Cardiovascular Epidemiology and Prevention Nathan D. Wong, PhD, FACC, FAHA Professor and Director,...
117
Cardiovascular Cardiovascular Epidemiology and Epidemiology and Prevention Prevention Nathan D. Wong, PhD, FACC, Nathan D. Wong, PhD, FACC, FAHA FAHA Professor and Director, Heart Professor and Director, Heart Disease Prevention Program, Disease Prevention Program, Division of Cardiology, University Division of Cardiology, University of California, Irvine of California, Irvine Adjunct Prof. Epidemiology (UCLA Adjunct Prof. Epidemiology (UCLA and UCI) and UCI) Immediate Past President, American Immediate Past President, American Society of Preventive Cardiology Society of Preventive Cardiology
-
Upload
keshawn-best -
Category
Documents
-
view
218 -
download
1
Transcript of Cardiovascular Epidemiology and Prevention Nathan D. Wong, PhD, FACC, FAHA Professor and Director,...

Cardiovascular Epidemiology and Cardiovascular Epidemiology and PreventionPrevention
Nathan D. Wong, PhD, FACC, FAHANathan D. Wong, PhD, FACC, FAHAProfessor and Director, Heart Disease Professor and Director, Heart Disease Prevention Program, Division of Cardiology, Prevention Program, Division of Cardiology, University of California, IrvineUniversity of California, IrvineAdjunct Prof. Epidemiology (UCLA and UCI)Adjunct Prof. Epidemiology (UCLA and UCI)Immediate Past President, American Society of Immediate Past President, American Society of Preventive CardiologyPreventive Cardiology

TextbooksTextbooks



Cardiovascular Epidemiology: Cardiovascular Epidemiology: Definitions, Concepts, Definitions, Concepts, Historical Perspectives and Historical Perspectives and StatisticsStatistics

DefinitionsDefinitions
• CORONARY ARTERY DISEASE (CAD) or CORONARY ARTERY DISEASE (CAD) or CORONARY HEART DISEASE (CHD) (often CORONARY HEART DISEASE (CHD) (often broadly referred to as ISCHEMIC HEART broadly referred to as ISCHEMIC HEART DISEASE (IHD): primarily myocardial DISEASE (IHD): primarily myocardial infarction and sudden coronary death, infarction and sudden coronary death, broader definition may include angina broader definition may include angina pectoris, atherosclerosis, positive pectoris, atherosclerosis, positive angiogram, and revascularization angiogram, and revascularization (perceutaneous coronary interventions, or (perceutaneous coronary interventions, or PCI such as angioplasty and stents)PCI such as angioplasty and stents)
• CARDIOVASCULAR DISEASE or CVD CARDIOVASCULAR DISEASE or CVD includes CHD, cerebrovascular disease, includes CHD, cerebrovascular disease, peripheral vascular disease, and other peripheral vascular disease, and other cardiac conditions (congenital, cardiac conditions (congenital, arrhythmias, and congestive heart failure)arrhythmias, and congestive heart failure)

Definitions (cont.)Definitions (cont.)• SURROGATE MEASURES include: carotid SURROGATE MEASURES include: carotid
intimal medial thickness (IMT), coronary intimal medial thickness (IMT), coronary calcium, angiographic stenosis, brachial calcium, angiographic stenosis, brachial ultrasound flow mediated dilatation (FMD)ultrasound flow mediated dilatation (FMD)
• Hard endpoints include myocardial Hard endpoints include myocardial infarction, CHD death, and strokeinfarction, CHD death, and stroke



Trends in cardiovascular procedures, United States: 1979–2009
Note: Inpatient procedures only. Source: National Hospital Discharge Survey, NCHS, and NHLBI.
©2011 American Heart Association, Inc. All rights reserved. Roger VL et al. Published online in Circulation Dec. 15, 2011

Direct and indirect costs (in billions of dollars) of major cardiovascular diseases and stroke (United States: 2008)
Source: National Heart, Lung, and Blood Institute.
©2011 American Heart Association, Inc. All rights reserved. Roger VL et al. Published online in Circulation Dec. 15, 2011

Projected Total Costs of CVD, 2015–2030 (in Billions 2008$) in the United States
Unpublished data tabulated by AHA using methods described in Circulation. 2011;123:933–944.
©2011 American Heart Association, Inc. All rights reserved. Roger VL et al. Published online in Circulation Dec. 15, 2011


So how long have we known that So how long have we known that women are just not small men???women are just not small men???










Prevalence of stroke by age and sex (NHANES: 2005–2008).Prevalence of stroke by age and sex (NHANES: 2005–2008).
Source: NCHS and NHLBI.
©2010 American Heart Association, Inc. All rights reserved. Roger VL et al. Published online in Circulation Dec. 15, 2010

Development of Atherosclerotic Plaques
NormalFatty streak
Foam cells
Lipid-rich plaque
Lipid core
Fibrous cap
Thrombus
Ross R. Nature. 1993;362:801-809.

PDAY: Percentage of Right Coronary Artery PDAY: Percentage of Right Coronary Artery Intimal Surface Affected With Early AtherosclerosisIntimal Surface Affected With Early Atherosclerosis
PDAY=PDAY= Pathobiological Determinants of Atherosclerosis in Youth.Strong JP, et al. JAMA. 1999;281:727-735.
Fatty streaks
Raised lesions
White15-19 20-24 25-29 30-34
0
10
20
30 Women
0
10
20
30
15-1920-2425-2930-34Black
Age (y)
0
10
20
30
White15-19 20-24 25-29 30-34
Men
Black15-19 20-24 25-29 30-34
0
10
20
30
Intimalsurface
(%)

Most Myocardial Infarctions Are CausedMost Myocardial Infarctions Are Causedby Low-Grade Stenosesby Low-Grade Stenoses
Pooled data from 4 studies: Ambrose et al, 1988; Little et al, 1988; Nobuyoshi et al, 1991; and Giroud et al, Pooled data from 4 studies: Ambrose et al, 1988; Little et al, 1988; Nobuyoshi et al, 1991; and Giroud et al, 1992.1992.(Adapted from Falk et al.)(Adapted from Falk et al.)Falk E et al, Circulation, 1995.

(Adapted from Glagov et al.)(Adapted from Glagov et al.)
Coronary RemodelingCoronary RemodelingCoronary RemodelingCoronary Remodeling
NormalNormalvesselvessel
MinimalMinimalCADCAD
ProgressionProgression
Compensatory expansionCompensatory expansionmaintains constant lumenmaintains constant lumen
Expansion Expansion overcome:overcome:
lumen narrowslumen narrows
SevereSevereCADCAD
ModerateModerateCADCAD
Glagov et al, Glagov et al, N Engl J MedN Engl J Med, 1987., 1987.

Intraluminal thrombusGrowth of thrombus
Intraplaque thrombus Lipid pool
Blood Flow
Atherosclerotic Plaque Rupture and Atherosclerotic Plaque Rupture and Thrombus FormationThrombus Formation
Adapted from Weissberg PL. Eur Heart J Supplements 1999:1:T13–18

• Eccentric, lipid-rich
• Fragile fibrous cap
• Prior luminal obstruction < 50%
• Visible rupture and thrombus
Constantinides P. Am J Cardiol. 1990;66:37G-40G.
Features of a Ruptured Atherosclerotic Plaque

Libby P. Circulation. 1995;91:2844-2850.
Vulnerable Plaque
•Thin fibrous cap•Inflammatory cell infiltrates: proteolytic activity•Lipid-rich plaque
Lumen LipidCore
Fibrous Cap
•Thick fibrous cap•Smooth muscle cells:
more extracellular matrix•Lipid-poor plaque
Stable Plaque
Lumen LipidCore
Fibrous Cap
Vulnerable Versus Stable Atherosclerotic Plaques

Correlation of CT angiography of the coronary arteries with intravascular ultrasound illustrates the ability of MDCT to demonstrate calcified and non-calcified coronary plaques (Becker et al., Eur J Radiol 2000) Non-calcified, soft, lipid-rich plaque in
left anterior descending artery (arrow) (Somatom Sensation 4, 120 ml Imeron 400). The plaque was confirmed by intravascular ultrasound (Kopp et al., Radiology 2004)
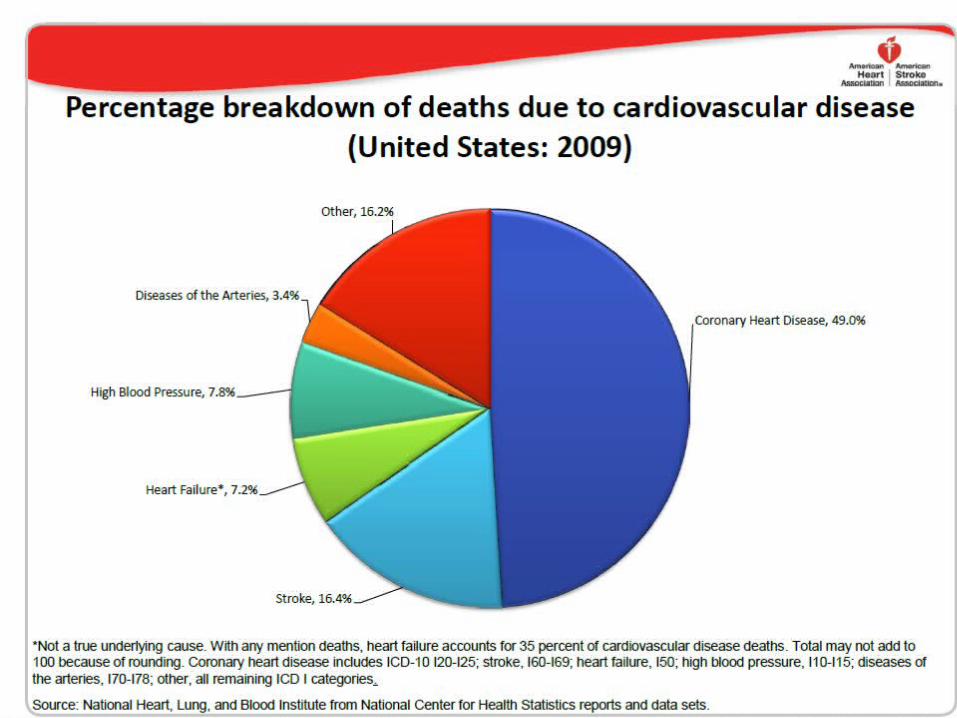
Pyramid of Risk Pyramid of Risk (Werner et al. (Werner et al. Canadian Journal of Canadian Journal of Cardiology Cardiology 1998; 14(Suppl) B:3B-10B)1998; 14(Suppl) B:3B-10B)

Approaches to Primary and Approaches to Primary and Secondary Prevention of Secondary Prevention of CVDCVD
• Primary prevention involves prevention of Primary prevention involves prevention of onset of disease in persons without onset of disease in persons without symptoms.symptoms.
• Primordial prevention involves the Primordial prevention involves the prevention of risk factors causative o the prevention of risk factors causative o the disease, thereby reducing the likelihood of disease, thereby reducing the likelihood of development of the disease.development of the disease.
• Secondary prevention refers to the Secondary prevention refers to the prevention of death or recurrence of disease prevention of death or recurrence of disease in those who are already symptomaticin those who are already symptomatic

Risk Factor Concepts in Risk Factor Concepts in Primary PreventionPrimary Prevention
• Nonmodifiable risk factorsNonmodifiable risk factors include age, sexc, include age, sexc, race, and family history of CVD, which can race, and family history of CVD, which can identify high-risk populationsidentify high-risk populations
• Behavioral risk factorsBehavioral risk factors include sedentary include sedentary lifestyle, unhealthful diet, heavy alcohol or lifestyle, unhealthful diet, heavy alcohol or cigarette consumption.cigarette consumption.
• Physiological risk factorsPhysiological risk factors include include hypertension, obesity, lipid problems, and hypertension, obesity, lipid problems, and diabetes, which may be a consequence of diabetes, which may be a consequence of behavioral risk factors.behavioral risk factors.

Population vs. High-Risk Population vs. High-Risk ApproachApproach
• Risk factors, such as cholesterol or blood pressure, have Risk factors, such as cholesterol or blood pressure, have a wide bell-shaped distribution, often with a “tail” of high a wide bell-shaped distribution, often with a “tail” of high values.values.
• The “high-risk approach” involves identification and The “high-risk approach” involves identification and intensive treatment of those at the high end of the “tail”, intensive treatment of those at the high end of the “tail”, often at greatest risk of CVD, reducing levels to often at greatest risk of CVD, reducing levels to “normal”.“normal”.
• But most cases of CVD do not occur among the highest But most cases of CVD do not occur among the highest levels of a given risk factor, and in fact, occur among levels of a given risk factor, and in fact, occur among those in the “average” risk group.those in the “average” risk group.
• Significant reduction in the population burden of CVD Significant reduction in the population burden of CVD can occur only from a “population approach” shifting the can occur only from a “population approach” shifting the entire population distribution to lower levels.entire population distribution to lower levels.

Expected Shifts in Cholesterol Distribution Expected Shifts in Cholesterol Distribution from High-Risk, Population, and from High-Risk, Population, and Combined ApproachesCombined Approaches

Population and Community-Population and Community-Wide CVD Risk Reduction Wide CVD Risk Reduction ApproachesApproaches
• Populations with high rates of CVD are those with Populations with high rates of CVD are those with Western lifestyles of high-fat diets, physical inactivity, Western lifestyles of high-fat diets, physical inactivity, and tobacco use.and tobacco use.
• Targets of a population-wide approach must be these Targets of a population-wide approach must be these behaviors causative of the physiologic risk factors or behaviors causative of the physiologic risk factors or directly causative of CVD.directly causative of CVD.
• Requires public health services such as surveillance Requires public health services such as surveillance (e.g.,BFRSS), education (AHA, NCEP), organizational (e.g.,BFRSS), education (AHA, NCEP), organizational partnerships (Singapore Declaration), and partnerships (Singapore Declaration), and legislation/policy (Anti-Tobacco policies)legislation/policy (Anti-Tobacco policies)
• Activities in a variety of community settings: schools, Activities in a variety of community settings: schools, worksites, churches, healthcare facilities, entire worksites, churches, healthcare facilities, entire communitiescommunities

A conceptual framework for public A conceptual framework for public health practice in CVD prevention. health practice in CVD prevention. (From Pearson et al., (From Pearson et al., J Public HealthJ Public Health. 2001; 29:69 –78) . 2001; 29:69 –78)

Communitywide CVD Communitywide CVD Prevention ProgramsPrevention Programs
• Stanford 3-Community Study (1972-75) Stanford 3-Community Study (1972-75) showed mass media vs. no intervention in showed mass media vs. no intervention in high-risk residents to result in 23% reduction high-risk residents to result in 23% reduction in CHD risk scorein CHD risk score
• North Karelia (1972-) showed public education North Karelia (1972-) showed public education campaign to reduce smoking, fat campaign to reduce smoking, fat consumption, blood pressure, and cholesterolconsumption, blood pressure, and cholesterol
• Stanford 5-City Project (1980-86) showed Stanford 5-City Project (1980-86) showed reductions in smoking, cholesterol, BP, and reductions in smoking, cholesterol, BP, and CHD riskCHD risk
• Minnesota Heart Health Program (1980-88) Minnesota Heart Health Program (1980-88) showed some increases in physical activity showed some increases in physical activity and in women reductions in smokingand in women reductions in smoking

Materials Developed for US Materials Developed for US Community Intervention Community Intervention TrialsTrials
• Mass media, brochures and direct mailMass media, brochures and direct mail• Events and contestsEvents and contests• ScreeningsScreenings• Group and direct educationGroup and direct education• School programs and worksite interventionsSchool programs and worksite interventions• Physician and medical setting programsPhysician and medical setting programs• Grocery store and restaurant projectsGrocery store and restaurant projects• Church interventionsChurch interventions• PoliciesPolicies


Foundations of CVD Foundations of CVD EpidemiologyEpidemiology
• Lack of reliable data on CVD noted as Lack of reliable data on CVD noted as early as 1880’s and in 1934 the Society early as 1880’s and in 1934 the Society of Geographic Pathology noted the of Geographic Pathology noted the frequency of atherosclerotic lesions frequency of atherosclerotic lesions by country, social class and by country, social class and occupation.occupation.
• In 1946 the first prospective study of In 1946 the first prospective study of CVD was launched by Ansel Keys in CVD was launched by Ansel Keys in Minnesota businessmen.Minnesota businessmen.





Cholesterol intake and CHD Death Rate: The Cholesterol intake and CHD Death Rate: The Seven Countries Study Seven Countries Study (n=12763 men aged 40-59)(n=12763 men aged 40-59)

Cholesterol and Mortality: Cholesterol and Mortality: WHO Monica WHO Monica (n=15 million men and women aged 25-64)(n=15 million men and women aged 25-64)

Migrant Studies Migrant Studies
• Ni-Hon-San Study showed Japanese Ni-Hon-San Study showed Japanese living in Japan to have the lowest living in Japan to have the lowest cholesterol levels and lowest rates of cholesterol levels and lowest rates of CHD, those living in Hawaii to have CHD, those living in Hawaii to have intermediate rates for both, and intermediate rates for both, and those living in San Francisco to have those living in San Francisco to have the highest cholesterol levels and the highest cholesterol levels and CHD incidenceCHD incidence


Framingham Heart Framingham Heart StudyStudy
• Longest running study of cardiovascular disease in Longest running study of cardiovascular disease in the worldthe world
• Began in 1948 with original cohort of 5,209 subjects Began in 1948 with original cohort of 5,209 subjects aged 30-62 at baselineaged 30-62 at baseline
• Biennial examinations, still ongoing, most of original Biennial examinations, still ongoing, most of original cohort deceasedcohort deceased
• Offspring cohort of 5,124 of children of original Offspring cohort of 5,124 of children of original cohort enrolled in 1971, and more recently and still cohort enrolled in 1971, and more recently and still being enrolled to better understand genetic being enrolled to better understand genetic components of CVD risk are up to 3,500 components of CVD risk are up to 3,500 grandchildren of the original cohort.grandchildren of the original cohort.
• Routine surveillance of cardiovascular disease events Routine surveillance of cardiovascular disease events adjudicated by panel of physiciansadjudicated by panel of physicians

Concept of cardiovascular Concept of cardiovascular “risk factors”“risk factors”
Kannel et al, Ann Intern Med 1961
Age, sex, hypertension, hyperlipidemia, smoking, diabetes, (family history), (obesity)
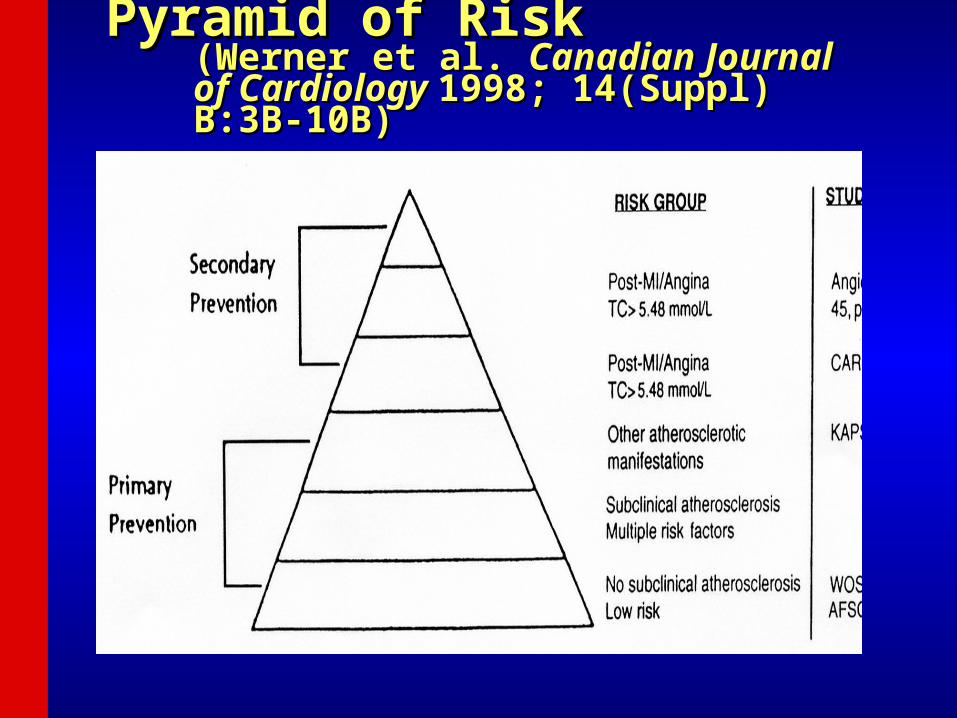
Framingham Most Significant Framingham Most Significant MilestonesMilestones
• 1960 Cigarette smoking found to increase the risk of heart 1960 Cigarette smoking found to increase the risk of heart diseasedisease
• 1961 Cholesterol level, blood pressure, and 1961 Cholesterol level, blood pressure, and electrocardiogram abnormalities found to increase the risk electrocardiogram abnormalities found to increase the risk of heart disease of heart disease
• 1967 Physical activity found to reduce the risk of heart 1967 Physical activity found to reduce the risk of heart disease and obesity to increase the risk of heart disease disease and obesity to increase the risk of heart disease
• 1970 High blood pressure found to increase the risk of 1970 High blood pressure found to increase the risk of strokestroke
• 1976 Menopause found to increase the risk of heart disease 1976 Menopause found to increase the risk of heart disease • 1978 Psychosocial factors found to affect heart disease 1978 Psychosocial factors found to affect heart disease • 1988 High levels of HDL cholesterol found to reduce risk of 1988 High levels of HDL cholesterol found to reduce risk of
deathdeath• 1994 Enlarged left ventricle (one of two lower chambers of 1994 Enlarged left ventricle (one of two lower chambers of
the heart) shown to increase the risk of strokethe heart) shown to increase the risk of stroke• 1996 Progression from hypertension to heart failure 1996 Progression from hypertension to heart failure
describeddescribed

9
Doubts about cholesterol as late as 1989



Total Cholesterol Distribution: Total Cholesterol Distribution: CHD vs Non-CHD PopulationCHD vs Non-CHD Population
Castelli WP. Atherosclerosis. 1996;124(suppl):S1-S9.1996 Reprinted with permission from Elsevier Science.
35% of CHD 35% of CHD Occurs in Occurs in People with People with TC<200 TC<200 mg/dLmg/dL
150 200
Total Cholesterol (mg/dL)
250 300
No CHD
CHD
Framingham Heart Study—26-Year Follow-up

Low HDL-C Levels Increase CHD Risk Even When Low HDL-C Levels Increase CHD Risk Even When Total-C Is NormalTotal-C Is Normal
Risk of CHD by HDL-C and Total-C levels; aged 48–83 yCastelli WP et al. JAMA 1986;256:2835–2838
02468
101214
< 40 40–4950–59 60< 200
230–259200–229
260
HDL-C (mg/dL) Tota
l-C (m
g/dL
)
14-y
in
cid
en
ce
rate
s (
%)
for
CH
D
11.24
11.91
12.50
11.91
6.56
4.67
9.05
5.53
4.85
4.153.77
2.782.06
3.83
10.7
6.6

61Messerli, F. H. Messerli, F. H. N Engl J MedN Engl J Med 1995 1995

CK Friedberg on Hypertension: CK Friedberg on Hypertension: Diseases of the Heart 1996Diseases of the Heart 1996
““There is a lack of correlation in There is a lack of correlation in most cases between the severity most cases between the severity and duration of and duration of hypertensionhypertension and and development of cardiac development of cardiac complications.”complications.”
___________________________________________________________
________________________________________________________
_______________________________________________________________



Relation of Non-Hypertensive Blood Relation of Non-Hypertensive Blood Pressure to Cardiovascular DiseasePressure to Cardiovascular DiseaseVasan R, et al. N Engl J Med 2001; 345:1291-1297Vasan R, et al. N Engl J Med 2001; 345:1291-1297
0%
2%
4%
6%
8%
10%
12%
Women Men
<120/80 mm Hg
120-129/80-84 mm Hg
130-139/85-89 mm Hg
10-year Age- Adjusted Cumulative Incidence
Hazard Ratio*
SBP Women Men
<120/80 1.0 1.0 120-129 1.5 1.3 130-139 2.5 1.6
H.R. adjusted for age, BMI, Cholesterol, Diabetes and smoking *P<.001
Framingham Study: Subjects Ages 35-90 yrs.
1.9
2.8
4.4
5.8
7.6
10.1


Extent of awareness, treatment and control of high blood Extent of awareness, treatment and control of high blood pressure by race/ethnicity pressure by race/ethnicity (NHANES : 2005-2006). (NHANES : 2005-2006). Source: NCHS and NHLBI.Source: NCHS and NHLBI.
70.178.8
69.1
45.4
79.0
46.1
74.7
82.3
46.5
67.6
52.1
35.2
010
203040
506070
8090
Awareness Treatment Controlled
Per
cen
t o
f P
op
ula
tio
n W
ith
H
yper
ten
sio
n
Total Population NH Whites NH Blacks Mexican Americans

Smoking Statement Issued in 1956 by Smoking Statement Issued in 1956 by American Heart AssociationAmerican Heart Association
““It is the belief of the committee that much It is the belief of the committee that much greater knowledge is neededgreater knowledge is needed before any before any conclusions can be drawn concerning conclusions can be drawn concerning relationships between smoking and relationships between smoking and death rates from coronary heart disease. death rates from coronary heart disease. The acquisition of such knowledge may The acquisition of such knowledge may well require the use of techniques and well require the use of techniques and research methods that have not hitherto research methods that have not hitherto been applied to this problem.”been applied to this problem.”
Circulation 1960; vol. 23Circulation 1960; vol. 23
___________________________________________________________
____________________________________________________________
___________________________________________________________

CHD Risk by Cigarette Smoking. Filter CHD Risk by Cigarette Smoking. Filter Vs. Non-filter. Framingham StudyVs. Non-filter. Framingham Study.. Men Men <55 Yrs.<55 Yrs.
0
50
100
150
200
250
Total CHD MyocardialInfarction
Non-SmokerReg. Cig. SmokerFilter Cig. Smoker
14-yr. Rate/1000
119
206210
59
112
210

Prevalence of students in grades 9 to 12 reporting current cigarette use by sex and race/ethnicity (YRBSS, 2009)
Source: MMWR Surveill Summ. 2010;59:1–142.NH indicates non-Hispanic.
©2011 American Heart Association, Inc. All rights reserved. Roger VL et al. Published online in Circulation Dec. 15, 2011

Prevalence of current smoking for adults > 18 years of age by race/ethnicity and sex (NHIS: 2007-2009)
All percentages are age-adjusted. NH indicates non-Hispanic. *Includes both Hispanics and non-Hispanics. Data derived from Centers for Disease Control and Prevention/National Center for Health Statistics, Health Data Interactive.
©2011 American Heart Association, Inc. All rights reserved. Roger VL et al. Published online in Circulation Dec. 15, 2011


Diseases of The HeartDiseases of The HeartCharles K Friedberg MD, WB Charles K Friedberg MD, WB Saunders Co. Philadelphia, 1949Saunders Co. Philadelphia, 1949
““The proper control of The proper control of diabetes diabetes is is obviously desirable even though obviously desirable even though there is there is uncertainty uncertainty as to whether as to whether coronary atherosclerosis is more coronary atherosclerosis is more frequent or severe in the frequent or severe in the uncontrolled diabetic” uncontrolled diabetic”
________________________________________________________________
______________________________________________________________
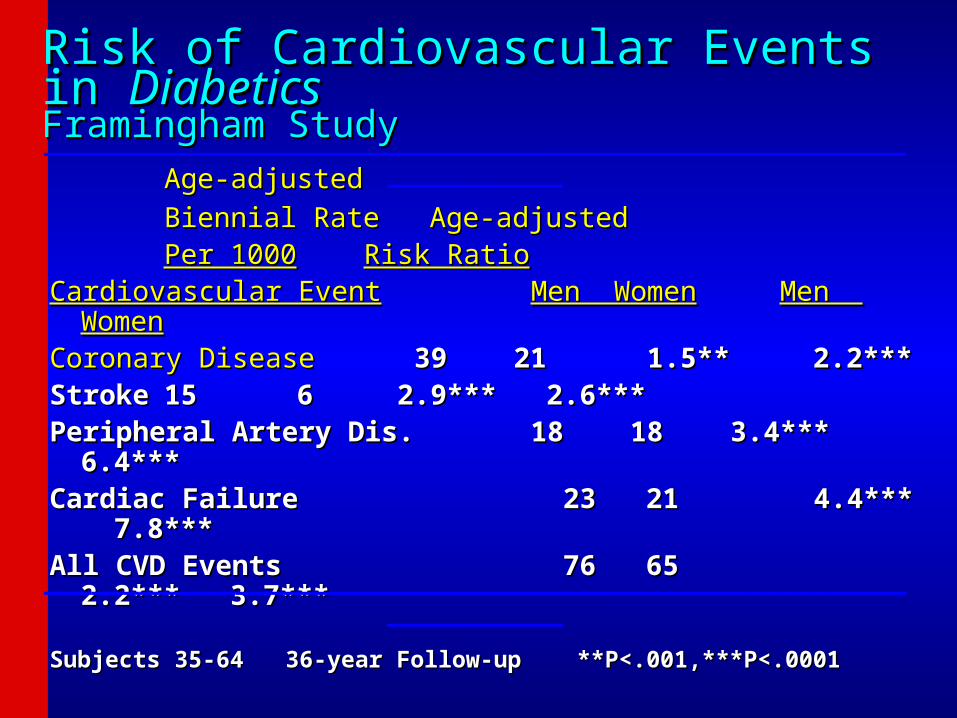
Risk of Cardiovascular Events in Risk of Cardiovascular Events in DiabeticsDiabetics Framingham StudyFramingham Study
Age-adjustedAge-adjusted
Biennial Rate Age-adjustedBiennial Rate Age-adjusted Per 1000Per 1000 Risk RatioRisk Ratio
Cardiovascular EventCardiovascular Event Men WomenMen Women Men WomenMen WomenCoronary DiseaseCoronary Disease 39 2139 21 1.5** 2.2*** 1.5** 2.2***StrokeStroke 15 615 6 2.9*** 2.6*** 2.9*** 2.6***Peripheral Artery Dis. 18 18Peripheral Artery Dis. 18 18 3.4*** 6.4*** 3.4*** 6.4***Cardiac FailureCardiac Failure 23 21 23 21 4.4*** 7.8*** 4.4*** 7.8***All CVD EventsAll CVD Events 76 65 2.2*** 76 65 2.2***
3.7***3.7***
Subjects 35-64 36-year Follow-up **P<.001,***P<.0001Subjects 35-64 36-year Follow-up **P<.001,***P<.0001
_________________________________________________________________
_________________________________________________________________


Skepticism About Importance of ObesitySkepticism About Importance of Obesity
Keys A, Aravanis C, Blackburn H, et al. Ann Intern Med 1972; 77:15-27.
Concluded that all the excess risk of coronary heart disease in the obese derives from its atherogenic accompaniments, illogically leaving the impression that obesity is therefore unimportant.
Mann GV. N Engl J Med 1974; 291:226-232.
“The contribution of obesity to CHD is either small or non-existent. It cannot be expected that treating obesity is either logical or a promising approach to the management of CHD”.
Barrett-Connor EL. Ann Intern Med 1985; 103:1010-1019
NIH consensus panel is equivocal about the role of obesity as a cause of CHD.

Relation of Weight Change to Changes in
Atherogenic Traits: The Framingham Study
Frantz Ashley, Jr. and William B Kannel
J Chronic Dis 1974
“Weight gain is accompanied by atherogenic alterations in blood lipids, blood pressure, uric acid and carbohydrate tolerance.”
“It seems reasonable to expect that correction of overweight will improve the coronary risk problem.”
“Avoidance of overweight would seem a desirable goal in the general population if the appalling annual toll from disease is to be substantially reduced.”

©2011 American Heart Association, Inc. All rights reserved. Roger VL et al. Published online in Circulation Dec. 15, 2011
Trends in the prevalence of obesity among US children and adolescents by age and survey year (National Health and Nutrition Examination Survey: 1971-1974, 1976-1980, 1988-1994, 1999-
2002 and 2005–2008)
Data derived from Health, United States, 2010: With Special Feature on Death and Dying. NCHS, 2011.

©2011 American Heart Association, Inc. All rights reserved. Roger VL et al. Published online in Circulation Dec. 15, 2011
Age-adjusted prevalence of obesity in adults 20–74 years of age, by sex and survey year (NHES: 1960–62; NHANES: 1971–74, 1976–80, 1988–94, 1999-2002 and 2005-08)
Data derived from Health, United States, 2010: With Special Feature on Death and Dying. NCHS, 2011.

Framingham Heart Study: Kannel et al., 1961

Why Use Risk Scores?
1)As early as 1976, former Framingham director Dr. William Kannel had noted risk functions provide an “economic and efficient method of identifying persons at high cardiovascular risk who need preventive treatment and persons at low risk who need not be alarmed about one moderately elevated risk characteristic” (AJC 1976)2)The ACC Bethesda Conference noted the intensity of treatment should match a person’s risk (Califf RM, JACC 1996).3)Studies show a physician’s estimate is only accurate 24% of the time (Pignone et al, BMC health Serv Res 2003).4)Routine use of global risk scores leads to greater use of guideline-based therapy and modest improvements in intermediate outcomes with no harm identified (Sheridan et al. BMC Health Serv Res 2008).

Key Risk Scores Used in CHD and CVD PredictionKey Risk Scores Used in CHD and CVD PredictionRisk Score (year) Endpoint Definition
Framingham, 1991 (Anderson) 10-year all CHD CHD death, MI, unstable angina, angina
Framingham, 1998 (Wilson) 10-year all CHD and hard CHD
CHD death, MI, unstable angina, angina
ATP III, 2001 (Framingham) 10-year hard CHD CHD death, nonfatal MI
PROCAM 2002 (Germany) 10-year hard CHD CHD death, non-fatal MI
European SCORE 2003 and after 10-year CVD death CVD death only (country and region specific)
QRISK 2007 (England and Wales)
10-year global CVD CVD death, MI, stroke, revascularization
Reynolds women (2007) and men (2008) (Boston, USA)
10-year global CVD CHD death, MI, stroke, revascularization
Framingham Global CVD 2008 10-year global CVD CVD death, all CHD, stroke, heart failure, claudication
Pooled Cohort Equations 2013 (USA)
10-year and lifetime ASCVD
Nonfatal/fatal MI & stroke

Point Total 10-Year Risk Point Total 10-Year Risk
<9 <1% 2011%
9 1% 2114%
10 1% 2217%
11 1% 2322%
12 1% 2427%
13 2% 25 30%
14 2%15 3%16 4%17 5%18 6%19 8%
Assessing CHD Risk in WomenAssessing CHD Risk in Women
Note: Risk estimates were derived from the experience of the Framingham Heart Study,
a predominantly Caucasian population in Massachusetts, USA.
Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285:2486-2497.
Step 1: Age
YearsPoints
20-34 -735-39 -340-44 045-49 350-54 655-59 860-64 1065-69 1270-74 1475-79 16
TC Points at Points at Points at Points atPoints at(mg/dL) Age 20-39 Age 40-49 Age 50-59 Age 60-69
Age 70-79 <160 0 0 0 0
0160-199 4 3 2 1
1200-239 8 6 4 2
1240-279 11 8 5 3
2280 13 10 7 4
2
HDL-C(mg/dL) Points
60 -1
50-59 0
40-49 1
<40 2
Step 3: HDL-Cholesterol
Systolic BP PointsPoints
(mm Hg) if Untreated if Treated
<120 0 0120-129 1 3130-139 2 4140-159 3 5160 4 6
Step 4: Systolic Blood Pressure
Step 5: Smoking Status
Points at Points at Points at Points at Points at Age 20-39 Age 40-49 Age 50-59 Age 60-69 Age 70-79
Nonsmoker 0 0 0 0 0Smoker 9 7 4 2 1
Age
Total cholesterol
HDL-cholesterol
Systolic blood pressure
Smoking status
Point total
Step 6: Adding Up the Points
Step 7: CHD Risk
Step 2: Total Cholesterol
ATP III Framingham Risk Scoring
© 2001, Professional Postgraduate Services®
www.lipidhealth.org

Risk Category LDL-C GoalInitiate
TLCConsider
Drug Therapy
High risk: CHD or CHD risk equivalents (10-year risk >20%)
<100 mg/dL (optional goal:
<70 mg/dL)
100 mg/dL
100 mg/dL (<100 mg/dL:
consider drug Rx)
Moderately high risk: 2+ risk factors (10-year risk 10% to 20%)
<130 mg/dL (optimal <100
mg/dL)
130 mg/dL
130 mg/dL (100-129 mg/dL:
consider Rx )
Moderate risk: 2+ risk factors (risk <10%)
<130 mg/dL130 mg/dL
160 mg/dL
Lower risk: 0-1 risk factor
<160 mg/dL160 mg/dL
190 mg/dL
Adapted from Grundy SM, et al. Adapted from Grundy SM, et al. CirculationCirculation. 2004;110:227-239.. 2004;110:227-239.
ATP III Update ATP III Update ( 2004 )( 2004 ) LDL-C Treatment TargetsLDL-C Treatment Targets

10-Year Framingham Total Cardiovascular Disease Risk Score (D’Agostino et al, 2008)
Global Risk Scoring: Class 1a ACCF/AHA Guideline for Assessment of Cardiovascular Risk in Asymptomatic Adults, Circulation 2010

Recommendation to begin with a global risk assessment using the Pooled Cohort Equations to estimate 10-year ASCVD Risk

Pooled Cohort Equations 10-year ASCVD Risk Calculator (Framingham, ARIC, CARDIA, and CHS)

Lifetime Risks of Cardiovascular Disease Death by Lifetime Risks of Cardiovascular Disease Death by Number of Risk Factors and Attained Age Number of Risk Factors and Attained Age (Berry et al. , 2012)(Berry et al. , 2012)
Men WomenOptimal risk factors: total cholesterol <180 mg/dl, blood pressure <120/80, non-smoking, non-diabetic.Major risk factors: current smoker, diabetes, treated cholesterol or untreated cholesterol >=240 mg/dl, treated hypertension or untreated systolic BP >=160 mmHg or diastolic BP>=100 mmHg.

Lifetime Risk of CHD Increases with Lifetime Risk of CHD Increases with Serum CholesterolSerum Cholesterol
0
10
20
30
40
50
60
Per
cen
t
Men Women
<200 mg
200-239 mg
>240 mg
Framingham Study: Subjects age 40 years
DM Lloyd-Jones et al Arch Intern Med 2003; 1966-1972
34
44
57
19
2933
Cholesterol
___________________________________________________________________________
_______________________________________________________________________________

Relation of Non-Hypertensive Blood Relation of Non-Hypertensive Blood Pressure to Cardiovascular DiseasePressure to Cardiovascular DiseaseVasan R, et al. N Engl J Med 2001; 345:1291-1297Vasan R, et al. N Engl J Med 2001; 345:1291-1297
0%
2%
4%
6%
8%
10%
12%
Women Men
<120/80 mm Hg
120-129/80-84 mm Hg
130-139/85-89 mm Hg
10-year Age- Adjusted Cumulative Incidence
Hazard Ratio*
SBP Women Men
<120/80 1.0 1.0 120-129 1.5 1.3 130-139 2.5 1.6
H.R. adjusted for age, BMI, Cholesterol, Diabetes and smoking *P<.001
Framingham Study: Subjects Ages 35-90 yrs.
1.9
2.8
4.4
5.8
7.6
10.1

Risk of Cardiovascular Events in Risk of Cardiovascular Events in DiabeticsDiabetics Framingham StudyFramingham Study
Age-adjustedAge-adjusted
Biennial Rate Age-adjustedBiennial Rate Age-adjusted Per 1000Per 1000 Risk RatioRisk Ratio
Cardiovascular EventCardiovascular Event Men WomenMen Women Men WomenMen WomenCoronary DiseaseCoronary Disease 39 21 39 21 1.5** 1.5** 2.2***2.2***StrokeStroke 15 6 15 6 2.9*** 2.6*** 2.9*** 2.6***Peripheral Artery Dis. 18 18Peripheral Artery Dis. 18 18 3.4*** 3.4*** 6.4***6.4***Cardiac FailureCardiac Failure 23 21 23 21 4.4*** 4.4*** 7.8***7.8***All CVD EventsAll CVD Events 76 65 2.2*** 76 65 2.2*** 3.7***3.7***
Subjects 35-64 36-year Follow-up **P<.001,***P<.0001Subjects 35-64 36-year Follow-up **P<.001,***P<.0001
_________________________________________________________________
_________________________________________________________________

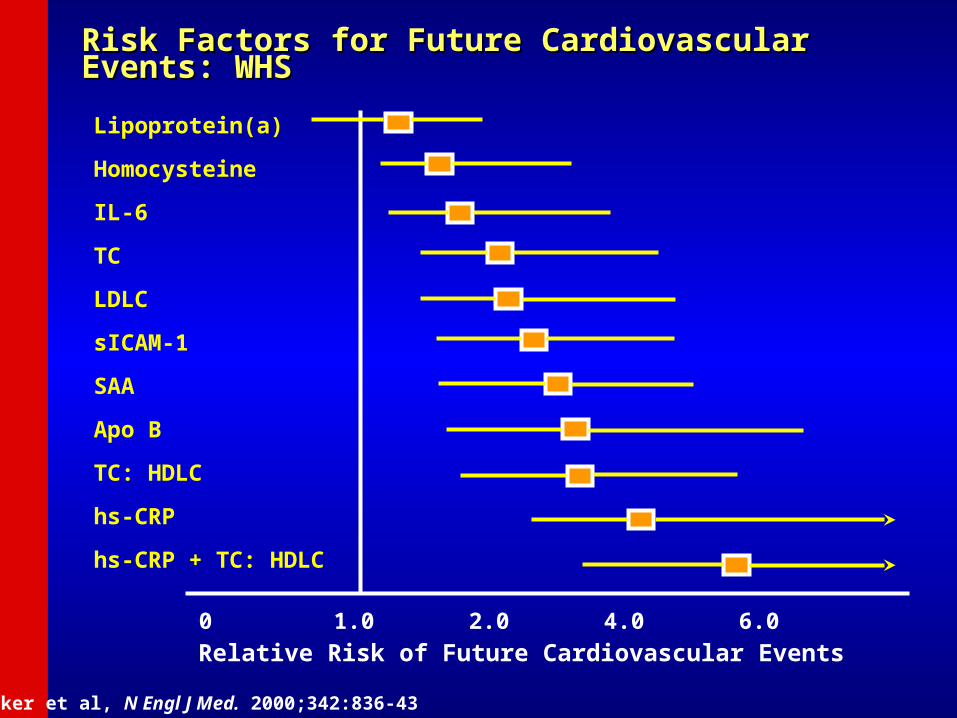
Risk Factors for Future Cardiovascular Events: WHSRisk Factors for Future Cardiovascular Events: WHS
0 1.0 2.0 4.0 6.0
Lipoprotein(a)
Homocysteine
IL-6
TC
LDLC
sICAM-1
SAA
Apo B
TC: HDLC
hs-CRP
hs-CRP + TC: HDLC
Relative Risk of Future Cardiovascular Events
Ridker et al, N Engl J Med. 2000;342:836-43

Cardiovascular Health Cardiovascular Health StudyStudy
• 5,201 Medicare eligible individuals aged 65-102 at baseline 5,201 Medicare eligible individuals aged 65-102 at baseline enrolled beginning 1992 at six field centers.enrolled beginning 1992 at six field centers.
• Assessment of newer and older risk factors.Assessment of newer and older risk factors.• Ongoing follow-up of cardiovascular events and mortalityOngoing follow-up of cardiovascular events and mortality• Subclinical disease measures included:Subclinical disease measures included:
– carotid B-mode ultrasound for carotid IMT at Year 2, carotid B-mode ultrasound for carotid IMT at Year 2, Year 7, and Year 11Year 7, and Year 11
– m-mode echocardiographic measures of left ventricular m-mode echocardiographic measures of left ventricular mass and dimensions, left atrial dimension done at mass and dimensions, left atrial dimension done at baseline (Year 2) (at UC Irvine) and follow-up (Year 7) baseline (Year 2) (at UC Irvine) and follow-up (Year 7) examinations. examinations.
– Ankle brachial index (ABI) for measurement of PAD Ankle brachial index (ABI) for measurement of PAD – Pulmonary function (FVC and FEV1)Pulmonary function (FVC and FEV1)


Cardiovascular Health Study: Cardiovascular Health Study: Combined intimal-medial thickness Combined intimal-medial thickness predicts total MI and strokepredicts total MI and stroke
Cardiovascular Health Study (CHS) (aged 65+): MI or stroke rate 25% over 7 years in those at highest quintile of combined IMT (O’Leary et al. 1999)

Multiethnic Study of Multiethnic Study of AtherosclerosisAtherosclerosis
• 6,814 adults aged 45-80 enrolled at 6 field centers, 6,814 adults aged 45-80 enrolled at 6 field centers, including Caucasians, African-Americans, including Caucasians, African-Americans, Hispanics, and Chinese beginning 2000.Hispanics, and Chinese beginning 2000.
• Extensive assessment of standard and novel risk Extensive assessment of standard and novel risk factors, unique blood cohort among 1000 factors, unique blood cohort among 1000 subjects.subjects.
• Multiple evaluations of carotid IMT, ABI, and Multiple evaluations of carotid IMT, ABI, and coronary calcium. Ancillary studies of LV size coronary calcium. Ancillary studies of LV size and extracoronary measures of calcification and extracoronary measures of calcification (Harbor-UCLA) and abdominal aortic calcium (UC (Harbor-UCLA) and abdominal aortic calcium (UC San Diego) in full or partial cohorts.San Diego) in full or partial cohorts.

MESA Study Design FeaturesMESA Study Design Features
Four examinations approximately two years apart, Four examinations approximately two years apart, exam 5 just completedexam 5 just completed
Major risk factors measured at each examMajor risk factors measured at each examCoronary calcium measured in entire cohort at Coronary calcium measured in entire cohort at
Exam 1, ½ cohort at Exam 2, ½ cohort at Exam Exam 1, ½ cohort at Exam 2, ½ cohort at Exam 3, and in about 1000 pts in Exam 4.3, and in about 1000 pts in Exam 4.
Carotid IMT measured at Exam 1 and 2-3.Carotid IMT measured at Exam 1 and 2-3.Cardiac MRI measured at Exam 1 and 2-3Cardiac MRI measured at Exam 1 and 2-3Ankle Brachial IndexAnkle Brachial IndexPulse wave analysisPulse wave analysisEndothelial function measuresEndothelial function measuresFollow-up for CVD events and incident DM, Follow-up for CVD events and incident DM,
mortalitymortality

Cumulative Incidence of Any Cumulative Incidence of Any Coronary Event by Coronary Coronary Event by Coronary Calcium Score: MESA Study Calcium Score: MESA Study (Detrano et al., NEJM 2008)(Detrano et al., NEJM 2008)

Intermediate Risk MESA Subjects (n=1330)
C-statistics:
FRS alone 0.623FRS+CAC 0.784 (p<0.001)FRS+CIMT 0.652 (p=0.01)FRS+FMD 0.639 (p=0.06)FRS+CRP 0.640 (p=0.03)FRS+FamHx 0.675 (p=0.001)FRS+ABI 0.650 (p=0.01)
Yeboah J et al, JAMA 2012

Coronary Artery Risk Development in Coronary Artery Risk Development in Young Adults (CARDIA)Young Adults (CARDIA) – 5,115 adults – 5,115 adults (half African-American) aged 18-30 at (half African-American) aged 18-30 at baseline in 1985 enrolled at 4 field baseline in 1985 enrolled at 4 field centers. centers. – Ongoing evaluation (Year 20 exam recently Ongoing evaluation (Year 20 exam recently
completed). completed). – Echocardiographic M-mode and 2D Echocardiographic M-mode and 2D
measures available at Year 5 and Year 10 measures available at Year 5 and Year 10 exams (UC Irvine Echo Reading Center) exams (UC Irvine Echo Reading Center)
– CT Coronary Calcium at Years 15 (Harbor-CT Coronary Calcium at Years 15 (Harbor-UCLA) and 20 (Wake Forest University)UCLA) and 20 (Wake Forest University)

NHANES Cross-Sectional and NHANES Cross-Sectional and Mortality Follow-up StudiesMortality Follow-up Studies
• NHES 1960, NHANES II 1976, NHES 1960, NHANES II 1976, NHANES III 1988-1994, and NHANES III 1988-1994, and NHANES IV 2000-2012 cross-NHANES IV 2000-2012 cross-sectional health survey and clinic sectional health survey and clinic exam dataexam data
• NHES, NHANES 2,3 Mortality NHES, NHANES 2,3 Mortality Follow-upFollow-up

---------------------------------------------------------------
15
0
5
10
20
25
30
35
40
Ev
ents
/10
0 P
ati
en
ts*
0 1 2 3 4-5
# of RFs (any combination)
• SBP >140 mm Hg orDBP >80 mm Hg
• TC >240 mg/dL
• BMI >27.3 kg/m2 (women) >27.8 kg/m2 (men)
• Current smoker
• Diabetes
Yusuf HR, et al. Prev Med. 1998;27:1-9.
Risk for CHD Increases with the Number of Risk Factors: NHANES/NHEFS
*Cumulative 21 yr. incidence *1971-1992.
6.3
15.3
22.3
29.7
35.0 Risk Factors (RFs)N = 12,932

<40 40-49 50-59 60-69 70-79 80+Age (y)
17% 16% 16% 20% 20% 11%
Distribution of HTN Subtypes in the untreated Distribution of HTN Subtypes in the untreated Hypertensive Population in NHANES III by AgeHypertensive Population in NHANES III by Age
ISH (SBP 140 mm Hg and DBP <90 mm Hg) SDH (SBP 140 mm Hg and DBP 90 mm Hg)IDH (SBP <140 mm Hg and DBP 90 mm Hg)
0
20
40
60
80
100
Numbers at top of bars represent the overall percentage distribution of untreated hypertension by age. Franklin et al. Hypertension 2001;37: 869-874.
Frequency of hypertensionsubtypes in all untreated
hypertensives (%)

Does DM Carry a CVD or Mortality Risk Equivalent?Does DM Carry a CVD or Mortality Risk Equivalent?US Men and Women Ages 30-74US Men and Women Ages 30-74(age, gender, and risk-factor adjusted Cox regression) NHANES II Follow-(age, gender, and risk-factor adjusted Cox regression) NHANES II Follow-Up (n=6255)Up (n=6255)(Malik and Wong, et al., (Malik and Wong, et al., Circulation 2004; 110: 1245-1250Circulation 2004; 110: 1245-1250))
0
1
2
3
4
5
6
7
Rel
ativ
e R
isk
CHD Mortality CVD Mortality Total Mortality
NoneMetSDiabetesCVDCVD+Diabetes
* p<.05, ** p<.01, **** p<.0001 compared to none
*
***
***
***
**
***
***
***
******
***

Mylifecheck.heart.orgMylifecheck.heart.org

24.533.8 31.7
76.8
15.0 17.18.2
3.2
32.9
23.2
22.9
38.441.2
30.4
72.2
33.2
45.2 46.641.7
61.4
0.0
20.0
40.0
60.0
80.0
100.0
CurrentSmoking
Body MassIndex
PhysicalActivity
Healthy DietScore
TotalCholesterol
BloodPressure
FastingPlasmaGlucose
Pe
rce
nta
ge
Poor Intermediate Ideal
Age-standardized prevalence estimates for poor, intermediate and ideal cardiovascular health for each of the seven metrics of
cardiovascular health in the AHA 2020 goals, among US adults >20 years of age, NHANES 2005-2006 (baseline available data as of
January 1, 2010).
©2010 American Heart Association, Inc. All rights reserved. Roger VL et al. Published online in Circulation Dec. 15, 2010
Fewer than 1% of US adults are at ideal levels for all 7 measures of cardiovascular health!

Ideal Cardiovascular Health and Ideal Cardiovascular Health and CVD Incidence: ARIC Study CVD Incidence: ARIC Study (Folsom et al, JACC 2011)(Folsom et al, JACC 2011)

Risk Factor ConsortiaRisk Factor Consortia• The Emerging Risk Factors Collaboration incorporating over 1.3 The Emerging Risk Factors Collaboration incorporating over 1.3
million person years at risk demonstratemillion person years at risk demonstrate– the independent predictive value of C-reactive protein with the independent predictive value of C-reactive protein with
CHD and stroke among 54 prospective studies (Lancet 2010)CHD and stroke among 54 prospective studies (Lancet 2010)– the clinical utility of C-reactive protein and fibrinogen (NEJM the clinical utility of C-reactive protein and fibrinogen (NEJM
2012)2012)– the limited role of adding the novel lipid markers the limited role of adding the novel lipid markers
apolipoprotein B, apolipoprotein A1, lipoprotein (a) and apolipoprotein B, apolipoprotein A1, lipoprotein (a) and lipoprotein-associated phospholipase A2 to traditional lipid lipoprotein-associated phospholipase A2 to traditional lipid measures (JAMA 2012). measures (JAMA 2012).
• The group also showed in 97 prospective studies the strong The group also showed in 97 prospective studies the strong relation of diabetes with deaths from vascular disease and other relation of diabetes with deaths from vascular disease and other causes (NEJM 2011).causes (NEJM 2011).

Multinational Registries of Multinational Registries of CAD PatientsCAD Patients
• Euroaspire I, II, III, IV (just completed Euroaspire I, II, III, IV (just completed 2013) – compares adherence to 2013) – compares adherence to recommended lifestyle and therapies in recommended lifestyle and therapies in secondary prevention across European secondary prevention across European countries.countries.
• Prospective Urban Rural Epidemiology Prospective Urban Rural Epidemiology (PURE) – 139,506 subjects enrolled (PURE) – 139,506 subjects enrolled among 600 communities in 17 low, among 600 communities in 17 low, middle and high income countries.middle and high income countries.

Yusuf S et al. Lancet. 2011;378(9798):1231-43
N.Amerrica/Europe
S.America
Middle East
S.Asia
China
Malaysia
AfricaPer
cen
tag
e(%
)
55.4%
32.8%
52.7%
11.6%14.9%
3.4%
15.5%
Antiplatelets
60
50
40
30
20
10
0
45.4%
37.0%
44.9%
11.9% 12.5%
1.9%6.8%
504540353025201510 5 0
Beta-blockers
46.8%
40.2%
26.2%
6.4% 12.8%
6.8%7.8%
504540353025201510 5 0
ACE-1/ARB
56.7%
19.0%
37.3%
4.8%
15.9%
1.4%2.0%
60
50
40
30
20
10
0
Statins
Big Gap in use ofEvidence Based Drugs for Secondary Prevention in China
PURE study
Per
cen
tag
e(%
)P
erce
nta
ge(
%)
Per
cen
tag
e(%
)

113
28.9
18.6
11.2
8.6
Placebo Only
Statin Only
Statin+ASA
Statin+ASA+BB
0 5 10 15 20 25 30 35
Coronary Event Rate (%)
Placebo 24% Statin 24% Statin+ASA 8% Statin+ASA+Beta Blocker 18%
Treatment in 4S 4444 Patients with CAD Only statin vs placebo randomized 5.4 years F/U
Interaction Between Therapies to Treat AtherosclerosisInteraction Between Therapies to Treat Atherosclerosis
70% Reduction


What are the Cost Savings from What are the Cost Savings from Prevention Strategies in the US?Prevention Strategies in the US?• Community-based programs to increase physical
activity, improve nutrition, prevent smoking would provide a $5.60 return on investment for every $1 spent within 5 years
• Comprehensive worksite wellness and school based programs would reduce medical costs by $3.27 and absenteeism costs by $2.73 for every $1 spent
• Building bike and pedestrian trials would save $3 in medical cost savings for every $1 spent
Weintraub et al. Circulation 2011

What are the Cost Savings from What are the Cost Savings from Prevention Strategies in the US?Prevention Strategies in the US?
• Reducing the population sodium intake to 1500 mg/day would save $26.2 billion in healthcare savings annually
• A 40% cigarette price increase from taxes would reduce smoking to 15.2% by 2025 with large gains in quality adjusted life years (QALYs) (13 milllion) saving $682 billion
• Eliminating exposure to second hand smoke would save $10 billion annually in healthcare costs
• Comprehensive coverage on smoking cessation programs results in a $3 return per $1 spent
• Adherence to ATP III lipid primary prevention guidelines would cost of $42,000 and BP therapy $37,100 per life year saved