Cardiorenal Syndrome
18
This lecture was conducted during the Nephrology Unit Grand Ground by Medical Student rotated under Nephrology Division under the supervision and administration of Prof. Jamal Al Wakeel, Head of Nephrology Unit, Department of Medicine and Dr. Abdulkareem Al Suwaida. Nephrology Division is not responsible for the content of the presentation for it is intended for learning and /or education purpose only.
description
crs
Transcript of Cardiorenal Syndrome

This lecture was conducted during the Nephrology Unit Grand Ground by Medical Student rotated under Nephrology Division under the supervision and administration of Prof. Jamal Al Wakeel, Head of Nephrology Unit, Department of Medicine and Dr. Abdulkareem Al Suwaida. Nephrology Division is not responsible for the content of the presentation for it is intended for learning and /or education purpose only.
Ahmad AL-KhorisiAhmad AL-KhorisiMedical Intern – King Saud UniversityMedical Intern – King Saud University
February 2010February 2010
Cardio - Renal Syndrome ( CRS ) Cardio - Renal Syndrome ( CRS )
Adapted from: Adapted from: Narayan Pokhrel, MD, Najindra Maharjan, MD, Bismita Dhakal, PharmD, and Rohit R Arora, MD FACC FAHA FACP FSCAI : “: “Cardiorenal syndrome: A literature review ””
CASE PRESENTATIONCASE PRESENTATIONA 71-year-old man presented to the A 71-year-old man presented to the emergency department (ED) with emergency department (ED) with complaints of severe shortness of breath complaints of severe shortness of breath and chest pain. His past medical history and chest pain. His past medical history was significant for hypertension, chronic was significant for hypertension, chronic heart failure (CHF)-New York Heart heart failure (CHF)-New York Heart Association (NYHA) class IV and chronic Association (NYHA) class IV and chronic kidney disease, with temporary dialysis kidney disease, with temporary dialysis performed three times for acute-on-performed three times for acute-on-chronic renal failure. chronic renal failure.
Bilateral crackles in the chest and pedal Bilateral crackles in the chest and pedal edema were found on clinical examination.edema were found on clinical examination.
Chest radiography showed cardiomegaly Chest radiography showed cardiomegaly with a small right pleural effusion and with a small right pleural effusion and pulmonary vascular congestion.pulmonary vascular congestion.
Echocardiography showed marked left Echocardiography showed marked left ventricular hypertrophy (LVH) with ventricular hypertrophy (LVH) with diastolic dysfunction, ejection fraction (EF) diastolic dysfunction, ejection fraction (EF) of 40%, and pulmonary artery systolic of 40%, and pulmonary artery systolic pressure of 45 mmHg to 50 mmHg.pressure of 45 mmHg to 50 mmHg.
His blood urea nitrogen level was 22 mmol/L His blood urea nitrogen level was 22 mmol/L and serum creatinine was 197.04 μmol/L .and serum creatinine was 197.04 μmol/L .
The patient was admitted with a diagnosis of The patient was admitted with a diagnosis of CHF exacerbation and was treated with CHF exacerbation and was treated with furosemide.furosemide.
During the course of treatment, he During the course of treatment, he developed acute-on-chronic renal failure developed acute-on-chronic renal failure with serum creatinine level rising to 4.7 with serum creatinine level rising to 4.7 mg/dL (415.29 μmol/L), necessitating mg/dL (415.29 μmol/L), necessitating hemodialysis. hemodialysis.

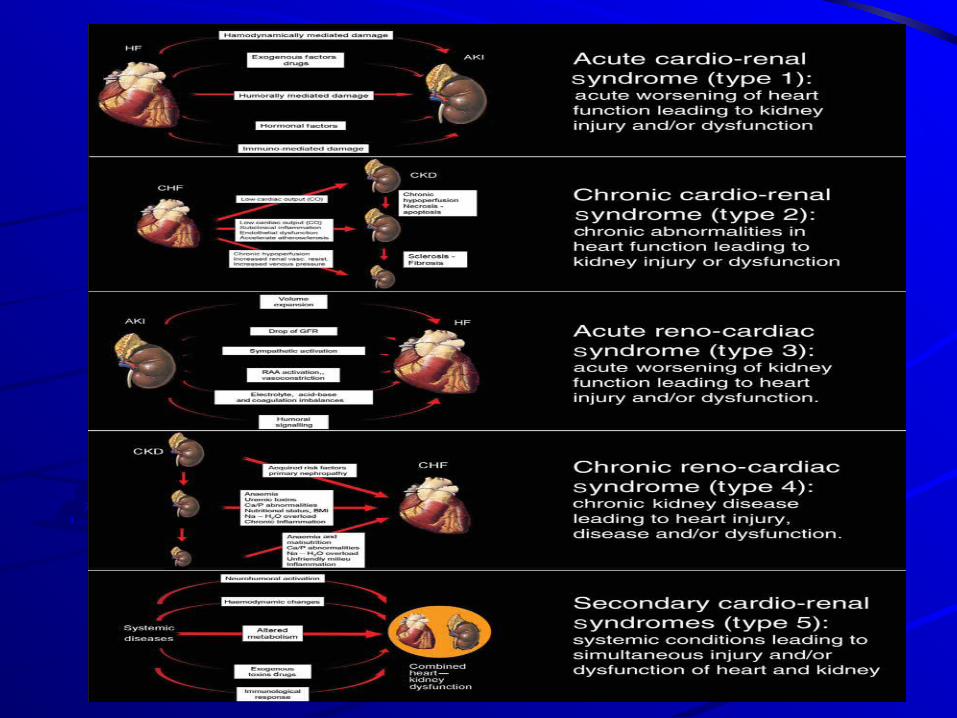
DEFINITION OF CRSDEFINITION OF CRSThe CRS can generally be defined as a The CRS can generally be defined as a pathophysiological disorder of the heart and kidneys pathophysiological disorder of the heart and kidneys whereby acute or chronic dysfunction in one organ whereby acute or chronic dysfunction in one organ may induce acute or chronic dysfunction in the other may induce acute or chronic dysfunction in the other organ.organ.
This proposed definition divides CRS into five This proposed definition divides CRS into five subtypes: type I, acute CRS; type II, chronic CRS; type subtypes: type I, acute CRS; type II, chronic CRS; type III, acute renocardiac syndrome; type IV, chronic III, acute renocardiac syndrome; type IV, chronic renocardiac syndrome; and type V, secondary CRS, renocardiac syndrome; and type V, secondary CRS, meaning systemic diseases such as diabetes, sepsis meaning systemic diseases such as diabetes, sepsis and amyloidosis causing simultaneous cardiac and and amyloidosis causing simultaneous cardiac and renal dysfunction .renal dysfunction .
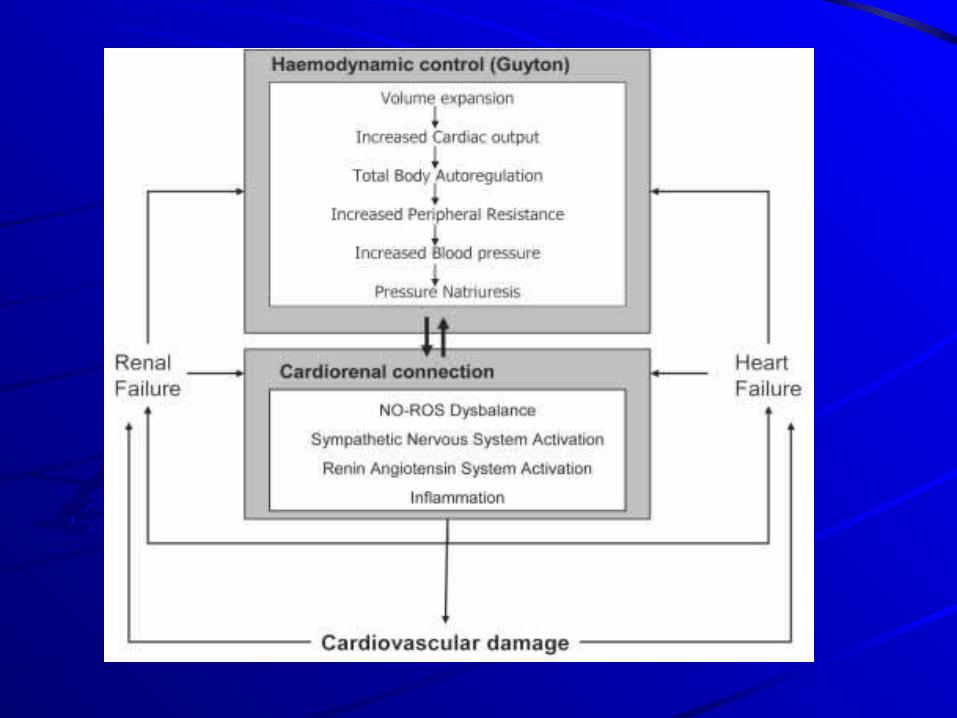
PATHOPHYSIOLOGYPATHOPHYSIOLOGYThe mechanism underlying the interplay of The mechanism underlying the interplay of cardiac failure and kidney dysfunction is cardiac failure and kidney dysfunction is still not completely understood.still not completely understood.
Decline in cardiac function causing Decline in cardiac function causing decrease in tissue perfusion, and thus, decrease in tissue perfusion, and thus, adversely affecting renal perfusion is well adversely affecting renal perfusion is well known and provide an explanation for known and provide an explanation for some aspects of cardiorenal syndrome.some aspects of cardiorenal syndrome.
Nonetheless, some studies proved worsening of Nonetheless, some studies proved worsening of kidney function had no correlation with ejection kidney function had no correlation with ejection fraction.fraction.
Similarly, changes in body weight and diuresis Similarly, changes in body weight and diuresis was not significantly related to the development was not significantly related to the development of kidney dysfunction amongst hospitalized of kidney dysfunction amongst hospitalized patients with heart failure.patients with heart failure.
These observations reflect that the These observations reflect that the pathophysiology of kidney dysfunction in the pathophysiology of kidney dysfunction in the context of heart disease is much more complex context of heart disease is much more complex than simple reduction of cardiac output. than simple reduction of cardiac output.
MANAGEMENTMANAGEMENTThe heterogeneous and complex The heterogeneous and complex pathophysiology of CRS makes patient pathophysiology of CRS makes patient management an intricate clinical management an intricate clinical challenge.challenge.
To date, there is no single success-To date, there is no single success-guaranteed treatment for CRS because guaranteed treatment for CRS because each patient has his or her own unique each patient has his or her own unique medical history, risk profile and medical history, risk profile and combination of comorbidities.combination of comorbidities.
Body weight of the patient is the single Body weight of the patient is the single most important indicator while managing most important indicator while managing CRS .CRS .
The patient needs continuous The patient needs continuous hemodynamic monitoring, especially if his hemodynamic monitoring, especially if his or her blood pressure is low and the filling or her blood pressure is low and the filling pressure is uncertain. pressure is uncertain.
It is better to restrict the intake of free It is better to restrict the intake of free water to less than 1000 mL per 24 h if the water to less than 1000 mL per 24 h if the patient is hyponatremic.patient is hyponatremic.
Diuretics :Diuretics :Despite limited clinical trial data suggesting a Despite limited clinical trial data suggesting a beneficial role, diuretics have long been beneficial role, diuretics have long been considered to be an initial and essential part of considered to be an initial and essential part of the management of CRS patients.the management of CRS patients.
The importance of diuretics is illustrated by data The importance of diuretics is illustrated by data from the Acute Decompensated Heart Failure from the Acute Decompensated Heart Failure National Registry (ADHFNR), which revealed that National Registry (ADHFNR), which revealed that 80.8% of patients enrolled in this registry were on 80.8% of patients enrolled in this registry were on chronic diuretic therapy at the time of chronic diuretic therapy at the time of presentation, and 88% were treated acutely with presentation, and 88% were treated acutely with an intravenous diuretic during their admission for an intravenous diuretic during their admission for ADHFADHF
Loop, thiazide and potassium-sparing Loop, thiazide and potassium-sparing diuretics provide diuresis and natriuresis in as diuretics provide diuresis and natriuresis in as quickly as 20 min after administration. quickly as 20 min after administration. Moreover, they provide effective short-term Moreover, they provide effective short-term symptomatic relief. However, the use of symptomatic relief. However, the use of diuretics is not free from drawbacks, such as diuretics is not free from drawbacks, such as long-term deleterious cardiovascular effects.long-term deleterious cardiovascular effects.
However, in the absence of definitive data, However, in the absence of definitive data, patients with volume overload should not be patients with volume overload should not be restricted from receiving loop or thiazide restricted from receiving loop or thiazide diuretics as necessary to alleviate symptoms diuretics as necessary to alleviate symptoms
Last massageLast massage
As renal dysfunction radically worsens the As renal dysfunction radically worsens the prognosis of patients with heart failure, prognosis of patients with heart failure, heart failure conversely worsens the heart failure conversely worsens the prognosis of patients receiving dialysis, prognosis of patients receiving dialysis, decreasing the probability of survival by as decreasing the probability of survival by as much as 50% .much as 50% .
For that more care is needed in a patient For that more care is needed in a patient with CRSwith CRS
Questions ?Questions ?
Thank YouThank You