Inappropriate Payments for Total Parenteral Nutrition (TPN) (OEI-12 ...
description

1
CARE OF THE PATIENT
RECEIVING
TOTAL PARENTERAL NUTRITION (TPN)
General Surgery
North York General Hospital
Revised July 2013.

2T A B L E O F C O N T E N T S
Introduction 3
Learning Objectives 3
Competency Process 3
What is TPN? 4
Indications for TPN administration 4
Composition of TPN solutions 5
Access routes for TPN administration 6
TPN Administration 8
Fluid management with TPN 9
Monitoring during TPN administration 10
Complications associated with TPN therapy 14
Documentation of TPN administration 18
References 26
TPN Post-Test 27

3INTRODUCTION
Total parenteral nutrition (TPN) is the provision of intravenous nutrients to patients whose
gastrointestinal (GI) tract is not functioning or cannot be accessed and to patients whose nutritional needs
cannot be met with oral diets or enteral feeding. The patient receives a combination of nutrients- crystalline
amino acids, dextrose, electrolytes, vitamins, minerals, trace elements and lipid/fat emulsion administered
intravenously.
Once limited to critical care areas, TPN is now present on post surgical floors and medical units, when
feeding by mouth is not possible, when a person's digestive system cannot absorb nutrients due to chronic
disease, or, alternatively, if a person's nutritional requirements cannot be met by enteral feeding (tube
feeding) and/or through oral diet.
Caring for patients receiving TPN requires additional knowledge and skill. This learning package has
been developed to provide information to nursing staff caring for patients receiving TPN for nutritional
support.
LEARNING OBJECTIVES
The Registered Nurse/Registered Practical Nurse will be able to:
1. Define the term TPN and state indications for administration.
2. Describe the composition of the TPN solution and the rationales for each solution.
3. Identify the access routes for administration of TPN.
4. Describe the assessments involved for patients on TPN.
5. State how to administer TPN and monitor the delivery of TPN.
6. State the complications associated with TPN administration.
7. State how to document TPN administration interventions.
8. Understand the collaborative multidisciplinary approach of TPN therapy.
COMPETENCY PROCESS
1) Review of self-directed learning package.
2) Complete and obtain a minimum of 80% on the TPN post-test.
3) Attend a lecture/review session with CNE and perform TPN administration competency in simulated
environment.
4) Perform one return demonstration of TPN administration on actual patient.

4WHAT IS TPN?
Total parental nutrition (TPN) is the practice of nourishing a patient intravenously, bypassing the usual
process of eating and digestion. It is a form of specialized nutrition, including amino acids, dextrose, fat
emulsion, vitamins, minerals and trace elements given intravenously.
The TPN solution is osmotically active and must be administered carefully to prevent trauma to the
vascular portal of entry. It is administered intravenously and can be administered through a peripherally
inserted central catheter (PICC), a central venous line (CVC) or a large peripheral line. In order to administer it
carefully, TPN is ALWAYS administered through an infusion pump. The sterile bags of nutrients are infused
continuously through the pump over a 12 hour or 24 hour period to prevent vascular trauma and metabolic
instability.
INDICATIONS FOR TPN ADMINISTRATION
TPN is administered for various reasons and over varying periods of times. TPN support is prescribed if
there is intolerance to oral intake or enteral feeds and if the patient is NPO for an extended period of time.
This is usually 3 days if the patient is moderately to severely malnourished or 7 days if the patient is well
nourished or mildly malnourished. Short-term TPN (7 to 10 days) or long-term TPN (>10 days) is used to treat
patients whose GI tract is not functioning or not accessible for various reasons.
Below is a chart which identifies the conditions where TPN administration is commonly prescribed.
Chart 1: Indications for TPN administration
PHYSIOLOGICAL
CONDITION
CLINICAL MANIFESTATION
Non functional
GI tract
• Massive small bowel resection/ GI surgery
• Paralytic ileus
• Small bowel ileus (dilated bowel with air/fluid levels on CT scan)
• Intestinal obstruction
• Trauma to abdomen, head , neck
• Severe malabsorption
• Intolerance to enteral feeding (protracted nausea/vomiting)
• Bowel infarction/bowel ischemia
• Chemotherapy, radiation therapy, bone marrow transplant
• High output small bowel fistula >500ml/d
• Mechanical small bowel obstruction
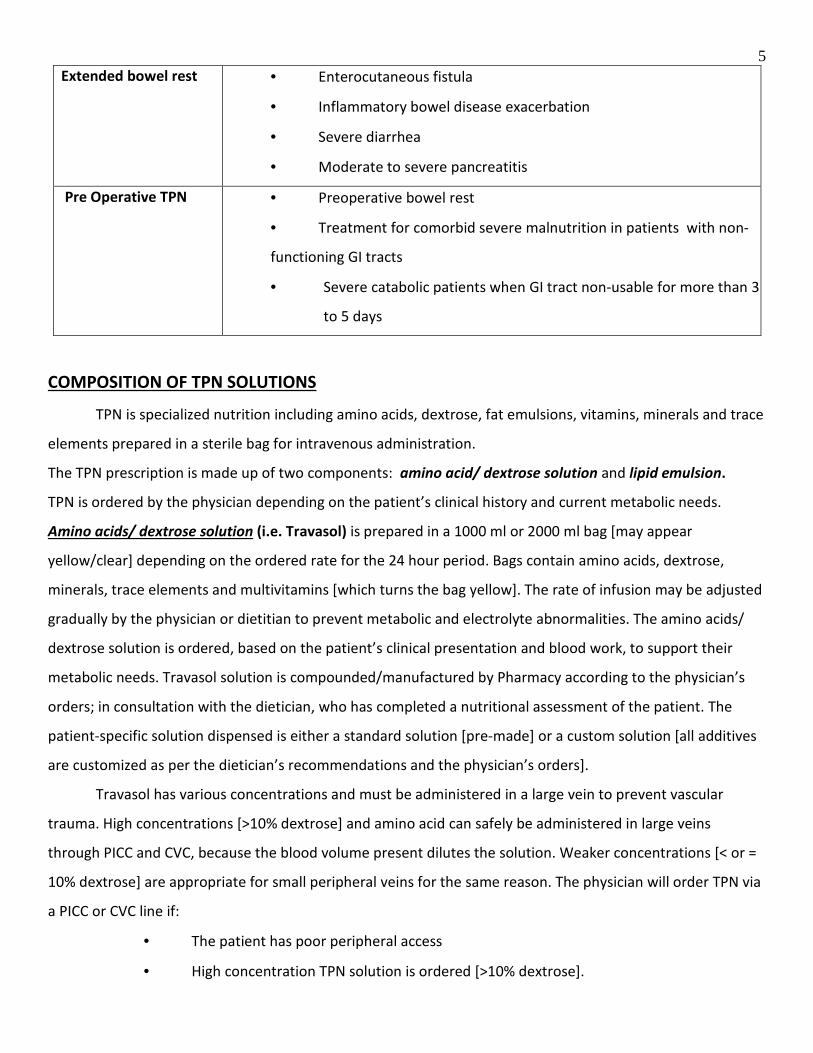
5 Extended bowel rest
• Enterocutaneous fistula
• Inflammatory bowel disease exacerbation
• Severe diarrhea
• Moderate to severe pancreatitis
Pre Operative TPN
• Preoperative bowel rest
• Treatment for comorbid severe malnutrition in patients with non-
functioning GI tracts
• Severe catabolic patients when GI tract non-usable for more than 3
to 5 days
COMPOSITION OF TPN SOLUTIONS
TPN is specialized nutrition including amino acids, dextrose, fat emulsions, vitamins, minerals and trace
elements prepared in a sterile bag for intravenous administration.
The TPN prescription is made up of two components: amino acid/ dextrose solution and lipid emulsion.
TPN is ordered by the physician depending on the patient’s clinical history and current metabolic needs.
Amino acids/ dextrose solution (i.e. Travasol) is prepared in a 1000 ml or 2000 ml bag [may appear
yellow/clear] depending on the ordered rate for the 24 hour period. Bags contain amino acids, dextrose,
minerals, trace elements and multivitamins [which turns the bag yellow]. The rate of infusion may be adjusted
gradually by the physician or dietitian to prevent metabolic and electrolyte abnormalities. The amino acids/
dextrose solution is ordered, based on the patient’s clinical presentation and blood work, to support their
metabolic needs. Travasol solution is compounded/manufactured by Pharmacy according to the physician’s
orders; in consultation with the dietician, who has completed a nutritional assessment of the patient. The
patient-specific solution dispensed is either a standard solution [pre-made] or a custom solution [all additives
are customized as per the dietician’s recommendations and the physician’s orders].
Travasol has various concentrations and must be administered in a large vein to prevent vascular
trauma. High concentrations [>10% dextrose] and amino acid can safely be administered in large veins
through PICC and CVC, because the blood volume present dilutes the solution. Weaker concentrations [< or =
10% dextrose] are appropriate for small peripheral veins for the same reason. The physician will order TPN via
a PICC or CVC line if:
• The patient has poor peripheral access
• High concentration TPN solution is ordered [>10% dextrose].

6The ingredients are individually listed on the bag and must be verified with the physician’s order on
the eMAR by the nurse hanging the bag, following the 8 rights of medication administration. In addition the
bag will be scanned with Caremobile (see pages 21 & 22).
Lipid emulsions are prepared in 100 ml or 250 ml bags and contains essential fatty acids [appears milky]. Lipid
emulsions are ordered to prevent fatty acid deficiency that causes scaly dermatitis, alopecia,
thrombocytopenia, and growth retardation in children.
At NYGH, lipids are dispensed in 20% solutions and are commonly run over a 12 hour period only.
Remove the bag from the sealed package, verify the physician’s order on the eMAR, including the rate of
administration, fill in the label provided including the rate, date/time and your initials. The bag will also be
scanned with the Caremobile (see pages 21 & 22).
ACCESS ROUTES FOR TPN ADMINISTRATION
TPN solutions must be carefully administered intravenously because it is osmotically active and can
cause trauma to the vascular portal of entry. For this reason, TPN is best administered through a large vein
and at NYGH; the preferred route for administration is through a PICC. A PICC is a peripherally inserted central
catheter which is inserted into the basilic, brachial or cephalic veins in the upper arm. A CVC may also be used
for TPN administration. A CVC is a multi-lumen central venous catheter inserted into the subclavian and
internal jugular vein. Alternately, if neither site is available, a large peripheral site maybe used to administer
TPN. If a peripheral IV is to be used, only dilute concentrations of TPN [< or =10% dextrose] can be
administered. Once an intravenous line is used for TPN nothing else can be administered through that line.
Large venous catheters such as PICC and CVC lines are inserted by physicians, radiologists or certified
RNs in the radiology department ONLY. Radiology is opened from Mondays to Fridays 0800 to 1600 hours. If
an order for TPN administration occurs outside of these hours [i.e. evenings, weekends and holidays], a large
peripheral IV may be used to start dilute concentrations of TPN instead.

7Below is a chart which summarizes the access routes and TPN administration plan of care.
Chart 2: Access routes and TPN administration plan of care
ACCESS TYPE PLAN OF CARE
PICC (PERIPHERALLY
INSERTED CENTRAL
VENOUS CATHETER)
• Catheterization of central venous system through the basilic or
cephalic vein [in the arm], advanced into basilica or cephalic vein, then
threaded up toward the heart into the right subclavian vein
• Inserted when TPN is expected to run > 1 week in patients who are
at high risk for phlebitis
CVC (CENTRAL
VENOUS CATHETER)
• Catheterization of subclavian or internal jugular vein
• Catheter related complications: sepsis, pneumothorax, embolism
• Solutions to infuse- either central or peripheral solutions
• Inserted when peripheral veins are unsuitable
PERIPHERAL
INTRAVENOUS
CATHETER
• Uses arm veins
• Solutions to infuse only < or =10% dextrose solution
-consider phlebitis of vein
Inserted when TPN expected to run less than 2 weeks & peripheral access is
“reasonable”
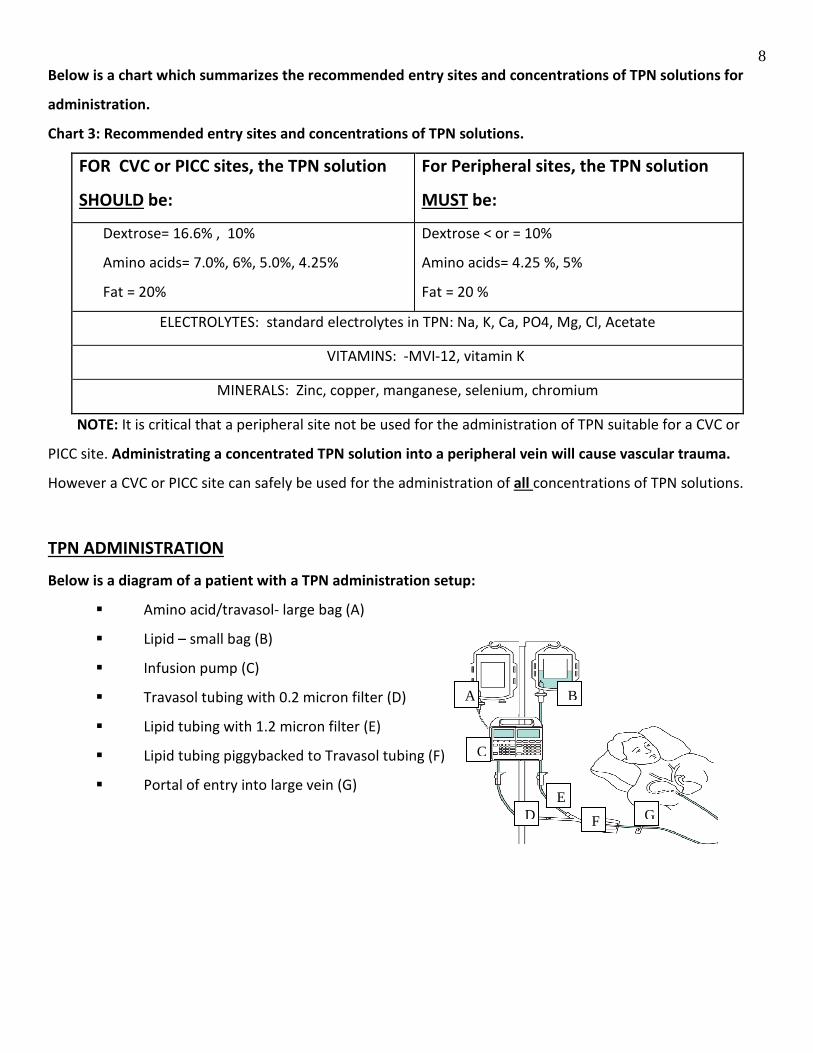
8Below is a chart which summarizes the recommended entry sites and concentrations of TPN solutions for
administration.
Chart 3: Recommended entry sites and concentrations of TPN solutions.
FOR CVC or PICC sites, the TPN solution
SHOULD be:
For Peripheral sites, the TPN solution
MUST be:
Dextrose= 16.6% , 10%
Amino acids= 7.0%, 6%, 5.0%, 4.25%
Fat = 20%
Dextrose < or = 10%
Amino acids= 4.25 %, 5%
Fat = 20 %
ELECTROLYTES: standard electrolytes in TPN: Na, K, Ca, PO4, Mg, Cl, Acetate
VITAMINS: -MVI-12, vitamin K
MINERALS: Zinc, copper, manganese, selenium, chromium
NOTE: It is critical that a peripheral site not be used for the administration of TPN suitable for a CVC or
PICC site. Administrating a concentrated TPN solution into a peripheral vein will cause vascular trauma.
However a CVC or PICC site can safely be used for the administration of all concentrations of TPN solutions.
TPN ADMINISTRATION
Below is a diagram of a patient with a TPN administration setup:
� Amino acid/travasol- large bag (A)
� Lipid – small bag (B)
� Infusion pump (C)
� Travasol tubing with 0.2 micron filter (D)
� Lipid tubing with 1.2 micron filter (E)
� Lipid tubing piggybacked to Travasol tubing (F)
� Portal of entry into large vein (G)
A
C
E D F
B
G

9TPN is NOT compatible with any other solutions and must be administered by itself. A dedicated
intravenous line should be labeled for TPN use only.
There are two different IV tubings used for TPN administration:
� Amino acids/Travasol - has a 0.2 micron filter to counteract the acidity of the amino acid
solution and filter out any impurities.
� Lipid emulsion - has a 1.2 micron filter to reduce the risk of particles entering the patient.
� Typically in a clean area with clean hands, prime TPN lines with 0.9% NaCl.
� TPN solutions must be connected to new sterile tubing q 24hrs.
� Swab connection ports with 2% Chlorhexidine gluconate and 70% isopropyl alcohol swabs prior
to connecting.
� When administering the lipid emulsion, piggyback the lipid tubing to the Travasol line below all
infusion filters and at the port closest to the patient.
An infusion pump must be used to regulate the administration of all TPN solutions. Our infusion pumps
have two regulators so one pump can regulate two different solutions running at different rates. This
pump should be plugged into the wall at all times but has a battery back up mechanism to temporarily
allow the pump to run should it need to be disconnected from the wall outlet. When the battery is low
the pump will alarm to notify you that it needs to be plugged into the wall outlet.
NOTE: Do not abruptly discontinue TPN (this is especially the case in patients who are on insulin), because
this may lead to hypoglycemia. If for whatever reason you run out of solution while awaiting another bag,
you can hang D5W at the same rate of the infusion in the mean time.
Do not obtain blood samples or CVP readings from same port as TPN infusions.
FLUID MANAGEMENT WITH TPN: Total Fluid Intake (TFI)
Patients often receive intravenous fluids from various sources, such as peripheral IVs, IV medications, and
continuous Travasol and lipid emulsion infusions. It is important that nurses monitor patients closely for any
signs or symptoms of fluid overload, such as pulmonary edema, shortness of breath, and hypoxia. To protect
against fluid overload, a physician should write an order for a Total Fluid Intake (TFI) amount. TFI identifies
the total fluid volume to be infused from ALL sources. A TFI order requires the nurse to calculate the patient’s
fluid administration from all sources and to adjust the peripheral IV rate accordingly to allow the TPN to be
administered as prescribed, while not exceeding the TFI amount.

10Consider this scenario: A patient on bowel rest is NPO, the physician’s order reads:
• IV 0.9% Normal Saline (NS) to be infused at 80 mL/hr
• Lipid emulsion to be infused at 20ml/hr for 12 hours
• Travasol to be infused at 42 ml/hr for 24 hours
• TFI = 122 mls/hr.
If all three solutions were running at the ordered rates (80 + 20 + 42 = 142mL/hr) the total fluid infused
would be 142 mls which is 20 mls over the ordered TFI of 122 mls/hr. To correct this, the peripheral IV
(0.9% NS) must be decreased to 60 mls/hr during the 12 hour period when the lipid infusion is running (60
+ 20 + 42 = 122 mL/hr). Then when the lipid emulsion is completed (from 0200 to 1400 hours), the IV 0.9%
NS must be increased back to 80 mL/hr along with the Travasol at 42mls/hr (80 + 42 = 122 mL/hr).
MONITORING DURING TPN ADMINISTRATION
The monitoring of a patient on TPN can be divided into 4 phases:
A. Planning
B. Assessment
C. Administration of TPN therapy
D. Evaluation
A. Planning during TPN administration
EXPECTED OUTCOME RATIONALE
Serum glucose will be within normal
limits.
- Indicates metabolic tolerance to dextrose in TPN solution
- Dextrose in TPN provides a good medium for bacterial growth at
IV insertion site
Intravenous line will remain patent,
free of pain, redness or inflammation.
- Ensures TPN solution is infusing into veins and not surrounding
tissue.
- Do not apply antibiotic ointment to catheter insertion site- will
cause fungal and AROs colonization.
- Dextrose content of CVC/ PICC solutions is higher than
peripheral solutions, increasing the risk of infection at site. For at
risk patients [i.e. diabetics], be vigilant in your aseptic practices.
**This is not always the case as 10% dextrose solution can be
provided centrally**
11Explain purpose of TPN support - Promotes understanding, reduces anxiety.
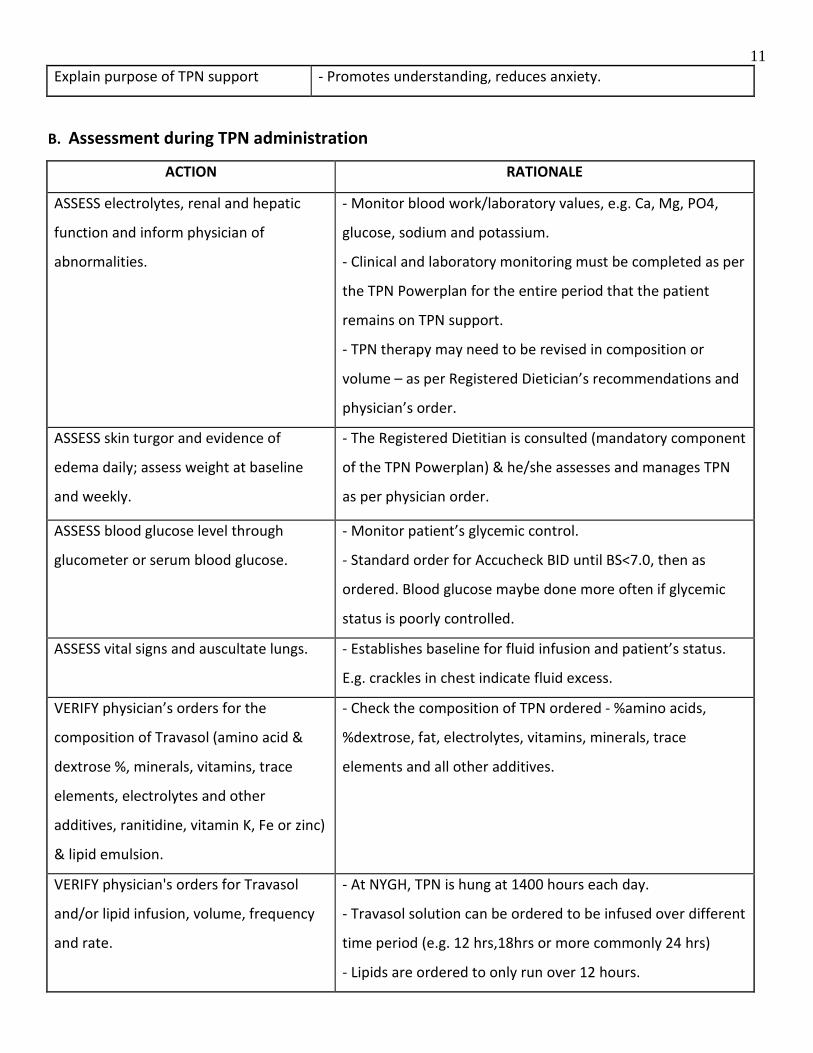
B. Assessment during TPN administration
ACTION RATIONALE
ASSESS electrolytes, renal and hepatic
function and inform physician of
abnormalities.
- Monitor blood work/laboratory values, e.g. Ca, Mg, PO4,
glucose, sodium and potassium.
- Clinical and laboratory monitoring must be completed as per
the TPN Powerplan for the entire period that the patient
remains on TPN support.
- TPN therapy may need to be revised in composition or
volume – as per Registered Dietician’s recommendations and
physician’s order.
ASSESS skin turgor and evidence of
edema daily; assess weight at baseline
and weekly.
- The Registered Dietitian is consulted (mandatory component
of the TPN Powerplan) & he/she assesses and manages TPN
as per physician order.
ASSESS blood glucose level through
glucometer or serum blood glucose.
- Monitor patient’s glycemic control.
- Standard order for Accucheck BID until BS<7.0, then as
ordered. Blood glucose maybe done more often if glycemic
status is poorly controlled.
ASSESS vital signs and auscultate lungs. - Establishes baseline for fluid infusion and patient’s status.
E.g. crackles in chest indicate fluid excess.
VERIFY physician’s orders for the
composition of Travasol (amino acid &
dextrose %, minerals, vitamins, trace
elements, electrolytes and other
additives, ranitidine, vitamin K, Fe or zinc)
& lipid emulsion.
- Check the composition of TPN ordered - %amino acids,
%dextrose, fat, electrolytes, vitamins, minerals, trace
elements and all other additives.
VERIFY physician's orders for Travasol
and/or lipid infusion, volume, frequency
and rate.
- At NYGH, TPN is hung at 1400 hours each day.
- Travasol solution can be ordered to be infused over different
time period (e.g. 12 hrs,18hrs or more commonly 24 hrs)
- Lipids are ordered to only run over 12 hours.
12VERIFY the Total Fluid Intake (TFI) ordered
by the physician.
- To prevent fluid overload from intravenous fluids.
C. Administration of TPN therapy
ACTION RATIONALE
Perform hand hygiene. - Reduces transmission of microorganisms
Outside of patient’s room, check:
- TPN orders are accurate with the
correct additives – 8 Rights of
administration.
- Expiration date of TPN solution.
- Color and clarity of TPN solution for
particulate matter. You may need to
agitate bag to remix solution.
- Connect TPN solutions to
appropriate IV tubings and prime
tubings so that all air bubbles are
removed, turn off flow with clamp.
- Prevents medication errors.
- The ingredients listed on each bag must be verified with the
physician’s order. In addition, the bags have a barcode that must
be scanned by the nurse with a Caremobile.
- When multivitamins are added, the Travasol bag will appear
yellow in color.
- Appearance of solution[s] should be equal throughout.
Deterioration of solution results in uneven administration of
nutrients.
- TPN solutions must be connected to new sterile tubing q 24hrs
to run solution from 1400 hrs to 1400 hours the next day.
- Prevents catheter related bacteremia.
- Prevents air embolus.
Inside patient’s room, check:
- Patient’s ID and ask him/her to state
name. Scan barcodes on TPN bags and
patient’s arm band with Caremobile
before TPN administration.
- Swab connection port with 2%
Chlorhexidine gluconate and 70%
isopropyl alcohol swabs and connect
- Ensures correct patient receives correct intravenous solution.
- Prevents transmission of bacteria into vein
13end of tubing to central/peripheral
catheter line.
- Program infusion pump as per
hospital protocol, ordered TPN rates
and TFI volume.
- TPN rates are ordered to meet patient’s nutritional needs- TPN
rates and TFI needed for documentation of fluid balances.
- Discard used supplies and perform
hand hygiene.
- Reduces transmission of infection.
D. Evaluation
ACTION RATIONALE
- Monitor flow rate hourly. - Too rapid or slow infusion can lead to metabolic disturbances.
- Monitor fluid intake every 4 hrs. - Prevent fluid imbalance from too fast or too slow infusions.
- Obtain weights as ordered (baseline
& weekly).
- Over time measurements will reflect weight loss/gain from
caloric intake or fluid retention.
- Monitor blood glucose frequently. - Indicates metabolic tolerance to dextrose in TPN solution and
patient’s glycemic status.
- Monitor intake and output
- Assess intakes - IV, PO, NG
- Assess outputs - NG, fistula, BM, colostomy /ileostomy, penrose,
chest tube, JP etc.
- Documentation in Cerner.
The following should be noted on the
patient’s chart:
- Time when TPN bag is hung, number of bags, and rate of
infusion.
- Site of IV catheter and verification of patency.
- Status of dressing and site condition, if visible.
- Vital signs and weight.
- Client tolerance to TPN.
- Client response to therapy and understanding of instructions.

14- Address patient’s response and
understanding of TPN.
- Manage the patient’s psychological
implications of NPO status.
- Encourage patient to ask questions and discuss feelings.
- Describe possible alternatives to satisfy oral craving- sucking on
ice chips or hard candy [if allowed].
- Offer activities for distraction.
- Encourage family to help alleviate patient fears/concerns.
COMPLICATIONS ASSOCIATED WITH TPN THERAPY
Complications of TPN therapy are usually related to the administration and the composition of the
solutions.
Chart 4: Complications associated with TPN therapy
Administration-related Complications
Sepsis
Symptoms: hypotension, tachycardia,
elevated or decreased temperature,
chills, tachypnea, disorientation, lethargy,
decreased urine output.
Actions:
- Inspect condition of peripheral, CVC, or PICC line for
inflammation, edema, tenderness at insertion site, and patency
of tubing.
- If localized, apply warm compress , notify physician
immediately
- If systemic, will need order for IV antibiotics. May indicate
need to establish new intravenous.
Pneumothorax
Symptoms: Sudden sharp chest pain made
worse by a deep breath or a cough,
shortness of breath, fatigue, tachycardia,
cyanosis.
Actions:
- Assess for signs of pneumothorax – notify physician
immediately.
- Maintain patient’s airway, apply oxygen if needed.
- Page CCRT if needed.
Embolism
Symptoms: Sudden respiratory distress,
decreased O2 saturation levels, shortness
of breath, coughing, chest pain,
hypotension.
Actions:
- Stop infusions. Clamp catheter.
- Assess for signs of embolism – notify physician immediately.
- Maintain patient’s airway, apply oxygen if needed.
- Position patient in trendelenburg position.
- Page CCRT if needed.
Catheter occlusion with PICC lines. Actions:

15Symptoms: Unable to flush line. - Watch for early signs of infection, infiltration, disruption to
patency.
- Do not try to unblock line. Patient may need to go back to
Interventional Radiology. May need to change access site.
Fluid excess and/or pulmonary edema.
Symptoms: Crackles in chest, hypoxia,
hypoxemia.
Actions:
- Establish baseline for fluid infusion through vital signs and
lung auscultation. Encourage patient to DB+C.
- Notify MD. Monitor O2 and give oxygen as ordered.
Composition of the solution-related complications
Nutritional imbalance.
Symptoms: metabolic disturbances,
poor skin turgor, edema.
Actions:
- Verify physician’s orders for nutrients, minerals, vitamins,
trace elements, electrolytes.
- Verify the caloric intake and patient weight is being
monitored.
- Ensure all patients requiring TPN support are asssessed and
followed by the Registered Dietitian. Remember to notify
him/her of any patients starting TPN support.
Hypoglycemia or hyperglycemia.
Symptoms: see Chart 5.
Actions:
- Compare blood glucose level with baseline blood glucose level
to assess tolerance to dextrose in TPN solution
- Call physician and Registered dietician as infusion rates and
composition may need to be changed.
Electrolyte imbalance.
Symptoms: see Chart 5.
Actions:
- Verify baseline and daily bloodwork and renal and hepatic
function to assess response to TPN solutions.
- Call physician and Registered dietician as infusion rates and
composition may need to be changed.
Chart 5: Symptoms of Metabolic Imbalance
Hyperkalemia Symptoms can be fairly non-specific:

16
- Malaise
- Palpitations
- Muscle weakness
Symptoms can be specific:
- Cardiac arrhythmia or sudden death.
Hypokalemia
Mild symptoms:
- Elevation of blood pressure
- Cardiac arrhythmias
- Muscular weakness
- Myalgia
- Muscle cramps
- Constipation
Severe symptoms:
- Flaccid paralysis
- Hyporeflexia
- Tetany
- Respiratory depression
- ECG changes
Hypocalcemia
Early signs:
- Personal tingling and paresthesia
- 'Pins and needles' sensation over the extremities of hands and feet.
- Tetany, carpopedal spasm are seen.
- Latent tetany
- Trousseau sign of latent tetany (eliciting carpal spasm by inflating the
blood pressure cuff and maintaining the cuff pressure above systolic)
- Chvostek's sign (tapping of the inferior portion of the zygomatic will
produce facial spasms)
- Tendon reflexes are hyperactive
- Life threatening complications
- Laryngospasm
- Cardiac arrhythmias
- ECG changes
17Hypercalcemia
- Fatigue, depression, confusion, anorexia, nausea, vomiting, constipation,
pancreatitis or increased urination
- If chronic, will result in urinary calculi (renal stones or bladder stones).
- Abnormal heart rhythms
- If severe hypercalcemia (above 15-16 mg/dL or 3.75-4 mmol/l) is
considered a medical emergency: at these levels, coma and cardiac arrest
can result.
Hypoglycemia
- Shaky
- Headache
- Hunger
- Anxious
- Mood swings
Hyperglycemia
- Excessive thirst
- Hunger
- Excessive urination
- Disorientation and confusion
Food for Thought
Cultural considerations:
• Consult religious leaders about continuous infusion of TPN solutions during fasting periods i.e.
Ramadan Devote Muslims may insist on fasting.
Evidence based practice indications:
LINKS: For additional information on total parenteral nutrition, go to the ASPEN [American Society for Parenteral Enteral
Nutrition] website at http://www.nutritioncare.org/
DOCUMENTATION OF TPN ADMINISTRATION
TPN administration practices follow the same principles in place for safely administering medications
to a patient [the 8 RIGHTS of medication administration]. The contents and volumes of the TPN solution are
each documented to reflect the care provided and to assist in the monitoring of the patient’s response to TPN.
The TPN flowchart provides a summary of the TPN therapy received by the patient. For the documenting
nurse, care must be taken to ensure details are correctly and completely documented (See below). The Intake
& Output fluid balance record is another important form to complete for a patient on TPN therapy. The
amount of fluid administered to a patient can cause adverse responses if it exceeds their body’s capacities.
Preventing serious complications like fluid overload or pulmonary edema is accomplished by monitoring the

18fluid intake by the patient from ALL sources. The TFI amount identified in the physician’s orders must be
mirrored on the total intake section of the Intake and Output record.
Charting TPN on the MAR
Steps Information
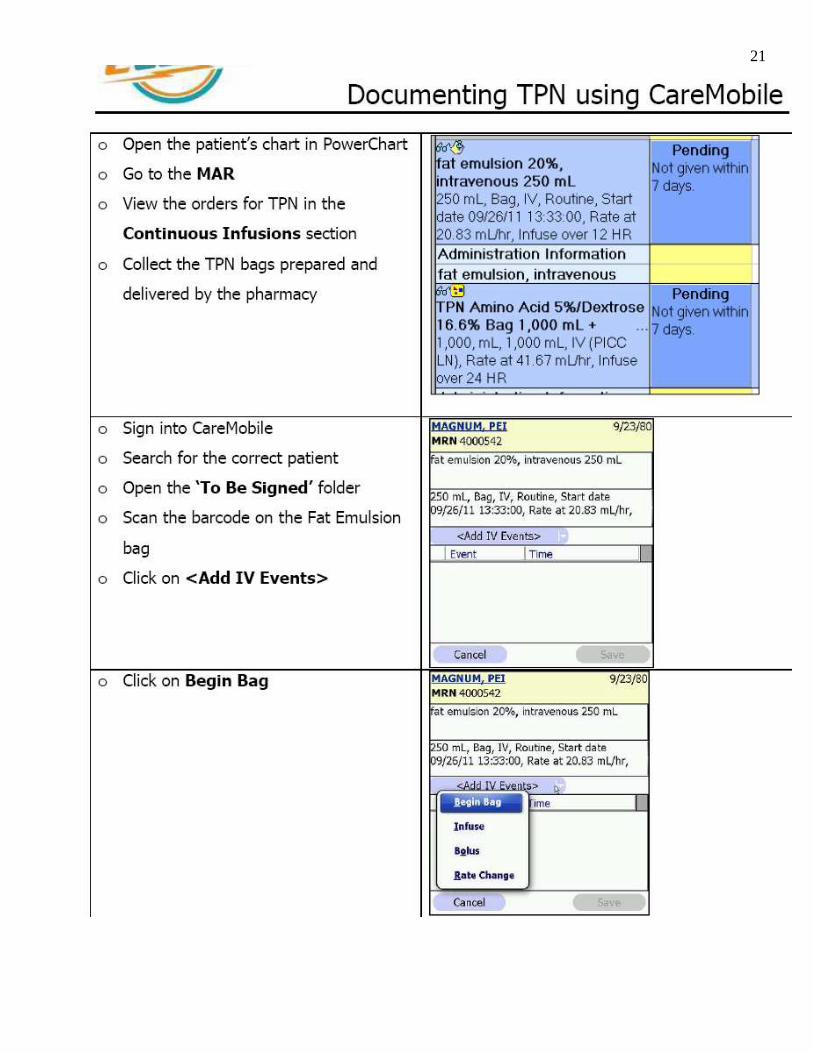
1) In the Menu, click on MAR.
(TPN will be found under the
Continuous Infusion Section)
2) Click on the administration
cell (In the column that is yellow,
the Blue box with the word
pending). The Administration
screen will display.
3) Read the screen to make sure
this is what you want to chart on.
Since you are going to hang a new
bag, click on Begin Bag in the
Event section.
4) At the bottom of the
administration screen, fill in the

19details.
• Performed date/time:
Will default to today and now.
* Change time to reflect the
time you hung the TPN bag
• Performed by: Will
default to your name
• Bag #: Once bag 1 is
documented, the subsequent
IV bags will default to the next
number.
• Site: If you are charting
the site for the first time, the
field will be mandatory (Select
the site)
• Volume: Volume of
bag defaulted from the order
detail.
• Rate: The infusion rate
5) Once you have filled out all
the necessary fields, click on
Apply.
6) Read your screen, making sure
the details that you just charted is
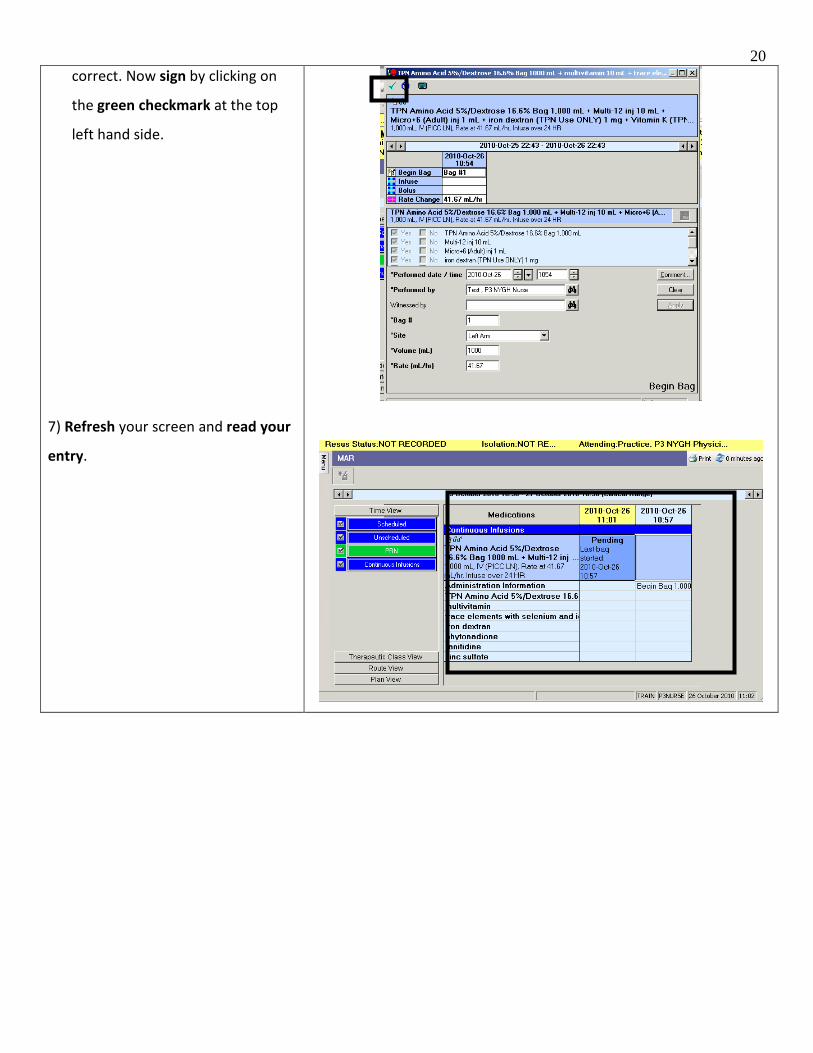
20correct. Now sign by clicking on
the green checkmark at the top
left hand side.
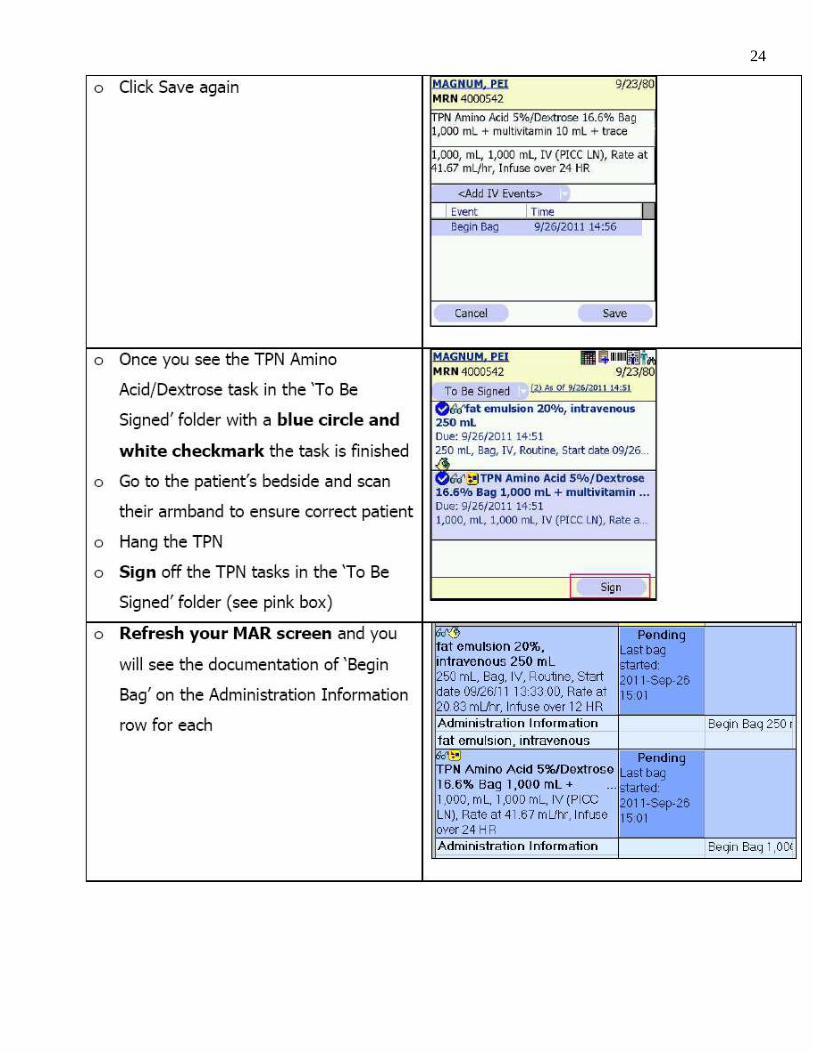
7) Refresh your screen and read your
entry.
21

22

23
24

25Cerner Site Assessment & TPN Intervention Documentation
Label on TPN Bag

26References
Dudek, S.G. [2006]. Nutrition Essentials for Nursing Practice (5th Edition). eBook available via the
University of Toronto Library at
http://ovidsp.tx.ovid.com.myaccess.library.utoronto.ca/spb/ovidweb.cgi
Ferreira, P (2007). Total parenteral nutrition. Powerpoint presentation available at North York General
Hospital at www.nygh.on.ca
Ohio State University: University Medical Center (1999). Health for life: Total parenteral nutrition.
Available at http://medicalcenter.osu.edu/pdfs/PatientEd/Materials/PDFDocs/nut-diet/tpn/tpn.pdf
Perry, A.G. & Potter, P.A. (2006). Clinical Nursing Skills and techniques: 6th
edition. Philadelphia: Elsevier
Mosby
Smith-Temple, J. & Young Johnson, J. [2002]. Nurses' Guide to Clinical Procedures eBook available via the
University of Toronto Library at http://ovidsp.tx.ovid.com.myaccess.library.utoronto.ca/spb/ovidweb.cg

27Total Parenteral Nutrition (TPN) Test
Name : Unit :
Date :
Circle True or False for each:
1. True False TPN therapy can be prescribed if there is intolerance to oral feeds and the patient is
NPO for 3 or more days.
2. True False TPN is not compatible with any other solution and must be administered by itself, with a
dedicated labeled IV line for TPN use only.
3. True False Travasol can be administered over 24 hours, while lipids are commonly over 12 hours.
4. True False Only TPN solutions of >10% dextrose can be administered into a peripheral IV site, to
prevent vascular trauma.
5. True False Performing the 8 rights of medication administration is not necessary when hanging a
TPN bag.
6. True False It is important to have a baseline electrolyte, renal and hepatic blood work prior
to initiating TPN.
Multiple choice: Circle the best answer
7. When hanging TPN, you must:
a) use aseptic technique
b) verify the MDs orders against the composition label on the bags
c) follow the 8 rights of medication administration
d) administer the infusion through a IV pump
e) all of the above
f) b only
8. Standard composition of TPN includes:
a) dextrose, amino acids, fats, antibiotics, minerals, electrolytes, vitamins
b) dextrose, amino acids, fats, minerals, electrolytes, anti-fungals, vitamins
c) dextrose, amino acids, fats, minerals, electrolytes, vitamins
d) none of the above

289. Patients receiving TPN will have their Laboratory values specifically monitored for:
a) electrolyte imbalances
b) increased WBC and thyroid levels
c) readjustment in TPN composition
d) assess renal and hepatic function
e) a, b, c
f) a, c, d
10. Fluid monitoring/management with patients receiving TPN is crucial in order to prevent fluid
overload. A patient’s TPN orders are as follows:
Travasol @ 45mls/hr
Lipid emulsion @ 20mls/hr
IV 0.09 % NaCl @ 75mls/hr
TFI order is 115mls/hr
a) If all 3 infusions are running at the same time as ordered, what is the TFI____________mls/hr
b) This makes the TFI over by _____________mls from the MD’s order for 115mls/hr.
c) You realize that in order to keep the TFI at 115mls/hr you have to:
i) increase the lipid emulsion infusion to 22mls/hr
ii) decrease the travasol solution to 25mls/hr
iii) decrease the NaCl infusion to 50 mls/hr for 12hrs while the Lipids are infusing then
increase it back to 75mls/hr when the lipids have infused
11. When hanging TPN tubing and connection port considerations include:
a) changing IV tubing Q 24 hours with aseptic technique
b) prime tubing with dextrose
c) swabbing connection ports with 2% chlorohexidine with alcohol
d) Tubing for Travasol has a 0.2 micron filter
e) Tubing for Lipid emulsion has a 1.2 micron filter
f) All of the above
g) a, b, d only

2912. During TPN administration the following is monitored:
a) PICC or peripheral IV insertion sites
b) Blood glucose and electrolytes
c) Intake and output
d) Potential fluid overload
e) Weight and nutritional status
f) All of the above
g) b, c, d only
13. Signs and symptoms of a patient experiencing fluid overload while receiving TPN are:
a) Crackles to lung fields, SOB, difficulty breathing
b) Vomiting, constipation, shaky, mood swings
c) Possible Pulmonary Edema
d) Hypertension, Distended jugular veins
e) All of the above
f) a, c, d only
14. An electrolyte imbalance of hypocalcemia can cause:
a) Tetany, facial spasms
b) “Pins and needles” over extremities
c) Hyperactive wrist reflexes and severe lethargy
d) Cardiac arrhythmias
e) All of the above
f) a, b, d only
15. Place the correct solution (either Travasol or Lipids) in column 1.
/20
Column 1
Prepared in 1000 or 2000 ml bag, contains varied concentrations of dextrose and
solution can be yellow from multivitamins.
Requires IV tubing with a 1.2 micron filter and is dispensed in 20% solutions.
Prepared in 100 or 250 ml bag, appears milky and usually administered over 12 hours.
Requires IV tubing with a 0.2 micron filter and is ordered, based on the patient’s
clinical presentation and blood work, to support their metabolic needs.