Capturing Clinical Data to Monitor, Evaluate, & Improve .../media/Files/Activity...
37
Capturing Clinical Data to Monitor, Evaluate, & Improve Health Care Delivery & Outcomes for Persons Living with HIV/AIDS William M. Tierney, MD President and CEO Regenstrief Institute, Inc. Associate Dean for Clinical Effectiveness Research Indiana University School of Medicine
Transcript of Capturing Clinical Data to Monitor, Evaluate, & Improve .../media/Files/Activity...

Indiana UniversitySchool of Medicine
Capturing Clinical Data to Monitor, Evaluate, & Improve
Health Care Delivery & Outcomes for Persons Living with HIV/AIDS
Capturing Clinical Data to Monitor, Evaluate, & Improve
Health Care Delivery & Outcomes for Persons Living with HIV/AIDS
William M. Tierney, MDPresident and CEO
Regenstrief Institute, Inc.Associate Dean for Clinical Effectiveness Research
Indiana University School of Medicine
William M. Tierney, MDPresident and CEO
Regenstrief Institute, Inc.Associate Dean for Clinical Effectiveness Research
Indiana University School of Medicine

Indiana UniversitySchool of Medicine
Points to be discussedPoints to be discussed
● Capturing the requisite clinical data– registries vs. electronic health records– defining the core dataset
● Models for capturing & integrating clinical data– key components of effective models– collecting from healthcare providers vs. patients – policies, incentives, and adherence
● Recommendations

Indiana UniversitySchool of Medicine
RegistriesRegistries
Funding Agency
Funding Agency

Indiana UniversitySchool of Medicine
Electronic health records Electronic health records
Funding AgencyFunding Agency
HIV ClinicHIV Clinic
Funding Agency
Funding Agency
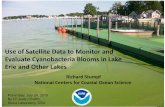
DISCORDANT COUPLES
70%
0%2%
12%
5%
4%
1% 3% 3%
MTRH Mosoriot Turbo Burnt Forest AmukuraChulaimboWebuyeNaitiriTeso
DISCORDANT COUPLES
70%
0%2%
12%
5%
4%
1% 3% 3%
MTRH Mosoriot Turbo Burnt Forest AmukuraChulaimboWebuyeNaitiriTeso

Indiana UniversitySchool of Medicine
Defining core data → who needs it?Defining core data → who needs it?
● Clinicians managing patients’ care● Health care system managers● Quality improvement programs● Ancillary upport programs● Patients and their families● Regulatory and funding agencies● Payers

Indiana UniversitySchool of Medicine
Example: HIV/AIDS in Africa Example: HIV/AIDS in Africa

Indiana UniversitySchool of Medicine

Indiana UniversitySchool of Medicine

Indiana UniversitySchool of Medicine

Indiana UniversitySchool of Medicine

Indiana UniversitySchool of Medicine
AMPATH: Academic Model Providing Access to Healthcare AMPATH: Academic Model Providing Access to Healthcare

Indiana UniversitySchool of Medicine

Indiana UniversitySchool of Medicine
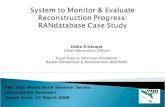
AMPATH patient enrollmentAMPATH patient enrollment
0
20,000
40,000
60,000
80,000
100,000
120,000
140,0002001NOV
DEC
2001JAN FEB
MAR APR
MAY
JUN
2002JUL AUG SEP
OCT
NOV DEC
2003JAN FEB
MAR APR
MAY
JUN
2003JUL AUG SEP
OCT
NOV DEC
2004JAN FEB
MAR APR
MAY
JUN
2004JUL AUG SEP
OCT
NOV DEC
2005JAN FEB
MAR APR
MAY
JUN
2005JUL AUG SEP
OCT
NOV DEC
2006JAN
2/1/2006
3/1/2006
4/1/2006
5/1/2006
6/1/2006
7/1/2006
8/1/2006
9/1/2006
10/1/2006
11/1/2006
12/1/2006
1/1/2007
2/1/2007
3/1/2007
4/1/2007
5/1/2007
6/1/2007
7/1/2007
8/1/2007
9/1/2007
10/1/2007
11/1/2007
12/1/2007
1/1/2008
2/1/2008
3/1/2008
4/1/2008
5/1/2008
6/1/2008
7/1/2008
8/1/2008
9/1/2008
10/1/2008
11/1/2008
12/1/2008
1/1/2009
2/1/2009
3/1/2009
4/1/2009
5/1/2009
6/1/2009
7/1/2009
8/1/2009
9/1/2009
10/1/2009
11/1/2009
12/1/2009
1/1/2010
2/1/2010
3/1/2010
4/1/2010
5/1/2010
6/1/2010
7/1/2010
8/1/2010
9/1/2010
10/1/2010
11/1/2010
12/1/2010
1/1/2011
2/1/2011
3/1/2011
Cumulative HIV+ Patients Enrolled: Nov ’01 – Mar ‘11

Indiana UniversitySchool of Medicine
AMPATH patient visitsAMPATH patient visits
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000Nov-01
Dec-01
Jan-02
Feb-02
Mar-02
Apr-0
2May-02
Jun-02
Jul-02
Aug-02
Sep-02
Oct-0
2
Nov-02
Dec-02
Jan-03
Feb-03
Mar-03
Apr-0
3May-03
Jun-03
Jul-03
Aug-03
Sep-03
Oct-0
3Nov-03
Dec-03
Jan-04
Feb-04
Mar-04
Apr-0
4May-04
Jun-04
Jul-04
Aug-04
Sep-04
Oct-0
4Nov-04
Dec-04
Jan-05
Feb-05
Mar-05
Apr-0
5
May-05
Jun-05
Jul-05
Aug-05
Sep-05
Oct-0
5Nov-05
Dec-05
Jan-06
Feb-06
Mar-06
Apr-0
6May-06
Jun-06
Jul-06
Aug-06
Sep-06
Oct-0
6Nov-06
Dec-06
Jan-07
Feb-07
Mar-07
Apr-0
7
May-07
Jun-07
Jul-07
Aug-07
Sep-07
Oct-0
7Nov-07
Dec-07
Jan-08
Feb-08
Mar-08
Apr-0
8May-08
Jun-08
Jul-08
Aug-08
Sep-08
Oct-0
8Nov-08
Dec-08
Jan-09
Feb-09
Mar-09
Apr-0
9May-09
Jun-09
Jul-09
Aug-09
Sep-09
Oct-0
9
Nov-09
Dec-09
Jan-10
Feb-10
Mar-10
Apr-1
0May-10
Jun-10
Jul-10
Aug-10
Sep-10
Oct-1
0Nov-10
Dec-10
Jan-11
Feb-11
Mar-11
Cumulative HIV+ Patient Visits: Nov ’01 – Mar ‘11

Indiana UniversitySchool of Medicine
AMPATH encounter forms AMPATH encounter forms
We got it wrongWe got it wrong

Indiana UniversitySchool of Medicine
AMPATH encounter forms AMPATH encounter forms

Indiana UniversitySchool of Medicine
AMPATH encounter forms AMPATH encounter forms

Indiana UniversitySchool of Medicine
AMPATH encounter forms AMPATH encounter forms

Indiana UniversitySchool of Medicine
AMPATH encounter forms AMPATH encounter forms

Indiana UniversitySchool of Medicine
AMPATH encounter forms AMPATH encounter forms

Indiana UniversitySchool of Medicine
AMPATH encounter forms AMPATH encounter forms

Indiana UniversitySchool of Medicine
AMPATH encounter forms AMPATH encounter forms

Indiana UniversitySchool of Medicine
AMPATH encounter forms AMPATH encounter forms

Indiana UniversitySchool of Medicine
AMPATH encounter forms AMPATH encounter forms

Indiana UniversitySchool of Medicine
AMPATH encounter forms AMPATH encounter forms

Indiana UniversitySchool of Medicine
AMPATH encounter forms AMPATH encounter forms

Indiana UniversitySchool of Medicine
AMPATH performance measuresAMPATH performance measures
● OBJECTIVE 1.1: Continue ART without interruption and increase enrolment● OBJECTIVE 1.2: Conduct home-based counseling and testing● OBJECTIVE 1.3: Improve and expand control of TB in the community and in HIV-TB co-infected patients ● OBJECTIVE 1.4: Provide support for social services, nutrition, economic, and psychosocial needs● OBJECTIVE 1.5: Strengthen clinic-based prevention programs● OBJECTIVE 1.6: Strengthen and expand community-based ART● OBJECTIVE 1.7: Enhance care coordination between AMPATH care sites● OBJECTIVE 2.1: Expand and strengthen community and workplace prevention programs● OBJECTIVE 2.2: Expand prevention and care programs for hazardous alcohol drinking● OBJECTIVE 2.3: Expand prevention and care programs for HIV-discordant couples● OBJECTIVE 2.4: Expand prevention and care programs for commercial sex workers and truckers.● OBJECTIVE 2.5: Expand prevention and care programs for patients at risk for STIs or who have STIs● OBJECTIVE 2.6: Expand prevention and care programs for children and adults with disabilities● OBJECTIVE 3.1: Assist communities and families to meet needs of orphans and vulnerable children● OBJECTIVE 3.2: Enhance economic security for AMPATH patients and their households● OBJECTIVE 3.3: Empower PLWHA to access legal services

Indiana UniversitySchool of Medicine
Capturing clinical dataCapturing clinical data
● Key components of effective models– standard minimum core dataset – only coded or numeric data– add items not usually captured– entered by the person collecting the dataØ clerksØ cliniciansØ ancillary support persons (e.g. social workers)
– take little if any extra time than normal duties
W.O.R.M.write once, read many times
W.O.R.M.write once, read many times●Health-related quality of life●Functional status●Severity of illness●Comorbid problems ●Socioeconomic issues
●Health-related quality of life●Functional status●Severity of illness●Comorbid problems ●Socioeconomic issues

Indiana UniversitySchool of Medicine
Combining data from multiple sourcesCombining data from multiple sources
● Interfaces between systems – different systems– different data– different coding– different output formats
● Requires standardizing data, coding, formats– requires custom programming in almost all cases– requires mapping of terms
● Push vs. pull
TOUGH!

Indiana UniversitySchool of Medicine
One solution → HIEs One solution → HIEs
● Upload data routinely from providers● Establish and maintain interfaces● Provide term mapping → interoperability

Indiana UniversitySchool of Medicine
Example: Indiana Network for Patient Care
Example: Indiana Network for Patient Care

Indiana UniversitySchool of Medicine
>60 hosps → >2M ED visits/yr All laboratoriesAll radiology centersIN Dept. of Public Health5 large payors→>600M claims19,000 physicians≈ 1,500 interfaces≈ 12 million individuals≈ 5 billion structured results
A Regenstrief Institute study indicated that nearly 60% of Indianapolis-area patients visit more than one area hospital system over a period of several years.
A Regenstrief Institute study indicated that nearly 60% of Indianapolis-area patients visit more than one area hospital system over a period of several years.
INPC

Indiana UniversitySchool of Medicine
Data captured in the INPC Data captured in the INPC
● Registration records → demographics● Text reports
– admission, discharge, outpatient visit notes– imaging, operative, and pathology reports
● Lab tests (numeric, coded)● Inpatient medications and immunizations● Outpatient medications (several PBMs)● Insurance claims

Indiana UniversitySchool of Medicine
Policies, incentives, & adherence Policies, incentives, & adherence
● Voluntary reporting● Required reporting
– by statute– to obtain funds for HIV/AIDS treatment
● Data extraction from EHRs – from individual systems – from health information exchanges
● Registries● Sentinel care systems
●Biased●Spotty adherence ●Not representative
●Biased●Spotty adherence ●Not representative
●Requires sanctions●Carrot and stick? ●Requires sanctions●Carrot and stick? ●Draconian●Most effective●Requires funding!
●Draconian●Most effective●Requires funding!
●Requires one or few national EHR systems → not in U.S.!
●Won’t have some key measures
●Requires one or few national EHR systems → not in U.S.!
●Won’t have some key measures
●HIEs are not sustainable●Won’t have some key measures ●HIEs are not sustainable●Won’t have some key measures ●Voluntary
●Biased ●Voluntary●Biased
●Most cost-effective●Selection process is
key to generalizability
●Most cost-effective●Selection process is
key to generalizability

Indiana UniversitySchool of Medicine
RecommendationsRecommendations
● For patients with frank AIDS or meeting CD4 criteria for anti-retroviral therapy– pay for care (already being done for most)– require minimum dataset for paymentØ core data → correct coding schemesØ standard transmission format
● For other HIV-infected patients – registry– consider prospectively selected sentinels

Indiana UniversitySchool of Medicine
Recommendations (2)Recommendations (2)
● Decide on the core (minimum) clinical data● Add key clinical data not typically in an EHR
– HIV risk factors, symptoms– severity of illness, HRQoL
● Include non-clinical measures– socioeconomic, psychosocial factors
● Obtain some key data directly from patients– direct queries (mail, e-mail)– online personal health records

Indiana UniversitySchool of Medicine
Thank you! Thank you!