Carbohydrates (Starches) are Good for People with · PDF fileCarbohydrates (Starches) are...
92
Carbohydrates (Starches) are Good for People with Diabetes John McDougall, MD PO Box 14039 Santa Rosa, CA 95402 www.drmcdougall.com
Transcript of Carbohydrates (Starches) are Good for People with · PDF fileCarbohydrates (Starches) are...

Carbohydrates (Starches) are Good for People with Diabetes
John McDougall, MD
PO Box 14039
Santa Rosa, CA 95402
www.drmcdougall.com

Disclosure Statement
Dr. McDougall’s Health & Medical Center Dr. McDougall’s Right Foods McDougall Adventures Inc. 12 National Best Selling McDougall Books

What Causes Diabetes?
Type-1 caused by insulin insufficiency
(Autoimmune damage, cow’s milk)
Type-2 caused by insulin resistance
(Insulin levels normal or high)

Obesity = Type-2 Diabetes
Excess body weight is the most important modifiable risk factor for the development of diabetes:
Risk ratios: 20.1 for overweight and obese 38.8 for morbid obesity
Overweight and obese (30 and 35 kg/m2) Morbid Obesity (> 35 kg/m2) Compared with a BMI <23 kg/m2
Nutr Met Cardiovasc Dis (2011), doi:10.1016/j.numecd.2011.03.009

Bariatric Surgery
A recent meta-analysis included 3188 patients with type-2 diabetes:
Am J Med. 2009 Mar;122(3):248-256.e5.
78.1% = complete resolution 86.6% = improved or resolved
Surgically-induced malabsorption and sickness

Type-2 Diabetes – the Expected Adaptation to Over-nutrition

Insulin Resistance
Definition: A state of reduced responsiveness to normal circulating levels of insulin Lipotoxicity: Abnormalities in fatty acid metabolism may result in inappropriate accumulation of lipids in muscle, liver, and beta-cells.
Hypertension. 2005 May;45(5):828-33.

Low-carbohydrate Diets (High-fat) *An apology: Non-starch, red, green, & yellow vegetables
Fat Protein
Meat, poultry, fish, cheese, and eggs
*

Origin of Low-Carb Diets
Nutr J. 2011 Mar 11;10:23.
…from 1915 until the discovery of insulin in 1922, prolonged fasting and permanent calorie restriction were championed in North America by Frederick Allen and Elliott Joslin.

Low-carb Diets to Rx Diabetes
“Meta-regression analyses show that hemoglobin A1c, fasting glucose, and some lipid fractions (triglycerides) improved with lower carbohydrate-content diets. Overall effect on weight was equivocal…”
J Am Diet Assoc. 2008 Jan;108(1):91-100.

Low-carb Induces Sickness
“Signs of improved health appear to accrue, as measured by
changes in a variety of “risk factors,” eg, cholesterol,
triglycerides, uric acid, glucose, blood pressure, and body weight.
Hence, the patient is declared healthier. However, this is not
necessarily a correct assessment. Similar benefits, for similar
reasons, are seen when patients undergo cancer chemotherapy,
and physicians do not brag about these results.”
John McDougall, MD
Mayo Clin Proc. 2004 Mar;79(3):431;

All Major Studies Show an Increase
in Disease and Death
from Low-carbohydrate Diets
No Studies of High-carbohydrate Diets Show Similar Effects

(1) Ignore the bulk of the science
Low-carbohydrate diets and all-cause and cause-specific
mortality: Two cohort Studies
Teresa T. Fung, ScD
Department of Nutrition, Simmons College; Department of Nutrition, Harvard School of Public
Health
Rob M. van Dam, PhD
Departments of Epidemiology and Public Health and Medicine, Faculty of Medicine, National
University of Singapore, Department of Nutrition, Harvard School of Public Health
Susan E. Hankinson, ScD and Meir Stampfer, M.D., DrPH
Department of Epidemiology, Harvard School of Public Health; Channing Laboratory, Department
of Medicine, Brigham and Women's Hospital and Harvard Medical School.
Walter C. Willett, M.D., DrPH and Frank B. Hu, M.D., PhD.
Department of Nutrition, Harvard School of Public Health; Channing Laboratory, Department of
Medicine, Brigham and Women's Hospital and Harvard Medical School
Abstract
Background—Data on the long-term association between low-carbohydrate diets and mortality
are sparse.
Objective—To examine the association of low-carbohydrate diets with mortality during 26 years
of follow-up in women and 20 years in men.
Design—A prospective cohort study of women and men, followed from 1980 (women) or 1986
(men) until 2006. Low-carbohydrate diets, either animal-based (emphasizing animal sources of fat
and protein), or vegetable-based (emphasizing vegetable sources of fat and protein) were
computed from multiple validated food frequency questionnaire assessed during follow-up.
Setting—Nurses' Health Study and Health Professionals' Follow-up Study
Participants—85,168 women (aged 34-59 years at baseline) and 44,548 men (aged 40-75 years
at baseline) without heart disease, cancer, or diabetes.
Measurement—Investigator documented 12,555 deaths (2,458 cardiovascular, 5,780 cancer) in
women and 8,678 deaths (2,746 cardiovascular, 2,960 cancer) in men.
Results—The overall low-carbohydrate score was associated with a modest increase in overall
mortality in pooled analysis (Hazard Ratio, HR, comparing extreme deciles=1.12 (95%
CI=1.01-1.24, p-trend=0.14). The animal low-carbohydrate score was associated with a higher all-
cause mortality (pooled HR comparing extreme deciles=1.23, 95% CI=1.11-1.37, p-trend=0.05),
Corresponding Author: Address for reprint requests: Teresa Fung, Department of Nutrition, Simmons College, Boston, MA 02115,617-521-2712 (phone), 617-521-3002 (fax), [email protected] or Dr. Frank Hu at [email protected] mailing address:Teresa Fung: Department of Nutrition, Simmons College, 300 The Fenway, Boston, MA 02115.Rob van Dam: Department of Epidemiology and Public Health, Yong Loo Lin School of Medicine, National University of Singapore,10 Medical Drive, Singapore 117597Susan Hankinson: Channing Laboratory, 181 Longwood Ave, Boston, MA 02115Meir Stamfer: Department of Epidemiology, Harvard School of Public Health, 677 Huntington Ave, Boston, MA 02115Walter Willett and Frank Hu: Department of Nutrition, Harvard School of Public Health, 677 Huntington Ave, Boston, MA 02115
NIH Public AccessAuthor ManuscriptAnn Intern Med. Author manuscript; available in PMC 2011 September 7.
Published in final edited form as:
Ann Intern Med. 2010 September 7; 153(5): 289–298. doi:10.1059/0003-4819-153-5-201009070-00003.
NIH-PA Author Manu
script
NIH-PA Author Manu
script
NIH-PA Author Manu
script
The animal low-carbohydrate score was
associated with a higher all-cause mortality.
Ann Intern Med. 2010 Sep 7;153(5):289-98

(1) Ignore the bulk of the science
Low carbohydrate-high protein diet and incidence ofcardiovascular diseases in Swedish women:prospective cohort study
OPENACCESS
Pagona Lagiou professor1 2
, Sven Sandin scientist3, Marie Lof scientist
3 4, Dimitrios Trichopoulos
professor2 5
, Hans-Olov Adami professor2 3
, Elisabete Weiderpass professor3 6 7
1Department of Hygiene, EpidemiologyandMedical Statistics, Universityof AthensMedical School, 75M. AsiasStreet, Goudi, GR-11527, Athens,
Greece; 2Department of Epidemiology, Harvard School of Public Health, Boston, MA02115, USA; 3Department of Medical Epidemiology and
Biostatistics, Karolinska Institutet, SE-171 77, Stockholm, Sweden; 4Department of Clinical and Experimental Medicine, University of Linköping,
SE-58185Linköping, Sweden; 5Bureauof EpidemiologicResearch, Academyof Athens, Athens, GR-10679, Greece; 6Cancer Registryof Norway,
Montebello,N-0310,Oslo,andDepartmentofCommunityMedicine,UniversityofTromso,Tromso,Norway; 7FolkhälsanResearchCenter,Samfundet
Folkhälsan, Helsinki, Finland
Abstract
Objective To study the long termconsequences of lowcarbohydrate
diets, generallycharacterisedbyconcomitant increases inproteinintake,
on cardiovascular health.
Design Prospective cohort study.
Setting Uppsala, Sweden.
ParticipantsFromarandompopulationsample,43396Swedishwomen,
aged 30-49 years at baseline, completed an extensive dietary
questionnaire and were followed-up for an average of 15.7 years.
Main outcome measures Association of incident cardiovascular
diseases(ascertainedbylinkagewithnationwideregistries), overall and
bydiagnosticcategory, withdecreasingcarbohydrate intake (in tenths),
increasing protein intake (in tenths), and an additive combination of
these variables (low carbohydrate-high protein score, from2 to 20),
adjusted for intake of energy, intake of saturated and unsaturated fat,
and several non-dietary variables.
Results A one tenth decrease in carbohydrate intake or increase in
protein intake or a 2 unit increase in the lowcarbohydrate-high protein
score were all statistically significantly associated with increasing
incidence of cardiovascular disease overall (n=1270)—incidence rate
ratio estimates 1.04 (95%confidence interval 1.00 to 1.08), 1.04 (1.02
to 1.06), and 1.05 (1.02 to 1.08). No heterogeneity existed in the
association of any of these scores with the five studied cardiovascular
outcomes: ischaemic heart disease (n=703), ischaemic stroke (n=294),
haemorrhagic stroke (n=70), subarachnoid haemorrhage (n=121), and
peripheral arterial disease (n=82).
Conclusions Low carbohydrate-high protein diets, used on a regular
basis and without consideration of the nature of carbohydrates or the
source of proteins, are associated with increased risk of cardiovascular
disease.
Introduction
Overweightandobesityareriskfactorsforseveralcommon
chronicdiseases,1 andtheyhavebecomeendemicinmost
economicallydevelopedcountriesandbeyond.2 3 Increased
physicalactivityisonewayofcounteractingexcessiveenergy
intake,butreducingthisintakeisalsoimportant.4Manydietary
regimenshavebeenproposedasconducivetoweightcontrol,
invokingvariousmechanismsincludingincreasedsatiety.56The
mostpopularamongthesedietsemphasisereductionof
carbohydrateintake, therebyencouraginghighproteinintake,7
ashighfatdietsaregenerallyavoidedinmostWesternsocieties.
Lowcarbohydrate-highproteindietsmayhaveshorttermeffects
onweightcontrol,8 9 butconcernshavealsobeenexpressed,
notablywithrespect tocardiovascularoutcomes.10 11 Although
lowcarbohydrate-highproteindietsmaybenutritionally
acceptableiftheproteinismainlyofplantoriginandthe
reductionofcarbohydratesappliesmainlytosimpleandrefined
ones, thegeneralpublicdonotalwaysrecogniseandacton
thesequalifications.
Duringthepastfewyears,severalcohortstudieshaveevaluated
thelongtermhealtheffectsoflowcarbohydrate-highprotein
diets,withemphasisoncardiovasculardiseases.IntheNurses’
HealthStudyintheUnitedStates,dietslowerincarbohydrate
andhigherinproteinwerenotassociatedwithincreased
incidenceofischaemicheartdisease.12Threesmallerstudiesin
Europe,however,indicatedstatisticallysignificantincreasesin
cardiovascularmortalityinrelationtolowcarbohydrate-high
BMJ 2012;344:e4026 doi: 10.1136/bmj.e4026 (Published 26 June 2012) Page 1 of 11
Research
RESEARCH
Low carbohydrate-high protein diets, used on a
regular basis… are associated with increased
risk of cardiovascular disease.
BMJ. 2012 Jun 26;344:e4026.

(1) Ignore the bulk of the science
Low-carbohydrate diets were associated with a
significantly higher risk of all-cause mortality…
PLoS One. 2013;8(1):e55030.

Elliott Joslin, MD
Elliott Proctor Joslin (1869–1962)
Prophetically wrote in 1927: “I believe the chief cause of premature atherosclerosis in diabetes, save for advancing age, is an excess of fat, an excess of fat in the body (obesity), an excess of fat in the diet, and an excess of fat in the blood. With an excess of fat diabetes begins and from an excess of fat diabetics die, formerly of coma, recently of atherosclerosis.”
Ann Clin Med 1927;5:1061.

Obesity Worldwide

Diabetes Worldwide

Meat Consumed Worldwide

Milk Consumed Worldwide

Diabetes Up 12 Times In 30 years
The estimated prevalence of diabetes among a representative sample of Chinese
adults was 11.6% and the prevalence of prediabetes was 50.1%. Projections
based on sample weighting suggest this may represent up to 113.9 million
Chinese adults with diabetes and 493.4 million with prediabetes. These findings
indicate the importance of diabetes as a public health problem in China.
The prevalence of diabetes was less than 1% in the Chinese population in 1980
JAMA. 2013;310(9):948-958

History of Starch Eating


High-carbohydrate Diets (Low-fat)
Starches (beans, corn, potatoes, rice, wheat, etc.)
Non-starch, red, green, & yellow vegetables and Fruits
Fat
Protein
Carbohydrate

Healthy Medical Students 2-days on carbohydrate-diet*
Arch Intern Med.1927; 40: 818-830.
*sugar, candy, pastry, white bread, baked potatoes, syrup, bananas, rice, oatmeal

Healthy Medical Students 2-days on high-protein diet*
Arch Intern Med.1927; 40: 818-830.
*lean meat, whites of eggs

Healthy Medical Students 2-days on high-fat diet*
Arch Intern Med.1927; 40: 818-830.
*olive oil, butter, mayonnaise (egg yolk, 20% cream)

One Healthy Medical Student high-fat vs. high carbohydrate diet
Arch Intern Med.1927; 40: 818-830.

Sugar Makes Diabetes Better
180
Seru
m G
luco
se m
g/d
L.
N Engl J Med. 1971 Mar 11;284(10):521-4.
“These data suggest that the high carbohydrate diet increased the sensitivity of peripheral tissues to insulin.”
45% vs. 85% Carbohydrate: FBS fell, OGT improved, fasting insulin lower

Classic Research, BMJ 1940
Br Med J. 1940 May 4;1(4139):719-22

Sugar Makes Diabetes Better
180
Seru
m G
luco
se m
g/d
L.
N Engl J Med. 1971 Mar 11;284(10):521-4.
“These data suggest that the high carbohydrate diet
increased the sensitivity of peripheral tissues to insulin.”
45% vs. 85% Carbohydrate: FBS fell, OGT improved, fasting insulin lower
(Over 10 days of feeding of formula feeding – dextrins and maltose)

Fruit Does Not Make Diabetes Worse
Eating less fruit had however no effect on HbA1c, weight loss or waist circumference.
“We recommend that the intake of fruit should not be restricted in patients with type 2
diabetes.”

Blood Sugar Non Toxic
JAMA. 2014;311(3):279-286.

Medication = Weight Gain = Diabetes
Downward Cycle

Diabetic Management
“…it is important to remember that ‘diabetic control’ means a lot more than ‘blood sugar control.’” T.D.R Hockaday, 1987
Mortality and Morbidity Heart disease Eye disease
Kidney disease
Scand J Gastroenterol Suppl. 1987;129:124-31.

Lessons from the Past, Directions for the Future
The WWI Starch Solution for Denmark
(1862-1945)
Served as the
manager of the
Danish National
Laboratory for
Nutrition Research in
Copenhagen and
food advisor to the
Danish government
during World War I.

Lessons from the Past, Directions for the Future
The WWI Starch Solution for Denmark
Madsen after 1 year of
eating potatoes and a little
fat
“Minimum need for protein was so
low for man that it could not be
reached; therefore, removing
meat would be of no adverse
consequence.”
From the book, Fuldkommen Sundhed og Vejen dertil (Perfect
Health and the Path to Get It), 1934 by Mikkel Hindhede

WWI: Britain &Germany
Blockade North Sea

Lessons from the Past, Directions for the Future
The WWI Starch Solution for Denmark
Note: People of all ages showed reduction in death

Lessons from the Past, Directions for the Future
Mortality from Diabetes in England and Wales during Wars
YEARS

Diet in the Etiology of AODM
During war, diabetic death rate falls due to food shortages England and Wales (pre- and post insulin use)
Proc Roy Soc Med. 1949; 42:323

Pritikin Longevity Center
J Appl Physiol. 2005 Jan;98(1):3-30.

James Anderson, MD University of Kentucky, College of Medicine
Metabolic Ward Study
Weight Maintaining Diet
Insulin Usage:
Average reduction
26 to 11 units daily
11 of 20 lean patients
discontinued insulin
CHO Initially = 43%
7 days average
CHO intervention = 70%
16 days average
Am J Clin Nutr. 1979 Nov;32(11):2312-21.

Neal Barnard, MD
Vegan diet = (10% of energy from fat, 15% protein, and 75% carbohydrate)
ADA diet = (40 % fat, 20% protein, 40% carbohydrate, < 200 mg cholesterol
Vegan ADA
Reduced Medication 21/49 13/50
HgB A1c* -1.23 0.38 P=.01
Weight (Kg) 6.5 3.1 P=.001
LDL (% change)* 21.2 10.7 P=.02
Urine protein 15.9 10.9 P=.013
*No medication changes
Randomized Clinical Trial in Individuals With Type 2 Diabetes
Diabetes Care. 2006 Aug;29(8):1777-83.

The Ultimate Diet
Am J Med. 1948 Apr;4(4):545-77

Walter Kempner, MD
Walter Kempner, MD
(1903 – 1997)
The Rice Diet
Duke University
Durham, NC
Decrease in heart size, improved kidney function, and hypertensive retinopathy reversal
Reversal of obesity, diabetes, hypertension, and heart failure.
Am J Med. 1948 Apr;4(4):545-77

Morbid Obesity Reversed

Morbid Obesity Reversed

Retinopathy Reversed
Postgrad Med. 1958 Oct;24(4):359-71.
Am J Med. 1959 Aug;27:196-211.
42-year-old male with an 18-year history of diabetes mellitus. Dietary compliance for 26 months.
Classical diabetic retinopathy: aneurysms, punctuate, preretinal or vitreous hemorrhage,
waxy exudates, neovascularization, and retinitis proliferans. Average observation 22 months,
20 of 44 diabetics showed improvement.
Retinal Physician April 2008

Retinopathy Rx Low-fat Diet
Postgrad Med. 1958 Oct;24(4):359-71. Am J Med. 1959 Aug;27:196-211.

Severe Kidney Disease Reversed

Nephropathy 1946, Thomas Addis argued from personal clinical experience that reduction in renal "work" by judicious dietary protein restriction was effective in minimizing further loss of kidney function in patients with chronic kidney insufficiency from a variety of causes.
J Clin Invest. 2006 Feb;116(2):288-96.
Thomas Addis, MD Stanford University
1881-1949

Nephropathy
Annu Rev Nutr. 1997;17:435-55.
A low-protein diet reduces the progression of their
kidney disease and death on average by 33% to 50%.

Coronary Insufficiency Reversed

Heart Enlargement Reversed
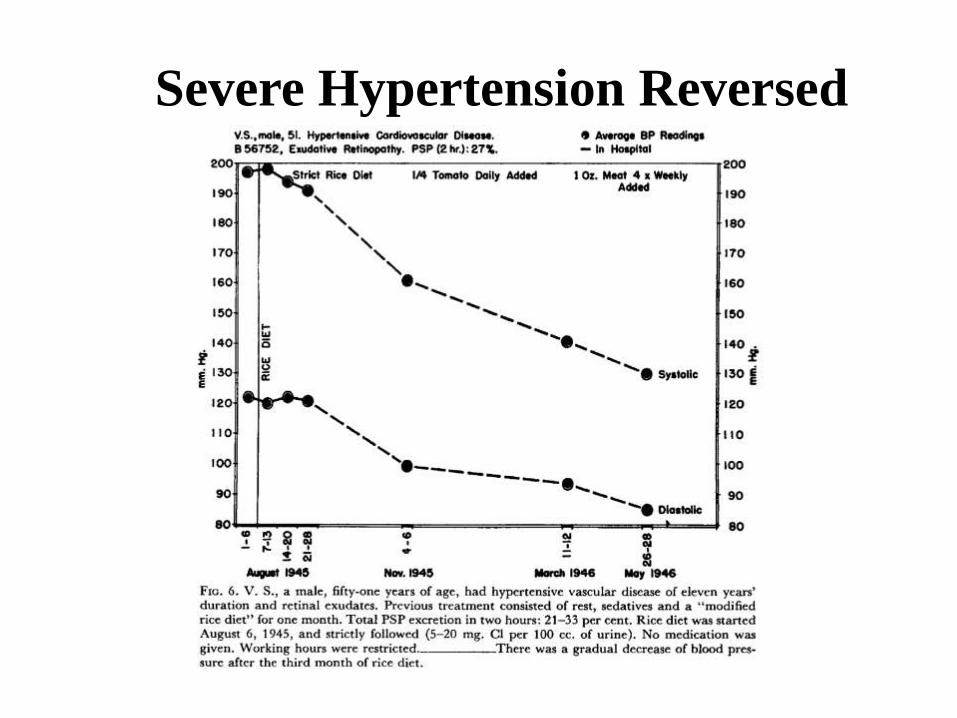
Severe Hypertension Reversed

*White sugar may be used as desired (ad libitum); on average a patient takes in about 100 grams
daily (400 calories) but, if necessary (to maintain body weight), as much as 500 grams (2000
calories) daily has been used.
Composition of the Rice Diet White Rice, Fruit, Juice, and Table Sugar (Vitamins)

Biography of Walter Kempner, MD

The McDougall Diet vs. The Rice Diet
Walter Kempner, MD was very influential on my career.
His published work showed me the power of diet therapy
and that nutritional deficiencies do not occur with simple
plant-based diets (even with the addition of lots of
sugar).

The McDougall Diet vs. The Rice
Diet
Before I was born (5-17-1947), Dr. Kempner had
disproven concepts that are still held as true by most
medical doctors today, such as:
“Diet has little to do with heart disease.”
“Additional protein improves health.”
“Carbohydrates cause diabetes.”

The McDougall Diet vs. The Rice Diet
The diet I recommend, the McDougall Diet, is for the
“living.”
The Rice Diet is one that I reserve for the
“nearly dead.”

10-Day Residential Program
Starch-based Meal Plans
Light Exercises
No Meditation, etc.
Medical Care
Medications Are Reduced
Can Be Held in Any Hotel
All-You-Can-Eat
(cafeteria style)

Weight Loss In 7 Days - Women
0
1
2
3
4
5
6
7 n = 1102
All 140-179 180-239 240-279 > 280
pounds
s
t
a
r
t
i
n
g
3.1
cafeteria-style eating

Weight Loss In 7 Days - Men
0
1
2
3
4
5
6
7
8
9
All 160-199 200-260 260-320 > 320
n = 580
pounds
s
t
a
r
t
i
n
g
3.6
cafeteria-style eating

Cholesterol Reductions In 7 Days n = 1692
mg
/dL
0
20
40
60
80
100
120
140
160
180
200
Day 1 Day 7 Average Maximum
22.3

Cholesterol Reductions In 7 Days
0
5
10
15
20
25
30
35
40
45
50
180-200 200-220 220-240 240-260 260-300 > 300
n = 1692
mg
/dL
s
t
a
r
t
i
n
g
The sicker they are
the better they get

BP Reductions in 7 Days
0
5
10
15
20
25
30
>160/100 140/90 to 160/100 120/80 to 140/90 110/70 to 120/80
mm
Hg
s
t
a
r
t
i
n
g
Systolic
Diastolic
23.9
14.5
High and
In need of Rx The sicker they are
the better they get

0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
45.00
50.00
Bas
elin
e
Mo
nth
1
Mo
nth
2
Mo
nth
3
Mo
nth
4
Mo
nth
5
Mo
nth
6
Mo
nth
7
Mo
nth
8
Mo
nth
9
Mo
nth
10
Mo
nth
11
Mo
nth
12
Po
st-6
wk
Po
st-6
mo
Fat
as a
pe
rce
nta
ge o
f C
alo
rie
s (%
)
Compliance Over 1 Year Based on % Fat
Diet Group
Control Group
OHSU Diet for Multiple Sclerosis Study McDougall Diet
OHSU / McDougall Diet & MS Study

166
168
170
172
174
176
178
180
182
Baseline Final Visit
172.4
174.3
181.1
171.1
Wei
gh
t (l
bs)
Average Weight Change in 1 Year
Control Group
Diet Group
N=29 N=32 N=27 N=26
OHSU Diet for Multiple Sclerosis Study McDougall Diet
OHSU / McDougall Diet & MS Study

150
155
160
165
170
175
180
185
Baseline Final Visit
172.4 174.3
181.1
162.0
Wei
gh
t (l
bs)
Average Weight Change in Compliant Patients
After 1 Year
Control Group
Diet Group
N=29 N=32 N=27 N=22
OHSU Diet for Multiple Sclerosis Study McDougall Diet OHSU / McDougall Diet & MS Study

0
20
40
60
80
100
120
140
160
180
200
Baseline Final Visit
112 106
56.2 56.8
89.2 86.8
186 180
LDL HDL Triglycerides Cholesterol
N=29 N=2
7
OHSU Diet for Multiple Sclerosis Study McDougall Diet OHSU / McDougall Diet & MS Study
Control Group Average Lipid Changes in 1 Year

0
20
40
60
80
100
120
140
160
180
Baseline Final Visit
101
83.6
57.8 57.1
95.0 91.7
178
159
Diet Group Average Lipid Changes in 1 Year
LDL HDL Triglycerides Cholesterol
N=3
1
N=2
2
OHSU Diet for Multiple Sclerosis Study McDougall Diet
OHSU / McDougall Diet & MS Study

Ad Libitum Starch Diet
10 Months 210 to 120 pounds 160/100 to 122/70 mmHg Glucose: 113 to 79 mg/dL Cholesterol: 181 to 123 mg/dL
http://drmcdougall.com/stars/elizabeth_teselle.htm

Ad Libitum Starch Diet
10 years ago 150 pounds Weight loss took 4 years
http://drmcdougall.com/stars/cathy_stewart.htm

Ad Libitum Starch Diet
http://drmcdougall.com/stars/mike_teehan.htm
331 to 165 Two years Cholesterol: 192 to 140 mgdL

Ad Libitum Starch Diet
http://drmcdougall.com/stars/joyce_rainwater.htm
Lost 110 pounds In 1991 (20 years ago)

Ad Libitum Starch Diet
Lost 149 pounds in 2 years Four years ago 146/86 to 105/64 mmHg Cholesterol:250s to 163 mg/dL
http://drmcdougall.com/stars/nettie_taylor.html

Ad Libitum Starch Diet Lost 77 pounds
http://drmcdougall.com/stars/donna_byrnes.html

Ad Libitum Starch Diet
http://drmcdougall.com/stars/karen_barron.html
Lost 100 pounds 7 years ago Cholesterol 281 to 142 mg/dL Glucose 103 to 78 mg/dL 140/90 to 115/75 mmHg

Ad Libitum Starch Diet
http://www.drmcdougall.com/stars/cloudy_rockwell.htm
Lost 92 pounds
In 2 years
1 ½ pounds a week
size 26 in jeans, to a size 4
Resolved stomach pains
knee and hip arthritis gone
"enough syndrome”
“not food approach”

John Figlar

John Figlar (MAPTB) Oct. 2010
372 pounds 120 Units Insulin One Diabetic Pill Three BP pills
Program Date: October 31, 2010 Weight 372.2 Blood sugar 131/219 Cholesterol 122/101 Triglycerides 113/101 Meds: Humunlin N 30 Humulin R 30 Actos 30 mg Varapamil 240 mg bid Benicar 40 mg Simvistatin 40 mg

John Figlar
April 11, 2011: 6 months Lost 98 pounds 142/84 mmHg Blood Sugars = 150 to 250 mg/dL No Medications

Drew Powell, 56

Drew Powell, 56
May, 2011 276 pounds Kombiglyze XR 5-1000 (metformin ER 1000mg / saxagliptin 5mg Blood sugars = +200 mg/dL HbA1c was 9.0 (04/21/2011)

Drew Powell, 56

Drew Powell, 56
August 12, 2011 In 90 days Down 30 pounds No Medications Blood sugars = 100 mg/dL HbA1c= 5.6 %

Drew Powell, 56
January 27, 2012 My HbA1c is 5.2% No medication My weight is 215 lbs. 37 inch waist My sleep apnea is gone I no longer use CPAP

Benjamin Eksouzian
Program Date: March 5, 2011 Weight: 313.4/310.2 Glucose: 152/129 Cholesterol 185/122 Triglycerides: 167/65 Medications: Glipizide: 5 mg bid Metformin 1000 mg bid Lisinopril 20 mg bid Lipitor 40 mg qd

Benjamin Eksouzian
4 Months later: July 12, 2011 268 pounds Lost 50 pounds No Medication Blood Sugars = 100 mg/dL Cholesterol = 202 mg/dL

Benjamin Eksouzian

Fat vs. Carbohydrate