Omnimediakit011512 13268360381394 Phpapp02 120117153552 Phpapp02

of 58
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
1/58
CARE OF CLIENT IN
ACUTE BIOLOGIC
CRISIS
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
2/58
OBJECTIVESGiven relevant questions, the students will be able to discuss
triage and principles in emergency nursing care.
1. identify clinical situations where the client is in acute biologiccrisis
2. distinguish acute biologic crisis situations in terms of:
a. etiologic factors
b. pathophysiology
c. clinical manifestations and laboratory exams
d. complications
e. emergency treatment/management
3. Given a list of emergency drugs, the students will be able to:
4. match these drugs with their corresponding actions andtherapeutic uses
5. list common side effects and adverse reactions
6. enumerate dosage and dosage administration
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
3/58
OBJECTIVES
7. determine/identify health care problems basedon:
a. health history
b. physical examination
c. laboratory examinations
8.Formulate relevant nursing diagnosis
9. Discuss/demonstrate appropriate nursinginterventions
10. Evaluate outcome of health care
11. Verbalize appreciation on the influence ofChristian values in health care
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
4/58
DEFINITION
Emergency Management refers tocare given to patients with urgent andcritical needs. However, becausemany people lack access to healthcare, the emergency department isincreasingly used for non-urgentproblems. Therefore, the philosophy ofemergency management has
broadened to include the concept thatan emergency is whatever the patientor the family considers it to be.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
5/58
Scope and Practice of
Emergency Nursing
1. The emergency nurse has had specializededucation, training, experience, andexpertise in assessing and identifyingpatients health care problems in crisis
situations.
2. The emergency nurse establishes priorities,monitors and continuously assesses acutelyill and injured patients, supports and attends
to families, supervises allied healthpersonnel, and teaches patients and familieswithin a time-limited, high-pressured careenvironment
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
6/58
3. Nursing interventions are accomplished interdependently, inconsultation with or under the direction of a physician or nursepractitioner. The strengths of medicine and nursing arecomplementary in an emergency situation. Appropriatenursing and medical interventions are anticipated based onassessment data. The emergency health care staff memberswork as a team in performing the highly technical hands-onskills required to care for patients in emergency situations.
4. Patients in the ER have a wide variety of actual or potentialproblems, and their condition may change constantly.Therefore, nursing assessment must be continuous, andnursing diagnoses change with the patients condition.Although a patient may have several diagnoses at a giventime, the focus is on the most life-threatening ones; often both
independent and interdependent nursing interventions arerequired.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
7/58
Issues in Emergency Nursing
Care1. Documentation of Consent and Privacy
2. Limiting Exposure to Health Risks
3. Violence in the Emergency Department
a. Safety is the first priority. Protection of the
department provides protection for the patients,families, and staff.
b. Metal detectors, silent alarm systems, and securedentry into the department assists in maintainingsafety.
c. Members of gangs and feuding families need to beseparated in the ER, waiting room and later in theward to avoid angry confrontations
d. Security personnel should be ready to assist at alltimes. The ER should be able to be locked against
entry if security is at all in question.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
8/58
Issues in Emergency Nursing Care
e. Patients from prison and those who are under guard need to behandcuffed to the bed and appropriately assessed to ensure thesafety of the hospital staff and other patients.
e.1. never release the hand or ankle restraint (handcuff)
e.2. always have a guard present in the room.
e.3 place the patient face down on the stretcher to
avoid injury from head-butting, spitting, or biting.
e.4 use restraints on any violent patient as needed.
e.5. administer medication if necessary to control
violent behavior until definitive treatment can be
obtained.
f. In the case of gunfire in the ER, self-protection is a priority.There is no advantage to protecting others if the caregivers arealso injured. Security officers and police must gain control of thesituation first, and then care is provided to the others.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
9/58
Issues in Emergency Nursing Care
4. Providing Holistic Carea. patient-focused interventions
the unconscious patient should be treated as ifconscious; that is, the patient should be touched,
called by name, and given an explanation of everyprocedure that is performed.
b. Family-focused interventions
The family is kept informed about where the patient is,how he/she is doing, and the care that is being given.
Allowing the family to stay with the patient, whenpossible also helps allay their anxieties
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
10/58
Guidelines in Helping Family Members
Cope with Sudden Death
1. Take the family to a private place.
2. Talk to the family together, so that they can mourntogether.
3. Reassure the family that everything possible was done;
inform them of the treatment rendered.4. Avoid using euphemisms such as passedon. Show the
family that you care by touching, offering coffee, water,and the services of the chaplain.
5. Encourage family members to support each other and toexpress emotions freely (grief, loss, anger,helplessness, tears, disbelief).
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
11/58
6. Avoid giving sedation to family members; this may maskor delay the grieving process, which is necessary to
achieve emotional equilibrium and to prevent prolongeddepression.
7. Encourage the family to view the body if they wish; thisaction helps to integrate the loss. Cover disfigured andinjured areas before the family sees the body. Go with
the family to see the body. Show acceptance by touchingthe body to give the family permission to touch.
8. Spend time with the family members to talk about thedeceased and what he/she meant to them; this permitsventilation of feelings of loss. Encourage the family to
talk about events preceding admission to the ER. Do notchallenge initial feelings of anger and denial.
9. Avoid volunteering unnecessary information (e.g., thepatient was drinking)
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
12/58
Principles of Emergency Care
By definition, emergency care is care thatmust be rendered without delay. In an ER,several patients with diverse health problems-some life threatening, some not may present
to the ED simultaneously. One of the firstprinciples of emergency care is triage.
TRIAGE comes from the French word trier,
meaning to
sort.
In the daily routine of the ER,triage is used to sort patients into groups basedon the severity of their health problems and theimmediacy with which these problems must betreated.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
13/58
Systems
Categories
1. Emergent patients have the highest priority theirconditions are life-threatening and they must be seenimmediately.
2. Urgent patients have serious health problems but notimmediately life-threatening ones; they must be seenwithin 1 hour.
3. Nonurgent patients have episodic illnesses that can beaddressed within 24 hours without increased morbidity.
4. Fast Track patients require simple first aid or basicprimary care and may be treated in the ER or safelyreferred to a clinic orphysicians office
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
14/58
Triage SystemsLevels
1. Resuscitation patients need treatment immediately to prevent
death.2. Emergent - patients may deteriorate rapidly and develop a major
life threatening situation or require time-sensitive treatment.
3. Urgent Patients have non-life threatening conditions but requiretwo or more resources to provide their care. If the patients vitalsigns deviate significantly from their baseline, they may require
up-triaging to the emergent category.4. Nonurgent- patients have non-life threatening conditions and likely
need only one resource to provide for their needs.
5. Minor category patients have no life-threatening conditions andlikely require no resources to provide their evaluation andmanagement.
Resources are defined as imaging studies, medicationsadministered IV or IM routes, and invasive procedures. Insertionof an indwelling catheter is an example of a one-resourceprocedure. Moderate sedation would be classified as a two-resource procedure because this requires frequent monitoringand IV medications.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
15/58
QUESTIONS - ER
The following questions reflect the minimum information thatshould be obtained from the patient or from the personwho accompanied the patient to the ER:
1. What were the circumstances, precipitating events, locationand time of the injury or illness?
2. When did the symptoms appear?
3. Was the patient unconscious after the injury or onset ofillness?
4. How did the patient get to the ER?
5. What was the health status of the patient before the injury orillness?
6. Is there a history of medical illness or previous surgeries? Ahistory of admissions to the hospital?
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
16/58
7. Is the patient currently taking any medications,
especially hormones, insulin, digitalis oranticoagulants?
8. Does the patient have any allergies, especiallyto eggs, latex, medications, or nuts?
9. Does the patient have any fears? Does thepatient feel that he or she is in a situation inwhich he/she is unsafe?
10. When was the last meal eaten?
11. When was the LMP?
12. Is the patient under a physicians care? Whatare the name and location of the physician?
13. What was the date of the patents most recenttetanus immunization?
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
17/58
Assess and Intervene A systematic approach to effectively establish and treat
health priorities is the primary / secondary approach.The primary survey focuses on stabilizing life-threatening conditions. The ER staff workcollaboratively and follow the ABCD (airway, breathing,circulation, disability method:
1. Establish a patent airway.
2. Provide adequate ventilation, employing resuscitationmeasures when necessary. (trauma patients musthave the cervical spine protected and chest injuriesassessed first).
3. Evaluate and restore cardiac output by controllinghemorrhage, preventing and treating shock, andmaintaining or restoring effective circulation. Thisincludes the prevention and management ofhypothermia.
4. Determine neurologic disability by assessing neurologic
function using the Glasgow Coma Scale.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
18/58
Secondary Survey
After these priorities have been addressed, the ER teamproceeds with the secondary survey. This includes thefollowing:
1. A complete health history and head-to-toe assessment
2. Diagnostic and laboratory testing3. Insertion or application of monitoring devices such as
ECG electrodes, arterial lines, or urinary catheters.
4. Splinting of suspected fractures
5. Cleansing, closure, and dressing of wounds6. Performance of other necessary interventions based on
the patients condition.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
19/58
SHOCK
Is a syndrome in which the circulation orperfusion of blood is inadequate to meettissue metabolic demands. Cellular anoxiawill ensue and lead to tissue death unless
the process is reversed.
During shock, the body struggles to survive,
calling on all its homeostatic mechanism torestore blood flow
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
20/58
Classifications of Shock
1. Hypovolemic shock refers to a state in which the volumecontained within the intravascular compartment isinadequate for perfusion of body tissue. There is usually a15%-25% reduction of intravascular volume.
e.g., hemorrhagic shock loss of whole blood about 1/3 of
his normal blood volume2. Cardiogenic shock which occurs when the heart has an
impaired pumping ability; it may be of coronary ornoncoronary event origin.
3. Septic shock- which is caused by an infection
4. Neurogenic shock- which is caused by alterations in vascularsmooth muscle tone, caused by either nervous systeminjury or complications associated with medications such asepidural anesthesia.
5. Anaphylactic shock which is caused by hypersensitivityreaction.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
21/58
Stages of Shock
1. Compensatory stage
the BP remains normal.
Vasoconstriction , increased HR, and
increased contractility of the heart stimulation of the SNS and subsequent
release of cathecolamines.
The body shunts blood from organs to the
brain and heart
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
22/58
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
23/58
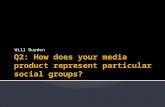
Compensatory Mechanism in Shock
Initial physiologic insult to shock state
Decrease in CO and tissue perfusion
SNS activation
Endocrine response
RAA activation
Vasoconstriction and activation of ADH - Preload
BP, HR, and Myocardial contractility Renal system conserves Na and H2O - Preload
vascular compliance, blood volume and CO
Restoration of tissue perfusion
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
24/58
Medical Management
1. identifying the cause of the shock, correcting
the underlying disorder so that shock does
not progress, and supporting those
physiologic processes that thus far haveresponded successfully to threat.
2. Fluid replacement and medication therapy
must be initiated to maintain an adequate BP
and reestablish and maintain adequate tissueperfusion.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
25/58
Nursing Management
1. Monitoring Tissue Perfusion
a.assess the patient at risk for shock systematically torecognize the subtle clinical manifestations of thecompensatory stage before the patients BP drops
b. Observe for changes in LOC, VS, urinary output, skinand laboratory values
c. Administer prescribed fluids and medications.
2. Reducing anxietya. provide brief explanations about the diagnostic and
treatment proceduresb. Speaking in a calm, reassuring voice and using
gentle touch also help ease the patients concerns.
3. . Promoting safety
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
26/58
2. Progressive Stage
the mechanisms that regulate BP can
no longer compensate
MAP (mean arterial pressure) falls
below normal limits.
Patients are clinically hypotensive; this
is defined as a SBP of
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
27/58
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
28/58
Assessment and Diagnostic
Findings
1. Respiratory Effects decompensation of the lungs increases the
likelihood that mechanical ventilation will beneeded.
Respirations are rapid and shallow; crackles areheard over the lung fields.
Decreased pulmonary blood flow causes arteriolarO2 levels to decrease and CO2 levels to increase.
The hypoperfused alveoli stop producing surfactant
and subsequently collapse. Pulmonary capillaries begin to leak, spilling their
contents, thus causing pulmonary edema, diffusionabnormalities (shunting), and additional alveolarcollapse.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
29/58
Assessment and Diagnostic
Findings
2. Cardiovascular Effect - ischemia and dysrhythmiadue to lack of adequate blood supply, the HR is rapid,sometimes exceeding 150 bpm. The patient may complain ofchest pain and even suffer a myocardial infarction.
Levels of cardiac enzymes increase. myocardial depression and ventricular dilation may further impair
the hearts ability to pump enough blood to the tissues to meetoxygen requirements.
3. Neurologic Effects- mental status deteriorates and occur withdecreased tissue perfusion and hypoxia. Initially, patient mayexhibit a subtle change in behavior or agitation and confusion.Subsequently, lethargy increases, and the patient begins to loseconsciousness.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
30/58
Assessment and Diagnostic
Findings3. Hepatic effects decreased blood flow to the liver impairs
the ability of the liver cells to perform metabolic andphagocytic functions. The patient is less able tometabolize medications and metabolic waste products,such as ammonia and lactic acid.
Metabolic activities of the liver (gluconeogenesis andglycogenolysis) are impaired. The patients become moresusceptible to infection as the liver fails to filter bacteriafrom the blood.
Liver enzymes and bilirubin levels are elevated and the
patient appears jaundiced.4. Renal Effects GFR decreases. ARF may develop
(increased BUN, crea), fluid and electrolytes shift, acid-base imbalances and a loss of renal-hormonal regulationof BP.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
31/58
Assessment and Diagnostic
Findings
5. GI effects can cause stress ulcers in the
stomach, putting the patient at risk for GI
bleeding. In the small intestine, the mucosa can
become necrotic and slough off, causing bloody
diarrhea.
6. Hematologic Effects the combination of
hypotension, sluggish blood flow, metabolic
acidosis, coagulation system imbalance, and
generalized hypoxemia can interfere with normalhemostatic mechanism.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
32/58
Medical Management
Will depend on the specific type of shock and itsunderlying cause. It also depends on the degree ofdecompensation in the organ system
1. optimizing intravascular volume
2. supporting the pumping action of the heart3. improving the competence of the vascular system
4. supporting the respiratory system
5.Early enteral nutritional support, aggressive
hyperglycemic control with IV insulin and use ofantacids, H2 receptor blockers or antipeptic agents toreduce the risk of GI ulceration and bleeding.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
33/58
Nursing Management
1. Preventing complicationsa. monitor the patient for early signs of complications.
It includes evaluating blood levels of medications,observing invasive vascular lines for signs ofinfection, and checking neurovascular status ifarterial lines are inserted.
b. frequent oral care, aseptic suction technique,turning, and elevating the head of the bed toprevent aspiration.
c. positioning and repositioning of the patient to promotecomfort and maintain skin integrity.
2. Promoting Rest and comfort to minimize thecardiac workload.
3. Supporting family members
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
34/58
3. Irreversible (refractory) Stage represents thepoint along the shock continuum at whichorgan damage is so severe that the patientdoes not respond to treatment and cannot
survive
Medical Management:
Is usually the same as for the progressive
stage. Strategies that may be experimentalmay be tried to reduce or reverse the severityof shock.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
35/58
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
36/58
Nursing Management
1. carry out prescribed treatments, monitoring the patient,preventing complications, protecting the patient from injury,and providing comfort.
2. Offer brief explanations to the patient about what ishappening is essential even if there is no certainty that thepatient hears or understands what is being said.
3. Simple comfort measures, including reassuring touches,should continue to be provided despite the patientsnonresponsiveness to verbal stimuli.
4. As it becomes obvious that the patient is unlikely to survive,the family must be informed about the prognosis and likely
outcome.5. Opportunities should be provided, throughout the patientscare, for the family to see, touch, and talk to the patient.
6. Close family friends or spiritual advisors may be of comfortto the family members in dealing with the inevitable deathof their loved one.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
37/58
Overall Management Strategies in Shock
1. Fluid replacement to restoreintravascular tone
Crystalloid
NSS LRs
Colloid Solutions
Dextran
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
38/58
Overall Management Strategies in
ShockComplications of Fluid Administration The most common and serious side effects of fluid
replacement are cardiovascular overload andpulmonary edema.
Management:1. Monitor frequently the urine output, changes in mental status, skin
perfusion, and changes in vital signs.
2. Lung sounds are auscultated frequently to detect signs fluidaccumulation. Adventitious lung sounds, such as crackles mayindicate pulmonary edema.
3. A CVP may be inserted to monitor the patients response to fluid
replacement.4. Vasoactive medications to restore vasomotor tone and improve cardiac
function.
5. Nutritional support to address the metabolic requirements that are oftendramatically increased in shock. Patient in shock may require 3000calories daily. The release of catecholamines early in shockcontinuum causes depletion of glycogen stores in about 8-10 hours.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
39/58
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
40/58
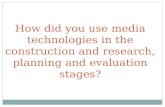
Risk Factors for Hypovolemic
Shock
A. External: Fluid Losses B. Internal: Fluid Shifts
1. Trauma 1. Hemorrhage
2. Surgery 2. Burns
3. Vomiting 3. Ascites
4. Diarrhea 4. Peritonitis
5. Diuresis 5. Dehydration
6. Diabetes Insipidus
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
41/58
Medical Management
Goals:
1. restore intravascular volume to reverse thesequence of events leading to inadequatetissue perfusion
2. redistribute fluid volume3. correct the underlying cause of the fluid loss
as quickly as possible.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
42/58
Hypovolemic Shock
Interventions:1. Treatment of the underlying cause
a. If hemorrhaging, applying pressure to thebleeding site or surgery to stop bleeding.
b. If due to diarrhea or vomiting, medications totreat diarrhea and vomiting are administeredwhile efforts are made to identify and treatthe cause
2. Fluid and Blood replacement
3. Redistribution of fluid
4. Pharmacologic therapy
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
43/58
Nursing Management
1. Administering blood and Fluid safely
2. Implementing other measures
a. oxygen is administered to increase the
amount of oxygen carried by available
hemoglobin in the blood.
b. The nurse must direct efforts to the safety
and comfort of the patient.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
44/58
CARDIOGENIC SHOCK
Occurs when the hearts ability to contract and to pumpblood is impaired and the supply of oxygen isinadequate for the heart and tissues
Types:
1. Coronary cardiogenic shock occurs when a significantamount of the left ventricular myocardium has beendamaged.
2. Noncoronary cardiogenic shock are related toconditions that stress the myocardium (e.g., severehypoxemia, acidosis, hypoglycemia, hypocalcemia,
and tension pneumothorax) as well as conditions thatresult in ineffective myocardial function (e.g.,cardiomyopathies, valvular damage, cardiactamponade, dysrhythmias)
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
45/58
Pathophysiology
Decreased cardiac contractility
Decreased stroke volume and cardiacoutput
Pulmonary congestion Decreased systemic tissue perfusion decreased coronary artery perfusion
Clinical Manifestations: Patients in cardiogenic shock mayexperience the pain of angina and develop dysrhythmiasand hemodynamic instability.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
46/58
Medical Management1. Correction of underlying cause
a. In the case of coronary cardiogenic shock, the patient may require thrombolytic
therapy, angioplasty, CABG, intra-aortic balloon pump therapy, or somecombination of these treatments.
b. In the case of noncoronary cardiogenic shock, interventions focus on correctingthe underlying cause, such as replacement of a faulty cardiac valve,correction of dysrhythmias, correction of acidosis and electrolytedisturbances, or treatment of the tension pneumothorax.
2. Initiation of First-Line treatmenta. supplying supplemental oxygen
b. controlling chest pain
c. providing selected fluid support
d. administering vasoactive medications
e. controlling HR with medication or by implementation of a transthoracic IVpacemaker.
3. Oxygenation via nasal cannula at 2-6 lpm
4. Pain control IV morphine sulfate.
6. Laboratory marker monitoring (cardiac enzymes)
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
47/58
Nursing Management
1. Preventing cardiogenic shocka. conserve patients energy
b. restore adequate cardiac function and tissueperfusion
2. Monitoring hemodynamic status:a. arterial lines
b. ECG
c. Cardiac, pulmonary and laboratory values
3. Administering medications and IV Fluids4. Maintaining Intra-aortic balloon counterpulsation
5. Enhancing safety and comfort
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
48/58
CIRCULATORY SHOCK
Occurs when blood volume is abnormallydisplaced in the vasculature (e.g., when bloodpools in peripheral blood vessels). Circulatoryshock can be caused either by a loss of
sympathetic tone or by release of biochemicalmediators from cells.
Classifications:
1. Septic shock2. Neurogenic shock
3. Anaphylactic shock
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
49/58
Pathophysiology
Precipitating event
Vasodilation
Activation of inflammatory response
Misdistribution of blood volume
Decreased venous return
Decreased cardiac output
Decreased tissue perfusion
Ri k F t f Ci l t Sh k
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
50/58
Risk Factors for Circulatory Shock
1. Septic Shock
a. Immunosuppressionb. Extremes of age (< 1 yr and > 65 yr)
c. Malnourishment
d. Chronic illness
e. Invasive procedures
2. Neurogenic Shock
a. Spinal cord injuryb. Spinal anesthesia
c. Depressant action of medications
d. Glucose deficiency
3. Anaphylactic Shock
a. Penicillin sensitivity
b. Transfusion reaction
c. Bee sting allergy
d. Latex sensitivity
e. Severe allergy to some foods or medications
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
51/58
Septic Shock
Septic Shock: shock associated with sepsis; characterized bysymptoms of sepsis plus hypotension and hypoperfusion despiteadequate fluid volume replacement
Medical Management:
1. Identification of the cause of infection. Specimens of blood, sputum,urine, wound drainage, and tips of invasive catheters are collected
for culture using aseptic technique.2. Any potential source must be eliminated. IV lines are removed and
reinserted at other body sites. Antibiotic-coated IV central linesmay be inserted to decrease the risk of invasive line-relatedbacteremia in high risk patients, such as elderly.
3. Fluid replacement must be instituted to correct the hypovolemia that
results from incompetent vasculature and the inflammatoryresponse.
4. Pharmacologic therapy.
5. Nutritional therapy
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
52/58
Nursing Management
1. All invasive procedures must be carried out withaseptic technique.
2. Monitor patient for signs of infection.
3. Administer prescribed IV fluids and medications,
including antibiotic agents and vasoactivemedications to restore vascular volume.
4. Laboratory values must be monitored.
5. Monitor hemodynamic status
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
53/58
Neurogenic Shock
vasodilation occurs as a result of a loss of balancebetween parasympathetic and sympathetic stimulation.The patient experiences a predominantparasympathetic stimulation that causes vasodilationlasting for an extended period leading to a relative
hypovolemic state. However, blood volume is adequate,because the vasculature is dilated; the blood volume isdisplaced, producing hypotensive state resulting to adrastic decrease in the patients systemic vascularresistance and bradycardia. Inadequate BP results inthe insufficient perfusion of tissues and cells.
Causes:1. Spinal cord injury, spinal anesthesia, or nervous system
damage.
2. Depressant effect of medications or from lack ofglucose.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
54/58
Medical Management
1. restoring sympathetic tone, either through
stabilization of a spinal cord injury or, in
the instance of spinal anesthesia, by
positioning the patient properly.2. If hypoglycemia is the cause, glucose is
rapidly administered
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
55/58
Nursing Management
1. Elevate and maintain the head of the bed elevated at least 30degrees to prevent neurogenic shock when a patient receivesspinal or epidural anesthesia. Elevation of the head helps preventthe spread of the anesthetic agent up to the spinal cord.
2. In suspected spinal cord injury, neurogenic shock may be preventedby carefully immobilizing the patient to prevent further damage to
the spinal cord.3. Support CV and neurologic function until the usually transient
episode of neurogenic shock resolves. Applying elasticcompression stockings and elevating the foot of the bed mayminimize the pooling of blood in the legs
4. Administration of heparin or LMWH (Lovenox) as prescribed,
application of elastic compression stockings, or use of pneumaticcompression of the legs may prevent thrombus formation.
5. Passive ROM of the immobile extremities helps promote circulation.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
56/58
Anaphylactic Shock
occurs rapidly and is life-threatening. Becauseanaphylactic shock occurs in patients alreadyexposed to an antigen and who have developedantibodies to it, it can often be prevented
It is caused by a severe allergic reaction when patientswho have already produced antibodies to a foreignsubstance (antigen) develop a systemic antigen-antibody reaction.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
57/58
Medical Management
1. removal of the causative antigen2. Epinephrine is given for its vasoconstrictive effect.
3. Diphenhydramine (Benadryl) is administered to reverse theeffects of histamine, thereby reducing capillary permeability.
4. Nebulized medications such as albuterol (Proventil), may begiven to reverse histamine-induced bronchospasm.
5. If cardiac and respiratory arrests are imminent or have occurred,CPR is performed. Endotracheal intubation or tracheotomymay be necessary to establish an airway.
6. IV lines are inserted to provide access for administering fluidsand medications.
Nursing Management: assess patient for allergies or previous reactions to antigens (e.g.,medications, blood products, foods, contrast agents, latex) andcommunicate the existence of allergies or reactions to others.
7/30/2019 careofpatientinacutebiologiccrisis2-101010004444-phpapp02
58/58