
CARDIAC SIGNAL PROCESSING FOR CLASSIFICATION OF ...
201
1 CARDIAC SIGNAL PROCESSING FOR CLASSIFICATION OF SUPRAVENTRICULAR TACHYCARDIA USING INTRACARDIAC SIGNALS By NAUMAN RAZZAQ A DISSERTATION Submitted to National University of Sciences and Technology in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY Supervised by DR SYED MUHAMMAD TAHIR ZAIDI College of Electrical and Mechanical Engineering National University of Sciences and Technology, Pakistan 2017
Transcript of CARDIAC SIGNAL PROCESSING FOR CLASSIFICATION OF ...

1
CARDIAC SIGNAL PROCESSING FOR CLASSIFICATION OF
SUPRAVENTRICULAR TACHYCARDIA USING INTRACARDIAC SIGNALS
By
NAUMAN RAZZAQ
A DISSERTATION
Submitted to
National University of Sciences and Technology
in partial fulfillment of the requirements for the degree of
DOCTOR OF PHILOSOPHY
Supervised by
DR SYED MUHAMMAD TAHIR ZAIDI
College of Electrical and Mechanical Engineering
National University of Sciences and Technology, Pakistan
2017

2
In the name of Allah, the most Merciful and the most Beneficent

3
ABSTRACT
CARDIAC SIGNAL PROCESSING FOR CLASSIFICATION OF
SUPRAVENTRICULAR TACHYCARDIA USING INTRACARDIAC SIGNALS
By
NAUMAN RAZZAQ
Electrophysiology study (EPS), a minimal invasive procedure, is performed in Cath
lab for investigation and therapeutic treatment of abnormality in cardiac rhythm using
Intracardiac Electrogram (IEGM) and Electrocardiogram (ECG) signals. IEGM signals
are acquired via catheters placed inside heart, and ECG signals are collected using
surface catheters. The complex patterns of IEGM signals are studied with different
protocols for identification of cardiac abnormalities. Study is carried out visually by
Electro physiologists using the monitor screens to determine key features and their
intervals, which is time consuming and highly dependent on individual expertise.
In this work, IEGM signals have been used to design an automated Supraventricular
Tachycardia (SVT) differentiation system during EPS. The system will assist the
electrophysiologist by reducing the manual working and time involved in diagnosis of
SVT arrhythmia. The research has been conducted in three phases. In Phase I,
preprocessing of the IEGMs have been undertaken for removal of power line interference
and electromyographic noises. In Phase II, classification of Atrioventricular Node
4
Reentrant Tachycardia and Atrioventricular Reentrant Tachycardia have been carried out
in time domain. In Phase III, non-parametric spectral estimation of IEGM signals have
been used for differentiation between Normal Sinus Rhythm, Atrial Tachycardia, Atrial
Flutter and Atrial Fibrillation.

5
To
Islamic Republic of Pakistan

6
ACKNOWLEDGEMENTS
I praise Almighty Allah Subhanahu wa Ta’ala for all his mercy and grace, the strength
that he gave me strength to accomplish this research and complete my PhD.
I would like to express my sincerest gratefulness for the guidance and support of all
my teachers whose intense efforts have made possible the efficacious completion of this
work. The knowledge that I obtained from them proved advantageous throughout the
path of my studies. I would like to express gratitude to my supervisor, Dr Syed
Muhammad Tahir Zaidi, both for accommodating me as his PhD student and for
imparting beneficial guidance, counseling and support over the years leading towards the
completion of this thesis. I would like to express my sincere gratitude to my GEC
members Dr Qaiser Chaudhry, Dr Hamid Mehmood Kamboh, Dr Imran Akhtar for their
precious time and guidance that I have received from them. I would address special
thanks to Dr Muhammad Salman who as a senior always selflessly helped and supported
me in my research work. I would like to convey my earnest appreciation to Col Nasir
Rasheed, Dr Umer Shabaz, Dr. Nauman Anwar, Dr Muhammad Khurram and Dr Atif
Ali, for their valuable time, consideration and encouragement. I gratefully acknowledge
the assistance I received from Lt Col Shafaat al Sheikh, Lt Col Rahat Ali, Dr Khalid
Munawar, Maj Dr Nauman and all colleagues with me in EME College.
I am obligated to my wife and children who have been very compliant / supportive and
have shown remarkable patience all the way along. I am also obliged to my family elders

7
and my sister who have been sources of encouragement for me and their prayers have
complemented me throughout my life.
I would also like to thankfully acknowledge National University of
Sciences and Technology (NUST) for the financial assistance they provided for my
studies and research.

8
TABLE OF CONTENTS
Abstract .................................................................................................................. 3
Acknowledgements ............................................................................................................. 6
Table of contents ................................................................................................................. 8
List of figures ................................................................................................................ 11
CHAPTER 1 INTRODUCTION
1.1 Choosing the Research in Intracardiac Signals ...................................................20
1.2 Problem Statement ........................................................................................22
1.3 Research Approach ........................................................................................22
1.4 Thesis layout ........................................................................................23
CHAPTER 2 CARDIAC ELECTROPHYSIOLOGY
2.1 Anatomy of Heart ........................................................................................27
2.2 Cardiac Conduction System ................................................................................28
2.3 Normal Sinus Rhythm ........................................................................................37
2.4 Arrhythmia ........................................................................................38
2.5 The Origins of Arrhythmia .................................................................................40
2.6 Supraventricular Tachycardia .............................................................................46
CHAPTER 3 ACQUISITION OF CARDIAC ELECTRIC SIGNALS
3.1 Electrocardiogram ........................................................................................53
3.2 The Intracardiac Electrogram .............................................................................62
3.3 Cardiac Catheterization for EP Study .................................................................64

9
CHAPTER 4 PRE-PROCESSING OF INTRACARDIAC SIGNALS
4.1 Scope of Pre-Processing .....................................................................................73
4.2 Power Line Interference ......................................................................................76
4.3 Base Line Wander ......................................................................................114
4.4 Electromyographic Noise ..................................................................................115
CHAPTER 5 TEMPORAL FEATURES OF INTRACARDIAC SIGNALS
5.1 Literature Review ......................................................................................122
5.2 Data Collection ......................................................................................123
5.3 Methodology ......................................................................................125
5.4 Feature Detection ......................................................................................135
5.5 Results ......................................................................................143
5.6 Summary ......................................................................................143
CHAPTER 6 IDENTIFICATION OF REENTRANT TACHYCARDIA
6.1 Literature Review ......................................................................................144
6.2 Dataset ......................................................................................145
6.3 Methodology ......................................................................................146
6.4 Identification of AVNRT ..................................................................................150
6.5 Identification of AVRT .....................................................................................154
6.6 Classification Algorithm between AVRT and AVNRT ...................................156
6.7 Summary ......................................................................................159
CHAPTER 7 FREQUENCY ANALYSIS FOR IDENTIFICATION OF AT
7.1 Literature Review ......................................................................................161
7.2 Dataset ......................................................................................163
10
7.3 Methodology ......................................................................................165
7.4 IEGM Pre- Processing ......................................................................................167
7.5 PSD Estimation ......................................................................................167
7.6 Extraction of Spectral Parameters from PSD....................................................169
7.7 Algorithm for Discrimination of Atrial Arrhythmias .......................................175
7.8 Results and Discussion .....................................................................................176
7.9 Accuracy Analysis .....................................................................................182
7.10 Summary ......................................................................................184
Conclusion and future Work
Conclusion ......................................................................................185
Future Recommendations ......................................................................................186
Acknowledgement ......................................................................................188

11
LIST OF FIGURES
Figure 1-1 Research approach and outcomes .......................................................... 24
Figure 2-1 The valves and chambers inside heart ................................................... 28
Figure 2-2 Cells of Electric Conduction System of Heart ....................................... 29
Figure 2-3 Phases of a cardiac AP. ......................................................................... 31
Figure 2-4 Phases of a AP of cardiac pacemaker cells. .......................................... 32
Figure 2-5 The AP patterns of various cardiac cells ............................................... 33
Figure 2-6 Depolarization –polarization cycle of Pacemaker Cell ......................... 33
Figure 2-7 Intrinsic Conduction system of the heart ............................................... 34
Figure 2-8 The sequence of electric excitation ........................................................ 36
Figure 2-9 Extrinsic conduction system controlled by ANS ................................... 38
Figure 2-10 Ventricular ectopic foci.......................................................................... 41
Figure 2-11 Right sided, septal and left sided APs ................................................... 42
Figure 2-12 Local and global reentry ........................................................................ 43
Figure 2-13 Normal versus reentry mechanism......................................................... 43
Figure 2-14 (a) AVNRT case, (b) AVRT case .......................................................... 45
Figure 2-15 Normal cardiac cycle versus pre-excited cycle ...................................... 46
Figure 2-16 Normal atrial activation versus Atrial Fibrillation ................................. 48
Figure 2-17 Normal cardiac conduction and AVNRT case....................................... 50
Figure 2-18 Orthodromic AVRT .............................................................................. 51
Figure 3-1 Accumulative effect of AP of various cardiac conduction cells ............ 54
Figure 3-2 Complete rhythm of depolarization/repolarization ................................ 55

12
Figure 3-3 The waveform/segment description of an ECG signal .......................... 56
Figure 3-4 Scheme of 10 electrodes placement (12 leads ECG) ............................. 57
Figure 3-5 The combination of limb leads .............................................................. 58
Figure 3-6 The combination of augmented limb leads ............................................ 59
Figure 3-7 The view angles in vertical plane .......................................................... 59
Figure 3-8 The view angles by six precordial leads in horizontal plane ................. 61
Figure 3-9 The complete three dimensional view by 12 leads ECG ....................... 61
Figure 3-10 Catheter placement procedure................................................................ 63
Figure 3-11 EP catheter electrode.............................................................................. 64
Figure 3-12 Bi-polar catheter configuration .............................................................. 65
Figure 3-13 Basic configuration of HRA, His, RVA and CS catheters .................... 66
Figure 3-14 Correlation between IEGM and ECG features ...................................... 67
Figure 3-15 Layout of EP study layout containing ECG and IEGM leads ............... 68
Figure 3-16 Propagation of ‘A’ wave sequentially from RA to CS leads ................. 69
Figure 3-17 Appearance of ‘A’-wave and ‘V’-wave ................................................. 70
Figure 3-18 Antegrade Versus Retrograde Pacing .................................................... 71
Figure 4-1 Stages of Arrhythmia Classification Algorithm ..................................... 73
Figure 4-2 Effect of inappropriate frequency band selection. ................................. 75
Figure 4-3 Effects of a notch filter for removal of PLI........................................... 75
Figure 4-4 IEGM data sampled at 2 kHz ................................................................. 80
Figure 4-5 Frequency spectrum of Raw IEGM signal............................................. 81
Figure 4-6 Proposed layout for elimination of PLI and its harmonics .................... 84
Figure 4-7 Intelligent DFT - Flow chart. ................................................................. 87

13
Figure 4-8 Working of intelligent DFT. .................................................................. 88
Figure 4-9 (a) Non-overlapping window (b) Half window overlapping ................. 91
Figure 4-10 Sliding window DFT and delay caused. ................................................ 92
Figure 4-11 Working of SSRLS. ............................................................................... 95
Figure 4-12. IEGM Test signal with sampling rate of 2000 samples/sec. ................. 96
Figure 4-13 Frequency spectrum of IEGM Test signal ............................................ 97
Figure 4-14 The composite test signal ....................................................................... 98
Figure 4-15 PLI corrupted IEGM signal ................................................................... 99
Figure 4-16 Frequency spectrum of PLI corrupted IEGM signal.............................. 99
Figure 4-17 PLI frequency estimation in stages ...................................................... 100
Figure 4-18 Frequency estimation through proposed scheme.. ............................... 101
Figure 4-19 Tracking of SSRLS adaptive filter during initialization period .......... 103
Figure 4-20 Filtered IEGM signal after initialization .............................................. 103
Figure 4-21 Frequency spectrum of tracked/filtered signals.. ................................. 104
Figure 4-22 Raw IEGM signal corrupted with PLI. ................................................ 105
Figure 4-23 Frequency spectrum of raw IEGM signal. ........................................... 105
Figure 4-24 Frequency spectrum of filtered IEGM. ................................................ 106
Figure 4-25 Filtration quality of SSRLS adaptive filter and notch filter. ............... 108
Figure 4-26 The filtered output with step change in PLI......................................... 109
Figure 4-27 The filtered outputs with ramp change in PLI. .................................... 110
Figure 4-28 Comparison of proposed system and notch filter with ramp change. .. 111
Figure 4-29 Frequency estimation by intelligent DFT ............................................ 112
Figure 4-30 Comparison of proposed system & notch filter with frequency shift. . 113

14
Figure 4-31 Filtered IEGM signal from proposed method. ..................................... 117
Figure 4-32 Preservation of ‘H’ feature with SG filter............................................ 118
Figure 4-33 EMG removal from IEGM through MA filter ..................................... 119
Figure 4-34 EMG removal from IEGM through IIR Filter ..................................... 120
Figure 4-35 EMG removal from IEGM through Median Filter .............................. 121
Figure 5-1 AFIC dataset containing 3xECGs and 9xIEGMs ................................ 124
Figure 5-2 MIT dataset containing 3xECGs and 5xIEGMs .................................. 125
Figure 5-3 Catheters arrangement for SVT arrhythmia detection ......................... 126
Figure 5-4 Proposed system for feature detection ................................................. 127
Figure 5-5 Straight Pacing. .................................................................................... 128
Figure 5-6 Extra Stimuli Pacing. ........................................................................... 129
Figure 5-7 Algorithm for detection of PES protocol ............................................. 131
Figure 5-8 HisP with pacing artifact ...................................................................... 132
Figure 5-9 HisP with pacing artifact removed. ...................................................... 133
Figure 5-10 IEGM of His catheter without envelop ................................................ 134
Figure 5-11 IEGM of His catheter after applying envelop detect ........................... 134
Figure 5-12 IEGM signals of His distal and proximal ............................................ 135
Figure 5-13 Onset of VRVA ...................................................................................... 136
Figure 5-14 Onset of AHRA ...................................................................................... 137
Figure 5-15 Earmarking of VHis-on and VHis-off ......................................................... 139
Figure 5-16 Marking of HHis-on on His IEGM......................................................... 140
Figure 5-17 Feature detection algorithm ................................................................. 142
Figure 6-1 Proposed methodology for detection of AVNRT/AVRT .................... 146

15
Figure 6-2 Extra stimulus pacing at HRA. ............................................................ 147
Figure 6-3 Correlation of electric activity in different electrodes. ......................... 149
Figure 6-4 Interval measurements. ........................................................................ 150
Figure 6-5 Slow-fast AVNRT and observation during EP study. ......................... 151
Figure 6-6 Presence of AH jump with extra stimulus pacing protocol. ................ 152
Figure 6-7 AH jump............................................................................................... 153
Figure 6-8 AH Interval and AH Jump measurement ............................................. 154
Figure 6-9 (a) Orthodromic AVRT (b) Antidromic AVRT................................... 155
Figure 6-10 Reentrant arrhythmia detection algorithm ........................................... 156
Figure 7-1 Pre-processing steps HRA-IEGM ........................................................ 166
Figure 7-2 Signal segment and Sub Segment for Estimation of PSD. .................. 168
Figure 7-3 Calculation of RI for reliability of DF ................................................. 170
Figure 7-4 PSD comparison of regular and irregular arrhythmias ....................... 171
Figure 7-5 The Description of APSR. ................................................................... 173
Figure 7-6 Differentiation Algorithm based on DF and APSR. ............................ 175
Figure 7-7 NSR case: DF is at 1.46 Hz and APSR value is 0.903. ....................... 177
Figure 7-8 AT Case: DF is at 2.68 Hz and APSR value is 0.993. ........................ 178
Figure 7-9 AT Differentiation from AF (3~4 Hz). ................................................ 178
Figure 7-10 AFL Differentiation from AF (4~5 Hz). .............................................. 179
Figure 7-11 AF Differentiation from AT (3~4 Hz). ................................................ 180
Figure 7-12 AF Differentiation from AFL (4~5 Hz). .............................................. 180
Figure 7-13 AF Detection (5~12 Hz) ...................................................................... 181

16
LIST OF TABLES
Table 4-1. Filtration requirement for ECG/IEGM signals ............................................ 74
Table 4-2 FFT, DFT and intelligent DFT comparison ................................................. 89
Table 5-1 Result of Feature Detection Algorithm .................................................... 143
Table 6-1 Result of Arrhythmia Detection ............................................................... 157
Table 6-2 Sensitivity, Specificity, PPV and NPV Results ....................................... 158
Table 7-1 ECG and IEGM Data – AFIC/NIHD ....................................................... 163
Table 7-2 ECG and IEGM Data – MIT Physiobank ................................................ 164
Table 7-3 IEGM Dataset (Verified Rhythms) .......................................................... 165
Table 7-4 RI and APSR comparison ........................................................................ 175
Table 7-5 Rhythm detection results by proposed method ....................................... 182
Table 7-6 Sensitivity, Specificity, PPV and NPV Results ....................................... 183

17
LIST OF ABBREVIATIONS
AP Action Potential
APs Accessory Pathways
AVNRT Atrioventricular Node Reentrant Tachycardia
AVRT Atrioventricular Reentrant Tachycardia
AT Atrial Tachycardia
AFL Atrial Flutter
AF Atrial Fibrillation
AV Atrio Ventricular
A wave Atrial Wave
ANS Autonomic Nervous System
APSR Average Power Spectral Ratio
AFIC Armed Forces Institute of Cardiology
ANC Adaptive noise cancellation
BLW Base Line Wander
bpm beats per minute
CS Coronary Sinus catheter
DF Dominant frequency
Dst Distal
DFT Discrete Fourier Transform
EPS Electrophysiology study
ECG Electrocardiography

18
EMG Electromyographic
FIR Finite Impulse Response
HRA High Right Atrium Catheter
His His bundle catheter
H wave His Bundle wave
IEGM Intracardiac Signals
ICD Implantable Cardioverter Defibrillator
IIR Infinite Impulse Response
ISSAD Intracardiac Signal Analysis And Display
LA Left Atrium
LV Left Ventricle
LBB Left Bundle Branch
LMS Least Mean Square
NIHD National Institute of Heart Diseases
NSR Normal Sinus Rhythm
PLI Power Line Interference
Prx Proximal
PES Programmed Electrical Stimulation
PSD Power Spectral Density
RI Regularity Index
RA Right Atrium
RV Right Ventricle
RVA Right Ventricular Apex Catheter

19
RLS Recursive Least Square
RBB Right Bundle Branch
SVT Supraventricular Tachycardia
SA Sinoatrial
SG Savitzky–Golay
SVC Superior Vena Cava
SSRLS State Space Recursive Least Square
V wave Ventricular wave
VT Ventricular Tachycardia
WHO World Health Organization

20
CHAPTER 1
INTRODUCTION
1.1 Choosing the Research in Intracardiac Signals
As per survey report held by World Health Organization (WHO), major cause of human
deaths are because of heart diseases [1, 2]. In 2013, deaths because of cardiac issues,
represented 31% of global deaths affecting about 17.3 million people [2]. Keeping in
view this trend, it is expected that the cardiac related deaths may touch the figure of 23.6
million in 2030 [3, 4]. Cardiac problem can be related to cardiovascular or arrhythmia
(abnormality in rhythm). If we take into account the arrhythmia’s statistics, approx 1 in
18 (or 5.30%) are affected from arrhythmia related disorders. In US, more than 850,000
people are hospitalized for a problem related to arrhythmia each year and 100,000
American have an implantable Defibrillator (ICD) [5].
Electrocardiogram (ECG) is the recording of cardiac signals from surface of patient’s
body and commonly used to gauge heart’s rhythm related problem however, sometimes
ECG does not fulfill the purpose. As an alternate, the invasive method is adopted known
as Electrophysiology (EP) study (named as EPS), in which heart‘s electric signals are
procured directly by inserting catheter electrodes inside the heart. The signals recorded
through EPS are known as Intracardiac Electrograms (IEGM). EPS has made a noticeable
evolution in the last three decades and has emerged as a major specialty in cardiology.
EPS is comparatively complicated field and it requires in depth understanding of several

21
diagnostic procedures and pacing protocols of IEGMs. That is why a very few
cardiologists opt to specialize in this field.
I am an electrical engineer and I did several specialization courses related to biomedical
field during my services in armed forces. When I joined for PhD, I was serving in Armed
Forces Institute of Cardiology (AFIC) as Biomed Engineer and being directly involved
with the Cardiac related equipment, I developed my interest to undertake research in this
field.
In Pakistan, the EPS setups are very few. One of major issue related to EPS is the non-
standardization of EPS protocols across the world and the heart is stimulated externally at
different loci under various protocols to study its behavior.
At present, the EP study is based on manual measurements on screen by the
electrophysiologist, that is a time consuming procedure because of manual marking of
features and their interval measurement and the procedure may prolong to many hours in
some cases.. It is highly desired that automated arrhythmia detection based on IEGMs be
developed, which will facilitate the electrophysiologist.
EPS is highly demanding field and has lot of potential for research in this area. Because
of technical in nature, EP study demands the involvement of an engineer in this field who
can investigate the IEGM signals and new methods can be explored with application of
different analysis tools. Lot of work can be found in literature for automated arrhythmia
detection based on ECG, however very few or no published material is available in the
field of automated arrhythmia classification based on IEGMs. Moreover, it has been
observed that the EP study is mostly based on time domain analysis by defining temporal

22
relationship between different features of IEGMs manually. The application of frequency
domain analysis for differentiation among different arrhythmias has vast room of
exploration in EP study.
1.2 Problem Statement
SVT encompasses all arrhythmias which are above ventricular, this includes arrhythmias
related to atrium, SA node and atrioventricular (AV) node [6]. SVT is a commonly found
arrhythmia, which affects over 570,000 people each year [7]. The SVT prevalence in the
general population is 0.229% of total human population [7, 8]. The vast majority of SVTs
are one of three types; atrioventricular nodal re-entrant tachycardia (AVNRT) which is
responsible for approximately 65% of cases, atrioventricular reentrant tachycardia
(AVRT) which is responsible for approximately 30% of cases, and atrial tachycardia
(AT) responsible for approximately 5% of cases [9-11].
In this research work, I choose SVT arrhythmias for differentiation of its various types by
analyzing IEGM signals. This research work intends to develop an automated arrhythmia
differentiator based on time and frequency domain analysis, to be applied on IEGMs
acquired during clinical EPS, designed specifically to focus on Supraventricular
Tachycardia (SVT).
1.3 Research Approach
The overall research aimed to develop a project named as “Intracardiac Signal Analysis
And Display” (ISSAD) which acquire, pre-process and classify among various
arrhythmias of SVT in first phase and to classify ventricular tachycardia (VT) as future

23
target (in next phase). For this purpose a research group headed by me as PhD Scholar
and 4~5 Master students, was formulated to cover the scope of this research. The
research approach and outcomes from this research are shown in Figure 1-1. Since this
field is quite complex, therefore the involvement of electrophysiologist and acquiring
sufficient medical related knowledge was the base line to move fwd. ECG databank of
various arrhythmias can be found at MIT Physiobank, however databank of IEGM
signals is rarely found.
The acquisition of SVT arrhythmia relevant IEGM dataset was a difficult task because
the complete range of gold standard dataset was not available on Physionet or any other
authentic resource. Therefore, the majority of required Patient’s dataset was collected
from AFIC/NIHD Pakistan and few from MIT Physionet database as available [12]..
These dataset was verified from expert electrophysiologist for the specific type of
arrhythmias and then it was referred as gold standard for research work.
Overall, research was focused on SVT and it conducted undertaken sequentially in three
main fields, 1) Pre-processing of IEGMs, 2) The classification of reentrant tachycardia in
time domain & 3) The classification of atrial tachycardias in frequency domain. As the
outcome of this research, the project ISAAD was successfully developed.
1.4 Thesis layout
The overall thesis can be grouped into two parts. Part I consist of chapters 1, 2 and 3
which generally cover the motivation, database acquisition and background knowledge
related to this topic. Part II consist of chapters 4, 5, 6 and 7 which present the proposed
methods, worked out of this research work. Since this thesis dissertation covers the
diverse fields including pre-processing and classification of IEGMs in time domain and

24
frequency domains, the related literature review have not been grouped together rather it
has been covered prior to related field.
Figure 1-1 Research approach and outcomes
The background knowledge and research work undertaken has been grouped into seven
chapters. The first chapter elaborates the brief background of the selected topic along
with motivation for its selection. The research problem has been formulated and its
objectives are defined in this chapter. The resource database has also been declared.

25
In second chapter, the anatomy of heart and role of electric conduction system in cardiac
functioning has been described. Different components of electric circuit and their
function/response are discussed with the aim to understand abnormalities associated with
conduction system. The normal and abnormal (arrhythmia) rhythms of heart are
explained. The mechanism, causes and types of different arrhythmias are defined. At the
end of this chapter, the different types of SVT have been elaborated in detail.
Third chapter describes the basic techniques developed for monitoring and recording of
cardiac electric activities. The concept, methodology, the outcomes of cardiac electric
signals recordings from body surface in form of ECG and its features have been briefly
explained. Thereafter the purpose and methodology of EP study in which electric signals
are recorded directly from catheters placed inside heart’s chambers have been introduced.
Different types of IEGM signals and its features have also been elaborated.
The fourth chapter deals with pre-processing of IEGMs for removal of Power Line
Interference (PLI) and Electromyographic Noise (EMG). In order to avoid loss of useful
information in IEGM signals and accurate extraction of ECG/IEGM features, the
adaptive filter design have been proposed in this chapter.
The fifth chapter deals with temporal feature detection of IEGM signals. Here, an
algorithm for accurate detection of IEGM’s feature and their validation has been
proposed. The pacing protocols and their automated identification has also been
presented in this chapter.
In sixth chapter, two major types of reentrant tachycardia that include AVRT and
AVNRT, are differentiated using IEGM signals in time domain. For analyzing reentrant
tachycardia, extra stimulus pacing of heart is done under a specific protocol and heart is

26
enforced to enter in tachycardia state. The foremost requirement is the IEGM feature
extraction and then determines the time gaps between different features.
In seventh chapter, the frequency domain analysis has been devised for differentiation of
atrial IEGMs. Non parametric estimation technique using Welch method is applied to
find Dominant frequency (DF) which represents atrial activation rate during various atrial
tachycardia. A new spectral parameter, Average Power Spectral Ratio (APSR), has been
identified for ensuring reliability of DF (for AF detection) as well as to differentiate AF
from other atrial arrhythmias.
Finally, the conclusions arising from this research work has been presented and the future
research work has been proposed to further improve this work and devise new algorithms
for detection of other arrhythmias.

27
CHAPTER 2
CARDIAC ELECTROPHYSIOLOGY
In this chapter, the anatomy of heart and role of electric conduction system in cardiac
functioning has been introduced briefly. Different components of electric circuit and
their function/response have also been discussed with the aim to understand
abnormalities associated with conduction system. The importance of electric pulses,
their sequence and timing relationship with cardiac output have also been
elaborated. With all these, the intrinsic and extrinsic conduction system of the heart
have been described.
2.1 Anatomy of Heart
The heart is a muscular organ, function as blood pump which circulate blood throughout
body. It can be considered as combination of two parallel circulatory pumps (right and
left pumps); right sided pump collects deoxygenated blood from the complete body
through veins and deliver it to lungs, the left sided pump collects oxygenated blood from
lungs and deliver it to whole body. Each pump (side) has further divided in two portions
i.e. the upper chamber (known as ‘Atria’) and the lower chamber (known as
‘Ventricle’)[13]. The atria can be considered as pre-pump and ventricle can be considered
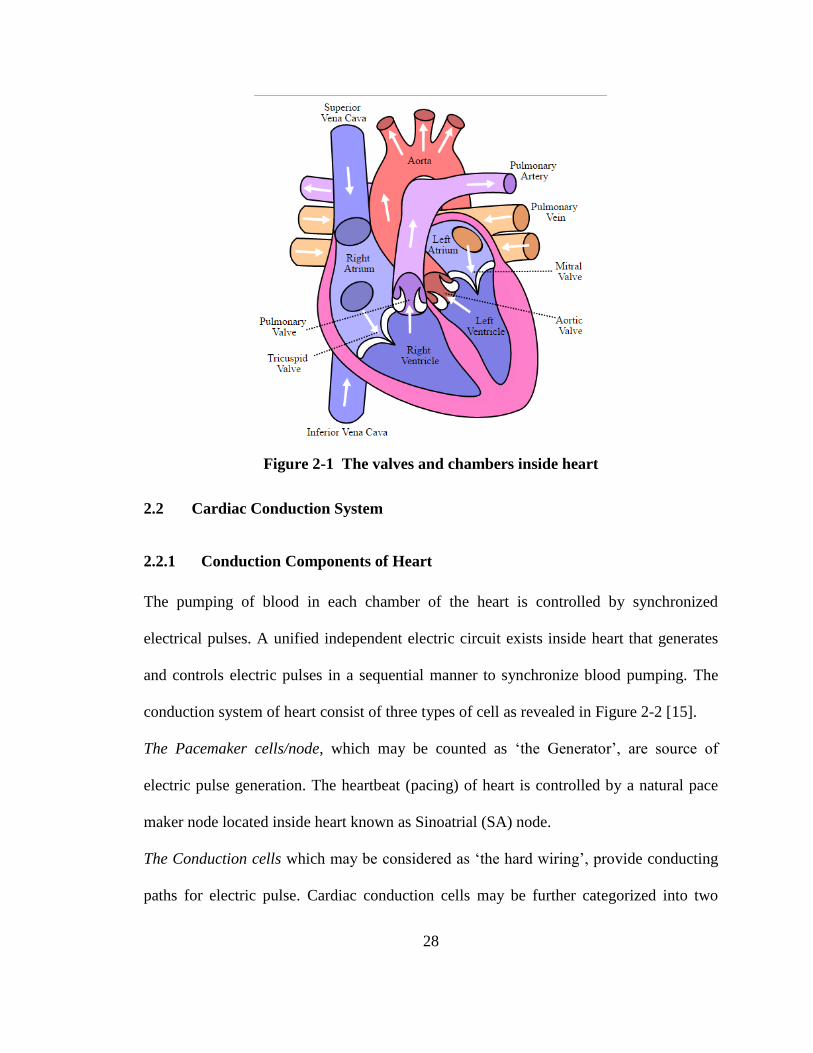
as main pump. Therefore, there are total four chambers inside heart named as Right
Atrium (RA), Right Ventricle (RV), Left Atrium (RA) and Left Ventricle (RV) as shown
in Figure 2-1. Each chamber has a one way valve at its output named as Tricuspid,
Pulmonary, Mitral and Aortic valves [14].
28
Figure 2-1 The valves and chambers inside heart
2.2 Cardiac Conduction System
2.2.1 Conduction Components of Heart
The pumping of blood in each chamber of the heart is controlled by synchronized
electrical pulses. A unified independent electric circuit exists inside heart that generates
and controls electric pulses in a sequential manner to synchronize blood pumping. The
conduction system of heart consist of three types of cell as revealed in Figure 2-2 [15].
The Pacemaker cells/node, which may be counted as ‘the Generator’, are source of
electric pulse generation. The heartbeat (pacing) of heart is controlled by a natural pace
maker node located inside heart known as Sinoatrial (SA) node.
The Conduction cells which may be considered as ‘the hard wiring’, provide conducting
paths for electric pulse. Cardiac conduction cells may be further categorized into two

29
basic parts as atrial and ventricle conducting cells depending upon their function as
shown in [16].
The Myocardial cells act as actuators, are muscle cells of heart which contract on
receiving electric pulses thus cause the blood pumping action.
Figure 2-2 Cells of Electric Conduction System of Heart [15]
2.2.2 Cardiac Electricity (Action Potential)
First, it is important to understand, how electricity is generated and flow inside heart. The
flow of electric pulse in heart is because of action potential (AP) generated in heart’s
conduction cells. The AP is biological electricity and is not like a normal electric current
that is because of flow of electrons. The AP can be defined as the rapid sequence of
changes in polarity of the excitable cell due to movement of sodium and potassium ions
across the cell membrane when triggered by an electric pulse [17]. In pacemaker cells,

30
this cyclic sequence is automatically self repeated and a pulse is generated after a specific
interval, which defines the heart rate. The AP sequence consists of different
distinguishing stages.
In normal or resting stage, the cardiac cells are polarized in a way that they are more
negatively charged from inside in relation to their outside surface. This polarization is
because of difference in concentration of mainly potassium, sodium, chloride and
calcium ions, however these ions can cross the membrane through channels in it. The
resting AP of cardiac cells is around -80 ~ -90 mV.
Because of some external (or automatic) electric stimulation, the negative ions from the
cardiac cell will flow out and will change polarization of cardiac cell. This process is
known as depolarization. A depolarized cardiac cell can stimulate its neighboring cell to
depolarize and when a row of cell are depolarized sequentially, it cause flow of electric
charge. When cardiac cell is depolarized, it’s potential reaches +10 ~ +30 mV.
Once depolarization is reached, the peak AP (around 30mv) and thereafter the cardiac
cell starts restoring to its rest (normal) state. This process is known as Repolarization.
Plateau is unique for contractile cardiac cell, in which AP is sustained around 0-10 mV
for considerable time duration before start of repolarization.
In some cases, on the termination of repolarization stage, the AP of the cell overshoots
the resting state becoming more negative than the normal polarity. This stage is known as
hyper polarization.

31
2.2.3 The AP Patterns
Contractile cardiac cells are Sodium dependant channel. Sodium channels are voltage
gated channels and are characterized with a Plateau just after repolarization has
started[18]. Plateau of ventricle AP has a longer duration as compared to atrial AP. A
complete cycle of change in AP of contractile cardiac cell is shown in Figure 2-3.
Figure 2-3 Phases of a cardiac AP. "0" (sharp rise in voltage) corresponds to
depolarization, “1” correspond to early repolarization, “2” is plateau, “3”
corresponds to repolarization and “4” is quite (resting) stage
Pacemaker cardiac cells are Calcium channel dependant and have ability to generate
impulsive AP without external trigger thus initiate a rhythmic depolarization/
repolarization cycle automatically[19]. A complete cycle of change in AP of pacemaker
cardiac cell is shown in Figure 2-4 which resembles to a sinusoidal wave.
The AP patterns of various cardiac cells are shown in Figure 2-5. Variations in these
pattern are because of difference in the properties of the cardiac cells and slope/duration
of different phases of these patterns define responses of each type of cardiac cell.

32
Figure 2-4 Phases of a AP of cardiac pacemaker cells. Phase "0" corresponds to
slow diastolic depolarization, Phases “1” and “2” corresponds to termination of
depolarization cycle and plateau, Phase “3” corresponds to slow repolarization and
Phase“4” is termination of depolarization (quite stage)
2.2.4 Refractory Period
The transient period when the cardiac cell is entering from depolarization stage to
repolarization stage, the cardiac cell is in refractory i.e. it cannot respond to new
stimulation and this period is known as Refractory Period. The initial portion of
refractory period is absolute refractory and former portion is relative refractory i.e. a
stronger stimulus if applied can reinitiate the depolarization. In contractile cardiac cell,
phase 1 and 2 are absolute refractory, whereas phase 3 is partial refractory and a strong
signal can initiate depolarization process. A complete cycle of change in AP of
contractile cardiac cell is shown in Figure 2-6.

33
Figure 2-5 The AP patterns of various cardiac cells [15]
Figure 2-6 Depolarization –polarization cycle of Pacemaker Cell

34
2.2.5 Intrinsic Conduction System
The overall conduction system of heart can be grouped into two main categories i.e.
intrinsic and extrinsic conduction system. The intrinsic conduction system of the
heart is an autonomous system which is a combination of different bioelectric
components (cardiac cells) including the Pacemaker node (The Generator), the
conduction cells (the hard wire) and myocardial cells (The actuators). The complete
picture of intrinsic conduction system is shown in
Figure 2-7. Following are major components of intrinsic conduction system.
Figure 2-7 Intrinsic Conduction system of the heart

35
The SA Node. The SA is located in upper right atrium at the verge of
SuperiorVenaCava (SVC) and it plays role of primary pacemaker of the heart. It
initiate the electric stimulus in a rhythm which determines the heart rate (60 beats
per minute under normal conditions).
Inter-nodal and Inter-atrial Pathways. Inter-nodal pathways are links between
SA node and AV node. These pathways spread out through right atrium and cause
the contraction of right atrium. Through these pathways, the electric pulse reaches
the AV node. Inter-atrial pathway is link between SA node and left atrium. This
pathway extends from right atrium to left atrium and carry the electric pulse to left
atrium for its contraction.
AV Node. The AV node is a specialized bundle of tissues that is located between
atrium and ventricular boundary. In a healthy heart, this is the only passage of
stimulus from atrium (upper portion) to ventricle (lower portion). Main role of
AV node is to delay the passage of electric pulse from atrium to ventricle so that
contraction of atrium may be completed before start of ventricle depolarization. It
also plays role of a secondary pacemaker that can initiate a small size electric
pulse (at the rate lower than the initiated by SA node), if pulse from SA node is
blocked.
Bundle of His. Bundle of His is a combination of conduction cells which carries
electric pulse from AV node to the apex of ventricular. It is further divided into

36
two branches for two sides of ventricles; one is right bundle branch (RBB) and
other is left bundle branch (LBB).
Purkinje Fibers. The right/left bundles branches are divided into many thin
pathways known as Purkinje Fibers. These fibers connect electric pulse to the
ventricle muscles and cause depolarization for contraction.
Figure 2-8 The sequence of electric excitation
The stimulus is initiated from SA node, distributed to right/left atrium and causes both
atria to depolarize (contract). After depolarization of both atria, the pulse reaches the AV
node and a conduction delay is enforced in AV node. After a specific delay caused in AV
node, the electric pulse enters the bundle of His and divided into two branches
RBB/LBB. Finally, the electric pulse reaches the Purkinje fibers and depolarizes both the
ventricles. The sequence of electrical excitation of heart is shown in Figure 2-8.

37
2.2.6 Extrinsic Conduction System
The intrinsic conduction system is self autonomous however autonomic nervous system
(ANS) has capability to modify the heartbeat in various circumstances to vary the blood
pumping rate and strength. The external control of heartrate by ANS is known as
extrinsic conduction system as shown in Figure 2-9. It has two subsystem named as
sympathetic and parasympathetic conduction stimulation which, are regulated by the
medulla oblongata. The extrinsic control is the result of a balance between both the
parasympathetic and the sympathetic stimulation system.
Sympathetic conduction stimulation enhances the heart rate under those circumstances in
which fast blood pumping is required e.g. physical fatigue, emotional stress etc. The
functioning of sympathetic stimulation involves thoracolumbar and sympathetic chain
neurons. It simultaneously influence the SA node, AV node and Purkinje
fibers/myocardium as depicted in Figure 2-9.
Parasympathetic conduction stimulation decreases the heart rate via Vagus nerve. It
controls mainly SA node to relax the action potential.
2.3 Normal Sinus Rhythm
If the intrinsic conduction system of the heart remains normal then AP of cardiac cells
follow a sequential rhythm which is initiated and controlled by primary pacemaker of
heart that is sinus node. Under normal conditions, heart rate remains 60-100 bpms and
further change in heart rate is controlled by extrinsic conduction system (regulated by
ANS) as per demand of the body. This rhythmic rise or decrease in heart beat if follow a
regular rhythm then it is also counted as normal. A rhythm is defined as Normal Sinus

38
Rhythm (NSR) if rhythm initiated by SA node, remains regular and heart rate is between
60 to 100 bpm [13, 20-23].
Figure 2-9 Extrinsic conduction system controlled by ANS
2.4 Arrhythmia
If heart rate is not 60-100 bpm (under normal condition) or rhythm is not solely
controlled by sinus node causing irregularity in rhythmic sequence, it is counted as
arrhythmia (abnormal rhythm)[16]. Arrhythmia is categorized in further types based on
location, heart rate and rhythm regularity etc.
2.4.1 Arrhythmia Based on Heart Rate
Based on heart rate, the abnormality is of two types as following.
39
Bradycardia. When heart beat goes slow i.e. heart Rate falls down 60 bpm. It is
mainly because of failure of SA or AV nodes to generate of pulse or transmit pulse
properly [24].
Tachycardia. When heart beat goes fast i.e. heart Rate increases above 100 bpm.
Tachycardia, sometime becomes very dangerous and need to be normalized rapidly.
2.4.2 Arrhythmia Based on Regularity
Based on rhythm regularity, the rhythm can be categorized into following two types.
Regular Rhythm. When heart follows normal depolarization of conduction path in a
sequential way, the rhythm is known as regular rhythm e.g. flutter, tachycardia.
Irregular Rhythm. When there is an irregularity in heart beat and heart rate becomes
erratic because of some cardiac tissues other than SA node, are generating the AP
automaticity e.g. fibrillation.
2.4.3 Arrhythmia Based on Location
Based on location, the arrhythmias can be categorized into different groups based on
location e.g. atrium, ventricle or nodes, however most commonly used groups are of two
types as following.
Ventricular Tachycardia. The ventricular tachycardia (VT) is the abnormal fast
rhythm because of improper AP occurring in lower chamber i.e. ventricle. VT is
dangerous and often becomes life threatening, if prolonged.
Supraventricular Tachycardia. The Supraventricular tachycardia (SVT) is the
abnormal fast rhythm because of improper AP occurs other than ventricular which
include upper chamber and AV node.

40
2.4.4 Arrhythmia Based on QRS Duration (ECG)
One of the popular differentiation of tachycardia is on basis of QRS duration i.e. width of
QRS is narrow or wide.
Narrow QRS. For a normal case, the QRS width remains below 120ms and are
differentiated as ‘Narrow QRS’[25].
Wide QRS. The cases in which QRS width is above 120ms are differentiated as
‘Wide QRS’[26].
2.5 The Origins of Arrhythmia
Once our focus is to classify different arrhythmias, then it is necessary to understand
origin/cause of arrhythmia especially when dealing with IEGMs, which are mostly
localized electric signals. The cause/source behind an abnormality in cardiac rhythm can
be categorized in following basic groups as under [16].
2.5.1 The Pacemaker Problem
The primary pacemaker of heart’s intrinsic system is SA node and secondary is AV node.
Both nodes are further regulated by extrinsic conduction system (ANS). Sometime SA
node generates electric pulse that either is too slow/fast or may not be regular; therefore,
sinus node is responsible for initiating an arrhythmia. Following arrhythmias may be due
to SA node issue.
Sinus rhythm
Sinus bradycardia
Sinus tachycardia
Sick sinus syndrome

41
Figure 2-10 Ventricular ectopic foci
2.5.2 Ectopic Beat
If some cardiac tissues other than the sinus node also achieve AP automaticity and start
generating an electrical activity (usually higher than SA node), will override the sinus
rhythm. Such cases are known as ectopic rhythms. Ectopic foci may be in atrium or
ventricle. Ventricular ectopic foci is depicted in Figure 2-10 and it causes prolongation of
QRS duration in ECG.
2.5.3 Accessory Pathway
The accessory pathway (APs) is undesired conduction path between any of two heart’s
chamber, it may be between atrium to atrium, ventricular to ventricular or atrium to
ventricular. AV node is only one conduction point between atria and ventricle, however
some time an APs is generated which creates abnormality in the rhythmic conduction
cycle.

42
Figure 2-11 Right sided, septal and left sided APs (from left to right) [27]
Based on location of APs, these are further categorized as right sided (from RA to RV),
septal (middle, bypasses AV node) and left sided (from LA to LV) as shown in Figure
2-11. Some of APs are capable of conducting only one way, based on the direction of
conduction these may be further defined as Antegrade APs (conduct from atrium to
ventricle) or Retrograde APs (conduct from ventricle to atrium) [27].
2.5.4 Reentry Mechanism
Reentry is the mechanism, which occurs when a propagating APs wave front does not
terminate after a sequential activation in cardiac conduction path and enter in a loop to re-
excite a portion of cardiac cells in the conduction path (once these cells are out of
refractory period). The majority of arrhythmias are because of Reentry mechanism. In a
reentry mechanism, refractory period of cardiac cells and multiple conduction pathways
are two important factors.

43
Figure 2-12 Local and global reentry
Re-entry tachycardia only occurs when, 1) when there exist dual pathways that is linked
with each other at both sides, 2) the conduction of APs through one pathway is faster as
compared to the other, 3) the faster pathway have longer refractory period as compared to
other pathway. The reentry can be distributed into two sub categories as local reentry and
global reentry as shown in Figure 2-12 [28].
(a) (b)
Figure 2-13 Normal versus reentry mechanism.
44
A comparison of normal pathway and local reentry is presented in the Figure 2-13. Here,
two conduction branches are present so electric pulse can travel through both branches
(named as ‘1’ and ‘2’) and both ‘1’ and ‘2’ join together to a third branch marked as ‘3’.
If AP responses of both branches are identical, then electric pulse will reach
simultaneously and there will be no reentry as seen in Figure 2-13(a). Now consider the
other way, if ‘2’ have unidirectional block (electric pulse can enter only one way) then
electric pulse would not enter in ‘2’ however after passing from ‘1’, the electric pulse can
reenter with certain delay in branch ‘2’. This reentry will cause ‘1’ to depolarized again
granted that ‘1’ is not in absolute refractory period as shown in Figure 2-13 (b). Here the
refractory period duration and time delay caused in unidirectional path is important.
AVNRT as shown in Figure 2-14(a) is a typical example of local reentry at AV node.
In AVNRT, an additional local path is formed inside AV node or in proximity of AV
node. The two pathways have different velocity of propagation, one is fast and other is
slow which causes reentry mechanism.
If reentry mechanism is not localized i.e. the reentry occurs between atria and ventricle,
then it is known as global reentry. For a normal case, the cardiac tissues between atrium
and ventricle are non conducting however for case of global reentry, an APs is
established through bundle of Kenth[28]. AVRT is a typical case of global reentry in
which two conduction pathways exists, one is normal conduction path and other is APs.
In typical AVRT, the electrical pulse passes through normal pathway then reenter into
atrium through APs and atrium is depolarized again before initiation of next normal
rhythm, as shown in Figure 2-14(b).

45
(a) (b)
Figure 2-14 (a) AVNRT case through additional local pathway, (b) AVRT case
through accessory pathway [28]
2.5.5 Conduction Blockade
Sometimes undesired delays and hindrance in the flow of AP in intrinsic/extrinsic
conduction system is generated which is referred as blockade in conduction of electric
pulse. The conduction blockade may be partial or complete and can occur anywhere in
the conduction path. Following are main types of conduction block.
SA node block. If SA node is functioning but AP is not able to reach atrial
myocardium and AV node, it is described as sinus block.
AV node block. Any blockade between AV node and right/left bundle branches is
defined as AV block. Different levels of AV blocks are categorized as 1st degree, 2
nd
degree and 3rd
degree Heart Block.
Bundle branch block (BBB). Blockade in any of right or left bundle branches is
referred as left bundle branch block (LBBB) and right bundle branch block (RBBB).

46
2.5.6 Pre-Excitation Syndrome
In pre-excitation syndrome, the electric pulse reaches from atrium to ventricular through
an APs before that the electric pulse reaches through normal conduction path, thus
ventricular gets excited prematurely known as pre-excitation syndrome. Wolff-
Parkinson-White (WPW) and Lown-Ganong-Levine (LGL) syndrome are types of the
pre-excitation syndrome. The comparison between a normal conduction cycle and pre-
excitation case is shown in Figure 2-15; where left sided figure shows a normal cycle and
right side shows pre-excitation syndrome.
Figure 2-15 Normal cardiac cycle on left side versus pre-excited cycle on right side
2.6 Supraventricular Tachycardia
The main focus of this research work is to classify the major arrhythmia related to SVT
therefore, different types of SVT arrhythmia are further elaborated here. SVT
encompasses all arrhythmias which are above ventricular, this includes arrhythmias

47
related to Atrium/SA node and AV node [6]. SVT is a commonly found arrhythmia that
affects over 570,000 people each year. Considering ECG, SVTs are mostly regular and
narrow QRS tachycardia. Majority of the SVTs cases are AVNRT (around 60-70%
cases), AVRT (around 25-30% cases) and AT (5-15% cases) [11]. SVT can be further
grouped into two main categories as under.
2.6.1 Tachycardia from atria
All tachycardia whose source is lying in upper chambers are grouped in this category; it
includes tachycardia related to SA node and both atriums. Following are major
tachycardia rising from atria.
Atrial Tachycardia
In Atrial tachycardia (AT), the rhythm is not fully controlled by SA node rather electric
pulse is initiated within atrium from some other source. The cause may be some ectopic
atrial tissues, which start generating electrical pulses at higher rate than pulse rate
(automaticity) of SA node, thus override the sinus rhythm. In case of AT, the atrial rate
remains between 100-250 bpm [20, 23, 29-31]. In ECG, it is characterized by abnormal
P-wave, regular ventricle rhythm however, ventricular rate may vary from atrial rate [6].
AT may be divided into further categories. For example, focal AT in which, only one
ectopic source of pulses exists whereas in multifocal AT, more ectopic sources exists
which generate pulses. If source of abnormal impulse generation is near or inside AV
which directly conduct to bundle of His without delay however, it is not linked with
reentry mechanism, it is known as junctional ectopic tachycardia [32].

48
Atrial Flutter
In Atrial Flutter (AFL), the tachycardia occurs because of local reentrant circuit
generated inside atria. The local reentry continuously self excites atrial tissues and bring
atria in tachycardia state however, these pulses are not transmitted at the same rate in
ventricle because of refractory period of AV node. Usually pulse reaching ventricles are
in A:V ratio of 2:1 or 3:1. In ECG, it is characterized by saw-toothed F wave, regular
atrial/ventricle rhythm and AV block causing lower ventricular activation rate which may
reach 4:1 [6]. In AFL, the atrial contractions are regular and activation rate remains in
between 230~430 bpm [20, 29, 33-35].
Figure 2-16 Normal atrial activation (regular) versus Atrial Fibrillation (irregular)
Atrial Fibrillations
Atrial Fibrillation (AF) is the type of atrial arrhythmia in which atrial activation rate is
rapid and completely irregular. Difference between a regular rhythm and irregular rhythm
is illustrated in Figure 2-16. Because of irregular atrial rate, the ventricular rate also

49
becomes irregular and sometimes it may become life threatening too. During AF, the
atrial rate can go beyond 600 bpm [36, 37]. In ECG, it is distinguished with the absence
of P-wave, instead of P-wave an vibrating base line is visible, irregular ventricle rhythm
and ventricular activation rate is increased between 100-180 bpm [6].
2.6.2 Tachycardia from AV Node
Mostly arrhythmias related to AV nodes are reentrant tachycardia and two most
commonly observed types are AVNRT and AVRT. Both of these tachycardia have
regular rhythm and narrow QRS complex in majority cases. Description of these
tachycardia is as under.
Atrial-Ventricular Nodal Reentry Tachycardia
AVNRT is because of local reentry and it is one of the most common (60-70% of SVT)
arrhythmia [11]. In a normal conduction system, AV node is the only point of conduction
between atria and ventricle. The significant role of AV node is to impose certain delay in
passing electric pulse from atria to ventricle and only one path should exists, from which
electric pulse passes. In AVNRT case, an abnormality appears in form of two pathways
in AV node as shown in Figure 2-17 and conduction velocity (time delay caused) of both
pathway is not same. One pathway is faster with longer refractory period than the second
pathway, which is slow with smaller refractory period. Out of these two pathways, is
used for normal antegrade conduction whereas the other provides retrograde conduction
and thus a reentry circuit is established. The most (80-90%) common type of AVNRT is
Slow-Fast AVNRT (also known as typical AVNRT) in which slow pathway provides
antegrade conduction and fast pathway provides retrograded conduction as shown in

50
Figure 2-17. In ECG, it is characterized by regular QRS with heart rate increased between
140-250 bpm. In most of cases (typical AVNRT, 90-95%), the P-wave is not visible
because atrial activation occurs almost simultaneously with ventricular activation thus P-
wave hides under the QRS. In some rare cases (atypical AVNRT, 5-10%), P-wave can
also be seen just prior or subsequent of QRS complex [11, 38, 39].
(a) (b)
Figure 2-17 Normal cardiac conduction and AVNRT case
Figure 2-17(a) shows a normal case in which the electric pulse passes early from left side
(fast) pathway and reaches bundle of His early and slow pathway (right) is blocked.
Figure 2-17(b) shows a case of AVNRT in which the left side (fast) pathway is still in
refractory period and blocks the passage of electric pulse; the pulse passes through slow
pathway (right) and reaches bundle of His. The moment the pulse reaches bundle of His,
the refractory period of left side (fast) pathway is over, the pulse reenter through left side
(fast) pathway and reaches RA (known as “echo”) causing atrial tachycardia. In this way,

51
a recurring loop is established which maintains state of tachycardia. The other type of
AVNRT is Fast-Slow AVNRT, which is relatively uncommon (10-20%) [18].
(a) (b)
Figure 2-18 (a) Orthodromic AVRT (retrograde conduction through APs)
(b) Antidromic AVRT (antigrade conduction through APs)
Atrioventricular Reentrant Tachycardia
Another common type of reentrant arrhythmia is AVRT (25-30% of SVT) [23]. The
cause of AVRT is linked with Wolff-Parkinson-White (WPW) Syndrome in which two
separate pathways exist between atria and ventricle; one is the normal pathway through
AV node whereas the other is APs usually generated through bundle of Kenth. The
presence of two pathways provide a reentry mechanism in which electric pulse passes

52
through fastest pathway from atria to ventricle and then reenter from slow pathway back
into atria hence cause tachycardia. Usual heart rate during AVRT remains between 200-
300 bpm. The AVRT can be divided into two main types, orthodromic/antidromic as
shown in Figure 2-18. In Orthodromic AVRT, the conduction occurs antegrade through
AV node and retrograde through APs. In ECG it is characterized by narrow (<120ms)
QRS. It is very common type of AVRT also known as typical AVRT. In Antidromic
AVRT, the conduction occurs antegrade through APs and retrograde through AV node. It
is uncommon type also known as atypical AVRT. In ECG, it is characterized by wide
QRS.

53
CHAPTER 3
ACQUISITION OF CARDIAC ELECTRIC SIGNALS
This chapter describes the basic techniques developed for monitoring and
recording of cardiac electric activity. In a basic clinical diagnosis, cardiac
electric activity is picked from body surface through electrodes and this method is
known as ECG. Although ECG is good enough to observe different types of
abnormality in cardiac conduction system still many characteristics are not
examined by ECG, therefore invasive method is opted as an alternative. In
invasive method, cardiac electric signals are picked directly from inside heart
through electrodes mounted on catheter. The acquired signals are known as
IEGM. IEGM provides complete depth for observation as well as facilitates the
treatment against abnormality. The invasive recording of electrical pulses is
known as EPS. The EPS is done under special protocols that require external
pacing to bring heart in tachycardia state. The key features of both ECG and
IEGM and their relationship with intrinsic conduction system are discussed in
detail in this chapter.
3.1 Electrocardiogram
ECG is recording of heart’s electric activity from body surface of a person. For
monitoring of electric excitation inside the heart, electrodes are placed at various points
in a predefined pattern. A cyclic wave of depolarization initiates from SA node and
culminates at myocardium, passes through conduction pathway that generates relative
positive/negative deflections on surface electrodes. The recorded ECG pattern having
positive/negative deflection is an accumulative effect of heart’s electrical activity as
shown in Figure 3-1.

54
.
Figure 3-1 Accumulative effect of AP of various cardiac conduction cells in a
rhythm

55
Figure 3-2 Complete rhythm of depolarization/repolarization of atrium and
ventricular
The fiducial points observed in an ECG pattern, are given specific names as P, Q, R, S, T
and U waves. The depolarization of atrial muscle (myocardial cells) is deflected as P
wave and depolarization of ventricular muscle are deflected as R wave. Repolarization of
ventricular muscle is deflected as T wave whereas the repolarization of atrial muscles has
small magnitude and overlaps with R wave so it is not visible in ECG. The complete
cycle of depolarization/ repolarization on time scale for a normal heartbeat is shown in
Figure 3-2. The various features/ waveforms description of an ECG signal is given in
Figure 3-3.
Since heart is a three dimensional organ which contains various types of conduction cells
so the exact reflection of electric activity can be understood with combination of many
electrodes (covering three dimensions). Multiple electrodes are required to be placed at
different location on body to depict different views of electrical activity inside the heart.

56
Figure 3-3 The waveform/segment description of an ECG signal
No of electrodes varies depending upon number of views required e.g. 3 leads ECG
(requires 3 or 4 ECG electrodes), 5 leads ECG (require 4 electrodes) and 12 leads ECG
(require 10 electrodes). It can be observed that lead is not same as an electrode; electrode
is a physical contact point from where electrical signals are picked through wires whereas
a lead is a specific view which may be a combination of more than two electrodes makes
a vector measurements [40].
Leads combination may be further categorized as unipolar and biopolar leads. Bipolar
leads are the standard leads that require two electrodes (one considered as positive and
other as negative/reference) to measure an electrical signal variations between them.
Unipolar lead provides additional view of electrical activity, in which signal from an
electrode is picked with reference to a complex negative/reference point that is
combination of two or more electrodes.

57
12 leads ECG is most popular diagnostic ECG combination being followed worldwide.
12 leads have total 12 view combinations made from 10 electrodes. Out of 10 electrodes,
four are limb electrodes named in relation their relative position close to four limbs as
RA (right arm), LA (left arm), RL (right leg) and LL (left leg); six electrodes are the
chest electrodes named as V1-V6 (precordial). The electrode placement on the body is
shown in Figure 3-4.
Figure 3-4 Scheme of 10 electrodes placement (12 leads ECG)
These 12 leads may be categorized into following three sets i.e. limb, augmented limb
and precordial leads. Limb leads are bipolar combination produced from four limb
electrodes (RA, LA, RL and LL). Out of these four electrodes, LL serve as
reference/negative electrode and rest three generate ECG leads with reference to LL.
These leads are named as ‘I’, ‘II’ and ‘III’ as shown in Figure 3-5. Three limb leads

58
provides three different views of the heart in a vertical (frontal) plane. The bipolar limb
lead combinations are produced as following.
I LA RA (3-1)
II LL RA (3-2)
LIII LL A (3-3)
Figure 3-5 The combination of limb leads
Augmented limb leads are unipolar combinations produced from three limb electrodes
(RA, LA and LL). Here one electrode is taken as positive point and combination of
remaining two electrodes makes the reference/negative point. The augmented leads are
named as ‘aVR’, ‘aVL’ and ‘aVF’. This arrangement adds new view angles (vectors) in a
vertical (front) plane as shown in Figure 3-6.
The unipolar augmented limb lead combinations are produced as following. Combining
three limb leads and three augmented limb leads, total six view angles are generated in
vertical plane as shown in Figure 3-7.

59
R2
(LA+LL)aVR A (3-4)
L2
(RA+LL)aVL A (3-5)
LL2
(RA+LA)aVF (3-6)
Figure 3-6 The combination of augmented limb leads
Figure 3-7 The view angles in vertical plane

60
The precordial leads are also unipolar and these covers the horizontal (transverse) plane
meaning that their view angle is perpendicular to vertical (frontal) plane. Each pericardial
electrode is taken as positive terminal to provide six horizontal views whereas the
reference/negative point is generated by averaging the three limb leads RA, LA and LL
(1
3(RA+LA+LL) ) as the center of Wilson triangle. The six unipolar precordial lead
combinations are generated as following.
1V1
3V1 (RA+LA+LL)
(3-7)
1V2
3V2 (RA+LA+LL)
(3-8)
1V3
3V3 (RA+LA+LL)
(3-9)
1V4
3V4 (RA+LA+LL)
(3-10)
1V5
3V5 (RA+LA+LL)
(3-11)
1V6
3V6 (RA+LA+LL)
(3-12)
The six view angles that are generated in horizontal plane from six precordial leads as
shown in Figure 3-8. The complete picture (views) by 12 leads in three-dimensional
domain is shown in Figure 3-9.

61
Figure 3-8 The view angles by six precordial leads in horizontal plane
Figure 3-9 The complete three dimensional view by 12 leads ECG

62
3.2 The Intracardiac Electrogram
The IEGM signals are the localized electrical activity recorded by the electrode catheter
placed directly inside the heart contrary to the ECG in which signals are picked from the
surface of body. ECG represents the vector analysis of electric pulse from different
angles in three domains however, these vectors are sometime unable to provide complete
picture. Therefore, we need to pick localized depolarization being occurred at different
locations of the heart’s conduction circuit. The ECG provides the superimposed picture
of all AP, whereas the IEGM records a timed depolarization/repolarization process for
desired portion of the conduction path. The IEGMs are recorded and analyzed in an EPS
to detect and treat the loci that are source of cardiac arrhythmia [24].
In EP study, specialized electrode catheter is inserted inside the body through some vein
(mostly femoral vein), then catheter is maneuvered to be placed inside the heart at
specific location as shown in Figure 3-10. Usually four catheters are inserted depending
upon the requirement of observation points. The signal from catheters are pre-processed,
amplified and recorded on a computer-based system.
During procedure, it is also required to change the heart-beating rate so an external
stimulus is provided at specific location inside the heart through catheter, under some
special protocols to observe cardiac response. This process is known as Pacing or
Stimulation.
Vital signs such as ECG, blood pressure (BP) and pulse oximetery are also monitored on
independent equipment so that patient safety can be ensured simultaneously. Defibrillator
equipment is also made readily available during EPS to counter abruptly induced
fibrillation state of the heart.

63
Figure 3-10 Catheter placement procedure
Mapping of AP at multiple points inside specific chamber can also be done through
specialized catheter e.g basket catheter, circular catheter etc. The purpose of mapping is
to correlate the electric activities simultaneously at different foci inside the heart.
After determining the cause of problem, it is required to burn the tissues that are
providing undesired conductivity and giving abnormality in heart rhythm. For this
purpose, RF (300-750 kHz) is delivered to the desired locus through the catheter that
produces heat and burn the desired tissues. This process is known as Ablation.

64
Figure 3-11 EP catheter electrode
3.3 Cardiac Catheterization for EP Study
3.3.1 IEGM Catheters
Catheter is a flexible insulated thin cable that is inserted into the heart. Catheters are of
different types and shapes. It has a handle/control at its rear end that is used to maneuver
it through blood veins and heart’s chamber, as shown in Figure 3-11. First role of catheter
is diagnostic however, these are also used for pacing and ablation purpose [41].
Multiple electrodes are mounted on a catheter. Catheter may be configured in unipolar or
bipolar mode. In bipolar mode, two adjacent electrodes are used as a pair as shown in
Figure 3-12. Bipolar electrodes are preferred for recording of localized AP activity. Inter
electrode spacing between two electrodes as well as between two pair of electrodes are a
design feature specified for different applications; a 2-5-2mm electrode spacing means
that gap between two +/- pair of electrodes is 2mm whereas gap between a pair to another
pair is 5mm.

65
Figure 3-12 Bi-polar catheter configuration
3.3.2 Basic Catheter Configuration
During an EP study, multiple catheters are placed simultaneously however, the basic EP
procedure requires following standard catheter configuration. These catheters are named
on basis of their location of employment as shown in Figure 3-13.
HRA Catheter. HRA (high right atrium) catheter is placed with the right atrium wall
near the SVA to record atrial activity initiated by SA node. Usually it is a quadripolar
type (contains 4 electrodes).
RVA Catheter. RVA (right ventricular apex) catheter is placed as close as possible
with the apex of right atrium. It records the electric activity of purkinje fibers and
myocardium of right ventricle. Usually it is also quadripolar type.
CS Catheter. CS (coronary sinus) catheter is placed in coronary sinus vein. It is used
to record the AP of the left side (LA and LV) of the heart. A steerable decapolar
catheter (contains 10 electrodes) is preferred.

66
HIS Catheter. His catheter is located near His bundle (located superior side of
tricusipid annalus) to record AP activity of AV node and of His bundle. A curved tip
steerable quadripolar catheter is preferred.
http://www.theeplab.com/B-The-Members-Center/E000-EP-Procedures/B-Catheter-Placement/EB00-Catheter-
Placement.php
Figure 3-13 Basic configuration of HRA, His, RVA and CS catheters and their
fluroscopic view in left anterior oblique (LAO) position
3.3.3 Basic Features of IEGMs
In one rhythm of ECG, ‘P’, ‘QRS’ and ‘T’ etc waves are taken as feature that reflects
accumulative depolarization/repolarization of atria/ventricle. In IEGMs, we record
localized depolarization near the electrode catheter (in bipolar configuration) so we get an

67
electric pulse when a depolarization wave front passes near the electrode catheter. In
IEGM, we have three distinct features named as following:
A-wave. It represent atrial depolarization and can be seen good in HRA catheter and
small amplitude A-wave can also be seen on His and CS catheters.
H-wave. It represent the depolarization in bundle of His. It is a small amplitude signal
and can be seen only in His catheter.
V-wave. It represent ventricular depolarization and posses a strong amplitude in RVA
catheter and it can also be seen good in His catheter.
Correlation between IEGM waves and ECG feature is shown in Figure 3-14 which
illustrate ‘A’,’V’ and ‘H’ waves in relation to normal ECG signal. In IEGM, the ‘A’ and
‘V’ wave features are observed on more than one pair of electrodes (bipolar) which
depicts the time gaps/durations of the electric pulse traveling from one point to other. The
sequence/time gap of a feature at different locations provides the evidence of conduction
path being followed and thus depicts the abnormality if any.
Figure 3-14 Correlation between IEGM and ECG features
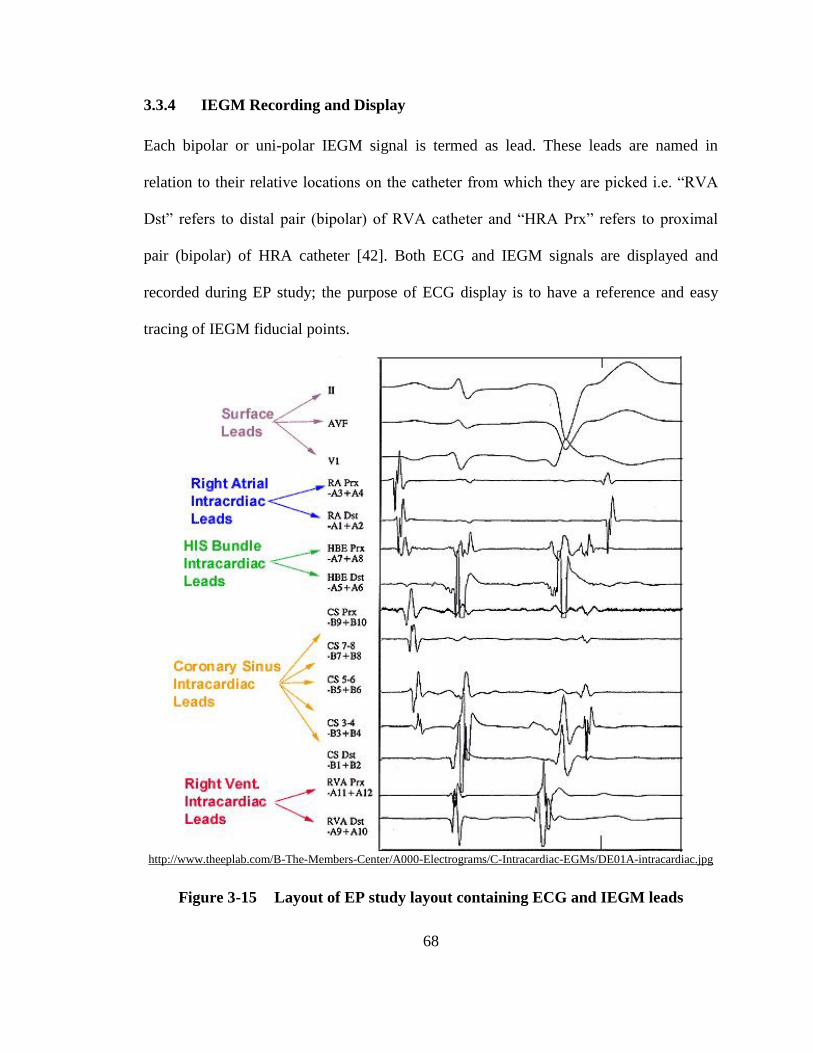
68
3.3.4 IEGM Recording and Display
Each bipolar or uni-polar IEGM signal is termed as lead. These leads are named in
relation to their relative locations on the catheter from which they are picked i.e. “RVA
Dst” refers to distal pair (bipolar) of RVA catheter and “HRA Prx” refers to proximal
pair (bipolar) of HRA catheter [42]. Both ECG and IEGM signals are displayed and
recorded during EP study; the purpose of ECG display is to have a reference and easy
tracing of IEGM fiducial points.
http://www.theeplab.com/B-The-Members-Center/A000-Electrograms/C-Intracardiac-EGMs/DE01A-intracardiac.jpg
Figure 3-15 Layout of EP study layout containing ECG and IEGM leads

69
http://www.theeplab.com/B-The-Members-Center/A000-Electrograms/C-Intracardiac-EGMs/DE01G-intracardiac4.jpg
Figure 3-16 Propagation of ‘A’ wave sequentially from RA to CS leads
Usually 2-3 different ECG leads selected by electrophysiologist, are displayed at the top
and then 8-12 different IEGM leads are displayed subsequently. It is preferred that order
of leads display is in a sequence in which electric pulse flow in normal conduction path.
The preferred layout contains first ECG leads, then HRA leads, His leads, CS leads and

70
RVA leads are displayed as shown in Figure 3-15. This figure shows the complete set of
waveforms that is available during basic EP study. This sequence facilitates to correlate
different features. For example, we can locate ‘A’ wave first in HRA catheter prior to ‘P’
wave in ECG, then it is progressively visible in His and CS catheter with delayed in time
axis because of natural conduction sequence; however ‘A’ is not visible in RVA catheter
as shown in Figure 3-16. ‘H’ wave is very small and is visible between A & V in HIS
catheter only.
Figure 3-17 Appearance of ‘A’-wave and ‘V’-wave

71
The V signal is most dominating and can easily first identified in RVA distal prior to R
wave in ECG, and progressively appear (delayed in time axis) in the other leads from
bottom to top as can be seen in Figure 3-17.
3.3.5 Programmed Electrical Stimulation
To observe the AP properties of the heart, external pacing (stimulation) at faster rate is
carried out and corresponding response is observed. In programmed electrical stimulation
(PES), a sequence of electric pulses are given in a specific pattern that overdrives the
natural pacing sequence of heart and tachycardia is induced. Activation pattern in
tachycardia, its initiation/termination and response to extra stimuli is observed closely.
The rate of pacing is also increased gradually under a specific protocol to study the
conduction and refractoriness of cardiac cells.
Figure 3-18 Antegrade Versus Retrograde Pacing
Stimuli are given in a combination of multiple stimulus (typically 6-8 pulses) in a
sequence known as drive train. Amplitude of stimulus should be typically 2-4 times of

72
diastolic threshold and have width 1-3ms (millisecond). Based on the location , pacing is
done in following two ways, as shown in Figure 3-18 [18].
Antegrade pacing. Pacing in atrium is carried out close to SA node (but not at SA
node) through HRA catheter.
Retrograde pacing. Pacing in ventricular is carried out through RVA catheter or
sometime His catheter. It provides insight of bottom up electrical conduction paths.

73
CHAPTER 4
PRE-PROCESSING OF INTRACARDIAC SIGNALS
Heart’s electrical activity when picked through invasive or non-invasive
electrodes have very low amplitude, thus IEGM/ECG is highly vulnerable to
noise. For accurate extraction of ECG/IEGM features, the noise removal is very
important, however removing noise from the IEGM/ECG signal may also distort
valuable contents therefore, optimal filter designing is required to avoid loss of
vital signal information. In this chapter, noise removal of PLI and EMG noises
are taken care off.
4.1 Scope of Pre-Processing
During EP study, the onset of IEGM features i.e. A, H and V waves are used to classify
the arrhythmia. The classification accuracy greatly depends upon signal to noise ratio
(SNR) of the IEGM. Therefore it is required to pre-process an IEGM signal such that
fiducial points remain preserved as much as possible. The pre-processing of an IEGM
includes removal of PLI, EMG and in some cases BLW as well. This is followed by
marking of fiducial points to extract features and finally arrhythmia classification as
shown in Figure 4-1.
Figure 4-1 Stages of Arrhythmia Classification Algorithm

74
Filtration requirement of different kind of cardiac signal for an EP study is as shown in
Table 4-1 [42].
Table 4-1. Filtration requirement for ECG/IEGM signals
ECG/IEGM High Pass Filter Low Pass Filter
Surface ECG 0.1Hz 100 Hz
Bi-polar IEGM 30 Hz 300 Hz
Uni-polar IEGM 1Hz 300 Hz
Uni-polar IEGM
(unfiltered) 0.1 Hz 400 Hz
Filtration requirement for bipolar signal is from 30-300 Hz and for unipolar signal is 1-
300 Hz [15, 42]. The useful features of ECG/IEGM may be spoiled if proper frequency
ranges are not taken care while performing pre-processing[43]. In most of cases, bipolar
IEGM configuration is used, so frequency range should be applied accordingly. Figure
4-2 illustrates the importance of inappropriate frequency ranges. In Figure 4-2(a),
ECG/IEGM both signals are filtered with the frequency range of 0.5-300 Hz which is not
suitable for a bipolar IEGM lead and will distort/override the small H wave. In Figure
4-2(b), ECG/IEGM both signals are filtered with the frequency range of 30-300 Hz which
is good for IEGM but inappropriate for ECG signal thus compromise the ECG features.
Figure 4-2(c) shows the appropriate way of pre-processing in which ECG signal is
filtered with 0.5-300 Hz and IEGM signal is filtered with 30-300 Hz and feature
information remains preserved.

75
(a) (b) (c)
Figure 4-2 Effect of inappropriate frequency band selection during pre-
processing [15].
Similarly if a notch filter is employed for removal of PLI, the ringing effect is generated
which distort the valuable information present in IEGMs as shown in Figure 4-3.
Figure 4-3 Effects of a notch filter for removal of PLI [15].

76
4.2 Power Line Interference
PLI and its harmonics is the most devastating noise even if the IEGM/ECG equipment is
operated on battery. The problem is further complicated when frequency of PLI is not
static, making the conventional notch filter completely ineffective. IEGM signals are
further complicated with presence of harmonics of PLI as well. The frequent variations in
PLI frequency poses a serious problem and it is further enhanced because of involvement
of multiple power sources being used in health care centers (in Pakistan), which include
1) the electric power provided from main grid, 2) the uninterruptable power supply (UPS)
and 3) generator power sources. Moreover, the frequency of main grid also varies largely
because of fluctuation of load on main grid. In this section, an intelligent adaptive noise
rejection filter has been proposed which tracks and eliminates PLI as well as its
harmonics. The proposed system can estimate the frequency of PLI and tune the adaptive
filter for precise elimination of PLI as well as its harmonics without requirement of an
auxiliary reference input. The proposed system is based on recursive state space model,
inherited with less computational complexity and performs well in a non-stationary
environment. The proposed system responds well to the ongoing variations in amplitude
and frequency of PLI present in IEGM signals. The proposed system does not require any
reference signal for tracking the PLI and its harmonics, it is capable to self adjust its
tracking frequency.
4.2.1 Literature Review - PLI
IEGM having a wider frequency band of interest (1-300 Hz) is more sensitive to various
kinds of noises; out of which PLI is most disruptive disturbance. For the case of IEGM
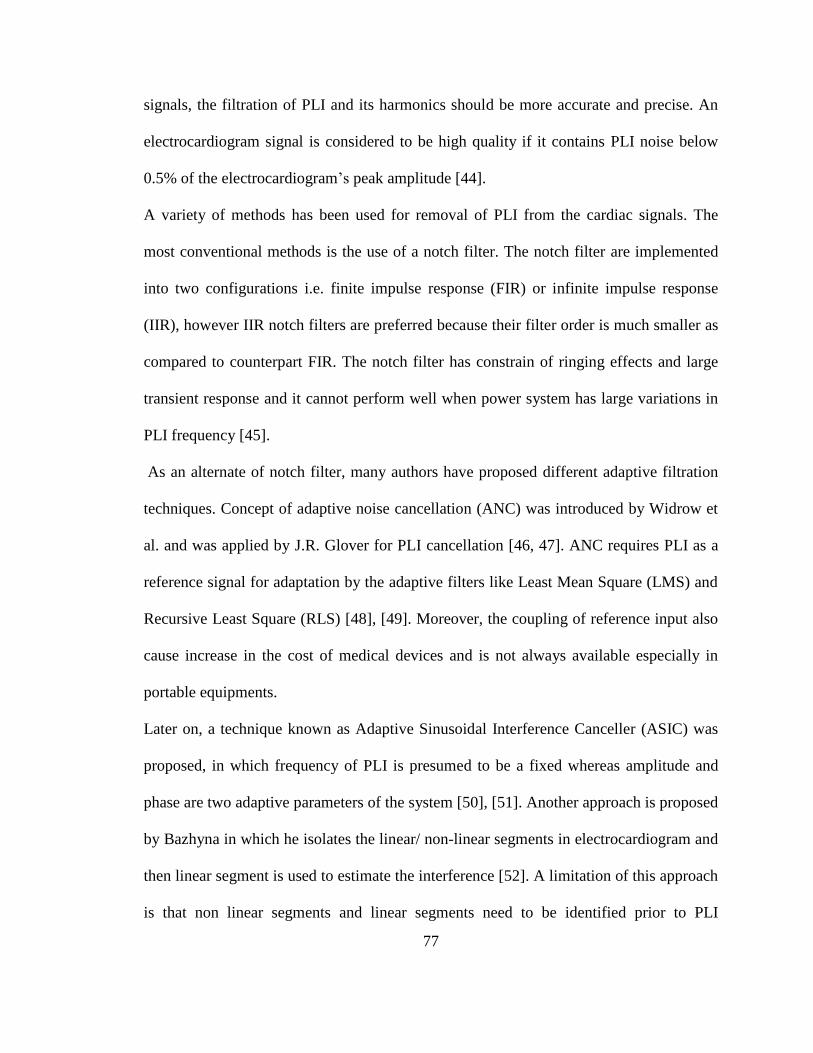
77
signals, the filtration of PLI and its harmonics should be more accurate and precise. An
electrocardiogram signal is considered to be high quality if it contains PLI noise below
0.5% of the electrocardiogram’s peak amplitude [44].
A variety of methods has been used for removal of PLI from the cardiac signals. The
most conventional methods is the use of a notch filter. The notch filter are implemented
into two configurations i.e. finite impulse response (FIR) or infinite impulse response
(IIR), however IIR notch filters are preferred because their filter order is much smaller as
compared to counterpart FIR. The notch filter has constrain of ringing effects and large
transient response and it cannot perform well when power system has large variations in
PLI frequency [45].
As an alternate of notch filter, many authors have proposed different adaptive filtration
techniques. Concept of adaptive noise cancellation (ANC) was introduced by Widrow et
al. and was applied by J.R. Glover for PLI cancellation [46, 47]. ANC requires PLI as a
reference signal for adaptation by the adaptive filters like Least Mean Square (LMS) and
Recursive Least Square (RLS) [48], [49]. Moreover, the coupling of reference input also
cause increase in the cost of medical devices and is not always available especially in
portable equipments.
Later on, a technique known as Adaptive Sinusoidal Interference Canceller (ASIC) was
proposed, in which frequency of PLI is presumed to be a fixed whereas amplitude and
phase are two adaptive parameters of the system [50], [51]. Another approach is proposed
by Bazhyna in which he isolates the linear/ non-linear segments in electrocardiogram and
then linear segment is used to estimate the interference [52]. A limitation of this approach
is that non linear segments and linear segments need to be identified prior to PLI

78
detection thus makes the system more complex. Koseeyaporn et al. use geometric
representation and PLI as a combination of sine and cosine waves [53]. They adjust the
amplitude of reference signal by varying the amplitude/phase of sine and cosine waves
using LMS algorithm. Islam S. Badreldin et al. presented the adaptive removal of PLI
noise and its harmonics from cardiac signal without sampling an external power line
reference [54], [55].
In this work, an adaptive configuration is applied which does not require a reference
signal to track and eliminate the PLI present in the IEGM signal effectively [56]. While
dealing with IEGM signals, we need to filter out PLI interference as well as its
harmonics. To cater for the PLI frequency variation, an online frequency estimation
technique is implemented which dynamically tunes adaptive filter with ongoing changes
in frequency thus making its functioning highly effective.
4.2.2 Problem Formulation
The desired frequency spectrum of a standard bipolar IEGM lead is 30-300 Hz and in
some cases electrophysiologist may prefer frequency band 0.1-400 Hz therefore,
sampling frequency of IEGM signal must be 1 kHz or greater [57, 58].
Ideally, a 50 Hz AC power system contains only fundamental frequency component of 50
Hz but practically, integral multiples of fundamental frequency known as harmonics are
also present. Generally only odd harmonics are present in the power system because of
half wave symmetry property [59]. For a standard ECG signal, we are interested in
frequency band of 1-80Hz, therefore we need to tackle only the 1st harmonic i.e.,
fundamental frequency however, for an IEGM signal, we need to take care of 3rd
and 5th

79
harmonics of PLI as well. Therefore, in case of 50 Hz power system, we need to track
and eliminate 50, 150, and 250 Hz frequency components simultaneously. In case larger
frequency band of IEGM lead is desired, the higher odd harmonics of PLI (i.e. 350, 450
Hz etc) may be taken into account.
As a case study, a raw IEGM signal recorded at National Institute of Heart Diseases
(NIHD) Pakistan, which is sampled at 2000 samples/sec, is selected as shown in Figure
4-4. The IEGM waveform shown in Figure 4-4 is in raw form i.e. it contains PLI along
with its harmonics and other noises as well. To observe frequency components of this
raw IEGM, its frequency spectrum is shown in Figure 4-5. The frequency spectrum
shown in Figure 4-5 clearly depicts the presence of fundamental frequency and odd
harmonics of PLI; it is also evident that there is no presence of even harmonics. For
IEGM, we apply low pass filter at 300 Hz which means that we need to tackle 1st
(fundamental frequency), 3rd
, and 5th
harmonics only.
IEGM signal corrupted with PLI and its harmonics can be represented by
[ [[ ] ] ] IEGM PLIy n x n x n (4-1)
where [ ]y n is IEGM signal corrupted by PLI, [ ]IEGM
nx is the pure IEGM signal and
[ ]PLI nx is the PLI noise consisting of 1st, 3
rd, and 5
th harmonics of PLI and can be
represented by
1 1 3 3 5 5[ ] sin( ) sin(3 ) sin(5 )
PLIx n n n n (4-2)

80
Where n is the discrete time index, ω is the normalized PLI frequency defined as
L s= 2 f / f ; Lf is the fundamental PLI frequency, sf is sampling frequency. 1α , 3α , 5α
are amplitudes of the 1st , 3
rd, and 5
th PLI harmonics respectively. 1φ , 3φ , and 5φ are phases
of the 1st , 3
rd, and 5
th PLI harmonics respectively.
0 0.5 1 1.5 2 2.5 3 3.5 4
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
0.4
0.6
0.8
1Corrupted IEGM Signal
Time (seconds)
No
rmali
zed
Am
pli
tud
e
Figure 4-4 IEGM data sampled at 2 kHz (No signal filtration/processing applied)
The state space model encompassing 1st, 3
rd, and 5
th harmonics of PLI is derived as
following:
Let the 1st harmonic i.e. 1 1
sin( )n be the first state of a sixth order state space
system and the second state is also 1st harmonic with a phase shift of / 2 as following.

81
2
1 1 1
1 1
sin( )
cos( )
[ ]
][
n
n
x n
x n
(4-3)
0 100 200 300 400
-60
-40
-20
0
20
40
60
80
100
120Frequency Spectrum of HRECG
Frequency (Hz)
Ma
gn
itu
de
(d
B)
Fundamental power frequency
3rd harmonic5th harmonic
7th harmonic
Figure 4-5 Frequency spectrum of Raw IEGM signal
Similarly, the 3rd
and 4th
states represent 3rd
harmonic of PLI.
4
3 3 3
3 3
sin(3 )
cos(3 )
[ ]
[ ]
n
n
x
x
n
n
(4-4)
And the 5th
and 6th
states represent 5th
harmonic of PLI.
6
5 5 5
5 5
sin(5 )
cos(5 )
]
]
[
[
n
n
x n
x n
(4-5)

82
Using trigonometric identities, we may rewrite the six states as
1 1 1
1 1 1
3 3 3
3 3 3
5 5 5
5 5 5
1
2
3
4
5
6
[ ]
[ ]
[ ] 3 3
[ ] 3 3
[ ] 5 5
[ ] 5 5
sin cos cos sin
(cos cos -sin sin )
sin cos cos sin
(cos cos -sin sin )
sin cos cos sin
(cos cos -sin sin )
n
n
n
n
n
n
x n n
x n n
x n n
x n n
x n n
x n n
(4-6)
Equation (6) may be rewritten as
1 1
1 1
3 3
3 3
5 5
5 5
1
2
3
4
5
6
cos sin
cos
3 3
3 3
5 5
5 5
sin
cos-sin
sincos sin
cos-sin cos
sincos sin
cos-sin cos
0 0 0 0[ ]
[ ] 0 0 0 0
[ ] 0 0 0 0
[ ] 0 0 0 0
[ ] 0 0 0 0
[ ] 0 0 0 0
x
x
x
x
x
x
n
n
n
n
n
n
(4-7)
Defining initial condition at n = 0, we have
1 1 1 1 3 31 2 3
4 3 3 5 5 5 55 6
[0] [0] [0]
[0] [0] [0]
x = α sinφ , x = α cosφ , x = α sinφ
x = α cosφ , x = α sinφ , x = α cosφ (4-8)
Putting initial conditions and considering states at n = 1 in (7) we get
1 1
2 2
3 3
4 4
5 5
6 6
cos sin
cos
3 3
3 3
5 5
5 5
-sin
cos sin
-sin cos
cos sin
-sin cos
0 0 0 0[1] [0]
[1] [0]0 0 0 0
[1] [0]0 0 0 0
[1] [0]0 0 0 0
[1] [0]0 0 0 0
[1] [0]0 0 0 0
x x
x x
x x
x x
x x
x x
(4-9)

83
Similarly, starting with initial states, we can recursively update states at any time
0n > .
The generalized form of (4-9) can be re-written as:
1 1
2 2
3 3
4 4
5 5
6 6
cos sin
cos
3 3
3 3
5 5
5 5
1]
1] -sin
1] cos sin
1] -sin cos
1] cos sin
1] -sin cos
0 0 0 0[ [ ]
[ [ ]0 0 0 0
[ [ ]0 0 0 0
[ [ ]0 0 0 0
[ [ ]0 0 0 0
[ [ ]0 0 0 0
x n x
x n x
x n x
x n x
x n x
x n x
n
n
n
n
n
n
(4-10)
Here
cos sin
cos
3 3
3 3
5 5
5 5
-sin
cos sin
-sin cos
cos sin
-sin cos
0 0 0 0
0 0 0 0
0 0 0 0
0 0 0 0
0 0 0 0
0 0 0 0
is state
transition matrix, which is marginally stable i.e. all its eigen values lie on the unit circle.
This transition matrix represents the state space model of 1st, 3
rd, and 5
th harmonics of
PLI, which is dependent on only one parameter i.e. normalized fundamental PLI
frequency.
4.2.3 Methodology
A state space recursive least square (SSRLS) adaptive filter configuration as shown in
Figure 4-6 is proposed for elimination of PLI from IEGM signal.

84
Proposed layout suggests the use of SSRLS as adaptive noise canceller, in which 1st, 3
rd,
and 5th
harmonics of PLI are adaptively tracked by SSRLS filter and then subtracted from
corrupted IEGM signal to get pure IEGM. The overall filtration performance depends
upon the tracking accuracy of the SSRLS filter. The performance of tracking depends on
the selection of frequency for tracking whereas the frequency of PLI is not constant
therefore, we need to estimate the fundamental frequency of PLI and tune the SSRLS
filter accordingly. For monitoring the frequency of PLI, an intelligent DFT (Discrete
Fourier Transform) is applied. A batch of data is processed to estimate fundamental PLI
frequency and the estimated frequency is fed to adaptive filter. The signal is fed to
adaptive filter through a delay block because of inherent delay involved in frequency
estimation process.
Figure 4-6 Proposed layout for elimination of PLI and its harmonics

85
The proposed combination allows us to adaptively adjust itself to any change in
frequency and tracks the amplitude/phase of 1st, 3
rd, and 5
th harmonics of PLI for
selective filtration without distorting the other frequency components of IEGM signal.
The description of each block is given in subsequent sections.
4.2.4 Frequency Estimation
Fundamental frequency of PLI is estimated prior to SSRLS filtration which is used for
tracking 1st, 3
rd, and 5
th harmonics by the SSRLS filter. For estimation of power line
fundamental frequency, an intelligent DFT algorithm is employed which provides high
resolution frequency estimation [56]. Intelligent DFT works on the assumption that
fundamental frequency of PLI dominates in the frequency band of 45-55 Hz of PSD
(Power Spectral Density) of a PLI corrupted IEGM. This assumption meets the criteria of
a good quality electrogram to have PLI component less than 0.5% of its peak amplitude
[44]. The intelligent DFT algorithm is intelligent in a sense that it provides high
resolution frequency estimation with less number of operation counts as well as performs
well with small data window size which makes it feasible for online frequency
estimation. DFT of N points sequence is calculated as.
1 2 /.
0
N j kn NX x enk n
(4-11)
where N defines the size of data window selected for DFT and xn refers to nth discrete
signal entity of selected window. k is the discrete frequency index defined by
( / ) sk N f f , where f is the frequency in hertz and sf is sampling frequency.

86
For the case of diverging PLI frequency, our requirement is to observe online PLI
frequency changes precisely. Since maximum variation in PLI frequency is limited to
10% , we need to focus on the frequency band of 45-55Hz (for 50 Hz power system) to
search for fundamental PLI frequency. Fast Fourier Transform (FFT) is commonly
employed method for PSD estimation, which transforms the complete frequency
spectrum (i.e. 2
sf), thus makes it inefficient for our requirement. Moreover FFT cannot
provide high resolution frequency estimation without zero padding when smaller window
size is selected for transformation into frequency domain as discussed in detail in [56].
On the other hand we can calculate DFT against desired discrete frequencies lying in
frequency band of 45-55Hz by direct application of (11). The frequency resolution
achieved through DFT can be calculated by
/df f (4-12)
where df is the frequency resolution, f is the desired frequency band and is the
number of frequency bins. If we increase the frequency resolution, we need to increase
the number of frequency bins thus require more computations to perform. Our desired
f is 45-55 Hz. To have frequency resolution of 0.01Hz through basic DFT algorithm,
we require 1,000 frequency bins.
In intelligent DFT algorithm, the frequency resolution is enhanced with less cumulative
number of the frequency bins. Here df is gradually increased by narrowing down f
gradually. Resultantly we achieve higher frequency resolution with much reduced
computational effort. No zero padding is used for enhancement of frequency resolution.

87
Application of Hanning windowing is useful in order to overcome the spectral leakage
issues. Functioning of intelligent DFT algorithm is depicted in flow chart shown in
Figure 4-7.
Figure 4-7 Intelligent DFT - Flow chart.

88
The search of 49.36 Hz frequency in three stages by the proposed algorithm is shown in
Figure 4-8, where frequency resolution of 0.01 Hz is achieved with only 30 frequency
bins (in 45-55 Hz frequency band) in three stages. In first stage, we select 10 frequency
bins, it will provide frequency resolution ( df ) of 1 Hz and out of these 10 frequency
bins, only two bins with highest magnitude are chosen to select a frequency band for next
stage. In next stage, we have to deal with bandwidth of 1 Hz and recalculate the DFT
with 10 frequency bins thus we achieve frequency resolution of 0.1 Hz. Therefore, df is
enhanced 10 times in each stage by just doubling the computation. Resultantly the df of
0.01 Hz is achieved in three stages with 30 frequency bins instead of 103 frequency bins
hence computational complexity is reduced manifolds.
Figure 4-8 Working of intelligent DFT: The resolution of PLI frequency
estimation is gradually enhanced in each subsequent stage and a resolution of
0.01Hz is achieved by performing DFT of 30 frequency bins only in three stages.
Enhancement of frequency estimation resolution in three stages.

89
A comparison between FFT, DFT and proposed intelligent DFT techniques has been
carried out in order to compare operation counts and time lag (delay caused because of
samples, if no zero padding is applied). Let 2sf KHz and desired 0.01df Hz . The
computational complexity and number of samples required to estimate the PLI signal in
the band of 45-55 Hz, through each technique, are given in Table 4-2. Proposed
algorithm achieves a explicit reduction in operation counts as compared to DFT and FFT.
Table 4-2 FFT, DFT and intelligent DFT comparison for PLI frequency search
with 0 01.df Hz
Parameters FFT DFT Intelligent DFT
No of samples
required (N)
/ sN f df
=2x105
10 cycles of 50Hz
PLI = 400
10 cycles of 50 Hz PLI
= 400
Delay involved 100 seconds 0.2 seconds 0.2 seconds
Frequency
selection range
( f )
f =1000
Hz
(by default
/ 2sf )
f =10 Hz
110Hzf (1
st iteration)
21Hzf (2
nd iteration)
30.1Hzf (3
rd iteration)
No of
frequency bins
( )
N =
2x105
/f df =103
110 (1
st iteration),
210 (2
nd iteration),
310 (3
rd iteration)
1 2 330
No of
operation count
(Computation
complexity)
22 log ( )N N
=7.05X106
N
= 4.0X105
N
=1.2X104

90
The high resolution frequency estimation is achieved with a small batch of data without
any zero padding. However to ensure a consistent outcome of intelligent DFT, minimum
size of data batch (N) is restricted to contain at least 10 cycles of the frequency to be
observed. For the case of PLI (50 Hz) frequency estimation with sampling frequency of 2
kHz, a batch of 500-1000 samples is an appropriate choice. Having a larger batch size
will cause lesser variation in outcome however, at the cost of delay incurred for
collection of complete batch.
For online monitoring of variations in PLI frequency, the intelligent DFT can be
implemented on successive data segments as sliding DFT [60]. If the selection of next
data window is done with a jump (gap) by number of samples equal to length of window,
the connective windows are non-overlapping.
Use of non-overlapping windows technique requires less number of windows over the
entire data length; renders minimum computational effort however, observation delay of
full window length is faced. To reduce observation time delay, the consecutive windows
can be overlapped; resultantly total numbers of windows over entire data length will
increase. Since computational effort of intelligent DFT algorithm is much reduced
therefore for each new window, intelligent DFT is reapplied without using the results of
previous (partially overlapped) window. The increase in computational cost will be only
in term of increased number of windows; conversely observation delay will also be
reduced in same proportion. Using the half window overlap configuration is an
appropriate choice.

91
Figure 4-9 (a) Non-overlapping window with observation delay of N samples, (b)
Half window overlapping with observation delay of N/2 samples
Suppose at discrete time instance n, a batch of data ( )x n consisting of N samples is
selected as following
- 1 - 2 -1( ) { , ,...., , }
n N n N n nx n x x x x (4-13)
For the case of half window overlap configuration means that the connective data
window slides by N/2 samples and is defined as
2 2 2 22 - 1 - 2 -1
( ) { , ,...., , }
N N N N
N
n n n nnx x x x x
(4-14)
The observation delays for the case of non overlapping window as well as half window
overlapping cases are shown in Figure 4-9.

92
Figure 4-10 Sliding window DFT and delay caused.
4.2.5 Delay Block
To counter the delay caused because of batch processing of DFT algorithm, a delay
block is used before adaptive filtration system as shown in Figure 4-6. The initial delay
caused is equal to size of the data window; thereafter the amount of delay (D) depends on
the number of samples we slide between two consecutive windows (overlap). The delay
caused by half window overlap configuration is shown in Figure 4-10. For example if
window size is the 500 samples and half window overlap configuration is used, the initial
delay will be 500 samples and thereafter delay will be 250 samples. The ongoing delay
can be reduced by increasing window overlap i.e. if window size of 500 samples is in ¾
overlap configuration, the delay will be of 125 samples.

93
4.2.6 SSRLS Adaptive Filter
The SSRLS is an adaptive filter which works in state space framework [61]. Let the
unforced discrete time state space system be described as follows.
[ 1] [ ] [ ]
[ ] [ ] [ ] [ ]
x n A n x n
y n C n x n v n (4-15)
where [ ]x n is the state vector at time index n and [ ]A n is the system matrix. [ ]y n is the
desired output vector, [ ]C n is output matrix and [ ]nv is output disturbance vector which
may be considered as observation noise.
Comparing (4-10) and (4-15), we have
1 2 3 4 5 6[ ] [ ] [ ] [ ] [ ] [ ][ ] T
x n x n x n x n x n x nx n (4-16)
and
cos sin
cos
3 3
3 3
5 5
5 5
-sin
cos sin
-sin cos
cos sin
-sin cos
0 0 0 0
0 0 0 0
0 0 0 0
0 0 0 0
0 0 0 0
0 0 0 0
A
(4-17)
SSRLS filter estimates the states ˆ[ ]x n on each observation [ ]y n . The working of
SSRLS algorithm is summarized here.
The estimated state vector and estimated output is given by
ˆ[ ] [ ] [ ] [ ]
ˆ ˆ[ ] [ ]
x n x n K n n
y n Cx n (4-18)

94
where ˆ[ ]x n is a posteriori state estimate and [ ]x n is the a priori state estimate,
defined as
ˆ[ ] [ -1]x n Ax n (4-19)
[ ] n is the prediction error, taken as
[ ] [ ] - [ ] n y n y n (4-20)
[ ]y n is the predicted output state defined as
ˆ[ ] [ -1]y n CAx n (4-21)
[ ]K n is the observer gain defined as
-1
[ ] [ ] T
K n n C (4-22)
[ ] n is recursively updated by
- -1
[ ] [ -1] T T
n A n A C C (4-23)
where λ is the forgetting factor which defines the selectivity of adaptive filter
and its value lies in the range of 0 < λ < 1 . The value of λ close to 1 means highly
selective filter i.e. it have narrow bandwidth.
Working of SSRLS adaptive filter is shown in Figure 4-11. The tracking of 1st,
3rd
, and 5th
harmonics of PLI are desired, therefore we choose C vector in (14) as
1 0 1 0 1 0C (4-24)
With this C vector, the estimated output ˆ( )y n will be as follows.
[ ] [ ] [ ]1 3 5
ˆ[ ] n n ny n x x x (4-25)

95
Figure 4-11 Working of SSRLS.
Comparing (4-3), (4-4), (4-5), and (4-25) we have
1 1 3 3 5 5sin( ) sin(3 ) sin(5 )ˆ[ ] n n ny n (4-26)
The output ˆ[ ]y n is the estimated PLI noise [ ]PLI
nx as defined in (4-2). Subtracting
ˆ[ ]y n from corrupted IEGM signal [ ]y n gives us pure IEGM signal [ ]IEGM
x n .
[ [] [ ] ] IEGM
x n y n y n (4-27)
For initialization, regularization or delayed recursion techniques are the choices; we
choose the delayed recursion technique because of superior convergence properties[61].
In order to start the recursion of SSRLS, we need to define the initial estimate of states
x̂[0] and initial observer gain K[0] at time k = 0 . The SSRLS filter starts with these
arbitrary values and then adaptively estimates the states of the system.

96
During the initial period, the selectivity of proposed adaptive filter is not taken very high
i.e. λ 0.95 because the value of is not certain. During the initial period, is also
estimated simultaneously by intelligent DFT. After the initial period, the SSRLS is tuned
with correct value of and thereafter λ is enhanced for highly selective narrow band
tracking. The wider band tracking during initialization, allows us to track the surrounding
frequency components of arbitrary for initial period.
4.2.7 Results
For testing /demonstration of proposed algorithm, an IEGM signal acquired from
National Institute of Heart Diseases (NIHD) at sampling rate of 2000 samples/second is
selected as test signal. This test signal is then normalized. Pure sample IEGM signal is
shown in Figure 4-12.
0 0.2 0.4 0.6 0.8 1
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
0.4
0.6
0.8
1IEGM Test Signal
Time (seconds)
No
rmali
zed
Am
pli
tud
e
Figure 4-12. IEGM Test signal with sampling rate of 2000 samples/sec.
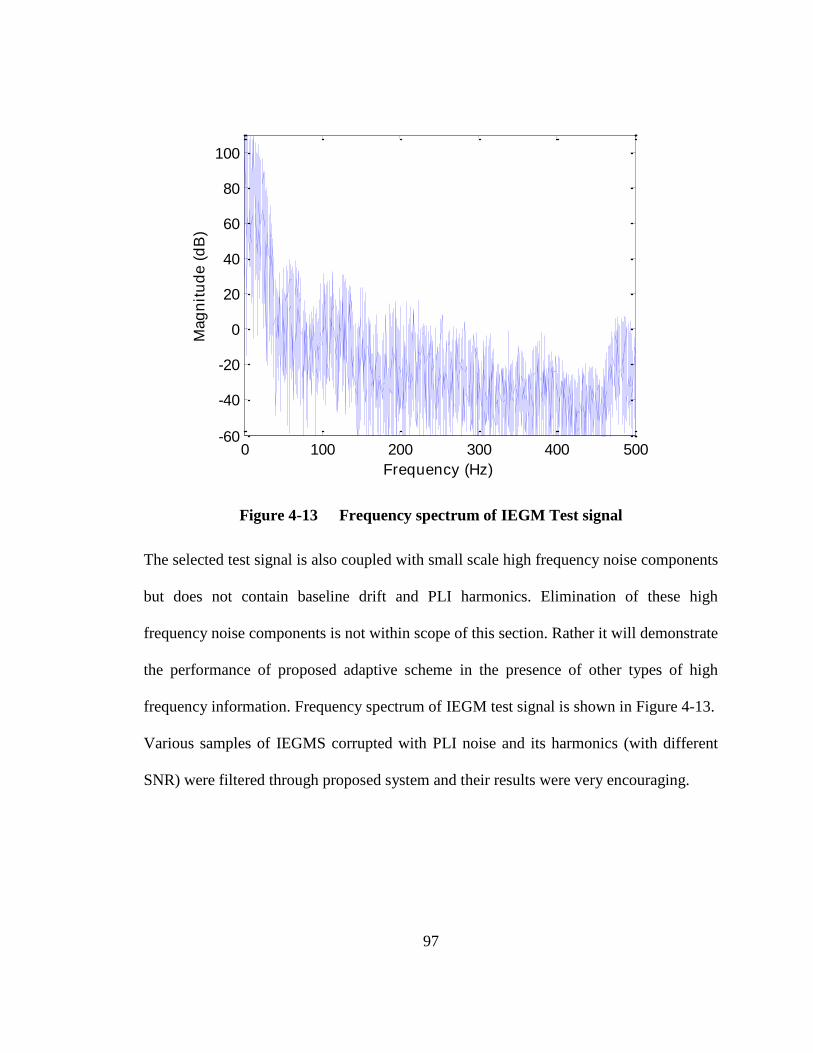
97
0 100 200 300 400 500-60
-40
-20
0
20
40
60
80
100
Frequency Spectrum of HRECG Test Signal
Frequency (Hz)
Mag
nit
ud
e (
dB
)
Figure 4-13 Frequency spectrum of IEGM Test signal
The selected test signal is also coupled with small scale high frequency noise components
but does not contain baseline drift and PLI harmonics. Elimination of these high
frequency noise components is not within scope of this section. Rather it will demonstrate
the performance of proposed adaptive scheme in the presence of other types of high
frequency information. Frequency spectrum of IEGM test signal is shown in Figure 4-13.
Various samples of IEGMS corrupted with PLI noise and its harmonics (with different
SNR) were filtered through proposed system and their results were very encouraging.

98
0 5 10 15 20 25 30 35 40 45
-0.1
-0.05
0
0.05
0.1
0.15
PLI Harmonic Components and Composite Signal
Time (mil iseconds)
No
rmali
zed
Am
pli
tud
e
1st Harmonic
3rd Harmonic
5th Harmonic
Composite PLI
Figure 4-14 The scale of 1st, 3
rd, and 5
th Harmonics of PLI in composite test signal
For a case study, PLI noise having fundamental frequency L
f = 50.38 Hz and its odd
harmonics is formulated with following proportion.
1 1 1sin 3 5
10 50 100sin sin
PLIx (4-28)
where L s= 2 f / f and 2sf KHz .
Relative amplitudes of 1st, 3
rd, and 5
th harmonics of PLI and resulting composite PLI
signal PLIx are shown in Figure 4-14.

99
0 0.5 1 1.5
-1
-0.5
0
0.5
1Corrupted IEGM Signal
Time (seconds)
No
rmali
zed
Am
pli
tud
e
Figure 4-15 PLI corrupted IEGM signal
0 100 200 300 400 500
-50
0
50
100
Frequency Spectrum of Simulated IEGM
Frequency (Hz)
Mag
nit
ud
e (
dB
)
Figure 4-16 Frequency spectrum of IEGM signal corrupted with 1st, 3
rd, and 5
th
harmonics of PLI.
The composite PLI is mixed with pure IEGM signal to construct a PLI corrupted IEGM
signal as defined in (1) and its SNR value is 7.46 dB (decibels). The corrupted IEGM
signal is shown in Figure 4-15. The frequency spectrum of corrupted IEGM signal is
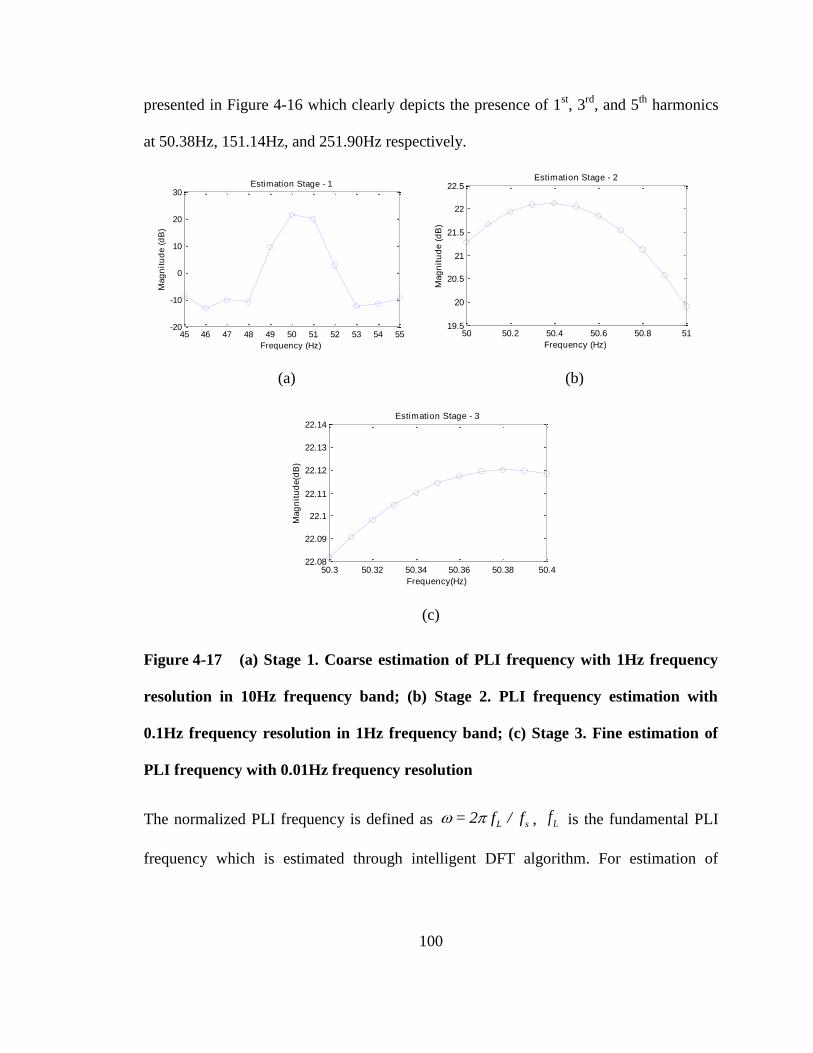
100
presented in Figure 4-16 which clearly depicts the presence of 1st, 3
rd, and 5
th harmonics
at 50.38Hz, 151.14Hz, and 251.90Hz respectively.
45 46 47 48 49 50 51 52 53 54 55-20
-10
0
10
20
30
Frequency (Hz)
Mag
nit
ud
e (
dB
)
Estimation Stage - 1
50 50.2 50.4 50.6 50.8 51
19.5
20
20.5
21
21.5
22
22.5
Frequency (Hz)
Mag
nit
ud
e (
dB
)
Estimation Stage - 2
(a) (b)
50.3 50.32 50.34 50.36 50.38 50.422.08
22.09
22.1
22.11
22.12
22.13
22.14
Frequency(Hz)
Mag
nit
ud
e(d
B)
Estimation Stage - 3
(c)
Figure 4-17 (a) Stage 1. Coarse estimation of PLI frequency with 1Hz frequency
resolution in 10Hz frequency band; (b) Stage 2. PLI frequency estimation with
0.1Hz frequency resolution in 1Hz frequency band; (c) Stage 3. Fine estimation of
PLI frequency with 0.01Hz frequency resolution
The normalized PLI frequency is defined as L s= 2 f / f , Lf is the fundamental PLI
frequency which is estimated through intelligent DFT algorithm. For estimation of

101
fundamental frequency of PLI, window size of 500 samples is selected and Hanning
windowing is applied to reduce spectral leakage.
0 1 2 3 4 5 6 7 8 950
50.1
50.2
50.3
50.4
50.5
50.6
50.7
50.8
50.9
51
Time (seconds)
Fre
qu
en
cy (
Hz)
Online Frequency Estimation
Actual fundamental frequency of PLI
Frequency estimation by intell igent DFT
Figure 4-18 Frequency estimation through proposed scheme. Maximum frequency
deviation remains within ±0.02 Hz of actual frequency.
Intelligent DFT algorithm is implemented with selection of 10 frequency bins ( ) in each
stage and starting with frequency band ( )f of 45-55Hz, we achieve frequency resolution
( )df of 0.01Hz in three stages. Results of first three stages are shown in Figure 4-17.
Estimation of fundamental frequency of PLI through intelligent DFT is shown in Figure
4-18. The frequency is estimated in range of 50.36 ~ 50.40 Hz against actual frequency of
50.38Hz and the maximum deviation from actual frequency remains within ±0.02 Hz.

102
For initialization of SSRLS adaptive filter, delayed recursion technique is
selected. SSRLS is a recursive filter, therefore we need to start with arbitrary values of
certain parameters which include , λ , ˆ[0]x and [0] . Initial values of these
parameters are set as λ =0.95, 0.1= rad/sample, ˆ[0] [0 0 0 0 0 0]T
x , and
[0] 0.1T
CI C which is equivalent as
1.1 0 1 0 1 0
0 0.1 0 0 0 0
1 0 1.1 0 1 0
0 0 0 0.1 0 0
1 0 1 0 1.1 0
0 0 0 0 0 0.1
[0]
Initial observer gain [0]K is determined by [0] . Tracking of composite PLI signal by
SSRLS filter during initialization period is shown in Figure 4-19. After the initial period,
the SSRLS is tuned with correct value of estimated by intelligent DFT and the state
transition matrix is modified. Simultaneously value of λ is also raised to 0.99 to enhance
tracking performance. Filtration error calculated as the difference between clean IEGM
signal and Filtered IEGM signal is shown in Figure 4-20, which is negligible after
initialization period.

103
0.15 0.2 0.25 0.3 0.35 0.4 0.45 0.5
-0.4
-0.2
0
0.2
0.4
0.6
Time (seconds)
No
rmali
zed
Am
pli
tud
e
PLI tracking during initial ization
Actual PLI component
PLI tracked by SSRLS
IEGM signal without PLI
Figure 4-19 Tracking of SSRLS adaptive filter during initialization period
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1 1.1 1.2
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
0.4
0.5
0.6
Time (seconds)
No
rmali
zed
Am
pli
tud
e
Fi l tered IEGM Signal
Fil tered IEGM Signal
Error
Initial ization Period
Figure 4-20 Filtered IEGM signal after initialization

104
50 100 150 200 250 300-50
0
50
100
Frequency (Hz)
Ma
gn
itu
de
(d
B)
Frequency Spectrum of tracked signal
Frequency spectrum of tracked signal
Frequency spectrum of corrupted HRECG
(a)
50 100 150 200 250 300-50
0
50
100
Frequency (Hz)
Ma
gn
itu
de
(d
B)
Frequency Spectrum of Filtered Signal
Frequency spectrum of filter output
Frequency spectrum of clean signal
(b)
Figure 4-21 (a) Frequency spectrum of tracked signal. (b) Frequency spectrum of
filtered IEGM signal with comparison to a clean IEGM signal.

105
0 2 4 6 8 10
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
0.4
0.6
0.8
1Corrupted IEGM Signal
Time (seconds)
No
rmali
zed
Am
pli
tud
e
Figure 4-22 Raw IEGM signal corrupted with PLI harmonics and other noises.
0 100 200 300 400 500
-50
0
50
100
Frequency Spectrum of Raw HRECG
Frequency (Hz)
Ma
gn
itu
de
(d
B)
Figure 4-23 Frequency spectrum of raw IEGM signal showing presence of 1st, 3
rd,
5th
, 7th
and 9th
harmonics of PLI.

106
0 100 200 300 400 500-100
-50
0
50
100
Frequency Spectrum of Filtered HRECG
Frequency (Hz)
Ma
gn
itu
de
(d
B)
Figure 4-24 Frequency spectrum of filtered IEGM, only 1st, 3
rd and 5
th harmonics
are eliminated.
The frequency spectrum of PLI tracking signal is shown in Figure 4-21 (a) which reflects
precise tracking of 1st, 3
rd, and 5
th harmonics of PLI by proposed system. The frequency
spectrum of 10,000 samples (5 sec) of filtered IEGM signal is shown in Figure 4-21 (b)
which shows complete elimination of 1st, 3
rd, and 5
th harmonics of PLI frequency.
To ascertain the functioning of proposed filter in real situation, IEGM signals which
contains PLI harmonics were also tested and output performance was same as was
observed with simulated test signal. A case of 10 seconds segment of IEGM signal
corrupted with PLI along with its harmonics and other noises is shown in Figure 4-22.
The frequency spectrum of corrupted signal is shown in Figure 4-23 which clearly
depicts the presence of PLI and its harmonics. Since the scope of this section is limited to
elimination of 1st, 3
rd, and 5
th harmonics of PLI only, the filtration of harmonic

107
components of PLI above 300 Hz and other noises are not handled during testing. The
frequency spectrum of filtered IEGM signal is shown in Figure 4-24. It can be observed
that 1st, 3
rd, and 5
th harmonics of PLI are completely eliminated whereas higher harmonic
components are still present. All frequency components above 300 Hz including PLI
harmonics can be filtered out through low pass filter in another stage.
4.2.8 Performance Analysis
Performance of proposed filter is compared with the notch filter. For our case study we
need three cascaded 2nd
order IIR notch filters for elimination of 1st, 3
rd, and 5
th
harmonics of PLI. First of all, it is assumed that PLI frequency is known and remains
fixed at 50.38 Hz. Therefore notch filters are tuned at Lf (50.38 Hz), 3x
Lf (151.14 Hz),
and 5xLf (251.90 Hz) to eliminate 1
st, 3
rd, and 5
th harmonic of PLI respectively. The
quality factor of these notch filters is taken as 100 for better characteristics. The clean
IEGM signal, corrupted IEGM signal, the output of notch filter and the output of
proposed filter are presented in Figure 4-25. It is evident that transition period of notch
filter is much greater than of the SSRLS adaptive filter.
Having the input SNR level of 7.46 dB, the output of proposed system achieves SNR
level of 31.46 dB whereas output of notch filter has the SNR level of 18.55 dB. The
performances of both filters were checked at various SNRs and difference in the output
SNRs of both filters was akin. For a case of high SNR where input SNR is 27.46 dB,
output SNRs of proposed system and notch filter are 49.72 dB and 37.73 dB respectively.
Similarly, for a case of low SNR where input SNR is 1.434 dB, the output of proposed
system and notch filter have SNRs 24.56 dB and 12.75 dB respectively.

108
-1
-0.5
0
0.5
1
No
rmali
zed
Am
pli
tud
e
0.5 1 1.5 2 2.5 3 3.5 4 4.5-1
-0.5
0
0.5
1
Time (seconds)
-1
-0.5
0
0.5
1Filtration comparison
Clean IEGM
-1
-0.5
0
0.5
1
PLI corrupted signal
SSRLS fi l ter output
Notch fi l ter output
Figure 4-25 Filtration quality of SSRLS adaptive filter and notch filter.
Let us now compare the performance of both the filters when there is a step change in
amplitude of PLI. The effect of step change in amplitude of PLI is produced by abruptly
increasing the amplitudes of 1st, 3
rd, and 5
th harmonics of PLI then it is mixed with pure
IEGM. The results of step change in PLI amplitude are shown in Figure 4-26 which
shows that SSRLS filter quickly adapt to track changes in amplitude and thus filter it out

109
from IEGM where as notch filter combination is unable to handle it fast and IEGM signal
remains corrupted for long duration. With this configuration, the SNR level of input
signal is 2.52 dB and the output of proposed system achieves SNR level of 27.81 dB
whereas output of notch filter has the SNR level of 17.07 dB.
-1
-0.5
0
0.5
1Filtration comparison
Clean IEGM
-1
-0.5
0
0.5
1
PLI corrupted signal
-1
-0.5
0
0.5
1
No
rmali
zed
Am
pli
tud
e
SSRLS fi l ter output
0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 5.5-1
-0.5
0
0.5
1
Time (seconds)
Notch fi l ter output
Step Change
Figure 4-26 The filtered outputs of proposed system and notch filters with step
change in amplitude of PLI disturbances.

110
-0.5
0
0.5
1Filtration comparison
Clean IEGM
-0.5
0
0.5
1
PLI corrupted signal
-0.5
0
0.5
1
No
rmali
zed
Am
pli
tud
e
SSRLS fi l ter output
0.5 1 1.5 2 2.5 3 3.5 4 4.5-1
-0.5
0
0.5
1
Time (seconds)
Notch fi l ter output
Figure 4-27 The filtered outputs of proposed system and notch filter with ramp
change in amplitude of PLI disturbances.
To observe ongoing continuous change in amplitude of PLI, effect of ramp
increase in amplitude of composite PLI signal is produced and results are presented in
Figure 4-27. In this case, the SNR level of input signal is 3.13 dB and the output of

111
proposed system achieves SNR level of 37.56 dB whereas output of notch filter has the
SNR level of 22.48 dB. The zoomed-in view of filtered outputs of SSRLS adaptive filter
and notch filter are presented in Figure 4-28. Note the variations in clean IEGM signal
are because of presence of high frequency components. Regardless of changing
amplitude of PLI, the output of proposed system matches with the minor variations of
pure IEGM signal whereas notch filter exhibits greater error.
5.08 5.1 5.12 5.14 5.16 5.18-0.06
-0.04
-0.02
0
0.02
0.04
0.06
0.08
Time (seconds)
No
rmali
zed
Am
pli
tud
e
Fi l tered Signal Comparison
Clean IEGM signal
SSRLS fi l ter output
Notch fi l ter output
Figure 4-28 The zoomed-in output comparison of proposed system and notch filter
with ramp change in amplitude of PLI disturbances.
Now let us compare the response of both the filters when PLI frequency variation occurs.
For simulation of frequency variation, fundamental frequency of PLI is changed from
50.38Hz to 51.75Hz at 5.3 seconds of IEGM data. The result of intelligent DFT algorithm
applied with 50% sliding window configuration is shown in Figure 4-29.

112
SSRLS adaptive filter is instantly tuned with the updated frequency estimation by
intelligent DFT. For having comparison of notch filter with SSRLS adaptive filter, notch
filter is also run in adaptive manner with continuous update of notch frequencies. The
results of both SSRLS adaptive filter and notch filter are shown in Figure 4-30 and it is
observed that SSRLS adaptive filter swiftly converge to change in frequency whereas
transition time of notch filter is much larger as compared to SSRLS adaptive filter. In this
case the SNR level of input signal is 7.46 dB and the output of proposed system achieves
SNR level of 22.14 dB whereas output of notch filter has the SNR level of 15.95 dB.
0 1 2 3 4 5 6 7 8 9 1049
49.5
50
50.5
51
51.5
52
52.5
53Estimated Frequency
Time (seconds)
Fre
qu
en
cy (
Hz)
Actual fundamental frequency of PLI
Frequency estimated by Sliding window DFT
Initial ization Period
Figure 4-29 Frequency estimation by intelligent DFT with sliding window
configuration
Comparing the results of SSRLS adaptive filter and notch filter, it can be straight way
concluded that performance of SSRLS adaptive filter is much better than the notch filter
combination. However, computational complexity of SSRLS adaptive filter is high as

113
compared to IIR notch filter because of involvement of matrices operation in state space
model therefore execution speed of SSRLS adaptive filter is less as compared to notch
filter.
-0.5
0
0.5
1
Filtration comparison
Clean IEGM
-0.5
0
0.5
1
PLI corrupted signal
-0.5
0
0.5
1
No
rmali
zed
Am
pli
tud
e
SSRLS fi l ter output
0.5 1 1.5 2 2.5 3 3.5 4 4.5-1
-0.5
0
0.5
1
Time (seconds)
Notch fi l ter output
Change in PLI frequency
Figure 4-30 The filtered outputs of proposed system and notch filters with change
in frequency of PLI.
114
The proposed system can be extended to filter 7th
and 9th
harmonics of PLI from
corrupted IEGM signals if we need frequency band is up to 500 Hz.
4.2.9 Summary – PLI Noise Removal
This research section implements a state space based adaptive filter for tracking and
elimination of PLI and its harmonics from IEGM signal. The SSRLS adaptive filter is
used which is recursive in nature. Unlike Kalman filter, SSRLS filter does not require
process/observation noise covariance for accurate tracking of PLI and its harmonics. The
PLI tracking accuracy of proposed filter depends on two parameters only; first is tuning
frequency and the second parameter is forgetting factor, which effects the bandwidth of
the tracking signal. For high selectivity, we can choose a higher value of forgetting factor
but at the same time, the high selectivity can affect the performance if tuning frequency is
not accurate. Power line frequency remains fluctuating therefore continuous update of the
tuning frequency is desired. For estimation of ongoing power line frequency, an
intelligent DFT based system has been incorporated which continuously estimates and
updates the adaptive filter’s tuning frequency. The proposed system does not require any
reference signal for tracking the PLI and its harmonics; it is capable to self adjust its
tuning frequency for highly precise filtration of 1st, 3
rd and 5
th harmonics of PLI. Separate
tracking of all harmonic components enables the proposed system to work well in non-
stationary environment without distorting underlying IEGM signal.
4.3 Base Line Wander
Base line wandering (BLW) is a low frequency noise (0.15 – 0.3 Hz) produced by
respiration, perspiration, body movements or poor electrode contact and distort ECG

115
interpretation [62]. Presence of BLW in ECG imposes problems in identification of
isoelectric line, wrong ST segment analysis, misreading of T peak as R peak, and
merging of P waves in BLW noise. It is normally represented as an additive sinusoidal
component (0.15 - 0.3 Hz) to ECG signal [57]. Many researchers have used AHA
standards and applied high pass digital FIR/IIR filters to remove BLW from ECG [63-
69]. Also a wide range of other BLW removal techniques are available in literature
including Moving Average filters [70-72], Median filter [73, 74], wavelet transform [75-
78], empirical mode decomposition [79] and adaptive filtering [80-83]. Since BLW can
be represented in term of a sinusoidal signal, so the same technique as discussed in
previous section (i.e. removal of PLI) can also be applied successfully for removal of
BLW. The overall scheme does not require reference signal for ECG de-noising.
While dealing with IEGMs, filtration requirement for bipolar signal is from 30-300 Hz
and for unipolar signal is 1-300 Hz [15, 42]; BLW being a low frequency noise (0.15 ~
0.3 Hz), does not distort the IEGM signals. Therefore, removal of BLW has not been
presented in this research work.
4.4 Electromyographic Noise
Electromyographic Noise (EMG) is a broad spectrum, randomized noise, which is
commonly observed in both ECG and IEGM [84, 85]. The EMG noise generally
considered as high frequency noise and its frequency range varies in between 1~10000
Hz and possesses 0.1~10 mV magnitude depending upon rate of movement and strength
of muscle activity [86]. In some literature the lower frequency range of EMG noise has
been taken above 10 Hz [87, 88]. Accuracy of classification algorithms is directly related

116
to the extent of noise removed from these signals. In clinical EPS, suitable selection of
high frequency noise removal technique during preprocessing of IEGMs is vital so that
most of the noise is removed without loss of signal characteristics.
4.4.1 Literature Review - EMG
In clinical EPS, one encounters signal subjected to various types of noise. Since ECG and
IEGMs both represent electrical activity of the heart, filtering techniques applied on the
ECG signals can be adapted and applied to the IEGMs while taking care of the desired
frequency ranges [89]. Noise sources that corrupt the clinical EP signals are similar to
those affecting the ECG signals. EMG noise removal techniques for electrical signals of
the heart range from simple FIR filters to IIR filters, moving average filters to windowing
methods and median filters [63, 90, 91]. Adaptive filtration has also been applied for
removal of EMG noises [92, 93]. Wavelet filters and Savitzky-Golay (S-G) filters have
also been employed for the purpose of noise removal [94-96].
The amplitude of some of IEGM features are very small and while filtration of high
frequency noise, there is chance of losing such features. For high frequency filtration, S-
G filter provides us a suitable choice to be applied on ECG and IEGM signals [94].
4.4.2 Proposed Method
The acquired IEGMs are first processed for removal of PLI distortion as discussed in
previous section thereafter, EMG noise is taken care off. For removal of EMG noise, S-G
filter is proposed [97]. The S-G filter is a type of FIR filter that performs smoothing
operation by using least-square polynomial fitting technique. For pre-processing of
IEGMs, S-G filter is advantageous because it retains the height and width of the

117
waveform peaks and its impulse response is symmetric so frequency response is purely
real [97]. In essence, they perform a least squares fit of the signal in such a way that
computing the fitting polynomial) of degree N at a central point in the data batch is
equivalent to convolving the input with a fixed impulse response. The fitting polynomial
is given as,
0
( )
N
k
k
k
p n a n (4-29)
where k
a are the polynomial coefficients. The luxury of using S-G filters is that the fitting
polynomial depends on the size of the data batch (2M+1) and degree (N) of the
polynomial but is independent of the actual values of input signal. This eliminates the
need for calculating the polynomial for each new data set and the polynomial is
calculated just once at the beginning of the smoothing operation [97].
Figure 4-31 Filtered IEGM signal from proposed method.

118
The proposed method was tested for noise removal from EMG corrupted IEGMs
acquired from AFIC/NIHD databank and results were successful. The S-G filter designed
for smoothing of IEGMs in this approach had M=7 and N=2. Figure 4-31 represents the
input and output of the S-G filter implemented on an IEGM signal. The magnified graph
of the result is presented in Figure 4-32. It shows how S-G filters preserve the height of
the H wave which is most critical in all characteristic features of IEGMs (i.e. A, H and V
waves). The result shows that the filtered output does not contain EMG noise whereas the
H wave is preserved for clear identification.
Figure 4-32 Zoomed view of S-G Filtered IEGM signal shows preservation of ‘H’
feature.

119
4.4.3 Comparison with other Filtering Techniques
The basic requirement of an ideal EMG filter suitable for IEGMs, can be defined as
following.
Size of characteristic waves in term of its peak and width are retained in the data.
The cutoff frequency of EMG filter ( as a low pass filter) must be above 400 Hz to
preserve genuine data content[27].
Taking into account these desired properties, the performance of S-G filter has been
compared with various filters on the same set of IEGMs data. Comparison is given as
following:
Figure 4-33 EMG removal from IEGM through Moving Average filter
4.4.3.1 Moving Average Filter
The moving average (MA) filter is a simple, fast processing, FIR low pass filter which is
commonly used for smoothing of a data array. Seventh order MA filter has been selected

120
for comparison purpose. The result of the filtered signal is shown in Figure 4-33. It shows
that MA filter removes the high frequency noise however, H waves has been
compromised such that the H wave in IEGM signal has been expanded in time which will
produce inaccuracy in temporal relationship of characteristic waves. Hence, MA filter is
not an appropriate option.
Figure 4-34 EMG removal from IEGM through IIR Filter
4.4.3.2 IIR Filter
Unlike FIR filter, an IIR filter has infinite response i.e. its impulse response does not
become exactly zero after passing a certain time. Although IIR filter is computationally
simple because of its lower order in comparison of FIR filter for same specifications of
filter however, on the other hand it also has stability and phase distortion issues. In our
comparison, a Butterworth low pass IIR filter is applied for removal of EMG noise from

121
IEGMs. Results are shown in Figure 4-34 and it shows that ringing effect are generated in
the filtered output where sharps transitions were present and did not perform satisfactory
smoothing.
4.4.3.3 Median Filter
The median filter determines the output value as the median of the data array. The
outcome of the median filter are shown in Figure 4-35 and it shows that it completely
overwhelm the small amplitude H wave, hence it is also not a suitable option as well.
Figure 4-35 EMG removal from IEGM through Median Filter
4.4.4 Summary – EMG noise
Having comparison of S-G filter with other filters, it can be easily concluded that S-G
filter removes the EMG noise and smoothens the IEGMs with minimum distortion in
height and width of characteristic waves as compared to other filtration options.

122
CHAPTER 5
TEMPORAL FEATURES OF INTRACARDIAC SIGNALS
In conventional clinical EPS, the key concept behind arrhythmia detection
algorithms is the temporal relationships of the feature points within the
electrograms under consideration. Classification of arrhythmias based on IEGMs
requires the analysis of the onsets of characteristics waves i.e. Atrial
depolarization wave (A), His bundle depolarization wave (H) and Ventricular
depolarization wave (V). Accuracy of arrhythmia detection depends upon
accurate detection of the feature points.
5.1 Literature Review
After pre-processing, the next phase of arrhythmia detection algorithm is the feature
detection. The automated feature detection and classification of IEGM signals is rarely
found in literature, however one may refer to different techniques applied on ECG signals
for feature detection [98-100]. Feature detection may be based on morphological,
template, statistical, time domain, frequency domain or hybrid technique (i.e.
combination of two or more methods). Morphological/template features are commonly
used in ECG signals [101-105]. The ECG signal is a superimposed signal of multiple AP
happening simultaneously at different locations of the heart whereas the IEGMs represent
mainly the localized AP and the shape of the characteristic waves in IEGMs differs
largely from one patient to another, so morphological analysis on these signals is not a
suitable method. ECG feature-point detection methods extract the P, QRS, and T wave
features. QRS complex detection methods involving slope of the complex, pattern

123
recognition method and pole-zero models with certain modifications may bear fruitful
results in feature detection for IEGMs [106-108]. Envelope detection can be used for the
purpose of feature point detection [100]. Arrhythmia classifiers have been developed
which make use of the properties of the cardiac signals defined in time-domain and
frequency-domain [109]. In clinical EPS, doctors use timing information of the
characteristic A, H and V waves to manually diagnose the disease and that is why time-
domain analysis forms the foundation of this research. This approach uses adaptive
thresholding techniques in combination with envelope detection for the localized
detection of feature points.
5.2 Data Collection
The acquisition of SVT arrhythmia relevant IEGM dataset was a difficult task because
the complete range of gold standard dataset was not available on Physionet or any other
authentic resource. Therefore, the majority of required Patient’s dataset was collected
from AFIC/NIHD Pakistan and few from MIT Physionet database as available [12].
These dataset was verified from expert electrophysiologist for the specific type of
arrhythmias and then it was referred as gold standard for research work.
The AFIC/NIHD dataset was recorded in bipolar configuration through 2-5-2 mm
catheters to avoid far field ventricular activity. It consists of 3 x ECG leads and 9 x
IEGMs bipolar signals as depicted in Figure 5-1. The recorded IEGMs are in the range of
-5mV to +5mV, which are digitized at 2 KHz sampling rate with 16 bits precision.
The MIT dataset was recorded in bipolar configuration from different positions of the
right atrium using 2-5-2 mm catheters sampled at 1000 samples/sec. The MIT dataset
consist of 3 x ECG leads and 5 x IEGMs bipolar signals, as depicted in Figure 5-2.

124
I
AFIC/NIHD Patients Dataset
aVF
V1
HRA
HISD
HISP
CS 9-10
CS 7-8
CS 5-6
CS 3-4
CS 1-2
0 1 2 3 4 5
RVA-D
Time(sec)
Figure 5-1 5 sec segment of AFIC dataset containing 3xECGs and 9xIEGMs

125
II
Physionet Patients Dataset
V1
aVF
CS 1-2
CS 3-4
CS 5-6
CS 7-8
0 1 2 3 4 5
CS 9-10
Time(sec)
Figure 5-2 The MIT dataset containing 3xECGs and 5xIEGMs
5.3 Methodology
Multiple catheters are inserted in the human heart for EP studies. For the scope of this
research, the focus remains mainly on the recordings from three catheters labeled as the
HRA, His and RVA as shown in Figure 5-3. Further, the IEGMs of CS catheter can be
used as reference for locating the side of APs, which has been recommended as future

126
work. While dealing with IEGMs, the A, V and H waves, their temporal relationship and
inter feature intervals helps to differentiate among arrhythmias [18]. The automated
differentiate among various SVT through IEGM signals can be done by marking A, V
and H waves. Out of all IEGM leads, the His lead is the only lead where we can mark all
the three features i.e. A,V and H waves on single lead directly. However, the marking of
H-wave is crucial and difficult as well as need extra caution.
External stimulation/pacing is applied to drive the heart at faster rate so as to observe the
cardiac response under specific protocols. The scheme of temporal features detection
from IEGMs is illustrated in Figure 5-4.
Figure 5-3 Catheters Arrangement for SVT arrhythmia detection
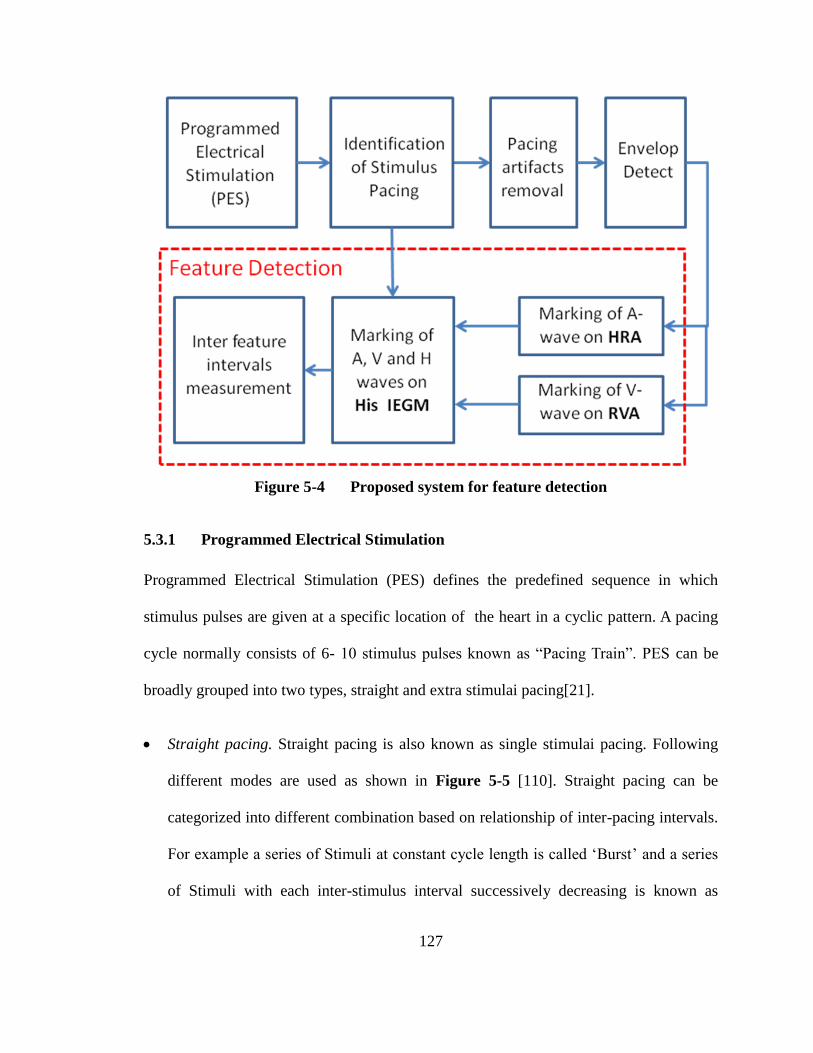
127
Figure 5-4 Proposed system for feature detection
5.3.1 Programmed Electrical Stimulation
Programmed Electrical Stimulation (PES) defines the predefined sequence in which
stimulus pulses are given at a specific location of the heart in a cyclic pattern. A pacing
cycle normally consists of 6- 10 stimulus pulses known as “Pacing Train”. PES can be
broadly grouped into two types, straight and extra stimulai pacing[21].
Straight pacing. Straight pacing is also known as single stimulai pacing. Following
different modes are used as shown in Figure 5-5 [110]. Straight pacing can be
categorized into different combination based on relationship of inter-pacing intervals.
For example a series of Stimuli at constant cycle length is called ‘Burst’ and a series
of Stimuli with each inter-stimulus interval successively decreasing is known as

128
‘Ramp’ as shown in Figure 5-5. In incremental pacing, pacing cycle length of each
Stimuli drive train is shortened by 10-50 msec from previous whereas in decremental
case it is vice versa.
Figure 5-5 Straight Pacing [110].
Extra stimuli pacing. In Extra stimuli pacing, additional pulses (extra stimuli) are
delivered at the end of a drive train [18]. It is useful especially for checking of
refractory period. Figure 5-6 shows a baseline drive of eight beats, which is delivered
at a constant cycle length (S1S1) by a stimulator. Another stimulus (S2) known as
extra stimulus is placed in succession to basic drive however, with reduced inter-
stimuli interval (S1S2); extra stimuli can be single, double or triple which are
designated as S2, S3, and S4, respectively. Generally, the extra stimuli are initiated at
80% to 90% of the drive cycle length. With the addition of each extra pulse, the
intervals are made shorter and shorter.

129
Figure 5-6 Extra Stimuli Pacing [110].
In this chapter, AVNRT and AVRT (reentrant tachycardia) have been focused to be
differentiated through time domain analysis. In reentrant tachycardia, the refractory
periods of dual/accessory pathways in AV conduction system are key factors. For
monitoring of refractory periods, the extra-stimulus (premature) pacing method can be
applied effectively [111]. For identification of AVNRT (typical) tachycardia, the most
suitable option is to apply extra-stimulus pacing through HRA catheter however, pacing
from other catheters can also be used for further confirmation of the APs location [8]. In
this study, extra-stimulus pacing is applied at HRA catheter for evaluation of AVNRT
(typical) with the PES protocol consisting of a basic drive train of eight stimuli (S1) with
pulse width of 2.0ms, followed by single extra-stimulus (S2). The protocol starts at
600/400ms (S1S1/S1S2) inter-stimuli/extra stimulus interval and S1S2 is decreased by
10ms in each subsequent pacing train.

130
5.3.2 Identification of Stimuli Pacing Train
Identification of stimuli pacing is required for four main reasons:
The timing of stimulus pulses are required to be determined,
The protocol of pacing has to be determined,
The pacing artifacts induced in other IEGM leads is required to be removed,
The location of pacing has to be verified as the reference while determining features
in other IEGMs e.g. stimuli in HRA IEGM are required to be used as reference for
identification of ‘A’ in His IEGM.
When pacing is carried out through any of catheter, the stimuli contain maximum
amplitude on a normalized IEGM and pulses can be easily identified and marked by
thresholding method. After identification of first pulse, the successive pulses are looked
within 800ms window from the preceding pulse as straight pacing always start with pulse
to pulse gap normally less than 700ms. The routine extra-stimulus pacing protocol
usually start at 600/400ms (S1S1/S1S2). The gap between first and second stimulus pulse
determines S1. When gap between two successive pulses is less than (S1S1-100ms), the
next pulse is counted as extra stimulus and gap between them is marked as S2. After
marking of 1st extra stimulus, 2
nd extra stimulus is looked within window having span of
(S1S2 - 50ms) and if found, it is marked as S3. For validation of identified stimuli pulse
train, some verification checks are performed e.g. the duration of each identified stimulus
should be less than 5ms to be counted as valid because usual stimulus pulses applied have
1-2ms pulse width (PW). Similarly, if number of detected stimuli in a pulse train is less
than six then it is taken as some artifact and are rejected to be a valid pulse train. The
algorithm for detection of pacing stimulus protocol is shown in Figure 5-7. The algorithm

131
can be extended for detection of further extra stimuli pulses, in the same way as applied
for detection of 1st and 2
nd extra stimulus pulses.
Figure 5-7 Algorithm for detection of PES protocol

132
5.3.3 Pacing Artifact Removal
In EP procedures, pacing is usually carried out through a single IEGM lead, however the
influence of this pulse is seen on other leads which, causes distortion known as pacing
artifacts [111]. Pacing artifacts are observed in all leads, therefore it is necessary to mark
the duration of stimulus and remove pacing artifacts from all leads especially, His IEGM.
For example, if pacing is done through HRA catheter, pacing pulses are marked in HRA
IEGM and pacing artifacts are eliminated successfully in His catheter by introducing a
10ms blanking interval in recorded His IEGM [98].
0 0.5 1 1.5 2
0
0.2
0.4
0.6
0.8
1
Time
Am
pli
tud
e
HisP with pacing arti fact
Pacing Artifact
Figure 5-8 HisP with pacing artifact
The detection of stimulus in HRA catheter is done with thresholding method. The pacing
artifacts are clearly visible in Figure 5-8 and in presence of these pacing artifacts, there is
likely chance of wrong detection of ‘A’ and ‘H’ waves. Therefore, the pacing artifacts are
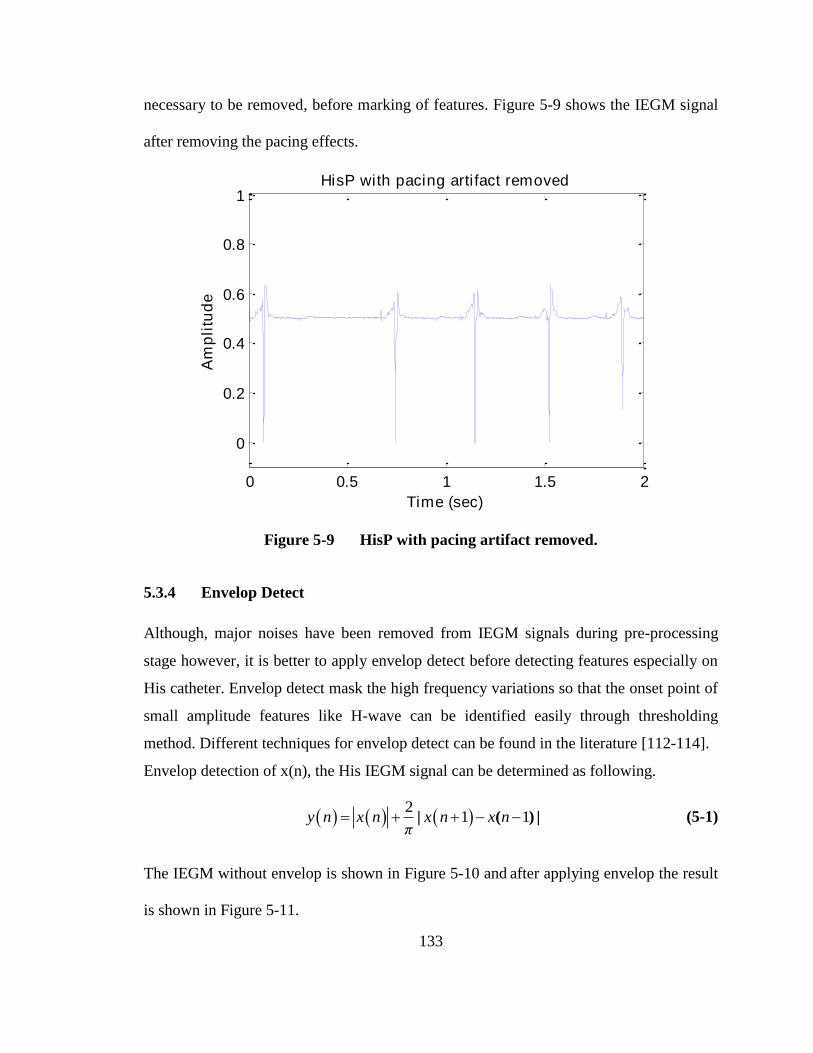
133
necessary to be removed, before marking of features. Figure 5-9 shows the IEGM signal
after removing the pacing effects.
0 0.5 1 1.5 2
0
0.2
0.4
0.6
0.8
1
Time (sec)
Am
pli
tud
e
HisP with pacing arti fact removed
Figure 5-9 HisP with pacing artifact removed.
5.3.4 Envelop Detect
Although, major noises have been removed from IEGM signals during pre-processing
stage however, it is better to apply envelop detect before detecting features especially on
His catheter. Envelop detect mask the high frequency variations so that the onset point of
small amplitude features like H-wave can be identified easily through thresholding
method. Different techniques for envelop detect can be found in the literature [112-114].
Envelop detection of x(n), the His IEGM signal can be determined as following.
2
1 1| ( ) | y n x n x n x nπ
(5-1)
The IEGM without envelop is shown in Figure 5-10 and after applying envelop the result
is shown in Figure 5-11.

134
Figure 5-10 IEGM of His catheter without envelop
Figure 5-11 IEGM of His catheter after applying envelop detect
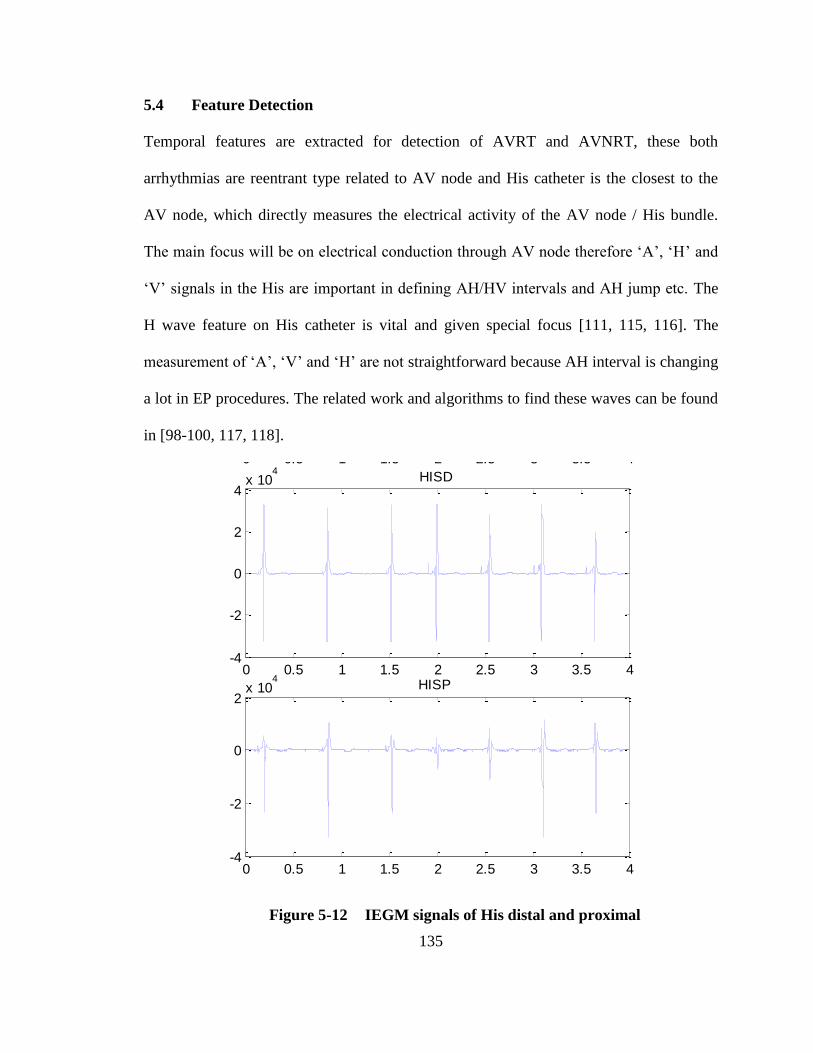
135
5.4 Feature Detection
Temporal features are extracted for detection of AVRT and AVNRT, these both
arrhythmias are reentrant type related to AV node and His catheter is the closest to the
AV node, which directly measures the electrical activity of the AV node / His bundle.
The main focus will be on electrical conduction through AV node therefore ‘A’, ‘H’ and
‘V’ signals in the His are important in defining AH/HV intervals and AH jump etc. The
H wave feature on His catheter is vital and given special focus [111, 115, 116]. The
measurement of ‘A’, ‘V’ and ‘H’ are not straightforward because AH interval is changing
a lot in EP procedures. The related work and algorithms to find these waves can be found
in [98-100, 117, 118].
0 0.5 1 1.5 2 2.5 3 3.5 4-5000
0
5000
10000lead I
0 0.5 1 1.5 2 2.5 3 3.5 4-4
-2
0
2
4x 10
4HISD
0 0.5 1 1.5 2 2.5 3 3.5 4-4
-2
0
2x 10
4HISP
Figure 5-12 IEGM signals of His distal and proximal

136
Figure 5-12, shows the real His_P and His_D IEGM signals. It is evident that HisP and
HisD show clear ‘V’ wave while ‘A’ and ‘H’ are not clearly visible in their waveform at
this scaling because ‘A’ and ‘H’ have very low threshold as compared to ‘V’. For
marking of A, V and H wave on His catheter, first we have to mark the A wave on HRA
catheter and V wave on RVA catheter.
0 0.5 1 1.5 2 2.5 3-0.5
-0.4
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
0.4
0.5
RVA
Time (sec)
No
rmali
zed
Am
pli
tud
e
RVA-D
V-wave
Figure 5-13 Onset of VRVA
5.4.1 “V” on RVA Catheter
Since the amplitude of VRVA (V wave on RVA catheter) is much larger than the actual
baseline, the onset of V wave is easiest to find as following.

137
Peak detection of VRVA. The peak of the V wave is marked on a normalized RVA
IEGM by empirically defined threshold, which is generally selected as 1/3 of
maximum value of RVA IEGM (VRVA-max) [111].
Marking onset of VRVA. The VRVA-on (onset of the VRVA) is searched within a 30ms
window prior to VRVA-max, such that onset is marked when VRVA crosses a threshold of
1/15 of VRVA-max [100, 111, 119]. The results are shown in Figure 5-13.
0 0.5 1 1.5 2 2.5 3 3.5 4-0.5
0
0.5HRA
Time (sec)
No
rmali
zed
Am
pli
tud
e
HRA-P
A(onset)
Figure 5-14 Onset of AHRA
5.4.2 “A” on HRA Catheter
Similarly, AHRA (A wave on HRA) and stimulus pulses dominates the HRA IEGM and
can be marked through thresholding technique as following.

138
Peak detection of AHRA. The AHRA-max (peak of A wave) is located on a normalized
HRA IEGM with reference to threshold level defined as 1/3 of maximum value of
HRA IEGM [111].
Marking onset of AHRA. The AHRA-on (onset of the AHRA) is searched prior to AHRA
within a 30ms window prior from the peak with reference to a threshold of 1/15 of
AHRA-max [100, 111, 119]. The results are shown in Figure 5-14.
5.4.3 “A”, “V” and “H” on His Catheter
Next, locate the onset of characteristic waves on the His catheter. The crucial step is the
measurement of ‘A’, ‘V’ and ‘H’ from the His channel which contains varying in time
pulses in consecutive heart beats and sometimes the thresholds of pulses are very low and
sometimes the pulses are even mixed into each other. His catheter recording contains the
AHis (A wave on His), HHis (H wave on His) and VHis (V wave on His) [120]. In His
channel, it is understood that in between every VV interval two important pulses are
present during a normal conduction system, one is ‘H’ and other is ‘A’. Out of A, H and
V waves, V wave has normally highest amplitude and H wave is smallest feature just
before the onset of V wave. Therefore it is preferred option to first detect ‘V’ on His
IEGM followed by ‘A’ and ‘H’ in sequence under certain criteria.
Once the ‘A’ pulse is detected, the only left item is the ‘H’ wave, which is present
between ‘A’ and ‘V’ waves. The identification of ‘H’ wave is most difficult especially in
presence of noise therefore some extra measures have to be taken for foolproof detection
of ‘H’ wave onset point. For a valid ‘H’ wave, the His catheter must be appropriately

139
placed and IEGM signal should be acquired such that it contains minimum noise.
Following features are marked on preprocessed (including envelop detection) His IEGM.
0 0.5 1 1.5 2-0.5
0
0.5
1RVA
Time (sec)
No
rmali
zed
Am
pli
tud
e
RVA-D
V-wave
0 0.5 1 1.5 2-0.5
0
0.5
1HISD
His-D
V-onset
V-offset
Figure 5-15 Earmarking of VHis-on and VHis-off
Marking VHis. ‘V’ appears first in RVA IEGM and then reflected in HRA IEGM,
therefore, VHis-max (the peak of V-wave on the His catheter) is searched within a
100ms window after VRVA-on [111]. The VHis-on (the onset of the VHis) is searched
within a 30ms window prior from its peak and is marked when VHis crosses a
threshold of 1/15 of VHis-max and the offset of the VHis (VHis-off) is searched after VHis-

140
max, when VHis crosses a threshold of 1/12 of VHis-max [111, 119]. Result is shown in
Figure 5-15.
Marking AHis. After marking of VHis-on, AHis-max (the peak of ‘A’ on the His catheter) is
marked as highest peak within a window starting 40ms after S2 (or AHRA-max) to 40ms
before VHis-on and AHis-on (the onset of the AHis) is marked prior to AHis when it crosses
a threshold of 1/12 of AHis-max [111]. Similarly, AHis-off (the offset of the AHis) is
marked after AHis-max, when AHis crosses a threshold of 1/12 of AHis-max [111].
2.55 2.6 2.65 2.7 2.75 2.8 2.85 2.9
-0.4
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
0.4
HISD
Time (sec)
No
rmali
zed
Am
pli
tud
e
HisD
V-on
V-off
H-on
Figure 5-16 Marking of HHis-on on His IEGM
Marking HHis. Detection of H wave is the most difficult and requires higher-level
precautions to avoid any false detection. The onset of H (HHis-on) is searched in the
window between the AHis-off and VHis-on [100]. First, peak of ‘H’ (HHis-max) is searched
in the window having span from (AHis-off + 50ms) to (VHis-on - 30ms) and HHis-on is

141
marked prior to HHis-max when it crosses a threshold of 1/12 of HHis-max [111]. The
marking of HHis-on is shown in Figure 5-16.
5.4.4 Validation of HHis-on
Since HHis is a small amplitude feature and normal ‘H’ wave is 10-25ms wide [120].
Validation of HHis-on is required to minimize the possibility of false detection. Following
checks are performed for validation of HHis-on.
HV interval. The first check disregards any H wave onset detected too near or too far
from the His on
V
location. HV interval ranges from 35-55ms therefore HHis-on which
correspond to an HV interval outside the range 35–55msec are rejected [27, 120].
Variance of His IEGM. The second check is associated with the variance of the
signal. Here the main idea is same as that used by doctors, i.e. if the recording is too
noisy then proper decisions cannot be made based on that; so that particular recording
is discarded and a new recording has to be acquired. Likewise, we say that if the
signal contains too much noise, then it is very likely that the detected onset point of
the H wave is faulty.
To incorporate this theme into our algorithm, HIS IEGM within the local search
window is divided into n parts. It is assumed that the HHis-on lies in the nth part of this
window and variance of this part is greater than other n-1 parts. If variance of the
region not containing HHis-on is found to be higher than the region detected to contain
HHis-on, then there is possibility of wrong detection. Therefore detection of HHis-on is
rejected for this activation. Feature detection algorithm is summarized in Figure 5-17.

142
Figure 5-17 Feature detection algorithm

143
5.5 Results
Table 5-1 shows the results of the feature detection algorithm. The algorithm developed
was tested against database of 20 patients collected from EP lab of AFIC/NIHD Pakistan.
The data contained more than 4500 useful activations. The percentage accuracy of V, A
and H waves found to be 95.06%, 89.93% and 98.33% respectively.
Table 5-1 Result of Feature Detection Algorithm
Feature
Points
Total
Activations
Correct
Detections
Wrong
Detections
Missed
Detections
Accuracy
(%)
A Wave 1230 1202 0 28 97.72
H Wave 1192 1148 8 36 96.31
V Wave 2156 2149 0 7 99.63
4578 4499 8 71 98.27
5.6 Summary
For automated arrhythmia detection during an EP study, the most important aspect is
accurate marking of ‘A’, ‘V’ and ‘H’ features on different IEGMs. These features have
different widths and amplitudes on different catheters. For accuracy of inter feature time
intervals, the selection onset of features is the best criteria. Moreover, the ‘H’ feature is
most sensitive to be identified because of its minute amplitude. In this chapter, the
method for marking of onset points of all features has been defined and to ensure
validation of ‘H’ feature, special checks are introduced to prevent false detection.

144
CHAPTER 6
IDENTIFICATION OF REENTRANT TACHYCARDIA
In this chapter, reentrant tachycardia, which include AVRT and AVNRT, are
analyzed using IEGM signals in time domain. For analyzing reentrant
tachycardia, extra stimuli pacing of heart is done under a specific protocol and
heart is enforced to enter in tachycardia state. The foremost requirement is the
IEGM feature detection and then determine the time gaps between different
features. Based on the outcomes of the induced tachycardia, the type of
arrhythmia can be verified. The feature detection has been covered in previous
chapter and those features and their time intervals are analyzed to differentiate
AVNRT and AVRT arrhythmia. The sequence of this chapter is as follow, first of
all different steps involved for EP evaluation are discussed, key features detection
method defined, proposed algorithms for classification of AVRT/AVNRT are
presented and then results of proposed method are discussed.
6.1 Literature Review
Automated arrhythmia detection algorithms have been developed extensively for surface
electrocardiograms (ECG) [121, 122]. The existing literature also includes algorithms
based on IEGMs developed for usage in Implantable Cardioverter Defibrillators (ICD)
[123]. However, programming routines specifically meant for clinical EPS are very
limited.
Among several types of tachycardia and bradycardia, the most common arrhythmia faced
by electrophysiologist is AVNRT. It is a type of reentry tachycardia which occurs due to

145
problem in Atrio-ventricular (AV) node in which 2 pathways exist instead of normal
single fast pathway which creates a loop and initiates tachycardia [15, 27]. The AVNRT
has conventionally divided into two types named as typical AVNRT (slow-fast) and
atypical AVNRT (fast slow) however majority cases (80-90%) belongs to typical
AVNRT and that’s why typical AVNRT has been focused in this work [124-126]. For
differentiation of AVNRT, no unanimously accepted method has been adopted [124].
Electrophysiologists apply various protocols for identification of AVNRT during an EP
study [127-129]. For AVNRT, one of criteria most commonly used is to observe AH
jump [126-128].
AVRT is considered as second most common type of reentrant tachycardia [23]. The
AVRT are of two types named as Orthodromic (typical) AVRT and Antidromic
(atypical) AVRT. Differentiation maneuvers between orthodromic and antidromic AVRT
have been defined well by K. Tanka et. al [130]. For initiation and persistence of AVRT,
the presence of APs between atria and ventricle is a compulsory criteria [131]. During
AVRT, the atria and ventricles contract sequentially and the parameters used to
distinguish AVRT from other tachycardias can be found in [18, 20, 27]. For AVRT case,
one criteria is that the A-V interval must be greater than V-A interval and second criteria
is that V-A interval must be greater than 35-65ms for a diagnosis in favour of AVRT [20,
118].
6.2 Dataset
20xPatient’s dataset has been collected from AFIC/NIHD Pakistan and MIT Physionet
database [12]. AFIC/NIHD dataset includes the verified cases of both AVRT and
AVNRT. The dataset contains IEGMs recorded from 2-5-2 mm quadripolar HRA, RVA

146
& His catheters and 2-5-2 mm decapolar CS catheter. For identification of AVRT and
AVNRT, primarily the data from HRA, RVA and His IEGMs are used; however, the CS
IEGM can be used in secondary stage to confirm the location of APs. The recorded
IEGMs are in the range of -5mV to +5mV, which are digitized at sampling rate of 2K
with 16 bit precision.
6.3 Methodology
Proposed methodology comprises multiple stages as shown in Figure 6-1 to detect
AVNRT/AVRT arrhythmia from pre-processed IEGM signal during EP study. The
description of these steps is as following.
Figure 6-1 Proposed methodology for detection of AVNRT/AVRT

147
6.3.1 Extra Stimuli Pacing
For identification of typical AVNRT, the extra-stimulai pacing in anti-grade mode at
HRA catheter have been used and ‘A’, ‘H’ and ‘V’ are marked on His IEGM as shown in
Figure 6-2. The pacing protocol starts with an S1S1 interval of 600ms and an S1S2 (extra
stimulus gap) is at least 60ms higher than the documented wenckebach interval. It is very
common to start at 600/400ms (S1S1/S1S2). If the patient heart rate is above 100bpm
(100bpm = 600ms), you will need to start at a faster cycle length for S1. Once stimulation
has begun, the S1S2 interval is gradually decreased by 10-20ms for each new pacing
train. The process is continued until the presence of AVNRT tachycardia is either verified
or ruled out.
Figure 6-2 Extra stimulus pacing at HRA and marking of A, H and V waves on
His catheter [120].
6.3.2 Atrial/Ventricle Activation Rate/Regularity
Depolarization/activation rate of both atria and ventricle is important to decide the type of
arrhythmia. Moreover, it is also important to observe that activation rate of both atria and
ventricle is same or different. For example, in AVNRT/AVRT, the A:V conduction is

148
usually 1:1 and in case of variations, the possibility of AVNRT/AVRT is declined.
Regularity of tachycardia is required to be checked. As in ECG signal, the R-R interval
determines beat-to-beat regularity, similarly in IEGM, the A-A interval extracted from
HRA and the V-V interval extracted from the RVA can be used to confirm regularity of
the rhythm.
6.3.3 Inter Feature Time Duration
The time intervals between A, V and H fudicial points are important features to be used
for detection of many arrhythmias as shown in Figure 6-3. AH interval measurement on
His catheter provides time gap between atrial wave appeared at inter-atrial tissues to first
depolarization at His bundle. The AH interval (equivalent to PR interval observed on
ECG) defines the propagation delay occurred at AV node and normal range of AH
interval is 60-125ms [120]. HV interval gives us the time gap of passing wave front from
bundle of His to Purkinje fibers. AH intervals (AHis-on to HHis-on) and HV intervals (HHis-on
to VHis-on) are measured and count as a feature for decision of arrhythmia classification.
AA or A1-A2 interval (time gap between AHis-on of 1st activation to AHis-on of 2
nd
activation) and HH or H1-H2 interval (time gap between HHis-on of 1st activation to HHis-on
of 2nd
activation) also counts as features.
6.3.4 Special Characteristic Verification
Once the electrophysiologist identify an arrhythmia then some special characteristic
related to that arrhythmia is verified/located. For AVNRT, AH interval provide us
information of AH jump. AA and VV interval tell us about atrial and ventricle rate
regularity as well as AV block. Also for the case of AVNRT, the measurement of VA

149
interval and AH/HA ratio facilitates us to differentiated between typical and atypical
AVNRT. For AVRT case, one criteria is that the A-V interval must be greater than V-A
interval [20, 118]. For the case of AVRT, the location of APs can also be verified with
the help of timings sequence in different IEGMs.
Figure 6-3 Importance/correlation of electric activity in different electrodes [18].

150
Figure 6-4 Interval measurements [18].
6.4 Identification of AVNRT
In AVNRT, two pathways exist in or around AV node, out of which one is faster as
compared to other. Typical AVNRT is characterized by regular rhythm, 1:1 atrial to
ventricle activation ratio and narrow QRS (QRS < 120ms) in ECG [125, 132, 133]. In
typical AVNRT, VA interval is lesser than 60ms and vice versa for atypical AVNRT
[134, 135]. AH/HA ratio of a typical AVNRT must be greater than unity [124]. AH jump

151
is the key feature which is used to classify AVNRT [136]. AH interval is the time
difference between AHis(On) and H His(On) and is measured for all the beats on His IEGM.
AH jump is basically an increase of time measurement between two successive AH
intervals when HRA catheter is stimulated with extra-stimulus technique in which each
time S1S2 interval is reduced gradually by 10–20ms. The effect of extra stimulus pulse
reflects on the ‘H’ wave in same proportion. There comes a stage when the AH interval
does not appear to be in proportion to extra stimulus rather it becomes significantly larger
than its previous one indicating the AH jump because of the reason that fast pathway has
become refractory and pulse is being passed though slow path as shown in Figure 6-5.
Figure 6-5 Slow-fast AVNRT and observation during EP study [125].

152
(a)
(b)
http://www.theeplab.com/B-The-Members-Center/F000-Cardiac-Arrhythmias/G-AVNRT/FG00-AVNRT.php
Figure 6-6 Presence of AH jump with extra stimulus pacing protocol change over
from (a) 600/300ms to (b) 600/290ms.

153
The AH interval is counted as valid AH jump if AH interval is increased by 50ms or
more with a 10ms (or 20ms) decrement in S1S2 interval. Figure 6-6 demonstrate the AH
jump, an extra stimulus pacing 600/300 is applied in Figure 6-6(a) which gives 146ms
AH interval. However in the next series of pacing when S1S2 has been decreased by
10ms i.e. with 600/290ms extra stimulus pacing protocol, we notice that AH interval
becomes 211ms which means 65ms (211-146) AH jump is achieved and AVNRT is
verified.
2.2 2.4 2.6 2.8 3 3.2 3.4
0.2
0.4
0.6
0.8
1
Time (sec)
Am
pli
tud
e
His with A, V and H measured
His
H
A
AH Jump
Figure 6-7 AH jump is clearly visible at third instance of the figure. In first two
instances, the AH interval is normal whereas at 3rd
instance AH interval is large
AH jump is clearly visible in simulation result as shown in Figure 6-7. The AH intervals
are drawn separately in Figure 6-8. This figure shows the presence of the AH jump at
instance #38. A simple classifier is used to check if AH jump is greater than 50ms or not.

154
33 34 35 36 37 38 390
100
200
AH
in
terv
al
(ms)
AH Interval Measurement
33 34 35 36 37 38 39-100
-50
0
50
100
150
Instance Number
A2H
2 -
A1H
1 (
ms)
AH Jump
AH Jump
Figure 6-8 AH Interval and AH Jump measurement
6.5 Identification of AVRT
In AVRT, an APs exists between atria and ventricle in addition to AV node. The
direction of electric pulse through APs can be antidromic (atypical) or orthodromic
(typical) based on which AVRT are further categorized as shown in Figure 6-9. Typical
AVRT is most common between two types. AVRT is usually verified through
constant/decremental retrograde pacing through RVA catheter and Antegrade pacing at
HRA catheter as shown in Figure 6-9 [137-139]. Typical AVRT is characterized by
regular rhythm, 1:1 atrial to ventricle activation ratio and narrow QRS (VA/AV < 1) in
ECG [132, 133]. Some additional criteria define that the VA interval in case of typical
AVRT should be greater than 60ms but must be lesser than AV interval [124, 126]. The
location of APs can be determined by monitoring the earliest reentrant activation

155
appearance at different locations of catheter. For the case of AVRT, following three
criteria can be defined
Right sided APs. If the earliest reentrant activation appears in the HRA catheter
Left sided APs. If the earliest reentrant activation appears in the CS catheter.
Septal (center) APs. If the earliest reentrant activation appears in the His catheter
(a) (b)
(c)
Figure 6-9 (a) Orthodromic AVRT (b) Antidromic AVRT (c) Antegrade versus
retrograde pacing for AVRT verification [137].

156
Figure 6-10 Reentrant arrhythmia detection algorithm
6.6 Classification Algorithm between AVRT and AVNRT
The proposed algorithm uses the basic features 'V’, ‘A’ and ‘H’ waves and determines
AVRT and AVNRT specific features i.e. AH jump, A-V interval and V-A intervals etc.
AH jump is the key feature to classify AVNRT and AV & VA intervals are key features
related AVRT. The structure of the algorithm is shown in Figure 6-10. Table 6-1 shows
the result of arrhythmia detection.

157
Table 6-1 Result of Arrhythmia Detection
Dataset of
Verified
Arrhythmia
Arrhythmia AVRT AVNRT
NSR & Misc
SVT
(except AV
node
reentrant)
Total events
No of Events 436 559 1133 2128
Arrhythmia
Detection
Result
AVRT 408 4 4 416
AVNRT 7 542 3 552
NSR & Misc
SVT
(except
reentrant)
9 5 1121 1135
Discarded
Events
12 8 5 25
The confusion matrix is defined as under to determine sensitivity, specificity, positive
prediction value (PPV) and negative prediction value (NPV) of an arrhythmia [140].
Gold-standard
arrhythmia present
Gold-standard
arrhythmia absent
Detection
positive True Positive (TP) False Positive (FP)
TP
TP FPPPV
Detection
negative False Negative (FN) True Negative (TN)
TN
TN FNNPV
TP
TP FNSensitivity
TN
TN FPSpecificity
Confusion matrices and determined sensitivity, specificity and PPV against AVRT and
AVNRT are as under.

158
AVRT AVRT arrhythmia Non-AVRT arrhythmia
AVRT
detected 408 8
PPV=
98.08%
AVRT not
detected 28 1684
NPV=
98.36%
Sensitivity=
93.58%
Specificity=
99.53%
AVNRT AVNRT arrhythmia Non-AVNRT
arrhythmia
AVNRT
detected 542 10
PPV=
98.19%
AVNRT not
detected 17 1157
NPV=
98.55%
Sensitivity=
96.96%
Specificity=
99.14%
Table 6-2 shows the accuracy of the proposed system in term of sensitivity, specificity
and PPV and NPV.
Table 6-2 Sensitivity, Specificity, PPV and NPV Results
Cardiac
arrhythmia
Sensitivity (%) Specificity (%) PPV (%) NPV (%)
AVRT 93.58 99.53 98.08 98.36
AVNRT 96.96 99.14 98.19 98.55

159
The results show that performance of the proposed algorithm for arrhythmia detection in
clinical EPS is comparable to manual diagnostic procedures.
6.7 Summary
Real patient data having AVNRT and AVRT events have been acquired from
AFIC/NIHD and events are verified by cardiologist to be used as gold standard for
checking accuracy of proposed work. An algorithm is presented for detection of AVNRT
and AVRT using IEGM features during an EP study. The proposed algorithm performs
well and gives sensitivity 96.96% for AVNRT and 93.58% for AVRT. The specificity
remained 99.14% for AVNRT and 99.53% for AVRT. The main significance to develop
this system is to reduce the time required by electrophysiologist for manual calculations
to find the different features and their time intervals for detection of AVNRT and AVRT
arrhythmias.

160
CHAPTER 7
FREQUENCY DOMAIN ANALYSIS FOR IDENTIFICATION OF
ATRIAL TACHYCARDIAS
Cardiac Electrophysiology (EP) encompasses study of the IEGM to analyze
different types of arrhythmias. Arrhythmias are investigated by pacing the heart
under a specific protocol and studying the response in return. The IEGM are
studied by the Electro physiologist visually (using the monitor screens), which is
time consuming and highly dependent on individual expertise. However, it has
also been observed that during an EP stimulation process, a patient may develop
Atrial Fibrillation (AF). In order to proceed further with the diagnosis /automated
detection of an arrhythmia, the patient has to be taken out of AF. Although
Electro physiologist, based on their expertise can identify AF by visual
monitoring of atrial IEGM, a need was felt for real time automated detection of
AF as well as its differentiation from AFL, AT and NSR.
To fulfill the requirement, a system (algorithm) is required to be designed with
consideration of following basic decisions.
The selection of time/statistical/frequency domain for the desired system.
The base of differentiation among NSR, AT, AFL and AF
Pre-processing requirement for extraction of atrial activity.
Suitable Location of IEGM catheter for monitoring of AF activity.
Baseline frequency range selection of atrial activations of NSR, AT, AFL and
AF.

161
PSD estimation response against activations of NSR, AT, AFL and AF.
Suitability of conventional PSD features (DF, RI, etc) for desired task.
Considering all above design parameters, frequency domain has been selected for
differentiation of atrial IEGMs in this work. Dominant frequency (DF) is estimated
using Welch method to find out atrial activation rate during NSR, AT, AFL and AF. A
new spectral parameter, Average Power Spectral Ratio (APSR), has been identified
for ensuring reliability of DF for AF detection as well as differentiation of AF from
other atrial arrhythmias. The proposed algorithm successfully detects and
differentiates between NSR, AT, AFL and AF with an accuracy of 99.53 %..
7.1 Literature Review
The atrial rate can be used for detection of AF as well as its differentiation from other
arrhythmias. Atrial rate for NSR normally ranges from 60- 100 bpm (beat per minute).
For AT, atrial rate has the range from 100- 240 bpm, however, in AFL the heart beats
goes up to 300 bpm [34]. During AF, the atrial rate can go beyond 300 bpms [36]. Atrial
rate calculation in time domain for NSR, AT, and AFL, being regular and periodic
signals is quite simple. However automated detection of AF, being an irregular signal
involves application of frequency/ time frequency/ statistical domain techniques [141-
151].
Using spectral estimation technique, Jason Ng et al and Rakesh et al have explained the
concept of DF to estimate the atrial activation rate [152, 153]. The DF is defined as the
frequency containing maximum power in frequency domain; Vassil et al. has indicated
that “it can be easily applied to estimate the local atrial activation rate in AF” [154]. This

162
concept has been employed in this section to find atrial activation rate for detection and
differentiation between NSR, AT, AFL and AF.
For periodic activations, like NSR, AT, and AFL, DF gives the robust estimation of
activation rate however, for irregular activation like AF, the estimation may not be as
robust. Therefore, DF analysis for AF is built upon selection of the lowest-noise signal.
An index, known as Regularity index (RI), has been frequently used to ensure the
reliability of DF [155-160]. Mostly, DF with RI > 0.2 has been considered reliable for AF
detection and its further analysis [157-160]. Millet J et al. used a set of 8 x spectral
parameters for differentiation of NSR, AFL and AF [150]. Later, Rieta J. et al. shortlisted
the set of parameters from 8 to 5 [161].
Based on atrial activation rate, DF ranges for NSR and regular atrial arrhythmias can be
well defined i.e. 1~1.7 Hz for NSR, 1.7~4 Hz for AT and 4~7 Hz for AFL. However for
AF, different researchers have come up with different DF ranges and the most accepted
range has been identified as 3~12 Hz [147, 150, 158-160, 162]. On closer examination of
these DF ranges, it can be observed that DF range of AF overlaps with AT in DF range of
3~4 Hz and with AFL in DF range of 4~7 Hz. These overlapping frequency ranges
restrict DF to be used as a single parameter for differentiation among AT, AFL and AF.
In this chapter, an algorithm has been proposed for detection of AF and its
differentiation from NSR, AT and AFL during an EP study using DF. For reliability of
DF, the RI parameter is used conventionally. As for as reliability of DF is concerned, RI
parameter works good but does not assist to differentiate AF from AT and AFL in their
overlapping frequency ranges therefore, we need another parameter for differentiation. A
new spectral parameter named as “Average Power Spectral Ratio” (APSR) has been

163
introduced which differentiates among AT, AFL and AF in their overlapping ranges as
well as determines the reliability of DF. This new parameter is less complex to be
calculated and provides more robust result as compared to RI thus eliminates the
requirement of RI for determining the reliability of DF.
Table 7-1 ECG and IEGM Data – AFIC/NIHD
CHANNEL NO LABEL DESCRIPTION
1 I ECG
2
3
4
5
6
7
8
9
10
11
12
aVF
V1
HRAD
HisD
HisP
CS 9-10
CS 7-8
CS 5-6
CS 3-4
CS 1-2
RVAD
“
“
HRA distal
His distal
His proximal
CS catheter
“
“
“
“
RV distal
7.2 Dataset
The majority of Patient’s dataset has been collected from AFIC/NIHD Pakistan and few
from MIT Physionet database as available [12]. AFIC/NIHD dataset includes the verified

164
episodes of NSR, AT, AFL and AF recorded from HRA of 20 patients. To avoid far field
ventricular activity, IEGMs are obtained through 2-5-2 mm catheters employing
electrode pairs in bipolar configuration as shown in Table 7-1. The recorded IEGMs are
in the range of -5mV to +5mV, which are digitized at 2000 Hz sampling rate with 16 bit
precision.
MIT Physionet dataset contains the IEGMs of 8 x patients for cases of AF and AFL. The
MIT dataset was recorded in bipolar configuration from different positions of the right
atrium using 2-5-2 mm catheters sampled at 1000 samples/sec. The MIT dataset consist
of 3 x ECG leads and 5 x IEGMs bipolar signals as depicted in Table 7-2. For this study,
the electrode pair (CS 1-2) which is placed close to the annulus of SVC, has been
selected. Although this configuration is not a standard EP setup, however the selected
electrode pair (CS 1-2) provides localized atrial activity in lieu of HRA catheter.
Table 7-2 ECG and IEGM Data – MIT Physiobank
CHANNEL NO LABEL DESCRIPTION
1 II ECG
2
3
4
5
6
7
8
V1
aVF
CS 1-2
CS 3-4
CS 5-6
CS 7-8
CS 9-10
“
“
CS catheter
“
“
“
“

165
The dataset used for the proposed algorithm consist of 4000 events of verified NSR, AT,
AFL and AF cases as shown in Table 7-3.
Table 7-3 IEGM Dataset (Verified Rhythms)
Atrial Rhythm Number of events
NSR 550
AT 700
AFL 350
AF 1400
Total 4000
7.3 Methodology
In this work, atrial IEGMs from High Right Atrium (HRA) and Superior Vena Cava
(SVC) have been used for differentiation of different SVT. In order to avoid far field
ventricular activity, IEGM are recorded using catheters with minimum inter electrode
spacing (IES) in bipolar configuration [163]. Pre-processing steps as suggested by
Botteron and Jason are applied to IEGM [164, 165]. Welch method is implemented on
pre-processed IEGM for PSD estimation as highlighted by Shafa-at [166, 167]. Spectral
parameters including DF, RI and APSR have been calculated from estimated PSD.
Patterns of DF in estimated PSD of NSR, AT, AFL and AF have been analyzed. APSR
and RI have been compared for regular and irregular arrhythmias. Lastly, an algorithm
has been evolved using DF and APSR parameters to differentiate between NSR, AT,
AFL and AF.
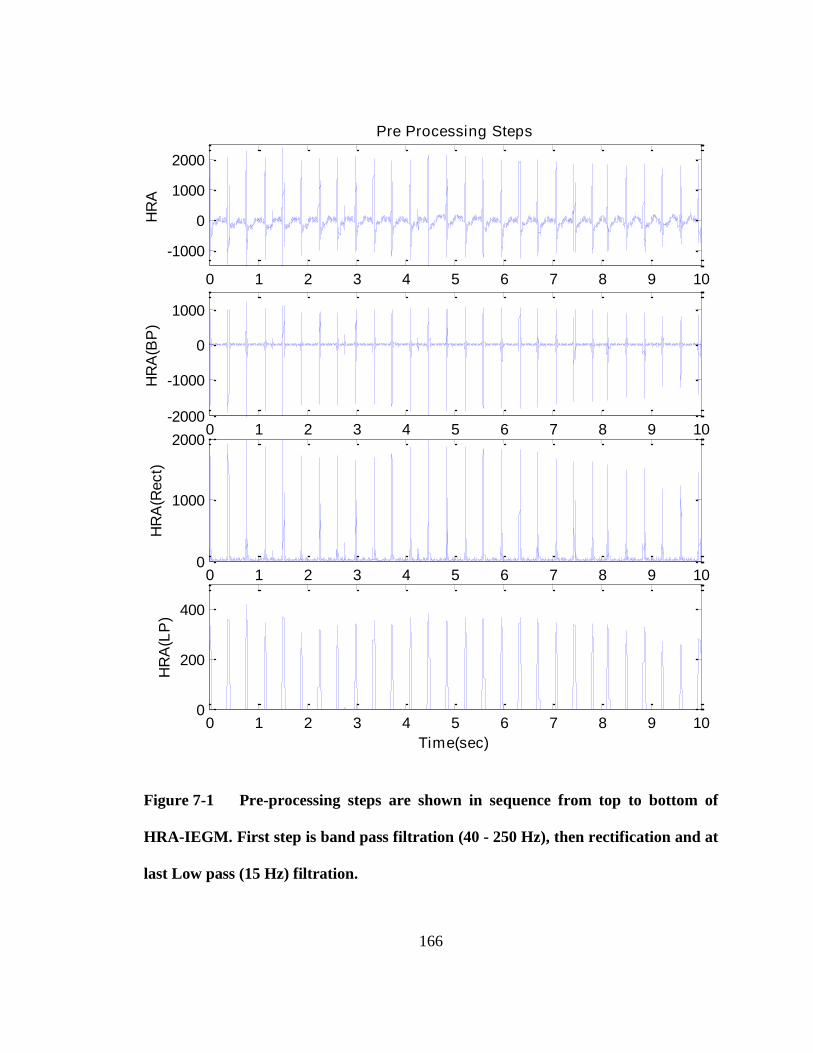
166
0 1 2 3 4 5 6 7 8 9 10
-1000
0
1000
2000H
RA
Pre Processing Steps
0 1 2 3 4 5 6 7 8 9 10-2000
-1000
0
1000
HR
A(B
P)
0 1 2 3 4 5 6 7 8 9 100
1000
2000
HR
A(R
ect)
0 1 2 3 4 5 6 7 8 9 100
200
400
HR
A(L
P)
Time(sec)
Figure 7-1 Pre-processing steps are shown in sequence from top to bottom of
HRA-IEGM. First step is band pass filtration (40 - 250 Hz), then rectification and at
last Low pass (15 Hz) filtration.

167
7.4 IEGM Pre- Processing
Pre-processing of IEGMs is carried out to obtain the signal corresponding to the local
depolarization and to restrict the frequency spectrum to physiological range [164, 168].
These include:
Band pass (40 - 250 Hz) filtering using 3rd order Butterworth filter,
Obtaining monophasic waveform by rectification and
Low pass filtering (15 Hz) using 3rd order Butterworth filter [167].
Pre-processing steps of an IEGM signal acquired from HRA catheter are shown step by
step in Figure 7-1.
7.5 PSD Estimation
For PSD estimation, a number of PSD estimation techniques have been applied in
literature; out of which Bartlett, Welch and Circular Welch method has been applied to
pre-processed IEGM for PSD estimation [166, 169, 170]. A comparison of these methods
has been performed and attached as Annexure ‘A’. Iit has been observed that Welch
method is found most suitable on the basis of the results accuracy.
In the Welch method, the signal segment is divided into P sub segments, with each sub
segment having length L. The sub segments are overlapped and modified periodograms
are computed from the overlapped P sub segments. Also, the periodogram are normalized
by the factor N to compensate for the loss of signal energy owing to the windowing
procedure [171]. Mathematically, it is calculated as
1
0
21
0
)()(1
)(ˆP
i
jnL
n
j
B eiCnxnhPLN
eP (7-1)

168
where P is no of sub segments, L is length of each sub segment, C is the overlap
between two consecutive sub segments, h(n) is windowing function and N is given by
L-1
2
n=0
1N = h(n)
L (7-2)
Length of the signal segment and sub segments has to be kept long enough to provide
the requisite frequency information however frequency resolution should be sufficiently
maintained while averaging the DFs [172]. With the experimentation, the optimum
results have been obtained for signal segment of 10 seconds duration which is divided
into nine sub segments of 2 seconds duration such that each sub segment have 50%
overlap with its consecutive sub segment.
Figure 7-2 Signal segment and Sub Segment for Estimation of PSD through
Welch method.
Modified periodogram of each sub segment with Hanning window, is taken. The average
of these nine spectral estimates gives Welch spectral estimate. Frequency resolution of
PSD is kept to be 0.1221 Hz. For real time monitoring, the signal segment is updated

169
after each second such that one new sub segment is included and one oldest sub segment
is excluded, keeping the same proportion of segment/sub segments. Figure 7-2 depicts the
signal segment and sub segments for estimation of PSD using Welch method.
7.6 Extraction of Spectral Parameters from PSD
7.6.1 Dominant Frequency
DF is referred as the frequency containing maximum PSD in frequency domain and it is
used to estimate of the local atrial activation rate [154, 173]. Usual atrial activation rate
of NSR remains within 60~100 bpm, AT within 100~240 bpm and AFL within 240~420
bpm [13, 20-23, 29-31, 33, 34]. Having estimation of PSD, the DF is determined as the
frequency having highest peak in estimated PSD in 1~12 Hz [152, 153]. For AF, the DF
range is considered 3~12 Hz. Following DF ranges are taken as the baseline of proposed
work, which also commensurate with bpm as indicated above.
NSR - 1~1.7 Hz
AT - 1.7~ 4 Hz
AFL - 4~7 Hz
AF - 3~12 Hz
It is important to note that DF range of AF overlaps with the DF ranges of AFL and AT,
therefore DF parameter alone cannot differentiate between AT, AFL and AF in their
overlapping ranges.

170
7.6.2 Regularity Index
In previous literature, RI parameter is used to establish the reliability of DF. In this work,
RI is calculated only for comparison with APSR. RI is calculated as the ratio of PSD area
under DF/harmonics (1 Hz base) to total PSD area between 1~12Hz as depicted in Figure
7-3[152]. RI is computed numerically using Simpson 3/8 and Trapezoidal rule [167].
Figure 7-3 Calculation of RI for reliability of DF

171
1 2 3 4 5 6 7 8 9 10 11 120
2
4
6
8
10
12
14
15x 10
9
Frequency (Hz)
PS
D
(a)
1 2 3 4 5 6 7 8 9 10 11 120
2
4
6
8
10
12
14
15x 10
8
Frequency (Hz)
PS
D
(b)
Figure 7-4 PSD comparison of regular and irregular arrhythmias with same DF
range:. (a) Case of AT having DF in 3 ~ 4 Hz. (b) Case of AF having DF in 3 ~4 Hz.

172
7.6.3 Average Power Spectral Ratio
The concept underlying APSR surfaced from observation of consistent DF patterns in
range of 3 ~ 7 Hz for the cases of regular arrhythmia (AT, AFL) and irregular arrhythmia
(AF). DF patterns of regular and irregular arrhythmia in their DF overlapping region are
shown in Figure 7-4.
It is obvious from this figure that for AT case (DF range 3~4 Hz) and AFL case (DF
range 4~5 Hz), the respective DFs manifest themselves in form of distinct peaks;
however for the case of AF (DF range 3 ~7 Hz), the DF is like a small mound. Taking
into account these specific patterns, the Power Spectral Ratio (PSR) has been defined as
( ) DF V
DF
PSD PSDPSR
PSD (7-3)
Where DFPSD is the PSD value of DF peak and
VPSD is the PSD value of the valley
with DF peak. APSR is defined as the average of two PSR linked with both valleys
astride DF peak i.e. 1 2( ) / 2V VPSR PSR and can be represented by.
1 2(1 )2
v v
DF
PSD PSDAPSR
PSD (7-4)
where 1vPSD and 2vPSD are the PSD values of two valleys astride DF. Peak and valleys of
a DF are depicted in Figure 7-5.
7.6.4 Comparison between RI and APSR
As already discussed, RI has been used to establish the reliability of DF for irregular
activations like AF, however reliable DF alone does not help to differentiate between AT,
AFL and AF in their overlapping DF ranges. APSR has been introduced in this work to
differentiate between NSR, AT, AFL & AF and ensures the reliability of DF as well.

173
To compare performance of RI and APSR, PSDs of verified events of regular (AT and
AFL) and irregular arrhythmias (AF) in the range of 3~7 Hz have been analyzed to find
out the values of RI and APSR for AT, AFL and AF events. The spread of RI and APSR
values against the verified dataset is summarized in Table 7-4 which, clearly shows that
the APSR value for a regular event, is always greater than 0.9 and for an irregular event,
APSR value remain within 0.20 ~ 0.81. Contrary to this, RI values of regular and
irregular arrhythmia overlap with each other. This indicates a clear isolation between
clusters of regular and irregular arrhythmias in APSR domain whereas these cluster
overlaps in RI domain which reflects that APSR is more suitable for differentiation
between regular and irregular arrhythmias as compared to RI.
1 2 3 4 5 6 7 8 9 10 11 120
5
10
15x 10
8
Frequency (Hz)
PS
D
PSD
Peaks
ValleysDFp
DFv1
DFv2
Figure 7-5 The Description of APSR showing the DF peak “ pDF ” at 3.54Hz and
its two valleys on the both sides of DF.

174
Table 7-4 RI and APSR feature extraction from regular/irregular tachycardia
in DF overlapping ranges
No of Events
RI APSR
Min Mean Max Min Mean Max
Regular
AT 1150 0.34 0.58 0.95 0.969 0.994 0.999
AFL 375 0.6 0.69 0.9 0.921 0.978 0.998
Irregular AF 1200 0.21 0.29 0.44 0.211 0.571 0.812
It can be learnt from the Table 4-1 that APSR with values greater than 0.20 (20%) can
also be used to ensure the reliability of DF. Also the isolated clusters of irregular and
regular arrhythmias for APSR indicates that APSR can be used for differentiation of
irregular arrhythmia (AF) from regular arrhythmia (AT and AFL) in frequency range of
3~7 Hz. Another advantage of APSR over RI is that it does not require finding and
eliminating the harmonics of DF as it is essentially required while calculating RI
parameter. Moreover numerical computations involved in calculation of spectral areas for
RI, makes RI more complex. Therefore, APSR presents less complex and more robust
solution for validation of DF as well as differentiation of regular and irregular
arrhythmias.

175
Figure 7-6 Differentiation Algorithm based on two parameters, DF and APSR.
7.7 Algorithm for Discrimination of Atrial Arrhythmias
DF along with APSR has been used to discriminate amongst NSR and various atrial
arrhythmias as indicated in Figure 7-6. DF is the principal decision making parameter
where as APSR validates the DF and also differentiates between a regular and irregular
arrhythmia in DF overlapping frequency ranges. Keeping in view, the result of Table 7-4,

176
APSR value of 0.85 is marked as threshold criteria between regular and irregular
arrhythmia.
PSD is estimated using Welch method for frequencies between 1~12 Hz. Reliability of
DF is ensured by discarding the events, with APSR < 0.20. Events with reliable DF
within range of 1~1.7 Hz are detected as NSR and within range of 1.7~4 Hz are detected
as AT. To differentiate between AT and AF in DF range of 3~4 Hz, APSR has been
analyzed and events are differentiated as AT if APSR is greater than 0.85.
Similarly, APSR has been used to differentiate between AFL and AF in DF range of 4~7
Hz and the events having APSR greater than 0.85 are differentiated as AFL. The events
having DF less than 0.85 in DF range of 4~7 Hz are differentiated as AF. The events
having DF between 7 Hz and 12 Hz, are differentiated as AF.
7.8 Results and Discussion
7.8.1 Case 1 – NSR detection (1~1.7 Hz)
Figure 7-7 shows the time domain HRA signal as well as estimated PSD acquired
through proposed algorithm for a verified case of NSR with a heart rate of 88 bpm. In this
case, DF is 1.46 Hz and APSR is 0.903. Since the value of APSR is greater than 0.2, the
DF is considered reliable and DF being less than 1.7 Hz, this case is differentiated as
NSR.
7.8.2 Case 2 – AT Detection (1.7~3 Hz)
Time domain representation of atrial IEGM for verified AT case and its estimated PSD is
shown in Figure 7-8. This event has the heart rate of 160 bpm with DF at 2.68 Hz and

177
value of APSR is 0.993. Since the DF lies in the range of 2~3 Hz and APSR > 0.2. This
event has been declared as AT.
0 1 2 3 4 5-5000
0
5000
10000
Normal Sinus Rhythm Case
HR
A
Time (secs)
1 2 3 4 5 6 7 8 9 10 11 120
5
10x 10
9
Frequency (Hz)
PS
D
PSD
DF
Figure 7-7 NSR case: DF is at 1.46 Hz and APSR value is 0.903; declared as NSR.
7.8.3 Case 3 – AT Differentiation from AF (3~4 Hz)
Figure 7-9 indicates the time domain ICEGM and estimated PSD of a verified AT case.
The atrial rate in this event is 230 bpm, the DF is observed at 3.78 Hz and value of APSR
is 0.998. DF is ascertained to be reliable because APSR is greater than 0.2. The DF lies in
the range of 3~4 Hz which is also shared by AF (DF range 3~12 Hz) however, the value
of APSR is greater than 0.85 so the event has been differentiated as AT.

178
0 1 2 3 4 5 6 7 8 9 10-2000
0
2000
4000
HR
A
Time(sec)
Atrial Tachycardia Case
1 2 3 4 5 6 7 8 9 10 11 120
2
4
6x 10
9
Frequency(Hz)
PS
D
PSD
DF
Figure 7-8 AT Case: DF is at 2.68 Hz and APSR value is 0.993; declared as AT.
0 1 2 3 4 5 6 7 8 9 10-2000
0
2000
4000
Artial Tachycardia Case
HR
A
Time (secs)
1 2 3 4 5 6 7 8 9 10 11 120
2
4x 10
10
Frequency (Hz)
PS
D
PSD
DF
Figure 7-9 AT Differentiation from AF (3~4 Hz): DF is at 3.78 Hz and APSR
value is 0.998; since APSR value is greater than 0.85, event is declared as AT.

179
7.8.4 Case – 4: AFL Differentiation from AF (4~7 Hz)
Time domain HRA signal and estimated PSD for verified event of AFL are shown in
Figure 7-10. In this case, DF is observed at 4.13 Hz and the value of APSR is 0.977.
Having DF in frequency range of 4~7 Hz could be the case of either AFL or AF; but in
this case APSR is greater than 0.85, therefore it is differentiated as case of AFL.
7.8.5 Case 5: AF Differentiation from AT (3~4 Hz)
Figure 7-11 indicates the time domain IEGM and estimated PSD of a verified AF event.
In this event, the DF is at 3.78 Hz and value of APSR is 0.731. However, DF lies in range
of 3~4 Hz which is common range of AT also. This event is declared as AF because
APSR lies between 0.2 and 0.85.
0 1 2 3 4 5 6 7 8 9 10-1
0
1
2
Atrial Flutter Case
HR
A
Time (secs)
1 2 3 4 5 6 7 8 9 10 11 120
500
1000
Frequency (Hz)
PS
D
PSD
DF
Figure 7-10 AFL Differentiation from AF (4~5 Hz): DF at 4.13 Hz and APSR
value of 0.977; since APSR value is greater than 0.85, event is declared as AFL.

180
0 1 2 3 4 5 6 7 8 9 10-2000
0
2000
Atrial Fibrillation Case
HR
A
Time (secs)
1 2 3 4 5 6 7 8 9 10 11 120
5
10
15x 10
8
Frequency (Hz)
PS
D
PSD
DF
Figure 7-11 AF Differentiation from AT (3~4 Hz): DF is at 3.78 Hz and APSR
value is 0.731; since APSR value is lesser than 0.85, event is declared as AF.
0 1 2 3 4 5 6 7 8 9 10-5000
0
5000
Atrial Fibrillation Case
HR
A
Time (secs)
1 2 3 4 5 6 7 8 9 10 11 120
1
2x 10
9
Frequency (Hz)
PS
D
PSD
DF
Figure 7-12 AF Differentiation from AFL (4~5 Hz): DF is at 4.27 Hz and APSR
value is 0.646; since APSR value is lesser than 0.85, event is declared as AF.

181
7.8.6 Case 6: AF Differentiation from AFL (>4 Hz)
Figure 7-12 depicts the time domain ICEGM and estimated PSD of a verified AF event.
Here DF is at 4.27 Hz and it is required to be differentiated from AFL. As APSR value
for this case is 0.646 (0.2< APSR < 0.85), therefore the case is confirmed as AF..
7.8.7 Case 7: AF Detection (5~12 Hz)
Figure 7-13 shows a case of AF where DF is observed at 6.47 Hz and value of APSR is
0.517 (0.2< APSR < 0.85) therefore this case is declared as AF.
0 1 2 3 4 5 6 7 8 9 10-5000
0
5000
10000
Atrial Fibrillation Case
HR
A
Time (secs)
1 2 3 4 5 6 7 8 9 10 11 120
2
4
6x 10
9
Frequency (Hz)
PS
D
PSD
DF
Figure 7-13 AF Detection (5~12 Hz): DF is at 6.47 Hz and APSR value is 0.517,
declared as AF.
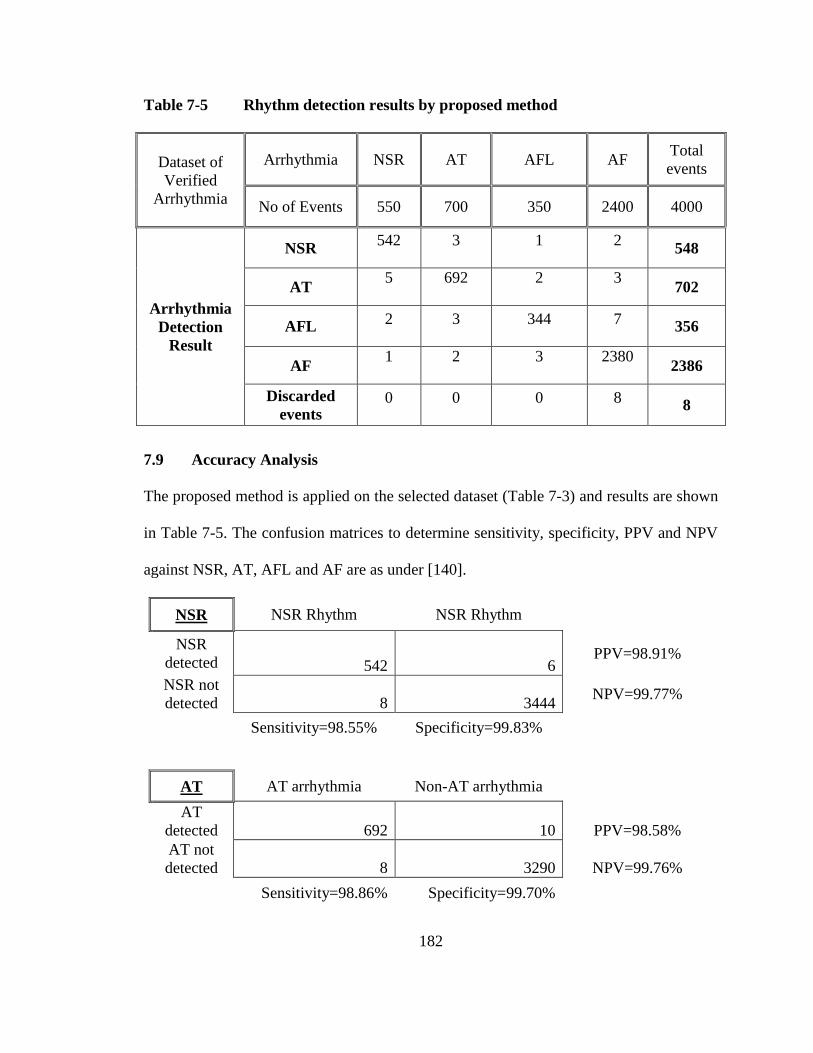
182
Table 7-5 Rhythm detection results by proposed method
Dataset of
Verified
Arrhythmia
Arrhythmia NSR AT AFL AF Total
events
No of Events 550 700 350 2400 4000
Arrhythmia
Detection
Result
NSR 542 3 1 2
548
AT 5 692 2 3
702
AFL 2 3 344 7
356
AF 1 2 3 2380
2386
Discarded
events 0 0 0 8
8
7.9 Accuracy Analysis
The proposed method is applied on the selected dataset (Table 7-3) and results are shown
in Table 7-5. The confusion matrices to determine sensitivity, specificity, PPV and NPV
against NSR, AT, AFL and AF are as under [140].
NSR NSR Rhythm NSR Rhythm
NSR
detected 542 6 PPV=98.91%
NSR not
detected 8 3444 NPV=99.77%
Sensitivity=98.55% Specificity=99.83%
AT AT arrhythmia Non-AT arrhythmia
AT
detected 692 10 PPV=98.58%
AT not
detected 8 3290 NPV=99.76%
Sensitivity=98.86% Specificity=99.70%

183
AFL AFL arrhythmia Non-AFL arrhythmia
AFL
detected 344 12 PPV=96.63%
AFL not
detected 6 3638 NPV=99.84%
Sensitivity=98.29% Specificity=99.67%
AF AF arrhythmia Non-AF arrhythmia
AF
detected 2380 6 PPV=99.75%
AF not
detected 20 1594 NPV=98.76%
Sensitivity=99.17% Specificity=99.63%
Table 7-6 shows the accuracy of the proposed system in term of sensitivity, specificity
and PPV and NPV [140].
Table 7-6 Sensitivity, Specificity, PPV and NPV Results
Cardiac
arrhythmia Sensitivity (%) Specificity (%) PPV (%) NPV (%)
NSR 98.55 99.83 98.91 99.77
AT 98.86 99.70 98.58 99.76
AFL 98.29 99.67 96.63 99.84
AF 99.17 99.63 99.75 98.76

184
7.10 Summary
The work presented in this chapter is the continuation of a project aimed at automated
detection of cardiac arrhythmias during an EP study. This work specifically detects and
differentiates among NSR, AT, AFL and AF using atrial IEGMs recorded from HRA and
SVC. After pre-processing of atrial IEGM, Welch spectral estimation method has been
used to estimate DF. A new spectral parameter, APSR has been introduced in this work.
It has been found that APSR can replace RI for ensuring the reliability of DF. Also,
APSR helps in differentiating between AT and AFL in DF range 3~4 Hz and between
AFL and AF in DF range 4~7 Hz. An automated arrhythmia differentiation can facilitate
the patient monitoring during EP study as well as it can be effectively used for additional
therapeutic application by implantable cardioverter defibrillators. The proposed algorithm
has been tested on 4000 verified events and achieved an accuracy of 99.53%.

185
CONCLUSION AND FUTURE WORK
Conclusion
Cardiac Electrophysiology (EP) study is a medical procedure to identify and treat
different types of arrhythmias. The objective of this thesis work was to automate the
detection process for major types of SVT. Both time domain analysis under special
protocols and frequency domain analysis have been applied for differentiation of various
types of SVTs. Real-world IEGM signals were used to check performance of proposed
algorithm. Pre-processing stage is very important for accurate extraction of critical
features. First, IEGMs are passed through noise removal stages, which removes the major
interferences like PLI and EMG noises. The removal of PLI noise is done through an
adaptive state space filter, which has capability to accurately filter out PLI noise. For
removal of EMG noise, Savitzky-golay filter is applied.
After noise removal, the SVT arrhythmia classification has been carried out through two
techniques. First technique is based on temporal features, in which special pacing
protocols are applied and changes in IEGMs are observed to detect reentrant tachycardia,
which include AVNRT and AVRT. Here marking of temporal features is critical; the
onset points of A, H & V waves on selected IEGMs are located to calculate their
temporal relationships. Special attention has been paid for reduction of false positives in
the feature extraction process. The results show that performance of the proposed
algorithm for arrhythmia detection in clinical EPS is comparable to manual diagnostic
procedures. Using the automated detection algorithm in a practical environment can
greatly reduce the manual work done by doctors. The main significance to develop this

186
system is to reduce or minimize the time required by electro physiologist for manual
calculations to find A, V and H waves feature when dealing in time domain.
The second technique is based on non parametric analysis (frequency domain analysis).
While applying frequency domain analysis, the proposed system is able to differentiate
between NSR, AT, AFL and AF. Real-world IEGM signals were used to test the
algorithm. An algorithm has been proposed in which modified Welch method is used for
PSD estimation and a new parameter named as APSR has been introduced which
confirms the reliability of DF and also assist to differentiate among different SVT
arrhythmia. For validation of classification result, the database of AFIC/NIHD and
physionet has been taken as reference and the results were verified by EP specialists.
Future Recommendations
For future researchers in this field, I would like to suggest the following:
1. Atypical AVNRT detection
Features detection in intracardiac domain has been successfully implemented which is
pre-requisite to any arrhythmia detection using temporal relationship of these features
and suitable pacing protocols. Algorithm has been developed for detection of
AVNRT/AVRT using temporal features. AVNRT can be divide into two main types,
which includes typical AVNRT (slow-fast) and atypical AVNRT (fast-slow and slow-
slow). Typical AVNRT is most common of all SVT arrhythmia and its database is easily
available, therefore its algorithm is tested successfully. However database of atypical
AVNRT (fast-slow) was not sufficient to be tested; It is recommended that sufficient
database of atypical AVNRT cases may be collected for detailed testing.

187
2. Sub categorization of AVRT arrhythmia
AVRT arrhythmia is further divided into two main types named as orthdromic (typical)
and antidromic (atypical) AVRT. Atypical AVRT needs to be further explored for
availability of large database and its testing by automated detection algorithm.
3. Hybrid combination of arrhythmia
Sometime it happens that two or more types of arrhythmias are also present whose
signature may be different from individual arrhythmia. Although such combinations are
rare, however these hybrid combinations needs to be further studied in depth for different
possibilities and their automated detection. AVNRT with bystanding accessory pathway
is one such type which often mixed up with antidromic AVRT.
4. Uncommon AV junction related arrhythmia
Algorithm for detection of other types of arrhythmias related to AV junction is required
to be developed. These include Non-paroxysmal junctional tachycardia, focal junctional
tachycardia, junctional tachycardia and WPW.
5. Algorithm to locate accessory pathway
The treatment/cure of AVRT is done by ablating the accessory pathway. Therefore, an
algorithm can be developed for mapping of the accessory pathway in the heart.
6. Sub categories of main SVT arrhythmias
In this work, the major categories of SVT arrhythmia have been differentiated. However,
it can be further extended to differentiate the sub categories of these arrhythmias.

188
7. Algorithm to detect VT arrhythmias
This thesis has laid the ground work for arrhythmia detection algorithm. The work
presented in this research can be modified to design detectors for ventricular Tachycardia
(VT) and its related types.
Acknowledgement
I would like to acknowledge the help and support extended to me for this research work
by
1. EP team of AFIC especially Lt Gen Imran Majeed and Col Azmat
2. Biomedical Dept, AFIC especially Lt Col (R) Mubashar
3. Cardiology Dept, Shifa International hospital especially Dr Habib

189
References
[1] W. H. Organization, "Cardiovascular diseases (CVDs): Fact sheet No. 317. 2011,"
Geneva: World Health Organization Google Scholar, 2011.
[2] E. J. Benjamin, M. J. Blaha, S. E. Chiuve, M. Cushman, S. R. Das, R. Deo, et al.,
"Heart disease and stroke statistics—2017 update: a report from the American
Heart Association," Circulation, vol. 135, pp. e146-e603, 2017.
[3] W. H. Organization, Global status report on noncommunicable diseases 2010:
Geneva: World Health Organization, 2011.
[4] C. D. Mathers and D. Loncar, "Projections of global mortality and burden of
disease from 2002 to 2030," Plos med, vol. 3, p. e442, 2006.
[5] T. F. Luescher and L. van den Berghe, "Circulation: Arrhythmia and
electrophysiology," ed: LIPPINCOTT WILLIAMS & WILKINS 530 WALNUT
ST, PHILADELPHIA, PA 19106-3621 USA, 2008.
[6] S. Goodacre and R. Irons, "Atrial arrhythmias.(ABC of Clinical
Electrocardiography)," British Medical Journal, vol. 324, pp. 594-598, 2002.
[7] R. L. Page, J. A. Joglar, M. A. Caldwell, H. Calkins, J. B. Conti, B. J. Deal, et al.,
"2015 ACC/AHA/HRS guideline for the management of adult patients with
supraventricular tachycardia," Circulation, vol. 133, pp. e506-e574, 2016.
[8] D. G. Katritsis, B. J. Gersh, and A. J. Camm, Clinical cardiology: Current
practice guidelines: OUP Oxford, 2013.
[9] K. W. Lee, N. Badhwar, and M. M. Scheinman, "Supraventricular tachycardia—
part II: history, presentation, mechanism, and treatment," Current problems in
cardiology, vol. 33, pp. 557-622, 2008.
[10] K. W. Lee, N. Badhwar, and M. M. Scheinman, "Supraventricular tachycardia—
part I," Current problems in cardiology, vol. 33, pp. 467-546, 2008.
[11] H. J. Wellens and M. B. Conover, The ECG in emergency decision making: WB
Saunders Company, 2006.
[12] A. L. Goldberger, L. A. Amaral, L. Glass, J. M. Hausdorff, P. C. Ivanov, R. G.
Mark, et al., "Physiobank, physiotoolkit, and physionet components of a new
research resource for complex physiologic signals," Circulation, vol. 101, pp.
e215-e220, 2000.
[13] K. Chatterjee, Cardiology : an illustrated textbook. New Delhi: Jaypee Brothers
Medical Publisher, 2013.
[14] 30 Mar2017). Heart. Available: http://www.innerbody.com/image/card01.html
[15] P. A. Iaizzo, Handbook of cardiac anatomy, physiology, and devices: Springer
Science & Business Media, 2009.
[16] M. S. Thaler, The only EKG book you'll ever need: Lippincott Williams &
Wilkins, 2010.
[17] "action potential," in The American Heritage® New Dictionary of Cultural
Literacy, 3rd ed. Houghton: Houghton Mifflin Company, 2005.
[18] A. Natale and O. Wazni, Handbook of Cardiac Electrophysiology: CRC Press,
2007.

190
[19] R. N. Fogoros. (2013). Electrophysiologic testing. Available:
http://www.dawsonera.com/depp/reader/protected/external/AbstractView/S97811
18399637
[20] P. J. Zimetbaum and M. E. Josephson, Practical clinical electrophysiology:
Lippincott Williams & Wilkins, 2009.
[21] K. Chatterjee, Manual of electrophysiology, 2015.
[22] M. A. Syed, S. V. Raman, and O. P. Simonetti. (2015). Basic principles of
cardiovascular MRI : physics and imaging technique. Available:
http://search.ebscohost.com/login.aspx?direct=true&scope=site&db=nlebk&db=n
labk&AN=1088855
[23] A. E. Buxton, H. Calkins, D. J. Callans, J. P. DiMarco, J. D. Fisher, H. L. Greene,
et al., "ACC/AHA/HRS 2006 key data elements and definitions for
electrophysiological studies and procedures: a report of the American College of
Cardiology/American Heart Association Task Force on Clinical Data Standards
(ACC/AHA/HRS Writing Committee to Develop Data Standards on
Electrophysiology)," Journal of the American College of Cardiology, vol. 48, pp.
2360-2396, 2006.
[24] R. N. Fogoros, Electrophysiologic testing: John Wiley & Sons, 2012.
[25] D. Bosen, "Narrow‐complex tachycardia," Nursing2016, vol. 33, p. 96, 2003.
[26] L. Weinberger, "Wide complex tachycardia," MedEdPORTAL Publications, vol.
7, p. 8499, 2011.
[27] F. D. Murgatroyd, Handbook of cardiac electrophysiology: a practical guide to
invasive EP studies and catheter ablation: Remedica, 2002.
[28] R. Klabunde, Cardiovascular physiology concepts: Lippincott Williams &
Wilkins, 2011.
[29] S. I. Goodacre, R. , "Atrial arrhythmias," British Medical Journal, pp. 594 - 597, 9 Mar
2002.
[30] A. S. Budzikowski. Atrial Tachycardia. Available:
http://emedicine.medscape.com/article/151456-
overview?pa=Yds7%2FnthyijjS35XFzhTe1ExvPR27BmI7vUOKGvDGDU0Ns5
bbFSO18%2Bbe1DtzeTD43mU9jD%2B1DtnxY47OmyybA%3D%3D#a2
[31] V. E. Friedewald, Supraventricular Tachycardia:(SVT/Paroxysmal
Supraventicular Tachycardia/PSVT): Springer, 2016.
[32] A. S. Batra and N. Mohari, "Junctional ectopic tachycardia: current strategies for
diagnosis and management," Progress in Pediatric Cardiology, vol. 35, pp. 49-
54, 2013.
[33] D. McGraw-Hill, "Concise Dictionary of Modern Medicine," ed: The McGraw-
Hill Companies, Inc,. http://medical-dictionary. thefreedictionary. com/(Stand
08.2016), 2002.
[34] M. Boyer and B. A. Koplan, "Atrial flutter," Circulation, vol. 112, pp. e334-e336,
2005.
[35] N. Saoudi, F. COSIO, A. WALDO, S. A. CHEN, Y. Iesaka, M. LESH, et al.,
"Classification of atrial flutter and regular atrial tachycardia according to
electrophysiologic mechanism and anatomic bases: a statement from a joint expert
group from the Working Group of Arrhythmias of the European Society of

191
Cardiology and the North American Society of Pacing and Electrophysiology,"
Journal of cardiovascular electrophysiology, vol. 12, pp. 852-866, 2001.
[36] A. J. Camm, P. Kirchhof, G. Y. Lip, U. Schotten, I. Savelieva, S. Ernst, et al.,
"Guidelines for the management of atrial fibrillation," European heart journal,
vol. 31, pp. 2369-2429, 2010.
[37] J. E. P. Waktare, "Atrial Fibrillation," Circulation, vol. 106, pp. 14-16, 2002.
[38] C. Tomasi, R. De Ponti, M. Tritto, A. L. Barilli, N. Bottoni, M. Zardini, et al.,
"Simultaneous dual fast and slow pathway conduction upon induction of typical
atrioventricular nodal reentrant tachycardia: electrophysiologic characteristics in a
series of patients," Journal of cardiovascular electrophysiology, vol. 16, pp. 594-
600, 2005.
[39] N. J. Kertesz, R. I. Fogel, and E. N. Prystowsky, "Mechanism of induction of
atrioventricular node reentry by simultaneous anterograde conduction over the
fast and slow pathways," Journal of cardiovascular electrophysiology, vol. 16,
pp. 251-255, 2005.
[40] wikipedia, "Electrocardiography," in wikipedia, ed. (2017, April 10): Wikipedia,
2017.
[41] C. M. Tracy, M. Akhtar, J. P. DiMarco, D. L. Packer, H. H. Weitz, W. L. Winters,
et al., "American College of Cardiology/American Heart Association Clinical
Competence Statement on invasive electrophysiology studies, catheter ablation,
and cardioversion," Circulation, vol. 102, pp. 2309-2320, 2000.
[42] H. Richard. Intro to Intracardiac [Online].
[43] K. Venkatachalam, J. E. Herbrandson, and S. J. Asirvatham, "Signals and signal
processing for the electrophysiologist," Circulation: Arrhythmia and
Electrophysiology, vol. 4, pp. 965-973, 2011.
[44] A. C. Metting van Rijn, A. Peper, and C. A. Grimbergen, "High-quality recording
of bioelectric events," Medical and Biological Engineering and Computing, vol.
28, pp. 389-397, 1990/09/01 1990.
[45] J. Piskorowski, "Digital Q-Varying Notch IIR Filter With Transient Suppression,"
Instrumentation and Measurement, IEEE Transactions on, vol. 59, pp. 866-872,
2010.
[46] B. Widrow, J. R. Glover, Jr., J. M. McCool, J. Kaunitz, C. S. Williams, R. H.
Hearn, et al., "Adaptive noise cancelling: Principles and applications,"
Proceedings of the IEEE, vol. 63, pp. 1692-1716, 1975.
[47] J. Glover, Jr., "Adaptive noise canceling applied to sinusoidal interferences,"
Acoustics, Speech and Signal Processing, IEEE Transactions on, vol. 25, pp. 484-
491, 1977.
[48] C. Chandrakar and M. Kowar, "Denoising ECG signals using adaptive filter
algorithm," International Journal of Soft Computing and Engineering (IJSCE),
vol. 2, pp. 120-123, 2012.
[49] M. Maniruzzaman, K. M. S. Billah, U. Biswas, and B. Gain, "Least-Mean-Square
algorithm based adaptive filters for removing power line interference from ECG
signal," in Informatics, Electronics & Vision (ICIEV), 2012 International
Conference on, 2012, pp. 737-740.

192
[50] H. So, "Adaptive algorithm for sinusoidal interference cancellation," Electronics
Letters, vol. 33, pp. 1910-1912, 1997.
[51] S. M. Martens, M. Mischi, S. G. Oei, and J. W. Bergmans, "An improved
adaptive power line interference canceller for electrocardiography," Biomedical
Engineering, IEEE Transactions on, vol. 53, pp. 2220-2231, 2006.
[52] A. Bazhyna, I. Christov, A. Gotchev, I. Daskalov, and K. Egiazarian, "Powerline
interference suppression in high-resolution ECG," in Computers in Cardiology,
2003, 2003, pp. 561-564.
[53] P. Koseeyaporn, J. Koseeyaporn, and P. Wardkein, "An enhanced adaptive
algorithm for PLI cancellation in ECG signals," in Information, Communications
and Signal Processing, 2009. ICICS 2009. 7th International Conference on, 2009,
pp. 1-5.
[54] I. Badreldin, D. El-Kholy, and A. El-Wakil, "A modified adaptive noise canceler
for electrocardiography with no power-line reference," in Biomedical Engineering
Conference (CIBEC), 2010 5th Cairo International, 2010, pp. 13-16.
[55] I. Badreldin, D. El-Kholy, and A. Elwakil, "Harmonic adaptive noise canceler for
electrocardiography with no power-line reference," in Electrotechnical
Conference (MELECON), 2012 16th IEEE Mediterranean, 2012, pp. 1017-1020.
[56] N. Razzaq, M. Butt, M. Salman, R. Ali, I. Sadiq, K. Munawar, et al., "An
intelligent adaptive filter for fast tracking and elimination of power line
interference from ECG signal," in Computer-Based Medical Systems (CBMS),
2013 IEEE 26th International Symposium on, 2013, pp. 251-256.
[57] R. Acharya, S. M. Krishnan, J. A. Spaan, and J. S. Suri, Advances in cardiac
signal processing: Springer, 2007.
[58] S. M. Alessio, Digital Signal Processing and Spectral Analysis for Scientists:
Concepts and Applications: Springer, 2015.
[59] F. De la Rosa, Harmonics and power systems: CRC Press, 2006.
[60] E. Jacobsen and R. Lyons, "The sliding DFT," Signal Processing Magazine,
IEEE, vol. 20, pp. 74-80, 2003.
[61] M. B. Malik, "State-space recursive least-squares: part I," Signal processing, vol.
84, pp. 1709-1718, 2004.
[62] L. Sörnmo and P. Laguna, Bioelectrical signal processing in cardiac and
neurological applications vol. 8: Academic Press, 2005.
[63] Y.-W. Bai, W.-Y. Chu, C.-Y. Chen, Y.-T. Lee, Y.-C. Tsai, and C.-H. Tsai, "The
combination of Kaiser window and moving average for the low-pass filtering of
the remote ECG signals," in Computer-Based Medical Systems, 2004. CBMS
2004. Proceedings. 17th IEEE Symposium on, 2004, pp. 273-278.
[64] S. Hargittai, "Efficient and fast ECG baseline wander reduction without distortion
of important clinical information," in Computers in Cardiology, 2008, 2008, pp.
841-844.
[65] M. Kaur, B. Singh, J. Ubhi, and S. Rani, "Digital filteration of ecg signals for
removal of baseline drift," in Proceedings of International Conference on
Computer Communication and Management (ICCCM 2011), 2011.
[66] R. Lakhwani, S. Ayub, and J. Saini, "Design and comparison of digital filters for
removal of baseline wandering from ECG signal," in Computational Intelligence

193
and Communication Networks (CICN), 2013 5th International Conference on,
2013, pp. 186-191.
[67] S. Luo and P. Johnston, "A review of electrocardiogram filtering," Journal of
Electrocardiology, vol. 43, pp. 486-496, 2010.
[68] P. Shetty and S. Bhat, "Analysis of various filter configurations on noise
reduction in ECG waveform," International Journal of Computing,
Communications & Instrumentation Engg.(IJCCIE), vol. 1, pp. 88-91, 2014.
[69] J. Van Alste and T. Schilder, "Removal of base-line wander and power-line
interference from the ECG by an efficient FIR filter with a reduced number of
taps," IEEE Transactions on Biomedical Engineering, pp. 1052-1060, 1985.
[70] A. D. BAKHSHI, A. AHMED, S. M. GULFAM, A. KHAQAN, A. YASIN, S.
IQBAL, et al., "Estimation of Baseline Wander Characteristics in ECG Signals
Using Adaptive Transversal Filter and Lomb’s Periodogram Analysis," Przegląd
Elektrotechniczny, vol. 89, pp. 107-110, 2013.
[71] J. R. Gradwohl, E. W. Pottala, M. R. Horton, and J. J. Bailey, "Comparison of two
methods for removing baseline wander in the ECG," in Computers in Cardiology,
1988. Proceedings., 1988, pp. 493-496.
[72] M. Kaur and B. Singh, "Comparison of different approaches for removal of
baseline wander from ECG signal," in Proceedings of the International
Conference & Workshop on Emerging Trends in Technology, 2011, pp. 1290-
1294.
[73] A. Fasano and V. Villani, "ECG baseline wander removal and impact on beat
morphology: A comparative analysis," in Computing in Cardiology Conference
(CinC), 2013, 2013, pp. 1167-1170.
[74] A. Hiasat, M. Al-Ibrahim, and K. Gharaibeh, "Design and implementation of a
new efficient median filtering algorithm," IEE Proceedings-Vision, Image and
Signal Processing, vol. 146, pp. 273-278, 1999.
[75] B. Arvinti, D. Toader, M. Costache, and A. Isar, "Electrocardiogram baseline
wander removal using stationary wavelet approximations," in Optimization of
Electrical and Electronic Equipment (OPTIM), 2010 12th International
Conference on, 2010, pp. 890-895.
[76] M. Dai and S.-L. Lian, "Removal of baseline wander from dynamic
electrocardiogram signals," in Image and Signal Processing, 2009. CISP'09. 2nd
International Congress on, 2009, pp. 1-4.
[77] P. B. Patil and M. S. Chavan, "A wavelet based method for denoising of
biomedical signal," in Pattern Recognition, Informatics and Medical Engineering
(PRIME), 2012 International Conference on, 2012, pp. 278-283.
[78] D. Zhang, "Wavelet approach for ECG baseline wander correction and noise
reduction," in Engineering in Medicine and Biology Society, 2005. IEEE-EMBS
2005. 27th Annual International Conference of the, 2005, pp. 1212-1215.
[79] J. Tang, Q. Zou, Y. Tang, B. Liu, and X.-k. Zhang, "Hilbert-Huang transform for
ECG de-noising," in Bioinformatics and Biomedical Engineering, 2007. ICBBE
2007. The 1st International Conference on, 2007, pp. 664-667.
[80] U. Biswas, A. Das, S. Debnath, and I. Oishee, "ECG signal denoising by using
least-mean-square and normalised-least-mean-square algorithm based adaptive

194
filter," in Informatics, Electronics & Vision (ICIEV), 2014 International
Conference on, 2014, pp. 1-6.
[81] M. Mneimneh, E. Yaz, M. Johnson, and R. Povinelli, "An adaptive Kalman filter
for removing baseline wandering in ECG signals," in Computers in Cardiology,
2006, 2006, pp. 253-256.
[82] A. C. Mugdha, F. S. Rawnaque, and M. U. Ahmed, "A study of recursive least
squares (RLS) adaptive filter algorithm in noise removal from ECG signals," in
Informatics, Electronics & Vision (ICIEV), 2015 International Conference on,
2015, pp. 1-6.
[83] B. Singh, P. Singh, and S. Budhiraja, "Various approaches to minimise noises in
ECG signal: A survey," in Advanced Computing & Communication Technologies
(ACCT), 2015 Fifth International Conference on, 2015, pp. 131-137.
[84] P. Tikkanen, Characterization and application of analysis methods for ECG and
time interval variability data: Oulun yliopisto, 1999.
[85] M. H. Limaye and M. V. Deshmukh, "ECG Noise Sources and Various Noise
Removal Techniques: A Survey."
[86] P. Bhaskar and M. Uplane, "High Frequency Electromyogram Noise Removal
from Electrocardiogram Using FIR Low Pass Filter Based on FPGA," Procedia
Technology, vol. 25, pp. 497-504, 2016.
[87] W. Rose, "Electromyogram analysis," Online course material. University of
Delaware. Retrieved July, vol. 5, p. 2016, 2011.
[88] P. W. Hodges and B. H. Bui, "A comparison of computer-based methods for the
determination of onset of muscle contraction using electromyography,"
Electroencephalography and Clinical Neurophysiology/Electromyography and
Motor Control, vol. 101, pp. 511-519, 1996.
[89] S. L. Joshi, R. A. Vatti, and R. V. Tornekar, "A survey on ECG signal denoising
techniques," in Communication Systems and Network Technologies (CSNT), 2013
International Conference on, 2013, pp. 60-64.
[90] S. Rani, A. Kaur, and J. Ubhi, "Comparative study of FIR and IIR filters for the
removal of Baseline noises from ECG signal," 2011.
[91] W.-h. Lin, M. Y.-M. Wong, L.-n. Pu, and Y.-t. Zhang, "Comparison of median
filter and discrete dyadic wavelet transform for noise cancellation in
electrocardiogram," in Engineering in Medicine and Biology Society (EMBC),
2010 Annual International Conference of the IEEE, 2010, pp. 2395-2398.
[92] M. Z. U. Rahman, R. A. Shaik, and D. Reddy, "Noise cancellation in ECG signals
using computationally simplified adaptive filtering techniques: Application to
biotelemetry," Signal Processing: An International Journal (SPIJ), vol. 3, pp. 1-
12, 2009.
[93] C.-H. Chang, H.-J. Ko, and K.-M. Chang, "Cancellation of high-frequency noise
in ECG signals using adaptive filter without external reference," in Biomedical
Engineering and Informatics (BMEI), 2010 3rd International Conference on,
2010, pp. 787-790.
[94] S. Hargittai, "Savitzky-Golay least-squares polynomial filters in ECG signal
processing," in Computers in Cardiology, 2005, 2005, pp. 763-766.

195
[95] J. S. Sørensen, L. Johannesen, U. S. L. Grove, K. Lundhus, J.-P. Couderc, and C.
Graff, "A comparison of IIR and wavelet filtering for noise reduction of the
ECG," in Computing in Cardiology, 2010, 2010, pp. 489-492.
[96] M. Khan, F. Aslam, T. Zaidi, and S. A. Khan, "Wavelet based ecg denoising
using signal-noise residue method," in Bioinformatics and Biomedical
Engineering,(iCBBE) 2011 5th International Conference on, 2011, pp. 1-4.
[97] R. W. Schafer, "What is a Savitzky-Golay filter?[lecture notes]," IEEE Signal
processing magazine, vol. 28, pp. 111-117, 2011.
[98] R. MacDonald, J. Jenkins, R. Arzbaecher, and R. Throne, "A software trigger for
intracardiac waveform detection with automatic threshold adjustment," in
Computers in Cardiology 1989, Proceedings., 1989, pp. 167-170.
[99] S. Greenhut, R. MacDonald, J. Jenkins, and R. Arzbaecher, "Real-time computer
acquisition, analysis, and display of electrophysiology studies," in Computers in
Cardiology 1990, Proceedings., 1990, pp. 573-576.
[100] L. Pang, K. Danehorn, I. Tchoudovski, and A. Bolz, "Automatic identification of
cardiac activations in the multi-channel Intracardiac ECGs," 2006.
[101] P. De Chazal, M. O'Dwyer, and R. B. Reilly, "Automatic classification of
heartbeats using ECG morphology and heartbeat interval features," IEEE
Transactions on Biomedical Engineering, vol. 51, pp. 1196-1206, 2004.
[102] P. de Chazal and R. B. Reilly, "A patient-adapting heartbeat classifier using ECG
morphology and heartbeat interval features," IEEE Transactions on Biomedical
Engineering, vol. 53, pp. 2535-2543, 2006.
[103] C. Ye, B. V. Kumar, and M. T. Coimbra, "Heartbeat classification using
morphological and dynamic features of ECG signals," IEEE Transactions on
Biomedical Engineering, vol. 59, pp. 2930-2941, 2012.
[104] P. de Chazal and R. B. Reilly, "Automatic classification of ECG beats using
waveform shape and heart beat interval features," in Acoustics, Speech, and
Signal Processing, 2003. Proceedings.(ICASSP'03). 2003 IEEE International
Conference on, 2003, pp. II-269.
[105] S. Raj, K. Maurya, and K. C. Ray, "A knowledge-based real time embedded
platform for arrhythmia beat classification," Biomedical Engineering Letters, vol.
5, pp. 271-280, 2015.
[106] I. Murthy and G. D. Prasad, "Analysis of ECG from pole-zero models," IEEE
transactions on biomedical engineering, vol. 39, pp. 741-751, 1992.
[107] S. Mehta, S. Saxena, and H. Verma, "Computer-aided interpretation of ECG for
diagnostics," International journal of systems science, vol. 27, pp. 43-58, 1996.
[108] M. L. Ahlstrom and W. J. Tompkins, "Automated high-speed analysis of Holter
tapes with microcomputers," IEEE Transactions on Biomedical Engineering, pp.
651-657, 1983.
[109] A. D. Bakhshi, M. A. Maud, K. M. Aamir, and A. Loan, "Aggregate spectrogram
based classification of Holter ECG signals for wireless sensor networks," in
Emerging Technologies (ICET), 2012 International Conference on, 2012, pp. 1-6.
[110] S. Saksena and A. J. Camm, Electrophysiological Disorders of the Heart: Expert
Consult: Elsevier Health Sciences, 2011.

196
[111] H. Vänttinen, J. Nousiainen, P. Mäkynen, and J. Malmivuo, "Windows software
for cardiac electrophysiology studies and ablation monitoring," Computer
methods and programs in biomedicine, vol. 61, pp. 221-231, 2000.
[112] S. Choi and Z. Jiang, "Comparison of envelope extraction algorithms for cardiac
sound signal segmentation," Expert Systems with Applications, vol. 34, pp. 1056-
1069, 2008.
[113] J. Liu, W. Liu, H. Wang, T. Tao, and J. Zhang, "A novel envelope extraction
method for multichannel heart sounds signal detection," in 2011 International
conference on computer science and information technology, IPCSIT, 2012, pp.
630-638.
[114] C. Jarne, "Simple empirical algorithm to obtain signal envelope in three steps,"
arXiv preprint arXiv:1703.06812, 2017.
[115] L. A. Borowitz and W. J. Combs, "Implantable medical device with his-purkinje
activity detection," ed: Google Patents, 2010.
[116] P. W. Macfarlane and T. D. V. Lawrie, Comprehensive electrocardiology: theory
and practice in health and disease vol. 2: Pergamon, 1989.
[117] A.-R. LeBlanc and A. Mokrane, "Improved beat-to-beat timing measurements of
His-bundle signal," IEEE transactions on biomedical engineering, vol. 41, pp.
1168-1177, 1994.
[118] F. Kusumoto, "Procedural Issues for Electrophysiologic Studies: Vascular Access,
Cardiac Chamber Access, and Catheters," Understanding Intracardiac EGMs and
ECGs, pp. 1-14.
[119] W. Nafees, B. Riaz, N. Razzaq, W. Iftikhar, and T. Zaidi, "Classification of Atrio-
Ventricular Reentrant Tachycardia using intracardiac signals," in Bioinformatics
and Bioengineering (BIBE), 2013 IEEE 13th International Conference on, 2013,
pp. 1-5.
[120] A. C. Rankin, F. R. Quinn, and A. P. Rae, "Clinical cardiac electrophysiology," in
Comprehensive Electrocardiology, ed: Springer, 2010, pp. 1133-1161.
[121] S. Z. Mahmoodabadi, A. Ahmadian, M. Abolhassani, J. Alireazie, and P. Babyn,
"ECG arrhythmia detection using fuzzy classifiers," in Fuzzy Information
Processing Society, 2007. NAFIPS'07. Annual Meeting of the North American,
2007, pp. 48-53.
[122] B. Raghavendra, D. Bera, A. S. Bopardikar, and R. Narayanan, "Cardiac
arrhythmia detection using dynamic time warping of ECG beats in e-healthcare
systems," in World of Wireless, Mobile and Multimedia Networks (WoWMoM),
2011 IEEE International Symposium on a, 2011, pp. 1-6.
[123] B. Kamousi, B. Lin, A. Al-Ahmad, H. Hsia, P. Zei, A. Natale, et al., "A
covariance-based algorithm: a novel technique for rhythm discrimination in
ICDs," in Engineering in Medicine and Biology Society, 2008. EMBS 2008. 30th
Annual International Conference of the IEEE, 2008, pp. 5478-5481.
[124] D. G. Katritsis and A. J. Camm, "Classification and differential diagnosis of
atrioventricular nodal re-entrant tachycardia," Europace, vol. 8, pp. 29-36, 2006.
[125] D. G. Katritsis and A. J. Camm, "Atrioventricular nodal reentrant tachycardia,"
Circulation, vol. 122, pp. 831-840, 2010.
197
[126] M. Al Mehairi, S. Al Ghamdi, K. Dagriri, and A. Al Fagih, "Simultaneous
antegrade dual AV node conduction initiates AV nodal re-entrant tachycardia (a
rare initiation mechanism)," Journal of the Saudi Heart Association, vol. 25, pp.
35-37, 2013.
[127] Y. I. Alihanoglu, B. S. Yildiz, D. I. Kilic, H. Evrengul, and S. Kose, "Clinical and
Electrophysiological Characteristics of Typical Atrioventricular Nodal Reentrant
Tachycardia in the Elderly–Changing of Slow Pathway Location With Aging–,"
Circulation Journal, vol. 79, pp. 1031-1036, 2015.
[128] S. Dora, N. Namboodiri, A. Valaparambil, and J. Tharakan, "Induction of
atrioventricular nodal reentry tachycardia with intravenous adenosine," Singapore
medical journal, vol. 48, pp. e130-2, 2007.
[129] P. Weismüller, S. Kuly, B. Brandts, K. Kattenbeck, C. Ranke, and H. J. Trappe,
"Is electrical stimulation during administration of catecholamines required for the
evaluation of success after ablation of atrioventricular node re-entrant
tachycardias?," Journal of the American College of Cardiology, vol. 39, pp. 689-
694, 2002.
[130] K. Tanaka and Y. Watanabe, "Type A Wolff-Parkinson-White Syndrome
Generating an Antidromic Atrioventricular (AV) Reentrant Tachycardia (AVRT)
and an Orthodromic AVRT with a Long RP Interval Initiated only after
Incomplete Impairment of an AV Accessory Pathway," Journal of Arrhythmia,
vol. 27, pp. 137-144, 2011.
[131] M. E. Josephson, Clinical cardiac electrophysiology: techniques and
interpretations: Lippincott Williams & Wilkins, 2008.
[132] C. Buttà, A. Tuttolomondo, D. Di Raimondo, G. Milio, S. Miceli, M. T. Attanzio,
et al., "The supraventricular tachycardias: Proposal of a diagnostic algorithm for
the narrow complex tachycardias," Journal of cardiology, vol. 61, pp. 247-255,
2013.
[133] U. N. Kumar, R. K. Rao, and M. M. Scheinman, "The 12-lead electrocardiogram
in supraventricular tachycardia," Cardiology clinics, vol. 24, pp. 427-437, 2006.
[134] G. D. Veenhuyzen, F. R. Quinn, S. B. Wilton, R. Clegg, and L. B. Mitchell,
"Diagnostic pacing maneuvers for supraventricular tachycardias: Part 2," Pacing
and Clinical Electrophysiology, vol. 35, pp. 757-769, 2012.
[135] G. D. Veenhuyzen, F. R. Quinn, S. B. Wilton, R. Clegg, and L. B. Mitchell,
"Diagnostic pacing maneuvers for supraventricular tachycardia: part 1," Pacing
and Clinical Electrophysiology, vol. 34, pp. 767-782, 2011.
[136] H. Richard, Arrhythmias, 2007.
[137] D. A. Pijnappels, J. van Tuyn, T. A. de Vries, A. van der Laarse, E. E. van der
Wall, M. J. Schalij, et al., "Electrophysiology: Basic."
[138] N. Varma, "Left ventricular conduction delays induced by right ventricular apical
pacing: effect of left ventricular dysfunction and bundle branch block," Journal of
cardiovascular electrophysiology, vol. 19, pp. 114-122, 2008.
[139] H. Calkins, J. Sousa, R. El-Atassi, S. Rosenheck, M. De Buitleir, W. H. Kou, et
al., "Diagnosis and cure of the Wolff-Parkinson-White syndrome or paroxysmal
supraventricular tachycardias during a single electrophysiologic test," New
England Journal of Medicine, vol. 324, pp. 1612-1618, 1991.

198
[140] M. Sokolova and G. Lapalme, "A systematic analysis of performance measures
for classification tasks," Information Processing & Management, vol. 45, pp. 427-
437, 2009.
[141] S. Hargittai, "Is it possible to detect atrial fibrillation by simply using RR
intervals?," in Computing in Cardiology Conference (CinC), 2014, 2014, pp. 897-
900.
[142] G. Hayes and P. D. Teal, "Real-time detection of atrial fibrillation using a low-
power ECG monitor," in Computing in Cardiology Conference (CinC), 2013,
2013, pp. 743-746.
[143] J. R. Schaefer, D. Leussler, L. Rosin, D. Pittrow, and T. Hepp, "Improved
detection of paroxysmal atrial fibrillation utilizing a software-assisted
electrocardiogram approach," PloS one, vol. 9, p. e89328, 2014.
[144] J. F. Martin-Garcia, I. Mora-Jiménez, A. Garcia-Alberola, and J. L. Rojo-Alvarez,
"Cardiac arrhythmia discrimination using evolutionary computation," in
Computing in Cardiology Conference (CinC), 2014, 2014, pp. 121-124.
[145] J. SLOCUM, A. SAHAKIAN, and S. SWIRYN, "Computer Discrimination of
Atrial Fibrillation and Regular Atrial Rhythms from Intra‐Atrial Electrograms,"
Pacing and Clinical Electrophysiology, vol. 11, pp. 610-621, 1988.
[146] K. M. Ropella, A. V. Sahakian, J. Baerman, and S. Swiryn, "Effects of
procainamide on intra-atrial [corrected] electrograms during atrial fibrillation:
implications [corrected] for detection algorithms," Circulation, vol. 77, pp. 1047-
1054, 1988.
[147] J. Slocum, A. Sahakian, and S. Swiryn, "Diagnosis of atrial fibrillation from
surface electrocardiograms based on computer-detected atrial activity," Journal of
electrocardiology, vol. 25, pp. 1-8, 1992.
[148] M. A. Wood, P. Moskovljevic, B. S. Stambler, and K. A. Ellenbogen,
"Comparison of bipolar atrial electrogram amplitude in sinus rhythm, atrial
fibrillation, and atrial flutter," Pacing and Clinical Electrophysiology, vol. 19, pp.
150-156, 1996.
[149] K. Tateno and L. Glass, "Automatic detection of atrial fibrillation using the
coefficient of variation and density histograms of RR and ΔRR intervals,"
Medical and Biological Engineering and Computing, vol. 39, pp. 664-671, 2001.
[150] J. Millet-Roig, J. Rieta, V. Zarzoso, A. Cebrian, F. Castells, C. Sanchez, et al.,
"Surface-ECG atrial activity extraction via blind source separation: spectral
validation," in Computers in Cardiology, 2002, 2002, pp. 605-608.
[151] R. JJ, J. Millet-Roig, V. Zarzoso, F. Castells, С. Sánchez, R. García-Civera, et al.,
"Atrial Fibrillation, Atrial Flutter and Normal Sinus Rhythm Discrimination by
Means of Blind Source Separation and Spectral Parameters Extraction."
[152] J. Ng and J. J. Goldberger, "Understanding and interpreting dominant frequency
analysis of AF electrograms," Journal of cardiovascular electrophysiology, vol.
18, pp. 680-685, 2007.
[153] R. Latchamsetty and A. G. Kocheril, "Review of dominant frequency analysis in
atrial fibrillation," Arbor, vol. 1001, p. 48103, 2009.

199
[154] V. B. Traykov, R. Pap, and L. Sághy, "Frequency domain mapping of atrial
fibrillation-methodology, experimental data and clinical implications," Current
cardiology reviews, vol. 8, p. 231, 2012.
[155] T. H. Everett IV, L.-C. Kok, R. H. Vaughn, J. R. Moorman, and D. E. Haines,
"Frequency domain algorithm for quantifying atrial fibrillation organization to
increase defibrillation efficacy," Biomedical Engineering, IEEE Transactions on,
vol. 48, pp. 969-978, 2001.
[156] T. H. Everett, J. G. Akar, L.-C. Kok, J. R. Moorman, and D. E. Haines, "Use of
global atrial fibrillation organization to optimize the success of burst pace
termination," Journal of the American College of Cardiology, vol. 40, pp. 1831-
1840, 2002.
[157] P. Sanders, O. Berenfeld, M. Hocini, P. Jaïs, R. Vaidyanathan, L.-F. Hsu, et al.,
"Spectral analysis identifies sites of high-frequency activity maintaining atrial
fibrillation in humans," Circulation, vol. 112, pp. 789-797, 2005.
[158] A. Arenal, T. Datino, L. Atea, F. Atienza, E. González-Torrecilla, J. Almendral, et
al., "Dominant frequency differences in atrial fibrillation patients with and
without left ventricular systolic dysfunction," Europace, vol. 11, pp. 450-457,
2009.
[159] W.-C. Tsai and Y.-J. Lin, "The Frequency Analysis and the Atrial Fibrillation," J
Biocatal Biotransformation 1: 2. doi: 10.4172/2324-9099.1000 e108, 2012.
[160] Y.-J. Lin, C.-T. Tai, T. Kao, H.-W. Tso, S. Higa, H.-M. Tsao, et al., "Frequency
analysis in different types of paroxysmal atrial fibrillation," Journal of the
American College of Cardiology, vol. 47, pp. 1401-1407, 2006.
[161] J. J. Rieta, F. Castells, C. Sánchez, V. Zarzoso, and J. Millet, "Atrial activity
extraction for atrial fibrillation analysis using blind source separation," IEEE
Transactions on Biomedical Engineering, vol. 51, pp. 1176-1186, 2004.
[162] A. J. Camm, P. Kirchhof, G. Y. Lip, U. Schotten, I. Savelieva, S. Ernst, et al.
(2010). Guidelines for the management of atrial fibrillation. 31.
[163] K. Nagashima, Y. Okumura, I. Watanabe, T. Nakai, K. Ohkubo, T. Kofune, et al.,
"Effects of inter-electrode spacing on complex fractionated atrial electrograms
and dominant frequency detection," Journal of interventional cardiac
electrophysiology, vol. 34, pp. 51-57, 2012.
[164] G. W. Botteron and J. M. Smith, "A technique for measurement of the extent of
spatial organization of atrial activation during atrial fibrillation in the intact
human heart," Biomedical Engineering, IEEE Transactions on, vol. 42, pp. 579-
586, 1995.
[165] J. Ng, A. H. Kadish, and J. J. Goldberger, "Technical considerations for dominant
frequency analysis," Journal of cardiovascular electrophysiology, vol. 18, pp.
757-764, 2007.
[166] P. D. Welch, "The use of fast Fourier transform for the estimation of power
spectra: A method based on time averaging over short, modified periodograms,"
IEEE Transactions on audio and electroacoustics, vol. 15, pp. 70-73, 1967.
[167] S.-a. A. Sheikh, A. Z. Majoka, K. U. Rehman, N. Razzaq, and T. Zaidi,
"Nonparametric Spectral Estimation Technique to Estimate Dominant Frequency
200
for Atrial Fibrillation Detection," Journal of Signal and Information Processing,
vol. 6, p. 266, 2015.
[168] W. Li, C. Yang, Y. Wang, D. Wang, Y. Chen, and Z. Wu, "Several insights into
the preprocessing of electrograms in atrial fibrillation for dominant frequency
analysis," BioMedical Engineering OnLine, vol. 15, p. 1, 2016.
[169] M. S. Bartlett, "Smoothing periodograms from time series with continuous
spectra," Nature, vol. 161, pp. 686-687, 1948.
[170] K. Barbe, R. Pintelon, and J. Schoukens, "Welch method revisited: nonparametric
power spectrum estimation via circular overlap," IEEE Transactions on signal
processing, vol. 58, pp. 553-565, 2010.
[171] E. C. Ifeachor and B. W. Jervis, Digital signal processing: a practical approach:
Pearson Education, 2002.
[172] K. J. Blinowska and J. Zygierewicz, Practical Biomedical Signal Analysis Using
MATLAB®: CRC Press, 2011.
[173] A. V. Panfilov and A. V. Holden, Computational biology of the heart: Wiley,
1997.

201
All Praises and Thanks be to Allah






![Classification of Arrhythmia from ECG Signals using MATLAB€¦ · ECG signal and arrhythmia affected signal with 96.5% accuracy [26]. In the paper Detection of Cardiac Arrhythmia](https://static.fdocuments.us/doc/165x107/6017481464a3214e134e0e6f/classification-of-arrhythmia-from-ecg-signals-using-matlab-ecg-signal-and-arrhythmia.jpg)











