Arrhythmia and cardiac defects are a feature of spinal muscular
Upload
fran-Category
view
305download
5description


CARDIAC ARRHYTHMIA RESEARCH ADVANCES
No part of this digital document may be reproduced, stored in a retrieval system or transmitted in any form orby any means. The publisher has taken reasonable care in the preparation of this digital document, but makes noexpressed or implied warranty of any kind and assumes no responsibility for any errors or omissions. Noliability is assumed for incidental or consequential damages in connection with or arising out of informationcontained herein. This digital document is sold with the clear understanding that the publisher is not engaged inrendering legal, medical or any other professional services.


CARDIAC ARRHYTHMIA RESEARCH ADVANCES
LYNN A. VESPRY EDITOR
Nova Biomedical Books New York

Copyright © 2007 by Nova Science Publishers, Inc. All rights reserved. No part of this book may be reproduced, stored in a retrieval system or transmitted in any form or by any means: electronic, electrostatic, magnetic, tape, mechanical photocopying, recording or otherwise without the written permission of the Publisher. For permission to use material from this book please contact us: Telephone 631-231-7269; Fax 631-231-8175 Web Site: http://www.novapublishers.com
NOTICE TO THE READER The Publisher has taken reasonable care in the preparation of this book, but makes no expressed or implied warranty of any kind and assumes no responsibility for any errors or omissions. No liability is assumed for incidental or consequential damages in connection with or arising out of information contained in this book. The Publisher shall not be liable for any special, consequential, or exemplary damages resulting, in whole or in part, from the readers’ use of, or reliance upon, this material. Independent verification should be sought for any data, advice or recommendations contained in this book. In addition, no responsibility is assumed by the publisher for any injury and/or damage to persons or property arising from any methods, products, instructions, ideas or otherwise contained in this publication. This publication is designed to provide accurate and authoritative information with regard to the subject matter covered herein. It is sold with the clear understanding that the Publisher is not engaged in rendering legal or any other professional services. If legal or any other expert assistance is required, the services of a competent person should be sought. FROM A DECLARATION OF PARTICIPANTS JOINTLY ADOPTED BY A COMMITTEE OF THE AMERICAN BAR ASSOCIATION AND A COMMITTEE OF PUBLISHERS. Library of Congress Cataloging-in-Publication Data Cardiac arrythmia research advances / Lynn A. Vespry (editor). p. ; cm. Includes bibliographical references and index. ISBN-13: 978-1-60692-539-3 1. Arrhythmia. I. Vespry, Lynn A. [DNLM: 1. Arrhythmia. WG 330 C26495 2007] RC685.A65C244 2007 616.1'28--dc22 2007021195
Published by Nova Science Publishers, Inc. New York

Contents
Preface vii
Expert Commentary
Commentary A Collateral Damage? 1 Carole C. Anderson
Short Communication The Promise of Biological Pacemakers 5
Alistair Lindsay
Chapter I Unravel the Complexity of Heart Rhythm: Modeling Approach 9 Jie Lian
Chapter II The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 33 Carole C. Anderson
Chapter III Autonomic Nervous System and Cardiac Arrhythmias 73 Maurizio Acampa, Maura Lamarina, Luca Puccetti, Francesca Guideri and Alberto Auteri
Chapter IV External Triggering, Modifying and Chronobiologic Factors for Ventricular Arrhythmias 93 Viktor Čulić
Chapter V Cardioembolism Prophylaxis in Non Valvular Atrial Fibrillation (NVAF): Medical Treatment, Pacing and Beyond 137 F. Corea, MA.Abbas, M.Cascelli, S. Micheli, M. Sessa, S.Benussi and G. Comi
Chapter VI Management of Wolff-Parkinson-White Syndrome 159 Béatrice Brembilla-Perrot

Lynn A. Vespry vi
Chapter VII Focus on Amiodarone in Prevention and Treatment of Cardiac Arrhythmia 177 J. Auer and B. Eber
Chapter VIII Ongoing Atrial Remodeling in Permanent Atrial Fibrillation: Value of Brain Natriuretic Peptide Monitoring for High-Risk Patient Identification 203 John Dernellis and Maria Panaretou
Chapter IX Cardiac Involvement in Parkinson’s Disease 217 Carl-Albrecht Haensch
Chapter X A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution Index Derived from Arterial Waveform Trace Obtained from Pulse Oximetry Signal – Feasibility, Reproducibility and Sensitivity to Acute Hemodynamic Interventions 231 Miroslav Mestan and Jiri Kvasnicka
Chapter XI Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 287 Tomás Muñoz
Index 327

Preface Cardiac arrhythmia is a term that denotes a disturbance of the heart rhythm. Cardiac
arrhythmias can range in severity from entirely benign to immediately life-threatening. A cardiac arrhythmia, also called cardiac dysrhythmia, is a disturbance in the regular rhythm of the heartbeat. Several forms of cardiac arrhythmia are life-threatening and a medical emergency. Cardiac arrhythmias sometimes are classified according to their origin as either ventricular arrhythmias (originating in the ventricles) or supraventricular arrhythmias (originating in heart areas above the ventricles, typically the atria). They also can be classified according to their effect on the heart rate, with bradycardia indicating a heart rate of less than 60 beats per minute and tachycardia indicating a heart rate of more than 100 beats per minute. This book presents new and important research in the field including an Expert Commentary on collateral damage.
Chapter I - The heart has a unique electrical system that controls the rhythm of the heartbeat. In a healthy heart, the sinoatrial (SA) node in the right atrium serves as the natural pacemaker, which generates rhythmic electrical pulses that spread across both atria. These electrical pulses are relayed to the ventricles via the atrio-ventricular junction (AVJ), a nodal structure that has complex electrophysiological properties. From the AVJ, the electrical signals travel along specialized conduction pathways that spread into the ventricles, causing them to contract and pump blood into the lungs and throughout the body.
Structural or functional abnormalities of the cardiac electrical conduction system can lead to heart rhythm disorders, or cardiac arrhythmias. Cardiac arrhythmias can result from disorders of impulse formation, impulse conduction or a combination of both. Disturbances in impulse formation involve too slow or too fast heart rate as a result of diseased SA node, or due to the development of an ectopic focus that takes over control of the intrinsic rhythm. Disorders in impulse conduction involve heart blocks, which result in slowed or blocked conduction through the myocardium. In addition, the pathological process of reentry is also an impulse conduction abnormality.
The artificial cardiac pacemaker is a medical device that controls the heartbeat. By delivering appropriately timed electrical impulses to the heart, the implantable pacemaker is a proven technology that treats various types of cardiac arrhythmia. Despite the progress of cardiac arrhythmia research and the advance of the pacemaker technology, much remains unknown about how the external pacing interacts with the heart’s intrinsic signal.

Lynn A. Vespry viii
Consequently, from the rhythm analysis perspective, the complexity of heart rhythm is further compounded by the consideration of cardiac pacing.
In this chapter, a model-based approach is introduced to unravel the complex heart rhythm in both physiological and pathological conditions, by taking into account the cardiac pacing. In this model, the intrinsic heart rhythm generator, the cardiac conduction pathway, and the external cardiac pacemaker are integrated into a closed-loop system. Examples are presented to illustrate how to use this model to generate and interpret various heart rhythms. The scientific merits and potential applications of this model are also discussed.
Chapter II - To prevent sudden cardiac death an increasing number of implantable cardioverter defibrillators (ICD) are implanted in people who are at risk of life-threatening arrhythmias. Research results demonstrate this rapidly expanding bio-electronic treatment remains poorly understood by recipients, their family members and by health professionals. Research into both the efficacy of ICDs and the degree of acceptability to recipients, family members and health professionals has provided equivocal results. Yet there has been little research designed to explore the essence of what it means to live with the effects of ICD bio-electronics and so health professionals involved in heart implantation with an ICD may discuss efficacy with recipients and their family members but have little other evidence to facilitate informed decision-making.
This chapter draws upon the results of a major research project that focused on the phenomenon of implantation of a person’s heart with a permanent bio-electronic ICD. Implantation was explored through the existential perspectives of participants from four groups: recipients of ICDs, family members of recipients; cardiac nurses and paramedical personnel; and cardiologists.
Hermeneutical phenomenological methods, including unstructured in-depth dialogue; content and thematic analysis of participants’ lived-through experiences; interpretation of authentic dialogue from participants’ drawing on literature, poetry, art; and the idiomatic meaning of words relating to the heart; were used in the research. The findings from this research are expressed in terms of how participants experienced body-liminality in many existential ways. The phenomenon of heart implantation with an ICD, is an experience of liminality; recipients live on the threshold of life and death and all participants’ lives are influenced by a betwixt/between liminal-perspective. Moreover, heart implantation with an ICD impacts on lived-temporality/time; lived-spatiality/movement; lived-emotionality; lived-sexuality/gender; and lived-relationality. Recipients and their family members experience a sense of security because the device is in place but this is always counterbalanced by the experience of dying and being revived multiple times or always being on the threshold of that experience.
This chapter explicates body-liminality as represented in the research results, giving powerful yet poignant exemplars from the dialogue of recipients, family members and health professionals. The chapter concludes with a discussion on how this information can be used to improve education, informed consent, negotiation, and support, in the care of patients with life threatening arrhythmias who are being considered for heart implantation with an ICD. Furthermore, this chapter can be a source of enlightenment for health professionals who may have dilemmas in relation to heart implantation with the bio-electronic ICD.

Preface ix
Chapter III - Autonomic nervous system activity exerts a potent influence on arrhythmogenesis. Regulation of cardiac neural activity is highly integrated and is achieved by circuitry at multiple levels. In recent years non-invasive techniques based on the electrocardiogram (ECG) have been used as markers of autonomic modulation of the heart, these include heart rate variability (HRV), baroreflex sensitivity (BRS), QT interval, and heart rate turbulence (HRT), a new method based on fluctuations of sinus rhythm cycle length after a single premature ventricular contraction. Among these techniques analysis of HRV has emerged as a simple, non-invasive method to evaluate the sympatho-vagal balance at the sinoatrial level.
The actual mechanisms by which the autonomic nervous system causes or prevents fibrillation, particularly in the ventricles, are complex. The neurotransmitters epinephrine and norepinephrine activate cardiac adrenergic receptors, with stimulation of G protein adenylyl-cyclase-cAMP protein kinase A pathway to alter the activity of a number of ion channels and transporters.
Cardiac sympathetic nerves are highly plastic and the coexistence of denervated and hyperinnervated area in the diseased myocardium could result in increased electrophysiological heterogeneity during sympathetic activation that can provoke ventricular arrhythmias via several mechanisms, including reentry, enhanced and abnormal automaticity, and triggered activity. Of these mechanisms, abnormal automaticity and triggered activity have most often been cited as causal factors of exercise-induced arrhythmias in subjects without organic heart disease also.
In particular, sympathetic nervous system activity may participate in the genesis of ventricular arrhythmias with short term effects (with enhancement of early and delayed afterdepolarizations and increased dispersion of repolarization) and long term effects (resulting in apoptosis, hypertrophy, fibrosis and sympathetic nerve sprouting).
In contrast to sympathetic stimulation, parasympathetic activity appears to protect the heart against arrhythmias. Vagal activity influences both ionotropic and chronotropic properties of the ventricular myocardium, increasing the threshold of the vulnerable period with the antifibrillatory effect.
Abnormalities of the autonomic nervous system have been demonstrated in diverse conditions such as diabetic neuropathy, coronary heart disease, heart failure, stroke: a dysregulation in the autonomic nervous control of the cardiovascular system associated to increased sympathetic and reduced parasympathetic tone plays an important role in coronary artery disease and in the genesis of life-threatening ventricular arrhythmias.
Chapter IV - Research on cardiac arrhythmias includes a variety of fields, levels and techniques. From the clinician’s point of view, an increasing awareness concerning external circumstances and events, and other exogenous factors that may be implicated in the triggering of cardiac arrhythmias make it important to provide appropriate recommendations for prevention in the patients suffering from arrhythmia.
A physiological adaptive response to the wide range of everyday situations and activities involves activation of the sympathetic nervous system. In susceptible patients with ischemic or other structural heart disease, sympathetic activation results in heterogeneous rather than homogeneous sympathetic activity which seems to be an important pathophysiologic event for the initiation of cardiac arrhythmias. Emotional stressors and physical activity are the best

Lynn A. Vespry x
described triggers caused by sympathetic arousal, while reports describing individuals experiencing ventricular arrhythmias after drinking caffeine or alcoholic beverages need further support using controlled data. An association with arrhythmia has also been reported for two groups of environmental factors, air pollutants and meteorologic variables. However, pathophysiologic mechanisms through which higher levels of sulfate, nitrogen dioxide, carbon monoxide, black carbon, and fine particle mass as well as very weak or very strong winds, periods of rising relative air moisture and falling atmospheric pressure may cause arrhythmia deserve further consideration.
Whilst external triggers increase the risk of arrhythmia within the time frame of several hours after exposure, modifying factors probably alter individual susceptibility to external triggers. Gender, age, psychosocial factors, polyunsaturated fatty acids, digitalis, beta-blocking and other antiarrhythmic therapy seem to be modifying factors that most significantly impact the myocardial vulnerability. Beyond all external and modifying influences and despite the fact that external triggers most likely occur randomly throughout time, diurnal, weekly and seasonal chronobiologic phenomena of variation in incidence of cardiac arrhythmias do exist. Regardless of population or climate, arrhythmic events tend to occur more frequently in the morning, on Mondays, and during the winter months, but the reasons for such a distribution are still speculative.
We must yet discover the precise processes included in the transition from the single ventricular ectopic beat all the way to malignant ventricular arrhythmias. Future investigations of external triggering, modifying and chronobiologic factors as well as measures and therapies aimed at blocking the adverse effects of these factors may improve prevention of cardiac arrhythmias and sudden cardiac death.
Chapter V - The great relevance of electrical cardiac stimulation has been recognized since the 50s when the first successful cardiac resuscitation by external stimulation was reported. In the last decades all over the world, millions of subjects with cardiac arrhythmias had been treated with pacemakers (PMs). Cardioembolism, often due to supraventricular arrhythmias, is one of the major killers in cerebrovascular diseases. In, age-adjusted, industrialized population, cardioemboli have the highest incidence rates, highest case fatalities as well as recurrence rates. Large prospective randomised trials demonstrated that anticoagulation with cumarins reduces the risk of ischemic stroke in high risk patients with AF by nearly 70%. Despite clear guidelines, there is evidence that anticoagulation is under used in patients with atrial fibrillation in a variety of clinical settings. Recent prospective clinical trials have demonstrated that more physiologic pacing mode (DDD) reduces the risk of atrial fibrillation (AF) compared to single chamber ventricular pacing (VVI) in patients with sinus node disease (SND). Previous studies have shown using PM diagnostic counter how, on a 5-year follow up, AF episodes have prevalence up to 40% in PM patients. Anticoagulation treatment for systemic embolic prevention should be considered in those patients who have a prior history of AF or device detected AF episodes. Unfortunately stroke prevention in pacemaker patients is far to be satisfactory according to recent surveys and should thereby be further optimised. PM patients are under close follow up, cardiac rhythm can be checked with feasible procedures thus guidelines need to be better attended.
A novel concept for prevention of embolic stroke is based on the use of metallic fine-wire tubular prosthesis, to avoid penetration of emboli originating from proximal sources into

Preface xi
the internal carotid artery. Blood can flow through the ‘protected’ artery into the brain, whereas the migration of emboli to the brain is avoided.
Closing the Left Atrial Appendage (LAA) might be another potential alternative in subjects who cannot take anticoagulants because of contraindications. First attempts at LAA exclusion were reported by cardiac surgeons either during open heart surgery or with a thoracoscopic intervention. Other techniques consists in the deployment of a self-expandable nitinol cages. It is delivered via a transseptal sheath. Small anchors along the struts prevent from embolization. Recently developed surgical instruments now enables thoracoscopic approaches, facilitating extension of epicardial AF ablation and excision of the left atrial appendage to patients with isolated AF
Still under appraisement whether similar surgical procedures are cost effective with the medical treatments to prevent embolic events.
Chapter VI - Sudden death (SD) might complicate the follow-up of patients with the Wolff-Parkinson-White syndrome (WPW) and might be the first event in patients with asymptomatic WPW. In these last patients, 7 to 63 year old, the reduction of the risk of life-threatening arrhythmias event by accessory pathway (AP) radiofrequency (RF) ablation was reported in 2003.
The risks of SD are increased in some clinical situations. Noninvasive studies are unable to predict correctly the risk of SD. The electrophysiological study (EPS) is the best means to detect the risk of life-threatening arrhythmias and evaluate the nature of the symptoms
The EPS methods used to study the WPW are well-defined. The maximal rate of conduction through the AP is evaluated and programmed atrial stimulation is used to determine the AP refractory period and to induce a tachycardia. These methods are performed in control state and repeated in adrenergic situation either during exercise test or during a perfusion of isoproterenol. The results of EPS differ with the methods used by authors. The incidence of atrial fibrillation (AF) induction is lower in transesophageal studies than in intracardiac studies. The incidence of atrioventricular re-entrant tachycardia (AVRT) induction is similar with both routes of study, low in asymptomatic patients (15%) and high in symptomatic patients (more than 80%). The induction of AF rapidly conducted through the AP (> 240 beats/min in control state, > 300 b/min after isoproterenol) is the sign of a WPW at risk of life-threatening arrhythmias, but the induction of AVRT is now also considered in association with the AP refractory period as a risk factor. The electrophysiological data differed according to the age of the patient with a shorter AP refractory period and a lower risk of AF induction in young patients than in adults but the total number of potentially dangerous forms did not change significantly during the life.
AP RF ablation is now considered the first line of treatment of symptomatic patients and asymptomatic patients with inducible rapid tachycardia.
Some controversies still exist as the limits of age to indicate EPS in asymptomatic patient, classically 6– to 35 years, but older adults and elderly have still a risk of serious arrhythmia as the first event and the minimal age to indicate AP RF ablation because of the risks of the procedure in young children.
Chapter VII - There is good evidence that amiodarone is effective against a variety of arrhythmias and that it possibly is superior to other drugs in some settings. Thus, amiodarone is currently the leading antiarrhythmic drug because of proven efficacy and safety. The

Lynn A. Vespry xii
electrophysiological actions of amiodarone are complex and incompletely understood. It has generally been classified as a Vaughan-Williams class III agent (Table 1), prolonging repolarization by inhibition of outward potassium channels. Amiodarone is particularly useful because its safety has been clearly demonstrated by a large body of evidence, including
several randomized trials. Compared with many other antiarrhythmic drugs, amiodarone causes few cardiovascular adverse effects; however, its overall tolerance is limited by considerable noncardiac toxicity. Although amiodarone will continue to give way to the implantable cardioverter defibrillator (ICD) as primary therapy for many patients presenting with sustained ventricular tachycardia (VT) or ventricular fibrillation (VF), it is likely that amiodarone use will continue in ICD patients to prevent ICD discharges. Pharmacological
therapy remains the major approach to management of AF, and use of amiodarone is likely to increase in future years. This review will analyze the evidence that amiodarone is a safe and effective antiarrhythmic drug.
Chapter VIII - Background: The progression of permanent atrial fibrillation (AF) is related to ongoing atrial remodeling, which may be detected by brain natriuretic peptide (BNP). We examined the prevalence and prognostic value of increased BNP concentrations in serial blood specimens from patients with persistent AF.
Methods and Results: Clinical, and echocardiographic data were collected prospectively at baseline and at 1 year in 193 outpatients (mean age, 62±11 years; 78% men; 63% coronary heart disease) with persistent AF and a left atrial diameter > 50 mm. Blood samples were collected at baseline and at 3, 6, and 12 months of follow-up. BNP concentrations >100 pg/mL were considered abnormal. In 100 patients (52%), BNP was consistently <100 pg/mL (group 1); 55 (28%) had a single abnormal BNP result (group 2); and 38 (20%) had >2 abnormal BNP results (group 3). At 18 months, hospitalisation for heart failure (HF) was 9%, 26%, and 40%, respectively (P<0.001). In a Cox proportional-hazards model, left atrial diameter at 12 months (HR=1.35; 95% CI, 1.09 to 1.67), highest BNP (HR=1.01; 95% CI, 1.007 to 1.013), and number of abnormal BNP samples (HR=2.34; 95% CI, 1.60 to 3.43) were independently associated with prognosis. A BNP rise of 10 pg/mL in any sample was associated with an excess of 10% (95% CI, 7% to 13%) in the incidence of combined end point.
Conclusions: Abnormal BNP concentrations were detected in about 50% of outpatients with persistent AF. This ongoing atrial remodeling was a strong predictor of worsening HF, suggesting a role of BNP-based monitoring to identify high-risk patients.
Chapter IX - Sympathetic neurocirculatory failure in Parkinson`s disease is common. Orthostatic hypotension is the most frequent symptom. Cardiovascular disturbances have so far been met with the highest degree of clinical and scientific interest. Histological studies have proven the presence of Lewi`s bodies in sympathetic and parasympathetic neurons and also in central structures associated with the autonomic regulation.
Extrasystoles occur in normal subjects, but are more frequently seen in Parkinson patients. Heart rate variability is a useful non-invasive test to assess autonomic dysfunction in PD. It allows a differentiation of the sympathetic and parasympathetic activation, which are related to a low-frequency (0.05 - 0.15 Hz; LF) and a high-frequency (0.15-0.5Hz; HF) component of the heart rate variability (HRV) signal, respectively. The resulting LF/HF ratio is a quantitative index of the sympatho-vagal balance. The physiological function of HRV is

Preface xiii
commonly known to be to buffer changes in blood pressure. In the PD-patients group (n=107, mean age 71 years, mean PD-duration 7.0 years, Hoehn and Yahr 3.0 ± 0.9) the LF/HF ratio was lower than in the control group in rest (2.19 vs. 1.25, p < 0.05); in deep respiration (3.3 vs. 2.4, p < 0.01) and in tilt-table testing (2.6 vs 1.9, p < 0.01). The LF/HF ratio in tilt-table testing was significantly more reduced in PD with OH than without (2.1 vs. 1.3, p < 0.05). Scintigraphy with 123I-Metaiodobenzylguanidine (MIBG) appears to be a highly sensitive and useful in demonstrating sympathetic postganglionic cardiac nerve disturbances. In the heart, MIBG uptake in all examined 57 Parkinson's (PD) patients was decreased (H/M-Ratio: 1.14 ± 0.16). Loss of sympathetic innervation of the heart seems to occur independent of orthostatic hypotension and baroreflex failure in PD. We found no correlation between myocardial MIBG uptake and sympathovagal balance, blood pressure or other autonomic findings. This results could be explained by different time course of loss of intact postganglionic sympathetic cardial innervation and disturbed baroreflex response or the involvement of central autonomic pathways in PD.
The significance of the abnormalities in cardiovascular regulation among PD patients is not fully known yet. It is possible that the dysbalance of the sympathetic and parasympathetic tone is connected with heart arrhytmias. The connection between autonomic dysregulation and arrhythmia related death has recently been considered in PD. The mortality of PD patients is almost twice that for age and sex-matched healthy control groups.
Chapter X - The hemodynamic effect of the atria on the net performance of the heart is called atrial contribution (AC). AC is either linked to ventricular filling or to the systolic function of the heart, i.e. to the systolic volume or cardiac output. Several non-invasive methods for the quantification of AC are described in literature but none of them are routinely used in cardiac pacing centres due to the time-consuming nature of the methods, the limited reproducibility of measured values and observer-dependency.
The aim of presented studies was to develop a method for determining optimal AV delay in patients treated by dual chamber pacing using an index (ACSp) that quantifies atrial contribution to the systolic volume of the left ventricle. The new method is based on the quantitative analysis of a beat-to-beat decrease in the amplitude of the pulse oximetry signal (SpO2). The change in the amplitudes is induced by a sudden drop of the stimulus to the right atrium, while maintaining the rate of ventricular stimuli at a constant level. The obtained ACSp is given as a percentage of the pulse amplitude of SpO2. The method is independent of the observer, non-invasive and relatively fast. In a group of 47 patients, remarkable similarities between ACSp and another atrial contribution index estimated using the tracings of invasively registered aortal pressure were demonstrated.
In all investigated AV intervals of 50 to 250 ms, significant interindividual variability of ACSp was discovered. The poorest hemodynamic effect was seen at AV delay of 50 ms (median ACSp of 10.4 % from 97 subjects). In 150 subjects, the following values of ACSp were obtained at AV delay of 200 ms: median 30 %, minimum 3.6 % and maximum 80.4 %. Blant and Altmans’s analyses of paired values obtained within the time range of either 10-20 minutes (average difference between two paired measurements –0.5 ± 6.1 %) or 24 hours (average difference between two paired measurements 2.1 ± 7.9 %) showed good reproducibility of ACSp. In a group of repeatedly investigated subjects, every individual demonstrated stable relationship between investigated AV delays and corresponding values

Lynn A. Vespry xiv
of ACSp. This method offers a fast and observer independent alternative compared to the other non-invasive methods employed for AV delay optimization.
An increase in ACSp follows reduction of preload induced by administration of furosemide. This suggests that when preload decreases cardiac output is preserved by an increase in AC enforced by sympathetic activation.
Chapter XI - Background: Atrial fibrillation (AF) is the most common sustained arrhythmia, and significant morbidity is associated with it: Palpitations, heart failure, angina, thromboembolic complications and tachycardia-induced cardiomyopathy. Some of these are also associated with atrial flutter (Afl). Therapy of these arrhythmias is based on prevention of thromboembolism and one of these two approaches: ventricular rate control or restoration of sinus rhythm. The decision to try to maintain sinus rhythm rather than controlling ventricular rate should be individual to each patient, based on analysis of the risk-benefit ratio for that patient.
External electrical cardioversion is a useful technique to restore sinus rhythm, but quite different rates of success have been reported (67-99%). This fact could be attributable to different patient selection, but also to differences in the technique of cardioversion. This work describes the author’s experience to recommend an effective protocol to perform electrical cardioversion of AF and Afl.
Patients and methods: At Txagorritxu Hospital, since 1998 to 2005, all patients that were considered candidates for elective electrical cardioversion of AF or Afl were admitted to an out-patient ward. The author himself performed all the procedures in the intensive care unit, and prospectively recorded the main variables involved: Age, Sex, Weight, Arrhythmia, Time after the onset of the arrhythmia, Heart disease, Left atrial size, Left Ventricular Ejection Fraction, Baseline vital signs, Anaesthetic drugs and doses, Induction and Recovery time, Secondary effects attributable to anaesthesia, Electrodes, Waveform, Electrode position, Restoration of sinus rhythm, Number of Shocks, Energy, Impedances, Antiarrhythmic and cardioactive drugs, and complications. Patients were discharged home after four hours.
Conditions associated with restoring sinus rhythm were identified. Several changes were sequentially introduced in the procedure, and thoroughly analysed, incorporating those which allowed better results.
Results: During this period, 373 procedures were performed (290 AF, 83 Afl). Seventy seven per cent were male, and 23% female, and their main characteristics were: Age 61.8 ± 10.6 years; Weight 81.7 ± 14.1 kg; Left atrial size 45.8 ± 5.3 mm; Left ventricular ejection fraction 56 ± 10,2 %; Time after the onset of the arrhythmia 90 (1-3600) days; 81% had heart disease (12% coronary, 17% valvular, 18% cardiomyopathy; 31% hypertensive); 96.5% were on pharmacologyc therapy (65 % amiodarone); 13% were shocked with metal paddles, 87% with adhesive pads; Dumped monophasic sinusoidal wave was employed in 33% of patients, and sinusoidal biphasic in 67%; Anterior-lateral (A-L) electrode position was first selected in 64% of patients, and anterior-posterior (A-P) in 36%, and 8% needed changing the electrode position; Sinus rhythm (SR) was restored in 91% of patients. Thromboembolic events were not observed. The main secondary effect was respiratory depression, without consequences, mainly associated with propofol-remifentanyl, a sedative strategy which allowed a rapid induction (110 sec) and recovery time (457 sec).

Preface xv
All patients with Afl were successfully cardioverted; Patients in AF were cardioverted to SR in 77% of cases using monophasic shocks, but in 94.21% using biphasic shocks (p= 0.0000, CI 8.31-26.09, OR 4,86). A-L electrode position allowed SR restored at first shock in 71.59% of patients, and A-P in 51.96% (p= 0.0057, CI 6.9 –33.9); With A-L position 1 (1-3) shock and 150 (100-700) joules of cumulated energy were needed, and with A-P position 1 (1-5) shock and 150 (150-900) joules (CI 0.26-0.84 for the number of shocks, and 57.39-172.13 for the cumulated energy). Impedance differences were not observed.
In a multivariate logistic regression model elaborated with the patients in AF, the waveform was the only variable that showed statistical significance.
Discussion: DC countershocks (including all the modifications of the technique) are maximally effective in cardioverting Afl. Given the variations of cardiac rate associated with this arrhythmia, early electrical cardioversion is recommended, ensuring adequate prevention of thromboembolic events; a curative ablation procedure may be considered when indicated.
Electrical cardioversion is also highly effective in patients with AF. None of the patients attributes (age, weight, sex, disease, ejection fraction, atrial size…) can be used to predict failure of the procedure. Best results in the author’s series were obtained using biphasic waveform through adhesive electrodes in A-L position.


In: Cardiac Arrythmia Research Advances ISBN: 978-1-60021-795-1 Editor: Lynn A. Vespry, pp. 1-3 © 2007 Nova Science Publishers, Inc.
Expert Commentary
Collateral Damage?
Carole C. Anderson
Griffith University School of Nursing and Midwifery;
Member Royal College of Nursing Australia; Member Australian College of Critical Care Nurses
Going public with a major research project resulted in valuable feedback from recipients
of implanted pacemakers and implantable cardioverter defibrillators (ICD). I had established a 1800 free-call phone contact number which was included in the project outline. Many cardiac patients within all levels of cardiac investigation into arrhythmias, diagnosis, and treatment, appreciated this service and made contact in relation to concerns, issues, and problems experienced with bio-electronic devices, such as pacemakers and ICDs. The number of cardiac patients during the course of conversation revealing they were uncertain as to whether their body had been implanted with a pacemaker or ICD, or expected to consider implantation without knowing which device, was barely credible. During extensive research on contemporary evidence dealing with cardiac devices, such a situation indicating the extent of lack of pre-implantation education and informed consent, failed to appear. However, participants in my research have stated emphatically when words were mentioned such as, sudden cardiac death; pacemaker; and ICD; their cognitive ability to absorb any further discussion disappeared. Already traumatised patients are then often abandoned by health professionals to ponder the purpose of getting up in the morning. Thereafter, most cardiac patients, consumed with the possibility of only one prospect, the prospect of dying, will consent to heart implantation without knowing the full implications seemingly unavoidable with bio-electronic devices. Thus, going public with my research substantiated, in a way I had not predicted, the depth of the problem of non-therapeutic communication in the specific area of life-threatening cardiac arrhythmia and heart implantation.
An issue of concern and complexity for cardiac patients is the medical expectation to take anti-arrhythmic medication in tandem with a bio-electronic device. Participants in my research have expressed degrees of scepticism about the purpose of being treated with both

Carole C. Anderson 2
technologies to achieve optimum arrhythmia management. While saving lives through establishing the efficacy of the most effective therapy is important, essentially many studies and randomised clinical trials (RCT) present a struggle for dominance between two technologies: antiarrhythmia medication and implantable bio-electronic devices, primarily ICDs. The results of major RCTs have been instrumental in transforming the ICD to a first-line intervention technology for sudden cardiac death (SCD) and life-threatening arrhythmias. Nevertheless, antiarrhythmia drug technology, as a competing therapy with ICDs, has not lost efficacy even though ICD therapy is held as superior. In following through with patients’ concern I found a consensus of opinion that the bio-electronic device was valued over the human body. Many patients expressed the belief that antiarrhythmia medication served to prolong the battery ‘life’ of the device more so than contributing to patient well-being.
By its very nature as a bio-electronic device, the ICD is a body-hazard. Heart implantation with an ICD has become the accepted therapy for patients with life-threatening arrhythmias, regardless of underlying morbidity. With the growing application of ICD therapy, concern about the long-term reliability of ICD leads is increasing. Lead failures in ICDs as a body-hazard has initiated many studies attempting to unravel the complexities of lead failures and yet such hazards continue to challenge modern bio-electronic innovation. Other body-hazards, but by no means all that cause patients concern and trauma include: over-sensing and under-sensing of arrhythmia; inappropriate and sustained shock therapy; electrical storm; cardiac annihilation; nosocomial infection; venous stenosis; diaphragmatic stimulation; generator erosion; electromagnetic interference; device recall; and psychosocial-hazard.
An expanding area of concern in contemporary research especially concerning the psychosocial-hazard impact of ICDs is filtering through the enormous content of medical and bio-electronic research. Anticipation of pain and fear of negative outcome changes patients’ lives indefinitely because of the constancy of having to deal with living on the edge of life and death; there can be no reprieve from constancy. Fear is no less constant for patients who have never experienced ICD shock therapy because of the possibility and the belief it is only a matter of time before the fear becomes a reality. Thus, the very presence of the ICD within a person’s body is sufficient to invoke vulnerability, ambivalence, and powerlessness. Although too numerous to discuss in this commentary, some of the psychosocial-hazards emanating from my research included perceived biological change concepts such as: alteration; invasion; destruction; spoil; ruin; dying; different; and loss. Perceived psychological change included: depression; anxiety; panic; embarrassment; entrapment; control; resentment; dependence; and anger. Perceived social changes included the concepts: stigma; labels; sexism; profession; lifestyle; income; relationships; alienation; value; misfit-ness; deprivation; and quality of life. This inadequate listing of the impact on patient’s lives begs the question: What can be done to assist patients of heart implantation with bio-electronic devices to reach a degree of adaptation?
Millions of dollars have been made available to science in the innovation, research and development of cardiac bio-electronic devices with a multitude of studies and RCTs funded to highlight efficacy for the treatment of SCD and cardiac arrhythmias. The complexity of cardiac bio-electronics is well recognised yet the complexity of the humanistic perspective in the same field is unrecognised to the extent of being almost invisible. Therefore, multi-

Collateral Damage? 3
national bio-electronic organisations have an ethical responsibility to be accountable for the lack of funding for research that offers equal opportunity to the humanistic perspective of patients who live each moment of life experiencing the existential impact of a multi-national bio-electronic product such as, pacemakers and ICDs. It may be that the majority of cardiac patients implanted with these devices will provide positive reports but there can be no denial of negative reports from a possible minority as discussed in this commentary. Can it be that these patients are to be written off as collateral damage? Or can it be that a multi-billion dollar industry prefers not to know how the dice will fall?


In: Cardiac Arrythmia Research Advances ISBN: 978-1-60021-795-1 Editor: Lynn A. Vespry, pp. 5-8 © 2007 Nova Science Publishers, Inc.
Short Communication
The Promise of Biological Pacemakers
Alistair Lindsay Department of Cardiology, Harefield Hospital, Harefield, England
Introduction
In modern day cardiology practice the insertion of electrical pacemaker devices is routine. Although the development of modern pacing devices revolutionised cardiological practice towards the end of the 20th century, electrical devices remain a palliation, rather than a cure, for an underlying disorder of cardiac rhythm. Thus in recent years the idea of a “biological” pacemaker, whereby artificial electrical components are replaced by cellular and genetic elements capable of producing intrinsic electrical activity, has taken several steps towards becoming a realistic therapeutic goal.
Background
A biological pacemaker can be defined as an artificially introduced cellular or genetic
element that is capable of producing electrical depolarization of the heart that originates from the site of its implantation. In the broadest terms a biological pacemaker should possess - 1) the ability to initiate a cardiac impulse proximal enough in the conducting system to allow physiological depolarisation of the ventricles and 2) the ability to last as long as and be as reliable as current electrical pacemaker devices1.
What possible advantages could this method of treatment have over the well-established electronic pacing systems used today? Biological systems offer the possibility of being more sensitive to the body’s autonomic nervous system, thus providing a more natural control of physiological heart rate compared to current rate sensing pacemakers. Implantation of biological systems into the correct anatomical location would also allow electrical conduction to mimic the heart’s intrinsic conduction system, such as the bundle of His, more closely than current pacing devices. Thirdly, many of the downfalls of electrical pacemaker insertion,

Alistair Lindsay 6
such as infection, battery replacement, and the potential induction of cardiac failure, could be significantly reduced, if not eliminated. For paediatric patients in particular, who face a lifetime of device changes, a biological pacemaker could prove to be a very effective cure.
Although several different molecular approaches have been successfully shown to initiate spontaneous electrical activity in mammalian hearts, developing a suitable molecular pacing strategy also necessitates developing a suitable method of delivery. A further hurdle involves examining the efficacy, reliability and safety of the new technique. This article will review all the above areas whilst emphasising future challenges to be faced before this ambitious therapy can become a reality.
Preliminary Work Several different methods of developing an intrinsic pacing system at the molecular level
have been attempted to date. An initial approach was performed by Edelberg in 20012. By injecting plasmids encoding
a beta-2 adrenergic receptor into the atria of pigs (at the site of earliest atrial potential found) faster mean heart rates were demonstrated 48 hours later in animals that received the injection than occurred in control animals. Although promising, the effects noted were brief, lasting only around twenty-four hours. Furthermore, this approach is limited by the fact that any overexpression of beta-receptors has the potential to worse sinoatrial node dysfunction 3.
In 2002 Miake and colleagues demonstrated an alternative method of biological manipulation of the pacing system4. Building on the fact that all cardiac cells possess pacemaker activity in the early embryonic heart, quiescent heart muscle cells were altered by adenoviral gene transfer of a dominant-negative form of Kir2. This gene family codes for an inward-rectifier potassium current (IK1) that normally hyperpolarises the cell membrane of ventricular myocytes and suppresses spontaneous electrical activity. Their simple hypothesis proved true; by inhibiting the IK1 current spontaneous electrical activity was produced. However, as is common with all potassium channel modifications, this also resulted in a prolonged action potential which can increase the potential for arrhythmias.
More recent reports have aimed at altering the inward pacemaker current If, which flows only at diastolic potentials and thus should not affect the duration of the action-potential5. This can be done by overexpressing the HCN gene (hyperpolarization-activated cyclic nucleotide-gated channel), which allows inward sodium current and thus membrane depolarisation. By injecting adenoviral constructs containing the HCN2 gene, Qu et al. were able to establish an If-based pacemaker in the atria of dogs5. This method has since been explored by other groups in more recent reports due to its improved safety profile 6, 7.
Embryonic stem cells that have differentiated along the cardiomyocyte line have also been successfully transferred and shown to have spontaneous electrical activity in vivo8. Xue et al. used a lentivirus vector to transfect spontaneously beating outgrowths of human embryoid bodies with green fluorescent protein, before the cells were injected subepicardially into the left ventricular wall of guinea pig hearts. The integrated syncitium was responsive to the beta-adrenergic agonist isoproterenol, and optical mapping confirmed successful depolarisation from the site of myocardial injection. In a separate experiment similiarly

The Promise of Biological Pacemakers 7
selected cells were injected into the myocardium of pigs with heart block and were found to create an adequate pacemaker current and produce stable idioventricular rhythms9.
An final strategy could involve the use of direct fetal and/or neonatal cell transplants10, which can be enzymatically isolated before being injected into the heart. This approach has shown similar efficacy to those described above when tested in porcine models.
Delivery
The final decision on an optimal biological pacing strategy may in part be determined by
how easy it is to deliver the artifial pacing elements to the appropriate areas of the heart. Naked DNA has been successfully transfected into the human heart, but this is technically difficult, inefficient and the effects are often very short lived. While more efficient, viral vectors also have problems in that they may cause allergic reactions. Furthermore persistent viruses such as retrovirus may be complicated by the possibility of malignancy, while the safer adenovirus is less permanent. A third option involves the direct introduction of cells, either embryonic stem cells or human mesenchymal stem cells (hMSCs) which are derived from bone marrow. However it is possible that implanted cells may be rejected, and that some form of immunosupression may become necessary. This leads to further concerns about neoplastic transformation.
Of course a good delivery system must be accurate, and it is yet to be seen where in the intrinsic conducting system any cell therapy is best placed. Exactly how this is best achieved also remains to be seen; focal delivery with catheters and needles may be needed, or cells could be cultured on a matrix designed to adhere to cardiomyocytes. Most importantly, it will be necessary to prove that any implanted cells remain where they are inserted, and do not migrate to other areas of the heart, or indeed the body, where they may cause harm.
Future Challenges In addition to the issues raised above, three main challenges emerge for the future: safety,
reliability and cost. Introduction of any new electrical system into the heart could in theory precipitate arrhythmia, and the absence of any malignant arrhythmia will be one of the most important caveats for any form of biological pacemaker. Only once a safe system is formulated, and rigourously tested in small animal models, will we be able to move on to test reliability in humans. In these cases, initial introduction is likely to be in combination with traditional electrical systems, thus allowing a backup mechanism in the event of failure of the biological system.
Finally, would a biological pacemaker be cost effective? It is far too early to answer this question. The field of gene therapy itself faces many challenges over the coming years - the development of a biological pacemaker is but one of them.

Alistair Lindsay 8
References
[1] Plotnikov AN, Sosunov EA, Qu J, et al. Biological pacemaker implanted in canine left bundle branch provides ventricular escape rhythms that have physiologically acceptable rates. Circulation. Feb 3 2004;109(4):506-512.
[2] Edelberg JM, Huang DT, Josephson ME, Rosenberg RD. Molecular enhancement of porcine cardiac chronotropy. Heart. Nov 2001;86(5):559-562.
[3] Rosen MR, Brink PR, Cohen IS, Robinson RB. Genes, stem cells and biological pacemakers. Cardiovasc Res. Oct 1 2004;64(1):12-23.
[4] Miake J, Marban E, Nuss HB. Biological pacemaker created by gene transfer. Nature. Sep 12 2002;419(6903):132-133.Qu J, Plotnikov AN, Danilo P, Jr., et al. Expression and function of a biological pacemaker in canine heart. Circulation. Mar 4 2003;107(8):1106-1109.
[5] Tse HF, Xue T, Lau CP, et al. Bioartificial sinus node constructed via in vivo gene transfer of an engineered pacemaker HCN Channel reduces the dependence on electronic pacemaker in a sick-sinus syndrome model. Circulation. Sep 5 2006;114(10):1000-1011.
[6] Kashiwakura Y, Cho HC, Barth AS, Azene E, Marban E. Gene transfer of a synthetic pacemaker channel into the heart: a novel strategy for biological pacing. Circulation. Oct 17 2006;114(16):1682-1686.
[7] Xue T, Cho HC, Akar FG, et al. Functional integration of electrically active cardiac derivatives from genetically engineered human embryonic stem cells with quiescent recipient ventricular cardiomyocytes: insights into the development of cell-based pacemakers. Circulation. Jan 4 2005;111(1):11-20.
[8] Kehat I, Khimovich L, Caspi O, et al. Electromechanical integration of cardiomyocytes derived from human embryonic stem cells. Nat Biotechnol. Oct 2004;22(10):1282-1289.
[9] Cai J, Lin G, Jiang H, et al. Transplanted neonatal cardiomyocytes as a potential biological pacemaker in pigs with complete atrioventricular block. Transplantation. Apr 15 2006;81(7):1022-1026.

In: Cardiac Arrythmia Research Advances ISBN: 978-1-60021-795-1 Editor: Lynn A. Vespry, pp. 9-31 © 2007 Nova Science Publishers, Inc.
Chapter I
Unravel the Complexity of Heart Rhythm: A Modeling Approach
Jie Lian Micro Systems Engineering Inc.,
Lake Oswego, Oregon 97035
Abstract
The heart has a unique electrical system that controls the rhythm of the heartbeat. In a healthy heart, the sinoatrial (SA) node in the right atrium serves as the natural pacemaker, which generates rhythmic electrical pulses that spread across both atria. These electrical pulses are relayed to the ventricles via the atrio-ventricular junction (AVJ), a nodal structure that has complex electrophysiological properties. From the AVJ, the electrical signals travel along specialized conduction pathways that spread into the ventricles, causing them to contract and pump blood into the lungs and throughout the body.
Structural or functional abnormalities of the cardiac electrical conduction system can lead to heart rhythm disorders, or cardiac arrhythmias. Cardiac arrhythmias can result from disorders of impulse formation, impulse conduction or a combination of both. Disturbances in impulse formation involve too slow or too fast heart rate as a result of diseased SA node, or due to the development of an ectopic focus that takes over control of the intrinsic rhythm. Disorders in impulse conduction involve heart blocks, which result in slowed or blocked conduction through the myocardium. In addition, the pathological process of reentry is also an impulse conduction abnormality.
The artificial cardiac pacemaker is a medical device that controls the heartbeat. By delivering appropriately timed electrical impulses to the heart, the implantable pacemaker is a proven technology that treats various types of cardiac arrhythmia. Despite the progress of cardiac arrhythmia research and the advance of the pacemaker technology, much remains unknown about how the external pacing interacts with the heart’s intrinsic signal. Consequently, from the rhythm analysis perspective, the complexity of heart rhythm is further compounded by the consideration of cardiac pacing.
In this chapter, a model-based approach is introduced to unravel the complex heart rhythm in both physiological and pathological conditions, by taking into account the

Jie Lian 10
cardiac pacing. In this model, the intrinsic heart rhythm generator, the cardiac conduction pathway, and the external cardiac pacemaker are integrated into a closed-loop system. Examples are presented to illustrate how to use this model to generate and interpret various heart rhythms. The scientific merits and potential applications of this model are also discussed.
I. Introduction The heart beats and pumps blood with a regular rhythm to meet the metabolic need of the
body. The normal heart rhythm is maintained through a highly specialized electrical conduction system that consists of the sinoatrial (SA) node, the atrioventricular (AV) node, and the His-Purkinje network (figure 1).
• The SA node serves as the physiological pacemaker that generates spontaneous
electrical activity, which is propagated throughout the right and left atria, stimulating the myocardium of the atria to contract. The conduction of the electrical impulse throughout the atria is seen on the surface electrocardiogram (ECG) as the P wave.
• The AV node functions as a relay station in the conduction system. Electrical signals from the atria must pass through the AV node to reach the ventricles. The electrical conduction delay in the AV node forms much of the PR segment on the ECG, and this delay coordinates the timing of atrial and ventricular contractions.
• The distal portion of the AV node is known as the Bundle of His, which is split into two bundle branches that respectively activate the left and right ventricles. Together, the Bundle of His and the AV node are called the AV Junction (AVJ). The two bundle branches taper out to numerous Purkinje fibers, which stimulate individual groups of myocardial cells to contract. The electrical depolarization of the ventricles forms the QRS complex, and the ventricular repolarization produces the T wave on the ECG.
SA nodeAV junction
Left bundle branchRight bundle branch
SA nodeAV junction
Left bundle branchRight bundle branch
Figure 1. Illustration of the cardiac electrical conduction system.

Unravel the Complexity of Heart Rhythm: A Modeling Approach 11
Any disturbance in the heart’s electrical system can cause irregular heart rhythm, known as cardiac arrhythmia. Sick SA node may cause heart rate too slow (bradycardia) to meet the metabolic need of the body, whereas abnormal automaticity of the SA node or an ectopic focus may result in too high heart rate (tachyarrhythmia) that causes symptoms or even death. Rhythm disorder can also arise from structural or functional block of the cardiac conduction pathway. For example, ventricular conduction block can form the substrate for reentry that triggers lethal ventricular tachyarrhythmia, whereas the conduction block in the AV node may cause atrial-ventricular dissociation, attributing to the rapid and irregular heart rhythm in atrial tachyarrhythmia.
First invented about a half-century ago, the artificial cardiac pacemaker is a medical device designed to regular the heartbeat. The implantable pacemaker monitors the native heart rhythm, and delivers electrical energy (pacing) to activate the proper heart chamber when needed, such as atrial pacing during sinus bradycardia, or ventricular pacing in the presence of AV conduction block. Modern pacemaker device can also adjust the pacing rate according to patient’s metabolic demand, time the pacing sequence to synchronize the contraction of multiple chambers, trigger special pacing algorithm to terminate the tachyarrhythmia or even prevent its occurrence, among many other functions.
Because of the complexity of the heart’s electrical system, study of the heart rhythm can be challenging. Even in normal sinus rhythm, the cardiac inter-beat (RR) intervals fluctuate at various time scales, a phenomenon known as heart rate variability [1], due to the modulation of autonomic nervous system. In pathological conditions, puzzling patterns of heart rhythms can occur due to many different types of cardiac disorders. The complexity of heart rhythm is further compounded by the consideration of cardiac pacing, due to the limited knowledge on the interaction between the heart’s intrinsic activity and the extrinsic cardiac pacing.
In this chapter, a model-based approach is introduced to unravel the complex heart rhythm in both physiological and pathological conditions, by taking into account the cardiac pacing. In this model, the intrinsic heart rhythm generator, the cardiac conduction pathway, and the external cardiac pacemaker are integrated into a closed-loop system. Particularly, a black-box model is used to characterize the input-output relationship of the AVJ, whose filtering property plays an important role in regulating the heart rhythm. Examples are presented to illustrate how to use this model to generate and interpret various types of heart rhythms. Further improvement of the model and its potential applications are also discussed.
II. Model Structure Figure 2 shows the schematic drawing of the model structure. As described in details
below, the model consists of four inter-connected components: the atrial source, the AV junction (AVJ), the ventricle conductor, and the ventricle lead [2].

Jie Lian 12
AV junction
VentricleConductor
VentricleLead
AtrialSource
Figure 2. Schematic diagram of the structure of the present model.
Atrial Source The atrial source module simulates the intrinsic heart rhythm generator, which produces a
series of electrical impulses. The output of atrial source can be regarded as a point process, that is, a sequence of
discrete impulses occurring in continuous time [3]. Thus, both deterministic and random processes can be used to simulate different types of normal or abnormal atrial rhythms. For example, the atrial intervals can be synthesized with desired power spectrum to simulate normal sinus rhythm with certain degree of heart rate variability [4]. The atrial rate can also be fixed or programmed to simulate various atrial pacing protocols that are used in electrophysiology study [5]. In another example, the short and stable atrial intervals during atrial flutter can be approximated by a narrow-peaked Gaussion distribution [6]. On the other hand, the arrival of atrial impulses during atrial fibrillation (AF) can be characterized as a Poisson process [2, 7, 8]. Besides the variation of atrial intervals, the strength of the atrial impulses can also be varied, for example, to simulate the strong atrial signal during sinus rhythm or atrial pacing, or the weak and turbulent electrical activity during AF [2, 5-7].
The impulses generated by atrial source continuously bombard the AVJ. Conversely, any retrograde penetration of the atrium by an activation wave escaping the AVJ after a retrograde AV conduction delay (see below) can collide with an imminent atrial impulse or reset the timing cycle of the atrial source.
AV Junction The kernel component of the model is the AVJ, which is treated as a lumped structure
with defined electrical properties mimicking those of individual AV nodal cells [2, 7]. As illustrated in figure 3(a), the action potential of the AV nodal cells has five phases.
The cell is depolarized (Phase 0) when its membrane potential crosses the depolarization threshold. Then the cell repolarizes (Phases 1-3) and returns to the resting potential (Phase 4). The refractory period, when no new action potential can be initiated, begins with Phase 0 and extends into Phase 3. The AV nodal cells can depolarize spontaneously due to gradual increase of the membrane potential in Phase 4. Such automaticity is usually suppressed by the

Unravel the Complexity of Heart Rhythm: A Modeling Approach 13
higher firing rate of the SA node, but may manifest in abnormal conditions, such as the SA nodal dysfunction or the AV junctional tachycardia.
time
mem
bran
e po
tent
ial
resting potential
depolarization threshold
refractory period
time
mem
bran
e po
tent
ial
resting potential
depolarization threshold
refractory period
a.
recovery time
VT
VR
refractory period
antegrade/retrograde impulses
recovery time
VT
VR
refractory period
antegrade/retrograde impulses
b.
Figure 3. (a) Illustration of the action potential of the AV nodal cells. (b) Illustration of the AVJ module, whose electrophysiological properties represent the overall behavior of all AV nodal cells.
These properties are abstracted in the AVJ module depicted in figure 3(b). The AVJ fires when its membrane potential (Vm) reaches the depolarization threshold (VT), as a result of either antegrade or retrograde activation. The activation of the AVJ starts a refractory period, when the AVJ is non-responsive to any stimulation. After the refractory period, the AVJ enters Phase 4, Vm returns to the resting potential (VR), and starts to rise linearly. Each impulse invading the AVJ during Phase 4 causes a step increase (strength-dependent) of Vm.

Jie Lian 14
The AVJ can be activated due to combined effect of spontaneous Phase 4 depolarization and the impulse bombardments.
The firing of the AVJ generates an activation wave, which starts an antegrade or retrograde AV conduction delay according to the direction of activation. If the AVJ is retrograde activated while an antegrade wave has not finished its AV conduction delay (or vice versa), a collision within the AVJ occurs that annihilates the activation waves in both directions.
Both the conduction delay and refractory period of the AVJ are known to depend on its recovery time, which is defined as the interval between the end of previous AVJ refractory period and the current AVJ activation time. Usually, longer recovery time is associated with faster AV conduction [9-12], and shorter AVJ refractory period [7]. It is also known that the AVJ refractory period can be prolonged by a concealed impulse [11, 12], while the degree of the refractory period extension may depend on both the timing and strength of the blocked impulse. These realistic properties are all taken into account when constructing the AVJ module [2].
Ventricle Conductor In this model, the ventricle is simplified as a conduction compartment with bi-directional
conduction delays. After finishing the antegrade AV conduction delay, an activation wave is generated in the ventricle and starts the antegrade ventricular conduction. The delivery of a ventricular pace (VP) also generates a retrograde activation wave in the ventricle toward the AVJ. When both antegrade and retrograde waves are present in the ventricle, a ventricular fusion beat manifests, causing the extinction of both waves [2, 13, 14]. The ventricle becomes refractory upon antegrade or retrograde activation, that is, no further activation wave can be generated in the ventricle until the end of its predefined refractory period.
Ventricle Lead For simplicity purpose, only ventricular lead with pacing and sensing capabilities is
considered at the moment (a more complete model incorporating atrial pacing and sensing is discussed in Section VI). The lead is implanted in the ventricle, and is connected to a pacing device operating in demand mode such as VVI. If an activation wave propagates to the lead after an antegrade ventricular conduction delay, a ventricular sense occurs that inhibits the scheduled VP, whereas the timeout of the pacing interval triggers the delivery of VP.
III. Model Framework It is also evident from figure 2 that the cardiac electrical conduction system and the
artificial pacemaker form a close-loop system – as it is in the real world.

Unravel the Complexity of Heart Rhythm: A Modeling Approach 15
The antegrade branch of the loop starts from the atrial source, which generates a train of impulse output feeding the AVJ, where the electrical signals are processed, then further propagate through the ventricle conductor, until reaching the ventricle lead. On the other hand, the retrograde branch of the loop starts from the VP delivered by the ventricle lead, which generates an activation wave passing through the ventricle conductor, then being processed in the AVJ, before further invading the atrial source.
Consequently, multi-level interactions may occur between these two opposite electrical conduction branches. For instance, the VP-induced retrograde wave may fuse with the antegrade wave in the ventricle, may be blocked by the refractory AVJ, may intercept the antegrade wave within the AVJ, and may also penetrate the atrium and reset the atrial source.
In this model, the AVJ is treated as a hypothetical equivalent cell whose electrophysiological properties represent the overall behavior of all AV nodal cells. A black-box modeling approach is used to characterize the input-output relationship of the AVJ: the input to the AVJ is the antegrade or retrograde invading impulses, while the output of the AVJ is the antegrade or retrograde activation waves conducting to the ventricle or atrium, respectively. Moreover, the functional behavior of the AVJ can be equated to multiple signal processing steps that involve blanking (refractory period), summation (Phase 4), thresholding (activation), and time delay (AV conduction).
From the system modeling perspective, the AVJ can also be regarded as a relay unit that connects its output (antegrade and retrograde activation waves) to the ventricle and atrium, which are respectively driven by two electrical sources, ventricular pacing and atrial impulse. The atrial impulse (atrial source) and the VP (ventricle source) compete for the activation of the AVJ, which serves as the common pathway for both antegrade and retrograde conductions.
The present model also provides a unified platform wherein previous knowledge or latest concepts on cardiac electrophysiology can be incorporated. For example, it has been recognized that the AV conduction not only depends on the recovery time, but also is affected by the autonomic modulation [15-17]. Other nonlinear dynamics of the AV conduction under specific conditions were also reported, such as alternans [18] and hysteresis [19, 20]. All these realistic features can be incorporated within the same model framework, by choosing different formulas to characterize the AV conduction delay and the AVJ refractory period [2, 7, 9-12]. Also as noted above, the present model allows different processes to generate various types of normal or abnormal atrial rhythms. Likewise, different pacing schemes can be applied to generate different patterns of VP intervals.
IV. Model Implementation In order to facilitate the use and further improvement of the present model, its software
(written in ANSI/ISO C) has been made freely available on PhysioNet [21], an on-line forum for the dissemination and exchange of recorded and simulated biomedical signals and archives of open source software [22]. The software architecture and design flowcharts of the computer model are also provided in an open access format [6].

Jie Lian 16
Figure 4 shows the top-level flowchart of the computer model. At the beginning of the simulation, the software loads the model parameters from an external configuration file, and then initializes variables that include various timers and counters. The simulation runs at the programmed sampling frequency. At each sampling time, the model adjusts the timers and updates the Vm (in a linearly increasing manner) if the AVJ is in Phase 4, and then handles possible event(s) as listed below. The simulation continues until the desired number of cardiac beats (RR intervals) is generated or the simulation time runs out, when the model logs statistics and exits.
Load model configuration
SimulationBegin
Model initialization
SimulationEnd
Max beats ORsimulation timeout
Log statisticsModel update
Event handling
Y
N
Figure 4. Top-level flowchart of the computer model.
The event handling routine is described in figure 5. Sequentially, the model checks its timers to detect the following events and calls for respective services if any:
• ventricle fusion (VtrFusion), • atrial impulse bombardment of AVJ (AnteHitAvj), • retrograde invasion of AVJ (RetrHitAvj), • ventricle sense (VtrSense), • ventricle pace (VtrPace), • antegrade AV conduction delay timeout (AnteEscAvj), and • retrograde AV conduction delay timeout (RetrEscAvj).

Unravel the Complexity of Heart Rhythm: A Modeling Approach 17
Then the model checks the status of the AVJ. If the AVJ is in Phase 4 and Vm ≥ VT, then services are called for AVJ activation (ActivateAvj) and the initiation of the refractory period (StartAvjRef). On the other hand, if the AVJ is in refractory period, then no action is taken until its timeout, when a service is called to start the Phase 4 (StartAvjPh4).
For detailed design flowchart of each event service, model parameters settings, and code implementations, readers are recommended to refer to [6, 21] for more information.
Event handling
Begin
Event handlingEnd
Detect ventricular fusion
VtrFusion service
Y
N
AF impulse hits AVJ
AnteHitAvj service
Retr. wave hits AVJ
RetrHitAvj service
Detect conducted VS
VtrSense service
Time for scheduled VP
VtrPace service
Ante. AVD timeout
AnteEscAvj service
RetrEscAvj service
Retr. AVD timeout
AVJ in Phase 4
Vm >= VT
ActivateAvj service
Y
Y
N
N
N
Y
Y
Y
Y
AVJ refr period timeout
N
N
N
N
N
N
Y
Y
Y
StartAvjPh4 service StartAvjRef service
Figure 5. Flowchart of the model event handling routine.
V. Model Applications In this section, some representative, though not exhaustive, examples are given to
demonstrate how to use the present model to simulate various types of cardiac rhythms in both physiological and pathological conditions.
Normal Sinus Rhythm First consider a simple case of normal sinus rhythm with predefined heart rate variability.
Figure 6 shows a train of model-generated 500 pairs of atrial intervals (PP intervals) and ventricular intervals (RR intervals) in normal sinus rhythm [6]. In this example, the atrial

Jie Lian 18
source was simulated as a sinus rhythm generator, according to a process described in [4]. Each atrial impulse (P wave) has supra-threshold strength, i.e., can bring Vm directly to VT. The mean ± standard deviation of the atrial rate was set to 60 ± 1 beats per minute. The time series of PP intervals also has predefined heart rate variability that is characterized by a low frequency (LF) band centered at 0.1 Hz and a high frequency (HF) band centered at 0.25 Hz, and with predefined LF/HF ratio of 0.5. Although the RR intervals generally match the corresponding PP intervals, slight difference between the two time series is evident, which can be attributed to the rate-dependent variation of the AV conduction delay.
Figure 6. An example of model-generated PP and RR intervals in normal sinus rhythm with predefined heart rate variability.
Programmed Atrial Pacing Figure 7 shows an example of applying the present model to simulate the programmed
atrial stimulation protocol [5]. Similarly, in this example, each atrial pacing pulse has supra-threshold strength to activate the AVJ. Following a train of S1 stimuli (basic cycle) at a cycle length of 250 ms, the atrium is alternatively paced with extra-stimuli S2 and S3 with respectively short (185 ms) and long (208 ms) coupling intervals. The short atrial intervals result in long AV conduction delay, whereas the long atrial intervals result in short AV conduction delay. Consequently, the alternans of atrial pacing intervals is offset by the associated alternans of AV conduction delay in opposite phases, resulting in relatively stable RR intervals around 197 ms. Hence, this simulation demonstrated that regular ventricular

Unravel the Complexity of Heart Rhythm: A Modeling Approach 19
rhythm could be generated by irregular atrial rhythm, a phenomenon that has been previously observed in an experimental study [23].
0.16
0.18
0.2
0.22
0.24
0.26
0 4 8 12 16 20
Beat number
Inte
rval
(s)
PP
RR
Figure 7. An example of using the model to simulate the programmed atrial stimulation protocol. Modified from [5] with permission (© 2006, IEEE).
Atrial Flutter By adjusting the arrival rate of the atrial impulses (or PP intervals) and the refractory
period of the AVJ, the present model can generate typical atrial flutter rhythm with Mobitz type I block [5]. Figure 8 shows one such example. Again, it was assumed that each atrial impulse (flutter P wave) had supra-threshold strength to activate the AVJ. The initial train of atrial flutter impulses has fixed cycle length of 250 ms, which corresponds to 1:1 AV conduction (i.e. every atrial impulse is conducted to the ventricle). Thereafter, the atrial flutter interval is step decreased to 180 ms, causing rhythm transition to 5:4 Wenckebach periodicity. As the AV conduction delay progressively increases, and RR interval gradually decreases, until blocking of an atrial flutter impulse occurs.
Figure 8. An example of model-generated atrial flutter rhythm with Mobitz type I block. Modified from [5] with permission (© 2006, IEEE).

Jie Lian 20
In a similar manner, various degrees of Mobitz type II block can be simulated using the present model [6]. Figure 9 shows five runs of model-generated 500-beat RR intervals in the presence of typical atrial flutter and Mobitz type II AV block. In this case, the arrival of atrial impulses was simulated as a Gaussian process, and each atrial impulse has supra-threshold strength. From the first to the fifth sequence, the mean PP interval was decreased from 500 ms to 100 ms (with a step-size of 100 ms), all with a standard deviation of 10 ms. The AVJ refractory period was set to vary between 250 ms and 500 ms. At a slower atrial rates (PP intervals of 400 ms and 500 ms), each atrial impulse is followed by a ventricular sense (1:1 AV conduction). At higher atrial flutter rates (PP intervals of 200 ms and 300 ms), every other atrial impulse is conducted to the ventricle (2:1 AV conduction). For even higher atrial flutter rates (PP interval of 100 ms), 3:1 AV conduction occurs.
PP = 500msA:V = 1:1
PP = 400msA:V = 1:1
PP = 300msA:V = 2:1
PP = 200msA:V = 2:1
PP = 100msA:V = 3:1
PP = 500msA:V = 1:1
PP = 400msA:V = 1:1
PP = 300msA:V = 2:1
PP = 200msA:V = 2:1
PP = 100msA:V = 3:1
Figure 9. An example of model-generated atrial flutter rhythm with Mobitz type II block.
Atrial Fibrillation Atrial fibrillation (AF) represents the most common sustained cardiac arrhythmia in
clinical practice, and has the hallmark of “irregularly irregular” ventricular response. The variation of RR interval during AF has been thought to result mainly from autonomic modulations of the electrophysiological properties of the atria and AVJ [24-27]. As a result, the RR interval distribution during AF may be of a variety of forms [7]. In addition, the RR intervals during AF are considered statistically independent of each other, except for a slight correlation between two adjacent beats [7,28,29].
Despite the apparent complexity of the ventricular rhythm in AF, with proper parameter settings, the present model can account for most principle statistically properties of the RR intervals in AF [2]. Figure 10 shows four representative examples of the model generated RR intervals (500 beats each, top panels), together with their histograms (middle panels) and the autocorrelation functions (bottom panels). In the case shown in figure 10(a), the excitation of

Unravel the Complexity of Heart Rhythm: A Modeling Approach 21
the AVJ is dominated by the arrival of AF impulses, while the rate of spontaneous Phase 4 depolarization is negligible. Marked by a single broad peak, the resulting RR interval histogram resembles the unimodal distribution that has been observed experimentally [30] and predicted theoretically [7]. In the case shown in figure 10(b), both the spontaneous Phase 4 depolarization and the AF bombardments significantly contribute to the AVJ excitation. The resulting RR interval histogram is characterized by multiple evenly spaced peaks superimposed on the pieces of smooth curves [7, 31]. In the case shown in figure 10(c), the AVJ has fast rate of spontaneous Phase 4 depolarization, while its membrane potential is also modulated by frequent but weak AF impulses. The resulting RR interval histogram has a narrow peak superimposed on a smooth background [7]. Figure 10(d) shows another case where effect of concealed conduction is considered. The AVJ excitation is predominantly controlled by the AF bombardments without consideration of the spontaneous Phase 4 depolarization. The resulting RR intervals show multimodal distribution that could be attributed to the blocked AF impulses [7, 8, 10-12]. As expected, in all examples shown in figure 10, the RR intervals separated by more than one beat are essentially uncorrelated [7, 10-12, 28, 29].
Atrial Fibrillation and Ventricular Pacing It has been known that VP at cycle length close to the mean spontaneous RR intervals
not only could eliminate the long ventricular pauses, but also could suppress short conducted ventricular cycles during AF [32]. Further experimental studies have demonstrated that, for faster intrinsic ventricular rate in AF, shorter pacing cycle length (PCL) is required in order to achieve >95% VP [33].
These observations can be reproduced using the present model [2]. Figure 11 shows two examples that respectively represent (a) slow vs. (b) fast intrinsic ventricular rates in AF. In each example, the PCL is gradually varied from a sufficiently large value that results in 100% ventricular sense to a necessarily small value that results in >95% VP. For each PCL setting, 500 RR intervals are plotted. In figure 11(a), relatively long intrinsic RR intervals (444 ± 166 ms) in AF are generated in the absence of VP. Progressively shortening PCL leads to more and more paced ventricular beats, until >95% RR intervals are captured by VP at PCL = 390 ms, which is >180 ms longer than the shortest spontaneous RR interval (203 ms). In figure 11(b), increasing the rate of AF impulses leads to shorter intrinsic RR intervals (283 ± 65 ms). In this case, however, in order to achieve >95% VP capture of the RR intervals, the PCL needs to be set to 270 ms, which is only 70 ms longer than the shortest spontaneous RR interval (200 ms).

Jie Lian 22
t im e ( s ) t im e ( s )
RR
Inte
rval
(s)
RR
Inte
rval
(s)
R R In t e r v a l ( s ) R R In t e r v a l ( s )
Bea
t %
Bea
t %
B e a t L a g B e a t L a g
Aut
ocor
r. C
oeff.
Aut
ocor
r. C
oeff.
( a ) ( b )
t im e (s ) t im e (s )
RR
Inte
rval
(s)
RR
Inte
rval
(s)
R R In te r v a l (s ) R R In te r v a l (s )
Bea
t %
Bea
t %
B e a t L a g B e a t L a g
Aut
ocor
r. C
oeff.
Aut
ocor
r. C
oeff.
( c ) (d )
Figure 10. Four examples of model generated RR intervals (top panels), their respective histograms (middle panels), and the autocorrelation functions (bottom panels). Modified from [2] with permission (© 2006, IEEE).

Unravel the Complexity of Heart Rhythm: A Modeling Approach 23
PCL=1000ms
PCL=700ms
PCL=520ms
PCL=450ms
PCL=390ms
time (s)
RR
Inte
rval
(s)
(a)
(b)PCL=600ms
PCL=380ms
PCL=320msPCL=295ms
PCL=270ms
time (s)
RR
Inte
rval
(s)
Figure 11. Two examples showing the effects of VP on ventricular rhythm in AF. Modified from [2] with permission (© 2006, IEEE).
These examples confirmed that VP not only can eliminate long ventricular cycles, but also can suppress short RR intervals in AF [32]. Consistent with previous findings, the difference between the PCL resulting in >95% VP and the shortest spontaneous RR interval, is shorter when the intrinsic ventricular rate is higher [33]. Detailed model analysis shows this could be explained by the AF-VP interactions. Specifically, the antegrade AF impulses may be blocked by the refractory AVJ due to earlier invasion by the VP-induced retrograde wave. In addition, the retrograde penetration of the atrium following VP may also prevent the immediate AF impulse from bombarding the AVJ [2].

Jie Lian 24
The effects of VP on ventricular rhythm in AF could also be pacing site-dependent [34]. For example, figure 12 compares the effects of VP between short (10 ms) vs. long (110 ms) ventricular conduction time (VCT), to simulate right ventricle apical pacing vs. His bundle pacing [35]. Similarly, the PCL was varied to yield percentage of VP from 0 to >95%, and 500 RR intervals were generated for each PCL setting.
VCT 10ms VCT 110ms
PCL10s
PCL850ms
PCL720ms
PCL600ms PCL
510ms
PCL10s
PCL850ms
PCL760ms
PCL670ms PCL
600ms
Figure 12. Examples showing the effects of VP on ventricular rhythm in AF are dependent on ventricular conduction time.
As shown in the figure, for a given model configuration (which determines the pattern of RR intervals), slightly longer PCL (difference <100 ms) is needed to achieve 95% VP when the VCT is increased from 10 ms to 110 ms. To achieve lower percentage of VP, the difference in required PCL (with respect to different VCT) becomes even smaller. In other words, the pacing site does plays, though limited, a role on rate stabilization in AF. Detailed model analysis further provides a mechanistic explanation to this observation: increasing the ventricular conduction time results in more ventricular fusion beats (i.e., downward shifting of the level of retrograde conduction). Nonetheless, when the PCL is reduced to achieve higher percentage of VP, more retrograde waves can conduct to the atrium, and the role of ventricular conduction time is diminished [35].

Unravel the Complexity of Heart Rhythm: A Modeling Approach 25
Atrial Fibrillation and Ventricular Rate Smoothing Previous studies have shown that some specially designed ventricular rate-smoothing
(VRS) algorithms could reduce the irregularity of the ventricular rate in AF [36-44]. However, the optimal use of these VRS algorithms remains uncertain [45], partially because the initial clinical trials [36-43] have been limited to small and specific patient population. In this regard, the present model provides a unique platform to quantitatively assess different VRS algorithms under various AF conditions [46, 47].
For example, figure 13 illustrates the rate stabilization effects of four previously reported VRS algorithms: MADIFF-VRS [38], Flywheel-VRS [40], dynamic overdrive pacing (DOP-VRS) [36], and Adaptive-VRS [44], respectively. For comparison purpose, the RR intervals during AF without VP, and with fixed rate VP at PCL = 800, 700, and 600 ms, are also shown.
(a) AF (b) Fix800
(c) Fix700 (d) Fix600

Jie Lian 26
(e) DOP-VRS (f) Flywheel-VRS
(g) MADIFF-VRS (h) Adaptive-VRS
Figure 13. Examples of RR intervals in AF with (a) No VP, (b) fixed rate VP with PCL = 800 ms, (c) fixed rate VP with PCL = 700 ms, (d) fixed rate VP with PCL = 600 ms, (e) DOP-VRS, (f) Flywheel-VRS, (g) MADIFF-VRS, and (h) Adaptive-VRS. Modified from [45] with permission (© 2005, IEEE).
The RR intervals of spontaneous AF are random and irregular (figure 13(a)). As expected, all VP protocols (figure 13(b)-(h)) effectively regularize the ventricular rate through VP, which not only eliminates long RR intervals, but also reduces the incidence of rapid intrinsic cycles. Fixed rate VP protocols (figure 13(b)-(d)) result in unconditional elimination of all RR intervals longer than the programmed PCL. In addition, higher pacing rate is associated with more suppression of the conducted beats. On the other hand, all four VRS algorithms (figure 13(e)-(h)) dynamically adjust the pacing rate. Particularly, the Adaptive-VRS (figure 13(h)) shows wider range of PCL, and the paced beats are intercalated with the sensed beats. In contrast, all other three VRS algorithms (figure 13(e)-(g)) result in more aggressive VP and fewer intrinsic RR intervals. Also note that while the Flywheel-VRS and Adaptive-VRS algorithms immediately take control of the rhythm from the beginning of the episodes, it takes more cycles for the DOP-VRS and MADIFF-VRS algorithms to reach the steady states (i.e., relatively stable range of PCL). Therefore, it is evident from this example that the model-based simulation can provide valuable insights into the behavior of various VRS algorithms.

Unravel the Complexity of Heart Rhythm: A Modeling Approach 27
VI. Future Study The above examples demonstrate that the present model is capable to simulate various
types of cardiac rhythms in both physiological and pathological conditions. Although a more direct validation of the model in real experiments is certainly needed to confirm its concrete behavior, the current model does provide an abstract representation of the native cardiac electrical conduction system and its interactions with the external cardiac pacing. Furthermore, the software architecture of the model is constructed in a modular manner. This modular design not only facilitates model change for achieving a particular aim, but also allows potentially more realistic features of the heart and device to be encapsulated into respective modular units.
As an example, figure 14 proposes the schematic diagram of an expanded model structure, in which the cardiac conduction system and the pacing device form a more complete close-loop consisting of eight modular units. The AVJ remains the kernel of the model, and its functional behaviors represent the overall electrophysiological properties of all the AV nodal cells. Besides the distal connection with the ventricle conductor, the AVJ also has proximal connection with the atrial conductor that is characterized by bi-directional conduction delays. The atrial conductor links the atrial source to the AVJ, while the ventricle conductor links the ventricle source to the AVJ. Like the original model, the atrial source generates the intrinsic heart rhythm of the atrial origin, whereas the ventricle source simulates the escape ventricular rhythm, albeit usually slow and suppressed. In addition, both the ectopic beat generator and the exogenous noise generator can be incorporated into the atrial and ventricle source modules, respectively. The ventricle lead can sense the antegrade-conducted wave, as well as the output of the ventricle source. The ventricle lead can also deliver VP that starts a retrograde conduction wave, meanwhile resets the ventricle source. Similarly, the atrial lead not only connects to the atrial conductor, but also is coupled to the atrial source. Finally, the atrial lead and the ventricle lead are linked together through the pacer, which simulates a dual-chamber implantable device that implements detailed logic control and pacemaker timing. It is conceivable that the integrated heart and pacer model proposed in figure 14 could offer further insights into the mechanisms of various heart rhythms.
AV junction
VentricleConductor
AtrialLead
VentricleLead
VentricleSource
AtrialSource
AtrialConductor
Pacer
Figure 14. Proposed schematic diagram of an expanded heart and pacer model structure.

Jie Lian 28
The present model has a number of applications. First and foremost, the model can help decipher many puzzling cardiac rhythms encountered in the real world. As demonstrated above, the present model can generate various patterns of normal and abnormal heart rhythms that are consistent with previous experimental observations (figures 6-13). Moreover, some seemingly conflicting observations could be explained in terms of a difference in model parameter settings [2, 35].
Second, the model provides an abstract representation of the atrial source and the cardiac conduction pathway, both of which are under autonomic control. Many abnormal cardiac rhythms have been thought to result from disturbances in autonomic modulation of the electrophysiological properties of the atria and/or the AVJ. Hence, the present model may become a useful tool to facilitate better understandings on the mechanisms of arrhythmia genesis, maintenance, and termination.
Furthermore, the model can be used to investigate the therapeutic behaviors of drug or device interventions in a simulation environment. On one hand, many anti-arrhythmic drugs are known to affect heart rhythm by modifying electrical properties of the heart, such as automaticity, conductivity, and refractoriness [48]. On the other hand, specially designed pacing protocols could be used for prevention or termination of various cardiac arrhythmias [49]. Therefore, the model-based heart rhythm analysis may guide the development of novel strategies for cardiac rhythm management.
Last but not least, the model can contribute to the development of advanced biomedical engineering techniques for cardiac arrhythmia research. For example, the present model can generate at least three closely coupled time series: PP intervals, RR intervals, and PR intervals (AV delays). By simulating various cardiac rhythms, the model-generated time series can be used to build a standard test platform for quantitative evaluation or comparison of different signal processing techniques that have been developed for heart rhythm analysis.
VII. Conclusion In summary, a modeling approach to unravel the complex heart rhythm is introduced in
this chapter. Detailed model structure is described within a unified yet flexible framework, and its open source implementation is disclosed in order to facilitate the use and further improvement of the model. Representative examples are provided to demonstrate the usage of the model for realistic simulation of various cardiac rhythms. Finally, further improvement of the model, as well as its scientific merits and potential applications are discussed.
Acknowledgements The author wishes to thank Drs. S. E. Greenhut, D. Müssig, V. Lang, and G. D. Clifford,
for helpful discussions at various stages during the development of the model.

Unravel the Complexity of Heart Rhythm: A Modeling Approach 29
References
[1] Malik M, Camm AJ. Heart rate variability. Armonk, NY: Futura, 1995. [2] Lian J, Müssig D, Lang V. Computer modeling of ventricular rhythm during atrial
fibrillation and ventricular pacing. IEEE Trans. Biomed. Eng, 2006; 53: 1512-1520. [3] Daley D, Vere-Jones D. An introduction to the theory of point process. 2nd Ed. New
York: Springer-Verlag, 2003. [4] McSharry PE, Clifford GD, Tarassenko L, Smith L. A dynamical model for
generating synthetic electrocardiogram signals. IEEE Trans. Biomed. Eng, 2003; 50: 289-294.
[5] Lian J, Müssig D, Lang V. Validation of a novel atrial fibrillation model through simulated atrial pacing protocols. Proc. 28th Ann. Int. Conf. IEEE Eng. Med. Biol. Soc, 2006: 4024-4027.
[6] Lian J, Clifford GD, Müssig D, Lang V. Open source model for generating RR intervals in atrial fibrillation and beyond. Biomed. Eng. Online, 2007; 6:9.
[7] Cohen RJ, Berger RE, Dushane TE. A quantitative model for the ventricular response during atrial fibrillation. IEEE Trans. Biomed. Eng, 1983; 30: 769-781.
[8] Moe GK, Abildskov JA. Observations on the ventricular dysrhythmia associated with atrial fibrillation in the dog heart. Circ. Res, 1964; 14: 447-460.
[9] Talajic M, Papadatos D, Villemaire C, Glass L, Nattel S. A unified model of atrioventricular nodal conduction predicts dynamic changes in Wenckebach periodicity. Circ. Res, 1991; 68: 1280-1293.
[10] Zeng W, Glass L. Statistical properties of heartbeat intervals during atrial fibrillation. Phys. Rev. E, 1996; 54: 1779-1784.
[11] Jorgensen P, Schafer C, Guerra PG, Talajic M, Nattel S, Glass L. A mathematical model of human atrioventricular nodal function incorporating concealed conduction. Bull. Math. Biol, 2002; 64: 1083-1099.
[12] Meijler FL, Jalife J, Beaumont J, Vaidya D. AV nodal function during atrial fibrillation: the role of electrotonic modulation of propagation. J. Cardiovasc. Electrophysiol, 1996; 7: 843-861.
[13] Wittkampf FH, de Jongste MJL, Meijler FL. Atrioventricular nodal response to retrograde activation in atrial fibrillation. J. Cardiovasc. Electrophysiol, 1990; 1: 437-447.
[14] Wittkampf FH, de Jongste MJL, Meijler FL. Competitive antegrade and retrograde atrioventricular junctional activation in atrial fibrillation. J. Cardiovasc. Electrophysiol, 1990; 1: 448-456.
[15] Warner MR, Loeb JM. Beat-by-beat modulation of AV conduction. I. Heart rate and respiratory influences. Am. J. Physiol, 1986; 251: H1126-H1133.
[16] Warner MR, de Tarnowsk JM, Whitson CC, Loeb JM. Beat-by-beat modulation of AV conduction. II. Autonomic neural mechanisms. Am. J. Physiol, 1986; 251: H1134-H1142.
[17] Leffler CT, Saul JP, Cohen RJ. Rate-related and autonomic effects on atrioventricular conduction assessed through beat-to-beat PR interval and cycle length variability. J. Cardiovasc. Electrophysiol. 1994; 5: 2-15.

Jie Lian 30
[18] Christini DJ, Stein KM, Markowitz SM, Mittal S, Slotwiner DJ, Iwai S, Lerman BB. Complex AV nodal dynamics during ventricular-triggered atrial pacing in humans. Am J. Physiol. Heart Circ. Physiol. 2001; 281: H865-H872.
[19] Shenasa M, Lacombe P, Godin D, Sadr-Ameli MA, Faugere G, Nadeau RA. Atrioventricular nodal conduction and refractoriness following abrupt changes in cycle length. Pacing. Clin. Electrophyiol. 1988; 11: 1281-1290.
[20] Zhao J, Billette J. Characteristics and mechanisms of the effects of heart rate history on transient AV nodal responses. Am. J. Physiol. 1996; 270: H2070-H2080.
[21] AFVP - A realistic ventricular rhythm model during AF and VP [cited on July 11, 2007]. Available from: http://physionet.org/physiotools /afvp/.
[22] Goldberger AL, Amaral LAN, Glass L, Hausdorff JM, Ivanov PCh, Mark RG, Mietus JE, Moody GB, Peng CK, Stanley HE. PhysioBank, PhysioToolkit, and PhysioNet: components of a new research resource for complex physiologic signals. Circulation, 2000; 101: e215-e220.
[23] Heethaar RM, de vos Burchart RM, Denier van der Gon JJ, Meijler FL. A mathematical model of A-V conduction in the rat heart. II. Quantification of concealed conduction. Cardiovasc. Res. 1973; 7: 542-556.
[24] Toivonen L, Kadish A, Kou W, Morady F. Determinants of the ventricular rate during atrial fibrillation. J. Am. Coll. Cardiol. 1990; 16: 1194-1200.
[25] Nagayoshi H, Janota T, Hnatkova K, Camm AJ, Malik M. Autonomic modulation of ventricular rate in atrial fibrillation. Am. J. Physiol. 1997; 272: H1643-H1649.
[26] Holmqvist F, Stridh M, Waktare JE, Brandt J, Sornmo L, Roijer A, Meurling CJ. Rapid fluctuations in atrial fibrillatory electrophysiology detected during controlled respiration. Am. J. Physiol. Heart Circ. Physiol, 2005; 289: H754-H760.
[27] Wasmund SL, Li JM, Page RL, Joglar JA, Kowal RC, Smith ML, Hamdan MH. Effect of atrial fibrillation and an irregular ventricular response on sympathetic nerve activity in human subjects. Circulation. 2003; 107: 2011-2015.
[28] Goldstein RE, Barnett GO. A statistical study of ventricular irregularity of atrial fibrillation. Comput. Biomed. Res, 1967; 1: 146-161.
[29] Bootsma BK, Hoelen AJ, Strackee J, Meijler FL. Analysis of R-R intervals in patients with atrial fibrillation at rest and during exercise. Circulation, 1970; 41: 793-794.
[30] Hashida E, Yoshitani N, Tasaki T. A study on the irregularity of the sequence of R-R intervals in chronic atrial fibrillation in man based on the time series analysis and the information theory. Jpn. Heart J, 1978; 19: 839-851.
[31] Soderstrom N. What is the reason for the ventricular arrhythmia in cases of auricular fibrillation? Am. Heart J, 1950; 40: 212-223.
[32] Wittkampf FH, de Jongste MJ, Lie HI, Meijler FL. Effect of right ventricular pacing on ventricular rhythm during atrial fibrillation. J. Am. Coll. Cardiol, 1988; 11: 539-545.
[33] Vereckei A, Vera Z, Pride HP, Zipes D. Atrioventricular nodal conduction rather than automaticity determines the ventricular rate during atrial fibrillation and atrial flutter. J. Cardiovasc. Electrophysiol, 1992; 3: 534-543.

Unravel the Complexity of Heart Rhythm: A Modeling Approach 31
[34] Padeletti L, Fantini F, Michelucci A, Pieragnoli P, Colella A, Musilli N, Ricciardi G, Buhr TA, Valsecchi S. Rate stabilization by right ventricular apex or His bundle pacing in patients with atrial fibrillation. Europace. 2005; 7: 454-459.
[35] Lian J, Müssig D, Lang V. On the role of ventricular conduction time in rate stabilization for atrial fibrillation. Europace, 2007; 9: 289-293.
[36] Wittkampf FH, de Jongste MJ. Rate stabilization by right ventricular pacing in patients with atrial fibrillation. Pacing Clin. Electrophysiol, 1986; 9: 1147-1153.
[37] Lau CP, Leung WH, Wong CK, Tai YT, Cheng CH. A new pacing method for rapid regularization and rate control in atrial fibrillation. Am. J. Cardiol, 1990; 65: 1198-1203.
[38] Greenhut SE, Fraser J, Steinhaus B, Feld G, Hughes W. Optimized standby rate reduces the ventricular rate variability in pacemaker patients with atrial fibrillation. Pacing Clin. Electrophysiol, 1996; 19: 1780-1785.
[39] Duckers HJ, van Hamel NM, Kelder JC, Bakema H, Yee R. Effective use of a novel rate-smoothing algorithm in atrial fibrillation by ventricular pacing. Eur. Heart J, 1997; 18: 1951-1955.
[40] Lee JK, Yee R, Braney M, Stoop G, Begemann M, Dunne C, Klein GJ, Krahn AD, van Hemel NM. Acute testing of the rate-smoothed pacing algorithm for ventricular rate stabilization. Pacing Clin. Electrophysiol, 1999; 22: 554-561.
[41] Simpson CS, Yee R, Lee JK, Braney M, Klein GJ, Krahn AD, Skanes AC. Safety and feasibility of a novel rate-smoothed ventricular pacing algorithm for atrial fibrillation. Am. Heart J, 2001; 142: 294-300.
[42] Tse HF, Newman D, Ellenbogen KA, Buhr T, Markowitz T, Lau CP. Effects of ventricular rate regularization pacing on quality of life and symptoms in patients with atrial fibrillation (Atrial fibrillation symptoms mediated by pacing to mean rates [AF SYMPTOMS study]). Am. J. Cardiol, 2004; 94: 938-941.
[43] Ciaramitaro G, Sgarito G, Solimene F, Maglia G, Vicentini A, di Donato G, Raciti G, Parrinello G, del Giudice GB. Role of rate control and regularization through pacing in patients with chronic atrial fibrillation and preserved ventricular function: the VRR study. Pacing Clin. Electrophysiol, 2006; 29: 866-874.
[44] Lian J, Müssig D, Lang V. Adaptive ventricular rate smoothing during atrial fibrillation: a pilot comparison study. Proc. 27th Ann. Int. Conf. IEEE Eng. Med. Biol. Soc, 2005; 3881-3884.
[45] Wood MA. Trials of pacing to control ventricular rate during atrial fibrillation. J. Interv. Card. Electrophysiol, 2004; 10(Suppl 1): 63-70.
[46] Lian J, Müssig D, Lang V. Quantitative comparison of ventricular rate smoothing algorithms for atrial fibrillation. (abstract) Heart Rhythm, 2006; 3(Suppl.): s150-s151.
[47] Lian J, Müssig D, Lang V. Ventricular rate smoothing for atrial fibrillation: a quantitative comparison study. Europace, 2007 May 16 [Epub ahead of print] doi:10.1093/europace/eum088.
[48] Fogoros. Antiarrhythmic drugs: A practical guide. Malden: Blackwell Science, 1997. [49] Trohman RG, Kim MH, Pinski SL. Cardiac pacing: the state of the art. Lancet, 2004;
364: 1701-1719.


In: Cardiac Arrythmia Research Advances ISBN: 978-1-60021-795-1 Editor: Lynn A. Vespry, pp. 33-72 © 2007 Nova Science Publishers, Inc.
Chapter II
The Liminal Body: Lament of the Implantable Cardioverter Defibrillator
Carole C. Anderson
Griffith University Faculty of Health and Science; Member Royal College of Nursing Australia; Member Australian
College of Critical Care Nurses
Abstract
To prevent sudden cardiac death an increasing number of implantable cardioverter defibrillators (ICD) are implanted in people who are at risk of life-threatening arrhythmias. Research results demonstrate this rapidly expanding bio-electronic treatment remains poorly understood by recipients, their family members and by health professionals. Research into both the efficacy of ICDs and the degree of acceptability to recipients, family members and health professionals has provided equivocal results. Yet there has been little research designed to explore the essence of what it means to live with the effects of ICD bio-electronics and so health professionals involved in heart implantation with an ICD may discuss efficacy with recipients and their family members but have little other evidence to facilitate informed decision-making.
This chapter draws upon the results of a major research project that focused on the phenomenon of implantation of a person’s heart with a permanent bio-electronic ICD. Implantation was explored through the existential perspectives of participants from four groups: recipients of ICDs, family members of recipients; cardiac nurses and paramedical personnel; and cardiologists.
Hermeneutical phenomenological methods, including unstructured in-depth dialogue; content and thematic analysis of participants’ lived-through experiences; interpretation of authentic dialogue from participants’ drawing on literature, poetry, art; and the idiomatic meaning of words relating to the heart; were used in the research. The findings from this research are expressed in terms of how participants experienced body-liminality in many existential ways. The phenomenon of heart implantation with an ICD, is an experience of liminality; recipients live on the threshold of life and death and all participants’ lives are influenced by a betwixt/between liminal-perspective. Moreover,

Carole C. Anderson 34
heart implantation with an ICD impacts on lived-temporality/time; lived-spatiality/movement; lived-emotionality; lived-sexuality/gender; and lived-relationality. Recipients and their family members experience a sense of security because the device is in place but this is always counterbalanced by the experience of dying and being revived multiple times or always being on the threshold of that experience.
This chapter explicates body-liminality as represented in the research results, giving powerful yet poignant exemplars from the dialogue of recipients, family members and health professionals. The chapter concludes with a discussion on how this information can be used to improve education, informed consent, negotiation, and support, in the care of patients with life threatening arrhythmias who are being considered for heart implantation with an ICD. Furthermore, this chapter can be a source of enlightenment for health professionals who may have dilemmas in relation to heart implantation with the bio-electronic ICD.
Introduction
What Is Liminality? Mention of the concept liminality appears to invoke a questioning look from most
people. Thus, there is a need to explain the intended application of liminality to enable understanding to develop as this chapter progresses. The notion of liminality was formulated by French ethnographer Arnold van Gennep (1960) to describe socio-cultural rites of passage. Rites of passage featured significant transitions in a person’s existential ontology and followed three sequential phases of movement through time, space and socio-cultural status; separation, liminality, and incorporation. For example, transition through the dying process during which time the person is separated from socio-cultural function and required by socio-cultural rituals to endure liminal interventions often involving physical pain and existential indeterminacy; liminality is a time and place where the person’s Being, or ontology, can dissolve into disorientation and a state of being in limbo on the threshold of life and death. During the liminal phase the person’s mind, body and behaviour is open to a new way of being incorporated and returned to a new socio-cultural status; no more the living-person but the dead-person. Should the person become lost in liminality there is the possibility of remaining in a liminal state of existence, such as a vegetative state. Thus, liminality marks a significant change of Being-in-the-world; being separate, being on the margin of life and death, or limen; Latin for threshold.
David Riesman (1954) wrote of people who were unable to embody the identities expected of them in various cultures and Victor Turner (1986) developed liminality to include being betwixt and between, having left past embodiment of self yet not arriving at future embodiment of self. Recently returning from the Arctic Circle where the eerie environment defied perception of night or day but rather an existential perception of being between both, I reflected on the television series The Twilight Zone (Serling, 1959). Through the various genres of science fiction, fantasy and horror Rod Serling captured humanities fears, hopes and complexities while including a moral or philosophical message from a central allegory, parable or fable. Mythology and science fiction stir the social imagination to envisage that which was thought to be impossible in actual human beings, yet as Donna

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 35
Haraway (2003, p. 429) concluded in relation to the notion of cyborg: “This is a struggle over life and death, but the boundary between science fiction and social reality is an optical illusion.” In this chapter, research participants express powerful socio-cultural perspectives on being involved in implantation of the human heart with a bio-electronic device known as an implantable cardioverter defibrillator (ICD).
The Equivocal ICD Science continues the liminal struggle to conquer the boundaries between life and death
in the increasing incidence of life threatening cardiac arrhythmias, such as ventricular tachycardia (VT); sudden cardiac death (SCD); cardiac conditions, such as types of cardiomyopathy; and heart failure. A worldwide survey on heart implantation of new and replacement pacemakers and ICDs is collated every four years and submitted to the World Symposium on Cardiac Pacing and Electrophysiology (Mond, Irwin, Morillo and Ector, 2004). Although the last survey was collated in 2005 the report will be presented at The Thirteenth World Symposium during 2007 (Furman, 2003). At this point in time the most up to date report published on increasing global trends in heart implantation with ICDs is provided from the ICD Registry of the Italian Association of Arrhythmology for the years 2001-2004 (Proclemer, Ghidina, Cicuttini, Gregori and Fioretti, 2006). An increase of 144.5% was reported and claimed to be similar to trends in other Western countries. Furthermore, prophylactic heart implantation of single chamber ICDs, dual chamber ICDs, and biventricular ICDs, increased four-fold in the same time-frame.
There are millions of heart implantations with ICDs worldwide, establishing the cardiac bio-electronic innovation as a multi-billion dollar industry (Maisel, 2005). Given the meteoric rise of acceptance by science and cardiology, and the complexity of the ICD, it is not surprising that malfunctions and hazards exist: the person’s heart implanted with an ICD and pacemaker dependent will receive greater than 100 million paced beats over the lifespan of the device (Maisel, 2005). Thus, it is imperative that legislation is in place to closely regulate the industry.
In the United States of America the Food and Drug Administration (FDA) requires notification of any cause, in cardiac implantable devices, that constitutes a hazard to consumers. The FDA (2000, p. 6) defines hazard:
A hazard is a potential source of harm. Hazards arise in the use of medical devices
due to the inherent risk of medical treatment, from device failure or malfunctions, and from device use. Hazards resulting from medical devices impact patients, family members and professional healthcare providers. By its very nature as a bio-electronic device, the ICD can and does present as a body-
hazard and in 2004 the FDA received 160,487 reports of adverse events. Additionally, in the month of June alone, 2005, 62,000 malfunctioning ICDs required recall (Maisel, 2005). Despite the plethora of studies advocating the efficacy of ICD therapy including well known randomized clinical trials (RCT) (Anderson, 2005), the phenomenon of heart implantation with a bio-electronic ICD is neither a cure for nor a guarantee against life threatening cardiac

Carole C. Anderson 36
arrhythmias and SCD. Thus, the ICD is located in the liminal space between life and death and the notion of ICD-efficacy remains equivocal. In this chapter humanistic research results add a further liminal dimension to heart implantation through phenomenological dialogue with recipients, family members of recipients, cardiac nurses and paramedical personnel, and cardiologists.
Technology, Know-How, Achievements, Are Not Enough
Karl Jaspers 1961
In this chapter, the philosophical underpinnings of hermeneutical phenomenology
expressed by Maurice Merleau-Ponty (1962) and van Manen (1990) re-awaken the phenomenon of heart implantation with a bio-electronic ICD in ways that question human interaction with bio-electronics. Such interaction allows the person to accept or decline bio-electronic devices “insofar as we do not permit them to claim us exclusively and thus to warp, confuse, and finally lay waste to our essence” (Heidegger, 1966, p. 54). Moreover, science is criticized in neglecting thoughts for the meaning of altering human existence through bio-electronics, described by Merleau-Ponty (1964, p. 160) as “thinking operationally: a sort of absolute artificialism, such as we see in the ideology of cybernetics.” Thus, Merleau-Ponty advocates a return “to the site, the soil of the sensible and opened world such as it is in our life and for our body: that actual body I call mine. Further, associated bodies must be brought forward along with my body.”
Science has been sustained by preconceived ideas about knowledge of the world and its phenomena through interpreting life-events-in-the-world according to causal properties and in rational, intellectual terms. Within classical science, what exists in the lived-world of the person is reduced to the status of object; consequently, the living body and the dying body are equally reducible to an object. This being the case, the body loses subjectivity and becomes a disembodied consciousness. Thus, scientific epistemology as unchallenged equally becomes uncertain of its absolute nature, but phenomenology is a philosophy that returns essences to the person as the authentic source of lived-knowledge.
The intentional arc is the core of Merleau-Ponty’s philosophy of embodiment. It is the fundamental level at which the lived-body and the lived-world come together in the past, present and future. The study results of the implanted heart presented in this chapter epitomize how embodiment in illness is constantly in the present: the person’s life and death, past and future, is a mere heart-beat either side of the present.
There are many facets to the intentional arc. It subtends the possibilities and the meanings within existence and situations. The intentional arc is a continuum that presents many different possibilities within phenomena. This continuum holds many different meanings of being-in-the-world. The intentional arc is the life of embodied consciousness; the life of time and space; it is the embodied unity of emotionality and sexuality; the intentional arc enables the person to have an embodied perspective on heart implantation albeit from a different world-view. When intentionality breaks down in illness, the person’s

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 37
world is fragmented and the intentional arc goes limp and cannot sustain the person: a state of liminality. Consequently, heart implantation with a bio-electronic ICD presents the possibility of embodiment, disembodiment and altered embodiment. Because intentionality is central to phenomenology, hermeneutical phenomenology is relevant to wanting to know and understand the phenomenon that is heart implantation.
Phenomenological Dialogue Going public was an appropriate method of inviting participants to engage in
phenomenological dialogue because participation stemmed from each person’s own volition. Merleau-Ponty (1962, p. 178) described phenomenological dialogue:
People can speak to us only a language, which we already understand, each word of
a difficult text awakens in us thoughts which were ours beforehand, but these meanings sometimes combine to form new thought which recasts them all, and we are transported to the heart of the matter, we find the source. During discussion with the gatekeeper of a struggling support group for ICD recipients,
validation for the need of research exploring heart implantation with a bio-electronic ICD was expressed: “We have been waiting for someone like you to come along.” This particular support group attached to a major cardiac hospital has since disbanded because of the absence of medical approval.
To enhance the understanding of any phenomenon Sandelowski (2002) advocates the embodiment of other dialogues and cautions against relying on the precariousness of a one-legged stool over the sturdiness of the four-legged chair. Thus, it was imperative for dialogue to be multi-vocal: the study results presented in this chapter are the authentic dialogue of nine recipients of heart implantation; eleven family members of recipients; sixteen cardiac nurses and paramedical personnel, and six cardiologists. While I sought to be engaged in dialogue with participants I maintained the purpose of dialogue in phenomenology; to remain in touch with the question of the nature of the phenomenon as the core of an essentially human experience. Other sources of insight, such as the notion of liminality, literature, poetry, and film, speak their own phenomenological dialogue, thus adding to the rigor and richness of interpretation (van Manen, 1990).
As I move on to present the lived-worlds of participants who are the makers of this chapter text, it is the task of the reader to decide whether the text is believable. In hermeneutic phenomenology there is a hermeneutic circle of interpretation and this is shared in a circular movement “between a background of shared meaning and a more finite, focused experience within it” (Thompson, 1990, p. 243). As the writer I identify movement and dialectical interaction between the whole and the part, and subsequently offer interpretation, however: “This complex world, with its multiple perspectives, is then connected to a constantly changing external world, in which nothing is firm or certain. Consequently, there can be no single truth” (Denzin, 1996, p. 237).

Carole C. Anderson 38
Heart Implantation as Body-Liminality
Hybrid Persons “Wow! My God, is that real? I thought it was a trick! It is not the sort of thing you expect
to see.” Such was the reactive response of a young female when viewing the chest x-ray of one of the recipients of heart implantation with an ICD. The chest x-ray was a visual, tangible, hermeneutical representation of the phenomenon of implantation. If Dilthey (1976, p. 161) had viewed the same chest x-ray he may have stated; “reality only exists for us in the facts of consciousness given by inner experience” and Bruner (1986) may have argued that words have outweighed the visual and language has become more valued than image. The image of the chest x-ray is an expression of interpretation, engagement with body hybridisation and placement in liminality. It enters into a dialogue with the viewer and evokes a medley of responses including spontaneous shock and disbelief.
When entities recognised as belonging to different domains become fused in the body, then hybridisation occurs (Werbner and Modood, 1997). May’s dialogue portrayed hybridisation in a brief yet graphic, disembodied account of fusion between the organic-body and the inorganic-body:
I had the surgery. They took the pacemaker out from the left hand side. The veins
had closed around the wires. They had to put the ICD in the right hand side during the same surgery. They put two new wires in, so when I woke up I had two lots of surgery, each side. And I was sore. And I can still feel them. My x-ray would have to be bionic. I have four of the leads and wires. I still have all the tie wires around my breastplate. This experience began with explantation of the inorganic object from May’s body, but
complete separation from past hybridisation was not to be. A permanent fusion between body and object wires meant that the inorganic object maintained a presence within her body. This presence may be viewed not as a side effect of implantation; it is the very life of it. Implantation of May’s heart and body with the ICD further complicated body-liminality. Together with tie wires from past open heart surgery, May saw her body as bionic in the image of her chest x-ray. May’s confusion with what was real is evident in her naming her sternum as a breastplate. The sternum is part of the organic body while a breastplate is a metal plate of armour (Ritter, 2005). As a hybrid person May was altogether lost in body-liminality.
When May first saw her own liminal body in its hybrid form she rushed about in disbelief showing the x-ray to everyone she knew. May needed convincing that her inner experience was actually her reality. Haraway (1990; 1993) argued that cyborgs are equally mythological and real. The mythological part of cyborg was unbelievable while the reality was shocking. By showing people her x-ray May hoped for validation of her disbelief. How could this shocking image actually be real or a true reproduction of what had been done to her body?
When I came out of hospital I made a point of showing everyone that x-ray. It was
like I needed to show everyone you know, look at me! Look at what has happened to me

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 39
… isn’t this shocking! It was like a ridiculous need. Yeah, I needed to show everyone I came across. Look at my x-ray. I guess it was like trying to help me get used to the idea of what was in there. It was whacky I know, but it went way beyond what was normal. A photograph of May’s chest x-ray could have been an entry in a symposium of body
photographs entitled The Liminal Body. This symposium of seven international photographic artists was held at the Australian Centre for Photography (ACP) in Sydney, Australia, and sponsored by the University of New South Wales. At this time the world celebrated the Olympian body striving for supremacy beyond the limitations of the every day body. In contrast, the photo-artists presented corporeal works “from medieval medical machinery to virtual genital modification; from the cadaver to the spiritual; from the catharsis of nightmare to the control of meaning; the body on the brink of life and death” (ACP, 2000, p. 1).
I said to people, I apologise but I have to show you this x-ray. But at the time I think
it was so shocking for me that I just had to show other people to get their reaction and talk it through. Reactions ranged from raucous laughter, you know? That someone could have so much wiring and still look normal, to absolute white-faced shock and feeling sick, and people would turn away. While May reached out to people for catharsis from the nightmare image of her liminal
body in its hybrid form, implantation meant neither life nor death, as mentioned in the ACP symposium, but something betwixt and between the two. People laughed in shocked embarrassment, people were white-faced with horror, people looked ill, and people turned away. Liminality was not a place people wished to enter.
In contrast Dell was passionate in not wanting to see her liminal body at any time and would rather have destroyed it. During our dialogue I asked Dell to go back to the time of implantation. Her response was immediate.
Even just that word is horrible. That makes me think like, a little alien: implanted
like the movie Alien. They implanted her with an alien. That is what it felt like. Yes. It was. It is. That is exactly what it was like. This little alien that I HATED and I would dream at night that I was putting my hand in my chest and ripping it out and throwing it off the side of a cliff. I absolutely HATED it with a passion. I begged them every time I went to see the [cardiologist] … please take it out, please take it out. I don’t want it. I just felt wrecked. I felt destroyed. I felt like I had been painting [her image on canvas] and someone had just drawn a knife down through it. May and Dell were both able to enter into a hermeneutical dialogue of experiences they
had lived through in relation to the phenomenon of implantation. Both spoke of disembodied image; an image in the form of an x-ray and a metaphorical image of a destroyed self-portrait. In both hermeneutical images there were similarities to Oscar Wilde’s portrait of Dorian Gray (Cornish, 1993) in which self and other co-existed but remained disembodied. Although May, Dell and Dorian Gray were endowed with extended life, they lived in horror of their own image.

Carole C. Anderson 40
May and Dell were also similar in portraying bio-electronic devices which were indeed the reality of implantation. The experience of heart implantation was foreign, evil, and alien. How can the horror effect of implantation for people, such as May and Dell, be understood and interpreted? This can only be achieved by drawing on relevant elements within our culture. Margaret Lock (1995, p. 391) wrote about the paradox of mixing self and other and warned that the “Shiva like character of invasive biomedical technologies: potential creators of happiness but, at the same time, destroyers of society as we know it: for it is now possible to manipulate nature/culture and self/other dichotomies of long standing: projects confined thus far to the realm of fantasy.” Shiva is The Ultimate Reality in Hinduism, believed to possess the dichotomous powers of reproduction and dissolution (Ritter, 2005). May related her experience of implantation, much of which has remained unchanged.
Yeah, when I first got it, I hated it; loathed it; detested it. I wished I hadn’t bothered
with it. It was difficult to get used to. The size of it felt like ten times the size. It was more the fact that it would move. It would move around when I went over a bump in the car. I would have to hang on to it. It made me hate it. I loathed it. It was definitely there, you could experience it. The foreign body inside me: it was more intrusive than I thought. It moved; it was unnatural. It is not supposed to be there. It was never intended to be there. Lying in bed at night, feeling and seeing it, jutting out. UGH! I would give myself the creeps. I didn’t like being by myself at first because I was scared if it goes off, what will happen if I am by myself. Once I was over the pain and the skin or whatever, it [ICD] began to twitch, TWITCHING. It was scary, to stand in the shower and watch this machine jumping out. May’s account is an example of culture and nature colliding in a person’s genuine
irrationality. Yet May’s account reads similar to a classic horror novel by award winning author Ira Levin: Rosemary’s Baby (Levin, 1967). Lines from Levin’s novel on evil: I can no longer associate; It gives me the creeps; Its like a wire inside me getting tighter and tighter; its moving, its alive; correspond so closely to May’s dialogue that it is possible to identify the cultural influence on her terror.
To place the ICD within a rational context it is necessary to see the ICD for the object it is. The ICD is electronic with action potential, thus it is capable of moving and twitching. However, the reality of the ICD as an object cannot ever negate the reality of terror in May’s experience. While Dell likened her hybrid person to having the miniature alien implanted within the human body of Lieutenant Ripley in the science fiction phenomenon, Alien (Fincher, 1992), May’s description was more cybernetic in that she referred to this machine. Nonetheless, implantation of their hearts with the other within their bodies brought horror, disgust, hate and terror into their lives.
May compared her scary experience to an experience of a different kind, convincing her that the implantation phenomenon was not natural.
A very good girlfriend had a baby. When she was extremely pregnant I could watch
it [baby] moving in her tummy. That wasn’t disgusting because it was natural and normal and exciting and supposed to be happy. But this [ICD] was not. There was nothing natural and normal and happy about this. It was so foreign and weird and wrong and … yeah, you know.

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 41
May and Dell both compared and contrasted their experience of the implantation
phenomenon with the evidence of a living entity within the body. However, Dell’s contrast was of the science fiction kind where Lieutenant Ripley was to become the mother of the alien baby that Ripley destroyed in order to save the world from alien invasion. Dell’s affinity with Ripley was that she wanted to destroy herself and the alien within, by suicide. Dell also drew on the cyborg concept in the film The Terminator (Hurd, 1984) to give meaning to her body experience.
I felt like … have you ever seen Terminator? That steel object you know the steel
robot? It has that layer of skin over the top of it. When he cuts into himself, he is a metal object underneath. And that is how I felt. I don’t know if it was a fear of what would happen to me it I was by myself. I was scared of my ICD going off. If I had someone there to distract me, I could put aside my suicidal thoughts. As soon as that person went away, and the house was quiet, straight away I would just want to go and find a knife. Simon spoke of science fiction when in dialogue about his experience of implantation by
referring to Robocop (Schmidt, 1987).
I’m not really fussed with it [ICD]. I’m cool. I guess you hear about it, you think of Robocop or whatever. I am waiting for them to grow me a heart. You ask someone who is healthy whether they think they should grow hearts and things like that, and then you ask someone who has some sort of problem and is on a waiting list for something: you get two very different opinions. Unlike the Terminator who was incapable of feeling pain or emotion, Robocop was a
reconstructed human being who experienced cybernetic hybridisation that saved his life, yet disallowed him to function as a socio-cultural Being. Devices, such as the titanium suit, were used in the film to create the illusion of an alternative reality, however disembodied. Simon’s reality was that he would endure the implanted heart until medical science furthered the genetic code of human existence. The Human Genome Project has encouraged the belief that editing the molecular code can alter, erase, revise, and reproduce like a computer program or a printed text (Lee, 1991).
Noel was familiar with the cyborg concept. “I have a machine inside me that can do these terrible things to my body.” His subsequent laugh was sardonic. “Ah, science fiction! Star Trek sort of thing. I don’t have to like it [ICD]. But I accept that it can save my life and has saved my life.” Implantation trapped liminal bodies in a bittersweet hybridised dichotomy where, to preserve life, terrible things needed to be endured. Whatever the outcome of future science, hybrid persons represented by May, Dell, Simon and Noel, would remain betwixt and between life and death, disembodied by implantation and subsequent body-liminality.

Carole C. Anderson 42
Threshold People in Other Body-Liminality Implantation of the heart and body is a surgical procedure. As with all surgery there is
the ever-present risk of infection. Hugh and Noel had not only the indeterminate hybrid-body disrupting their lives; they were to find themselves in another liminal existence that Victor Turner (1969) described as threshold people. The liminality of these two men was to include a further level of threshold being-in-the-world when they experienced a staphylococcus infection post-implantation. Hugh stated:
They just take you in, put it [ICD] in and sew you up. But I did have a problem.
After mine went in I got golden staph. I was in hospital for 3 months to get rid of the staph. Two of us got implanted the same day. They had to take his [ICD] out again. They could not clear the infection up and leave it [ICD] in there. It certainly … it affects you psychologically. It has taken from 1999 till now and I am just coming down off anti-depressant tablets. Even now it affects me. It was devastating. Acquiring nosocomial wound infection after the implantation of Hugh’s heart and body,
as well as suffering memory loss after a sudden cardiac death episode, was powerful in its body-devastation. The post-implantation infection complicated Hugh’s experience of liminal detachment from his known-body and the powerful feelings of devastation drained his resilience. In his distress Hugh was unable to reflect on the meaning of devastation. Noel described his experience with nosocomial wound infection.
The scar tissue was all pus and stuff like that. The infection looked like open pus that
didn’t look like it was going to heal. It was very liquid. My mother had Discord Lupus and I saw a lot of her body was pus where she was losing her skin and flesh. It kind of reminded me of those times when I used to change her bandages. It wasn’t a pleasant experience. Nosocomial wound infection is not only a state where the body is dislocated in a
wasteland of liminality; it is also a no-person’s-land where there is no illness classification and, therefore, no health system responsibility (Gardner, 1998). In the above excerpt this is demonstrated by Noel being the one who took responsibility for changing his mother’s bandages. Patients with liquid, discharging wounds are disembodied by an invasive entity that is foreign to the body-as-previously-known. Noel equated his disrupted, leaking, and socially unacceptable body to that of his mother’s. In losing skin and flesh the body is broken-down to reveal a persona as Victor Turner (1969, p. 95) observed: “It is as though they are being reduced or ground down.” It was as though the foreign organism coupled with implantation in an attempt to separate the body from the integrity of skin and flesh. Conversely, the body opened up in response to invasive and foreign other in an attempt to expel the unwanted entities that rendered the body as unpleasant.

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 43
Being Betwixt and Between Life and Death Being between life and death represents the deeper level at which heart implantation with
an ICD became the epitome of anguish to all recipients. This deeper level of other body-liminality drew all recipients in this study into the black of depression. Dell’s time of depression led her to the brink of suicide where she existed betwixt and between life and death.
I just climbed straight into the deepest depression. I was so depressed. I was suicidal.
I wanted to be dead. The fact that I had always anticipated being dead at 22, and the fact that I wasn’t, was strange in the fact itself: apart from having a metal object in my chest that I absolutely hate. Dell’s Ars Moriendo; The Craft of Dying (Stark, 2001), had begun when she was a child.
Medieval Christian tradition concentrated on becoming intimate with death as a way of understanding and preparing for the moment of leaving the body. “I discovered that I was going to die when I was twelve years of age. Quite a few people told me this; several doctors.” After a near death experience, Dell had accepted and prepared for death as nothing to fear. Dying was part of Dell’s living and was represented by the peace and the “upward light” she had already experienced.
Reaching my 22nd birthday was quite an amazing event for me. Besides I knew I
was pretty much down to a matter of days then, and I was just leading a very merry life style. Making the most of every single day, every second; I was having a wonderful time. The double apprenticeship of living and the art of dying (Lamont, 1973) was Dell’s Ars
Moriendo. The art of dying was fact in Dell’s belief system. However, the fact of heart implantation with an ICD became Dell’s reality. Consequently, she felt her body was wrecked and destroyed. The ICD was the symbol of her absolute hate. Dell had served her apprenticeship of living every second, only to be cheated of the art of dying. Thus, she considered her alternative dissolution.
I spent hours walking along the train line just wanting to jump. Hours and hours. I
would just be, wanting to slice my wrists. I thought I’d drive over the bridge and maybe just turn my wheel and slip off the side and it would look like an accident. Geez, I was tempted. Dell wanted the ICD removed; “please take it out,” but family and the cardiologist
refused her pleading, “you will die!” In a state of depression Dell, whose intention was to transform life into nothingness, turned to objects of everyday living, such as a train; a knife; a car. In the paradox of how objects are used “we go to the opposite extreme by distorting our own contribution in perception so as to make of it a power of creating ex nihilo [nothingness]” (Merleau-Ponty, 1962, p. 23).
In contrast, after facing mortality from numerous perspectives Dell arrived at a place where she thought of suicide as meaning quitter.

Carole C. Anderson 44
While I don’t condemn people who suicide, I do understand, far too closely, how they do it. You have got to love someone other than yourself, more. I’d rather take whatever, and live with it [ICD], no matter how unhappy I am, than upset everybody else to that extent. What was it about implantation of the heart with an ICD that compelled Dell to be
aggressive in the pathology of suicidal intention? The biological and psychological discontent that has been socially constructed as suicide is very real (Hacking, 1999). While all recipients in this study were not as aggressive in their discontent as was Dell, all suffered deeply in their reality of implantation. For example, Jade “was a heavy smoker. I thought well, stuff it. I didn’t particularly care if I died, really.” Dell elaborated on what depression meant:
Black. Black. No one can help you. To see the world functioning around you, but
you are not part of it. Depression is like hell. My own idea of hell … if I were to go to hell, it would be that black depression. The nature of heart implantation replaced one life threatening illness with another,
thereby sustaining body-liminality, betwixt and between life and death. The sacrosanct privilege (Hacking, 1999) of a person’s body is part of life, and how life
is lived is part of the determination of what kind of body a person identifies with.
My vision of it [ICD] is a metal object just waiting in there. Waiting in my chest to get me when I was not expecting it; in ways to take me down when I didn’t want it to. My whole body. My heart being far more important than any other part of my body, and it is alien. You know when it actually did discharge I could taste metal in my mouth for days afterwards. It was really bizarre. That is it. For me it [ICD] is like that big [arms wide] and it took up that much space. The scar was a huge, big, red, ugly, horrible thing. It is not natural to have a metal object in your chest. Dell was not able to accept the agonising responsibility for what had happened to her
body, as she perceived, against her will. Dell envisioned the ICD as a threat to the sacrosanct privilege of what her body meant to her as a person. In this way Dell’s perception was correct. The ICD could and would take her down at any time. Dell’s sense of taste persisted in reminding her of the power that the ICD maintained over her body and her living. An alien object within the most treasured space of her body invaded her lived situation. Its bizarre presence could be tasted; felt exaggerated in size; and held a supernatural component in Dell’s perception. Dell reflected more on being not natural.
It is like evil. It is an unknown entity. It is sort of like a … it is not a natural object
compared to a flower. I think that is very much how I felt. I felt like I was something natural but had been halved open and the inside of me was then replaced with something not natural, and evil in a sense. To have to recover your-self from that … when it takes up so much space.

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 45
Perceiving the body as the epitome of all things natural and good, such as a flower, lays the foundations for devastating dichotomies, such as replaced with something not-natural and likened to evil. Again, the body was located in a liminal place where body-identity and reality were blurred. Dell and other recipients perceived their bodies as blossoming in the beauty of youth, only to be open to a sense of malevolence.
All recipients in this study became depressed in their struggle to recover from a sense of malevolence. In her journal Jade wrote, “I feel I am on the road up the melancholy mountain again;” Hugh “was becoming hard to live with. I was up to 200mgs [antidepressant] a day;” Noel “could not get to sleep so I would get up and play [computer] games until it distracted me. I really needed distraction;” for Jock “it has been a total change of lifestyle;” Stan “was pretty screwed in the head. You go and approach somebody and they just tell you to piss off;” Simon felt “by the end of it I was all bitter and twisted;” May “went into a period of depression. Yeah, it was definitely a depression;” Jay’s cardiologist recommended “an anxiety disorder clinic. I don’t think the medical problems were as bad as the psychological. I have negative thoughts and feel depressed.” Dell added meaning to the psychological effects of heart implantation:
Nothing is good, you hate yourself; you hate everything about yourself; you can’t
bear to look at yourself; you don’t want to be near you; you don’t like yourself as a person. You can see everyone else, but you feel totally alienated, like you are in a glass jar. There is no laughing or smiling when you are depressed. Being in a glass jar could be an analogy for Virginia Woolf’s (1948, p. 10) metaphor of
the body as a glass sheet through which the soul can only gaze at the body-situation. In illness-melancholia we cannot know our own body or any other. “To look these things squarely in the face would need the courage of a lion tamer; a robust philosophy; a reason rooted in the bowels of the earth.” Hence, heart implantation alienates a person in body-liminality where boundaries between depression, blackness, hell, nothing, and alienation, are but a blur.
Being on the Brink of Life and Death Accounts of being in intensive care units (ICU) portray how impersonal, invasive,
modern bio-electronics compel a person to grapple with the most intimate issues and questions regarding mortality (Frank, 1995). Being in a coma, after a sudden cardiac death episode, exerts tension on the bonds between bodies and persons, and on the boundaries between the living and the dead. Hugh experienced three sudden cardiac death episodes and each time his heart was revived before nature separated his person from his body. Although Hugh could remember nothing of his ICU experience, he was aware that his failed heart had taken him to the brink of irreversible death.
The heart is life isn’t it. Your heart is your life. I mean it is not like you can do
without it. It is not like losing a kidney or something like that. It is the centre point of life.

Carole C. Anderson 46
Margaret Lock (2000, p. 234) wrote; “the altruistic act of organ donation permits meaning to be created out of sudden death.” This is where dispute involves nature and culture, the belief in the site of living or dying, or the believed vegetable returning to functioning life. Such was the experience of Dell after a second episode of sudden cardiac death. Prior to heart implantation Dell was to make the transition across body-liminality; being between life and death.
I was in a coma and on a life support machine. The doctors spoke to Mum and Dad
about organ donation. They warned them that I might be a vegetable. Vegetable to me means being like a piece of this grass [plucked a piece of grass]. You are there, but you are not taking part in the conversation. … Just there, part of the scenery.
Futility is a term often used in ICU when a person is defined as qualitatively having a
poor quality of life in the future (Goh and Mok, 2001). The predicted outcome for the psychological wellbeing of a person, given the definition of futile, after being retrieved from the brink of death, defies imagination. The prediction of a person’s vegetative state in ICU inevitably leads to the possibility of organ harvesting. Thus, Dell’s Being, as she perceived, was reduced to a blade of grass. In his aptly titled literary work, The Lazarus Case, John Lantos appealed to people in this situation to embrace uncertainty, to expect and to tolerate a range of outcomes (Lantos, 2001). However, neither organ donation nor transplantation was part of Dell’s moral value.
I would never have a heart transplant. I know that. The heart is … I know it is a very
old fashioned view but I believe that is where your soul is. That is where you feel things. That is what makes you, you … is in your heart. I don’t want to lose that. I am not prepared to lose that. You know, I am happy, I am dying; it is not scary. I’d much rather not have one [ICD] and die. It was Dell’s worldview that others should not be permitted to control her living and her
dying. Dell valued sudden cardiac death as a good death (Evans and Walsh, 2002). Having control over the circumstances of her death meant that she would choose her own dying trajectory. Implantation with an ICD meant Dell was controlled on the brink of life and death indefinitely and she was unable to go gently in that good night [death] (Ackerman, 1997).
In contrast to Hugh and Dell, Jade attended transplant clinic while her life was sustained by implantation of her heart with an ICD. Jade had lost both small daughters to sudden cardiac death at a time when children were not considered for implantation. Jade’s heart and her daughters were synonymous in meaning to her and she wanted her heart to continue beating as a gift of life for them. Jade captured her experience in its entirety. Jade’s situation was a constant ebb and flow between life and death.
The physical feeling having a dirty great hole in my insides that can only be filled by
their Being seems to be growing. My heart is still breaking painfully and yearning for my babies. It has been like having my heart cut out and being told to go on living. After Jock experienced a sudden cardiac arrest, he believed that he had been given yet a
further chance at living. Jock had been dying twice before, pre-implantation. Implantation of

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 47
his heart with an ICD was like a third life yet he knew he lived each day between life and death.
I can remember being in the ambulance and someone calling me. I have vague
recollections, sort of flashes. I probably consider this [survival] … I guess this is being silly but I think this is like my third life sort of thing. Before I got my valve replacement I was going down hill very fast. I could feel myself slowly sleeping more and more. I was just lying there going to sleep; I did not have any energy. I am not looking forward to a discharge from my defibrillator. I think that will probably happen seeing it has been so close several times. IT IS ONLY A MATTER OF TIME. In Jock’s reflection he re-opens his past, present and future experiences of living between
life and death. In this way Jock was recalling the notion of his own transience-in-the-world. At one point in time Jock had been moving ever closer toward the end of life and death rather than existing between. His slowly sleeping more and more represented his past closeness to death; implantation of his heart with the ICD represented his present retrieval from death; and his conviction of a future matter of time represented further closeness toward living between life and death.
Implantation as Being Linked to Body-Liminality Most family members initially became involved in heart implantation through
resuscitation attempts during the liminal state of sudden cardiac death. This allowed family members a window of opportunity to reach across the threshold between life and death in the retrieval bid that “finds its way to the core of my personal life and becomes inextricably linked with it” (Merleau-Ponty, 1962, p. 347). Thereafter, family members remain linked by their own body-liminality to the phenomenon of heart and body implantation with an ICD. Moreover, whatever the circumstance of heart implantation, family members would live with the constancy of potential sudden death of their loved one.
Being Linked on the Threshold of Sudden Cardiac Death, Pre-Implantation: Spouses’ Perspective
The phenomenon of heart implantation began for most family members in this study with
the trauma of witnessing the potential cardiac death of a loved one. This in itself portrays a liminal state in which family members’ lives would never again be the same. Witnessing the collapse of a spouse in the family home has been described as “an environment for conflict” (Sque, 2001, p. 106). Yet, this description appears inadequate in the context of the threshold of life and death. Writers dealing with sudden death in the home, focus mainly on interventions for family needs (Costain-Schou and Hewison, 1999). Thus, it was frustrating not to find literature that gave insight into the lived-world of the spouse in the throes of frantic resuscitation. Kara related her profoundly poignant attempts to retrieve her spouse who suffered a sudden cardiac death episode at home.

Carole C. Anderson 48
We were sitting around after dinner talking about what happened at the carnival and he [spouse] just slumped from the waist over, made strange noises and [young son] screamed. Then I threw him on the floor and started CPR for about 10 minutes. What began as an idyllic family interaction after an afternoon carnival, suddenly ended
in a liminal struggle over life and death. Kara’s introduction to the phenomenon of heart implantation was “devastation,” which took her to the threshold of the potential death of her spouse. Kara continued in more depth.
I just looked at him ... I slapped him across the face and [choked with emotion] …
Initially I thought he’s had a stroke. Then I just threw him on the floor and commenced cardiac and CPR. I guess while you are doing it, you don’t think about it. But after he was vomiting and it was revolting and fairly traumatic. I remember my knees were all scraped and my mouth was out here like this [indicated swollen]. I must have been fairly aggressive for the mouth to be all banged up and on my knees, because it is a wooden deck. Pulling him off the chair and his head hit the chair. Then back on the floor. It wasn’t a genteel thing. It was a pretty rushed thing. The pre-implantation experience for Kara, as for Zoe, was one of dissonance and the
potential liminal state of widowhood; “What I think about is not how he would die, why, or if he would suffer, but just that he would not be around anymore.” Kara’s instincts told her that her spouse was entering the ultimate liminality; irretrievable death (van Gennep, 1960), where he would be lost to her and their young family. This liminal situation was incongruous with what Kara was prepared to accept. In desperation Kara aggressively fought to prevent a stroke or sudden cardiac death from taking her spouse over the threshold into death, which excluded her. Kara’s vividly described body-liminality linkage brings to mind lines six and seven from the poem by Dylan Thomas entitled, And Death Shall Have No Dominion; “Though they go … Though they sink … And death shall have no dominion” (Thomas, 1969, p. 245). Even though resuscitation attempts were revolting and traumatic, Kara refused to allow death to have dominion. Her encounter with what was to be heart implantation with an ICD began with her being on her knees “all banged up.”
In pre-implantation experience, Bev’s linkage to body-liminality differed, yet was similar. Bev similarly felt devastated as she observed her spouse living a life that “was not as he wanted it to be.”
He would just sit down and he would be asleep within five minutes. He would have
to stop half way up the stairs and sit down. If we went out anywhere, we could not be any longer than one hour because he could not stay awake, and he was always out of breath. That was no way to live life. Um, it was very hard. It was happening to somebody who had been active before and then all of a sudden to go down like a sack of potatoes. In a pre-implantation situation, Bev could only observe her spouse in liminal sleep, a
life-threatening sleep where all others were excluded. In this way her spouse was gradually slipping away. Conversely, Bev described the crisis as sudden. Her metaphor, like a sack of potatoes, related to inertness and the unceremonious state of a person (Ritter, 2005). Pre-implantation devastation affected Bev in a way that “was not helping my health. My blood

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 49
pressure went sky high.” Bev was living her own body-liminality as “a living hell!” Subsequently, Bev’s spouse suffered a sudden cardiac death episode while travelling.
When he had the cardiac arrest he started turning blue, and purple, and every other
colour [nervous laugh]. And then, I saw all the blood run from the gash in his head. … I was just thankful there was an off duty ambulance man. … The ambulance man, he said, “lady, we have been to about 200 of these and your husband is the third one to survive.” So the odds are not good. You realise that it is a fine line, you know. Bev’s linkage on the threshold of sudden cardiac death was different in three major
circumstances. First, there were no young children present to compound the traumatic effects. Second, her spouse’s episode occurred in a public place rather than within the family home where memories surface on a daily basis. Third, Bev was fortunate to have a health professional nearby to render assistance. However, being witness to physical trauma and sudden death involving spouses was a commonality in a liminal state of their own; “I thought he had gone.” Bev captured the meaning of the threshold state between life and death; it is a fine line. Kara and Bev attempting to retrieve their spouses from the ultimate liminality of death describe vigorous CPR. It was a frantic action to maintain the physical body-connections that allow life to be lived through the body. In this way, “I find in the body, message-wires sent by the internal organs to the brain, which are installed by nature to provide the soul with the opportunity of feeling its body” (Merleau-Ponty, 1962, p. 76). In other words, vigorous CPR was the only way of forestalling the crossing of a fine line between life and death and endowed their spouse with the opportunity to hold on to Being. Parents would also struggle, within a liminal space, to maintain the message-wires of the physical body with Being, in relation to their child’s liminal state.
Being Linked to Body-Liminality, Pre-Implantation: Parents’ Perspective The death of a child has been viewed as the most traumatic and the worst event a mother
could endure (Rosof, 1994). As a mother, Jill’s pre-implantation experience on the threshold of life and death held double jeopardy; she temporarily lost living touch with her loved one and with her child. This would remain as part of the meaning of heart implantation with an ICD.
My middle size [2nd child] daughter was calling me. I went into the bathroom and
[1st child] was vomiting. She was unconscious. I dragged her out of the bathroom. What was it? Was it a stinger in the surf? Was it a toxin? What could account for this collapse? In about 10 seconds I was outside screaming for somebody else to ring an ambulance. Once again, an idyllic family situation switched to mayhem in an instant. Such an instant,
when a child who has been carefree and happy surfing is snatched into sudden cardiac death, defies usual expression. Jill’s spontaneous expletive was; “This was the Oh! Fuck! situation” that strikes dissonance, discord and indescribable distress into the Being of a mother. Each

Carole C. Anderson 50
was separate from the other by a liminal state; the mother losing a child; and the dying child. Jill elaborated.
I took over. Kneeling over her. Watching her. I got a great sense as a nurse, when a
patient dies. You just know. I actually got hold of her and shook her vigorously. She actually reverted. Self reverted out of VF into VT. They carried [her] outside while they were charging the defib[rillator], to get her clear of everything. I was just a mother then. I was holding the [baby] screaming in my arms, had the [2nd child] looking absolutely terrified. She told me later on that she thought [1st child] was dead. At that stage I guess technically she was. I couldn’t go outside to watch the defibbing because I felt that was just something I couldn’t do.
The desperation in Jill’s dialogue is almost palpable. Her dual identity as mother and
nurse combined as she watched over her child and her patient. Jill fought vigorously to hold onto her child who was leaving her to enter into cardiac death where neither the nurse nor the mother could cross the threshold. Jill could only scream, “DON’T DO THIS” and hope that somehow, somewhere across the threshold, her child would hear and respond. With the possibility of losing one child, Jill clung desperately to her other children. The threatening presence of death was terrifying in its unpredictability.
Mothers have described the sudden death of a child as deeply altering their sense of self as a mother; part of their self as a person dies with the child; and a profound sense of sadness becomes part of their embodiment (Gudmundsdottir, 2000). This situation was to become part of heart implantation with an ICD. Having nursing backgrounds, Kara, Bev and Jill agreed:
When you are working in the hospital and you have a terminally ill patient, you
know in the end they are going to die, you can accept that, you know. But not when it is somebody very close to you, you can’t! Body-liminality existed for both mother and child. The special bond between mother and
child is different yet similar to the bond between father and child. Overcome with emotion, Scott related his traumatic encounter with his child in ICU. This
encounter would remain with Scott to form part of the essence of heart implantation.
In ICU I had to hold her down. They did not have enough nurses to hold her. She still had the [urinary] catheter. I had to because she said she wanted to get out of the bed all the time. I kept saying: “you have a catheter; you just go to the toilet where you are.” She could not understand. I will never forget that. She just did not understand. Her mind was not with it. She was in a terrible state. The primal urge of needing to relieve bodily functions is an all too familiar scenario in
ICU for health professionals. However, for a loving father trying to protect his child from further harm by physical restraint was, for Scott, an unforgettable trauma. Clark Moustakas (1996, p. 4) wrote an account of restraining his five-year-old daughter following open-heart surgery. As a father, Moustakas felt “the most intolerable realisation that she was beyond my

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 51
reach, beyond my voice and touch. She was in pitiful plight; entirely by herself.” Such is the nature of heart implantation, where there is no crossing the threshold by family members; there exists a liminal state for both father and child. As a younger sibling, Beth’s link to body-liminality presented a different perspective to spouses and parents.
Being Linked to Body-Liminality, Pre-Implantation: A Sibling’s Perspective Sibling relationships are ever changing and complex whether the bond is one of harmony
or conflict (Ashton and Ashton, 2000). Furthermore, siblings have a bond that is not always shared with other members of their family. When one sibling has a life-threatening illness, the impact on a sibling, especially a sibling of the same gender, can be so deeply imbedded as to remain hidden until a sudden death episode eventuates (Faux, 1991). Beth was a youngster when her older sibling suffered the first of two sudden cardiac death episodes; “that affected me quite deeply … it was really hard for me to accept that [she] couldn’t come and play with me when I was a kid. … It is hard for children to understand I think.” This was Beth’s linkage to heart implantation and body-liminality. It was also her own liminal state; “I was often terribly afraid that she would die and leave me.”
Beth witnessed her sibling’s second cardiac death episode as a young adult and found that “from a very early age there was a lot of pressure to cope,” was more than she could bear.
She just dropped down, just totally. She was holding a bottle of water and she just
fell to the side and I remember seeing this water spraying everywhere. She just hit the ground with a loud, WHACK on the head. We started doing the whole rescue thing and I was trying to clear out her mouth but she had clamped her teeth in a seizure thing. It must have been some sort of muscle spasm with the heart going into VT. I knew, because her colour went strange. I started to really get upset and one of the gym ladies said, “shouldn’t you be starting CPR now?” So I rolled her over onto her back. She was still making this gasping sound like her teeth clamped. I think I was just sitting there holding on to her foot or something while they were working on her. I couldn’t think. The paramedics came and you know it is bad when the paramedic comes in and goes, “holy shit!” I knew it was bad anyway. They had to cut her T-shirt and cut her bra and start doing things with the paddles. I had to keep holding on to her. I don’t know why. I could not let go of her. I felt somehow I was keeping her there by keeping contact. Not even a life-time of living with her sibling’s illness could prepare the young, adult
Beth for the responsibility of attempting to reclaim her older sibling from the liminality of pre-implantation death. Being witness to the throes of a sibling’s death struggle involving the discoloured body, the contortions of seizure, and the gasping sounds of escaping life, rendered Beth powerless and paralysed. This sense of total paralysis within reality engenders an inability to act, to think, to do the things that are normally spontaneous; it is a liminal wasteland; “I was totally overloaded.” Beth was trained in CPR yet when faced with her sibling’s potential sudden death, the self became childlike, helpless and out of control (Lewis, 1992). In such situations the self can experience the sensations of physical freezing, leadenness and numbness (Wurmser, 1995). Beth’s pre-implantation experience of reaching

Carole C. Anderson 52
across the threshold of sudden cardiac death became a physical holding on and keeping her sibling there by keeping contact. It was unthinkable “to let her go” because Beth believed from early childhood, “that was my job, my responsibility.” The time of Beth’s “worst fear” had eventuated, yet no amount of preparation could sustain her in a liminal hour of need. Time could never erase what heart implantation would mean for Beth during reflection; “You know, you just think, this is it, this horror we have been living with has finally emerged.”
Family members realised their crises through the unique language of body-liminality. The symptomatology of the body (Frank, 1995) that lingers betwixt and between life and death, speaks a language already described in the preceding pages of this chapter. Thus, family members would be confronted with heart implantation on a different level in the constancy of altered family living, and the impact of the liminal-body and the ICD. Such confrontation would include engagement with healthcare professionals.
Implantation as Engagement with Body-Liminality
Body-liminality for cardiac nurses and paramedical personnel is different from recipients
and family members because of their primary professional perspective. Recipients and family members became involved in heart implantation through uncontrollable life-circumstances. In contrast, health professionals made an individual choice to engage in the area of cardiology and to include the associated knowledge of the study phenomenon in their life-world. In this way, the group unknowingly chose van Gennep’s (1960) three-stage rites of passage where liminal separation from mainstream place-in-the-world locates people in a liminal transition before incorporation into their chosen place-in-the-world [van Gennep’s emphasis]. While cardiac nurses chose cardiology as part of their professional life, the paramedical practitioners unintentionally became involved in cardiology.
Why would cardiac nurses choose this specific liminal state? Elizabeth Teather (1999, p. 1) suggests, “Our passages, intensely personal, thread their way through, impact upon and are influenced by the institutional fabric of social life.” Hence, cardiac nurse’s perspectives on heart implantation with an ICD are vital sources to assist understanding in this chapter, because of intensely personal life-choices that impact upon recipients and family members. Cardiac nurses contribute more significantly than paramedical personnel in this chapter because of their closeness to the phenomenon of implantation.
Synonyms listed for the word engagement include: embodiment, incorporation and responsibility (Dictionary.reference.com., 2007). Engagement with the liminal body impacts on embodiment and what it means to implant a person’s heart with a permanent ICD. However, do cardiac nurses and paramedical professionals understand what has been incorporated into their life-world? It befalls health professionals to take individual responsibility for developing as much understanding of the study phenomenon as possible, as Rae stated: “I don’t think we understand exactly what people go through, having an ICD put in. I mean I don’t understand totally either.” The etymological origin of engagement is from the late Middle English ingage, meaning to pledge something. During the 17th century the meaning expanded: involve oneself in an activity (Ritter, 2005). Thus, implantation as

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 53
engagement with body-liminality, in this chapter, is to be involved with hybridisation of a person’s body and heart with a permanent ICD. Cardiac nurses attempted to portray how they perceived engagement with body-liminality from their threshold location. Laurie Spurling (1977, p. 28) explained the embodied perspective.
Indeed, my visual field, since it is animated and patterned by my phenomenal body
which is oriented towards its tasks and interests at hand and engaged in marking out possible areas of activity in the world, is also a phenomenal field. Now the fact that my perception is embodied means that it is perspectival. If I attend to my actual perceptual experience, I will become aware that I only see ‘profiles’ of any object, that is, I see it at any given moment from one side at a time. Now, of course, subsequent perceptions can ‘fill out’ the perceived object as I move round it and view it from different sides and angles: nevertheless, at any given moment, I can see no more than my perspective allows. Lea offered a concise account of her perspective in relation to tasks and interests at hand
in the phenomenal field of engaging with implantation as body-liminality.
Certainly it is very frightening being taken down there and everyone is gowned and gloved and [person is] put on a hard table. The injections, then they put this thing [ICD] in. People are talking above them and around them and to them. But yeah, it is a very frightening experience for a person. There is a sense of powerlessness that happens. But knowing what is happening and how it is going to work; how it all works down there; why there are green gowns. They have an oxygen mask on. Knowing, before they go in, I think it all helps with that experience and make it less traumatic. There are many existential barriers outlined in Lea’s account of heart implantation with
an ICD. The cardiac nurse refers to the ICD as this thing. This appears as a dilemma on a pre-reflective level in engagement with heart implantation. The barriers of gowns and gloves locate both cardiac nurses and the person in liminal-necessity because this is how it all works down there. The mass of technology, that is heart implantation’s phenomenal field, renders the person afraid and powerless. Being aware of the person’s trauma places responsibility on the cardiac nurse thus, the cardiac nurse outlines the procedural barriers that will traumatise the person. However, the dilemma remains; being told of these unfamiliar barriers and contexts appears inadequate in allaying the certainty of fear and powerlessness that is heart implantation as body-liminality. Raabe (2001, p. 187-9) perceives this professional perspective as an unreasonable attempt at neutrality. Thinking the person “is knowing,” simply because he/she has been told, “can seem alarmingly remote, uninterested, apathetic, and patronising.” In their awareness of patients’ powerlessness, is it possible for cardiac nurses to “break out of a perspective that is causing [them] to be stuck in a seemingly unsolvable problem [dilemma]?” The phenomenon that is heart implantation is explored more closely in this chapter.

Carole C. Anderson 54
Being Involved With Actual Perceptual Implantation Most cardiac nurse participants in this study avoided giving their perspective on the
actual heart implantation procedure. However, several nurses were willing to share their thoughts. Rae drew on her extensive experience as a cardiac nurse to ‘fill out’ her perspective of heart implantation with a permanent ICD and its context.
I suppose it is a cold area. That would be the first thing you would be conscious of.
A lot of people gowned; you can only see their eyes. There are a lot of things going on around you and you probably feel vulnerable. Powerless, like I am in their hands; do I trust them? They are the things I think that would probably go through my mind if I were lying there. The consciousness of being in a cold area sets the scene for heart implantation as
crossing over the threshold into body-liminality. A person desires and needs body-warmth. Thus, a cold context was the first of many dehumanising sensations during heart implantation. Jody also recognised this coldness in her poem, Fire and Ice, written as a prelude to her phenomenological dialogue. The poem is a contrasting metaphor that personifies fire as the warm-blooded human heart implanted with the ice-cold metal ICD:
The fire of the person is being dampened because the heart is not working to
potential. There is no longer that flame [of wellbeing]. The fact that the heart is at risk, the person is at risk. That cold thing [ICD]: … having to accept a foreigner, and to rely on it. Gowned figures unrepresentative of people, except for their eyes, add to the mystery of
“things going on,” and heart implantation evokes vulnerability. Vulnerability leads to powerlessness and trust is questioned because of the context of heart implantation. Overpowering a person already in a life-threatening, liminal, void can create body-sensations “so extreme that no human caring can assuage” (Gadow, 1988, p. 8). Rae continued to reflect.
Lots of light. Strange noises. Things that you are not used to. I think the
vulnerability is exacerbated because they will then come along and pull off the sheet. This exposes your chest while they put the drapes on. You sort of lose a lot of pride and privacy. While the staff are very reassuring and they explain everything as they go, I think people still feel very vulnerable. Perhaps even frightened about what is going to happen. In this situation, senses become heightened because of tortuous lights, strange noises,
unfamiliar things, and smells. In this liminal situation, consistently referred to as vulnerability, the person is deprived of any thread of security attached to the covering sheet when it is pulled away from the body. Consequently, heart implantation becomes more of a reality as the chest is exposed. Being exposed and deprived of pride and privacy, even temporarily and with nonsensical reassuring, the Being within the physical chest is objectified. Merleau-Ponty (1962, p. 253) recognised deprivation:

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 55
To invert an object is to deprive it of its significance. Its being as an object is, therefore, not a being-for-the-thinking-subject, but a being-for-the-gaze, which meets it at a certain angle, and otherwise fails to recognise it. Rae emphasised heart implantation as the person being out of control.
[Implantation] probably impacts on people’s self esteem, feeling that everybody is doing this to me and I don’t have any say. Like out of control. Well, not being able to have a say in what is happening. I think like someone who has had a stroke, they can’t even wipe their nose because they don’t have any control. Returning briefly to the word “chest” as being significant as the site of implantation and
as the part of a person’s body where the heart is located. The etymology of chest is from the Greek kiste meaning box (Ritter, 2005). Metaphorically, the heart, which is culturally and socially treasured, is locked within a person’s treasure-chest. In terms of this treasure-chest, heart implantation impacts on self-esteem, renders the person invisible, out of control, without voice and, therefore unheard. Jody interpreted her poem capturing the intrusion:
In the middle of this warm human being is this ice cold pond and it [ICD] needs to
be there. The person didn’t ask for it; doesn’t want it, but they are paying [personal price] for it. It exists. The person has to put up with it or, um, the alternative is not the desirable thing. Thus, heart implantation is disembodiment because the person is not in control of his/her
body but is controlled by the protocols of the implantation procedure. The rules of control in the implantation procedure are forbidding and unforgiving, to use Rae’s analogy, in the event the person attempts to wipe his/her nose. In her awareness, Rae, as a cardiac nurse, is similarly a liminal captive of control because of her inability to cross the control boundaries (Lawler, 2002). Rae continued to relate implantation:
They have probably had some local anaesthetic from the physician. Then machines
coming around them, the x-ray machine, fluoroscope. If they are claustrophobic, they are probably feeling quite hemmed in, unable to get away; a bit like a prisoner. Even if they are not claustrophobic they are probably feeling that. I think just that feeling of being imprisoned in that area and not being able to get away. They are conscious of smells, stuff that the drapes have been in and they have been sterilised. They have a smell about them. All that type of thing and they would probably feel quite nauseated. Implantation imprisons the person within its insurmountable technology. These
technologies of heart implantation include the pharmacology of anaesthetics, the machines, the drapes, the sterilisation, the smells, and each bio-technology already mentioned. W. Norris Clarke (1972) argued that intended beneficence in developing bio-technology tends to produce depersonalising and dehumanising effects. Principally, the negative effects are endured by those who are excessively subordinated by the bio-technology, such as those involved in heart implantation with a permanent ICD. Being imprisoned in the heart implantation context is what Clarke (1972, p. 257) termed as “suppression of human

Carole C. Anderson 56
freedom.” Thus, cardiac nurses’ engagement with heart implantation is a state of body-liminality because they are within the service of bio-electronics rather than self-regulating solutions for the human problems that technological advances present. Rae expanded on how she felt about the person’s body under the drapes, the visible body-area selected for implantation:
It is just a part of the body that is being operated on. I don’t have any … I am able to
switch myself off and just say, OK, we are putting in an ICD and that is here [body-part]. I am not sort of feeling, oh, my goodness they are cutting through the skin or anything like that. I am able to just see it as a procedure. Put in an IV or something, it is just something you do. Writing about his life-threatening experience of procedures in ICU, David Rier (2000, p.
73) stated: “In this I was alone.” He felt defined in empirical terms, with health professionals gazing at an array of bio-technology as a priority before acknowledgment of his person. He found this situation disconcerting and incomprehensible because he felt competent in communicating how he felt. Thus, heart implantation is defined as engaging with body-liminality because the cardiac nurse is “able to switch myself off,” and “to just see it as a procedure.” In other words, the cardiac nurse is disengaging and detaching from the person during heart implantation. Disengagement removes the cardiac nurse from the person and displaces both in liminal-aloneness.
Rae also confirmed that the focus was primarily the implantation procedure of the ICD:
I suppose for the person inserting it [ICD] … it does to a great degree. But they would also be conscious of monitors, breathing patterns, communicating with whoever is [there]. They always have an anaesthetist there even though they don’t always have a full anaesthetic. So yeah, communicating, looking at observations, what is the blood pressure now, what is happening on that screen, and where are we with the wire? I suppose they are fairly well focused, they are taking in the big picture as well as the little picture. With no mention of the person’s subjective-body that has been depersonalised with many
descriptors, such as imprisoned and out of control, he/she becomes submerged beneath preoccupation with technological apparatus. Thus, heart implantation as engagement with bio-electronic-body-liminality reveals itself to be irresistible. Rae’s dialogue portrays cardiac nurses’ consciousness to be of “monitors, breathing patterns, communicating” with medical personnel, “looking at obs” such as blood pressure readings, and the fascinating screen that shows “where are we with the wire [pacing wire].” The word ‘we’ signifies group engagement in and preoccupation with the implantation procedure. A question about the person under the drapes breaks the big bio-electronic-picture. Is it feasible that focus can be divided between the person and the bio-electronics and yet both receive full-attention? Rae continued.
Well, from my experience, most of the staff that I have worked with in that area has
always been conscious of the patient. They will ask the patient, are you feeling OK? Is everything alright? Are you warm enough? It won’t be long now. Do you have any pain? Sort of just how they are feeling and how they are dealing with it. And reassuring them

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 57
that they are a body … not a body [difficulty here] … a person under there, and they are not being forgotten while all this is happening. My dual perspective as a cardiac nurse and as a person who experienced electro-
physiological studies and cardiac ablation, contrasts with Rae’s statement. Without any warning I lost consciousness during the six-hour procedure. No doubt this was a vasovagal episode. On regaining consciousness I signalled to a cardiac nurse who was watching the screen and told her, “I lost it [consciousness].” Her immediate contradiction, “No, you didn’t,” was not warm, concerned, or reassuring. I remember a feeling of dismay and dismissal. My claim was not documented. Losing consciousness is not something a person imagines. This was not an isolated incident. During a second procedure of cardiac ablation I experienced left-arm radiating pain and again told a cardiac nurse. Time passed and the cardiologist continued with ablation until I signalled him that I was in distress. His response, “why didn’t you tell anyone,” was curt and nullifying. The cardiac nurse had left the area.
As a cardiac nurse and cardiac researcher I know these experiences are not isolated and are in need of expression because nurses may choose not to care, but negative meanings may result in cardiac nurses choosing to disengage from patient involvement (Montgomery, 1997).
Rae moved on to the defibrillation phase of heart implantation when the patient is
control-shocked for purposes of testing the ICD:
It always gives me a bit of a shiver. It makes me a bit goosy. Just because I think that was an electric shock. There is always a convulsion. It is probably not as dramatic as when you have a patient in an arrest situation. That to me is always more spine-tingling. I have to give them a shock there and then, because the adrenaline is rushing and everybody is sort of on edge; save that body, come what may. [Conversely], in the procedure of an ICD, it is more of a controlled situation. … It is just part of the procedure. Thus, the person enters hybridisation and body-liminality through electric shock and the
throes of convulsion. It is spine-tingling science reality. Philosopher, Nicholas Berdyaev (1972, p. 209) argues that the hybridisation of body and bio-electronics deals a terrible blow to emotionality and human feelings. Bio-electronics “endangers the heart, which can scarcely bear the contact of cold metal and is unable to live in metallic surroundings. The process of the destruction of the heart as the centre of emotional life is characteristic of our times.” Defibrillation is a liminal dilemma for many cardiac nurses. I have witnessed many physical reactions from cardiac nurses during an in-hospital cardiac arrest; the most severe being the inability to securely hold fully charged defibrillator paddles because of anxiety. The distressing pressure to be engaging with “save this body” is very real in the clinical setting. Lea responded when asked what implantation meant to her as a cardiac nurse.
Having a device, a metal device put into their bodies and it is designed to do a
function and in this case it is an ICD. It is designed to defib[rillate] them out of a life threatening situation and all that goes with that, such as the surgery, all the procedures,

Carole C. Anderson 58
the pain involved, and the uncertainty of it all comes into the term ‘implantation.’ [Another word for implantation?] I don’t know … I don’t know that. Lea was unable to step outside her clinical perspective, which encapsulated implantation
as engagement with body-liminality. However, “uncertainty” was similar to Jody’s descriptor, “intrusion.” Jody’s interpretation aligned with Nicholas Berdyaev’s perspective.
It is the thought of having something artificial inside the body. Everything that the
heart represents to the person is being threatened, physically, emotionally and spiritually. The absolute, sheer terror of having the heart tampered with. Intrusion is … the person did not ask for it [ICD]. Jody’s phrase, having the heart tampered with, suggests that this is the immediate point
of jeopardy for the person. A synonym phrase for “tampered with” is “being altered” (Ritter, 2005). Philosophical counsellor Shlomit Schuster (1999) drew on philosopher Emile Durkheim to point out that it is a person’s altered state of self rather than the circumstance that causes absolute, sheer terror. Thus, how cardiac nurses and others enter into engagement with a person’s altered body-state emanates from their perspective on extending life through liminal hybridisation of heart and ICD. Being engaged with body-liminality is different to being engaged in body-liminality as cardiologists revealed in their dialogue.
Implantation as Engagement in Body-Liminality
The existential knowledge to be found in the dialogue of cardiologists in this study,
demonstrates the persuasion that scientific knowledge can exert over a patient’s decision-making in relation to implantation. Cardiologists are the innovators, the initiators, and the group whose engagement in body-liminality, through the hybridisation of human-body and cybernetic-bio-electronics, can illuminate how and why the liminal-body is possible. Through an understanding of the cardiologist’s existential perspective it may be possible for recipients of ICDs, family members, cardiac nurses and paramedical personnel to confront the liminal-body. Without this understanding there is the potential for a “turning point where I become conscious that I [self] can be annihilated” (Jaspers, 1986, p. 112) in the liminality of heart implantation.
Cardiologists’ engagement in body-liminality through implantation of a person’s heart with a permanent bio-electronic ICD may be described as Kierkegaard’s (1968) leap of faith. In this study, cardiologists’ leap of faith epitomises their existential and professional acceptance of the challenge to extend life while potentially extending death, the ultimate liminality. Cardiology has a cultural history of engagement in body-liminality-states, in that life must be lived forward, but understood backwards. This historical flow began with resuscitation and external defibrillation. Attempts have also been made to minimise cardiac-related symptoms with medication technology. These leaps of faith are intended to reverse cardiac death from within the hospital setting and to extend life-within-the-world by implantation with the bio-electronic ICD.

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 59
From the era of bio-electronics, including pacemakers and ICDs, cardiology has engaged in a new paradigm of heart-related illness. Cardiac-related illnesses are an unacceptable peculiarity to be managed by the intractable systems of biomedicine and bio-power (Foucault, 1976). In this way a person’s responsibility for his/her life trajectory falls under the agency of cardiology. Thus, as cardiologist Sean concluded:
We might find all these wonderful things and suggest all these odd and
Frankensteinian type procedures and devices and so on. But unless we find out exactly what is important to the patient, we might be barking up the wrong tree. We might be doing something that the patient really does not want, or does not understand. And that is doomed to failure at some stage. Body-liminality in a life-threatening illness has been described as a black box (Little et
al, 1998) where a person is set apart from others in the disturbing boundedness of life-and-death (Giddens, 1990). Sustained body-liminality resembles black holes of experience (Hawking, 1988) where survivors of life-threatening illness, such as a sudden cardiac death episode, are confined in an oscillating life-and-death vernacular between body and self. Cardiologist Gary used the phrase, “change in body-habitus.” This use of the vernacular by the cardiologist shows his body-self engagement in body-liminality through the implantation of a person’s heart with a permanent ICD. Sean added meaning in the way that his perspective involved people.
I think there is always something more to learn about peoples’ hearts, and I think
one of the things that interest me is how peoples’ attitudes and opinions actually influence what happens to their heart’s physiology. I think that is one of the major challenges in cardiology … is to integrate the psychological and physical aspects of cardiac function.
Being-in-the-World of Engagement in Implantation Professor of Medicine, Psychiatry, and Medical Humanities, Timothy Quill (2001)
argues it is an unduly simplistic notion that patients have autonomy in life-threatening situations, such as heart implantation. Cardiologists offer information, present options, relay statistically relevant risks and benefits, and make recommendations in relation to the highly technical ICD. The life-threatening event or the recommendation, whichever happens first, is the beginning of body-liminality. Sean explained “you have to make it [implantation] simple enough so that they do understand.” He continued with how he would offer heart implantation information.
You go onto what the positive aspects are. What the chances of success are. What
the chances of failure are and tell the patients what they are. And then say, is that what you want? Here are the options. You can do nothing and carry on as you are, right, with these risks. You can have drug therapy, which most of them are already taking … forever. These are the pluses and minuses of that. Or you can have this procedure and have this device. They are the options.

Carole C. Anderson 60
The dichotomies of implantation outlined by Sean are far from simple; positive opposed to negative, success opposed to failure, risks opposed to benefits, pluses opposed to minuses, medication opposed to the ICD. Similarly, cardiologist and ethicist Neil spoke of dichotomies:
One must of course follow the medical development and at least have some basic
knowledge of ICDs. It is therefore important to know when ICD therapy might be indicated and to understand the possible advantages and disadvantages associated with it. Thus, body-liminality is spiked with dichotomies because heart implantation continues as
a life and death threshold. Patient decision-making as a passive role has been equated with physician paternalism
that controls and dominates the patient’s options (Quill and Brody, 1996). The question of whether the cardiologist’s knowledge and power presented a barrier within engagement in implantation prompted the following response from Gary.
I don’t think so. Patients come for help. I mean I tell them what I can do and I …
they make the decision. I make the recommendation but they choose to go ahead. I don’t say, like, you need it [ICD]. I say, like, this is what your life is going to be like with it [ICD]. If you want to go ahead … fine. I make the recommendation … they choose. I don’t choose for them. I don’t insist they have anything. So it is their choice. While Gary rejected the notion of personal barriers between patients and cardiologists,
Timothy Quill (2001) experienced difficulty with a patient who refused invasive technological treatment from the perspective that the physician was not the person living the treatment. Similarly, Sean responded to this notion.
You mean because I have not been there myself? Um, I think there are barriers
between everyone in any situation. And that is why all the cards have to be put on the table. Patients often say to me, “What would you do?” And I say, “Well, that is not a fair question because this is not me, this is your life and I am here to give you advice. I am not here to live your life for you.” That takes a bit of getting round sometimes. The ways of engagement in heart-implantation, as in any life-threatening state of body-
liminality, are multifaceted and complex. Timothy Quill (2001) strongly recommended technology-dominated approaches to patients in life-threatening situations. He also recognised other engagements, such as paternalism and control. Conversely, the too-passive physician alienates patients in body-liminality through the absence of a negotiating partnership. Sharon Kaufman (1997, p. 191) wrote of the “most laissez-faire approach” as being within the statement, “Its his [her] decision. Its your job to inform him [her] of the options.” However, Sean added, “It is very hard to give them [patients] information in a neutral way, because we are all enthusiastic for new technology and um, we think we know what we are doing” [sardonic laugh].
Cardiologist Beau used the descriptor “border-line,” which definitively locates engagement in body-liminality for all involved in life-threatening cardiac implantation.

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 61
You realise that what you are doing does have … no matter what you do somebody is going to die. You are never going to get through a year, ah, a year without somebody dying. You are going to operate on people, you are going to choose people who are border-line, whether you should be doing them or not. You give them a chance and you tell them that. You know this is a chance, and you may not make it through.
Beau relegated cardiac survival to a life-death-liminality described by H. Evans (1993, p.
83) as an “ever-widening chasm” of bio-electronic body-hybridisation. The concept of “chance” in relation to medical science yielded more than six hundred articles from the ProQuest database. Engagement in chance by cardiologists would place enormous stress on a person already close to death; ultimate body-liminality. Laura Landro (2003, p. 2) cautioned about “too much responsibility on patients for safety, because it may end up shifting blame for error to the victim.” In contrast to Beau’s perspective, cardiologist and ethicist Rhys’s perspective on heart implantation included engagement in the least amount of chance:
I am still very much in doubt if this [implantation] is the right way to treat people in
most cases. But, for some, where the diagnosis is absolutely correct and there is scientific evidence for a successful outcome, I recommend it. Undoubtedly the quantitative epistemology of medical science (Gallagher and Durant,
1993) that aims for “correct diagnosis,” “scientific evidence,” and a “successful outcome,” is invaluable in decreasing physiological chance. However, as cardiologist and ethicist Neil argued, this epistemology can be coupled with patient wellbeing.
The physician is confronted with several medical and ethical questions when
deciding whether or not a patient should be offered an ICD. Does the patient have a sufficiently high risk of a sudden cardiac arrest, which can motivate an ICD? How will the therapy influence the patient’s physical and psychological wellbeing? In fact, generally speaking I am neither particularly interested in nor good at high technology devices medicine. I consider myself being more of a generalist, or perhaps humanist, than a sub-specialist. Similar to Rhys, Neil’s concern related to the efficacy of heart implantation with an ICD
as indulging in “high technology devices” that hybridise a person’s body and alter his/her “physical and psychological wellbeing.” This engagement in an altering potentiality is what I have presented in this chapter to be implantation as body-liminality. Neil’s perspective is tempered with a humanistic empathy for a person’s wellbeing that relegates the bio-electronic ICD to a secondary consideration. Professor of Psychology, Martin Hoffman (2000, p. ii), considered such a perspective as “empathy’s contribution to altruism and compassion for others in physical, psychological, or economic distress.” Nonetheless, ICD bio-electronics does have its advocates. Cardiologist Zane viewed the ICD as the “solution:”
We cardiologists thought for many years that pills would save these patient’s lives.
They didn’t. The solution was a device that could work for outpatients. Not many other treatments have so direct an impact on life and death as an ICD. It is thrilling to handle such a treatment.

Carole C. Anderson 62
Returning to the concept of efficacy in relation to ICDs, Warren Strugatch (2002, p. 6) emphasised the point that high-power technology is considered “synonymous with efficacy” by cardiologists. Furthermore, cardiologists were portrayed as more committed to advancing invasive bio-electronics, such as laser surgery and implantation, because this bio-technology has been touted extensively in professional journals and seminars. This argument by Strugatch (2002) would thus partly explain why it was a struggle to get cardiologists’ attention when challenging the efficacy of unquestioning engagement in implantation of a person’s heart as body-liminality.
As already stated Sean was asked by potential recipients of ICDs, “What would you do?” Sean thought this an unfair question. However, during dialogue I asked, “Would you have an ICD?” Sean’s response held reservations.
I think it would depend on the circumstance. You know, if I had an event, if I was in
a situation, which was um … consistent with current medical practice and evidence then I will do it. Um, I don’t know if you watch Star Trek, but Spock says there are always alternatives, Captain! [laugh] … you know? And so you put the alternatives. You say well, if we do nothing then your risk of death is X% in 2-3 years. And with the device it is a bit less. It might give you 5 years or something like that. And some of them say, well, I will take it. And they are allowed to change their mind later on. Sean’s dialogue encompasses the liminality-effect. He related to acceptance of the ICD
in the first person “I” while considering the “circumstance” of a cardiac “event,” and while engaging in the cardiologist’s comfort zone of construing the body in terms of “current medical practice and evidence.” However, a reference to the hybridised and unemotional Spock from a popular science fiction television program, Star Trek, provided relief from delving into his first person issue of mortality. Thus, the ultimate liminality of life and death risk is dissociated in the context of second person “you,” and third person, “them.” Death, as the ultimate liminality is given the unknown quantitative value of X%.
The ontological question of whether Gary would accept implantation of his heart with a permanent ICD sparked a philosophical debate. His final response was initially dissociative yet with a different persona to Sean.
I don’t know if I can help you. I guess … [fumbled with study sheets]. Well, if you
want to know what patients feel about it, you have to ask them. If I needed one [ICD], I don’t know what I would feel … until I needed one. I mean it is something I don’t even think about. [Why?] Sure. Well, there is no point in crossing bridges until you come to them. I don’t go around thinking about problems. I guess I spend too much time dealing with them. Yeah. I don’t think about having one personally. There would be no question. If I had … if I was at risk of sudden cardiac arrest, I would have one. The procrastination expressed by Gary suggests that there are cardiologists [and other
practitioners] who become so engrossed in other peoples’ life and death liminality, and possibly the power and prestige that surrounds such mystique (Tassano, 1995), that a sense of untouchability evolves.
The concept of being untouchable because of power and prestige brings to mind the film entitled, The Doctor (Ziskin, 1991). This film was based on the autobiography of physician

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 63
Edward Rosenbaum, entitled, A Taste of My Own Medicine. The title is self-effacing in that the character is a cardiologist who has long treated patients as ‘other people,’ who have life-threatening illness, until he is diagnosed with throat cancer. Thereafter he becomes part of a long line of patients on the other side of body-liminality, lost in a mechanised health care system. As a patient, Edward Rosenbaum was forced to see the bureaucratic hospital image, physicians, and medical treatments, from a patient’s perspective. A technically competent physician disdainfully informed him of his diagnosis, which he was unable to assimilate. In the film, as in reality, Edward Rosenbaum initiated an educational program for medical students to instil empathy and humanism, insisting they be treated as patients for a time to experience directly the humiliations of modern medicine. The film has become required viewing in several medical schools as a lesson in humanitarian care (Clark, 2001, p.146). Hence, the perspective of “no point in crossing bridges” into body-liminality prevents the cardiologist from attaining a humanistic understanding of heart implantation with an ICD.
The meaning of implantation of the heart with a permanent ICD appeared, from Beau’s dialogue, to revolve around physical symptoms. His response to the phenomenological question of personal implantation was initially strained.
Um … well, it would be for a life-threatening condition. I would accept it, very
willing, very gratefully, very willingly. If I was given the opportunity, if I had a VF arrest or something like that. I mean it would save my life next time, so I wouldn’t have a problem with it at all. I mean there would be a comparative as to whether you were waiting for it to go off or not. But I mean what do you do without it? Do you wait for your heart to defibrillate and not survive? I don’t think there is really much … it is a difficult situation.
As a cardiologist, the thought of dying from a life-threatening illness when highly bio-
electronic life-saving devices, such as the ICD, are available was not compatible with Beau’s worldview. Lacking clarity surrounding the goals of medical science and life-extension is not usually part of the medical dialogue (Quill, 2001). Furthermore, a lack of support for medical bio-electronic intervention could cast doubt on professional dedication. However, Beau questioned the difficult situation of choosing between life-extension and living in wait for the ICD to go off or not. Thus, engagement in implantation engenders body-liminality for cardiologists. The above dialogue begged the question of whether Beau considered his own mortality:
Oh. No. I mean it is like anybody thinking about their [his/her] mortality. I don’t
really think about it. I mean, why worry about it? It is something I might have to face in the future, but I can’t do anything about it. Zane supported the worldview discussed above; “I am positive. And it [ICD] supports
my task as a doctor, but one must consider all its impact, not to forget quality of life.” In supporting the task of being a cardiologist who extends and prolongs life, it would be imperative to establish and maintain an awareness of body-liminality in relation to heart implantation with an ICD. Only through communicating such awareness can health professionals hope to convey benevolence to recipients and family members.

Carole C. Anderson 64
Conclusion For mere living is not a good, but living well
Seneca (AD 3-65) While it has not been possible within the confines of a book chapter to include the full
impact of the existential themes that framed the results of my research, the concept of liminality, in the context of heart implantation with a bio-electronic ICD, presents a powerful and thought provoking lens through which scientific personnel can examine their personal approach to practice. Moreover, there is the potential for all persons involved in heart implantation to be more aware of their own humanness, vulnerability and ultimate mortality. Thus, what valuable education can be gleaned from this chapter that may be used to lessen existing body-liminality experienced by concerned groups?
Over centuries, views on the ultimate liminal state, mortality, has varied little. The philosopher, Seneca, cited by contemporary philosopher Louis Pojman (1992, p. 34) wrote:
Life has carried some men [women] with the greatest rapidity to the harbour, the
harbour they were bound to reach if they tarried on the way, while others it has fretted and harassed. To such a life, as you are aware, one should not always cling. For mere living is not a good, but living well. Accordingly, the wise man will live as long as he ought, not as long as he can. He will mark in what place, with whom, and how he is to conduct his existence, and what he is about to do. He always reflects concerning the quality, and not the quantity of his life. There is no disputing that the bio-electronics of ICDs can and does save lives but the
evidence in this chapter demonstrates that bio-electronics carries a duty of care for science and healthcare professionals to be responsible and accountable for consideration of recipients’ quality of life. It appears from the evidence that science is captivated by the notion of “save that body,” yet this is but the beginning of duty of care, as cardiologist Sean concluded: “Unless we find out exactly what is important to the patient, we might be barking up the wrong tree.” Thus, the importance of negotiation, collaboration, informed consent, counseling, and support groups needs to be imperatives in heart implantation.
The evidence in this chapter is from a larger human-science project. As such, it is not intended to be generalisable across other cardiac research populations. This may be considered by some researchers to be a limitation. However, included in the strength and value of a humanistic approach to research, is that if the research is conducted and reported in a sufficiently rigorous manner the findings will be transferable to other groups. Reflections on the chapter suggest how the findings may be transferred to those who live with life-threatening illness, their family members and the health professionals engaged.
The results of empirical research, such as RCTs, identify that there are significant sequelae in relation to biological hazards, psychosocial hazards, and quality-of-life hazards that range across the phenomenon of heart implantation with an ICD. Other studies expand on this knowledge by classifying and categorising the identified hazards in RCTs. The knowledge already accumulated needs to be further expanded to include the humanistic issues of existential experience. Human research that emanates directly from the lived-world

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 65
of key players who experience ICD hazards from different worldviews can provide insight into the experience of recipients and their family members and as such can deepen the awareness of health professionals. In this way, the service of health professionals could be less fragmented and hence, move forward to ameliorate an area of practice in cardiology that is lacking both in understanding and in advocacy.
Evidence presented in this chapter reveals that life-threatening cardiac trauma triggered body-liminality and existential crisis for all participants. This included the whole person: the physical, emotional, psychological, social, spiritual, and cultural beliefs, in relation to the meaning of implanting the heart. This chapter revealed a fragmented service by health professionals, which contributed to professional frustration, professional constraints, professional dilemmas, and professional loss of authenticity.
In this chapter, there is a body of evidence that shows how health professionals perceive engaging with and engaging in heart implantation with a bio-electronic ICD. Health professionals perceive that life-extension lies within hybridisation: the alliance of body and bio-electronics. Sudden cardiac death episodes and life-threatening cardiac arrhythmias are treated as emergencies that require a curative direction towards heart implantation with an ICD. However, as health professionals in this chapter stated, implantation with an ICD is not a cure, and often it is not even a solution for improving a person’s long-term quality of life. This indicates that health professionals are beginning to question the appropriateness of using implantation with an ICD as the first line treatment in all cases. Yet health professionals are confined within the boundaries of the status quo to implant bio-electronics (Sandison et al., 2001).
Cardiac nurses, especially, recognised the value of patient choice as a result of being fully informed in relation to implantation. Cardiac nurses also recognised that the absence of being-fully-informed is part of the nature of heart implantation with an ICD. Despite their efforts, cardiac nurses were overwhelmed with “not enough time” to prepare recipients and family members for a life-changing event within which their quality-of-life (QOL) would never be the same. The complexities of QOL are unique to each individual to the extent that cardiac nurses require the professional authority of referral to a clinical psychologist. An area that is not addressed by health professionals in relation to heart implantation is the philosophical approach of palliation. Some recipients expressed that being-fully-informed would have resulted in choosing to live without heart implantation. This is the essence of choice and refusing a life-extending therapy, such as heart implantation is part of palliative philosophy. Explantation of the ICD because of poor QOL also emerged as part of the essence of implantation and thus locates the non-recipient in the palliative paradigm.
Critical care nurses from Australia and the United States of America have formed The InnoVision Group through a study by Davidson et al., (2003) that proposed the potential for palliative philosophy to be embraced in the long-term care of patients with life-threatening cardio-respiratory diagnoses. As Davidson’s evidence shows, health professionals are inadequately prepared to deal with the constant presence of potential death and dying. In addition, Davidson advocated that palliative philosophy could benefit health professionals because there was a search for structure and meaning in the dying experience; negotiation, planning and treatment was not person-focused; and there was health professional discomfort in dealing with death and dying.

Carole C. Anderson 66
With cardiac-related illness listed as the world’s most prominent cause of death, all participants could have benefited from the availability of a team of health professionals to deal with moving beyond the physical, the science, the bio-electronics, to focus on the person and the family members. Within such a team cardiac nurses want “to be equal partners in cardiology,” because they experience an empathic hope for recipients and family members which disintegrates into the futility of frustration and dilemma. Within such a team, the inclusion of a clinical psychologist is an imperative because the task of one-to-one interaction is time consuming and specialised. A clinical psychologist, conducting individual, family or group consultations is person-focused and removed from the fascination of bio-electronics. A clinical psychologist could provide the time required to assist potential recipients, recipients and family members to arrive at self-determination according to their beliefs and values on life and death issues. In other words, to arrive at what the person wants to do.
Advocating Patient-Based Practice This chapter has presented the liminal impact of being-a-patient through life-threatening
illness. Patients and family members are confronted with health professionals who have an unfamiliar culture, unfamiliar terminology, and overwhelming bio-technology. There is distrust of and hesitancy in handing over the life a person perceives may be out of control. Cardiac nurses could be more helpful with these patients if they were trained in specific counseling techniques. Dealing with triggers of fear and vulnerability, such as SCD, cardiac nurses require the counseling and negotiation skills needed by recipients and family members. None of the cardiac nurses stated possessing any additional or specialised training in counseling, yet throughout their careers they deal with death and dying. Some cardiac nurses described themselves as educators but recipients and family members used the descriptor “technicians.” Furthermore, a cardiologist’s delivery of cardiac arrhythmia diagnosis was described by the patient: “Like being hit in the face with a wet sponge.”
Cardiac nurses and cardiologists risk becoming adversaries of recipients and family members when bio-electronics is perceived to be more highly valued than quality of life. Timothy Quill (2001, p. 49) provided an outline of negotiation that could benefit health professionals in a time of critical decision-making in relation to heart implantation with a permanent ICD. The following principles on different frames of reference could assist recipients and family members to participate in interactive information access and discussion. These principles are inclusive of all key players in heart implantation, rather than exclusive of recipients and family members.
• Listen and learn about each other’s position • Separate the person from the problem • Invent solutions of mutual gain • Call in a third party: For example, a clinical psychologist or nurse counselor • Take a ‘time-out’

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 67
• Give in on nonessential areas • Explore the likely effects of each choice • Know your bottom line Research demonstrates that physicians have inadequate understanding of their patients’
beliefs and values with regard to life-threatening illness and decision-making (Karlawish, Quill and Meier, 1999). Negotiation between the key players in heart implantation with an ICD requires a dialogue to achieve consensus-based decision-making that is acceptable for all concerned. In negotiation, the dialogue of decision-making is designed to achieve an understanding of the diagnosis and the prognosis; it is designed to discuss the benefits and the burdens of different treatment options and different frames of reference. All participants are required to understand the meaning of emotionally charged terms, such as “permanent,” “life-threatening,” and “electric shock.” Negotiation requires reaching a preference for treatment that maximises human dignity and quality-of-life, based on guidance and support according to evidence-based practice.
Alternative treatments for SCD episodes and life-threatening arrhythmias, that are currently under trial, include the at-home defibrillator (Stolberg, 2002), and the defibrillator vest (Gessman, 2006). These alternatives may allow patients and family members a period of ‘time-out,’ which enable families to remain in control of the decision-making. During ‘time-out,’ patients and families can reach long-term decisions through their chosen support source, such as a nurse counselor or clinical psychologist. Unfortunately, the study results in this chapter showed cardiac nurses felt time-constrained and unauthorised to enter into any negotiation. Gay summarised the cardiac nurse situation: “At the end of the day, when you go to educate this patient, you are telling them they are prone to dying. I can’t get round that, no matter if I dress it up or dress it down.” Thus, evidence indicates this area of cardiology is lacking in support for all the key players in heart implantation with an ICD.
Support groups are viewed as one of the most powerful intervention sources for patients and family members struggling with the effects of life-threatening illness (Lugton, 2002). The support group existing at the time of my study was the only group catering for recipients of ICDs and family members in one state within Australia. In another state of Australia, there were two support groups, one of which met just once a year. More humanistic studies are needed so that the key players in heart implantation will be more aware of the support needs that have been explored in this chapter. As the incidence of heart implantation with an ICD increases, it is evident that body-liminality is an ontology that prevents key players from reaching understanding and hope. There will always be a liminal threshold between life and death, but that need not prevent key players in heart implantation from seeking and finding empathic sources of support and hope of understanding. The value of this chapter lies in the hope that the exploration of heart implantation with an ICD will bring key players one step closer to understanding this phenomenon. As David Kessler wrote, cited in Cotter (1999, p. 321): “Hope is a journey, not a destination; its value lies in the exploration. Hope is the way we live life and the journey of hope should last until we end.”

Carole C. Anderson 68
Continuing Research As a beginning, researchers could be more innovative with their research design.
Numerous RCTs have shown that recipients of ICDs will survive longer than non-recipients treated with medication. Having established the efficacy of ICDs, health science researchers have, thus far, avoided changing the research questions. There is the potential to develop and enrich the extension of life with bio-electronics by following through with research questions that explore bio-psycho-social hazards, associated with implantation, the human toll these hazards extract, and ways in which the liminal traumas of implantation can be reduced. Health science researchers have not yet completed their task while there are participants in studies, such as this chapter, who are concerned, worried, questioning, and experiencing dilemmas. A family member captured the situation: “The medical people must address this problem. They are just losing half the battle.”
References
Ackerman, F. (1997). Goldilocks and Mrs. Illych: A critical look at the philosophy of hospice. Cambridge Quality of Healthcare Ethics, 6(3), 314-324.
ACP. Australian Centre for Photography. (2000). The liminal body. Paddington, NSW: Australian Centre for Photography.
Anderson, C. C. (2005). The body electric: A review of literature on implantable cardioverter defibrillators. Collegian, (12)3, 29-35.
Ashton, J. and Ashton, D. (2000). Dealing with the chronic/terminal illness or disability of a child: Anticipatory mourning. In T. A. Rando (Ed.), Clinical dimensions of anticipatory mourning. Champaign: Research Press.
Berdyaev, N. (1972). Man and machine. In C. Mitcham and r. Mackey (Eds.), Philosophy and technology. New York: The Free Press.
Bruner, E. M. (1986). Experience and its expressions. In V. W. Turner and E. M. Bruner (Eds.), The anthropology of experience. Chicago: University of Illinois Press.
Clark, R. A. (2001). How Hollywood films portray illness. The New England Journal of Public Policy, 2, 138-166.
Clarke, W. N. (1972). Technology and man: A Christian view. In C. Mitcham and R. Mackey (Eds.), Philosophy and technology. New York: The Free Press.
Cornish, F. H. (1993). The picture of Dorian Gray. Oxford: Heinemann. Costain-Schou, K. and Hewison, J. (1999). Experiencing cancer: Quality of life in treatment.
Buckingham: Open University Press. Cotter, A. (1999). From this moment on: A guide for those recently diagnosed with cancer.
New York: Random House. Davidson, P., Introna, K., Daly, J., Paull, G., Jarvis, R., Angus, J., Wilds, T., Cockburn, J.,
Dunford, M. and Dracup, K. (2003). Cardiorespiratory nurses’ perceptions of palliative care in non-malignant disease: Data for the development of clinical practice. American Journal of Critical Care, 12(1), 47-53.

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 69
Denzin, N. (1996). The facts and fictions of qualitative research. Qualitative Inquiry, 2(2), 230-241.
Dictionary.reference.com (2007). (Accessed 2nd February 2007). http://dictionary. reference.com/
Dilthey, W. (1976). Dilthey: Selected writings. Cambridge: Cambridge University Press. Evans, H. H. (1993). High tech vs ‘high touch’: The impact of medical technology on patient
care. In J. M. Clair and r. M. Allman (Eds.), Sociomedical perspectives on patient care. Kentucky: The University Press of Kentucky.
Evans, N. and Walsh, H. (2002). The organization of death and dying in today’s society. Nursing Standard, 16(25), 33-38.
Faux, S. A. (1991). Sibling relationships in congenitally impaired children. Journal of Pediatric Nursing, 6(3), 175-184.
FDA. Food and Drug Administration. (2000). Medical device use – Safety: Incorporating human factors engineering into risk management. New York: U.S. Department of Health and Human Services.
Fincher, D. (Executive Producer) and Cameron, J. (Writer/Director). (1992). Alien 111. Hollywood: 20th Century Fox.
Foucault, M. (1976). Power/Knowledge. New York: Harvester Press. Frank, A. W. (1995). The wounded storyteller. Chicago: The University of Chicago Press. Furman, S. (2003). The Twelth World Symposium of Cardiac Pacing and Electrophysiology.
Pacing and Clinical Electrophysiology, 26, 1-3. Gallagher,E. B. and Durant, J. R. (1993). Foreword. In J. M. Clair and R. M. Allman (Eds.),
Sociomedical perspectives on patient care. Kentucky: The University Press of Kentucky. Gardner, G. (1998). The human dimension of nosocomial wound infection: A study in
liminality. Nursing Inquiry, 5, 212-219. Gessman, L. (2006). External defibrillation trial underway at Cooper. Cooper Cardiac News,
2(2), New Jersey: Cooper Heart Institute. (Accessed 2nd February 2007). http://www.cooperhealth.org/heart/cardiac/index.htm
Giddens, A. (1990). The consequences of modernity. Cambridge: Polity Press. Goh, A. Y. and Mok, Q. (2001). Identifying futility in a paediatric critical care setting: A
prospective observational study. Archives of Disease in Childhood, 84(3), 265-268. Gudmundsdottir, M. (2000). When the world of the family is shattered: Narratives of loss and
healing practices after the sudden death of a child. (Abstract). San Francisco: University of California.
Hacking, I. (1999). The social construction of what? Cambridge: Harvard University Press. Haraway, D. (1990). A manifesto for cyborgs: Science, technology and social feminism in the
1980s. In L. J. Nicholson, (Ed.), Feminism/Postmodernism. London: Routledge. Haraway, D. (1993). The biopolitics of postmodern bodies: Determinations of self in immune
system discourse. In S.Lindebaum and M. Lock (Eds.), Knowledge, power and practice. Berkeley: University of California Press.
Haraway, D. (2003). A cyborg manifesto: Science, technology, and socialist-feminism in the late twentieth century. In R. C.Scharff and V. Dusek (Eds.), Philosophy of technology. Oxford: Blackwell Publishing.
Hawking, S. W. (1988). A brief history of time. London: Bantam Books.

Carole C. Anderson 70
Heidegger, M. (1966). Discourse on thinking. New York: Harper and Row. Hoffman, M. L. (2000). Empathy and moral development: Implications for caring and
justice. Cambridge: Cambridge University Press. Hurd,G. A. (Producer) and Cameron J. (Writer/Director). (1984). Hollywood: 20th Century
Fox. Jaspers, K. (1961). The future of mankind. Chicago: University of Chicago Press. Jaspers, K. (1986). Karl Jaspers: Basic philosophical writings. New Jersey: Humanities
Press. Karlawish, J. H., Quill, T. and Meier, D. M. (1999). A consensus-based approach to
providing palliative care to patients who lack decision-making capacity. Annals of Internal Medicine, 130(10), 835-840.
Kaufman, S. R. (1997). Decision making, responsibility, and advocacy in geriatric medicine: Physician dilemmas with elderly in the community. In G. E. Henderson, N. M. P. King, R. P. Strauss, S. E. Estroff and L. R. Churchill (Eds.), The social medicine reader. London: Duke University Press.
Kierkegaard, S. (1968). Concluding unscientific postscript. Princeton: Princeton University Press.
Lamont, R. (1973). The double apprenticeship: Life and the process of dying. In E. Wyschogrod (Ed.), The phenomenon of death. New York: Harper and Row.
Landro, L. (2003). The informed patient: Errors? You’re first line of defence. Wall Street Journal, March 13, 2. New York.
Lantos, J. D. (2001). The lazarus case: Life and death issues in neonatal intensive care. Baltimore: Johns Hopkins University Press.
Lawler, J. (2002). Knowing the body and embodiment – methodologies, discourses and nursing. In A. M. Rafferty and M. Traynor (Eds.), Exemplary research for nursing and midwifery. London: Routledge.
Lee, T. F. (1991). The human genome project: Cracking the genetic code of life. New York: Plenum Press.
Levin, I. (1967). Rosemary’s baby. London: Michael Joseph. Lewis,M. (1992). Shame: The exposed self. New York: The Free Press. Little, M., Jordens, C. F. C., Paul, K., Montgomery, K. and Philipson, B. (1998). Liminality:
A major category of the experience of cancer illness. Social Science and Medicine, 47(10), 1485-1494.
Lock, M. (1995). Transcending mortality. Organ transplants and the practice of contradictions. Medical Anthropology Quarterly, 9(3), 390-393.
Lock, M. (2000). On dying twice: Culture, technology and the determination of death. In M. Lock, A. Young and A. Cambrosio (Eds.), Living and working with the new medical technologies. Cambridge: Cambridge University Press.
Lugton, J. (2002). Communicating with dying people and their relatives. Oxford: Radcliffe Medical Press.
Maisel, W. H. (2005). Safety issues involving medical devices: Implications of recent implantable cardioverter defibrillator malfunctions. Journal of the American Medical Association, (294)8, 955-958.

The Liminal Body: Lament of the Implantable Cardioverter Defibrillator 71
Merleau-Ponty, M. (1962). Phenomenology of perception. London: Routledge and Kegan Paul Ltd.
Merleau-Ponty, M. (1964). Eye and mind. Evanston: Northwestern University Press. Mond, H. G., Irwin, M., Morillo, C. and Ector, C. (2004). The world survey of cardiac pacing
and cardioverter defibrillators: Calendar year 2001. Pacing and Clinical Electrophysiology, (27), 955-964.
Montgomery, C. L. (1997). Coping with the emotional demands of caring. Advanced Practice Nursing Quarterly, 3(1), 76-84.
Moustakas, C. (1996). Loneliness. New Jersey: Jason Aronson Inc. Pojman, L. P. (1992). Life and death. Boston: Jones and Bartlett Publishers. Proclemer, A., Ghidina, M., Ciruttini, G., Gregori, D. and Fioretti, P. M. (2006). Impact of
the main implantable cardioverter defibrillator trials for primary and secondary prevention in Italy: A survey of the national activity during the years 2001-2004. Pacing and Clinical Electrophysiology, (29), S20-S28.
Quill, T. E. and Brody, H. (1996). Physician recommendations and patient autonomy: Finding a balance between physician power and patient choice. Annals of Internal Medicine, 125, 763-769.
Quill, T. E. (2001). Caring for patients at the end of life. Oxford: Oxford University Press. Raabe, P. B. (2001). Philosophical counseling. Westport: Praeger. Rier, D. A. (2000). The missing voice of the critically ill: A medical sociologist’s first-person
account. Sociology of Health and Illness, 22(1), 68-93. Riesman, D. (1954). Individualism reconsidered and other essays. Illinois: The Free Press. Ritter, R. M. (2005). New Oxford dictionary for writers and editors. (2nd ed.), Oxford: Oxford
University Press. Rosof, B. D. (1994). The worst loss. New York: Henry Holt. Sandison, T., Meischke, H. W., Schaeffer, S. M. and Eisenberg, M. S. (2001). Barriers and
facilitators to the prescription of automated external defibrillators for home use in patients with heart disease: A survey of cardiologists. Heart and Lung, 30(3), 210-215.
Schmidt, A. and Verhoeven, P. (Director). (1987). Robocop. Hollywood: Metro Goldwyn Mayer Studios.
Serling, R. (1959). The twilight zone. Los Angeles: Columbia Broadcasting System. Sandelowski, M. (2002). Reembodying qualitative inquiry. Qualitative Health Research,
12(1), 104-115. Schuster, S. C. (1999). Philosophy practice. Westport: Praeger. Spurling, L. (1977). Phenomenology and the social world. London: Routledge and Kegan
Paul. Sque, M. (2001). Being a carer in acute crisis: The situation for relatives of organ donors. In
S. Payne and C. Ellis-Hill (Eds.), Chronic and terminal illness. Oxford: Oxford University Press.
Stark, P. (2001). Last breath. London: Macmillan. Stolberg, S. G. (2002). Food and drug agency approves cardiac defibrillator for the home, to
save critical minutes. New York Times, November 13, New York: New York Times Company.

Carole C. Anderson 72
Strugatch, W. (2002). Struggling to get doctors’ attention. New York Times, December 15, 6-8. New York: New York Times company.
Tassano, F. (1995). The power of life or death. London: Duckworth. Teather, E. K. (1999). Embodied geographies. London: Routledge. Thomas, D. (1969). And death shall have no dominion. In J. Colmer and D. Colmer (Eds.),
Mainly modern. Adelaide: Rigby Limited. Turner, V. (1969). The ritual process, structure and anti-structure. New York: Ithaca. Turner, V. (1986). Dewey, Kilthey, and drama: An essay in the anthropology of experience.
In V. W. Turner and E. M. Bruner (Eds.). The anthropology of experience. Urbana: University of Illinois Press.
van Gennep, A. (1960). The rites of passage. London: Routledge and Kegan Paul. van Manen, M. (1990). Researching lived experience. New York: State University of New
York Press. Werbner, P. and Modood, T. (1997). Debating cultural hybridity. London: Zed Books. Woolf, V. (1948). The moment. New York: Harcourt, Brace and Company. Wurmser, L. (1995). The mask of shame. New York: Jason Aronson. Ziskin, L. (Producer) and Haines, R. (Director). (1991). The doctor. Hollywood: Touchstone
Pictures.

In: Cardiac Arrythmia Research Advances ISBN: 978-1-60021-795-1 Editor: Lynn A. Vespry, pp. 73-92 © 2007 Nova Science Publishers, Inc.
Chapter III
Autonomic Nervous System and Cardiac Arrhythmias
Maurizio Acampa*1, Maura Lamarina1, Luca Puccetti1, Francesca Guideri2 and Alberto Auteri1
Department of Clinical Medicine and Immunological Sciences University of Siena, Siena, Italy;
1 Section of Internal Medicine, 2 Section of Clinical Immunology.
Abstract
Autonomic nervous system activity exerts a potent influence on arrhythmogenesis. Regulation of cardiac neural activity is highly integrated and is achieved by circuitry at multiple levels. In recent years non-invasive techniques based on the electrocardiogram (ECG) have been used as markers of autonomic modulation of the heart, these include heart rate variability (HRV), baroreflex sensitivity (BRS), QT interval, and heart rate turbulence (HRT), a new method based on fluctuations of sinus rhythm cycle length after a single premature ventricular contraction. Among these techniques analysis of HRV has emerged as a simple, non-invasive method to evaluate the sympatho-vagal balance at the sinoatrial level.
The actual mechanisms by which the autonomic nervous system causes or prevents fibrillation, particularly in the ventricles, are complex. The neurotransmitters epinephrine and norepinephrine activate cardiac adrenergic receptors, with stimulation of G protein adenylyl-cyclase-cAMP protein kinase A pathway to alter the activity of a number of ion channels and transporters.
Cardiac sympathetic nerves are highly plastic and the coexistence of denervated and hyperinnervated area in the diseased myocardium could result in increased
* Correspondence to be sent to: Maurizio Acampa, MD; Dipartimento di Medicina Clinica e Scienze
Immunologiche, Sezione di Medicina Interna, Policlinico ‘Le Scotte’, viale Bracci, 53100 Siena, Italy. Telephone number: +39(0)577585741; Fax number:+39(0)57744114; E-mail address: [email protected]

Maurizio Acampa, Maura Lamarina, Luca Puccetti et al. 74
electrophysiological heterogeneity during sympathetic activation that can provoke ventricular arrhythmias via several mechanisms, including reentry, enhanced and abnormal automaticity, and triggered activity. Of these mechanisms, abnormal automaticity and triggered activity have most often been cited as causal factors of exercise-induced arrhythmias in subjects without organic heart disease also.
In particular, sympathetic nervous system activity may participate in the genesis of ventricular arrhythmias with short term effects (with enhancement of early and delayed afterdepolarizations and increased dispersion of repolarization) and long term effects (resulting in apoptosis, hypertrophy, fibrosis and sympathetic nerve sprouting).
In contrast to sympathetic stimulation, parasympathetic activity appears to protect the heart against arrhythmias. Vagal activity influences both ionotropic and chronotropic properties of the ventricular myocardium, increasing the threshold of the vulnerable period with the antifibrillatory effect.
Abnormalities of the autonomic nervous system have been demonstrated in diverse conditions such as diabetic neuropathy, coronary heart disease, heart failure, stroke: a dysregulation in the autonomic nervous control of the cardiovascular system associated to increased sympathetic and reduced parasympathetic tone plays an important role in coronary artery disease and in the genesis of life-threatening ventricular arrhythmias.
Introduction The evidence for a tight link between the nervous system, malignant arrhythmias and
sudden death has been acknowledged for over a century. As early as 1859, Einbrodt demonstrated that vagal stimulation can protect against electrically induced ventricular fibrillation [1]. The relationship between autonomic nervous system activity and cardiac arrhythmias have been investigated furthermore by Levy [2] in 1913: chloroform induced ventricular tachyarrhythmias in animals were abolished by cardiac sympathetic denervation, suggesting that ventricular arrhythmias can be evoked by stimulating certain areas in the hypothalamus.
The concept that neural activity exerts a potent influence on arrhythmogenesis was highlighted in the 1970’s [3, 4] and has continued to receive affirmation in contemporary literature [5, 6], suggesting links between emotional states, neural control and cardiac function; emotional stress is recognized as an important contributing factor to arrhythmias and sudden cardiac death [7, 8]. It has been known for many years that, as a general rule, parasympathetic stimulation in the atrium is profibrillatory but antifibrillatory in the ventricles, whereas sympathetic stimulation appears to be profibrillatory for both chambers. However, the actual mechanisms by which the autonomic nervous system causes or prevents ventricular fibrillation remain for the most part elusive.
Neurocardiology investigates these interactions examining neuroanatomy and physiology of neurocardiologic axis and discussing how neural activation may control ionic channels, pumps, and exchangers at the level of the myocardial cell, potentially inducing cardiac arrhythmias.

Autonomic Nervous System and Cardiac Arrhythmias 75
Cardiac Autonomic Nervous System: Anatomy and Physiology
Anatomy
The autonomic nervous system (ANS) is a visceral and largely involuntary
motor/effector system that is traditionally divided into sympathetic (thoracolumbar) and parasympathetic (craniosacral) divisions, each with a central and a peripheral component [9], that are closely integrated and regulated by a central autonomic neuronal network (CAN). The CAN maintains integral relationships with visceral sensory neurons via afferent input from the vagus nerve and relays transmission through the nucleus tractus solitarius to the hypothalamus, amygdala, and forebrain [10]. The ANS provides the main nerve supply to the heart, by means of its two anatomic branches: geographic proximity of nerve endings affects neural modulation; therefore, pathways of innervation are important [11].
The sympathetic nerves (superior, middle, inferior and thoracic cardiac nerves) arise from the superior cervical, the middle cervical, the vertebral and the cervicothoracic (stellate) ganglia and lower cervical sympathetic trunk. Parasympathetic fibers (superior, inferior and thoracic cardiac branch) leave the thoracic vagus nerves and recurrent laryngeal nerves. Parasympathetic and sympathetic nerves interconnect to form ventral and dorsal cardiopulmonary plexus, from which relatively large and discrete cardiac nerves emerge to supply the ventricles: the right and left coronary cardiac nerves and the left lateral cardiac nerves. A number of smaller nerves also supply the heart, and there are many anatomic variations among individuals with regard to the precise wiring diagram of the heart. In general, the right-sided sympathetic and vagal fibers are predominant at the sinus node, and fibers from the left sympathetic trunk and vagal nerves are predominant at the atrioventricular node. Parasympathetic pathways to the atria have been well characterized in dogs and, to some degree, in patients, with a concentration of ganglia in various fat pads directing innervation to specific sites. In the ventricles, major sympathetic trunks appear localized in the epicardium alongside coronary arteries, with transmural penetration to innervate the rest of the myocardium. In addition, the right-sided sympathetic nerves usually supply the anterior surface of the ventricle, while the left-sided sympathetic nerves supply the posterior surface. The major parasympathetic ventricular pathways are epicardial until crossing the AV groove, where vagal trunks appear to penetrate the myocardium to become located predominantly in the ventricular subendocardium.
Physiology The central nervous system, through its modulation of autonomic activity, is important in
maintaining homeostasis in the cardiovascular system and in integrating cardiovascular responses with behaviors.
As with the Chinese philosophy of yin and yang so the vagal and sympathetic drives to the heart can be characterized as polar opposites [12]: whereas one "limb" of the autonomic efferent nervous system, represented by sympathetic efferent neurons, enhances cardiac

Maurizio Acampa, Maura Lamarina, Luca Puccetti et al. 76
indexes [13], the other, represented by parasympathetic efferent neurons, depresses them [14]. The sympathovagal balance hypothesis suggests that activation of sympathetic versus parasympathetic efferent neurons normally is accompanied by inhibition of the other efferent
limb [15]. In fact, at the sinus node, parasympathetic stimulation is prepotent, whereas the reverse
occurs in the ventricles, where sympathetic effects dominate. Parasympathetic stimulation reduces norepinephrine release from sympathetic nerve terminals while also opposing postganglionic sympathetic actions. Sympathetic stimulation counters vagal effects primarily by direct stimulation of α and β receptors.
However, a more subtle interpretation of the yin–yang principle shows that it is the interrelation of the opposites that is crucial. So with the autonomic control of the heart, the interaction between sympathetic and parasympathetic, which is classically characterized as opposite and reciprocal, can, under physiological and pathophysiological circumstances, be both synchronous and synergistic.
For both the sympathetic and parasympathetic systems, the preganglionic innervation is largely cholinergic, with terminals releasing acetylcholine at the ganglion synapses. For the sympathetic system, norepinephrine is the major neurotransmitter, but other postganglionic neurotransmitters are also important, among which are substance P, dopamine, and vasoactive intestinal polypeptide [16, 17]. Regulation of cardiac neural activity is highly integrated and is achieved by circuitry at multiple levels; higher brain centers operate through elaborate pathways within the hypothalamus and medullary cardiovascular regulatory sites. The intrinsic cardiac nerves and fat pads appear to provide local neural coordination independent of higher brain centers.
Synergistic interactions occur among neurons located in the cerebral cortex [18] and in the intrinsic cardiac nervous system [19]: the various reflexes involved depend on specific linkages in the medulla, spinal cord, and intrathoracic ganglia initiated by transduction of the cardiovascular system [20].
At the level of the myocardial cell, considerable progress has been made to define the intimate role of the autonomic receptors as they influence G proteins to control ionic channels, pumps, and exchangers.
At present, nine adrenoceptor (AR) subtypes have been identified: α1A-, α1B-, α1D-, α2A-, α2B-, α2C-, β1-, β2-, and β3AR [21]. In the heart, β1- and β2-AR are the most powerful physiologic mechanism to acutely increase cardiac performance.
In the human heart, β1- and β2-AR coexist, whereby β1-AR predominate; in general, the ratio β1-:β2-AR is about 70%:30% in the atria and 80%:20% in the ventricles. On the other hand, total β-AR number appears to be equally distributed over atria and ventricles [21]. Both β-AR subtypes couple to the Gs-protein, thereby elevating the intracellular level of cyclic AMP and cause positive inotropic and chronotropic effects, in vitro as well as in vivo. In atria, stimulation of both β1- and β2-AR can evoke maximal increases in force of contraction and heart rate, whereas in ventricles, only stimulation of β1-AR causes a maximal increase in force of contraction, while stimulation of β2-AR causes only submaximal increase [21].
In addition to β1-, β2-, and β3-AR, it had been postulated, in humans, the presence of an additional “putative β4AR”: this “receptor” was characterized by insensitivity against

Autonomic Nervous System and Cardiac Arrhythmias 77
classical β-AR-antagonists such as propranolol, and it was potently activated by CGP 12177 (a potent antagonist at classical β1- and β2-AR).
The existence of α1-AR in the human heart has been demonstrated by molecular biology and biochemical methods, as well as, in functional studies; however, the α1-AR subtype present in the human heart is not well characterized [21].
The density of human cardiac α1-AR is only 10% –15% of that of β-AR; they couple presumably via Gq/11-protein to inositol phosphate formation [22] and mediate positive inotropic effects [23]. The existence of α2-AR in the human heart has been demonstrated by molecular biology methods; the α2-AR plays functionally a role in presynaptic regulation of noradrenaline release in the human heart.
In cardiac myocytes it is essential to maintain cellular excitability; the channels involved in action potential generation at the sarcolemma are regulated by various cellular signalling pathways, including the adrenergic receptors stimulation [24].
Neurohumoral regulation of the cardiac voltage-gated sodium current, INa, via β-adrenergic stimulation is of a particular interest in light of the effects that it may have under conditions of cardiac stress and disease. β-adrenergic receptors regulate the current produced via adult cardiac sodium channels by at least two known mechanisms [24]: direct (membrane-delimited) and indirect.
The indirect mechanism is dependent on the phosphorylation of sarcolemmal channels by protein kinase A (PKA) at serine residues in the intracellular linker between domains I and II. The phosphorylation of sodium channels results in the alteration of the voltage-dependent availability, current decay kinetics and whole-cell INa amplitude. The direct mechanism depends upon the action of the Gsα protein itself, resulting in a change in the number of functional channels at the level of the sarcolemma.
The stimulation of β-adrenergic receptors also regulates voltage-gated calcium and potassium channels [24]. β-adrenergic receptor stimulation appears to alter voltage-gated calcium current via a dual mechanism, similar to that of sodium channels. The fast direct mechanism of β-adrenergic stimulation produce an increase in IcaL depending on direct action of Gsα; the indirect mechanism is dependent on the phosphorylation of calcium channels by PKA in the presence of anchoring proteins at the plasma membrane, which results in an increase in open channel probability and, therefore, overall cellular calcium current. Similarly, IKur has been shown to increase in response to β-adrenergic stimulation: phosphorylation of potassium channels alters its interactions with and regulation by associated beta subunits.
Both the currents (potassium and calcium currents) have important roles in the shape and duration of the cardiac action potential. The L-type calcium channel depolarizes relatively slowly in the first part of the action potential and is responsible for the influx of calcium that is the trigger for calcium sparks, increasing action potential duration. Similarly IKur is important in determining the rate at which cardiomyocytes return to their resting membrane potential, thereby making it important in the refractory period duration and cellular excitability.

Maurizio Acampa, Maura Lamarina, Luca Puccetti et al. 78
Physiopathology There is a cardiac neuronal hierarchy that can be represented as a redundant control
system made up of spatially distributed cell stations comprising afferent, efferent, and interconnecting neurons; these represent anatomically distinct loci where afferent and efferent neuronal elements functionally interact [20]. If any component within this hierarchy becomes deranged, imbalance in cardiac motor control may arise [25]. At various levels, extracardiac sympathetic and parasympathetic efferent neurons can be involved in the genesis of cardiac arrhythmias [17, 26], when maximally activated, initiating atrial [27] or ventricular [28] arrhythmias. In accord with that, ventricular fibrillation can occur when sufficient populations
of intrinsic cardiac neurons are activated by locally applied neurochemicals such as adrenoceptor agonists, angiotensin II, or endothelin I [29]. The activation of select populations of cholinergic efferent neurons, located throughout the intrinsic cardiac nervous
system, that innervate either the sino-atrial or atrio-ventricular node, can suppress sinusal stimulus or atrio-ventricular nodal transmission, respectively. The excessive activation of select groups of intrinsic cardiac neurons can induce atrial or ventricular arrhythmias; depending on the group of neurons involved, these arrhythmias can degenerate into fibrillation [20]. Thus removal of select neuronal elements responsible for such events may be contemplated for rhythm control. In the presence of regional myocardial ischemia, components within the intrinsic cardiac nervous system undergo pathological change, with a consequent remodeling of the cardiac neuronal hierarchy that alters its spatially and temporally organized reflexes destabilizing efferent neuronal control of regional cardiac electrical and mechanical events.
Sympathetic nervous system activity participate in the genesis of ventricular tachyarrhythmias [30]. The precise mechanism by which sympathetic activity promotes cardiac arrhythmias is speculative; the ultimate manifestation of the arrhythmias probably is the end result of a variety of interacting factors. Three major types of electrophysiological effects have been identified: short-term, intermediate-term and long-term effects [30]. Ventricular arrhythmias can occur shortly (less than 60 minutes) after events associated with an increase of sympathetic activity (short-term effect): there are many mechanisms by which sympathetic can alter myocardial electrophysiological properties with possible ventricular arrhythmias. Important effects are those mediated by myocardial ischemia (resulting from an increased myocardial oxygen demand due to an increased heart rate and/or contractility with consequent reduced oxygen supply due to vasoconstriction), thrombosis (due to activation of platelets or hemostatic factors) or plaque rupture (due to shear stress); moreover, electrophysiological effects may be mediated by myocardial fibers stretching, after stimulation of beta receptors, as a consequence of altered blood pressure [31].
Chronic elevations in sympathetic activity may exerts long term effects increasing susceptibility to ventricular arrhythmias over relatively long periods of time. In fact, the association among increased sympathetic activity, myocardial dysfunction, ventricular arrhythmias and sudden death has been recognized for several years [32]. A recent research in transgenic mouse models demonstrates that overexpression of elements of adrenergic pathways result in cardiomyopathic phenotypes [33]. In particular, mice overexpressing β1-adrenergic receptors demonstrate large areas of interstitial replacement, fibrosis, marked

Autonomic Nervous System and Cardiac Arrhythmias 79
myocite hypertrophy, myofibrillar disarray and cell death (apoptosis) [34]; overexpression of β2-adrenergic receptors results in similar cardiomyopathy only after longer periods of observation; overexpression of α1b- adrenergic receptors results in the development of dilated cardiomyopathy with enlargement of all four cardiac chambers and cardiomyocytes disarray in the failing hearts. These effects suggest that myocardial hypertrophy in patients with heart failure is largely due to β1-adrenergic receptors [35], that mediate also myocyte apoptosis by means of activation of calcineurin via increased intracellular calcium through L-type channels [36].
These effects produce several structural changes in myocardial tissue (cell death with confluent scar tissue, interstitial fibrosis, disruption of gap junctions) that determine a nonuniform anisotropic conduction with barriers to propagation and loss of electrotonic modulation of repolarization that may contribute to both macro- and micro-reentry.
Incresead sympathetic activity may produce also some effects that have time courses between short- and long-term effects, that is intermediate-term effects. These effects result in a sympathetic-mediated alteration in gene expression of ionic channels [37]. For example, Zhang et al. [38] reported that decreased transcription of the Kv4.3 gene (that encode for a large portion of channel Ito) occurs over a period of hours with a maximum effect by 24 hours in response to α-adrenergic stimulation; the reduction in Ito is responsible for the increased action potential duration (APD) in heart failure and hypertrophy and is associated with repolarization heterogeneities, contributing to the initiation of sustained ventricular tachyarrhythmias [39].
Finally, by means of these various mechanisms, in the normal ventricle, sympathetic stimulation shortens action potential duration and the QT interval in the scalar ECG and can reduce the dispersion of repolarization. However, in pathologic states associated with reduced repolarization reserve (e.g., heart failure and channelopathies such as the long QT syndrome [LQTS]), sympathetic stimulation is a potent stimulus for the generation of arrhythmias, perhaps by enhancing the dispersion of repolarization or by generation of afterdepolarizations: in these states the increased action potential duration that underlies QT prolongation predisposes to early afterdepolarizations (EADs) and EADs, augmented by adrenergic activity, seemed to be a plausible mechanism for “torsades de pointes”.
Parasympathetic stimulation modestly prolongs ventricular refractoriness and the QT interval in the normal heart, reflected by a longer QT interval during vagal stimulation in animal studies and during sleep in humans.
Assessement of Cardiac Autonomic Activity Autonomic assessment has played an important role in elucidating the role of the
autonomic nervous system in diverse clinical and research settings [40]. Because the anatomic location of the cardiovascular autonomic nervous system renders it
inaccessible to simple direct physiological testing, a group of clinical tests measuring cardiovascular autonomic function and dysfunction has been developed to circumvent this problem by measuring the end-organ responses to various physiological and pharmacological perturbations.

Maurizio Acampa, Maura Lamarina, Luca Puccetti et al. 80
In recent years non-invasive techniques based on the electrocardiogram (ECG) have been used as a marker of autonomic modulation of the heart [41], these include heart rate variability (HRV), baroreflex sensitivity (BRS), QT interval, and heart rate turbulence (HRT), a new method based on fluctuations of sinus rhythm cycle length after a single premature ventricular contraction. Among these techniques analysis of HRV has emerged as a simple, noninvasive method to evaluate the sympatho-vagal balance at the sinoatrial level.
Autonomic nervous system tone has been studied primarily in human subjects by employing the tool of HRV, which relies on the principle that the pattern of beat-to-beat control of the sinoatrial node provides a reflection of autonomic activity. Heart rate responds dynamically to physiologic perturbations mediated by the autonomic nervous system via efferent vagal and sympathetic nerve impulses. Even at rest heart rate fluctuates cyclically. High frequency (HF) cyclic fluctuations are modulated by ventilation, mediated entirely by changes in vagal outflow. Slower fluctuations occur due to baroreflexes or due to thermoregulation. The greatest variation of heart rate occurs with circadian changes, particularly the difference between night and day heart rate, mediated by complex and poorly understood neurohormonal rhythms. Exercise and emotion also have profound effects on heart rate. Fluctuations in heart rate reflect autonomic modulation and have prognostic significance in pathological states. On the basis of the different frequency response characteristics of sympathetic and parasympathetic modulation of heart rate, frequency analysis of heart rate variability is often used as a tool to determine "autonomic balance" or sympathetic and parasympathetic nervous system activity.
There are two common settings in which HRV is measured. First, HRV is assessed under controlled laboratory conditions with short-term measurements before and after tilt, drugs, controlled ventilation, or other maneuvers selected to challenge the autonomic system. Secondly, HRV can be determined from 24-hour electrocardiographic (ECG) recordings made while subjects perform their usual daily activities. Twenty-four-hour ECG recordings are particularly useful for risk stratification in a variety of pathological entities, but can also be useful for quantifying autonomic dysfunction. Methods for quantifying HRV are categorized as: time domain, spectral or frequency domain, geometric, and nonlinear. A short discussion of each will follow.
Methods of Measurements of Cardiac Autonomic Activity The variations in heart rate may be evaluated by a number of methods [42]. Perhaps the
simplest to perform are the time domain measures. In time domain analysis, the intervals between adjacent normal R waves (NN intervals) are measured over the period of recording. A variety of statistical variables can be calculated directly from the intervals and others can be derived from the differences between intervals.
Either fast Fourier transformation or autoregression techniques can be used to quantify cyclic fluctuations of R-R intervals. Traditionally, spectral analysis has been done in short-term laboratory studies; often standard 5-minute ECG segments are analyzed. According to the Task Force of The European Society of Cardiology and The North American Society of Pacing and Electrophysiology these frequencies are classified into 1) ultra-low frequencies

Autonomic Nervous System and Cardiac Arrhythmias 81
(ULF; 5-h cycle length) that include the circadian rhythm; 2) very low frequencies (VLF; 25-s cycle length) that are supposed to be affected by temperature regulation and humoral systems; 3) low frequencies (LF; 6-s cycle length in humans) that are sensitive to changes in cardiac sympathetic (and presumably parasympathetic) nerve activity; and 4) high frequencies (HF; 2.5- to 6.0-s cycle length in humans) that are synchronized to the respiratory rhythm and are primarily modulated by cardiac parasympathetic innervation.
The exact physiologic mechanism responsible for VLF is a matter of dispute [43], but, like most other forms of HRV, VLF power is abolished by atropine, suggesting that it uses a parasympathetic efferent limb. Very low frequency power is also reduced by about 20% by ACE inhibition, suggesting that, at least in part, it reflects the activity of the renin-aldosterone system. Others have suggested that VLF power reflects thermoregulation or vasomotor activity. Bernardi [44] showed that physical activity can exert a large effect on VLF power. In addition, sleep-disordered breathing can cause exaggerated values for VLF power, seen as clear peaks on plots of the HRV power spectrum during the night. The HF component corresponds to the frequency of respiration and is driven by the vagus as indicated by the strong respiratory pattern of cardiac vagal motoneurons in the nucleus ambiguus. The LF component has been ascribed to sympathetic modulation of cardiac pacemaker activity, because a variety of studies demonstrated that acute interventions that increase sympathetic
nervous system activity, such as orthostatic perturbations, mental stress, or handgrip exercise increases LF spectral power of heart rate. In addition to acute perturbations of cardiac sympathetic nerve activity, feedback oscillations generated by the baroreceptor reflex also appear to contribute to LF spectral power of heart rate as it was demonstrated that sinoaortic denervation markedly reduces the LF component [43].
R-R interval power spectra also have been computed using data from 24-hour ECG recordings and categorized into total power and four mutually exclusive power bands, ultra low, very low, low, and HF power. Total and ultra-low frequency power are best calculated from a R-R interval tachogram of the entire 24-hour recording. Instead of computing the 24-hour power spectrum, spectral analysis often is performed on 5-minute segments from 24-hour recordings. The lowest frequency band in the 24-hour R-R interval power spectrum is ULF power, which quantifies fluctuations in R-R intervals with periods between every 5 minutes and once per 24 hours (ULF <0.003 Hz). Although the physiologic basis for ULF and VLF power are far less clear than HF and LF power, they have proven to be more powerful risk predictors in cardiovascular diseases.
Nonlinear phenomena are certainly involved in the genesis of HRV. They are determined by complex interactions of hemodynamic, electrophysiological, and humoral variables as well as by the autonomic and central nervous regulations. It has been speculated that analysis of
HRV based on the methods of nonlinear dynamics might elicit valuable information for physiological interpretation of HRV and for the assessment of the risk of sudden death.
Nonlinear methods are based on the chaos theory and fractals. Chaos has been defined as the study of multivariable, nonlinear and nonperiodic systems. Chaos describes natural systems in a different way because it can account for nature’s randomness and nonperiodicity [45]. Perhaps the theory of chaos may help in better understanding HR dynamics, taking into account that the healthy heartbeat is slightly irregular and to some extent chaotic. In the near future nonlinear fractal methods may give new insights into HR dynamics in the context of

Maurizio Acampa, Maura Lamarina, Luca Puccetti et al. 82
physiological changes and in high risk situations, particularly in patients after MI or in the context of sudden death [45]. Recent data suggest that fractal analysis in comparison to standard HRV measurements seems to detect abnormal patterns of RR fluctuations more efficiently. The parameters that have been used to measure nonlinear properties of HRV include 1/f scaling of Fourier spectra, H scaling exponent, and Coarse Graining Spectral Analysis (CGSA) [46]. For data representation, Poincaré sections, low-dimension attractor plots, singular value decomposition, and attractor trajectories have been used. For other quantitative descriptions, the D2 correlation dimension, Lyapunov exponents, and Kolmogorov entropy have been used.
Modern techniques for the estimation of spontaneous BRS (baroreceptor reflex sensitivity) are based on a variety of signal processing schemes and derive information on the baroreflex function from different perspectives [47]. Thus factors such as respiration and other non-stationary agents may have different influences on the estimates provided by each of these approaches. Notwithstanding such individual specificity, however, it has been observed that in several physiological and pathophysiological conditions these techniques often provide comparable information on BRS changes over time, particularly when the estimates are averaged over time windows of a few minutes. The tilting test is used to evaluate blood pressure variability and autonomic nervous responses, especially BRS during changes of body position. In this instance, BRS is expressed as the ratio between heart rate (HR) variation and systolic blood pressure variation (delta RR/delta SBP). The results were the same as those produced by all other tests including sequential method, squatting test, the neck chamber method, and tilting test.
Cardiac Dysautonomia and Risk of Ventricular
Arrhythmias in Specific Diseases Abnormalities of the autonomic nervous system have been demonstrated in various
conditions such as diabetic neuropathy, coronary heart disease, heart failure, stroke: a dysregulation in the autonomic nervous control of the cardiovascular system, associated to increased sympathetic and reduced parasympathetic tone, plays an important role in coronary artery disease and in the genesis of life-threatening ventricular arrhythmias.
Coronary Artery Disease Sudden cardiac death is a major cause of morbidity and mortality in patients with
coronary artery diseases and myocardial infarction. Beta-blocker therapy significantly reduces the incidence of sudden death after myocardial infarction [48] suggesting a close association between ventricular arrhythmias and sympathetic activity in these patients.
Regional interruption of vagal and sympathetic innervation occurs after myocardial infarction and this interruption depend on the type and the extent of myocardial necrosis.
The infarction destroys nerves in the infarct zone and renders distal myocardial segments denervated or at least neurally dysfunctional. Denervation supersensitivity with exaggerated

Autonomic Nervous System and Cardiac Arrhythmias 83
shortening of ventricular effective refractory periods and enhanced inducibility of ventricular fibrillation in the presence of cathecolamines follow such changes. Nerve sprouting following injury has been shown in several animal models as well as in the explanted hearts: the functional significance of reinnervation after infarction is unclear. Vracko suggested [49] that human myocardial nerve fibers regenerate after necrotizing injuries and at least some of the resulting scar-associated fibers have structural features differing from those in uninjured myocardium: these structural differences might be associated with functional alterations that could affect the triggering of ventricular arrhythmias. Recently, Chen et al. [50] found that cardiac sympathetic nerves are highly plastic: the coexistence of denervated and hyperinnervated area, resulting after nerve injury, may cause an increased electrophysiological heterogeneity during sympathetic activation, leading to ventricular arrhythmia and sudden cardiac death.
The chronic non-uniform increase of neurotransmitters, through alterations in the expression of ionic channels (calcium and potassium channels), create spatial dispersion of action potential duration.
In particular, sympathetic hyperinnervation causes an increase of expression of L-type calcium channels resulting in a prolongation of QTc interval on ECG. On the other side, the surviving rim of myocardial fibers on the epicardial surface of a transmural infarct (epicardial border zone) shows a reduced peak L-type inward calcium current with delayed recovery of the fast inward sodium current, resulting in an altered excitability and post-repolarization refractoriness, promoting conduction block and reentry during premature stimulation [51]. Electrical remodelling after infarction result in hypertrophy, action potential duration prolongation and marked heterogeneity of the time course of repolarization: these changes could be explained by the reduction of transient outward potassium currents. Action potential prolongation and augmented calcium influx increase the susceptibility to early afterdepolarization and delayed afterdepolarization-triggered activity in hyperinnervated regions. If the triggered beat propagates throughout the rest of the heart, the pre-existing spatial dispersion of action potential duration and, thus, myocardial refractoriness, facilitate the initial of tachyarrhythmias [52].
Analysis of heart rate variability by conventional time and frequency domain methods, as well as by newer methods derived from nonlinear system theory, has offered a novel approach for studying the abnormalities in cardiovascular neural regulation in ischemic heart disease. In the late 80’s and in the course of the 90’s [53, 54], most studies have reported that reduced HRV was a powerful predictor of cardiac mortality, arrhythmic events and sudden death in high risk post-MI patients, and it was furthermore independent of other risk stratifers, such as left ventricle ejection fraction, ventricular ectopic activity or late potentials.
Heart rate variability has been shown to be altered among patients with an ischemic heart. There are also obvious differences in various measures of heart rate variability between patients with uncomplicated coronary artery disease and those with coronary artery disease with complicated myocardial infarction. Impaired high-frequency oscillations of heart rate is the most prominent feature in patients with uncomplicated coronary artery disease, suggesting mainly an impairment in vagal autonomic regulation. Patients with prior myocardial infarction have a reduced overall heart rate variability, with a reduced very-low frequency and low frequency spectral component that provide prognostic information. Recent

Maurizio Acampa, Maura Lamarina, Luca Puccetti et al. 84
studies have shown that the new nonlinear measures, particularly fractal analysis methods of heart rate dynamics, can detect subtle changes in heart rate behavior that are not easily detected by traditional analysis methods from ambulatory recordings. Patients with prior myocardial infarction have steeper power-law slope analyzed from the ultra and very low-frequency spectral bands, and they also have more random short-term heart rate dynamics analyzed by the detrended fluctuation method. A large body of data indicate that reduced overall heart rate variability is associated with an increased risk of mortality and nonfatal cardiac events in patient with ischemic heart disease. Of particular note, recent studies indicate that fractal analysis methods perform even better than the traditional analysis methods of heart rate variability as predictors of death and the onset of life-threatening arrhythmic events in post-infarction populations [55].
Heart Failure Heart failure (HF) is a serious, debilitating condition with poor survival rates (50% 5-
year mortality rate) and an increasing level of prevalence. Although many deaths are due to pump failure nearly half of all deaths occur suddenly, primarily from ventricular tachycardia degenerating to ventricular fibrillation. HF is associated with neuro-hormonal activation and alterations in autonomic control [56]: although these compensatory neuro-hormonal mechanisms provide valuable support for the heart in normal physiological circumstances, they also have a fundamental role in the development and subsequent progression of chronic HF. The sympathetic nervous system is a critical component of neuro-hormonal response observed in HF; in the early stages of the syndrome, an intrinsic decrease in myocardial function leads to an increase in sympathetic activity with consequent increase of heart rate and cardiac contractility that compensate the decreased cardiac output. However, as heart failure worsens, sympathetic activity is further increased in an attempt to compensate for a progressive loss of cardiac function. Unfortunately, chronic exposure of the heart to elevated levels of catecholamines released from sympathetic nerve terminals and the adrenal gland may lead to further pathologic changes in the heart, resulting in a continued sympathetic hyperactivity and a progressive deterioration in cardiac structure and function.
Changes of human cardiac α- and β-AR in chronic HF have been recently reviewed in great detail.
In HF, there is an increase in sympathetic activity and in plasma noradrenaline levels, but functional responsiveness of cardiac β-AR is diminished. This reduction is due to a decrease in β1-AR density and an uncoupling of β2-AR from the Gs-protein-adenylyl cyclase pathway.
In fact, as previously described, in the human heart, β1- and β2-AR coexist, whereby β1-AR predominate; in general, the ratio β1-:β2-AR is about 70%:30% in the atria and 80%:20% in the ventricles, but in heart failure, β1-adrenergic receptor is selectively down-regulated resulting in an approximate 50:50 ratio of β1 to β2 subtypes [21].
In addition, β2-adrenergic receptor seems to be uncoupled from activation of adenylyl cyclase [57]. This latter effect seems to be due to β-adrenergic receptor phosphorylation by specific kinases (GRK2 that phosphorylates both β-adrenergic receptor subtypes in an

Autonomic Nervous System and Cardiac Arrhythmias 85
agonist-dependent manner; PKA and PKC that phosphorylate β-adrenergic receptors in an agonist-independent manner).
Moreover, amount and activity of the inhibitory Gi protein that further dampens β-AR mediated effects is enhanced. Finally, the amount and activity of the neuronal uptake transporter (uptake-1) that causes reuptake of neuronally released noradrenaline into the sympathetic nerve endings is decreased. This decrease in uptake-1 results in increased noradrenaline concentrations at the receptor site that can further contribute to βAR desensitization and down-regulation.
During the last decade, growing evidence has accumulated that β1- and β2-AR genes have genetic polymorphisms that are of functional importance. Many studies investigating possible associations between β-AR genotypes and cardiovascular diseases have been performed; the results are, however, rather inconsistent.
Recent studies have shown that β1- and β2-AR are polymorphic. There are at least two functionally important single nucleotide polymorphisms (SNPs) in
the β1-AR gene [21]: 1) a Ser49Gly polymorphism in the extracellular N-terminus and 2) an Arg389Gly polymorphism in the 4 intracellular loop, which participates in G-protein coupling. Because of the great importance of β1AR in the regulation of heart rate and contractility, attempts have been made to identify possible associations between the Ser49Gly and Arg389Gly β1AR polymorphisms and heart failure. The allelic distribution of Ser49Gly polymorphism has been associated with long-term survival (decreased mortality risk in subjects with Gly49) of patients with heart failure [58] and two studies in patients with dilated cardiomyopathy found that the Gly49 β1AR variant is associated with a lower risk of heart failure [59] or a decreased 5-year mortality risk [58].
Wagoner et al. [60] found that peak oxygen consumption (VO2) during exercise (i.e., a clinically relevant measure of the capacity of the heart to increase cardiac output) was significantly lower in CHF-patients homozygous for Gly389 than in those homozygous for Arg389.
There are at least three functional important SNPs in the β2AR gene: Arg16Gly, Gln27Glu, and Thr164Ile [21]. Although β2AR are expressed in the heart at lower concentrations in comparison with β1-AR subtype, several association studies have investigated a possible role of the three polymorphisms in HF. The role of the Thr164Ile β2AR in HF remains to be questionable but Thr164Ile variant was associated with reduced survival and depressed exercise capacity in patients with heart failure [61]. It has recently been reported that patients with dilated cardiomyopathy and homozygous for the Gln27 β2AR variant had a significantly higher risk for heart failure than patients with the Arg16 and Gln27 β2AR. Furthermore patients with HF homozygous for the Gln27 allele were less likely to respond to the β-blocker carvedilol compared with Gln27 allele suggesting that Gln27 influences the responsiveness of heart failure patients to b-blocker therapy [62].
HRV is significantly different in CHF patients compared to controls. Moreover, some variables derived from HRV analysis showed significant independent prognostic capacity. In particular, the reduction of variance (expressed as SDNN) and low-frequency spectral component of HRV (ranging from 0.03 to 0.15 Hz) seem related to an increased mortality in CHF. Bilchick et al [63] suggest that HRV was the sole independent predictor of overall mortality and was significantly associated with sudden death in this population; in fact

Maurizio Acampa, Maura Lamarina, Luca Puccetti et al. 86
analyzing retrospectively electrocardiographic data from 179 patients in the Veterans Affairs' Survival Trial of Antiarrhythmic Therapy in Congestive Heart Failure these authors showed that patients with SDNN <65.3 ms had a significantly increased risk of sudden death.
Stroke Considerable evidence has been collected over the past 20 years suggesting that acute
stroke may determine a major derangement of cardiovascular function [64]. Stroke has been shown to produce changes in autonomic function, increase the incidence of cardiac arrhythmias, cause myocardial damage, and raise plasma catecholamine levels [65]. The most
important consequence of these changes is an increased susceptibility to sudden death. In patients with acute stroke, the incidence of sudden death as a result of arrhythmic causes has been reported to be 6% [66]. In humans, stroke in both hemispheres has been shown to produce changes in autonomic mechanisms, which lead to myocardial necrosis, arrhythmias,
and even sudden death through related mechanisms. However, the localization of stroke may have differential effects. Lane et al [67] have shown that right hemisphere infarction is associated with a greater number of supraventricular tachycardia, and they speculated that a decrease in cardiac parasympathetic activity in right-sided infarction may cause the probable reciprocal rise in the sympathetic tone. Experimental and clinical studies indicate that certain parts of the cerebral hemisphere, such as the insula, amygdala, and lateral hypothalamus exert influence in the autonomic control of the heart [68]. Of these, the insular cortex within the middle cerebral artery (MCA) territory is the most important cortical area that controls both parasympathetic- and sympathetic-mediated cardiovascular regulation. The insula is frequently involved in stroke because of MCA occlusion, which is a frequent cause of ischemic stroke [69].
Cardiac abnormalities seem to be more frequent in patients with right-sided strokes [70, 71, 72], whereas concurrent insular damage may further impair autonomic function and constitute, at least in the acute phase, increased risk of adverse cardiovascular events.
The suppression of HRV has been described in both hemispheric and brain stem strokes with the use of provocative cardiovascular reflex tests and with traditional time and frequency domain measures of HRV but also the Poincaré measures; moreover, all the spectral components of HRV have been shown to be abolished or significantly decreased in brain-dead patients [73].
Diabetes Mellitus Diabetic cardiomyopathy is a frequent and important complication of diabetes mellitus; it
seems to develop independently of the appearance of circulatory or vascular disorders and its physiological basis is not completely known [74].
Cardiovascular autonomic neuropathy, a common form of autonomic dysfunction found in patients with diabetes, causes abnormalities in heart rate control, as well as defects in central and peripheral vascular dynamics [75]. Individuals with parasympathetic dysfunction

Autonomic Nervous System and Cardiac Arrhythmias 87
have a high resting heart rate most likely because of vagal neuropathy that results in unopposed increased sympathetic outflow. Persons with a combined parasympathetic/sympathetic dysfunction have slower heart rates. With advanced nerve dysfunction, heart rate is fixed. Reduction of heart rate variability is the earliest indicator of cardiovascular autonomic neuropathy. In diabetics, consistent alterations in spectral properties are a frequent early finding: initially a reduction of heart rate variability (total spectral power) is followed by progressive functional denervation, which is associated to severe autonomic dysfunction. The spectral methodology provides some useful potential advantages in respect to the more traditional approach employing several simple bedside tests appearing a convenient method to assess various degrees of diabetic autonomic dysfunction [76].
Clinical manifestations of cardiovascular autonomic neuropathy include exercise intolerance, orthostatic hypotension, asymptomatic ischemia, painless myocardial infarction, and increased risk of mortality due to higher risk of arrhythmias. Diabetic patients show a higher incidence of cardiac arrhythmias, including ventricular fibrillation and sudden death [77].
The electrocardiogram of diabetic patients shows several alterations from normal patterns; the most frequent are those related to cardiac repolarization (the QT interval and T wave): a prolonged QT interval and QT dispersion are associated with higher risk of ventricular arrhythmias [78]. Recently, different alterations in cardiac ionic currents have been described in myocytes isolated from diabetic hearts, mainly a reduction in potassium repolarizing currents. Three different mechanisms could be involved in these alterations [79]: direct metabolic alterations of the cardiac myocyte (such as impaired activity of protein kinases and phosphatases, intracellular pH regulation, intracellular calcium handling, and others), impaired support of extra cardiac factors regulating cardiac activity (such as sympathetic regulation of heart rate and contractility), altered levels of insulin and other trophic factors.
Autonomic neuropathy in diabetes cause an altered sympathetic control of cardiac activity. Degenerate noradrenergic nerve profiles, reduced noradrenaline turnover, reduced noradrenaline content in the stellate ganglion, decreased response to transmural sympathetic stimulation produce an altered cardiac inotropic and chronotropic response. The integrity of several cardiac ionic currents is directly dependent on the integrity of the sympathetic nervous system; in fact there is a trophic effect of sympathetic innervation on the development of L-type calcium channels, sodium channels and on transient outward potassium current. Furthermore, noradrenaline is necessary not only for the development of the current, but also for its maintenance in adult hearts. The sympathetic regulation of transient outward K+ current could have great importance in the genesis of cardiac complications in different pathologies. In type 1 diabetes there is a reduction of cardiac sympathetic activity but the incubation of cardiac myocytes with noradrenaline restores potassium current amplitude to healthy values and this effect is mediated by β-AR. However, acute noradrenaline exposure induced a decrease in the current amplitude by means of α1-AR activation. β-AR mediate also the trophic effect of long lasting exposure of diabetic cardiac myocytes to noradrenaline.

Maurizio Acampa, Maura Lamarina, Luca Puccetti et al. 88
References
[1] Einbrodt: Ueber Herzreizung und ihr Verhaeltnis zum Blutdruck. Akademie der Wissenschaften (Vienna). Sitzungsberichte. 1859; 38: 345.
[2] Levy AG. The exciting causes of ventricular fibrillation in animals under chloroform anesthesie. Heart. 1913; 4: 319-326.
[3] Lown B, Verrier RL. Neural activity and ventricular fibrillation. N. Engl. J. Med. 1976; 294:1165–1170.
[4] El Sherif N. Reentrant ventricular arrhythmias in the late myocardial infarction period. Effect of the autonomic system. Circulation. 1978; 58:103-110.
[5] Schwartz PJ, Vanoli E, Stramba-Badiale M, De Ferrari GM, Billman GE and Foreman RD. Autonomic mechanisms and sudden death. New insights from analysis of baroreceptors reflexes in conscious dogs with and without myocardial infarction. Circulation. 1988; 78: 969-979.
[6] Schwartz PJ, Billman GE, Stone HL. Autonomic mechanisms in ventricular fibrillation induced by myocardial ischemia during exercise in dogs with healed myocardial infarction. An experimental preparation for sudden cardiac death. Circulation. 1984; 69(4): 790-800.
[7] Schwartz PJ, Zaza A, Locati E, Moss AJ. Stress and sudden death. The case of the long QT syndrome. Circulation. 1991; 83(4 Suppl): II71-II80.
[8] Schwartz PJ. The autonomic nervous system and sudden death. Eur. Heart J. 1998; 19 Suppl F: F72-80.
[9] Barron KD, Chokrovrty S. Anatomy of the autonomic nervous system: brain and brainstem. In: Low PA eds. Clinical Autonomic Disorders. Little, Brown and Company. Boston Toronto London; 1993: 3-15.
[10] Loewy AS. Central autonomic pathways. In: Loewy AS, Spyer KM. eds. Central regulation of autonomic functions. New York, NY: Oxford University Press; 1990:88-103.
[11] Kawashima T. The autonomic nervous system of the human heart with special reference to its origin, course, and peripheral distribution. Anat. Embryol. (Berl) 2005; 209(6):425-438.
[12] Paton JF, Boscan P, Pickering AE, Nalivaiko E. The yin and yang of cardiac autonomic control: vago-sympathetic interactions revisited. Brain Res. Brain Res. Rev. 2005; 49(3):555-565.
[13] Randall WC, Armour JA, Geis WP, and Lippincott DB. Regional cardiac distribution of sympathetic nerves. Fed. Proc. 1972; 31: 1199–1208.
[14] Levy MN and Martin PJ. Neural control of the heart. In: Handbook of Physiology. The cardiovascular system: The Heart. Bethesda, MD: Am. Physiol. Soc, sect. 2, vol. 1, 1979, p. 581–620.
[15] Hillarp NA. Peripheral autonomic mechanisms. In: Handbook of Physiology. Neurophysiology. Bethesda, MD: Am Physiol Soc, vol. II, sect. I, p. 979–1006, 1960.
[16] Levy MN. Neural control of cardiac function. Baillieres Clin. Neurol. 1997; 6(2):227-244.

Autonomic Nervous System and Cardiac Arrhythmias 89
[17] Oppenheimer S. Cerebrogenic cardiac arrhythmias: cortical lateralization and clinical significance. Clin. Auton. Res. 2006; 16(1):6-11.
[18] Oppenheimer SM and Hopkins DA. Suprabulbar neuronal regulation of the heart. In: Neurocardiology, edited by Armour JA and Ardell JL. New York: Oxford University Press, 1994, p. 309–342.
[19] Ardell JL. Neurohumoral control of cardiac function. In: Heart Physiology and Pathophysiology, edited by Sperelakis N, Kurachi Y, Terzic A, and Cohen MV. New York: Academic, 2001, p. 45–59.
[20] Armour JA. Cardiac neuronal hierarchy in health and disease. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2004; 287: R262-R271.
[21] Brodde O-E, Bruck H, Leineweber K. Cardiac adrenoceptors: physiological and pathophysiological relevance. J. Pharmacol. Sci. 2006; 100: 323-337.
[22] Bristow MR, Minobe W, Rasmussen R, Hershberger WE, Hoffman BB. Alpha-1 adrenergic receptors in the nonfailing and failing human heart. J. Pharmacol. Exp. Ther. 1988; 247:1039–1045.
[23] Li K, He H, Li C, Sirois P, Rouleau JL. Myocardial α1-adrenoceptor:inotropic effect and physiologic and pathologic implications. Life Sci. 1997; 60:1305–1318.
[24] Shibata EF, Brown TLY, Washburn ZW, Bai J, Revak TJ and Butters CA. Autonomic regulation of voltage-gated cardiac ion channels. J. Cardiovasc. Electrophysiol. 2006; 17 (Suppl1): S34-S42.
[25] Zipes DP. Cardiac innervation and its importance in the genesis of some cardiac arrhythmias. In: Challenges in Cardiology, edited by Rackley CE. Mount Kisco, NY: Futura, 1992, vol. 1, p. 1–27.
[26] Davis AM, Natelson BH. Brain-Heart interactions. The neurocardiology of arrhythmia and sudden cardiac death. Texas Heart Institute Journal. 1993; 20: 158-169.
[27] Schauerte P, Scherlag BJ, Patterson E, Scherlag MA, Matsudaria K, Nakagawa H, Lazzara R, and Jackman WM. Focal atrial fibrillation: experimental evidence for a pathophysiologic role of the autonomic nervous system. J. Cardiovasc. Electrophysiol. 2001; 12: 592–599.
[28] Cardinal R. Autonomic modulation of myocardial electrical properties and cardiac rhythm. In: Neurocardiology, edited by Armour JA and Ardell JL. New York: Oxford University Press, 1994, p. 165–191.
[29] Armour JA. Comparative effects of endothelin and neurotensin on intrinsic cardiac neurons. Peptides. 1996; 17: 1047–1052.
[30] Anderson KP. Sympathetic nervous system activity and ventricular tachyarrhythmias: recent advances. Ann. Noninvasive Electrocardiol. 2003; 8:75-89.
[31] Lerman BB, Engelstein ED, Burkhoff D. Mechanoelectrical feedback—Role of beta-adrenergic receptor activation in mediating load-dependent shortening of ventricular action potential and refractoriness. Circulation. 2001; 104:486–490.
[32] Meredith IT, Broughton A, Jennings GL, et al. Evidence of a selective increase in cardiac sympathetic activity in patients with sustained ventricular arrhythmias. N. Engl. J. Med. 1991;325: 618–624.

Maurizio Acampa, Maura Lamarina, Luca Puccetti et al. 90
[33] Engelhardt S, Hein L, Wiesmann F, et al. Progressive hypertrophy and heart failure in beta1-adrenergic receptor transgenic mice. Proc. Natl. Acad. Sci. USA. 1999; 96:7059–7064.
[34] Bisognano JD, Weinberger HD, Bohlmeyer TJ, et al. Myocardial-directed overexpression of the human beta(1)-adrenergic receptor in transgenic mice. J. Mol. Cell. Cardiol. 2000; 32:817–830.
[35] Morisco C, Zebrowski DC, Vatner DE, et al. Beta-adrenergic cardiac hypertrophy is mediated primarily by the beta(1)-subtype in the rat heart. J. Mol. Cell. Cardiol. 2001; 33:561–573.
[36] Saito S, Hiroi Y, Zou Y, et al. Beta-adrenergic pathway induces apoptosis through calcineurin activation in cardiac myocytes. J. Biol. Chem. 2000; 275:34528–34533.
[37] Aimond F, Alvarez JL, Rauzier JM, et al. Ionic basis of ventricular arrhythmias in remodeled rat heart during long-term myocardial infarction. Cardiovasc. Res. 1999; 42: 402–415.
[38] Zhang TT, Takimoto K, Stewart AFR, et al. Independent regulation of cardiac Kv4.3 potassium channel expression by angiotensin II and phenylephrine. Circ. Res. 2001; 88: 476–482.
[39] Pak PH, Nuss HB, Tunin RS, et al. Repolarization abnormalities, arrhythmia and sudden death in canine tachycardia-induced cardiomyopathy. J. Am. Coll. Cardiol. 1997; 30: 576–584.
[40] Freeman R. Assessment of cardiovascular autonomic function. Clin. Neurophysiol. 2006; 117(4):716-730.
[41] Sztajzel J. Heart rate variability: a non-invasive electrocardiographic method to measure the autonomic nervous system. Swiss Med. Wkly. 2004; 134: 514-522.
[42] Task Force of the European Society of Cardiology and the North American Society of Pacing Electrophysiology. Heart rate variability: standards of measurement, physiological interpretation, and clinical use. Circulation. 1996;93:1043–65.
[43] Eckberg DL. Physiological basis for human autonomic rhythms. Ann. Med. 2000; 32(5): 341-349.
[44] Bernardi L, Valle F, Coco M, Calciati A, Sleight P. Physical activity influences heart rate variability and very-low-frequency components in Holter electrocardiograms. Cardiovasc. Res. 1996; 32(2): 234-237.
[45] Lombardi F. Chaos theory, heart rate variability, and arrhythmic mortality. Circulation. 2000; 101: 8-10.
[46] Huikuri HV, Makikallio TH, Perkiomaki J. Measurement of heart rate variability by methods based on nonlinear dynamics. J. Electrocardiol. 2003; 36 (Suppl): 95-99.
[47] Parati G, Di Rienzo M, Mancia G. How to measure baroreflex sensitivity: from the cardiovascular laboratory to daily life. J. Hypertension. 2000; 18: 7-19.
[48] Zicha S, Tsuji Y, Shiroshita-Takeshita A, Nattel S. Beta-blockers as antiarrhythmic agents. Handb. Exp. Pharmacol. 2006; 171: 235-266.
[49] Vracko R, Thorning D, Frederickson RG. Nerve fibers in human myocardial scars. Hum. Pathol. 1991; 22: 138-146.

Autonomic Nervous System and Cardiac Arrhythmias 91
[50] Chen LS, Zhou S, Fishbein MC, Chen PS. New perspectives on the role of autonomic nervous system in the genesis of arrhythmias. J. Cardiovasc. Electrophysiol. 2007; 18: 123-127.
[51] Chen PS, Chen LS, Cao JM, Sharifi B, Karagueuzian HS, Fishbein MC. Sympathetic nerve sprouting, electrical remodeling and the mechanisms of sudden cardiac death. Cardiovasc. Res. 2001; 50: 409-416.
[52] Zipes DP, Rubart M. Neural modulation of cardiac arrhythmias and sudden cardiac death. Heart Rhythm. 2006; 3: 108-113.
[53] Bigger JT, Fleiss JL, Rolnitzky LM, Steinmann RC. Frequency domain measures of heart rate pediod variability to assess risk late after myocardial infarction. J. Am. Coll. Cardiol. 1993;21:729–36.
[54] Quintana M, Storck N, Lindblad LE, Lindvall K, Ericson M. Heart rate variability as a means of assessing prognosis after myocardial infarction. A 3-year follow-up study. Eur. Heart J. 1997; 18:789–97.
[55] Huikuri HV, Makikallio TH. Heart rate variability in ischemic heart disease. Auton. Neurosci. 2001;90: 95-101.
[56] Watson AM, Hood SG, May CN. Mechanisms of sympathetic activation in heart failure. Clin. Exp. Pharmacol. Physiol. 2006; 33: 1269-1274.
[57] Lohse MJ, Vilardaga JP and Bunemann M. Direct optical recording of intrinsic efficacy at a G protein-coupled receptor. Life Sci. 2003; 74:397-404.
[58] Borjesson M, Magnusson Y, Hjalmarson A and Andersson B. A novel polymorphism in the gene coding for the beta(1)-adrenergic receptor associated with survival in patients with heart failure. Eur. Heart J. 2000; 21:1853-1858.
[59] Forleo C, Resta N, Sorrentino S, Guida P, Manghisi A, De LucaV, et al. Association of β-adrenergic receptor polymorphisms and progression of heart failure in patients with idiopathic dilated cardiomyopathy. Am. J. Med. 2004; 117:451–458.
[60] Wagoner LE, Craft LL, Zengel P, McGuire N, Rathz DA, Dorn GW, et al. Polymorphisms of the β1-adrenergic receptor predict exercise capacity in heart failure. Am. Heart J. 2002;144: 840–846.
[61] Wagoner LE, Craft LL, Singh B, Suresh DP, Zengel PW, Mcguire N, Abraham WT, Chenier TC, Dorn GW and Liggett SB. Polymorphisms of the β2-adrenergic receptor determine exercise capacity in patients with heart failure. Circ. Res. 2000; 86: 834-840.
[62] Kaye DM, Smirk B, Williams C, Jennings G, Esler M and Holst D. Beta-adrenoceptor genotype influences the response to carvedilol in patients with congestive heart failure. Pharmacogenetics. 2003; 13: 379-382.
[63] Bilchick KC, Fetics B, Djoukeng R, Fisher SG, Fletcher RD, Singh SN, Nevo E, Berger RD. Prognostic value of heart rate variability in chronic congestive heart failure (Veterans Affairs' Survival Trial of Antiarrhythmic Therapy in Congestive Heart Failure). Am. J. Cardiol. 2002; 90: 24-28.
[64] Oppenheimer SM, Lima J. Neurology and the heart. J. Neurol. Neurosurg. Psychiatry. 1998; 64: 289–297.
[65] Barron SA, Rogovski Z, Hemli J. Autonomic consequences of cerebral hemisphere infarction. Stroke. 1994; 25: 113–116.

Maurizio Acampa, Maura Lamarina, Luca Puccetti et al. 92
[66] Silver FI, Norris JW, Lewis AJ, Hachinski VC. Early mortality following stroke: a prospective review. Stroke. 1984; 15: 492–496.
[67] Lane RD, Nallace JD, Petrosky PP, Schwartz GE, Gradman AH. Supraventricular tachycardia in patients with right hemisphere stroke. Stroke. 1992; 23: 362–366.
[68] Tokzoglu SL, Batur MK, Topcuglu MA, Sarbas O, Kes S, Oto A. Effects of stroke localization on cardiac autonomic balance and sudden death. Stroke. 1999; 30: 1307–1311.
[69] Colivicchi F, Bassi A, Santini M, Caltagirone C. Cardiac autonomic derangement and arrhythmias in right-sided stroke with insular involvement. Stroke. 2004; 35: 2094-2098.
[70] Naver HK, Blomstrand C, Wallin G. Reduced heart rate variability after right-sided stroke. Stroke. 1996; 27: 247–251.
[71] Orlandi G, Fanucchi S, Strata G, Pataleo L, Landucci Pellegrini L, Prontera C, Martini A, Murri L. Transient autonomic nervous system dysfunction during hyperacute stroke. Acta Neurol. Scand . 2000; 102: 317–321.
[72] Tokzoglu SL, Batur MK, Topcuglu MA, Sarbas O, Kes S, Oto A. Effects of stroke localization on cardiac autonomic balance and sudden death. Stroke. 1999; 30: 1307–1311.
[73] Korpelainen J, Sotaniemi K, Mäkikallio A, Huikuri H, Myllylä V. Dynamic behavior of heart rate in ischemic stroke. Stroke. 1999; 30: 1008–1013.
[74] Resnick HE, Howard BV. Diabetes and cardiovascular disease. Annu. Rev. Med. 2002; 53: 245-267.
[75] Maser RE, Lenhard MJ. Cardiovascular autonomic neuropathy due to diabetes mellitus: clinical manifestations, consequences, and treatment. J. Clin. Endocrinol. Metab. 2005; 90: 5896-5903.
[76] Pagani M. Heart rate variability and autonomic diabetic neuropathy. Diabetes Nutr. Metab. 2000; 13: 341-346.
[77] Ewing DJ, Boland O, Neilson JM, Cho CG, Clarke BF: Autonomic neuropathy, QT-interval lengthening, and unexpected deaths in male diabetic patients. Diabetologia. 1991; 34:182–185.
[78] Robillon JF, Sadoul JL, Benmerabet S, Joly-Lemoine L, Fredenrich A, Canivet B. Assessment of cardiac arrhythmic risk in diabetic patients using QT dispersion abnormalities. Diabetes Metab. 1999; 25: 419-423.
[79] Casis O, Echevarria E. Diabetic cardiomyopathy: electromechanical cellular alterations. Curr. Vasc. Pharmacol. 2004; 2: 237-248.

In: Cardiac Arrythmia Research Advances ISBN: 978-1-60021-795-1 Editor: Lynn A. Vespry, pp. 93-135 © 2007 Nova Science Publishers, Inc.
Chapter IV
External Triggering, Modifying and Chronobiologic Factors for Ventricular
Arrhythmias
Viktor Čulić* Division of Cardiology, Department of Medicine,
University Hospital Split, Split, Croatia
Abstract
Research on cardiac arrhythmias includes a variety of fields, levels and techniques. From the clinician’s point of view, an increasing awareness concerning external circumstances and events, and other exogenous factors that may be implicated in the triggering of cardiac arrhythmias make it important to provide appropriate recommendations for prevention in the patients suffering from arrhythmia.
A physiological adaptive response to the wide range of everyday situations and activities involves activation of the sympathetic nervous system. In susceptible patients with ischemic or other structural heart disease, sympathetic activation results in heterogeneous rather than homogeneous sympathetic activity which seems to be an important pathophysiologic event for the initiation of cardiac arrhythmias. Emotional stressors and physical activity are the best described triggers caused by sympathetic arousal, while reports describing individuals experiencing ventricular arrhythmias after drinking caffeine or alcoholic beverages need further support using controlled data. An association with arrhythmia has also been reported for two groups of environmental factors, air pollutants and meteorologic variables. However, pathophysiologic mechanisms through which higher levels of sulfate, nitrogen dioxide, carbon monoxide, black carbon, and fine particle mass as well as very weak or very strong winds, periods of rising relative air moisture and falling atmospheric pressure may cause arrhythmia deserve further consideration.
* Correspondence: Dr. Viktor Čulić; Division of Cardiology; Department of Medicine; University Hospital Split;
Spinčićeva 1; 21000 Split, Croatia; e-mail: [email protected]

Viktor Čulić 94
Whilst external triggers increase the risk of arrhythmia within the time frame of several hours after exposure, modifying factors probably alter individual susceptibility to external triggers. Gender, age, psychosocial factors, polyunsaturated fatty acids, digitalis, beta-blocking and other antiarrhythmic therapy seem to be modifying factors that most significantly impact the myocardial vulnerability. Beyond all external and modifying influences and despite the fact that external triggers most likely occur randomly throughout time, diurnal, weekly and seasonal chronobiologic phenomena of variation in incidence of cardiac arrhythmias do exist. Regardless of population or climate, arrhythmic events tend to occur more frequently in the morning, on Mondays, and during the winter months, but the reasons for such a distribution are still speculative.
We must yet discover the precise processes included in the transition from the single ventricular ectopic beat all the way to malignant ventricular arrhythmias. Future investigations of external triggering, modifying and chronobiologic factors as well as measures and therapies aimed at blocking the adverse effects of these factors may improve prevention of cardiac arrhythmias and sudden cardiac death.
Introduction New data about genetic, cellular, biochemical, pathophysiologic, clinical and
epidemiologic mechanisms and features of occurrence of ventricular arrhythmias become available continuously. One of the most important challenges for both basic investigators and clinicians dealing with the arrhythmias is to integrate growing knowledge and to provide appropriate update and recommendations for the patients suffering from arrhythmia. Ventricular tachyarrhythmias, primarily ventricular tachycardia and ventricular fibrillation, are common precursors to sudden cardiac death [1-3]. Every effort to prevent ventricular tachyarrhythmias may prove useful and life-saving and therefore has its place in both individual and public health level.
Fulfilled everyday life consists of a variety of activities, interpersonal communications, changes in emotional state, basic physiological needs, and other situations that can hardly be predicted or prepared for. Last several decades brought major advances in the field of triggering acute cardiac events by daily events. The clinical features of triggering were most clearly demonstrated for acute myocardial infarction whose one half of onsets is preceded by external triggers, whereas in other half possible triggers could not be identified. Emotional stress, heavy or moderate physical activity, ingestion of a meal, and exposure to bed weather conditions have been defined as the most frequent triggers [4,5].
Growing concern has been raised regarding the triggering of ventricular tachyarrhythmias as well. Although the use of new technologies and research models provides expansion of the knowledge about the external triggering, there is still much to learn about external influences on arrhythmogenesis. This chapter brings experimental and clinical data explaining how daily activities and events may cause ventricular arrhythmias. For some of such external triggers pathophysiologic background of triggering is well known, for some it is mostly speculative.
A majority of external triggers of acute cardiac events cause the pathophysiological cascade that may be referred to as sympathetic triggering pathway [4]. General scheme of this pathway is depicted in figure 1. Prototypes of the circumstances that induce such a response

External Triggering, Modifying and Chronobiologic Factors… 95
are physical activity and emotional stress and the period of elevated risk for an event lasts during and probably up to two hours after the exposure [4-6]. The sympathetic triggering pathway starts with the arousal of the sympathetic nervous system and includes mechanisms such as increase in arterial blood pressure, heart rate, myocardial contractility and vasoconstrictive stimuli. These mechanisms favor development of myocardial ischemia or atherothrombosis of disrupted coronary plaque with consequent acute coronary syndrome, the conditions that facilitate cardiac arrhythmias. Apart from these mechanisms, heterogeneous sympathetic activity has been proposed as an independent proarrhythmic mechanism associated with sympathetic arousal [7]. Endogenous processes related to body response to an external trigger and involved in initiation of cardiac event have been termed internal triggering mechanisms [4-6].
Figure 1. Daily events and environmental influences cause sympathetic activation as a normal adaptive reaction. That sympathetic reaction initiates several pathophysiologic processes that may be referred to as internal triggering mechanisms because they create an environment of an increased risk of acute cardiac disease and may cause triggering. Therefore, external circumstances may serve as triggers of “acute cardiac events triangle” including acute coronary syndromes, ventricular arrhythmia and sudden cardiac death.

Viktor Čulić 96
In susceptible patients, every imbalance of autonomic nervous system may trigger malignant ventricular tachyarrhythmia and cause sudden cardiac death [8]. It is difficult to distinguish between external triggers of cardiac events and to define only some of them as exclusive arrhythmia triggers. However, any explanation of the triggering mechanisms should consider much complex interplay among underlying pathological conditions. At the end, the “acute cardiac event” triangle may occur (figure 1). In this triangle, acute coronary syndrome and cardiac arrhythmia may induce development of each other, both possibly leading to sudden cardiac death.
Although it seems logic to assume that external triggers occur on a random basis, the evidence of chronobiologic rhythms of arrhythmias and other acute cardiac events can be found in practically all investigations and populations around the globe. A daily rhythm with a morning peak, a weekly rhythm with a Monday peak and seasonal variation with a winter peak incidence are the major patterns of chronobiology that must be further explored. The probable mechanisms of morning excess in cardiovascular events have been identified. In contrast, we do not fully understand biologic and pathophysiologic mechanisms of weekly and seasonal variation. These two variations likely result from the interactions among endogenous and exogenous triggering factors and modifying factors affecting myocardial vulnerability (figure 2).
Figure 2. Ischemic heart disease and other cardiac or genetic disorders may create the pathomorphologic substrate for myocardial vulnerability. In vulnerable myocardium, there is a circadian, and perhaps weekly and seasonal variation in risk, but the actual moment of onset is often determined by activities, events and environmental factors that have been implicated as external triggers. Modifying factors do not determine development of myocardial substrate or the very moment of triggering, but may influence myocardial vulnerability and in combination with external triggers may contribute to chronobiologic variations in the occurrence of ventricular arrhythmias

External Triggering, Modifying and Chronobiologic Factors… 97
Development of the field of triggering of acute cardiac events, including arrhythmias, sought for an appropriate terminology for the new knowledge. The term vulnerable patient has been proposed [9,10] for the patients with high likelihood of suffering from one of the incidents from the acute cardiac event triangle in the near future. The patient vulnerability consists of three basic components of vulnerability: plaque, blood and myocardium. Vulnerable plaque refers to atherosclerotic lesions prone to disruption and development of atherothrombosis. Vulnerable blood describes state of increased coagulability favoring thrombogenesis, while vulnerable myocardium refers to the heart prone to malignant ventricular arrhythmia. Presence and intensity of each of these components define the patient vulnerability. Vulnerability develops over the years and decades, and usually results from the presence of traditional, also termed chronic [4,5], risk factors such as diabetes, smoking, hypertension, hyperlipidemia, homocysteine, etc. For cardiac arrhythmias, the term modifying factors has been proposed for the factors that may increase myocardial vulnerability through biochemical, pathophysiologic or electrophysiologic processes without affecting the underlying heart disease and to distinguish them from the factors that may be defined as chronic [6].
Vulnerable myocardium is in most cases a consequence of ischemic heart disease, whether with or without prior myocardial injury caused by atherosclerotic lesions of coronary arteries or other pathological substrate such as myocardial fibrosis, inflammation, ischemia or previous myocardial infarction. Nonischemic vulnerable myocardium is present in the reminder of patients having some type of cardiomyopathy or valvular heart disease, and in those with a wide spectrum of congenital syndromes (long QT, Brugada and WPW syndrome, polymorphic ventricular tachycardia, etc) or other acquired conditions with arrhythmia propensity (drug-induced long QT syndrome, commotio cordis, etc). When sudden cardiac death occurs without atherothrombosis leading to acute coronary syndromes, a terminal arrhythmic episode is facilitated by alteration in autonomic tone or electrolyte status, metabolic or inflammatory factors, previous myocardial injury, vasospasm or embolia to the coronary artery.
Like any other living cell or tissue, the myocardium is an open system. A variety of transient influences may affect its vulnerability over the course of day, week or month. The term modifying factors is introduced for such influences that may directly change susceptibility to arrhythmia under external or other trigger independently of possible influence of such factors on eventual underlying structural heart disease. Integration of external triggers, internal triggering mechanisms, modifying factors, chronobiologic rhythms, myocardial vulnerability, and chronic risk factors into one concept provides more complete picture of arrhythmogenesis.
External Triggering Factors
Emotional Stress The proposal that an acute emotional arousal can trigger life-threatening arrhythmias is
well funded. The mechanisms of increased risk of arrhythmic event during the emotionally

Viktor Čulić 98
stressful events have been recognized. Animal model studies have shown that anger-like stresses may increase the myocardial vulnerability and may provoke abnormalities in rhythm, while these consequences may be prevented by a ß-adrenergic blockade [11,12]. The T-wave alternans is an index of beat-to-beat variation in T-wave morphology and is accepted as a marker of cardiac electrical instability [13,14]. This instability represents the prediction of likelihood of an arrhythmic event in a susceptible patient. Acute mental stress elicits increase in T-wave alternans, irrespectively of and to much greater extent to the increase in heart rate [15]. However, T-wave alternans is held to be at least partially independent of heart rate due to the temporospatial heterogeneity of the process of repolarization, corresponding to the myocardial electrical instability and arrhythmia propensity [16,17].
Emotional arousal may induce the increase in QT variability [18]. Increased QT variability has also been proposed as a marker of myocardial repolarization lability and increased risk for malignant tachyarrhythmias [19,20]. In patients with implantable cardioverter-defibrillator, emotional stress increases electrical termination thresholds during electrophysiological testing, altered circuit of ventricular tachycardia and accelerates its rate [21]. Finally, emotional stress can induce ventricular arrhythmias uncovering latent proarrhythmic conditions [22].
The triggering role of emotional stress for cardiac arrhythmia is supported in the clinical settings. At first, informal case series have linked acute episodes of emotional distress with ventricular tachycardia, cardiac arrest or sudden cardiac death [23-26]. Successively, more firm evidence has been obtained. Independently of physical activity or meteorologic condition, acute episode of emotional stress may trigger ventricular ectopic beats [27] and ventricular tachycardia [6]. In patients with implantable cardioverter-defibrillators, moderate levels of emotional stress, notably anger, were more likely during the periods preceding shock for spontaneous ventricular tachycardia or fibrillation than during control periods [28,29].
Emotional and physical stressors are the most powerful external triggers of acute cardiac events in general. They both cause sympathetic arousal and operate via internal triggering mechanisms of the sympathetic triggering pattern (figure 1). Nonetheless, there are indications that emotional stress may be more potent trigger of ventricular arrhythmias than physical activity in the same patient. Weighting the association of physical activity, emotional stress and a number of meteorologic conditions with the episodes of ventricular tachycardia, our study has shown the greatest independent association for emotional stress. The association was stronger in women and those under the age of 65 [6]. In the study adjusting the individual heart rate during exercise and during emotional stress, QT interval shortening in response to exercise was normally more pronounced than it was in the response to emotional stress [30]. However, such a QT adaptation was not seen in patients with type 1 and type 2 variants of long QT syndrome. Considering myocardial vulnerability assessed by T-wave alternans, proarrhythmic condition occurs at substantially lower heart rates during emotional stress than during exercise [15].
The increase in serum potassium concentration during the exercise probably results from release from the skeletal muscles, correlates with the level of activity [30,31] and inversely correlates with changes in QT interval in healthy people [30]. In contrast, no change in serum potassium associated with emotional stress and QT interval values has been observed [30].

External Triggering, Modifying and Chronobiologic Factors… 99
Furthermore, the overall catecholamine secretion is held to be similar during emotional and physical stress, but with a tendency toward a higher adrenaline and lower noradrenaline response during emotional than during physical stress [30,32]. In addition to other proarrhythmic effects via adrenergic system, adrenaline induces hypokalemia [33-37] by increasing intracellular potassium flux in skeletal muscles [38]. Hypokalemia is a well known risk factor for ventricular arrhythmia [39-42] and greater levels of serum potassium may be a protective factor during the periods of physical activity compared with acute episodes of emotional stress.
Several studies suggested that, apart from hypokalemia, disturbed cardiac repolarization due to increase in circulating adrenaline could be additional independent mechanism contributing to an arrhythmia occurrence [33,36]. Adrenaline also causes significant falls in serum magnesium and calcium [35], both being potentially proarrhythmic factors. It is tempting to speculate that the difference in adrenaline compared to noradrenaline secretion ratio between emotional stress and physical activity [30,32] may be the next distinguishing mechanism. In physiological settings, adrenaline induces significant increase in heart rate and systolic blood pressure, and a significant decrease in diastolic blood pressure [35,36]. These effects are mediated primarily through ß-1 and ß-2 adrenergic receptors, and are coupled with increased myocardial contractility. In contrast to that, the most pronounced cardiovascular effect of noradrenaline is the general increase in blood pressure through arteriolar vasoconstriction mediated by α-1 adrenergic receptors [43,44]. Therefore, in addition to electrolyte disbalance and other metabolic changes, the increased automaticity, chronotropic and dromotropic effects, and heterogeneous sympathetic stimulation could be the second, neurocardiac segment of more proarrhythmic effect of adrenaline versus noradrenaline. The third potential segment could be the hemodynamic difference. Coronary blood flow and cardiac oxygen supply mostly take place during diastole. In the presence of coronary disease or other pathological substrate, fall in diastolic blood pressure caused by adrenaline may hypothetically decrease already compromised coronary flow, and favor occurrence of myocardial ischemia and ventricular arrhythmia.
Clinical reports investigating the myocardial infarction and transient left ventricular apical ballooning syndrome further support differences between the triggering by emotional stress and by physical activity. Emotional stress more significantly increases the relative risk of acute myocardial infarction in women [45] and more often precedes onset among them [5,46]. Emotional stress also more often precedes the onset of inferior than anterior infarction [47], as well as the infarction with later development of a Q-wave in electrocardiogram versus those without a Q-wave [48].
The transient left ventricular apical ballooning syndrome or takotsubo cardiomyopathy is a disorder whose pathophysiology is not well understood [49-51]. Although raw data suggest that its onset is preceded by physical and emotional stress in 38 and 27% of cases, respectively [49], controlled data are still missing. However, some data convincingly suggest that emotional stress has the pivotal role in the triggering of this disorder primarily affecting women [50-52]. A greater possibility of transient vasoconstriction associated with emotional stress has been proposed as a common distinguishing mechanism for above described differences in triggering [4,5,46-52].

Viktor Čulić 100
In conclusion, the linkage between emotional stress and arrhythmia is likely threefold: a direct neurocardiac impact, an indirect effect on myocardial ischemia, and adrenaline caused metabolic changes. A hypothesis that some individuals, due to psychological factors, have a greater susceptibility to arrhythmic events triggered by emotional stress has also been put forward. As discussed below, patients with depression, anxiety or those with type A or type D personality could be to some extent more vulnerable population in the context of emotional triggering.
Physical Activity The role of physical activity in the occurrence of myocardial infarction has been
extensively investigated. It has been estimated that the hazard period for myocardial infarction lasts for an hour after the physical exertion. The estimated relative risk of triggering is about 100 for sedentary people. Habitual physical activity progressively lower the risk down to the relative risk of about only two for those who exercise five or more times per week [5,53,54]. No information of this type has been obtained for the cardiac arrhythmias. Furthermore, physical activity seems to be a more frequent precipitator of myocardial infarction in men than in women [46], in those with anterior than in those with inferior infarction [47], as well as in those with Q wave than in those with non-Q wave infarctions [48].
Studies in patients with implantable cardioverter-defibrillator showed that even mild-to-moderate activities, such as slow walking or shopping, may provide sufficient sympathetic activation to trigger ventricular arrhythmias [25,26]. Activity of the adrenergic and autonomic nervous system is involved in T-wave alternans induced by physical activity and this response is related to adverse cardiac events in patients at high risk for arrhythmia [55-57]. However, after correction for the heart rate increase, T-wave alternans is less pronounced with physical activity than with emotional stress [15].
There are two specific situations where physical activity is the important trigger of arrhythmic events. In the patients with inherited long QT syndrome type 1, the mutation strikes potassium channel subunit KCNQ1 and physical activity is a typical trigger of ventricular tachyarrhythmias [58]. Another peculiarity is the occurrence of the right ventricular outflow tract tachycardia in young patients without a structural heart disease. Although this arrhythmia in general appears to be more frequent in women [59-61], external triggers, primarily exercise, have been associated with the majority of arrhythmia episodes in men, and with less than half of episodes in women [62].
As noted above, the risk for an arrhythmia seems to be lower with physical than with emotional stressors in the same patient [6]. Yet, possible underlaying mechanisms are hypothetical as described in the part of text regarding emotional stress. Similar to triggering by emotional stress, some population subgroups may have a greater propensity to triggering of arrhythmia by physical stress. Our investigation on external triggers of ventricular arrhythmias has provided some results in that direction suggesting the complexity of network of mechanisms that determine the transition of single ventricular ectopic beat to a malignant arrhythmia. We observed a strong positive association of physical activity of the level of 4 or

External Triggering, Modifying and Chronobiologic Factors… 101
more METs with ventricular ectopic beats in individuals under the age of 65 and women, but no such association in elderly and men [27]. On the contrary, the association between physical activity and ventricular tachycardia varied according to gender and the type of weather parameters included in the models [6]. For instance, in consideration of fixed meteorologic situation for 2-hour periods, physical activity increased the risk of ventricular tachycardia in men. However, in consideration of dynamic changes of meteorologic variables in 3-hour periods, we observed a “protective” effect of physical activity in men and those under the 65 years of age. Similar patterns were present in the counterpart groups but without reaching the level of statistical significance.
Several hypotheses can be made. Such a nonuniform relationship between single ectopic beats and more complex arrhythmias, as well as apparently diverse effect of physical activity in the wider circumstantial and ambient framework suggest a multifaceted nature of pathogenesis of the malignant arrhythmia. A variety of endogenous and exogenous, acute and chronic, triggering and modifying factors interact with each other in their influence on the ventricular arrhythmias. At present, it appears that all these factors interfere with the triggering potential of physical activity more drastically than with the potentials of other external triggers. Nonetheless, there is still much to be revealed in this regard.
Caffeine Similar to alcohol consumption, recent data suggest a J-shaped association between
coffee drinking and heart disease, with moderate consumption as an optimal option [63,64]. Caffeine usually makes the person more alert, clear-minded and better in performing different tasks. The acute effects of coffee intake include increased sympathetic tone, and blood pressure [65-67], the internal triggering mechanisms of a typical sympathetic triggering pathway for acute cardiac events [4]. Baylin and coworkers have suggested that coffee intake may trigger myocardial infarction, especially among those who drink up to a cup of coffee per day in average, those with multiple chronic cardiovascular risk factors or those with a sedentary lifestyle. The hazard period appears to extend over an hour after the intake [68].
Clinical evidence suggests that moderate ingestion of caffeine does not affect prevailing cardiac rhythm and rate or cause clinically significant ventricular or supraventricular arrhythmia [69-71]. This seems to relate to the patients with ischemic heart disease, postinfarction patients, and even to the patients with known life-threatening arrhythmia [72,73].
Caffeine toxicity is often a consequence of self-intended poisoning. Occasionally, it may cause tachyarrhythmias such as supraventricular tachycardia, atrial fibrillation, ventricular tachycardia, and ventricular fibrillation [66,74-76]. An example of such an extraordinary circumstance is the occurrence of ventricular fibrillation and cardiac death in a young female with the mitral valve prolapse immediately after ingestion of the equivalent of eight cups of coffee in a form of guarana “natural energy” drink [77]. Possibility that coffee may trigger sudden cardiac death is supported in a case-crossover study by Šelb-Šemerl and Šelb [78]. Drinking one to five cups per day significantly contributed to that risk during the first hour

Viktor Čulić 102
after consumption, particularly in men, overweight or obese, regular smokers, physical active persons and those with family history of myocardial infarction or sudden cardiac death.
In a broader sense, other possible external triggers like mental or behavioral stress may play a synergistic role in caffeine effects on blood pressure [79]. In conclusion, the mechanisms explaining some effects of caffeine are not completely clear, and neither is the role of caffeine in cardiovascular risk, both acute and chronic. Moreover, coffee intake has been implicated as a contributing factor for a circadian [68,80] and even perhaps for a weekly pattern of cardiovascular incidents [80].
Alcohol Alcohol is causally related to the considerable number of various medical conditions.
Low-to-moderate consumption confers a lower incidence and mortality from coronary heart disease compared to both non-drinking and intake of above-moderate amounts of alcohol. The lowest risk has been found at fewer than two drinks per day [81-83], and putative protective mechanisms include the effects on lipids and haemostatic factors [82-84]. However, besides positive effects, alcohol has a numerous deleterious effects on cardiovascular and other systems in the human body.
Heavy alcohol consumption can have a direct toxic effect on the heart resulting in alcoholic cardiomyopathy [82,84,85] an underlying condition for the future arrhythmic episodes. In this cardiomyopathy, the damage to the ventricular conduction system and myocardium is mainly mediated by acetaldehyde, rather than by a nutritional or electrolyte disturbance. The adverse effects of acute alcohol ingestion may require a combination with chronic excessive drinking. While administration of alcohol in habitual non-drinkers shows no delay in His-ventricular conduction [86], achieving alcohol blood levels of 0.3-1 g/l in patients with palpitations or light-headedness who moderate or heavy drink may cause such a conduction delay and a range of supraventricular and ventricular arrhythmias [87]. In dogs fed with a diet containing 36% of calories as alcohol, the greater susceptibility of the myocardium to circulating ß-agonists and lowered electrical threshold for ventricular fibrillation was observed in comparison with controls [88]. In one study in patients with ischemic heart disease, alcohol induces an increase in the number of ectopic beats [89].
An important pattern of heavy drinking, also called “binge drinking”, has been in particular linked to sudden coronary death, but also to the increased risk of coronary heart disease in general [81-83,90,91]. The binge drinking has been quantitatively defined as the consumption of five or more drinks per occasion for men, and four or more drinks for women. Alternative definition for binge is the consumption of 14 glasses of wine over the three days of weekend. The first half of the picture of increased risk for arrhythmic events associated with binge can be found in the above described acute effects of alcohol. The second half may come from the effects of withdrawal after episodes of binge. One suggestion in this regard comes from an experimental study in rats susceptible to isoproterenol-induced ventricular fibrillation [92]. Both fatal and non-fatal arrhythmias were significantly more frequent in the group exposed to alcohol withdrawal. Moreover, alcohol withdrawal produced a decrease in serum potassium level, one additional proarrhythmic mechanism. In another

External Triggering, Modifying and Chronobiologic Factors… 103
study, administration of adrenaline did not reduce the lowered electrical threshold for ventricular fibrillation in alcohol fed dogs, but did reduce that threshold in the group not-treated with alcohol [88]. This may suggest that recuperation of the previously occupied ß-receptors by alcohol with its withdrawal, coupled with lowered ventricular fibrillation threshold induced by alcohol consumption, could cause an exaggerated propensity for ventricular arrhythmia in the presence of catecholamine stimulation.
Altogether, above experimental evidence may explain which acute and chronic effects of alcohol as well as its withdrawal may play the role in facilitating arrhythmogenesis. Lastly, there is a great likelihood of situations with coexistence of external triggers of arrhythmia such as cigarette smoking, coffee, cocaine or marijuana use. Superimposition of their effects may contribute to the risk of an arrhythmic event, but verification of such a scenario is difficult in the clinical setting.
Results of the one case-crossover study show that intake of up to 5.5 international units of alcohol per drinking day elevated the relative risk of triggering sudden cardiac death during the first two hours after consumption [78]. Population subgroups at potentially greater risk of triggering included smokers, regular coffee drinkers, overweigh or obese and individuals under chronic psychosocial stress. Surprisingly, the relative risk correlated both with the level and with intensity of habitual physical activity. This directly opposes our comprehension of beneficial cardiovascular effects of regular and intense physical activity, including protective effect against external triggering [4,5], and warrants for a more thorough research of this apparent controversy [65].
Cocaine Cocaine (benzoylmethylecgonine) is an alkaloid extract from the leaf of the Erythroxylon
coca plant, and may be taken by smoking, nasal inhalation, or injection. The peak effect depends on the route of administration and ranges from 1 to 90 minute due to varying cocaine pharmacokinetics.
Cocaine has been implicated in causing a wide range of rhythm disturbances including sinus bradycardia and tachycardia, supraventricular arrhythmias, ventricular tachycardias, Torsades de Pointes and cardiac arrest [93-98]. However, definite causal relationship and clear triggering effect based on the controlled data, as it has been suggested for the myocardial infarction [99], has not been obtained. Pentel and his group [100], however, found no convincing effect of smoking multiple consecutive doses of cocaine on ventricular ectopy or ST-segment changes. Still, cocaine has a variety of theoretical proarrhythmic effects.
Cocaine is a sympathomimetic drug and agonist of α-1, ß-1 and ß-2 adrenergic receptors. It produces adrenergic stimulation by increasing the concentration of norepinephrine and dopamine at postsynaptic receptor sites. The effect is caused by blockade of presynaptic reuptake of these neurotransmitters. Cocaine may also enhance the catecholamine release from central and peripheral stores [101-103]. In addition, the potentiation of sympathetic effects results from the reduced vagal activity caused by cocaine [104,105]. Increased adrenergic stimulation induces increase in heart rate, blood pressure and left ventricular

Viktor Čulić 104
contractility, whereas vasoconstriction can occur in both stenotic and nonstenotic segments [106-108]. Thusly, proarrhythmic effects of cocaine are partly exerted by precipitating myocardial ischemia, or sometimes even myocardial infarction, in patients with coronary heart disease. Both myocardial ischemia and adrenergic stimulation substantially lower the threshold for ventricular fibrillation.
Cocaine has sodium channel antagonist properties [101,109]. Because of that, it prolongs the QTc interval which may predispose to polymorphous ventricular tachycardia, like Torsades de Pointes. In addition to moderate QTc prolongation, the repolarization changes observed after cocaine use include nonspecific ST-T segment abnormalities, T-wave amplitude decrease and U-wave amplitude increase [105,109,110]. Afterdepolarizations and triggered ventricular arrhythmias may be facilitated by increased intracellular calcium concentration, another effect of cocaine administration [111].
Both cocaine and methadone cause a significant increase in heart rate, and QTc prolongation, mostly without changing QRS duration [109,112,113]. Both of these drugs are blockers of delayed rectifier potassium channels. Their parallel use (which is a realistic scenario in addicts treated with methadone), may potentially multiply the risk for Torsades de Pointes. Another dangerous combination is the concomitant use of cocaine and alcohol. It has been estimated that this common way of abuse increase the risk of acute cardiac event by a factor 40, and the risk of sudden death by a factor 25 [114].
The expansion of cocaine use (nearly one million Americans have abused cocaine [115]) makes the importance of cocaine as a trigger of cardiovascular incidents permanently increasing. Mittleman and coworkers [99] have reported that the risk of onset of myocardial infarction was elevated 24 times over baseline in an hour after the use of cocaine. Regarding cardiac arrhythmias, the precise triggering features such as the risk elevation or susceptible population subgroups are not defined as yet. Keeping in mind that sudden cardiac death in young persons is sometimes linked to cocaine use, it raises the question whether cocaine requires previously vulnerable myocardium to induce arrhythmia, or superimposition of several triggers and modifying factors may be sufficient to initiate malignant arrhythmia.
Marijuana Marijuana is another abusive substance that has been linked to arrhythmia triggering. The
most common use of marijuana is smoking either the pure substance or mixed with tobacco leaves. Episodes of sinus tachycardia and ventricular ectopic beats have been linked with cannabis intake [116-122]. Only circumstantial evidence suggested that marijuana use may be a trigger of ventricular tachycardia or fibrillation causing sudden cardiac death. One case report described an episode of ventricular tachycardia with right bundle-branch block accompanied with very slow coronary blood flow (TIMI 1-2) in a 34-year old male several hours after a glass pipe marijuana smoking [123]. At first, tachycardia was inducible in the electrophysiologic laboratory, but after three days of cessation of marijuana and verapamil administration normal coronary flow was seen and no ventricular tachycardia was inducible on electrophysiologic testing.

External Triggering, Modifying and Chronobiologic Factors… 105
In an autopsy study from Norway, the only drug found in postmortem serum samples of six young adults with sudden death was the tetrahydrocannabinol, a marker of the very recent cannabis use [124]. In a 48-year old male patient who undergone coronary artery bypass graft surgery and had persisting stenotic coronary disease, ventricular fibrillation was documented shortly after smoking a marijuana cigarette [125].
The most convincing evidence for the triggering role of marijuana for acute cardiac events came from a case-crossover study by Mittleman et al. [126], who found 4.8 times increased risk of myocardial infarction within the first hour after the marijuana use as compared to periods of non-use.
The primary mechanisms by which the acute cannabis administration may induce coronary arrhythmias are the stimulation of ß-adrenergic receptors and possible blockade of the parasympathetic nervous system [117,120,127]. Furthermore, there is a possibility that cannabis enhances triggered activity in the Purkinje fibers. Another hypothetical mechanism is that cannabis use may affect coronary microcirculation, and induce vasoconstriction and ventricular arrhythmia in patients susceptible to developing myocardial ischemia. Myocardial ischemia may also be favored by increased carboxyhemoglobin levels and production of oxidant gases by marijuana smoking [119-122,125].
Air Pollutants The association between elevated air pollution and increased hospital admissions for
cardiovascular disease and increased cardiovascular mortality has clearly been established [128-130]. Short term increments in air pollutants have been linked to the triggering of onset of myocardial infarction [131-134] and hospitalizations for heart failure decompensation [135-137]. Both gaseous and particulate matter pollutants have been implicated in adverse cardiovascular effects. Gaseous pollutants like ozone, sulfur and nitrogen dioxide, and carbon monoxide are largely industrial and vehicle derived. Particulate matter is a complex mixture of various components including elemental and organic carbon compounds, transition metals, metal oxides, nitrates, sulfates and acid condensates. Among metallic compounds, iron, nickel, copper, zinc and vanadium are capable of causing pathophysiologic changes in living organisms [138-142].
It has been observed that hospital admissions for arrhythmia are 50% increased during the periods of smog than before and after such periods [143]. The most important investigation from the field of air pollution and arrhythmia occurrence, the one by Dockery et colleagues [144], reported on the nonsignificant increase in risk of ventricular tachycardia recorded by implanted cardioverter defibrillators associated with 2-day mean level of motor vehicle pollutants and fossil fuel combustion sources. However, significant associations between air pollution and ventricular arrhythmias were observed among patients whose arrhythmia occurred within the previous 3 days. Conclusion proposed by the authors is that pollutants such as fine particle mass, carbon monoxide, nitrogen dioxide, black carbon, sulfate and others may facilitate ventricular tachyarrhythmias in the presence of other precipitating factors. A case-crossover analysis of that data, which allow matching the time of arrhythmia event with pollutant concentrations, revealed a stronger significant connection

Viktor Čulić 106
between ventricular arrhythmia and mean particulate matter less than 2.5 µm in aerodynamic diameter and ozone in the 24 hours before the arrhythmic episodes [145].
An interesting study was conducted in the cars of nine healthy male US highway patrol troopers. In-vehicle particulate matter of diameter less than 2.5 μm was positively associated with ectopic beats, heart beat cycle length, and parameters of heart rate variability [146]. Another study strongly suggests the interplay among air pollutants and meteorologic condition in impact on ventricular arrhythmia [147]. In that study, the concentration of nitrogen dioxide and carbon monoxide on the same day showed positive associations with implanted cardioverter defibrillator discharge. Significance of such relationships disappeared after adjustment for meteorologic variables. Moreover, the level of particulate matter pollutants highly correlated with each other and with gaseous pollutants. Gaseous pollutants, on the other hand, even more closely correlated with each other.
In contrast to these observations, some investigations suggest that air pollution does not affect cardiovascular morbidity and mortality, including arrhythmias [148,149]. Perhaps, contradictory findings come from a number of methodological issues. One of the most important questions in analysis of the impact of air pollution on cardiac arrhythmia is to define the appropriate time and the lag between exposure and the event. Another important question is abovementioned complexity of interrelations among pollutants and weather variables. These interdependencies and separate effects of each and every environmental and atmospheric factor are going to be extremely difficult to distinguish and estimate. Conflicting results regarding the impact of air pollutants on cardiovascular incidents in the published studies could be partly due to the multiplicity of the studies' outcomes, the different types and levels of pollution and the general research methodologies. There are suggestions [150] that the difference between the pollutant concentration on the event day and the concentrations on the control days may be very small which seriously limits the statistical power and may influence the findings. Therefore, this difference, not the level, should likely be the exposure term for investigations the effects of air pollution. As to the design, another problem is the lack of appropriate statistical methodology to completely separate above described interdependencies between pollutants themselves, and their close correlations with meteorologic variables.
Current knowledge about processes that may link air pollution with ventricular arrhythmia is limited and the exact mechanisms of the association between air pollution and heart rhythm, processes of depolarization, repolarization and arrhythmogenesis are not clear. Figure 3 depicts acute pulmonary and cardiovascular responses to inhaled pollutants that may serve as mechanisms of increased risk of ventricular arrhythmia. Although further exploration is necessary, experimental studies set the stage for biologic plausibility of involvement of these processes in the triggering of arrhythmias. One of the proposed pathways is the alteration in autonomic nervous system produced by inhalation of pollutants which happens 1 to 4 hours after the exposure. The first step is initiation of oxidative stress directly or by creation of acute pulmonary inflammation mediated by cytokines. Direct stimulation of nasopharyngeal and airway receptors may be involved in autonomic effects. Irritation and inflammation of the airways can influence cardiovascular autonomic function [151-153]. Proinlammatory cytokines IL-1ß and TNF-α could affect action potentials and myocardial contractility [154-157] directly facilitating the cardiac arrhythmias [158]. The rapid decrease

External Triggering, Modifying and Chronobiologic Factors… 107
of heart rate variability and increase of heart rate representing decreased parasympathetic input to the heart correlates with the elevation of the particulate matter pollutants [129,130,159-162]. The patients with ischemic heart disease, diabetes or hypertension seem to be more susceptible to autonomic disturbance associated with air pollution [159].
Figure 3. Schematic diagram illustrating putative internal triggering mechanisms leading from inhalation of gaseous and particulate matter pollutants to acute cardiac events triangle. Air pollution can induce increase in all three components of vulnerability within several hours of exposure.

Viktor Čulić 108
An important factor associated with arrhythmia propensity is the repolarization abnormality. Electrocardiogram measures of such abnormalities represented by repolarization duration, morphology and variability strongly suggest an immediate effect of air pollution on myocardial vulnerability [128,130,163]. The T-wave alternans, a marker of myocardial vulnerability and electrical instability, increases in dogs with inhalation of residual oil fly ash [164]. Nonetheless, air pollution components probably act differently on the complex repolarization process.
The direct chemical effect of air pollutants on cardiac ion channels has been proposed as additional triggering mechanism for cardiac arrhythmia. Particle components may first enter the systemic circulation [165] and then reach the heart [166]. The chemical composition of particulate matter could be involved in direct cardiac toxicity through effect on the ions on the myocyte channels occurring within 4 hours of exposure [138]. Disturbed function of the ion channels and electrophysiological myocardial malfunction may be important promotors of arrhythmogenesis in the vulnerable myocardium.
All these findings suggest that inhaled particle affect the autonomic control of the cardiac electrophysiology and myocardial repolarization process. In addition, air pollution induces several pathophysiologic mechanisms that within the short term period can increase the risk of myocardial ischemia and acute coronary syndrome, and indirectly within the terms of acute cardiac event triangle, can increase the risk of arrhythmia and sudden cardiac death (figure 3). Several excellent reviews summarize putative pathophysiological mechanisms leading from exposure to air pollution to adverse acute and chronic cardiovascular effects [128-130]. Disturbed balance between sympathetic and parasympathetic system results in increased heart rate, blood pressure and enhanced myocardial contractility, processes that favor myocardial ischemia. Enhanced systemic inflammation has been linked to both progression and instabilization of atherosclerotic lesions, producing vulnerable coronary plaques. Nevertheless, the intensity of inflammatory processes has been proposed as an important independent marker of the future risk of a coronary event [167,168]. Airway inflammation induced by air pollution likely cause systemic hypercoagulability [169,170] and increased blood viscosity [171]. Increased plaque vulnerability, coupled with blood vulnerability significantly increase the propensity for an acute coronary syndrome [4,9,10]. Besides short-term increase in risk of acute cardiac events, including cardiac arrhythmias, systemic inflammation likely participate in long-term risk for respiratory and cardiovascular diseases.
Air pollution obviously can increase all three aspects of patient vulnerability: plaque, blood and myocardium. Particulate air pollutants are described in terms of aerodynamic size. Particles of aerodynamic diameter between 2.5 and 0.1 μm are called fine particulates, are sedimented out in the gas exchange lung regions and are linked to the majority of adverse cardiovascular effects of air pollution. Particles smaller than 0.1 μm in diameter are referred to as ultrafine. They are too small to sediment out in lungs during breathing. They are breath out without deposition or are deposited on alveolar walls by diffusion. Since ultrafine particles could hypothetically reach higher particle number concentration within pulmonary tissue than larger particles and are capable of carrying large concentrations of toxic air pollutants, it is now believed that ultrafine particles are at least partly responsible for cardiovascular effects otherwise attributed to larger particulate matter [128]. Further

External Triggering, Modifying and Chronobiologic Factors… 109
elucidation of aerodynamic properties and behavior of particles, depending on particle diameter, density and shape as well as the role of gaseous pollutants is necessary. However, mechanisms of increased risk as well as quantification of personal exposure and hazard for triggering arrhythmia by air pollution should also be better defined.
Meteorologic Factors A crucial question in examination of the relationship between weather and cardiovascular
diseases is whether exposure to meteorologic factors, or rather their influence on humans, differs between indoors and outdoors. Although it is clear that differences do exist, especially keeping in mind that there is an increasing amount of air conditioned spaces, it is now appreciated that such differences are not substantial [6,172-176]. Adaptation to atmospheric environment is one of the less well understood areas of human physiology because of a number of methodological issues similar to those considered with air pollution and interfering effects of other triggering and modifying factors. Few data, whether from human or animal models, can be found on association between arrhythmias and specific meteorologic parameters or about pathophysiologic changes that could explain causative relations between them. Thus, we are at the beginning of elucidation of popular wisdom often referred to as “it’s the weather” which sometimes may be apparent in the clinical settings.
The frequency of both single ventricular ectopic beats and ventricular tachyarrhythmia show a positive correlation with the atmospheric temperature within the positive range of temperature [6,27,177]. In animal models, exposure to high temperature is associated with dehydration, increased blood viscosity, endothelial damage, arterial hypotension and increased cardiac output [178]. There is an observation that below 0 degrees of Celsius the frequency of ventricular tachyarrhythmias also rises with the lowering temperature [177]. Cold exposure induces sympathetic activation, a typical sympathetic triggering pathway with its internal triggering mechanisms, similar to the one associated with triggers like physical or emotional stress [4-6]. These data suggest a V- or U-shaped relationship between atmospheric temperature and ventricular arrhythmias, where very cold and very hot conditions increase the risk, whereas temperatures around 0 degrees of Celsius seem to be less endangerous. One of the most contributing studies on the relationships between fatal and nonfatal coronary diseases, atmospheric temperature and temperature, The Lille – WHO MONICA Project [173], revealed that after adjustment for each other, both of these meteorologic variables correlated with cardiovascular event rates. More myocardial infarctions and cardiac deaths have been observed with decreasing temperature; a 10°C decrease in atmospheric pressure has been associated with an 11% increase in events rate. This effect has been more pronounced with advancing age.
Our work connected periods of higher atmospheric pressure with a greater likelihood of ventricular tachycardia in women [6] and with a greater likelihood of single ectopic beats in those under 65 [27]. Two studies offer information that may help explaining these findings. Increase in myocardial contractility, arterial pressure and oxygen consumption have been observed in rats exposed to elevated ambient pressure [179,180], whereas coronary blood flow has not been changing [179]. We also observed more ventricular tachycardia episodes

Viktor Čulić 110
[6] but not frequency of single ectopic beats [27] during lowering of barometric pressure. Independently of the influence of air pollutants, blood oxygen saturation seems to be highly positively related to current barometric pressure, while pulse rate seems to exhibit an inverse association to the pressure [181]. Lowering ambient pressure has also been linked to the increase of blood pressure and heart rate [182]. In the Lille – WHO MONICA Project [173], the effect of atmospheric pressure on the occurrence of myocardial infarction and coronary deaths was more pronounced in older population subgroups, and both increases and decreases in atmospheric pressure from 1016 milibars were associated with increases in the event rates.
We have described a greater frequency of ventricular arrhythmias during periods of increasing relative air moisture [6]. The only similar data can be found in one study investigating acute coronary syndromes in the greater Athens area, Greece, reporting a positive association of events with relative air moisture [183]. We speculated that increasing air moisture may burden adaptive cardiovascular mechanisms in patients with preexisting cardiac disease through impaired sweat evaporation and thermal regulation on the organism level [6].
The pioneer information has been provided on the association between wind and cardiac arrhythmias. Wind speed showed a U-shaped pattern of correlation with the frequency of ventricular tachycardia, with the lowest occurrence between three and nine meters per second [6], whereas with single ventricular ectopic beats wind speed displayed a positive linear correlation [27]. The recorded wind speeds were within the range from zero to 21 meters per second. Such an influence on ventricular tachycardia persisted to be significant after accounting for the triggering potential of physical and emotional stress, the rest of meteorologic variables and other modifying and chronic risk factors. Because of that, we proposed that, for more complex arrhythmic events, modest wind-mediated stimuli in the range from three to nine meters per second may have less adverse, or even beneficial effects. We have drawn the idea of the beneficial effect from the higher frequency of tachycardia episodes at lower wind speeds. On the contrary, strong winds increased likelihood of both ventricular extrasystolia and tachycardia. In a Switzerland study, heavy wind activity has been independently of other meteorologic variables linked to the daily hospitalization rates for acute myocardial infarction [184]. Biologic effects of such winds may partly be due to rapid perturbations in atmospheric pressure made by wind-induced turbulences [6,185]. Therefore, the wind may have more marked triggering potential than some other meteorologic variables.
Our group has also reported that southerly and southeasterly wind components are independently associated with the likelihood of ventricular tachycardia occurrence only in women [6]. Although it is difficult to provide plausible pathophysiologic explanation, perhaps other factors associated with winds of these directions, for example ionic components of such air masses, some unrecognized associated meteorologic influences or mood changes, mediate their adverse effects. It is interesting that the frequency of ventricular ectopic beats showed similar dependence on the wind direction in the univariate analysis, but was abolished when adjustments were made for other external triggering factors [27].
Findings on the atmospheric pressure and air moisture could be representative for the perception of the influence of weather variables on humans. It appears that in the presence of vulnerable myocardium, any change of homeostasis may act as a trigger of arrhythmic

External Triggering, Modifying and Chronobiologic Factors… 111
episode. The triggering potential is directly related to the trigger type or intensity of the change as well as to the vulnerability of the myocardium.
Ventricular ectopic beats are involved and sometimes are prerequisite for triggering malignant arrhythmia [1,186,187]. A particular caution and a distinction must be made for the runs of 2 or more consecutive ventricular depolarizations during exercise or at recovery which is consistent with an increase in long-term cardiovascular mortality [188,189]. However, in all population subgroups, circadian variation of ventricular ectopic beats seems not to be altered by external triggers [27]. This could represent an independent baseline rhythm of benign ectopy associated with daily variation in sympathetic activity. Data obtained on the differences between triggering of ventricular ectopic beats [27] and ventricular tachycardia [6] by meteorologic and other triggers are indicative of complexity of the genesis of malignant cardiac arrhythmia. The main message is that greater number of single ectopic beats does not linearly increase the likelihood of malignant arrhythmia and that occurrence of the latter is driven by more complex mechanisms.
The occurrence of ventricular ectopic beats during exercise in apparently healthy individuals is considered to be a normal response to such activity and has not been linked to the increase in cardiovascular mortality [190-193]. It is consistent with our finding of a greater association of single ventricular ectopic beats [27] but not ventricular tachycardia [6] in younger individuals in response to physical activity and meteorologic changes. In this population, such a response likely represents a normal reactivity to surrounding circumstances and good adaptive ability. In contrast, physical activity and meteorologic variables have less significant impact on ectopic beats in elderly patients. One may expect that persistently increased sympathetic tone, accompanying comorbidities such as essential arterial hypertension or heart failure which is more often in the elderly, reduce the extent of response to external stimuli.
Meteorologic influences may be considered the “second order” triggers because events like emotional or physical stress are surely much more powerful with more intense and concentrated effect. Above all, separate influences and interactions between specific air pollutants and meteorologic parameters are very difficult to distinguish and to explore. This is probably the main reason for conflicting data from the studies of impact of these environmental factors on cardiovascular health. It is to be noted that a number of studies observed no association between meteorologic variables and cardiovascular diseases including arrhythmias. As discussed above with methodological problems in investigation of the influence of air pollution, the same applies to the meteorologic variables. The important issue is to define the appropriate exposure terms as well as the time and leg between exposure and the event. The nature of impact of meteorologic factors is likely more acute and thereby likely more significant for cardiac arrhythmias than is the impact of air pollutants.
Modifying Factors The term chronic risk factors [4-6] is used for the traditional well-known risk factors
(diabetes, smoking, hypertension, hyperlipidemia, etc.) for cardiovascular diseases in order to describe their long-time action required to produce morphological changes on cardiovascular

Viktor Čulić 112
system. In the same time, this emphasizes the distinction from the short-time effect of external triggers. In these relations, modifying factors would be variables other than typical chronic risk factors which may change the individual susceptibility to an acute cardiac event or to a particular external trigger. The effect of modifying factors is not as sudden and intense as the effect of external triggers, it is usually reversible and transient, but more lasting in comparison to external triggers. In comparison to chronic risk factors, modifying factors usually are not directly involved in the development of irreversible pathomorphologic changes of the heart and cardiovascular system. However, modifying factors through the influence on biochemical, pathophysiologic or electrophysiologic processes may increase myocardial vulnerability without changing the condition of the heart disease.
Gender Gender is an irreversible and unchangeable factor, and as such, it seemingly must be
defined as chronic risk factor. However, since its influence is mediated through hormones, whose levels significantly change during the life span, in women even on the monthly basis, the gender may be even more accurately defined as modifying factor in terms of arrhythmogenesis. Moreover, due to hormone changes over the time, the age may also be considered a modifying variable.
The mechanisms underlaying gender-specific differences in arrhythmogenesis are still largely unknown. The “gender gap” consists of a clear male predominance in idiopathic ventricular fibrillation in symptomatic cases of Brugada syndrome, in contrast to higher incidence of atrioventricular nodal reentrant tachycardias [194,195] and perhaps a lower incidence of sudden cardiac death independent of the coronary disease in women [196]. The triggers of the repetitive monomorphic ventricular tachycardia, originating from the right ventricular outflow tract seems to vary according to gender as well [62]. In men, tachycardia is more likely to occur, in about 90% of cases, in association with typical sympathetic triggers such as exercise, caffeine or other stressful events. In women, the onset seems to be related to the hormonal status, with a greater susceptibility primarily during the menses, but also in the premenstrual phase or during markedly irregular cycle.
Among patients with long QT syndrome, regression of phenotypic manifestations, including the QT and QTc duration, and the risk of Torsades de Pointes, occurs in affected males, but not in affected females after puberty [197-201]. The heart contains receptors for both androgens and estrogens and their influence may contribute to the “gender gap”. On the one hand, estrogen exerts cardioprotective sympatholytic and vagotonic effects [202,203]. Favorable effects may include increased heart rate variability and baroreceptor sensitivity [204,205] and lowered blood pressure and heart rate [204,206]. In contrast, estrogen may favor QT prolongation, adverse effects on ventricular repolarization, and vulnerability to arrhythmia independently of autonomic influences [207,208]. Furthermore, estrogens could inhibit calcium uptake in myocytes [209] or increase sensitivity to circulating cathecolamines, for example during pregnancy [210]. Progesterone, however, may contrast favorable cardiovascular effects of estrogen [211], while androgens may prevent QT prolongation in adult males [212]. Sex hormones may also underlay gender differences in the

External Triggering, Modifying and Chronobiologic Factors… 113
density and distribution of various ion channels in myocytes of the ventricular endocardium, epicardium and M cells [213].
Detailed mechanisms linking sex hormones and arrhythmias warrant further exploration. Putative mechanisms may include direct hormonal effects on myocytes, hormonal impact on autonomic tone, and impact on the various ion channels expression. It remains to be seen whether the suggested susceptibility for triggering the events by emotional stress in women and physical activity in men really exists, or some behavioral differences or differences in confounding factors play the role. The fact that Monday increase in cardiovascular events is larger in men raises questions about such a susceptibility and other gender-specific triggering and modifying factors.
Psychosocial Factors A large body of evidence attests to the impact of chronic emotional stress and
psychological factors in the etiology of cardiovascular diseases. In long-time perspective, and in addition to the numerous proatherogenic effects, depression and anxiety have several adverse pathophysiological effects on arrhythmogenesis. Patients with anxiety, depression and related syndromes have reduced heart rate variability and impaired vagal control [214-217]. Such alterations in autonomic tone increase the overall susceptibility to ventricular tachyarrhythmias. Psychosocial factors have been suspected to lower the thresholds for ventricular arrhythmia and sudden cardiac death [218]. In men, anxiety has been associated with the occurrence of sudden cardiac death in a dose dependent manner, but has not been associated with the occurrence of myocardial infarction [219,220]. In women, prospective data suggest that high levels of phobic anxiety at least partially increase the risk of fatal coronary heart disease, particularly from sudden cardiac death [221].
Two types of personality, type A and type D, continue to receive attention considering their influence on atherosclerosis and coronary disease. Although type A behavior pattern, a syndrome characterized by competition, hostility, and exaggerated commitment to work, receives great interest, no firm evidence of correlation between this type of behavior and the risk of coronary artery disease has been established [222]. However, recent evidence suggests that type D personality could be an independent predictor of cardiac events [223]. Coronary patients with this type of personality report high levels of emotional stress, chronic tension and anger, a low level of subjective well-being, pessimism, negative affection, and low level of perceived social support.
Therefore, depressed and anxious patients, and perhaps those with type A or type D personality could be generally more subjected to arrhythmogenic potential of external triggers. Still, there is a question to what extent the effect of psychosocial factors can be separated from accompanying unhealthy lifestyle habits, some of which may also serve as external triggers, for example smoking, drug or alcohol abuse. While psychosocial factors could be involved in weekly variation in arrhythmia occurrence, their contribution to seasonal variation is held to be rather important.

Viktor Čulić 114
Polyunsaturated Fatty Acids Some 30 years ago, it was suggested that fish oil fatty acids might prevent fatal
arrhythmia in humans [224]. There is accumulating clinical evidence supporting this notion [225-227]. The observed reduction of relative risk for sudden cardiac death associated with n-3 polyunsaturated fatty acids was between 20% and 80%. This seems to be the major beneficial cardiovascular effect since no reduction in nonfatal myocardial infarction was observed in the trials. Although not all studies dealing with this issue have been able to demonstrate antiarrhythmic properties associated with fish oils, the evidence was rather suggestive and in 2003, the European Society of Cardiology published guidelines that recommended inclusion of fish oils as standard therapy for postinfarction management [228]. Proposed mechanism of beneficial effect includes the modulation of conductance of myocyte ion channels. The most affected would be the fast, voltage dependent sodium current and the L-type calcium current [229,230] leading to the electrical stabilization of the myocytes and reduction of the myocardial vulnerability.
Medication A number of cardiovascular and other drugs, especially antiarrhythmics, can be
considered modifying factors. Detailed description of their mechanisms of action can be found in other chapters of this book and elsewhere. Herein, only few of them for whom the evidence of impact on the process of triggering or the influence on chronobiologic rhythms exists will be briefly mentioned.
The most important are ß-adrenergic receptor antagonists, characterized as class II in the Vaughan Williams classifications of antiarrhythmic agents. Their ability to protect from triggering by emotional stress, physical activity or meteorologic stress, as well as the association with abolition of morning and Monday peaks of arrhythmic episodes are described in the appropriate parts of this chapter. Such a protection is most probably the result of blockade of several internal triggering mechanisms of the sympathetic triggering pathway.
There is a body of evidence suggesting adverse effect of digoxine in women. In addition to an increased risk of death among women but not men with heart failure [231], we observed that in general population digoxine therapy increases the likelihood of episodes of ventricular tachycardia only in women, particularly during the daytime [6]. Although there are indications that interaction between digoxin and female hormones or hormone replacement therapy may underlay adverse cardiovascular effect [232], the mechanisms of such an interaction cannot be identified.
Finally, intriguing data opens the possibility that statins [233] and anxiolytics [6] may act as antiarrhythmic modifying factors but further exploration of such observations is necessary.

External Triggering, Modifying and Chronobiologic Factors… 115
Chronobiologic Rhythms
The moment of initiation of cardiac arrhythmias is subjected to chronobiologic variations of cardiovascular diseases. One of the most interesting facts of the chronobiology of cardiac arrhythmias and other acute events is that despite of all the external triggering situations and environmental influences these patterns do exist. Chronic risk factors, congenital and acquired abnormalities underly vulnerable myocardium. The vulnerability continuously fluctuates and changes the susceptibility to arrhythmia. This could mean that susceptibility to external triggers fluctuates accordingly. It is very likely that interrelations among various external triggering situations and modifying factors determine temporal patterns of arrhythmia occurrence (figure 2). Unraveling the endogenous and exogenous factors underlaying chronobiologic phenomena may help understanding additional mechanisms of arrhythmogenesis.
Circadian Variation Most of acute cardiovascular diseases show variation in their occurrences throughout the
day. Cardiac arrhythmias also display a typical pattern of morning peak and nighttime trough [234-237]. Although it is more evenly distributed over the course of a day than ventricular arrhythmias, asystole also occurs less often during the night [238]. The two exceptions among arrhythmias regarding the circadian distribution are the Brugada syndrome [239] and paroxysmal atrial fibrillation [240,241], both having a primary peak at night.
Circadian pattern of ventricular arrhythmia likely has its background in the interplay among physiological, biochemical and genetic factors. The circadian variation in myocardial electrophysiology and vulnerability has chiefly been attributed to the pathophysiologic consequences of the autonomic nervous system activity. The variation in sympathetic activity underlays morning increase in catecholamine levels, blood pressure, platelet aggregability and diurnal variation in endothelial function. These changes are consistent with the typical sympathetic triggering pathway of facilitation of acute cardiac event triangle, depicted in figure 1. Probably because of that, ß-blockade is important in suppression of the morning peak of malignant arrhythmia [242] and sudden cardiac death [243].
Electrophysiologic parameters of ventricular action potential duration and repolarization follow circadian variation and confirm morning susceptibility to arrhythmias. The QT interval has been found to exhibit such a variation with a shorter corrected QT interval during waking hours that during sleep [244-246]. The dispersion of the corrected QT intervals is greater during daytime than during sleep [244,247]. Ventricular refractoriness is shorter during daytime and longest during the night when patients are asleep [244,248-250]. In electrophysiologic terms, this may explain why the initiation of reentrant circuits within the injured or otherwise vulnerable myocardium and facilitation of arrhythmias follow the typical circadian pattern in susceptible patients.
Another data provides additional insight into the circadian variation of biological and electrophysiologic behavior of the myocardium. The expression of many genes, including the clock genes, varies during the 24-hours. Variation in the expression of cardiac L-type

Viktor Čulić 116
calcium, and especially potassium channels, may contribute to the temporal variation in ventricular arrhythmias. In rat model, it has been observed that, among all the cardiac potassium channels, those termed Kv1.5 and Kv4.2 exhibit significant circadian variation [251]. Daily expression of these two channel types is reverse to each other, both of them seem to be subjected to light stimulation, and Kv1.5 may be partially affected by the ß-adrenergic activity. This opens a wide new area of possible research of the arrhythmogenesis.
Weekly Variation
Recent meta-analysis [252] has shown that cardiovascular events are slightly more
frequent on Mondays than on other days of week. One of every 100 events is attributed to this excess and effect is more pronounced in men. Several studies, including those with patients with implantable cardioverter-defibrillators, have confirmed the same pattern for ventricular arrhythmia [253-255]. It was observed that the Monday peak is not present in those receiving ß-adrenergic blockers, the similar effect as noted for the circadian variation [255]. This may point toward the role of sympathetic nervous system and cathecolamines, but the caution in interpretation and linking of these phenomena has been deployed [255].
Although several mechanisms for weekly variation have been proposed, there are uncertainties about their plausibility. It has been suggested that Monday peak implies a relationship with the workweek-associated stress [252,255]. Results of the study by Peters et al [254] revealed that the circadian variation in implanted cardioverter defibrillators is similar for each day of the week. The authors proposed that lack of difference in variations between weekend and weekdays suggest that underlying mechanisms for daily and weekly pattern may be different and likely unrelated to the standard workweek.
In addition to work-related stress, the majority of investigators propose the alcohol consumption (binge drinking in particular) as the second underlying mechanisms. However, since alcohol intake peaks on Fridays and Saturdays, there is a one-to-two day distance period from the Monday peak of events. Hypothetical link bridging this time gap is the destabilization of coronary disease that may be related to disturbed metabolism of proinflammatory cytokines and increased T-helper 1 lymphocyte activity as a result of increased alcohol intake [256]. Such changes, through activated inflammatory and autoagressive processes, could increase the myocardial vulnerability or may precipitate acute coronary event leading to acute cardiac event triangle. Further possible explanation is the habitual coffee intake. It may be hypothesized that the first day of the work week and “getting ready” for the job, usually starts with a relative excess in coffee after the weekend decrease in consumption. The assumed relative decrease in tolerance could result in more intense reaction, consistent with the sympathetic triggering pathway, to next stronger coffee consumption on Monday [80].
Seasonal Variation Cardiovascular events generally occur more frequently in the winter months compared to
other seasons. Several studies have shown this phenomenon for ventricular arrhythmias

External Triggering, Modifying and Chronobiologic Factors… 117
[257,258], and a study from Switzerland [259] revealed winter and spring exacerbation of ventricular electrical instability demonstrated by increased frequency of arrhythmia clusters and electrical storms in patients with implanted cardioverter-defibrillators.
As in cases of other two chronobiologic phenomena, one possibility is that exposure to triggers vary over the course of year. This may be assumed primarily for both groups of environmental triggers - for meteorologic stress and for air pollution. Cold exposure is the primary meteorologic trigger associated with the winter time provoking sympathetic triggering pattern of arrhythmic events. Seasonal variation in air pollution may also in part contribute to the phenomenon. It has been suggested that particulate matter pollutants from fall and winter are the strongest stimulators of proinflammatory processes. This has been shown by production of reactive oxygen species and interleukine release in normal human bronchial epithel cells and alveolar macrophages [260].
In contrast to environmental triggers, physical activity seems not to be involved, since average physical activity is significantly reduced during winter [261,262]. Nevertheless, emotional stress may be further contributor to the increased winter cardiovascular hazard. First because there is an association between the physical activity, positive affection and general well-being while there is an inverse relation with depression, anxiety and negative affection [263-265]. Shorter daylight periods, more clouds, rain and snowfalls probably contribute to this phenomenon called “seasonality” [266-268]. Seasonality also includes changes in appetite, food and nutritional habits which may underly the higher cholesterol levels during winter [266]. Altogether, mood disturbances, less light and other seasonal factors may through hormonal, metabolic or hemodynamic changes affect cardiac electrophysiology and increase myocardial vulnerability in susceptible patients. Some investigators postulated an annual cycle of adrenal and thyroid functions [269]. Others found a higher blood pressure, urinary sodium, and norepinephrine excretion and plasma concentration in patients with essential hypertension during winter and suggested that this may be a physiological response to cold environment [270]. However, all putative explanations require further studies.
Conclusions Cardiovascular responses to daily events and ambient changes do not occur in isolation
from other body systems. Among the systems that significantly contribute to that response, nervous system takes the leading position. Pathophysiologic consequences of exposure to a variety of triggers include the sympathetic arousal. However, this may create an environment of increased risk of acute cardiac event triangle including acute coronary syndromes, cardiac arrhythmias and sudden cardiac death. Whether some external event will act as the actual arrhythmia trigger, to a major extent depends on the condition of ventricular myocardium.
The simple cardiac rhythm disturbances, primarily ventricular ectopic beats, do not always trigger more complex or fatal arrhythmias and often represent a “side effect” of adaptation to the change of homeostasis. There is no linear relationship among single ectopic beats, non-sustained ventricular tachycardia, sustained ventricular tachycardia, and ventricular fibrillation. Sometimes it is difficult to define the nature of the arrhythmia and to

Viktor Čulić 118
decide whether it represents relative benign sign of electrical instability and ventricular dysfunction. Nonetheless, in patients with ischemic heart disease or heart failure, any ventricular rhythm disturbance suggests an adverse prognosis.
Considering external triggering, it is likely that the importance of superimposition of triggers is still underappreciated. In everyday life, there is a possibility of creation of triggering circulus viciosus which may underly a number of unexplained sudden cardiac deaths, particularly in young, apparently healthy people. An anecdotal example could be a young hypertonic and hypercholesterolemic manager, smoking and drinking alcohol or coffee in the state of emotional stress on the day when atmospheric pressure is falling and air pollution is elevated. Susceptible population may highly benefits from the future advances in early recognition and treatment of myocardial vulnerability and our ability to sever the link between vulnerable myocardium, arrhythmia initiation and fatal consequence.
There are several priorities for both clinical approach and further research. They can be arranged in four levels. The first level is to find and to eliminate, if possible, morphological substrate for ventricular arrhythmias by surgical, invasive or other procedures. Second is to find ways to reduce myocardial vulnerability by means of finding and developing protective modifying factors. Third is to block pathophysiologic mechanisms of inasmuch possible external triggers as possible by appropriate antiarrhythmic therapy. Fourth is to reduce the risk of arrhythmia by avoiding exposure to external triggers, especially their superimposition, when possible.
We can now be sure that external events can trigger cardiac arrhythmia and that there are factors that may influence the process and the risk of such triggering. We need more detailed understanding of the exogenous triggers, modifying factors and chronobiologic variations of cardiac arrhythmias at all the relevant levels. The final goal should be an integrated approach aiming to unravel the sequence of events from the human environment, through pathophysiologic mechanisms down to the subcellular and genetic level leading to improved strategies to prevent such a potentially catastrophic event.
References
[1] Zipes DP, Wellens HJ. Sudden cardiac death. Circulation. 1998;98:2334–51. [2] Myerburg RJ, Kessler KM, Castellanos A. Sudden cardiac death: structure, function,
and time-dependence of risk. Circulation. 1992;85:I2–10. [3] Bayes de Luna A, Coumel P, Leclercq JF. Ambulatory sudden cardiac death:
mechanisms of production of fatal arrhythmia on the basis of data from 157 cases. Am. Heart J. 1989;117:151–9.
[4] Čulić V. Acute risk factors for myocardial infarction. Int. J. Cardiol. 2007;117:260–9.
[5] Čulić V, Eterović D, Mirić D. Meta-analysis of possible external triggers of acute myocardial infarction. Int. J. Cardiol. 2005;99:1–8.
[6] Čulić V, Eterović D, Mirić D, Giunio L, Lukin A, Fabijanić D. Triggering of ventricular tachycardia by meteorologic and emotional stress: protective effect of ß-blockers and anxiolytics in men and elderly. Am. J. Epidemiol. 2004;160:1047–58.

External Triggering, Modifying and Chronobiologic Factors… 119
[7] Du X-J, Dart AM. Role of sympathoadrenergic mechanisms in arrhythmogenesis. Cardiovasc. Res. 1999;43:832–4.
[8] Pozzati A, Pancaldi LG, Di Pasquale G, Pinelli G, Bugiardini R. Transient sympathovagal imbalance triggers "ischemic" sudden death in patients undergoing electrocardiographic Holter monitoring. J. Am. Coll. Cardiol. 1996;27:847–52.
[9] Naghavi M, Libby P, Falk E, Casscells W, Litovsky S, Rumberger J, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part I. Circulation. 2003;108:1664–72.
[10] Naghavi M, Libby P, Falk E, Casscells W, Litovsky S, Rumberger J, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part II. Circulation. 2003;108:1772–8.
[11] Verrier RL, Hagestad EL, Lown B. Delayed myocardial ischemia induced by anger. Circulation. 1987;75:249–54.
[12] Verrier RL, Lown B. Behavioral stress and cardiac arrhythmias. Annu. Rev. Physiol. 1984;46:155–76.
[13] Rosenbaum DS, Jackson LE, Smith JM, Garan H, Ruskin JN, Cohen RJ. Electrical alternans and vulnerability to ventricular arrhythmias. N. Engl. J. Med. 1994;330:235–41.
[14] Adam DR, Smith JM, Akselrod S, Nyberg S, Powell AO, Cohen RJ. Fluctuations in T-wave morphology and susceptibility to ventricular fibrillation. J. Electrocardiol. 1984;17:209–18.
[15] Kop WJ, Krantz DS, Nearing BD, Gottdiener JS, Quigley JF, O’Callahan M, DelNegro AA, Friehling TD, Karasik P, Suchday S, Levine J, Verrier RL. Effects of acute mental stress and exercise on T-wave alternans in patients with implantable cardioverter defibrillators and controls. Circulation. 2004;109:1864–9.
[16] Nearing BD, Verrier RL. Modified moving average analysis of T-wave alternans to predict ventricular fibrillation with high accuracy. J. Appl. Physiol. 2002;92:541–9.
[17] Verrier RL, Nearing BD. Electrophysiologic basis for T wave alternans as an index of vulnerability to ventricular fibrillation. J. Cardiovasc. Electrophysiol. 1994;5:445–61.
[18] Quigley JF, Kop WJ, Rubenstein AH. Stress-induced QT variability in ICD patients. (abstract). Pacing Clin. Electrophysiol. 2001;24:621.
[19] Zareba W, Bayes de Luna A. QT dynamics and variability. Ann. Noninvasive. Electrocardiol. 2005;10:256–62.
[20] Haigney MC, Zareba W, Gentlesk PJ, Goldstein RE, Illovsky M, Mc Nitt S, Andrews ML, Moss AJ, for the Multicenter Automatic Defibrillator Implantation Trial II investigators. QT interval variability and spontaneous ventricular tachycardia or fibrillation in the Multicenter Automatic Defibrillator Implantation Trial (MADIT) II patients. J. Am. Coll. Cardiol. 2004;44:1481–7.
[21] Lampert R, Jain D, Burg MM, Batsford WP, McPherson CA. Destabilizing effects of mental stress on ventricular arrhythmias in patients with implantable cardioverterdefibrillators. Circulation. 2000;101:158–64.

Viktor Čulić 120
[22] Carpeggiani C, Landisman C, Montaron MF, Skinner JE. Cryoblockade in limbic brain (amygdala) prevents or delays ventricular fibrillation after coronary artery occlusion in psychologically stressed pigs. Circ. Res. 1992;70:600–6.
[23] Reich P, DeSilva RA, Lown B, et al. Acute psychological disturbances preceding life-threatening ventricular arrhythmias. JAMA. 1981;246:233–5.
[24] Tavazzi L, Zotti AM, Rondanelli R. The role of psychologic stress in the genesis of lethal arrhythmias. Eur. Heart J. 1986;7 (Suppl A):99–106.
[25] Rissanen V, Romo M, Siltanen P. Premonitory symptoms and stress factors preceding sudden death from ischaemic heart disease. Acta Med. Scand. 1978;204:389-96.
[26] Engel GL. Sudden and rapid death during psychological stress. Ann. Intern. Med. 1971;74:771–82.
[27] Čulić V, Silić N, Mirić D. Triggering of ventricular ectopic beats by emotional, physical and meteorologic stress: role of age, sex, medications, and chronic risk factors. Croat. Med. J. 2005;46:894–906.
[28] Fries R, Konig J, Schafers HJ, Bohm M. Triggering effect of physical and mental stress on spontaneous ventricular tachyarrhythmias in patients with implantable cardioverter-defibrillators. Clin. Cardiol. 2002;25:474–8.
[29] Lampert R, Joska T, Burg MM, Batsford WP, McPherson CA, Jain D. Emotional and physical precipitants of ventricular arrhythmia. Circulation. 2002;106:1800–5.
[30] Paavonen KJ, Swan H, Piipppo K, Hokkanen L, Laitinen P, Viitasalo M, Toivonen L, Kontula K. Response of the QT interval to mental and physical stress in types LQT1 and LQT2 of the long QT syndrome. Heart. 2001;86:39–44.
[31] Lindinger MI. Potassium regulation during exercise and recovery in humans: implications for skeletal and cardiac muscle. J. Mol. Cell. Cardiol. 1995;27:1011–22.
[32] Goldberg AD, Becker LC, Bonsall R, Cohen JD, Ketterer MW, Kaufmann PG, Krantz DS, Light KC, McMahon RP, Noreuil T, Pepine CJ, Raczynski J, Stone PH, Strother D, Taylor H, Sheps DS. Ischemic, hemodynamic, and neurohormonal responses to mental and exercise stress. Experience from the Psychophysiological Investigations of Myocardial Ischemia Study (PIMI). Circulation. 1996;94:2402–9.
[33] Lee S, Harris ND, Robinson RT, Yeoh L, Macdonald IA, Heller SR. Effects of adrenaline and potassium on QTc interval and QT dispersion in man. Eur. J. Clin. Invest. 2003;33:93–8.
[34] Darbar D, Smith M, Morike K, Roden DM. Epinephrine-induced changes in serum potassium and cardiac repolarization and effects of pretreatment with propranolol and diltiazem. Am. J. Cardiol. 1996;77:1351–5.
[35] Hansen O, Johansson BW, Gullberg B. Metabolic, hemodynamic, and electrocardiographic responses to increased circulating adrenaline: effects of pretreatment with class 1 antiarrhythmics. Angiology. 1991;42:990–1001.
[36] Struthers AD, Reid JL, Whitesmith R, Rodger JC. Effect of intravenous adrenaline on electrocardiogram, blood pressure, and serum potassium. Br. Heart J. 1983;49:90–3.
[37] Brown MJ, Brown DC, Murphy MB. Hypokalemia from beta2-receptor stimulation by circulating epinephrine. N. Engl. J. Med. 1983;309:1414–9.

External Triggering, Modifying and Chronobiologic Factors… 121
[38] Editorial. Adrenaline and potassium: everything in flux. Lancet. 1983;2:1401–3. [39] Friedensohn A, Faibel HE, Bairey O, Goldbourt U, Schlesinger Z. Malignant
arrhythmias in relation to values of serum potassium in patients with acute myocardial infarction. Int. J. Cardiol. 1991;32:331–-8.
[40] Nordregaug JE, von der Lippe G. Serum potassium concentrations are inversely related to ventricular, but not to atrial, arrhythmias in acute myocardial infarction. Eur. Heart J. 1986;7:204–9.
[41] Nordregaug JE, Johannessen KA von der Lippe G. Serum potassium concentration as a risk factor of ventricular arrhythmias early in acute myocardial infarction. Circulation. 1985;71:645–9.
[42] Johansson BW, Dziamski R. Malignant arrhythmias in acute myocardial infarction. Relationship to serum potassium and effect of selective and non-selective beta-blockade. Drugs. 1984;28 Suppl 1:77–85.
[43] Clutter WE, Bier DM, Shah SD, Cryer PE. Epinephrine plasma metabolic clearance rates and physiologic thresholds for metabolic and hemodynamic actions in man. J. Clin. Invest. 1980;6:94–101.
[44] Silverberg AB, Shah SD, Haymond MW, Cryer PE. Norepinephrine: hormone and neurotransmitter in man. Am. J. Physiol. 1978;234:E252–6.
[45] Mittleman MA, Maclure M, Sherwood JB, Mulry RP, Tofler GH, Jacobs SC, Friedman R, Benson H, Muller JE, for the Determinants of Myocardial Infarction Onset Study Investigators. Triggering of acute myocardial infarction onset by episodes of anger. Circulation. 1995;92:1720–5.
[46] Čulić V, Eterović D, Mirić D, Rumboldt Z, Hozo I. Gender differences in triggering of acute myocardial infarction. Am. J. Cardiol. 2000;85:753–6.
[47] Mirić D, Eterović D, Giunio L, Dujić Ž, Fabijanić D, Hozo I, Kuzmanić A, Božić I, Čulić V. Triggers of acute myocardial infarction regarding its site. Int. J. Cardiol. 1997;60:67–71.
[48] Čulić V, Mirić D, Eterović D. Different circumstances, timing, and symptom presentation at onset of Q wave versus non-Q wave acute myocardial infarction. Am. J. Cardiol. 2002;89:456–60.
[49] Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review. Eur. Heart J. 2006;27:1523–9.
[50] Sharkey SW, Lesser JR, Zenovich AG, Maron MS, Lindberg J, Longe TF, Maron BJ. Acute and reversible cardiomyopathy provoked by stress in women from the United States. Circulation. 2005;111:472–4.
[51] Wittstein IS, Thiemann DR, Lima JA, Baughman KL, Schulman SP, Gerstenblith G, Wu KC, Rade JJ, Bivalacqua TJ, Champion HC. Neurohumoral features of myocardial stunning due to sudden emotional stress. N. Engl. J. Med. 2005;352:539–48.
[52] Čulić V. Apical ballooning syndrome, emotional stress and women. Eur. Heart J. 2006;27:2907–8.

Viktor Čulić 122
[53] Willich SN, Lewis M, Löwel H, Arntz H, Schubert F, Schroder R, for the Triggers and Mechanisms of Myocardial Infarction Study Group. Physical exertion as a trigger of acute myocardial infarction. N. Engl. J. Med. 1993;329:1684–90.
[54] Mittleman MA, Maclure M, Tofler GH, Sherwood JB, Goldber RJ, Muller JE, for the Determinants of Myocardial Infarction Onset Study Investigators. Triggering of acute myocardial infarction by heavy physical exertion. Protection against triggering by regular exertion. N. Engl. J. Med. 1993;329:1677–83.
[55] Ikeda T, Saito H, Tanno K, Shimizu H, Watanabe J, Ohnishi Y, Kasamaki Y, Ozawa Y. T-wave alternans as a predictor for sudden cardiac death after myocardial infarction. Am. J. Cardiol. 2002;89:79–82.
[56] Klingenheben T, Zabel M, D’Agostino RB, Cohen RJ, Hohnloser SH. Predictive value of T-wave alternans for arrhythmic events in patients with congestive heart failure. Lancet 2000;356:651–2.
[57] Gold MR, Bloomfield DM, Anderson KP, El-Sherif NE, Wilber DJ, Groh WJ, Estes NA 3rd, Kaufman ES, Greenberg ML, Rosenbaum DS. A comparison of T-wave alternans, signal averaged electrocardiography and programmed ventricular stimulation for arrhythmia risk stratification. J. Am. Coll. Cardiol. 2000;36:2247–53.
[58] Schwartz PJ, Priori SG, Spazzolini C, Moss AJ, Vincent GM, Napolitano C, Denjoy I, Guicheney P, Breithardt G, Keating MT, Towbin JA, Beggs AH, Brink P, Wilde AAM, Toivonen L, Zareba W, Robinson JL, Timothy KW, Corfield V, Wattanasirichaigoon D, Corbett C, Haverkamp W, Schulze-Bahr E, Lehmann MH, Schwartz K, Coumel P, Bloise R. Genotype-phenotype correlation in the long-QT syndrome: gene-specific triggers for life-threatening arrhythmias. Circulation. 2001;103:89–95.
[59] Callans DJ, Menz V, Schwartzman D, Gottlieb CD, Marchlinski FE. Repetitive monomorphic tachycardia from the left ventricular outflow tract: electrocardiographic patterns consistent with a left ventricular site of origin. J. Am. Coll. Cardiol. 1997;29:1023–7.
[60] Movsowitz C, Schwartzman D, Callans DJ, Preminger M, Zado ES, Gottlieb CD, Marchlinski FE. Idiopathic right ventricular outflow tract tachycardia: narrowing the anatomic location for successful ablation. Am. Heart J. 1996;131:930–6.
[61] Grimm W, List-Hellwig E, Hoffmann J, Menz V, Hahn-Rinn R, Klose KJ, Maisch B. Magnetic resonance imaging and signal-averaged electrocardiography in patients with repetitive monomorphic ventricular tachycardia and otherwise normal electrocardiogram. Pacing Clin. Electrophysiol. 1997;20:1826–33.
[62] Marchlinski FE, Deely MP, Zado ES. Sex-specific triggers for right ventricular outflow tract tachycardia. Am. Heart J. 2000;139:1009–13.
[63] Happonen P, Voutilainen S, Salonen JT. Coffee drinking is dosedependently related to the risk of acute coronary events in middle-aged men. J. Nutr. 2004;134:2381–6.
[64] Panagiotakos DB, Pitsavos C, Chrysohoou C, Kokkinos P, Toutouzas P, Stefanadis C. The J-shaped effect of coffee consumption on the risk of developing acute coronary syndromes: the CARDIO2000 case-control study. J. Nutr. 2003;133:3228–32.

External Triggering, Modifying and Chronobiologic Factors… 123
[65] Čulić V. Triggering of sudden cardiac events by coffee and alcohol consumption: what do we know? Croat. Med. J. 2005;46:150–1.
[66] Strubelt O, Diederich KW. Experimental treatment of the acute cardiovascular toxicity of caffeine. J. Toxicol. Clin. Toxicol. 1999;37:29–33.
[67] Nurminen ML, Niittynen L, Korpela R, Vapaatalo H. Coffee, caffeine and blood pressure: a critical review. Eur. J. Clin. Nutr. 1999;53:831–9.
[68] Baylin A, Hernandez-Diaz S, Kabagambe EK, Siles X, Campos H. Transient exposure to coffee as a trigger of a first nonfatal myocardial infarction. Epidemiology. 2006;17:506–17.
[69] Frost L, Vestergaard P. Caffeine and risk of atrial fibrillation or flutter: the Danish Diet, Cancer, and Health Study. Am. J. Clin. Nutr. 2005;81:578–82.
[70] Myers MG. Caffeine and cardiac arrhythmias. Ann Intern Med 1991;114:147–50. [71] Newcombe PF, Renton KW, Rautaharju PM, Spencer CA, Montague TJ. High-dose
caffeine and cardiac rate and rhythm in normal subjects. Chest. 1988;94:90–4. [72] Graboys TB, Blatt CM, Lown B. The effect of caffeine on ventricular ectopic activity
in patients with malignant ventricular arrhythmia. Arch. Intern. Med. 1989;149:637–9.
[73] Myers MG, Harris L, Leenen FH, Grant DM. Caffeine as a possible cause of ventricular arrhythmias during the healing phase of acute myocardial infarction. Am. J. Cardiol. 1987;59:1024–8.
[74] Chopra A, Morrison L. Resolution of caffeine-induced complex dysrhythmia with procainamide therapy. J. Emerg. Med. 1995;13:113–7.
[75] Price KR, Fligner DJ. Treatment of caffeine toxicity with esmolol. Ann. Emerg. Med. 1990;19:44–6.
[76] Zimmerman PM, Pulliam J, Schwengels J, MacDonald SE. Caffeine intoxication: a near fatality. Ann. Emerg. Med. 1985;14:1227–9.
[77] Cannon ME, Cooke CT, McCarthy JS. Caffeine-induced cardiac arrhythmia: an unrecognized danger of healthfood products. Med. J. Aust. 2001;174:520–1.
[78] Šelb Šemerl J, Šelb K. Coffee and alcohol consumption as triggering factors for sudden cardiac death: case-crossover study. Croat. Med. J. 2004;45:775–80.
[79] Greenberg W, Shapiro D. The effects of caffeine and stress on blood pressure in individuals with and without a family history of hypertension. Psychophysiology. 1984;24:151–6.
[80] Čulić V. Coffee and myocardial infarction. Epidemiology. 2007;18:282. [81] Corrao G, Rubbiati L, Bagnardi V, Zambon A, Poikolainen K. Alcohol and coronary
heart disease: a meta-analysis. Addiction. 2000;95:1505–23. [82] Lucas DL, Brown RA, Wassef M, Giles TD. Alcohol and the cardiovascular system.
Research challenges and opportunities. J. Am. Coll. Cardiol. 2005;45:1916–24. [83] Rehm J, Sempos CT, Trevisan M. Alcohol and cardiovascular disease--more than one
paradox to consider. Average volume of alcohol consumption, patterns of drinking and risk of coronary heart disease - a review. J. Cardiovasc. Risk. 2003;10:15–20.
[84] Zakhari S. Alcohol and the cardiovascular system: molecular mechanisms for beneficial and harmful action. Alcohol Health Res. World. 1997;21:21–9.

Viktor Čulić 124
[85] Schreiber SS, Oratz M, Rothschild MA, Reff F, Evans C. Alcoholic cardiomyopathy. II. The inhibition of cardiac microsomal protein synthesis by acetaldehyde. J. Mol. Cell. Cardiol. 1974;6:207–15.
[86] Gould L, Reddy CVR, Becker W, Oh K, Kim SG. Electrophysiologic properties of alcohol in man. J. Electrocardiogr. 1978;11:219–26.
[87] Greenspon AJ, Schaal SF. The 'holiday heart': electrophysiological studies of alcohol effects in alcoholics. Ann. Intern. Med. 1983;98:135–9.
[88] Patel R, McArdle JJ, Regan TJ. Increased ventricular vulnerability in a chronic ethanol model despite reduced electrophysiologic responses to catecholamines. Alcohol. Clin. Exp. Res. 1991;15:785–9.
[89] Kentala E, Luurila O, Salaspuro MP. Effects of alcohol ingestion on cardiac rhythm in patients with ischaemic heart disease. Ann. Clin. Res. 1976;8:408–14.
[90] Suhonen O, Aromaa A, Revnanen A, Knekt P. Alcohol consumption and sudden coronary death in middle-aged Finnish men. Acta Med. Scand. 1987;221:335–41.
[91] Wannamethee G, Shaper AG. Alcohol and sudden cardiac death. Br. Heart J. 1992;68:443–8.
[92] Guideri G, Gutstein WH, Olivetti G, Anversa P. Effects of alcohol on isoproterenol-induced ventricular fibrillation in adult rats. J. Cardiovasc. Pharmacol. 1988;12:479–85.
[93] Nanji AA, Filipenko JD. Asystole and ventricular fibrillation associated with cocaine intoxication. Chest. 1984;85:132–3.
[94] Sherief HT, Carpentier RG. Electrophysiological mechanisms of cocaine-induced cardiac arrest. A possible cause of sudden cardiac death. J. Electrocardiol. 1991;24:247–55.
[95] Om A, Ellenbogen KA, Vetrovec GW. Cocaine-induced bradyarrhythmias. Am. Heart J. 1992;124:232–4.
[96] Bauman JL, Grawe JJ, Winecoff AP, Hariman RJ. Cocaine-related sudden cardiac death: a hypothesis correlating basic science and clinical observations. J. Clin. Pharmacol. 1994;34:902–11.
[97] Gamouras GA, Monir G, Plunkitt K, Gursoy S, Dreifus LS. Cocaine abuse: repolarization abnormalities and ventricular arrhythmias. Am. J. Med. Sci. 2000;320:9–12.
[98] Lange RA, Hillis LD. Cardiovascular complications of cocaine use. N. Engl. J. Med. 2001;345:351–8.
[99] Mittleman MA, Mintzer D, Maclure M, Tofler GH, Sherwood JB, Muller JE. Triggering of myocardial infarction by cocaine use. Circulation. 1999;99:2737–41.
[100] Pentel PR, Thompson T, Hatsukami DK, Salerno DM. 12-lead and continuous ECG recordings of subjects during inpatient administration of smoked cocaine. Drug Alcohol. Depend. 1994;35:107–116.
[101] Lange RA, Hillis LD. Cardiovascular complications of cocaine use. N. Engl. J. Med. 2001;345:351–8.
[102] Kloner RA, Hale S, Alker K, Rezkalla SH. The effects of acute and chronic cocaine use on the heart. Circulation. 1992;85:407–19.

External Triggering, Modifying and Chronobiologic Factors… 125
[103] Gradman AH. Cardiac effects of cocaine: a review. Yale J. Biol. Med. 1988;61:137–47.
[104] Billman GE, Lappi MD. Effects of cocaine on cardiac vagal tone before and during coronary artery occlusion: cocaine exacerbates the autonomic response to myocardial ischemia. J. Cardiovasc. Pharmacol. 1993;22: 869–76.
[105] Moliterno DJ, Willard JE, Lange RA, Negus BH, Boehrer JD, Glamann DB, Rossen JD, Winniford MD, Hillis LD. Coronary-artery vasoconstriction induced by cocaine, cigarette smoking, or both. N. Engl. J. Med. 1994;330:454–9.
[106] Ritchie JM, Greene NM. Local anesthetics. In: Gilman AG, Rall TW, Nies AS, Taylor P, eds. Goodman and Gilman’s The Pharmacologic Basis of Therapeutics. New York, NY: Pergamon Press; 1990:311–31.
[107] Lange RA, Cigarroa RG, Yancy CW Jr, Willard JE, Popma JJ, Sills MN, McBride W, Kim AS, Hillis LD. Cocaine-induced coronary-artery vasoconstriction. N. Engl. J. Med. 1989;321:1557–62.
[108] Crumb WJ, Clarkson CW. Characterization of cocaine-induced block of sodium channels. Biophys. J. 1990;57:589–99.
[109] Magnano AR, Talathoti NB, Hallur R, Jurus DT, Dizon J, Holleran S, Bloomfield DM, Collins E, Garan H. Effect of acute cocaine administration on the QTc interval of habitual users. Am. J. Cardiol. 2006;97:1244–6.
[110] Magnano AR, Holleran S, Ramakrishnan R, Reiffel JA, Bloomfield DM. Autonomic modulation of the U wave: sympathomimetic stimulation and vagal inhibition in normal individuals. Pacing Clin. Electrophysiol. 2004;27:1484–92.
[111] Wit AL, Rosen MR. After depolarizations and triggered activity. In: Fozzard HA, Haber E, Jennings RB, Katz AM, Morgan HE, eds. The heart and cardiovascular system: scientific foundations. Vol. 2. New York: Raven Press, 1986:1449–90.
[112] Martell BA, Arnsten JH, Krantz MJ, Gourevitch MN. Impact of methadone treatment on cardiac repolarization and conduction in opioid users. Am. J. Cardiol. 2005;95:915–8.
[113] Justo D, Gal-Oz A, Paran Y, Goldin Y, Zeltser D. Methadone-associated Torsades de Pointes (polymorphic ventricular tachycardia) in opioid-dependent patients. Addiction. 2006;101:1333–8.
[114] Keegan A. Cocaine plus alcohol, a deadly mix. NIDA Notes. 1991;6:18. [115] Substance Abuse and Mental Health Services Administration. Summary of Findings
From the 1999 National Household Survey on Drug Abuse (DHHS Publication No. SMA 00-3466). Rockville, Maryland: Substance Abuse and Mental Health Services Administration, 2000.
[116] Renault PF, Schuster CR, Heinrich R, Freeman DX. Marihuana: standardized smoke administration and dose effect curves on heart rate in humans. Science. 1971;174:589–91.
[117] Kiplinger GF, Manno JE. Dose–response relationships to cannabis in human subjects. Pharmacol. Rev. 1971;23:339–47.
[118] Kochar MS, Hosko MJ. Electrocardiographic effects of marihuana. JAMA. 1973;225:25–7.

Viktor Čulić 126
[119] Aronow WS, Cassidy J. Effect of marihuana and placebo–marihuana smoking on angina pectoris. New Engl J Med 1974;291:65–7.
[120] Gregg J. Cardiovascular effects of cannabinol during oral surgery. Anesth. Analg. 1976;5:203–13.
[121] Sidney S. Cardiovascular consequences of marijuana use. J. Clin. Pharmacol. 2002;42(11 Suppl):64S–70S.
[122] Jones RT. Cardiovascular system effects of marijuana. J. Clin. Pharmacol. 2002;42(11 Suppl):58S–63S.
[123] Rezkalla SH, Sharma P, Kloner RA. Coronary no-flow and ventricular tachycardia with habitual marijuana use. Ann. Emerg. Med. 2003;42:365–9.
[124] Bachs L, Morland H. Acute cardiovascular fatalities following cannabis use. Forensic Sci. Int. 2001;124:200–3.
[125] Lindsay AC, Foale RA, Warren O, Henry JA. Cannabis as a precipitant of cardiovascular emergencies. Int. J. Cardiol. 2005;104:230–2.
[126] Mittleman MA, Lewis RA, Maclure M, Sherwood JB, Muller JE. Triggering myocardial infarction by marijuana. Circulation. 2001;103:2805–9.
[127] Beaconsfield P. Marijuana smoking: cardiovascular effects in man and possible mechanisms. New Engl. J. Med. 1972;287:209–12.
[128] Delfino RJ, Sioutas C, Malik S. Potential role of ultrafine particles in associations between airborne particle mass and cardiovascular health. Environ. Health Perspect. 2005;113:934–46.
[129] Pope CA III, Burnett RT, Thurston GD, Thun MJ, Calle EE, Krewski D, Godleski JJ. Cardiovascular mortality and long-term exposure to particulate air pollution: epidemiological evidence of general pathophysiological pathways of disease. Circulation. 2004;109:71–7.
[130] Brook RD, Franklin B, Cascio W, Hong Y, Howard G, Lipsett M, Luepker R, Mittleman MA, Samet J, Smith SC Jr, Tager I, for the Expert Panel on Population and Prevention Science of the American Heart Association. Air pollution and cardiovascular disease: a statement for healthcare professionals from the Expert Panel on Population and Prevention Science of the American Heart Association. Circulation. 2004;109:2655–71.
[131] Ruidavets JB, Cournot M, Cassadou S, Giroux M, Meybeck M, Ferrieres J. Ozone air pollution is associated with acute myocardial infarction. Circulation. 2005;111:563–9.
[132] Zanobetti A, Schwartz J. The effect of particulate air pollution on emergency admissions for myocardial infarction: a multicity case-crossover analysis. Environ. Health Perspect. 2005;113:978–82.
[133] D’Ippoliti D, Forastiere F, Ancona C, Agabiti N, Fusco D, Michelozzi P, Perucci CA. Air pollution and myocardial infarction in Rome: a casecrossover analysis. Epidemiology. 2003;14:528–35.
[134] Peters A, Dockery DW, Muller JE, Mittleman MA. Increased particulate air pollution and the triggering of myocardial infarction. Circulation. 2001;103:2810–5.
[135] Wellenius GA, Bateson TF, Mittleman MA, Schwartz J. Particulate air pollution and the rate of hospitalization for congestive heart particulate air pollution and the rate of

External Triggering, Modifying and Chronobiologic Factors… 127
hospitalization for congestive heart failure among medicare beneficiaries in Pittsburgh, Pennsylvania. Am. J. Epidemiol. 2005;161:1030–6.
[136] Morris RD, Naumova EN. Carbon monoxide and hospital admissions for congestive heart failure: evidence of an increased effect at low temperatures. Environ. Health Perspect. 1998;106:649–53.
[137] Morris RD, Naumova EN, Munasinghe RL. Ambient air pollution and hospitalization for congestive heart failure among elderly people in seven large US cities. Am. J. Public Health. 1995;85:1361–5.
[138] Graff DW, Cascio WE, Brackhan JA, Devlin RB. Metal particulate matter components affect gene expression and beat frequency of neonatal rat ventricular myocytes. Environ. Health Perspect. 2004;112:792–8.
[139] Campen MJ, Nolan JP, Schladweiler MC, Kodavanti UP, Costa DL, Watkinson WP. Cardiac and thermoregulatory effects of instilled particulate matter-associated transition metals in healthy and cardiopulmonary-compromised rats. J. Toxicol. Environ. Health. 2002;A 65:1615–31.
[140] Kim S, Shen S, Sioutas C. Size distribution and diurnal and seasonal trends of ultrafine particles in source and receptor sites of the Los Angeles basin. J. Air Waste Manage. Assoc. 2002;52:297–307.
[141] Oberdörster G. Pulmonary effects of inhaled ultrafine particles. Int. Arch. Occup. Environ. Health. 2001;74:1–8.
[142] Miller FJ, Gardner DE, Graham JA, Lee RE Jr, Wilson WE, Bachmann JD. Size considerations for establishing a standard for inhalable particles. J. Air Pollut. Control. Assoc. 1979;29:610–5.
[143] Wichmann HE, Mueller W, Allhoff P, Beckmann M, Bocter N, Csicsaky MJ, Jung M, Molik B, Schoeneberg G. Health effects during a smog episode in West Germany in 1985. Environ. Health Perspect. 1989;79:89–99.
[144] Dockery DW, Luttmann-Gibson H, Rich DQ, Link M, Mittleman MA, Gold DR, Koutrakis P, Schwartz JD, Verrier RL. Association of air pollution with increased incidence of ventricular tachyarrhythmias recorded by implanted cardioverter defibrillators. Environ. Health Perspect. 2005;113:670–4.
[145] Rich DQ, Schwartz J, Mittleman MA, Link M, Luttmann-Gibson H, Catalano PJ, Speizer FE, Dockery DW. Association of short-term ambient air pollution concentrations and ventricular arrhythmias. Am. J. Epidemiol. 2005;161:1123–32.
[146] Riediker M, Cascio WE, Griggs TR, Herbst MC, Bromberg PA, Neas L, Williams RW, Devlin RB. Particulate matter exposure in cars is associated with cardiovascular effects in healthy young men. Am. J. Respir. Crit. Care Med. 2004;169:934–40.
[147] Vedal S, Rich K, Brauer M, White R, Petkau J. Air pollution and cardiac arrhythmias in patients with implantable cardioverter defibrillators. Inhal. Toxicol. 2004;16:353–62.
[148] Sullivan J, Sheppard L, Schreuder A, Ishikawa N, Siscovick D, Kaufman J. Relation between short-term fine-particulate matter exposure and onset of myocardial infarction. Epidemiology. 2005;16:41–8.
[149] Sullivan J, Ishikawa N, Sheppard L, Siscovick D, Checkoway H, Kaufman J. Exposure to ambient fine particulate matter and primary cardiac arrest among persons

Viktor Čulić 128
with and without clinically recognized heart disease. Am. J. Epidemiol. 2003;157:501–9.
[150] Künzli N, Schindler C. A call for reporting the relevant exposure term in air pollution case-crossover studies. J. Epidemiol. Community Health. 2005;59:527–30.
[151] Carr MJ, Undem BJ. Inflammation-induced plasticity of the afferent innervation of the airways. Environ. Health Perspect. 2001;109(suppl 4):567–71.
[152] Yeates DB. Neurally mediated cardiopulomonary and systemic responses to inhaled irritants and antigens. In: Particle-Lung Interactions (Gehr P, Heyder J, eds). New York:Marcel Dekker, 2000, 603–26.
[153] Yeates DB, Mauderly JL. Inhaled environmental/occupational irritants and allergens: mechanisms of cardiovascular and systemic responses. Introduction. Environ. Health Perspect. 2001;109(suppl 4):479–81.
[154] Li YH, Rozanski GJ. Effects of human recombinant interleukin-1 on electrical properties of guinea pig ventricular cells. Cardiovasc. Res. 1993;27:525–30.
[155] Yokoyama T, Vaca L, Rossen RD, Durante W, Hazarika P, Mann DL. Cellular basis for the negative inotropic effects of tumor necrosis factor-alpha in the adult mammalian heart. J. Clin. Invest. 1993;92:2303–12.
[156] Finkel MS, Oddis CV, Jacob TD, Watkins SC, Hattler BG, Simmons RL. Negative inotropic effects of cytokines on the heart mediated by nitric oxide. Science. 1992;257:387–9.
[157] DeMeules JE, Pigula FA, Mueller M, Raymond SJ, Gamelli RL. Tumor necrosis factor and cardiac function. J. Trauma. 1992;32:686–92.
[158] Weisensee D, Bereiter-Hahn J, Schoeppe W, Low-Friedrich I. Effects of cytokines on the contractility of cultured cardiac myocytes. Int. J. Immunopharmacol. 1993;15:581–7.
[159] Park SK, O'Neill MS, Vokonas PS, Sparrow D, Schwartz J. Effects of air pollution on heart rate variability: the VA normative aging study. Environ. Health Perspect. 2005;113:304–9.
[160] Liao D, Duan Y, Whitsel EA, Zheng ZJ, Heiss G, Chinchilli VM, Lin HM. Association of higher levels of ambient criteria pollutants with impaired cardiac autonomic control: a population based study. Am. J. Epidemiol. 2004;159:768–77.
[161] Peters A, Perz S, Döring A. Increases in heart rate during an air pollution episode. Am. J. Epidemiol. 1999;150:1094–8.
[162] Pope CA III, Verrier RL, Lovett EG. Heart rate variability associated with particulate air pollution. Am. Heart J. 1999;138:890–9.
[163] Henneberger A, Zareba W, Ibald-Mulli A, Rückerl R, Cyrys J, Couderc JP, Mykins B, Woelke G, Wichmann HE, Peters A. Repolarization changes induced by air pollution in ischemic heart disease patients. Environ. Health Perspect. 2005;113:440–6.
[164] Godleski JJ, Verrier RL, Koutrakis P, Catalano P, Coull B, Reinisch U, Lovett EG, Lawrence J, Murthy GG, Wolfson JM, Clarke RW, Nearing BD, Killingsworth C. Mechanisms of morbidity and mortality from exposure to ambient particles. Res. Rep. Health Eff. Inst. 2000;91:5–88.

External Triggering, Modifying and Chronobiologic Factors… 129
[165] Nemmar A, Hoet PHM, Vanquickenborne B, Dinsdale D, Thomeer M, Hoylaerts MF, Vanbilloen H, Mortelmans L, Nemery B. Passage of inhaled particles into the blood circulation in humans. Circulation. 2002;105:411–4.
[166] Calderon-Garciduenas L, Gambling TM, Acuna H, Garcia R, Osnaya N, Monroy S, Villarreal-Calderon A, Carson J, Korens HS, Devlin RB. Canines as sentinel species for assessing chronic exposures to air pollutants: part 2. Cardiac. Pathol. Toxicol. Sci. 2001;61:356–67.
[167] Libby P. Inflammation in atherosclerosis. Nature. 2002;420: 868–74. [168] Davies MJ. The pathophysiology of acute coronary syndromes. Heart. 2000;83:361–
6. [169] Seaton A, MacNee W, Donaldson K, Godden D. Particulate air pollution and acute
health effects. Lancet. 1995;345:176–8. [170] Seaton A, Soutar A, Crawford V, Elton R, McNerlan S, Cherrie J, Watt M, Agius R,
Stout R. Particulate air pollution and the blood. Thorax. 1999;54:1027–32. [171] Peters A, Doering A, Wichmann HE, Koenig W. Increased plasma viscosity during
an air pollution episode: a link to mortality? Lancet. 1997;349:1582–7. [172] Weerasinghe DP, MacIntyre CR, Rubin GL. Seasonality of coronary deaths in New
South Wales, Australia. Heart. 2002;88:30–4. [173] Danet S, Richard F, Montaye M, Beauchant S, Lemaire B, Graux C, Cottel D,
Marecaux N, Amouyel P. Unhealthy effects of atmospheric temperature and pressure on the occurrence of myocardial infarction and coronary deaths. A 10-year survey: the Lille-World Health Organization MONICA Project. Circulation. 1999;100:E1-7.
[174] Seretakis D, Pagona L, Lipworth L, Signorello LB, Rothman KJ, Trichopoulos D. Changing seasonality of mortality from coronary heart disease. JAMA. 1997;278:1012–4.
[175] Keatinge WR, for the Eurowinter Group. Cold exposure and winter mortality from ischaemic heart disease, cerebrovascular disease, respiratory disease and all causes in warm and cold regions of Europe. Lancet. 1997;349:1341–6.
[176] Pan W-H, Li L-A, Tsai M-J. Temperature extremes and mortality from coronary heart disease and cerebral infarction in elderly Chinese. Lancet. 1995;345:353–5.
[177] Fries RP, Heisel AG, Jung JK, Schieffer HJ. Circannual variation of malignant ventricular tachyarrhythmias in patients with implantable cardioverter-defibrillators and either coronary artery disease or idiopathic dilated cardiomyopathy. Am. J. Cardiol. 1997;79:1194–7.
[178] Keatinge WR, Coleshaw SR, Easton JC, Cotter F, Mattock MB, Chelliah R. Increased platelet and red cell counts, blood viscosity and plasma cholesterol levels during heat stress, and mortality from coronary and cerebral thrombosis. Am. J. Med. 1986;81:795–800.
[179] Stuhr LE, Risberg J, Bergo GW, Tyssebotn I. Cardiovascular effects of verapamil and quinidine at normal and elevated ambient pressure. Aviat. Space Environ. Med. 2001;72:373–9.
[180] Stuhr LE, Ask JA, Tyssebotn I. Increased cardiac contractility in rats exposed to 5 bar. Acta Physiol. Scand. 1989;136:167–76.

Viktor Čulić 130
[181] Dockery DW, Pope CA III,Kanner RE, Martin Villegas G, Schwartz J. Daily changes in oxygen saturation and pulse rate associated with particulate air pollution and barometric pressure. Res. Rep. Health Eff. Inst. 1999;83:1–19.
[182] Sato J, Takanari K, Omura S, Mizumura K. Effects of lowering barometric pressure on guarding behavior, heart rate and blood pressure in a rat model of neuropathic pain. Neurosci. Lett. 2001;299:17–20.
[183] Panagiotakos DB, Chrysohoou C, Pitsavos C, Nastos P, Anadiotis A, Tentolouris C, Stefanadis C, Toutouzas P, Paliatsos A. Climatological variations in daily hospital admissions for acute coronary syndromes. Int. J. Cardiol. 2004;94:229–33.
[184] Goerre S, Egli C, Gerber S, Defila C, Minder C, Richner H, Meier B. Impact of weather and climate on the incidence of acute coronary syndromes. Int. J. Cardiol. 2007;118:36–40.
[185] Delyukov A, Didyk L. The effects of extra-low-frequency atmospheric pressure oscillations on human mental activity. Int. J. Biometeorol. 1999;43:31–7.
[186] Jalife J. Ventricular fibrillation: mechanisms of initiation and maintenance. Annu. Rev. Physiol. 2000;62:25–50.
[187] Yusuf S, Lopez R, Sleight P. Heart rate and ectopic prematurity in relation to sustained ventricular arrhythmias. Br. Heart J. 1980;44:233–9.
[188] Jouven X, Zureik M, Desnos M, Courbon D, Ducimetiere P. Long-term outcome in asymptomatic men with exercise-induced premature ventricular depolarizations. N. Engl. J. Med. 2000;343:826–33.
[189] Udall JA, Ellestad MH. Predictive implications of ventricular premature contractions associated with treadmill stress testing. Circulation. 1977;56:985–9.
[190] Drory Y, Pines A, Fisman EZ, Kellermann JJ. Persistence of arrhythmia exercise response in healthy young men. Am. J. Cardiol. 1990;66:1092–4.
[191] Fleg J, Lakatta E. Prevalence and prognosis of exercise-induced nonsustained ventricular tachycardia in apparently healthy volunteers. Am. J. Cardiol. 1984;54:762–4.
[192] Nair CK, Aronow WS, Sketch MH, Pagano T, Lynch JD, Mooss AN, Esterbrooks D, Runco V, Ryschon K. Diagnostic and prognostic significance of exercise-induced premature ventricular complexes in men and women: a four year follow-up. J. Am. Coll. Cardiol. 1983;1:1201–6.
[193] Bruce RA, DeRouen TA, Hossack KF. Value of maximal exercise tests in risk assessment of primary coronary heart disease events in healthy men. Five years’ experience of the Seattle heart watch study. Am. J. Cardiol. 1980;46:371–8.
[194] Brugada P, Brugada J. Further characterization of the syndrome of right bundle branch block, ST elevation, and sudden cardiac death. J. Cardiovasc. Electrophysiol. 1997;8:325–31.
[195] Rodriguez LM, de Chillou C, Schlapfer J, Metzger J, Baiyan X, van der Dool A, Smeets JLRM, Wellens HJJ. Age at onset and gender of patients with different types of supraventricular tachycardias. Am. J. Cardiol. 1992;70:1213–5.
[196] Kannel WB, Wilson PWF, D’Agostino RB, Cobb J. Sudden coronary death in women. Am. Heart J. 1998;136:205–12.

External Triggering, Modifying and Chronobiologic Factors… 131
[197] Locati EH, Zareba W, Moss AJ, Schwartz PJ, Vincent GM, Lehmann MH, Towbin JA, Priori SG, Napolitano C, Robinson JL, Andrews M, Timothy K, Hall WJ. Age- and sex-related differences in clinical manifestations in patients with congenital long-QT syndrome: findings from the International LQTS Registry. Circulation. 1998;97:2237–44.
[198] Lehmann MH, Timothy K, Frankovich D, Fromm B, Keating M, Locati E, Schwartz PJ, Moss AJ, Taggart RT, Towbin JA, Vincent GM. Age-sex influence on rate corrected QT interval and QT-heart rate relationship in families with genotypically characterized long QT syndrome. J. Am. Coll. Cardiol. 1997;29:93–9.
[199] Stramba-Badiale M, Spagnolo D, Bosi G, Schwartz PJ. Are gender differences in QTc present at birth? Am. J. Cardiol. 1995;75:1277–8.
[200] Rautaharju PM, Zhou SH, Wong S, Calhoun HP, Berenson G, Prineas R, Davignon A. Sex differences in the evolution of electrocardiographic QT interval with age. Can. J. Cardiol. 1992;8:690–5.
[201] Merri M, Benhorin J, Alberti M, Locati EH, Moss AJ. Electrocardiographic quantitation of ventricular repolarization. Circulation. 1989;80:1301–8.
[202] Liu CC, Kuo TB, Yang CC. Effects of estrogen on gender-related autonomic differences in humans. Am. J. Physiol. Heart Circ. Physiol. 2003;285:H2188–93.
[203] Du XJ, Dart AM, Riemersma RA. Sex differences in the parasympathetic nerve control of rat heart. Clin. Exp. Pharmacol. Physiol. 1994;21:485–93.
[204] De Meersman RE, Zion AS, Giardina EG, Weir JP, Lieberman JS, Downey JA. Estrogen replacement, vascular distensibility, and blood pressures in postmenopausal women. Am. J. Physiol. Heart Circ. Physiol. 1998;274:H1539–44.
[205] Vongpatanasin W, Tuncel M, Mansour Y, Arbique D, Victor RG. Transdermal estrogen replacement therapy decreases sympathetic activity in postmenopausal women. Circulation. 2001;103:2903–8.
[206] Huikuri HV, Pikkujamsa SM, Airaksinen KEJ, Ikaheimo MJ, Rantala AO, Kauma H, Lilja M, Kesaniemi YA. Sex-related differences in autonomic modulation of heart rate in middle-aged subjects. Circulation. 1996;94:122–5.
[207] Nakagawa M, Ooie T, Ou B, Ichinose M, Takashi N, Hara M, Yonemochi H, Saikawa T. Gender differences in autonomic modulation of ventricular repolarization in humans. J. Cardiovasc. Electrophysiol. 2005;16:278–84.
[208] Kadish AH. The effect of gender on cardiac electrophysiology and arrhythmias. In: Zipes DP, Jalife J, eds. Cardiac Electrophysiology: From Cell to Bedside. 2nd ed. Philadelphia, Pa: WB Saunders Co; 1995:1268–75.
[209] Collins P, Rosano GM, Jiang C, Lindsay D, Sarrel PM, Poole-Wilson PA. Cardiovascular protection by oestrogen - a calcium antagonist effect? Lancet. 1993;341:1264–5.
[210] Brodsky M, Doria R, Allen B, Sato D, Thomas G, Sada M. New-onset ventricular tachycardia during pregnancy. Am. Heart J. 1992;123(4 Pt 1):933-41.
[211] Christ M, Seyffart K, and Wehling M. Attenuation of heartrate variability in postmenopausal women on progestin-containing hormone replacement therapy. Lancet. 1999;353:1939–40.

Viktor Čulić 132
[212] Drici MD, Burklow TR, Vedanandam H, Glazer RI, Woosley RL. Sex hormones prolong the QT interval and downregulate potassium channel expression in the rabbit heart. Circulation. 1996;94:1471–4.
[213] Liu DW, Antzelevitch C. Characteristics of the delayed rectifier current (IKr and IKs) in canine ventricular epicardial, midmyocardial, and endocardial myocytes. A weaker IKs contributes to the longer action potential of the M cell. Circ. Res. 1995;76:351–65.
[214] Carney RM, Freedland KE, Stein PK. Anxiety, depression, and heart rate variability. Psychosom. Med. 2000;62:84–7.
[215] Carney RM, Saunders RD, Freedland KE, Stein P, Rich MW, Jaffe AS. Association of depression with reduced heart rate variability in coronary artery disease. Am. J. Cardiol. 1995;76:562–4.
[216] Kawachi I, Sparrow D, Vokonas PS, Weiss ST. Decreased heart rate variability in men with phobic anxiety (data from the Normative Aging Study) Am. J. Cardiol. 1995;75:882–5.
[217] Watkins LL, Grossman P. Association of depressive symptoms with reduced baroreflex cardiac control in coronary artery disease. Am. Heart J. 1999;37:453–7.
[218] Kubzansky LD, Kawachi I. Going to the heart of the matter: negative emotions and coronary heart disease. J. Psychosom. Res. 2000;48:323–37.
[219] Kawachi I, Colditz GA, Ascherio A, Rimm Eric B, Giovannucci E, Stampfer MJ, Willett WC. Coronary heart disease/myocardial infarction: prospective study of phobic anxiety and risk of coronary heart disease in men. Circulation. 1994;89:1992–7.
[220] Haines AP, Imeson JD, Meade TW. Phobic anxiety and ischaemic heart disease. BMJ. 1987;295:297–9.
[221] Albert CM, Chae CU, Rexrode KM, Manson JE. Phobic anxiety and risk of coronary heart disease and sudden cardiac death among women. Circulation. 2005;111;480–7.
[222] Rozanski A, Blumenthal JA, Kaplan J. Impact of psychological factors on the pathogenesis of cardiovascular disease and implications for therapy. Circulation. 1999;99:2192–217.
[223] Denollet J, Pedersen SS, Vrints CJ, Conraads VM. Usefulness of type D personality in predicting five-year cardiac events above and beyond concurrent symptoms of stress in patients with coronary heart disease. Am. J. Cardiol. 2006;97:970–3.
[224] Gudbjarnason S, Hallgrimsson J. The role of myocardial membrane lipids in the development of cardiac necrosis. Acta Med. Scand. 1975;suppl 587:17–26.
[225] Marchioli R, Barzi F, Bomba E, Chieffo C, Di Gregorio D, Di Mascio R, Franzosi MG, Geraci E, Levantesi G, Maggioni AP, et al. Early protection against sudden death by omega-3 polyunsaturated fatty acids after myocardial infarction: time-course analysis of the results of the Gruppo Italiano per lo Studio della Sopravvivenza nell’Infarto Miocardico (GISSI)-Prevenzione. Circulation. 2002;105:1897–903.
[226] Albert CM, Campos H, Stampfer MJ, Ridker PM, Manson JE, Willett WC, Ma J. Blood levels of long-chain omega-3 fatty acids and the risk of sudden death. N. Engl. J. Med. 2002;346:1113–8.

External Triggering, Modifying and Chronobiologic Factors… 133
[227] Burr ML, Fehily AM, Gilbert JF, Rogers S, Holliday RM, Sweetnam PM, Elwood PC, Deadman NM. Effects of changes in fat, fish, and fibre intakes on death and myocardial reinfarction: Diet and Reinfarction Trial (DART). Lancet. 1989;2:757–61.
[228] De Backer G, Ambrosioni E, Borch-Johnsen K, Brotons C, Cifkova R, Dallongeville J, Ebrahim S, Faergeman O, Graham I, Mancia G, et al, for the Third Joint Task Force of European and Other Societies on Cardiovascular Disease Prevention in Clinical Practice. European guidelines on cardiovascular disease prevention in clinical practice: Third Joint Task Force of European and Other Societies on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2003;24:1601–10.
[229] Leaf A, Xiao YF, Kang JX, Billman GE. Prevention of sudden cardiac death by omega-3 polyunsaturated fatty acids. Pharmacol. Ther. 2003;98:355–77.
[230] Lee KW, Lip GY. The role of omega-3 fatty acids in the secondary prevention of cardiovascular disease. QJM. 2003;96:465–80.
[231] Rathore SS, Wang Y, Krumholz HM. Sex-based differences in the effect of digoxin for the treatment of heart failure. N. Engl. J. Med. 2002;347:1403–11.
[232] Furberg CD, Vittinghoff E, Davidson M, Herrington DM, Simon JA, Wenger NK, Hulley S. Subgroup interactions in the Heart and Estrogen/Progestin Replacement Study: lessons learned. Circulation. 2002;105:917–22.
[233] Vyas AK, Guo H, Moss AJ, Olshansky B, McNitt SA, Hall WJ, Zareba W, Steinberg JS, Fischer A, Ruskin J, Andrews ML; MADIT-II research Group. Reduction in ventricular tachyarrhythmias with statins in the Multicenter Automatic Defibrillator Implantation Trial (MADIT)-II. J. Am. Coll. Cardiol. 2006;47:769–73.
[234] Englund A, Behrens S, Wegscheider K, Rowland E. Circadian variation of malignant ventricular arrhythmias in patients with ischemic and nonischemic heart disease after cardioverter defibrillator implantation. European 7219 Jewel Investigators. J. Am. Coll. Cardiol. 1999;34:1560–8.
[235] Mallavarapu C, Pancholy S, Schwartzman D, Callans DJ, Heo J, Gottlieb CD, Marchlinski FE. Circadian variation of ventricular arrhythmia recurrences after cardioverter-defibrillator implantation in patients with healed myocardial infarcts. Am. J. Cardiol. 1995;75:1140–4.
[236] Tofler GH, Gebara OC, Mittleman MA, Taylor P, Siegel W, Venditti FJ Jr, Rasmussen CA, Muller JE. Morning peak in ventricular tachyarrhythmias detected by time of implantable cardioverter/defibrillator therapy. The CPI Investigators. Circulation. 1995;92:1203–8.
[237] Wood MA, Simpson PM, London WB, Stambler BS, Herre JM, Bernstein RC, Ellenbogen KA. Circadian pattern of ventricular tachyarrhythmias in patients with implantable cardioverter-defibrillators. J. Am. Coll. Cardiol. 1995;25:901–7.
[238] Thakur RK, Hoffmann RG, Olson DW, Joshi R, Tresch DD, Aufderheide TP, Ip JH. Circadian variation in sudden cardiac death: effects of age, sex, and initial cardiac rhythm. Ann. Emerg. Med. 1996;27:29–34.
[239] Matsuo K, Kurita T, Inagaki M, Kakishita M, Aihara N, Shimizu W, Taguchi A, Suyama K, Kamamura S, Shimomura K. The circadian pattern of the development of

Viktor Čulić 134
ventricular fibrillation in patients with Brugada syndrome. Eur. Heart J. 1999;20::465–70.
[240] Yamashita T, Murakawa Y, Hayami N, Sezaki K, Inoue M, Fukui E, Omata M. Relation between aging and circadian variation of paroxysmal atrial fibrillation. Am. J. Cardiol. 1998;82:1364–7.
[241] Yamashita T, Murakawa Y, Sezaki K, Inoue M, Hayami N, Shuzui Y, Omata M. Circadian variation of paroxysmal atrial fibrillation. Circulation. 1997;96:1537–41.
[242] Behrens S, Ehlers C, Bruggemann T, Ziss W, Dissmann R, Galecka M, Willich SN, Andresen D. Modification of the circadian pattern of ventricular tachyarrhythmias by beta-blocker therapy. Clin. Cardiol. 1997;20:253–7.
[243] Peters RW, Muller JE, Goldstein S, Byington R, Friedman LM. Propranolol and the morning increase in the frequency of sudden cardiac death (BHAT Study). Am. J. Cardiol. 1989;63:1518–20.
[244] Guo YF, Stein PK. Circadian rhythm in the cardiovascular system: considerations in non-invasive electrophysiology. Card. Electrophysiol. Rev. 2002;6:267–72.
[245] Molnar J, Rosenthal JE, Weiss JS, Somberg JC. QT interval dispersion in healthy subjects and survivors of sudden cardiac death: circadian variation in a twenty-four-hour assessment. Am. J. Cardiol. 1997;79:1190–3.
[246] Bexton RS, Vallin HO, Camm AJ. Diurnal variation of the QT interval - influence of the autonomic nervous system. Br. Heart J. 1986;55:253–8.
[247] Ishida S, Nakagawa M, Fujino T, Yonemochi H, Saikawa T, Ito M. Circadian variation of QT interval dispersion: correlation with heart rate variability. J. Electrocardiol. 1997;30:205–10.
[248] Simantirakis EN, Chrysostomakis SI, Marketou ME, Kochiadakis GE, Vardakis KE, Mavrakis HE, Vardas P. Atrial and ventricular refractoriness in paced patients; circadian variation and its relationship to autonomic nervous system activity. Eur. Heart J. 2001;22:2192–200.
[249] Kong QT Jr, Goldberger JJ, Parker M, Wang T, Kadish AH. Circadian variation in human ventricular refractoriness. Circulation. 1995;92:1507–16.
[250] Cinca J, Moya A, Figueras J, Roma F, Rius J. Circadian variations in the electrical properties of the human heart assessed by sequential bedside electrophysiologic testing. Am. Heart J. 1986;112:315–21.
[251] Yamashita T, Sekiguchi A, Iwasaki YK, Sagara K, Iinuma H, Hatano S, Fu LT, Watanabe H. Circadian variation of cardiac K+ channel gene expression. Circulation. 2003;107:1917–22.
[252] Barnett AG, Dobson AJ. Excess in cardiovascular events on Mondays: a meta-analysis and prospective study. J. Epidemiol. Community Health. 2005;59:109–14.
[253] Arntz HR, Willich SN, Schreiber C, Bruggemann T, Stern R, Schultheiss HP. Diurnal, weekly, and seasonal variation of sudden death. Population-based analysis of 24,061 consecutive cases. Eur. Heart J. 2000;21:315–20.
[254] Peters RW, McQuillan S, Gold MR. Interaction of septadian and circadian rhythms in life-threatening ventricular arrhythmias in patients with implantable cardioverter-defibrillators. Am. J. Cardiol. 1999;84:555–7.

External Triggering, Modifying and Chronobiologic Factors… 135
[255] Peters RW, McQuillan S, Resnick SK, Gold MR. Increased Monday incidence of life-threatening ventricular arrhythmias. Experience with a third-generation implantable defibrillator. Circulation. 1996;94:1346–9.
[256] Čulić V. Excess in cardiovascular events on Mondays: could atherosclerotic plaques be more vulnerable after the weekend because of alcohol related cytokine dysregulation? J. Epidemiol. Community Health. 2005;59:911.
[257] Page RL, Zipes DP, Powell JL, Luceri RM, Gold MR, Peters R, Russo AM, Bigger JT Jr, Sung RJ, McBurnie MA, for the AVID Investigators. Seasonal variation of mortality in the Antiarrhythmics Versus Implantable Defibrillators (AVID) study registry. Heart Rhythm. 2004;1:435–40.
[258] Muller D, Lampe F,Wegscheider K, Schultheiss HP, Behrens S. Annual distribution of ventricular tachycardias and ventricular fibrillation. Am. Heart J. 2003;146:1061–5.
[259] Stuber T, Eigmann C, Delacrtaz E. Seasonal variation of ventricular arrhythmia clusters in defibrillator recipients. PACE. 2006;29:816–20.
[260] Becker S, Dailey LA, Soukup JM, Grambow SC, Devlin RB, Huang YCT. Seasonal variations in air pollution particle-induced inflammatory mediator release and oxidative stress. Environ. Health Perspect. 2005;113:1032–8.
[261] Matthews CE, Freedson PS, Hebert JR, Stanek EJ 3rd, Merriam PA, Rosal MC, Ebbeling CB, Ockene IS. Seasonal variation in household, occupational, and leisure time physical activity: longitudinal analyses from the seasonal variation of blood cholesterol study. Am. J. Epidemiol. 2001;153:172–83.
[262] Dannenberg AL, Keller JB, Wilson PW, Castelli WP. Leisure time physical activity in the Framingham Offspring Study. Description, seasonal variation, and risk factor correlates. Am. J. Epidemiol. 1989;129:76–88.
[263] Craft LL, Landers DM. The effect of exercise on clinical depression and depression resulting from mental illnes: a meta-analysis. J. Sport Exerc. Psychol. 1998;20:339–57.
[264] Suhail K, Cochrane R. Seasonal changes in affective state in samples of Asian and white women. Soc. Psychiatry Psychiatr. Epidemiol. 1997;32:149–57.
[265] Hedge AL, Woodson H. Prevalence of seasonal changes in mood and behavior during the winter months in central Texas. Psychiatry Res. 1996;62:265–71.
[266] Čulić V. Seasonal distribution of acute myocardial infarction: a need for a broader perspective. Int. J. Cardiol. 2006;109:265–6.
[267] Sher L. Seasonal distribution of myocardial infarction and seasonal mood changes. J. Am. Coll. Cardiol. 1999;33:2088–9.
[268] Kasper S, Wehr TA, Bartko JJ, Gaist PA, Rosenthal NE. Epidemiological findings of seasonal changes in mood and behavior. A telephone survey of Montgomery County, Maryland. Arch. Gen. Psychiatry. 1989;46:823–33.
[269] Dunnigan MGHarland WA, Fyfe T. Seasonal incidence and mortality of ischaemic heart-disease. Lancet. 1970;2:793–7.
[270] Hata T, Ogihara T, Maruyama A, Mikami H, Nakamaru M, Naka T, Kumahara Y, Nugent CA. The seasonal variation of blood pressure in patients with essential hypertension. Clin. Exp. Hypertens. 1982;A4:341–54.


In: Cardiac Arrythmia Research Advances ISBN: 978-1-60021-795-1 Editor: Lynn A. Vespry, pp. 137-158 © 2007 Nova Science Publishers, Inc.
Chapter V
Cardioembolism Prophylaxis in Non Valvular Atrial Fibrillation (NVAF):
Medical Treatment, Pacing and Beyond
F. Corea1*, MA.Abbas1,2, M.Cascelli3, S. Micheli4, M. Sessa1, S.Benussi5 and G. Comi1
1 U. Neurologica, Istituto di Neurologia Sperimentale (INSPE) Vita-Salute University, Istituto di Ricovero e Cura a Carattere
Scientifico (IRCCS) San Raffaele, Milano, Italy. 2 Sohag University, Sohag, Egypt.
3 U.O Anestesia e Rianimazione, Ospedale San Giovanni Battista, Foligno, Italy.
4 Neurologic Clinic, Department of Medical and Surgical Specialties and Public Health, University of Perugia, Italy. 5 Division of Cardiac Surgery, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS) San Raffaele, Milano, Italy
Abstract
The great relevance of electrical cardiac stimulation has been recognized since the 50s when the first successful cardiac resuscitation by external stimulation was reported. In the last decades all over the world, millions of subjects with cardiac arrhythmias had been treated with pacemakers (PMs). Cardioembolism, often due to supraventricular arrhythmias, is one of the major killers in cerebrovascular diseases. In, age-adjusted, industrialized population, cardioemboli have the highest incidence rates, highest case fatalities as well as recurrence rates. Large prospective randomised trials demonstrated that anticoagulation with cumarins reduces the risk of ischemic stroke in high risk patients with AF by nearly 70%. Despite clear guidelines, there is evidence that anticoagulation is under used in patients with atrial fibrillation in a variety of clinical
* Address for correspondence: FC Stroke Unit, Dip. Neurologia, Vita-Salute University; IRCCS San Raffaele, via Olgettina 48, 20132 Milano, Italy; tel +39022643-2813; fax +39022643-2951; e mail: [email protected]

F. Corea, MA.Abbas, M.Cascelli et al. 138
settings. Recent prospective clinical trials have demonstrated that more physiologic pacing mode (DDD) reduces the risk of atrial fibrillation (AF) compared to single chamber ventricular pacing (VVI) in patients with sinus node disease (SND). Previous studies have shown using PM diagnostic counter how, on a 5-year follow up, AF episodes have prevalence up to 40% in PM patients. Anticoagulation treatment for systemic embolic prevention should be considered in those patients who have a prior history of AF or device detected AF episodes. Unfortunately stroke prevention in pacemaker patients is far to be satisfactory according to recent surveys and should thereby be further optimised. PM patients are under close follow up, cardiac rhythm can be checked with feasible procedures thus guidelines need to be better attended.
A novel concept for prevention of embolic stroke is based on the use of metallic fine-wire tubular prosthesis, to avoid penetration of emboli originating from proximal sources into the internal carotid artery. Blood can flow through the ‘protected’ artery into the brain, whereas the migration of emboli to the brain is avoided.
Closing the Left Atrial Appendage (LAA) might be another potential alternative in subjects who cannot take anticoagulants because of contraindications. First attempts at LAA exclusion were reported by cardiac surgeons either during open heart surgery or with a thoracoscopic intervention. Other techniques consists in the deployment of a self-expandable nitinol cages. It is delivered via a transseptal sheath. Small anchors along the struts prevent from embolization. Recently developed surgical instruments now enables thoracoscopic approaches, facilitating extension of epicardial AF ablation and excision of the left atrial appendage to patients with isolated AF
Still under appraisement whether similar surgical procedures are cost effective with the medical treatments to prevent embolic events.
Introduction
Atrial fibrillation is characterized by normal QRS complexes occurring at a rapid and irregular rate in the absence of identifiable P-waves. The irregular ventricular response reflects arrival of atrial impulses at the atrio-ventricular node at times that may or may not correspond to the refractory period of the node from a previous discharge. Stroke volume is decreased during atrial fibrillation because the ventricles do not have sufficient time to fill optimally between cardiac cycles.[1]
Atrial fibrillation, an “old” arrythmia that was first identified in 1909, has assumed increasing importance as the global demographic tide results in a burgeoning population of elderly individuals.
The impact of atrial fibrillation on mortality and morbidity is substantial, as are the socioeconomic consequences in relationship to hospital admissions, chronic disease management and disabilities.[2]
Atrial fibrillation is considered as one of the three growing cardiovascular epidemics in the 21° century in conjunction with congestive heart failure, type II diabetes mellitus and the metabolic syndrome.[3]
The two terms currently used to describe AF, paroxysmal and chronic, require a time frame. It is proposed that if an AF episode lasts longer than 7 days, the condition should be considered chronic. For the first symptomatic, non-self-terminating episode that is fewer than 7 days long, the term recent onset AF may be used, or recent discovery if the AF is

Cardioembolism Prophylaxis in Non Valvular Atrial Fibrillation… 139
asymptomatic or if the duration cannot be determined. Attacks of paroxysmal AF may differ in their duration, frequency, and functional tolerance (figure 1).
Figure 1. Definitions from the statements of American College of Cardiology/American Heart Association/European Society of Cardiology (ACC/AHA/ESC) joint committee.
Epidemiology Pooled data from studies of chronic atrial fibrillation in North America, Britain and
Iceland suggest a prevalence of 0,5% to 1% in the general population.[4] In the Framingham study atrial fibrillation prevalence increases with age, from about 2%
in the general population, to 5 % in people older than 65 years, and 10% in people older than 75 years.[5].
There is a strong likelihood that the incidence and prevalence of atrial fibrillation may be substantially underestimated. Thirty percent of patients enrolled in the Cardiovascular Health Study and approximately 45% of patients in the Stroke Prevention in Atrial Fibrillation (SPAF-III) study had atrial fibrillation detected incidentally when electrocardiography was performed for an unrelated reason.[6]
The median age of patient is 75 years; approximately 70% of patients are between the age of 65 and 85 years, and 84% are older than 65 years.[7]

F. Corea, MA.Abbas, M.Cascelli et al. 140
From a population-based study in subjects older than 65 years the prevalence in men (9,1%) was greater than that in women (4,8%).[8]
In the Framingham study, after adjustment for age and other risk factors, atrial fibrillation developed in men at 1.5 times the rate in women.[5]
The bulk of our knowledge of the epidemiology of atrial fibrillation is based predominantly on white population. In the Cardio-vascular Health Study there was a trend toward a lower incidence of atrial fibrillation during follow-up in blacks, but they made up only 5% of the total population in that study.[9]
Atrial fibrillation, an independent risk factors for stroke, is associated with a four to five fold higher risk than in the unaffected population.[10]
This rhythm disorder is implication in approximately 75.000 strokes per year and is probably the major cause of embolic stroke[11]; emboli arising from the heart account for at least 20% of ischemic strokes.[12] Patients with paroxysmal or intermittent atrial fibrillation have annualized stroke rate (3.2%) similar to that in patients with chronic or sustained atrial fibrillation (3.3%).[13]
The yearly risk of stroke in all non-valvular atrial fibrillation patients varies depending on coexisting diseases but, in general, is approximately 5%.[14]
The coexistence of comorbid conditions (hypertension, diabetes, congestive heart failure, coronary artery disease and prior cardiac surgery) in patients with atrial fibrillation may compound the risk of stroke.
The risk of stroke attributable to atrial fibrillation increases with age and the propensity of the elderly for stroke may be related to a higher prevalence of comorbid conditions.[2]
Risk Factors for Stroke Risk factors for stroke may be categorized in non-modifiable biological factors (such as
age, gender, race/ethnicity); proatherosclerotic/prothrombotic factors (hypertension, diabetes, dyslipidaemia, other serologic and haemostasis factors); cardiac comorbidity (atrial fibrillation, congestive heart failure and coronary artery disease); lifestyle factors, which play an increasing role, e.g. smoking, physical inactivity, alcohol consuption. These traditional risk factors are extended by rapidly growing efforts in elucidation genetic backgrounds for stroke. Genetic polymorphisms of functionally or pathophysiologically important proteins are investigated in the setting of case-control-studies for their role as candidate genes.[15]
Concepts of the pathophysiology of stroke and atrial fibrillation implicate stasis and thrombus formation in a structurally abnormal and dilated atrium or ventricle.[16]
AF is not a putative risk factor for stroke but rather a “marker” for other conditions predisposing to stroke, including aortic atherosclerosis, cerebrovascular disease, mitral annular calcification or valvular prolapse in which platelet activation may play a larger role in the initiation of thrombus formation.[17]
Increased left atrial volume is associated with an incremental deterioration of diastolic function and provides further predictive information in regard to the development of atrial fibrillation and stroke. Since it is well established that atrial stretch and dilatation increases the vulnerability of the atrium to the development of atrial fibrillation, a logical focus of

Cardioembolism Prophylaxis in Non Valvular Atrial Fibrillation… 141
further investigation into the causes of atrial fibrillation will involve an understanding of the relationship between arterial compliance, diastolic function, atrial volume, and inflammation. In this respect, left atrial volume may be a surrogate or marker of multiple other processes that lead to the development of atrial fibrillation [18], and in turn left atrial volume may be a surrogate for arteriosclerotic vascular disease.[19]
Atrial fibrillation coexists with LV dysfunction in a significant proportion of the population with congestive heart failure (CHF). Atrial fibrillation is diagnosed in 10% to 35% of patients with CHF during the course of the disease and is related to the clinical severity of its symptoms.[20]
Congestive heart failure was a powerful independent predictor of the occurrence of AF in the Framingham study, in both symptomatic and asymptomatic LV dysfunction.[21]
Diastolic dysfunction is a common accompaniment of aging and is a precursor to hypertension, obesity, diabetes, and coronary artery disease.
Hypertension is a powerful independent predictor of stroke in patients with nonrheumatic AF.[22] In a recent large trial, a history of hypertension was strongly associated with findings of left atrial stasis and thrombi on transesophageal echocardiography[23] and the presence or absence of complex aortic plaque, which determined high or moderate risk of thromboembolism, respectively. Perhaps in some patients the presence of hypertension acts as a marker of a noncompliant atherosclerotic aorta, which increases the impedance to left atrial and left ventricular (LV) emptying, promoting chamber dilatation and stasis, in addition to the potential for atheroembolic cerebrovascular disease.[2]
Novel risk factors for atrial fibrillation are: inflammation C- reactive protein (a sensitive marker of inflammation); metabolic syndrome (is pro-inflammatory); diabetes; obesity and obstructive sleep apnea. In patients with sleep apnea, hypoxia induces pulmonary artery vasoconstriction and increased right-sided pressures which act as a stimulus for (atrial natriuretic peptide) ANP release; levels of which are elevated in atrial fibrillation.[24]
Lone AF occurs in the absence of structural heart disease, as determined by the physical examination, electrocardiography, chest radiography and echocardiography. The prevalence of lone AF depends on the age of the population under consideration and whether AF is paroxysmal or chronic; it ranges from 2% to 31%. The risk of stroke in subjects with lone AF is governed largely by the presence and extent of additional risk factors (age older than 60 years, history of hypertension, ect.).
In addition to age, chronicity may be a risk factor for stroke in the lone AF population. An explanation for chronicity as a risk factor may be provided by the echocardiographic documentation of increased left atrial dimensions in patients with chronic versus paroxysmal AF. An increased left atrial dimension previously has been shown to be a risk factor for stroke.[2]
Non Valvular Atrial Fibrillation and Stroke Prevention
Not all patients with AF benefit from thromboprophylactic treatment. The decision to
treat depends on the balance between the risk of thromboemboli without treatment and the

F. Corea, MA.Abbas, M.Cascelli et al. 142
risks of thromboemboli and hemorrhage with treatment in each patient, as well as the patient's willingness to accept the potential risks, costs, and inconvenience of treatment in order to possibly benefit.[25]
Strategies for reducing the risk of stroke and systemic thromboembolism in patients with AF have been studied in several randomized controlled trials over the past decade.
The choices of thromboprophylactic agents for atrial fibrillation include warfarin, which is the most effective but also the most risky treatment, and aspirin, which is less effective than warfarin but safer.[ 14]
The important independent prognostic factors for an increased risk of stroke among individuals with AF are increasing age, a history of previous TIA or stroke, hypertension, diabetes mellitus, and transthoracic echocardiographic evidence of moderate to severe left ventricular systolic dysfunction.[26] Echocardiographic evidence of left atrial enlargement and left atrial spontaneous echo densities ("smoke"), possibly indicative of stasis of blood, are also significant risk factors for stroke.[14]
The major risk factors for anticoagulant-associated intracranial hemorrhage include fragile intracranial blood vessels (previous symptomatic cerebrovascular disease, computed tomography brain scan evidence of small vessel disease ["leukoaraioisis"]), high blood pressure (poorly controlled hypertension) and excessive anticoagulation (INR > 3.5) or factors predisposing to it, such as confusion, dementia, inadequate anticoagulant monitoring, alcoholic liver disease and a tendency to falls.26 Increasing age is a risk factor for all of these risk factors, and is thus a potent risk factor for anticoagulant-associated hemorrhage.
Five large randomized controlled primary prevention trials have shown that, in people with chronic non-valvular AF, warfarin reduced the risk of stroke by about two-thirds (68%; 95% CI, 50%-79%; P < 0.001), from about 4.5% to 1.4% per year overall, with little increase in frequency of major bleeding (warfarin, 1.2%; control, 1.0%), or intracranial hemorrhage (warfarin, 0.3% per year; control, 0.1% per year).[27] This means that warfarin will prevent about 30 strokes per 1000 patient-years of treatment at a cost of at least two serious bleeding episodes per 1000 patients treated for one year. In the Cochrane Group Stroke Trials Register treatment with adjusted-dose warfarin to achieve INRs of 2 to 3 reduces stroke, disabling or fatal stroke, and death for patients with non-valvular AF. The benefits were not substantially offset by increased bleeding among these participants in randomized clinical trials. Limitations include relatively short follow up and imprecise estimates of bleeding risks from the selected participants enrolled in the trials. For primary prevention of stroke in AF patients, about 25 strokes and about 12 disabling or fatal strokes would be prevented yearly for every 1000 atrial fibrillation patients given oral anticoagulants (OACs).[28]
Three primary trials have shown that, in people with AF, aspirin reduced the incidence of stroke by 22% (95% CI, 2%-38%), from 5.2% (placebo) to 3.7% (aspirin) per year. Aspirin was not associated with any significant excess of intracranial hemorrhage (aspirin, 0.16%; control, 0.13%) or major extracranial bleeding (aspirin, 0.5%; control, 0.6%).[29] This means that aspirin might prevent about 10 to 20 strokes per 1000 patient-years of treatment, depending on the type of patient treated and their baseline risk of stroke, with little risk of major bleeding. A speculative interpretation of these data is that, in patients with AF, aspirin prevents strokes due to atherothromboembolism, but not cardiogenic embolism. This interpretation is based on the magnitude of the effect (a 20% relative risk reduction), which is

Cardioembolism Prophylaxis in Non Valvular Atrial Fibrillation… 143
very similar to the effect of aspirin in patients with symptomatic atherothromboembolism of the brain, heart and limbs.
In the Cochrane Group Stroke Trials Register aspirin appears to reduce stroke and major vascular events in patients with non-valvular AF similar to its effect in other high-risk patients (ie by about 25%). For primary prevention among AF patients with an average stroke rate of 4% per year, about 10 strokes would likely be prevented yearly for every 1000 AF patients given aspirin.[30]
Aspirin may be indicated for individuals in AF who are at fairly low absolute risk of stroke, such as those without any of the independent thromboembolic risk factors listed above, or those at risk of an anticoagulant-related hemorrhage which exceeds the risk of stroke (more than 1% per year).[14]
For patients with AF who are at high risk of stroke, adding aspirin (325 mg daily) to low-intensity, fixed-dose warfarin, adjusted to an INR of 1.2-1.5, was not as effective in preventing stroke or systemic thromboembolism as standard adjusted-dose warfarin therapy, maintaining an INR of 2.0-3.0 (event rates, 7.9% per year v. 1.9% per year, respectively; P < 0.0001), and there is no difference in the rates of major bleeding.[31]
Timing for anticoagulation in secondary stroke prevention need to be better understood according to recent metanalysis [12] (figure 2).
Study
or sub-category
Camerlingo
IST heparin any dose
TOAST
FISS bis
Total (95% CI)
OR (random)
95% CI
Favours treatment
0.1
Favours control
0.2 0.5 1 2 5 10
OR (random)
95% CI
0 . 4 9 [ 0 . 2 6 , 0 . 9 3 ]
0 . 9 0 [ 0 . 6 7 , 1 . 2 2 ]
1 . 2 3 [ 0 . 5 7 , 2 . 6 3 ]
1 . 0 6 [ 0 . 6 3 , 1 . 7 8 ]
0 . 9 5 [ 0 . 7 4 , 1 . 2 1 ]
Figure 2: Modified from Paciaroni et Al. metanalysis. Odds ratios (OR) for individual outcomes were calculated for each trial and data from all the trials were pooled using the Mantel-Haenszel method. In six trials anticoagulants were started within 24-48 hours after stroke onset while in one trial they were started within the first 3 hours. In this trial, death or disability were reduced by anticoagulant treatment (58.5% vs. 74.1%, OR=0.49, 95% CI: 0.26-0.93). In acute cardioembolic stroke, early anticoagulation is associated with a not significant reduction in recurrence of ischemic stroke, no substantial reduction in death and disability and an increased intracranial bleeding. The benefit observed in patients treated within 3 hours suggests the need for further trials on the efficacy of early administration of anticoagulants in acute cardioembolic stroke.
Current guidelines recommend oral anticoagulation for high-risk individuals with AF but these inherent limitations lead to substantial underprescribing, particularly in elderly patients at greatest risk. This has stimulated the development of new agents with improved benefit-risk profiles, such as ximelagatran, the first of the oral direct thrombin inhibitors, which has a

F. Corea, MA.Abbas, M.Cascelli et al. 144
wider therapeutic margin and low potential for drug interactions, allowing fixed dosing without anticoagulation monitoring. Ximelagatran has been evaluated for stroke prevention in AF in the Stroke Prevention using an Oral Direct Thrombin Inhibitor in Atrial Fibrillation (SPORTIF) program, the largest clinical trials of antithrombotic therapy for stroke prevention in AF to date. The phase III trials of ximelagatran in AF, SPORTIF III and V, found a fixed oral dose of ximelagatran (36 mg twice daily) comparable to dose-adjusted warfarin (INR 2.0 to 3.0) in preventing stroke and systemic thromboembolic complications among high-risk patients with AF. Results from the population of over 7000 patients in SPORTIF III and V demonstrate noninferiority of ximelagatran compared with warfarin. Data from SPORTIF III show an absolute reduction in stroke and systemic embolic events with ximelagatran compared with warfarin of 1.6% per year versus 2.3% per year, respectively ( P = 0.10). SPORTIF V further supports noninferiority between the two agents with an absolute risk reduction of 0.45%, well within the predefined noninferiority margin (95% confidence interval -0.13-1.03; P = 0.13). Although event rates for major bleeding did not differ significantly with ximelagatran versus warfarin in either study, combined rates for major and minor bleeding were significantly reduced with ximelagatran. The overall net clinical benefit, taking into account effects on stroke or systemic embolic events, major bleeding, and death, was also greater with ximelagatran compared with warfarin in both studies. Elevated serum transaminase enzymes were observed in approximately 6% of patients given ximelagatran in these trials. These typically occurred 1 to 6 months after initiating treatment and usually abated without clinical sequelae whether or not treatment was continued. Given the consistency of response, the favorable overall benefit-risk ratio and the convenience of fixed oral dosing, ximelagatran may increase the number of patients with AF eligible for anticoagulation and amplify the potential for prophylaxis against stroke.[32]
NVAF and Pacing Techniques Atrial fibrillation (AF) and subsequent embolic events are potential serious complications
in paced patients with sinus node disease (SND) (figure 3) [33]. Ventricular single chamber permanent cardiac pacing undoubtedly eliminates symptoms related to extremely low cardiac rate and bradycardia-related symptoms, but also contributes to increased morbidity due to onset of permanent atrial fibrillation (PAF)[34]. Dual-chamber pacemakers may be more efficient than ventricular pacemakers in improving quality of life and exercise tolerances and in reducing morbidity. Many studies have shown the superiority of atrial and dual chamber cardiac pacing in reducing atrial fibrillation risk and in preventing complications. As SND is the most frequent indication for permanent pacing, the investigation of the optimal pacing mode for these patients is important both clinically and economically [34].

Cardioembolism Prophylaxis in Non Valvular Atrial Fibrillation… 145
Figure 3. Dual-chamber pacing: The risk of AF increased by 1% for each per cent increase in ventricular pacing in the DDDR mode when compared with only 0.7% for each per cent increase in the VVIR mode.
AF is a common complication in patients with permanent pacemaker. Although its incidence is influenced by the presence of structural heart disease, hypertension, congestive heart failure, or AF before pacemaker implantation, the pacing mode may also have a significant influence on the development of AF [35]. Dual-chamber pacing preserves atrioventricular synchrony. However, in randomized trials comparing VVI(R) with DDD(R) pacing, AF is only slightly less frequent in the dual-chamber mode. This is most likely due to unnecessary ventricular pacing, which is frequent in dual-chamber pacing. At nominal values, dual-chamber devices usually do not permit intrinsic AV conduction but promote delivery of the ventricular stimulus at an inappropriate time in an inappropriate place. Programming of long AV delays facilitates spontaneous AV conduction but usually cannot completely avoid unnecessary ventricular pacing and causes other problems in the dual-

F. Corea, MA.Abbas, M.Cascelli et al. 146
chamber mode. Atrial septal lead placement can improve left-sided AV synchrony and promote spontaneous AV conduction. Programming of the AAI(R) mode seems superior to the dual-chamber mode but cannot be used if AV conduction is impaired intermittently or permanently. Therefore, dedicated algorithms enhancing spontaneous AV conduction in the dual-chamber mode are desirable for a large proportion of pacemaker patients.[35]
Classification of Pacemakers Pacemakers consist of a small, battery-powered electrical generator and one or more
electrodes (leads). In single-chamber pacemakers, the lead is positioned on the right ventricle or right atrium. The lead senses whether intrinsic depolarization has taken place within the heart. When this does not occur, an electrical impulse is sent from the generator to paced chamber via the lead and contraction is initiated. Dual-chamber pacemakers have two leads, one positioned on the right ventricle and one on the right atrium.
The North American Society of Pacing and Electrophysiology (NASPE) and the British Pacing and Electrophysiology Group (BPEG) jointly revised pacemaker nomenclature in 2002.21 This established the Generic Code for Anti-bradycardia Pacing. The Generic Code is composed of elements (‘positions’) describing: the chamber paced (position I), chamber sensed (position II), response to sensing (position III) and rate modulation (position IV) (see table 1).
Table 1. Adapted from Bernstein and colleagues.
Definition of generic pacing codes (NASPE/BPEG) Position I II III IV Category Chamber paced Chamber
sensed Response to sensing Rate modulation
Codes A = Atrium A = Atrium O = None O = None V = Ventricle V = Ventricle T = Triggered R = Rate-modulated D = Dual
(atrium and ventricle)
D = Dual (atrium and ventricle)
I = Inhibited D = Dual (triggered and inhibited)
Position II indicates the chamber where spontaneous depolarization is detected if it
occurs outside the pulse generator’s preset refractory periods. The action of the pacemaker in response to spontaneous cardiac depolarization is
described by position III. The pacemaker’s pulse may be inhibited (the escape interval is reset without pacing if a spontaneous beat is sensed) or triggered (with the emission of a pulse when it is sensed that no spontaneous beats have occurred).
Position IV describes the incorporation of an extrinsic sensor to provide ‘rate modulation’ or ‘rate responsiveness’.
Physiological pacing is a general attribute for any type of pacing that has the capacity of preserving the physiological AV synchrony. This is achieved by replicating as closely as

Cardioembolism Prophylaxis in Non Valvular Atrial Fibrillation… 147
possible the sequence of contraction started in the atrium and transmitted to the ventricle with appropriately calibrated timing. Dual-chamber and single atrial chamber pacing with rate-responsiveness are physiological pacing modes.
Dual-chamber pacing has steadily increased as a proportion of all pacemaker insertions in the past 10 years and accounted for 58.5% of the total in 2003. Use of dual-chamber devices has exceeded single chamber since 1995/96. Of dualchamber devices inserted in 2003, about half were rate responsive (DDDR) and half not (DDD). About 40% of implants were ventricular: 16.4% of the total were VVI and 24% VVIR. The use of atrial pacemakers was considerably less, only 1.1% of the total, and has fallen by about half in the past 10 years. The majority of pacemakers were inserted for heart block or SND (77%).
Definition and Etiology of SND SND is an irreversible dysfunction of the sinus node, a small area situated in the right
atrial wall composed of cells that depolarize spontaneously and act as the heart’s natural pacemaker. SND includes a spectrum of arrhythmias with diverse underlying mechanisms such as sinus bradycardia, sinus arrest, sinoatrial (SA) block, SND and the bradycardia–tachycardia syndrome. A failure in sinus activity may result in sinus pause or sinus arrest, i.e. failure of the atria to start a timely contraction. Sinus exit block occurs when depolarisation waves fail to travel across atrial tissues.
SND is mainly the result of chronic fibrotic degenerative processes or calcification of the sinus node and/or the surrounding atrial tissues. These processes become more common with increasing age and may occur over years. Commonly coexisting anatomical findings in SND are coronary arteriosclerosis, with associated ischemic heart disease (IHD) or calcification of the aorta.
Pacemaker Syndrome Pacemaker syndrome is a symptom complex related to the presence of a ventricular
pacemaker. It has been attributed to the superimposition of atrial and ventricular contractions. Pacemaker syndrome is predominantly associated with singlechamber ventricular pacing. However, it has been reported in dual-chamber pacing, despite the potential to programme AV delay in dual-chamber devices. Symptoms of pacemaker broadly suggest low cardiac output and may resemble congestive heart failure, such as dizziness, weakness and fatigue, shortness of breath on exertion or when lying flat, and ankle swelling.
Haemodynamic Consequences of VVI Pacing Leading to AF Adverse haemodynamic and electrophysiological effects of VVI pacing during sinus
rhythm have been well observed. Singlechamber ventricular pacing may predispose to chronic atrial fibrillation through different suggested mechanisms:

F. Corea, MA.Abbas, M.Cascelli et al. 148
1. Loss of AV Synchrony Adverse haemodynamic consequences of VVI pacing during sinus rhythm are most
prominent if retrograde conduction is present. Particularly, at a VA interval of 100 ms, there may be a strong ‘negative atrial kick’ caused by atrial contraction against closed AV valves. This may reduce cardiac output and lead to pacemaker syndrome due to reflexes causing a fall in peripheral vascular resistance, and it should also be noted that ventricular pacing with retrograde 1:1 conduction causes a strong increase in atrial pressure and regurgitation into the pulmonary veins. These so-called z-waves or ‘cannon waves’ may lead to a considerable distension of pulmonary veins, which may represent a potent trigger for AF. Even if no retrograde conduction is present, interference between sinus rate and VVI pacing rate leads to a periodicity in which P-waves shift until they appear after a ventricular pace, mimicking retrograde conduction. As focal electrical activity in the pulmonary veins and acute atrial stretch have been recognized as two of the most important AF triggers in patients with and without structural heart disease, it may be concluded that asynchronous ventricular pacing in the VVI mode with or without retrograde conduction is a potential trigger for AF induction.
2. Mitral Regurgitation
While permanent or intermittent atrial contraction against closed AV valves causes atrial/pulmonary venous distension as one trigger of AF, another AF trigger is represented by mitral regurgitation caused by right ventricular pacing [36,37,38,39] which can sometimes be reversed by dual chamber pacing [36, 38,]. Owing to mitral regurgitation, ventricular pacing leads to an elevation in pulmonary capillary wedge pressure and increases the risk of AF.
3. Neuroendocrine Reflexes
Elevated atrial natriuretic peptide levels observed in patients with VVI pacing may further document atrial pressure increase with the potential to induce AF. Likewise, it has been shown in animal and human studies that ventricular pacing reduces coronary blood flow, increases tissue norepinephrine levels, and deteriorates the relationship between left ventricular output and myocardial oxygen consumption [40]. By these mechanisms, VVI pacing may produce ischemia which may promote the development of AF.
4. Atrial Remodeling
Asynchronous ventricular pacing induces electrical and mechanical atrial remodeling, which may facilitate the induction of AF and thrombus formation in the left-atrial appendage.[40,41]
5. Comorbidity
Other factors that increase the problem is that ventricular pacemakers are mostly reserved for elderly patients, patients with more severe general diseases, or patients with a higher prevalence of paroxysmal atrial fibrillation. Even in series in which the overall prevalence of preimplant atrial fibrillation is reported as similar for patients with ventricular and physiological pacemakers, it seems likely that paroxysmal atrial fibrillation was significantly more severe (in terms of years of history or duration of each paroxysm) in patients who received ventricular pace-makers.

Cardioembolism Prophylaxis in Non Valvular Atrial Fibrillation… 149
AF in VVI and DDD Pacing In accordance with this picture of how VVI pacing may cause AF, retrospective and non-
randomized studies show a yearly AF incidence of 7% with VVI pacing in contrast to 2% in patients with AAI or DDD pacing [42]. Also, several large-scale randomized trials confirm that AF develops more frequently in VVI(R) than in DDD(R) pacing mode. However, in these studies, the absolute difference in AF development converges to 1.2% and is thus much smaller than expected, given the adverse effects of VVI pacing as outlined earlier in contrast to dual-chamber pacing which attempts to reproduce physiological atrioventricular pacing. For instance, in patients with sick sinus syndrome, the MOST trial showed little difference between VVIR and DDDR pacing for various clinical endpoints [43]. The development of AF differed (absolutely) by only 2.1%. However, patients required antibradycardia pacing for only 58% of the time in VVIR mode, whereas ventricular pacing was present for 90% of the time in patients randomized to DDDR pacing [43]. This is even more remarkable as only patients with sinus node disease were included; therefore, ventricular pacing was unnecessary in the vast majority of patients and was due to programming of a short AV delay. In a subanalysis of the MOST study, it looked as if ventricular pacing was even more deleterious in the DDDR mode than in the VVIR mode: The risk of AF increased by 1% for each per cent increase in ventricular pacing in the DDDR mode when compared with only 0.7% for each per cent increase in the VVIR mode. This observation poses the question why right ventricular pacing in atrioventricular synchronous or sequential pacing may be at least as harmful as asynchronous ventricular pacing [44,45].
AF, Pacing and Stroke Several large randomized clinical trials have established that AF, which commonly
occurs in patients with sinus node dysfunction, is associated with an annual risk of stroke of approximately 5%, which may be significantly lowered to 1.7% with appropriate anticoagulant therapy. Patients with AF had a 70% higher relative risk of stroke than patients without AF, even after adjustment for important clinical predictors. The most common indication for implantation of a permanent pacemaker is sick sinus syndrome. It is estimated that the yearly incidence of stroke in this population is approximately 6% to 10% [33,36-39,46]. Independent risk factors for stroke in paced patients are history of cerebrovascular disease, ventricular pacing mode, and history of paroxysmal atrial fibrillation; consequently, it would be appropriate to chronically anticoagulate patients with any of these risk factors.
Many studies have suggested that single-chamber ventricular pacing has a strong influence on the incidence of chronic atrial fibrillation and stroke [47,48). A significantly higher occurrence of cerebral ischemic events (stroke or transient ischemic attacks) in VVI paced patients was reported in previous studies, also many trials have suggested that physiologic pacing may decrease the incidence of AF [39,40,41,42] and significant reduction of cardiovascular mortality associated with DDD pacing has been observed in patients with sick sinus syndrome.

F. Corea, MA.Abbas, M.Cascelli et al. 150
Early observational studies of patients with sinus node dysfunction estimated the yearly incidence of stroke at 6% to 10% [33,49]. In a nonrandomized study of 507 patients paced for sinus node dysfunction, the actuarial incidence of stroke was 3% at one year and 5% at five years [50]. In the first small, randomized trial of physiologic pacing in sinus node dysfunction, the thromboembolic event was 11.5% in patients followed for a mean of 40 months [40]. In the MOST study, the incidence of stroke in the first year after implant was 2.2% (95% CI 1.6 to 2.9). The high use of antithrombotic therapy in the MOST study, particularly in patients with AF, may have contributed to the low stroke rate [51].
In the CTOPP study, where the annual rate of stroke was low (ventricular pacing _ 1.1%, physiologic pacing _ 1%) and only 42% of patients were paced for sinus node dysfunction, no association was found, but this may be due to short mean follow-up time or a small sample size.
In addition to atrial fibrillation as the mechanism linking ventricular pacing with embolic stroke, other factors must be involved in this association, because stroke is predicted by VVI pacing independent of atrial fibrillation. Alternative mechanisms may include the existence of ventriculoatrial conduction in the absence of atrial fibrillation, subclinical "atrial hypervulnerability," and short-lived, occult episodes of paroxysmal atrial fibrillation. A pooled analysis found no difference in rates of stroke between pacemaker subtypes, with 1% of individuals paced with dual chamber reporting stroke and 2% in ventricular pacing[52].
The role of antithrombotic therapy in the prevention of stroke in patients with AF has been assessed in a number of large multicenter trials [53]. Therapeutic anticoagulation is known to markedly reduce the risk of stroke in patients with AF [53]. The annual risk of stroke in patients without antithrombotic therapy ranged from 1% in those younger than 65 years to 8.1% in those older than 75 years with more than one risk factor, such as hypertension, prior stroke, or diabetes. By comparison, the annualized rate of stroke in those patients treated with antithrombotic therapy was between 1% and 1.7% [53]. On the basis of these studies, antithrombotic therapy is now recommended as primary prevention for ischemic stroke, except in those patients who are under age 65 years and have no risk factors [54,55]. Although patients paced for sinus node dysfunction represent a different population of patients than those with primary AF, antithrombotic therapy may influence their risk of stroke.
Follow up and Optimization of Cardiac Pacing Pacemaker implantation is only the initial phase in the lifelong management of the
patient with a pacemaker. The challenge of this treatment lies in the comprehensive follow up of the device. As the number of implanted devices increases so does the burden of follow up. This is compounded by increasing data provided by devices and increasing sophistication in programming therapy and detection algorithms. There are some general guidelines on pacemaker follow up provided by national organizations, but very little provided in the way of detail. This is reflected in the immense variation in the manner of pacemaker follow up both nationally and internationally. Like most medical interventions pacemaker follow up has

Cardioembolism Prophylaxis in Non Valvular Atrial Fibrillation… 151
to be tailored to the individual. The fundamental principles of pacemaker follow up are listed in table 2.
Table 2. Fundamental principles of pacemaker follow up optimization
• Evaluation of correct device function and patient safety (to national standards).
• Optimization of system function and maximization of device longevity.
• Aim to comprehensively troubleshoot pacemaker problems/complications.
• Provision of patient/family support and education.
• Appropriate storage of data.
• Scheduling of next visit or device replacement.
The frequency of pacemaker follow up varies from centre to centre. Follow up can be
divided into three phases: • Early surveillance: in most cases a first follow up after discharge from hospital
should be within four to six weeks. • Maintenance period: follow every six or 12 months. In the pediatric population this
should be at least every six months. • Intensified monitoring period: more intense follow up will be necessary as the device
approaches the end of its battery life. A history should be taken from all patients to identify whether there are likely to be any
pacemaker related problems or clinical problems that may be aided by alternate device programming. Specifically, change in symptoms such as presyncope, syncope, dyspnoea, lethargy, palpitations, and chest pain should be defined. A full medication review should be considered as part of the follow up process.
Electrogram Storage Most pacemakers have the ability to record electrograms along with annotated markers
when predefined events occur. Marker annotation allows an understanding of device behaviour. The real value is in the analysis of the recorded endocardial electrograms. Experience of endocardial electrograms is extensive from implantable cardioverter-defibrillators (ICDs) that document therapy events. Stored electrograms have provided the clinician with an invaluable tool in aiding clinical follow up of arrhythmias. Most devices now will allow a number or pre-programmed events to be recorded, varying from a few seconds to several minutes.
Each event may also include two sections: an onset recording, and post trigger period—that is, after detection criteria made. Recording the onset section greatly enhances arrhythmia diagnosis [56]. Activating the facility to record electrograms reduces battery longevity by only a small amount—for example, two days in a year. The recorded electrograms allow

F. Corea, MA.Abbas, M.Cascelli et al. 152
analysis of potentially non-symptomatic events, although the time of recording is made and subsequently can be correlated with symptom history.
Stored electrograms at the time of symptoms will establish whether the cause is an arrhythmia or device related problem. This allows the device to be used and the clinical data applied in a similar manner to an implanted loop recorder [57]. Additional asymptomatic stored electrograms may include prognostically significant ventricular arrhythmias or asymptomatic atrial arrhythmias that may indicate the need for formal anticoagulation. A limitation of stored electrograms is the compression of the data in order to record adequate electrogram sequences. This can produce less clear endocardial recordings in some cases.
Mode Switching and Atrial Arrhythmia Algorithms/Treatments The ventricular rate of DDD pacemakers is dependant on the atrial rate. Therefore, there
is the potential for very fast ventricular rates to be tracked by the pacemaker should the patient develop an atrial tachycardia. This is not an unusual occurrence in paced patients. A significant number of patients with sinus node disease have tachycardia–bradycardia syndrome and there is also an increasing incidence of atrial fibrillation with increasing age. It has been demonstrated that the incidence of atrial fibrillation in paced patients is as high as 13% with an overall risk of 2–3% per year developing atrial fibrillation [58].
Three specialized pacing algorithms have been developed for prevention of atrial fibrillation.
The First of These Is Preferential Atrial Pacing
The aim of the algorithm is to pace the atrium at a rate slightly above the sinus rate and thereby prevent abrupt pauses. The device periodically looks for sinus beats to ensure the rate is maintained just above the intrinsic rate and must have the ability to differentiate premature atrial complexes (PACs) from physiologic sinus beats.
The Second Algorithm Is the PAC Response
Upon detection of a PAC, the device initiates atrial pacing. Two variations on this theme exist. The first simply increases the pacing rate to above the preceding physiologic rate for a sustained period (usually several minutes). The second iteration is directed at abbreviating the post-extrasystolic pause by introducing paced atrial beats immediately after the PAC with progressively longer coupling intervals in order to gradually bring the rate back to the intrinsic rate.
The Third Type of Algorithm Is the ‘Post-Atrial Fibrillation Termination Response’
The atrium is most vulnerable to development of atrial fibrillation immediately after an atrial fibrillation episode has terminated as a consequence of the electrophysiologic remodeling (shortening and dispersion of the atrial refractoriness) that occurs during the atrial fibrillation episode. This algorithm invokes atrial pacing for a sustained duration immediately

Cardioembolism Prophylaxis in Non Valvular Atrial Fibrillation… 153
upon atrial fibrillation termination and then gradually returning to the sinus rate in order to suppress PACs and prevent bradycardia that may contribute to atrial fibrillation recurrence.
Mechanical Means for Reducing the Embolic Risk A new concept for prevention of embolic stroke is based on the use of a metallic fine
wire tubular device to avoid penetration of emboli originated from heart into the internal carotid artery. This self-expandable device (D-fence ®, Mindguard) is percutaneously deployed into the carotid bifurcation with its mesh covering the orifice of the internal carotid artery. Blood can flow unhindered through the “protected” artery into the brain, whereas the entry of embolic material is avoided. Emboli larger than 300 μm are rinsed away from the brain toward a non hazardous territory, namely, the external carotid circulation. [59,60]
A manufacturing industry had tested the safety of this device in hundreds of in vivo animal experiments. The implantation has been performed in some patients with atrial fibrillation who had high risk for stroke but could not take oral anticoagulation. Post procedure angiographic and subsequent ultrasound assessments demonstrated absence of blood flow compromise during a follow-up period of up to 7 months. Unfortunately clinical trials in Germany and Italy were interrupted because of increased risk of thrombosis of the devices.
Closing the left atrial appendage (LAA) might be another potential alternative in subjects who cannot take anticoagulants because of contraindications [61]. First attempts at LAA exclusion were reported by cardiac surgeons either during open heart surgery or at thoracoscopic intervention. The procedure called percutaneous left atrial appendage transcatheter occlusion (PLAATO) is a new implant to close the LAA by endovascular approach [63]. The device consists of a self-expandable nitinol cage. It is delivered via a transseptal sheath. Small anchors along the struts prevent from embolizing. After the implantation patients are placed on antiplatelet. The results of the dog model and the first clinical experience in humans have been very promising even if the procedure is complex.
Also the ease of patent foramen oval or atrial septal defect closure with the Amplatzer septal occluder technique encouraged also to use this device for LAA closure without general anesthesia [62].
Mini invasive left atrial approaches are today adopted in cardiac surgery. Recent advances in the understanding of the pathogenesis of AF and development of new ablation technologies enable surgeons to perform pulmonary vein ablation, create linear left atrial lesions, and remove the left atrial appendage rapidly and safely. Recently developed surgical instruments now enables thoracoscopic approaches, facilitating extension of epicardial AF ablation and excision of the left atrial appendage to patients with isolated AF and no other indication for cardiac surgery. [63] .

F. Corea, MA.Abbas, M.Cascelli et al. 154
Conclusion Unfortunately stroke prevention in NVAF / pacemaker patients is far to be satisfactory
according to recent surveys and should thereby be further optimized. PM patients are under close follow up, cardiac rhythm can be checked with feasible procedures thus guidelines need to be better attended.
Still to be evaluated in a larger population or randomized trial is whether similar surgical procedures such as mini invasive thoracoscopic ablation or the Amplatzer technique compares with the complex PLAATO. As well as if LAA closure is competitive with oral anticoagulation with warfarin or the new generation anticoagulants to prevent embolic events [64, 65]
References
[1] Robert K. Stoelting. The electrocardiogram and analysis of cardiac dysrhythmias. In Robert K. Stoelting (edit), Pharmacology and Physiology in Anestethetic Practice (Lippincott Williams and Wilkins, Philadel, Pennsylvania, 1999)
[2] Sumeet S. Chugh, MD, FAAC, Joseph L. Blackshear, MD, FACC, Win-Kuang Shen, MD, FAAC, Stephen C. Hammil, MD, FAAC, Bernard J. Gersh, MB, CHB, Dphil, FAAC. Epidemiology and Natural History of Atrial Fibrillation: Clinical Implications. Journal of the American College of Cardiology. 2001; 37(2): 371-378.
[3] Braunwald E. Shattuck Lecture. Cardiovascular medicine at the turn of the millennium: triumphs, concerns and oppoutunities. New England Journal of Medicine. 1997; 337: 1360-1369.
[4] Flegel KM, Shipley MJ, Rose G. Risck of stroke in non reheumatic atrial fibrillation. Lancet. 1987; 1:526-529.
[5] Wolf PA, Abbot RD, Kannel WB. Atrial fibrillation as an independent risk factor for strke: the Framinghan Study. Stroke. 1991; 22: 983-988.
[6] Page RL, Wilkinson WE, Clair WK, McCarthy EA, Pritchett EL. Asymptomatic arrythmias in patients with symptomatic paroxysmal atrial fibrillation and paroxysmal supraventricular tachycardia. Circulation. 1994; 89: 224-227.
[7] Feinberg WM, Blackshear JL, Laupacis A, Kronmal R, Hat RG. Prevalence, age distribution and gender of patiens with atrial fibrillation: analysis and implications. Arch. Int. Med. 1995; 155: 469-473.
[8] Furberg CD, Psaty BM, Manolio TA, Gardin JM, Smith VE, Rautaharju PM. Prevalence of atrial fibrillation in elderly subjects ( the Cardiovascular Health study). Am. J. Cardiol. 1994; 74: 236-241.
[9] Psaty BM, Manolio TA, Kuller LH, et al. Incidence of and risk factors for atrial fibrillation in older adults. Circulation. 1997; 96: 2455-2461.
[10] Cairns JA, Connolly SJ. Nonrheumatic atrial fibrillation: risk of stroke and role of antithrombotic therapy. Circulation. 1991; 84: 469-481.
[11] Wolf PA, D’Agostino RB, Belanger AJ, Kannel WB. Probability of stroke: a risk profile from the Framingham study. Stroke. 1991; 22: 312-318.

Cardioembolism Prophylaxis in Non Valvular Atrial Fibrillation… 155
[12] Paciaroni M, Agnelli G, Micheli S, Caso V. Efficacy and safety of anticoagulant treatment in acute cardioembolic stroke. Stroke. 2007;
[13] Hart RG, Pearce LA, Rothbart RM, McAnulty JH, Asinger RW, Halperin JL. Stroke with intermittent atrial fibrillation: incidence and predictors during aspirin therapy. Stroke Prevention in Atrial Fibrillation Investigators. J. Am. Coll. Cardiol. 2000; 35: 183-187.
[14] Grame JH. Non-valvular atrial fibrillation and stroke prevention. MJA. 2001; 174: 234-248.
[15] Khaw AV, Kessler Ch. Stroke: epidemiology, risk factors, and genetics. Hamostaseologie. 2006; 26(4): 287-297.
[16] Bogousslavsky J, Cachin C, Regli F, Despland PA, Van Melle G, Kappenberger L. Cardiac sources of embolism and cerebral infarction – clinical consequences and vascular concomitants: the Lausanne Stroke Registry. Neurology. 1991; 41: 855-859.
[17] The SPAF III Writing Committee for the Stroke Prevention in Atrial Fibrillation Investigators. Patients with nonvalvular atrial fibrillation at low risk of stroke during treatment with aspirin: Stroke Prevention in Atrial Fibrillation III study. J. Am. Med. Assoc. 1998;279:1273–7.
[18] Tsang TSM, Barnes ME, Gersh BJ, Bailey KR, Seward JB. Left atrial volume as a morphophysiologic expression of left ventricular diastolic dysfunction and relation to cardiovascular risk burden. American Journal of Cardiology. 2002;90(12):1284–1289.
[19] Tsang TS, Barnes ME, Gersh BJ, et al. Prediction of risk for first age-related cardiovascular events in an elderly population: The incremental valve of echocardiography. Journal of the American College of Cardiology. 2003;42:1199–1205.
[20] Dries DL, Exner DV, Gersh BJ, Domanski MJ, Waclawiw MA,Stevenson LW. Atrial fibrillation is associated with an increased risk for mortality and heart failure progression in patients with asymptomatic and symptomatic left ventricular systolic dysfunction: a retrospective analysis of the OLVD trials. Studies Of Left Ventricular Dysfunction. J. Am. Coll. Cardiol. 1998;32:695–703.
[21] Vaziri SM, Larson MG, Benjamin EJ, Levy D. Echocardiographic predictors of nonrheumatic atrial fibrillation: the Framingham Heart study. Circulation. 1994;89:724 –30.
[22] The SPAF III Writing Committee for the Stroke Prevention in Atrial Fibrillation Investigators. Patients with nonvalvular atrial fibrillation at low risk of stroke during treatment with aspirin: Stroke Prevention in Atrial Fibrillation III study. J. Am. Med. Assoc. 1998;279:1273–7.
[23] Zabalgoitia M, Halperin JL, Pearce LA, Blackshear JL, Asinger RW, Hart RG. Transesophageal echocardiographic correlates of clinical risk of thromboembolism in nonvalvular atrial fibrillation. Stroke Prevention in Atrial Fibrillation III Investigators. J. Am. Coll. Cardiol. 1998;31:1622– 6.
[24] Gersh BJ et al. The changing epidemiology and natural history of nonvalvular atrial fibrillation: clinical implications. Trans. Am. Clin. Climatol. Assoc. 2004; 115: 149-160.

F. Corea, MA.Abbas, M.Cascelli et al. 156
[25] Laupacis A, Albers G, Dalen J, et al. Antithrombotic therapy in atrial fibrillation. Chest. 1998; 114 (5 Suppl): 579S-589S.
[26] Atrial Fibrillation Investigators. Echocardiographic predictors of stroke in patients with atrial fibrillation. A prospective study of 1066 patients from 3 clinical trials. Arch. Intern. Med. 1998; 158: 1316-1320.
[27] Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomised controlled trials. Arch. Intern. Med. 1994; 154: 1449-1457.
[28] Aguilar MI, Hart R. Oral anticoagulants for preventing stroke in patients with non-valvular atrial fibrillation and no previous history of stroke or transient ischemic attacks. Cochrane Database Syst. Rev. 2005 Jul 20; (3): CD001927.
[29] Hart RG, Benavente O, McBride R, Pearce LA. Antithrombotic therapy to prevent stroke in patients with atrial fibrillation: A meta-analysis. Ann. Intern. Med. 1999; 131: 492-501.
[30] Aguilar MI, Hart R. Antiplatelet therapy for preventing stroke in patients with non-valvular atrial fibrillation and no previous history of stroke or transient ischemic attacks. Cochrane Database Syst. Rev. 2005 Oct 19; (4): CD001925.
[31] Adjusted-dose warfarin versus low-intensity, fixed-dose warfarin plus aspirin for high risk patients with atrial fibrillation: the Stroke Prevention in Atrial Fibrillation III randomised clinical trial. Lancet. 1996; 348: 633-638.
[32] Olsson SB, Halperin JL. Prevention of stroke in patients with atrial fibrillation. Semin. Vasc. Med. 2005; Aug 5(3): 285-292.
[33] Fairfax AJ, Lambert CD, Leatham A. Systemic embolism in chromic sinoatrial disorder. N. Engl. J. Med. 1976;295:190–2.
[34] Corea F, Tambasco N. Cardiac pacing: atrial fibrillation may go unrecognised. Lancet Neurol. 2005 May;4(5):265.
[35] Israel CW. The role of pacing mode in the development of atrial fibrillation. Europace. 2006;8:89–95.
[36] Bathen J, Sparr S, Rokseth R. Embolism in sinoatrial disease. Acta Med. Scand. 1978;203:7–11.
[37] Breivik K, Ohm OJ, Segadal L. Sick sinus syndrome treated permanent pacemaker in 109 patients. Acta Med. Scand. 1979;206:153–9.
[38] Rosenqvist M, Vallin H, Edhag KO. Clinical and electrophysiological course of sinus node disease: five-year follow-up study. Am. Heart J. 1985;109:513–22.
[39] Fisher M, Kase CS, Stelle B, Mills RM, Jr. Ischemic stroke after pacemaker implantation in sick sinus syndrome. Stroke. 1988;19: 712–5.
[40] Andersen HR, Thuesen L, Bagger JP, Vesterlund T, Thomsen PEB. Prospective randomized trial of atrial versus ventricular pacing in sick-sinus syndrome. Lancet. 1994;344:1523–8.
[41] Andersen HR, Nielsen JC, Thomsen PEB, et al. Long-term follow-up of patients from a randomized trial of atrial versus ventricular pacing for sick-sinus syndrome. Lancet. 1997;350:12010–6.

Cardioembolism Prophylaxis in Non Valvular Atrial Fibrillation… 157
[42] Lamas GA, Orav J, Stambler BS, et al. Quality of life and clinical outcomes in elderly patients treated with ventricular pacing as compared with dual-chamber pacing. N. Engl. J. Med. 1998;338:1097–104.
[43] Lamas GA, Lee KL, Sweeney MO for the MOST Investigators. Ventricular pacing or dual-chamber pacing for sinus-node dysfunction. N. Engl. J. Med. 2002;346:1854–62.
[44] Sweeney MO, Hellkamp AS, Ellenbogen KA, Greenspon AJ, Freedman RA, Lee KL et al. Adverse effect of ventricular pacing on heart failure and atrial fibrillation among patients with normal baseline QRS duration in a clinical trial of pacemaker therapy for sinus node dysfunction. Circulation. 2003;107:2932–37.
[45] Tse HF and Lau CP, Prevalence and clinical implications of atrial fibrillation episodes detected by pacemaker in patients with sick sinus syndrome. Heart. 2005;91: 362-364
[46] Sutton R, Kenny RA. The natural history of sick sinus syndrome. Pacing Clin. Electrophysiol. 1986;9:1110–4.
[47] Santini M, Alexidou G, Ansalone G, Cacciatore G, Cini R, Turitto G. Relation of prognosis in sick sinus syndrome to age, conduction defects and modes of permanent cardiac pacing. Am. J. Cardiol. 1990;65:729-735.
[48] Hesselson AB, Parsonnet V, Bernstein AD, Bonavita G. Deleterious effects of long-term single-chamber ventricular pacing in patients with sick sinus syndrome: the hidden benefits of dualchamber pacing. J. Am. Coll. Cardiol. 1992;19:1542-1549.
[49] Rosenqvist M, Vallin H, Edhag KO. Clinical and electrophysiological course of sinus node disease: five-year follow-up study. Am. Heart J. 1985;109:513–22.
[50] Sgarbossa EB, Pinski SL, Maloney JD, Simmons TW, Wilkoff BL, Castle LW et al. Chronic atrial fibrillation and stroke in paced patients with sick sinus syndrome. Relevance of clinical characteristics and pacing modalities. Circulation. 1993;88:1045–53.
[51] Greenspon AJ, Hart RG, Dawson D, Hellkamp AS, Silver M, Flaker GC, Schron E, Goldman L, Lee KL, Lamas GA, for the MOST Study Investigators. Predictors of Stroke in Patients Paced for Sick Sinus Syndrome. J. Am. Coll. Cardiol. 2004;43:1617–22.
[52] Castelnuovo E, Stein K, Pitt M, Garside R, Payne E. The effectiveness and cost-effectiveness of dual-chamber pacemakers compared with single-chamber pacemakers for bradycardia due to atrioventricular block or sick sinus syndrome: systematic review and economic evaluation. Health Technol. Assess. 2005 Nov;9(43):iii, xi-xiii, 1-246.
[53] Atrial Fibrillation Investigators. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Arch. Intern. Med. 1994;154:1449–57.
[54] Goldstein LB, Adams R, Becker K, et al. Primary prevention of ischemic stroke: a statement for healthcare professionals from the Stroke Council of the American Heart Association. Circulation. 2001;103:163–82.
[55] Hart RG, Bailey RD. An assessment of guidelines for prevention of ischemic stroke. Neurology. 2002;69:977–82.

F. Corea, MA.Abbas, M.Cascelli et al. 158
[56] Nowak B, Sperzel J, Rauscha F, et al. Diagnostic value of onset-recordings and marker annotations in dual chamber pacemaker stored electrograms. Europace. 2003;5:103–9.
[57] Machado C, Johnson D, Thacker JR, et al. Pacemaker patient-triggered event recording: accuracy, utility and cost for the pacemaker follow-up clinic. Pacing Clin. Electrophysiol. 1996;19:1813–8.
[58] Lamas GA, Pashos CL, Normand SL, et al. Permanent pacemaker selection and subsequent survival in elderly Medicare pacemaker recipients. Circulation. 1995;91:1063–9.
[59] Grad Y, Vermani R, Nishri B, Lieber B B, Assaf Y, Schneiderman J, et al. A new permanent arterial filtration device for embolic stroke prevention- the diverter. Cerebr. UASC Dis. 2002; 13(suppl 3):48.
[60] Grad Y, Nishri B, Tanne D, Lieber BB, Yodfat O. The diverter –embolic stroke prevention using a new permanent arterial filtration device. ASAIO. 2002; 48(3):199.
[61] Ostermayer S, Reschke M, Billinger K, Trepels T, Buschek F, Bayard Y, Sievert H. Percutaneous closure of the left atrial appendage. J. Interv. Cardiol. 2003; 16(6):553–556.
[62] Meier B, Palacios I, Windecker S, Rotter M, Cao QL, Keane D, et al. Transcatheter left atrial appendage occlusion with Amplatzer devices to obviate anticoagulation in patients with atrial fibrillation. Catheter Cardiovasc. Interv. 2003; 60(3):417–422.
[63] Benussi S. Treatment of atrial fibrillation. Eur. J. Cardiothorac. Surg. 2004 Dec;26 Suppl 1:S39-41; discussion S41.
[64] Bornstein N, Corea F, Galllai V, Parnetti L. Heart-brain relationship: atrial fibrillation and stroke. Clin. Exp. Hypertens. 2002 Oct-Nov;24(7-8):493-9.
[65] Corea F, Spinelli M, Tambasco N, Silvestrelli G, Parnetti L. Secondary prevention of cardioembolic stroke: oldest and newest promises. Clin. Exp. Hypertens. 2006 Apr-May;28(3-4):413-20.

In: Cardiac Arrythmia Research Advances ISBN: 978-1-60021-795-1 Editor: Lynn A. Vespry, pp. 159-175 © 2007 Nova Science Publishers, Inc.
Chapter VI
Management of Wolff-Parkinson-White Syndrome
Béatrice Brembilla-Perrot * Cardiology, CHU of Brabois, 54500 Vandoeuvre, France
Abstract
Sudden death (SD) might complicate the follow-up of patients with the Wolff-Parkinson-White syndrome (WPW) and might be the first event in patients with asymptomatic WPW. In these last patients, 7 to 63 year old, the reduction of the risk of life-threatening arrhythmias event by accessory pathway (AP) radiofrequency (RF) ablation was reported in 2003.
The risks of SD are increased in some clinical situations. Noninvasive studies are unable to predict correctly the risk of SD. The electrophysiological study (EPS) is the best means to detect the risk of life-threatening arrhythmias and evaluate the nature of the symptoms
The EPS methods used to study the WPW are well-defined. The maximal rate of conduction through the AP is evaluated and programmed atrial stimulation is used to determine the AP refractory period and to induce a tachycardia. These methods are performed in control state and repeated in adrenergic situation either during exercise test or during a perfusion of isoproterenol. The results of EPS differ with the methods used by authors. The incidence of atrial fibrillation (AF) induction is lower in transesophageal studies than in intracardiac studies. The incidence of atrioventricular re-entrant tachycardia (AVRT) induction is similar with both routes of study, low in asymptomatic patients (15%) and high in symptomatic patients (more than 80%). The induction of AF rapidly conducted through the AP (> 240 beats/min in control state, > 300 b/min after isoproterenol) is the sign of a WPW at risk of life-threatening arrhythmias, but the induction of AVRT is now also considered in association with the AP refractory period as a risk factor. The electrophysiological data differed according to the age of the patient with a shorter AP refractory period and a lower risk of AF induction in young patients
* Address for reprints :B Brembilla-Perrot; Cardiologie; CHU de Bravíos; 54500 Vandoeuvre; France; Tel : (33) (0) 383153142; Fax : (33) (0) 3 83154226; E-mail : b.brembilla-perrot@chu-nancy. fr

Béatrice Brembilla-Perrot 160
than in adults but the total number of potentially dangerous forms did not change significantly during the life.
AP RF ablation is now considered the first line of treatment of symptomatic patients and asymptomatic patients with inducible rapid tachycardia.
Some controversies still exist as the limits of age to indicate EPS in asymptomatic patient, classically 6– to 35 years, but older adults and elderly have still a risk of serious arrhythmia as the first event and the minimal age to indicate AP RF ablation because of the risks of the procedure in young children.
Keywords: Wolff-Parkinson-White syndrome, sudden death, Electrophysiologic study. The Wolff-Parkinson-White syndrome (WPW) is associated with a risk of
atrioventricular re-entrant tachycardia, but a patient with a preexcitation syndrome on ECG may be also asymptomatic. The main problem is that some of these asymptomatic patients or those with re-entrant tachycardia may be at risk of sudden death. The risk is very low, but at the time of the curative treatment of Wolff-Parkinson-White syndrome (WPW) by accessory pathway radiofrequency ablation [1, 2], it is particularly important to detect the forms at risk of sudden death. Sudden death in WPW syndrome is related to the degeneration of atrial fibrillation with high ventricular rates into ventricular fibrillation (figure 1). Some data are clear, but many controversies still persist.
Figure 1. transformation of a rapid atrial fibrillation into ventricular fibrillation.

Management of Wolff-Parkinson-White Syndrome 161
What Is Known in Wolff-Parkinson-White Syndrome
1) Natural History of WPW (table 1)
The risk of sudden death in the WPW syndrome is reported as relatively high in old
studies in symptomatic patients [3, 4] (1.5%), but is considered as low in asymptomatic patients [5-7]. A recent study [8] reports a sudden cardiac death risk of 0.02%/patient/year.
Previous studies [9, 10] have shown that ventricular fibrillation can be the first event of the Wolff-Parkinson-White syndrome. In the studies of Turner Montoya [9] and Timmermans [10], ventricular fibrillation was the first manifestation of the WPW syndrome in respectively 26 and 53% of their series. The studies in patients with aborted sudden death indicated that in most of these patients, atrial fibrillation with a rapid conduction over the accessory pathway is the main finding (table 2).
Table 1. Natural history of WPW syndrome
Prevalence in population: 1/1000 Before one year: spontaneous disappearance 50 % Asymptomatic patient: risk of sudden death 1 to 2 % (0.02 %/patient/an) Asymptomatic patient with inducible rapid atrial fibrillation: risk of sudden death: 7 %
Table 2. Data of patients resuscitated of sudden cardiac arrest in WPW
(AP = accessory pathway)
Male 85 % No symptoms before event: 50 % Adrenergic event at the time of event: sport+++, stress, post-operative period, fever… Inducible rapid atrial fibrillation (RR < 250 in control state, < 200 ms after isoproterenol) at electrophysiological study Minors factors : multiple AP’s, septal location, digitalis, associated heart disease
2) Methods of Evaluation • The pattern of WPW syndrome on 12 lead ECG provides some not specific
informations: the intermittent WPW is more frequently benign than permanent WPW. Posteroseptal location is more frequently noted in patients at risk of rapid arrhythmias [9, 10]. When several patterns of preexcitation syndrome are noted, multiple accessory pathways can be present and often the sign of a possible malignant form.
• Several non invasive studies were proposed but their diagnosis value is low:

Béatrice Brembilla-Perrot 162
The abrupt disappearance of WPW syndrome during an exercise stress testing was proposed as a sign of long refractory period of accessory pathway [11-13]; however the abrupt disappearance syndrome rarely is observed, even in patients without risk of rapid arrhythmias; more, it can be noted in patients with a short accessory period refractory period [14].
Pharmacological tests were used several years ago; the disappearance of the pattern of WPW syndrome after the injection of a class I antiarrhythmic drug was reported as a sign of long refractory period of the accessory pathway [15]; however, many false positive tests were reported [16].
• Electrophysiologic study appears as the most reliable method to establish the prognosis of WPW syndrome [17].
Patients might be studied by transesophageal route [18, 19] or intracardiac route. The
first route is indicated in asymptomatic patients and the second in symptomatic patients to perform the catheter ablation of the accessory pathway in a second time; the advantages of esophageal route is that the patient is not hospitalized and is leaving hospital after electrophysiologic study.
Electrophysiologic studies in WPW syndrome should performed in the room used for electrophysiology, with an external defibrillator ready to be used, because a ventricular fibrillation can be induced in asymptomatic or symptomatic patients [20].
Surface electrocardiograms and esophageal or intracardiac electrogram are simultaneously recorded on paper at speeds of 25 or 100 mm/sec. Cardiac stimulation is performed with a programmable stimulator which is connected to a pulse amplifier that can deliver pulses at width of 16 ms with a 29 mA output in the case of esophageal stimulation. But esophageal stimulation can be now performed with the same stimulator that stimulator used for intracardiac study, a biphasic stimulator which delivers pulses of 8 to 20 mA and up to 10 ms duration. For a simple electrophysiological study, only one catheter is required: a bipolar silicone esophageal lead or one bipolar intracardiac catheter. A multipolar catheter electrode is used for the mapping of left atrium in patients who need a catheter ablation of the accessory pathway.
The classical protocol is as following: • Incremental atrial pacing is performed until second degree atrioventricular block
occurred. The maximal rate of 1/1 conduction trough the accessory pathway is noted. • Programmed atrial stimulation at a basic cycle length of 600 and 400 ms with the
introduction of one and two extrastimuli is performed: the disappearance of WPW syndrome indicates the accessory pathway refractory period. The method also is used to induce a supraventricular tachycardia, generally an orthodromic tachycardia, rarely an antidromic tachycardia or an atrial tachycardia or fibrillation.
• These data should be studied under adrenergic situations, except in patients who have a form at risk of sudden death in control state. Two methods are used: atrial pacing might be repeated during an exercise testing [21, 22], which is the most physiological situation, but is difficult to perform. Many authors prefer the infusion

Management of Wolff-Parkinson-White Syndrome 163
of isoproterenol, a beta-adrenergic drug and which is easier to use during an electrophysiologic study. Isoproterenol (0.02 to 1 µg.min-1) is infused to increase the sinus rate to at least 130 beats.min-1 and the pacing protocol is repeated [21-23].
At the end of the protocol, using the following definitions, the prognosis of WPW
syndrome can be established: using the results noted in patients with WPW and aborted sudden death, the electrophysiological characteristics of the patients at risk of sudden death are perfectly known.
• Sustained atrial fibrillation or reciprocating tachycardia is defined as a tachycardia
that is longer than 1 minute. The exact duration of induced tachycardia to be considered as pathological is still controversed and varies from 30 sec up to 5 minutes [24].
• Conduction over the accessory atrioventricular connection is evaluated by the measurement of the shortest atrial cycle length at which there is 1 to 1 conduction over the accessory connection and the shortest atrial tachycardia cycle length at which there is 1 to 1 conduction over the accessory connection.
• The Wolff-Parkinson-White syndrome is considered as representing a risk of sudden death when the following association is noted: sustained atrial fibrillation is induced and the shortest RR interval between preexcited beats is less than 250 ms in the control state in adults, less than 220 ms in children [25] or less than 200 ms during isoproterenol infusion [26].
• Pappone et al consider all patients with inducible re-entrant tachycardia or other arrhythmias at risk of events [27].
3) Results of Electrophysiological Studies • The exact nature of the prexcitation syndrome is assessed. Most of the WPW
syndromes are related to a atrioventricular accessory connection or Kent bundle: the degree of preexcitation increases during premature atrial stimulation until the refractory period of accessory pathway is reached. Sometimes, the preexcitation syndrome is related to a nodoventricular accessory pathway or Mahaim bundle; the degree of preexcitation remains unchanged during premature atrial stimulation.
• The accessory pathway refractory period depends on the driven cycle length. The more it is short, the more also accessory pathway refractory period decreases.
• Beta adrenergic stimulation results in shortening of the anterograde accessory pathway refractory period and in increasing in ventricular rates during atrial pacing and during atrial fibrillation [28].
• Atrial fibrillation is easily induced during intracardiac studies by salvos of rapid atrial stimulation and is not specific [29]. The induction of an atrial fibrillation by intracardiac programmed stimulation is obtained in 27 % [21, 30], 41 % [24], 56 % [28] or 75 % [24] of the patients, according to the studies, in asymptomatic patients and in patients with only documented reentrant tachycardia; atrial fibrillation is

Béatrice Brembilla-Perrot 164
induced in 95 % of those with documented atrial fibrillation [24]. The important variations of the incidence of induced atrial fibrillation depends on the technique of programmed stimulation, on the interpretation of the duration of induced arrhythmia and on the use of isoproterenol infusion or other means to reproduce the effects of adrenergic stimulation. In our experience, the induction of an atrial fibrillation by transesophageal pacing has a best clinical significance [29]: the induction is rare from 10 to 30 % according to the age in patients without documented atrial fibrillation and remained sensitive to induce atrial fibrillation in those with documented atrial fibrillation (95 %). The incidence of atrial fibrillation induction also depends on the presence of an associated heart disease and the age of the patient: the induction of atrial fibrillation is rarely noted in children younger than 10 years, is induced in 20 % of teenagers and adults without heart disease and becomes relatively frequent in elderly patients (31%) [31].
• Ventricular tachyarrhythmias also are easily used in asymptomatic or symptomatic patients by programmed ventricular stimulation and are not specific in patients with WPW syndrome: the induction of a ventricular fibrillation is noted in 4 % of WPW syndrome and the induction of nonsustained multiform ventricular tachycardia in 37 % of them [32].
• Antidromic tachycardia which is a reciprocating tachycardia using the accessory pathway for the anterograde conduction and the normal AV conduction system for the retrograde conduction is a rare finding (5%), more frequently noted in young patients with a good retrograde normal VA conduction or in patients with several accessory pathways and seems more frequent in patients at risk of rapid arrhythmias.
• Orthodromic tachycardia which is a reciprocating tachycardia using the normal AV conduction system for the anterograde conduction and the accessory pathway conduction for the retrograde conduction, is rarely induced in asymptomatic patients (less than 10%) [33, 34], but represents the most frequent tachycardia of symptomatic patients complaining tachycardia and palpitations (90 %) [24] (figure 2).
• The incidence of forms considered at risk of rapid arrhythmias (figure 3) is similar in patients with symptomatic and asymptomatic patients and concerns 10 % of the total population with WPW syndrome [33, 34], independently on the age of the patient [31]. The clinical significance of the electrophysiological form at risk of sudden death in asymptomatic patients was controversed until Pappone et al report a decrease of rapid arrhythmias in asymptomatic patients and with inducible tachycardia, treated by the preventive ablation of the accessory pathway compared to those who were not treated [35, 36]. Previous studies using the intracardiac evaluation of WPW syndrome noted a low incidence of adverse events during a mean follow-up of 4 years [37, 38].
More the presence of syncope could not increase the risk to find a potential dangerous
form in adults [39]; in young patients (less than 25 years) the significance of syncope seems different and associated with occurrence of atrial fibrillation with a rapid ventricular response (sensitivity 64 %, specificity 100 %) [40]; we reported also recently a high incidence of

Management of Wolff-Parkinson-White Syndrome 165
malignant forms in patients with syncope; other patients had syncope directly related to reciprocating tachycardia [41].
Figure 2. induction of AVRT, the most frequent tachycardia in WPW syndrome.
Figure 3. Induction of antidromic tachycardia in control state (220 b/min).

Béatrice Brembilla-Perrot 166
4) Indications of Electrophysiological Studies in WPW (table 3) • The indications of electrophysiological studies are now large in symptomatic
patients, complaining of frequent sustained tachycardias, who require generally during the same procedure and in a second time the catheter ablation of accessory pathway. The study should be performed by catheterism.
• In patients with syncope and no documented tachycardias, electrophysiological study is required and might be performed initially by transesophageal route.
• In patients who have a documented rapid or syncopal atrial fibrillation, electrophysiological study is not indicated, because the catheter ablation of the accessory pathway is recommended. The location of the Kent bundle is easier in sinus rhythm and the induction of an atrial fibrillation should be avoided.
• In asymptomatic patients, the indications of electrophysiological study are more debatable [42]. At first, if the study is indicated, esophageal route should be preferred, because the probability to find a form at potential risk of sudden death remains rare (10 %). Most of the patients have a low-risk WPW syndrome. The main interest is to allow the patients in 90 % of cases to continue their activities in presence of an electrophysiological form without signs of risk of rapid atrial arrhythmias. Some indications of electrophysiological study are actually recommended: most of sudden deaths have the peculiarity to occur during exercise [43]. Because of the important development of sports from the infancy to the elderly, it is important to detect those patients with WPW at risk of sudden death who practice a sportive activity [44]; the indication generally, begins after 10 years, because the risk of induction of a rapid atrial fibrillation is very low and the level of sport still limited. In adults, only those who practice a sport at a high level (for example bicycle) are studied. The competitive athlete should be studied in all ranges of age. The study is also recommended in professions with a high level of sportive activity (policeman, soldier, fireman…)
Table 3. indications of esophageal or intracardiac electrophysiologic study (EPS)
(AS : anteroseptal, AVRT : atrioventricular re-entrant tachycardia)
Esophageal EPS Intracardiac EPS (before ablation) Asymptomatic patient 8-35 years Documented rapid tachyarrhythmia Asymptomatic patient > 35 ans : sportive activity, job at risk, before surgery
Frequent and symptomatic AVRT (after 10/12 years)
Limited symptoms ; possible AS AP location Atypical symptoms (syncope without tachycardia)

Management of Wolff-Parkinson-White Syndrome 167
5) Treatment of WPW
Methods • The radiofrequency ablation of the accessory pathway is currently used since more
than 15 years [1, 2]. The success is obtained in 90 % of cases in left lateral or posteroseptal accessory pathway location. Generally left sided accessory pathway are reached by retrograde aortic approach, but sometimes a left lateral pathway can be only reached by transseptal approach. In the case of a right lateral accessory pathway occasionally associated with Ebstein’anomaly, the risk of failure is important (50 %) because the catheter is not stable [45]. The location of accessory pathway in anteroseptal position remains associated with a high risk of complete atrioventricular block and the ablation could require the use of cryoablation. At least, some accessory pathways can not be successfully treated by the endocardial application of radiofrequency energy [46].
As in all the procedures of catheterism, some complication may occur either related to
the radiation exposure or to the puncture with a risk of haematoma, aneurismal varix, thrombosis or pericardial infusion; the radiofrequency current application is associated with a risk of cardiac tamponade, coronary artery stenosis, atrioventricular block or embolic events [47, 48].
• The medical treatment still should be considered in some patients [49]; all class I
antiarrhythmic drugs had been shown to increase the accessory pathway refractory period Isoproterenol reverse their effects and the adjunction of betablokers is useful either to prevent this effect and to avoid the exercise-related tachycardia. Isoproterenol test was previously used to verify the efficacy of antiarrhythmic drug before the time of catheter ablation of accessory pathway. The loss of efficacy of some antiarrhythmic drugs was demonstrated after isoproterenol administration [50].
Antiarrhythmic drugs are also the first line of treatment in acute arrhythmias related to
WPW. Ca blockers and digitalis are prohibited in this indication because they can precipitate the occurrence f a ventricular fibrillation in patients with atrial fibrillation.
Indications (table 4)
Radiofrequency ablation of accessory pathway is now considered as the first line of treatment of symptomatic patients and asymptomatic patients with inducible rapid tachycardia [51, 52].
Pappone et al reported for the first time, the interest of prophylactic ablation of accessory pathway [35, 36] in asymptomatic Wolff-Parkinson-White syndrome when atrioventricular reciprocating tachycardia or atrial fibrillation was induced; they initially reported a study in 212 patients with asymptomatic Wolff-Parkinson-White syndrome aged 7 to 63 years; 3 deaths were reported in young adults (21, 22 and 25 years old). Then they reported life threatening arrhythmias in 2 children among 60, 5 to 12 year old considered as having high risk for arrhythmias [27]. All these life threatening arrhythmias occurred in control groups

Béatrice Brembilla-Perrot 168
and none occurred in the patients in whom prophylactic catheter ablation was performed. Catheter ablation was also recommended by Vignati [53] in only symptomatic children older than 12 years of age.
The risk of atrial fibrillation frequently persists in adults aged more 50 years after the ablation of the accessory pathway and these patients should be followed [54].
Antiarrhythmic drugs are indicated in symptomatic patients who refuse the ablation, in symptomatic patients with an anteroseptal accessory pathway, in patients in whom catheter ablation has failed, in young children in whom the spontaneous disappearance of the accessory pathway can be expected and in children of small size or anxious who need a general anesthesia to perform the catheterism. The complications of ablation are more frequent in pediatric population than in adults [47, 48].
Table 4. Treatment indications (AF : atrial fibrillation)
Ablation Medical treatment No treatment Spontaneous ou inducible rapid AF Child < 10/12 years No induced tachycardia Recurrent or very symptomatic AVRT AS AP location Ablation failure
Controversies 1) The limits of age for the indications of the electrophysiological study in asymptomatic
patient are discussed; classically the study is recommended in patients aged from 6 to 35 years [27].
If these indications are largely admitted in teenagers and adults less than 40 years, the indications in children or elderly are more controversial:
• In children, the intracardiac study requires a general anesthesia in those younger than
10-12 years. The data of electrophysiological study differ from the adults: the conduction in accessory
pathway and normal AV conduction system is more rapid without probably clinical significance: in the study of Bromberg [25] a cycle length < 220 ms in basal state is considered at risk of severe arrhythmias; the value of less than 240 ms is retained by Pappone [36] in children less than 18 years; the value of less than 250 ms is admitted as a sign of a dangerous form in adults. More, the spontaneous increase in conduction velocity in accessory pathways with age was reported in children and the disappearance of the Wolff-Parkinson-White syndrome can be expected, but this is inconstant and not predictable [55]. The induction of atrial fibrillation by intracardiac electrophysiologic study is particularly high in young children [56] and therefore difficult to interpret. We recommend the esophageal route, which limits the induction of atrial fibrillation in children and can be used early in life [57].
However, some sudden deaths as the first event were reported in children [25, 33]. Sarrubi [56] reported this event in a child 8 year-old. In the study of Pappone [36] the

Management of Wolff-Parkinson-White Syndrome 169
youngest child, who had previously spontaneous episodes of rapid atrial fibrillation on Holter monitoring and died suddenly, was 10 year-old. In our experience, the youngest asymptomatic child who died suddenly was 12 year-old [20]. Also, the indications should be large in children competitive athlete and in all children [58].
• In elderly, the shortest atrial pacing cycle length with 1=1 anterograde conduction
via the bypass tract increased progressively with age [59-62]. However, the propensity for atrial fibrillation was shown to be higher in older patients compared to younger patients [63]. While the exact mechanism is uncertain, degenerative changes associated is the most commonly proposed mechanism and the dispersion of atrial refractoriness increases progressively with age [63]. The risk to have a severe arrhythmia as the first manifestation of WPW syndrome in an old patient was previously reported [64, 65]. High level sportive activity is rare in elderly, but other causes for adrenergic tone increase might be encountered: for example, an important surgery was the cause of the development of a ventricular fibrillation of a 72 year old asymptomatic patient old in our experience [20].
Therefore, because of the increase of the sport in all ranges of age and in particularly in
young children or after 60 years, the risk of occurrence of a potentially severe arrhythmia in an asymptomatic WPW patient should be not underestimated. The reliability and the simplicity of transesophageal study in WPW permits to easily detect these forms at risk of severe arrhythmia.
• The minimal age to indicate the accessory pathway radiofrequency ablation is
discussed, because the risks of the procedure in young children are higher than in adults [66] with a radiation exposure which should not be underestimated [67].
The relatively low risk of clinical events, except in children with syncope and
tachycardia, the alternative of treatment with the indication of antiarrhythmic drugs in small children, should be compared to the risks related to a procedure of accessory pathway radiofrequency ablation, particularly in patients with anteroseptal accessory pathway, because of the high risk of iatrogenic complete atrioventricular block in this location [47]. The indication of prophylactic ablation in young asymptomatic children remains to demonstrate [36] without risks related to the catheterism and ablation [46, 47, 66, 67]. In the study of Pappone [36], complications related to electrophysiological study occurred in 5 of the 165 children; 3 of the 20 patients who underwent ablation (15 percent) had complications related to the ablation procedures. The experience of the electrophysiologist should be also taken in account.
• Some authors recommend the ablation of accessory pathway in asymptomatic
patients, because they had a job at risk or they are competitive athletes, but there are no recommendations in these subjects except in those in whom electrophysiologic study has shown a tachycardia induction.

Béatrice Brembilla-Perrot 170
In conclusion, the electrophysiological study is the best means to define the prognosis of a patient with the WPW syndrome. The method is easily performed in consultation by transesophageal route. The indications should be large to avoid the misdiagnosis of a form at risk of rapid arrhythmias. This last form is relatively rare in asymptomatic patients. Most of these patients (>85%) would be allowed to continue their activities, without specific treatment, because they have a benign form of Wolff-Parkinson-White syndrome. In remaining patients, the development of the curative treatment of this disease by radiofrequency application on the accessory pathway permits to offer the possibility to this patient to continue the sport or some professions with stress or exercise. The accessory pathway catheter ablation has a grade I indication in symptomatic adults and asymptomatic patients with inducible tachycardia.
References
[1] Warin JF, Haissaguerre M, Lemetayer P, Guillem JP, Blanchot P. Catheter ablation of accessory pathways with a direct approach. Results in 35 patients. Circulation. 1988; 78 : 800-15
[2] Jackman WM, Wang X, Friday KJ et al. Catheter ablation of accessory atrioventricular pathway (Wolff-Parkinson-White syndrome) by radiofrequency current. N. Engl. J. Med. 1991; 321 : 1605-11
[3] Klein GL, Bashore TM, Sellers TD, Pritchett ELC, Smith WM, Gallagher JS. Ventricular fibrillation in the Wolff Parkinson White syndrome. N. Engl. J. Med. 1979; 15 : 1080-5
[4] Brembilla-Perrot B, Aliot E, Louis P, et al.Devenir de 195 patients atteints de syndrome de Wolff-Parkinson-White. Arch. Mal. Coeur. 1987; 180 : 271-7
[5] Beckman NL, Lamb LE. The Wolff-Parkinson-White electrocardiogram; follow-up study of five to twenty-eight years. N. Engl. J. Med. 1968 ; 278 : 492
[6] Guize L, Soria C, Lavergne T, Le Heuzey JY. Long-term follow-up in large cohort of subjects with Wolff-Parkinson-White syndrome. Eur. Heart J. 1990 ; 11 : 305 (abstr)
[7] Munger TM, Packer DL, Hammill SC et al. A population study of the natural history of Wolff-Parkinson-White syndrome in Olmsted county, Minnesota, 1953-1989. Circulation. 1993; 87 : 866-73
[8] Fitzsimmons PJ, Mc Whirter PD, Peterson DW, Kruyer WB. The natural history of Wolff-Parkinson-White syndrome in 228 military aviators : a long-term follow-up of 22 years. Am. Heart J. 2001 ; 142 : 530-6
[9] Torner Montoya P, Brugada P, Smeets J et al. Ventricular fibrillation in the Wolff-Parkinson-White syndrome. Eur. Heart J. 1991 ; 12 : 144-50
[10] Timmermans C, Smeets J LRM, Rodriguez LM, Vrouchos G, Van Den Dool A, Wellens HJJ. Aborded sudden death in the Wolff-Parkinson-White syndrome. Am. J. Cardiol. 1995 ; 76 : 492-4
[11] Levy S, Broustet JP, Clementy J, Vircoulon P, Guern P, Bricaud H. Syndrome de Wolff Parkinson White . Correlation entre l’exploration électrophysiologique et

Management of Wolff-Parkinson-White Syndrome 171
l’effet de l’épreuve d’effort sur l’aspect électrocardiographique de preexcitation. Arch. Mal. Coeur. 1979 ; 72 : 634-640
[12] Bricker JT, Porter CBJ, Garson A, Gillette PC, Mc Vey P, Traweek M, Mc Namara DG. Exercise testing in children with Wolff Parksinson White syndrome. Am. J. Cardiol. 1985; 55 : 1001-4
[13] Strasberg B, Ashley WW, Wyndham CRC, Bauerfeind RA, Swiryn SP, Dhingra RC, Rosen KM. Treadmill exercise testing in the Wolff Parkinson White syndrome. Am. J. Cardiol. 1980; 45 : 742-8
[14] Daubert C, Ollitraut J, Descaves C, Malso P, Ritter P, Gouffault J. Failure of the exercise test to predict the anterograde refractory period of the accessory pathway in Wolff Parkinson White syndrome. Am. J. Cardiol. 1986; 57 : 782-6
[15] Wellens HJJ, Bar FW, Dassen WR, Brugada P, Vanast EJ, Farre J. Effects of drugs in the Wolff Parkinson White syndrome . Importance of initial length of effective refractory period in the accessory pathway. Am. J. Cardiol. 1980; 46 : 665-9
[16] Critelli G, Gallagher JJ, Perticone F, Caltorti I, Monda V, Condorelli M. Evaluation of non invasive tests for identifying patients with preexcitation syndrome at risk of rapid ventricular response. Am. Heart J. 1984; 108 : 905-9
[17] Sharma AD, Yee R, Guiraudon G, Klein GJ. Sensitivity and specificity of invasive and noninvasive testing for risk of sudden death in Wolff-Parkinson-White syndrome. J. Am. Coll. Cardiol. 1987 ; 10 : 373-41
[18] Vignati G, Mauri L, Lunati M, Gasparini M, Figini A. Transoesophageal electrophysiological evaluation of paediatric patients with Wolff-Parkinson-White syndrome. Eur. Heart J. 1992 ; 13 : 220-2
[19] Brembilla-Perrot B, Spatz F, Khaldi E, Terrier de la Chaise A, Le Van D, Pernot C. Value of esophageal pacing in evaluation of supraventricular tachycardia. Am. J. Cardiol. 1990; 65 : 22-30
[20] Brembilla-Perrot B, Dechaux JP. Ventricular fibrillation induced by transesophageal atrial pacing in asymptomatic Wolff-Parkinson-White syndrome. Am. Heart J. 1992 ; 123 : 536-7
[21] Crick JC, Davies DW, Holt P, Curry PVL, Sowton E. Effect of exercise on ventricular response to atrial fibrillation in Wolff Parkinson White syndrome. Br. Heart J. 1985; 54 : 80-5
[22] Mabo P, Kermarrec A, Gras J, Paillard F, Bédossa M, Daubert CC. Influence de l’effort sur la perméabilité des voies accessoires et le comportement des arythmies supraventriculaires dans le syndrome de Wolff Parkinson White. Arch. Mal. Coeur. 1992; 85 : 1443-8
[23] Wellens HJJ, Brugada P, Roy D, Weiss J, Barr FW. Effect of isoproterenol on the anterograde refractory period of the accessory pathway in patients with the Wolff-Parkinson-White syndrome. Am. J. Cardiol. 1981 ; 50 : 180-4
[24] Rinne C, Klein GJ, Sharma AD et al. Relation between clinical presentation and induced arrhythmias in the Wolff-Parkinson-White syndrome. Am. J. Cardiol. 1987 ; 60 : 576-9
[25] Bromberg BT, Lindsay BD, Cain ME. Impact of clinical history and electrophysiologic characterization of accessory pathways on mangement strategies

Béatrice Brembilla-Perrot 172
to reduce sudden death among children with Wolff-Parkinson-White syndrome. J. Am. Coll. Cardiol. 1996 ; 27 : 690-5
[26] Brembilla-Perrot B, Terrier de la Chaise A, Marçon F, Cherrier F, Pernot C. Le test à l’Isuprel doit-il être systématique dans le syndrome de Wolff-Parkinson-White. Arch. Mal. Coeur. 1988; 81 : 1227-33
[27] Pappone C, Santinelli V, Rosario S, Rosanin S, Vicedomini G, Nardi S, Pappone A, Tortorielli V, Manguso F, Mazzone P, Guletta S, Oreto G, Alfieri O. Usefulness of invasive electrophysiologic testing to stratify the risk of arrhythmic events in asymptomatic patients with Wolff-Parkinson-White pattern. J. Am. Coll. Cardiol. 2003; 41 : 239-44
[28] Yamamoto T, Yeh SJ, Lin FC, Wu D. Effects of isoproterenol on accessory pathways conduction in intermittent concealed Wolff Parkinson White syndrome. Am. J. Cardiol. 1990; 65 : 1438-42
[29] Brembilla-Perrot B, Beurrier D. La voie oesophagienne est -elle préférable à la voie endocavitaire pour évaluer le syndrome de Wolff-Parkinson-White. Arch. Mal. Coeur. 1995; 88 : 353-8
[30] Michelucci A, Padeletti L, Monizzi D et al. Atrial electrophysiologic properties of patients with asymptomatic Wolff-Parkinson-White syndrome. Eur. J. Cardiol. 1988; 9 : 479-83
[31] Brembilla-Perrot B, Holban I, Houriez P, Claudon O, Beurrier D, Vançon AC. Influence of age on the potential risk of sudden death in asymptomatic Wolff-Parkinson-White syndrome. PACE. 2001 ; 24 : 1514-8
[32] Brembilla-Perrot B, Terrier De La Chaise A, Isaaz K, Marçon F, Cherrier F, Pernot C. Inducible multiform ventricular tachycardia in Wolff-Parkinson-White syndrome. Br. Heart J. 1987 ; 58 :89-95
[33] Brembilla-Perrot B, Ghawi R. Electrophysiological characteristics of asymptomatic Wolff-Parkinson-White syndrome. Eur. Heart J. 1993; 14 : 511-5
[34] Milstein S, Sharma AD, Klein GI. Electrophysiologic profile of asymptomatic Wolff-Parkinson-White pattern. Am. J. Cardiol. 1986; 57 : 1097-100
[35] Pappone C, Santinelli V, Manguso F, Augello G, Santinelli O, Vicedomini G, Guletta S, Mazzone, Tortorielli V, Pappone A , Dicandia C, Rosanio S. A randomized study of prophylactic catheter ablation in asymptomatic patients with the Wolff-Parkinson-White syndrome. New Engl. J. Med. 2003; 349: 1803-11
[36] Pappone C, Manguso F, Santinelli V, Vicedomini G, Sala S, Paglino G; Mazzone P, Lang CC, Gulletta S, Augello G, Santinelli O, Santinelli V. Radiofrequency ablation in children with asymptomatic Wolff-Parkinson- White syndrome. N. Engl. J. Med. 2004; 351 : 1197-205
[37] Klein GJ, Yee R, Sharma AD. Longitudinal electrophysiologic assessment of asymptomatic patients with the Wolff-Parkinson-White electrocardiographic pattern. N. Engl. J. Med. 1989; 320 : 1229-33
[38] Leitch JW, Klein GJ, Yee R, Murdock C. Prognostic value of electrophysiology testing in asymptomatic patients with Wolff-Parkinson-White pattern. Circulation. 1990; 82 : 1718-23

Management of Wolff-Parkinson-White Syndrome 173
[39] Auricchio A, KleinH, Trappe HJ, Wenzlaff P. Lack of prognostic value of syncope in patients with Wolff-Parkinson-White syndrome. J. Am. Coll. Cardiol. 1991 ; 17 : 152-8
[40] Paul T, Guccione P, Garson A. Relation of syncope in young patients with Wolff-Parkinson-White syndrome to rapid ventricular response during atrial fibrillation. Am. J. Cardiol. 1990 ; 65 : 318-21
[41] Chometon F, Brembilla-Perrot B. Influence de l’âge sur la cause présumée des syncopes survenant chez un sujet ayant un aspect de syndrome de Wolff-Parkinson-White. Arch. Mal. Cœur. 2007; 100 : 34 - 39
[42] Steinbeck G. Should radiofrequency current ablation be performed in asymptomatic patients with the Wolff-Parkinson-White syndrome? PACE. 1993 ; 16 : 649-657
[43] Wiedermann CJ, Becker AE, Hopperwieser T, Mühlberger V, Knapp E. Sudden death in young competitive athlete with Wolff-Parkinson-White syndrome. Eur. Heart J. 1987; 8 : 651-5
[44] Biffi A, Ammirati F, Caselli G, Fernando M, Cardinale M, Faletra E, Mazzuca V, Verdile L, Santini M. Usefulness of transesophageal pacing during exercise for evaluating palpitations in top-level athletes. Am. J. Cardiol. 1993; 72: 922-6
[45] Calkins H, Yong P, Miller JM, Olshansky B, Carlson M, Saul JP, Huang SK, Liem LB, Klein LS, Moser SA, Bloch DA, Gillette P, Prystowsky E, the ATAKR Multicenter Investigators Group. Catheter ablation of accessory pathways, atrioventricular nodal re-entrant tachycardia, and the atrioventricular junction: final results of prospective multicenter clinical trial. Circulation.1999; 99 : 262-70
[46] Wellens HJJ. Catheter ablation of arrhythmias. N. Engl. J. Med. 2004; 351: 1172-4 [47] Bertram H, Bökenkamp R, Peuster M, Hausdorf G, Paul T. Coronary artery stenosis
after radiofrequency catheter ablation of accessory atrioventricular pathways in children with Ebstein’s malformation. Circulation. 2001; 103 : 538-43
[48] Schuffer MS, Silka MJ, Ross BA, Kugler JD and Participating Members of the Pediatric Electrophysiology Society. Inadvertent atrioventricular block during radiofrequency catheter ablation. Results of the Pediatric Radiofrequency Ablation Registry. Circulation. 1996; 94 : 3214-20.
[49] Brembilla-Perrot B. Traitement pharmacologique des syndromes de préexcitation ventriculaire de l’adulte et de l’enfant. Monographies de cardiologie, J Laham, B Brembilla-Perrot, Ed Masson 2003 ; 107-119
[50] Brembilla-Perrot B, Admand Ph, Le Helloco A, Pernot C. Loss of efficacy of flecainide in the Wolff Parkinson White syndrome after isoproterenol administration. Eur. Heart J. 1985; 6 : 1074-8
[51] Wellens HJ. When to perform catheter ablation in asymptomatic patients with a Wolff-Parkinson-White electrocardiogram. Circulation. 2005 ; 112 : 2201-07
[52] Pappone C Santinelli V. Catheter ablation should be performed in asymptomatic patients with Wolff-Parkinson-White Syndrome. Circulation. 2005; 112 : 2207-16
[53] Vignati G, Balla E, Mauri L, Launati M, Figini A. Clinical and electrophysiologic evolution of the Wolff-Parkinson-White syndrome in children: impact on approaches to management. Cardiol. Young. 2000; 10: 303-6

Béatrice Brembilla-Perrot 174
[54] Dagres N, Clague JR, Kottkamp H, Hindricks G, Breithardt G, Borggrefe M. Impact of radiofrequency catheter ablation of accessory pathways on the frequency of atrial fibrillation during long-term follow-up. High recurrence rate of atrial fibrillation in patients older than 50 years of age. Eur. Heart J. 2001 ; 22 : 423-7
[55] Perry JC, Garson Ajr. Supraventricular tachycardia due to Wolff-Parkinson-White syndrome in children ; early disappearance and late recurrence. J. Am. Coll. Cardiol. 1990; 16 : 1215-20
[56] Sarubbi B, D’Alto M, Vergara P, Calvanese R, Mercurio B, Russo MG, Calabro R. Electrophysiological evaluation of asymptomatic ventricular pre-excitation in children and adolescents. Int. J. Cardiol. 2005; 98 : 207-14
[57] Brembilla-Perrot B, Marchal C, Cloez JL, Lethor JP, Tisserand A, Simon JP, Marçon.F. Etude électrophysiologique par voie transesophagienne d’un enfant de moins de 10 ans, non sédaté, ayant un syndrome de Wolff-Parkinson-White. Arch. Mal. Cœur; in press.
[58] Brembilla-Perrot B, Marçon F, Bosser G, Lucron H, Burger G, Beurrier D, Houriez P. Faisabilité et interêts de l’étude électrophysiologique par voie transoesophagienne dans le syndrome de Wolff-Parkinson-White de l’enfant et l’adolescent. Arch. Mal. Cœur. 2005 ; 98 : 25-30
[59] Michelucci A, Padeletti L, Mezzani A, Giovannini T, Miceli M, Cupelli V, Mussante R. Relationship between age and anterograde refractoriness of the accessory pathway in Wolff- Parkinson-White patients. Cardiology. 1989; 76 : 220-3
[60] Fau W, Peter T, Gang ES, Mandel W. Age-related changes in the clinical and electrophysiologic characteristics of patients with Wolff-Parkinson-White syndrome : comparative study between young and elderly patients. Am. Heart J. 1991 ; 122 : 741-7
[61] Chen SA, Chiang CE, Yang CJ, Chang CC, Wu TJ, Wang SP, Chiang BN, Chang MS. Accessory pathway and atrioventricular mode reentrant tachycardia in elderly patients : clinical features, electrophysiologic characteristics and results of radiofrequency ablation. J. Am. Coll. Cardiol. 1994; 23 : 702-8
[62] Rosenfeld LE, Van Zetta AM, Bastford WP. Comparison of clinical and electrophysiologic features of preexcitation syndrome in patients presenting initially after age 50 years with those presenting at younger age. Am. J. Cardiol. 1991; 67 : 709-12
[63] Michelucci A, Padeletti L, Fradella GA, Lower RM, Monizzi D, Gioni A, Fontani F. Aging and atrial electrophysiologic properties in man. Int. J. Cardiol. 1984 ; 5 : 75-81
[64] Parmeggiani L, Adamec R, Perrenoud JJ. Flutter auriculaire 1/1 : une des modalités de découverte d’un syndrome de Wolff-Parkinson-White. A propos d’une observation chez un adulte. Arch. Mal. Coeur. 1998; 77 : 111-7
[65] Brembilla-Perrot B, Houriez P, Beurrier D, Louis P, Boursier M, Khalifé K. Atrial fibrillation with a very rapid ventricular response as the first clinical arrhythmia in a 76-year-old- man. PACE. 2003; 26 : 1769-70

Management of Wolff-Parkinson-White Syndrome 175
[66] Vitello R, McCrindle BW, Nykanen D, Freedom RM, Benson L. Complications associated with pediatric cardiac catheterization. J. Am. Coll. Cardiol. 1998; 32 : 1243-40
[67] Bacher K, Bogaert E, Lapere R, De Wolf D, Thierens H. Patient-specific dose and radiation risk estimation in pediatric cardiac catheterization. Circulation. 2005; 111 : 83-89


In: Cardiac Arrythmia Research Advances ISBN: 978-1-60021-795-1 Editor: Lynn A. Vespry, pp. 177-201 © 2007 Nova Science Publishers, Inc.
Chapter VII
Focus on Amiodarone in Prevention and Treatment of Cardiac Arrhythmia
J. Auer* and B. Eber IInd Department of Internal Medicine, Division of Cardiology
and Intensive Care, General Hospital Wels, Austria
Abstract
There is good evidence that amiodarone is effective against a variety of arrhythmias and that it possibly is superior to other drugs in some settings. Thus, amiodarone is currently the leading antiarrhythmic drug because of proven efficacy and safety. The electrophysiological actions of amiodarone are complex and incompletely understood. It has generally been classified as a Vaughan-Williams class III agent (Table 1), prolonging repolarization by inhibition of outward potassium channels. Amiodarone is particularly useful because its safety has been clearly demonstrated by a large body of evidence, including several randomized trials. Compared with many other antiarrhythmic drugs, amiodarone causes few cardiovascular adverse effects; however, its overall tolerance is limited by considerable noncardiac toxicity. Although amiodarone will continue to give way to the implantable cardioverter defibrillator (ICD) as primary therapy for many patients presenting with sustained ventricular tachycardia (VT) or ventricular fibrillation (VF), it is likely that amiodarone use will continue in ICD patients to prevent ICD discharges. Pharmacological therapy remains the major approach to management of AF, and use of amiodarone is likely to increase in future years. This review will analyze the evidence that amiodarone is a safe and effective antiarrhythmic drug.
* Correspondence to: Dr Johann Auer, FESC; Professor of Medicine and Cardiology; II nd Medical Department,
Division of Cardiology and Intensive Care; General Hospital Wels; Grieskirchnerstraße 42; 4600 Wels, Austria; Tel.:++43 7242 415 2215; Fax: ++43 7242 415 3992; e-mail: [email protected]

J. Auer and B. Eber 178
Table 1. Vaughan-Williams classification of antiarrhythmic drugs
Class Cellular effects Agents Ia Depress phase 0 of action potential;
slow conduction; prolong repolarization
Quinidine, disopyramide, procainamide
Ib Minimal effect of phase 0 of normal tissue; depress phase 0 in ischemic tissue; shortening or no change in repolarization
Lidocaine, mexiletine, tocainide, dilantin, phenytoin
Ic Depress phase 0 markedly; slow conduction markedly; little effect upon repolarization
Flecainide, propafenone
II �-Adrenergic receptor blockers; increase action potential and refractory period of Purkinje fibres; depress phase 4 depolarization
�-Adrenergic receptor blockers
III Prolong action potential duration (repolarization) Amiodarone, sotalol, bretylium, ibutilide, dofetilide
IV Block L-type calcium channels Verapamil, diltiazem
Introduction Amiodarone was initially developed about three decades ago for angina. On the basis of
the number of prescriptions filled in retail pharmacies, amiodarone was the most-often-prescribed antiarrhythmic agent, accounting for almost one fifth of the total antiarrhythmic prescriptions in 1998. Amiodarone accounted for 34.5% of prescriptions in Europe, 32.8% in North America, 73.8% in Latin America, and 0.3% in Japan and the Philippines. Amiodarone use has increased globally in 1998 at a rate greater than that of the whole antiarrhythmic
market, with striking growth in North America, a 20.0% increase from 1997 to 1998. Amiodarone is used to manage virtually all forms of supraventricular and ventricular tachycardia. This review focuses on amiodarone for prevention and treatment of arrhythmias. Arrhythmias, most commonly requiring antiarrhythmic therapy—sustained ventricular
tachycardia (VT), ventricular fibrillation (VF), and atrial fibrillation (AF)—because they are the most clinically significant and have been the focus of most studies published, will be discussed. This review will analyze the evidence that amiodarone is a safe and effective antiarrhythmic drug.
Pharmacokinetic Considerations To exploit the antiarrhythmic properties of amiodarone fully, the clinician needs to be
familiar with its pharmacokinetics, because they differ markedly from those of other cardiac drugs. Amiodarone is markedly lipophilic, which may account for some of its unusual
pharmacokinetic features[1,2] It is incompletely absorbed (35% to 65%) after oral administration[3]. It is taken up very extensively by tissue, with marked interindividual variation[4]. Estimates of the elimination half-life of amiodarone vary, depending on how it has been measured. The relatively short half-life for disappearance of amiodarone from

Focus on Amiodarone in Prevention and Treatment of Cardiac Arrhythmia 179
plasma after intravenous administration is likely a measure of drug redistribution from
vascular space into tissue and not true body elimination[5]. After long-term oral therapy, amiodarone has a true elimination half-life of up to more than eight weeks[6]. Slow distribution to tissue results in a requirement of very long loading periods, up to several months, before reaching steady-state tissue concentrations. Large loading doses of oral therapy, typically 800 to 1600 mg/d in 3 to 4 divided doses, can accelerate the onset of activity. However, even with loading, arrhythmia recurrence during the first months of therapy does not necessarily predict long-term inefficacy. Amiodarone plasma concentration measurements are of marginal clinical utility for several reasons. Amiodarone is deethylated to an active metabolite desethyl-amiodarone, concentrations of which exceed those of the parent compound during long-term therapy. There is also marked intersubject variability in plasma concentrations of amiodarone and desethyl-amiodarone concentrations associated with arrhythmic suppression[7]. Plasma concentrations >2.5 mg/L have been associated with increased risk of toxicity[8]. The optimal dose of amiodarone has not been systematically
studied. Generally doses of 200 to 400 mg/d have been used during long-term therapy of supraventricular and ventricular arrhythmia, but doses as low as 100 mg/d have been shown to be effective in some patients.
Mechanisms of Action The electrophysiological actions of amiodarone are complex and incompletely
understood. Amiodarone has generally been classified as a Vaughan-Williams class III agent, prolonging repolarization by inhibition of outward potassium channels[9]. It also has been shown to have use-dependent class I activity, inhibition of the inward sodium currents[10], and class II activity. The antiadrenergic effect of amiodarone, however, is different from that of ß-blocker drugs because it is noncompetitive and additive to the effect of ß-blockers[11].
Amiodarone depresses automaticity of the sinoatrial node, resulting in slowing of the heart rate in sinus rhythm. It both slows conduction and increases refractoriness of the AV node[12], properties useful in the management of supraventricular arrhythmia. Its class III activity results in increases in atrial and ventricular refractoriness and in prolongation of the QTc interval. Amiodarone prolongs VT cycle length by 20% to 25% during long-term therapy[13]. The effects of oral amiodarone on sinoatrial and AV nodal function are maximal within two weeks, whereas the effects on VT and ventricular refractoriness tend to emerge more gradually during oral therapy, becoming maximal at ten weeks.
Cardiac and Non Cardiac Adverse Events Caused by Amiodarone
There is good evidence that amiodarone is effective against a variety of arrhythmias and
that it possibly is superior to other drugs in some settings. These benefits do not explain why
amiodarone has become the most used antiarrhythmic drug. Clinical decision making balances assessment of effectiveness against risk of adverse outcomes, and amiodarone has

J. Auer and B. Eber 180
been shown to be a relatively safe drug, especially in patients with serious heart disease.
Amiodarone can result in severe toxicity of lung, liver, thyroid, nerves, and skin. However, early concern about its noncardiac side effects[14] has been replaced by appreciation of its low cardiovascular toxicity[20].
To help understand the evidence that amiodarone is relatively safe, one should understand the safety concerns regarding other antiarrhythmic drugs. On the basis of the results of several clinical trials and subsequent meta-analysis, considerable evidence accumulated in the early 1990s that many antiarrhythmic drugs increase the risk of death in the very patients who could benefit most from effective arrhythmia prevention, those with serious underlying myocardial and coronary artery disease[21,22]. Although the mechanism of this adverse effect is unclear, proarrhythmic and adverse hemodynamic actions are the most likely culprits.
The cardiovascular safety of amiodarone can be assessed from various case series and from randomized trials.
Assessment of the risk of proarrhythmic effects of drugs can be difficult because few features distinguish a proarrhythmic effect from breakthrough of the underlying arrhythmia.
The only finding that is virtually diagnostic of drug-induced arrhythmia is torsade de pointes (Table 2), polymorphic VT in the presence of marked QT interval prolongation.
Even so, QT prolongation occurs in virtually all amiodarone-treated patients, with resolution in many cases after drug discontinuation and/or heart rate acceleration[15], and polymorphic VT can occur spontaneously; thus, there is some lack of reliability even from case studies and follow-up studies reporting torsade de pointes. Ultimately, the most reliable safety data come from randomized, controlled trials. The incidence of this complication appears to be low (<0.5%)[24]. The clinician should be watchful because the individual patient receiving amiodarone may have an adverse arrhythmic event. He or she can be confident that these are rare and that the overall risk of death from arrhythmia or any cause with amiodarone is likely reduced.
Amiodarone is generally well tolerated in patients with CHF. Several randomized trials of amiodarone in patients with severe left ventricular dysfunction have reported that it is well tolerated and may significantly reduce admission to hospital for CHF and improve functional class[17].
Amiodarone may induce severe bradycardia requiring a permanent pacemaker, but reports of severe complications caused by bradycardia induced by amiodarone are not common[24]. The 1-year risk of bradycardia requiring medication discontinuation in the meta-analysis of double-blind, placebo-controlled, primary prevention trials was 2.4% on amiodarone and 0.8% on placebo[18]. In summary, there is considerable evidence that amiodarone has less cardiovascular toxicity than other antiarrhythmic drugs. This is based largely on an analysis of the results of several placebo-controlled trials of both amiodarone and other drugs and on meta-analysis of these trials. With amiodarone, there is neutral or slightly improved mortality. Large follow-up studies of amiodarone confirm this view.
Amiodarone may result in serious noncardiac toxicity, particularly pulmonary infiltrates, hepatic dysfunction, thyroid dysfunction, and peripheral neuropathy. Pulmonary toxicity can be severe and occasionally fatal[16]. The diagnosis is most often made by observing patchy interstitial infiltrates on chest x-ray, usually associated with a subacute presentation of

Focus on Amiodarone in Prevention and Treatment of Cardiac Arrhythmia 181
dyspnea. Typically, once the differential diagnosis of pulmonary edema has been excluded, amiodarone discontinuation is indicated. Estimates of the risk of pulmonary toxicity during long-term oral therapy vary and may be dose related. The most reliable estimate of the 1-year risk of this complication comes from double-blind, placebo-controlled, randomized trials, because there is a tendency to overdiagnose the condition in patients receiving open-label amiodarone. Meta-analysis of the double-blind trials indicates an absolute 1% net risk
(amiodarone rate less placebo rate) of this complication during 1 year, with some fatal cases reported[20]. The same meta-analysis[20] also reported that the 1-year net risk of events (severe enough to cause study drug discontinuation) was 0.6% for hepatic toxicity, 0.3% for peripheral neuropathy, and 0.9% for hyperthyroidism. Hypothyroidism was quite common, occurring in 6% during the first year of treatment, but usually it is easily managed by thyroid hormone replacement concurrent with continuation or discontinuation of amiodarone. During long-term management of patients on amiodarone, routine toxicity screening is required. This includes periodic (usually every 6 months) measurement of thyroid (sensitive serum T4), hepatic (AST), and pulmonary function (chest x-ray), as well as clinical evaluation.
Table 2. Risk factors for the development of drug-induced torsade de pointes
Female gender Hypokalemia, hypomagnesemia Bradycardia Diuretic use High doses or concentrations (quinidine is an exception) Recent conversion from atrial fibrillation Congestive heart failure or cardiac hypertrophy Rapid intravenous infusion Baseline ECG showing QT prolongation, T wave lability ECG during drug therapy showing marked QT prolongation, T wave lability, T wave morphologic changes, increased QT dispersion Congenital long QT syndrome
Prevention of Life-Threatening Arrhythmias
Over the decade from 1985 to 1995, many trials were done to assess the effect of
amiodarone in the prevention of death in patients who had never had a sustained ventricular arrhythmia but were nonetheless at high risk of death from arrhythmia (congestive heart failure or after myocardial infarction)[17,18,19,20,21,22,23]. Most of the trials screened potentially eligible patients by means of left ventricular ejection fraction assessment, Holter
ECG, or both to identify a particularly high-risk group. A meta-analysis of these trials based on individual patient data yielded a relative risk reduction in all-cause mortality of 13% to 15%, which was of borderline statistical significance (p=0.03)[24]. The reduction in all-cause death was due to a relative 29% decrease in arrhythmic deaths (p=0.003), which accounted for somewhat less than half of all deaths. There was no effect of amiodarone on nonarrhythmic deaths. The treatment benefit was uniform across the CHF and post–

J. Auer and B. Eber 182
myocardial infarction trial patients and was independent of major prognostic variables, such as left ventricular function. Because there is good evidence that ß-blocking drugs reduce
sudden death after myocardial infarction[25], it is tempting to attribute the prophylactic benefit of amiodarone against sudden death to its antiadrenergic effect. However, the available data indicate that this is unlikely because amiodarone interacts positively with ß-blocker therapy in post–myocardial infarction patients. In both the European Myocardial Infarction Amiodarone Trial (EMIAT) and Canadian Amiodarone Myocardial Infarction Arrhythmia Trial (CAMIAT), two of the large randomized trials of amiodarone after myocardial infarction, patients receiving ß-blockers at baseline had a statistically significantly better effect from amiodarone than those not receiving a ß-blocker. This significant interaction remains even after adjustment for differences in baseline prognostic variables. This finding suggests that the amiodarone effect in reducing arrhythmic death is separate from and complementary to the effect of ß-blockers in these patients.
Widespread clinical experience indicates that amiodarone is useful against VT and VF; thus, it was used in the major multicenter trials as best medical therapy for these lethal conditions. Yet, hard evidence that amiodarone is effective against VT and VF is scant. The
initial acceptance of amiodarone was based almost entirely on uncontrolled clinical experience. Subsequently, several randomized trials were performed, but in these, amiodarone was compared with other questionable drug treatments or evaluated as primary
prophylaxis against arrhythmic death. Nonetheless, about three decades of clinical experience worldwide and a clear-cut reduction in arrhythmic death in the randomized placebo-controlled prophylactic trials provided somewhat indirect but convincing evidence that
amiodarone might be effective against VT/VF recurrence, although the degree of benefit remained imprecise. On the other hand, it is now clear from randomization trials that amiodarone is not as effective as the ICD for prevention of lethal arrhythmia. What is the proper role of amiodarone in the prevention of recurrent VT and VF? Amiodarone will surely continue to be useful for control of VT/VF as an adjunct to ICD therapy. The potential benefits of amiodarone in ICD patients require more careful evaluation in randomized studies. Amiodarone has not lived up to the expectation that it would be a highly effective prophylactic agent in post–myocardial infarction or heart failure patients. The primary prevention trials have shown quite clearly that amiodarone reduced arrhythmic death, but the beneficial effect on all-cause mortality, if there is actually one, is too small to justify routine prophylactic use.
Current guidelines clearly indicate that the available antiarrhythmic drugs other than beta blockers should not be used as primary therapy in the management of ventricular arrhythmias and the prevention of SCD. The efficacy of non– beta-blocker antiarrhythmic drugs is equivocal at best, and each drug has significant potential for adverse events including proarrhythmia.
Recent studies indicate that the overall long-term survival benefit from amiodarone is controversial, with most studies showing no clear advantage over placebo. A few studies and one meta-analysis of several large studies have shown reduction in SCD using amiodarone for LV dysfunction due to prior myocardial infarction and nonischemic dilated cardiomyopathy[26,27,28], but the SCD-HeFT trial showed no survival benefit from amiodarone compared with placebo[29,30]. Chronic administration of amiodarone is

Focus on Amiodarone in Prevention and Treatment of Cardiac Arrhythmia 183
associated with complex drug interactions and a host of adverse side effects involving the lung, liver, thyroid, and skin. As a general rule, the longer the therapy and the higher dose of amiodarone, the greater is the likelihood that adverse side effects will require discontinuance of the drug. Sotalol, like amiodarone, is effective in suppressing ventricular arrhythmias, but it has greater proarrhythmic effects and has not been shown to provide a clear increase in survival; worsening ventricular arrhythmias occur in 2% to 4% of treated patients[31].
Overall, the available antiarrhythmic drugs other than beta blockers should not be used as primary therapy in the management of ventricular arrhythmias and the prevention of SCD. The efficacy of non– beta-blocker antiarrhythmic drugs is equivocal at best, and each drug has significant potential for adverse events including proarrhythmia.
Amiodarone therapy may be considered in special situations[23]; secondary subset analyses indicate possible survival benefit when amiodarone is combined with beta blockers[32,33]. However, the SCD-HeFT study showed no benefit in patients with NYHA functional class II HF and potential harm in patients with NYHA functional class III HF and EF equal to or less than 35%[29]. Azimilide was shown to decrease the risk of appropriate and inappropriate shocks in patients with ICDs[34]. Both sotalol and amiodarone have also been shown to reduce the frequency of ICD shock therapy[35,36].
Patients with Ventricular Tachyarrhythmias Who Do Not Meet Criteria for an Implantable Cardioverter-Defibrillator
Beta blockers are the first-line therapy, but if this therapy at full therapeutic dose is not
effective, then amiodarone or sotalol can be tried with monitoring for adverse effects during administration.
Patients with Implantable Cardioverter-Defibrillators Who Have Recurrent Ventricular Tachycardia/Ventricular Fibrillation with Frequent Appropriate Implantable Cardioverter-Defibrillator Firing
This scenario, in its extreme, has been called defibrillator (tachycardia) storm, and it
requires the addition of antiarrhythmic drugs and/or catheter ablation for control of the recurrent VT and associated ICD shocks. Sotalol is effective in suppressing atrial and ventricular arrhythmias[34]; the combination of beta blockers and amiodarone is an alternative approach. Because many such patients have low EF and poor renal function, amiodarone and beta blockers rather than sotalol can be the first-line therapy for defibrillator storm. Sotalol should be avoided in patients with severely depressed LV function or significant HF. Animal studies[37,38] and a case report showed the benefits of neural modulation via spinal cord approaches[39]. Intravenous amiodarone has been useful.

J. Auer and B. Eber 184
Patients with Implantable Cardioverter-Defibrillators Who Have Paroxysmal or Chronic Atrial Fibrillation with Rapid Rates and Inappropriateiimplantable Cardioverter-Defibrillator Firing
Control of the rapid ventricular response to atrial tachyarrhythmias is essential, and
combination therapy with a beta blocker and/or a calcium channel blocker is useful. Amiodarone has been used off-label for rate control if other therapies are contraindicated, not tolerated, or ineffective. Ablation of the AV node may be required when pharmacological therapy is not effective.
Implantable Cardioverter Defibrillator in Prevention of Arrhythmic Death
Ventricular fibrillation is a leading cause of preventable death in patients with heart
disease and use of an ICD is key in reducing mortality from cause[40,41].. A large prospective randomized comparative study compared ICD therapy with Class III antiarrhythmic drug therapy, predominantly empiric amiodarone[42]. In survivors of cardiac arrest and hemodynamically unstable VT, survival was greater with ICD therapy. Unadjusted survival estimates for the ICD and drug therapy were 89.3% versus 82.3%, respectively, at 1 year, 81.6% versus 74.7% at 2 years, and 75.4% versus 64.1% at 3 years. Estimated relative risk reduction with ICD therapy was 39% at 1 year and 31% at 3 years.
Either spontaneous or inducible sustained ventricular fibrillation or tachycardia is a leading indication for an ICD[43]. Clinical trial results from MADIT II indicate that, in the near future, patients with cardiac pump failure (without arrhythmia) will become the main ICD recipients[44].
A combination of ICD therapy with drugs or ablation is also frequently used. Currently the largest clinical experience is with combined antiarrhythmic drug and ICD therapy.
Current guidelines suggest[45] that ICD therapy,compared with conventional or traditional antiarrhythmic drug therapy, has been associated with mortality reductions from 23% to 55% depending on the risk group participating in the trial, with the improvement in survival due almost exclusively to a reduction in SCD. The trials may be subcategorized into 2 types: primary prevention (prophylactic) trials in which the subjects have not experienced a life-threatening ventricular arrhythmia or a symptomatic equivalent and secondary prevention trials involving subjects who have had an abortive cardiac arrest, a life-threatening VT, or unexplained syncope with work-up suggesting a high probability that a ventricular tachyarrhythmia was the cause of the syncope.
Several prospective multicenter clinical trials have documented improved survival with ICD therapy in high-risk patients with LV dysfunction due to prior MI and nonischemic cardiomyopathy[23,46,47,48,49,50,51,52]. Important ICD advancements continue to occur in the transvenous implantation procedure, generator size reduction, system longevity, arrhythmia detection, and multiprogrammable features. However, it is important to remember that device failure, although rare, can occur. Current ICDs include options for single-chamber, dual-chamber, and biventricular cardiac resynchronization pacing for nonshock

Focus on Amiodarone in Prevention and Treatment of Cardiac Arrhythmia 185
termination of ventricular arrhythmia in addition to multilevel shock discharge for VT or VF. Problems associated with ICD therapy include inappropriate shock discharge mostly for AF with rapid ventricular response, defibrillator storm with appropriate recurrent ICD discharge for recurrent ventricular tachyarrhythmias or inappropriate discharge for a multiplicity of reasons, infections related to device implantation, and exacerbation of HF when a high percentage of the heartbeats are paced from the RV apex, especially when ventricular function is already compromised. It is probably advisable to limit RV pacing to a minimum for any given patient. Possible solutions include the selection of an appropriately low minimum rate and an appropriately long AV interval. Avoidance of overly aggressive rate acceleration in rate-modulated modes and, in some recent pacemaker models, the use of an automatic pacing mode selecting algorithms that strongly favor atrial over ventricular pacing[53]. The HF is likely to occur in the setting of advanced LV dysfunction with the ICD unit programmed to dualchamber (DDD) pacing at heart rates that dominate the rhythm, thus contributing to paced ventricular desynchronization. The ACC/AHA/NASPE 2002 Guidelines Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices, the ACC/AHA 2004 Guidelines for Management of Patients With ST-Elevation Myocardial Infarction, the ESC 2001 and 2003 Guidelines on Prevention of SCD, the ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure, and the ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult include a large number of recommendations on ICD therapy which merit attention[54,55]. Details and background references are provided in the full-text guidelines, which are on the ACC, AHA, HRS (formerly known as NASPE), and ESC Websites. The findings from the SCD-HeFT trial provide additional evidence that the ICD is effective in high-risk cardiac patients with ischemic and nonischemic cardiomyopathy[23]. Differences in the recommendations in these guidelines from those previously published reflect primarily data from new studies. Detailed discussion on the considerations for therapy recommendations is found in the Introduction. However, there are inconsistencies among guidelines regarding the EF cutoff used in the recommendations.
Therapy of Symptomatic Ventricular Tachycardia
Amiodarone has been widely used to control symptomatic ventricular arrhythmias, primarily to prevent recurrence of VT and VF. Although amiodarone is accepted as effective against VT and VF, there is little supportive evidence from placebo-controlled studies. Nonetheless, amiodarone is approved for use against VT and VF by most regulatory agencies worldwide and has a high profile as a useful drug[56]. Its high rate of use against VT or VF is based largely on considerable clinical experience and concern about the safety of other drugs.
Amiodarone suppresses ventricular premature depolarizations (VPDs) and episodes of nonsustained VT[57]. This is clearly demonstrated in several of the primary prevention trials of amiodarone in post–myocardial infarction and congestive heart failure (CHF) patients in whom baseline and follow-up 24-hour ambulatory ECGs were performed.
There have not been any placebo-controlled trials of amiodarone against sustained VT and VF. Virtually all available publications merely report the outcomes of patients with

J. Auer and B. Eber 186
resuscitated cardiac arrest or recurrent VT treated with amiodarone[58,59]. Most reports conclude that amiodarone is an effective agent[60,61] although some suggest that amiodarone is not as effective as claimed by early enthusiastic reports[62]. It is not possible to draw any firm conclusions about the efficacy of amiodarone from these uncontrolled reports. Nonetheless, they formed the basis for regulatory approval[63].
The largest follow-up report of amiodarone treatment included 589 patients with supraventricular arrhythmia, 83% of whom had VT or VF (17% nonsustained VT)[64]. The 5-year cumulative risk of sudden death was 22%; of total death, 46%. The cumulative risk of drug failure, defined as sudden death, ventricular arrhythmia recurrence, or drug discontinuation at 5 years, was 50%. Amiodarone has been compared in a nonrandomized retrospective trials to other antiarrhythmic therapy for the management of VT[65] with an advantage with amiodarone.
The Cardiac Arrest in Seattle: Conventional Versus Amiodarone Drug Evaluation (CASCADE) study is the only randomized trial of amiodarone against other antiarrhythmic drugs for treatment of VF[66]. High-risk survivors of out-of-hospital VF were randomized to receive either amiodarone or "conventional" antiarrhythmic therapy, which consisted primarily of Vaughan-Williams class I antiarrhythmic drug therapy, guided by serial ambulatory ECG monitoring or electrophysiological testing. Approximately halfway through the study, all patients received an implantable cardioverter-defibrillator (ICD) in addition to randomized therapy. The risk of the primary outcome, which was a composite of cardiac death, sustained VT/VF, or syncopal ICD shock, was significantly reduced by amiodarone. At 4 years of follow-up, event-free survival was 52% for amiodarone and 36% for conventional care, a 44% higher rate. Cardiac death and all-cause mortality rates were also lower on amiodarone. Although small, this study provides considerable support for a benefit of amiodarone over class I drugs. There is evidence from other sources, however, that class I drugs are proarrhythmic and may increase all-cause mortality (CAST and [67]). Accordingly, the observed difference in outcomes in the CASCADE study may have been due to harmful effect of conventional therapy, a beneficial effect of amiodarone, or most likely, their combination. In summary, the direct evidence that amiodarone prevents recurrent VT and VF is based mostly on clinical experience and not on randomized trials.
The general view that amiodarone is the most useful drug for VT and VF, notwithstanding the rather modest evidence from randomized trials, led to its being adopted as the standard medical therapy in several recent randomized secondary prevention trials evaluating the ICD. In the Canadian Implantable Defibrillator Study (CIDS) and Antiarrhythmics Versus Implantable Defibrillators (AVID) study, patients with either VF or sustained VT were randomized to receive an ICD or medical therapy[68,69]. In CIDS, medical therapy was amiodarone; in AVID, it was amiodarone or sotalol. Amiodarone was 1 of 3 drugs that were randomly compared with the ICD in the Cardiac Arrest Study, Hamburg (CASH), which enrolled only cardiac arrest survivors[70]. All three studies observed improved survival with the ICD compared with amiodarone, with relative risk reductions ranging from 20% to 40%. In the AVID study, all-cause mortality was statistically significantly reduced by ICD therapy, whereas in both CASH and CIDS, ICD therapy was associated with non-significant reductions in all-cause death. A combined analysis of the

Focus on Amiodarone in Prevention and Treatment of Cardiac Arrhythmia 187
three trials has shown that they are consistent and that there is a statistically significant
mortality reduction of 27% with the ICD compared with amiodarone.
Sustained Ventricular Tachycardia in Left Ventricular Dysfunction due to Prior
Myocardial Infarction Current guidelines suggest that the treatment of sustained VT in patients with chronic
CHD should be tempered by the clinical manifestations produced by the tachycardia, as well as the frequency of episodes. Patients who present with sustained monomorphic VT that does not precipitate cardiac arrest or cause severe hemodynamic instability are usually, but not always, at relatively low risk for SCD (2% yearly)[71,72]. Twelve-lead ECGs should be obtained during episodes of sustained VT, and the morphology assessed to be certain that it is consistent with location of prior MI(s). The possibility should be considered that patients with prior MI may develop sustained VT unrelated to the infarction, due to other mechanisms such as bundle-branch reentry or idiopathic VT. If episodes are relatively infrequent, the ICD alone may be the most appropriate initial therapy, because antitachycardia pacing therapies or high-energy shock therapy may reduce the need for hospitalization and pharmacological antiarrhythmic therapy. Suitable adjunctive therapies include catheter ablation, surgical resection, and pharmacological therapy with agents such as sotalol or amiodarone. Curative therapy of sustained VT using either surgical resection or catheter ablation should be considered in patients with frequent recurrences of VT unresponsive to antiarrhythmic drugs. Patients in whom the tachycardia is hemodynamically stable may be considered for curative catheter ablation. The major limitation to catheter ablation is the fact that most patients with sustained VT resulting from prior MI have multiple tachycardias, and it is often difficult to ablate all tachycardias completely, using currently available RF ablation technology. Some patients have only 1 or 2 tachycardia circuits and may be cured of their arrhythmia by catheter ablation. However, they may develop new VT in the future using a different circuit. Although all morphologically distinct tachycardias may not be cured by catheter ablation, the tachycardia substrate may be modified sufficiently to decrease the frequency of arrhythmia episodes. Ablation of the tachycardia using surgery to resect or modify the arrhythmia substrate is an alternative therapy that may be suitable for patients in whom catheter ablation is unsuccessful. Following correction of ischemia, patients who present with sustained VT that causes severe hemodynamic compromise may benefit from EP testing. Such testing will occasionally reveal curable arrhythmias such as bundlebranch reentry. In addition, the results of testing often help in appropriate programming of implantable defibrillators. The ICD is the primary therapy for such patients.

J. Auer and B. Eber 188
Amiodarone for Therapy of Arrhythmias in Heart Failure
Heart failure is often complicated by arrhythmias that significantly contribute to
mortality and morbidity. Amiodarone is the major pharmacologic option for treatment of symptomatic arrhythmias[73]. In selecting antiarrhythmic pharmacotherapy, the severity of heart failure and cause of heart failure are important considerations. AF occurs with increasing frequency as the severity of heart failure increases. With AF, anticoagulation and rate control are the most important therapeutic goals. Attempted maintenance of sinus rhythm with amiodarone or dofetilide is a reasonable consideration for selected patients, although the benefit of treatment strategies that seek to maintain sinus rhythm has not been demonstrated. Ongoing trials will provide further guidance for arrhythmia management.
In contrast, ICD´s are the best protection from death caused by ventricular arrhythmias, but their benefit will probably be less in heart failure populations than has been observed in trials that have not focused on heart failure populations. ICD´s are first-line therapy for high-risk patients who have been resuscitated from sustained ventricular tachycardia or ventricular fibrillation, who have inducible ventricular tachycardia in the setting of previous myocardial infarction, or who have unexplained syncope.
Acute Treatment of Ventricular Tachycardia
and Ventricular Fibrillation Intravenous amiodarone is available for rapid control of recurrent VT or VF, and its
effectiveness has recently been evaluated in randomized controlled trials[74,75]. The target patient populations of these trials were patients with recurrent in-hospital, hemodynamically unstable VT or VF with two episodes within the past 24 hours. Additionally, patients were required to have failed to respond to or be intolerant of other antiarrhythmics like lidocaine,
procainamide, and bretylium. Study patients were severely ill; about a quarter were on a mechanical ventilator or intra-aortic balloon pump before enrollment, and 10% were
undergoing cardiopulmonary resuscitation at the time of enrollment. These studies failed to provide clear evidence of amiodarone efficacy. This result may be
related to the "active-control" study design used, a lack of adequate statistical power, high rates of supplemental amiodarone boluses, and high crossover rates. Nonetheless, these
studies provide some evidence that IV amiodarone (1 g/d) is moderately effective during a 24-hour period against VT and VF.
Several years ago, the Amiodarone in the Out-of-Hospital Resuscitation of Refractory Sustained Ventricular Tachycardia (ARREST) study was presented[76]. With amiodarone added to the advanced cardiac life support protocol, the number of patients admitted to hospital alive increased significantly from 35% to 44% (P<0.03).
Although amiodarone appears useful in short-term management of VT and VF, its role compared with other antiarrhythmic drugs is unclear. On the basis of a meta-analysis of class I and III drugs[20,21], the proarrhythmic potential of amiodarone probably is lower than that

Focus on Amiodarone in Prevention and Treatment of Cardiac Arrhythmia 189
of lidocaine or procainamide; however, its use as a primary agent probably should wait until the results of direct comparative trials become available. Amiodarone is a reasonable alternative to lidocaine, procainamide, and bretylium.
Consistent with the AHA/ERC 2005 guidelines[77], intravenous amiodarone has replaced intravenous lidocaine and other antiarrhythmic medications for the management of resistant ventricular tachyarrhythmias causing repeated episodes of ventricular tachyarrhythmias[78]. Amiodarone need not be given routinely to the individual who responds to initial defibrillation with a stable rhythm. If there is sufficient clinical evidence that a cardiac arrest was heralded by the onset of an ACS, intravenous lidocaine may still be used for resistant arrhythmias. Beta blockers may be preferred for ACSs if not already being taken.
Amiodarone in Atrial Fibrillation in Patients
with and without Heart Failure Pharmacological control of AF is a useful clinical goal and a reasonable clinical trial
outcome. Management of AF entails a variety of approaches in different patients and at different times. These include maintenance of sinus rhythm, conversion of AF to sinus rhythm, control of ventricular rate, and primary prevention of AF. Amiodarone has been evaluated with randomized trials in all of these setting
All randomized trials of amiodarone for long-term maintenance of sinus rhythm in patients with recurrent AF have used active-control groups. Some studies compared amiodarone with quinidine[79], sotalol[80] and other antiarrhythmic drugs. It is therefore likely that amiodarone is effective for maintenance of sinus rhythm in the patient with
recurrent AF, and there is modest evidence of superiority over other agents.Several studies evaluated intravenous amiodarone for conversion of acute AF to sinus rhythm[81].
Control of ventricular rate in AF was evaluated in a few placebo-controlled studies, which reported significantly lower ventricular rates with amiodarone[82]. Thus, amiodarone is effective for acute conversion of AF and has a beneficial effect on heart rate in AF.
Several active-control short-term conversion studies comparing intravenous amiodarone with oral quinidine for management of acute AF have been reported[83]. There was no significant difference in 24-hour conversion rates or control of ventricular response.
In another study amiodarone and flecainide had similar rates of acute AF conversion[84]. Comparative studies of intravenous amiodarone and propafenone in postoperative AF
observed little difference between drugs, although there was a small trend in favor of amiodarone at 24 hours[85].
Primary prevention of AF is a worthwhile goal that has been studied in a heart failure trial and extensively in patients recovering from open-heart surgery, in whom AF occurs in about 30% of patients.
A few studies reported a modest reduction in postoperative AF after open-heart surgery receiving amiodarone beginning 1 to 3 days before surgery[86].
Finally, in a subanalysis of Congestive Heart Failure–Survival Trial of Antiarrhythmic Therapy (CHF-STAT), a mortality trial of prophylactic amiodarone in heart failure, patients

J. Auer and B. Eber 190
on amiodarone were significantly less likely to develop AF than those on placebo, and patients with AF at baseline were also more likely to convert to sinus rhythm if they received amiodarone[87].
In patients with congestive heart failure and reduced left ventricular function, the new class III antiarrhythmic drug dofetilide was effective in converting atrial fibrillation, preventing its recurrence, and reducing the risk of hospitalization for worsening heart failure, but dofetilide had no effect on mortality[88].
In summary, there is reasonable evidence from many rather small, randomized controlled trials that amiodarone is effective for conversion of AF and maintenance of sinus rhythm. However, the available active-control studies provide little evidence that it is superior to other effective drugs. It should be noted that active-control studies inherently pose a greater challenge to the demonstration of efficacy than do placebo-controlled trials, because the differences one can expect to observe in comparison with other effective agents are usually small. Thus, active-control studies need to be more rigorously designed and include larger numbers of patients. The Canadian Trial of Atrial Fibrillation[89] reported a significant reduction in AF recurrence with amiodarone compared with either sotalol or propafenone. In addition, a large substudy of the AFFIRM trial (Atrial Fibrillation Follow-up Investigation of Rhythm Management) is comparing amiodarone to other drugs for control of AF[90].
Current guidelines[91] suggest that before administering any antiarrhythmic agent, reversible precipitants of AF should be identified and corrected. Most are related to coronary or valvular heart disease, hypertension, or HF. Patients who develop AF in association with alcohol intake should abstain from alcohol consumption. Indefinite antiarrhythmic treatment is seldom prescribed after a first episode, although a period of several weeks may help stabilize sinus rhythm after cardioversion. Similarly, patients experiencing breakthrough arrhythmias may not require a change in antiarrhythmic drug therapy when recurrences are infrequent and mild. Beta-adrenergic antagonist medication may be effective in patients who develop AF only during exercise, but a single, specific inciting cause rarely accounts for all episodes of AF, and the majority of patients do not sustain sinus rhythm without antiarrhythmic therapy. Selection of an appropriate agent is based first on safety, tailored to whatever underlying heart disease may be present, considering the number and pattern of prior episodes of AF[92].
In patients with lone AF, a beta blocker may be tried first, but flecainide, propafenone, and sotalol are particularly effective. Amiodarone and dofetilide are recommended as alternative therapies. Quinidine, procainamide, and disopyramide are not favored unless amiodarone fails or is contraindicated. For patients with vagally induced AF, however, the anticholinergic activity of long-acting disopyramide makes it a relatively attractive theoretical choice. In that situation, flecainide and amiodarone represent secondary and tertiary treatment options, respectively, whereas propafenone is not recommended because its (weak) intrinsic beta-blocking activity may aggravate vagally mediated paroxysmal AF. In patients with adrenergically mediated AF, beta blockers represent first-line treatment, followed by sotalol and amiodarone. In patients with adrenergically mediated lone AF, amiodarone represents a less appealing selection. Vagally induced AF can occur by itself, but more typically it is part of the overall patient profile. In patients with nocturnal AF, the possibility of sleep apnea should be considered. When treatment with a single antiarrhythmic

Focus on Amiodarone in Prevention and Treatment of Cardiac Arrhythmia 191
drug fails, combinations may be tried. Useful combinations include a beta blocker, sotalol, or amiodarone with a class IC agent. The combination of a calcium channel blocker, such as diltiazem, with a class IC agent, such as flecainide or propafenone, is advantageous in some patients. A drug that is initially safe may become proarrhythmic if coronary disease or HF develops or if the patient begins other medication that exerts a proarrhythmic interaction. Thus, the patient should be alerted to the potential significance of such symptoms as syncope, angina, or dyspnea and warned about the use of noncardiac drugs that might prolong the QT interval. The optimum method for monitoring antiarrhythmic drug treatment varies with the agent involved as well as with patient factors. Prospectively acquired data on upper limits of drug-induced prolongation of QRS duration or QT interval are not available. With class IC drugs, prolongation of the QRS interval should not exceed 50%. Exercise testing may help detect QRS widening that occurs only at rapid heart rates (use-dependent conduction slowing). For class IA or class III drugs, with the possible exception of amiodarone, the corrected QT interval in sinus rhythm should be kept below 520 ms. During follow-up, plasma potassium and magnesium levels and renal function should be checked periodically because renal insufficiency leads to drug accumulation and predisposes to proarrhythmia. In individual patients, serial noninvasive assessment of LV function is indicated, especially when clinical HF develops during treatment of AF.
In stable patients with CAD, beta blockers may be considered first, although their use is supported by only 2 studies and data on efficacy for maintenance of sinus rhythm in patients with persistent AF after cardioversion are not convincing. Sotalol has substantial beta-blocking activity and may be the preferred initial antiarrhythmic agent in patients with AF who have ischemic heart disease because it is associated with less long-term toxicity than amiodarone. Amiodarone increases the risk of bradyarrhythmia requiring permanent pacemaker implantation in elderly patients with AF who have previously sustained MI[93] but may be preferred over sotalol in patients with HF[94]. Neither flecainide nor propafenone is recommended in these situations, but quinidine, procainamide, and disopyramide may be considered as third-line choices in patients with coronary disease.
Patients with heart failure are particularly prone to the ventricular proarrhythmic effects of antiarrhythmic drugs because of myocardial vulnerability and electrolyte imbalance. Randomized trials have demonstrated the safety of amiodarone and dofetilide (given separately) in patients with HF[95], and these are the recommended drugs for maintenance of sinus rhythm in patients with AF in the presence of HF.
Amiodarone for Treatment of Atrial Fibrillation
after Cardiac Surgery More than 200 000 patients undergo coronary artery bypass grafting (CABG) annually
worldwide[96]. Atrial fibrillation occurs in about 30% (10% to 65%) of patients after cardiac surgery[97], usually on the second or third postoperative day[98]. Postoperative atrial fibrillation is associated with increased morbidity and mortality and longer, more expensive hospital stays. Prophylactic use of beta-adrenergic blockers reduces the incidence of postoperative atrial fibrillation and should be administered before and after cardiac surgery to

J. Auer and B. Eber 192
all patients without contraindication[99]. Prophylactic amiodarone (started up to 7 days before surgery) and atrial overdrive pacing should be considered in patients at high risk for postoperative atrial fibrillation (for example, patients with previous atrial fibrillation or mitral valve surgery)[100,101]. These prophylactic therapies are particularly attractive options if management of postoperative atrial fibrillation with anticoagulation alone or rate control alone is expected to be difficult. For patients who develop atrial fibrillation after cardiac surgery, a strategy of rhythm management or rate management should be selected. For patients who are hemodynamically unstable or highly symptomatic or who have a contraindication to anticoagulation, rhythm management with electrical cardioversion, amiodarone, or both is preferred. Intravenous amiodarone leads to conversion to sinus rhythm within 12 to 24 hours in 40% to 90% of patients with atrial fibrillation after cardiac surgery[102]. Although this rate is similar to that noted with other antiarrhythmic agents, amiodarone therapy provides effective rate control, has a lower risk for proarrhythmia, and is easily converted to oral therapy. For these reasons, amiodarone is preferred for patients who will require ongoing antiarrhythmic therapy after hospital discharge. Treatment of the remaining patients should focus on rate control because most will spontaneously revert to sinus rhythm within 6 weeks after discharge. All patients with atrial fibrillation persisting for more than 24 to 48 hours and without contraindication should receive anticoagulation.
Thus, atrial fibrillation frequently complicates cardiac surgery, but many cases can be prevented with appropriate prophylactic therapy (beta-adrenergic blockers and/or amiodarone).
Current guidelines suggest[90] that unless contraindicated, treatment with an oral beta blocker to prevent postoperative AF is recommended for patients undergoing cardiac surgery. (Class I recommendation; level of evidence: A). Administration of AV nodal blocking agents is recommended to achieve rate control in patients who develop postoperative AF. (level of evidence: B).
Preoperative administration of amiodarone reduces the incidence of AF in patients undergoing cardiac surgery and represents appropriate prophylactic therapy for patients at high risk for postoperative AF (Class II a recommendation)
Treatment of Amiodarone-Induced Thyreotoxicosis
Amiodarone treatment results in a large iodine load and affects thyroid status by
decreasing peripheral deiodination of thyroxine (T4) to tri-iodothyronine (T3), leading to an increase in serum T4 and decrease in T3 [103]. Serum thyrotropin (TSH) levels increase in the early phase of treatment (1 to 3 months) and typically return to normal thereafter[104]. Amiodarone also can induce thyroid dysfunction, with the relative proportion of patients developing thyrotoxicosis or hypothyroidism dependent on dietary iodine content. In iodine-replete areas, such as the United Kingdom and United States, about 3% become
thyrotoxic[105], with a higher prevalence in iodine-deficient areas[106]. Withdrawal of amiodarone often is undesirable because it may provoke life-threatening arrhythmias and may

Focus on Amiodarone in Prevention and Treatment of Cardiac Arrhythmia 193
worsen cardiovascular manifestations caused by thyrotoxicosis. This makes amiodarone-induced thyrotoxicosis (AIT) a difficult condition to manage.
The pathogenesis of AIT is poorly understood, but current opinion suggests that there are 2 forms: type 1 and type 2[107]. Type 1 AIT occurs in subjects with an abnormal thyroid (goiter or latent autoimmune disease), with the iodine load triggering autonomous thyroid hormone production. Type 2 develops in subjects who have an apparently normal gland and may reflect thyroid hormone release from a destructive thyroiditis. Some suggest that type 1 be treated with thionamides combined with potassium perchlorate to deplete intrathyroidal iodine stores, and that type 2 be treated with high-dose glucocorticoids[108]; however, both perchlorate and glucocorticoids are associated with significant side effects. Recent data suggest that continuing amiodarone has no adverse influence on response to treatment of AIT. First-line complications of other drugs, and differentiating between 2 possible types of AIT does not influence management or outcome[109].
Conclusions Amiodarone is currently the leading antiarrhythmic drug because of proven efficacy and
safety. There is reasonable evidence of effectiveness against several clinical important arrhythmias. However, good randomized trials evaluating the efficacy of amiodarone are still needed, especially comparative studies against other drugs for control of AF and a placebo-controlled trial against VT. Amiodarone is particularly useful because its safety has been clearly demonstrated by a large body of evidence, including several randomized trials. Compared with many other antiarrhythmic drugs, amiodarone causes few cardiovascular adverse effects; however, its overall tolerance is limited by considerable noncardiac toxicity.
Although amiodarone has given way to the ICD as primary therapy for the majority of patients presenting with sustained VT or VF, it is likely that amiodarone use will continue in ICD patients to prevent ICD discharges. Pharmacological therapy remains a major approach to management of AF, and use of amiodarone is likely to increase in future years.
References
[1] Chatelain P, Laruel R. Amiodarone partitioning with phospholipid bilayers and erythrocyte membranes. J. Pharm. Sci. 1985;74:783–784.
[2] Goldschlager N, Epstein AE, Naccarelli G, Olshansky B, Singh B. Practical guidelines for clinicians who treat patients with amiodarone. Practice Guidelines Subcommittee, North American Society of Pacing and Electrophysiology. Arch. Intern. Med. 2000;160:1741-8.
[3] Holt DW, Tucker GT, Jackson PR, Storey CGA. Amiodarone pharmacokinetics. Am. Heart J. 1983;106:840–847.
[4] Giardina EGV, Schneider M, Barr MI. Myocardial amiodarone and desethylamiodarone concentrations in patients undergoing cardiac transplantation. J. Am. Coll. Cardiol. 1990;16:943–947.

J. Auer and B. Eber 194
[5] Roden DM. Pharmacokinetics of amiodarone: implications for drug therapy. Am. J. Cardiol. 1993;72:45F–50F.
[6] Haffajee CI, Love JC, Canada AT, Lesko LJ, Asdourian G, Alpert JS. Clinical pharmacokinetics and efficacy of amiodarone for refractory tachyarrhythmias. Circulation. 1983;67:1347–1355.
[7] Connolly SJ, Gupta RN, Hoffert D, Roberts RS. Concentration response relationships of amiodarone and desethylamiodarone. Am. Heart J. 1988;115:1208–1213.
[8] Mahmarian JJ, Smart FW, Moyé LE, Young JB, Francis MJ, Kingry CL, Verani MS, Pratt CM. Exploring the minimal dose of amiodarone with antiarrhythmic and hemodynamic activity. Am. J. Cardiol. 1994;74:681–686.
[9] Singh BN, Vaughan Williams EM. The effect of amiodarone, a new anti-anginal drug, on cardiac muscle. Br. J. Pharmacol. 1970;39:657–667.
[10] Mason JW, Honegham LM, Katzung BG. Block of inactivated sodium channels and of depolarization-induced automaticity in guinea pig papillary muscle by amiodarone. Circ. Res. 1984;55:277–285.
[11] Charlier R. Cardiac actions in the dog of a new antagonist of adrenergic excitation which does not produce competitive blockade of adrenoceptors. Br. J. Pharmacol. 1970;39:668–674.
[12] Heger JJ, Prystowsky EN, Jackman WM, Naccareli GV, Warfel KA, Rinkenberger RL, Zipes DP. Amiodarone: clinical efficacy and electrophysiology during long-term therapy for recurrent ventricular tachycardia or ventricular fibrillation. N. Engl. J. Med. 1981;305:539–545.
[13] Mitchell LB, Wyse G, Gillis AM, Duff HJ. Electropharmacology of amiodarone therapy initiation. Circulation. 1989;80:34–42.
[14] Morady F, Sauve MJ, Malone P, Shen EN, Schwartz AB, Bhandari A, Keung E, Sung RJ, Scheinman MM. Long-term efficacy and toxicity of high-dose amiodarone therapy for ventricular tachycardia or ventricular fibrillation. Am. J. Cardiol. 1983;52:975–979.
[15] Leroy G, Haiat R, Barthelemy M, Lionnet F. Torsade de pointes during loading with amiodarone. Eur. Heart J. 1987;8:541–543.
[16] Rady MY, Ryan T, Starr NJ. Preoperative therapy with amiodarone and the incidence of acute organ dysfunction after cardiac surgery. Anesth. Analg. 1997;85:489–497.
[17] Cairns JA, Connolly SJ, Gent M, Roberts R. Post myocardial infarction mortality in patients with ventricular premature depolarizations. Circulation. 1991;84:550–557.
[18] Singh SN, Fletcher RD, Fisher SG, Singh BN, Lewis HD, Deedwania PC, Massie BM, Colling C, Lazzeri D. Amiodarone in patients with congestive heart failure and asymptomatic ventricular arrhythmia. N. Engl. J. Med. 1995;333:77–82.
[19] Julian DG, Camm AJ, Frangin G, Janse MJ, Munoz A, Schwartz PJ, Simon P, for the EMIAT Investigators. Randomized trial of effect of amiodarone on mortality in patients with left ventricular dysfunction after recent myocardial infraction: EMIAT. Lancet. 1997;349:667–674.
[20] Cairns JA, Connolly SJ, Roberts RS, Gent M, for the CAMIAT Investigators. Randomized trial of outcome after myocardial infarction in patients with frequent or

Focus on Amiodarone in Prevention and Treatment of Cardiac Arrhythmia 195
repetitive ventricular premature depolarizations: CAMIAT. Lancet. 1997;349:675–682.
[21] Doval HC, Nul DR, Grancelli HO, Perrone SV, Bortman GR, Curiel R, for Grupo de Estudio de la Sobrevida en la Insuficiencia Cardiaca en Argentina (GESICA). Randomized trial of low-dose amiodarone in severe congestive heart failure. Lancet. 1994;344:493–498.
[22] Hamer AWF, Arkles B, Johns JA. Beneficial effects of low dose amiodarone in patients with congestive cardiac failure: a placebo-controlled trial. J. Am. Coll. Cardiol. 1989;14:1768–1774.
[23] Garguichevich JJ, Ramos JL, Gambarte A, Gentile A, Hauad S, Scapin O, Sirena J, Tibaldi M, Toplikar J. Effect of amiodarone therapy on mortality in patients with left ventricular dysfunction and asymptomatic complex ventricular arrhythmias: Argentine Pilot Study for Sudden Death (EPAMSA). Am. Heart J. 1995;130:494–500.
[24] Amiodarone Trials Meta-Analysis Investigators. Effect of prophylactic amiodarone on mortality after acute myocardial infarction and in congestive heart failure: meta-analysis of individual data from 6500 patients in randomized trials. Lancet. 1997;350:1417–1424.
[25] Teo KK, Yusuf S, Furberg CD. Effects of prophylactic antiarrhythmic drug therapy in acute myocardial infarction: an overview of results of randomized controlled clinical trials. J. Am. Med. Assoc. 1993;270:1589–1595.
[26] Connolly SJ. Meta-analysis of antiarrhythmic drug trials. Am. J. Cardiol. 1999;84:90R–3R.
[27] Steinberg JS, Martins J, Sadanandan S, et al. Antiarrhythmic drug use in the implantable defibrillator arm of the Antiarrhythmics Versus Implantable Defibrillators (AVID) study. Am. Heart J. 2001;142:520 –9.
[28] Farre J, Romero J, Rubio JM, et al. Amiodarone and “primary” prevention of sudden death: critical review of a decade of clinical trials. Am. J. Cardiol. 1999;83:55D–63D.
[29] Cleland JG, Ghosh J, Freemantle N, et al. Clinical trials update and cumulative meta-analyses from the American College of Cardiology: WATCH, SCD-HeFT, DINAMIT, CASINO, INSPIRE, STRATUS-US, RIO-Lipids and cardiac resynchronisation therapy in heart failure. Eur. J. Heart Fail. 2004;6:501– 8.
[30] Bardy GH, Lee KL, Mark DB, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N. Engl. J. Med. 2005;352:225–37.
[31] Kuhlkamp V, Mewis C, Mermi J, et al. Suppression of sustained ventricular tachyarrhythmias: a comparison of d,l-sotalol with no antiarrhythmic drug treatment. J. Am. Coll. Cardiol. 1999;33:46 –52.
[32] Janse MJ, Malik M, Camm AJ, et al. Identification of post acute myocardial infarction patients with potential benefit from prophylactic treatment with amiodarone. A substudy of EMIAT (the European Myocardial Infarct Amiodarone Trial). Eur. Heart J. 1998;19:85–95.
[33] Boutitie F, Boissel JP, Connolly SJ, et al. Amiodarone interaction with beta-blockers: analysis of the merged EMIAT (European Myocardial Infarct Amiodarone Trial) and

J. Auer and B. Eber 196
CAMIAT (Canadian Amiodarone Myocardial Infarction Trial) databases. The EMIAT and CAMIAT Investigators. Circulation. 1999;99:2268 –75.
[34] Dorian P, Borggrefe M, Al-Khalidi HR, et al. Placebo-controlled, randomized clinical trial of azimilide for prevention of ventricular tachyarrhythmias in patients with an implantable cardioverter defibrillator. Circulation. 2004;110:3646 –54.
[35] Pacifico A, Hohnloser SH, Williams JH, et al. Prevention of implantable-defibrillator shocks by treatment with sotalol. d,l- Sotalol Implantable Cardioverter-Defibrillator Study Group. N. Engl. J. Med. 1999;340:1855– 62.
[36] Connolly SJ, Dorian P, Roberts RS, et al. Comparison of betablockers, amiodarone plus beta-blockers, or sotalol for prevention of shocks from implantable cardioverter defibrillators: the OPTIC Study: a randomized trial. JAMA. 2006;295:165–71.
[37] Issa ZF, Zhou X, Ujhelyi MR, et al. Thoracic spinal cord stimulation reduces the risk of ischemic ventricular arrhythmias in a postinfarction heart failure canine model. Circulation. 2005;111: 3217–20.
[38] Issa ZF, Ujhelyi MR, Hildebrand KR, et al. Intrathecal clonidine reduces the incidence of ischemia-provoked ventricular arrhythmias in a canine postinfarction heart failure model. Heart Rhythm. 2005;2:1122–7.
[39] Mahajan A, Moore J, Cesario DA, et al. Use of thoracic epidural anesthesia for management of electrical storm: a case report. Heart Rhythm. 2005;2:1359–62.
[40] Connolly SJ, Hallstrom AP, Cappato R. Meta-analysis of the implantable cardioverter defibrillator secondary prevention trials. AVID, CASH and CIDS studies: Antiarrhythmics vs Implantable Defibrillator study. Cardiac Arrest Study Hamburg. Canadian Implantable Defibrillator Study. Eur. Heart J. 2000;21:2071-78.
[41] Auer J, Berent R, Eber B. Amiodarone in the prevention and treatment of arrhythmia. Curr. Opin. Investig. Drugs. 2004;47:636-43.
[42] The AVID investigators. A comparison of antiarrhythmic drug therapy with implantable defibrillators in patients resuscitated from near fatal ventricular arrhythmias. N. Engl. J. Med. 1997;337:1576-83.
[43] Glikson M, Friedman PA. The implantable cardioverter defibrillator. Lancet. 2001;357:1107-17.
[44] Moss AJ, Zareba W, Hall WJ. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N. Engl. J. Med. 2002;346:877-83.
[45] Zipes DP, Camm AJ, Borggrefe M, Buxton AE, Chaitman B, Fromer M, Gregoratos G, Klein G, Moss AJ, Myerburg RJ, Priori SG, Quinones MA, Roden DM, Silka MJ, Tracy C. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: a report of the American College of Cardiology/ American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death). J. Am. Coll. Cardiol. 2006;48:e247– e346.
[46] Moss AJ, Hall WJ, Cannom DS, et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia.

Focus on Amiodarone in Prevention and Treatment of Cardiac Arrhythmia 197
Multicenter Automatic Defibrillator Implantation Trial Investigators. N. Engl. J. Med. 1996;335:1933– 40.
[47] Bigger JT Jr. Prophylactic use of implanted cardiac defibrillators in patients at high risk for ventricular arrhythmias after coronary-artery bypass graft surgery. Coronary Artery Bypass Graft (CABG) Patch Trial Investigators. N. Engl. J. Med. 1997;337:1569 –75.
[48] The Antiarrhythmics versus Implantable Defibrillators (AVID) Investigators. A comparison of antiarrhythmicdrug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. N. Engl. J. Med. 1997;337:1576–83.
[49] Buxton AE, Lee KL, Fisher JD, et al. A randomized study of the prevention of sudden death in patients with coronary artery disease. Multicenter Unsustained Tachycardia Trial Investigators. N. Engl. J. Med. 1999;341:1882–90.
[50] Moss AJ, Zareba W, Hall WJ, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N. Engl. J. Med. 2002;346:877– 83.
[51] Lee DS, Green LD, Liu PP, et al. Effectiveness of implantable defibrillators for preventing arrhythmic events and death: a metaanalysis. J. Am. Coll. Cardiol. 2003;41:1573– 82.
[52] Ezekowitz JA, Armstrong PW, McAlister FA. Implantable cardioverter defibrillators in primary and secondary prevention: a systematic review of randomized, controlled trials. Ann. Intern. Med. 2003;138:445–52.
[53] Wilkoff BL, Cook Jr., Epstein AE, et al. Dual-chamber pacing or ventricular backup pacing in patients with an implantable defibrillator: the Dual Chamber and VVI Implantable Defibrillator (DAVID) trial. JAMA. 2002;288:3115–23.
[54] Priori SG, Aliot E, Blomstrom-Lundqvist C, et al. Task Force on Sudden Cardiac Death of the European Society of Cardiology. Eur. Heart J. 2001;22:1374–450.
[55] Hunt SA. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). J. Am. Coll. Cardiol. 2005;46:e1– 82.
[56] The Cardiac Arrhythmia Suppression Trial (CAST) Investigators. Effect of encainide and flecainide on mortality in infarction. N. Engl. J. Med. 1989;321:406–412.
[57] Mahmarian JJ, Smart FW, Moyé LE, Young JB, Francis MJ, Kingry CL, Verani MS, Pratt CM. Exploring the minimal dose of amiodarone with antiarrhythmic and hemodynamic activity. Am. J. Cardiol. 1994;74:681–686.
[58] Herre JM, Sauve MJ, Malone P, Griffin JC, Helmy I, Langberg JJ, Goldberg H, Scheinman MM. Long term results of amiodarone therapy in patients with recurrent sustained ventricular tachycardia or ventricular fibrillation. J. Am. Coll. Cardiol. 1989;13:442–449.
[59] Fogoros RN, Anderson KP, Winkle RA, Swerdlow CD, Mason JW. Amiodarone: clinical efficacy and toxicity in 96 patients with recurrent, drug-refractory arrhythmias. Circulation. 1983;68:88–94.

J. Auer and B. Eber 198
[60] Kaski JC, Girotti LA, Messuti H, Rutitzky B, Rosenbaum MB. Long-term management of sustained, recurrent, symptomatic ventricular tachycardia with amiodarone. Circulation. 1981;64:273–279.
[61] Podrid PJ, Lown B. Amiodarone therapy in symptomatic sustained refractory atrial and ventricular tachyarrhythmias. Am. Heart J. 1981;101:374–379.
[62] Fogoros RN, Fielder SB, Elson JJ. Empiric amiodarone versus "ineffective" drug therapy in patients with refractory ventricular arrhythmias. Pacing Clin. Electrophysiol. 1988;11:1009–1017.
[63] Winkle RA. Amiodarone and the American way. J. Am. Coll. Cardiol. 1985;6:822–824.
[64] Weinberg BA, Miles WM, Klein LS, Bolander JE, Dusman RE, Stanton MS, Heger JJ, Langefeld C, Zipes DP. Five-year follow-up of 589 patients treated with amiodarone. Am. Heart J. 1993;125:109–120.
[65] Greene HL, Graham EL, Werner JA, Sears GK, Gross BW, Gorham JP, Kudenchuk PJ, Trobaugh GB. Toxic and therapeutic effects of amiodarone in the treatment of cardiac arrhythmias. J. Am. Coll. Cardiol. 1983;2:1114–1128.
[66] CASCADE Investigators. Cardiac Arrest in Seattle: Conventional versus amiodarone drug evaluation. Am. J. Cardiol. 1991;67:578–584.
[67] Coplen SE, Antman EM, Berlin JA, Hewitt P, Chalmers TC. Efficacy and safety of quinidine therapy for maintenance of sinus rhythm after cardioversion: a meta-analysis of randomized control trials. Circulation. 1990;82:1106–1116.
[68] The Antiarrhythmics Versus Implantable Defibrillators (AVID) Investigators. A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. N. Engl. J. Med. 1997;337:1576–1583.
[69] Connolly SJ, Gent M, Roberts RS, Dorian P, Roy D, Sheldon RS, Mitchell LB,Green MS, Klein GJ, O'Brien B. Canadian implantable defibrillator study (CIDS) : a randomized trial of theimplantable cardioverter defibrillator against amiodarone. Circulation. 2000;101:1297-302.
[70] Kuck KH, Cappato R, Siebels J, Ruppel R.Randomized comparison of antiarrhythmic drug therapy with implantabledefibrillators in patients resuscitated from cardiac arrest : the Cardiac ArrestStudy Hamburg (CASH). Circulation. 2000;102:748-54.
[71] Sarter BH, Finkle JK, Gerszten RE, et al. What is the risk of sudden cardiac death in patients presenting with hemodynamically stable sustained ventricular tachycardia after myocardial infarction? J. Am. Coll. Cardiol. 1996;28:122–9.
[72] Brugada P, Talajic M, Smeets J, et al. The value of the clinical history to assess prognosis of patients with ventricular tachycardia or ventricular fibrillation after myocardial infarction. Eur. Heart J. 1989;10:747–52.
[73] Stevenson WG, Ellison KE, Sweeney MO, Epstein LM, Maisel WH. Management of arrhythmias in heart failure. Cardiol. Rev. 2002;10:8-14.
[74] Scheinman MM, Levine JH, Cannom DS, Friehling T, Kopelman HA, Chilson DA, Platia EV, Wilbur DJ, Kowey PR, for the Intravenous Amiodarone Multicenter

Focus on Amiodarone in Prevention and Treatment of Cardiac Arrhythmia 199
Investigators Group. Dose-ranging study of intravenous amiodarone in patients with life-threatening ventricular tachyarrhythmias. Circulation. 1995;92:3264–3272.
[75] Levine JH, Massumi A, Scheinman MM, Winkle RA, Platia EV, Chilson DA, Gomes JA, Woosley RL. Intravenous amiodarone for recurrent sustained hypotensive ventricular tachyarrhythmias. J. Am. Coll. Cardiol. 1996;27:67–75.
[76] Kudenchuk PJ, Cobb LA, Copass MK, Cummins RO, Doherty AM, Fahrenbruch CE, Hallstrom AP, Murray WA, Olsufka M, Walsh T.Amiodarone for resuscitation after out-of-hospital cardiac arrest due to ventricular fibrillation. N. Engl. J. Med. 1999;341:871-8.
[77] 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2005;112:IV1–203. Cardiol. 1987; 59:1107–10.
[78] Dorian P, Cass D, Schwartz B, et al. Amiodarone as compared with lidocaine for shock-resistant ventricular fibrillation. N. Engl. J. Med. 2002;346:884 –90.
[79] Zehender M, Hohnloser S, Müller B, Meinertz T, Just H. Effects of amiodarone versus quinidine and verapamil in patients with chronic atrial fibrillation: results of a comparative study and a 2-year follow-up. J. Am. Coll. Cardiol. 1992;19:1054–1059.
[80] Kochiadakis GE, Igoumenidis NE, Marketou ME, Solomou MC, Kanoupakis EM, Vardas PE. Low-dose amiodarone versus sotalol for suppression of recurrent symptomatic atrial fibrillation. Am. J. Cardiol. 1998;81:995–998.
[81] Galve E, Rius T, Ballester R, Artaza MA, Arnau JM, Garcia-Dorado D, Soler-Soler J. Intravenous amiodarone in treatment of recent-onset atrial fibrillation: results of a randomized, controlled study. J. Am. Coll. Cardiol. 1996;27:1079–1082.
[82] Donovan KD, Power BM, Hockings BEF, Dobb GJ, Lee K-Y. Intravenous flecainide versus amiodarone for recent-onset atrial fibrillation. Am. J. Cardiol. 1995;75:693–697.
[83] McAlister HF, Luke RA, Whitlock RM, Smith WM. Intravenous amiodarone bolus versus oral quinidine for atrial flutter and fibrillation after cardiac operations. J. Thorac. Cardiovasc. Surg. 1990;99:911–918.
[84] Donovan KD, Power BM, Hockings BEF, Dobb GJ, Lee K-Y. Intravenous flecainide versus amiodarone for recent-onset atrial fibrillation. Am. J. Cardiol. 1995;75:693–697.
[85] Di Biasi P, Scrofani R, Paje A, Cappiello E, Mangini A, Santoli C. Intravenous amiodarone vs propafenone for atrial fibrillation and flutter after cardiac operation. Eur. J. Cardiothorac. Surg. 1995;9:587–591.
[86] Hohnloser SH, Meinertz T, Dammbacher T, Steiert K, Jähnchen E, Zehender M, Fraedrich M, Just H. Electrocardiographic and antiarrhythmic effects of intravenous amiodarone: results of a prospective, placebo-controlled study. Am. Heart J. 1991;121:89–95.
[87] Deedwania PC, Singh BN, Ellenbogen K, Fisher S, Fletcher R, Singh SN, for the Department of Veterans Affairs CHF-STAT Investigators. Spontaneous conversion and maintenance of sinus rhythm by amiodarone in patients with heart failure and atrial fibrillation. Circulation. 1998;98:2574–2579.

J. Auer and B. Eber 200
[88] Torp-Pedersen C, Moller M, Bloch-Thomsen PE, Kober L, Sandoe E, Egstrup K,Agner E, Carlsen J, Videbaek J, Marchant B, Camm AJ. Dofetilide in patients with congestive heart failure and left ventriculardysfunction. Danish Investigations of Arrhythmia and Mortality on DofetilideStudy Group. N. Engl. J. Med. 1999;341:857-65.
[89] Roy D, Talajic M, Dorian P, Connolly S, Eisenberg MJ, Green M, Kus T, LambertJ, Dubuc M, Gagne P, Nattel S, Thibault B. Amiodarone to prevent recurrence of atrial fibrillation. Canadian Trial of Atrial Fibrillation Investigators. N. Engl. J. Med. 2000;342:913-20.
[90] Atrial fibrillation follow-up investigation of rhythm management -- the AFFIRM study design. The Planning and Steering Committees of the AFFIRM study for the NHLBI AFFIRM investigators. Am. J. Cardiol. 1997;79:1198-202.
[91] Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Halperin JL, Le Heuzey J-Y, Kay GN, Lowe JE, Olsson SB, Prystowsky EN, Tamargo JL, Wann S, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Hunt SA, Nishimura R, Ornato JP, Page RL, Riegel B, Priori SG, Blanc J-J, Budaj A, Camm AJ, Dean V, Deckers JW, Despres C, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J, Osterspey A, Zamorano JL. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation—executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation). Circulation. 2006;114:700-752.
[92] Prystowsky EN. Management of atrial fibrillation: therapeutic options and clinical decisions. Am. J. Cardiol. 2000;85:3–11.
[93] Essebag V, Hadjis T, Platt RW, et al. Amiodarone and the risk of bradyarrhythmia requiring permanent pacemaker in elderly patients with atrial fibrillation and prior myocardial infarction. J. Am. Coll. Cardiol. 2003;41:249 –54.
[94] Cairns JA, Connolly SJ, Roberts R, et al. Randomised trial of outcome after myocardial infarction in patients with frequent or repetitive ventricular premature depolarisations: CAMIAT. Canadian Amiodarone Myocardial Infarction Arrhythmia Trial Investigators [published erratum appears in Lancet 1997 Jun 14;349(9067):1776]. Lancet. 1997;349:675–82.
[95] Singh SN, Fletcher RD, Fisher SG, et al. Amiodarone in patients with congestive heart failure and asymptomatic ventricular arrhythmia. Survival Trial of Antiarrhythmic Therapy in Congestive Heart Failure. N. Engl. J. Med. 1995;333:77– 82.
[96] Force T, Hibberd P, Weeks G, Kemper AJ, Bloomfield P, Tow D. Perioperative myocardial infarction after coronary artery bypass surgery. Clinical significance and approach to risk stratification. Circulation. 1990;82:903-12.
[97] Aranki SF, Shaw DP, Adams DH, Rizzo RJ, Couper GS, VanderVliet M. Predictors of atrial fibrillation after coronary artery surgery. Current trends and impact on hospital resources. Circulation. 1996;94:390-7.

Focus on Amiodarone in Prevention and Treatment of Cardiac Arrhythmia 201
[98] Auer J, Weber T, Berent R, Puschmann R, Hartl P, Ng CK, Schwart C, Lehner E, Strasser U, Lassnig E, Lamm G, Eber B. A comparison between oral antarrhythmic drugs in the prevention of atrial fibrillation after cardiac surgery: The Pilot Study of Prevention of Postoperative Atrial Fibrillation (SPPAF), a randomised placebo-controlled trial. Am. Heart J. 2004;147:636-43.
[99] Andrews TC, Reimold SC, Berlin JA, Antman EM. Prevention of supraventricular arrhythmias after coronary artery bypass surgery. A meta-analysis of randomized control trials. Circulation. 1991;84:III236-44.
[100] Daoud EG, Strickberger SA, Man KC, Goyal R, Deeb GM, Bolling SF. Preoperative amiodarone as prophylaxis against atrial fibrillation after heart surgery. N. Engl. J. Med. 1997;337:1785-91.
[101] Blommaert D, Gonzalez M, Mucumbitsi J, Gurné O, Evrard P, Buche M, et al. Effective prevention of atrial fibrillation by continuous atrial overdrive pacing after coronary artery bypass surgery. J. Am. Coll. Cardiol. 2000;35:1411-5.
[102] Cochrane AD, Siddins M, Rosenfeldt FL, Salamonsen R, McConaghy L, Marasco S. A comparison of amiodarone and digoxin for treatment of supraventricular arrhythmias after cardiac surgery. Eur. J. Cardiothorac. Surg. 1994;8:194-8.
[103] Franklyn JA, Davis JR, Gammage MD. Amiodarone and thyroid hormone action. Clin. Endocrinol. 1985; 22: 257–264.
[104] Figge HL, Figge J. The effects of amiodarone on thyroid hormone function: a review of the physiology and clinical manifestations. J. Clin. Pharmacol. 1990; 30: 588–595.
[105] Newman CM, Price A, Davies DW. Amiodarone and the thyroid: a practical guide to the management of thyroid dysfunction induced by amiodarone therapy. Heart. 1998; 79: 121–127.
[106] Martino E, Safran M, Aghini-Lombardi F. Environmental iodine intake and thyroid dysfunction during chronic amiodarone therapy. Ann. Intern. Med. 1984; 101: 28–34.
[107] Bartalena L, Grasso L, Brogioni S. Serum interleukin-6 in amiodarone-induced thyrotoxicosis. J. Clin. Endocrinol. Metab. 1994; 78: 423–427.
[108] Bartalena L, Brogioni S, Grasso L. Treatment of amiodarone-induced thyrotoxicosis, a difficult challenge: results of a prospective study. J. Clin. Endocrinol. Metab. 1996; 81: 2930–2933.
[109] Osman F, Franklyn JA, Sheppard MC, Gammage MD. Successful treatment of amiodarone-induced thyrotoxicosis. Circulation. 2002;105:1275-7.


In: Cardiac Arrythmia Research Advances ISBN: 978-1-60021-795-1 Editor: Lynn A. Vespry, pp. 203-215 © 2007 Nova Science Publishers, Inc.
Chapter VIII
Ongoing Atrial Remodeling in Permanent Atrial Fibrillation: Value of
Brain Natriuretic Peptide Monitoring for High-Risk Patient Identification
John Dernellis* and Maria Panaretou Department of Cardiology, Vostanion Hospital, Mytilini, Greece
Abstract
Background: The progression of permanent atrial fibrillation (AF) is related to ongoing atrial remodeling, which may be detected by brain natriuretic peptide (BNP). We examined the prevalence and prognostic value of increased BNP concentrations in serial blood specimens from patients with persistent AF.
Methods and Results: Clinical, and echocardiographic data were collected prospectively at baseline and at 1 year in 193 outpatients (mean age, 62±11 years; 78% men; 63% coronary heart disease) with persistent AF and a left atrial diameter > 50 mm. Blood samples were collected at baseline and at 3, 6, and 12 months of follow-up. BNP concentrations >100 pg/mL were considered abnormal. In 100 patients (52%), BNP was consistently <100 pg/mL (group 1); 55 (28%) had a single abnormal BNP result (group 2); and 38 (20%) had >2 abnormal BNP results (group 3). At 18 months, hospitalisation for heart failure (HF) was 9%, 26%, and 40%, respectively (P<0.001). In a Cox proportional-hazards model, left atrial diameter at 12 months (HR=1.35; 95% CI, 1.09 to 1.67), highest BNP (HR=1.01; 95% CI, 1.007 to 1.013), and number of abnormal BNP samples (HR=2.34; 95% CI, 1.60 to 3.43) were independently associated with prognosis. A BNP rise of 10 pg/mL in any sample was associated with an excess of 10% (95% CI, 7% to 13%) in the incidence of combined end point.
* Address for correspondence: Dr. John Dernellis, 1 Kathigitou Karakatsani St, 811 00 Mytilini, Greece. Tel. and
Fax. (+30) 2251 0 26 588; Email: [email protected]

John Dernellis and Maria Panaretou 204
Conclusions: Abnormal BNP concentrations were detected in about 50% of outpatients with persistent AF. This ongoing atrial remodeling was a strong predictor of worsening HF, suggesting a role of BNP-based monitoring to identify high-risk patients.
Keywords: atrial fibrillation, atrial remodeling, brain natriuretic peptide, heart failure, prognosis.
Introduction There is a strong association between atrial fibrillation (AF) and heart failure (HF): not
only do 50% of patients with AF develop HF, but the prevalence of AF increases with the severity of HF and with age. [1,2] The prevalence of AF approximates 20% in HF trial populations and 40% in community epidemiologic studies. There is a reciprocal association between the two conditions. HF increases the risk of AF 4.5-fold and 5.9-fold in men and women, respectively. [2-4] Progression of HF manifests clinically as a loss of functional capacity, declining quality of life, deterioration of ventricular function, and high hospitalization and mortality rates, with important consequences for public health. [5,6]
The ventricular pump dysfunction and neuroendocrine changes that characterize the HF syndrome are associated with high-frequency depolarisation of the fibrillating atrium. [7] This induces atrial remodelling and has generated the concept AF-dependent cardiomyopathy. [8] Atrial remodelling refers to the constellation of atrial changes – in electrophysiology, ion channels, biochemistry, anatomy, histology, and mechanics – resulting from persistent AF. [9] Atrial remodelling is the currently accepted mechanism for the progression and clinical development of AF. Although several factors contribute to this remodelling, activation of the sympathetic, neurohormonal and natriuretic peptides systems plays a key role. [10]
Circulating brain natriuretic peptide (BNP) is elevated in AF and in HF and correlates directly with functional class. [11] In normal human hearts there is a low level of BNP expression. In HF, the atria content of BNP increases 10-fold. [12] BNP secretion appears to be regulated mainly by wall tension. In addition to their beneficial effects on neurohormones, renal function and hemodynamics, there is evidence that BNP may directly inhibit myocyte and vascular smooth muscle hypertrophy and interstitial fibrosis. [13]
We hypothesized that the leak of BNP during the phase of permanent AF may be a sign of ongoing subclinical atrial remodelling. This study (1) examined the prevalence of increased concentrations of BNP in serial blood samples collected from ambulatory patients
with permanent AF and (2) tested the hypothesis that persistently increased concentrations of BNP in these patients are associated with a worse long-term outcome.
Methods Our Institutional Committee approved this study, and all patients granted their written
informed consent to participate. 115 consecutive patients from the Outpatient Department, with a diagnosis of permanent AF present for > 3 months and a left atrial diameter (LAD) >

BNP Predict Atrial Remodeling 205
50 mm, were prospectively included in the study if they fulfilled at least one of the following
criteria. History of hospitalisation for a symptomatic and persistent episode of AF which cannot
be cardioverted to sinus rhythm. Permanent AF indicates the inability of pharmacologic or electrical cardioversion to restore sinus rhythm. [14]
History of hospitalization because of permanent AF, including the following manifestations: (a) palpitations, chest pain, shortness of breath, dyspnea, fatigue, polyuria or lightheadedness, (b) tachyarrhythmia on electrocardiogram (ECG).
History of stroke, and additionally signs and symptoms of AF (dyspnea on exertion, palpitations, chest pain, or fatigue) and ECG evidence of AF.
History of AF on ECG at the time of initial evaluation or during a hospitalization. In addition, all patients had to have remained clinically stable for > 3 months after a
hospital admission for cardiac decompensation. Patients were excluded if they had (1) an acute coronary syndrome in the previous 3
months (unstable angina, acute myocardial infarction, or a percutaneous or surgical revascularization procedure); (2) the presence of a life-limiting malignancy, hepatic or renal disease, or a baseline creatinine concentration >2.5 mg/dL; or (3) refusal to participate in the study.
Study Protocol On initial evaluation, a clinical examination was performed. The functional class was
graded according to number of METS reached during a specific activity, determined by a specific questionnaire, [15] and classified as class I if the exercise capacity was >7 METS, class II if between 5 and 7 METS, class III if between 2 and 5 METS, and class IV if it was <2 METS. A chest roentgenogram and ECG were obtained in all patients.
Baseline therapy included angiotensin-converting enzyme inhibitors or angiotensin receptor blockers (68% of patients), β-adrenergic blockers (65%), diuretics (34%), calcium channel antagonists (49%), digoxin (63%), amiodarone (21%), antiplatelet agents (55%), and antithrombotics (91%).
2D Echocardiography Two-dimensional and M-mode echocardiograms were performed at baseline and at 12
months. A Hewlett Packard, Image Point echograph and a 2.5 MHz transducer was used, and the studies were recorded on videocassette with recorder. The measurements were made in both modes, and left atrial diameter (LAD) was measured by directing the M-Mode echo beam to the aortic root; the ventricular volumes and left ventricular ejection fraction (LVEF) were calculated by Simpson’s modified method. [16]

John Dernellis and Maria Panaretou 206
Laboratory Screening Fasting blood samples were obtained for measurements of chemistry panel.
Measurements of BNP were carried out from fresh plasma sample with an AxSYM system (produced by Axis-Shield Diagnostics, Ltd., Dundee, UK). BNP was measured quantitatively by means of a Microparticle Enzyme Immunoassay (MEIA). EDTA plasma was used for AxSYM BNP assay. Samples were collected in plastic collection tubes. BNP binds to the coated micro-particles with monoclonal antibody to form antigen-antibody complexes. Fluorescent product 4-methylumbelliferone was yielded with specific process and is measured by the optical assembly. The AxSYM BNP assay demonstrated imprecision <12% in a study run according to the National Committee for Clinical Laboratory standards (NCCLS) protocol ER5-A. [17] The analytic sensitivity of the assay was <15 pg/ml in a study where the AxSYM BNP Standard Calibrator A (0 pg/ml) was assayed multiple times. Concordance with a commercially available diagnostic kit was 91.4%. [18] The primary physicians were unaware of the troponin results, and the laboratory was not informed of the patient’s
condition.
Follow-up Schedule Patients were followed up in our Outpatient Department, with visits scheduled at 3, 6,
and 12±3 months. Blood samples were drawn for measurements of BNP. Functional capacity, LAD, and LVEF were measured at baseline in all patients and at 12 months in the survivors.
Definitions and Study End Points The combined primary end point of the study was all-cause mortality and hospitalization
for HF at 18 months of follow-up. The development of signs and/or symptoms of cardiac decompensation requiring an increase in doses of diuretics or addition of other drugs was defined as worsening HF. Visits to the emergency room for decompensated HF were defined as emergency visits for HF. Hospitalisation for worsening HF that required the administration of intravenous diuretics, inotropes, and/or vasodilators for >12 hours was defined as hospitalisation for HF.
Statistical Analysis Patients were included in group 1 if all BNP measurements were within normal limits,
group 2 with a single abnormal sample, and group 3 with > 2 abnormal ones. All patients had >3 samples during the study period. Categorical variables are expressed as percentages, and they were compared by use of the Pearson Χ2 test; a Fisher exact test correction was used to compare patients with versus without events. Continuous variables are presented as mean±SD and were compared among the 3 groups by 1-way ANOVA using the Bonferroni test as a post

BNP Predict Atrial Remodeling 207
hoc contrast analysis. The Mann-Whitney t or U tests were used for comparisons of independent samples. Comparisons of variables between baseline and 12 months were made with the Wilcoxon matched-pairs signed-rank test. To establish the optimal BNP cutoff point
for prognostic purposes, the area under the receiver operating characteristic (ROC) curve corresponding to the highest BNP level ever obtained during follow-up in an individual patient was determined with regard to combined end point. Differences with probability values <5% were considered statistically significant. Hospitalization-free survival curves were constructed by the Kaplan-Meier method and compared by log-rank test. Cox proportional-hazards model was built using variables significantly associated with the
combined study end point in univariate analysis with BNP. All statistical analyses were performed with the SPSS 8.0 program.
Results The mean age was 62±11 years, and 78% were men. Ischemic heart disease was present
in 63% of patients, 27 (14%) had been hospitalized for management of HF in the previous year, and 25% of patients were in HF functional class III–IV (table 1).
The results of the BNP measurements are detailed in table 2. Two patients (1%) who died
within the first 3 months had a single BNP measurement, 99% had >2, 95% had >3, and 92% had 4 BNP specimens.
Table 1. Baseline Characteristics of Each Study Group
Group 1 Group 2 Group 3 P Patients, n (%) 100 (52) 55 (28) 38 (20) ... Age, y (mean±SD) 61±11 64±9 61±11 0.113 Male, n (%) 76 (76) 45 (82) 29 (76) 0.688 Hypertension, n (%) 55 (55) 31 (56) 29 (76) 0.063 Diabetes, n (%) 22 (22) 6 (11) 7 (18) 0.230 Previous myocardial infarction, n (%) 11 (11) 24 (44) 18 (47) 0.001 Ischemic heart disease, n (%) 58 (58) 36 (65) 28 (74) 0.214 Functional class III–IV, n (%) 29 (29) 14 (25) 6 (16) 0.281 Hospitalization in last year, n (%) 11 (11) 11 (20) 5 (13) 0.299
Table 2. Rates of Abnormal BNP Samples at Baseline and at 3, 6, and 12 Months
Months of Follow-Up Baseline 3 6 12
Patients with samples available, n (%)* 193 (100) 191 (99) 185 (96) 180 (93) BNP > 100 pg/mL, n (%)+ 45 (23) 54 (55) 54 (57) 47 (51) Mean value±SD, pg/mL 103±75 105±74 108±83 100±79 Range, pg/mL 28–352 30–334 29–388 34–387
*Percentages are relative to the entire patient population. +Percentages are relative to the total number of patients with samples available.

John Dernellis and Maria Panaretou 208
Grades of Atrial Remodeling
There were 100 (52%), 55 (28%), and 38 (20%) patients included in groups 1, 2, and 3,
respectively. The baseline characteristics are compared among groups in table 1. History of previous myocardial infarction increased from group 1 to group 3. The physical findings and baseline laboratory evaluation are detailed in table 3. Renal function, LVEF and LAD worsened as the degree of BNP levels increased.
Table 3. Baseline Physical Findings, ECG, Biochemistry, and Echocardiogram
Group 1 Group 2 Group 3 P Blood pressure, mm Hg Systolic 121±11 118±9 120±10 0.185 Diastolic 75±8 74±9 75±9 0.834 Heart rate, bpm 75±8 76±6 75±8 0.729 Creatinine, mg/dL 1.36±0.07 1.43±0.04 1.47±0.06 0.001 C-reactive protein, mg/dL 2.84±1.23 2.70±1.37 2.92±1.34 0.692 LV ejection fraction, (%) 56.6±3.5 53.0±3.2 51.5±2.7 0.001 LAD, mm 56.4±2.5 61.1±2.1 65.3±2.2 0.001
Evolution of Functional Capacity, LVEF, and LAD Functional class, LVEF and LAD worsened between baseline and 1 year in groups 2 and
3 and remained unchanged in group 1 (table 4).
Table 4. Changes in Functional Capacity, LVEF, and LAD Between Baseline and 12 Months Among Study Groups
Group Baseline 12 Months P Functional class 1 1.7±1.0 1.7±0.7 NS 2 1.9±0.9 2.2±1.0 0.001 3 2.2±0.9 2.8±0.9 0.001 P (among groups) 0.05 0.001 LVEF, % 1 56.6±3.5 55.6±6.2 NS 2 53.0±3.2 50.4±3.0 0.001 3 51.5±2.7 46.5±2.4 0.001 P (among groups) 0.001 0.001 Left atrial diameter, mm 1 56.4±2.5 56.3±2.6 NS 2 61.1±2.1 64.2±2.3 0.001 3 65.3±2.2 71.7±2.5 0.001 P (among groups) 0.001 0.001

BNP Predict Atrial Remodeling 209
BNP and Long-Term Outcomes Worsening HF was observed in 14%, 31%, and 45% of patients in groups 1, 2, and 3,
respectively (P<0.001), and emergency visits for HF in 10%, 29%, and 42% of patients, respectively (P<0.001). Hospitalisations for HF were 9% in group 1, 26% in group 2, and 40% in group 3 (P<0.001). Respective overall death rates were 1%, 11%, and 24% (P<0.001).
Survival time free of hospitalization for decompensated HF was 17.6, 15.2, and 13.2 months in groups 1, 2, and 3 (P<0.001, figure 1). Survival time free of death was 18.0, 17.0, and 15.2 months in groups 1, 2, and 3 (P<0.001, figure 2).
Time (months)
0 2015105
.7
.6
1.1
1.0
.9
.8
.5
Group 3= 61%
P<0.001
Group 1= 91%
Group 2= 75%
Hosp
ital
isat
ion f
ree
surv
ival
Figure 1. Hospitalization (for HF) – free survival according to degree of atrial remodelling. Group 1: all BNP samples within normal limits; group 2: a single BNP sample abnormal; group 3: >2 abnormal BNP measurements.

John Dernellis and Maria Panaretou 210
Time (months)
2 20148
.7
1.1
1.0
.9
.8 Group 3= 76%
P<0.001
Group 1= 99%
Group 2= 89%
Dea
th f
ree
surv
ival
Figure 2. Death – free survival according to degree of atrial remodelling. Group 1: all BNP samples within normal limits; group 2: a single BNP sample abnormal; group 3: >2 abnormal BNP measurements.
Highest Level of BNP and Outcome: Importance of BNP Index The area under the ROC curve of highest BNP level was 0.75 (95% CI, 0.66 to 0.82) to
predict the combined end point, and a 177-pg/mL cutoff showed a sensitivity of 74% and specificity of 76% (figure 3).
Figure 3. Highest level of BNP and outcome. Area under ROC curve of highest BNP level obtained during follow-up related to combined end point.

BNP Predict Atrial Remodeling 211
Prognostic Role of BNP Monitoring Variables associated with the combined end point are shown in table 5. In the Cox
proportional-hazards model, the variables independently associated with the primary end point were LAD at 12 months (hazard ratio [HR]=1.35), highest BNP value (HR=1.01), and number of abnormal BNP results (HR=2.34). Thus, for each increment of 10 pg/mL in BNP obtained in any sample, there was an excess of 10% (95% CI, 7% to 13%) in the incidence of death or hospitalization for worsening heart failure.
Table 5. Prediction of Death or Hospitalization for Heart
Failure by Cox Proportional Hazard Model
P HR (95%CI) LAD at 12 months (mm)) 0.01 1.35 (1.09–1.67) Highest BNP (pg/ml) 0.001 1.01 (1.007–1.013) Number of abnormal BNP results (Groups 1 to 3) 0.001 2.34 (1.60–3.43)
Discussion
This study demonstrated that leaks of BNP by monitoring of serial concentrations during
the follow-up of optimally treated outpatients with permanent AF is a frequent finding that identifies a high-risk population in the long term and suggests an ongoing internal process of atrial remodeling despite an otherwise stable clinical condition. Furthermore, the presence of persistently increased BNP concentrations is a powerful independent predictor of death or hospitalization for HF.
Changes in atrial size are consistent with the observation that AF begets AF. Recently, the effect of persistent AF on changes in atrial size were investigated in 15 patients; [19] during an average of 20.6 months mean left atrial volume significantly increased. In another study, atrial size was evaluated at six-months of follow-up after cardioversion in patients in whom sinus rhythm persisted compared with those in whom AF recurred. [20] Importantly, in the patients in whom sinus rhythm was maintained, left atrial volume decreased; in contrast atrial size was increased in patients in whom AF recurred. In dogs subjected to sustain AF, electrophysiologic, anatomic and pathologic changes were noted to occur over time. [21] There was biatrial enlargement, disruption of the sarcoplasmic reticulum, increase in mitochondrial size, decreases in atrial refractoriness and the ability to sustain AF.
The relationship between BNP, AF and HF has been studied in various clinical settings. In the ambulatory care setting, both symptomatic and asymptomatic patients with chronic, stable systolic HF may present with a wide range of plasma BNP levels. [11] Patients in the "normal BNP" diagnostic range (<100 pg/mL) were less likely to have AF. In acute HF the impact of AF on the diagnostic performance of BNP was studied. [22] Patients were prospectively classified according to the presence or absence of permanent or paroxysmal AF. In patients without HF, AF was associated with significantly higher BNP levels. Conversely, in patients with HF, BNP levels did not differ significantly between patients with

John Dernellis and Maria Panaretou 212
and without AF. In another study, [23] it has been found that AF influences cardiac BNP release during haemodynamic stress in HF.
Evolutionary Patterns of Atrial Remodeling and Prognostic Role of BNP Monitoring
At baseline, the clinical characteristics of groups 2 and 3 were indicative of higher risk.
These 2 groups had larger left atrial diameters, and lower LVEF. Over time, functional class, LVEF and LAD deteriorated significantly in groups 2 and 3. The incidence of study end points was consistent with a population at risk followed up in HF patients. [24-26] BNP monitoring identified a population with permanent AF at high risk for hospitalization for HF. More importantly, BNP monitoring and atrial remodeling were independent predictors of the study end point. Previous studies, particularly in patients hospitalised for decompensated HF, have confirmed the prognostic value of BNP.
Two mechanisms of atrial remodelling in permanent AF could be hypothesized. First, in the ambulatory setting, patients may have low-grade ongoing haemodynamic stress, either by an increase in atrial stress or by other phenomena causing left ventricular systolic or diastolic dysfunction. This identifies high-risk patients with higher remodelling vulnerability. Second,
in the event of additional atrial remodelling, or because of their greater susceptibility to minor events, such as a pressure or volume overload, these patients rapidly develop decompensated HF. Under these new conditions, the marker may increase further, as has been described in patients with acute dyspnea, in whom it is difficult to distinguish between BNP increases from HF versus from true pulmonary disease. [27]
Clinical Implications Because atrial remodelling has been related to the progression of HF, monitoring of BNP
offers a means of identifying a subgroup of patients with remodelling vulnerability and at increased risk. Patients with permanent AF might be monitored periodically through BNP. The association between high levels of BNP and ventricular remodelling was recently reported, suggesting that uptitration of β-blockers and ACE inhibitors, drugs with anti-remodelling effects, should be recommended. [28,29] This contribution for should be tested via the efficacy of several drugs on the production or mitigation of atrial remodelling and impact on risk or clinical benefit.
In conclusion, the serial detection of increased BNP concentrations in ambulatory patients with permanent AF was associated with an unfavorable clinical evolution. Long-term monitoring of atrial remodeling was a strong prognosticator, suggesting that this strategy may
play a useful role in the detection of high-risk patients.

BNP Predict Atrial Remodeling 213
References
[1] Yamada T, Fukunami M, Shimonagata T, Kumagai K, Ogita H, Asano Y, Hirata A, Masatsugu H, Hoki N. Prediction of paroxysmal atrial fibrillation in patients with congestive heart failure: a prospective study. J. Am. Coll. Cardiol. 2000;35(2):405-13.
[2] Kannel WB, Wolf PA, Benjamin EJ, Levy D. Prevalence, incidence, prognosis and predisposing conditions for atrial fibrillation: population-based estimates. Am. J. Cardiol. 1998;82:2N-9N.
[3] Fuster V, Ryden L, Asinger R, Cannom D, Crijns H, Frye R, Halperin J, Kay G, Klein W, Levy S, McNamara R, Prystowsky E, Wann L, Wyse D. ACC/AHA/ESC Guidelines for the Management of Patients With Atrial Fibrillation: Executive Summary A Report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation) Circulation. 2001;104:2118-50.
[4] Allessie MA, Boyden PA, Camm AJ, Kleber AG, Lab MJ, Legato MJ, Rosen MR, Schwartz PJ, Spooner PM, Van Wagoner DR, Waldo AL. Pathophysiology and prevention of atrial fibrillation. Circulation. 2001;103(5):769-77.
[5] Adams KF. New epidemiologic perspective concerning mild-to-moderate heart failure. Am. J. Med. 2001;110:6S–13S.
[6] Cleland J. Is the prognosis of heart failure improving? Eur. J. Heart Failure. 1999;1:229–241.
[7] Nattel S. Atrial electrophysiological remodeling caused by rapid atrial activation: underlying mechanisms and clinical relevance to atrial fibrillation. Cardiovasc. Res. 1999;42(2):298-308.
[8] Schoonderwoerd BA, Van Gelder IC, van Veldhuisen DJ, Tieleman RG, Grandjean JG, Bel KJ, Allessie MA, Crijns HJ. Electrical remodeling and atrial dilation during atrial tachycardia are influenced by ventricular rate: role of developing tachycardiomyopathy. J. Cardiovasc. Electrophysiol. 2001;12(12): 1404-10.
[9] Yue L, Melnyk P, Gaspo R, Wang Z, Nattel S. Molecular mechanisms underlying ionic remodeling in a dog model of atrial fibrillation. Circ. Res. 199916;84(7):776-84.
[10] Morton JB, Byrne MJ, Power JM, Raman J, Kalman JM. Electrical remodeling of the atrium in an anatomic model of atrial flutter: relationship between substrate and triggers for conversion to atrial fibrillation. Circulation. 2002;105(2):258-64.
[11] Tang WH, Girod JP, Lee MJ, Starling RC, Young JB, Van Lente F, Francis GS. Plasma B-type natriuretic peptide levels in ambulatory patients with established chronic symptomatic systolic heart failure. Circulation. 2003;108(24):2964-6.
[12] Ferrari R, Ceconi C, Curello S, Visioli O. The neuroendocrine and sympathetic nervous system in congestive heart failure. Eur. Heart J. 1998;19(suppl F):F45-F51.
[13] Ogawa Y, Itoh H, Nakao K. Molecular biology and biochemistry of natriuretic peptide family. Clin. Exp. Pharmacol. Physiol. 1995;22:49-53.

John Dernellis and Maria Panaretou 214
[14] Dernellis J, Panaretou M. Relationship between C-reactive protein concentrations during glucocorticoid therapy and recurrent atrial fibrillation. Eur. Heart J. 2004;25(13):1100-1107.
[15] Goldman L, Hashimoto B, Cook EF, Loscalzo A. Comparative reproducibility and validity of systems for assessing cardiovascular functional class: advantages of a new specific activity scale. Circulation. 1981;64:1227–1234.
[16] Dernellis JM, Panaretou MP. Effects of digoxin on left atrial function in heart failure. Heart. 2003;89(11):1308-15.
[17] National Committee for Clinical Laboratory Standards. Evaluation of precision performance of clinical chemistry devices; Approved Guideline. NCCLS Document EP5-A, Wayne, PA: NCCLS, 1999.
[18] National Committee for Clinical Laboratory Standards. Method comparison and bias estimation using patient samples; Approved Guideline. NCCLS Document EP9-A, Wayne, PA: NCCLS, 1995.
[19] Sanfilippo AJ, Abascal VM, Sheehan M, Oertel LB, Harrigan P, Hughes RA, Weyman AE. Atrial enlargement as a consequence of atrial fibrillation. A prospective echocardiographic study. Circulation. 1990;82(3):792-7.
[20] Gosselink AT, Crijns HJ, Hamer HP, Hillege H, Lie KI. Changes in left and right atrial size after cardioversion of atrial fibrillation: Role of mitral valve disease. J. Am. Coll. Cardiol. 1993;22:1666-1672.
[21] Morillo CA, Klein GJ, Jones DL, Guiraudon CM. Chronic rapid atrial pacing. Structural, functional, and electrophysiological characteristics of a new model of sustained atrial fibrillation. Circulation. 1995 Mar 1;91(5):1588-95.
[22] Knudsen CW, Omland T, Clopton P, Westheim A, Wu AH, Duc P, McCord J, Nowak RM, Hollander JE, Storrow AB, Abraham WT, McCullough PA, Maisel A. Impact of atrial fibrillation on the diagnostic performance of B-type natriuretic peptide concentration in dyspneic patients: an analysis from the breathing not properly multinational study. J. Am. Coll. Cardiol. 2005; 46(5):838-44.
[23] Gould PA, D'Agostino J, Schneider HG, Kaye DM. Influence of atrial fibrillation on cardiac brain natriuretic peptide release during haemodynamic stress in heart failure. Eur. J. Heart Fail. 2005;
[24] Rich MW. Heart failure disease management: a critical review. J. Card Fail. 1999;5:64–75.
[25] McAlister FA, Lawson FME, Teo KK, Armstrong PW. A systematic review of randomized trials of disease management programs in heart failure. Am. J. Med. 2001;110: 378–384.
[26] Fonarow GC, Stevenson LW, Walden JA, Livingston NA, Steimle AE, Hamilton MA, Moriguchi J, Tillisch JH, Woo MA. Impact of a comprehensive heart failure management program on hospital readmission and functional status of patients with advanced heart failure. J. Am. Coll. Cardiol. 1997;30:725–732.
[27] Maisel A, Hollander JE, Guss D, McCullough P, Nowak R, Green G, Saltzberg M, Ellison SR, Bhalla MA, Bhalla V, Clopton P, Jesse R; Rapid Emergency Department Heart Failure Outpatient Trial investigators. Primary results of the Rapid Emergency Department Heart Failure Outpatient Trial (REDHOT): a multicenter study of B-type

BNP Predict Atrial Remodeling 215
natriuretic peptide levels, emergency department decision making, and outcomes in patients presenting with shortness of breath. J. Am. Coll. Cardiol. 2004;44(6):1328-33.
[28] Atisha D, Bhalla MA, Morrison LK, Felicio L, Clopton P, Gardetto N, Kazanegra R, Chiu A, Maisel AS. A prospective study in search of an optimal B-natriuretic peptide level to screen patients for cardiac dysfunction. Am. Heart J. 2004;148(3):518-23.
[29] Suttner SW, Boldt J. Natriuretic peptide system: physiology and clinical utility. Curr. Opin. Crit. Care. 2004;10(5):336-41.


In: Cardiac Arrythmia Research Advances ISBN: 978-1-60021-795-1 Editor: Lynn A. Vespry, pp. 217-230 © 2007 Nova Science Publishers, Inc.
Chapter IX
Cardiac Involvement in Parkinson’s Disease
Carl-Albrecht Haensch* Department of Neurology and Clinical Neurophysiology of the University of
Witten/Herdecke; HELIOS Klinikum Wuppertal; Heusnerstr. 40; D-42283 Wuppertal; Germany
Abstract
Sympathetic neurocirculatory failure in Parkinson`s disease is common. Orthostatic hypotension is the most frequent symptom. Cardiovascular disturbances have so far been met with the highest degree of clinical and scientific interest. Histological studies have proven the presence of Lewi`s bodies in sympathetic and parasympathetic neurons and also in central structures associated with the autonomic regulation.
Extrasystoles occur in normal subjects, but are more frequently seen in Parkinson patients. Heart rate variability is a useful non-invasive test to assess autonomic dysfunction in PD. It allows a differentiation of the sympathetic and parasympathetic activation, which are related to a low-frequency (0.05 - 0.15 Hz; LF) and a high-frequency (0.15-0.5Hz; HF) component of the heart rate variability (HRV) signal, respectively. The resulting LF/HF ratio is a quantitative index of the sympatho-vagal balance. The physiological function of HRV is commonly known to be to buffer changes in blood pressure. In the PD-patients group (n=107, mean age 71 years, mean PD-duration 7.0 years, Hoehn and Yahr 3.0 ± 0.9) the LF/HF ratio was lower than in the control group in rest (2.19 vs. 1.25, p < 0.05); in deep respiration (3.3 vs. 2.4, p < 0.01) and in tilt-table testing (2.6 vs 1.9, p < 0.01). The LF/HF ratio in tilt-table testing was significantly more reduced in PD with OH than without (2.1 vs. 1.3, p < 0.05). Scintigraphy with 123I-Metaiodobenzylguanidine (MIBG) appears to be a highly sensitive and useful in demonstrating sympathetic postganglionic cardiac nerve disturbances. In the heart, MIBG uptake in all examined 57 Parkinson's (PD) patients was decreased (H/M-Ratio: 1.14 ± 0.16). Loss of sympathetic innervation of the heart seems to occur
* Carl-Albrecht Haensch: Email: [email protected]

Carl-Albrecht Haensch 218
independent of orthostatic hypotension and baroreflex failure in PD. We found no correlation between myocardial MIBG uptake and sympathovagal balance, blood pressure or other autonomic findings. This results could be explained by different time course of loss of intact postganglionic sympathetic cardial innervation and disturbed baroreflex response or the involvement of central autonomic pathways in PD.
The significance of the abnormalities in cardiovascular regulation among PD patients is not fully known yet. It is possible that the dysbalance of the sympathetic and parasympathetic tone is connected with heart arrhytmias. The connection between autonomic dysregulation and arrhythmia related death has recently been considered in PD. The mortality of PD patients is almost twice that for age and sex-matched healthy control groups. Parkinson`s disease is a continuously progressive degenerative disorder of the central,
peripheral and autonomic human nervous systems. Affecting an estimated 1% of the population over the age of 65 years, it causes tremor, bradykinesia, rigidity, and the loss of postural reflexes [31]. In addition to major motor symptoms, patients with Parkinson`s disease (PD) are known to suffer from disturbances of the autonomic nervous system. The most common autonomic dysfunction is orthostatic hypotension. However, symptoms of dysautonomia are variable, and include cardiovascular symptoms, gastrointestinal, urogenital, sudomotor and thermoregulatory dysfunction, pupillary abnormalities, sleep and respiratory disorders [58]. About 60-80 % of PD-patients shows signs of autonomic dysfunction, some leading to severe complications such as urinary tract infections, falls and megacolon. Such nonmotor features are often not formally assessed and may be frequently misdiagnosed, so the true prevalence remains poorly defined [28, 42, 58]. Magerkurth et al. estimated that about 50% of PD patients rated the impact of the symptoms of autonomic failure on their daily lives as "a lot" or "very much" due to orthostatic dizziness, bladder dysfunction and constipation, which were more statistically significant than in age-matched controls [50]. The combined effects of aging and PD on the autonomic nervous system result in a high prevalence of orthostatic hypotension when dopamine agonists are prescribed, frequently not recognized by patients or their doctors unless systematically examined for [49]. The high prevalence of orthostatic hypotension likely contributes to the high prevalence of falls, and hip fracture, reported in these patients [48].
In addition to the dopaminergic system, the degenerative process of PD also involves noradrenergic locus coeruleus, the dorsal motor vagal nucleus and the cholinergic nucleus basalis of Meynert [40]. Lewy bodies which are eosinophilic intracytoplasmic inclusions, accompany the nerve cell loss with reactive gliosis in structures involved in autonomic regulation, are found in multiple areas of brain, spinal cord and in sympathetic and parasympathetic neurons [13, 14, 41]. Baroreceptor afferent activity, relayed and integrated in central medullary autonomic nuclei such as the nucleus tractus solitarius, increases vagal and inhibits sympathetic discharge to the heart, and inhibits vasoconstrictor discharge to resistance vessels. Because the PD process seems to involve the central nuclei as well as the peripheral autonomic ganglia and also the hypothalamus, the cardiovascular dysregulation may be of both central and peripheral origin [77]. Thus the cardiovascular autonomic control and reactivity system may be injured at multiple sites.

Cardiac Involvement in Parkinson’s Disease 219
First Complaints, Early Diagnosis and Autonomic Disturbances
In average it takes two years to diagnose Parkinson´s disease after the onset of first
complaints. Because parkinsonism is common among elderly people and its prevalence increases markedly with age, there are important public health concerns as the worldwide life expectations grow steadily. PD belongs to the most frequent neurodegenerative illnesses and concerns up to one per cent of people older than 65 years. Although usually the onset of classic symptoms like rest tremor, bradykinesia, and rigidity allows the correct diagnosis, the early diagnosis is often difficult. Clinical signs of dysautonomia are often non-specific, and dizziness due to orthostatic hypotension may be difficult to recognize [37, 53]. The latter is important for two reasons: Recently, some drugs may have had a neuroprotective effect when given in an early state of the disease. Though there exist well-established regimes for the treatment of PD, in the beginning nonspecific symptoms can cause diagnostic mistakes. Concerning the relationship between patient and doctor, a late diagnosis often leads to a loss of confidence. Partially unnecessary and expansive investigations should be avoided.
It was the aim of our previous study based on a group of 73 patients (42 female, 31 male; mean age 69 ± 11 [39-87] years) suffering from PD to find out subjective complaints in early stages, motives for visit and the time lag from the first onset of unspecific complaints until diagnosis [35]. Clinical diagnosis of idiopathic definite PD was made according to the criteria set forth by the U.K. Parkinson's Disease Society Brain Bank [39]. The method was based on on anonymous, structured questionnaire about 26 items. We estimated the mean interval between onset of discomforts until diagnosis to be about 2 years (± 4,4 [0-20] y.). First onset of shoulder or brachial pain (72 % vs. 47%; p= 0,001), sleep disturbance (72 % vs. 47 %; p=0,001), inappetence (36% vs. 14 %; p=0,008), “internally tremblement“ (81% vs., 56 %; p<0,001) and dysarthrophonia (72 % vs. 58 %; p=0,018) correlate significantly with a delayed (more than 2 years) diagnosis finding. Moreover, Parkinsonian patients (46%) often complain of psychopathological features like depression as primary symptom of PD. A variety of autonomic nervous system symptoms, such as constipation (49.3%), sexual dysfunction (28.8%), mouth dryness (58.9%), sleep disturbance (50.7%), sweating (38.4%) or inappetence (16.4%) occurs already in the first six months of clinical course.
Otherwise, most frequently (36.5%) tremors led to visits. Sleep impairment is present in about 50% of the patients. These sleep disturbances are due in part to nocturnal akinesia, painful dystonia, depression or a sleep-apnea syndrome. Among the patients with a delayed diagnosing (more than 2 years), the described vague and subtle however typical early symptoms were significantly more frequent than in those patients without a delayed diagnosing. Our results were based on retrospective questioning, which is subject to the methodical restriction of a “recall bias” (distorted memory ability illness-causes). For example, depression and cognitive impairment may influence that self-report.
It can also be assumed that our patient group was more conscious of their symptoms as they were confronted with similar questions during neurological investigation and history taking, and this may have produced a higher sensitivity.

Carl-Albrecht Haensch 220
Figure 1. Preclinical and premotor complaints significantly more frequently noticed in delayed diagnosed PD.
Among the patients with a delayed diagnosing (more than two years), early symptoms were significantly more frequent (figure 1). The opportunity for diagnostic confusion is greatest early on in the clinical course, when some of the more distinctive clinical features may not have yet developed. Symptoms at the time of the first diagnosis and at the beginning of the first clinical manifestation of PD are often not identical. Those patients with subtle symptoms were diagnosed significantly later. As diagnosis can be made unchanged only clinically, physicians must be aware of this “soft” signs in early stages of PD.
Because of the therapeutic success in the beginning, PD should be diagnosed as early as possible. Diagnostic mistakes may occur early in the course of the disease. Neuroprotective therapeutic approaches can be utilized optimally only with early onset of treatment. Although the hallmark of PD is a syndrome of movement disorders, in early stages, clinical symptoms are often very subtle.
Autonomic Function Tests The cardiovascular autonomic function tests use based on blood pressure and heart rate at
rest and after various stimulations under standardized environmental conditions with a room temperature of 20° C [17, 61]. 107 PD-patients were tested (mean age 71 years, mean PD-duration 7.0 years, Hoehn and Yahr 3.0 ± 0.9). All tests were done in the morning. Finger arterial pressure was measured beat-to-beat continuously and non-invasivily using the volume clamp method with the Portapres device (TNO TPD, Amsterdam, The Netherlands). The cuff was placed on the second phalanx of the third finger. A synchronous recording of a standard 4 channel ECG, respiratory effort measured by thoracic strain gauges and the Portapres signal was performed simultaneously with the fan device (Schwarzer GmbH, Munich, Germany). The duration of recording was approximately 45 minutes. After the rest phase, a head-up tilt table, testing with a 70° upright position within 20s with an electrically driven tilt table, was performed. The Valsalva manoeuvre was performed by asking the subject to blow into a

Cardiac Involvement in Parkinson’s Disease 221
mouthpiece attached to an aneroid pressure gauge at a pressure of 40 mm Hg and to hold pressure for 15 s. A return of the cardiovascular parameters to baseline was waited for in between each test. The Valsalva ratio, the diastolic blood pressure in phase II, the latency between the minimum blood pressure in phase III of the Valsalva manoeuvre and the maximum in phase IV were qualified [16]. The response was considered to be normal if the diastolic pressure increased before the end of straining and if the systolic blood pressure during phase IV increased to a value exceeding the baseline in not more than 7 s. Orthostatic hypotension was diagnosed based on the Consensus statement on the definition of orthostatic hypotension using a decrease of at least 20 mm Hg in systolic blood pressure or at least 10 mm Hg within 3 minutes of standing [1-3, 45]. Myocardial adrenergic function was analyzed by imaging with 123I-Meta-iodobenzylguanidine (MIBG) using single-photon emission computed tomography (SPECT) technique in patients with PD. MIBG is an analog of norepinephrine and a tracer for sympathetic neuron integrity and function. Cardiac MIBG uptake was assessed qualitatively for heart visualisation on planar studies by an nuclear medicine specialist, who was unaware of the autonomic function status.
Premature Ventricular Contractions Standard cardiovascular autonomic responses to physiological stimuli have provided
much evidence suggesting mild autonomic nervous system disturbances in PD [12]. The most frequent cardiac rhythm disturbances in PD are premature ventricular contractions (PVCs), often appearing as monomorphic, single PVCs, or rarely as bigeminy, trigeminy or pairs. Extrasystoles occur in normals, but are more frequently (16.25 % vs. 55 %; Chi2 = 19.3, p < 0.001) seen in PD [36]. The clinical significance of the significantly higher frequency of premature ventricular contractions in PD, than in normals, is unknown. It is possible that the postganglionic sympathetic dysfunction in cardiac innervation leads to susceptibility for cardiac dysrhythmia. In the great majority of instances, sustained dysrhythmias do not arise simply in association with speeding or slowing of heart rate. Usually there are one or more premature beats as well. Recently, we described reduced baroreflex sensitivity in PD not limited to experimental reflex conditions, but causing an impaired blood pressure regulation that occuring spontaneously [36].
Heart Rate Variability The function of Heart rate variability is commonly known to be buffer changes in blood
pressure [70]. Analysis of Heart rate variability (HRV) has been used as a measure of cardiac autonomic control. It can be performed in two main ways, by statistical operations on R-R intervals (time-domain analysis) or by spectral analysis of a series of successive R-R intervals (frequency-domain analysis). It allows a differentiation of the sympathetic and parasympathetic activation, which are related to a low-frequency (LF) and a high-frequency (HF) component of the heart rate variability (HRV) signal, respectively.

Carl-Albrecht Haensch 222
0 22020018016014012010080604020 260240
Tachogramm
400
1200
0
200
400
600
800
1000
PS
D/T
2 [
MS
2]
0.01 0.11 0.300.21 0.40 0.50
Frequenz [Hz]
A/D- Change
R wave identification
Arrhythmia ?
Beat-to-beat interval time series
Fast fourier transform (FFT)
or Autoregressive analysis
FFT-Diagramm
Analysis of heart rate variability in the frequency domain
Figure 2. Analysis of heart rate variability in the frequency domain.
The resulting LF/HF ratio is a quantitative index of the sympatho-vagal balance. The HF component is similar in shape and centre to the frequency of the respiratory signal and is generally considered a marker of vagal activity, although a sympathetic influence has been advocated on the basis of inconclusive studies using ß-blockers. The LF component seems to depend on more complex mechanisms. Manoeuvres enhancing the sympathetic drive or abnormal conditions associated with sympathetic hyperactivity led to a marked relative increase in the LF component. Many factors influence heart rate and explain the great variability of the parameters recorded, such as age [5, 26], drugs, breathing frequency [71], orthostatic stress [20, 21] and physical exercise [69]. The laboratory should be environment

Cardiac Involvement in Parkinson’s Disease 223
controlled, especially for temperature. International recommendations includes suggestions for the analysis of heart rate variability, blood pressure monitoring, tilt-table testing, Valsalva manoeuvre [2, 4, 6, 17, 24]. The measurement of autonomic parameters using power spectrum analysis of heart rate does not require the active participation of patients.
In the PD-patients group (n=107, mean age 71 years, mean PD-duration 7.0 years, Hoehn and Yahr 3.0 ± 0.9) the LF/HF ratio was lower than in the control group in rest (2.19 vs. 1.25, p < 0.05); in deep respiration (3.3 vs. 2.4, p < 0.01) and in tilt-table testing (2.6 vs 1.9, p < 0.01). The LF/HF ratio in tilt-table testing was significantly more reduced in PD with orthostatic hypotension than without (2.1 vs. 1.3, p < 0.05). Diminished variability of standard RR intervals and spectral measures of HR variability have been reported in PD [33, 37, 43, 44, 51, 55-57, 59, 64, 73, 74]. Cautious interpretation of heart rate variability is required regarding the neural complexity [27]. Two studies have evaluated tonic cardiovascular control patterns, reporting dysregulation both in de novo PD patients [33] and in advanced PD [51]. A previous study support the hypothesis that sympathetic and parasympathetic balance in control of heart activity are impaired in Parkinson's disease and that this dysfunction can be assessed by frequency-domain analysis of HR changes [34]. Based on clinical experience, it is assumed that autonomic dysfunction progresses along with the underlying PD, but little is known about the association between the decline of motor function and autonomic failure [47]. In accordance with a study by Haapaniemi, the size of reduction of LF/HF-ratio correlated to the UPDRS-score, might be a objective marker for disease progression in PD. However, because the association was not strong, the mechanisms causing the motor disability in PD may differ from those leading to impairment of the cardiovascular regulation [33].
The significance of the abnormalities in cardiovascular regulation among Parkinson’s disease patients is not fully known yet. The conventional time and frequency domain measures of HR variability, previously proved useful in predicting cardiac arrhythmia and mortality in coronary heart disease [11, 22]. The prevailing hypothesis is that because an intact neurocardiac autonomic regulation is essential for a normal heart rate variability, a decrease of this parameter may reflect the autonomic dysfunction associated with cardiac electrical instability [10]. Adrenergic hyperactivity and/or lack of presumably protective parasympathetic tone are the suggested pathophysiological mechanisms of sudden cardiac death [67].
It is possible that the dysbalance of the sympathetic and the parasympathetic tone is connected with the arrhythmias developing in the ischemic heart muscles [70]. The connection between autonomic dysregulation and arrhythmia-related death has recently been considered in other, non-cardiovascular diseases, such as depression [32]. Analogously, we can presume a connection between the autonomic dysbalance and the high mortality among PD-patients [8, 9].
Imaging of the Autonomic Nervous System Cardiac 123I-Metaiodobenzylguanidine (MIBG) scintigraphy is a sensitive tool for
detecting cardiac sympathetic denervation in PD [25]. Many recent studies have agreed on

Carl-Albrecht Haensch 224
the remarkable finding that all patients with PD and orthostatic hypotension have a loss of cardiac sympathetic innervation [15, 18, 19, 30, 60, 62, 65, 66, 72]. MIBG uptake was assessed using the ratio of the heart to the upper mediastinum (H/M) according to planar scintigraphic data. In the heart, MIBG uptake in all examined 57 PD-patients was decreased (H/M-Ratio: 1.14 ± 0.16). Loss of sympathetic innervation of the heart seems to occur independent of orthostatic hypotension and baroreflex failure in PD. We found no correlation between myocardial MIBG uptake and sympathovagal balance, blood pressure or other autonomic findings. These results could be explained by different time course of loss of intact postganglionic sympathetic cardial innervation and disturbed baroreflex response or the involvement of central autonomic pathways in PD.
Figure 3. Decreased cardiac uptake in 123I-metaiodobenzylguanidine scintigraphy in a patient with PD.
Impaired autonomic cardiovascular regulation has been associated with an increased risk of mortality both in patients with heart disease and in randomly selected general populations [33]. Sympathetic denervation leeds to denervation hypersensitivity, which is a phenomenon characterized by inadequately strong response of the denervated tissues to the physiological neurotransmitters [54]. Hypersensitivity occurs in the heart when the circulating catecholamines react with a live but sympathetically denervated myocardial tissue. The denervation hypersensitivity creates a predilection for the appearance of cardiac arrhythmias.

Cardiac Involvement in Parkinson’s Disease 225
The mortality of Parkinson’s disease patients is almost twice that for age and sex-matched healthy control groups [9]. The 20-year follow-up study by Ben-Shlomo and Marmot suggested that this increased mortality is connected with an increase in heart ischemia-related deaths [8]. On the other hand Orimo et al. showed echocardiographic normal left ventricular function in 36 PD patients with myocardial sympathetic nerve damage demonstrated by 123I-metaiodobenzylguanidine scintigraphy [62]. No changes in left ventricular function were observed by echocardiography studies in PD, although recently some new studies were carried out regarding valvular heart disease; associated with ergot derivative dopamine agonists therapy [7, 23, 38, 46, 63, 68, 75, 76, 78-80].
It is now clear that there is a fundamental abnormality in reflex control mechanisms like baroreceptor dysfunction in the syndrome of heart failure. Still unresolved is whether the protean abnormalities in afferent and efferent sympathetic nervous system function in heart failure are fundamental to the clinical manifestations of the syndrome or are merely epiphenomena indicative of the severity of the physiological derangement [29].
Cardiovascular dysfunction may occur in parkinsonian patients for a variety of reasons. Patients more are usually than 50 years old and on various drugs (both antiparkinsonian and for associated medical disorders), some of which may have cardiovascular effects. Autonomic failure increases with age and also is recognized in parkinsonian patients who have the disorder multiple system atrophy, in which there is substantial cardiovascular dysfunction [52]. Our results indicate that both parasympathetic and sympathetic deficits may occur in PD. Thus, recognition of cardiovascular dysfunction and its causes in parkinsonian patients is of importance in diagnosis, in determining prognosis, and finally in management.
References
[1] (1996) Consensus statement on the definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy. J. Neurol. Sci. 144:218-219
[2] (1996) Consensus statement on the definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy. The Consensus Committee of the American Autonomic Society and the American Academy of Neurology. Neurology. 46:1470
[3] (1996) The definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy. J. Auton. Nerv. Syst. 58:123-124
[4] (1996) Heart rate variability: standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation. 93:1043-1065
[5] Agelink MW, Malessa R, Baumann B, Majewski T, Akila F, Zeit T, Ziegler D (2001) Standardized tests of heart rate variability: normal ranges obtained from 309 healthy humans, and effects of age, gender, and heart rate. Clin. Auton. Res. 11:99-108
[6] Baron R (1999) Heart rate variability. Electroencephalogr. Clin. Neurophysiol. Suppl. 50:283-286

Carl-Albrecht Haensch 226
[7] Baseman DG, O'Suilleabhain PE, Reimold SC, Laskar SR, Baseman JG, Dewey RB, Jr. (2004) Pergolide use in Parkinson disease is associated with cardiac valve regurgitation. Neurology. 63:301-304
[8] Ben-Shlomo Y, Marmot MG (1995) Survival and cause of death in a cohort of patients with parkinsonism: possible clues to aetiology? J. Neurol. Neurosurg. Psychiatry. 58:293-299
[9] Bennett DA, Beckett LA, Murray AM, Shannon KM, Goetz CG, Pilgrim DM, Evans DA (1996) Prevalence of parkinsonian signs and associated mortality in a community population of older people. N. Engl. J. Med. 334:71-76
[10] Bernardi L (2000) The autonomic nervous system in heart disease. In: Appenzeller O (ed) The autonomic nervous system. Part II. Elsevier, Amsterdam; New York, pp 425-452
[11] Bigger JT, Jr., Steinman RC, Rolnitzky LM, Fleiss JL, Albrecht P, Cohen RJ (1996) Power law behavior of RR-interval variability in healthy middle-aged persons, patients with recent acute myocardial infarction, and patients with heart transplants. Circulation. 93:2142-2151
[12] Bolis L, Licinio J, Govoni S (2003) Handbook of the autonomic nervous system in health and disease. Marcel Dekker, New York
[13] Braak H, Bohl JR, Muller CM, Rub U, de Vos RA, Del Tredici K (2006) Stanley Fahn Lecture 2005: The staging procedure for the inclusion body pathology associated with sporadic Parkinson's disease reconsidered. Mov. Disord. 21:2042-2051
[14] Braak H, Ghebremedhin E, Rub U, Bratzke H, Del Tredici K (2004) Stages in the development of Parkinson's disease-related pathology. Cell Tissue Res. 318:121-134
[15] Braune S (2001) The role of cardiac metaiodobenzylguanidine uptake in the differential diagnosis of parkinsonian syndromes. Clin. Auton. Res. 11:351-355
[16] Braune S, Auer A, Schulte-Monting J, Schwerbrock S, Lucking CH (1996) Cardiovascular parameters: sensitivity to detect autonomic dysfunction and influence of age and sex in normal subjects. Clin. Auton. Res. 6:3-15
[17] Braune S, Baron R, Low P (1999) Assessment of blood pressure regulation. Electroencephalogr Clin. Neurophysiol. Suppl. 50:287-291
[18] Braune S, Reinhardt M, Bathmann J, Krause T, Lehmann M, Lucking CH (1998) Impaired cardiac uptake of meta-[123I]iodobenzylguanidine in Parkinson's disease with autonomic failure. Acta Neurol. Scand. 97:307-314
[19] Braune S, Reinhardt M, Schnitzer R, Riedel A, Lucking CH (1999) Cardiac uptake of [123I]MIBG separates Parkinson's disease from multiple system atrophy. Neurology. 53:1020-1025
[20] Butler GC, Yamamoto Y, Hughson RL (1994) Heart rate variability to monitor autonomic nervous system activity during orthostatic stress. J. Clin. Pharmacol. 34:558-562
[21] Butler GC, Yamamoto Y, Xing HC, Northey DR, Hughson RL (1993) Heart rate variability and fractal dimension during orthostatic challenges. J. Appl. Physiol. 75:2602-2612

Cardiac Involvement in Parkinson’s Disease 227
[22] Chakko S, Mulingtapang RF, Huikuri HV, Kessler KM, Materson BJ, Myerburg RJ (1993) Alterations in heart rate variability and its circadian rhythm in hypertensive patients with left ventricular hypertrophy free of coronary artery disease. Am. Heart J. 126:1364-1372
[23] Chung EJ, Yoon WT, Kim JY, Lee WY (2006) Valvular heart disease in a patient with Parkinson's disease treated with a low daily dose and a low cumulative dose of pergolide. Mov. Disord. 21:586-587
[24] Claus D, Schmitz J, Nouri S (1999) Value and limits of cardiovascular autonomic function tests. Electroencephalogr. Clin. Neurophysiol. Suppl. 50:288-292
[25] Courbon F, Brefel-Courbon C, Thalamas C, Alibelli MJ, Berry I, Montastruc JL, Rascol O, Senard JM (2003) Cardiac MIBG scintigraphy is a sensitive tool for detecting cardiac sympathetic denervation in Parkinson's disease. Mov. Disord. 18:890-897
[26] Dawson SL, Robinson TG, Youde JH, Martin A, James MA, Weston PJ, Panerai RB, Potter JF (1999) Older subjects show no age-related decrease in cardiac baroreceptor sensitivity. Age Ageing. 28:347-353
[27] Devos D, Kroumova M, Bordet R, Vodougnon H, Guieu JD, Libersa C, Destee A (2003) Heart rate variability and Parkinson's disease severity. J. Neural. Transm. 110:997-1011
[28] Dewey RB, Jr. (2004) Autonomic dysfunction in Parkinson's disease. Neurol. Clin. 22:S127-139
[29] Francis G, Cohn J (1999) Cardiac failure and the autonomic nervous system. In: Bannister R, Mathias CJ (eds) Autonomic failure: a textbook of clinical disorders of the autonomic nervous system. Oxford University Press, Oxford; New York, pp 477-486
[30] Goldstein DS (2003) Imaging of the autonomic nervous system: focus on cardiac sympathetic innervation. Semin. Neurol. 23:423-433
[31] Grubb BP, Olshansky B, Huang SK (1998) Syncope: mechanisms and management. Futura Pub. Co., Armonk, NY
[32] Guinjoan SM, Bernabo JL, Cardinali DP (1995) Cardiovascular tests of autonomic function and sympathetic skin responses in patients with major depression. J. Neurol. Neurosurg. Psychiatry. 59:299-302
[33] Haapaniemi TH, Pursiainen V, Korpelainen JT, Huikuri HV, Sotaniemi KA, Myllyla VV (2001) Ambulatory ECG and analysis of heart rate variability in Parkinson's disease. J. Neurol. Neurosurg. Psychiatry. 70:305-310
[34] Haensch C-A, Jörg J (2001) Disturbed Sympatho-Vagal Balance in Heart Rate Variability as Marker of Progression in Parkinson's Disease. J. Neural. Sci. 187:133
[35] Haensch C-A, Jörg J (1999) Preclinical symptoms in delayed diagnosed Parkinson`s disease. J. Neural. Transm. 106: XI
[36] Haensch CA, Jorg J (2006) Beat-to-beat blood pressure analysis after premature ventricular contraction indicates sensitive baroreceptor dysfunction in Parkinson's disease. Mov. Disord. 21:486-491

Carl-Albrecht Haensch 228
[37] Holmberg B, Kallio M, Johnels B, Elam M (2001) Cardiovascular reflex testing contributes to clinical evaluation and differential diagnosis of Parkinsonian syndromes. Mov. Disord. 16:217-225
[38] Horvath J, Fross RD, Kleiner-Fisman G, Lerch R, Stalder H, Liaudat S, Raskoff WJ, Flachsbart KD, Rakowski H, Pache JC, Burkhard PR, Lang AE (2004) Severe multivalvular heart disease: a new complication of the ergot derivative dopamine agonists. Mov. Disord. 19:656-662
[39] Hughes AJ, Daniel SE, Kilford L, Lees AJ (1992) Accuracy of clinical diagnosis of idiopathic Parkinson's disease: a clinico-pathological study of 100 cases. J. Neurol. Neurosurg. Psychiatry. 55:181-184
[40] Jellinger K (1987) The pathology of parkinsonism. In: CD Marsden, Fahn S (eds) Movement Disorder. 2. Butterworths, London, pp 124-165
[41] Jellinger KA (1991) Pathology of Parkinson's disease. Changes other than the nigrostriatal pathway. Mol. Chem. Neuropathol. 14:153-197
[42] Jost WH (2003) Autonomic dysfunctions in idiopathic Parkinson's disease. J. Neurol. 250 Suppl 1:I28-30
[43] Kallio M, Haapaniemi T, Turkka J, Suominen K, Tolonen U, Sotaniemi K, Heikkila VP, Myllyla V (2000) Heart rate variability in patients with untreated Parkinson's disease. Eur. J. Neurol. 7:667-672
[44] Kallio M, Suominen K, Bianchi AM, Makikallio T, Haapaniemi T, Astafiev S, Sotaniemi KA, Myllya VV, Tolonen U (2002) Comparison of heart rate variability analysis methods in patients with Parkinson's disease. Med. Biol. Eng. Comput. 40:408-414
[45] Kaufmann H (1996) Consensus statement on the definition of orthostatic hypotension, pure autonomic failure and multiple system atrophy. Clin. Auton. Res. 6:125-126
[46] Kim JY, Chung EJ, Park SW, Lee WY (2006) Valvular heart disease in Parkinson's disease treated with ergot derivative dopamine agonists. Mov. Disord. 21:1261-1264
[47] Korchounov A, Kessler KR, Yakhno NN, Damulin IV, Schipper HI (2005) Determinants of autonomic dysfunction in idiopathic Parkinson's disease. J. Neurol. 252:1530-1536
[48] Kuchel GA (2004) Autonomic nervous system in old age. Karger, Basel; New York [49] Kujawa K, Leurgans S, Raman R, Blasucci L, Goetz CG (2000) Acute orthostatic
hypotension when starting dopamine agonists in Parkinson's disease. Arch. Neurol. 57:1461-1463
[50] Magerkurth C, Schnitzer R, Braune S (2005) Symptoms of autonomic failure in Parkinson's disease: prevalence and impact on daily life. Clin. Auton. Res. 15:76-82
[51] Mastrocola C, Vanacore N, Giovani A, Locuratolo N, Vella C, Alessandri A, Baratta L, Tubani L, Meco G (1999) Twenty-four-hour heart rate variability to assess autonomic function in Parkinson's disease. Acta Neurol. Scand. 99:245-247
[52] Mathias CJ (1998) Cardiovascular autonomic dysfunction in parkinsonian patients. Clin. Neurosci. 5:153-166

Cardiac Involvement in Parkinson’s Disease 229
[53] Mathias CJ, Mallipeddi R, Bleasdale-Barr K (1999) Symptoms associated with orthostatic hypotension in pure autonomic failure and multiple system atrophy. J. Neurol. 246:893-898
[54] Matveev M, Prokopova R, Nachev C (2006) Normal and abnormal circadian characteristics in autonomic cardiac control: new opportunities for cardiac risk prevention. Nova Science Publishers, New York
[55] Meco G, Pratesi L, Bonifati V (1991) Cardiovascular reflexes and autonomic dysfunction in Parkinson's disease. J. Neurol. 238:195-199
[56] Mesec A, Sega S, Kiauta T (1993) The influence of the type, duration, severity and levodopa treatment of Parkinson's disease on cardiovascular autonomic responses. Clin. Auton. Res. 3:339-344
[57] Mesec A, Sega S, Trost M, Pogacnik T (1999) The deterioration of cardiovascular reflexes in Parkinson's disease. Acta Neurol. Scand. 100:296-299
[58] Micieli G, Tosi P, Marcheselli S, Cavallini A (2003) Autonomic dysfunction in Parkinson's disease. Neurol. Sci. 24 Suppl. 1:S32-34
[59] Mihci E, Kardelen F, Dora B, Balkan S (2006) Orthostatic heart rate variability analysis in idiopathic Parkinson's disease. Acta Neurol. Scand. 113:288-293
[60] Oka H, Mochio S, Yoshioka M, Morita M, Onouchi K, Inoue K (2006) Cardiovascular dysautonomia in Parkinson's disease and multiple system atrophy. Acta Neurol. Scand. 113:221-227
[61] Oribe E (1999) Testing autonomic function. In: Vinken PJ, Bruyn GW, Appenzeller O (eds) The autonomic nervous system Part I. Elsevier, Amsterdam; New York, pp 595-648
[62] Orimo S, Ozawa E, Nakade S, Sugimoto T, Mizusawa H (1999) (123)I-metaiodobenzylguanidine myocardial scintigraphy in Parkinson's disease. J. Neurol. Neurosurg. Psychiatry. 67:189-194
[63] Peralta C, Wolf E, Alber H, Seppi K, Muller S, Bosch S, Wenning GK, Pachinger O, Poewe W (2006) Valvular heart disease in Parkinson's disease vs. controls: An echocardiographic study. Mov. Disord. 21:1109-1113
[64] Pursiainen V, Haapaniemi TH, Korpelainen JT, Huikuri HV, Sotaniemi KA, Myllyla VV (2002) Circadian heart rate variability in Parkinson's disease. J. Neurol. 249:1535-1540
[65] Reinhardt MJ, Jungling FD, Krause TM, Braune S (2000) Scintigraphic differentiation between two forms of primary dysautonomia early after onset of autonomic dysfunction: value of cardiac and pulmonary iodine-123 MIBG uptake. Eur. J. Nucl. Med. 27:595-600
[66] Saiki S, Hirose G, Sakai K, Kataoka S, Hori A, Saiki M, Kaito M, Higashi K, Taki S, Kakeshita K, Fujino S, Miaki M (2004) Cardiac 123I-MIBG scintigraphy can assess the disease severity and phenotype of PD. J. Neurol. Sci. 220:105-111
[67] Schwartz PJ, La Rovere MT, Vanoli E (1992) Autonomic nervous system and sudden cardiac death. Experimental basis and clinical observations for post-myocardial infarction risk stratification. Circulation. 85:I77-91

Carl-Albrecht Haensch 230
[68] Scozzafava J, Takahashi J, Johnston W, Puttagunta L, Martin WR (2006) Valvular heart disease in pergolide-treated Parkinson's disease. Can. J. Neurol. Sci. 33:111-113
[69] Stein PK, Ehsani AA, Domitrovich PP, Kleiger RE, Rottman JN (1999) Effect of exercise training on heart rate variability in healthy older adults. Am. Heart J. 138:567-576
[70] Szili-Török T, Dibó G, Kardos A, Paprika D, Rudas L (1999) Abnormal cardiovascular autonomic regulation in Parkinson's disease. Journal of Clinical and Basic Cardiology. 2:245-247
[71] Taylor JA, Eckberg DL (1996) Fundamental relations between short-term RR interval and arterial pressure oscillations in humans. Circulation. 93:1527-1532
[72] Tipre DN, Goldstein DS (2005) Cardiac and extracardiac sympathetic denervation in Parkinson's disease with orthostatic hypotension and in pure autonomic failure. J. Nucl. Med. 46:1775-1781
[73] Turkka JT (1987) Correlation of the severity of autonomic dysfunction to cardiovascular reflexes and to plasma noradrenaline levels in Parkinson's disease. Eur. Neurol. 26:203-210
[74] Turkka JT, Tolonen U, Myllyla VV (1987) Cardiovascular reflexes in Parkinson's disease. Eur. Neurol. 26:104-112
[75] Van Camp G, Flamez A, Cosyns B, Goldstein J, Perdaens C, Schoors D (2003) Heart valvular disease in patients with Parkinson's disease treated with high-dose pergolide. Neurology. 61:859-861
[76] Van Camp G, Flamez A, Cosyns B, Weytjens C, Muyldermans L, Van Zandijcke M, De Sutter J, Santens P, Decoodt P, Moerman C, Schoors D (2004) Treatment of Parkinson's disease with pergolide and relation to restrictive valvular heart disease. Lancet. 363:1179-1183
[77] Wakabayashi K, Takahashi H (1997) Neuropathology of autonomic nervous system in Parkinson's disease. Eur. Neurol. 38 Suppl 2:2-7
[78] Waller EA, Kaplan J, Heckman MG (2005) Valvular heart disease in patients taking pergolide. Mayo Clin. Proc. 80:1016-1020
[79] Yamamoto M, Uesugi T, Nakayama T (2006) Dopamine agonists and cardiac valvulopathy in Parkinson disease: a case-control study. Neurology. 67:1225-1229
[80] Zanettini R, Antonini A, Gatto G, Gentile R, Tesei S, Pezzoli G (2007) Valvular heart disease and the use of dopamine agonists for Parkinson's disease. N. Engl. J. Med. 356:39-46

In: Cardiac Arrythmia Research Advances ISBN: 978-1-60021-795-1 Editor: Lynn A. Vespry, pp. 231-286 © 2007 Nova Science Publishers, Inc.
Chapter X
A Novel Approach to Optimization of Paced AV Delay Using Atrial
Contribution Index Derived from Arterial Waveform Trace Obtained from
Pulse Oximetry Signal – Feasibility, Reproducibility and Sensitivity to Acute
Hemodynamic Interventions
Miroslav Mestan* and Jiri Kvasnicka*
Abstract
The hemodynamic effect of the atria on the net performance of the heart is called atrial contribution (AC). AC is either linked to ventricular filling or to the systolic function of the heart, i.e. to the systolic volume or cardiac output. Several non-invasive methods for the quantification of AC are described in literature but none of them are routinely used in cardiac pacing centres due to the time-consuming nature of the methods, the limited reproducibility of measured values and observer-dependency.
The aim of presented studies was to develop a method for determining optimal AV delay in patients treated by dual chamber pacing using an index (ACSp) that quantifies atrial contribution to the systolic volume of the left ventricle. The new method is based on the quantitative analysis of a beat-to-beat decrease in the amplitude of the pulse oximetry signal (SpO2). The change in the amplitudes is induced by a sudden drop of the stimulus to the right atrium, while maintaining the rate of ventricular stimuli at a constant level. The obtained ACSp is given as a percentage of the pulse amplitude of SpO2. The method is independent of the observer, non-invasive and relatively fast. In a group of 47
* Affiliation of both authors: Academic Department of Internal Medicine; Faculty of Medicine in Hradec Kralove;
Charles University Prague; University Hospital; Sokolska 581, Hradec Kralove; ZIP code: 500 05, Czech Republic

Miroslav Mestan and Jiri Kvasnicka 232
patients, remarkable similarities between ACSp and another atrial contribution index estimated using the tracings of invasively registered aortal pressure were demonstrated.
In all investigated AV intervals of 50 to 250 ms, significant interindividual variability of ACSp was discovered. The poorest hemodynamic effect was seen at AV delay of 50 ms (median ACSp of 10.4 % from 97 subjects). In 150 subjects, the following values of ACSp were obtained at AV delay of 200 ms: median 30 %, minimum 3.6 % and maximum 80.4 %. Blant and Altmans’s analyses of paired values obtained within the time range of either 10-20 minutes (average difference between two paired measurements –0.5 ± 6.1 %) or 24 hours (average difference between two paired measurements 2.1 ± 7.9 %) showed good reproducibility of ACSp. In a group of repeatedly investigated subjects, every individual demonstrated stable relationship between investigated AV delays and corresponding values of ACSp. This method offers a fast and observer independent alternative compared to the other non-invasive methods employed for AV delay optimization.
An increase in ACSp follows reduction of preload induced by administration of furosemide. This suggests that when preload decreases cardiac output is preserved by an increase in AC enforced by sympathetic activation.
Introduction
Atrial Function Beginnings of modern investigation of atrial function are connected with studies using
asynchronous ventricular pacing together with simultaneous registration of arterial and venous blood pressures [[81]]. That study in anesthetized dogs confirmed a hypothesis that the atria are not only conduit between the systemic and pulmonary veins and both ventricles. Gessel demonstrated that properly timed and in time finished atrial systole, preceding ventricular systole, may significantly increase the pulse pressure. That increase could be up to 55% of the pulse pressure generated by so-called “reference” beat with ineffective atrial kick; i.e. atrial systole occurred completely at the same time as the ventricular one in that reference beat.
The modern research of atrial functions has lasted almost 100 years. One may document four main targets of properly timed atrial systole. The targets include optimal stress of the ventricular wall at the end of diastole, maintenance of a low mean pressure in the left atrium, presystolic closure of the atrioventricular (AV) valves with prevention of regurgitation on these valves, and prevention of undesirable vagal reflexes induced by acute dilation of the atrial myocardium when the atria contract against closed atrioventricular valves.
The pressure inside the left atrium is a necessary force which expels the blood into the left ventricle and overwhelms losses of kinetic energy consumed for dilation of the ventricle. The left atrium serves as a passive reservoir for the blood expelled by the right ventricle, as the conduit and it has own contractile function and may create some amount of kinetic energy [[82]]. Only when excessive preload is present, the length of the atrial myocardium may exceed some critical point when the “booster function” of the atria disappears and the atria become serving as the conduit only [[83],[84],[85]].

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 233
Properly timed atrial contraction creates high enddiastolic pressure inside the left ventricle despite mean left atrial pressure remaining low [[86],[87]]. Atrial contraction help achieve optimal length of the ventricular myocardium’s sarcomeres, crucial for maximum myocardial contractility by the Frank-Starling’s law. Braunwald reported [[88]] that enddiastolic pressure in the ventricle is a stimulus determining the force of ventricular contraction and the mean pressure in the atrium is a “hemodynamical price” which must the organism pay for that stimulus. Because optimal strength of the ventricular myocardium is achieved for only a short time immediately before ventricular systole begins, the supply of the myocardium with the oxygenated blood is not significantly impaired. When atrial fibrillation develops in patients with systolic dysfunction, the mean pressure inside the left atrium must equal the enddiastolic pressure in the left ventricle. Pathologically increased pressure then transmits into the pulmonary capillary bed and helps develop heart failure symptoms [[87],[88]].
The atria play an important role for closure of the atrioventricular valves [[86],[87],[89],[90]]. The fast increase in the enddiastolic pressure inside the ventricle, in combination with beginning of relaxation of the atrial myocardium, creates conditions for turn of pressure gradient and finally for backward blood flow from the ventricle back to the atrium. The atrioventricular valves close sooner; i.e. before the ventricular systole begins. This also prevents presystolic regurgitation of blood which may cause the loss of optimal strength of the ventricular myocardium before expected contraction.
Atrial functions are influenced by the rich vegetative innervation which may very quickly change atrial myocardium contractility [[91]]. First evidence about parasympathetic influence on the atrial function was published by Gessel on the model “heart with lungs” [[92]]. Sympathetic and parasympathetic influence on effectiveness of atrial contraction was documented in detail by Mitchell in experiments with anaesthetized dogs [[93]]. When they kept mean pressure in the left atrium at a constant level, they induced a significant increase in atrial contribution to systolic work of the left ventricle by sympathetic stimulation. On the other hand, when they used parasympathetic stimulation, atrial contribution was almost completely removed despite atrioventricular synchrony that had been maintained.
A general agreement exists that the atria are involved in regulations of the heart performance directly (immediate hemodynamic effect) and indirectly via secretion of vasoactive substances and reflexes of the vegetative nervous system. Indirect regulations influence preload and afterload of the ventricles and change inotropic status of the myocardium [[94],[95]].
Definition of Atrial Contribution In cardiology, functional effect of atrial contraction is called atrial contribution (AC).
However, the definition of AC is not simple. Some authors reported AC as some volume of blood which atrial contraction adds to the
final volume of the ventricle at the end of diastole. This type of AC can be called atrial contribution for ventricular filling (ACVF). Many methods were used for registration of changes in enddiastolic filling of the left ventricle, including catheterization of the heart

Miroslav Mestan and Jiri Kvasnicka 234
[[96]], echocardiography with Doppler [[97],[98],[99]], tissue Doppler imaging [[100],[101]], isotope angiography [[102]], and nuclear magnetic resonance [[103],[104]]. Helene von Bibra with co-authors found ACVF of 11 to 45 % when pacing mode changed from VVI to DDD.
An atrial action related to expelling blood from the heart into the arterial bed represents the other type of atrial contribution. There are essentially two alternatives –measurement of atrial contribution either to cardiac output (ACCO) or to systolic volume (ACSV). Some papers on ACCO or ACSV compared two pacing modes (asynchronous ventricular pacing and sequential dual chamber pacing). The other publications dealt with the issue of optimal timing between atrial and ventricular systoles and influence of that timing on cardiac output (CO) and physical capacity of subjects. When a subject with preserved atrial contraction is paced in VVI mode then atrial contractions precede the ventricular ones in different time intervals and final systolic volumes (SV) must vary. If atrial contraction occurs at the same time as the ventricular one (i.e. against closed atrioventricular valves), final atrial contribution is zero and such beats with simultaneous atrial and ventricular contraction served as references for quantification of changes either in CO or SV, respectively [[105]], or in pulse pressure in the artery [[81]].
For measurements of ACCO or ACSV, following techniques were employed: measurements based on Fick principle [[106]], isotope ventriculography [[107],[108]], dye dilution [[96],[109],[110]], thermodilution [[111],[112]], angiography with planimetry [[113]], changes in pulse pressure [[86],[88],[114],[115]], measurements with aortal flowmeter [[116]], echocardiography with Doppler [[117],[118]], plethysmography of peripheral arteries [[119],[120]], bioimpedance [[121],[122]], and continuous and noninvasive registration of blood pressure by the finger probe [[123],[124]].
Magnitude of ACCO obtained at steady state was reported between 10-20% with isolated values reaching up to 35%. Published values of ACSV were slightly higher than ACCO, minimum about 20-35% and values of about 50% were not rare when beat-to-beat changes in SV were evaluated in patients with complete AV block and VVI stimulation [[120]]. Extreme values of ACSV were registered in experiment using higher heart rate of more than 100/min [[125]]. Ruskin and coauthors measured ACSV of 41 up to 145% when comparing SV of reference beat (see above) and those with preceding atrial contraction. A very important result from several studies was that one cannot easily extrapolate magnitude of ACSV to ACCO. Regulation of CO is more complex and one isolated value of SV cannot grasp all of them.
Is It Useful to Know Magnitude of Atrial Contribution? Atrial contraction plays a much more important role in patients with increased stiffness
of the left ventricular wall (e.g. aortal stenosis, arterial hypertension) than in healthy individuals [[126],[127]]. In patients with the stiffened left ventricle, a difference between enddiastolic pressure inside the left ventricle and mean pressure inside the left atrium is remarkably higher than in healthy population. In patients with myocardial infarction, a magnitude of SV decreased. However, the ACSV in these patients increased significantly in comparison with a group of healthy volunteers [[96]]. Greenberg and coworkers published

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 235
ACSV decreases when filling pressure of the left ventricle increases and the lowest values of ACSV were registered in patients with a history of heart failure [[128]]. They reported high variability of ACSV and offered an explanation of that by great interindividual variability of functional curves of the left atrial myocardium. Other authors reported that an atrial role for maintenance of overall performance of the heart is more important when dysfunction of the heart becomes mild or moderate (too developed). When the dysfunction is severe, the atria becomes exhausted and their role is negligible [[112],[129],[130]]. Clinical experience with remarkable worsening of heart failure patients, in whom atrial fibrillation develops, is known and is in line with previously mentioned conception [[88]]. Majority of permanently paced patients is represented by older people. Increasing age is associated with worsen elasticity of the left ventricle. Several publications reported increased importance of the preserved atrial contractility and atrioventricular synchrony in these patients together with increasing age [[85],[98],[101],[131]].
Sigwart and coworkers registered acute changes in pressures inside the heart chambers, SV and ACSV [[113]]. They prove a rapid increase in ACSV from 26±5 to 57±9 % in time interval of 30-60 s when they occluded the left anterior descending artery by an angioplasty balloon. They demonstrated that the magnitude of atrial contribution may be very dynamic in an individual patient. The work supports the suggestion that sympathetic activity plays important role in regulation of atrial contractile function. Other researches sought for possible relationships between sequential cardiac pacing and several echocardiographic characteristics (e.g. ejection fraction, enddiastolic diameter of the left ventricle, E/A ratio). They were not successful [[133]]. They reported a great variability of CO when comparing VVI and DDD pacing. DDD pacing with preserved atrial kick improved CO of in average 39±21 % with a range of 10 to 94 %.
Dernellis et al. compared patients with hypertrophic cardiomyopathy with (HOCM) and without (HCM) obstruction of the left ventricular outflow tract to the control group [[134]]. The active contribution of the left atrium to the load of the left ventricle, estimated from the Doppler signal obtained from the mitral ostium, was higher in patients with HOCM or with HCM than in controls. The atrial contribution to filling was enhanced on rising from a supine to an upright position.
Important questions remain without known answers: Is it useful to quantify atrial contribution routinely? One may conclude any clinically important outcome from the numeric value of atrial contribution? Missing of a method which could fast, noninvasively, and objectively quantify atrial contribution makes the searching for answers difficult.
Definition of Optimal AV Delay Optimal timing of atrial contraction is crucial for a final hemodynamical effect of the
atrial contraction. Optimal length of AV delay (AVD) is given by the time of transmission of a pressure wave from the atrium into the ventricle within the peristaltic atrial contraction. Definition of optimal AV delay may be formulated in the reverse order – by definition of too short and too long AV delays.

Miroslav Mestan and Jiri Kvasnicka 236
Too short AV delay starts the atrial contraction at the end of diastole. The atrial systole is not yet finished when the ventricular systole begins together with a steep rise in the intraventricular pressure. Closure of the atrioventricular valves is not due to change in direction of atrioventricular pressure gradient driven by relaxation of the atria. This is the ventricular contraction what closes the atrioventricular valves so that some degree of systolic regurgitation occurs. The loss of blood from the ventricle at the beginning of systole attenuates the final ventricular contraction in accordance with the Frank-Starling’s law.
Too long AV delay impairs the net performance of the heart in a more complex way. The atrium has relatively shorter time to fill with the blood from the venous bed. Prolongation of the atrial myocardium’s sarcomeres has not to achieve appropriate degree and the force of the atrial contraction may be finally attenuated. The atrial systole occurs too soon in diastole when, especially in cases with shorter RR interval, a phase of fast ventricular filling has yet to be finished. The situation, when the atrial systole is completely finished, before the ventricular systole should start, creates conditions for pressure changes resulting in the re-opening of the atrioventricular valves. Enddiastolic regurgitation of blood may occur. A loss of blood from the ventricle again prevents achievement of appropriate ventricular wall stress and consequently ventricular contractility may be diminished [[86],[88],[135],[136]].
Another research clearly showed that issue of the optimal AV delay length is critically dependent on heart rate [[114],[123],[137]]. Optimal timing of AV delay is also dependent on pacing mode, and the place where both chambers are paced [[138]]. In sensed and paced atrial contractions, there is an interindividually wide time interval (e.g. in DDD mode of about 140 ms) between a delivery of the pacing impulse to the atrial myocardium, successful electrical excitation and actual mechanical systole of both atria [[139],[140]].
Iwase marked the AV interval of 150 up to 200 ms as optimal based on his research with quantification of ACVF [[98]]. Haskell and French published similar results and concluded that the majority of subjects have the optimal AV delay within the range of 140-170 ms, and shorter AV delays should be used only after echocardiographic proof of their benefit [[141]]. In experiments using echocardiography, the optimal AV interval assessed during sensed atrial activity was not beneficial for that case, when both the atria and ventricles were paced and vice versa [[142],[143]].
Optimization of AV Interval in Current Clinical Practice The hemodynamical benefit of AV delay optimization is not exactly assessed yet.
However, based on current knowledge, it does not influence the heart performance only at resting conditions. Although the heart rate plays more important role for maintenance of CO during physical activities than atrioventricular timing do, appropriate setting of AV delay is not redundant. Modern pulse generators use the length of AV delay in timing cycles which are of key importance regarding achievable upper limit of heart rate in a particular patient [[139],[144]].
Within the last 15 years, researchers try to optimize AV delay using some automatic devices including sensors for measurement of length of QT interval [[145],[146]],

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 237
accelerometric measurement of endocardial movements in the apex of the right ventricle [[143]], and they sought after new echocardiographic parameters [[147]].
Interest in AV delay optimization increased significantly when cardiac resynchronization therapy (CRT) became the common approach in treatment of severe heart failure [[148],[149]]. Proper timing of atrioventricular synchrony is considered as important as multisite pacing of the ventricles and even more important than interventricular timing [[150]]. CRT remains the only part of routine pacing practice where some attempt of AV delay optimization remains standard component of the treatment setting. One cannot exclude that AV delay optimization is one of the most important factors responsible for clinical improvement of patients with chronic heart failure on CRT. In the practice of the last 10-15 years, two echocardiographic methods dominated in AV delay setting [[151],[152]]. Both of these methods are based on improvement of ventricular filling at the end of diastole, and on attenuation or prevention of mitral regurgitation. CRT is a treatment approach targeting an improvement of systolic left ventricular performance. It is surprising that the methods used in CRT patients for optimization of AV delay are based on diastolic functions of the heart.
Even in prestigious research pacing centres, detailed assessment of optimal AV delay is not routinely performed in all patients. This is probably due to the missing of noninvasive, fast and cheap method for AV delay optimization. Particularly such method is missing which uses systolic volume or cardiac output. Since 2005, some qualms have emerged about clinical results achieved by echocardiography when used for AV timing. This led to further research on that field and new approaches were published. Changes in the blood pressure and the pulse pressure registered noninvasively by Finometer device were innovatively used in Great Britain [[124],[150]].
Noninvasive In Vivo Measurements of Oxygen Saturation by Pulse Oximetry and Characteristics of Pulse Oximetry Signal Trace
Pulse oximetry systems registering pulse oximetry signal (SpO2) has become one of the
most valuable equipment, for intensive care units, operating theatres, and ambulances. Their popularity is based mainly on their ease to use, mobility and valuable information provided – instantaneous heart rate and numeric value of SpO2.
Registration of oxygen saturation by some device started in 1935 when Matthes developed the first device using red and green light filter. During the Second World War, when pilots during difficult maneuvers were blacking out at high “G” forces, Millikan constructed optical device with ear probe. Shaw together with Hewlett-Packard introduced first absolute-reading ear oximeter by using eight wavelengths. Aoyagi 1972 started registration of SpO2 by a device using conventional pulse oximetry with only two wavelengths. The device used the ratio of red (RL) and infrared (IRL) light absorption of pulsating components at the measuring site. This type of device became commercially available in 1981 [[153]].
Pulse oximetry devices from all manufacturers have essentially two targets. They aim to provide a number of SpO2 in percent, which is as close as possible to real blood oxygen saturation, measured from the specimen of arterial blood. Second target is to properly register

Miroslav Mestan and Jiri Kvasnicka 238
heart rate. Current effort of pulse oximeter manufacturers is stressed on improvement of SpO2 registration. They try to accurately register SpO2 and heart rate not only at stable conditions but especially at extreme conditions (e.g. ambulances, intrauterine monitoring) or in patients in severe status (e.g. cold patients, patients with shock) or in noncompliant ones (e.g. newborns).
Principle of SpO2 registration lies in the fact that oxyhemoglobin (HbO) absorbs RL and IRL in a different way than hemoglobin (Hb) [[154]].The device periodically emits impulses of RL, IRL and in a defined period, measures surrounding ambient light. The frequency of these emissions and absorptions is of about 50-60 Hz. The probe emits lights with known wavelengths (e.g. red light 660 nm, infrared light 940 nm). Both lights spread through optic environment (e.g. finger, ear) between two branches of the probe. During transmission through finger, both lights are absorbed. Finger, in that case, represents environment for light’s irradiation. That environment is assembly from static component (e.g. soft tissues, bone, nail, skin) and dynamic component (e.g. in particular arterial blood, then venous blood, moving artifacts). The amplitude of the static component (DC signal) is affected by the intensity of the light source, sensitivity of the detector, and amount of constant absorbers that are present (sample thickness). These same factors will affect the dynamic component (AC signal). AC signal is also affected by the perfusion (amount of blood volume change per pulse), and oxygen saturation. To make any useful, comparisons between the absorption at the red wavelength and the infrared wavelength, the AC signals must be scaled by the DC signals. Dividing the AC level by the DC level (at each wavelength) gives a corrected or scaled AC level that is no longer a function of the incident intensity.
This scaling process performed by electronics, mathematics, or otherwise, yields values that are compensated for variations in incident light intensity and represent the relative absorption of light at two wavelengths that is only due to the hemoglobin in the arterial blood. The numeric ratio of the corrected red value to that of the corrected infrared value yields a result that is easily converted to oxygen saturation. The pulse oximeter’s focus on just the “dynamic” arterial flow, along with the compensation process, neatly circumvent nearly all of the obstacles that have plagued the classic oximetry technique. Pulse oximetry uses a simple concept to defeat complex problem. The simplicity, however, is deceptive [[155]]. Some weighed averaging process is involved to construction of the SpO2 number which is displayed on the screen of the device. This is the reason why this SpO2 number is absolutely unusable for our purposes described in this chapter.
Everything important in pulse oximetry happens in AC signal. The greatest differences between the most important manufactures of pulse oximetry devices (e.g. Nellcor, Ohmeda, Masimo) exist in their approach to improve the quality of AC signals.
Waveform of pulse oximeter devices is real photoplethysmographic waveform. The aim of its use in pulse oximetry is simple. It gives information that the pulse oximeter has pulsing arterial blood as the source of its signal. The work presented further in this chapter uses a hypothesis assuming that waveform of SpO2 tracing and waveforms of invasively registered blood pressure tracing are analogous. Sudden changes in the pulse amplitude of SpO2 may behave in a similar way as sudden changes in the pulse pressure which are closely connected to SV changes. In the past, these changes in SV or the pulse pressure were used in studies on AC. The principle of registration allows only beat-to-beat changes in the pulse amplitude of

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 239
SpO2. That is due to extreme sensitivity of SpO2 to different artifacts, and due to automatic re-scaling incorporated in pulse oximeters.
All manufacturers of patients’ bedside monitors equip their devices with automatic re-scaling systems. These systems should maintain the amplitude of SpO2 tracing maximum possible to use optimal space on the screen dedicated to SpO2. In the 1990’s, some firms Hellige, Hewlett-Packard or Nellcor used an approach which was unfriendly to our purpose. If the instantaneous pulse amplitude exceeded the part of the display dedicated to SpO2, maximum and/or minimum values on SpO2 tracing were substituted by the minimum and/or maximum values from the scale on the display. These “cuts” to the tracing made it unusable for determining of atrial contribution index described hereafter in this chapter. Patients’ bedside monitors manufactured by Marquette (USA) were the only suitable monitors we had available for our work in 1995.
Since 1995, we have not found any paper in literature reporting the use of photoplethysmographic tracing from the pulse oximetry for estimation of any hemodynamic variable. We could test two oximetric probes – an ear probe and a finger probe. Signal obtained from the finger probe was significantly more stable and less vulnerable to artifacts. In 1995, first results of a new pulse oximetric system Masimo SET were published. Since that time, great advances have been achieved on the field of pulse oximetry research owing to leading firms Masimo, Nellcor, and Ohmeda [[156],[157],[158]]. One may speculate that the differences in the tracings of SpO2 on the monitor Eagle 4000 compared to different monitors and systems are probably low. Although filtration and post-processing of AC signal may differ among manufacturers, the photoplethysmographic principle remains the same.
Theoretical Basis for Design of the New Method Estimating the Atrial Contribution Index Derived from Pulse Oximetry Signal
Main function of the heart is to pump blood coming from the veins in the amount driven
by needs of the peripheral tissues into the arteries. Measurement of ACVF gives only limited, indirect information about behavior of the ventricle at the end of diastole. We had the following reasons for refusing ACVF quantification when a novel method should be designed. Most papers on ACVF used echocardiography [[85],[97],[98],[118],[133],[134],[159],[160]]. Doppler signal obtained on the mitral orifice itself shows only instantaneous status of pressure gradients present there. It says nothing about the real amount of blood flowing through mitral valve and consequently, that it is really added into the ventricle at the end of diastole. It is impossible to measure real volumes of blood exchanged through the mitral valve based only on Doppler echo without knowledge about the volume of the atrium and real area of the mitral valve. Ormiston published a paper on changes of diameter of the mitral orifice which is not calcified [[161]]. In addition, Triulzi reported that the size of the left atrium and the left ventricle decreases when preload is diminished. Doppler echocardiographic parameters have low sensitivity and specificity when preload and/or afterload of the left ventricle changes [[162]]. All routinely used Doppler parameters from the mitral orifice are affected with heart rate and length of PR interval [[163]].

Miroslav Mestan and Jiri Kvasnicka 240
It is impossible to derive ACSV from ACVF because the latter does not take into account effect of afterload, and of contractile status of the myocardium. The backward flow of blood into the pulmonary veins might play some role in complicated relationship between ACVF and ACSV [[164],[165]]. Despite all these facts, nowadays methods based on Doppler echocardiography measuring ACVF serve mainly in CRT for AV delay optimization.
In our opinion, systolic function of the heart is more important than diastolic function. The new method should be targeted to atrial contribution to systolic function. We treated evaluation of ACCO as problematic, and inappropriately technically difficult. Cardiac output is not an easily measurable hemodynamic parameter when only simple and noninvasive techniques should be employed. One can obtain the best results from catheterization methods based on the Fick principle, by dilution with dye or by thermodilution. Measurement of CO based on Fick principle cannot be quickly repeated within time interval of 1-2 minutes. The dye dilution method for CO estimation is well documented, widely spread and its use was tested with tenths of years practice. Precise data exists that the measurements are repeatable in time steps of 1 minute with average error between individual values of about 10-20 % [[166]]. When a newly developed noninvasive method will have a similar error between obtained individual values, one can talk about success.
From studies on atrial contribution to cardiac output, evidence was obtained about AV delays shorter than 50 ms and longer than 300 ms, which are hemodynamicaly compromising [[105]]. Author published as well that atrial contraction may help best to ventricular performance when heart rate is in interval between 50-90/min [[105],[167]].
There is another issue as far as CO is concerned. The generally accepted rule is that the magnitude of CO is dictated by needs of peripheral tissues unless severe disease limiting CO is present (e.g. mitral stenosis, severe heart failure due to myocardial infarction). One may speculate that at rest or during mild physical activity, magnitude of CO should not change due to manipulation with the pulse generator setting in healthy, permanently paced patients. Warner and Toronto published results from an experiment done on anesthetized dogs with artificially induced complete AV block examined at rest and during constant mild physical effort [[168]]. Changes in heart rate induced by pulse generator led to such changes in SV, in which the magnitude of CO was maintained on the same level. A similar situation in human subjects was reported by Sowton [[169]]. He established asynchronous ventricular stimulation in individual with preserved sinus rhythm. When pacing had been started, CO decreased first but in time, but within the delay of several minutes, CO returned to almost the same level as when being on sinus rhythm. The same author, reported in another paper, confirmation of Warner’s conclusions [[169]]. When heart rate changed, SV reacts in such way to maintain CO of similar magnitude. Nishimura designed experiment when first administered alfa-sympathomimetic substances in order to increase systolic blood pressure, and then they administered nitroglycerin in order to decrease systemic blood pressure and pulmonary capillary wedge pressure. During these both hemodynamic interventions, resting CO remained statistically unchanged [[164]]. Another experiment showed acute change in heart rate from 70/min up to 112/min leading to stabilization of CO within time interval of 3 up to 7 minutes in a group of 5 patients [[167]]. Compensatory increase in SV in order to increase CO when heart rate was maintained strictly constant as well as subjects who were exposed to exercise testing was described in a study measuring CO by Fick method [[106]].

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 241
Different regulatory components in the circulation do have different onset time and different inertia of their effect. To our knowledge, only Sowton published a paper dealing with the velocity and course of CO changes due to different hemodynamic interventions [[167]]. The rest of experiments using ACCO either did not notice exact time interval between intervention and registration of CO or they measured CO in different time intervals after intervention. Some authors estimated CO in 1-2 minutes after pacing changed [[109]]. Others waited for “stabilization” of the circulation (e.g. 10 minutes) in echocardiographic studies and then they used averaged values of CO [[117]]. All this research does not have evidence that the time interval chosen for CO changes evaluation is right indeed. In addition, waiting for “stabilization” of circulation leads to further undesirable prolongation of examination. The most important question still without answer remains: How long of a time interval should elapse between two CO measurements in order to evaluate effect of any intervention?
Another key issue exists as far as cardiac output is concerned. Nowadays, invasive approach for CO estimation is ethically and economically unacceptable in routine everyday practice if it is used for atrial contribution estimation and AV delay optimization in permanently paced patients. Only noninvasive methods remain – nuclear cardiology, bioimpedance, and preferably echocardiography. All these methods are considerably less accurate when compared to invasive methods. Their use is only acceptable because they are noninvasive. As far as echocardiography is concerned, observer-dependency is the major disqualifying factor. Since the 1980’s, large amount of papers comparing CO values from echocardiography and from invasive techniques exists [[170],[171],[172]]. Davies and coworkers published interesting paper on CO estimated by Doppler echocardiography and by invasive techniques using thermodilution and Fick principle. In a group of 12 patients, they published not only correlation analysis (i.e. common statistical mistake) but even Bland and Altman’s analysis of agreement between methods. When comparing CO from Doppler echocardiography, correlation coefficient of 0.81 was computed when compared to thermodilution and that of 0.76 when compared to Fick method, respectively. Mean difference between CO from thermodilution and CO from echo was 0.32±0.48 l/min and limit of agreement reached value of 0.96 l/min. Authors considered these results as clinically acceptable when one wants to replace invasive approach by cheap and easily available echo. If we consider these results regarding magnitude of CO changes, limit of agreement of 0.96 l/min represents at least 20 % of resting CO value. If dye dilution technique has error about 10-20%, then echocardiography has to have a much higher error. It disqualifies echocardiographic evaluation of ACCO from our scope when development of new method was planned. Similar unconvincing data on echocardiographic measurement were communicated by author of this chapter with Frieder Braunschweig from Karolinska Hospital later on Europace in Prague 2005 [[173]].
In a paper written by an echocardiographist, targeting cardiac pacing laboratories, it is clearly commented on that echocardiography does not measure directly values of SV or CO but only some indices which might help to estimate changes in SV or CO. It highlights many limitations, and simplifications which are connected with that type of examination [[174]]. Echocardiographic textbook lists limitation of echo when CO is measured and comments some pitfalls in interpretation of results [[175]].

Miroslav Mestan and Jiri Kvasnicka 242
Studies based on comparison of CO when subjects are paced in DDD and VVI mode should take into the consideration superiority of parasympathicus when on VVI mode. This parasympathetic superiority is due to reflex reactions present in patients with preserved atrial contraction in whom retrograde ventriculo-atrial conduction is present and sometimes contraction of the atrium against the closed atrioventricular valve occurs.
Measurement of ACSV remains acceptable method of choice when evaluating benefit of properly timed atrial contraction for systolic function of the ventricle. It is more simple and reliable at resting conditions. There is no need to multiply the result by heart rate and there is no affection due to ventriculo-atrial conduction. Simple extrapolation of ACSV to ACCO is not possible. Beat-to-beat changes reflect only changes in the heart functions, i.e. in myocardial contractility (frequency phenomena) and/or in ventricular filling. That was the most interesting idea and advantage we’ve taken into account when designing new method.
Idea to use beat-to-beat changes in order to quantify atrial contribution is not new. Sophisticated experiment in anaesthetized dogs with surgically induced complete AV block and sequential pacing showed that sudden drop of atrial contraction induced a decrease of 20±5 % in SV [[116]]. Measurement of aortal flow was quite complicated and in the other research, authors tried to replace that by registration of pulse pressure. Several research attempts have been made to compute systolic volume from pulse pressure; unfortunately they were not successful [[176],[177],[178],[179]].
Proposal of the new method was inspired by three experiments. Fagrell and Lindvall studied possibility to replace echocardiographically registered SV by digitally registered pulse volume in the peripheral artery [[120]]. Second experiment used photoplethysmography for registration of pulse wave in the peripheral artery [[119]]. Authors registered the soonest occurrence of pulse wave after QRS complex and the greatest amplitude of that wave when “optimal AV delay” was set. Third research confirmed possibility of idea that sudden drop of atrial contraction could induce some decrease in the pulse pressure [[115]] and served as a reference for development of the new method. Values of ACSV from the pulse pressure were about 29.3±8.9 % in patients with sick sinus syndrome, and about 10.8±2.1 % in those with severe congestive heart failure and complete AV block at AV delay of 170 ms.
Optimal heart rate in human individuals is about 55-90/min at rest. Evidence exists that ACCO may change significantly when heart rate is greater than 100/min [[105]]. Even value of optimal AV delay changes in heart rate faster than at rest [[114],[123],[124]]. That was the reason why we designed the method to use resting heart rates (i.e. 65-95/min) despite we needed 100 % atrioventricular pacing.
Aim of the Research Because suitable method for quantification of atrial contribution to systolic volume of the
left ventricle is still missing we designed a series of studies with following aims: • to develop a fast, cheap, noninvasive and observer-independent method for
estimation of an atrial contribution index

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 243
• to compare the atrial contribution index derived from pulse oximetry signal with a similar index derived from the invasively registered pulse pressure
• to assess reproducibility and repeatability of the method and of the atrial contribution index
• to use the atrial contribution index for AV delay optimization in sequentially paced patients
• to investigate whether acute hemodynamic changes may influence values of the atrial contribution index and find possible clinical use of our results
Methods and Design of Studies The whole research was planned like a series of consequent studies on limited numbers
of subjects. Organization of the next study was dependent on the positive results from the previous one. Research started 1995 with building of equipment and single-purpose software (SW hereafter in this chapter).
Patients All studies included in our research were evaluated and approved by the local ethics
committee. All enrolled subject gave their written informed consent with the participation in the study. All enrolled patients were older than 18 years and in all of them, permanent cardiac pacing with the dual chamber pulse generator had been indicated and implanted from medical indications before they were asked about possible participation in the studies. Indications for permanent cardiac pacing in our patients were second or third degree AV blocks (AVB), sick sinus syndrome (SSS), and hypersensitivity of the carotic sinus (only in one patient).
None of enrolled subjects has an implanted artificial arterio-venous shunt for hemodialysis treatment. None of them has hemodynamicaly important heart valve’s defect either stenotic or regurgitant, and none of them has shunt on the level of the heart or great vessels. Systolic function of the left ventricle and gender were not criteria for enrollment. Patients were excluded from the studies if they were addicted to drugs or alcohol.
Total number of 94 patients was enrolled to our research from four cardiac pacing centres. These centres were in University Hospital in Hradec Kralove, in regional hospital in Usti nad Orlici, in Hospital Na Homolce in Prague, and in Karolinska Hospital in Stockholm. Some of the patients were examined repeatedly in order to assess reproducibility of the method and of the index. Relevant detailed specification of study subgroups will be mentioned hereafter in the Results section.

Miroslav Mestan and Jiri Kvasnicka 244
Pulse Generators and Their Programming In all patients, only dual chamber pulse generators were used. The atrial electrode was
placed into the upper part of the right atrium. The ventricular electrode was placed into the apex of the right ventricle. None of our patients has any type of multisite pacing.
All used pulse generators had to fulfill the following technical criteria. First, pulse generator had to be able to change pacing modes at the same ventricular rate which had been programmed like base (minimum) rate. Second, absolutely constant rate of ventricular beats had to be kept while AV delay was changing. Preservation of constant resting programmed AV delay between individual visits at the pacemaker clinic was the last request. Function “rate-responsive AV delay” was allowed. List of used pulse generators is given in Table 1. List of pulse generators excluded from study including reasons for that is given in Table 2. During the participation of patients in the studies, pacing modes DDD, DDI and VVI were programmed.
Table 1. List of used dual chamber pulse generators
Pulse generator Manufacturer Physios Biotronik Kairos Biotronik Synchrony II St.Jude Medical Paragon II St.Jude Medical Trilogy DC+ St.Jude Medical Trilogy DR+ St.Jude Medical Entity DR St.Jude Medical Affinity DR St.Jude Medical Prodigy DR Medtronic Sigma DR Medtronic Thera DR Medtronic
Table 2. List of manufacturers of pulse generators excluded
from the studies due to technical reasons
Manufacturer Reason for exclusion from study Ela Medical pulse generators have their own automatic procedure changing AV delay Vitatron pacing rate increases to 100/min when magnet is placed over pulse generator Sorin Biomedica pacing rate increases to 100/min when magnet is placed over pulse generator
Measurement of Vital Signs and Anthropometric Data Body weight was taken on the same scale with range from 0 up to 200 kg with accuracy
of 0.2 kg. Noninvasive blood pressure was taken by physician using standard tonometer with column of mercury. The catheter-tip manometer (Millar Instruments, Inc.) was used for continuous measurement of blood pressure in the ascending aorta. The catheter was indwelled via 7F sheath into the femoral artery under fluoroscopic control and placed into the

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 245
ascending aorta. ECG registration was performed via three line cable directly by the patient monitor Eagle 4000. The ECG signal from the II limb lead was chosen because pacing spikes have positive and QRS complex negative deflection in that lead. In order to see well pacing impulses, unipolar pacing configuration on pacing electrodes was programmed.
Exclusively, only transthoracal echocardiography was employed in the studies. Examinations were performed by the same skilled cardiologist. All patients were examined in 2D mode, with pulse, continuous and color Doppler echocardiographic examinations in order to obtain information about size of the heart chambers, ejection fraction of the left ventricle, and to exclude any hemodynamicaly moderate or severe valvular defect or shunt on level of the heart and great vessels. Special attention had been paid to the mitral and aortal valves.
In several patients, isotope ventriculography (first pass technique) was performed in order to estimate ejection fraction of the left ventricle. Statistical Methods
For every statistical assessments used in the studies, significance level α=0.05 had been
chosen. Some particular studies gave not-normal distribution of data. In these cases, median and interquartile range (first quartile – third quartile) were used in order to describe distribution of variables. In the other cases, arithmetic mean (mean) and standard deviations (SD) were used for description of data. Assessment of atrial contribution indexes’ agreement was made by Blant and Altman’s method [[180]]. Wilcoxon’s non-parametric test, the same test with Bonferoni’s correction (significance level α=0.0167), Fisher’s exact test, Mann-Whitney U-test, and ANOVA were used for assessment of our results. Important notices regarding statistical analyses will be mentioned hereafter in the Results section of this chapter.
A New Method for Estimation of Atrial Contribution Index Using a Pulse Oximetry
Signal Tracing
Principle of the Method This newly introduced method serves for estimation of an atrial contribution to systolic
volume of the left ventricle in sequentially paced patients [[181]]. The method is based on beat-to-beat induced changes in either the pulse amplitude of the pulse oximetry signal tracing or in the pulse pressure (reference method for comparison). One can use the method only at rest. Extreme pulse oximeter’s sensitivity to any moving excludes measurements during even minimum physical activity.
Principle of the method is very simple and Figure 1 makes it better to understand it. During any changes of the pulse generator’s parameters, the ventricular rate is maintained strictly constant in order to exclude influence of so-called “frequency phenomena” [[182]]. Sudden change of pacing mode from DDI to VVI causes a drop of atrial stimulus and consequently of the atrial contraction. A decrease in the pulse amplitude of SpO2 occurs in

Miroslav Mestan and Jiri Kvasnicka 246
the condition when the atrium does not help the ventricle achieve optimal contractile force. Such a fast hemodynamic change emerges so unexpectedly that no regulatory mechanism in the circulation is able to react in time. The last pulse amplitude in DDI mode is hereafter called BeatDDI. The amplitude of first beat in VVI mode is called BeatVVI. Final value of the atrial contribution index (ACSp) was counted using formula:
ACSp = [(BeatDDI-BeatVVI)/BeatDDI] x 100 [%] The high sensitivity of the pulse oximeter was a real problem. In order to eliminate as
much artifacts as was possible, we proposed arbitrarily criteria for the SpO2 tracing’s stability. Both these criteria do have relationship to amplitude BeatDDI because of its key role in the formula for ACSp computation. First criterion said that the difference between the amplitude BeatDDI and the pulse amplitude of beat immediately preceding BeatDDI must be within limit -4 to +5 % of the amplitude BeatDDI. Second criterion compared the difference of positions of two minimum values on SpO2 tracing - first in BeatDDI and second in the beat immediately preceding BeatDDI. The difference must be within interval -3 to +4 % of the amplitude BeatDDI. For better understanding of both criteria, see Figure 1 and the table in Figure 3. If any of both criteria was not fulfilled, single-purpose software (SW) prevented further automatic processing of data and required a repetition of the measurement at the same particular AV delay.
Figure 1. Tracings of ECG and pulse oximetry signal (SpO2). A change of pacing mode from DDI to VVI occurred at the 4th beat. Sudden drop of atrial contraction caused an acute decrease in pulse amplitude of SpO2 from amplitude Beat DDI to amplitude BeatVVI. Minimum values on SpO2 tracing (indicated by arrows) and comparison of amplitudes BeatDDI and pulse amplitude of a beat immediately preceding BeatDDI were used for evaluation of SpO2 tracing’s quality. The continuous rise in amplitude of SpO2 tracing apparent at 5th and 6th beat occurred due to automatic re-scaling of SpO2 tracing, and changes in a finger’s circulation.

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 247
Hardware, Software, and other Equipment The new method is not too demanding as far as hardware is concerned. The bedside
patients monitor and personal computer were necessary for the measurements. The bedside monitor has to be able export on-line simultaneously registered data of ECG, the invasively registered blood pressure (BP), and SpO2 via standard Ethernet connection to personal computer with Windows system installed. The bedside monitor Eagle 4000 (Marquette, USA) has been used through all studies. Tracings were displayed with 25 mm/s shift. The sampling frequencies for ECG, BP, and SpO2 were 240 Hz, 120 Hz, and 60 Hz respectively. The monitor exports not absolute but relative units of monitored variables in order to display the tracings even on the central unit monitor. A scaling of BP was fixed and we used range 0 to 200 mm Hg. On the other hand, the scaling of SpO2 is relative at any condition. The scaling of ECG is also fixed and isoelectric line was systematically shifted from the value 0 on the monitor. Figure 2 shows simultaneous recordings of all three variables displayed as the same way as they were on the screen of the computer. The personal computer has standard Windows system installation together with standard Ethernet connection for communication with the monitor.
As far as software is concerned, a packed of single-purpose software (SW) has been created. The tasks of SW include transform on-line data from the monitor into the text file, post-processing of data, and creation and printing of protocol in case of accepted measurement.
First part of SW was aimed to transform raw on-line data into the text file. All three variables (ECG, BP and SpO2) and later only ECG and SpO2 were registered in packets simultaneously.
Next part of SW has been developed by the author of this chapter using program Famulus 3.5. The software Famulus is dedicated for mathematic models, their displaying either as tables or as graphs [[183],[184],[185]]. Many of figures used in this chapter are in fact screens of the computer during processing of data with SW.
Last used software was text editor MS Word. It serves for final formatting of the text and printing.

Miroslav Mestan and Jiri Kvasnicka 248
Figure 2. Screen showing simultaneous tracings of ECG, invasively registered aortal blood pressure (BP), and pulse oximetry signal (SpO2). A drop of atrial impulse and consequently of an atrial contraction is apparent at the 4th beat. A decrease in pulse pressure and in pulse amplitude of SpO2 follows. Phase shift between BP tracing and SpO2 tracing is caused by post-processing of the signals. Units on a y axis are only relative, given by automatic scaling in the monitor of living functions.
Detailed Description of Methodology
Subjects were placed into the supine position during examination. The pulse oximetry
probe was placed on the finger of the dominant hand. Success of measurement critically lay on good information of subject about further steps. They were informed that the finger with the probe must not move until all measurements were done. In order to eliminate any possible influence of the venous blood pressure on SpO2, the hand was elevated above a level of the chest.
Another issue represents changes in blood flow caused by the intrathoracic pressure changes during the breathing cycle. That may significantly affect quality of SpO2 so that we had to instruct patients about special course of breathing. The breathing must be kept within normal, resting excursions of the chest (i.e. without excessive breathing in and/or out). Immediately the calm breathing out was finished, we asked patients to stop breathing in and hold a breath for a several seconds (i.e. up to 15 s).
Pulse generator was set to DDI mode. Base pacing rate was set to value which assure 100 % of atrio-ventricular pacing. That rate remained unchanged during the whole course of measurement.
Demographic and anthropometric data about subjects were saved into a text file. A unique serial number has been assigned to each individual patient and his/her series of

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 249
measurement. All the data were finally used into the protocol from examination. The unique serial number served for construction of a name of the text file as well, including data from accepted measurement for archive purposes. It was of critical importance because the number in the file’s name served for automatic reading of data from the hard disc for final assessment.
Person sitting at the computer started transport of on-line data from the monitor to the computer. Patient was asked for short hold of breath and quality of SpO2 was checked on the screen of computer. When quality seemed to be good, the technician suddenly changed pacing mode from DDI to VVI for a several beats. From that moment, subject could continue in a normal way of breathing. Obtained data of ECG, BP, and SpO2 were stored on the hard disc.
Since that time, data has been processed off-line. The data file was open in SW. Every pacing spike was marked and displayed in order to perform visual check of the appropriate detection of all spikes, and exclusion of possible false detections of spikes on ECG. Automatic detection of pacing impulses and the length of particular AV delays (AVDs) made it possible to detect BeatDDI and BeatVVI. The lengths of individual AVDs had to remain constant as well. If not, we had to refuse such a measurement. The SpO2 tracing was analyzed in order to exactly check quality of measurements. It was possible to continue only when both criteria of tracing’s quality were fulfilled. In the case of low-quality measurement, SW stopped further processing of data and required a repetition of measurement. Value of ACSp was then computed. Signals’ tracings and evaluation table was then displayed on the screen (Figure 3).
Accepted measurement was saved into the text file on the hard disc. Data file contained demographic and anthropometric data about subject, unique serial number, pacing rate, particular AVD, indexes which make it easy to detect again positions of amplitudes in question, and all simultaneous data of ECG, BP, and SpO2.
All these above steps were necessary for to get one successful measurement of ACSp at particular AVD. Hereafter in this chapter, these steps will be called “basal ACSp measurement”.
The atrial contribution indexes were measured for all chosen AVDs sort in ascending order. Set of these atrial contribution indexes obtained in a given range of AVDs will be hereafter called “series of ACSp”. After first series of ACSp was finished, measurements of ACSp for the same set of AVDs were repeated once more. Finally in every subject for every particular AVD, two basal ACSp measurements (series ACSpa and ACSpb) were done in order to obtain data for analyses of reproducibility.

Miroslav Mestan and Jiri Kvasnicka 250
Figure 3. There is screen of personal computer with graphs containing simultaneous tracings of ECG and invasively registered blood pressure (left up), graph displaying simultaneous tracings of ECG and pulse oximetry signal (left down), and a table showing assessment of basal measurement of atrial contribution including evaluation of tracings’ quality (right). In the table, there are length of original AV delay in DDI mode, type of pacing mode’s change, and heart rate. In the lower part of the table, second row of figures represents atrial contribution index values in %. Values in left column were obtained from blood pressure (BP), in right column from pulse oximetry (SpO2).
Final assessment of optimal AV delay used other part of SW. Firstly; particular AV delays in question were checked in a menu of SW. Then it was necessary to fill in unique serial numbers of two series of ACSp. Software read data files automatically from the hard disc. Every particular basal ACSp measurement has been displayed again in order to visually check correctness of data. When all data files were read, SW computed arithmetic mean (ACSpmean) from both basal ACSp measurements for every chosen AV delay. Relationship between AV delays in question and corresponding ACSpmean served for optimization of AV delay (Figure 4).

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 251
Figure 4. A screen shows final assessment of all basal measurements of atrial contribution index (ACSp). On the left side, there is a graph displaying relationship of mean ACSp and particular AV delays (AVD). A table on the right side contains four columns with complete results of individual ACSp measurements. First column contains length of used AVD in ms. Next two columns show two series of basal ACSp measurements (marked with unique serial number in header 4002 and 4003). Values from 2nd and 3rd column are displayed as triangles in the graph. Fourth column contains arithmetic means of ACSp for every particular AVD. Means are displayed as rectangles connected with the line in the graph. Menu up in the graph serves for further work with the software.
All final assessment was then saved into the text file opened in MS Word. The text editor made final formatting of the text, attached the graph of relationship between AVD and ACSpmean, and printed the protocol (Figure 5). Print of the protocol was possible within 5 minutes after the last basal ACSp measurement finished.

Miroslav Mestan and Jiri Kvasnicka 252
Figure 5. Protocol from examination of atrial contribution index (ACSp) with assessment of an optimal AV delay was available within 5 minutes after last measurement of ACSp finished.

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 253
Results
Development of the Method and Its Limitations When development of the method started, we needed some reference method used in the
past which would resemble our design of atrial contribution index. This was the reason why we used the invasively registered pulse pressure in the ascending aorta. We computed similar atrial contribution index derived from BP using the same formula mentioned above. This index is hereafter in this chapter marked like ACBP (i.e. ACBPa, ACBPb, and ACBPmean). These indexes were obtained simultaneously together with atrial contribution indexes derived from the pulse oximetry signal.
The method and automatic SW was designed to search for the optimal AV delay within the range of 50 up to 250 ms. From technical reasons (filtration of ECG during post-processing inside the monitor), the smallest steps between particular AV delays may be of minimum 25 ms.
Support for the upper extremity in the elevated position was critically important to make the position as comfortable as possible. If patients felt the elevated position of the hand uncomfortably, they had a tendency to move during measurements. We also found it useful to exercise the kind of breathing mentioned in the methodology description before the real measurement started. Subjects became familiar with the method and could recognize nothing wrong happens with them. Both these precautions increased the success rate of measurements and prevented unnecessary repetition due to unacceptable quality of signal either of SpO2 or BP.
In 20 patients of ours, echocardiographic data from M-mode, two-dimensional, and Doppler examination was available. Data about systolic function was also available from isotope ventriculography. Absence of apparent relationships between ACSp and several routinely examined hemodynamic variables was disappointing. Atrial contribution index derived from SpO2 did not have any relationship to ejection fraction of the left ventricle, left atrial size at the beginning of diastole, enddiastolic and endsystolic diameter of the left ventricle. Our findings are in accordance with literature [[111],[118],[186]].
Eight years experience makes it possible to formulate essential limitations of the method. It is absolutely impossible to measure ACSp during any physical activity due to extreme sensitivity of pulse oximetry to different moving artifacts. The value of SpO2, provided by pulse oximeter, need not be affected, because the device displays that as weighed average with some delay between real measurement of SpO2 and displaying the result. Photoplethysmographic tracing of SpO2 is affected immediately by any movement or any circulatory change due to even normal breathing.
Next limitation is of similar nature as the one mentioned above. It is impossible to examine subject suffering from any disease causing tremor or shaking. Etiology of the disease does not play any role.
Noncompliance of a subject, regarding the breathing style or requirements of calm position without moving, was other major limitation of the method.

Miroslav Mestan and Jiri Kvasnicka 254
Numerous ectopic electric ventricular activities were another problem limiting possibility to get satisfactory SpO2 tracing. When ventricular extrasystoles are more frequent than 5/min, the measurement becomes almost impossible.
Of course, subject must be equipped with the suitable pulse generator without changes of basal programmed rate or AV delay length while programmed. Attempt to measure ACSp at heart rate of more than 100/min lead to problems with automatic detection on ECG.
Analysis of Agreement between Atrial Contribution Indexes Derived from Pulse Oximetry Signal and Pulse Pressure
The key question at the beginning of the method’s development was whether it is
possible to replace invasively registered blood pressure tracing with the SpO2 tracing. Registration of blood pressure directly in the arterial bed is risky, unpleasant from the view of patients, and expensive. On the other hand, one can measure that very precisely. Pulse oximetry signal is very easy to obtain and suitable devices became widely spread in healthcare facilities in the last 15 years.
We enrolled 50 subjects in this study. We did not have any special exclusion criteria (e.g. ejection fraction of the left ventricle, gender) because we wanted to examine relationship between ACSp and ACBP on heterogeneous population. The catheter-tip manometer was successfully placed into the ascending aorta in the whole group of patients.
We had to exclude 3 subjects from the final evaluation. We could not obtain SpO2 tracing of acceptable quality in two men due to non-compliance during breathing. One female subject suffered from shaking due to brain atherosclerosis so that we obtained unacceptable SpO2 tracing.
Forty-seven subjects were included in the final assessment. In all of them, we obtained two series of basal measurements of ACSp (ACSpa, ACSpb) and ACBP (ACBPa, ACBPb). Then we calculated mean values of atrial contribution indexes derived from both SpO2 and BP (ACSpmean and ACBPmean).
First of all, reproducibility of ACSp and ACBP had to be assessed. Analyses were done following the method proposed by Bland and Altman. Table 3 and Table 4 contain description data relating to analysis of reproducibility. Graphic evaluation is given on Figure 6 and Figure 7. Mean difference between basal measurements from two series was near 0 in both, ACBP and ACSp. Limit of agreement for ACBP reached its maximum at AV delay of 150 ms. Limit of agreement for ACSp was wider than for ACBP. It reached its maximum at AV delay of 200 ms.

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 255
Figure 6. A graph displays Bland and Altman’s analysis of reproducibility of atrial contribution index derived from the pulse pressure in the ascending aorta (ACBP) obtained from 47 subjects. Mean difference of values obtained from first (ACBPa) and second (ACBPb) series of basal measurements was near 0 and it is represented by a solid line in the graph. Used AV delays differ by the density of points.
Figure 7. A graph displays Bland and Altman’s analysis of reproducibility of atrial contribution index derived from the pulse oximetry signal (ACSp) obtained from 47 subjects. Mean difference of values obtained from first (ACSpa) and second (ACSpb) series of basal measurements was near 0 and it is represented by a solid line in the graph. Used AV delays differ by the density of points.

Miroslav Mestan and Jiri Kvasnicka 256
Table 3. Analysis of reproducibility of the atrial contribution index derived from the invasively registered blood pressure in the ascending aorta (ACBP). Differences were counted from first and second series of basal ACBP measurements (ACBPa-ACBPb).
AV delay (ms) 50 100 150 200 250 number of subjects 47 47 47 47 47 mean difference (%) -1,3 -0,1 -1,2 -1,4 -0,1 SD of differences (%) 4,0 1,7 4,3 4,0 4,1 2SD (%) 8,0 3,4 8,6 8,0 8,2 mean - 2SD (%) -9,3 -3,5 -9,8 -9,4 -8,3 mean + 2SD (%) 6,7 3,3 7,4 6,6 8,1
Table 4. Analysis of reproducibility of the atrial contribution index derived from the pulse amplitude of the pulse oximetry signal (ACSp). Differences were counted from
first and second series of basal ACSp measurements (ACSpa-ACSpb). AV delay (ms) 50 100 150 200 250 number of subjects 47 47 47 47 47 mean difference (%) -0,9 -0,4 -1,1 -1,2 0,4 SD of differences (%) 4,8 4,0 3,9 5,0 4,6 2SD (%) 9,6 8,0 7,8 10,0 9,2 mean - 2SD (%) -10,5 -8,4 -8,9 -11,2 -8,8 mean + 2SD (%) 8,7 7,6 6,7 8,8 9,6
Regression analysis proven that linear relationship exists between ACBPmean and
ACSpmean (Figure 8). It is apparent that a little shift to the benefit of ACBPmean exists. Numerical expression of that shift is displayed in Table 5. Limits of agreement in all AV delays in question were less than 10 % and that means that the agreement of both indexes is clinically acceptable. Graphic expression of the analysis is given in Figure 9.
Figure 8. A regression graph of mean values of atrial contribution index derived from the pulse pressure (ACBPmean) and atrial contribution index derived from pulse amplitude of pulse oximetry signal (ACSpmean)

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 257
obtained in 47 subjects. There is systematic shift of distribution line to the benefit of ACBPmean. Used AV delays differ by the density of points.
Figure 9. Bland and Altman’s analyses of agreement between mean atrial contribution index derived from the blood pressure (ACBPmean) and atrial contribution index derived from pulse amplitude of pulse oximetry signal (ACSpmean) obtained in 47 subjects. Every individual AV delay has its own graph. Solid black line represents a mean of differences between ACBPmean and ACSpmean. The mean difference in all examined AV delays shifted to the benefit of ACBPmean. It is also apparent that range of differences on y axis do not increase with increasing mean value on x axis.

Miroslav Mestan and Jiri Kvasnicka 258
Table 5. Bland and Altman’s analysis of agreement of the atrial contribution index derived from the pulse pressure (ACBP) and the atrial contribution index derived from
the pulse oximetry signal (ACSp). Mean difference between indexes (ACBP-ACSp) is systematically shifted to the benefit of ACBP
AV delay (ms) 50 100 150 200 250 number of subjects 47 47 47 47 47 mean difference (%) 2,7 5,0 5,1 5,5 5,1 SD of differences (%) 3,5 4,1 4,4 4,2 4,4 2SD (%) 7,0 8,2 8,8 8,4 8,8 mean - 2SD (%) -4,3 -3,2 -3,7 -2,9 -3,7 mean + 2SD (%) 9,7 13,2 13,9 13,9 13,9
Descriptive statistics of obtained values of ACBP and ACSp are given in Table 6 and
Table 7, respectively. Mean values of ACBP were higher than that of ACSp. Range of ACBP and ACSp was quite wide.
Table 6. Descriptive statistics of atrial contribution indexes derived from the pulse
pressure related to the corresponding AV delays AV delay (ms)
mean ACBP (%)
SD min max median distribution
50 13,1 11,7 -10,3 54 13,3 normal 100 27,4 12,8 0,2 58,5 28 normal 150 36,4 14,7 3,7 61 36,3 normal 200 39,1 15 9,5 69,6 39,8 normal 250 38,7 15,5 11,2 76,2 39,4 normal
Table 7. Descriptive statistics of atrial contribution indexes derived from the pulse
amplitude of the pulse oximetry signal related to the corresponding AV delays AV delay (ms)
mean ACSp (%)
SD min max median distribution
50 10,4 10,6 -14,4 45,5 11 normal 100 22,4 12,1 -3,3 50,6 22,8 normal 150 31,4 14 -0,2 59,7 30,1 normal 200 33,5 14,7 6,2 71,8 34,6 normal 250 33,6 15,2 5,3 81,4 34,6 normal Time shift between ACBP and ACSp was expectable. That was caused by a distance
between the catheter-tip manometer and the finger oximetric probe, and by changing velocity of pressure/volume wave in the arterial bed [[187],[188],[189]].

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 259
An AV Delay Optimization Using Atrial Contribution Indexes ACBP and ACSp
One can call the optimal AV delay a time period between atrial and ventricular impulses
which yields the greatest value of atrial contribution index. Great value of atrial contribution index generally means that sudden drop of the atrial contraction lead to the greatest decrease in the pulse amplitude of tracing used (BP or SpO2).
We used ACBP for assessment of optimal AV delays because the pressure tracing has been chosen as a reference. In a group of 47 patients, we found the optimal AV delay of 150 ms in 17 patients, 200 ms in 18 patients, and 250 ms in 12 patients, respectively.
In 14 individuals from 47 examined (29.8 %), the optimal AV delay assessed by ACBP differed from the optimal AV delay assessed using ACSp. In 5 patients with optimal AVD of 150 ms, the optimal AVD assessed using ACSp was 200 ms. In 9 subjects with optimal AVD 200 ms from ACBP, the optimal AVD from ACSp reached 150 ms in 6 patients, and 250 ms in 3 of them, respectively. Example of that situation obtained from patient no. 320 is displayed on Figure 10. In this subject, the optimal AVD assessed from ACBP was 150 ms (right graph). The optimal AVD estimated from ACSp was 200 ms (left graph). The difference between adjacent values in both ACBP and ACSp were less than 2% in all cases where the optimal AV delays derived from alternative tracings differed. In other words, the curves describing the relationship between AV delay and atrial contribution index were flat without clear maximum showing the optimal AV delay. This issue will be further demonstrated and discussed hereafter in this chapter.
Figure 10. A graph of relationship between AV delay and atrial contribution index derived from pulse amplitude of pulse oximetry signal (ACSp) is in left, similar graph for atrial contribution index derived from the pulse pressure (ACBP) is in right. Similarity of both graphs is apparent. Triangles represent values of basal measurements of ACSp and ACBP, rectangles represents mean values of ACSp and ACBP respectively.

Miroslav Mestan and Jiri Kvasnicka 260
In that group of 47 patients, the curve of relationship between AVD and ACBP has these shapes: rising shape in 12 patients, shape with peak in 30 subjects, and flat shape in only 5 patients, respectively. Flat shape of the curve made it impossible to distinguish which AV delay is optimum.
Evaluation of Reproducibility of the Atrial Contribution Index Derived from the Pulse Oximetry Signal Obtained within Tenths of Minutes
In order to evaluate the reproducibility of atrial contribution index derived from the pulse
oximetry signal, we performed Bland and Altman’s analysis of all paired values of atrial contribution indexes obtained from both series of basal measurements. We had enrolled total number of 94 patients since 1996 and we used all successful measurements of ACSp obtained at steady state without any hemodynamical intervention. A total number of 153 measurements were obtained for that analysis.
We also evaluated the time consumed for measurements of two series of basal ACSp measurements in our patients. Around year the 2000, complete semiautomatic version of SW has been introduced into the research. That SW allowed measuring ACSp pretty fast. Median time period needed for one patient was 13 minutes, range 8 min 20 sec (record minimum) up to 23 minutes.
Descriptive statistics of ACSp obtained in years 1996-2002 is given in Table 8. Data did not have normal distribution. Bland and Altman’s analysis is then given in Table 9. Lower counts of measurements in AV delays of 125, 175, and 225 ms is due to later introducing (since 1999) of semiautomatic SW with better AVD diagnostic to practice. Figures are acceptable when sensitivity of pulse oximetry is taken into consideration. Limits of agreement only slightly exceed 10 % in AV delays longer than 100 ms. It may be explained that measurements in AVD of 50 and 100 ms were often many times repeated. The hemodynamicaly compromising properties of these AV delays made it difficult to measure ACSp at once. Repetitions made the measurements of better quality in AV delays of 50 and 100 ms. On the other hand, in AV delays longer than 150 ms, most of measurements were accepted at once. Graphic expressions of reproducibility analyses are in Figure 11 and Figure 12.

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 261
Figure 11. Bland and Altman’s analyses of reproducibility of atrial contribution index derived from pulse amplitude of pulse oximetry signal (ACSp) made from all measurements performed from 1996 to 2002. In the right corner of every graph, value of particular AV delay and number of obtained measurement are indicated. Good reproducibility of ACSp is apparent because the solid line, which represents mean difference between two basal measurements (ACSpa and ACSpb), is near 0.

Miroslav Mestan and Jiri Kvasnicka 262
Figure 12. Bland and Altman’s analyses of reproducibility of atrial contribution index derived from pulse amplitude of pulse oximetry signal (ACSp) made from all measurements performed from 1996 to 2002. In the right corner of every graph, value of particular AV delay and number of obtained measurement are indicated. Good reproducibility of ACSp is apparent because the solid line, which represents mean difference between two basal measurements (ACSpa and ACSpb), is near 0.
Table 8. Descriptive statistics of all atrial contribution indexes derived form the pulse
oximetry signal, which were measured in 1996-2002. Distribution of data was not normal, median and interquartile range is provided.
AV delay (ms)
50 100 125 150 175 200 225 250
N of measurements
97 115 42 153 56 150 48 116
median ACSp (%)
10,4 23,2 29,9 29 30,7 30 28,3 26,8
1st quartil ACSp (%)
0,9 14,9 19,8 21 20,2 22,4 18,5 19,7
3rd quartil ACSp (%)
16,3 29,5 35,7 39,8 41,4 40,3 38,3 38,7
minimum ACSp (%)
-14,4
-3,3 5,8 -0,2 8,2 3,55 6,55 2,5
maximum ACSp (%)
45,5 50,6 51,4 63,6 72,7 80,4 68,2 81,4

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 263
Table 9. Bland and Altman’s analyses of reproducibility of the atrial contribution index from the pulse oximetry signal. Data were collected in 1996-2002
AV delay (ms) 50 100 125 150 175 200 225 250 number of subjects
97 115 42 153 56 150 48 116
mean difference (%)
-0,2 0,0 0,8 0,3 0,4 -0,5 -0,2 -0,9
SD of differences (%)
4,9 4,5 6,0 5,2 4,4 6,1 5,9 5,9
2SD (%) 9,8 9,0 12,0 10,4 8,8 12,2 11,8 11,8 mean - 2SD (%)
-10,0
-9,0
-11,2
-10,1
-8,4
-12,7
-12,0
-12,7
mean + 2SD (%)
9,6 9,0 12,8 10,7 9,2 11,7 11,6 10,9
Evaluation of Reproducibility of the Atrial Contribution Index Derived from the Pulse Oximetry Signal Obtained within 24 Hours
Design of a small study made in 2001 was planed with two repeated measurements at a
steady state with a time delay of 24 hours between them. We enrolled 22 out-patients irrespective of their age, gender and systolic function of the left ventricle. No hemodynamical intervention was used and long-term medication was not modified. All measurements were performed within morning hours.
In order to evaluate hemodynamic condition during measurements, body weight and blood pressure was evaluated. We used constant programmed basal rate in both days of measurement. Stability of body weight, systolic and diastolic blood pressure were evaluated by Wilcoxon’s test due to missing of normal distribution of data (see Table 10).
Table 10. Results of Wilcoxon’s test comparing body weight, systolic and diastolic blood
pressure with time delay of 24 hours. Analyses were made for the study evaluating 24-hours reproducibility of the atrial contribution index.
N=20 day 1 day 2 P body weight (kg) 77,5 ± 15,7 77,4 ± 15,6 0,722 systolic BP (mm Hg) 136 ± 18 133 ± 17 0,509 diastolic BP (mm Hg) 81 ± 10 78 ± 11 0,237
Acceptable results were yielded from 20 of total 22 patients. One female and one male
patient had numerous ectopic ventricular activity and these ventricular extrasystoles made the measurement impossible.
We obtained maximum mean value of the atrial contribution index in the first day (ACSpday1) and similarly, we have got another maximum index in the second day (ACSpday2).

Miroslav Mestan and Jiri Kvasnicka 264
We constructed regression graph from ACSpday1 and ACSpday2 (Figure 13). A strong linear relationship between both indexes by Pearson’s coefficient r=0.921 was obtained.
In each day of the study, a pair of basal ACSp measurement was obtained. Analysis of reproducibility of these paired values for day 1 and day 2 was performed. Results are tabulated in Table 11 and Table 12. Mean ACSp indexes were calculated for each day and the highest values in each day were chosen for further comparison (ACSpday1, ACSpday2). Mean difference between maximum mean ACSp from first and second day (ACSpday1-ACSpday2) was 2.1±7.9 %. Limit of agreement was 15.7 %. These results were slightly worse than the reproducibility of ACSp obtained within time interval of tenths of minutes but still remain clinically interesting and acceptable (Figure 14).
Figure 13. A graph displays regression analysis of mean atrial contribution indexes derived from pulse amplitude of pulse oximetry signal obtained first and second day of measurement (ACSpday1, ACSpday2) in a group of 20 patients. Only 1 value from 20 is outlier.
Figure 14. Bland and Altman’s analysis of reproducibility of atrial contribution index derived from pulse amplitude of pulse oximetry signal from 20 subjects who were repeatedly measured in 24 hours (ACSpday1, ACSpday2).

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 265
Table 11. Analysis of reproducibility of the atrial contribution index derived from the pulse amplitude of the pulse oximetry signal obtained in day 1. Differences were counted
from first and second series of basal ACSp measurements (ACSpday1a-ACSpday1b) AV delay (ms) 50 100 125 150 175 200 225 number of subjects 3 18 20 20 20 17 9 mean difference (%) 4,2 -0,4 2,3 0,0 1,1 -0,4 -4,3 SD of differences (%) 2,1 5,1 3,1 4,7 9,1 5,5 5,6 2SD (%) 4,2 10,2 6,2 9,4 18,2 11,0 11,2 mean - 2SD (%) 0,0 -
10,6 -
3,9 -
9,4 -
17,1 -
11,4 -15,5
mean + 2SD (%) 8,4 9,8 8,5 9,4 19,3 10,6 6,9
Table 12. Analysis of reproducibility of the atrial contribution index derived from the pulse amplitude of the pulse oximetry signal obtained in day 2. Differences were counted
from first and second series of basal ACSp measurements (ACSpday2a-ACSpday2b) AV delay (ms) 50 100 125 150 175 200 225 number of subjects 3 19 20 20 20 17 9 mean difference (%) -3,0 1,1 -
0,6 -0,2 0,7 1,2 -2,0
SD of differences (%) 5,2 4,2 4,3 4,5 3,4 5,8 5,2 2SD (%) 10,4 8,4 8,6 9,0 6,8 11,6 10,4 mean - 2SD (%) -
13,4 -
7,3 -
9,2 -9,2 -6,1 -
10,4 -
12,4 mean + 2SD (%) 7,4 9,5 8,0 8,8 7,5 12,8 8,4
Usefulness of Atrial Contribution Index (ACSp) for AV Delay Optimization We sought for an optimal AV delay within AV delays of 50, 100, 125, 150, 175, 200,
225, and 250 ms respectively. Several patients with preserved atrio-ventricular conduction did not allow measuring ACSp in AV delays of more than 200 ms. We yielded a total of 199 assessments of the optimal AV delay in a total number of 94 patients during years 1996-2002. Six estimations were omitted. One patient suffered from paroxysmal atrial fibrillation. Two patients did not breathe in the required way. One patient was excluded due to tremor. The last two patients could not be evaluated because of numerous ectopic ventricular activities.
When we described possible relationships between AVD and ACSp, we could arbitrarily define these four basic types of curve:
• “Curve with a peak” is curve with clearly pronounced peak showing the optimal AV
delay (Figure 15). • “Combined curve” shows type of dependency of atrial contribution index (ACSp) on
length of AV delay (AVD) in a patient, in whom prolongation of AVD from hemodynamicaly compromising values of 50 and 100 ms leads to rise in ACSp until some critical value is reached. Further prolongation of AVD does not lead to other

Miroslav Mestan and Jiri Kvasnicka 266
significant changes in ACSp. An optimal AVD seems to be one value within the range 150 to 225 ms. In some patients, next prolongation of AVD might lead to some decrease in ACSp (Figure 16).
• “Flat curve” has very similar values of ACSp for broad spectrum of AVD in question. The differences between ACSp are within limits of possible error of the method (Figure 17).
• “Upward curve” was a type of dependency of atrial contribution index (ACSp) on length of AV delay (AVD) in a patient, in whom the longest evaluated AVD (250 ms) gives the highest value of ACSp (Figure 18).
Figure 15. This is a graph of dependency of atrial contribution index (ACSp) on length of AV delay (AVD) in a patient, in whom one can clearly mark a particular value of AVD as optimal. In that case the optimal AVD is 225 ms. The type of dependency has been arbitrarily called “type with a peak”. This is the most valuable type of dependency for AV delay optimization.

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 267
Figure 16. This is a graph of dependency of atrial contribution index (ACSp) on length of AV delay (AVD) in a patient, in whom prolongation of AVD from hemodynamicaly compromising values of 50 and 100 ms leads to rise in ACSp until some critical value is reached. Further prolongation of AVD does not lead to other significant changes in ACSp. An optimal AVD seems to be one of value within range 150 to 225 ms. In some patients, next prolongation of AVD might lead to some decrease in ACSp. This most frequent type of dependency in our study group has been arbitrarily called “combined type”.
Figure 17. This is a graph of dependency of atrial contribution index (ACSp) on length of AV delay (AVD) in a patient, in whom it is not possible to say that some particular AVD is optimal. This type of dependency in our study group has been arbitrarily called “flat type”.

Miroslav Mestan and Jiri Kvasnicka 268
Figure 18. This is a graph of dependency of atrial contribution index (ACSp) on length of AV delay (AVD) in a patient, in whom the longest evaluated AVD (250 ms) gives the highest value of ACSp. This type of dependency in our study group has been arbitrarily called “upward curve”.
The total number of 193 assessments of relationship between AV delays and ACSp were further evaluated. The difference between number of assessments and number of patients is due to repeated measurements in some of them. From all mentioned 193 assessments, we found a combined curve or curve with a peak in 108 examinations so that it allowed us to assess the optimal AV delay’s length. The flat curve was registered in total of 47 measurements. That curve disallows assessment of the optimal AV delay. In such affected patients, we did not change nominal length of AV delay of 180 ms. The optimal AV delay of 250 ms was registered from the upward curve in 38 measurements. We never have measured AV delay longer than 250 ms. AV delays 100 ms and shorter were hemodynamicaly compromising in all 47 assessments. We decided not to examine these AV delays any more. An example is given in Figure 20.
The time gap between these repeated measurements mentioned above differs from 24 hours up to years. In 22 patients, we obtained repeated measurement with time interval more than 1 year to each of them. Examples are on Figure 19 and Figure 20. This stability of relationship between AVD and ACSp as far as the shape of the curve is concerned was new and surprising to us. Absolute values of ACSp varied because it is not possible to maintain completely the same hemodynamic situation in time and the method has its own error.

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 269
Figure 19. Three graphs of dependency of atrial contribution index on AV delay obtained in one subject of ours in time. The similarity of curves’ shape is apparent despite absolute values of index of atrial contribution change.

Miroslav Mestan and Jiri Kvasnicka 270
Figure 20. Three graphs of dependency of atrial contribution index on AV delay obtained in one subject of ours in time. The similarity of curves’ shape is apparent. In all three graphs one can see negative value of atrial contribution index at hemodynamicaly compromising AV delay of 50 ms.

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 271
Study on the Influence of Fluid and Diuretic Administration on the Index of Atrial Contribution
Previous echocardiographic studies imply that the preload reduction may enhance the
atrial contribution to the ventricular filling [[99],[159],[190]]. Notwithstanding the inaccuracies of the Doppler method, nitroglycerin induces a purely pharmacologic effect. On the contrary, diuretic causes loss of sodium and water without remarkable dilation of arteries – a condition that mimics real life. When we had the fast, fully noninvasive, and objective method, we decided to explore possible ACSp changes induced by acute hemodynamic interventions with fluid and diuretic [[191]].
Twenty-four out-patients were enrolled into the study. They all gave informed consent to the study, which was approved by the local ethics committee. The mean age was 60 ± 12 years (range 20 – 75 years). Ejection fraction of the left ventricle (EF) varied widely from 24 to 77 % (mean 53 ± 12 %). Detailed description of subjects including indications for cardiac pacing and long-term medication is given in Table 13.
We performed echocardiography in 2D-mode in all patients. In all patients, echocardiography excluded moderate or severe congenital or acquired valvular disease, shunts of the heart or the great vessels. Ejection fraction of less than 50% was considered as systolic dysfunction of the left ventricle. Left ventricular hypertrophy (LVH) was indicated if the interventricular septum or the posterior wall of the left ventricle exceeded 11 mm.
All patients were paced for different types of symptomatic bradycardia (Table 13). Two were treated for diabetes mellitus, five for coronary heart disease and eight for arterial hypertension. During the study, long-term medications (Table 13) were not changed and the activity sensor of the pulse generator was switched off.
In the study, the ACSp was estimated at the end of 3 periods: 1st – steady state period (refer to index steady), 2nd – post infusion state (refer to index infusion) and 3rd – post diuretic state (refer to index diuretic). The post infusion state was achieved by intravenous infusion of saline at 5 ml/kg of body weight over 30 minutes. The dose of 5 ml/kg of body weight was chosen to minimise the risk of inducing acute pulmonary oedema in patients with systolic dysfunction of the left ventricle (Table 13). Another reason was because the two heaviest patients weighed 100 and 102 kg. The volume of infusion was 500 ml. This required at least 25 min to be delivered into the peripheral vein. At the end of each period, the patients passed urine and the body weight (W), systolic (BPs) and diastolic (BPd) blood pressure were measured concurrently with the ACSp. After the second series of measurements (end of post infusion state), furosemide (1mg/kg body weight) was administered as an intravenous bolus. A loop diuretic was chosen for its natriuretic and negligible direct arteriodilating effect. Effects of loop diuretic are similar to various situations in real life where loss of sodium and water occurs e.g., sweating.
The ACSp was estimated at AVDs of 125, 150, 175, 200, 225 and 250 ms in all patients with intrinsic AV conduction longer than 250 ms. In all patients, the ACSp was measured for AV intervals from 125 to 200 ms. For further evaluation, optimal AV delay was used i.e. the delay, for which the ACSp was highest at the end of steady state.

Table 13. Patients included in the study with hemodynamic intervention with infusion of fluid and diuretic administration Patient No. Age Sex Pacing EF (%) AH LVH Diur BB CaB Other treatment S-E 1 70 M SSS 24 Yes Yes No Yes No ACEI V-O 2 69 M AV III 35 Yes Yes Yes No Yes - Val-O 3 70 M SSS 36 No Yes No No No - O-V 4 67 M AV II 45 No No No No No - V-R 5 63 M AV II 45 No No No No No propafenon Z-P 6 49 M SSS 45 Yes No Yes Yes No - P-H 7 73 F SSS 49 No No No No No - D-M 8 75 M SSS 51 No Yes No No No - B-V 9 43 M HCS 52 No No No No No propafenon T-J 10 70 F AV II 52 No No No Yes No - R-D 11 29 F SSS 52 No No No No No - Dol-M 12 58 F AV III 53 Yes Yes Yes Yes Yes - S-V 13 68 M SSS 53 No No No No Yes Digoxin R-V 14 44 F AV III 55 No No No No No midodrine, fludrocortison P-Z 15 39 M AV III 58 No No No No No - N-J 16 60 F SSS 68 No No No No No anti-epileptic agent F-Č 17 73 M SSS 55 Yes Yes Yes No No ACEI, amiodaron J-S 18 53 M AV III 64 No No No Yes No propafenon M-N 19 69 M SSS 55 Yes No Yes Yes No ACEI P-M 20 56 F AV III 72 No No No No No - J-V 21 54 F SSS 62 Yes No No Yes No - M-Z 22 62 M SSS 45 No No No Yes No ACEI J-K 23 59 M SSS 77 Yes No Yes Yes No - J-R 24 58 M SSS 69 No No No Ni No amiodaron
M – male, F – female, SSS – sick sinus syndrome, AV II – second-degree AV block, AV III – complete AV block, HCS – carotid sinus syndrome, EF – ejection fraction of the left ventricle, AH – presence of arterial hypertension in personal history, LVH – hypertrophy of the left ventricle. Long-term medication is indicated by: Diur-diuretic, BB – betablocker, CaB – calcium channel blocker, ACEI – angiotensin converting enzyme inhibitor.

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 273
A change of at least 30 % was chosen as a criterion of significant change in ACSp after administration of diuretic. This value correlates with studies dealing with similar issues of acute changes in the magnitude of atrial contribution following some hemodynamic intervention.
Since the distribution of the source data was not normal in the whole group of 24 patients, we used medians and interquartile ranges (1st quartile – 3rd quartile) as well as nonparametric statistical tests for the description of data. The changes in variables in the first group of 16 patients were evaluated using Wilcoxon’s test with Bonferoni’s correction for multiple comparisons to avoid false results. The changes in variables in the whole group of 24 subjects were validated by Wilcoxon’s test (Table 15). Due to the heterogeneity of the observed group (including patients with LVH, low EF and combinations of these, see Table 13), further testing had to be performed in order to assess if variations in results were due specifically to these disorders. Using Fisher’s exact test, the ACSp changes in all participants were examined with respect to present combinations of depressed function and/or hypertrophy of the left ventricle. Fluid infusion was skipped in the last eight patients. Statistical analysis by Mann-Whitney U-test was performed to find any impact of fluid infusion on changes in ACSp induced by administration of diuretic in groups with and without infusion (Table 16).
The study has several limitations. Only an indirect index of the atrial contribution to the systolic ventricular output (ACSp) was measured. For ethical reasons we could not measure parameters that could quantify the mean pressure in the left atrium (pulmonary capillary wedge pressure) and the cardiac output invasively. However, changes in blood pressure and cardiac output induced by diuretics have been well described in the past [[192],[193],[194],[195]]. The schedule of the study and the study population with chronotropic incompetence and with conduction disturbances did not allow us to measure special indexes of intrinsic sympathomimetic activity.
The changes in body weight, systolic and diastolic blood pressures and ACSp for the first 16 patients are shown in Table 14. When comparing findings at the end of the post infusion state with the steady state, there were significant increases in body weight and systolic blood pressure (for both P<0.010). The changes in diastolic blood pressure were small (P=0.080). There were only negligible changes in ACSp (P=0.897) after intravenous administration of fluids. This may be due to the small volume of fluid load given. None of our patients exhibited signs of the left ventricular failure during the study, indicating that their atria probably operated on the flat portion of the pressure-volume curve. In this case, a much larger volume load would be necessary to increase pressure inside the atria substantially to produce some decrease in ACSp [[83]]. Our results also showed that exclusion of the infusion from the study protocol did not affect the response to diuretic.
As the infusion of fluid did not lead to any significant changes in ACSp in the first 16 subjects, fluid administration was skipped in the last 8 patients. These 8 patients received diuretic immediately after the measurements of Wsteady, BPssteady, BPdsteady and ACSpsteady.

274 Miroslav Mestan and Jiri Kvasnicka
Table 14. Medians and interquartile ranges of body weight (W), systolic (BPs) and diastolic (BPd) blood pressures and atrial contribution index (ACSp) obtained in steady state, after administration of fluid and after injection of furosemide
in the first 16 subjects.
N=16 W (kg) BPs (mm Hg) BPd (mm Hg)
ACSp (%)
Steady state 79 (73.3 - 86.5) 135 (125 - 148) 80 (70 - 89) 27 (19.8 - 42.8) Post infusion
79.4 (73.3 - 86.9)1)
140 (130 - 160)1)
80 (70 - 90) 25.9 (20.2 - 42.4)
Post diuretic 77.8 (72.4 - 85.6)2),3)
130 (120 - 139)4)
70 (66 - 80) 38.1 (26.9 - 62.4)2),3)
1) P<0.010 post infusion state compared to steady state 2) P<0.001 post diuretic state compared to steady state 3) P<0.001 post diuretic state compared to post infusion state 4) P<0.005 post diuretic state compared to post infusion state.
After the diuretic, body weight (Wdiuretic) was significantly lower when compared to
Wsteady and Winfusion (for both P<0.001). The systolic blood pressure (BPsdiuretic) was decreased when compared with BPsinfusion (P<0.005) but there were no significant changes when compared to BPssteady (P=0.186). The diastolic blood pressure (BPddiuretic) showed an insignificant drop when compared to BPdsteady (P=0.085) and BPdinfusion (P=0.021). These changes were accompanied by a rise in ACSp (Table 14). The median of ACSpdiuretic was higher than ACSpsteady and ACSpinfusion (for both P<0.001). For example see Figure 21.
Figure 21. Example of an extreme decrease in pulse amplitude of the pulse oximetry signal (vertical arrow), induced by changing the pacing mode from DDI to VVI. Gray vertical arrow marks the loss of atrial activation on ECG. Fast hypohydration induced by furosemide led to a significant increase in atrial contribution index (in that case up to 91.2 %).

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 275
Medians (interquartile ranges) of measured parameters in all 24 patients are given in Table 15. Compared with the steady state, administration of the diuretic was followed by a decrease in W (P<0.001) and in BPd (P=0.041). The ACSp increased significantly (P<0.001, Figure 22). There was an insignificant drop in the BPs (P=0.134).
Possible relationships of ACSp reactions to administration of diuretic with combination EF and LVH were explored by Fisher’s exact test. The null hypothesis of no relation was not rejected (P=0.395). The increase in ACSp during dehydration was noted in all our patients with two exceptions (patient no. 14 and 24) regardless of presence of systolic dysfunction or hypertrophy of the left ventricle.
Figure 22. A graph displays changes in atrial contribution index (ACSp) at steady state, in subgroup of 16 subjects after saline infusion of 5 ml/kg of body weight, and in 2 hours after intravenous bolus of furosemide of a dose of 1 mg/kg of body weight. In majority of subjects ACSp increased after the administration of diuretic independently on fact whether the infusion was administered or not.
Table 15. Medians and interquartile ranges obtained in all 24 subjects are tabulated. Results of Wilcoxon’s test for body weight (W), systolic (BPs) and diastolic (BPd) blood pressures and atrial contribution index (ACSp) in steady state and after administration
of diuretic are in the last row.
N=24 Weight (kg) BPs (mm Hg) BPd (mm Hg) ACSp (%)
Steady state 78.6 (65.7-86.5)
130 (116-140)
80 (70-89)
30.4 (20.2-47.1)
Post diuretic 77 (64.4-85.6)
120 (120-134)
73 (66-80)
43.3 (30.6-80.9)
Wilcoxon's test P < 0.001 P = 0.134 P = 0.041 P <0.001
Differences in body weight, BPs, BPd, and ACSp between post diuretic state and steady
state are shown in Table 16. As P-values indicate, there were no deviations caused by infusion of fluid.

276 Miroslav Mestan and Jiri Kvasnicka
Table 16. Evaluation of changes induced by a diuretic in the group of patients who received intravenous fluid (N=16) and who did not (N=8). Means and standard
deviations of differences in body weight (W), systolic (BPs) and diastolic (BPd) blood pressures and the atrial contribution index (ACSp) obtained when post diuretic state
was compared to steady state are tabulated. Example Wsteady indicates the body weight in steady state; Wdiuretic indicates body weight after diuretic. P-values were obtained
from Mann-Whitney U-test
N=16 N=8 Wdiuretic-Wsteady (kg) -1.1±0.4 -1.4±0.5 P=0.322 BPsdiuretic-BPssteady (mm Hg) -4±9 -5±15 P=0.975 BPddiuretic-BPdsteady (mm Hg) -4±9 -2±5 P=0.463 ACSpdiuretic-ACSpsteady (%) 15.8±14.3 21.5±25.4 P=0.481
When measuring ACSpdiuretic, we could notice the following changes. The occurrence of
ectopic beats increased remarkably in three subjects. In one patient, an increase in resting heart rate emerged so that the last ACSp measurement had to be done with increased basal programmed rate of 90/min. In two patients, spontaneous AV conduction became faster and it was not possible to quantify ACSp in AV delays of 200 ms and longer. An increment in resting heart rate combined simultaneously with shortening of spontaneous AV conduction appeared in one subject. We believe that occurred due to instantaneously increased sympathetic activity after acting of diuretic.
Patient no. 14 suffered from neurally mediated syncope with vasodepressive and cardioinhibitory component. She was on long-term treatment with fludrocortison and midodrin to prevent further presyncopal episodes. Despite a decrease in body weight of 1 kg, the AC decreased from 21.1% in steady state to 17.7% in post diuretic state. This is compatible with the hypothesis that sympathetic activity plays an important role in the force of atrial contraction.
Conclusion
Development of the Method Quantifying Atrial Role for the Systolic Volume of the Left Ventricle, Its Feasibility and Reproducibility
A novel original method for estimation of the atrial contribution index to systolic volume
of the left ventricle in sequentially paced patients has been developed. In principle, the method is based on quantitative analysis of a beat-to-beat induced decrease in pulse amplitude of the pulse oximetry signal due to sudden drop of stimulus for the right atrium. The ventricular rate must be kept strictly constant while changing pacing mode. Resulting atrial contribution index (ACSp) is given as a percentage of the original pulse amplitude of pulse oximetry signal. Finally, we proposed a new method with design using a drop of atrial impulse by changing pacing mode from DDI to VVI. When that design is used, the risk of possible affection of results by frequency phenomena is minimized. In the first beat after

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 277
changing pacing mode, we need not be afraid from possible affection of pulse amplitude by ventriculo-atrial conduction.
The method is fast, cheap, observer-independent, and fully noninvasive. In the study comparing values of atrial contribution indexes derived from the pulse
pressure (ACBP) and from the pulse amplitude of pulse oximetry signal (ACSp), the difference of an average 4.7% for the benefit of ACBP was found. We consider such a systematic shift as clinically acceptable and it allows the use of completely noninvasive ACSp instead of ACBP yielded by invasive approach.
In a group of 47 subjects, following values of ACSp were found when examining at AV delay of 200 ms: mean 33.5%, median 34.6%, minimum 6.2%, and maximum 71.8%.
Results of measurements obtained from 94 consequently enrolled subjects (in some of them repeatedly) proven clinically acceptable reproducibility of the method. The lowest reproducibility was achieved in AV delay of 200 ms. Mean difference between two values of ACSp obtained shortly (in 5 to 10 minutes) after the first one was –0.5 ± 6.1 %. In a group of 20 subjects, mean difference between two mean values of ACSp obtained in a time interval of 24 hours was –2.1 ± 7.9 %. Reproducibility of ACSp in a time interval of 24 hours was then slightly worse than the one in a time interval of tenths of minutes. That still remained clinically acceptable for the noninvasive method.
Major limitations of the method are not numerous. It is impossible to quantify ACSp during any physical activity. Furthermore, one cannot use the method when a patient suffers from any tremor, when numerous ectopic electrical activities are present, and in clearly non-compliant patients.
Optimization of AV Delay by the Atrial Contribution Index ACSp The curve expressing relationship between length of atrioventricular conduction and
value of ACSp divides examined subjects into two groups. For the first group, the flat curve is characteristic when AV delay of wide range from 125 up to 250 ms offers similar atrial contribution to systolic volume of the left ventricle. In the second group, there is an apparent maximum value of ACSp, which allows determining of optimal paced AV interval at rest.
The method allows optimization of paced, not sensed, AV delay. At least, the method can quickly select a group of patients in whom searching for optimal AV delay is problematic or almost impossible, and save the time consumed by other current employed methods for AV delay optimization. These patients represented about 23% of our study group.
Novel discovery of unexpected stability of relationship between AVD and ACSp was surprising. That relationship remains intraindividually stable within a time period of years.
We did not find any clinic or echocardiographic parameter which could help to predict the shape of the curve showing the relationship between AV delays and ACSp.

278 Miroslav Mestan and Jiri Kvasnicka Variations in Atrial Contribution Index ACSp Caused by Acute Hemodynamic Changes Induced by Fluid and Diuretic Administration
The results show that administration of a diuretic decreases the body weight. The drop in
weight is accompanied by an increase in the atrial contribution index (and most likely also with the atrial contribution itself) and a less apparent decrease in blood pressure. In six of our patients, the magnitude of ACSp reached values of more than 80 %; i.e. after administration of furosemide 80 % or more of the blood that filled the ventricle was expelled into the ventricle by atrial contraction. The explanation seems to be an increase in the active participation of atria (more forceful contraction) in the physiological response to the short-lasting dehydration and, presumably, to a consequent drop in the cardiac output. Acceleration of spontaneous atrio-ventricular conduction and/or intrinsic resting heart rate observed in several individuals from the studied group suggests possible increased sympathetic activation after acting of diuretic.
Increase in ACSp was likely to be caused by increased contractility of the atrial myocardium, mediated by sympathetic activity. However, the schedule of the study and the study population with chronotropic incompetence and with conduction disturbances did not allow us to measure special indexes of intrinsic sympathomimetic activity.
We have also demonstrated that atrial contribution seems to increase during dehydration (due to diuretics or perhaps due to a dehydration of any type) to maintain cardiac output, regardless of underlying systolic function or pathology of the ventricular wall.
Acknowledgement The studies were supported by two grants of the Internal Grant Agency of the Ministry of
Health, Czech Republic, No. 3677-3/1996, and No. NA/5403-3, 1999. The studies were also supported by research project MZO 00179906. Paper on study examining influence of fluid, and diuretic on the atrial contribution index was published by Oxford University Press [191]].
References
[81] Gesell RA. Auricular systole and its relation to ventricular output. Am. J. Physiol. 1911;29:32-63.
[82] Yellin EL; Sonnenblick EH; Frater RWM. Dynamic determinants of left ventricular filling: an overview. Baan J, Arntzenius AC, Yellin EL. Cardiac dynamics. The Hague, Boston, London: Martinus Nijhoff Publishers bv, 1980: 145-58.
[83] Payne RM; Stone HL; Engelken EJ. Atrial function during volume loading. J. Appl. Physiol. 1971;31(3):326-31.
[84] Myreng Y; Smiseth OA; Risoe C. Left ventricular filling at elevated diastolic pressures: relationship between transmitral Doppler flow velocities and atrial contribution. Am. Heart J. 1990;119(3, Part 1):620-6.

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 279
[85] Cottini E; Giacone G; Cosentino M; Cirino A; Rando G; Vintaloro G. Evaluation of left ventricular diastolic function by pulmonary venous and mitral flow velocity patterns in endurance veteran athletes. Archives of Gerontology and Geriatrics. 1996;22(Supplement 1):179-86.
[86] Brockman SK. Dynamic function of atrial contraction in regulation of cardiac performance. Am. J. Physiol. 1963;204(4):597-603.
[87] Mitchell JH; Shapiro W. Atrial function and the hemodynamic consequences of atrial fibrillation in man. Am. J. Cardiol. 1969;23:556-67.
[88] Braunwald E; Frahm CJ. Studies on Starling's law of the heart. IV. Observations on the hemodynamic functions of the left atrium in man. Circulation. 1961;24:633-42.
[89] Little RC. Effect of atrial systole on ventricular pressure and closure of the A-V valves. Am. J. Physiol. 1951;166:289-95.
[90] Brockman SK. Mechanism of the movements of the atrioventricular valves. Am. J. Cardiol. 1966;17:682-90.
[91] Levy MN; Martin PJ. Chapter 21 - Autonomic neural control of cardiac function. Sperelakis N. Physiology and pathophysiology of the heart. 3rd ed. ed. Kluwer Academic Publishers; 1995. p. 413-30.
[92] Gesell RA. Cardiodynamics in heart block as affected by auricular systole, auricular fibrillation, and stimulation of the vagus nerve. Am. J. Physiol. 1916;40:267-313.
[93] Mitchell JH; Gilmore JP; Sarnoff SJ. The transport function of the atrium. Factors influencing the relation between mean left atrial pressure and left ventricular end diastolic pressure. Am. J. Cardiol. 1962;9:237-47.
[94] Daubert J-C; Ritter P; Mabo P; Druelles P. Chapter 3. Hemodynamic response to cardiac pacing in DDD mode. Barold SS, Mugica J. New perspectives in cardiac pacing. Mount Kisco, New York: Futura Publishing Co.; 1988. p. 27-44.
[95] Seino Y; Shimai S; Nagae Y; Ibuki C; Takano T; Tanaka S; Hayakawa H. Cardiodynamic and neurohormonal importance of atrial contribution in rate-responsive pacing. Am. J. Cardiol. 1993;72(1):36-40.
[96] Rahimtoola SH; Ehsani A; Sinno MZ; Loeb HS; Rosen KM; Gunnar RM. Left atrial transport function in myocardial infarction. Am. J. Med. 1975;59:686-93.
[97] von Bibra H; Wirtzfeld A; Hall R; Ulm K; Blömer H. Mitral valve closure and left ventricular filling time in patients with VDD pacemekers. Assessment of the onset of left ventricular systole and the end of diastole. Br. Heart J. 1986;55:355-63.
[98] Iwase M; Sotobata I; Yokota M; Takagi S; Jing HX; Kawai N; Hayashi H; Murase M. Evaluation by pulsed Doppler echocardiography of the atrial contribution to left ventricular filling in patients with DDD pacemakers. Am. J. Cardiol. 1986;58:104-9.
[99] Triulzi MO; Castini D; Ornaghi M; Vitolo E. Effects of preload reduction on mitral flow velocity pattern in normal subjects. Am. J. Cardiol. 1990;66:995-1001.
[100] Gessner M; Blazek G; Kainz W; Gruska M; Gaul G. Application of pulsed-Doppler tissue imaging in patients with dual chamber pacing: the importance of conduction time and AV delay on regional left ventricular wall dynamics. Pacing And Clinical Electrophysiology: PACE. 1998;21(11, Part 2):2273-9.

280 Miroslav Mestan and Jiri Kvasnicka
[101] Thomas L; Levett K; Boyd A; Leung DYC; Schiller NB; Ross DL. Changes in Regional Left Atrial Function with Aging: Evaluation by Doppler Tissue Imaging. European Journal of Echocardiography. 2003;4(2):92-100.
[102] Muntinga HJ; van den Berg F; Knol HR; Schuurman JJ; van der Wall EE. Quantification of the atrial contribution to diastolic filling during radionuclide angiography. Nucl. Med. Commun. 1997;18(7):642-7.
[103] Hartiala JJ; Mostbeck GH; Foster E; Fujita N; Dulce MC; Chazouilleres AF; Higgins CB. Velocity-encoded cine MRI in the evaluation of left ventricular diastolic function: Measurement of mitral valve and pulmonary vein flow velocities and flow volume across the mitral valve. Am. Heart J. 1993;125(4):1054-66.
[104] Hartiala JJ; Foster E; Fujita N; Mostbeck GH; Caputo GR; Fazio GP; Winslow T; Higgins CB. Evaluation of left atrial contribution to left ventricular filling in aortic stenosis by velocity-encoded cine MRI. Am. Heart J. 1994;127(3):593-600.
[105] Benchimol A; Duenas A; Liggett MS; Dimond EG. Contribution of atrial systole to the cardiac function at a fixed and a variable ventricular rate. Am. J. Cardiol. 1965;16:11-21.
[106] Karlöf I. Haemodynamic effect of atrial triggered versus fixed rate pacing at rest and during exercise in complete heart block. Acta Med. Scand. 1975;197:195-206.
[107] Nitsch J; Seiderer M; Büll U; Lüderitz B. Evaluation of left ventricular performance by radionuclide ventriculography in patients with atriovenricular versus ventricular demand pacemakers. Am. Heart J. 1984;107:906-11.
[108] Videen JS; Huang SK; Bazgan ID; Mechling E; Patton DD. Hemodynamic comparison of ventricular pacing, atrioventricular sequential pacing, and atrial synchronous ventricular pacing using radionuclide ventriculography . Am. J. Cardiol. 1986;57:1305-8.
[109] Samet P; Castillo C; Bernstein WH. Hemodynamic consequences of sequential atrioventricular pacing. Subjects with normal hearts. Am. J. Cardiol. 1968;21:207-12.
[110] Kruse I; Arnman K; Conradson T-B; Rydén L. A comparison of the acute and long-term hemodynamic effects of ventricular inhibited and atrial synchronous ventricular inhibited pacing. Circulation. 1982;65(5):846-55.
[111] Reiter MJ; Hindman MC. Hemodynamic effects of acute atrioventricular sequential pacing in patients with left ventricular dysfunction. Am. J. Cardiol. 1982;49:687-92.
[112] DiCarlo Jr. LA; Morady F; Krol RB; Baerman JM; de Buitleir M; Schork MA; Sereika SM; Schurig L. The hemodynamic effects of ventricular pacing with and without atrioventricular synchrony in patients with normal and diminished left ventricular function. Am. Heart J. 1987;114(4):746-52.
[113] Sigwart U; Grbic M; Goy JJ; Kappenberger L. Left atrial function in acute transient left ventricular ischemia produced during percutaneous transluminal coronary angioplasty of the left anterior descending coronary artery. Am. J. Cardiol. 1990;65(5):282-6.
[114] Carleton RA; Passovoy M; Graettinger JS. The importance of the contribution and timing of left atrial systole. Clin. Sci. (Colch) 1966;30:151-9.

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 281
[115] Kvasnička J; Tauchman M; Kovář D; Jandík J; Gajdošová I; Rejchrt P. Atrial contribution to ventricular ejection in sequentially paced patients. Physiol. Res. 1996;45:159-63.
[116] Mitchell JH; Gupta DN; Payne RM. Influence of atrial systole on effective ventricular stroke volume. Circulation Research. 1965;17:11-8.
[117] Stewart WJ; Dicola VC; Harthorne JW; Gillam LD; Weyman AE. Doppler ultrasound measurement of cardiac output in patients with physiologic pacemakers. Effects of left ventricular function and retrograde ventriculoatrial conduction. Am. J. Cardiol. 1984;54(3):308-12.
[118] Labovitz AJ; Williams GA; Redd RM; Kennedy HL. Noninvasive assessment of pacemaker hemodynamics by Doppler echocardiography: importance of left atrial size. J. Am. Coll. Cardiol. 1985;6(1):196-200.
[119] Eliakim M; Sapoznikov D; Weinman J. Assessment of the atrial contribution to cardiac performance by a noninvasive photoplethysmographic technique. Cardiology. 1973;58:7-13.
[120] Fagrell B; Lindvall K. Non-invasive beat-to-beat analysis of stroke volume and digital pulse volume in patients with complete heart block and artificial pacing. Acta Med. Scand. 1979;205:185-90.
[121] Eugene M; Lascault G; Frank R; Fontaine G; Grosgogeat Y; Teillac A. Assessment of the optimal atrio-ventricular delay in DDD paced patients by impedance plethysmography. Eur. Heart J. 1989;10(3):250-5.
[122] Bellot P. Bioimpedance in the pacemaker clinic. AACN Clinical Issues. 1999;10(3):414-8.
[123] Semrád B; Fišer B. Vztah mezi intervalem PR a velikostí tepového tlaku u nemocných s umělými srdečními stimulátory. Vnitr. Lek. 1973;19(1):35-40.
[124] Whinnett ZI; Davies JE; Willson K; Chow AW; Foale RA; Davies DW; Hughes AD; Francis DP; Mayet J. Determination of optimal atrioventricular delay for cardiac resynchronization therapy using acute non-invasive blood pressure. Europace. 2006;8(5):358-66.
[125] Ruskin J; McHale PA; Harley A; Greenfield Jr. JC. Pressure-flow studies in man: Effect of atrial systole on left ventricular function. J. Clin. Invest. 1970;49:472-8.
[126] Matsuda Y; Toma Y; Ogawa H; Matsuzaki M; Katayama K; Fujii T; Yoshino F; Moritani K; Kumada T; Kusukawa R. Importance of left atrial function in patients with myocardial infarction. Circulation. 1983;67(3):566-71.
[127] Matsuzaki M; Tamitani M; Toma Y; Ogawa H; Katayama K; Matsuda Y; Kusukawa R. Mechanism of augmented left atrial pump function in myocardial infarction and essential hypertension evaluated by left atrial pressure-dimension relation. Am. J. Cardiol. 1991;67:1121-6.
[128] Greenberg B; Chatterjee K; Parmley WW; Werner JA; Holly AN. The influence of left ventricular filling pressure on atrial contribution to cardiac output. Am. Heart J. 1979;98(6):742-51.
[129] Benchimol A; Ellis JG; Dimond EG. Hemodynamic consequences of atrial and ventricular pacing in patients with normal and abnormal hearts. Effect of exercise at a fixed atrial and ventricular rate. Am. J. Med. 1965;39:911-22.

282 Miroslav Mestan and Jiri Kvasnicka
[130] Dernellis JM; Stefanadis CI; Zacharoulis AA; Toutouzas PK. Left atrial mechanical adaptation to long-standing hemodynamic loads based on pressure-volume relations. Am. J. Cardiol. 1998;81:1138-43.
[131] Miyatake K; Okamoto M; Kinoshita N; Owa M; Nakasone I; Sakakibara H; Nimura Y. Augmentation of atrial contribution to left ventricular inflow with aging as assessed by intracardiac Doppler flowmetry. Am. J. Cardiol. 1984;53(4):586-9.
[132] Thomas L; Levett K; Boyd A; Leung DYC; Schiller NB; Ross DL. Compensatory changes in atrial volumes with normal aging: is atrial enlargement inevitable? J. Am. Coll. Cardiol. 2002;40(9):1630-5.
[133] Pearson AC; Janosik DL; Redd RM; Buckingham TA; Labovitz AJ; with technical assistance of Mrosek D. Hemodynamic benefit of atrioventricular synchrony: prediction from baseline Doppler-echocardiographic variables. J. Am. Coll. Cardiol. 1989;13(7):1613-21.
[134] Dernellis JM; Tsiamis E; Stefanadis C; Pitsavos C; Toutouzas P. Effects of postural changes on left atrial function in patients with hypertrophic cardiomyopathy. Am. Heart J. 1998;136(6):982-7.
[135] Skinner Jr. NS; Mitchell JH; Wallace AG; Sarnoff SJ. Hemodynamic effects of altering the timing of atrial systole. Am. J. Physiol. 1963;205(3):499-503.
[136] Ogawa S; Dreifus LS; Shenoy PN; Brockman SK; Berkovits BV. Hemodynamic consequences of atrioventricular and ventriculoatrial pacing. Pacing Clin. Electrophysiol. 1978;1:8-15.
[137] Mehta D; Gilmour S; Ward DE; Camm AJ. Optimal atrioventricular delay at rest and during exercise in patients with dual chamber pacemakers: a non-invasive assessment by continuous wave Doppler. Br. Heart J. 1989;61:161-6.
[138] Hettrick DA; Euler DE; Pagel PS; Musley SK; Warman EN; Ziegler PD; Mehra R. Atrial pacing lead location alters the effects of atrioventricular delay on atrial and ventricular hemodynamics. Pacing And Clinical Electrophysiology: PACE. 2002; 25(6):888-96.
[139] Daubert C; Ritter P; Mabo P; Varin C; Leclercq C. Chapter 10. AV delay optimization in DDD and DDDR pacing. Barold SS, Mugica J. New perspectives in cardiac pacing. Vol. 3. Mount Kisco, New York: Futura Publishing Co.; 1993. p. 259-87.
[140] Gold M; Leman R; Niazi I; Giudici M; Kim M; Yu Y; Arcot-Krishnamurthy S; Strakna J. Is nominal AV delay offset optimal for heart failure patients receiving cardiac resynchronization therapy? Europace Supplements. 2005;7(Supplement 1):168.
[141] Haskell RJ; French WJ. Physiological importance of different atrioventricular intervals to improved exercise performance in patients with dual chamber pacemakers. Br. Heart J. 1989;61:46-51.
[142] Janosik DL; Pearson AC; Buckingham TA; Labovitz AJ; Redd RM. The hemodynamic benefit of differential atrioventricular delay intervals for sensed and paced atrial events during physiologic pacing. J. Am. Coll. Cardiol. 1989;14(2):499-507.

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 283
[143] Ritter P; Padeletti L; Gillio Meina L; Gaggini G. Determination of the optimal atrioventricular delay in DDD pacing. Comparison between echo and peak endocardial acceleration measurements. Europace. 1999;1(2):126-30.
[144] Rydén L; Karlsson Ö; Kristensson B.-E. The importance of different atrioventricular intervals for exercise capacity. Pacing Clin. Electrophysiol. 1988;11:1051-62.
[145] Ishikawa T; Sugano T; Sumita S; Nakagawa T; Hanada K; Kosuge M; Kobayashi I; Kimura K; Tochikubo O; Usui T; Umemura S. Optimal atrioventricular delay setting determined by evoked QT interval in patients with implanted stimulus-T-driven DDDR pacemakers. Europace. 2001;3(1):46-51.
[146] Ishikawa T; Sugano T; Sumita S; Toda N; Kosuge M; Kobayashi I; Matsusita K; Ohkusu Y; Kimura K; Usui T; Umemura S. Optimal atrioventricular delay setting determined by QT sensor of implanted DDDR pacemaker. Pacing Clin. Electrophysiol. 2002;25(2):195-200.
[147] Porciani MC; Corbucci G; Fantini F; Musilli N; Sabini A; MA; Colella A; Pieragnoli P; Demarchi G; Padeletti L. A perspective on atrioventricular delay optimization in patients with a dual chamber pacemaker. Pacing Clin Electrophysiol 2004;27(3):333-8.
[148] Auricchio A; Stellbrink C; Sack S; Block M; Vogt Ju; Bakker P; Huth C; Schondube F; Wolfhard U; Bocker D. Long-term clinical effect of hemodynamically optimized cardiac resynchronization therapy in patients with heart failure and ventricular conduction delay. J. Am. Coll. Cardiol. 2002;39(12):2026-33.
[149] Auricchio A; Ding J; Spinelli JC; Kramer AP; Salo RW; Hoersch W; KenKnight BH; Klein HU. Cardiac resynchronization therapy restores optimal atrioventricular mechanical timing in heart failure patients with ventricular conduction delay. J. Am. Coll. Cardiol. 2002;39(7):1163-9.
[150] Whinnett ZI; Davies JE; Willson K; Manisty CH; Chow AW; Foale RA; Davies DW; Hughes AD; Mayet J; Francis DP. Haemodynamic effects of changes in atrioventricular and interventricular delay in cardiac resynchronisation therapy show a consistent pattern: analysis of shape, magnitude and relative importance of atrioventricular and interventricular delay. Heart. 2006;92(11):1628-34.
[151] Ritter P; Dib JC; Lelievre T. Quick determination of the optimal AV delay at rest in patients paced in DDD mode for complete AV block. (abstract). EUR. J.C.P.E. 1994;4:A163.
[152] Ishikawa T; Sumita S; Kimura K; Kikuchi M; Kosuge M; Kuji N; Endo T; Sugano T; Sigemasa T; Kobayashi et al. Prediction of optimal atrioventricular delay in patients with implanted DDD pacemakers. Pacing And Clinical Electrophysiology: PACE. 1999;22(9):1365-71.
[153] Evolution of pulse oximetry [Web Page]. Available at http://www.masimo.com/aboutmasimo/evolution.htm. (Accessed February 2007).
[154] Monitoring oxygen saturation with pulse oximetry [Web Page]. 2001; Available at http://www.nellcor.com/_Catalog/PDF/Edu/MON_F.a.00838v1 Clinical Mono Pul.pdf. (Accessed February 2007).
[155] Wukitsch MW; Petterson MT; Tobler DR; Pologe JA. Pulse oximetry: Analysis of theory, technology, and practice. J. Clin. Monit. 1988;4:290-301.

284 Miroslav Mestan and Jiri Kvasnicka
[156] Nellcor Education Web page [Web Page]. Available at http://www.nellcor.com/educ/index.aspx. (Accessed February 2007)
[157] Masimo SET Pulse Oximeter Bibliography [Web Page]. Available at http://www.masimo.com/cpub/ClinicalStudies_SET.htm. (Accessed February 2007)
[158] Bebout, DE, Mannheimer, PD. Effect of cold-induced peripheral vasoconstriction on pulse amplitude at various pulse oximeter sensor sites [Web Page]. 14 October 2002; Available at http://www.nellcor.com/_Catalog/PDF/Edu/ASA 2002 Poster.pdf. (Accessed February 2007).
[159] Choong CY; Herrmann HC; Weyman AE; Fifer MA. Preload dependence of Doppler-derived indexes of left ventricular diastolic function in humans. J. Am. Coll. Cardiol. 1987;10(4):800-8.
[160] Iwase M; Nagata K; Izawa H; Yokota M; Kamihara S; Inagaki H; Saito H. Age-related changes in left and right ventricular filling velocity profiles and their relationship in normal subjects. Am. Heart J. 1993;126(2):419-26.
[161] Ormiston JA; Shah PM; Tei C; Wong M. Size and motion of the mitral valve anulus in man. 1. A two-dimensional echocardiographic method and findings in normal subjects. Circulation. 1981;64:113-20.
[162] Voller H; Uhrig A; Spielberg C; von Ameln H; Schroder K; Bruggemann T; Schroder R. Acute alterations of pre- and afterload: are Doppler-derived diastolic filling patterns able to differentiate the loading condition? Int. J. Card. Imaging. 1993;9(4):231-40.
[163] Galderisi M; Benjamin EJ; Evans JC; D'Agostino RB; Fuller DL; Lehman B; Levy D. Impact of heart rate and PR interval on Doppler indexes of left ventricular diastolic filling in an elderly cohort (the Framingham Heart Study). Am. J. Cardiol. 1993;72(15):1183-7.
[164] Nishimura RA; Abel MD; Hatle LK; Tajik JA. Relation of pulmonary vein to mitral flow velocities by transesophageal Doppler echocardiography. Circulation. 1990;81(5):1488-97.
[165] Douchet MP; Quiring E; Vi-Fane R; Bronner F; Messier M; Pasco A; Chauvin M; Wihlm JM; Brechenmacher C. Optimizing the hemodynamic performance of the DDD pacemaker: impact of the atrioventricular delay on the pulmonary venous flow pattern. Pacing Clin. Electrophysiol. 1998;21(11 Pt 2):2261-8.
[166] Benchimol A; Li Y-B; Legler JF; Dimond EG. Rapidly repeated determinations of the cardiac output with the indicator-dilution technic. Am. J. Cardiol. 1964;790-7.
[167] Sowton E. Haemodynamic studies in patients with artificial pacemakers. Br. Heart J. 1964;26:737-45.
[168] Warner HR; Toronto AF. Regulation of cardiac output through stroke volume. Circ. Res. 1960;8:549-52.
[169] Sowton E. Artificial pacemaking and sinus rhythm. Br. Heart J. 1965;27:311-8. [170] Nishimura RA; Callahan MJ; Schaff HV; Ilstrup DM; Miller FA; Tajik JA.
Noninvasive measurement of cardiac output by continuous-wave Doppler echocardiography: initial experience and review of the literature. Mayo Clin. Proc. 1984;59(7):484-9.

A Novel Approach to Optimization of Paced AV Delay Using Atrial Contribution… 285
[171] Kiowski W; Randall OS; Steffens TG; Julius S. Reliability of echocardiography in assessing cardiac output. A comparative study with a dye dilution technique. Klin. Wochenschr. 1981;59(19):1115-20.
[172] Davies JN; Allen DR; Chant AD. Non-invasive Doppler-derived cardiac output: a validation study comparing this technique with thermodilution and Fick methods. Eur. J. Vasc. Surg. 1991;5(5):497-500.
[173] Braunschweig F; Bruns H-J; Ersgard D; Reites P; Linde C. Optimization of the AV-delay in cardiac resynchronization therapy using an implanted hemodynamic monitor. Europace. 2005;7(Supplement 1):212-3.
[174] Schuster AH; Nanda NC. Doppler echocardiography and cardiac pacing. Pacing Clin. Electrophysiol. 1982; 5:607-12.
[175] Feigenbaum H. Chapter 4. Hemodynamic information derived from echocardiography. Feigenbaum H. Echocardiography. 5th ed. ed. Philadelphia: Lea and Febiger; 1994. p. 181-238.
[176] Hamilton WF; Remington JW. The measurement of the stroke volume from the pressure pulse. Am. J. Physiol. 1947;148:14-24.
[177] Warner HR; Swan HJC; Connolly DC; Tompkins RG; Wood EH. Quantitation of beat-to-beat changes in stroke volume from the aortic pulse contour in man. J. Appl. Physiol. 1953;5:495-507.
[178] Bourgeois MJ; Gilbert BK; von Bernuth G; Wood EH. Continuous determination of beat-to-beat stroke volume from aortic pressure pulses in the dog. Circulation Research. 1976;39(1):15-24.
[179] Guier WH; Friesinger GC; Ross RS. Beat-by-beat stroke volume from aortic-pulse-pressure analysis. IEEE Trans. Biomed. Eng. 1974;BME-21(4):285-92.
[180] Bland JM; Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;i:307-10.
[181] Měšťan M; Kvasnička J; Rejchrt P. A new method of estimation of the optimal AV delay by using pulse oximetry in DDD paced patients. Acta Medica. (Hradec Králové) 1998;41(3):135-9.
[182] Katz AM. Chapter 15. Regulation of myocardial contractility (inotropy) and relaxation (lusitropy). Katz AM. Physiology of the heart. 3rd ed. ed. Philadelphia: Lippincott Williams and Wilkins; 2001. p. 368-97.
[183] Dvořák L, Ledvinka T, Sobotka M. Famulus 3.5. Příručka uživatele. 1. edition. Jihlava: Wimpy, 1992.
[184] Dvořák L, Ledvinka T, Sobotka M. Famulus 3.5. Referenční příručka. 1. edition. Jihlava: Wimpy, 1992.
[185] Dvořák L, Ledvinka T, Sobotka M. Famulus 3.5. Základní aplikační knihovny. 1. edition. Jihlava: Wimpy, 1992.
[186] Buckingham TA; Janosik DL; Pearson AC. Pacemaker hemodynamics: clinical implications. Prog. Cardiovasc. Dis. 1992;34(5):347-66.
[187] Westerhof N; Sipkema P; van den Bos GC; Elzinga G. Forward and backward waves in the arterial system. Cardiovasc. Res. 1972;6(6):648-56.
[188] Stergiopulos N; Westerhof BE; Westerhof N. Physical basis of pressure transfer from periphery to aorta: A model-based study. Am. J. Physiol. 1998;274:H1368-H1392.

286 Miroslav Mestan and Jiri Kvasnicka
[189] Asmar R. Chapter 2. Arterial pulse wave. Asmar R. Arterial stiffness and pulse wave velocity. Clinical applications. Éditions scientifiques et médicales Elsevier SAS ed. Paris: Elsevier; 1999. p. 17-23.
[190] Keren G; Milner M; Lindsay JJ; Goldstein S. Load dependence of left atrial and left ventricular filling dynamics by transthoracic and transesophageal Doppler echocardiography. Am. J. Card. Imaging. 1996;10(2):108-16.
[191] Mestan M; Babu A; Kvasnicka J. The influence of fluid and diuretic administration on the index of atrial contribution in sequentially paced patients. Europace. 2006;8(4):273-8.
[192] Schmieder RE; Messerli FH; deCarvalho JG; Husserl FE. Immediate hemodynamic response to furosemide in patients undergoing chronic hemodialysis. Am. J. Kidney Dis. 1987;9(1):55-9.
[193] Struyker-Boudier HA; Smits JF; Kleinjans JC; van Essen H. Hemodynamic actions of diuretic agents. Clin. Exp. Hypertens. [A] 1983;5(2):209-23.
[194] Franchi F; Malfanti PL; Scardi A; Pedenovi P; Bisi G; Barletta GA; Fabbri G. Hemodynamics in borderline hypertension: acute effect of furosemide. Circulation. 1984;71(6):331-40.
[195] Sica DA. Current concepts of pharmacotherapy in hypertension: thiazide-type diuretics: ongoing considerations on mechanism of action. J. Clin. Hypertens. (Greenwich) 2004;6(11):661-4.

In: Cardiac Arrythmia Research Advances ISBN: 978-1-60021-795-1 Editor: Lynn A. Vespry, pp. 287-326 © 2007 Nova Science Publishers, Inc.
Chapter XI
Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter
Tomás Muñoz
Abstract
Background: Atrial fibrillation (AF) is the most common sustained arrhythmia, and significant morbidity is associated with it: Palpitations, heart failure, angina, thromboembolic complications and tachycardia-induced cardiomyopathy. Some of these are also associated with atrial flutter (Afl). Therapy of these arrhythmias is based on prevention of thromboembolism and one of these two approaches: ventricular rate control or restoration of sinus rhythm. The decision to try to maintain sinus rhythm rather than controlling ventricular rate should be individual to each patient, based on analysis of the risk-benefit ratio for that patient.
External electrical cardioversion is a useful technique to restore sinus rhythm, but quite different rates of success have been reported (67-99%). This fact could be attributable to different patient selection, but also to differences in the technique of cardioversion. This work describes the author’s experience to recommend an effective protocol to perform electrical cardioversion of AF and Afl.
Patients and methods: At Txagorritxu Hospital, since 1998 to 2005, all patients that were considered candidates for elective electrical cardioversion of AF or Afl were admitted to an out-patient ward. The author himself performed all the procedures in the intensive care unit, and prospectively recorded the main variables involved: Age, Sex, Weight, Arrhythmia, Time after the onset of the arrhythmia, Heart disease, Left atrial size, Left Ventricular Ejection Fraction, Baseline vital signs, Anaesthetic drugs and doses, Induction and Recovery time, Secondary effects attributable to anaesthesia, Electrodes, Waveform, Electrode position, Restoration of sinus rhythm, Number of Shocks, Energy, Impedances, Antiarrhythmic and cardioactive drugs, and complications. Patients were discharged home after four hours.
Conditions associated with restoring sinus rhythm were identified. Several changes were sequentially introduced in the procedure, and thoroughly analysed, incorporating those which allowed better results.

Tomás Muñoz 288
Results: During this period, 373 procedures were performed (290 AF, 83 Afl). Seventy seven per cent were male, and 23% female, and their main characteristics were: Age 61.8 ± 10.6 years; Weight 81.7 ± 14.1 kg; Left atrial size 45.8 ± 5.3 mm; Left ventricular ejection fraction 56 ± 10,2 %; Time after the onset of the arrhythmia 90 (1-3600) days; 81% had heart disease (12% coronary, 17% valvular, 18% cardiomyopathy; 31% hypertensive); 96.5% were on pharmacologyc therapy (65 % amiodarone); 13% were shocked with metal paddles, 87% with adhesive pads; Dumped monophasic sinusoidal wave was employed in 33% of patients, and sinusoidal biphasic in 67%; Anterior-lateral (A-L) electrode position was first selected in 64% of patients, and anterior-posterior (A-P) in 36%, and 8% needed changing the electrode position; Sinus rhythm (SR) was restored in 91% of patients. Thromboembolic events were not observed. The main secondary effect was respiratory depression, without consequences, mainly associated with propofol-remifentanyl, a sedative strategy which allowed a rapid induction (110 sec) and recovery time (457 sec).
All patients with Afl were successfully cardioverted; Patients in AF were cardioverted to SR in 77% of cases using monophasic shocks, but in 94.21% using biphasic shocks (p= 0.0000, CI 8.31-26.09, OR 4,86). A-L electrode position allowed SR restored at first shock in 71.59% of patients, and A-P in 51.96% (p= 0.0057, CI 6.9 –33.9); With A-L position 1 (1-3) shock and 150 (100-700) joules of cumulated energy were needed, and with A-P position 1 (1-5) shock and 150 (150-900) joules (CI 0.26-0.84 for the number of shocks, and 57.39-172.13 for the cumulated energy). Impedance differences were not observed.
In a multivariate logistic regression model elaborated with the patients in AF, the waveform was the only variable that showed statistical significance.
Discussion: DC countershocks (including all the modifications of the technique) are maximally effective in cardioverting Afl. Given the variations of cardiac rate associated with this arrhythmia, early electrical cardioversion is recommended, ensuring adequate prevention of thromboembolic events; a curative ablation procedure may be considered when indicated.
Electrical cardioversion is also highly effective in patients with AF. None of the patients attributes (age, weight, sex, disease, ejection fraction, atrial size…) can be used to predict failure of the procedure. Best results in the author’s series were obtained using biphasic waveform through adhesive electrodes in A-L position.
Basics of Atrial Fibrillation Atrial fibrillation (AF) is the most common sustained arrhythmia[1]. More than 2.3
million patients in the United States and 4.5 million in the European Union have AF[2]. Its prevalence increases steadily with advancing age, as shown by different studies[3,4,5,6], rising rapidly after age 65. This arrhythmia is encountered in 4 out of 1000 people in the general population, 1 out of 25 in people over 60, and 1 out of 10 in people over 80.
AF can be found in persons without demonstrable underlying disease (lone atrial fibrillation), or associated with different clinical conditions (hyperthyroidism, acute myocardial infarction, hypertension, valvular heart disease…); Sometimes it is related to acute reversible causes (alcohol intake, electrocution…).
The most useful classification of AF is related to its presentation[1,7], so when this arrhythmia is discovered in a patient, we can designate it as:

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 289
• First detected episode: AF is diagnosed for the first time in that patient. • Recurrent AF: Two or more episodes have been detected in the same patient • Paroxysmal AF: AF terminates spontaneously • Persistent AF: AF is sustained beyond one week • Permanent AF: Restoration (and maintenance) of sinus rhythm is not considered
possible. The underlying electrophysiological mechanism of AF is reentry[8]. An important
advance in the understanding of this arrhythmia was due to Moe[9], who established the multiple wavelet hypothesis. Recent research support increasing evidence of ectopic focus initiation of AF[10], although the maintenance of the arrhythmia requires multiple wavefronts with different activation patterns[11]. When AF initiates, the depolarization wavefront (independently of its source) fragments into multiple daughter wavelets that wander randomly throughout the atria giving rise to new wavelets that collide with each other[11], causing disorganized atrial depolarisations without effective atrial contraction[12]. The ECG correlation of this event is the absence of the P wave, and the electrical activity of the atria is demonstrated as small irregular baseline undulations of variable amplitude and morphology, sometimes only detected by intraatrial leads. The lost of effective atrial contraction is responsible for some problems associated with this arrhythmia, as will be discussed later.
Atrial wavefronts arrive into the AV node, over which AV conduction occurs (in the absence of accessory pathways). The conductivity and refractoriness condition of the AV node influenced by the autonomic tone and cardioactive drugs, as well as the rate of arriving atrial impulses, are the determinants of the ventricular rate[13]. Some authors consider that the main mechanism determining ventricular response is concealed conduction[14]. Some impulses enter the AV node but do not conduct to the ventricle, causing a state of refractoriness which is encountered by new impulses. The consequence is a completely irregular ventricular response, and the ECG shows QRS complexes at an irregularly irregular rhythm. A rapid ventricular rate is responsible for most patient symptoms and complications associated with AF[15,16].
Although AF can be discovered in assymptomatic persons, this arrhythmia is associated with significant morbidity: Palpitations, heart failure, angina, syncope, thromboembolic complications or tachycardia-induced cardiomyopathy[1]. Palpitation is the most common complain of patients in AF, occurring in 59-77% of patients[15]. Fatigue and dyspnea are also frequent symptoms, reflecting inappropriate heart rates, or even different degrees of heart failure. Pathologic fibrotic changes in the atria that result from the arrhythmia[17] also let these patients prone to diastolic failure. The lost of the atrial contribution to diastolic filling may not be tolerated by patients affected by hypertrophic cardiomyopathy, and syncope, shock and sudden death have been reported[18,19]. A rapid ventricular rate can trigger ischemia in coronary patients. A persistently rapid ventricular response can result in cardiomyopathy, a reversible phenomenon that dilates the left ventricle depressing its ejection fraction[20,21,22], and indeed a potentially curable cause of heart failure.
Systemic embolism is probably the most dreadful complication of AF, especially when the brain is the affected organ. The lost of atrial contraction favours circulatory stasis and clot formation, mainly in the left atrial appendage. Also a hypercoagulable state appears to exist

Tomás Muñoz 290
in patients with AF[23,24]. This arrhythmia is a predictor for stroke[25]; As shown by different authors[26,27], the risk of stroke in patients with AF is 5 to 7 times greater than in controls in sinus rhythm. In other words, 20 to 25 percent of ischemic strokes are cardioembolic. Prevention of thromboembolic events is a major principle of the management of this arrhythmia, as will be discussed later.
Basics of Atrial Flutter Thought there exist different forms of atrial flutter, the common or typical form involves
a reentry circuit in the right atrium, around the tricuspid annulus, passing through an isthmus of heart muscle located between the inferior vena cava and the tricuspid valve (cavotricuspid isthmus)[28]. This circuit goes counterclockwise around itself at 240-320 beats per minute. The ECG shows a saw-tooth pattern of regular atrial activation (f waves) particularly visible in leads II, III, aVF, and V1.
The ventricular rate depends on the degree of block at the AV node level. Being 2:1 blocks the most common spontaneous degree of block, heart rates of 140-150 are often encountered in patients with atrial flutter. This rapid heart rate, analogous to that due to atrial fibrillation, can be associated with palpitations, angina, heart failure and, if sustained, tachymyocardiopathy. It is difficult to control the heart rate in some patients, and when negative chronotropic medications are prescribed, high degrees of AV block result, causing symptomatic bradychardia[29].
Another important issue is that effective contraction of the atria is lost, and contrary to previous recommendations, people with atrial flutter are at increased risk of embolic complications compared with the general population[30].
Management of Atrial Fibrillation and Atrial Flutter
The three major topics in the management of patients with AF are[1,13,31]: • Prevention of thromboembolic events • Restoration and maintenance of sinus rhythm • Ventricular rate control. As it has been exposed before, AF is a major factor associated with thromboembolic
events. An annual risk of stroke of 3-8% has been observed[32], although in these patients the prevalence of carotid atherosclerosis is not superior than in sinus rhythm patients[33]. For that reason, several studies have been done with the aim of discovering the main risk factors associated with stroke, and the benefits of different therapies[34,35,36,37,38,39]. Although evidence is not complete[40], the following are the most accepted recommendations[1, 41,42,43,44]:

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 291
• Main patient-related criteria for stroke are Congestive heart failure, Hypertension, Age > 75 , Diabetes and previous Stroke (acronym CHADS2, corresponding one point for each factor but previous Stroke which points two[45]). Thromboembolic risk increases progressively with CHADS2 score. Also, Mitral valve stenosis and prosthetic heart valve must be considered high risk factors.
• Less validated risk factors are female gender, coronary artery disease, moderately depressed left ventricular ejection fraction or 65 to 74 years of age.
• Patients with CHADS2 score >2 or more than one risk factor should receive oral anticoagulation. Patients with only one risk factor may be treated with low dose aspirin or coumarines. Young patients with lone AF without any risk factor should not receive oral anticoagulation.
• Oral anticoagulation should target an International Normalized Ratio (INR) of 2 to 3 (3 to 3.5 in patients with prosthetic heart valves, or who have sustained embolic events during treatment with low intensity anticoagulation).
• Combining oral anticoagulation and aspirin has not shown any benefit. Oral anticoagulation therapy is superior to clopidogrel plus aspirin[46].
• Electrical or pharmacological cardioversion of AF of unknown duration or duration greater than 48 hours needs effective oral anticoagulation for 3 weeks before and 4 weeks after the procedure.
• Anticoagulation prior to cardioversion is not needed in patients with AF of less than 48 hours duration.
• A transesophageal echocardiography (TEE) allows performing cardioversion in patients with AF of more than 48 hours duration if evidence against left atrial thrombus formation is obtained[47,48,49,50,51,52,53]. In these patients anticoagulation should be immediately started with unfractionated or low molecular weight heparin concurrently with a vitamin-K antagonist. Oral anticoagulation should be given for 4 weeks after the procedure although some authors withdraw it after one week if another TEE rules out cardiac thrombosis[54].
The initial management strategy of patients with AF – rate or rhythm control - is still
subject of controversy[55]. When rhythm control strategy is chosen, sinus rhythm is restored performing pharmacological or electrical cardioversion. If cardioversion is unsuccessful, rate control approach should be used. AF recurs in many patients, so repeated cardioversions and antiarrhythmic drugs are often required. In selected patients, ablative procedures may be considered[56,57,58,59]. When rate control approach is chosen, AF is accepted as the definite rhythm, and the ventricular response is controlled with medication. Each strategy has its own problems. Ventricular rate control can be difficult in some patients, and symptoms may persist; most patients will need anticoagulation for life. Rhythm control can fail, and AF recurrences can be badly tolerated. These patients can also be exposed to heart failure and thromboembolic complications; if antiarrhythmic drugs are prescribed, a risk of proarrhythmia and sudden death exists.
Several randomised trials have compared both strategies, and the acronyms PIAF[60], STAF[61], RACE[62], HOT CAFÉ[63] and principally AFFIRM[64] are well known by the medical community. Although neither approach was encountered inherently better than the

Tomás Muñoz 292
other, a trend towards higher mortality in the rhythm control strategy was seen, and this conclusion was also suggested by a meta-analysis[65] and a Cochrane review[66].
It is the author’s opinion that it would be oversimplistic to conclude that rate control should be the better choice for all patients. When sinus rhythm is maintained, outcomes and quality of life improve, as is shown in the subgroup analysis of the trials mentioned[67,68,69] and several other studies[70,71,72]. The main complication in the AFFIRM Study was an excess of stroke in the rhythm control group, due to a lack of anticoagulation during AF recurrences. The population selected for this study has also been subject of controversy, because predominantly elderly patients at high risk for recurrences and embolic complications were enrolled[73]. Perhaps the most important lesson derived from this trial is being cautious in stopping anticoagulation[74]. The decision to try to maintain sinus rhythm rather than controlling ventricular rate should be individual to each patient, based on analysis of the risk-benefit ratio for that patient.
Which patients finally do benefit from rhythm control strategy? Those who remain in sinus rhythm. So, how can we identify them? Are antiarrhythmic drugs safe and effective in maintaining sinus rhythm in patients cardioverted from AF? These questions are not completely answered yet, so the author will express his own interpretation of evidence based on previous research.
Having so many things in common with AF, several aspects of the management of atrial flutter are essentially the same, including antiembolic prophylaxis. Electrical cardioversion is highly effective in terminating episodes of this arrhythmia, which can also be terminated by atrial overdrive pacing[75]. As recurrences are common, drugs to control the ventricular rate and antiarrhythmic medications are often needed. Ablative procedures offer another treatment option, and the best results are obtained in typical isthmus-dependent atrial flutter[76,77,78]. A thorough discussion about the different subtypes of atrial flutter and their particularities in mapping and ablation is beyond the scope of this work.
Approach to the Patient with Atrial Fibrillation The diagnosis of AF, which requires ECG recording, should be followed by a complete
evaluation of the patient[1,31,79] including at least: • History and physical examination, Cardiovascular disease, Chronology of the
arrhythmia, Clinical tolerance, Precipitating causes, and Previous episodes and its treatment.
• Twelve leads ECG. • Chest radiography. Cardiovascular and pulmonary pathology. • Transthoracic echocardiogram. AF associated with cardiopathy, left atrial size, left
ventricular function. • Blood and Analysis: Cell count, coagulation, renal, hepatic and thyroid function. If AF with a rapid ventricular rate results in acute cardiovascular decompensation
(hypotension, angina, acute pulmonary edema…), immediate electrical cardioversion should

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 293
be attempted[1]. If AF is well tolerated by the patient, the decision to cardiovert will be largely based on the complete evaluation of that patient. The benefits of restoration of sinus rhythm must be weighed against the likelihood of successful cardioversion and long term maintenance of sinus rhythm. Prevention of embolic events should always be a priority in the management of the patient, and the previously described recommendations should be followed.
If AF is secondary to a reversible cause (anaemia, pulmonary infection, thyrotoxicosis, pericarditis…), cardioversion should be postponed until the precipitating cause will be treated and controlled. Meanwhile, rate control drugs and oral anticoagulation are started.
Patients with a first episode of AF should be given the opportunity to undergo one cardioversion procedure[80]. For patients with AF of less than 48 hours duration, it is our hospital practice to intend cardioversion immediately. Patients are informed about and offered both electrical and pharmacological cardioversion. Electrical cardioversion is our preferred choice in patients with at least 6 hours of fasting; this approach avoids the risk of proarrhytmia, is highly effective and allows a prompt discharge home. Antiarrhythmic drugs are administered to patients with a full stomach, or to those who select this option (or prefer to wait for spontaneous conversion). If antiarrhythmic medication is not effective, the patient is offered electrical cardioversion before 48 hours since the onset of the arrhytmia had passed to avoid the need of anticoagulation.
Several drugs can be used to restore sinus rhythm: • “Classic” drugs such as Quinidine[81] and Procainamide are not considered a first-
line therapy due to their proarrhytmic potential and pharmacokinetic disadvantages[1,82].
• Propafenone (600 mg) or Flecainide (300 mg) in a single oral loading dose[83,84] are often administered to young patients without structural heart disease in our Emergency Room, where efficacy and tolerance can be assessed. The most feared complication of these drugs is the occurrence of fast atrial tachycardias with 1:1 atrio-ventricular conduction[85,86,87]. To avoid this complication, a beta-blocker or a nonhydropyridine calcium channel antagonist is given before administering the class Ic agent[1]. Self-administration of Propafenone or Flecainide has also been proven safe and useful in outpatients with paroxysmal symptomatic AF, the so called “pill-in-the-pocket” approach[88].
• Ibutilide and Dofetilide are antiarrhythmic agents with proven efficacy in restoring sinus rhythm in patients with AF[89,90,91,92]. New drugs like Pilsicainide[93] seem promising. But since they are not commercialised in his country, the author has no experience with them.
• Neither Lidocaine[94] nor Sotalol[1] are helpful for this indication. • Amiodarone is a class III antiarrhythmic drug which have proven useful not only in
terminating AF, but also in enhancing electrical cardioversion and preventing recurrences[95,96]. Therefore, it is commonly used in our hospital although important side effects are of concern. This drug will be discussed thoroughly later.

Tomás Muñoz 294
Electrical cardioversion is performed under a strict protocol (which will be described in detail later), as first-line therapy or as a rescue treatment when medication fails. As evidence about pre and post-cardioversion needs of anticoagulation in with acute onset AF is lacking[97,98], it is our practice to start anticoagulation in patients whom a high probability of recurrences is expected. Patients cardioverted at first shock are discharged home without antiarrhythmic medication. When immediate recurrences of AF are observed, 300 mg amiodarone are infused, and a new DC-shock is given. When effective, these patients are discharged home with oral amiodarone and oral anticoagulation. Since there is no difference in the long-term maintenance of sinus rhythm between patients with and without immediate recurrences, we think that this approach is justified, as other authors advocate[99].
When a new episode of atrial fibrillation is encountered in a patient who has remained in sinus rhythm for a significant period of time (more than 6 – 12 months), whether or not another elective cardioversion is indicated depends on the characteristics of that patient. We are in favour of a second procedure in:
• Patients with lone AF. • Patients without antiarrhythmic medication. • Recurrence of AF after withdrawal of antiarrhythmic medication. • This is the patient preference. We are reluctant to attempt electrical cardioversion more than twice in the same patient.
An exception is done in the following cases: • AF with unacceptable symptoms which are not ameliorated by rate control. We have
encountered this problem in patients with hypertrophic cardiomyopathy. • AF triggered by a correctable cause, which has not been controlled yet. • Relapse of AF after a long period in sinus rhythm (more than 18 – 24 months). All these patients receive antithrombotic prophylaxis with antivitamine-K agents at least
for 3 weeks before and 4 weeks after the procedure and most of them are antiarrhythmic agents also. Selection of antiarrhythmic medication is based on the characteristics of the patient (age, heart disease, comorbilities…)[100]. Young patients without structural heart disease are given Propafenone or Flecainide; Coronary patients are given Amiodarone or Sotalol; Patients with low left ventricular ejection fraction are given Amiodarone. If undesirable effects attributable to Amiodarone are observed, an alternative drug (if possible) is chosen, usually Sotalol. Drugs to ensure ventricular rate control are also prescribed to these patients (Digoxine, Beta-blocker or Calcium antagonist) when necessary.
As recent studies have demonstrated, inflammation, oxidative stress and remodelling are implicated in the pathophysiology of AF[101,102,103,104,105]. Clinical trials with Angiotensin-Converting-Enzime (ACE) inhibitors[106], Angiotensin-Receptor-Blocking (ARBs) agents[107,108], Espironolactone[109], Statins[110,111] or even vitamin-C[101] have found reduction in AF relapses. Omega-3 fatty acids are objects of active research[112]. ACE inhibitors may improve acute success of electrical cardioversion[113], and Losartan may reduce new-onset AF[114]. A recently published meta-analysis concludes that an overall

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 295
effect of 18% risk reduction in new-onset AF can be attributed to ACE-inhibitors or ARBs[115]. Among these non-antiarrhythmic drugs, ACE-inhibitors are the agents most commonly prescribed by our group.
In spite of our efforts, many patients are going to develop persistent AF. In a study published one decade ago, only 10% of patients once cardioverted remained in sinus rhythm four years later[116]. The Canadian Registry of Atrial Fibrillation has reported a probability of progression to chronic AF of 8.6% by one year and 24.7% by 5 years[117]. More optimistic researchers consider that it is possible to prevent or markedly reduce atrial fibrillation recurrences in more than 60% of patients[13]. Selected cases can benefit from ablative[118] or surgical procedures[119,120,121,122]. Anyway, it makes no sense to keep on performing electrical cardioversions and administering antiarrhythmic drug therapy to patients who have relatively short periods of sinus rhythm between relapses of AF[1]. When persistent AF is established, rate control and antiembolic treatment should be warranted.
Patients with atrial flutter can be managed with the same approach. When frequent relapses occur, ablative therapies are a better choice than antiarrhythmic drugs.
Basics of Electrical Cardioversion First experiences with electricity in circulatory physiology are attributed to Peter
Abildgaard in 1775, who used electricity to induce and revert cardiac arrest in animals[123,124]. The first successful defibrillation was performed by Beck in 1947[125], who administered alternating current directly to the heart of a patient. In 1956, Zoll described external shocks[126]. But it is not until 1962, due to Lown's works[127], when electrical cardioversion turns into a real therapeutic option to treat cardiac arrhythmias.
Reentry is the electrophysiological basis of numerous arrhythmias, including AF and atrial flutter[123]. Electrical cardioversion, delivering energy in the form of direct current (DC shock), causes myocardial cells to depolarise. It is important to avoid electrical stimulation during the vulnerable phase of the cardiac cycle (60 to 80 milliseconds before to 20 to 30 milliseconds after the apex of the T-wave) so R-wave synchronization is mandatory. If a sufficient mass (critical mass) of heart cells have been depolarised, the reentry wavefront encounters these cells in refractory period and are blocked[128]. This causes an asystolia phase, after which the automatic heart cells initiate a new impulse. Ideally, sinus node cells initiate the normal depolarisation sequence, which is transmitted along the cardiac conduction system, and normal sinus rhythm is restored[129,130,131].
The following are important considerations when performing external electrical cardioversion:
• There is not a quantity of energy specific to a particular arrhythmia. A critical mass
of myocardial cells have to be depolarised to interrupt the reentrant wavefront[132]. This circuit involves a larger amount of tissue in some arrhythmias than in others (larger in AF than in atrial flutter), so different levels of energy are recommended[133].

Tomás Muñoz 296
• An adequate current density must reach the myocardial tissue thought thoracic structures, so waveform, electrode size and position, patient complexion, respiratory phase as well as several other factors affecting cardioversion success[134].
• The arrhythmia wavefronts collide with the heart tissue in the refractory period after being depolarised by the shock, and are blocked. This means that an asystole period ensues, which can be specially prolonged when multiple cardiodepressant drugs have been administered. Symptomatic bradyarrhythmia may also develop, and patients with previous disorders of conduction are particularly at risk.
• Not only the sinus node but any automatic focus in the heart can initiate the sequence of depolarisation, and sometimes new wavefronts are developed which restart the arrhythmia.
• Electrical cardioversion allows termination of a certain sequence of cardiac activation at that moment of time, and has no effect upon the circumstances or factors that trigger the arrhythmia. It is not wise to perform multiple electrical cardioversions to a patient who is unable to maintain sinus rhythm for a reasonable time.
Basic Operation of Defibrillators Although the first defibrillations were carried out using alternating current produced by
huge transformers, it was soon evident that it was detrimental to the myocardium (as well as to other thoracic tissues). As a result of this, direct current (DC) devices came into use in the second half of the 20th century.
Basically, a defibrillator consist of a bank of capacitors (fast-discharging current storage devices), a main switch and a set of electrodes, which are applied to the patient's thorax. The capacitors can be charged from batteries (something essential for portable systems) or the electric grid. Almost all modern manual systems include an ECG recorder with QRS complex detection (the highest amplitude wave), enabling the synchronisation of the discharge and the electrical systole when the switch is pressed, and the possibility of performing cardioversions.
This basic device charges electricity in its capacitors, which are formed by two conductive surfaces (plates) separated by an insulating layer (dielectric). The capacitance (the energy stored, measured in microfarads) of those capacitors depends on the voltage and the area of the plates. When the discharge switch is pressed, a current is applied to the patient. This electric current (measured in Amperes) in the myocardium is the real defibrillating agent; therefore considering the factors which oppose it –that is to say, the electrical resistance measured in Ohms- is crucial[135,136,137]. This electrical resistance depends on the size, the material and position of the electrodes, the type of conductor gel, the pressure exerted on the thorax, and fundamentally on the patient’s thorax characteristics[138], hence the widely used term "thoracic impedance".
Making a comparison between electricity and blood circulation is often useful for physicians to better understand these concepts[135]: Then, the capacitance can be considered the equivalent of the preload; the voltage (difference of electrical potential) of the vascular

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 297
pressures (difference between mean artery pressure and central venous pressure, for instance); the flow of electric charge (electric current or amperage) similar to the cardiac output; the thoracic impedance to the vascular resistances.
Under the above-mentioned conditions, the defibrillator is charged with a particular preload, which determines a certain pressure difference (voltage) between the pair of electrodes applied to the patient; the patient's thorax resists the flow of electricity (impedance); by pressing the switch, a current (amperage) travels between the electrodes, flowing through the myocardium and achieving defibrillation[139]. The relationship between current (I), voltage (V) and resistance (R) is described by Ohm's law: V = I*R. Therefore, in the case of a patient with high impedance, a higher voltage level will be required to achieve the same current through the myocardium[123].
Since defibrillators do not allow directly choosing the amperage, but the energy, the relationship between these concepts will be shown. As mentioned above, when the main switch of the defibrillator is pressed, a short-lasting current starts to flow. In that short period of time, it is possible to construct curves representing the instantaneous values of amperage or voltage, the product of which is Power (measured in Watts). The integral of that Power curve over time (or, for the sake of simplicity, Power divided by Time) gives the Energy (measured in Joules), which is the adjustable parameter via the defibrillator controls[123].
Current(amps)
Time (milliseconds)
Figure 1.

Tomás Muñoz 298
Voltage (volts)
Time (milliseconds)
Figure 2.
Power (watts)
Energy(joules)
Time (milliseconds)
Figure 3.
It is important to emphasize that it is the amperes which defibrillate. The relationship between amperes and joules depends on impedance and time. An energy of 2 J can thus match with: a current of 2 amperes flowing trough a resistance of 1Ωfor 1 second; a current of 1A through a resistance of 1Ωfor 2 seconds; a current of 1A through a resistance of 2Ωfor 1 second[136]. According to this, defibrillating a patient with high impedance (that is to say, achieving enough amperes through the myocardium) means selecting a higher energy level, increasing the voltage or extending the duration of the shock. These concepts have influenced the development of the defibrillator[137].
Back to the basic defibrillator described above, and which is solely made up of the capacitor (C), the switch and the output electrodes, when a shock is delivered (against the impedance of the patient, R), it can be observed that the curve of electrical current shows a sharp exponential, with a high current peak (exponential waveform). When there was

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 299
evidence that this high current peak was detrimental to the myocardium, an induction coil was added to the circuit[123], which resulted in a softer curve, called monophasic truncated exponential waveform or monophasic damped sine waveform.
c RCurrent(amps)
Time (milliseconds)
Figure 4 .
c R
inductance
Current(amps)
Time (milliseconds)
Figure 5.
It is worth observing the effect of the impedance on the form of the current curve. An increase in the impedance reduces the maximum amperage (with the result that successful defibrillation cannot be achieved using the same energy level), and the form of the curve varies accordingly. One should notice that the monophasic damped sine waveform delivered using low impedance, presents a morphology similar to that of biphasic waveforms[123], which will be commented on later.

Tomás Muñoz 300
c R= 25ΩCurrent(amps)
Time (milliseconds)
Figure 6.
c R= 75ΩCurrent(amps)
Time (milliseconds)
Figure 7 .
Some defibrillators keep the same morphology in a wide range of impedance values, according to the resistance of the spiral inductor. When the amperage curve does not oscillate under the axis line, it is called critically damped sine waveform (Edmark's and Pantridge's waveform); when the curve has a negative a component and oscillates under the axis line, it is called underdamped sine waveform (Gurvich's or Lown's waveform)[123]. This last waveform turned out to be most effective in defibrillation as well as in cardioversion, being thus the most widely used in the devices of the past four decades.
The damped sine waveform requires the use of large capacitors and inductors, too huge to be fitted in implantable devices[140]. In addition, current peaks generated by underdamped discharges were to be avoided in these systems. It had also been proved that the final phase of the critically damped waveforms was profibrillatory[141,142], and as a result of it, new

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 301
devices implementing a cut of this phase were designed, enabling an immediate fall to zero of the current. This trapezoidal waveform called monophasic truncated exponential waveform was more effective than the previously used waveforms.
Current(amps)
Time (milliseconds)
Figure 8.
Since the truncated exponential waveform (without the low current final phase) and the underdamped sine waveform (with oscillations under the axis line) improved the effectiveness of the defibrillation, it was researched how to combine both. This led to the design of new devices, which enabled the flow of current in one direction (phase 1), and after a period of time, reversed it (phase 2): the result is the biphasic truncated exponential waveform[135,136,137].
Current(amps)
Time (milliseconds)
Figure 9.

Tomás Muñoz 302
This type of waveform has proved to be superior to the former ones both in tests and day-to-day clinics, by achieving defibrillation or cardioversion with the use of less energy[133]. The moment when the polarity is reversed is different for every device. Not only does the use of biphasic waveforms in high impedance situations reduce the high current peak, but it extends the wavelength as well[135,136]. Some manufacturers modify the duration of the phases in order to adapt the discharge to different impedance values; This feature receives the name of biphasic exponential waveform with impedance compensation.
100 Ω100 J
Current(amps)
Time (milliseconds)
Figure 10.
40 Ω100 J
Current(amps)
Time (milliseconds)
Figure 11.
On the contrary, others have gone for a different concept in the design of biphasic waveforms, trying to keep the same waveform morphology in a wide range of thoracic impedances. The aim consists in reducing the initial current peak (associated with myocardial

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 303
damage), keeping a nearly constant current flow during phase 1[137]. This is achieved by using digitally controlled resistors, which increase or reduce the electrical resistance as required to compensate patient's low or high impedance. The duration of phases 1 and 2 is preset in 6 and 4 milliseconds. The resulting morphology gives name to this type of waveform, called rectilinear biphasic waveform.
6 4
Current(amps)
Time (milliseconds)
Figure 12.
Different research works draw contradictory conclusions about which biphasic waveform is superior[143,144,145,146]. Designing the optimum adaptation to the patient's impedance, even adding a third phase (triphasic waveform) are current research fields in the design of the defibrillators of the future[147].
Our Experience Since July 1998 to December 2005, at Txagorritxu Hospital, all elective electrical
cardioversions of AF and atrial flutter were performed by the author himself. During this time, different techniques were employed, with different rates of success. All variables involved in the procedure were prospectively recorded, in order to generate a data base that allowed successive analyses to identify which factors were associated with better results. The following description of our experience is presented.
Elective Cardioversion Protocol After being considered candidates for electrical cardioversion by their cardiologist,
patients were transferred to our hospital and given an appointment. Current recommendations of antithrombotic prophylaxis were strictly followed. Antiarrhythmic drugs and any other cardiovascular medication were left to the referring cardiologist preferences.

Tomás Muñoz 304
Patients were admitted to an outpatient ward, with at least 8 hours of fasting. In this Unit, cardiac rate, temperature and arterial pressure were recorded, and the stability of the patient confirmed. An ECG was obtained, to demonstrate the persistence of the arrhythmia. A peripheral venous catheter was inserted, and a blood sample obtained to confirm that analytic parameters were correct for the procedure, with utmost attention to Potassium and Coagulation (INR > 2). Written consent was always obtained after full explanation of the procedure, possible outcomes and complications.
Patients were transferred to the Intensive Care Unit for the procedure. Supplemental oxygen (50%) was provided with a Venturi mask, and oxygen saturation monitored by pulse-oximetry. Blood pressure was monitored non-invasively. Three different ECG leads were continuously monitored. Implantable antiarrhythmia devices and pacemakers were reprogrammed to avoid interference with the procedure (VVI 40 per minute, therapies disconnected). All the equipment necessary for resuscitation was immediately available (suction, bag-valve mask, oropharyngeal airways, laryngoscopes, endotracheal tubes, ventilator, venous catheters, transvenous and transthoracic pacemaker, fluoroscopy, medications...). Hairy chests were shaved to reduce impedance. The procedure was assisted by a registered critical care nurse (medications and monitoring) and the staff intensivist responsible for the patient (airway, arrhythmia recognition and defibrillation). Student nurses and residents were also allowed to participate, for educational purposes.
Once correct function of monitoring and equipment had been confirmed, the anaesthetic drug was administered by slow infusion in one minute for each drug: we have used Etomidate (0,15 mg.kg-1 immediately after Midazolam 1 mg), Propofol alone (1 mg.kg-1) and Propofol plus Remifentanil (0,5 mcg.kg-1). Adequate lost of consciousness was determined by cessation of response to verbal commands and tactile stimulation. If necessary, a second sedative dose was given. Vital signs were continuously monitored and recorded.
Different defibrillators have been used for the procedure: Physio-Control Lifepak 10, Hewlett-Packard CodeMaster 100, Agilent Smart Biphasic. Synchronized DC shocks were administered through hand-held electrode paddles coated with conductive paste or adhesive disposable electrodes placed in apex-anterior or posterior-anterior position. Electrode placement onto implantable devices was always avoided. When using a monophasic defibrillator, the energy level selected for the first shock was 200 Joules (J) for AF. If this first shock was ineffective, higher energies were delivered in the second (300 J) or third (360 J) shock. When using a biphasic defibrillator, energies selected for successive shocks were 150 to 200 J. Before 2001, a maximum of three shocks were delivered, but since that date five shocks were allowed, changing the electrode position for the latest two. Independently of the waveform used, we always started with 50 J in patients with atrial flutter.
After the shocks, if necessary, bag mask ventilation was provided. Volume was administered in cases of hypotension, and a few patients needed transient transcutaneous pacing. Amiodarone was infused to patients with immediate recurrences, before delivering more shocks. Movement, myoclonus, pain, and any other adverse effects were also recorded. Pacemakers and implantable defibrillators were checked and reprogrammed to optimise the new rhythm. A twelve leads ECG was obtained.
Patients were monitored in the Intensive Care Unit 15 minutes after full recovery of consciousness, then they were admitted again to the outpatient ward. Oral paracetamol was

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 305
given and Sulphadiacyn ointment applied onto the skin exposed to the electrical shock. They were allowed to ambulate after the first hour, and had lunch after the second. They were specifically asked about recall. If no problem was detected, patients were discharged home with written instructions. All the procedures were completed in less than four hours (10:00 am to 14:00 pm).
Results Sequential analyses of the results of the cardioversion protocols applied have been made,
and the interested reader can refer to the referenced published material[148,149,150,151]. Only the most important features are highlighted here.
Between June-1998 and December-2005, 373 elective electrical cardioversion procedures were performed in our Intensive Care Unit, 290 (78%) for AF and 83 (22%) for atrial flutter. Two hundred and eighty six (77%) were male, and 87 (23%) female. Main characteristics of this population were:
• Age: 61,8 ± 10,6 years (range 15 – 84) • Weight: 81,7 ± 14,1 Kilograms (48 – 140) • Left atrial size: 45,8 ± 5,3 mm (28 – 63) • Left ventricular ejection fraction: 56 ± 10,2 % (13 – 80) • Days in AF or atrial flutter: 151,5 ± 296, 4 (range 1 – 3600, median 90) • Basal cardiac rate: 84,4 ± 21,9 beats per minute (36 – 161) • Basal medium blood pressure: 109 ± 15, 9 mmHg (72 – 162) Three hundred and two patients (81%) had structural heart disease: 45 ischemic, 63
valvular, 66 cardiomyopathy, 116 hypertensive, and 39 cor pulmonale. Only 71 patients (19%) had no basal cardiopathy. Most of then (360 patients, 96.5%) were taken cardiovascular medication: 33 digoxin, 242 (65%) amiodarone, 100 a betablocker, 48 a calcium channel antagonist, 30 an antiarrhythmic-Ic, and 103 an ACE inhibitor or ARB. Half of this patients were taken two or more of this drugs. Only 13 patients (3.5%) were not treated with any cardiovascular medication.
Four different anaesthetic protocols were followed: 25 patients (7%) received etomidate, 25 (7%) propofol, 203 (54%) propofol plus remifentanil, and 120 (32%) propofol-lipuro plus remifentanil. A rapid induction (110 ± 31 seconds) and recovery time (457 ± 153 seconds) were obtained with these drugs. Four patients, all of them having received etomidate, presented myoclonic movements. Nine percent of patients who received propofol referred local pain at infusion, 28 patients (14%) when the drug was administered in the conventional lipid emulsion and 8 (7%) when lipuro was added, but this difference did not reach statistical significance (NS). Twelve patients sedated without opiate (24%) moved when being shocked, and 15 (4.6%) when remifentanil was also administered (NS). Only one patient remembered being shocked, and this patient did not received opiate. Two patients (4%) in the non-opiate group needed bag-mask ventilation, and 173 (53 %) in the sedative plus opiate group (p < 0,0001). All of them recovered promptly.

Tomás Muñoz 306
Five patients needed fluid administration to recover from hypotension and bradycardia, but this complication was attributed to the previous hemodynamic situation. Two patients needed transient transcutaneous pacing, and one of them, with advanced heart block, implantation of a definite pacemaker. All but these two patients could be discharged home after the cardioversion. None of our patients presented any embolic complication.
Four different cardioversion techniques were employed, attending to the electrode position (anterior-lateral or anterior-posterior), electrode type (metal paddles or adhesive disposable electrodes) and waveform (damped sinusoidal monophasic or truncated sinusoidal biphasic): Monophasic DC shocks through metal paddle electrodes in anterior-lateral (A-L) position were administered to 50 patients (13%); Monophasic DC shocks through adhesive disposable electrodes in A-L position were administered to 75 patients (20%); Biphasic DC shocks through adhesive disposable electrodes in A-L position were administered to 113 patients (30%); Biphasic DC shocks through adhesive disposable electrodes in anterior-posterior (A-P) position were administered to 135 patients (37%).
Sinus rhythm was restored in 339 patients (91%); All patients in atrial flutter were successfully cardioverted, independently of the technique employed. Patients in AF were cardioverted to SR in 77% of cases using monophasic shocks, but in 94.21% using biphasic shocks (p < 0.0001, CI 8.31-26.09, OR 4,86). A-L electrode position allowed SR being restored at first shock in 71.59 % of patients, and A-P in 51.96 % ( p= 0.0057, CI 6.9 –33.9); When A-L position was selected, one (1-3) shock and 150 (100-700) Joules of cumulated energy were needed, and when A-P position was selected one (1-5) shock and 150 (150-900) Joules (CI 0.26-0.84 for the number of shocks, and 57.39-172.13 for the cumulated energy) were necessary. Seven patients first assigned to the A-P electrode position could not be cardioverted with this position, but sinus rhythm was restored when another shock was delivered in A-L position. Current intensities employed were 21,7 ± 7,7 Amperes, and impedances measured were 73,4 ± 16,8 Ohms. Impedance differences between A-L and A-P electrode positions were not observed.
None of the patients attributes analysed (age, weight, sex, heart disease, left ventricular ejection fraction, left atrial size…) was associated with the result of the cardioversion. A trend towards a facilitation of sinus rhythm restoration in patients with AF was observed when the cardioversion procedure was performed during the first week of evolution of the arrhythmia (90% of patients cardioverted at first shock, p = 0.059). The contrary was observed when the cardioversion was performed beyond three months (55 % of patients cardioverted at first shock, p = 0.063).
None of the medications prescribed was associated with the result of the cardioversion, but Amiodarone was useful when immediate recurrences developed; we saw this event in 9 patients, and after infusing 300 mg Amiodarone in 10 minutes, a new shock was delivered, and sinus rhythm restored in 8 cases. Seven of them were still in sinus rhythm six months later.
To determine which variables were associated with the restoration of normal sinus rhythm to patients in chronic AF, all the variables recorded were included in a multivariate logistic regression model. Only the biphasic waveform kept statistical significance.
The utility of the biphasic waveform is best shown calculating the number needed to treat (NNT). Sinus rhythm was restored in 77 cases with monophasic shocks, and in 179 with

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 307
biphasic shocks; Electrical cardioversion failed in 23 patients with monophasic shocks, and in 11 with biphasic shocks. Then the absolute risk reduction is 17,21 % (CI 8,32 – 26,1), and the NNT 6 (3,8 – 12).
Our Recommendations Strict adherence to guidelines[1] is our first and most important recommendation. As
several aspects are not completely defined or local differences may be relevant, our own cardioversion protocol is proposed, and its most important features discussed. Since AF and atrial flutter are so common, we have tried to made things as simple as possible; not every patient can be managed in a tertiary hospital by an expert electrophysiologist. Radically different opinions can be found, so it is the reader interested in developing a cardioversion program who should make his own decision.
Selection of Patients for Cardioversion When AF or atrial flutter are triggered by a correctable cause, this should be treated and
controlled before attempting cardioversion. Atrial flutter response to electrical cardioversion is excellent, so this treatment should be
applied soon. If flutter relapses, electrophysiologic mapping and ablation should be intended. If a curative procedure is not possible or fails, cardioversion and antiarrhythmic medication can be tried. When frequent relapses occur, a rate control strategy should be applied. It is easier to keep the ventricular rate controlled in AF than in atrial flutter.
Almost every patient with a first episode of AF should be given the opportunity to undergo one electrical cardioversion, and more opportunities can be offered to patients with lone AF, including antiarrhythmic drugs prescription. Patients with short periods of sinus rhythm between relapses of AF should be treated with a rate control strategy. Patient with marked unfavourable features to keep sinus rhythm (long time in AF, large left atrial size, advanced age, structural heart disease…) should be managed with the rate control strategy, and electrical cardioversion offered only if symptoms are unacceptable. Nevertheless, the clinical predictive value of these risk factors for difficulty in maintaining sinus rhythm is low, and even the AFFIRM investigators consider that they should not be used to justify withholding rhythm control efforts in patients who may benefit from sinus rhythm[152].
Selected very symptomatic and difficult to manage patients are candidates for ablative procedures, and should be transferred to a experienced electrophysiologist.
Timing of Electrical Cardioversion Electrical cardioversion should be intended as soon as possible, because AF begets
AF[123]. Unstable patients should undergo cardioversion without delay. The decision to cardiovert AF lasting less than 48 hours should be taken soon, because after this period,

Tomás Muñoz 308
antiembolic prophylaxis is mandatory. Electrical cardioversion in patients with AF lasting more than 48 hours (or of unknown duration) should await effective oral anticoagulation for 3 weeks, unless a TEE rules out intracavitary thrombosis.
Antiembolic Treatment As we have remarked before, strict adherence to guidelines is of paramount importance.
Recent research highlights the reluctance of physicians to prescribe oral anticoagulation[153]. Electrical cardioversion of AF of unknown duration or duration greater than 48 hours needs effective oral anticoagulation (INR > 2) for 3 weeks before and 4 weeks after the procedure. The TEE approach can be used to hasten the cardioversion. It is advisable to prolong the anticoagulation period in high risk patients (based on the CHADS2 score) to warrant protection in case of arrhythmia recurrence.
Defibrillator and Waveform Biphasic waveform was the only variable in our study associated with a better result
when cardioverting patients in AF. Atrial flutter response to cardioversion was excellent, independently of the defibrillator and waveform utilized. Most authors [154, 155, 156, 157, 158, 159] coincide in reporting the superiority of biphasic waveforms. Which biphasic waveform is better, sinusoidal truncated or rectilinear, has not yet been established[160]. It is the author’s opinion that all elective cardioversions in patients with AF should be done with a biphasic defibrillator.
Electrode Type, Size and Position The placement of defibrillation electrodes on the thorax determines the transthoracic
current pathway for external defibrillation. The most important features to consider are impedance reduction, lessening of myocardial (and chest wall) damage while ensuring adequate delivery of energy (density of current) to the heart and simplicity of application.
As the diameter of the electrodes increases, the impedance decreases[123], but when very large paddles are used, defibrillation effectiveness falls, as much of the current is not going through the heart. Larger electrodes also cause less myocardial necrosis[161]. The optimal electrode size proposed by most authorities is about 12 cm[123].
Metal paddles coated with conductive paste are the classical interface to defibrillation, and several authors have found reduced transthoracic impedance with them[123,162]. These electrodes are optimal when immediate DC shocks are needed. Application of metal paddles directly onto the patient’s chest results in very high impedance and important skin burns[163], so application of conductive gel is mandatory. The conductive properties of some commercially available gels are suboptimal[164]; Gels used for echocardiography are very poor conductors of electricity and should not be used for cardioversion.

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 309
Disposable self-adhesive electrode pads provide several advantages in the elective cardioversion setting: Reduction in the personal involved in the procedure, reduction of skin burn, and with most current defibrillators immediate transthoracic pacing. In our series, adequate impedances have been measured with these electrodes, making sure that they were correctly placed onto hairless skin[165]; Hirsute chests were always shaved.
Although several authors recommend placing the electrodes in A-P position for cardioverting AF[166,167], recent research using biphasic waveforms do not support this idea[168,169,170]. A-A position allowed restoration of sinus rhythm in our patients using less energy and less number of shocks. This electrode position is well known by the medical community because it is commonly taught at the CPR courses[171,172]. For that reasons, we recommend A-A electrode position as first choice but in patients with implantable devices; We always avoid delivering a DC shock directly onto this devices, and routinely check them after the procedure. If the initial electrode position is not successful, the electrode pads are changed to the alternative one.
Energy Selected We start with 50 Joules when cardioverting atrial flutter, independently of the waveform
applied[173]. If this first shock is not effective, a second shock of 100 J is delivered. Higher energies are needed to cardiovert AF, because it is necessary to depolarise more
cardiac mass to interrupt the multiple atrial wavefronts. If a monophasic defibrillator is employed, 200 to 360 J are often necessary. Using a biphasic defibrillator, as we recommend, allows to select energies in the range of 150 to 200 J[174], although higher[175] and lower[176] energies have been proposed by other authors. In our experience, sinus rhythm was restored at first 150 J biphasic shock in more than 70 % of patients (employing the A-A electrode position), so this is the energy level that we recommend for the first shock. It is important to consider that the higher the energies the greater probability of skin burn[161], heart damage[177] and atrial stunning[178].
Antiarrhythmic Medication Several antiarrhythmic drugs have been essayed to enhance the results of the electrical
cardioversion, and to help keeping sinus rhythm: Propafenone, Flecainide, Calcium Channel Antagonists, Sotalol, Amiodarone… Inhomogeneous results have been published with all of them, and undesirable effects are of concern.
We do not routinely prescribe antiarrhythmic drugs. We try to avoid them in patients without structural heart disease with a first episode of AF and if the arrhythmia relapses, Propafenone or Flecainide are given and a new electrical cardioversion planned.
In patients with coronary disease, Sotalol is commonly prescribed. Beta-blockers or Calcium channel antagonist are used as rate control drugs in patients with different cardiopathies. Although some authors have found a beneficial effect in reducing AF

Tomás Muñoz 310
recurrences with this drugs[99,179,180], different conclusions have also been published[181].
Amiodarone is the antiarrhythmic agent most often prescribed in our hospital, because of its superior efficacy[182,183,184] and its relatively favourable side-effects profile[185]. This drug can also be used in patients with depressed systolic function[1]. Bradycardia, hypotension, QT prolongation and even acute hepatotoxicity have been reported with intravenous use of Amiodarone[186,187], but the more important undesirable effects are present with its chronic use: Corneal deposits leading to "halo-vision", blue-grey discoloration or hypersensitisation of the skin to sunlight, both hypothyroidism and hyperthyroidism, gastric reflux, liver toxicity with elevated liver enzymes, and pulmonary fibrosis. Due to its long half-life (weeks), the side effects of this drug often take weeks or months to develop, so they must be systematically assessed. Thyroid hormones and liver enzymes should be frequently monitored.
When first prescribed, oral Amiodarone is kept for 4 to 6 weeks[188], tapering to the lowest dose (200 mg three times a week). If AF relapses after stopping the drug, Amiodarone is reintroduced. Non-symptomatic thyroid dysfunction is the most common undesirable effect encountered in our patients, and it is our practice to stop the drug immediately. We do not prolong treatment with this drug for more than 6 months, and if AF relapses, an alternative antiarrhythmic agent is given. It is our believe that a rate control strategy is a better option for most patients than Amiodarone for life. Alternative Class – III agents are under development[189,190].
Sedative and Analgesic Medication The ideal anaesthetic approach for electrical cardioversion should warrant both a rapid
loss of consciousness and a rapid recovery, maintaining respiratory and hemodynamic stability[191]. Several drugs have been administered for this purpose: diazepam, thiopentone, propofol, etomidate, midazolam, and methohexital. Although electrical cardioversion is a painful procedure[192], adding opiates is not a general practice. Some studies comparing different dosages and combinations of these drugs have been published, with quite different conclusions[192, 193,194,195,196,197,198,199,200,201,202].
We have used two different sedative approaches: Slight sedation with a low dose of propofol or etomidate, and deep anaesthesia with propofol plus remifentanil. Both techniques allowed a rapid induction and recovery time, and the need of bag-valve-mask ventilation for a few seconds or minutes when deep analgosedation is used was the main difference. While some authors regard this as an important complication, we believe that administering deep anaesthesia is worthwhile. Recall is inexistent with this approach, and we are able to administer repeated DC shocks and to change the electrode position. There are not movement interferences and the interpretation of the ECG is facilitated. More over, a slight sedation approach is not absolutely free from airway complications. Advanced airway management skills are mandatory for any medical team performing electrical cardioversions.
Though in the majority of papers on electrical cardioversion the sedative approach is not described, the sedative protocol used in some studies have been judged so inadequately by

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 311
some anaesthesiologists, that they have set a formal complaint, considering that the anaesthetic cover should not be left to a cardiologist[203]. This opinion is not shared by all the medical community[204]. In the era of cost-containment, reducing the personal in charge of the procedure has been judged as an interesting option[205], so even nurse-led elective cardioversion protocols have been developed[206]. The possibility of performing DC cardioversion as an ambulatory procedure has also been remarked[207,208]. Our opinion is that it does not matter who performs the cardioversion, the really important thing is that several skills and knowledge are necessary. Airway management and ventilation, arrhythmia recognition, management of antiarrhythmic and sedative drugs, basic programming of pacemakers and implantable defibrillators, and advanced cardiac life support leadership experience.
Alternative Techniques of Electrical Cardioversion Higher energies have been employed in patients with AF refractory to conventional
monophasic shocks. Some authors report favourable outcomes sychronizing two defibrillators to deliver 720 J monophasic shocks[209]. Patients with high transthoracic impedance may benefit from this technique, although given the superior efficacy of the biphasic waveform, we prefer (and have obtained better results) using biphasic DC shocks.
Intracardiac cardioversion has proven useful in restoring sinus rhythm in a wide range of patients[210,211]. Transthoracic impedance is not yet a problem, and very low energies can be successfully employed. Atrial pacing can also be attempted during this technique[212]. Transoesopagic cardioversion[213] also enables application of low energies. Due to the more invasiveness and complexity of this internal techniques, they should be reserved for selected, very symptomatic patients, refractory to external biphasic shocks.
References
[1] ACC/AHA/ESC 2006 Guidelines for the Management of Patients With Atrial Fibrillation—Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines. Circulation. 2006;114:700-752.
[2] Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285:2370 –5.
[3] Kannel W, Abbott R, Savage D et al. Epidemiologic features of chronic atrial fibrillation: The Framingham study. N. Engl. J. Med. 1982, 306: 1018-22.
[4] Furberg CD, Psaty BM, Manolio TA, Gardin JM, Smith VE, Rautaharju PM. Prevalence of atrial fibrillation in elderly subjets (the Cardiovascular Health Study). Am. J. Cardiol. 1994; 74: 236-41.

Tomás Muñoz 312
[5] Krahn AD, Manfreda J, Tate RB, Mathweson FA, Cuddy TE. The natural history of atrial fibrillation: incidence, risk factors and prognosis in the Manitoba Follow-up Study. Am. J. Med. 1995; 98: 476-84.
[6] Chugh SS, Blackster JL et al. Epidemiology and Natural History of Atrial Fibrillation: Clinical Implications. J. Am. Coll. Cardiol. 2001; 37: 371-8.
[7] Lévy S. Classification system of atrial fibrillation. Curr. Opin. Cardiol. 2000; 15: 54-7.
[8] Garrey WE. The nature of fibrillary contraction of the heart: its relation to tissue mass and form. Am. J. Physiol. 1914;33:397–414.
[9] Moe GK, Abildskov JA. Atrial fibrillation as a self-sustaining arrhythmia independent of focal discharge. Am. Heart J. 1959;58:59–70.
[10] Nattel S. New ideas about atrial fibrillation 50 years on. Nature. 2002; 415: 219-26. [11] Konings KTS, Kirchhof CJ, Smeets JRLM, et al. High-density mapping of
electrically induced atrial fibrillation in humans. Circulation. 1994;89:1665–1680. [12] Falk RH, Podrid PJ. Atrial Fibrillation: Mechanisms and Management. New York,
Raven, 1992. [13] Prystowsky EN, Katz A. Atrial Fibrillation. In Topol EJ: Textbook of Cardiovascular
Medicine. Lippincott Williams and Wilkins. 2nd Edition. Pg. 1403-28. [14] Langendorf R, Pick AL, Katz LN. Ventricular response in atrial fibrillation: role of
concealed conduction in the AV junction. Circulation. 1965;32:69–75. [15] Prystowsky EN, Margiotti R, Fogel RI, et al. Atrial fibrillation with and without heart
disease: clinical characteristics and proarrhythmia risk. Circulation. 1996;94(8):I-191.
[16] Bhandari AK, Anderson JL, Gilbert EM, et al. Correlation of symptoms with occurrence of paroxysmal supraventricular tachycardia or atrial fibrillation: a transtelephonic monitoring study. Flecainide Supraventricular Tachycardia Study Group. Am. Heart J. 1992;124:381–386.
[17] Davies MJ, Pomerance A. Pathology of atrial fibrillation in man. Br Heart J 1972;34:520–525.
[18] Robinson K, Frenneaux MP, Stockins B, et al. Atrial fibrillation in hypertrophic cardiomyopathy: a longitudinal study. J. Am. Coll. Cardiol. 1990;15:1279–1285.
[19] Madariaga I, Carmona JR, Mateas FR, et al. Supraventricular arrhythmias as the cause of sudden death in hypertrophic cardiomyopathy. Eur. Heart J. 1994;15:134–137.
[20] Packer DL, Bardy GH, Worley SJ, et al. Tachycardia-induced cardiomyopathy: a reversible form of left ventricular dysfunction. Am. J. Cardiol. 1986;57:563–570.
[21] Keiny JR, Sacrez A, Facello A, et al. Increase in radionuclide left ventricular ejection fraction after cardioversion of chronic atrial fibrillation in idiopathic dilated cardiomyopathy. Eur. Heart J. 1992;13:1290–1295.
[22] Brugada P. Left Ventricular Dysfunction in a Patient with Chronic Atrial Fibrillation: Consider a Tachycardiomyopathy, a Curable Cause of Heart Failure. In Brugada J; Atrial Fibrillation, a Practical Approach. 2000 Prous Science. Barcelona.

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 313
[23] Heppell RM, Berkin KE, McLenachan JM, et al. Haemostatic and haemodynamic abnormalities associated with left atrial thrombosis in non-rheumatic atrial fibrillation. Heart. 1997;77:407–411.
[24] Sohara H, Amitani S, Kurose M, et al. Atrial fibrillation activates platelets and coagulation in a time-dependent manner; a study in patients with paroxysmal atrial fibrillation. J. Am. Coll. Cardiol. 1977;29:106–112.
[25] Halperin JL, Hart RG. Atrial fibrillation and stroke: new ideas, persisting dilemmas. Stroke. 1988; 19: 37–41.
[26] Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991; 22: 983-8.
[27] Atrial Fibrillation Investigators. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomized controlled trials. Arch. Intern. Med. 1994;154:1449 –57.
[28] Cosio FG, Lopez GM, Goicolea A, Arribas F. Electrophysiologic studies in atrial flutter. Clin. Cardiol. 1992; 15: 667.
[29] Pastor A, Esteban E, Montero MA, García B, López L. Diagnóstico electrocardiográfico y tratamiento agudo de los episodios de fibrilación y flutter auricular. Rev. Esp. Cardiol. 1996; 49 (Supl 2): 22-31.
[30] Ghali WA, Wasil BI, Brant R, Exner DV, Cornuz J. Atrial flutter and the risk of thromboembolism: A systematic review and meta-analysis. Am. J. Med. 2005 Feb;118(2):101-7.
[31] Snow V, Weiss KB, LeFevre M, Macnamara R, Bass E, Green LA, Michl K et al. Management of Newly Detected Atrial Fibrillation: A clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann. Intern. Med. 2003; 139: 1009-17.
[32] Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991; 22: 983-8.
[33] Hart RG, Halperin JL. Atrial fibrillation and stroke: concepts and controversies. Stroke. 2001;32: 803– 8.
[34] Petersen P, Boysen G,Godtfredsen J, Andersen ED, Andersen B. Placebo-controlled, randomised trial of warfarin and aspirin for prevention of thromboembolic complications in chronic atrial fibrillation. The Copenhagen AFASAK study. Lancet. 1989; 1:175–9.
[35] Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. EAFT (European Atrial Fibrillation Trial) Study Group. Lancet. 1993; 342: 1255–62.
[36] Adjusted-dose warfarin versus low-intensity, fixed-dose warfarin plus aspirin for high-risk patients with atrial fibrillation: Stroke Prevention in Atrial Fibrillation III randomised clinical trial. Lancet. 1996; 348: 633-8.
[37] Hart RG, Pearce LA, McBride R, Rothbart RM, Asinger RW. Factors associated with ischemic stroke during aspirin therapy in atrial fibrillation: analysis of 2012 participants in the SPAF I-III clinical trials. The Stroke Prevention in Atrial Fibrillation (SPAF) Investigators . Stroke. 1999; 30: 1223–9.

Tomás Muñoz 314
[38] Hart RG, Benavente O, McBride R, Pearce LA. Antithrombotic therapy to prevent stroke in patients with atrial fibrillation: a meta-analysis. Ann. Intern. Med. 1999; 131: 492–501.
[39] Go AS et al. Implications of Stroke Risk Criteria on the Anticoagulation Decision in Nonvalvular Atrial Fibrillation. Circulation. 2000; 102: 11-13.
[40] Potier K, Parris R. Best evidence topic report. Anticoagulation post-cardioversion of acute atrial fibrillation in the emergency department. Emerg. Med. J. 2005 Apr;22(4):275-6.
[41] Albers WA et al. Antithrombotic Therapy in Atrial Fibrillation. Chest. 2001; 119: 194S-206S.
[42] Singer DE, Albers GW, Dalen JE, Go AS, Halperin JL, Manning WJ. Antithrombotic Therapy in Atrial Fibrillation: The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;12: 429S-56S.
[43] Stellbrink C, Schimpf T. Anticoagulation during Cardioversion in Patients with Atrial Fibrillation: Current Clinical Practice. Am. J. Cardiovasc. Drugs. 2005;5(3):155-62.
[44] Goldstein LB, Adams R, Alberts MJ, Appel LJ, Brass LM, Bushnell CD, Culebras A, DeGraba TJ, Gorelick PB, Guyton JR, Hart RG, Howard G, Kelly-Hayes M, Nixon JV, Sacco RL; American Heart Association; American Stroke Association Stroke Council. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council: cosponsored by the Atherosclerotic Peripheral Vascular Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2006 Jun 20;113(24):e873-923.
[45] Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: Results from the National Registry of Atrial Fibrillation . JAMA. 2001; 285: 2864-70.
[46] ACTIVE Writing Group on behalf of the ACTIVE Investigators; Connolly S, Pogue J, Hart R, Pfeffer M, Hohnloser S, Chrolavicius S, Pfeffer M, Hohnloser S, Yusuf S. Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W): a randomised controlled trial. Lancet. 2006 Jun 10;367(9526):1903-12.
[47] Klein AL et al. Cardioversion guided by transesophageal echocardiography: the ACUTE Pilot Study. Ann. Intern. Med. 1997; 126: 200-9.
[48] Klein AL et al. Use of trasesophageal echocardiography to guide cardioversion in patients with atrial fibrillation. N. Eng. J. Med. 2001; 344: 1411-20.
[49] Murray et al. Natiolal Use of the Transesophageal Echocardiographic-Guided Approach to Cardioversion for Patients in Atrial Fibrillation. Am. J. Cardiol. 2000; 85: 239-44.
[50] Roiger A, Eskilsson J, Olsson B. Transoesophageal echocardiography-guided cardioversion of atrial fibrillation or flutter; Selection of a low-risk group for inmediate cardioversion. Eur. Heart J. 2000; 21: 837-47.

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 315
[51] Jagasia DH, Williams B, Ezekowitz MD. Clinical implication of antiembolic trials in atrial fibrillation and role of transesophageal echocardiography in atrial fibrillation. Curr. Opin. Cardiol. 2000; 15: 58-63.
[52] Labovitz AJ, Bransford TL. Evolving role of echocardiography in the management of atrial fibrillation. Am. Heart J. 2001; 141: 518-27.
[53] Thambidorai SK, Murray RD, Parakh K, Shah TK, Black IW, Jasper SE, Li J, Apperson-Hansen C, Asher CR, Grimm RA, Klein AL; ACUTE Investigators. Utility of Transesophageal Echocardiography in Identification of Thrombogenic Milieu in Patients With Atrial Fibrillation (an ACUTE Ancillary Study). Am. J. Cardiol. 2005 Oct 1;96(7):935-41.
[54] De Luca I, Sorino M, De Luca L, Colonna P, Del Salvatore B, Corliano L. Pre and post-cardioversion transesophageal echocardiography for brief anticoagulation therapy with enoxaparin in atrial fibrillation patients: a prospective study with a 1-year follow-up. Int. J. Cardiol. 2005 Jul 20; 102(3) : 447-54.
[55] Nattel S, Opie LH. Controversies in atrial fibrillation. Lancet. 2006; 367: 262-72. [56] Haïsaguerre M, Shah D, Jaïs P, Hocini M, Yamane T, Deisenhofer I, Garrige S,
Clémenty J. Mapping Guided Ablation of the Pulmonary Veins for Cure of Paroxysmal Atrial Fibrillation. In Brugada J: Atrial Fibrillation, a practical approach. 2000 Prous Science. Barcelona. Pg. 175-186.
[57] Pappone C, Santinelli V. Atrial fibrillation ablation: state of the art. Am. J. Cardiol. 2005 Dec 19;96(12A):59L-64L.
[58] Riley MJ, Marrouche NF. Ablation of atrial fibrillation. Curr. Probl. Cardiol. 2006 May;31(5):361-90.
[59] Fisher JD, Spinelli MA, Mookherjee D, Krumerman AK, Palma EC. Atrial fibrillation ablation: reaching the mainstream. Pacing Clin. Electrophysiol. 2006 May;29(5):523-37.
[60] Hohnloser SH, Kuck KH, Lilienthal J. Rhythm or rate control in atrial fibrillation-pharmacological intervention in atrial fibrillation (PIAF): a randomised trial. Lancet. 2000; 356: 1789-94.
[61] Carlsson J, Miketic S, Windeler J et al. STAF Investigators. Randomized trial of rate-control versus rhythm-control in persistent atrial fibrillation: The Strategies of Treatment of atrial Fibrillation (STAF) study. J. Am. Coll. Cardiol. 2003; 41: 1690-6.
[62] Hagens VE, Vermeulen KM, TenVergert EM, Van Veldhuisen DJ, Bosker HA, Kamp O, Kingma JH, Tijssen JGP, Crijns HJGM, Van Gelder IC. Rate control is more cost-effective than rhythm control for patients with persistent atrial fibrillation - results from the RAte Control versus Electrical cardioversion (RACE) study. Eur. Heart J. 2004;25(17):1542-9.
[63] Opolski G, Torbicki A, Kosior DA et al. Rate control versus Rhythm control in patients with nonvalvular persistent atrial fibrillation: the results of the Polish How to Treat Chronic Atrial Fibrillation (HOT CAFÉ) Study. Chest. 2004; 126: 476-86.
[64] Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, Schron EB, Kellen JC, Greene HL, Mickel MC, Dalquist JE, Corley SD; Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) Investigators. A comparison of rate

Tomás Muñoz 316
control and rhythm control in patients with atrial fibrillation. N. Engl. J. Med. 2002 Dec 5;347(23):1825-33.
[65] de Denus S, Sanoski CA, Carlsson J, Opolski G, Spinler SA. Rate versus rhythm control in patients with atrial fibrillation: a meta-analysis. Arch. Intern. Med. 2005; 165: 258-62.
[66] Mead G, Elder A, Flapan A, Kelman A. Electrical cardioversion for atrial fibrillation and flutter. Cochrane Database Syst. Rev. 2005 Jul 20;(3):CD002903.
[67] Corley SD, Epstein AE, DiMarco JP et al. Relationships between sinus rhythm, treatment, and survival in the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) Study. Circulation. 2004; 109: 1509-13.
[68] Hagens; Ranchor; Van Sonderen; Bosker; Kamp; Tijssen; Kingma; Crijns; Van Gelder. Effect of rate or rhythm control on quality of life in persistent atrial fibrillation. Results from the rate control versus electrical cardioversion (Race) study. J. Am. Coll. Cardiol. 2004 Jan 21;43(2):241-7.
[69] Thrall G, Lane D, Carroll D, Lip GY. Quality of life in patients with atrial fibrillation: a systematic review. Am. J. Med. 2006 May;119(5):448.e1-19.
[70] Azpitarte J, Baún O, Moreno E et al. In Patients with Chronic Atrial Fibrillation and Left Ventricular Systolic Dysfunction, Restoration of Sinus Rhythm Confers Substantial Benefit. Chest. 2001; 120: 132-8.
[71] Vora A, Karnad D, Goyal V, Naik A, Gupta A, Lokhandwala Y, Kulkarni H, Singh BN. Control of heart rate versus rhythm in rheumatic atrial fibrillation: a randomized study. J. Cardiovasc. Pharmacol. Ther. 2004; 9: 265-73.
[72] Singh SN, Tang XC, Singh BN, Dorian P, Reda DJ, Harris CL, Fletcher RD, Sharma SC, Atwood JE, Jacobson AK, Lewis HD Jr, Lopez B, Raisch DW, Ezekowitz MD; SAFE-T Investigators. Quality of life and exercise performance in patients in sinus rhythm versus persistent atrial fibrillation: a Veterans Affairs Cooperative Studies Program Substudy. J. Am. Coll. Cardiol. 2006 Aug 15;48(4):721-30.
[73] AFFIRM Investigators. Atrial Fibrillation Follow-up Investigation of Rhythm Management. Baseline characteristics of patients with atrial fibrillation: the AFFIRM Study. Am. Heart J. 2002 Jun;143(6):991-1001.
[74] Crijns HJ. Rate versus rhythm control in patients with atrial fibrillation: what the trials really say. Drugs. 2005;65(12):1651-67.
[75] Blomstrom-Lundqvist C, Scheinman MM et al. ACC/AHA/ESC Guidelines for the Management of patients with supraventricular arrhythmias. J. Am. Coll. Cardiol. 2003 Oct 15;42(8):1493-531.
[76] Touboul, P, Saoudi, N, Atallah, G, et al. Electrophysiologic basis of catheter ablation in atrial flutter. Am. J. Cardiol. 1989; 64:795.
[77] Lee, SH, Tai, CT, Yu, WC, et al. Effects of radiofrequency catheter ablation on quality of life in patients with atrial flutter. Am. J. Cardiol. 1999; 84:278.
[78] Calkins, H, Canby, R, Weiss, R, et al. Results of catheter ablation of typical atrial flutter. Am. J. Cardiol. 2004; 94:437.
[79] Page RL. Clinical practice. Newly diagnosed atrial fibrillation. N. Engl. J. Med. 2004;351(23):2408-16.

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 317
[80] Schoonderwoerd BA, Van Gelder IC, Crijns HJGM. External Electrical Cardioversion of Atrial Fibrillation. In Brugada J; Atrial Fibrillation, a Practical Approach. 95-102. Barcelona.2000 Prous Science.
[81] Coplen SE, Antman EM et al. Efficacy and safety of quinidine therapy for maintenance of sinus rhythm after cardioversion. A meta-analysis of randomized control trials. Circulation. 1990; 82: 1106-16.
[82] Capucci A, Villani GQ, Piepoli M. Pharmacological Cardioversion of Atrial Fibrillation. In Brugada J; Atrial Fibrillation, A Practical Approach. 77- 94. Barcelona. 2000 Prous Science.
[83] Boriani G et al. Oral propafenone to convert recent-onset atrial fibrillation in patients with and without underlying heart disease. A randomized, controlled trial. Ann. Intern. Med. 1997; 126: 621-5.
[84] Khan IA. Single Oral Loading Dose of Propafenone for Pharmacological Cardioversion of Recent-Onset Atrial Fibrillation. J. Am. Coll. Cardiol. 2001; 37: 542-7.
[85] Ashan A, Aldridge R, Bowes R. 1:1 atrio-ventricular conduction in atrial flutter with digoxin and flecainide. Int. J. Cardiol. 1993; ; 39: 88-90.
[86] Botto GL, Bonini W, Broffoni T et al. Regular ventricular rhythm before conversion of recent onset atrial fibrillation to sinus rhythm. Pacing Clin. Electrophysiol. 1994; 17: 2114-7.
[87] El-Harari MB, Adams PC. Atrial flutter with 1:1 atrio-ventricular conduction caused by propafenone. Pacing Clin. Electrophysiol. 1998; 21: 1999-2001.
[88] Alboni P, Botto GL, Baldi N, Luzi M, Russo V, Gianfranchi L, Marchi P, Calzolari M, Solano A, Baroffio R, Gaggioli G. Outpatient treatment of recent-onset atrial fibrillation with the"pill-in-the-pocket" approach. N. Engl. J. Med. 2004 Dec 2;351(23):2384-91.
[89] Bianconi L et al. Comparison of intravenously administered dofetilide versus amiodarone in the acute termination of atrial fibrillation and flutter. Eur. Heart J. 2000; 21: 1265-75.
[90] Zhang N, Guo JH, Zhang HCh, Li XB, Zhang P, Xn Y. Comparison of intravenous ibutilide vs. propafenone for rapid termination of recent onset atrial fibrillation. Int. J. Clin. Pract. 2005; 59(12):1395-400.
[91] Korantzopoulos P, Kolettis TM, Papathanasiou A, Naka KK, Kolios P, LeontaridisI, Draganigos A, Katsouras CS, Goudevenos JA. Propafenone added to ibutilide increases conversion rates of persistent atrial fibrillation. Heart. 2006 May;92(5): 631-4.
[92] Mountantonakis SE, Moutzouris DA, Tiu RV, Papaioannou GN, McPherson CA. Ibutilide to expedite ED therapy for recent-onset atrial fibrillation flutter. Am. J. Emerg. Med. 2006 Jul;24(4):407-12.
[93] Okishige K, Fukunami M, Kumagai K, Atarashi H, Inoue H; Pilsicainide Suppression Trial for Persistent Atrial Fibrillation II Investigators. Pharmacological conversion of persistent atrial fibrillation into sinus rhythm with oral pilsicainide: pilsicainide suppression trial for persistent atrial fibrillation II. Circ. J. 2006; 70(7):945.

Tomás Muñoz 318
[94] Marrouche NF et al. High-dose bolus Lidocaine for chemical cardioversion of atrial fibrillation: A prospective, ramdomized, double-blind crossover trial. Am. Heart J. 2000; 139: 26.
[95] Vardes PE et al. Amiodarone as a First-Choice Drug for Restoring Sinus Rhythm in Patients with Atrial Fibrillation. Chest. 2000; 117: 1538-45.
[96] Hofmann R, Steinwender C, Kammler J, Kypta A, Leisch F. Effects of a high dose intravenous bolus amiodarone in patients with atrial fibrillation and a rapid ventricular rate. Int. J. Cardiol. 2006 Jun 7;110(1):27-32.
[97] Potier K, Parris R. Best evidence topic report. Anticoagulation before cardioversion of acute atrial fibrillation in the emergency department. Emerg. Med. J. 2005 Apr;22(4):275.
[98] Potier K, Parris R. Best evidence topic report. Anticoagulation post-cardioversion of acute atrial fibrillation in the emergency department. Emerg. Med. J. 2005 Apr;22(4):275-6.
[99] Sticherling C, Behrens S, Kamke W, Stahn A, Zabel M. Comparison of acute and long-term effects of single-dose amiodarone and verapamil for the treatment of immediate recurrences of atrial fibrillation after transthoracic cardioversion. Europace. 2005 Nov;7(6):546-53.
[100] Arnsdorf MF. Antiarrhythmic drugs to maintain sinus rhythm after cardioversion in atrial fibrillation: Clinical trials. UpToDate 14.1 May 9, 2005. Available at http://www. uptodateonline.com. Accessed May, 2006.
[101] Korantzopoulos P, Kolettis TM, Kountouris E, Dimitroula V, Karanikis P, Pappa E, Siogas K, Goudevenos JA. Oral vitamin C administration reduces early recurrence rates after electrical cardioversion of persistent atrial fibrillation and attenuates associated inflammation. Int. J. Cardiol. 2005 Jul 10;102(2):321-6.
[102] Lombardi F, Terranova P. Renin-angiotensin system block and atrial fibrillation. Curr. Med. Chem. 2005;12(11):1331-7.
[103] Dilaveris P, Giannopoulos G, Synetos A, Stefanadis C. The role of renin angiotensin system blockade in the treatment of atrial fibrillation. Curr. Drug Targets Cardiovasc. Haematol. Disord. 2005;5:387-403.
[104] Ehrlich JR, Hohnloser SH, Nattel S. Role of angiotensin system and effects of its inhibition in atrial fibrillation: clinical and experimental evidence. Eur. Heart J. 2006 Mar;27(5):512-8.
[105] Kalus JS, Coleman CI, White CM. The impact of suppressing the renin-angiotensin system on atrial fibrillation. J. Clin. Pharmacol. 2006 Jan;46(1):21-8.
[106] Healey JS, Baranchuk A, Crystal E, Morillo CA, Garfinkle M, Yusuf S, Connolly SJ. Prevention of atrial fibrillation with Angiotensin-converting enzyme inhibitors and Angiotensin receptor blockers a meta-analysis. J. Am. Coll. Cardiol. 2005 Jun 7;45(11):1832-9.
[107] Madrid AH, Escobar C, Rebollo JMG, Marín I, Bernal E, Nannini S, Limón L, Peng J, Moro C. Angiotensin receptor blocker as adjunctive therapy for rhythm control in atrial fibrillation: results of the irbesartan-amiodarone trial. Card. Electrophysiol. Rev. 2003 Sep;7(3):243-6.

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 319
[108] Healey JS, Morillo CA, Connolly SJ. Role of the renin-angiotensin-aldosterone system in atrial fibrillation and cardiac remodeling. Curr. Opin. Cardiol. 2005 Jan;20(1):31-7.
[109] Lozano HF, Conde CA, Florin T, Lamas GA. Treatment and prevention of atrial fibrillation with nonantiarrhythmic pharmacologic therapy. Heart Rhythm. 2005 Sep;2(9):1000-7.
[110] Ozaydin M, Varol E, Aslan SM, Kucuktepe Z, Dogan A, Ozturk M, Altinbas A. Effect of atorvastatin on the recurrence rates of atrial fibrillation after electrical cardioversion. Am. J. Cardiol. 2006 May 15;97(10):1490-3.
[111] Patti G, Chello M, Candura D, Pasceri V, D'Ambrosio A, Covino E, Di Sciascio G. Randomized trial of atorvastatin for reduction of postoperative atrial fibrillation in patients undergoing cardiac surgery: results of the ARMYDA-3 (Atorvastatin for Reduction of MYocardial Dysrhythmia After cardiac surgery) study. Circulation. 2006 Oct 3;114(14):1455-61.
[112] Reiffel JA, McDonald A. Antiarrhythmic effects of omega-3 fatty acids. Am. J. Cardiol. 2006 Aug 21;98(4A):50i-60i.
[113] Van Noord T, Crijns HJ, van den Berg MP, Van Veldhuisen DJ, Van Gelder IC. Pretreatment with ACE inhibitors improves acute outcome of electrical cardioversion in patients with persistent atrial fibrillation. BMC Cardiovasc Disord. 2005 Jan 24;5(1):3.
[114] Wachtell K, Lehto M, Gerdts E, Olsen MH, Hornestam B, Dahlof B, Ibsen H, Julius S, Kjeldsen SE, Lindholm LH, Nieminen MS, Devereux RB. Angiotensin II receptor blockade reduces new-onset atrial fibrillation and subsequent stroke compared to atenolol: the Losartan Intervention For End Point Reduction in Hypertension (LIFE) study. J. Am. Coll. Cardiol. 2005 Mar 1;45(5):712-9.
[115] Anand K, Mooss AN, Hee TT, Mohiuddin SM. Meta-analysis: inhibition of renin-angiotensin system prevents new-onset atrial fibrillation. Am. Heart J. 2006 Aug;152(2):217-22.
[116] Van Gelder IC, Crijns HJ, Tieleman RG, et al. Chronic atrial fibrillation.Success of serial cardioversion therapy and safety of oral anticoagulation. Arch. Intern. Med. 1996;156:2585–92.
[117] Kerr CR, Humphries KH, Talajic M, Klein GJ, Connolly SJ, Green M, Boone J, Sheldon R, Dorian P, Newman D. Progression to chronic atrial fibrillation after the initial diagnosis of paroxysmal atrial fibrillation: results from the Canadian Registry of Atrial Fibrillation. Am. Heart J. 2005;149:489-96.
[118] Oral H, Morady F. How to select patients for atrial fibrillation ablation. Heart Rhythm. 2006 May;3(5):615-8.
[119] Williams J, Ungerleider R, Lofland G et al. Left atrial isolation: New technique for the treatment of supraventricular arrhythmias. J. Cardiovasc. Surg. 1980; 80: 373-80.
[120] Guiraudon G, Campbell C, Jones D et al. Combined sino-atrial node atrio-ventricular node isolation: A surgical alternative to His bundle ablation in patients with atrial fibrillation. Circulation. 1985; 72: 111-220.

Tomás Muñoz 320
[121] Cox JL, Schuessler RB, D´Agostino HJ et al. The surgical treatmente of atrial fibrillation : III. Development of a definite surgical procedure. J. Cardiovasc. Surg. 1991; 101: 569-83.
[122] Defauw J, Guiraudon G, vanHemel N et al. Surgical therapy of paroxysmal atrial fibrillation with the corridor operation. Ann. Thorac. Surg. 1992; 53: 564-71.
[123] Ewy GA. Transthoracic Electrical Defibrillation and Cardioversion. In Topol EJ: Textbook of Cardiovascular Medicine. Lippincott Williams and Wilkins. 2nd Edition.
[124] Annual Reports of the Royal Humane Society for the Recovery of the Apparently Drowned. London 1774; 1: 31.
[125] Beck CS, Pritchard VM, Feil HS. Ventricular fibrillation of long duration abolished by electric shock. JAMA. 1947;135:985-90.
[126] Zoll, PM, Linenthal, AJ, Gibson, W, et al. Termination of ventricular fibrillation in man by externally applied electric countershock. N. Engl. J. Med. 1956; 254:727.
[127] Lown B, Amarasingham R, Neumann J. New method for terminating cardiac arrythmias. JAMA. 1962, 182: 548-55.
[128] Zipes, DP, Fischer, J, King, RM, et al. Termination of ventricular fibrillation in dogs by depolarizing a critical amount of myocardium. Am. J. Cardiol. 1975; 36:37.
[129] Greene TO, Mittleman RS. Cardioversion and Defibrillation. In Rippe JM, Irwin RS, Fink MP, Cerra FB, Curley FJ, Heard SO: Procedures and Techniques in Intensive Care Medicine. Little, Brown and Company 1995, page 81-92.
[130] Zipes DP. Electrical Therapy of Cardiac Arrhythmias. In Braunwald E: Heart Disease. 5th edition, 1997. Saunders, page 619-20.
[131] Sweeney MO. Cardioversion and Defibrillation. EI Irwin and Rippe. Intensive Care Medicine. Little, Brown and Company 5th edition, 2003, page 73-80.
[132] Witkowski, FX, Kerber, RE. Currently known mechanisms underlying direct current external and internal cardiac defibrillation. J. Cardiovasc. Electrophysiol. 1991; 2:562.
[133] Deakin CD, Nolan JP. European Resuscitation Council Guidelines for Resuscitation 2005. Section 3. Electrical therapies: automated external defibrillators, defibrillation cardioversion and pacing. Resuscitation. 2005; 67S1: S25-S37.
[134] Podrid PJ. Basic principles and technique of cardioversion and defibrillation. UpToDate (14.2) January 19, 2005. Available at http://www. uptodateonline.com. Accessed May, 2006.
[135] Smart Biphasic, A Proven, Fixed, Low-Energy Defibrillation Waveform. En http:// www.medical.philips.com/main/products/resuscitation/biphasic_technology/biphasic_overview.html
[136] Medtronic Physio.control. Defibrillation with ADAPTIVTM Biphasic Technology. En http://www.biphasic.com/reference/adaptiv_summary.pdf
[137] Bziphasic Technology Overview. En http://www.zoll.com/page.aspx?id=286 [138] Kerber RE, Grayzel J, Hoyt R, et al. Transthoracic resistance in human defibrillation:
influence of body weight, chest size, serial shocks, paddle size and paddle contact pressure. Circulation. 1981;63:676–682.

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 321
[139] Geddes LA, Niebauer MJ, Babbs CF, Bourland JD. Fundamental criteria underlying the efficacy and safety of defibrillating current waveforms. Med. Biol. Eng. Comput. 1985;23:122-30.
[140] Jones JL. Waveforms for implantable cardioverter defibrillators (ICDs) and transchest defibrillation. In: Tacker WA Jr, ed. Defibrillation of the heart, ICDs, AEDs, and manual. St. Louis: Mosby–Year Book, 1994:46–81.
[141] Kerber RE. Transthoracic Cardioversion of Atrial Fibrillation and Flutter: Standard Techniques and New Advances. Am. J. Cardiol. 1996; 78 (suppl 8A): 22-6.
[142] Thohman RG, Parrillo JE. Direct current cardioversion: Indications, techniques and recent advances. Crit. Care Med. 2000; 28 (Suppl): N170-N173.
[143] Achleitner U, et al. Waveform analysis of biphasic external defibrillators. Resuscitation. 2001;50:61-70.
[144] Snyder DE, et al. External series resistors accurately model waveform time course, but not cardiac dose in animal models of defibrillation. Resuscitation. 2003;56:238[abstract].
[145] Jones JL, et al. Predictions from misleading pig model are potentially harmful to humans. Resuscitation. 2003;59:365-367.
[146] Jones et al. Dysfunction and safety factor strength-duration curves for biphasic defibrillator waveforms. Journal of the Am. Physiological. Society. 1994;H263-271.
[147] Huang J, KenKnight BH, Rollins DL, et al. Ventricular defibrillation with triphasic waveforms. Circulation. 2000;101:1324–1328.
[148] Muñoz T, Castedo JF, Castañeda A, Dudagoitia JL, Poveda Y, Iribarren S. Sedación para cardioversión eléctrica; Comparación de dosis bajas de Propofol y Etomidato. Med. Intensiva. 2002; 26: 98-103.
[149] Muñoz T, Poveda Y, Dudagoitia JL, Martínez S, Vinuesa C, Hernández M, Iribarren S. Comparación de onda monofásica y bifásica en la cardioversión eléctrica de la fibrilación auricular. Med. Intensiva. 2005; 29: 79-82.
[150] Muñoz T, Martínez S, Vinuesa C, Poveda Y, Dudagoitia JL, Iribarren S, Hernández M. Comparación de dos posiciones de electrodos en la cardioversión eléctrica de la fibrilación auricular. Med. Intensiva. 2006; 30: 137-42.
[151] Muñoz T, Martínez S, Vinuesa C, Dudagoitia JL, Poveda Y, Iribarren S, Castillo C, Hernández M, Ruiz JM, Aretxabala N. Cardioversión eléctrica de fibrilación auricular con electrodos en posición anteroapical versus anteroposterior. Med. Intensiva. 2006; 30 (Suppl 1): 4 (abstract).
[152] Raitt MH, Volgman AS, Zoble RG, Charbonneau L, Padder FA, O'Hara GE, Kerr D; AFFIRM Investigators. Prediction of the recurrence of atrial fibrillation after cardioversion in the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) study. Am. Heart J. 2006 Feb;151(2):390-6.
[153] Glazer NL, Dublin S, Smith NL, French B, Jackson LA, Hrachovec JB, Siscovick DS, Psaty BM, Heckbert SR. Newly Detected Atrial Fibrillation and Compliance With Antithrombotic Guidelines. Arch. Intern. Med. 2007 167: 246-252.
[154] Mittal S et al. Transthoracic cardioversion of atrial fibrillation. comparison of rectilinear biphasic versus damped sine wave monophasic shocks. Circulation. 2000; 101: 1282-7.

Tomás Muñoz 322
[155] Rho RW, Page RL. Biphasic versus monophasic shock waveform for conversion of atrial fibrillation. Card. Electrophysiol. Rev. 2003 Sep;7(3):290-1.
[156] Koster, RW, Dorian P, Chapman FW, Schmitt PW, O'Grady SG, Walker RG. A randomized trial comparing monophasic and biphasic waveform shocks for external cardioversion of atrial fibrillation. Am. Heart J. 2004 May;147(5):e20.
[157] Gurevitz OT, Ammash NM, Malouf JF, Chandrasekaran K, Rosales AG, Ballman KV, Hammill SC, White RD, Gersh BJ, Friedman PA. Comparative efficacy of monophasic and biphasic waveforms for transthoracic cardioversion of atrial fibrillation and atrial flutter. Am. Heart J. 2005 Feb;149(2):316-21.
[158] Alatawi F, Gurevitz O, White RD, Ammash NM, Malouf JF, Bruce CJ, Moon BS, Rosales AG, Hodge D, Hammill SC, Gersh BJ, Friedman PA. Prospective, randomized comparison of two biphasic waveforms for the efficacy and safety of transthoracic biphasic cardioversion of atrial fibrillation. Heart Rhythm. 2005 Apr;2(4):382-7.
[159] Niebauer MJ, Chung MK, Brewer JE, Tchou PJ. Reduced cardioversion thresholds for atrial fibrillation and flutter using the rectilinear biphasic waveform. J. Interv. Card. Electrophysiol. 2005 Jul;13(2):145-50.
[160] Alatawi F, Gurevitz O, White RD, Ammash NM, Malouf JF, Bruce CJ, Moon BS, Rosales AG, Hodge D, Hammill SC, Gersh BJ, Friedman PA. Prospective, randomized comparison of two biphasic waveforms for the efficacy and safety of transthoracic biphasic cardioversion of atrial fibrillation. Heart Rhythm. 2005 Apr;2(4):382-7.
[161] Dahl, CF, Ewy, GA, Warner, ED, et al. Myocardial necrosis from direct current countershock. Effect of paddle electrode size and time interval between discharges. Circulation. 1974; 50:956.
[162] Kirchhof P, Monnig G, Wasmer K, Heinecke A, Breithardt G, Eckardt L, Bocker D. A trial of self-adhesive patch electrodes and hand-held paddle electrodes for external cardioversion of atrial fibrillation (MOBIPAPA). Eur. Heart J. 2005 Jul;26(13):1292-7.
[163] Ambler JJS, Sado DM, Zideman DA, Deakin CD. The incidence and severity of cutaneous burns following external DC cardioversion. Resuscitation. 2004; 613: 281-8.
[164] Ewy, GA, Taren, D. Comparison of paddle electrode pastes used for defibrillation. Heart Lung. 1977; 6:847.
[165] Bissing JV, Kerber RE. Effect of shaving the chest of hirsute subjects on transthoracic impedance to self-adhesive defibrillation electrode pads. Am. J. Cardiol. 2000;86:587–589.
[166] Botto GL et al. External Cardioversion of atrial fibrillation: role of paddle position on technical efficacy and energy requirements. Heart. 1999; 82: 726-30.
[167] Kirchhof P, Borggrefe M, Breithardt G. Effect of electrode position on the outcome of cardioversion. Card. Electrophysiol. Rev. 2003 Sep;7(3):292-6.
[168] Chen CJ, Guo GBF. External cardioversion in patients with persistent atrial fibrillation: a reappraisal of the effects of electrode pad position and transthoracic impedance on cardioversion success. Jpn. Heart J. 2003 Nov;44(6):921-32.

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 323
[169] Siaplaouras S, Buob A, Rotter C, Bohm M, Jung J. Randomized comparison of anterolateral versus anteroposterior electrode position for biphasic external cardioversion of atrial fibrillation. Am. Heart J. 2005 Jul;150(1):150-2.
[170] Walsh SJ, McCarty D, McClelland AJ, Owens CG, Trouton TG, Harbinson MT, O'mullan S, McAllister A, McClements BM, Stevenson M, Dalzell GW, Adgey AA. Impedance compensated biphasic waveforms for transthoracic cardioversion of atrial fibrillation: a multi-centre comparison of antero-apical and antero-posterior pad positions. Eur. Heart J. 2005 ; 26: 1298-302.
[171] Tormo C, Ruano M, Bonastre J. Tratamiento eléctrico de las arritmias. In Ruano M, Tormo C. Manual de soporte vital avanzado. Masson , Barcelona. 3ª edición 2004. Pag. 121- 38.
[172] Nolan JP, Deakin CD, Soar J, Böttiger BW, Smith G. European Resuscitation Council Guidelines for Resuscitation 2005. Section 4. Adult advanced life support. Resuscitation. (2005) 67S1, S39—S86.
[173] Pinski SL et al. A comparison of 50-J versus 100-J shocks for direct-current cardioversion of atrial flutter. Am. Heart J. 1999; 137: 439-42.
[174] Deakin CD, Nolan JP. European Resuscitation Council Guidelines for Resuscitation 2005. Section 3. Electrical therapies: automated external defibrillators, defibrillation cardioversion and pacing. Resuscitation. 2005; 67S1: S25-S37.
[175] Rashba EJ, Gold MR, Crawford FA, Leman RB, Peters RW, Shorofsky SR. Efficacy of transthoracic cardioversion of atrial fibrillation using a biphasic, truncated exponential shock waveform at variable initial shock energies. Am. J. Cardiol. 2004 Dec 15;94(12):1572-4.
[176] Miracapillo G, Costoli A, Addonisio L, Severi S. Initial energy for biphasic external electrical cardioversion of atrial fibrillation. Ital. Heart J. 2005 Sep;6(9):757-60.
[177] Kosior DA, Opolski G, Tadeusiak W, Chwyczko T, Wozakowska-Kaplon B, Stawicki S, Filipak KJ, Rabczenko D. Serum troponin I and myoglobin after monophasic versus biphasic transthoracic shocks for cardioversion of persistent atrial fibrillation. Pacing Clin. Electrophysiol. 2005 Jan;28 Suppl 1:S128-32.
[178] Deakin CD, Ambler JJ. Post-shock myocardial stunning: a prospective randomised double-blind comparison of monophasic and biphasic waveforms. Resuscitation. 2006 Mar;68(3):329-33.
[179] De Simone A et al. Pretreatment with verapamil in patients with persistent or chronic atrial fibrillation who underwent electrical cardioversion. J. Am. Coll. Cardiol. 1999; 34: 810-4.
[180] Villani GQ et al. Effects of diltiazem pretreatment on direct-current cardioversion in patients with persistent atrial fibrillation: A single-blind, randomized, controlled study. Am. Heart J. 2000; 140: e12.
[181] Hemels ME, Van Noord T, Crijns HJ, Van Veldhuisen DJ, Veeger NJ, Bosker HA, Wiesfeld AC, Van den Berg MP, Ranchor AV, Van Gelder IC. Verapamil versus digoxin and acute versus routine serial cardioversion for the improvement of rhythm control for persistent atrial fibrillation. J. Am. Coll. Cardiol. 2006 Sep 5;48(5):1001-9.

Tomás Muñoz 324
[182] Kosior DA, Opolski G, Wozakowska-Kaplon B, Rabczenko D. Serial Antiarrhythmic Therapy: Role of Amiodarone in Prevention of Atrial Fibrillation Recurrence - A Lesson from the HOT CAFE Polish Study. Cardiology. 2005 May 22;104(1):35-44
[183] Singh BN, Singh SN, Reda DJ, Tang XC, Lopez B, Harris CL, Fletcher RD, Sharma SC, Atwood JE, Jacobson AK, Lewis HD Jr, Raisch DW, Ezekowitz MD; Sotalol Amiodarone Atrial Fibrillation Efficacy Trial (SAFE-T) Investigators. Amiodarone versus sotalol for atrial fibrillation. N. Engl. J. Med. 2005 May 5;352(18):1861-72.
[184] Vijayalakshmi K, Whittaker VJ, Sutton A, Campbell P, Wright RA, Hall JA, Harcombe AA, Linker NJ, Stewart MJ, Davies A, de Belder MA.A randomized trial of prophylactic antiarrhythmic agents (amiodarone and sotalol) in patients with atrial fibrillation for whom direct current cardioversion is planned. Am. Heart J. 2006 Apr;151(4):863.e1-6.
[185] Hofmann R, Steinwender C, Kammler J, Kypta A, Leisch F. Effects of a high dose intravenous bolus amiodarone in patients with atrial fibrillation and a rapid ventricular rate. Int. J. Cardiol. 2006 Jun 7;110(1):27-32.
[186] Ratz Bravo AE, Drewe J, Schlienger RG, Krahenbuhl S, Pargger H, Ummenhofer W. Hepatotoxicity during rapid intravenous loading with amiodarone: Description of three cases and review of the literature. Crit. Care Med. 2005 Jan;33(1):128-34.
[187] Patel AA, White CM, Gillespie EL, Kluger J, Coleman CI. Safety of amiodarone in the prevention of postoperative atrial fibrillation: a meta-analysis. Am. J. Health Syst. Pharm. 2006 May 1;63(9):829-37.
[188] Martinez EA, Bass EB, Zimetbaum P; American College of Chest Physicians. Pharmacologic control of rhythm: American College of Chest Physicians guidelines for the prevention and management of postoperative atrial fibrillation after cardiac surgery. Chest. 2005 Aug;128(2 Suppl):48S-55S.
[189] Hayashi M, Tanaka K, Kato T, Morita N, Sato N, Yasutake M, Kobayashi Y, Takano T. Enhancing Electrical Cardioversion and Preventing Immediate Reinitiation of Hemodynamically Deleterious Atrial Fibrillation with Class III Drug Pretreatment. J. Cardiovasc. Electrophysiol. 2005 Jul;16(7):740-7.
[190] Kathofer S, Thomas D, Karle CA. The novel antiarrhythmic drug dronedarone: comparison with amiodarone. Cardiovasc. Drug Rev. 2005 Fall;23(3):217-30.
[191] Soifer BE. Procedural Anesthesia at the Bedside. Crit. Care Clin. 2000; 16:7-28. [192] Parlak M, Parlak I, Erdur B, Ergin A, Sagiroglu E. Age effect on efficacy and side
effects of two sedation and analgesia protocols on patients going through cardioversion: a randomized clinical trial.
[193] Canessa R, Lema G, Urzua J, Dagnino J, Concha M. Anesthesia for elective cardioversion: a comparison of four anesthetic agents. J. Cardiothorac. Vasc. Anesth. 1991; 5: 566-8.
[194] Hullander RM, Leivers D, Wingler K. A Comparison of Propofol and Etomidate for Cardioversion. Anesth. Analg. 1993; 77: 690-4.
[195] Jan KT, Wang KY, Lo Y, Lu BK, Liu K. Anesthesia for elective cardioversion: a comparison of thiopentone and propofol. Acta Anaesthesiol. Sin. 1995; 33: 35-9.

Electrical Cardioversion of Atrial Fibrillation and Atrial Flutter 325
[196] Kick O, Bohrer H, et al. [Etomidate versus propofol for anesthesia in ambulatory cardioversion]. Anasthesiol. Intensivmed. Notfallmed. Schmerzther. 1996; 31: 288-92 (abstract).
[197] Stoneham MD. Anaesthesia for cardioversion. Anaesthesia. 1996; 51: 565-70. [198] roch MJ et al. Valoración comparativa del etomidato, propofol y midazolam en la
cardioversión electiva. Med. Intensiva. 1999; 23: 209-15. [199] Karthikeyan S, Balachandran S, Cort J, Cross MH, Parsloe M. Anaesthesia for
cardioversion: a comparison of sevoflurane and propofol. Anaesthesia. 2002 Nov;57(11):1114-9.
[200] Herregods LL, Bossuyt GP, De Baerdemaeker LE, Moerman AT, Struys MM, Den Blauwen NM, Tavernier RM, Mortier E. Ambulatory electrical external cardioversion with propofol or etomidate. J. Clin. Anesth. 2003 Mar;15(2):91-6.
[201] Coll-Vinent B, Sala X, Fernandez C, Bragulat E, Espinosa G, Miro O, Milla J, Sanchez M. Sedation for cardioversion in the emergency department: analysis of effectiveness in four protocols. Ann. Emerg. Med. 2003 Dec;42(6):767-72.
[202] Maltepe F, Kocaayan E, Ugurlu BS, Akdeniz B, Guneri S. Comparison of remifentanil and fentanyl in anaesthesia for elective cardioversion. Anaesth. Intensive Care. 2006 Jun;34(3):353-7.
[203] Harrison SJ, Mayet J. Physician administered sedation for DC cardioversion. Heart. 2002 Aug;88(2):117-8.
[204] Tobin MG, Pinski SL, Tchou PJ, Ching EA, Trohman RG. Cost effectiveness of administration of intravenous anesthetics for direct-current cardioversion by nonanesthesiologists. Am. J. Cardiol. 1997 Mar 1;79(5):686-8.
[205] Goldner B et al. Electrical cardioversion of atrial fibrillation or flutter with conscious sedation in the age of cost containment. Am. Heart J. 1998; 136: 961-4.
[206] Shelton RJ, Allinson A, Johnson T, Smales C, Kaye GC. Four years experience of a nurse-led elective cardioversion service within a district general hospital setting. Europace. 2006 Jan;8(1):81-5.
[207] Botkin SB, Dhanekula LS, Olshansky B. Outpatient cardioversion of atrial arrhythmias: efficacy, safety, and costs. Am. Heart J. 2003 Feb;145(2):233-8.
[208] Herregods LL, Bossuyt GP, De Baerdemaeker LE, Moerman AT, Struys MM, Den Blauwen NM, Tavernier RM, Mortier E. Ambulatory electrical external cardioversion with propofol or etomidate. J. Clin. Anesth. 2003 Mar;15(2):91-6.
[209] Saliba W, Jurati N, Chung MK, Niebauer MJ, Erdogan O, Trohman R, et al. Higher Energy synchronized external, direct current cardioversion for refractory atrial fibrillation. J. Am. Coll. Cardiol. 1999; 34: 2031-4.
[210] Grönfeld GC, Ehrlich JR, Hohnloser SH. Internal electrical cardioversión in atrial fibrillation. In Brugada J. Atrial Fibrillation. A practical approach. Prous science. 2000. Barcelona. Pg. 103-8.
[211] Lévy S. Internal Defibrillation: Where we Have Been and Where we Should be Going? J. Interv. Card. Electrophysiol. 2005 Aug;13 Suppl 1:61-6.
[212] Lin WH, Saksena S, Prokash A, Shinas K. Multisite atrial pacing in refractory atrial fibrillation associated with bradyarrythmias. In Brugada J. Atrial Fibrillation. A practical approach. Prous science. 2000. Barcelona. Pg 69-76.

Tomás Muñoz 326
[213] Santini M et al. Transoesophageal low-energy cardioversion of atrial fibrillation. Results with the oesophageal-right atrial lead configuration. Eur. Heart J. 2000; 21: 848-55.

Index
A
access, 15, 66 accounting, 110, 178 accuracy, 119, 158, 244 acetylcholine, 76 achievement, 236 acid, 105 action potential, 6, 12, 13, 40, 77, 79, 83, 89, 106,
115, 132, 178 activation, ix, xii, xiv, 12, 13, 14, 15, 17, 29, 74, 76,
78, 79, 83, 84, 87, 89, 90, 91, 93, 95, 100, 109, 140, 204, 213, 217, 221, 232, 274, 278, 289, 290, 296
acute coronary syndrome, 95, 96, 97, 108, 110, 117, 122, 129, 130, 205
adaptation, 2, 98, 117, 282, 303 adenovirus, 7 adjunctive therapy, 318 adjustment, 106, 109, 140, 149, 182 adolescents, 174 adrenal gland, 84 adrenaline, 57, 99, 100, 103, 120 adrenoceptors, 89, 194 adults, xi, 160, 163, 164, 166, 168, 169, 170, 311 adverse event, 35, 164, 182, 183 advocacy, 65, 70 aetiology, 226 afternoon, 48 age, x, xi, xii, xiii, xv, 43, 51, 94, 98, 101, 109, 112,
120, 131, 133, 137, 139, 140, 141, 142, 147, 150, 152, 154, 155, 157, 159, 160, 164, 166, 168, 169, 172, 174, 203, 204, 207, 217, 218, 219, 220, 222,
223, 225, 226, 227, 235, 263, 271, 288, 291, 294, 306, 307, 325
agent, xii, 177, 178, 179, 182, 186, 189, 190, 191, 272, 293, 296, 310
aging, 128, 134, 141, 218, 282 agonist, 6, 85, 103 air pollutants, x, 93, 105, 106, 108, 110, 111, 129 air pollution, 105, 106, 108, 109, 111, 117, 118, 126,
127, 128, 129, 130, 135 airways, 106, 128, 304 akinesia, 219 alcohol, 101, 102, 103, 104, 113, 116, 118, 123, 124,
125, 135, 140, 190, 243, 288 alcohol abuse, 113 alcohol consumption, 101, 102, 103, 116, 123, 190 alcohol withdrawal, 102 alcoholic cardiomyopathy, 102 alcoholic liver disease, 142 alcoholics, 124 aldosterone, 81, 319 algorithm, 11, 31, 152 alienation, 2, 45 allele, 85 allergens, 128 allergic reaction, 7 alternative, xi, xiv, 6, 41, 43, 55, 138, 153, 169, 183,
187, 189, 190, 232, 259, 294, 309, 310, 319 alternatives, 62, 67, 234 alters, 77, 78, 282 altruism, 61 alveolar macrophage, 117 alveolar macrophages, 117 ambient air, 127 ambivalence, 2 American Heart Association, 126, 139, 157, 196,
197, 199, 200, 213, 311, 314

Index 328
amplitude, xiii, 77, 87, 104, 231, 238, 239, 242, 245, 246, 248, 256, 257, 258, 259, 261, 262, 264, 265, 274, 276, 277, 284, 289, 296
amygdala, 75, 86, 120 anatomy, 204 androgens, 112 anesthetics, 125, 325 anger, 2, 98, 113, 119, 121 angina, xiv, 126, 178, 191, 287, 289, 290, 292 angiography, 234, 280 angioplasty, 235 angiotensin converting enzyme, 272 angiotensin II, 78, 90 angiotensin receptor blockers, 205 animal models, 7, 83, 109, 321 animals, 6, 74, 88, 295 annihilation, 2 annotation, 151 annual rate, 150 ANOVA, 206, 245 ANS, 75 anthropology, 68, 72 antibody, 206 anticholinergic, 190 anticoagulant, 142, 143, 149, 155 anticoagulation, x, 137, 142, 143, 150, 152, 153,
154, 158, 188, 192, 291, 292, 293, 294, 308, 314, 315, 319
antidepressant, 45 antigen, 206 anxiety, 2, 45, 57, 100, 113, 117, 132 anxiety disorder, 45 aorta, 141, 147, 244, 253, 254, 255, 256, 285 aortic stenosis, 280 apnea, 219 apoptosis, ix, 74, 79, 90 appetite, 117 Argentina, 195 argument, 62 arithmetic, 245, 250, 251 arousal, x, 93, 95, 97, 98, 117 arrest, 57, 63, 147 arrhythmia, vii, ix, x, xi, xiii, x xv, 2, 7, 9, 28, 30,
83, 89, 90, 93, 94, 95, 96, 97, 98, 99, 100, 101, 103, 104, 105, 106, 108, 109, 111, 112, 113, 115, 116, 117, 118, 120, 122, 123, 130, 133, 135, 151, 152, 160, 164, 169, 174, 179, 180, 181, 182, 184, 186, 187, 188, 194, 196, 200, 218, 223, 287, 288, 289, 290, 292, 295, 296, 304, 306, 308, 309, 311, 312
arterial hypertension, 111, 234, 271, 272 arteries, 234, 239, 271 arteriosclerosis, 147 artery, xi, 83, 86, 97, 120, 125, 138, 141, 153, 167,
173, 197, 200, 201, 234, 235, 242, 244, 280, 297 ash, 108 assessment, 79, 81, 134, 157, 172, 179, 181, 191,
237, 245, 249, 250, 251, 252, 254, 259, 268, 281, 282
asymptomatic, xi, 87, 130, 139, 141, 152, 155, 159, 160, 161, 162, 163, 164, 166, 167, 168, 169, 170, 171, 172, 173, 174, 194, 195, 200, 211
atherosclerosis, 113, 129, 140, 254, 290 atherosclerotic plaque, 135 athletes, 169, 173, 279 atmospheric pressure, x, 93, 109, 110, 118, 130 atria, vii, xiii, 6, 9, 10, 20, 28, 75, 76, 84, 147, 204,
231, 232, 233, 235, 236, 273, 278, 289, 290 atrial fibrillation, x, xi, xii, 12, 29, 30, 31, 89, 101,
115, 123, 134, 137, 138, 139, 140, 141, 142, 144, 147, 148, 149, 150, 152, 153, 154, 155, 156, 157, 158, 159, 160, 161, 163, 164, 166, 167, 168, 169, 171, 173, 174, 178, 181, 190, 191, 192, 199, 200, 201, 203, 204, 213, 214, 233, 235, 265, 279, 288, 290, 294, 295, 311, 312, 313, 314, 315, 316, 317, 318, 319, 320, 321, 322, 323, 324, 325, 326
atrial flutter, x 12, 19, 20, 30, 199, 213, 287, 290, 292, 295, 303, 304, 305, 306, 307, 309, 313, 316, 317, 322, 323
atrial natriuretic peptide, 141, 148 atrial septal defect, 153 atrioventricular block, 8, 157, 162, 167, 169, 173 atrioventricular node, 75 atrium, 12, 15, 18, 23, 24, 74, 140, 146, 147, 152,
204, 213, 232, 233, 235, 236, 239, 242, 246, 279 atrophy, 225, 226, 228, 229 attention, 56, 62, 72, 113, 185, 245, 304 attitudes, 59 Australia, 1, 33, 39, 65, 67, 129 Austria, 177 authenticity, 65 authority, 65 autoimmune disease, 193 automaticity, ix, 11, 12, 28, 30, 74, 99, 179, 194 autonomic activity, 75, 80 autonomic nervous system, ix, 5, 11, 73, 74, 75, 79,
80, 82, 88, 89, 90, 91, 92, 96, 100, 106, 115, 134, 218, 219, 221, 226, 227, 229, 230
autonomic neuropathy, 86, 87, 92 autonomic pathways, xiii, 88, 218, 224

Index 329
autonomy, 59, 71 autopsy, 105 availability, 66, 77 averaging, 238 awareness, ix, 53, 55, 63, 65, 93
B
baroreceptor, 81, 82, 112, 225, 227 barriers, 53, 60, 79 batteries, 296 BD, 119, 128, 171 behavior, 13, 15, 26, 27, 84, 92, 109, 113, 115, 130,
135, 226, 239 beliefs, 66, 67 beneficial effect, 110, 114, 182, 186, 189, 204, 309 benign, vii, 111, 118, 161, 170 beta blocker, 182, 183, 184, 190, 191, 192 beverages, x, 93 bias, 214, 219 binge drinking, 102, 116 biochemistry, 204, 213 biological systems, 5 birth, 131 black hole, 59 bladder, 218 blame, 61 bleeding, 142, 143, 144 blocks, 243, 290 blood, vii, xii, xiii, 9, 10, 48, 49, 56, 78, 82, 95, 97,
99, 101, 102, 103, 104, 108, 109, 112, 115, 117, 120, 123, 129, 130, 131, 135, 142, 148, 153, 203, 204, 206, 217, 220, 221, 223, 224, 226, 227, 232, 233, 234, 236, 237, 238, 239, 240, 244, 247, 248, 250, 254, 256, 257, 263, 271, 273, 274, 275, 276, 278, 281, 296, 304, 305
blood flow, 99, 104, 109, 148, 153, 233, 239, 248 blood pressure, xiii, 49, 56, 78, 82, 95, 99, 101, 102,
103, 108, 110, 112, 115, 117, 120, 123, 130, 131, 135, 217, 220, 221, 223, 224, 226, 227, 232, 234, 237, 238, 240, 244, 247, 248, 250, 254, 256, 257, 263, 271, 273, 274, 275, 276, 278, 281, 305
blood vessels, 142 body weight, 263, 271, 273, 274, 275, 276, 278, 320 bonds, 45 bone marrow, 7 bradyarrhythmia, 191, 200, 296 bradycardia, vii, 11, 103, 144, 146, 147, 152, 153,
157, 180, 271, 306 bradykinesia, 218, 219
brain, xi, xii, 49, 76, 86, 88, 120, 138, 142, 143, 153, 158, 203, 204, 214, 218, 254, 289
brain stem, 86 brainstem, 88 breathing, 56, 81, 108, 214, 222, 248, 249, 253, 254 Britain, 139 buffer, xiii, 217, 221 bundle branch block, 130 burn, 309 bypass graft, 197
C
cadaver, 39 caffeine, x, 93, 101, 102, 112, 123 calcification, 140, 147 calcium, 77, 79, 83, 87, 99, 104, 112, 114, 116, 131,
178, 184, 191, 205, 272, 293, 305 calcium channel blocker, 184, 191, 272 Canada, 194 cancer, 63, 68, 70 candidates, x 287, 303, 307 cannabis, 104, 105, 125, 126 capillary, 148, 233, 240, 273 carbon, x, 93, 105, 106 carbon monoxide, x, 93, 105, 106 carboxyhemoglobin level, 105 cardiac activity, 87 cardiac arrest, 46, 49, 57, 61, 62, 98, 103, 124, 127,
161, 184, 186, 187, 189, 198, 199, 295 cardiac arrhythmia, vii, ix, x, 1, 2, 9, 11, 20, 28, 35,
36, 65, 66, 74, 78, 86, 87, 89, 91, 93, 94, 95, 96, 97, 98, 100, 104, 106, 108, 110, 111, 115, 117, 118, 119, 123, 127, 137, 198, 223, 224, 295
cardiac catheterization, 175 cardiac muscle, 120, 194 cardiac myocytes, 77, 87, 90, 128 cardiac operations, 199 cardiac output, xiii, x 84, 85, 109, 147, 148, 231,
232, 234, 237, 240, 241, 273, 278, 281, 284, 285, 297
cardiac pacemaker, vii, viii, 9, 10, 11, 81 cardiac risk, 229 cardiac surgery, 140, 153, 191, 192, 194, 201, 319,
324 cardiac tamponade, 167 cardiologist, 39, 43, 45, 57, 58, 59, 60, 61, 62, 63,
64, 66, 245, 303, 311 cardiomyopathy, x 35, 79, 86, 90, 92, 97, 99, 102,
121, 124, 184, 204, 287, 288, 289, 305, 312

Index 330
cardiovascular disease, 81, 85, 92, 105, 108, 109, 111, 113, 115, 123, 126, 132, 133, 223
cardiovascular function, 86, 214 cardiovascular morbidity, 106 cardiovascular risk, 101, 102, 155 cardiovascular system, ix, 74, 75, 76, 82, 88, 112,
123, 125, 134 carotid sinus, 272 cast, 63 catecholamines, 84, 124, 224 catharsis, 39 catheter, 50, 162, 166, 167, 168, 170, 172, 173, 174,
183, 187, 244, 254, 258, 304, 316 catheters, 7, 304 causal relationship, 103 CE, 89, 135, 174, 199 cell, 6, 7, 8, 12, 15, 74, 76, 77, 78, 79, 97, 129, 132,
218 cell death, 79 central nervous system, 75 cerebral cortex, 76 cerebral hemisphere, 86, 91 cerebrovascular disease, x, 129, 137, 140, 141, 142,
149 certainty, 53 channels, xii, 74, 76, 77, 79, 83, 87, 104, 108, 116,
125, 177, 178, 179, 194 chaos, 81 chemical composition, 108 chest radiography, 141 childhood, 52 children, xi, 46, 49, 50, 51, 69, 160, 163, 164, 167,
168, 169, 171, 172, 173, 174 chloroform, 74, 88 cholesterol, 117, 129, 135 chronobiology, 96, 115 cigarette smoking, 103, 125 circadian rhythm, 81, 134, 227 circadian rhythms, 134 circulation, 129, 153, 241, 246, 296 classification, 42, 178, 288, 314 claustrophobic, 55 clinical depression, 135 clinical diagnosis, 228 clinical disorders, 227 clinical examination, 205 clinical presentation, 171 clinical symptoms, 220 clinical trials, x, 2, 25, 35, 138, 142, 144, 149, 153,
156, 180, 184, 195, 313
closure, 153, 154, 158, 232, 233, 279 clusters, 117, 135 coagulation, 292, 313 cocaine, 103, 104, 124, 125 cocaine use, 104, 124 codes, 6, 146 coding, 91 coffee, 101, 102, 103, 116, 118, 122, 123 cognitive ability, 1 cognitive impairment, 219 cohort, 170, 226, 284 collaboration, 64 collateral, vii, 3 collateral damage, vii, 3 coma, 45, 46 combination therapy, 184 combined effect, 14, 218 combustion, 105 communication, 1, 247 community, 70, 204, 226, 291, 309, 311 comorbidity, 140 compassion, 61 compensation, 238, 302 competition, 113 complex interactions, 81 complexity, viii, 1, 2, 9, 11, 20, 35, 100, 106, 111,
223, 311 compliance, 141, 254 complications, x 87, 124, 144, 151, 168, 169, 180,
193, 218, 287, 289, 290, 291, 292, 304, 310, 313 components, 5, 11, 30, 78, 90, 97, 105, 107, 108,
110, 127, 237, 241 compounds, 105 comprehension, 103 computation, 246 computed tomography, 142, 221 computing, 81 concentration, 75, 98, 103, 104, 106, 108, 117, 121,
179, 205, 214 conception, 235 concrete, 27 conduction, vii, viii, xi, 5, 9, 10, 11, 12, 14, 15, 16,
18, 19, 20, 21, 24, 27, 28, 29, 30, 31, 79, 83, 102, 125, 145, 148, 150, 157, 159, 161, 162, 163, 164, 168, 169, 172, 178, 179, 191, 242, 265, 271, 273, 276, 277, 278, 279, 281, 283, 289, 293, 295, 296, 312, 317
conductivity, 28, 289 conductor, 11, 15, 27, 296 confidence, 144, 219

Index 331
confidence interval, 144 configuration, 16, 24, 245, 326 conflict, 47, 51 confrontation, 52 confusion, 38, 142, 220 congestive heart failure, 91, 122, 127, 138, 140, 141,
145, 147, 181, 185, 190, 194, 195, 200, 213, 242 consciousness, 36, 38, 54, 56, 57, 304 consensus, 2, 67, 70 consent, 1, 304 constant rate, 244 constipation, 218, 219 constraints, 65 construction, 238, 249 consumers, 35 consumption, 101, 102, 103, 116, 122, 124 control, vii, ix, xi, xiii, x 2, 5, 6, 9, 26, 27, 28, 31, 39,
46, 51, 55, 56, 57, 60, 66, 67, 74, 76, 78, 80, 82, 84, 86, 87, 88, 89, 98, 106, 108, 113, 122, 128, 131, 132, 140, 142, 159, 161, 162, 163, 165, 167, 182, 183, 184, 185, 188, 189, 190, 192, 193, 198, 201, 217, 218, 221, 223, 225, 229, 230, 235, 244, 279, 287, 290, 291, 292, 293, 294, 295, 307, 309, 310, 315, 316, 317, 318, 320, 323, 324
control group, xiii, 167, 189, 217, 218, 223, 225, 235, 292
controlled studies, 185, 189 controlled trials, 142, 156, 180, 185, 188, 190, 197,
313 conversion, 181, 189, 190, 192, 199, 213, 293, 317,
322 conversion rate, 189, 317 conviction, 47 convulsion, 57 copper, 105 cor pulmonale, 305 coronary angioplasty, 280 coronary arteries, 75, 97 coronary artery bypass graft, 105, 191 coronary artery disease, ix, 74, 82, 83, 113, 129,
132, 140, 141, 180, 197, 227, 291 coronary heart disease, ix, xii, 74, 82, 102, 104, 113,
123, 129, 130, 132, 203, 223, 271 correlation, xiii, 20, 82, 110, 113, 122, 134, 218,
224, 241, 289 correlation analysis, 241 correlation coefficient, 241 correlations, 106 cortex, 86 costs, 142, 325
counseling, 64, 66, 71 coupling, 18, 85, 152 covering, 54, 153 creatinine, 205 critical value, 265, 267 Croatia, 93 crossing over, 54 cultural beliefs, 65 cultural influence, 40 cultural perspective, 35 culture, 40, 46, 66 cycles, 21, 23, 26, 138, 236 cyclic AMP, 76 cytokines, 106, 116, 128
D
danger, 123 database, 61 death rate, 209 deaths, 84, 92, 109, 110, 118, 129, 166, 167, 168,
181, 225 decay, 77 decision making, 179, 215 decisions, 67, 200 decomposition, 82 defects, 86, 157 defibrillation, 57, 58, 69, 189, 295, 297, 299, 300,
301, 302, 304, 308, 320, 321, 322, 323 defibrillator, xii, 35, 47, 57, 67, 70, 71, 98, 100, 106,
133, 135, 162, 177, 183, 185, 186, 195, 196, 197, 198, 296, 297, 298, 304, 308, 309, 321
definition, 46, 102, 221, 225, 228, 233, 235 degenerate, 78 dehydration, 109, 275, 278 delivery, 6, 7, 14, 66, 145, 236, 308 demand, 11, 14, 78, 280 dementia, 142 denial, 3 density, 77, 84, 109, 113, 255, 257, 296, 308, 312 Department of Health and Human Services, 69 depolarization, 5, 10, 12, 13, 21, 106, 146, 178, 194,
289 deposition, 108 deposits, 310 depression, x 2, 43, 44, 45, 100, 113, 117, 132, 135,
219, 223, 288 depressive symptoms, 132 deprivation, 2, 54 derivatives, 8

Index 332
desensitization, 85 desires, 54 destruction, 2, 57 desynchronization, 185 detachment, 42 detection, 150, 151, 152, 184, 212, 249, 254, 296 diabetes, 86, 87, 92, 97, 107, 111, 138, 140, 141,
142, 150, 271 diabetes mellitus, 86, 92, 138, 142, 271 diabetic neuropathy, ix, 74, 82, 92 diabetic patients, 87, 92 diastole, 99, 232, 233, 236, 237, 239, 253, 279 diastolic blood pressure, 99, 221, 263, 273, 274 diastolic pressure, 221, 278, 279 diet, 102 dietary iodine, 192 differential diagnosis, 181, 226, 228 differentiation, xii, 217, 221, 229 diffusion, 108 dilated cardiomyopathy, 79, 85, 91, 129, 182, 312 dilation, 213, 232, 271 direct action, 77 disability, 68, 143, 223 discharges, xii, 177, 193, 300, 322 discomfort, 65 discourse, 69 disease progression, 223 disorder, 5, 11, 99, 140, 156, 218, 225 dispersion, ix, 74, 79, 83, 87, 92, 115, 120, 134, 152,
169, 181 dissociation, 11 distress, 42, 49, 57, 61 distribution, x, 12, 20, 21, 85, 88, 94, 113, 115, 127,
135, 154, 179, 245, 257, 258, 273 diuretic, 271, 272, 273, 274, 275, 276, 278, 286 dizziness, 147, 218, 219 DNA, 7 doctors, 43, 46, 72, 218 dogs, 75, 88, 102, 103, 108, 211, 232, 233, 240, 242,
320 dominance, 2 donors, 71 DOP, 25, 26 dopamine, 76, 103, 218, 225, 228, 230 dopamine agonist, 218, 225, 228, 230 dopaminergic, 218 dosing, 144 double-blind trial, 181 down-regulation, 85 dream, 39
drug interaction, 144, 183 drug therapy, 59, 181, 184, 186, 190, 194, 195, 196,
198, 295 drug treatment, 182, 191, 195 drug use, 195 drugs, xi, x 28, 31, 80, 104, 114, 167, 168, 169, 171,
177, 178, 179, 180, 182, 183, 184, 185, 186, 187, 188, 189, 190, 191, 193, 201, 206, 212, 219, 222, 225, 243, 287, 289, 291, 292, 293, 295, 296, 303, 305, 307, 309, 310, 311, 318
duration, xiii, 6, 77, 79, 83, 104, 108, 112, 115, 139, 148, 152, 157, 162, 163, 164, 178, 191, 217, 220, 223, 229, 291, 293, 298, 302, 303, 308, 320, 321
dyspnea, 181, 191, 205, 212, 289 dystonia, 219
E
earth, 45 echocardiogram, 292 education, viii, 1, 34, 64, 151 Education, 284 educators, 66 Egypt, 137 elasticity, 235 elderly, xi, 70, 101, 111, 118, 127, 129, 138, 140,
143, 148, 154, 155, 157, 158, 160, 164, 166, 168, 169, 174, 191, 200, 219, 284, 292, 311
elderly population, 155 electric charge, 297 electric current, 296, 297 electrical properties, 12, 28, 89, 128, 134 electrical resistance, 296, 303 electricity, 295, 296, 297, 308 electrocardiogram, ix, 10, 29, 73, 80, 87, 99, 120,
122, 154, 170, 173, 205 electrodes, xv, 146, 245, 288, 296, 297, 298, 304,
306, 308, 309, 322 electrolyte, 97, 99, 102, 191 electrolyte imbalance, 191 electromagnetic, 2 emboli, x, xi, 138, 140, 153 embolism, 142, 155, 156, 289 embolization, xi, 138 embryoid bodies, 6 embryonic stem cells, 7 emission, 146, 221 emotion, 41, 48, 50, 80 emotional distress, 98 emotional state, 74, 94

Index 333
emotionality, viii, 34, 36, 57 empathy, 61, 63 encoding, 6 endocardium, 113 endurance, 279 energy, xv, 11, 47, 101, 167, 187, 232, 288, 295,
296, 297, 298, 299, 302, 304, 306, 308, 309, 322, 323, 326
engagement, 38, 52, 53, 56, 58, 59, 60, 61, 62, 63 England, 5 enlargement, 79, 142, 211, 214, 282 enrollment, 188, 243 entrapment, 2 entropy, 82 environment, 28, 34, 47, 95, 109, 117, 118, 222, 238 environment control, 223 environmental conditions, 220 environmental factors, x, 93, 96, 111 environmental influences, 95, 115 enzyme inhibitors, 205, 318 enzymes, 144, 310 epicardium, 75, 113 epidemiologic studies, 204 epidemiology, 140, 155 epinephrine, ix, 73, 120 epistemology, 36, 61 equipment, 237, 243, 304 erosion, 2 erythrocyte membranes, 193 estrogen, 112, 131 ethanol, 124 ethics, 243, 271 ethnicity, 140 etiology, 113 Europe, 129, 178 European Union, 288 evaporation, 110 evil, 40, 44, 45 evolution, 131, 173, 212, 283, 306 examinations, 245, 268 excision, xi, 138, 153 excitability, 77, 83 excitation, 20, 174, 194, 236 exclusion, xi, 138, 153, 244, 249, 254, 273 excretion, 117 exercise, ix, xi, 30, 74, 81, 85, 87, 88, 91, 98, 100,
111, 112, 119, 120, 130, 135, 144, 159, 162, 166, 167, 170, 171, 173, 190, 205, 230, 240, 253, 280, 281, 282, 283, 316
exercise performance, 282, 316
exertion, 100, 122, 147, 205 exports, 247 exposure, x, 84, 87, 94, 95, 106, 107, 108, 109, 111,
117, 118, 123, 126, 127, 128, 129, 167, 169 external influences, 94 external shocks, 295 extinction, 14 extrapolation, 242 eyes, 54
F
fabric, 52 facilitators, 71 failure, xii, xiii, xv, 6, 7, 35, 59, 60, 84, 85, 147, 167,
168, 184, 186, 188, 195, 214, 217, 218, 223, 224, 225, 226, 227, 228, 229, 230, 235, 237, 273, 288, 289
faith, 58 false positive, 162 false positive tests, 162 family, viii, 6, 33, 34, 35, 36, 37, 43, 47, 48, 49, 51,
52, 58, 63, 64, 65, 66, 67, 68, 69, 102, 123, 151, 213
family history, 102, 123 family members, viii, 33, 34, 35, 36, 37, 47, 51, 52,
58, 63, 64, 65, 66, 67 family support, 151 fasting, 293, 304 fat, 75, 76, 133 fatal arrhythmia, 102, 114, 117, 118 fatigue, 147, 205 fatty acids, 114, 132, 133, 294, 319 FDA, 35, 69 fear, 2, 41, 43, 52, 53, 66 fears, 34 feedback, 1, 81, 89 feelings, 42, 57 females, 112 feminism, 69 fever, 161 fibers, 10, 75, 78, 83, 90, 105 fibrillation, ix, x, x 20, 30, 31, 73, 78, 98, 101, 103,
104, 119, 130, 134, 138, 139, 140, 141, 144, 148, 150, 152, 154, 155, 161, 162, 163, 166, 168, 170, 171, 174, 184, 191, 199, 200, 279, 287, 288, 312, 313, 314, 315, 317, 319, 320
fibrosis, ix, 74, 78, 79, 97, 204, 310 film, 37, 41, 62 films, 68

Index 334
filtration, 158, 239, 253 fires, 13 firms, 239 fish, 114, 133 fish oil, 114 fixed rate, 25, 26, 280 flame, 54 fluctuations, ix, 30, 73, 80, 81, 82 fluid, 271, 272, 273, 274, 275, 276, 278, 286, 306 food, 117 foramen, 153 forebrain, 75 fossil, 105 fractal analysis, 82, 84 fractal dimension, 226 France, 159 freedom, 56 freezing, 51 frustration, 65, 66 fuel, 105 funding, 3 fusion, 14, 16, 24, 38
G
ganglion, 76, 87 gases, 105 gel, 296, 308 gender, viii, 34, 51, 101, 112, 113, 130, 131, 140,
154, 181, 225, 243, 254, 263, 291 gender differences, 112, 131 gender gap, 112 gene, 6, 7, 8, 79, 85, 91, 122, 127, 134 gene expression, 79, 127, 134 gene therapy, 7 gene transfer, 6, 8 general anesthesia, 153, 168 generation, 77, 79, 135, 154 genes, 85, 115, 140 genetic code, 41, 70 genetic disorders, 96 genetic factors, 115 genetics, 155 genotype, 91 Germany, 127, 153, 217, 220 gift, 46 gland, 193 glass, 45, 104 glasses, 102 global trends, 35
glucocorticoids, 193 goals, 63 God, 38 goiter, 193 grants, 278 graph, 250, 251, 255, 256, 257, 259, 261, 262, 264,
266, 267, 268, 275 grass, 46 Great Britain, 237 Greece, 110, 203 groups, viii, x, 6, 10, 33, 64, 67, 78, 93, 101, 117,
206, 208, 209, 212, 273, 277 growth, 178 guidance, 67, 188 guidelines, x, 114, 133, 137, 143, 150, 154, 157,
182, 184, 185, 187, 189, 190, 192, 193, 196, 200, 307, 308, 324
H
haemostasis, 140 half-life, 178, 310 hands, 54 happiness, 40 harm, 7, 35, 50, 51, 183 harmony, 51 harvesting, 46 hate, 40, 43, 45 hazards, xii, 2, 35, 64, 68, 203, 207, 211 HE, 30, 92, 121, 125, 127, 128, 129, 134 healing, 69, 123 health, viii, 1, 33, 34, 42, 48, 49, 50, 52, 56, 63, 64,
65, 66, 68, 89, 111, 126, 129, 226 health care, 63 health care system, 63 health effects, 129 heart block, vii, 7, 9, 147, 279, 280, 281, 306 heart disease, ix, x 71, 74, 83, 84, 91, 93, 96, 97,
100, 101, 102, 107, 112, 118, 128, 132, 133, 141, 145, 147, 148, 161, 164, 180, 184, 190, 191, 207, 224, 226, 227, 228, 229, 230, 288, 293, 294, 305, 306, 307, 309, 312, 317
heart failure, ix, xii, x 35, 74, 79, 82, 84, 85, 90, 91, 105, 111, 114, 118, 133, 141, 155, 157, 181, 182, 188, 189, 190, 191, 195, 196, 197, 198, 199, 203, 204, 211, 213, 214, 225, 233, 235, 237, 240, 282, 283, 287, 289, 290, 291
heart rate, vii, ix, xii, 5, 6, 9, 11, 12, 17, 18, 30, 73, 76, 78, 80, 81, 82, 83, 84, 85, 86, 87, 90, 91, 92, 95, 98, 99, 100, 103, 104, 106, 107, 108, 110,

Index 335
112, 113, 125, 128, 130, 131, 132, 134, 179, 180, 185, 189, 191, 217, 220, 221, 222, 223, 225, 227, 228, 229, 230, 234, 236, 237, 238, 239, 240, 242, 250, 254, 276, 278, 284, 289, 290, 316
heart rate (HR), 82 heart valves, 291 heat, 129 heavy drinking, 102 hemodialysis, 243, 286 hemoglobin, 238 hemorrhage, 142, 143 hepatotoxicity, 310 heterogeneity, ix, 74, 83, 98, 273 high blood pressure, 142 hip, 218 histogram, 20, 22 histology, 204 homeostasis, 75, 110, 117 homocysteine, 97 hormone, 112, 114, 121, 131, 181, 193, 201 hospice, 68 hospitalization, 110, 126, 127, 187, 190, 204, 205,
206, 209, 211, 212 host, 183 hostility, 113 House, 68 human dignity, 67 human embryonic stem cells, 8 human experience, 37 human genome, 70 human subjects, 30, 80, 125, 240 humanism, 63 humanistic perspective, 2 husband, 49 hybrid, 38, 39, 40, 41, 42 hybridity, 72 hyperactivity, 84, 222, 223 hyperlipidemia, 97, 111 hypersensitivity, 224, 243 hypertension, 97, 107, 111, 117, 123, 135, 140, 141,
142, 145, 150, 190, 281, 286, 288 hyperthyroidism, 181, 288, 310 hypertrophic cardiomyopathy, 235, 282, 289, 294,
312 hypertrophy, ix, 74, 79, 83, 90, 181, 204, 227, 271,
272, 273, 275 hypokalemia, 99 hypomagnesemia, 181 hypotension, xii, 109, 217, 218, 221, 224, 292, 304,
306, 310
hypotensive, 199 hypothalamus, 74, 75, 76, 86, 218 hypothesis, 6, 76, 100, 124, 204, 223, 232, 238, 276,
289 hypothyroidism, 192, 310 hypoxia, 141 hysteresis, 15
I
iatrogenic, 169 ICD, viii, xii, 1, 2, 33, 34, 35, 36, 37, 38, 40, 41, 42,
43, 44, 46, 47, 48, 49, 50, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 119, 177, 182, 183, 184, 186, 187, 188, 193
identity, 45, 50 ideology, 36 idiopathic, 91, 112, 129, 187, 219, 228, 229, 312 illusion, 35, 41 images, 39 imagination, 34, 46 imaging, 122, 221, 234, 279 immune system, 69 implants, 147 implementation, 17, 28 in vitro, 76 in vivo, 6, 8, 76, 153 incidence, x, xi, xii, 26, 35, 67, 82, 86, 87, 94, 96,
102, 112, 127, 130, 135, 137, 139, 140, 142, 145, 149, 150, 152, 155, 159, 164, 180, 191, 192, 194, 196, 203, 211, 212, 213, 312, 322
inclusion, 66, 114, 226 income, 2 indeterminacy, 34 indication, 144, 149, 153, 166, 167, 169, 170, 184,
293 indices, 241 indirect effect, 100 induction, xi, x 6, 148, 159, 163, 164, 165, 166, 168,
169, 288, 299, 305, 310 inductor, 300 industry, 3, 35, 153 inertia, 241 infancy, 166 infarction, 82, 83, 86, 91, 99, 100, 129, 155, 182,
187, 197 infection, 2, 6, 42, 293 inferior vena cava, 290 inflammation, 97, 106, 108, 141, 294, 318 informed consent, viii, 1, 34, 64, 204, 243, 271

Index 336
ingestion, 94, 101, 102, 124 inhibition, xii, 76, 81, 124, 125, 177, 179, 318, 319 inhibitor, 305 initiation, ix, 17, 79, 93, 95, 106, 115, 118, 130, 140,
194, 289 injections, 53 injuries, 83 innovation, 2, 35 inositol, 77 input, 11, 15, 75, 107 insertion, 5 insight, 37, 47, 65, 115 instability, 98, 108, 117, 118, 187, 223 instruments, xi, 138, 153 insulin, 87 integration, 8 integrity, 42, 87, 221 intensity, 97, 103, 108, 111, 143, 156, 238, 291, 313 intensive care unit, x 45, 237, 287 intentionality, 36 interaction, 11, 36, 37, 48, 66, 76, 114, 182, 191, 195 interactions, 15, 23, 27, 74, 76, 77, 88, 89, 96, 111,
133 interface, 308 interference, 2, 148, 304 interleukine, 117 interpersonal communication, 94 interpretation, viii, 33, 37, 38, 58, 76, 81, 90, 116,
142, 164, 223, 225, 241, 292, 310 interrelations, 106, 115 interval, 14, 19, 20, 21, 23, 29, 79, 81, 83, 87, 92, 98,
104, 115, 120, 125, 146, 148, 163, 179, 185, 191, 219, 226, 230, 235, 236, 239, 240, 241, 246, 264, 268, 277, 284, 322
intervention, xi, 2, 63, 67, 138, 153, 241, 260, 263, 272, 273, 315
intoxication, 123, 124 intra-aortic balloon pump, 188 intravenously, 317 iodine, 192, 193, 201, 229 ion channels, ix, 73, 89, 108, 113, 114, 204 ions, 108 iron, 105 irradiation, 238 ischaemic heart disease, 120, 124, 129, 132 ischemia, 87, 97, 104, 105, 108, 148, 187, 196, 225,
280, 289 ischemic stroke, x, 86, 92, 137, 140, 143, 150, 157,
290, 313, 314 isolation, 117, 319
isotope, 234, 245, 253 Israel, 156 Italy, 71, 73, 137, 153 iteration, 152
J
Japan, 178 justice, 70
K
K+, 87, 134 kidney, 45 kinetics, 77 knees, 48
L
land, 42, 260 language, 37, 38, 52 latency, 221 Latin America, 178 laughing, 45 laughter, 39 leadership, 311 leaks, 211 left atrium, 162, 232, 233, 234, 235, 239, 273, 279 left ventricle, xiii, 83, 231, 232, 233, 234, 235, 239,
242, 243, 245, 253, 254, 263, 271, 272, 273, 275, 276, 277, 289
legislation, 35 leisure, 135 leisure time, 135 lens, 64 lesions, 97, 108, 153 lethargy, 151 levodopa, 229 LIFE, 319 life span, 112 lifespan, 35 lifestyle, 2, 45, 113, 140 lifetime, 6 likelihood, 97, 98, 103, 109, 110, 111, 114, 139, 183,
293 limitation, 64, 152, 187, 241, 253 linkage, 48, 49, 51, 100 links, 27, 74 lipids, 102, 132

Index 337
liver, 180, 183, 310 liver enzymes, 310 localization, 86, 92 location, 5, 53, 79, 122, 161, 166, 167, 168, 169,
187, 282 locus, 218 longevity, 151, 184 longitudinal study, 312 loss of consciousness, 310 love, 44 low risk, 155, 169, 187 low temperatures, 127 lying, 47, 54, 147
M
machinery, 39 magnesium, 99, 191 magnet, 244 major depression, 227 males, 112 malignancy, 7, 205 management, xii, 2, 28, 114, 138, 150, 173, 177,
179, 181, 182, 183, 186, 188, 189, 192, 193, 196, 197, 198, 200, 201, 207, 214, 225, 227, 290, 291, 292, 293, 310, 311, 315, 324
manipulation, 6, 240 manufacturing, 153 mapping, 6, 162, 292, 307, 312 marijuana, 103, 104, 105, 126 market, 178 mathematics, 238 matrix, 7 meanings, 36, 37, 57 measurement, 90, 163, 181, 207, 223, 225, 234, 236,
241, 244, 246, 247, 248, 249, 250, 251, 252, 253, 254, 261, 262, 263, 264, 268, 276, 281, 284, 285
measures, x, 80, 83, 86, 91, 94, 108, 223, 238 mechanical ventilator, 188 median, xiii, 139, 232, 245, 258, 262, 274, 277, 305 mediastinum, 224 Medicare, 158 medication, 1, 58, 60, 68, 151, 180, 190, 191, 263,
271, 272, 291, 293, 294, 303, 305, 307 medulla, 76 memory, 42, 219 memory loss, 42 men, xii, 42, 64, 100, 101, 102, 112, 113, 114, 116,
118, 122, 124, 130, 132, 140, 203, 204, 207, 254 mental activity, 130
mercury, 244 Merleau-Ponty, 36, 37, 43, 47, 49, 54, 71 mesenchymal stem cells, 7 meta-analysis, 116, 123, 134, 135, 156, 180, 181,
182, 188, 195, 198, 201, 292, 294, 313, 314, 316, 317, 318, 324
metabolic changes, 99, 100 metabolic syndrome, 138, 141 metabolism, 116 metal oxides, 105 metaphor, 45, 48, 54 mice, 78, 90 microcirculation, 105 migration, xi, 138 military, 170 minority, 3 mitral regurgitation, 148, 237 mitral stenosis, 240 mitral valve, 101, 192, 214, 239, 280, 284 mitral valve prolapse, 101 mixing, 40 mobility, 237 modeling, 15, 28, 29 models, 7, 94, 101, 185, 247 modernity, 69 modules, 27 moisture, x, 93, 110 molecular biology, 77 molecular mechanisms, 123 molecular weight, 291 monoclonal antibody, 206 mood, 110, 117, 135 mood change, 110, 135 Moon, 322 moral development, 70 morbidity, x 2, 82, 128, 138, 144, 188, 191, 287, 289 morning, x, 1, 94, 96, 114, 115, 134, 220, 263 morphology, 98, 108, 119, 187, 289, 299, 300, 302 mortality, xiii, 43, 45, 62, 63, 64, 70, 82, 83, 84, 85,
87, 90, 92, 102, 105, 106, 111, 126, 128, 129, 135, 138, 149, 155, 180, 181, 182, 184, 186, 188, 189, 190, 191, 194, 195, 197, 204, 206, 218, 223, 224, 226, 292
mortality rate, 84, 186, 204 mortality risk, 85 motion, 284 motives, 219 motor control, 78 motor function, 223 mouse model, 78

Index 338
movement, viii, 34, 37, 220, 253, 310 movement disorders, 220 MRI, 280 multiplicity, 106, 185 muscle cells, 6 muscles, 99, 223 mutation, 100 myocardial infarction, 82, 83, 87, 88, 90, 91, 94, 97,
99, 100, 101, 102, 103, 104, 105, 109, 110, 113, 114, 118, 121, 122, 123, 124, 126, 127, 129, 132, 135, 181, 182, 185, 188, 194, 195, 196, 197, 198, 200, 205, 207, 208, 226, 229, 234, 240, 279, 281, 288
myocardial ischemia, 78, 88, 95, 99, 100, 104, 105, 108, 119, 125
myocardial necrosis, 82, 86, 308 myocardium, vii, ix, 7, 9, 10, 73, 74, 75, 83, 96, 97,
102, 104, 108, 110, 115, 117, 118, 232, 233, 235, 236, 240, 278, 296, 297, 298, 299, 320
myoclonus, 304 myocyte, 79, 87, 108, 114, 204 myoglobin, 323
N
naming, 38 necrosis, 128, 132, 322 needles, 7 negative emotions, 132 negotiating, 60 negotiation, viii, 34, 64, 65, 66, 67 nerve, ix, xiii, 30, 74, 75, 76, 80, 81, 83, 84, 85, 87,
91, 131, 217, 218, 225 nerve fibers, 83 nerves, ix, 73, 75, 76, 82, 88, 180 nervous system, ix, 73, 74, 75, 76, 78, 80, 89, 117,
218, 226, 227, 228, 229, 233 Netherlands, 220 network, 10, 75, 100 neural mechanisms, 29 neuroendocrine, 204, 213 neurohormonal, 80, 120, 204, 279 neurons, xii, 75, 76, 78, 89, 217, 218 neuropathic pain, 130 neuropathy, 87, 92, 181 neuroprotective, 219 neurotensin, 89 neurotransmitter, 76, 121 neurotransmitters, ix, 73, 76, 83, 103, 224 New England, 68, 154
New South Wales, 39, 129 nickel, 105 nigrostriatal, 228 nitrates, 105 nitric oxide, 128 nitrogen, x, 93, 105, 106 nitrogen dioxide, x, 93, 105, 106 noise, 27 nonlinear dynamics, 15, 81, 90 norepinephrine, ix, 73, 76, 103, 117, 148, 221 normal aging, 282 normal distribution, 245, 260, 263 North America, 80, 90, 139, 146, 178, 193, 225 Norway, 105 nuclear magnetic resonance, 234 nuclei, 218 nucleus, 75, 81, 218 nucleus tractus solitarius, 75, 218 null hypothesis, 275 nurses, viii, 33, 36, 37, 50, 52, 53, 54, 56, 57, 58, 65,
66, 67, 68, 304 nursing, 50, 70
O
obesity, 141 observations, 21, 28, 56, 106, 114, 124, 229 obstruction, 235 obstructive sleep apnea, 141 occlusion, 86, 120, 125, 153, 158 oedema, 271 oil, 108 oils, 114 old age, 228 older adults, xi, 154, 160, 230 older people, 226, 235 omega-3, 132, 133, 319 open heart surgery, xi, 38, 138, 153 opiates, 310 optimization, x 151, 232, 236, 237, 240, 241, 243,
250, 266, 277, 282, 283 organ, 46, 71, 79, 194, 289 organism, 42, 110, 233 organization, 69 organizations, 150 orthostatic hypotension, xiii, 87, 218, 219, 221, 223,
224, 225, 228, 229, 230 ostium, 235 outpatients, xii, 61, 203, 204, 211, 293

Index 339
output, 11, 12, 15, 27, 148, 162, 234, 240, 273, 278, 298
overload, 212 overweight, 102 oxidative stress, 106, 135, 294 oxygen, 53, 78, 85, 99, 109, 130, 148, 237, 238, 283,
304 oxygen consumption, 85, 109, 148 oxyhemoglobin, 238 ozone, 105, 106
P
pacing, vii, viii, x, xiii, 5, 6, 7, 8, 9, 10, 11, 12, 14, 15, 18, 21, 24, 25, 26, 27, 28, 29, 30, 31, 56, 71, 138, 144, 145, 146, 147, 148, 149, 150, 152, 156, 157, 162, 163, 164, 169, 171, 173, 184, 187, 192, 197, 201, 214, 231, 232, 234, 235, 236, 237, 240, 241, 242, 243, 244, 245, 246, 248, 249, 250, 271, 274, 276, 279, 280, 281, 282, 283, 285, 292, 304, 306, 309, 311, 320, 323, 325
PACs, 152, 153 pain, 2, 34, 40, 41, 56, 57, 58, 151, 205, 219, 304,
305 palliative, 65, 68, 70 palliative care, 68, 70 palpitations, 102, 151, 164, 173, 205, 290 paralysis, 51 parameter, 20, 28, 223, 240, 277, 297 parasympathetic nervous system, 80, 105 parents, 51 parkinsonism, 219, 226, 228 paroxysmal supraventricular tachycardia, 154, 312 particle mass, x, 93, 105, 126 particles, 108, 126, 127, 128, 129, 206 particulate matter, 105, 106, 107, 108, 117, 127 partnership, 60 passive, 60, 232 paternalism, 60 pathogenesis, 101, 132, 153, 193 pathology, 44, 226, 228, 278, 292 pathophysiological cascade, 94 pathophysiological mechanisms, 108, 223 pathophysiology, 99, 129, 140, 279, 294 pathways, vii, 9, 75, 76, 77, 78, 106, 126, 161, 164,
167, 168, 170, 171, 172, 173, 174, 289 patient care, 69 peptides, 204 perception, 34, 43, 44, 53, 71, 110 perceptions, 53, 68
perchlorate, 193 perfusion, xi, 159, 238 pericarditis, 293 periodicity, 19, 29, 148 peripheral neuropathy, 180 permit, 36, 145 personal history, 272 personal life, 47, 52 personality, 100, 113, 132 persuasion, 58 pessimism, 113 pH, 87 phalanx, 220 pharmacokinetics, 103, 178, 193, 194 pharmacology, 55 pharmacotherapy, 188, 286 phenomenology, 36, 37 phenotype, 122, 229 phenytoin, 178 Philippines, 178 phobic anxiety, 113, 132 phosphorylation, 77, 84 photographs, 39 physical activity, ix, 81, 93, 94, 95, 98, 99, 100, 101,
103, 111, 113, 114, 117, 135, 240, 245, 253, 277 physical exercise, 222 physical stressors, 98 physiology, 59, 74, 109, 201, 215, 295 pigs, 6, 7, 8, 120 placebo, 126, 142, 180, 181, 182, 185, 189, 190,
193, 195, 199, 201 planning, 65 plaque, 78, 95, 97, 108, 119, 141 plasma, 77, 84, 86, 117, 121, 129, 179, 191, 206,
211, 230 plasma membrane, 77 plasticity, 128 platelets, 78, 313 plausibility, 106, 116 plethysmography, 234, 281 plexus, 75 PM, x, 123, 131, 132, 133, 138, 154, 213, 284, 311,
320 Poincaré, 82, 86 polarity, 302 pollutants, 105, 106, 107, 108, 111, 117, 128 pollution, 105, 106, 107, 108, 117, 126, 127 polymorphism, 85, 91 polymorphisms, 85, 91, 140 polypeptide, 76

Index 340
polyunsaturated fat, x, 94, 114, 132, 133 polyunsaturated fatty acids, x, 94, 114, 132, 133 polyuria, 205 poor, 46, 65, 84, 183, 308 population, x, 25, 85, 94, 100, 104, 110, 111, 114,
118, 128, 137, 138, 139, 140, 141, 144, 149, 150, 151, 154, 161, 164, 168, 170, 207, 211, 212, 213, 218, 226, 234, 254, 273, 278, 288, 290, 292, 305
positive correlation, 109 postmenopausal women, 131 potassium, xii, 6, 77, 83, 87, 90, 98, 100, 102, 104,
116, 120, 121, 132, 177, 179, 191, 193 power, 12, 43, 44, 59, 60, 62, 69, 71, 72, 81, 84, 87,
106, 188, 223 prediction, 46, 98, 282 predictors, 81, 84, 149, 155, 156, 212 preexcitation syndrome, 160, 161, 163, 171, 174 preference, 67, 294 pregnancy, 112, 131 premature contraction, 130 premature ventricular contractions, 221 prematurity, 130 pressure, xiii, 49, 51, 57, 99, 109, 129, 130, 148,
208, 212, 218, 220, 230, 232, 233, 234, 235, 236, 237, 238, 239, 240, 242, 243, 244, 245, 248, 250, 253, 254, 255, 256, 258, 259, 273, 277, 279, 281, 282, 285, 296, 297, 304, 320
pressure gauge, 221 prestige, 62 prevention, ix, x, x xv, 28, 71, 93, 94, 133, 138, 142,
143, 144, 150, 152, 153, 154, 155, 157, 158, 178, 180, 181, 182, 183, 184, 185, 186, 189, 195, 196, 197, 201, 213, 229, 232, 237, 287, 288, 311, 313, 314, 319, 324
primary prophylaxis, 182 privacy, 54 probability, 77, 166, 184, 207, 294, 295, 309 probe, 234, 237, 238, 239, 248, 258 production, 105, 117, 118, 193, 212 profession, 2 professions, 166, 170 prognosis, xii, 67, 91, 118, 130, 157, 162, 163, 170,
198, 203, 204, 213, 225, 312 prognostic value, xii, 173, 203, 212 program, 41, 62, 63, 144, 207, 214, 247, 307 programming, 149, 150, 151, 187, 311 pro-inflammatory, 141 prolapse, 140 propagation, 29, 79
prophylactic, 35, 167, 169, 172, 182, 184, 189, 192, 195, 324
prophylaxis, 144, 201, 292, 294, 303, 308 propranolol, 77, 120 prosthesis, x, 138 protective mechanisms, 102 protein kinases, 87 protein synthesis, 124 proteins, 76, 77, 140 protocol, xiv, 18, 19, 162, 163, 188, 206, 247, 249,
251, 273, 287, 294, 307, 310 psychological stress, 120 psychologist, 65, 66, 67 psychosocial factors, x, 94, 113 psychosocial stress, 103 puberty, 112 public health, 94, 204, 219 pulmonary edema, 181, 292 pulse, xiii, 18, 110, 130, 146, 162, 231, 232, 234,
236, 237, 238, 239, 240, 242, 243, 244, 245, 246, 248, 250, 253, 254, 255, 256, 257, 258, 259, 260, 261, 262, 263, 264, 265, 271, 274, 276, 277, 281, 283, 284, 285, 286, 304
pumps, 10, 74, 76 pus, 42 P-value, 275, 276
Q
QRS complex, 10, 138, 242, 245, 289, 296 QT interval, ix, 73, 79, 80, 87, 98, 115, 119, 120,
131, 132, 134, 180, 191, 236, 283 QT prolongation, 79, 112, 180, 181, 310 qualitative research, 69 quality of life, 2, 31, 46, 63, 64, 65, 66, 144, 204,
292, 316 quartile, 245, 273 questioning, 34, 68, 219
R
race, 140 radiation, 167, 169, 175 radiography, 292 rain, 117 randomized controlled clinical trials, 195 range, vii, ix, xiii, 26, 46, 64, 93, 102, 103, 109, 110,
211, 232, 235, 236, 244, 245, 247, 249, 253, 257,

Index 341
260, 262, 266, 267, 271, 277, 300, 302, 305, 309, 311
reactive gliosis, 218 reactive oxygen, 117 reactivity, 111, 218 reading, 237, 249 reality, 2, 6, 35, 38, 40, 41, 43, 44, 45, 51, 54, 57, 63 recall, 2, 35, 219, 305 recalling, 47 receptor sites, 103, 127 receptors, ix, 6, 73, 76, 77, 78, 85, 89, 99, 103, 105,
106, 112 recognition, 118, 225, 304, 311 recovery, xiv, 14, 15, 83, 111, 120, 288, 304, 305,
310 recurrence, x, 137, 143, 153, 174, 179, 182, 185,
186, 190, 200, 308, 318, 319, 321 redistribution, 179 reduction, xi, xiv, 79, 83, 84, 85, 87, 114, 142, 143,
144, 149, 159, 181, 182, 184, 187, 189, 190, 223, 232, 271, 279, 294, 307, 308, 309, 319
reflection, 47, 52, 80 reflexes, 76, 78, 88, 148, 218, 229, 230, 232, 233 refractory, xi, 12, 13, 14, 15, 17, 19, 20, 23, 77, 83,
138, 146, 159, 162, 163, 167, 171, 178, 194, 197, 198, 295, 296, 311, 325
regenerate, 83 Registry, 35, 131, 155, 173, 295, 314, 319 regression, xv, 112, 256, 264, 288, 306 regression analysis, 264 regulation, xii, xiii, 77, 81, 83, 85, 86, 87, 88, 89, 90,
110, 120, 217, 218, 221, 223, 224, 226, 230, 235, 279
regulations, 81, 233 relapses, 294, 295, 307, 309, 310 relationship, xiii, 11, 15, 74, 101, 109, 116, 117, 131,
134, 138, 141, 148, 158, 211, 213, 219, 232, 240, 246, 251, 253, 254, 256, 259, 260, 264, 268, 277, 278, 284, 297, 298
relationships, 2, 51, 69, 75, 106, 109, 125, 194, 235, 253, 265, 275
relatives, 70, 71 relaxation, 233, 236, 285 relevance, x, 89, 137, 213 reliability, 2, 6, 7, 169, 180 remodelling, 83, 204, 209, 210, 212, 294 renin, 81, 318, 319 replacement, 6, 35, 47, 78, 114, 131, 151, 181 reproduction, 38, 40 research design, viii, 33, 68
resection, 187 resentment, 2 residues, 77 resilience, 42 resistance, 148, 218, 296, 297, 298, 300, 320 resolution, 180 resources, 200 respiration, xiii, 30, 81, 82, 217, 223 respiratory, xiv, 29, 65, 81, 108, 129, 218, 220, 222,
288, 296, 310 respiratory disorders, 218 responsiveness, 84, 85, 146, 147 resting potential, 12, 13 retail, 178 reticulum, 211 retrovirus, 7 returns, 12, 13, 36 rhythm, vii, viii, x, xiv, 5, 9, 10, 11, 12, 17, 19, 20,
23, 24, 26, 27, 28, 29, 30, 78, 81, 89, 96, 98, 101, 103, 106, 111, 117, 123, 124, 133, 134, 138, 140, 154, 185, 188, 189, 190, 192, 200, 205, 211, 221, 240, 287, 288, 289, 291, 292, 293, 295, 304, 306, 307, 311, 315, 316, 317, 318, 323, 324
rhythms, viii, 8, 10, 11, 12, 15, 17, 27, 28, 80, 90, 96, 97, 114
right atrium, vii, xiii, 9, 146, 231, 244, 276, 290 right hemisphere, 86, 92 right ventricle, 10, 24, 146, 232, 237, 244 rigidity, 218, 219 risk assessment, 119, 130 risk factors, 97, 110, 111, 115, 118, 120, 140, 141,
142, 143, 149, 150, 154, 155, 290, 291, 307, 312 risk management, 69 risk profile, 143, 154 room temperature, 220 Rouleau, 89
S
SA node, vii, 9, 10, 11, 13 sadness, 50 safety, xi, 6, 7, 61, 151, 153, 155, 177, 180, 185,
190, 191, 193, 198, 317, 319, 321, 322, 325 sample, xii, 150, 203, 206, 209, 210, 211, 238, 304 sampling, 16, 247 saturation, 110, 130, 237, 238, 283, 304 saving lives, 2 scaling, 82, 238, 239, 246, 247, 248 scar tissue, 42, 79 scepticism, 1

Index 342
school, 63 scientific knowledge, 58 search, 65, 215, 253 searching, 235, 277 seasonal factors, 117 seasonality, 117, 129 Second World, 237 secretion, 99, 204, 233 security, viii, 34, 54 sedative, xiv, 288, 304, 305, 310 sedentary lifestyle, 101 sediment, 108 seizure, 51 selecting, 185, 188, 298 self esteem, 55 self-esteem, 55 sensations, 51, 54 sensing, 2, 5, 14, 146 sensitivity, ix, 73, 80, 82, 90, 112, 164, 206, 210,
219, 221, 226, 227, 238, 239, 245, 246, 253, 260 sensors, 236 separation, 34, 38, 52 septum, 271 series, xv, 12, 18, 28, 34, 98, 148, 161, 180, 221,
242, 243, 248, 249, 250, 251, 254, 255, 256, 260, 265, 271, 288, 309, 321
serine, 77 serum, 98, 99, 102, 105, 120, 121, 144, 181, 192 severity, vii, 141, 188, 204, 225, 227, 229, 230, 322 sex, xiii, xv, 113, 120, 131, 133, 218, 225, 226, 288,
306 sex hormones, 113 sexism, 2 sexuality, viii, 34, 36 shame, 72 shape, 77, 109, 222, 260, 268, 269, 270, 277, 283 shear, 78 shock, xv, 2, 38, 39, 57, 67, 98, 183, 185, 186, 187,
199, 238, 288, 289, 294, 295, 296, 298, 304, 305, 306, 309, 320, 322, 323
shock therapy, 2, 183, 187 shortness of breath, 147, 205, 215 sibling, 51 siblings, 51 sick sinus syndrome, 149, 156, 157, 242, 243, 272 side effects, 180, 183, 193, 293, 310, 324 sign, xi, 118, 159, 161, 162, 168, 204 signalling, 77 signals, vii, 9, 10, 15, 29, 30, 238, 248 significance level, 245
signs, xiv, 166, 205, 206, 218, 219, 220, 226, 273, 287, 304
similarity, 269, 270 simulation, 16, 18, 26, 28 sine wave, 299, 300, 301, 321 sinoatrial node, 6, 80, 179 sinus, ix, x, xiv, 8, 11, 12, 17, 18, 73, 75, 76, 80,
103, 104, 138, 144, 147, 148, 149, 150, 152, 153, 156, 157, 163, 166, 179, 188, 189, 190, 191, 192, 198, 199, 205, 211, 240, 243, 284, 287, 289, 290, 291, 292, 293, 294, 295, 296, 306, 307, 309, 311, 316, 317, 318
sinus rhythm, ix, xiv, 11, 12, 17, 18, 73, 80, 147, 148, 166, 179, 188, 189, 190, 191, 192, 198, 199, 205, 211, 240, 284, 287, 289, 290, 291, 292, 293, 294, 295, 296, 306, 307, 309, 311, 316, 317, 318
sites, 75, 76, 218, 284 skeletal muscle, 98 skills, 66, 310, 311 skin, 40, 41, 42, 56, 180, 183, 227, 238, 305, 308,
309, 310 sleep apnea, 141, 190 sleep disturbance, 219 smog, 105, 127 smoke, 125, 142 smokers, 102, 103 smoking, 97, 103, 104, 105, 111, 113, 118, 126, 140 smooth muscle, 204 smoothing, 25, 31 social change, 2 social construct, 69 social life, 52 social support, 113 society, 40, 69 sodium, 6, 77, 83, 87, 104, 114, 117, 125, 179, 194,
271 software, 15, 16, 27, 243, 246, 247, 251 soil, 36 sounds, 51 species, 117, 129 specificity, 82, 164, 171, 210, 239 spectral component, 83, 85, 86 spectrum, 12, 81, 97, 147, 223, 266 speed, 110 spinal cord, 76, 183, 196, 218 spine, 57 sports, 166 sprouting, ix, 74, 83, 91 SPSS, 207 stability, 246, 268, 277, 304, 310

Index 343
stabilization, 24, 25, 31, 114, 240, 241 stages, 28, 84, 219, 220 standard deviation, 18, 20, 245, 276 standards, 90, 151, 206, 225 stasis, 140, 141, 142, 289 statistics, 16, 258, 260, 262 steel, 41 stem cells, 6, 8 stenosis, 2, 167, 173, 234, 291 sterilisation, 55 sternum, 38 stigma, 2 stimulus, xiii, 78, 79, 141, 145, 231, 233, 245, 276,
283 stomach, 293 storage, 151, 296 storms, 117 strain, 220 strategies, 28, 118, 119, 171, 188, 291 stratification, 80, 122, 200, 229 strength, 12, 13, 14, 18, 19, 20, 64, 233, 321 stress, 61, 74, 77, 78, 81, 94, 95, 98, 99, 100, 102,
109, 110, 111, 113, 114, 116, 117, 118, 119, 120, 121, 123, 129, 130, 132, 161, 162, 170, 212, 214, 222, 226, 232, 236
stress factors, 120 stressful events, 98, 112 stressors, ix, 93, 100 stretching, 78 strikes, 49, 100 stroke, ix, x, 48, 55, 74, 82, 86, 92, 138, 140, 141,
142, 143, 144, 149, 150, 153, 154, 155, 156, 157, 158, 205, 281, 284, 285, 290, 291, 292, 311, 313, 314, 319
stroke volume, 281, 284, 285 structural changes, 79 students, 63 subacute, 180 subgroups, 100, 103, 104, 110, 111, 243 subjective well-being, 113 subjectivity, 36 success rate, 253 suffering, ix, 42, 93, 94, 97, 219, 253 suicide, 41, 43, 44 sulfate, x, 93, 105 sulfur, 105 superimposition, 104, 118, 147 superiority, 144, 189, 242, 308 supernatural, 44 supply, 75, 78, 99, 233
suppression, 26, 55, 86, 115, 179, 199, 317 supraventricular arrhythmias, vii, x, 103, 137, 201,
316, 319 supraventricular tachycardia, 86, 101, 130, 162, 171 surgical resection, 187 surveillance, 151 survival, 47, 61, 84, 85, 91, 158, 182, 183, 184, 186,
196, 207, 209, 210, 316 survival rate, 84 survivors, 59, 134, 184, 186, 206 susceptibility, x, 78, 83, 86, 94, 97, 100, 102, 112,
113, 115, 119, 212, 221 sweat, 110 swelling, 147 Switzerland, 110, 117 sympathetic denervation, 74, 223, 227, 230 sympathetic nervous system, ix, 74, 81, 84, 87, 93,
95, 116, 213, 225 symptom, xii, 121, 147, 152, 217, 219 symptoms, xi, 11, 31, 58, 63, 120, 132, 141, 144,
151, 152, 159, 161, 166, 191, 205, 206, 218, 219, 220, 227, 233, 289, 291, 294, 307, 312
synchronization, 295 syndrome, xi, 8, 79, 84, 88, 97, 98, 99, 100, 108,
112, 113, 115, 120, 121, 122, 130, 131, 134, 147, 148, 152, 156, 159, 160, 161, 162, 163, 164, 165, 166, 167, 168, 169, 170, 171, 172, 173, 174, 181, 204, 219, 220, 225, 272
systemic circulation, 108 systems, 5, 7, 59, 76, 81, 102, 117, 204, 214, 237,
239, 296, 300 systolic blood pressure, 82, 99, 221, 240, 273, 274
T
tachycardia, vii, xi, xiv, 13, 90, 92, 98, 100, 101, 103, 104, 109, 110, 112, 117, 122, 147, 152, 159, 160, 162, 163, 164, 165, 166, 167, 168, 169, 170, 173, 174, 178, 183, 184, 187, 188, 213, 287, 289
targets, 232, 237 technical assistance, 282 technician, 249 technology, vii, 2, 9, 53, 55, 56, 58, 60, 61, 62, 66,
68, 69, 70, 187, 283, 320 teenagers, 164, 168 teeth, 51 telephone, 135 television, 34, 62 temperature, 81, 109, 129, 223, 304 tension, 45, 113, 204

Index 344
terminal illness, 68, 71 terminally ill, 50 terminals, 76, 84 territory, 86, 153 theory, 7, 29, 30, 81, 83, 90, 283 therapeutic approaches, 220 therapeutic goal, 5, 188 therapy, x, xii, xiv, 2, 6, 7, 35, 60, 61, 65, 82, 85, 94,
114, 118, 123, 131, 132, 133, 134, 143, 144, 149, 150, 151, 154, 155, 156, 157, 177, 178, 179, 181, 182, 183, 184, 186, 187, 188, 190, 192, 193, 194, 195, 197, 198, 201, 205, 214, 225, 237, 281, 282, 283, 285, 288, 291, 293, 294, 313, 314, 315, 317, 319, 320
thiazide, 286 thinking, 36, 55, 62, 63, 70 thorax, 296, 297, 308 threat, 44 threshold, viii, ix, 12, 13, 18, 19, 20, 33, 34, 42, 47,
48, 49, 50, 51, 52, 53, 54, 60, 67, 74, 102, 103, 104
thresholds, 98, 113, 121, 322 thrombin, 143 thrombosis, 78, 129, 153, 167, 291, 308, 313 thrombus, 140, 148, 291 thyroid, 117, 180, 183, 192, 193, 201, 292, 310 thyroiditis, 193 thyrotoxicosis, 192, 201, 293 thyrotropin, 192 TIA, 142 time frame, x, 94, 138 time series, 18, 28, 30 time-frame, 35 timing, 10, 12, 14, 27, 121, 147, 234, 235, 236, 237,
280, 282, 283 tin, 57 tissue, 79, 97, 108, 148, 178, 224, 234, 279, 295,
296, 312 titanium, 41 TNF, 106 TNF-α, 106 tobacco, 104 tonic, 223 toxic effect, 102 toxicity, xii, 101, 108, 123, 177, 179, 180, 191, 193,
194, 197, 310 toxin, 49 tradition, 43 training, 66, 230 trajectory, 46, 59
transcatheter, 153 transcription, 79 transducer, 205 transduction, 76 transformation, 7, 80, 160 transient ischemic attack, 149, 156 transition, x, 19, 34, 46, 52, 94, 100, 105, 127 transition metal, 105, 127 transitions, 34 transmission, 75, 78, 235, 238 transmits, 233 transplantation, 46, 193 transport, 249, 279 trauma, 2, 47, 49, 50, 53, 65 tremor, 218, 219, 253, 265, 277 trend, 140, 189, 292, 306 trial, 31, 67, 69, 141, 143, 149, 150, 154, 156, 157,
173, 182, 184, 185, 186, 189, 190, 193, 194, 195, 196, 197, 198, 200, 201, 204, 292, 313, 314, 315, 317, 318, 319, 322, 324
tricuspid valve, 290 triggers, x, 11, 14, 66, 93, 94, 95, 96, 97, 98, 100,
101, 102, 103, 104, 109, 111, 112, 113, 115, 117, 118, 119, 122, 148, 213
trust, 54 TSH, 192 tumor, 128 tumor necrosis factor, 128 turbulence, ix, 73, 80 turnover, 87 type 1 diabetes, 87
U
UK, 206 ultrasound, 153, 281 uncertainty, 46, 58 underlying mechanisms, 116, 147, 213 uniform, 83, 181 United Kingdom, 192 United States, 35, 65, 121, 192, 288 unstable angina, 205 urinary tract, 218 urinary tract infection, 218 urine, 271 users, 125

Index 345
V
vagus, 75, 81, 279 vagus nerve, 75, 279 validation, 27, 37, 38, 285 validity, 214 values, xiii, 66, 67, 81, 87, 98, 121, 145, 207, 231,
232, 234, 235, 238, 239, 240, 241, 243, 246, 250, 254, 255, 256, 258, 259, 260, 264, 265, 266, 267, 268, 269, 277, 278, 297, 300, 302
valvular heart disease, 97, 190, 225, 230, 288 vanadium, 105 variability, ix, xii, xiii, 11, 12, 17, 18, 29, 31, 73, 80,
82, 83, 87, 90, 91, 92, 98, 106, 107, 108, 112, 113, 119, 128, 131, 132, 134, 179, 217, 221, 222, 223, 225, 226, 227, 228, 229, 230, 232, 235
variable, xv, 112, 218, 239, 280, 288, 289, 308, 323 variables, x, xiv, 16, 80, 81, 85, 93, 101, 106, 109,
110, 111, 112, 182, 206, 211, 245, 247, 253, 273, 282, 287, 303, 306
variance, 85 variation, x, 12, 18, 20, 80, 82, 94, 96, 98, 111, 113,
115, 116, 117, 129, 133, 134, 135, 150, 178 vasoconstriction, 78, 99, 104, 105, 125, 141, 284 vasomotor, 81 vasospasm, 97 vector, 6 vein, 153, 271, 280, 284 velocity, 168, 241, 258, 279, 280, 284, 286 ventilation, 80, 304, 305, 310, 311 ventricle, 11, 14, 15, 16, 19, 20, 27, 75, 79, 140, 146,
147, 232, 233, 234, 235, 236, 239, 242, 246, 253, 271, 272, 278, 289
ventricular arrhythmias, vii, ix, x, 74, 78, 82, 83, 87, 88, 89, 90, 93, 94, 96, 98, 100, 101, 102, 104, 105, 109, 110, 115, 116, 118, 119, 120, 121, 123, 124, 127, 130, 133, 134, 135, 152, 182, 183, 185, 188, 195, 196, 197, 198
ventricular fibrillation, xii, 74, 78, 83, 84, 87, 88, 94, 101, 102, 104, 105, 112, 117, 119, 120, 124, 134, 135, 160, 161, 162, 164, 167, 169, 177, 178, 184, 188, 194, 197, 198, 199, 320
ventricular tachycardia, xii, 35, 84, 94, 97, 98, 101, 103, 104, 105, 109, 110, 111, 112, 114, 117, 118, 119, 122, 125, 126, 130, 131, 135, 164, 172, 177, 178, 188, 194, 197, 198
verapamil, 104, 129, 199, 318, 323 vessels, 218, 243, 245, 271 viral vectors, 7 viruses, 7
viscosity, 108, 109, 129 vision, 44, 310 visual field, 53 vitamin C, 318 voice, 51, 55, 71 vomiting, 48, 49 vulnerability, x, 2, 54, 64, 66, 94, 96, 97, 98, 107,
108, 111, 112, 114, 115, 116, 117, 118, 119, 124, 140, 191, 212
W
waking, 115 walking, 43, 100 warrants, 103 wavelengths, 237, 238 wavelet, 289 weakness, 147 well-being, 2, 117 Western countries, 35 wind, 110 wind speeds, 110 windows, 82 wine, 102 winning, 40 winter, x, 94, 96, 116, 117, 129, 135 wires, 38, 49 withdrawal, 102, 103, 294 women, 64, 98, 99, 100, 101, 102, 109, 110, 112,
113, 114, 121, 130, 132, 135, 140, 204 work-related stress, 116 worldview, 46, 63 worry, 63 wound infection, 42, 69 wrists, 43
Y
yang, 75, 76, 88 yield, 24 yin, 75, 76, 88 young adults, 105, 167 young men, 127, 130
Z
zinc, 105

Index 346
Β
β2-adrenergic receptor, 79, 84, 91
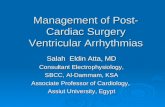

![Automatic Detection of Cardiac Arrhythmia through ECG ...€¦ · Cardiac Arrhythmia [3], also known as irregular heartbeat, is a group of conditions in which the heartbeat is irregular,](https://static.fdocuments.us/doc/165x107/607210056cc22557db7f5efb/automatic-detection-of-cardiac-arrhythmia-through-ecg-cardiac-arrhythmia-3.jpg)