
Care for the Caregiver: Assessing and Addressing the “Cost” of Caring Mary Lou O’Gorman, MDiv,...
33
Care for the Caregiver: Assessing and Addressing the “Cost” of Caring Mary Lou O’Gorman, MDiv, BCC Executive Director of Pastoral Care and CPE Saint Thomas Health Nashville, Tennessee [email protected]
-
Upload
claud-hawkins -
Category
Documents
-
view
213 -
download
0
Transcript of Care for the Caregiver: Assessing and Addressing the “Cost” of Caring Mary Lou O’Gorman, MDiv,...

Care for the Caregiver: Assessing and Addressing
the “Cost” of Caring
Mary Lou O’Gorman, MDiv, BCCExecutive Director of Pastoral Care and CPE
Saint Thomas HealthNashville, Tennessee
Objectives
Describe the causes, symptoms and impact of moral distress, compassion fatigue, burnout and other sources of staff distress.
Describe the cultural, organizational, professional and personal factors that contribute to that distress.
Identify strategies and “best practices” that provide care for the caregiver.

The Schwartz Center April 2013
Burnout suffered by More than a third of nurses
More than a quarter of physicians
Numbers are increasing
Caregivers needSupport, opportunities to share
Joys and challenges
Time for patient/family interactions
Their health and wellbeing to be valued

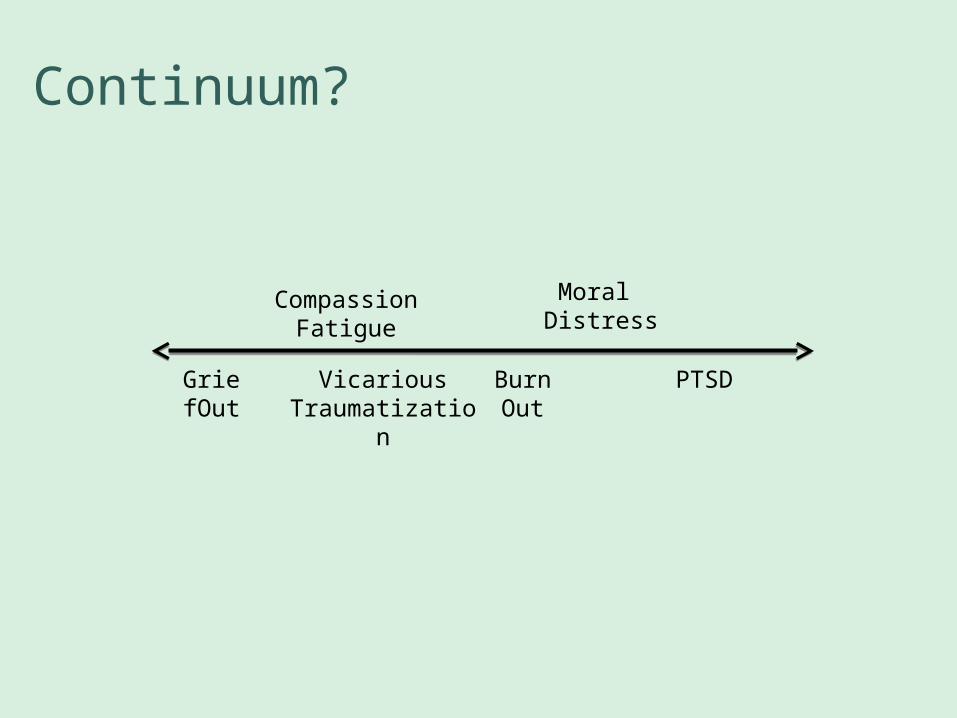
Continuum?
CompassionFatigue
GriefOut
Moral Distress
PTSDBurn Out
Vicarious Traumatization

Moral Distress Defined…
“…the pain or anguish affecting the mind, body or relationships in response to a situation in which the person is aware of a moral problem, acknowledges moral responsibility, and makes a moral judgment about the correct action; yet as a result of real or perceived constraints, participates in perceived moral wrongdoing.”
Alvita Nathaniel MSN, RNCSIn Nursing World, July 28, 2002

…moral distress defined
“Painful feelings and/or the psychological disequilibrium that occurs when one knows the right thing to do, but institutional constraints make it nearly impossible to pursue the right course of action.”
Jameton A. Nursing Practice: The Ethical Issues. NJ:Prentiss-Hall. 1984

…moral distress defined
1993 Jameton distinguished:Initial: frustration, anger and anxiety due to
Institutional obstaclesInterpersonal conflict about values
Reactive: due to failure to address initial distress
2000 Webster and Baylis included:Failure to pursue “right” course of action due to
Error in judgmentPersonal failingCircumstances beyond control
May feel cherished beliefs violated Compromised integrity

…distressBurn out
Individual or group stress related to one’s relationship with the work environment.
Feel overwhelmed.
Compassion fatigueGradual lessening, over time of ability to be compassionate.The price one pays for caring.Emotional stress experienced from exposure to the suffering of others.

…distressSecondary Traumatic Stress (STS)
Presence of Post-Traumatic Stress Disorder (PTSD) in the caregiver.Due to relationship and/or proximity.
Both STS and CF are caused by exposure to patients who have been traumatized or are suffering, not to the traumatic event itself.
Vicarious traumatization

“It's possible I am pushing through solid rockin flintlike layers, as the ore lies, alone;I am such a long way in I see no way through,and no space: everything is close to my face,and everything close to my face is stone.
I don't have much knowledge yet in grief --so this massive darkness makes me small.You be the master: make yourself fierce,
break in:then your great transforming will happen to me,and my great grief cry will happen to you.”
-Rilke

Other/Related Distress…
Grief outRepeated, sustained and often unresolved grief and loss.
JadingProcess leading to exhaustion from being overdriven to perform long, continued labor and/or severe or tedious tasks. Leaves one angry, even mean.
Continuum?
CompassionFatigue
GriefOut
Moral Distress
PTSDBurn Out
Vicarious Traumatization

Caregiving: A Moral Endeavor
PracticeFundamentally ethical
Roots of the caring professionsHotel Dieu: “House of God”
Nursing : The Finest Art. An Illustrated History
Promotion of ideal patient careRespect for personsRole as advocateSafe and best care
Caregiver-patient relationship is complexPatient focused caringSome distress is unavoidable

Constraints/Barriers
Organizational
Professional
Personal

Organizational BarriersHospitals/other settings
Biomedical focusTechnologyLack of timeFailure of team
Leadership dynamicsLack of collaborationConflict
Patient/client with sudden, critical illnessWishes unknown
Sustained proximity when others walk away

Contributing Factors
Cure orientation Technology
Death a failureDiscomfort with own mortality
Belief “doing everything” a sign of faithfulness
StaffingInsufficient
Novice staff
High patients acuity

Professional BarriersStaffing
So low, care is inadequate
Lack of time, skill
Novice staff
Multiple deaths in close succession
High patient/client acuity
Organizational changeQuality, safety
Cost-cutting: Doing more with less
Leadership dynamics
Effectiveness of teamPower imbalance
Lack of collaboration

….professionalRole and relevance questions
Limited role in decision making
Belief that decisions contradict best interests
Confusion about plan
Communication failuresIn team, between teams
Too many partners or consultants
Patient and/or family
Technological imperative/futilityDoing everything vs. the right thing
Belief “doing everything” a sign of faithfulness
Death a failureDiscomfort with own mortality

….professional
Nature of relationshipsCloseness/identification
Dynamics with patient and/or family
ConflictAssertive/aggressive patients/clients and families
Intra or interdisciplinary conflict
Outside pressures Organizational, professional, personal
Economy
Politics
Sustained proximity when others walk away

Personal
Psychological/emotional
Closeness/identification with patient/client
Boundaries
Isolation
Feelings of powerlessness or helplessness
Feelings of failure or guilt
Inability to talk about feelings

…personal
Grief and LossLack of time to process
Accumulated grief and loss
Lack of closure
Compromise of one’s standard of careInadequate staffing
Inability to meet perceived needs of patient
Lack of resources, services
Futility

Symptoms of Distress
FatigueEmotional, physical
Somatic concernsDiet, sleep, physical illness
Absenteeism
Poor or inappropriate careRecipients of care
Self
Feelings of inadequacyPersonal, professional
Feeling victimized

…symptoms of distress
Irritability, anger, insults, resentment, conflictsAnxietyFrustrationDepression Blaming othersSee self as having lost
IntegrityAuthenticity
Distancing oneselfIsolation
Friends, familyColleagues
Loss of meaningCrisis of faith

Addressing Distress…
Cause analysis
Self awareness/self monitoringLimits, issues
Address issues in real timeDebriefing
“Talk about it”
Ethical decision-making Referral
Skill-building
Grief work

…addressing distressEngage in work of “letting go”
At the bedsideFunerals, journal, phone callsSacred/holy
Story tellingSelf-care
BalanceSpiritual practiceTherapy
Find own voice/AdvocacyCourage
Develop sources of supportProfessional relationshipsSocial relationships
“Play”
Resources to Address StaffDistress
Spiritual nurture provided on a regular basis
Staff follow-up
Support Groups
CISM
Schwartz Rounds
Provide places of sanctuary

“To heal a person, one must first be a person.”
-Abraham Heschel

Healing Teams/Environments
Interdisciplinary/CollaborativeRole modelingMentoringSkill building and education
ConversationAffirmation of positiveEncouraging when negative
Flexible and creativeTrusting environment
Safe place to talk
BereavementStrong leader

Effective Organizations

Organizational ObligationsRecurring issues/systemic causes of moral distress identified and monitored
Corrective action
Adequate financial and people resourcesEthics resourcesPalliative careConflict resolutionInterdisciplinary forums to discuss complex “situations”
Mechanisms to address futile careAccountability for practice and behaviorSkill building, education, mentoringBereavement mechanism
Areas where death is frequent
Opportunities for breaks and places of “Sanctuary”

Chaplains
Needed skills to address staff distress
Are involved in clinical arenaAccessible
Part of the team
Incarnate the presence of the Source of all Hope
Ministry to care providers is part of the job description

Pastoral LeadershipAdvocates for patient’s wishes and goals
Develops and maintains strong team relationships
Possesses strong communication skills
Possesses skill in ethical decision-making and in conflict resolution
Attends and participates in significant patient/family conferences
Uses appropriate referrals to address issues
Is courageous

QUESTIONS?


















