cardiac cycle
80
CARDIAC CYCLE Dr.Praveen Nagula ,1 st Year PG
-
Upload
praveen-nagula -
Category
Education
-
view
2.865 -
download
4
Transcript of cardiac cycle

CARDIAC CYCLE
Dr.Praveen Nagula ,1st Year PG

Carl John Wiggers Sir Thomas Lewis
Otto Frank Ernest H Starling

Adolf Eugen Fick
William Harvey
Willem Einthoven

IntroductionPrincipal function of cardiovascular system is to deliver oxygen
and nutrients to and remove carbon dioxide and wastes from metabolizing tissues.
It is by two specialized circulations in series1.a low resistance pulmonary driven by right heart2.a high resistance systemic driven by left heartSystolic pressure in the vascular system refers to the peak pressure reached during the systole,not the mean pressure.
The diastolic pressure refers to the lowest pressure during diastole.

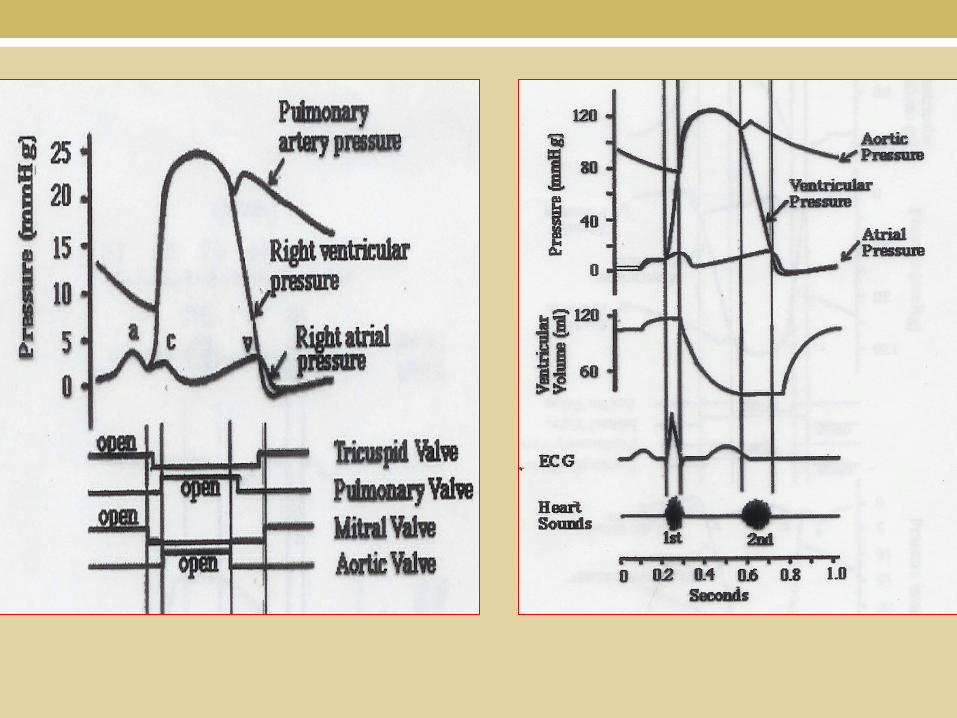
WIGGERS DIAGRAMEVENTS IN CARDIAC CYCLE DETERMINANTS OF MYOCARDIAL PERFORMANCEPRESSURE VOLUME LOOPPHYSIOLOGICAL VS PATHOLOGICAL HYPERTROPHY

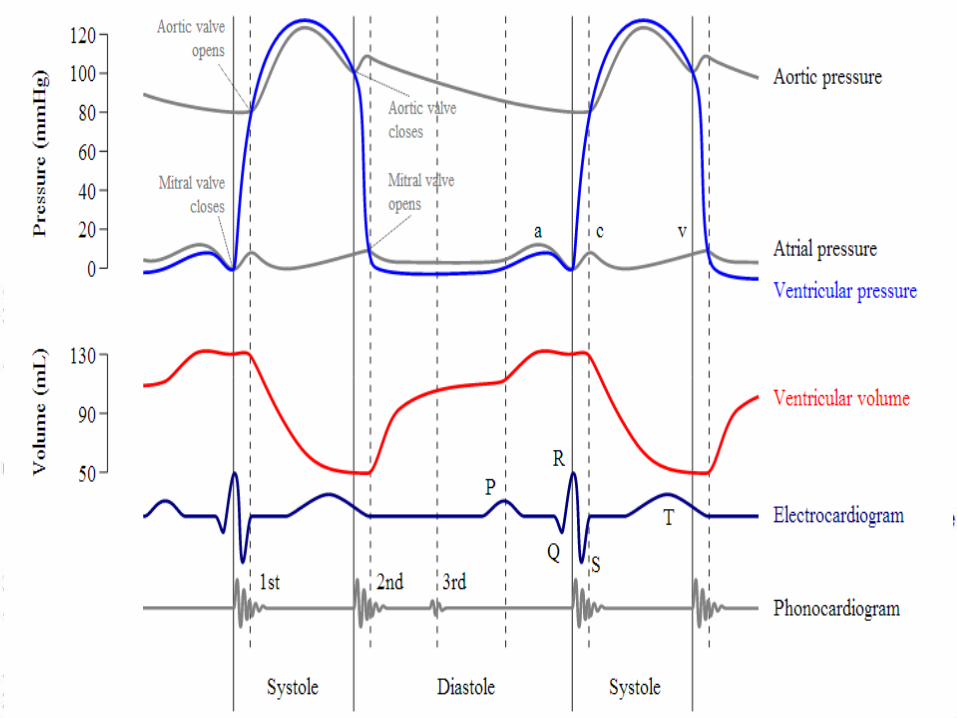
Wiggers diagram The X axis is used to plot time, The Y axis contains all of the following on a single grid:
Blood pressureAortic pressureVentricular pressureAtrial pressure
Ventricular volumeElectrocardiogramArterial flow (optional)Heart sounds (optional)JVP
Illustration of the coordinated events makes it easier to correlate the changes during the cardiac cycle.



WIGGERS DIAGRAMEVENTS IN CARDIAC CYCLE DETERMINANTS OF MYOCARDIAL PERFORMANCEPRESSURE VOLUME LOOPPHYSIOLOGICAL VS PATHOLOGICAL HYPERTROPHY

Electrical
events
of the
Cardiac
cycle

Cardiac cycle• The cardiac cycle describes pressure,volume and flow
phenomena in the ventricles as a function of time.• Similar for both LV and RV except for the timing,levels of
pressure.
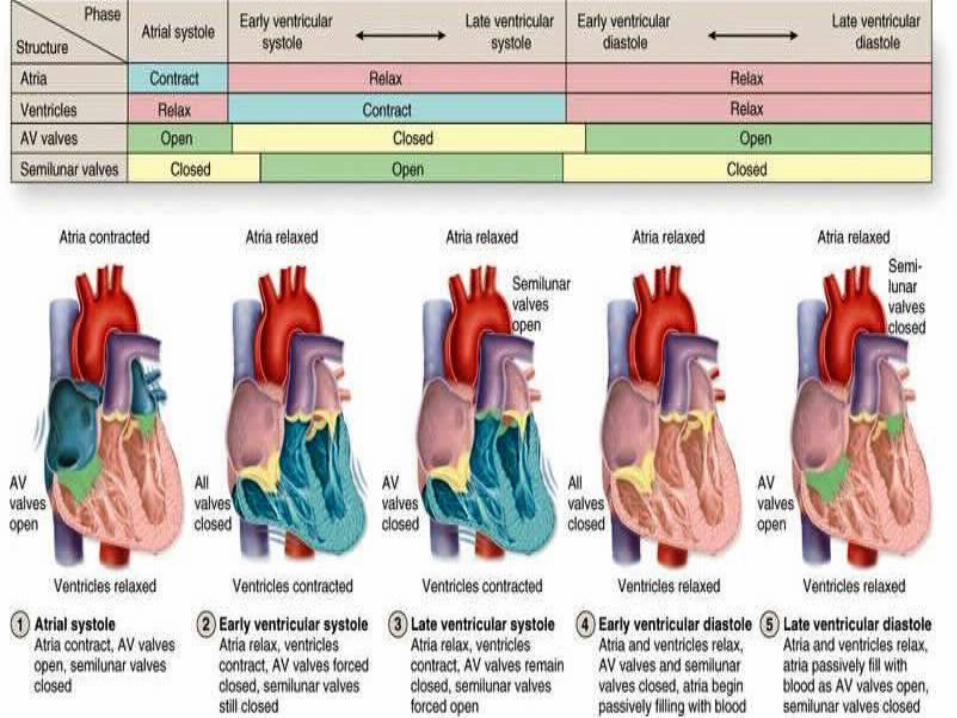
Mechanical events in Cardiac cycle
• Systole• Isovolumic contraction• Maximal ejection• Reduced ejection
• Diastole • Isovolumic relaxation• Rapid filling phase• Slow filling phase /diastasis• Atrial systole

• The letters are arbitrarily allocated so that atrial systole(a) coinicides with the a wave and (c ) with the c wave of JVP.
• Isovolumic contraction(b)
• Maximal Ejection( c)
LV CONTRACTION
• Isovolumic relaxation(e)
• Start of relaxation and reduced ejection (d)
LV RELAXATION
• Rapid phase(f)• Slow filling
(diastasis)(g)• Atrial systole or
booster(a)
LV FILLING

LV contraction• Actin myosin contraction triggered by arrival of Calcium ions
at contractile proteins.• ECG – peak of R wave• LV pressure >LA pressure (10-15mm Hg) • Followed approx. 50msec by M1.• Delay of M1 – inertia of the blood flow – valve is kept open.• Isovolumic contraction as volume is fixed.• Increased pressure as more fibers enter contractile state. • LV pressure >Aorta – Aortic valve opens – silent event
clinically.
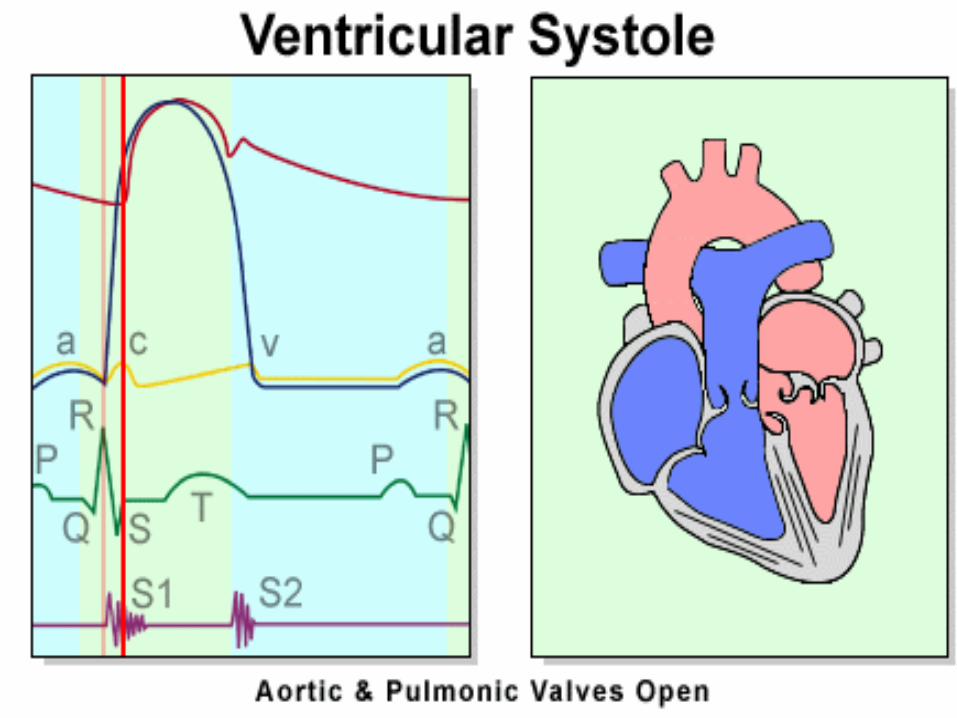

• Phase of rapid ejection:• Pressure gradient across the aortic valve• Elastic properties of aorta,arterial tree (systolic expansion)• LV pressure rises to peak and then falls.


LV relaxation• Activated phospholamban causes calcium transfer into SR.• Decreases contractile apparatus function – phase of reduced ejection –
blood flow from LV to aorta decreases but maintained by aortic recoil – WINDKESSEL EFFECT*.
• Aortic valve closes as LV pressure drops• Isovolumic relaxation• Mitral valve opens – clinically silent event.
† Giovanni Borelli,Stephen Hales,Fick(mathematical foundation).
†WINDKESSEL in german AIRCHAMBER or elastic resorvoir.

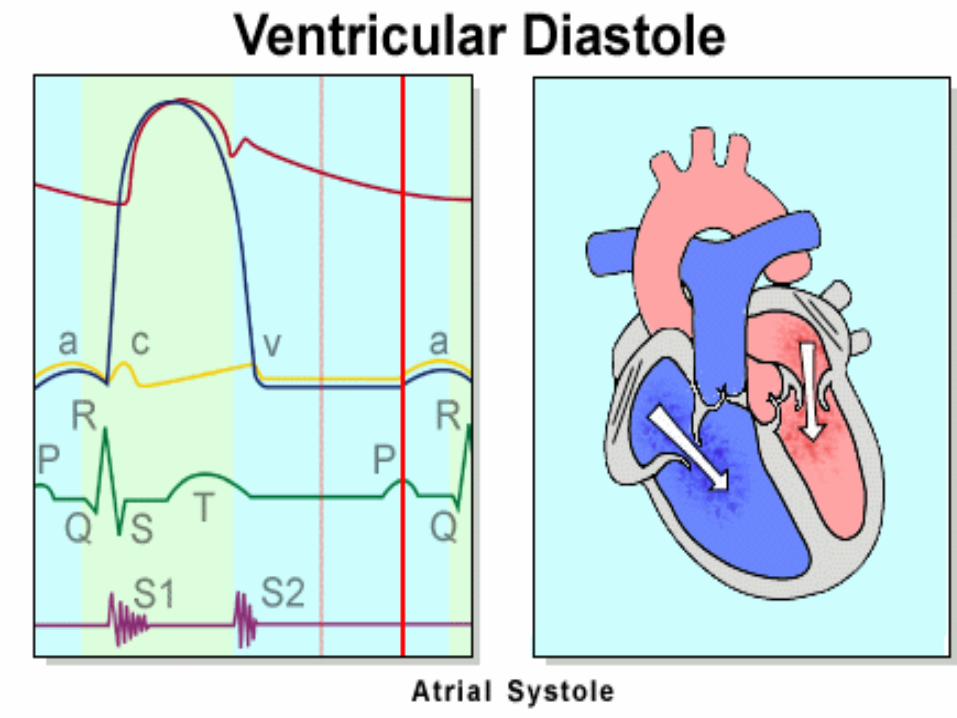
LV filling• Rapid filling phase – active diastolic relaxation of LV.• LA- LV pressures equalize - diastasis. • LA booster atrial systole – important in exercise and LVH.• First phase of diastole –isovolumic phase – no ventricular filling.• Most of ventricular filling –rapid filling phase.• Diastasis -5% • Final atrial booster phase -15%.• The sucking effect of ventricle – myosin is pulled into the space between the two anchoring segments of titin.• Dominant backward pressure wave –diastolic coronary filling.

Physiologic systole,diastole• It is related to the events occuring at the cellular level ,by
change of pressure and the electrical events.• Physiological systole –start of isovolumic contraction to the
peak of ejection phase.• Physiological diastole – commences as pressure falls.• Fits well in pressure volume curve .

Cardiological systole,diastole• It is related to the valve closures.• Systole – M1-A2 • Thereby starts later than physiological systole and ends later.• Diastole – A2-M1


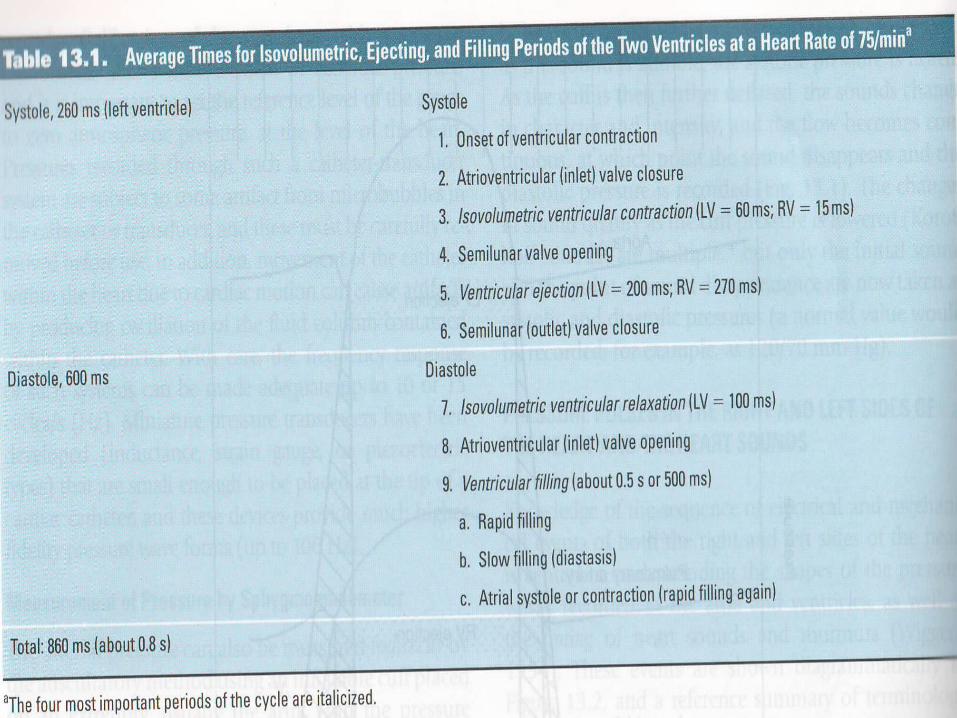
Protodiastole• Proto –means original,first• The period of start of ventricular relaxation.• Lasts until the semilunar valves are closed.• It is 0.04 sec.

ECHO cardiac cycleRapid filling phase of diastole
Atrial systole


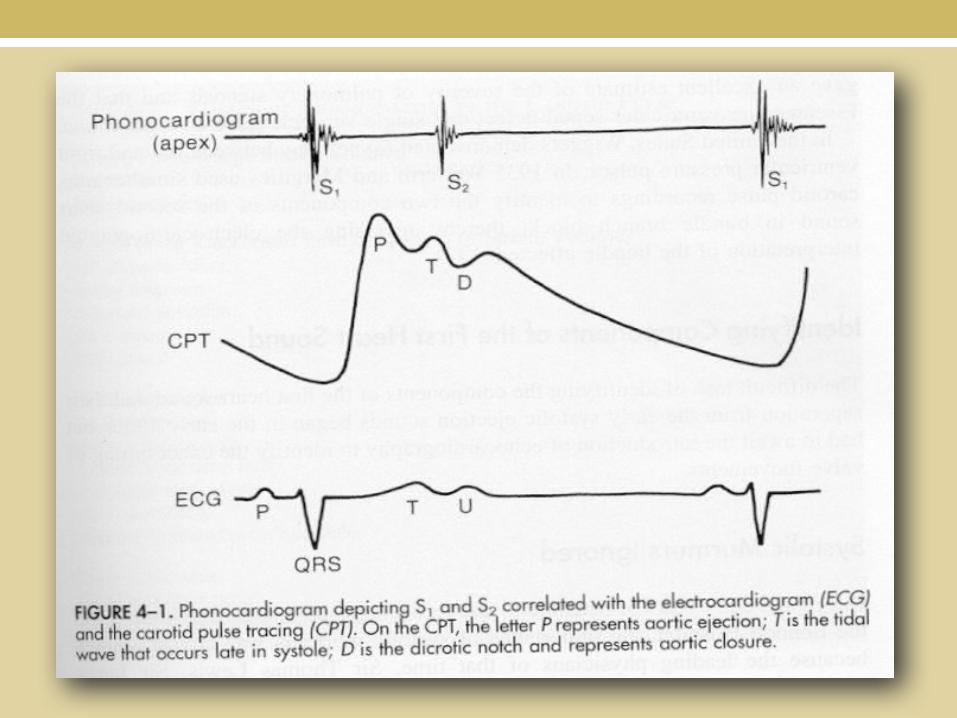
PhonocardiogramA graphic recording of cardiac soundA specially designed microphone on the chest wall.Sound waves amplified, filtered and recorded.
Doppler Echocardiography has replaced the phonocardiography

Carotid Pulse Tracing (CPT)Reflects the pressure and possible small volume changes
in a segment of the carotid artery with each cardiac cycle.
P (percussion wave) is the first peak and is related to aortic ejection. 80 msec after the first heart sound.
T (tidal wave) is the second wave and occurs late in systole.
D (dicrotic notch) coincides with aortic closure (A2), plus the traveling time of the pulse to the neck (.01-.05 sec).

Causes of Abnormalities in the Carotid Pulse

Jugular Venous Pulse tracing

JUGULAR VENOUS PULSE
Reflects volume change in the internal jugular vein and closely resembles the pressure changes in the right atrium.
A wave atrial contraction.C wave onset of ventricular contraction.X descent atrial diastole.V wave atrial filling before AV valves open.Y descent AV valves open filling of the ventricles.

Apex cardiogram

Apex cardiogramRecords low-frequency vibrations over the apical impulse.Deflections not delayed.A –atrial contraction.C –onset of LV contraction.E – peak of the ascent (initial ejection from LV to aorta)O – opening of the mitral valve.RF –rapid filling waveSF – slow filling wave.

WIGGERS DIAGRAMEVENTS IN CARDIAC CYCLE DETERMINANTS OF MYOCARDIAL PERFORMANCEPRESSURE VOLUME LOOPPHYSIOLOGICAL VS PATHOLOGICAL HYPERTROPHY

Determinants of myocardial mechanical performance
3 main determinants
Loading conditions
(preload,afterload)
Contractile state
Heart rate
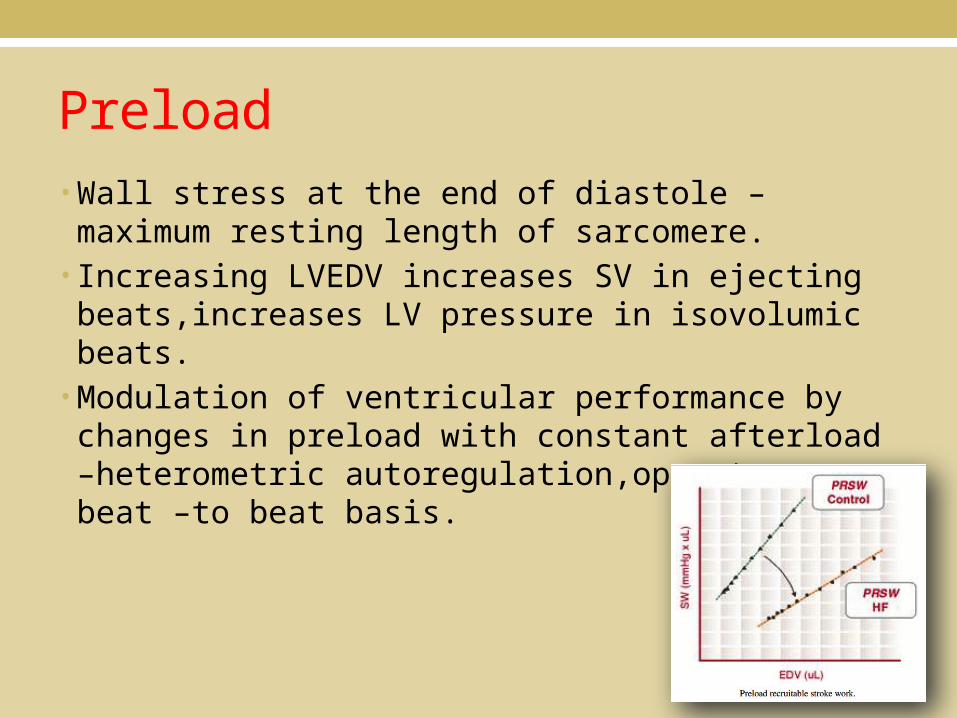
Preload• Wall stress at the end of diastole – maximum resting length of sarcomere.• Increasing LVEDV increases SV in ejecting beats,increases LV pressure in isovolumic beats.• Modulation of ventricular performance by changes in preload with constant afterload –heterometric autoregulation,operates on a beat –to beat basis.

Frank Starling mechanism• Starling – venous pressure in RA – heart volume • Within physiological limits – the larger the volume of the heart
–greater the energy of its contraction – the greater the amount of chemical change at each contraction.• LV volume – Cardiac Output• Stroke volume related to LVEDV – modern version• Real time 3D ECHO – global LV volume,endocardial function• LV volume surrogate markers – LVEDP ,PCWP.
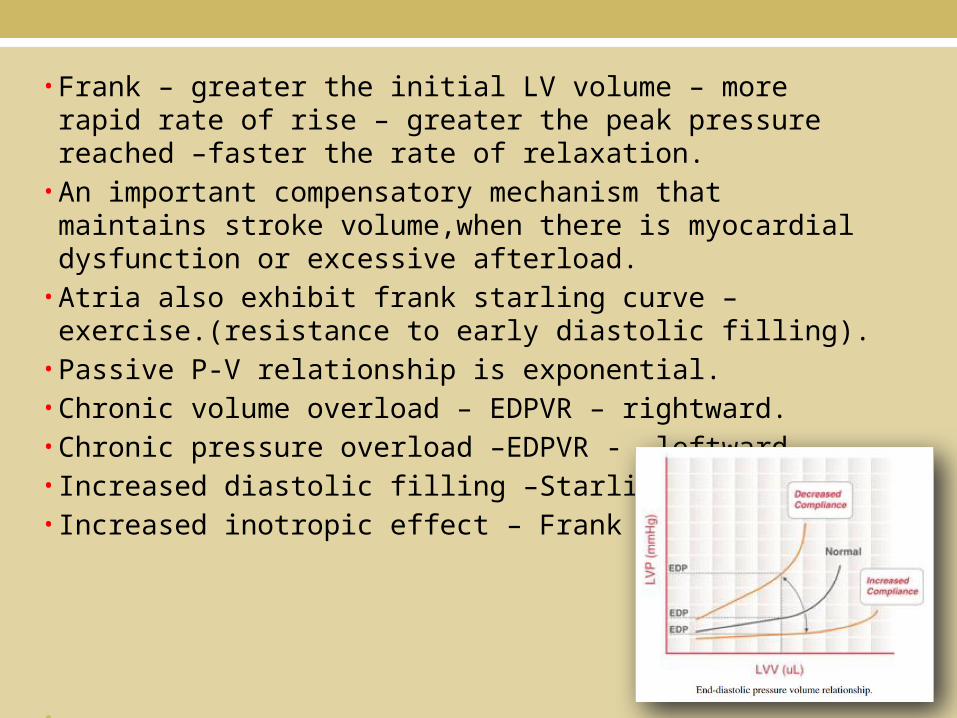
• Frank – greater the initial LV volume – more rapid rate of rise – greater the peak pressure reached –faster the rate of relaxation.• An important compensatory mechanism that maintains stroke
volume,when there is myocardial dysfunction or excessive afterload.• Atria also exhibit frank starling curve – exercise.(resistance to
early diastolic filling).• Passive P-V relationship is exponential.• Chronic volume overload – EDPVR – rightward.• Chronic pressure overload –EDPVR - leftward.• Increased diastolic filling –Starling.• Increased inotropic effect – Frank
•
Afterload Exact definition – wall stress during LV ejection.Tension in the LV wall that resists ventricular ejection or as the
arterial input impedance.In clinical practice the arterial blood pressure is often taken as
synonymous with afterload while ignoring aortic compliance (increase in stiff aorta).

Anrep effect• Homeometric autoregulation• Under experimental conditions
sudden marked increase in aortic pressure is produced,LVEDP initially rises and the stroke volume then recovers.• Increased LV wall tension –
increases Cytosolic Na - Calcium

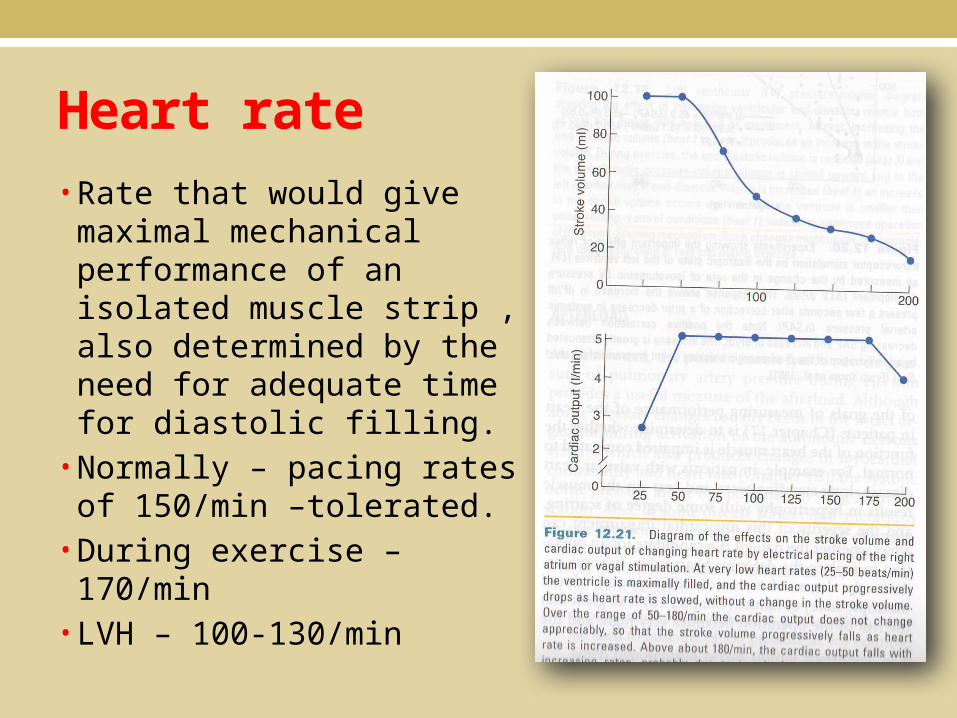
Heart rate• Rate that would give maximal
mechanical performance of an isolated muscle strip , also determined by the need for adequate time for diastolic filling.• Normally – pacing rates of
150/min –tolerated.• During exercise – 170/min• LVH – 100-130/min


Bowditch phenomenonTreppe effect Positive inotropic effect of activationForce freqeuncy relation• “increased heart rate – increases force of ventricular contraction”• HR – negative staircase effect• More rapid stimulation – more sodium and calcium ions enter the
myocardial cell that can be handled by sodium pump and the mechanisms for calcium exit - decreased force.
Clinical implicationsAF with varying interval.In HF – phenomenon is muted or lost.Post extrasystolic potentiation ,inotropic effect of paired pacing –
increased contractile state.


Contractility• It is the inherent capacity of the myocardium to contract independently of changes in the preload and afterload.• An increased contractile function –assosciated with greater degree of relaxation – LUSITROPIC effect• Important regulator of My02 uptake• Increased contractile function – exercise,adrenergic stimulation,digitalis,other inotropic agents.

Ventricular relaxationFour factors are of chief interest in influencing relaxation.1.cytosolic calcium must fall to cause the relaxation
phase(ATP,phospholamban).2.the inherent viscoelastic properties of the myocardium.
(hypertrophy)3.increased phosphorylation of troponin I enhances the rate of
relaxation.4.systolic load influences relaxation(increased systolic
load,increased lusitropic effect)(Brutsaert).
Impaired relaxation is an early event of angina pectoris(decreased ATP –decreased early diastole filling).
-dp/dt = (rate of isovolumetric relaxation)* *Glanz method P(t)= P0e-t⁄τE +Pα
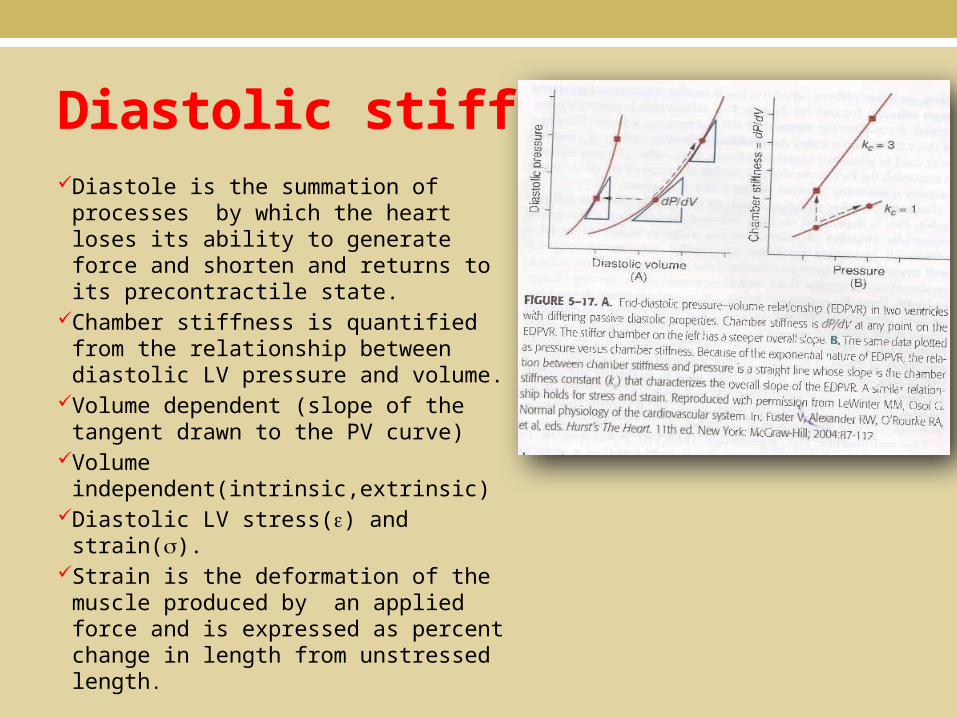
Diastolic stiffnessDiastole is the summation of
processes by which the heart loses its ability to generate force and shorten and returns to its precontractile state.
Chamber stiffness is quantified from the relationship between diastolic LV pressure and volume.
Volume dependent (slope of the tangent drawn to the PV curve)
Volume independent(intrinsic,extrinsic)
Diastolic LV stress() and strain().Strain is the deformation of the muscle
produced by an applied force and is expressed as percent change in length from unstressed length.


Time varying elastance conceptVentricular volume and loading are altered under conditions of
unvarying contractility.(frank starling preparations are load independent).
At any time t,following the onset of contraction,the P-V relation is linear
P(t) = E(t)-{V(t)-Vo},E –time varying elastance,Vo is volume at zero pressure or dead volume.
Ventricle behaves like a spring with a stiffness(elastance) that increases during contraction,decreases during relaxation.
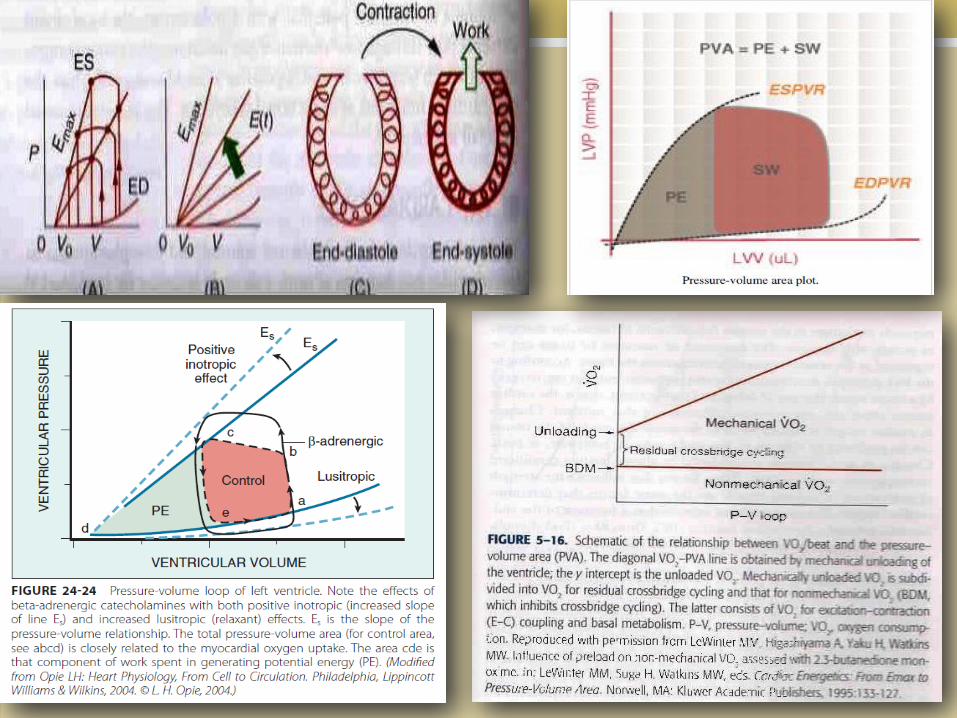
PVA area bounded by the LV P-V loop is a measure of the total mechanical energy of LV contraction.

FormulaeEjection fraction = (stroke volume/end diastolic
volume100). Wall tension = (P.r)/2h(P pressure,r radius,h wall
thickness)EA = PES/SV , [E- effective arterial resistance,PES-end
systolic pressure,SV- stroke volume}.EA/Ees ratio (index of ventriculo arterial coupling,pump
performance).Fick equation VO2 = Q(AVO2)V/P = compliance.P/V =stiffnessCardiac output = stroke volumeHRPVA = PE+SWPE = PES(VES-V0)/2 – PED(VED-V0)/4PVA MV02

Normal values
PRESSURES (mm Hg)
Right atrium mean 0-5
a wave 1-7
v wave 1-7
Right ventricle peak systolic/end diastolic 17-32/1-7
Pulmonary artery peak systolic/end diastolic 17-32/1-7
mean 9-19
PCWP 4-12
LA mean 4-12
a wave 4-15
v wave 4-15
LV peak systolic/end diastolic 90-140/5-12
Aorta peak systolic/end diastolic 90-140 /60-90
mean 70-105
Resistance (dynes/cm2) SVR 900-1400
PVR 40-120
Oxygen consumption index (L-min/m2) 115-140
Cardiac index (L-min/m2) 2.8-4.2

WIGGERS DIAGRAMEVENTS IN CARDIAC CYCLE DETERMINANTS OF MYOCARDIAL PERFORMANCEPRESSURE VOLUME LOOPPHYSIOLOGICAL VS PATHOLOGICAL HYPERTROPHY

Pressure volume loop• Best of the current approaches to the assessment of the
contractile behaviour of the intact heart.• Es,the pressure – volume relationship .• Changes in the slope of this line joining the different Es points
are generally good load independent index of the contractile performance of the heart.• Enhanced inotropic effect, Es shifted upward and to the left.• Lusitropic effect shifted Es downward and to right.• The P-V relationship is linear in smooth muscle,curvilinear in
cardiac muscle(exponential).




Atrial Pressure Volume Loop

Atrial function1.Blood receiving reservoir chamber2.contractile chamber (booster pump)3.conduit4.volume sensor of the heart (ANP) – diuresis.5.mechanoreceptors (Bainbridge reflex – VR - HR).
Rapid atrial repolarization – increased Ito ,I K Ach.During atrial pacing,the preload is increased and the atria are
distended,so that the volume part of the loop is small and the pressure part of the loop is much enlarged.

Pressure volume loop diagram in various pathological scenarios
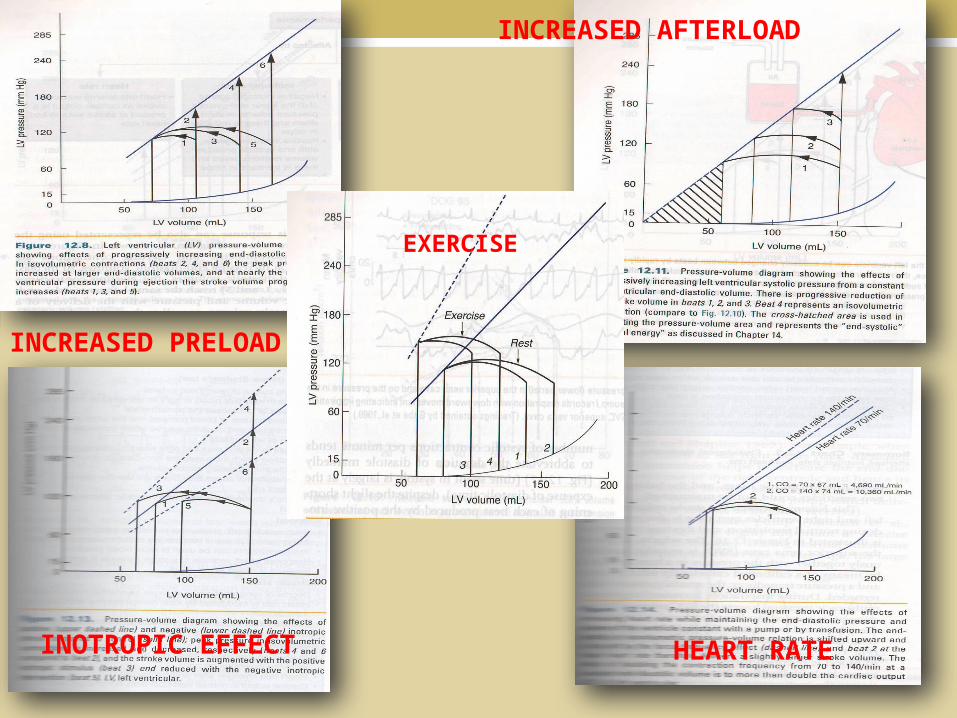
INCREASED PRELOAD
INCREASED AFTERLOAD
INOTROPIC EFFECT HEART RATE
EXERCISE


WIGGERS DIAGRAMEVENTS IN CARDIAC CYCLE DETERMINANTS OF MYOCARDIAL PERFORMANCEPRESSURE VOLUME LOOPPHYSIOLOGICAL VS PATHOLOGICAL HYPERTROPHY
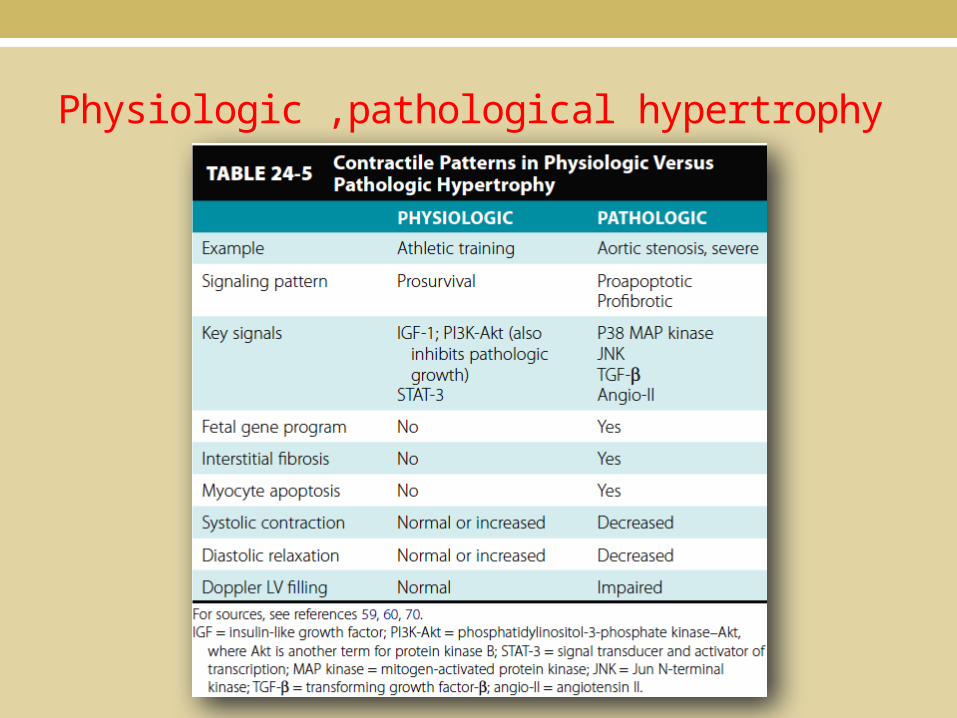
Physiologic ,pathological hypertrophy

Meerson,studied the cardiac hypertrophic response to experimental constriction of aorta.- compensatory hypertrophy.
Increased wall stretch,as a result of an increased intraventricular LV pressure (Systolic stress correction hypothesis,Grossman)- myocytes grow in width and thicken.
Benefici
al
hypertroph
y
Pathological hypertrophyResponse to a sustained
LV pressure overload
ERK,Akt(protein kinaseB)P38MAPkinase,JNK,TGF-B

Chronic elevation of the preload was associated with Akt activation without fibrosis,little apoptosis,better function,and lower mortality.
Chronic elevation of afterload (AS) caused maladaptive hypertrophy,increased fibrosis,rapid failure,increased mortality.
Increased release of angiotensin II from myocardium.TGF B maldaptive hypertrophy in AS (diastolic dysfunction)Cardiac steatosis in insulin resistance – increased TG


Isometric versus isotonic contractionAn isometric exercise is a form of exercise involving the static
contraction of a muscle without any visible movement in the angle of the joint.
The term "isometric" combines the Greek words "isos" ("equal" or "same") and "metron" ("distance" or "measure"), meaning that in these exercises the length of the muscle and the angle of the joint do not change, though contraction strength may be varied.
This is in contrast to isotonic contractions, in which the contraction strength does not change, though the muscle length and joint angle do.


WIGGERS DIAGRAMEVENTS IN CARDIAC CYCLE DETERMINANTS OF MYOCARDIAL PERFORMANCEPRESSURE VOLUME LOOPPHYSIOLOGICAL VS PATHOLOGICAL HYPERTROPHYRV CARDIAC CYCLE

RV cycle
References1.Ganong’s Review of Medical Physiology,24th Edition.2.Guyton and Hall,Textbook of Medical Physiology.3.Best and Taylor’s Physiological Basis of Medical
Practice,13th edition.4.HURST’S,THE HEART ,13th edition 5.Braunwald’s Heart Disease,9th edition6.Circulation Journal.7.European Heart Journal.
THE WONDERFUL DAY
11-12-13