infre-quent that it was unclear whether they were really happening. the repeated moving of a finger might lead to the stirring of valentinelli’s hand. another limb might move the next day.
“it was so gradual we had to look back over our notes for the last week to tell us if there really was an improving trend,” Dr. green says. “then one day, two weeks after surgery, he opened his eyes.”
the family’s biggest smiles were generated the day valentinelli looked at his wife and said, “hi, Beautiful.”
“he’d never said that to me in 50 years,” Mary valentinelli says, “never in 50 beautiful, happy years of marriage!”
valentinelli’s recovery gradually accelerated. after weaning him off the ventilator, a respiratory therapist worked to strengthen his breathing. valentinelli said he felt like a 2-year-old trying to learn to walk again. that soon changed with the forceful intervention of his wife pestering him to get out of bed and exercise.
“i don’t remember any of it,” valentinelli says three months after his hospital stay. “they tell me i died twice on the way to the hospital and had to be resuscitated. i guess i’m glad i don’t remember it.
“My only problem is i don’t know exactly who to thank—Dryden ambulance, Cortland regional Medical Center, tlC, my family, my St. Joseph’s doctors and nurses? i’m just one lucky guy to be given another chance. i do think there’s a reason why i’m still here. am i being given a second chance for something i did in life? i don’t know.”
Maybe it’s because he’s a good judge. While valenti-nelli was unconscious at St. Joseph’s, he was re-elected to another term as Dryden town justice by a landslide. l
Whom does Joseph Valentinelli have to thank for his recovery from a life-threatening coronary valve failure? These are just five of the nearly 200 estimat-ed St. Joseph’s staff members who helped in a multitude of ways. Photographed in the intensive care unit after Valentinelli’s discharge are (from left to right) Alex Skripnichuk, RN; Salil Gupta, MD, neph-rologist; Valentinelli; G. Randall Green, MD, cardiac surgeon; Kathryn Mancarella, RN, CCRN; and Stacey Magdziuk, RN, CCRN.

a h i g h e r l e v e l o F C a r e
6 Caring ConneCtion l St. JoSeph’S hoSpital health Center l Spring 2009 l www.sjhsyr.org
a h i g h e r l e v e l o F C a r e
Judy Bethmann knows how hard the first mate on a 34-foot cabin cruiser has to work—especially when that first mate has only 23 percent of her lung capacity left.
Bethmann and her husband, Fred, love the water and love boats. During the summer, their home is their cabin cruiser. like many active boaters, they spend their winters ashore wishing they were back afloat.
three years ago that passion would have come to an end had it not been for Judy Bethmann’s tough decision that was made a little easier by her new friends at St. Joseph’s hospital health Center’s pulmonary rehabilitation program.
“My primary care physician first used the word ‘emphysema’ 10 years ago,” she recalls, “but i was feeling absolutely wonderful. i was also foolish. i kept smoking, and it really started taking its toll.”
three years ago, when she learned that she had lost more than 75 percent of her lung capacity, even mild exercise left her panting. going up and down between decks grew difficult. threading her way to the bow to
deal with the anchor or mooring lines was exhausting, and could have been dangerous.
that’s when she learned about St. Joseph’s pul-monary rehabilitation program consisting of classes to help patients better understand their lung problems combined with a medically supervised exercise training regimen to improve endurance and help the body use oxygen more efficiently. Bethmann also learned that enrolling in the exercise program would require her to use supplemental oxygen. She imagined herself pulling a bottle of oxygen behind her on wheels like a car lugging a boat trailer.
“When i imagined being tied to an oxygen bottle, i went home and cried for three days straight,” Beth-mann says. “the respiratory therapists said i needed to exercise, but also needed oxygen for safety’s sake. i knew in my heart they were right, but i still wanted to put it off.
“that’s when i told myself that i needed to get my rear in gear and call the oxygen company. no one was going to do it but me.”
Pulmonary Rehabilitation Helps Couple enjoy Life—Afloat or Ashore
When she’s not crew-ing aboard the family 34-foot cabin cruiser, Judy Bethmann has plenty of energy to pilot her own out-board, It’s About Time.

www.sjhsyr.org l Spring 2009 l St. JoSeph’S hoSpital health Center l Caring ConneCtion 7
Sue Woods, a registered respiratory therapist who developed the program more than 15 years ago, describes the exercise phase as a fundamental condi-tioning of the body’s muscles, and, as Judy Bethmann has learned, the lungs are muscles, too.
“our goal is to help people take the lung function they have and make it more efficient at oxygenating their system,” Woods says. “We help them understand that it will be slow, gradual and safe. We don’t want them to be working all that hard. Most are amazed at what they can achieve.”
When Bethmann started out, she was skeptical. She was already exhausted, so how was she supposed to exercise? She learned that the rehabilitation center’s respiratory therapists weren’t going to let her overdo the exercise. each exercise program is individually designed, and each person’s heart rate, blood pressure and oxygen levels are regularly monitored.
Bethmann says she feels safe at the rehabilitation center. She realizes that “six-pack abs and thin thighs” aren’t the goal here, wellness is. the fact is, though, she has lost 25 pounds and attributes it both to the regular exercise and the classes involving nutrition.
the oxygen system Bethmann once dreaded is now an old friend. While exercising, she wears an oxygen container housed in an over-the-shoulder bag that looks more like a casual purse than a medical device. at home and on the boat she has installed an oxygen concen-trator for use while she sleeps. the air we breathe is a mixture of gases, with about 70 percent being nitrogen rather than pure oxygen. the oxygen concentrator works by absorbing nitrogen from the air, thereby increasing the proportion of oxygen. the oxygen-rich air is fed through a tube to the nose.
“i was a little uncomfortable sleeping with the cannula at first,” Bethmann says, “but now i’m uncomfortable if i don’t go to bed with it. it’s kind of like linus and his security blanket.”
Sue Woods tells her patients that supplemental oxygen, whether from a canister or concentrator, should be viewed as a tool that helps them be more active and independent. it has certainly been true for Bethmann, but she credits the therapists at the rehabili-tation center for her progress.
“if this place weren’t here, i’m not sure i could have done it on my own,” Bethmann says, “and i am certain we wouldn’t have been able to continue enjoying our boat. i really needed their guidance and the ‘cheer-leading.’ they’re great cheerleaders who care and want you to do the best you can.” l
“our goal is to help people take the
lung function they have and make
it more efficient at oxygenating their
system. We help them understand
that it will be slow, gradual and safe.
We don’t want them to be working all
that hard. Most are amazed at what
they can achieve.”— Sue WooDS
Bethmann’s participation in the pulmonary rehabilitation exercise program has allowed her body to make the most of her remaining lung capacity.

a h i g h e r l e v e l o F C a r e
8 Caring ConneCtion l St. JoSeph’S hoSpital health Center l Spring 2009 l www.sjhsyr.org
as many men seem to do, Stuart gardner tried to ignore, or at least live with, the pain in his right hip. after all, he was only 47 and still an active outdoorsman and busy consultant
working on large projects for utility companies in the northeast.
after walking a hundred yards into the woods, he says he’d be limping like “Festus” in the old Gunsmoke television series, but he’d always been able to press on. he told himself that enough was enough, however, the day he could barely stand after being seated at his desk all day.
“i finally came to the realization that i wasn’t getting any better,” gardner says from his home in Canton, nY. “i decided to do something about it.”
gardner essentially had two choices, according to orthopedic surgeon Seth greenky, MD. he could have traditional hip replacement surgery, or he could try a relatively new procedure called hip resurfacing that seems to work especially well for young, active patients (mostly men) who dread the thought of being forced to give up their active, sometimes strenuous, lifestyle.
“hip resurfacing has taken off in this country because it allows people to resume their active lifestyles with very few restrictions,” Dr. greenky says. “after recovery, they can go out and ski if they want to. this
is possible because hip resurfacing preserves the femur or thigh bone, unlike a traditional total hip replacement surgery.”
the human hip joint is a ball-and-socket design with the ball at the top of the femur or thighbone. that ball fits into a socket-shaped bone in the pelvis. in traditional hip replacement surgery, the ball-shaped end of the thighbone is removed and a tapered metal stem is literally hammered into the core of the remaining bone. a metal ball is then attached to the stem and the ball fits into the socket in the pelvis.
in hip resurfacing, Dr. greenky explains, the femur remains whole. instead of removing the ball-shaped section at the top of the femur, it is trimmed down and shaped so that a metal surface fits securely around it. the resurfaced portion of the femur then fits into the socket as in a regular hip replacement surgery.
New Hip Resurfacing Procedure Has Him Back on His Feet and Skis
“hip resurfacing has taken off in this
country because it allows people to
resume their active lifestyles with
very few restrictions.” —SeTH GReeNKY, MD
Without a newly resurfaced hip joint, Stu Gardner would most likely be unable to stack the piles of lumber that will go into the barn he’s converting into a weekend camp.

www.sjhsyr.org l Spring 2009 l St. JoSeph’S hoSpital health Center l Caring ConneCtion 9
There are significant differences between traditional joint replacement surgery and the hip resurfacing procedure used to restore Stu Gardner’s ability to lead the active lifestyle he enjoys, according to Seth Greenky, MD, St. Joseph’s orthopedic surgeon.
“the pelvic side of the surgery is essentially the same as a regular hip replacement,” Dr. greenky says, “but preserving all of the femur has a long-range ben-efit. if the resurfaced joint has to be replaced in 10 or 20 years, then we still have the all of the femur left and we can perform a traditional hip replacement.”
the resurfacing also has other benefits. there is a reduced risk of dislocation because the resurfaced ball is larger than the ball in a regular surgery. there also is a greater range of motion.
Stuart gardner, who had his hip resurfaced a year ago, went skiing this winter, something he probably wouldn’t have risked with a traditional hip replacement.
“i hadn’t skied for six or seven years, so i was careful and stuck to the beginner and intermediate slopes,” gardner says, “but the fact is i have no restric-tions on my activities. i went hunting last fall, too. i didn’t have any luck, but it was great to be outdoors with no pain.”
For all of its advantages, hip resurfacing is not, Dr. greenky says, an option for everyone. it is generally restricted to men under the age of 60, and women over child-bearing age, but still under the age of 50. the caution to women of child-bearing age is because the metal surfaces rubbing against each other create tiny metal particles that travel through the body and release metal ions. the ions are excreted through the kidneys.
there are no data suggesting that metal ions are harmful, but research still is being done, Dr. greenky says.
“and because hip resurfacing is relatively new, we really don’t know how long the benefits will last,” Dr. greenky says.
Dr. greenky also says the resurfacing surgery takes longer and demands more skill on the part of the surgeon. St. Joseph’s surgeons perform the most total joint replacements of any hospital in Central new York and have been performing resurfacing since 2007.
When gardner’s hip was resurfaced, he entered St. Joseph’s on a Wednesday morning, had surgery that afternoon and was released from the hospital Friday afternoon.
“i was surprised at the minimal amount of discomfort or pain,” gardner says, “i didn’t need the pain medications i was given at the hospital, although i was encouraged to take them during the two weeks of physical therapy that followed so i could push myself harder.”
gardner went back to work the Monday following surgery, although he confined himself to his apartment making conference calls. he was driving his truck after three weeks and his car after that.
“the experience was all pretty positive,” he recalls. “it’s definitely an option that people in my circumstance should consider. it’s good being back to doing the things i enjoy.” l

a h i g h e r l e v e l o F C a r e
10 Caring ConneCtion l St. JoSeph’S hoSpital health Center l Spring 2009 l www.sjhsyr.org
one of the first photographs taken of newly born giovanna Josephine terrinoni shows a bracelet slipped loosely over her hand onto her tiny forearm. that wouldn’t be so
startling unless you knew the bracelet was actually her father’s wedding band.
giovanna Josephine terrinoni was born 14 weeks early on July 27, 2008. She weighed just 877 grams, that’s about an ounce shy of two pounds. She was one of the smallest and youngest ever cared for in St. Joseph’s hospital health Center’s intensive care nursery. She was also certainly loved—by her parents, of course, but also by the staff of doctors and nurses who cared for her around the clock until she went home 71 days later on oct. 5, 2008, weighing 5 pounds, 3 ounces.
numbers are vitally important in the treatment of less-than-full-term infants. temperature, pulse rate, blood pressure, oxygen and carbon dioxide levels, weight and a dozen other variables—all give important clues to the health and progress of one so little.
Until the day before her daughter’s birth, veda terrinoni had no indication that anything odd was happening.
“it was a wonderful first pregnancy,” she says, “no problems at all.”
there were no problems, that is, until the afternoon of Saturday, July 26, when she started experiencing abdominal cramps.
“this was my first child, so i didn’t really know what to expect,” she recalls. “the cramps weren’t very strong, so i just let them go. By 7 o’clock that night, though, the cramps were coming every 10 or 15 minutes.”
veda terrinoni can recite the next 24 hours, hour by hour, as if each were engraved on her memory:
7 p.m. Saturday Called obstetrician10 p.m. Drove to St. Joseph’s; treated for dehydration2 a.m. Sunday Medicated to ease contractions3 a.m. 2 centimeters dilated; contractions stronger8 a.m. Contractions stop; “feeling great;” bed rest2 p.m. Contractions resume6 p.m. Water breaks; 6 centimeters dilated
“that’s when they told me i would probably deliver in 30 minutes,” veda remembers. “all of a sudden there seemed to be 8 million people in my room. not knowing what we were going to see, and scared of what we might see, we started imagining all sorts of things.”
the delivery itself, however, was as routine as any 14-week premature birth can be, according to neo-natolo gist Jonathan Chai, MD, who brought giovanna into the world. Baby giovanna was intubated in the delivery room and placed on a mechanical ventilator for two days. Surfactant—a compound that makes it easier for the baby’s lungs to expand—also was administered. Within two days, however, Baby giovanna was breathing on her own, somewhat of a rarity for an infant born so early in the normal 40-week process.
“Dr. Chai did warn us that early births like gio-vanna’s are often what he described as a roller coaster ride,” the baby’s mother says. “We thought we were prepared.”
although giovanna was breathing on her own after two days, within two weeks (on the day of veda ter-rinoni’s baby shower), the roller coaster plunged, and giovanna went into respiratory failure. She was treated with steroids and put back on a mechanical ventilator. as a precaution, giovanna also was treated for a respira-tory infection, although later lab tests were negative.
“the terrinoni’s baby was following a common path,” Dr. Chai says. “there is often improvement, and then things slowly get worse. the fact is that the lungs of babies born so early are fragile and not really meant to be breathing air yet.”
at the same time, Dr. Chai says, ventilators also can harm a baby’s lungs. instead of letting babies decide when to breathe, the ventilator breathes for them and that can damage the fragile lung tissues. So the less the ventilator is used, he says, the better.
“We also are more aggressive with nutrition,” Dr. Chai says. “Current research says more nutrition, earlier, leads to better outcomes. newborns tend to lose weight after delivery, so we try to minimize that weight loss.”
Following the episode with respiratory failure, giovanna gradually gained weight and strength. By the time of her release to the “real world,” she was “off” any medications or medical devices except for a sleep apnea monitor to use at home.
the nursery sponsors a developmental clinic for low-birthweight babies to assess their progress, and at giovanna’s latest visit, she weighed 13 pounds. Dr. Chai called her “bright, alert, happy and very social.”
“to me, she’s a huge success,” Dr. Chai says,
Love and ‘Round-the-Clock Attention Bring Little Giovanna Home
only when you realize that the silver “brace-let” around Giovanna Terrinoni’s forearm is actually her father’s wedding band, do you begin to appreciate the challenges the tiny newborn presented to Jonathan Chai, MD, and the medical and nursing staff of St. Joseph’s intensive care nursery.
PHo
To C
ou
RTeSY o
F TeRRINo
NI FA
MILY
PHo
To C
ou
RTeSY o
F TeRRINo
NI FA
MILY

www.sjhsyr.org l Spring 2009 l St. JoSeph’S hoSpital health Center l Caring ConneCtion 11
“because of how early she was and how well she’s doing. You hope they’re all like that.”
to Dr. Chai, who grew up in the Syracuse area, St. Joseph’s intensive care nursery is one of the finest in the state—of course, he’s admits he’s partial. he says he has worked in several neonatal intensive care nurseries and that St. Joseph’s is ideal in terms of staff and size. it’s not too big to lose the personal touch, and it’s not too small to be lacking in trained staff and medical resources.
St. Joseph’s intensive care nursery is staffed around the clock with neonatologists as well as registered and advanced practice nurses. it is sized right to facilitate better communication among the staff. the staff also has the time to be very family oriented, and that’s important because the nursery has other patients to monitor beside the babies—the parents.
“We concentrate on the baby, of course,” says Dr. Chai, “but situations like this are incredibly stressful on the parents, too. they feel helpless, and that could last for weeks or months. helping them contribute something to the baby’s care, bond with the baby, and continue that over a long period is critically important.”
giovanna’s parents, veda and Chad terrinoni, immediately recall that treatment.
“i’ll admit,” says Chad terrinoni, “i was scared because i thought she might not make it. For a while i resisted getting attached to her, but the nurses encour-aged me to become involved, convincing me that she would make it. after those two weeks she just kept improving.”
after giovanna went home, each nurse in the nursery called to see how she was doing.
“i could go on and on about how wonderful the nurses and doctors were,” veda terrinoni says. “My daughter made it because of all the energy and time and skill that they put into her treatment. i plan to take giovanna back every year on her birthday.” l
St. Joseph’s intensive care nursery is using a new, state-of-the-art cooling therapy to treat newborns within hours of birth who show
signs of brain injury.“Controlled reduction of body temperature has been shown to
improve outcomes in pediatric and adult trauma victims,” explains Jonathan Chai, MD, neonatologist. “Recent studies have shown that cooling may help full-term newborns who are suffering a lack of oxygen at birth. It is only used to treat those who are most severely affected. Babies treated with therapeutic cooling have a lower mortality rate and better neurodevelopmental outcomes.”
St. Joseph’s was the first Central New York hospital to open an intensive care nursery and the first to deploy cycled lighting. Its nurse practitioners have presented important research across the country on infant sleep position to prevent sudden infant death syndrome, and St. Joseph’s neonatologists run the region’s only pediatric sleep center. In addition, the nursery is the only one in the region that participates in a collaborative database, the Vermont oxford Network (VoN), which allows it to compare outcomes with other intensive care nurseries around the world.
ICN Uses New Cooling Therapy
When Giovanna Terrinoni went home, she had many of her intensive care nursery friends wishing her well. They were (from left to right): neonatologist Jonathan Chai, MD, Molly Delgobbo, RN, Lynn Lantry, RN, Valerie Potash, NNP, and Denise Hiser-Ruddick, RN.
Alert and social, Giovanna Terrinoni has changed a lot since her 71-day stay in St. Joseph’s intensive care nursery. As any parent knows, the lives of her father, Chad, and mother, Veda, have changed forever, too.

a h i g h e r l e v e l o F C a r e
12 Caring ConneCtion l St. JoSeph’S hoSpital health Center l Spring 2009 l www.sjhsyr.org
imagine trying to fill in the squares of the Sunday crossword puzzle holding a foot-long pencil near its eraser. the resulting scribbles would be very hard to read.
now imagine performing delicate surgery to remove a cancerous prostate gland under the same circumstances, but instead using a cutting instrument and not a pencil. the stakes, however, are a lot higher because an imprecise move may result in a patient’s incontinence and loss of sexual potency.
experienced urologists have been performing lap-aroscopic surgery for years under similar circumstances and often with good results. But, the standard of care in prostate surgery has been raised dramatically in the last few years with the introduction of the davinci® surgical robot like the one in room 12 of St. Joseph’s hospital health Center’s surgical suite. Just ask elan Salzhauer, MD, and his recent patient, lou Santy of phoenix, nY.
Santy, who is 64 and just as energetic as the fam-ily’s cocker spaniel racing around the back yard, under-went successful robot-assisted laparoscopic surgery on
nov. 19 to remove his cancerous prostate. he entered the hospital at 6 a.m. that morning and left the follow - ing day at 11 a.m. he was told to take it easy for two weeks and to not lift anything weighing more than 10 pounds. had Santy undergone the traditional “open” procedure to remove his prostate and not robot-assisted laparoscopic surgery, he would have been in the hos-pital two to three days, and his at-home recovery time would have been between four and six weeks. During the traditional surgery he might have lost 1,200 milli - liters of blood—about a quart. With the robot, his blood loss was around 200 ml—about three-fourths of a cup. With a six- to eight-inch midline incision required in traditional surgery—from just below the navel to the pubic bone—the pain most likely would have endured, as well. the robot-assisted laparoscopic surgery requires only five or six incisions about a centi-meter long (less than half an inch). one of these inci-sions is made just slightly longer to remove the prostate.
“the only time i’d been in a hospital was when i was 5 and having my tonsils out, so i really didn’t want to go,” Santy says with a smile, “but everything Dr. Salzhauer told me to expect, happened. i stopped taking any pain medications the first week i was home. the entire experience was much better than i expected.”
With any surgery, experience makes a real differ-ence, and with the longest running robotic prostate surgery program in Syracuse, St. Joseph’s urologists have performed four to five times more robotic pros-tatectomies than any other Central new York hospital. in the first year of the robot’s use, Dr. Salzhauer says, St. Joseph’s performed more prostatectomies than any other community-based hospital in the country. Dr. Salzhauer has performed about 200 robotic pros-tatectomies. he admits that he was a skeptic, at first.
“i was schooled in the traditional ‘open’ prostatec-tomy and the non-robot-assisted laparoscopic proce-dures,” Dr. Salzhauer says. “i had seen the robot, but never used it until i came to St. Joseph’s and had Dr. roberts (William roberts, MD) as a mentor.
“once i witnessed the greatly reduced blood loss, the precision with which the surgery could be performed, and the shortened recovery time for the patient, i embraced the robotic technology.”
prostate cancer is the second leading cause of cancer deaths in men behind lung cancer, even though the cancer is generally slow growing, can be detected early, and can be treated with surgery or radiation. in lou Santy’s case, a routine test recommended for men over 50 detected elevated pSa (prostate-specific antigen) levels. a biopsy confirmed that Santy had prostate cancer.
“Dr. Salzhauer and i discussed the risks and benefits of each treatment, including ‘watchful waiting’ to monitor the cancer’s growth,” Santy says, “but the final decision was mine.
“My wife, tina, and i talked about it, too. if i didn’t have the surgery now, i’d probably have to have it later,
Thanks to Robotic Surgery, Quality of Life Remains
Not long after success-ful robotic prostate cancer surgery, Lou Santy was healed and ready to tackle replumbing a base-ment recreation room.

www.sjhsyr.org l Spring 2009 l St. JoSeph’S hoSpital health Center l Caring ConneCtion 13
so why not do it now when i’m in better shape? and if it spread from the prostate, it would be a whole dif-ferent ballgame. We decided i should have the surgery now, so i could stop worrying and get on with my life.”
there are risks to prostate surgery with the two most common being incontinence (loss of bladder con-trol) and the loss of potency. that’s why Dr. Salzhauer views the surgery as a three-legged stool with each leg being important.
“the general concept with any prostate surgery is the same,” Dr. Salzhauer says. “With a skilled surgeon, the cancer control was always good with the traditional approach, but the quality of life issues are important, as well.”
the prostate, an organ about the size and shape of a walnut, is hard to reach because it’s nestled below the bladder and fully encircles part of the urethra. it is partially obstructed by the public bone, as well. at the same time, nerves that control sexual function run along both sides of the prostate. the prostate also abuts two sets of sphincter muscles that control the bladder. the upper sphincter muscles are intentionally removed during surgery, but, in the past, there was a very good chance of damaging the lower set of sphincter muscles causing incontinence.
“there’s a fine line between removing all of the cancer and damaging the nerves or sphincter,” Dr. Sal-zhauer says. “too little is not good because you want to be sure to remove all of the cancer, and too much is not good because you don’t want to damage the nerves or voluntary sphincter. You can’t do one at the expense of the other, and with the open procedure it was often a foregone conclusion that there was a good chance of incontinence. there was a lot of blood loss and that made it hard for the surgeon to see the area clearly.”
the robotic approach has dramatically improved the odds of not only removing the cancer, but also sparing the nerves and lowering the chances of impotence and incontinence. even with the minimally invasive laparoscopic approach, it takes a very skilled
surgeon to operate using the cutting and other tools located at the end of a foot-long extension. however, with the robotic system, the robot’s “wrist” and “hands” greatly increase the surgeon’s precision because they twist, turn and flex right at the surgical site. they can even safely move in ways a human wrist can’t.
the davinci robot camera also produces three-dimensional images, giving the surgeon a more realistic view of the site rather than the typical two-dimensional cameras. the surgeon also can magnify the area 10 times its normal size.
“We used to hunch over, twist our necks and squint to look into the area,” Dr. Saulzhauer says. “now it’s like being only inches away, although i’m sitting at the robot’s console several feet away from my patient.”
the added precision allows Dr. Salzhauer to gently coax the prostate away from the nerves surrounding it. he also can more accurately discern the lower bundle of sphincter muscles as he separates them from the prostate itself.
only after the prostate is removed, the bladder reconnected to the remaining urethra, and the small incisions closed, can Dr. Salzhauer and his specially trained team of physician assistant and nurses relax. there is, Dr. Salzhauer says, more to the treatment of patients like lou Santy than the surgeon. it is, he says, a team approach that is responsible for St. Joseph’s successful robotic surgery program.
“From the time a patient walks into the hospital until they leave, they are served by nurses, physician assistants, anesthesiologists and others who have specialized in robotic procedures. this provides them experience and consistency of care.”
lou Santy is an enthusiastic veteran of that care.“if the robot wasn’t available, i might well have
postponed my surgery or turned to radiation therapy,” Santy says. “i’m glad it was available, though. i no longer have prostate cancer, and i suffered no bad side effects.” l
With the daVinci® surgical robot looming over his shoulder, elan Salzhauer, MD, Santy’s surgeon, was instrumental in his patient’s rapid, complication-free recovery from prostate cancer surgery.

a h i g h e r l e v e l o F C a r e
14 Caring ConneCtion l St. JoSeph’S hoSpital health Center l Spring 2009 l www.sjhsyr.org
Marcia Bracy clearly recalls her panic at not being able to breathe the morning of Dec. 5, 2008, but that’s about all. her next clear memory came many hours later as three men in white coats stood at the foot of her bed.
as she recalls, one of the trio, ahmad nazem, MD, looked down at her, smiled, and welcomed her back, saying simply: “You are my miracle patient.”
Whether or not we believe in miracles (Dr. nazem and Bracy happen to), the Fulton, nY, resident’s brush with death and her recovery from a heart attack provide a clear example of St. Joseph’s hospital health Center’s ability to muster the skilled doctors, nurses, team spirit and technical resources required to pull the critically ill back from the brink, which, Dr. nazem says, his patient clearly approached.
Bracy also benefited from the foresight required of today’s hos-pitals in searching for and investing in technology to improve the treatment available to patients. one such investment played a major role in Bracy’s successful outcome.
prior to her December heart attack, Marcia Bracy says there were no indications that anything was wrong. Despite the fact that the main arteries that supply blood and life-giving oxygen to her heart were almost totally blocked, common symptoms like chest pain, shortness of breath, fatigue, disturbed sleep, dizziness or indigestion were absent.
there was clearly a serious problem that morning, however.Under normal circumstances, Bracy would have been rushed
from Fulton to St. Joseph’s by ambulance. She would have gone immediately to the hospital’s emergency department where an electrocardiogram (eKg) would have confirmed that she was having a heart attack. From there she would have been transferred upstairs to the cardiac catheterization lab where, as a prelude to angioplasty or surgery, an angiogram would have revealed which coronary ar-teries were blocked and how seriously.
From her arrival in the emergency department until she entered the “cath lab,” about 20 critical minutes would have passed during which her heart muscle might have continued to sustain damage. But, thanks to a recent St. Joseph’s investment in new “remote telemetry” hardware and software, the Menter ambulance crew was able to transmit an eKg directly to St. Joseph’s emergency department while they were speeding south on i-81 to Syracuse. as a result, the emergency department could tell she was in the midst of a heart attack and sent her directly to the cath lab where the angiogram proved she needed immediate surgery.
“She was very sick when she reached St. Joseph’s,” therese Whitt, MD, director of the hospital’s emergency department, recalls. “When this happens, the goal in any heart attack therapy is to unblock the arteries and get blood and oxygen to the heart muscle as quickly as possible. Because of the remote telemetry, we gained about 20 min-utes by alerting the aMi (acute myocardial infarction) team that she was on her way directly to them.”
Dr. Whitt had seen the remote telemetry work in other parts of the country and suggested that St. Joseph’s patients—especially those who live farther away from Syracuse—might benefit from the equip-ment. the equipment, purchased with $50,000 in grants from the St. Joseph’s Foundation and Franciscan Management Services, was offered to Central new York ambulance services. Menter was the first to have it up and running—only five days before Bracy suffered her heart attack. of the 37 remote telemetry systems purchased by St. Joseph’s, eight have been installed in area ambulances.
the new equipment bought some time for Bracy, but her survival would require more than that.
Dr. nazem, a 17-year veteran at St. Joseph’s, was on call when the cath lab notified him that Bracy definitely needed surgery.
“Mrs. Bracy had no more than a thread of blood supply to her heart,” Dr. nazem recalls, holding his thumb and forefinger nearly together. “her blood pressure was extremely low. her heart had no pumping function. We had to place her on a heart-lung machine before her coronary artery bypass, so that her heart could rest while we harvested her vein and mammary arteries. this saved her heart muscle. otherwise, we probably would have lost her. typically, patients are placed on the heart-lung machine during their surgery.”
the surgical team even cooled Bracy’s heart to stop it, thereby slowing her metabolism and reducing the need for oxygen.
“We did everything we could to take the load off her heart and save heart muscle before we even performed the triple bypass she needed,” Dr. nazem says.
emergency surgery is challenging because surgeons never know exactly what they are going to encounter once the incision has been made. as Dr. nazem says: “You know the principles, but you have to act spontaneously as conditions change. that was the case with Mrs. Bracy, too. Due to fact that her aorta was very calcified, for example, we had to create only one hole high up in the aorta and create a y-shaped graft.”
From start to finish, Bracy’s unusual surgery took about five and a half hours.
Marcia Bracy left the hospital six days after the surgery, but her stay was followed by continuing care from St. Joseph’s home health Care.
“i feel good, i really do,” says Bracy. “i’m very fortunate. Dr. nazem told my family how serious it had been. i know they saved my life.”
Dr. nazem looks upon a case like Marcia Bracy’s as a privilege— the chance for surgical and post-operative teams to work together in overcoming the most daunting odds. it is, he says, the doctors’ job to set an optimistic tone. When a doctor is positive, it moves the whole team to a positive state of mind, he says.
“i say, ‘this person needs us and we are going to send her back to the family.’ a higher power has sent us here and we have an obli-gation. that,” Dr. nazem insists, “is when miracles happen.” l
Skill, Teamwork and New TechnologyCombine to Create a ‘Miracle Patient’
Marcia Bracy (left) didn’t know about the mobile telemetry equipment nor the cardiac team led by Ahmad Nazem, MD, (right) that saved her life until she awoke following surgery.

www.sjhsyr.org l Spring 2009 l St. JoSeph’S hoSpital health Center l Caring ConneCtion 15
The Mission of St. Joseph’sWe are passionate healers dedicated to honoring the Sacred
in our sisters and brothers.
Our Core Valuesin the spirit of good Stewardship, we heal by practicing: Compassion through our kindness, concern and genuine caring; Reverence in honoring the dignity of the human spirit; Excellence by expecting the best of ourselves and others; Integrity by being and speaking the truth.
St. Joseph’s hospital health CenterCelebrating 140 Years

a h i g h e r l e v e l o F C a r e
1855 1860 1869 1870 1872 1878 1884 1888 1895
Sisters of St. Francis founded in philadelphia, pa.
Sisters of St. Francis come to Syracuse to teach immigrant children
Sisters open St. Joseph’s hospital—Syracuse’s first hospital—on prospect hill
new York state’s first incorporation of St. Joseph’s; the hospital charter provides that “in the admittance and treatment of patients, no distinction shall ever be made because of theological belief, nationality or color”
St. Joseph’s becomes first teaching hospital in Syracuse
St. Joseph’s hospital aid Society forms (forerunner to board of directors)
two wings built, adding 75 beds
Women’s auxiliary forms; St. Joseph’s expands to 120 beds
re-incorporation
in new York state as an institution “established and
maintained for the purpose of caring
for disabled and indigent persons of
the city of Syracuse, irrespective of creed,
race or color”
16 Caring ConneCtion l St. JoSeph’S hoSpital health Center l Spring 2009 l www.sjhsyr.org
In April 1869, five Franciscan sisters purchased an old dance hall and saloon for $12,000. The sisters purchased the buildings on the far left and far right and later constructed the three-story structure in the center to join the two. With 15 beds, St. Joseph’s—Syracuse’s first hospital—opened for patients on May 6, 1869.
A four-story pavilion (far left) was added to St. Joseph’s in 1897 to accommodate advances in surgery. It had three operating rooms. one of these was an amphi-theater used for the clinical instruction of medical students.
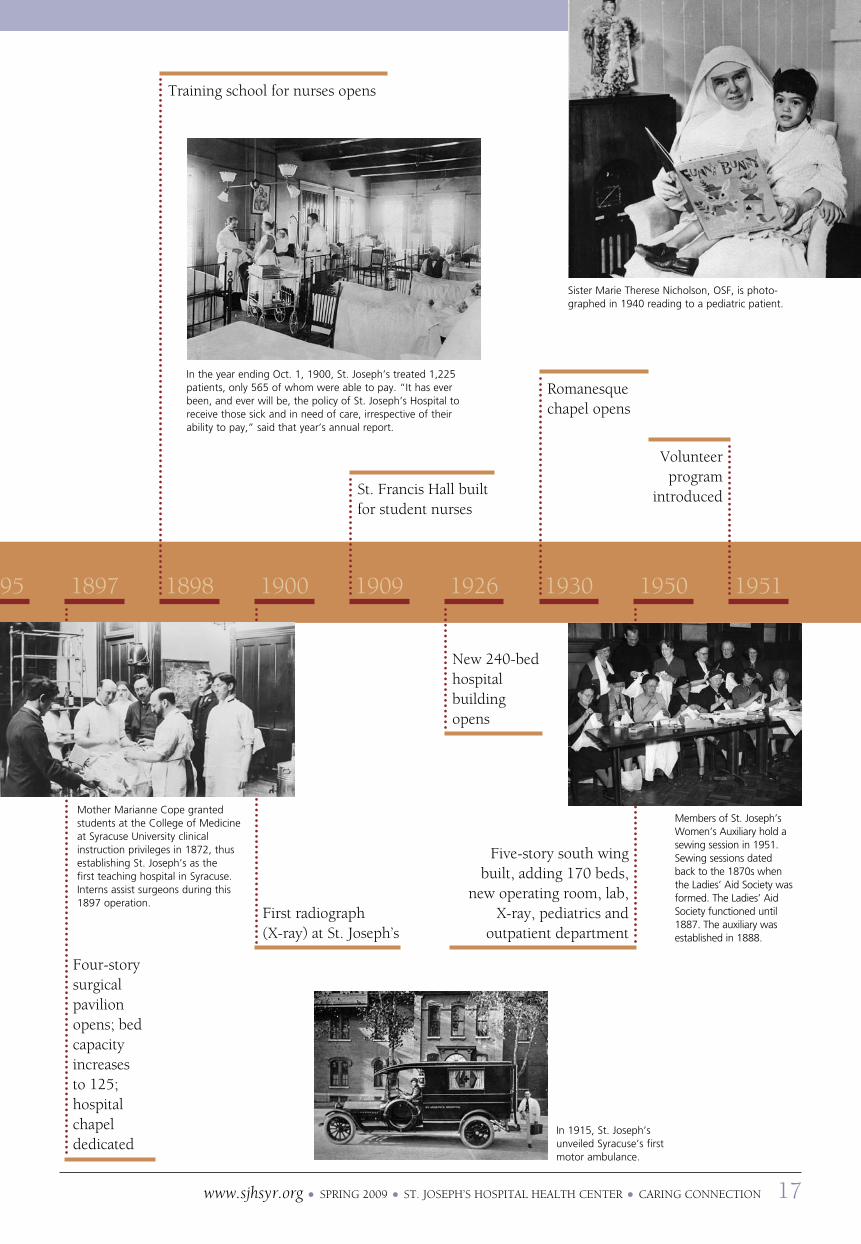
Mother Marianne Cope granted students at the College of Medicine at Syracuse university clinical instruction privileges in 1872, thus establishing St. Joseph’s as the first teaching hospital in Syracuse. Interns assist surgeons during this 1897 operation.
www.sjhsyr.org l Spring 2009 l St. JoSeph’S hoSpital health Center l Caring ConneCtion 17
In the year ending oct. 1, 1900, St. Joseph’s treated 1,225 patients, only 565 of whom were able to pay. “It has ever been, and ever will be, the policy of St. Joseph’s Hospital to receive those sick and in need of care, irrespective of their ability to pay,” said that year’s annual report.
In 1915, St. Joseph’s unveiled Syracuse’s first motor ambulance.
Sister Marie Therese Nicholson, oSF, is photo-graphed in 1940 reading to a pediatric patient.
Members of St. Joseph’s Women’s Auxiliary hold a sewing session in 1951. Sewing sessions dated back to the 1870s when the Ladies’ Aid Society was formed. The Ladies’ Aid Society functioned until 1887. The auxiliary was established in 1888.
1895 1897 1898 1900 1909 1926 1930 1950 1951
Four-story surgical pavilion opens; bed capacity increases to 125; hospital chapel dedicated
training school for nurses opens
First radiograph (X-ray) at St. Joseph’s
St. Francis hall built for student nurses
new 240-bed hospital building opens
romanesque chapel opens
Five-story south wing
built, adding 170 beds, new operating room, lab,
X-ray, pediatrics and outpatient department
volunteer program
introduced

a h i g h e r l e v e l o F C a r e
In 1958, St. Joseph’s performs the first successful open heart surgery in Central New York on 10-year-old Sharon Melfi.
St. Joseph’s performs first open heart surgery in Central new York; Monsignor toomey cardio-pulmonary laboratory set up on fifth floor
First intensive care unit opens; Marian hall (school of nursing) opens
1952 1958 1960 1967 1968 1969 1971 1974
gift shop opens
First hemodialysis treatment at St. Joseph’s
In 1966, a young candy striper cuts electrocardio-
gram tapes that will be added to patient charts.
St. Joseph’s Family practice residency program accredited and outpatient primary care center opens
St. Joseph’s administra-tor Sister Patricia Ann Mulherin prepares to break ground for St. Joseph’s $20-million expansion in June 1972. The project included an emergency department suite, enlarged outpatient department and patient beds.
James abbott appointed first lay administrator
First male nursing students accepted; intensive care unit splits into medical
iCU and surgical iCU
18 Caring ConneCtion l St. JoSeph’S hoSpital health Center l Spring 2009 l www.sjhsyr.org
100th anniversary; name changed to St. Joseph’s hospital health Center
Nurses take a minute to look over items—including magazines (Sports Illustrated), toys (Howdy Doody) and candy bars (oh Henry!)—for sale in St. Joseph’s first gift shop. The current gift shop is located in approximately the same spot.
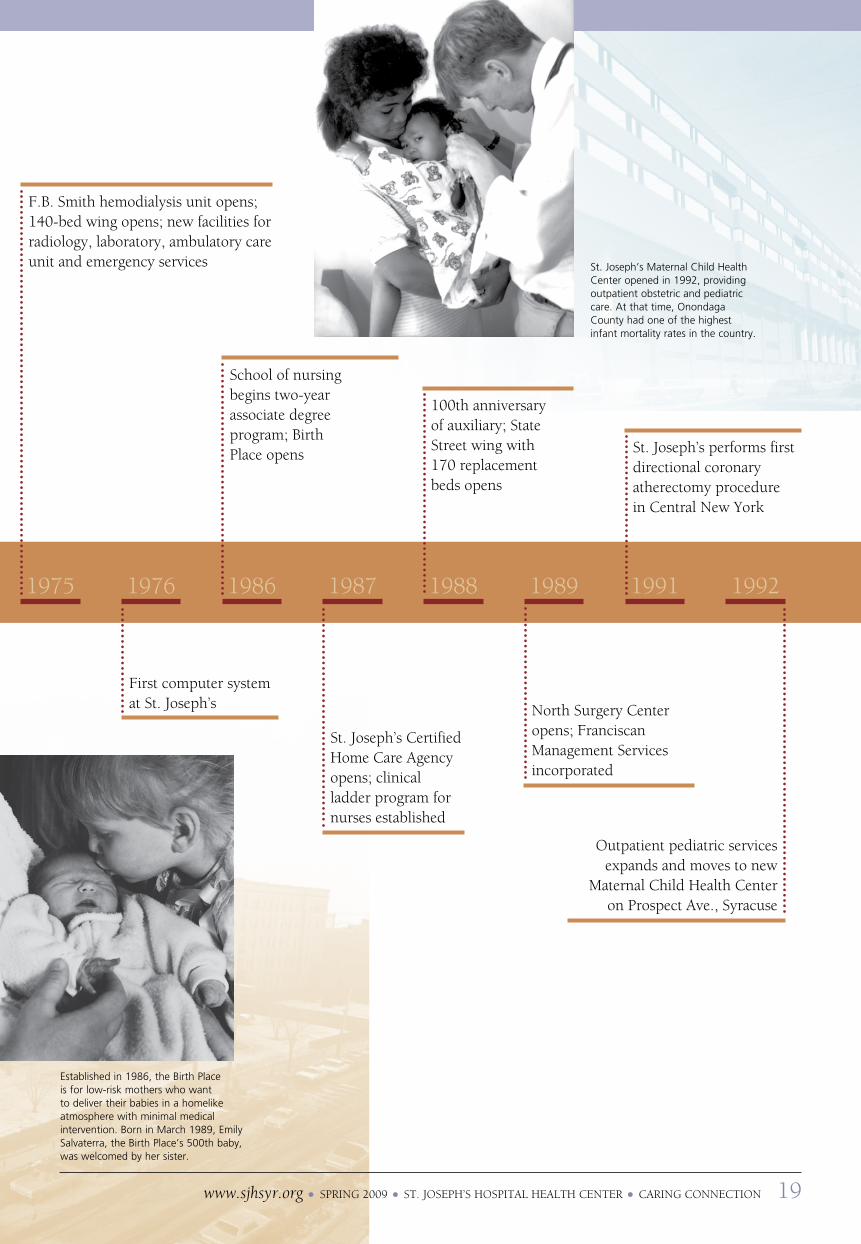
established in 1986, the Birth Place is for low-risk mothers who want to deliver their babies in a homelike atmosphere with minimal medical intervention. Born in March 1989, emily Salvaterra, the Birth Place’s 500th baby, was welcomed by her sister.
St. Joseph’s Maternal Child Health Center opened in 1992, providing outpatient obstetric and pediatric care. At that time, onondaga County had one of the highest infant mortality rates in the country.
1975 1976 1986 1987 1988 1989 1991 1992
F.B. Smith hemodialysis unit opens; 140-bed wing opens; new facilities for radiology, laboratory, ambulatory care unit and emergency services
First computer system at St. Joseph’s
School of nursing begins two-year associate degree program; Birth place opens
St. Joseph’s Certified home Care agency opens; clinical ladder program for nurses established
100th anniversary of auxiliary; State Street wing with 170 replacement beds opens
north Surgery Center opens; Franciscan Management Services incorporated
St. Joseph’s performs first directional coronary atherectomy procedure in Central new York
outpatient pediatric services expands and moves to new
Maternal Child health Center on prospect ave., Syracuse
www.sjhsyr.org l Spring 2009 l St. JoSeph’S hoSpital health Center l Caring ConneCtion 19

Part of a $22- million project that included renovated and expanded operat-ing room and labor/delivery/recovery suites, the hospital’s new laboratory opened in 1993.
a h i g h e r l e v e l o F C a r e
20 Caring ConneCtion l St. JoSeph’S hoSpital health Center l Spring 2009 l www.sjhsyr.org
1993 1994 1995 1996 1997 1998 1999 2000 20 01
More than a year in the planning and making, St. Joseph’s quilters crafted a piece to commemo-rate the 100th anniversary of St. Joseph’s School of Nursing in 1998.
Chapel, comprehensive psychiatric emergency program added; operating room suite and laboratory renovated and expanded
125th anniversary; labor/delivery/ recovery suite expanded and reno-vated; St. Joseph’s opens its first family practice satellite, the Westside Family health Center, 216 Seymour St., Syracuse
area’s first mall-based health screening/ information center, St. Joseph’s Wellness place, opens in great northern Mall, Clay
new York State Department of health finds St. Joseph’s is new York state’s top hospital for successful coronary artery bypass surgery based on mortality rates of patients between Jan. 1, 1994, and Dec. 31, 1994
electrophysiology lab—used to diagnose and treat cardiac arrhythmias—opens
St. Joseph’s School of nursing celebrates 100th anniversary; neonatal intensive care nursery moves adjacent to labor/delivery/recovery, the Birth place and postpartum
First Central new York hospital to perform endovascular repair of abdominal aortic aneurysm using technology approved by FDa just months before
St. Joseph’s School of nursing begins new Weekend program, the only one of its kind in the community
northeast Surgery Center, the only hospital-based, outpatient surgery center in the area providing over-night recovery on-site, opens in Fayetteville
on-site Mri services begin
on-site MRI services begin at St. Joseph’s in 2000. The equipment featured a shortened platform to help patients who were claustrophobic as well as virtual vision that allowed patients to watch TV and movies through a headset.
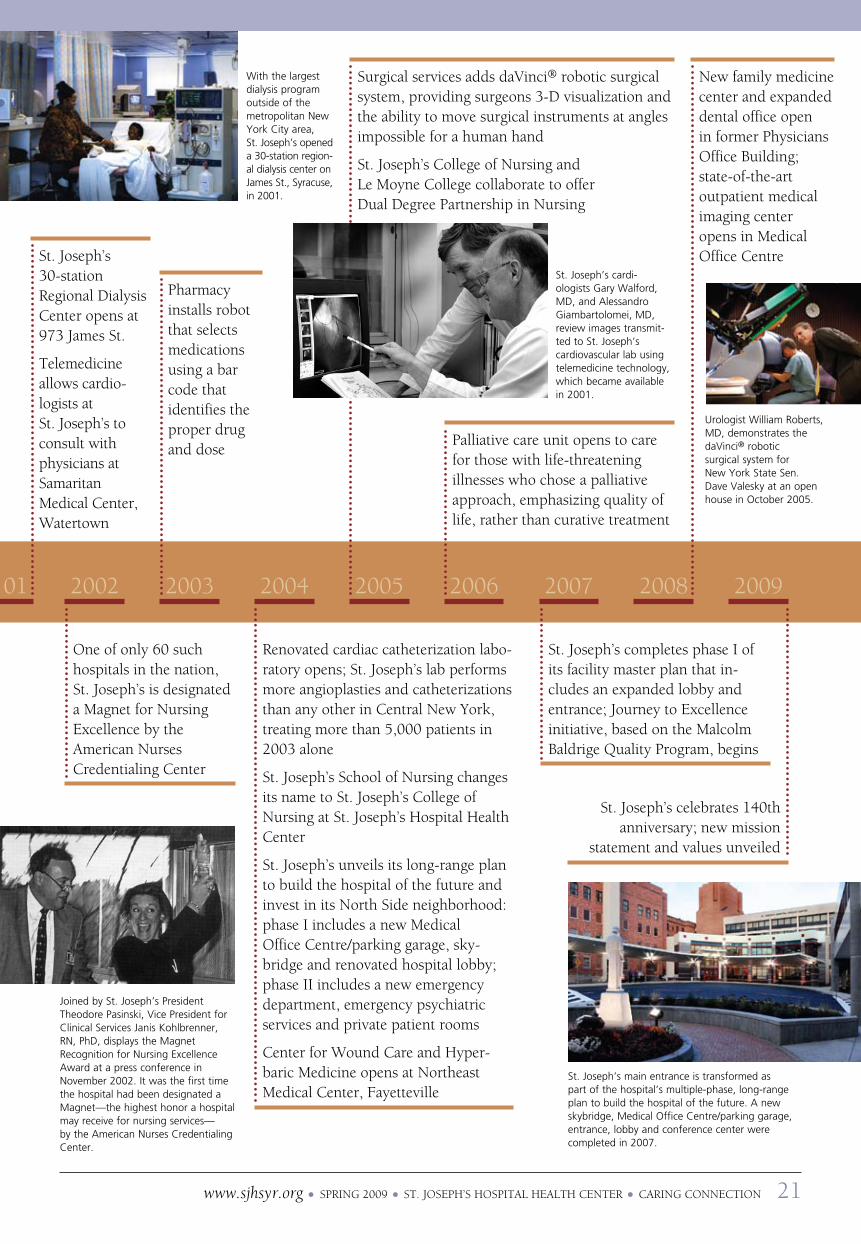
With the largest dialysis program outside of the metropolitan New York City area, St. Joseph’s opened a 30-station region-al dialysis center on James St., Syracuse, in 2001.
Joined by St. Joseph’s President Theodore Pasinski, Vice President for Clinical Services Janis Kohlbrenner, RN, PhD, displays the Magnet Recognition for Nursing excellence Award at a press conference in November 2002. It was the first time the hospital had been designated a Magnet—the highest honor a hospital may receive for nursing services— by the American Nurses Credentialing Center.
20 01 2002 2003 2004 2005 2006 2007 2008 2009
St. Joseph’s 30-station regional Dialysis Center opens at 973 James St.
telemedicine allows cardi o-logists at St. Joseph’s to consult with physicians at Samaritan Medical Center, Watertown
one of only 60 such hospitals in the nation, St. Joseph’s is designated a Magnet for nursing excellence by the american nurses Credentialing Center
pharmacy installs robot that selects medications using a bar code that identifies the proper drug and dose
www.sjhsyr.org l Spring 2009 l St. JoSeph’S hoSpital health Center l Caring ConneCtion 21
renovated cardiac catheterization labo-ratory opens; St. Joseph’s lab performs more angioplasties and catheterizations than any other in Central new York, treating more than 5,000 patients in 2003 alone
St. Joseph’s School of nursing changes its name to St. Joseph’s College of nursing at St. Joseph’s hospital health Center
St. Joseph’s unveils its long-range plan to build the hospital of the future and invest in its north Side neighborhood: phase i includes a new Medical office Centre/parking garage, sky-bridge and renovated hospital lobby; phase ii includes a new emergency department, emergency psychiatric services and private patient rooms
Center for Wound Care and hyper-baric Medicine opens at northeast Medical Center, Fayetteville
Surgical services adds davinci® robotic surgical system, providing surgeons 3-D visualization and the ability to move surgical instruments at angles impossible for a human hand
St. Joseph’s College of nursing and le Moyne College collaborate to offer Dual Degree partnership in nursing
palliative care unit opens to care for those with life-threatening illnesses who chose a palliative approach, emphasizing quality of life, rather than curative treatment
St. Joseph’s completes phase i of its facility master plan that in-cludes an expanded lobby and entrance; Journey to excellence initiative, based on the Malcolm Baldrige Quality program, begins
new family medicine center and expanded dental office open in former physicians office Building; state-of-the-art outpatient medical imaging center opens in Medical office Centre
St. Joseph’s celebrates 140th anniversary; new mission
statement and values unveiled
St. Joseph’s main entrance is transformed as part of the hospital’s multiple-phase, long-range plan to build the hospital of the future. A new skybridge, Medical office Centre/parking garage, entrance, lobby and conference center were completed in 2007.
St. Joseph’s cardi-ologists Gary Walford, MD, and Alessandro Giambartolomei, MD, review images transmit-ted to St. Joseph’s cardiovascular lab using telemedicine technology, which became available in 2001.
urologist William Roberts, MD, demonstrates the daVinci® robotic surgical system for New York State Sen. Dave Valesky at an open house in october 2005.

a h i g h e r l e v e l o F C a r e
Dear Friend of St. Joseph’s, “Each difficult moment has the potential to open my eyes and open my heart.”
~Myla Kabat-Zinn, author
on a recent trip to the village of Kalaupapa in hawaii, my eyes were opened to the enormity of the many tasks faced by our Blessed Mother Marianne Cope after she left St. Joseph’s hospital to min-ister to those in need on the island of Molokai. as the result of an isolation law enacted to exile individuals with leprosy, Kalaupapa became an island prison for almost 8,000 men, women and children who were torn from their families because they were afflicted with the feared disease. Yet, this remarkable woman saw it as a privilege to “be one of the chosen ones” who would work, live and die with these islanders. i cannot begin to describe how humbling it was, as i toured the island, to walk many of the same paths Mother Marianne had once graced.
all these years later, her “difficult moments” still carry the potential to open hearts to the possibilities that abound when we seek to improve the world around us. as you read further about my recent journey on page 23, i invite you to consider those you know who give freely of themselves despite life’s adversities.
anne Frank once wrote, “how wonderful it is that nobody need wait a single moment before starting to improve the world.” this quote captures the giving spirit not only of Mother Marianne but also of the Sisters of St. Francis and the physicians, nurses and staff of St. Joseph’s who continue the sisters’ legacy of caring.
St. Joseph’s works hard to make a difference toward improving the “world” of health care for Central new York residents. to accomplish this, St. Joseph’s hospital and the hospital’s Foundation work hand-in-hand to raise funds to enhance patient care and comfort throughout the hospital’s network of services. in 2008, the Foundation raised $2.8 million in revenue through fund-raising programs. Further, the hospital and St. Joseph’s hospital Foundation together raised an additional $2.3 million which includes a $1.8 million grant from new York state to provide electronic health record technology for 74 physicians at nine sites, including physician practices and St. Joseph’s primary care centers that provide care to the underserved. another 14 federal, state, corporate and foundation grants were received and, thanks to the community’s generosity, the annual gala and golf tournament netted nearly $600,000.
For more information about the many opportunities St. Joseph’s hospital health Center Foundation has to fit your giving interests and capabilities, please call me at 315-703-2137 or visit our Web site. We appreciate your gift at any level.
Sincerely,
Margaret Martinvice president
FoUnDation reporto u r
973 James St., Suite 250Syracuse, NY 13203Phone: 315-703-2137Fax: 315-703-2139e-mail: [email protected] online: www.sjhsyr.org/foundation
22 Caring ConneCtion l St. JoSeph’S hoSpital health Center l Spring 2009 l www.sjhsyr.org
Margaret Martin, Sister Alicia Damien Lau, and Donald Martin on the island of Molokai, Hawaii

www.sjhsyr.org l Spring 2009 l St. JoSeph’S hoSpital health Center l Caring ConneCtion 23
The primary founder of St. Joseph’s Hospital and a
leader in the Sisters of St. Francis, Blessed Mother
Marianne Cope left Syracuse in 1883 to minister to
leprosy patients in Hawaii. With six other sisters,
she responded to a plea from the Hawaiian gov-
ernment emissary for “hospital sisters” to minister
to those with the disease. Mother Marianne never
returned to Syracuse. In 1888, she extended the sis-
ters’ care of leprosy patients to Kalaupapa, Molokai.
There she established a home for female patients
and, after the death of Father Damien De Veuster,
took over the home he had established for men
and boys. Mother Marianne would spend 35 years
caring for those with leprosy on Molokai until her
death in 1918. She was inducted into the National
Women’s Hall of Fame in Seneca Falls, NY, in 2005.
That same year, Mother Marianne was beatified by
the Roman Catholic Church—a step in the process of
being declared a saint. Mother Marianne’s remains
are located at the Motherhouse of the Sisters of
St. Francis in Syracuse.
it was a clear, sunny day as my husband, Don, and i left the honolulu airport on Jan. 25, 2009, for the island of Molokai. the aircraft was a very small twin-engine, six-passenger plane. our pilot, rob,
who had retired from the air Force, guaranteed us and three other passengers a smooth 25-minute flight. as we flew out over the pacific, we looked back at the spec-tacular view of honolulu. over to the east, we could see Diamond head, Coco head, hanauma Bay and rabbit island. to the east of oahu, we soon saw the island of lanai and, in the distance, Maui.
as we approached the island of Molokai, we saw a very short runway that looked the length of a golf pencil. We were met at the airport by Sister alicia Damien lau. as she drove us into Kalaupapa—a colony founded in 1866 by Father Damien De veuster for those who had leprosy—Sister alicia stopped at a cemetery and pointed out that many years ago it was divided into Catholic and protestant burial grounds. those with leprosy would claim additional plots for their family members, so they could be buried together. today, the residents and their families are all buried in one cemetery, and Catholics and protestants are no longer separated.
When we approached the little settlement of Kalaupapa, we could see people preparing to celebrate Blessed Mother Marianne Cope’s Feast Day and her 171st birthday (which is Jan. 23). We attended a mass at St. Francis Church that included several musicians from St. John’s vianney Church in Kailua, oahu, Sis-ters of St. Francis, Kalaupapa residents (patients), and members of the broader community. in addition, guests from Syracuse, ohio, California, Seattle, honolulu and the national park Service attended. Father Felix van-
debroek (originally from Belgium) celebrated the mass. Franciscan sister Candida oroc reflected on the gospel in place of the homily. Draped with a lovely lei, Blessed Mother Marianne’s three-foot portrait was on display near the pulpit. as i sat and looked at her portrait, i couldn’t help but reflect on Blessed Mother Marianne’s message, “i am not afraid of any disease.” She was such a strong and beautiful sister.
When the mass was finished, many of the parish-ioners gathered to sing songs in the church. everyone was so happy and we enjoyed the music from guitars, keyboard, ukulele and flute. one of the residents who was singing with the group introduced himself to Don and me. he was curious to learn where we were from and what our connection was to Mother Marianne and Kalaupapa. he had been a resident at Kalaupapa for several years.
When the celebration was completed, we went to the parish hall for a brunch. We greatly enjoyed talking to the visitors and people from the Kalaupapa community. after a few minutes everyone started singing hawaiian
A Rare Visit to Kalaupapa
Boats dropped those with leprosy off at the base of Molokai’s steep cliffs. Many patients drowned trying to make it to shore.
Mother Marianne Cope, who ministered to lepers on Molokai from 1888 until her death, is depicted in a mosaic on Kalaupapa.

a h i g h e r l e v e l o F C a r e
songs, as the beautiful sun shone. Spontaneous singing seemed to break out everywhere.
there is so much history at Kalaupapa. Sister Frances therese Souza graciously took us on a tour of the island. Kalaupapa is managed by the hawaii State Department of health and the national park Service. there are still enforceable state laws that prohibit people from entering the settlement. these laws are enforced to protect the privacy of the residents. Don and i were very fortunate to be sponsored by the Sisters of St. Francis.
leprosy, or hansen’s Disease as it is called today, was very contagious among the polynesian native popu-lations, as they had not developed any immunity to the disease that was introduced to the islands by european trading ship crews. the disease was so feared that those who contracted the disease were forcibly sent to quar-antine at Kalaupapa.
there are still 23 residents on the register—14 live in the settlement at Kalaupapa and the rest live in honolulu. the average age is 77 years. When Mother Marianne and the sisters arrived in Kalaupapa in 1888, they took care of thousands of patients with leprosy. Mother Marianne and the sisters established the Bishop home for girls that still stands today. the last patients arrived on the island in 1969.
as we toured more of the island, we saw a small gas station and a little store that is only open three days a week. there also was a small building where the resi-dents and their families would meet for some quiet time together. Down the middle of this building was a wire fence. Because leprosy was so contagious, the residents would sit on one side of the wire fence and their family members would sit on the other. i can’t imagine how difficult it was for residents and family members to part after a visit.
on the north side of the island we could see sharp sea cliffs. this is where thousands of people with lep-rosy were dropped off boats in high waters to face quarantine in Kalaupapa. Many people did not make it to shore and died in the deep waters. the natural topography of Molokai guaranteed the effectiveness of the quarantine, although it is said that Father Damien found a walking route over the sheer mountain cliff to the other side of the islands.
We stopped to visit Father Damien De veuster’s gravesite. the canonization of Father Damien, which will declare him a saint in the roman Catholic Church, is anticipated later this year. a celebration is expected in a little church that is located by his gravesite.
When we arrived back at the center of Kalaupapa, we visited Mother Marianne’s chapel and gravesite. as i sat quietly in the beautiful chapel, i had an opportunity to reflect on the memorable day. i couldn’t help but think that Mother Marianne walked these grounds day after day and gave her life to help the many patients with leprosy. Mother Marianne was a very caring, courageous and compassionate sister.
it was time to leave Kalaupapa and return to oahu. When we arrived at the airport, we heard the members of the St. John’s choir singing and playing their instruments. they were waiting for a plane to arrive from honolulu. it was returning a resident who had been hospitalized. When the resident arrived, she was greeted with music, hugs and kisses. the singing continued as we boarded our plane for oahu. and, yes, there were hugs for us. as the plane made its way to the end of the runway, it turned and picked up speed back down the runway past the airport. the people from Kalaupapa were standing by the fence waving to us up in the air for a safe trip back to oahu. it was a very quiet trip back over the pacific, as Don and i were both trying to absorb the wonderful and memorable events of the day.
the community of Kalaupapa will remain as the residence of choice for any remaining patients for as long as they are physically able to stay there. the longer range outlook for Kalaupapa is murkier. there are literally thousands of unmarked graves on the peninsula, and honor and respect will dictate that little or no development will occur there.
all in all, our visit was a rare opportunity to learn about and see firsthand the compassionate care pro-vided to those afflicted with hansen’s Disease in hawaii. as important, we saw and met with the Sisters of St. Francis who now carry on the work of Father Damien De veuster and Blessed Mother Marianne Cope.
Don and i want to acknowledge our heartfelt thanks to Sister alicia Damien lau for arranging our special day and for awakening us to the true spirit of caring and giving. this once-in-a-lifetime opportunity has in-fused me personally and professionally with a renewed sense of wonder at the sacred work of Mother Marianne and the sacred healing that continually takes place at St. Joseph’s. l
This memorial was erected by the people of the Kalaupapa settlement at Mother Marianne’s Molokai gravesite. Mother Marianne Cope’s remains now are located at the Motherhouse of the Sisters of St. Francis in Syracuse.
24 Caring ConneCtion l St. JoSeph’S hoSpital health Center l Spring 2009 l www.sjhsyr.org

Giving online is safe, secure and easy. Just go to www.sjhsyr.org/foundation.
‘What Can I Do?’patients and their families often ask, “what can i do to help St. Joseph’s?” as a non-profit with a clear mission to help all in our community, no matter their circum-stances, we struggle to find the financial resources necessary to maintain the very highest quality of care for all. payments from patients and insurance companies fund basic operating expenses of the hos-pital, but they can’t cover the extra things that make St. Joseph’s special. that’s why the contributions we receive from patients, their families and other community mem-bers are so important.
Do you want to honor a loved one while helping future patients? Was there a nurse who touched your heart while you were a patient and you now would like to recog-nize him or her through a donation to St. Joseph’s College of nursing? Do you want to help ensure that future generations have access to advanced medical technology such as the davinci® robot or the hospital’s 64-slice Ct scanner?
to learn more about giving opportuni-ties, please call us at 315-703-2137 or visit our Web site at www.sjhsyr.org/foundation.
Help Us Help Others
www.sjhsyr.org l Spring 2009 l St. JoSeph’S hoSpital health Center l Caring ConneCtion 25
St. Joseph’s is more than a health care organization; it is a vital part of the Central New
York community. Not only do patients often remark that they feel they have “become
friends” with the nurses and clinical staff, but members of the St. Joseph’s family also find
that they frequently bond with patients and their families. Every day, we receive letters
from former patients and their family members who were so inspired by the quality of the
care received at St. Joseph’s Hospital Health Center that they take the time to write and
tell us. These letters mean so much to all of us at St. Joseph’s. The following letter from a
grateful patient touched our hearts.
Dear St. Joseph’s Hospital Staff:
Thank you! Thank you! Thank you!
You people are wonderful! My quadruple bypass on
Nov. 14, 2008, was a success, thanks to the wonderful
team of Dr. Nazem and all the wonderful nurses who
stood by me during those first critical three days after
my surgery. You were especially kind to my wife, Janet,
and my family—Brian, Holly and Cindy—by keeping them
informed of my progress. The care I received during my
stay with you made my recovery a breeze.
Today is Jan. 6, 2009. I am doing everything by the
book. I am feeling GReAT!!! I get home at night feeling
so good! It’s unbelievable to me that I had the major
surgery I did.
Again, St. Joseph’s staff: Thank you! Thank you!
Thank you! I tell everyone, “St. Joe’s is the only place in
Syracuse, NY, to have this type of work done!”
You are #1!
Again, thank you,
Timothy Lynn
Timothy Lynn
Syracuse, NY

a h i g h e r l e v e l o F C a r e
Success stories abound at St. Joseph’s Hospital. Not only does the hospital provide an environment filled with care and support for patients, St. Joseph’s College of Nursing does the same for its students. Nursing stu-dents come to the college from all corners of Central New York, the state and beyond. Most come with personal goals to help others while improving their own positions in life. The curriculum is challenging and the hours are long, but the majority succeed in their nursing programs. Generous philan-thropists provide funds that help to bring these goals into reach through scholarships, mentoring programs, dorm and classroom improvements, and other college capital and equipment needs.
Yailin oramas, RN, emigrated from Cuba to Texas where she joined her father
who had also come to the u.S. eventually, she relocated to Syracuse to live with her older sister and niece. oramas attended Nottingham High School and graduated in 2005. Throughout this time, her dream was to become a nurse like her mother.
This became a reality when she was accepted and enrolled into St. Joseph’s College of Nursing for the fall of 2005.
With no transportation of her own, oramas walked to the college from many miles away, sometimes having to arrive at the hospital before 7 a.m. eventually, when college faculty came to understand her cir-cumstances, her clinical instructor suggested she inquire about living in the residence hall. oramas soon moved into Marian Hall and not only went to school full time, but also began working as a student nurse aide as many hours as possible. Further, a long- lasting relationship was built between oramas and the college’s assistant dean for students, Nicole Blumin.
To her disappointment, working too many hours became a stumbling block and she had to repeat one of her courses. oramas also found herself wondering how she could earn enough money to continue to live in the residence hall. Yet, when the summer of 2006 arrived, she was awarded an alumni stipend that would allow her to remain. This scholarship allowed oramas to save enough money from working as a stu-dent nurse aide to pay her tuition and assist her family.
Changing to the Weekend Program in her second year, oramas worked full time and went to school every other weekend.
ultimately earning a 3.38 grade point aver-age with the Class of 2008, she just missed earning graduation with honors (3.4). She did, however, earn the Karen Loveland Payment Award. This scholarship, given by the family of Karen Loveland Payment, Class of 1976, is in memory of Payment, a staff nurse at St. Joseph’s Hospital Health Center for 19 years. This scholarship is awarded to a graduate who has demonstrated determina-tion and dedication in the face of significant obstacles or hardship in pursuit of a career in nursing. oramas says, “It came as quite a surprise and just as I opened the envelope and saw the check for $1,000, I knew that I would save it to go back to school.”
Her determination, combined with fund-ing from several college supporters, made it possible for her to tap into multiple college services. oramas was the recipient of two scholarships. While she attended St. Joseph’s, she participated in the mentor and student tutoring programs, received hands-on train-ing through the clinical learning lab, studied to improve her english language skills and graduated.
Now a u.S. citizen, oramas works on unit 1-5 and is preparing to pursue her bachelor of science degree, made possible by one of her two college scholarships. Grateful for the many opportunities St. Joseph’s and those who support the college have made available to her, she is thrilled to have realized her dream.
College CornerBeating Overwhelming Odds
Yailin oramas, RN
HAS yoUr lIFE BEEN ToUCHED By A NUrSE?
The quality of nursing at St. Joseph’s has been recognized as among the best in the nation. You can help ensure that it stays that way by contributing to the nursing programs and infrastructure needs at St. Joseph’s. Contact Connie Semel, BS, RN, ’74, director of development, St. Joseph’s College of Nursing, at 315-448-5303 or [email protected]. You may also use the enclosed donation envelope and write “College of Nursing” on your check.
26 Caring ConneCtion l St. JoSeph’S hoSpital health Center l Spring 2009 l www.sjhsyr.org

www.sjhsyr.org l Spring 2009 l St. JoSeph’S hoSpital health Center l Caring ConneCtion 27
you have questions.
We have answers!Q: “What is St. Joseph’s Hospital Foundation and what does it do?”
A: St. Joseph’s Hospital Foundation’s primary purpose is to raise funds to enhance patient care and comfort throughout St. Joseph’s network. Since 1976, the Foundation has worked to create a positive impact on the health of the community and Central New York region by identifying and developing projects, raising money and by care-fully managing the endowed funds entrusted to the Foundation. The Foundation raises funds to maintain primary care centers that serve uninsured and underserved families, to provide for patient comfort and care, for employee education, and for hospital pro-grams, technology, research and capital needs through several means which include:
lAnnual Golf Classic
lAnnual Gala
lAnnual Appeal
lendowments, including the St. Joseph’s Hospital endowment for Mission Services and St. Joseph’s Medical Technology endowment
lNaming opportunities for capital projects
lWalkways of Caring (inscribed benches and bricks)
lThe 1869 Society (a planned giving program)
lCircle of Caring (a membership program for St. Joseph’s supporters)
lApproved grants
Q: “How do I buy a brick or bench?”
A: At St. Joseph’s, engraved bricks and benches along the Hospital’s Walkways of Caring and the College of Nursing’s Caritas Park are read by thousands of people who visit the hospital each year. They become a part of the healing atmosphere that perm eates St. Joseph’s and their inscriptions carry messages of hope, love, dignity and caring. To purchase a brick or bench, honor a hero, support the hospital’s mission, express gratitude for a special nurse, or leave a message for future generations, please contact the Foundation at 315-703-2137. Additional information is also available online at the Foundation Web site: www.sjhsyr.org/foundation.
help us celebrate 17 years of successful St. Joseph’s golf tournaments on Sept. 11 at the Turning Stone
Resort & Casino. exclusively this year, both the world-class Shenendoah and Kaluhyat golf courses will be reserved for morning and afternoon shotgun starts for you to come “take your big swing!”
Not only will this be a day filled with fun and camara-derie, on-course contests and raffle drawings, but it also will be a day filled with plenty of food and refreshments. Golfers will start their day with a continental breakfast on the patio. For those teeing off in the morning, an awards ceremony and buffet lunch will be provided. Afternoon golfers will end their round with a cocktail reception, din-ner and an awards presentation. All tournament partici-pants are invited to attend the evening events. overnight accommodations will be available at a discounted rate.
Presenting sponsor of this year’s tournament is Franciscan Management Services.
St. Joseph’s Golf Classic is the largest charity golf event in Central New York. With your support, this year’s event is expected to be an even greater success!
So, take a swing in support of health care! Proceeds will be used to provide education and career development opportunities for the nursing staff and student nurses throughout the St. Joseph’s Hospital Health Center network.
To register to play or for sponsorship information, call the Foundation at 315-703-2137 or visit www.sjhsyr.org/foundation.
GOLF: Get Into the Swing!Friday, Sept. 11, 2009 n Turning Stone resort & CasinooNE DAy. TWo CoUrSES!
Planned Giving Pointer
2
Wondering What Planned Giving Is All About?
St. Joseph’s Hospital Foundation is always ready to explore with you, your family, and/or your financial advisor giving opportunities that would best suit your philanthropic and financial objectives. After all, determining which gift is a perfect fit for you is just as important as actually making it.
To learn about giving strategies that will allow you to make a meaningful charitable gift and how that might be of personal benefit for you as a donor, contact St. Joseph’s Hospital Foundation at 315-703-2137 or visit www.sjhsyr.org/foundation.

Community Relations Office301 Prospect Ave.
Syracuse, NY 13203
ADDRESS SERVICE REQUESTED
Non-Profit
Organization
US Postage Paid
Permit No. 3560
Syracuse, NY
St. Joseph’s Caring Connection is published by St. Joseph’s hospital health Center, 301 prospect ave., Syracuse, nY 13203. Copyright © 2009 by St. Joseph’s hospital health Center. all rights reserved. no part of this publication may be reproduced without prior written consent of St. Joseph’s hospital health Center.
if you know someone who would like to receive Caring Connection or be removed from our mailing list, contact the editor c/o St. Joseph’s Marketing/ Com mun ications office, 973 James St., Suite 245, Syracuse, nY 13203, or call 315-703-2140.
Denise Jochem-RobeRtson editor Manager, Marketing
maRgaRet maRtin vice president, Marketing, Communications and Development
Contact UsSt. Joseph’s Hospital Health Center301 Prospect Ave., Syracuse, NY 13203www.sjhsyr.org
General information . . . . . . . . . . 448-5111
Patient information . . . . . . . . . . 448-5113
Resource line (physician and program information). . . . . . . 703-2138
Foundation office (giving opportunities) . . . . . . . 703-2137
Marketing/Communications office . . . . . . . . . . . . . . . . . . . . 703-2140
College of nursing. . . . . . . . . . . . 448-5040
Volunteer office . . . . . . . . . . . . . 448-5186
All telephone numbers are in area code 315.
S t . J o S e p h ’ S
ConneCtionCaring
Intensive Care Unit Recognized for Excellence
For the second year in a row, St. Joseph’s Hospital Health Center’s
medical intensive care unit (MICu) has earned the Beacon Award for Critical Care excellence, placing it among the top ICus in New York state as well as the nation. St. Joseph’s is the only MICu in Central New York to win the award. only 120 intensive care units, out of approximately 6,000 across the country, have received the Beacon Award.
The American Association of Critical-Care Nurses (AACN) awards the Beacon to critical care units that achieve the highest quality patient outcomes possible as well as demonstrate excellence and innovation in patient care. The AACN evaluates units on criteria, including recruitment and reten-tion, leadership and organizational ethics, education, training and mentoring, as well as evidence-based practice. The American Association of Critical-Care Nurses is the largest specialty nursing organization in the world, representing the interests of more than 500,000 acute and critical care nurses.
St. Joseph’s MICu is a 15-bed critical care unit, specializing in the care of the critically ill patient, including those with cardiac dysfunctions, renal disease, respira-tory dysfunction and other medical illnesses that require critical care nursing support.
Smile—New Visitor Pass System in Place
A new visitor pass management system identifies and monitors visitors to
St. Joseph’s. Visitors who enter the hospi-tal’s main lobby now receive a visitor pass that includes their photo, destination, and date and time of their visit.
After hospital security staff and vol-unteers scan the visitor’s driver’s license, the visitor’s information is automatically entered into a database. A visitor pass is printed on a label that is then worn for the duration of the visit. The process takes only a few minutes. Previously, visitor pass infor-mation was written by hand without the help of the electronic database and photos were not included.
“We’ve had a good response from visi-tors,” says Tom Wentworth, security services coordinator. “I think everybody recognizes that this system is in place to help all of us.”
uP lTo lDATe
www.sjhsyr.org
resource line(physician & program
information)
315-703-2138


















