
Capital & Coast DHB Board Financial Overview September 2018
105
CCDHB Financial Overview Page 1 September 2018 Capital & Coast DHB Board Financial Overview September 2018 Julie Patterson, Interim Chief Executive Officer Michael McCarthy, Chief Financial Officer CCDHB Public 7 November 2018 - Item 1.9 Chief Executive's Report 68
Transcript of Capital & Coast DHB Board Financial Overview September 2018

CCDHB Financial Overview Page 1 September 2018
Capital & Coast DHBBoard Financial OverviewSeptember 2018
Julie Patterson, Interim Chief Executive OfficerMichael McCarthy, Chief Financial Officer
CCDHB Public 7 November 2018 - Item 1.9 Chief Executive's Report
68
CCDHB Financial Overview Page 2 September 2018
INANCIAL PERFORMANCE RESULT AND OVERVIEWSummary
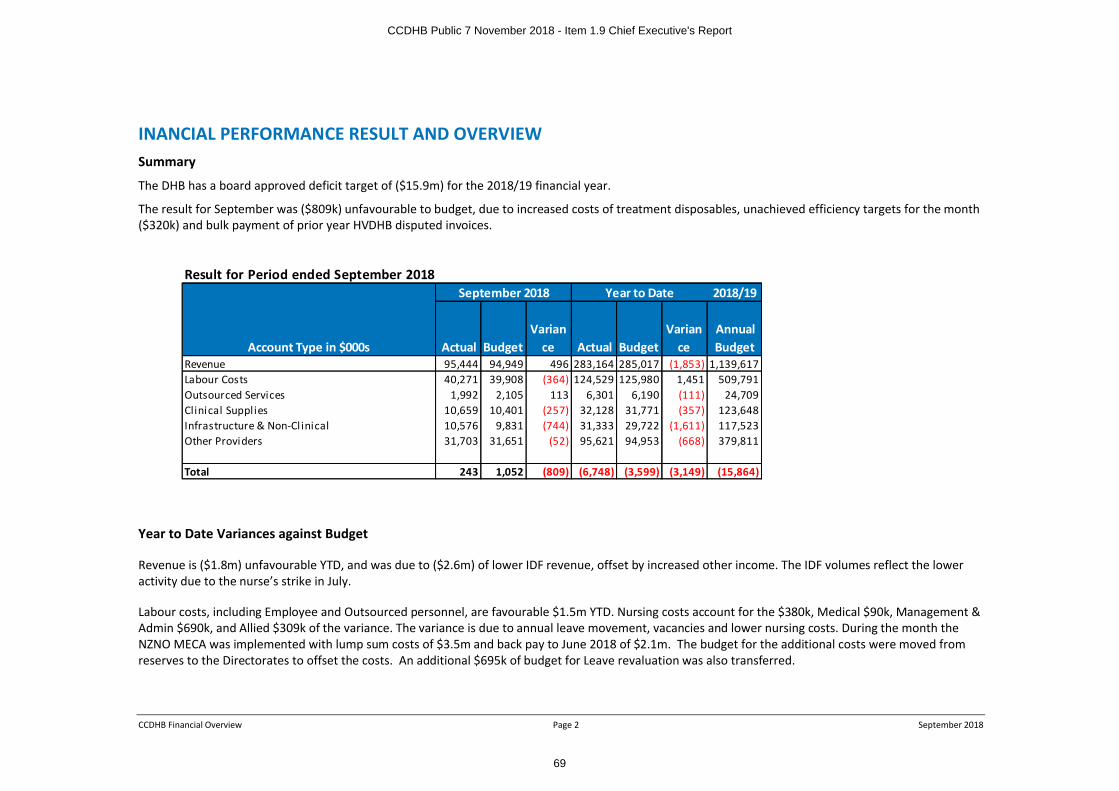
The DHB has a board approved deficit target of ($15.9m) for the 2018/19 financial year.
The result for September was ($809k) unfavourable to budget, due to increased costs of treatment disposables, unachieved efficiency targets for the month ($320k) and bulk payment of prior year HVDHB disputed invoices.
Year to Date Variances against Budget
Revenue is ($1.8m) unfavourable YTD, and was due to ($2.6m) of lower IDF revenue, offset by increased other income. The IDF volumes reflect the lower activity due to the nurse’s strike in July.
Labour costs, including Employee and Outsourced personnel, are favourable $1.5m YTD. Nursing costs account for the $380k, Medical $90k, Management & Admin $690k, and Allied $309k of the variance. The variance is due to annual leave movement, vacancies and lower nursing costs. During the month the NZNO MECA was implemented with lump sum costs of $3.5m and back pay to June 2018 of $2.1m. The budget for the additional costs were moved from reserves to the Directorates to offset the costs. An additional $695k of budget for Leave revaluation was also transferred.
Result for Period ended September 20182018/19
Account Type in $000s Actual Budget Varian
ce Actual Budget Varian
ce Annual Budget
Revenue 95,444 94,949 496 283,164 285,017 (1,853) 1,139,617Labour Costs 40,271 39,908 (364) 124,529 125,980 1,451 509,791Outsourced Services 1,992 2,105 113 6,301 6,190 (111) 24,709Clinical Supplies 10,659 10,401 (257) 32,128 31,771 (357) 123,648Infrastructure & Non-Cl inical 10,576 9,831 (744) 31,333 29,722 (1,611) 117,523Other Providers 31,703 31,651 (52) 95,621 94,953 (668) 379,811
Total 243 1,052 (809) (6,748) (3,599) (3,149) (15,864)
September 2018 Year to Date
CCDHB Public 7 November 2018 - Item 1.9 Chief Executive's Report
69
CCDHB Financial Overview Page 3 September 2018
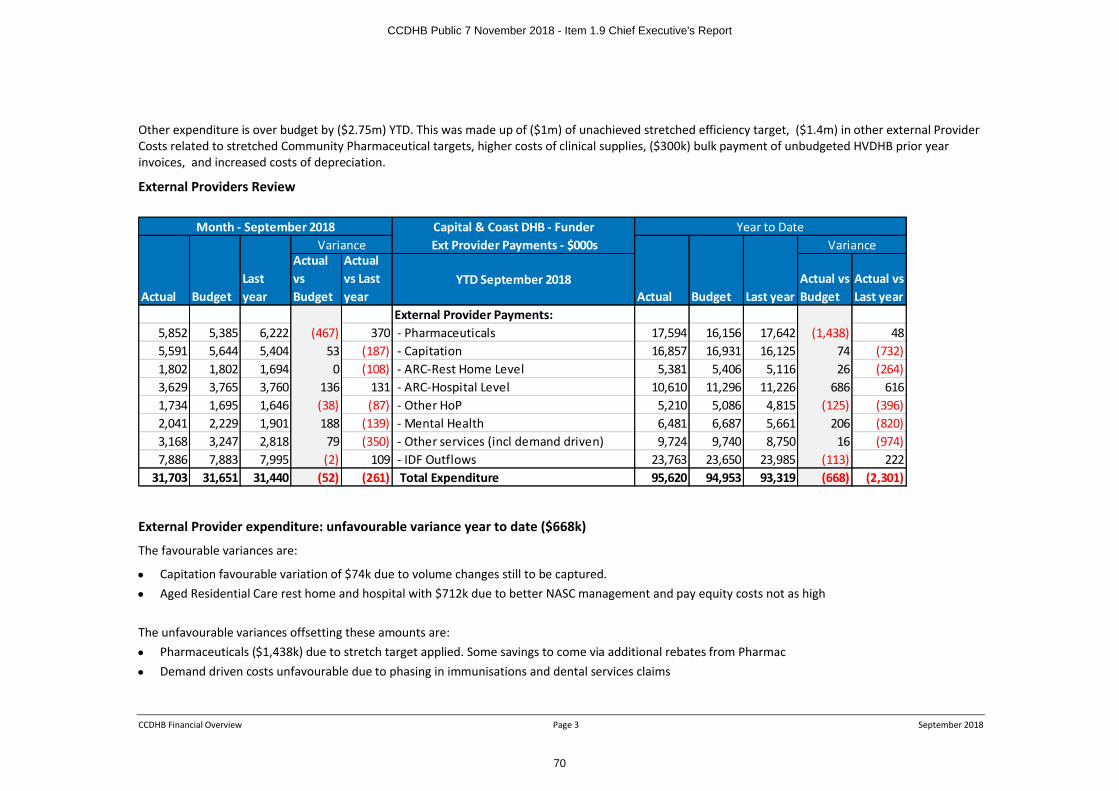
Other expenditure is over budget by ($2.75m) YTD. This was made up of ($1m) of unachieved stretched efficiency target, ($1.4m) in other external Provider Costs related to stretched Community Pharmaceutical targets, higher costs of clinical supplies, ($300k) bulk payment of unbudgeted HVDHB prior year invoices, and increased costs of depreciation.
External Providers Review
External Provider expenditure: unfavourable variance year to date ($668k)
The favourable variances are:
∑ Capitation favourable variation of $74k due to volume changes still to be captured. ∑ Aged Residential Care rest home and hospital with $712k due to better NASC management and pay equity costs not as high
The unfavourable variances offsetting these amounts are:∑ Pharmaceuticals ($1,438k) due to stretch target applied. Some savings to come via additional rebates from Pharmac ∑ Demand driven costs unfavourable due to phasing in immunisations and dental services claims
Capital & Coast DHB - Funder Ext Provider Payments - $000s
Actual BudgetLast year
Actual vs Budget
Actual vs Last year
YTD September 2018Actual Budget Last year
Actual vs Budget
Actual vs Last year
External Provider Payments:5,852 5,385 6,222 (467) 370 - Pharmaceuticals 17,594 16,156 17,642 (1,438) 485,591 5,644 5,404 53 (187) - Capitation 16,857 16,931 16,125 74 (732)1,802 1,802 1,694 0 (108) - ARC-Rest Home Level 5,381 5,406 5,116 26 (264)3,629 3,765 3,760 136 131 - ARC-Hospital Level 10,610 11,296 11,226 686 6161,734 1,695 1,646 (38) (87) - Other HoP 5,210 5,086 4,815 (125) (396)2,041 2,229 1,901 188 (139) - Mental Health 6,481 6,687 5,661 206 (820)3,168 3,247 2,818 79 (350) - Other services (incl demand driven) 9,724 9,740 8,750 16 (974)7,886 7,883 7,995 (2) 109 - IDF Outflows 23,763 23,650 23,985 (113) 222
31,703 31,651 31,440 (52) (261) Total Expenditure 95,620 94,953 93,319 (668) (2,301)
Variance VarianceMonth - September 2018 Year to Date
CCDHB Public 7 November 2018 - Item 1.9 Chief Executive's Report
70

CCDHB Financial Overview Page 4 September 2018
Employee FTE Financial Reporting to Ministry of Health (MOH Accrued FTE)
For financial accounting purposes MOH require an accrued FTE measure (as shown in the table below). This measure includes all hours on an accrual basis including leave accruals, overtime and casual hours. As an FTE measure this is highly volatile for a 24/7 facility due to the divisor being set based on the number of working days in the month. The Year to Date total is an average for the year. The average $ per FTE is impacted by MECA increases year on year.
Capital & Coast DHBMOH Accrued FTE
Actual Budget Last yearActual vs Budget
Actual vs Last year
YTD September 2018
Actual Budget Last yearActual vs Budget
Actual vs Last year
Annual Budget Average FTE Last year
FTE992 1,003 842 11 (150) Medical 963 971 865 8 (98) 952 865
2,483 2,533 2,223 49 (260) Nursing 2,361 2,399 2,236 39 (125) 2,400 2,236752 782 686 30 (66) Allied Health 742 756 705 14 (37) 736 705147 153 145 6 (2) Support 142 149 144 7 1 145 144918 948 830 30 (88) Management & Administration 910 934 853 23 (57) 913 853
5,292 5,419 4,726 127 (566) Total FTE 5,119 5,209 4,802 91 (317) 5,145 4,802Average $ per FTE
13,100 12,752 13,698 (349) 598 Medical 42,064 42,253 42,142 189 78 171,571 174,0976,453 6,176 6,724 (277) 270 Nursing 20,514 20,349 20,381 (165) (134) 84,155 86,3745,968 6,027 6,467 58 499 Allied Health 19,417 19,885 19,744 468 328 80,837 78,9174,236 4,254 4,521 19 285 Support 13,799 13,848 13,503 49 (296) 55,657 54,9555,685 5,868 6,033 184 349 Management & Administration 17,891 18,580 17,889 689 (2) 77,033 70,9977,435 7,264 7,740 (172) 304 Cost per FTE all Staff 23,758 23,861 23,559 104 (199) 97,793 97,412
AnnualVariance Variance
Month - September 2018 Year to Date
CCDHB Public 7 November 2018 - Item 1.9 Chief Executive's Report
71

CCDHB Financial Overview Page 5 September 2018
CCDHB STATEMENTS OF FINANCIAL POSITION
Aug -18 Capital & Coast DHB
Balance Sheet
Actual Actual BudgetSeptember 2017
At June 2018
Actual vs Budget
Actual vs September 2017 Notes
YTD September 2018
22 22 102 102 21 (81) (81) 1 Bank
2,795 3,477 19,825 23,411 17,581 (16,347) (19,933) 1 Bank NZHP
10,346 10,255 9,269 8,769 9,693 986 1,486 1 Trust funds
51,216 51,606 48,185 48,185 49,190 3,422 3,422 2 Accounts receivable
8,504 8,780 8,880 8,880 8,067 (99) (99) Inventory/Stock
5,183 5,655 6,789 6,789 3,075 (1,135) (1,135) Prepayments
78,065 79,795 93,050 96,136 87,628 (13,255) (16,341) Total current assets
551,744 553,128 552,613 459,424 555,233 515 93,703 Fixed assets
11,613 11,947 11,947 9,859 11,626 0 2,088 Work in Progress - CRISP
26,420 25,801 18,145 7,950 18,466 7,656 17,851 Work in progress
589,777 590,876 582,704 477,234 585,324 8,171 113,642 3 Total fixed assets
5,448 5,448 6,468 6,468 5,986 (1,020) (1,020) Investments in New Zealand Health Partnership
1,150 1,150 1,150 1,150 1,150 (1) (1) Investment in All ied Laundry
6,598 6,598 7,618 7,618 7,136 (1,020) (1,020) Total investments
674,439 677,268 683,372 580,988 680,088 (6,104) 96,281 Total Assets
0 0 0 0 0 0 0 Bank overdraft HBL
68,955 69,687 69,625 76,172 65,484 (63) 6,485 4 Accounts payable, Accruals and provisions
166 166 244 244 247 79 79 7 Loans - Current portion
4,115 6,173 6,170 0 (0) (3) (6,173) 6 Capital Charge payable
593 593 593 593 593 0 0 Insurance l iabi lity
30,170 26,496 25,792 24,212 24,750 (705) (2,285) 5 Current Employee Provisions
48,192 48,849 49,489 45,230 49,212 640 (3,619) 5 Accrued Employee Leave
7,242 10,051 7,423 7,423 17,818 (2,627) (2,627) 5 Accrued Employee salary & Wages
159,433 162,015 159,336 153,875 158,104 (2,679) (8,140) Total current liabilities
55 55 302 302 55 247 247 Crown loans
10,401 10,313 9,275 8,845 9,746 (1,038) (1,468) Restricted special funds
605 605 605 605 605 0 0 Insurance l iabi lity
5,642 5,642 5,868 5,868 5,642 226 226 Long-term employee provisions
16,703 16,615 16,050 15,620 16,048 (565) (995) Total non-current liabilities
176,136 178,631 175,387 169,495 174,151 (3,244) (9,135) Total Liabilities
498,304 498,638 507,986 411,492 505,936 (9,348) 87,145 Net Assets
764,628 764,402 764,631 769,398 768,845 (228) (4,996) Crown Equity
0 0 0 0 (3,484) 0 0 Capital repaid
136,496 136,813 136,776 23,671 136,404 37 113,142 Reserves
(402,820) (402,577) (399,421) (381,576) (395,830) (3,154) (21,000) Retained earnings
498,304 498,639 507,986 411,493 505,936 (9,347) 87,145 Total Equity
Month : September 18
Variance
CCDHB Public 7 November 2018 - Item 1.9 Chief Executive's Report
72

CCDHB Financial Overview Page 6 September 2018
Capital & Coast DHB
Statement of Cashflows
Actual Budget Last yearActual vs Budget
Actual vs Last year Notes
YTD September 2018Actual Budget Last year
Actual vs Budget
Actual vs Last year
Operating Activities
98,679 95,624 91,624 3,055 7,055 Receipts 293,170 285,181 275,681 7,989 17,489
Payments
39,537 41,913 37,413 2,376 (2,124) Payments to employees 128,554 127,440 113,410 (1,114) (15,144)
54,276 51,938 51,727 (2,338) (2,549) Payments to suppliers 164,727 156,534 155,551 (8,193) (9,177)
0 0 0 0 0 Capital Charge paid 0 0 0 0 0
733 246 246 (487) (487) GST (net) (505) (420) (420) 85 85
94,545 94,097 89,386 (448) (5,159) Payments - total 292,776 283,553 268,540 (9,223) (24,236)
4,134 1,528 2,239 2,607 1,896 6 Net cash flow from operating Activities 394 1,628 7,141 (1,234) (6,747)
Investing Activities
83 74 74 (9) (9) Receipts - Interest 448 248 248 (200) (200)
0 0 0 0 0 Receipts - Other 0 0 0 0 0
83 74 74 (9) (9) Receipts - total 448 248 248 (200) (200)
Payments
334 0 0 (334) (334) Investment in associates 334 0 0 (334) (334)
3,291 1,474 1,050 (1,817) (2,241) Purchase of fixed assets 13,969 5,976 3,919 (7,994) (10,050)
3,626 1,474 1,050 (2,151) (2,575) Payments - total 14,304 5,976 3,919 (8,328) (10,384)
(3,543) (1,400) (976) (2,160) (2,584) 7 Net cash flow from investing Activities (13,855) (5,727) (3,671) (8,528) (10,584)
Financing Activities
0 6,000 0 (6,000) 0 Equity - Capital 0 6,000 0 (6,000) 0
0 0 0 0 0 Other Equity Movement 0 0 0 0 0
0 0 0 0 0 Other 0 0 0 0 0
0 6,000 0 (6,000) 0 Receipts - total 0 6,000 0 (6,000) 0
Payments
0 0 0 0 0 Interest payments 81 0 0 (81) (81)
0 0 0 0 0 Payments - total 81 0 0 (81) (81)
0 6,000 0 (6,000) 0 8 Net cash flow from financing Activities (81) 6,000 0 (6,081) (81)
592 6,127 1,262 (5,554) (689) Net inflow/(outflow) of CCDHB funds (13,542) 1,901 3,470 (15,843) (17,413)
13,162 23,069 31,020 9,907 17,858 Opening cash 27,296 27,295 28,812 (1) 1,516
98,762 101,698 91,698 (2,954) 7,046 Net inflow funds 293,619 291,430 275,930 1,789 17,289
98,171 95,571 90,436 (2,600) (7,734) Net (outflow) funds 307,161 289,529 272,460 (17,632) (34,702)
592 6,127 1,262 (5,554) (689) Net inflow/(outflow) of CCDHB funds (13,542) 1,901 3,470 (15,843) (17,413)
13,754 29,196 32,283 (15,442) (18,529) Closing cash 13,754 29,196 32,283 (15,442) (18,529)
Variance
Year to DateMonth : September 18
Variance
CCDHB Public 7 November 2018 - Item 1.9 Chief Executive's Report
73

CCDHB Financial Overview Page 7 September 2018
Notes to the Balance Sheet and Cashflows
A) Notes to Balance Sheet:
1. The DHB’s cash balance at the end of September is lower than budget as the DHB has not drawn on budgeted equity injection.
2. Accounts receivable is $3.4m higher than budget due to timing differences. The 2 largest debtors are Hutt Valley DHB totalling $4.5M and Ministry of Health $4.6m.
3. Work in progress is higher than budgeted, with the Children’s Hospital and other project work running earlier than anticipated.
4. Accounts payable, accruals and provisions are in line with budget.
5. The employee salary accruals are higher than budgeted due to timing differences.
B) Notes to Cash flow statement:
6. The net cash receipts and payments from operating activities is in line with budget but lower than the prior year due to the payment of the NZNO settlement.
7. Cash flow on purchase of fixed assets is higher than budgeted due to the Children’s Hospital and other project work running earlier than anticipated.
8. There is a budgeted $6m equity injection this month but the DHB did not require this as yet, so this was not requested from the Ministry.
C) Ratios
9. Current Ratio – This ratio determines the DHB’s ability to pay back its short term liabilities. DHB’s current ratio is 0.49 (Aug 18: 0.49);
10. Debt to Equity Ratio - This ratio determines how the DHB has financed the asset base. DHB’s total liability to equity ratio is 26:74 (Aug 18 26:74).
CCDHB Public 7 November 2018 - Item 1.9 Chief Executive's Report
74

CCDHB Financial Overview Page 8 September 2018
Cash Forecast
This cash projection excludes the $15.9m deficit support. The cash forecast shows that we will need to draw down on deficit support to avoid going into overdraft. In January, there is a capital charge payment due of $15m. The working capital facility limit is $55.8m.
-70
-60
-50
-40
-30
-20
-10
0
10
20
30
40
50
60
70
80
90
100
110
120
130
140
01/0
7/18
08/0
7/18
15/0
7/18
22/0
7/18
29/0
7/18
05/0
8/18
12/0
8/18
19/0
8/18
26/0
8/18
02/0
9/18
09/0
9/18
16/0
9/18
23/0
9/18
30/0
9/18
07/1
0/18
14/1
0/18
21/1
0/18
28/1
0/18
04/1
1/18
11/1
1/18
18/1
1/18
25/1
1/18
02/1
2/18
09/1
2/18
16/1
2/18
23/1
2/18
30/1
2/18
06/0
1/19
13/0
1/19
20/0
1/19
27/0
1/19
03/0
2/19
10/0
2/19
17/0
2/19
24/0
2/19
03/0
3/19
10/0
3/19
17/0
3/19
24/0
3/19
31/0
3/19
07/0
4/19
14/0
4/19
21/0
4/19
28/0
4/19
05/0
5/19
12/0
5/19
19/0
5/19
26/0
5/19
02/0
6/19
09/0
6/19
16/0
6/19
23/0
6/19
$m
Week
Cash Forecast
Borrowing Limit Danger Zone Weekly Actual Cash Balance Weekly Forecasted Cash Balance
CCDHB Public 7 November 2018 - Item 1.9 Chief Executive's Report
75

PUBLIC
Capital & Coast District Health Board Page 1 [Oct 2018]
BOARD DECISION
Date: 7 November 2018
Author Rachel Haggerty, Director, Strategy, Innovation and Performance
Endorsed by Fran Wilde, Chair, Health System Committee
Subject HEALTH SYSTEM COMMITTEE RECOMMENDATIONS
RECOMMENDATIONS
The Health System Committee recommends to the Board that it:
(a) Agrees to the formation of eight Community Health Networks, noting that some flexibility will be required during the next phase of implementation planning;
(b) Endorses the focus on initiatives to improve service delivery models in Kāpiti with the intention of improving health outcomes and reducing the burden of travel for avoidable hospital care for the people of Kāpiti;
(c) Endorses the work of the Kāpiti Health Advisory Group and the need for collaboration between CCDHB and KHAG on developing Community Health networks and locality planning for Kāpiti;
(d) Endorses CCDHB, KHAG and community stakeholders collaborating on service development and Locality planning for the Kāpiti locality having regard for the five priority areas identified by KHAG above;
(e) Endorses the localities focus on South Porirua and the development of services to support the formation of the CHN within this locality. Noting, the importance of community responsiveness and the Committee’s request that staff bring back to the Board a graphic showing how CHNs and localities relate to each other;
(f) Writes to Government Ministers responsible for Housing asking they consider legislative amendments to regulate for safer home heating for all citizens;
(g) Writes to the Minister of Health in support of investment opportunities for healthy housing assessment and advice services to whānau with children experiencing asthma and acute upper respiratory tract infection;
(h) Discusses the issue of access to information on hours and qualifications level of the aged residential care and support workforce to the National DHB Chairs and Chief Executives meeting for discussion.
APPENDICES
1. Draft HSC Minutes 24 October 2018;2. Kapiti Health Advocacy Group (KHAG) presentation to Health System Committee.
1. PURPOSE
This report summarises the key discussions at Health System Committee on 24 October 2018 held at the Kāpiti District Council Chambers in Paraparaumu. The minutes of the meeting are attached as appendix one. The full papers from this meeting are available on Boardbooks.
2. DECISIONS
2.1 Community Health Networks – CCDHB Framework
Strategy Innovation and Performance (SIP) staff outlined the proposed Community Health Network (CHN) Framework and approach for implementing eight CHNs across the CCDHB district. There was robust discussion about the difference between a locality and a CHN and staff described how a CHN is an organising system for health services within a locality. The Committee request that staff create a graphic to show more clearly the relationship between a locality approach and a CHN. Committee members considered implementing CHNs will be a positive step for our local health system while being mindful of the need to
CCDHB Public 7 November 2018 - 3 FOR DECISION
76

PUBLIC
Capital & Coast District Health Board Page 2 [Oct 2018]
continue to emphasise equity factors and cultural responsiveness, which should be reflected more clearly in the proposed outcomes framework.
2.2 Kapiti – Delivering Care in the Community
This paper outlined the priorities identified by CCDHB to support the localities approach in Kapiti. It was considered at the same time as the presentation from the Kapiti Health Advocacy Group (see item 5 below).
2.3 Porirua –Supporting Equity and Outcomes
This paper outlined how CCDHB is approaching its localities work within Porirua. Effort is concentrated in support of South Porirua including reconfiguration of existing primary care funding and additional investment to support service integration as a first step. The Committee reiterated to staff the need to be clear about the differences between localities and CHNs. The Committee consider it is important to ensure there is authentic engagement and a strong community voice in this localities work and it is important to look beyond health sector partners to wider partners as the localities approach begins to be implemented. The Committee has advised staff that timelines are important and that we start to demonstrate progress with this work as it has been widely discussed with the community.
3. DISCUSSION ITEMS
3.1 Regional Public Health (RPH) Bi-Monthly performance update
The Committee noted the wide range of activity being delivered by RPH in Porirua and the need to be more joined up with the activity underway within the DHB. This will become more critical as the CHN and localities work gathers pace.
3.2 Healthy Housing update
RPH provided the committee with additional advice on the impact of its healthy housing initiatives in response to an action from the August HSC meeting. The report identifies substantial opportunity to improve health outcomes and suggests there are opportunities for enhanced investment in healthy housing assessments. Investing in healthy housing assessments for whānau with certain respiratory conditions, which do not currently meet criteria for funding (eg, asthma) would have a measurable impact on health outcomes including a reduction in hospital admissions for these conditions. The Committee considers the Board should write to Ministers endorsing an investment focus in this area.
3.3 MHAIDS Bi-monthly performance report
The Committee noted the report and the ongoing demand pressures on the MHAIDS service. The current suicide cluster within Porirua was discussed and staff noted they are working closely with wider social services to ensure the community receives the appropriate supports.
3.4 Maternity Quality Report
The Committee noted the report and discussed with staff the importance of good engagement with consumers, particularly Māori and Pacific new mums about their experiences. It was highlighted that there is a need to ensure that complaints processes are simple and fit for purpose.
The Committee also briefly discussed the primary birthing facility feasibility study and asked for a progress update on this work.
3.5 Investment and Performance – PHOS, Older Persons Services and Community Pharmacies
The Committee noted the report and its role in continuing to strengthen our understanding of how well our investments through national contracts meet the needs of our communities. Of particular interest being to understand the impact of these contracts on helping to address health equity. The Committee observed that having the data is valuable for highlighting the gap in outcomes particularly for Maori and Pacific but it is disheartening to see we are still to see an observable change in this area.
CCDHB Public 7 November 2018 - 3 FOR DECISION
77

PUBLIC
Capital & Coast District Health Board Page 3 [Oct 2018]
The Committee discussed the need to understand the skill mix and working conditions in our Aged Residentialfacilities. It considers this is an issue that should be raised at the national DHB Chairs and CEs meeting with a view to a collective DHB approach to the Ministry for access to relevant information.
4. FOR INFORMATION
4.1 CCDHB/RPH Submissions on legislation
Two submissions were prepared by RPH in support of legislative change to the Residential Tenancies Act (1986) and the establishment of Healthy Homes Standards. Both proposals would have a substantial health benefit for people living in rental accommodation through improved housing quality and more security of tenure. These submissions were prepared on our behalf in response to discussion at the August 2018 HSC meeting.
5. PRESENTATION BY KĀPITI HEALTH ADVOCACY GROUP (KHAG)
The Kāpiti Health Advocacy Group (KHAG) gave a presentation to the Committee outlining their priority areas and objectives for the health and wellbeing of the Kāpiti community. The presentation is attached as Appendix 2.
KHAG has given considerable thought to its priorities, which align well with the direction CCDHB has identified for Kāpiti. This reflects the ongoing emphasis on engagement with the KHAG and the community. The Committee considers these priorities provide a useful starting point for an ongoing collaborative approach between CCDHB, KHAG and other stakeholders in ongoing planning and implementing the localities approach for Kāpiti.
CCDHB Public 7 November 2018 - 3 FOR DECISION
78

1CCDHB Minutes – 24 October 2018
CAPITAL AND COAST DISTRICT HEALTH BOARDDRAFT Minutes of the Health System Committee (HSC)
Held on Wednesday 24 October 2018 at 9.30amKapiti District Council Chambers, 175 Rimu Road, Paraparaumu
PUBLIC SECTIONPRESENT:BOARD: Dame Fran Wilde (Chair)
Ms ‘Ana CoffeyMs Sue KedgleyDr Roger BlakeleyMs Eileen BrownMs Sue DriverDr Tristram Ingham
STAFF: Ms Julie Patterson, Interim Chief Executive arrives 9.39amMs Catherine Epps, Executive Director, Allied Health, Technical and ScientificMs Arawhetu Gray, Director, Māori Health ServicesMichael McCarthy, Chief Financial OfficerMr John Tait, Chief Medical Officer
CCDHB PRESENTERS: Ms Astuti Balram, Manager, Integrated Care, items 2.1 and 2.2Te Pare Meihana, General Manager, Child, Youth and Localities item 2.3Peter Gush, Service Manager, Regional Public Health, items 3.1 and 3.5Nigel Fairley, General Manager, 3DHB MHAIDSCarolyn Coles, Associate Director of Midwifery, item 3.3Wendy Devereux, MQSP Coordinator, item 3.3Sandra Williams, General Manager, Primary and Complex Care, item 3.4
KHAG PRESENTERS: Kathy Spiers, Kāpiti Health Advocacy GroupAdrian Gregory, Kapiti Health Advocacy GroupSandra Daly, Kapiti Health Advocacy GroupMarilyn Stevens, Kapiti Health Advocacy GroupNgaire Cook, Kapiti Health Advocacy GroupConrad Petersen, Kapiti Health Advocacy GroupSandra Forsyth, Kapiti Health Advocacy Group
GENERAL PUBLIC: One member of the public was present____________________________________________________________________________
1 PROCEDURAL BUSINESS
1.1 PROCEDURALThe Karakia was led by Tristram Ingham. Committee Chair, Dame Fran Wilde, welcomed the public, members and the DHB staff.
1.2 APOLOGIESApologies received from Andrew Blair and Tino Fa’amatuainu Pereira
1.3 INTERESTS1.3.1 Interest RegisterCommittee members to advise any changes to the Committee Secretary.
CCDHB Public 7 November 2018 - 3 FOR DECISION
79
2CCDHB Minutes – 24 October 2018
1.4 CONFIRMATION OF PREVIOUS MINUTESThe minutes of the CCDHB Health System Committee held on 26 September, taken with public present, were confirmed as a true and correct record.
Moved: Roger Blakely Seconded: Sue Kedgely Carried:
1.5 MATTERS ARISING
1.6 ACTION LIST
The reporting timeframes on the other open action items were noted.
1.7 HSC Work ProgrammeThe Committee noted the plan.
Actions:1. Committee Secretary to start on 2019 Work Programme.
Note the agenda items are presented in the order that the Board considered them.
2 FOR DECISION
2.1 Community Health Networks – the CCDHB Framework
The paper was taken as read.
The Committee:
a. Noted that as identified in the Health System Plan, Community Health Networks are CCDHBs mechanism to organise health services to meet the needs of the population in the network.
b. Noted the attached framework provides a detailed description of the Community Health Networks as a supplement to the Health System Plan. It has been developed in partnership with the stakeholders from across the sector through the Integrated Care Collaborative (ICC). It provides the platform for establishing the Networks in the future.
c. Noted the framework has been endorsed by the Integrated Care Collaborative which includes representatives of primary and secondary care.
d. Endorsed the outcome measures for Networks as outlined in the paper and the development of Network specific measures as they are established
e. Noted that Health Care Homes and primary care practices will form the core of the Networks, supported by connected specialist services.
f. Endorsed the formation of eight Community Health Networks, noting that some flexibility will be required during the next phase of implementation planning.
i. Endorsed the initial focus on Porirua South and Kāpiti in the establishment of Community Health Network prototypes.
Discussion:∑ Prior to discussing the paper, the Committee asked Arawhetu to provide an overview of how
the Community Health Networks, Healthcare Homes, PHOs, NGOs RPH and the Localitiesapproach fit in together. The Committee asked for a diagram to be developed and brought back to a future meeting to show the interconnections between these. It was noted this diagram would also be useful for engaging with communities.
CCDHB Public 7 November 2018 - 3 FOR DECISION
80

3CCDHB Minutes – 24 October 2018
∑ The Community Health Networks (CHN) is a developmental process. As a concept it is wellsupported by the Integrated Care Collaborative (ICC) and the document incorporates feedback from PHOs. Primary healthcare is excited about the opportunities for strengthening relationships through this new way of working.
∑ There was discussion around being careful not to confuse demographic and geographic means of determining an area suitable for a network. Staff clarified that both demographics and geography was used to define the proposed network areas.
∑ It was noted that we need to think beyond primary health care and consider the role of public health within a network.
∑ Eileen asked whether there are sufficient resources to implement the proposed approach and Sue Driver noted we need to look at our skill levels in coordinating potentially competing groups. Staff noted that investment proposals would be put forward to support network infrastructure and governance.
∑ The Committee acknowledged that CHNs are a step forward in terms of health systemmaturity. They will provide a vehicle for change.
∑ The Chair asked that the Committee receive six monthly reports on progress with implementation as well as any issues in particular for Kāpiti and Porirua.
∑ Tristram suggested that equity measures and cultural responsiveness be more explicit in the outcomes framework
∑ Sue Driver suggested that the Cost quadrant of the proposed outcomes framework should be refined to reflect efficient use of resources and cost-effectiveness rather than simply cost.
HSC recommends the Board:
a) Notes the Committee has considered the proposed framework for implementing Community Health Networks and endorses this mechanism for connecting health services within our communities.
b) Note that Health Care Homes and primary care practices will form the core of the Networks supported by connect specialist services for effectiveness and efficiency.
c) Note the CHN framework has been endorsed by the Integrated Care Collaborative which includes representatives of primary and secondary care.
d) Agrees to the formation of eight Community Health Networks, noting that some flexibility will be required during the next phase of implementation planning.
e) Note that SIP will report six monthly to the Committee on progress with implementing CHNs including any issues and how these are resolved.
Actions:1. Staff to develop a diagram for presenting at a future Committee meeting showing the
interconnections between PHOs, NGOs, Health Care Homes, RPH within Community Health networks and the relationship with Localities.
2. SIP to provide the Committee with six monthly implementation progress updates including any issues, particularly for Kāpiti and Porirua.
3. Outcome measures to include equity and cultural responsiveness4. Look at feasibility of developing outcomes measures that reflect efficiency and cost-
effectiveness rather than simply reduced costs
Moved: Eileen Brown Seconded: Sue Driver Carried:
2.2 Kapiti – Delivering care in the community
See end of minutes - paper was considered at the end of the meeting along with the presentation from the Kapiti Health Advocacy Group.
CCDHB Public 7 November 2018 - 3 FOR DECISION
81

4CCDHB Minutes – 24 October 2018
2.3 Porirua – Supporting Equity and Outcomes
The paper was taken as read.
The Committee:
a) Noted we are prioritising the development of our localities approach in Porirua through targeted investment during 2018/19 and the establishment of a localities plan grounded in partnership, reciprocity and strong communication and engagement.
b) Noted the focus on South Porirua to reconfigure existing funding as well as additional marginal investment in key service development/integration priorities:
∑ Nurse-led services to work with family groups in our Pacific neighbourhoods with multiple and complex health services.
∑ Youth services for young people who need greater support including sexual health, mental health and addiction and gender/sexual identity.
∑ Services to support mothers and families with babies and young children who need greater support in this start of life.
c) Endorsed the focus on South Porirua and the development of services to support the formation of the Community Health Network within this locality.
Discussion:∑ ‘Ana noted there is still some confusion between Community Health Networks and Localities
approaches. There needs to be responsive community engagement and discussion that enables a community led rather than a network discussion. She invites the SIP team to present to Porirua City Council and meet with community representatives, in particular, on the issues of children and youth. There are lots of conversations taking place on social media, noting concern with recent suicides. As a DHB, we need to figure out how we can engage with these conversations.
∑ Eileen Brown queried whether we are well equipped to be responsive to urgent and immediate issues such as recent suicides when they arise.
∑ The Porirua locality plan is still in development. The timeline is to be advised. Sue Driver noted we do need to become clearer on timelines.
∑ Porirua has a strong community. Both Roger and Tristram felt that it would be an opportunity lost if the approach did not begin with the voice of the Porirua community.
∑ Tristram Ingham noted we should include non-health sector partners in our engagement.
HSC recommends the Board:
a) Endorses the localities focus on South Porirua and the development of services to support the formation of the Community Health Network within this locality, noting the importance of community responsiveness and the Committee’s request that staff bring back to the Board a graphic showing how community health networks and localities relate to each other.
Actions:1. Report to the Board on the progress of Community Health Network in Porirua at a future
meeting. 2. Staff to present the localities work to the Porirua City Council following invitation by ‘Ana
Coffey.
Moved: Roger Blakely Seconded: ‘Ana Coffey Carried:
CCDHB Public 7 November 2018 - 3 FOR DECISION
82
5CCDHB Minutes – 24 October 2018
3 FOR DISCUSSION
3.1 Regional Public Health Bi-Monthly Performance Report
The paper was taken as read.
The Committee:
a) Noted the update on work in Porirua.
b) Noted the update on alcohol related harm reduction (including Kapiti).
c) Notes the update on public health nurse services in primary and intermediate schools in the CCDHB area.
d) Noted the update on influenza surveillance and SHIVERS II research project
e) Noted the update on the Australasian Tuberculosis conference 2018.
f) Noted the RPH 2017-2018 visual ‘snapshot.’
Discussion:∑ Committee was interested to see the range of activities being delivered by RPH within Porirua
and noted this work needs to be joined up with the activity underway to develop Community Health Networks and establish localities approaches.
∑ Sue Driver noted she still struggles to see the strategic framework that RPH is working within and the need to make connections between the DHB’s strategic direction and that of RPH.
∑ Chair requested staff work towards future Committee papers incorporating an RPH perspective rather than separate papers so that issues can be considered from multiple perspectives in a coherent way.
∑ ‘Ana noted the liquor licensing activity and asked about the evidence of the impact of this activity on reducing alcohol harm including hospital admissions for this community.
∑ Chair suggests that the RPH work programme updates could be reduced to six monthly to allow a more thorough discussion.
HSC recommends the Board:
a) Note the paper.
Actions:∑ RPH to provide evidence on how liquor licencing impacts hospital admissions in the Porirua
community∑ CCDHB staff to look at how RPH perspectives could be incorporated into future issues based
Committee papers. ∑ RPH performance report be reduced to a six month frequency.
3.5 Healthy Housing Update
The paper was taken as read.
The Committee:
a) Noted the information provided as an update from the housing discussion of HSC August 2018 meeting.
b) Considered the investment opportunity proposed for healthy housing assessment and advice services to be provided by Well Homes to those whānau with children experiencing Asthma and Acute upper respiratory tract infection.
CCDHB Public 7 November 2018 - 3 FOR DECISION
83

6CCDHB Minutes – 24 October 2018
c) Noted the interim report on Well Homes services provided for Pacific whānau 1 March – 31 August 2018 as interim data prior to definitive qualitative analysis that will emerge from the Well Homes programme evaluation being done in 2019.
Discussion:∑ Roger recommended to Regional Public Health to get the discount rate linked into the
Wellbeing Budget. ∑ Eileen Brown requested that the submissions on the Healthy Homes Standards and the
Residential Tenancies Act (1986) to be made publicly available. ∑ Letter to the Chair of Greater Wellington Regional Council on the Housing Improvement
Regulation has been prepared and to be sent and copied to the Committee.∑ Chair recommends to write separate letter to the Government to regulate safe home heating
for all citizens.∑ Discussed the list of potentially avoidable hospitalisations due to the home environment
diseases (PAHHE) and the exclusion of some key illnesses from Ministry of Health criteria for funding for healthy housing assessment – notably asthma and acute upper respiratory tract infections including croup. The Committee agreed this was an investment opportunity that would support achieving health equity. The Chair suggested the Board should write to the Minister in support of extending investment to this group.
HSC recommends the Board:a) Note the paper
o To write to Government Ministers responsible for Housing asking they consider legislative amendments to regulate for safer home heating for all citizens
o To write to the Minister of health in support of investment opportunities for healthy housing assessment and advice services to whānau with children experiencing asthma and acute upper respiratory tract infection.
Actions:1. Load the Healthy Housing paper onto the resource centre in Board books
2. Publish the submissions to the consultations on the Healthy Homes Standards and the Residential Tenancies Act (1986) on the website
3. RPH to draft a letter on behalf of the Board to Government Ministers asking them to consider legislative change that would support safer home heating methods.
4. RPH to draft a letter on behalf of the CCDHB to the Minister of Health asking that extending investment in healthy housing assessments to whanau with asthma or acute upper respiratory conditions be considered. ..
Moved: Eileen Brown Seconded: Sue Kedgley Carried:
3.2 MHAIDS Bi-Monthly Performance Report
The paper was taken as read.
The Committee:
a) Noted MHAID Service formally opened a new space for the MHAID Service Consumer Advisory Group, this is based at Kenepuru in the Te Manaaki building.
b) Noted the Ministry of Health has released the Suicide Facts: Data Tables for 1996 – 2015 with some significant findings, as listed in this report.
CCDHB Public 7 November 2018 - 3 FOR DECISION
84

7CCDHB Minutes – 24 October 2018
c) Noted The final Kahukura project for the Regional Rehabilitation and Extended Care Inpatient Service’s (RRS) current model of care (MoC) has been completed. A model of care clinical group is being established to lead the implementation of the operational recommendations.
Discussion:∑ The Ministry of Health has confirmed a cluster of suicides in Porirua and CASA has been
activated. We are working closely with schools, NGOs and Porirua Council, to ensure we respond in the best way.
∑ There was a question from ‘Ana Coffey linked to the earlier discussion on the number of suicides in Porirua and community use of social media. ‘Ana asked if the DHB utilised social media to connect with parents, communities on suicide prevention and postvention information. Staff noted that we do not use social media for this particular issue as it has pluses and minuses but that we can look at this issue once again and report back our findings.
∑ Staff noted we are also changing our prevention/intervention/postvention approach and the Board has previously agreed to a zero tolerance for suicides project, which is progressing.
∑∑ Tristram Ingham asks if there is a strategy in place within the next 6 to 12 months to reduce
demand for acute services. Since 1 October 2018, measures have been put in place to remediate the demand levels. Further upstream investment needs to be worked through and discussed.
∑ The Committee asked for an update on the current status of the MHAIDS Integration project.
HSC recommends the Board:b) Notes the report. .
Actions:
1. Staff to re-look at the use of social media as a means of engaging with communities and report back to the Committee
3.3 Maternity Quality Report
The paper was taken as read.
The Committee:a) Noted the publication of the Women’s Health Service Annual Clinical Report 2017.
b) Noted the publication of the Maternity Quality & Safety Programme Plan 2018-2019.
c) Noted the Ministry of Health development of maternity services whole of system work programme.
d) Noted strategic work the service is undertaking to improve equity in relation to women and babies.
Discussion:∑ Timeline on the development of the feasibility study on a primary birthing facility in central
Wellington was requested. A survey has gone out to the consumers and health providers. The information is being collated currently and we are waiting for the finalised results.
∑ MQSP consists of 2 LMCs representative and 2 consumer group representatives who feedback to and from DHB, they are involved on the development of projects, feedback outcomes affected by the communities. The LMCs network is independent across all DHBs. CCDHB has regular meetings with the LMCs. Operation Managers and Clinical Leaders attend these meetings as well. These meetings provide a platform for the LMCs to voice their concerns. If women in the community have a complaint forms are available for consumers to feedback anonymously.
CCDHB Public 7 November 2018 - 3 FOR DECISION
85

8CCDHB Minutes – 24 October 2018
∑ ‘Ana noted it was important that all consumers had a voice and there would be value in engaging with the Sub Regional Pacific Health Advisory Board and the Maori Partnership Board on ways to ensure the voices of young Māori and Pacific women could be heard.
HSC recommends the Board:a) Note the paper.
Actions:
1. Staff to discuss the Maternity Quality Report with the Maori Partnership Board and the Sub Regional Pacific Health Advisory Board
Moved: ‘Ana Coffey Seconded: Eileen Brown Carried:
3.4 Investment and Performance – PHOs, Older Persons Services and Community Pharmacies
The paper was taken as read.
The Committee:a) Noted that from 1 December this year the Budget 2018 initiatives to provide people with
greater access to primary care which will include access to low-cost general practice visits to all community service card holders; and free general practice visits for children under the age of 14.
b) Noted that in 2018/19 CCDHB will invest $67 million in local providers under the nationally negotiated Aged Residential Care Agreements for services that include rest home, continuing care, dementia and psychogeriatric services;
c) Noted that in 2018/19 CCDHB will invest $86 million in local providers under the nationally negotiated Community Pharmacy Services Agreements for services that include dispensing and other services provided by community pharmacies and the costs of the pharmaceuticals dispensed;
d) Noted the dashboards continue to show similar trends in performance and equity gaps. HealthCare Homes and the 1 December implementation of the lower cost general practices fees for community services care holders and thirteen year olds is expected to reduce barriers to access and improve health outcomes for our population.
e) Noted this reporting is part of our process of improving our understanding of how our investments in the national agreements for community pharmacy, primary health organisations and aged residential care, are working for our population including equity (or not) of access to health services, ensuring these services are high quality and safe, and understanding how they improve health outcomes in our community.
Discussion:∑ Members asked about qualifications for Aged Residential Care workers. The aged residential
care and support workforce do require qualifications and the pay scale is related to qualification. However, we as DHB do not have the information on the hours and qualifications for the aged residential care and support workforce within specific facilities thisinformation is collected by the Ministry but not shared with the DHBs.
∑ Sue Kedgley suggests that the DHBs collectively request that the national agreement be amended to require the release of information on qualifications and hours to DHBs.
∑ Tristram pointed out that equity has been a hot topic and he is disappointed to see that equity is still not translating in performance. Community Health Networks and Locality approaches will see an improvement. The Māori Health Strategy includes an action plan including specifics, timeframe and KPIs to address equity.
CCDHB Public 7 November 2018 - 3 FOR DECISION
86

9CCDHB Minutes – 24 October 2018
∑ The Committee to look more closely at the dashboard at the next meeting. ∑ Eileen commented that from 1 December 2018 the Budget 2018 initiatives to provide people
with greater access to primary care is good news.
HSC recommends the Board:a) Notes the paper.b) To take the issue of access to information on hours and qualifications level of the aged
residential care and support workforce to the National DHB Chairs and Chief Executives meeting for discussion.
Actions:1. To work with the DHBs to requests from the Ministry for the information on the qualifications
level and hours of the aged residential care and support workforce.
4 FOR INFORMATION
4.1 CCDHB/Regional Public Health Submission on Legislation
The paper was taken as read.
The Committee:
a) Noted the attached submissions prepared by Regional Public Health on behalf of the Committee for the Healthy Housing Standards and the Residential Tenancies Act (1986).
HSC recommends to the Board:a) To note the paper.
PRESENTATION BY KĀPITI HEALTH ADVOCACY GROUP
Kathy Spiers (Chair) introduced the Group. The group has been established for 18 months and they meet on the monthly basis. Kathy also introduced Mayor Guru briefly talked about history Kāpiti health, the community health work, transport issues, accessibility. He would like to work with CCDHB on the KāpitiLocality plan. Adrian Gregory gave a presentation on the purpose, objectives and priorities of Kāpiti Health Advocacy Group.
The Committee noted the presentation.
Discussion:∑ There are opportunities for CCDHB and KHAG to align their priorities in terms of health needs and
locality.∑ There needs more inclusion of the voices of the younger people. KHAG has been working with primary
schools and counsellors. KHAG is also doing their best to get greater representation across all demographics to address the equity issue.
∑ Otaki boundary. KHAG said this issue needs to be recognise and find a short and medium term solutions. It has to do with how effectively communicate with the residents of Otaki through social media. The CEs of CCDHB and MidCentral are meeting on 1 November to discuss this issue and plan to put together a MOU. Julie will report back to the Board after the meeting.
HSC recommends to the Board:
a) That CCDHB and Kāpiti Health Advocacy Group (KHAG) and its stakeholders collaborate proactively on the development of a Kāpiti Health and Wellbeing Locality Plan based on the five priority areas and that the planning group should:
CCDHB Public 7 November 2018 - 3 FOR DECISION
87

10CCDHB Minutes – 24 October 2018
∑ Reflect on the implementation of the Otaki Health and Wellbeing Plan and the establishment of the Otaki Health and Wellbeing Advisory Group
∑ Establish and sustain open, two-way channels of communication∑ Adopt an effective community engagement and communication plan∑ Maintain an evidence-based annual review of progress towards and, post-implementation, the
outcomes of the Locality Plan.
Sue Kedgley and Roger Blakely left at 12.20pm
2 FOR DECISION
2.2 Kāpiti – Delivering Care in the Community
The paper was taken as read.
The Committee:
a) Noted CCDHB is prioritising the development of our localities approach in Kāpiti, as well as Porirua, through targeted service development and investment during 2018/19.
b) Noted that with the Kāpiti community our locality focus is supporting service delivery models that support care closer to home to improve outcomes and ensure people do not travel unnecessarily for hospital and specialist care that is avoidable.
c) Noted the progress of an acute and urgent care model development, telehealth trial, Health of Older People service development and medication management service development alongside Healthcare Home development are priorities within Kāpiti.
d) Noted the change to the shuttle service from Kenepuru to Wellington Hospital increasing the number of patients from Kāpiti using the shuttle.
e) Endorsed the ongoing development of the initiatives to improve service delivery models in Kāpiti with the intention of improving health outcomes and reducing the burden of travel for avoidable hospital care for the people of Kāpiti.
HSC recommends the Board:
a. Endorse the focus on initiatives to improve service delivery models in Kāpiti with the intention of improving health outcomes and reducing the burden of travel for avoidable hospital care for the people of Kāpiti.
b. Note and endorse the work of the Kāpiti Health Advisory Group and the need for collaboration between CCDHB and KHAG on developing Community Health networks and locality planning for Kāpiti.
Moved: Tristram Ingham Seconded: Eileen Brown Carried:
The Chair noted that Catherine Epps will be leaving CCDHB and this will be her last meeting. The Chair thanked Catherine for her support.
The meeting closed at 12.50.
5 DATE OF NEXT MEETING
28 November 2018, 9.30am, Board Room, Level 11, Grace Neill Block, Wellington Regional Hospital.
CCDHB Public 7 November 2018 - 3 FOR DECISION
88

Kāpiti Health Advocacy Group
Presentation to CCDHB
Health System Committee
24 October 2018
Kāpiti Health Advocacy Group
Kāpiti Coast District Council
CCDHB Public 7 November 2018 - 3 FOR DECISION
89
The Kāpiti Health Advocacy Group
u The Group was initiated by Mayor Gurunathan
u Its first meeting was on 22 March 2017 and was attended by 32 people from across community health, wellbeing and social groups
u A workshop was held on ‘What is Working Well, What is not Working Well, Where are the Gaps?’
u The work of the Health Advocacy Group, which is chaired by Kathy Spiers, covers the health needs of the Kāpiti Coast community from Paekakariki to Ōtaki
u The Kāpiti Hospital Petition Group was also formed as a result of this first meeting
CCDHB Public 7 November 2018 - 3 FOR DECISION
90
Our Stakeholders
u The Kāpiti Coast community
u Kāpiti Coast District Council
u Capital & Coast District Health Board #
u MidCentral District Health Board (Ōtaki Health & Wellbeing Plan)
u Compass PHO & Central PHO
u Wellington Free Ambulance & St John Ambulance Services
u Home Support Services
u NGO’s and like organisations across the health and wellbeing spectrum
u Local iwi
# KHAG acknowledges the support of Jane Presto re the development of a CCDHB Locality Plan
CCDHB Public 7 November 2018 - 3 FOR DECISION
91

Purposes & Objectives
PURPOSES
Our Purposes are to:
u Identify health needs of Kāpiti’s population of 52, 762
u Prioritise identified needs
u Advocate for improved health services
u Enhance health services across the community in partnership with our stakeholders
u Evaluate long-term outcomes
OBJECTIVES
Our Objectives are to:
u Gather information that will assist in identifying the community’s health and associated needs
u Empower our community to articulate their health and social needs
u Identify where needs are not adequately being met
u Identify other factors that impact on or are determinants of health status
u Identify potential for resources to be regenerated, reallocated or remodelled
CCDHB Public 7 November 2018 - 3 FOR DECISION
92
Aligned with CCDHB’s strategic purpose and investment in services…
u Simplify service delivery for those people who have good knowledge and resources
u Intensify service delivery for those who are vulnerable to achieve equity
u Work with communities to improve health and wellbeing
u Act early to improve outcomes and make better use of time and money
u Work together in interdisciplinary teams to provide better solutions in homes, communities and hospitals
u Innovate using technology to improve knowledge, choice and access to healthcare
u Efficient use of resources in homes, communities and hospitalsRef: CCDHB Public 21 February 2018 – Item 3.2 Recommendations from CPHAC
CCDHB Public 7 November 2018 - 3 FOR DECISION
93

Priorities 2018
1. Access to Services (including Transport)
2. Urgent Care (otherwise referred to as Accident & Out of Hours)
3. Mental Health Services
4. Care of Older People
5. Care for people with Disabilities
NB: children and young people are incorporated under priorities 1, 2 3, and 5
CCDHB Public 7 November 2018 - 3 FOR DECISION
94
Priority 1 – Access to ServicesISSUES
u Services at Wellington & Kenepuru but…
u The barriers to accessing these from Kāpiti - cost/affordability, timing (e.g. of appointment), ease (young, old, disabled) and discomfort - impact across multiple facets of our community
u Access to Urgent Care is also constrained by cost, after-hours times and policy changes (e.g. free to Under 14’s, Community Card holders)
OPPORTUNITIES
u Improved transport options –already a trial scheme underway at Kenepuru, and an improved Kāpiti Health Shuttle under investigation
u Extend and enhance health services in Kāpiti e.g. exploit potential at the Kāpiti Health Centre
u Planning for the implementation of digital health services to be delivered in or close to home
CCDHB Public 7 November 2018 - 3 FOR DECISION
95

Priority 2 – Urgent CareISSUES
u The Ōtaki boundary is an anomaly (DHB, PHO, Ambulance etc), compounded by inconsistencies in practice and lack of transparency for patients
u Reducing ‘unnecessary’ visits to A&E and A&M
u Availability of and demand on ‘after-hours’ services
u Planning for urgent care provision in a major civil defence emergency in Kāpiti/Ōtaki – the community/KHAG does not feel fully engaged
OPPORTUNITIES
u Initially providers need to provide clarity and transparency for their patients. The Ōtaki community should be included in any future consultation on reconfiguration
u Capitalise on proven positive impacts of Health Care Home & ambulance/PHO initiatives
u No current or short-term or opportunities are apparent
u Some planning is taking place – involve KHAG/the community as a stakeholder in that process
CCDHB Public 7 November 2018 - 3 FOR DECISION
96

Priority 3 – Mental HealthISSUES
u Unsurprisingly a major area of need -services across the spectrum appear to be under- resourced with inadequate provision for patients
u A Kāpiti-based crisis service is needed
u Clinical pathways for mild to moderate presenting need to be developed and resourced in GP practices
u Additional resources and an integrated approach is needed for mental health provision for young people, including those at risk of suicide
u Planning needed to meet the needs of older people with depression, anxiety, dementia and abuse
u Specialist support services needed for perinatal mental health as Kāpiti’s population grows
OPPORTUNITIES
u There are a considerable number of local organisations actively engaging with mental health issues across our community. There seems to be overlap/duplication but the international evidence suggests that there could be significant gains by integrating these local services with DHB/PHO funded services
u While a national review of mental health services is underway, which may well introduce some systemic changes, the review is unlikely to look in any detail at local conditions such as those in Kāpiti, so…
u Our recommendation is that the stakeholders jointly undertake a local review of mental health services in Kāpiti/Ōtaki , with an up-front commitment to acting on its findings
CCDHB Public 7 November 2018 - 3 FOR DECISION
97

Priority 4 – Older PeopleISSUES
u 28.6% of Kāpiti’s population – 15,089
u Their priorities include: access to services, transport, care co-ordination, restorative services, home care, health literacy, mental health…
u The combination of longer life expectancy with demand for longer-term independent living has not been well recognised or responded to by providers
u Too few services are provided at or out of Kāpiti Health Centre
u Health and wellbeing services are not well integrated and don’t address the recommendations made in the Health Aging Strategy 2016 or the NZ Health Strategy
OPPORTUNITIES
u A ‘One Stop Shop’ partnering across agencies, incorporating health and wellbeing services, built on 21st century knowledge of the aging process, and a focal point for provider/workforce collaboration and development
u Advocacy, counselling and communication to empower users and their whanau
u Enhancement of preventative measures, engaging people in their own long-term health care
u Involving user service groups (Parkinson, Stroke etc) to advantage those with long-term care needs
u Focus services closer to home – enhance services at Kāpiti Health Centre and increase availability of digital health services
CCDHB Public 7 November 2018 - 3 FOR DECISION
98
Priority 5 – People with DisabilitiesISSUES
u Multiple and chronic disabilities impact negatively on employment, disease, obesity, activity, access to/affordability of medical care…
u Access to and distance from accident, medical and outpatient clinics not located in Kāpiti… including access arrangements at stations (GWRC)
u Too few clinics at Kāpiti Health Centre
u Accessibility factors not well embedded in planning etc
u Relatively weak integration of local and national agencies with local user groups to provide well-informed, user-focused services
OPPORTUNITIES
u Include disabilities in CCDHB’s up-coming Health Needs Analysis as the basis for the development of a Kāpiti disabilities health & wellbeing strategy
u Continue, and reinforce, the work already underway on disability and access-sensitive transport solutions
u Review the current service provision for disabled users in Kāpiti and enhance services at Kāpiti Health Centre
u Adopt the proposed health & wellbeing strategy as a primary template in future planning and consenting processes
u Adopt an integrated approach to disability health and wellbeing provision
CCDHB Public 7 November 2018 - 3 FOR DECISION
99
In conclusion…We propose that the Advocacy Group (from January 2019, the Kāpiti Health Advisory Group) and its stakeholders collaborate proactively on the development of a Kāpiti Health & Wellbeing Locality Plan focused on these five priority areas. And that the planning group should…
u Reflect on the implementation of the Ōtaki Health & Wellbeing Plan, and the establishment of the Ōtaki Health & Wellbeing Advisory Group
u Establish and sustain open, two-way channels of communication
u Adopt an effective community engagement and communication plan
u Maintain an evidence-based annual review of progress towards and, post-implementation, the outcomes of the Locality Plan
A graphic illustrating what this proposed approach would look like is shown on the following, final slide…
CCDHB Public 7 November 2018 - 3 FOR DECISION
100

CCDHB/MDHB(Service providers to Kāpiti)
KCDCLobbies DHBs
Advocates – uses influenceMaintains health database for the
District Monitors health outcomes and re-
assesses priorities Communicates with the public
Community Health Forum (Meets 2-3 times per annum)
Joint LocalityPlanning Team
(DHBs, KHAG & ŌHWAG)
Informs and advises
WFA MediaNGO/ Private Sector
WREMO
Community Wellbeing: proposed Health model for Kāpiti
Advisory Group (current KHAG Executive)
CCDHB Public 7 November 2018 - 3 FOR DECISION
101
Page 1 of 9
BOARD DISCUSSION
Date: 26 October 2018
Author: Leigh McLachlan, Acting Health & Safety Manager
Endorsed By: Thomas Davis, General Manager Corporate Services
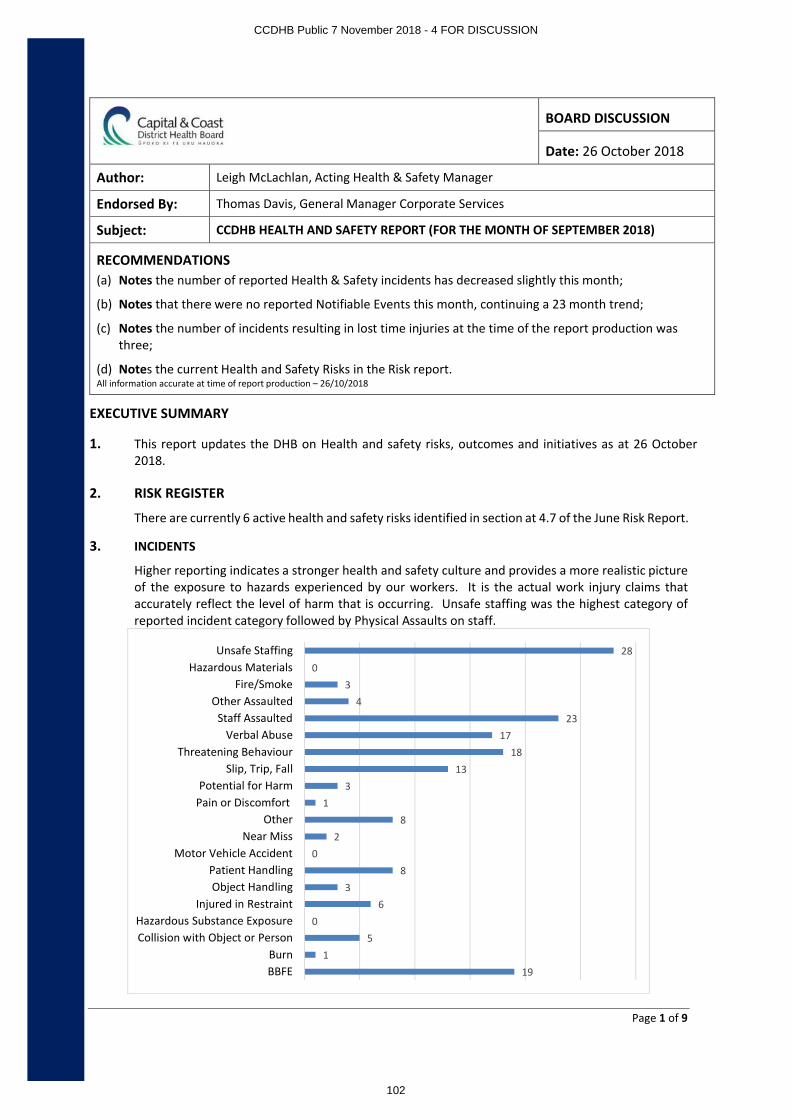
Subject: CCDHB HEALTH AND SAFETY REPORT (FOR THE MONTH OF SEPTEMBER 2018)
RECOMMENDATIONS(a) Notes the number of reported Health & Safety incidents has decreased slightly this month;
(b) Notes that there were no reported Notifiable Events this month, continuing a 23 month trend;
(c) Notes the number of incidents resulting in lost time injuries at the time of the report production was three;
(d) Notes the current Health and Safety Risks in the Risk report.All information accurate at time of report production – 26/10/2018
EXECUTIVE SUMMARY
1. This report updates the DHB on Health and safety risks, outcomes and initiatives as at 26 October2018.
2. RISK REGISTER
There are currently 6 active health and safety risks identified in section at 4.7 of the June Risk Report.
3. INCIDENTS
Higher reporting indicates a stronger health and safety culture and provides a more realistic picture of the exposure to hazards experienced by our workers. It is the actual work injury claims that accurately reflect the level of harm that is occurring. Unsafe staffing was the highest category of reported incident category followed by Physical Assaults on staff.
191
50
63
80
28
13
1318
1723
43
028
BBFEBurn
Collision with Object or PersonHazardous Substance Exposure
Injured in RestraintObject Handling
Patient HandlingMotor Vehicle Accident
Near MissOther
Pain or DiscomfortPotential for Harm
Slip, Trip, FallThreatening Behaviour
Verbal AbuseStaff Assaulted
Other AssaultedFire/Smoke
Hazardous MaterialsUnsafe Staffing
CCDHB Public 7 November 2018 - 4 FOR DISCUSSION
102

Page 2 of 9
3. Performance Summary
Definitions∑ Injury Claims - Any work related injury resulting in an ACC claim∑ MFO Claims - Medical Fee Only Claims. Any work related injury which results in an ACC claim for treatment but
with no lost time
Performance Indicator
Curr
ent
Mon
th
Prev
ious
M
onth
Stat
us Trend(Past 12 months)Increased - Decreased - No Change
H&S Incidents
∑ Total Number of Reported Incidents 162 166
- Number of Reported Incidents - Non MHAIDS 105 100
- Number of Reported Incidents - MHAIDS 57 66
∑ Number of Incidents involving visitors 0 0
∑ Number of Incidents involving contractors 0 1
∑ Number of Notifiable Events 0 0
Key Performance Indicators
Indicator(*=estimated)
Excluding MHAIDS MHAIDS
Current Month
Previous Month % Change
Target(By June
2019)
Current Month
Previous Month % Change
Target(By June
2019)
ACC Injury Claims 6 11 -45% N/A 3 6 -50% N/A
MFO Claims 4 9 -55% N/A 2 4 -50% N/A
LTIFR - 12 mth 7 8 -12% 7 13 15 -13% 12
Severity Rate - 12 mth 11 11 - 9 11 12 -8% 8
TRIFR - 12 mth 6 6 - 5 8 8 - 7TRIFR - 12 mth Including BBFE
11 11 - 9 10 10 - 8
Notifiable Events 0 0 - 0 0 0 - 0
Performance Indicator
Curr
ent
Mon
th
Prev
ious
M
onth
Targ
et
Stat
us
Trend(Past 12 months)
- Meeting Target - Below Target
∑ % of Pre-Employment Health Screening completed prior to start+ NA 88% 100%
∑ % of H&S Fundamentals Managers completed 78% 81% 90%
∑ % of Managers Injury Management completed 61% 75% 90%
∑ % of Incidents closed within 14 days (April 2018) 61% 73% 100%
∑ No. of H&S Rep vacancies 21% 16% 20% Data not available as yet
∑ No. of H&S Reps who have attended training 73% 66% 80% Data not available as yet+Submission of Pre-employment Health Declarations with less than 2 weeks start date is usual cause
CCDHB Public 7 November 2018 - 4 FOR DISCUSSION
103

Page 3 of 9
∑ LTIFR - Lost Time Injury Frequency Rate. The number of lost-time injuries (per million hours worked) within a given accounting period relative to the total number of hours worked in the same accounting period
∑ Severity Rate - The average number of lost days experienced as compared to the number of incidents experienced i.e. Number of lost days divide by the number of lost time injuries
∑ TRIFR -- Number of incidents where injuries/illness occurred requiring medical treatment by a medical professional (Number of injury claims X 200,000 / Number of hours worked)
CCDHB Public 7 November 2018 - 4 FOR DISCUSSION
104

Page 4 of 9
3.1 Lag Indicators (last 13 months)
……………………….. Trend
05
10152025
Blood or Body Fluid Exposure (BBFE)
0
5
10
15
Slip, Trip, Fall
01020304050
Physical Assaults - MHAIDS
0
10
20
30
Physical Assaults - Non MHAIDS
02468
1012
Patient Handling
02468
10
Object Handling
CCDHB Public 7 November 2018 - 4 FOR DISCUSSION
105

Page 5 of 9
3.2 Lost Time Injuries (LTI)
Current Month
Category of Incident Directorate Department Days Lostto Date
Patient Handling Medicine, Cancer & Community
Ward 6 South 7
Patient Handling Medicine, Cancer & Community
ORA Inpatients - Ward 4 4
Physical Assault MHAIDs Haumietiketike (ID Inpatient) 4
Past 13 months
September,2017
October, 2017
November,2017
December, 2017
January,2018
February, 2018
March,2018
April,2018
May,2018
June,2018
July,2018
August,2018
September,2018
General LTI's 8 5 4 6 5 2 10 4 3 3 4 2 2
Total Days Lost 70 64 24 37 36 9 78 181 10 36 47 19 11
020406080100120140160180200
0
2
4
6
8
10
12
Tota
l No.
of D
ays
Lost
No.
of L
TI's
General (Excluding MHAIDS)
September,2017
October, 2017
November,2017
December,2017
January, 2018
February,
2018
March,2018
April,2018
May,2018
June,2018
July,2018
August,2018
September,2018
MHAIDS LTI's 4 3 3 3 3 0 1 1 0 3 1 2 1
Total Days Lost 74 9 26 8 88 0 40 9 0 30 3 43 4
0102030405060708090100
0112233445
Tota
l No.
of D
ays L
ost
No.
of L
TI's
MHAIDS
CCDHB Public 7 November 2018 - 4 FOR DISCUSSION
106

Page 6 of 9
4. Workplace Injury Management 4.1 Cost – Past 13 months
4.2 Statistics 4.3 Claims by Directorate – Past 13 Months
∑ Patient and object handling injuries continue to be the most common causes for claims, accounting for 39% of all claims over the past 12 months
∑ Lumbar sprain injuries remain the most frequent type of injury reported
$0
$5,000
$10,000
$15,000
$20,000
$25,000
$30,000
$35,000
$40,000
$45,000
Sep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18ACCPP Case & Claims ManagementMedical FeesTop-up (payment employeee would have received if in work over and above base salary i.e. shift allowance)Weekly Compensation - 1st Week - Employee not in Work or not working full hoursWeekly Compensation - Employee not in Work (week 2+) or not working full hours
0
41
6
87
1
73
58
Chief Executive's Office
Clinical & Support Services
Corporate Services
Medicine, Cancer & Community
Strategy Innovation & Performance
MHAIDS
Surgery, Women and Children
CCDHB Public 7 November 2018 - 4 FOR DISCUSSION
107

Page 7 of 9
5. Workplace Violence and Aggression Statistics
6. OTHER BUSINESS
6.1 Steering Committees
∑ Health & Safety Steering Committee - This Committee meets every two months. ∑ Preventing Workplace Violence Steering Committee - This Committee is meeting on a monthly basis
and is in the process of developing a work plan.∑ Moving & Handling Steering Committee - This Committee is meeting on a monthly basis and is in the
process of developing a work plan.
0
2
4
6
8
10
12
14
16
18
Oct -16
Nov- 16
Dec- 16
Jan -17
Feb -17
Mar- 17
Apr -17
May- 17
Jun -17
Jul -17
Aug- 17
Sep -17
Oct -17
Nov- 17
Dec- 17
Jan -18
Feb -18
Mar- 18
Apr -18
May- 18
Jun -18
Jul -18
Aug- 18
Sep -18
General (Excluding MHAIDS) - Last 24 Months
0
5
10
15
20
25
30
35
40
Oct -16
Nov- 16
Dec- 16
Jan -17
Feb -17
Mar- 17
Apr -17
May- 17
Jun -17
Jul -17
Aug- 17
Sep -17
Oct -17
Nov- 17
Dec- 17
Jan -18
Feb -18
Mar- 18
Apr -18
May- 18
Jun -18
Jul -18
Aug- 18
Sep -18
MHAIDS - Last 24 Months
CCDHB Public 7 November 2018 - 4 FOR DISCUSSION
108

Page 8 of 9
7. Employee Support
7.1 EAP
Last 12 Months
0
20
40
60
80
100
120
Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18Total number of Clients: New clients: Total number of Sessions:
0
20
40
60
80
100
Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18
Work Related v Non-Work Related Referrals
Non Work Related Work Related
$0.00
$2,000.00
$4,000.00
$6,000.00
$8,000.00
$10,000.00
$12,000.00
$14,000.00
$16,000.00
$18,000.00
Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18
Monthly Cost
CCDHB Public 7 November 2018 - 4 FOR DISCUSSION
109

Page 9 of 9
7.2 Monthly Referrals to EAP: - Work related reasons for referrals (as stated by worker)
- By Directorate
5
2
9
3
1
1
0 1 2 3 4 5 6 7 8 9 10
Job Performance
Professional development
Training
Workplace change
Pressure/Stress
Relationships
Harassment
Mentoring/Supervision
Employment Conditions
Management
Drug & Alcohol
Workplace safety
Critical Incident Debriefing
0 5 10 15 20 25 30
Not stated
SIP
Executive Office
Corporate Services
Clinical and Support Services
Mental Health (MHAID)
Mental Health
Medicine, Cancer & Community
Surgery, Women's & Children's
Chief Operating Office
EAP for September
H&S
Personal
Work
CCDHB Public 7 November 2018 - 4 FOR DISCUSSION
110

PUBLIC
1
BOARD INFORMATION
Date: 18 October 2018
Authors Anne Stewart, Acting Executive Director (Operational) Quality Improvement & Patient SafetySarah Jackson, Acting Executive Director (Clinical) Quality Improvement & Patient Safety
Endorsed by Julie Patterson, Interim Chief ExecutiveJohn Tait, Chief Medical OfficerAndrea McCance, Executive Director Nursing and MidwiferyCatherine Epps, Executive Director Allied Health Technical & Scientific
Subject QUALITY AND SAFETY REPORT
RECOMMENDATIONS
It is recommended that the Board:
(a) Notes the progress with the implementation of the Clinical Governance Review;
(b) Notes the quarterly results of the National Patient Experience Survey;
(c) Notes the success of the Poster winner at the HQSC Scientific Symposium;
(d) Notes the quarterly results of the HQSC quality and safety markers;
(e) Notes the CCDHB quarterly results in the updated HQSC quality measures dashboard.
APPENDICES
1. CCDHB Quality and Safety Marker Results;2. Summary of CCDHB measures from HQSC dashboard;3. Photo of winner of HQSC Scientific Symposium poster competition.
1. INTRODUCTION
The purpose of this report is to inform the board of the quality, improvement and patient safety activity within the Capital & Coast District Health Board (CCDHB) Hospital & Health Services for the period July 2018 to September2018.
One of the core functions of CCDHB is to maintain and improve the safety and quality of our health and disability services. We focus on patient safety and patient experience as the key indicators of our progress. Growing evidence indicates that better patient experience, developing partnerships with consumers, and patient and family-centred care are linked to improved health, clinical, financial, service, and patient satisfaction outcomes.
At CCDHB, quality of care is underpinned by the “Triple Aim”, an international healthcare improvement policy (adopted in New Zealand by the Health Quality and Safety Commission) that outlines a plan for better healthcare systems. Through our clinical governance structures we are able to provide direction and leadership of priorities for quality, continuous improvement and patient safety, and influence behaviours, and system and process design to enable the DHB to achieve these priorities.
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
111

PUBLIC
2
2. CLINICAL GOVERNANCE UPDATE
Good progress is being made on implementing the recommendations from the Clinical Governance review. This includes development of a clinical governance framework and progress with the improvements to the sub-committees.
∑ A Clinical Governance Framework has been developed and is included in this agenda as a separate item. ∑ The Credentialing Committee is due to meet for the first time on 20th November with a view to undertaking
the first service credentialing in April. ∑ The Family Violence Committee has its first meeting on 29 October and the Point of Care Testing Committee
has also recently met. ∑ The Patient Quality Safety Indicators meeting has been dis-established and is re-forming as the Patient Safety
Committee. ∑ A new Chair for the Death Review Committee (to change name to Morbidity and Mortality Committee) has
been identified as the current Chair plans to retire next year. The current and proposed chair are leading discussions with the Departmental Leads for M&M about improving the processes around M&M meetings (becoming multi-disciplinary, standardised format and reporting) and it is planned to have a meeting early next year to formalise these changes.
∑ The terms of reference for the clinical governance sub-committees are being reviewed and standardised to give greater clarity and purpose to their function and responsibility.
∑ Discussions have been had with the chairs of a number of other committees and there is a plan underway to get all the chairs together in early December for a combined session about clinical governance, their roles as chairs of clinical governance committees as well as what support they need.
An area of concern is ensuring we have the appropriate resource to support these committees.
3. CONSUMER ENGAGEMENT AND PARTICIPATION
3.1 Compliments & ComplaintsThe number of complaints received remains within normal variation. The three main complaint issues relate tostandard of care, communication and administration/process.
100% of complaints received in August were first acknowledged by letter or email within the five day timeframe. 65% of our August complaints were closed within the 20 working day time frame. There are a number of factors impacting on completion timeframes with the main one being availability of clinical staff to review and respond.The timeframe does not take into account extensions that have been granted as the system calculates the number from the date the complaint is first entered.
Numbers of complaints and compliments per monthSep-17 Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18
Complaints 71 60 96 54 68 84 103 78 74 70 85 83 90Compliments 85 74 86 43 74 67 85 97 62 81 99 110 48
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
112
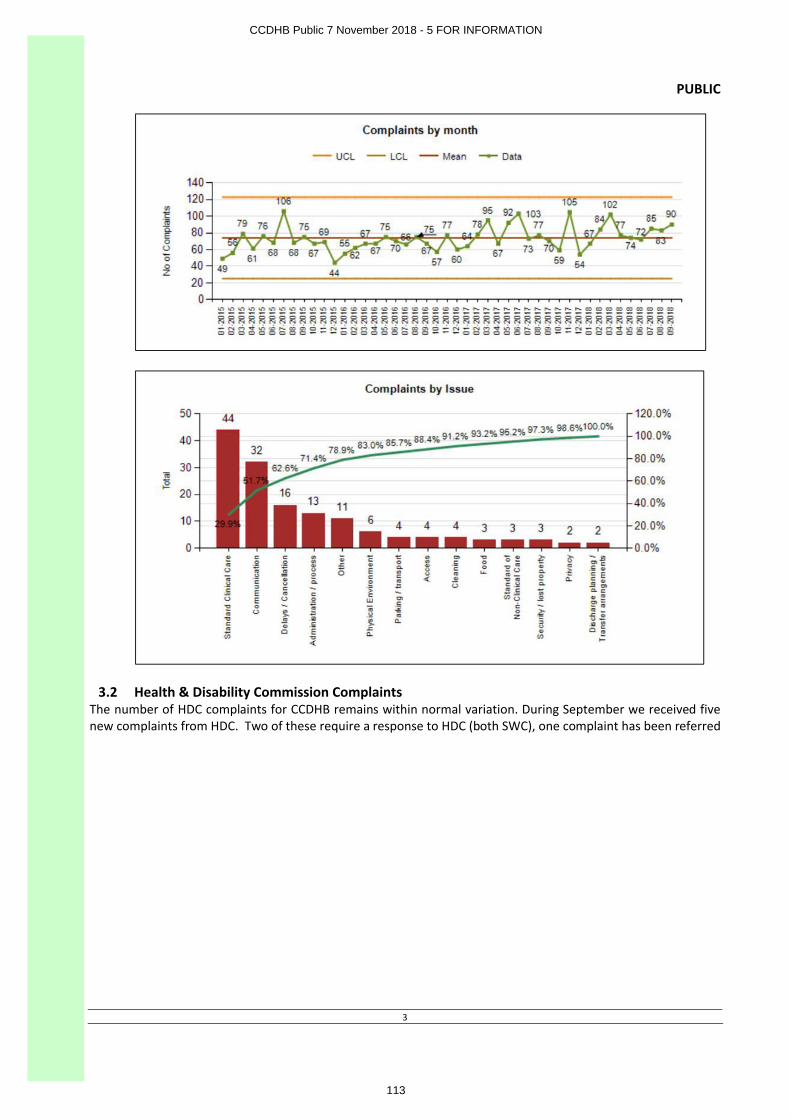
PUBLIC
3
3.2 Health & Disability Commission ComplaintsThe number of HDC complaints for CCDHB remains within normal variation. During September we received five new complaints from HDC. Two of these require a response to HDC (both SWC), one complaint has been referred
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
113

PUBLIC
4
to the advocacy service, one complaint requires a response directly to the complainant, and one is for comment only. Three complaints were closed.
3.3 CCDHB National Quarterly Patient Experience SurveyDHBs are required to participate in a national patient experience survey as part of the Health Quality and Safety Commission (HQSC) work programme. Results for quarter 4 are in the table below:
HQSC National Adult Patient Experience Survey: Q4 (Aug Results)
Quarters by HQSC 3 4 1 2 3 4 1 2 3
Quarters by MOH 1 2 3 4 1 2 3 4 1
Date Aug 2016
Nov2016
Feb 2017
May 2017
Aug 2017
Nov 2017
Feb2018
May2018
Aug2018
Communication (CCDHB AP Target 8.4)
CCDHB 8.5 8.3 8.2 8.3 8.3 8.0 8.4 8.5 8.4
NZ 8.3 8.4 8.3 8.5 8.3 8.4 8.3 8.5 8.6
Co-ordination (CCDHB AP Target 8.4)
CCDHB 8.3 8.3 8.1 8.4 8.4 7.9 8.4 8.4 8.3
NZ 8.3 8.4 8.3 8.5 8.4 8.6 8.3 8.6 8.5
Partnership (CCDHB AP Target 8.6)CCDHB 8.8 8.5 8.3 8.8 8.5 7.9 8.4 8.7 8.5
NZ 8.5 8.6 8.5 8.7 8.5 8.5 8.4 8.7 8.5
Physical and emotional needs (CCDHB AP Target 8.5)
CCDHB 8.6 8.3 8.4 8.5 8.4 8.1 8.7 8.7 8.5
NZ 8.7 8.7 8.6 8.8 8.6 8.8 8.6 8.8 8.7
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
114

PUBLIC
5
Response RateCCDHB 32% 30% 31% 34% 29% 13% 28% 29% 27%
NZ 27% 27% 28% 24% 26% 23% 28% 17% 24%
There is currently a small group from Learning & Development & QIPS looking at communication training needs at CCDHB. The first area being looked at is the Open communication training with a view to enhancing the current programme.
3.4 Co-design improvement programmeIn September the HQSC led co-design programme commenced with the first workshop. We have five project teams (consisting of up to five staff and 1-2 consumers) taking part in the programme. ∑ Kōrero Mai – patient, family and whānau escalation of a deteriorating patient∑ Patient centred scheduling (post stroke) - a project based at Kenepuru. ∑ Meeting the needs of patients, whanau and communities when they/their whanau are staying in the
Wellington Heart & Lung unit. We also want to ensure patients have the right information and support when they are discharged to reduce the likelihood of further readmissions.
∑ Facilitating a more consumer friendly pathway for Spinal (as a starting point) injury presentations to access the most appropriate treatment and service in the timeliest manner (right care, right place, right time).
∑ Review of disability alerts.
These projects will support the CCDHB Improvement Plan System level improvement measures for patient experience within HHS as well as supporting improvements in other parts of the system.
4. CLINICAL EFFECTIVENESS
4.1 Certification Surveillance Audit CCDHB inpatient services
We are making good progress on actions for the 16 corrective actions from the April Certification surveillance audit of hospital and mental health services at CCDHB. There were three moderate actions submitted during September and remaining 13 are due by 17th December.
4.2 HQSC - Quality Safety MarkersThe Health Quality & Safety Commission is driving improvement in the safety and quality of New Zealand’s health care through the national patient safety campaign Open for better care. The quality and safety markers (QSMs) help evaluate the success of the campaign nationally and determine whether the desired changes in practice and reductions in harm and cost have occurred.
There have been excellent results this quarter for Hand hygiene, Surgical Site Infection Orthopaedic and Cardiac Surgery, and Patient deterioration. Some improvement needed in the Safe Surgery checklist around engagement and in Falls assessments.
The CCDHB Quality and Safety Marker results for the period April to June 2018 are in Appendix 1.
4.3 HQSC Dashboard of health system qualityThe Health Quality Safety Commission dashboard provides a summary of a range of measures together in one place. The latest update of results for CCDHB is available in Appendix 2.
4.4 Hospital Acquired complicationsThere has been a continued focus on the hospital acquired complications as highlighted in the April 2018 the Health Roundtable (HRT) Executive Briefing. Following the analysis of post-operative sepsis further work has occurred to improve clinical documentation and coding to improve data capture. An improvement programme is underway
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
115

PUBLIC
6
focusing on reducing the rate of line associated bacteremia focusing on equipment, practice and culture and empowering patients. This links into patient safety week which is focusing on hand hygiene and empowering patients.
4.5 Clinical Ethics Advisory Group (CEAG)The CEAG has received an average of one referral per month during 2018. Themes have been: CEAG support around treatment decision making where there is lack of clarity and possible conflict of values; post-event discussion about the ethical issues of treatment already given and identification of correct follow up action; the CEAG’s views on ways in which student health practitioners work with patients; privacy issues; human rights; capacity to consent and justification and morality of forced administration of medication.
The CEAG Chair and Clinical Ethics Advisor have both pursued additional education in clinical ethics – the Chair completing a course at Harvard School of Medicine Bioethics Centre in June – and have presented at clinical ethics events. The clinician education role of the CEAG has included two Grand Rounds, an in-house study session for CEAG members, presentations at international conferences and teaching sessions with medical, nursing and midwifery staff.
5. QUALITY IMPROVEMENT & PATIENT SAFETY
5.1 Improvement Movement - Improvement TrainingThe improvement training continues with the two models of 1hr taster sessions and 12 week programmes running concurrently. The one day Frontline Leadership Programme (FLP) sessions also continue.In addition the improvement team have developed an enhancing data literacy training session to support the implementation of the data visualisation programme (Qlik).The sixth 12 week programme commenced in September with 12 participants and they will graduate in December.
2018 Improvement movement campaign details as of September:
Training Type Numbers trained to date 2018 Target % of target
Stream 1: Join the Movement! 1 hour taster sessions 143 415 34.5%
Stream 2: 12 week improvement training 24 45 53.3%Stream 3: FLP 1 day training 39 40 97.5%Stream 4: Enhancing data literacy training 12 40 30%Total number of staff trained in improvement methodology 238 500 47.6%
5.2 RMO Quality Improvement and Clinical Leadership ResidencyFollowing a successful trial of RMO improvement training in conjunction with the RDA and Synergia earlier in the year we decided to run our own in-house programme. Two RMOs per quarter will participate in the 12 week improvement training programme, complete their own project and learn about clinical leadership through the quality and patient safety lens. This revised programme began in September and further participants will be selected through an expression of interest process.
5.3 Poster winner at HQSC Scientific SymposiumThere was another success for a participant of one of our 12 week programmes. Ward 5 North’s Associate Charge Nurse Manager Connie Rodrigues and Physiotherapist Shana Hall presented a poster at the recent HQSC Quality Improvement Scientific Symposium held in Wellington. (See Appendix 3)
They were awarded the prize for best poster for their work analysing inpatient de-conditioning and enabling patients to be more active on 5 North – the acute oncology, haematology and renal ward.
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
116
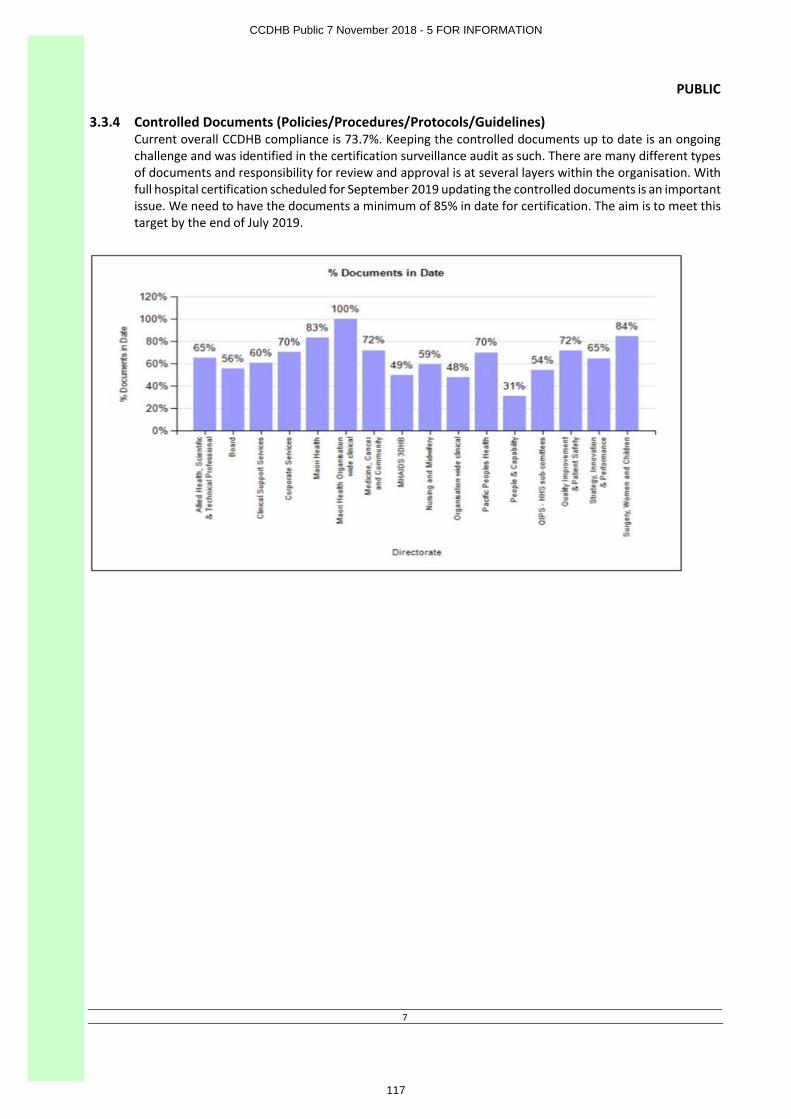
PUBLIC
7
3.3.4 Controlled Documents (Policies/Procedures/Protocols/Guidelines)Current overall CCDHB compliance is 73.7%. Keeping the controlled documents up to date is an ongoing challenge and was identified in the certification surveillance audit as such. There are many different types of documents and responsibility for review and approval is at several layers within the organisation. With full hospital certification scheduled for September 2019 updating the controlled documents is an important issue. We need to have the documents a minimum of 85% in date for certification. The aim is to meet this target by the end of July 2019.
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
117

PUBLIC
8
Appendix 1
QUALITY & SAFETY MARKERS - CCDHB results 2017/2018The Health Quality & Safety Commission is driving improvement in the safety and quality of New Zealand’s health care through its quality improvement programmes. The quality and safety markers help evaluate the success of the programmes and determine whether the desired changes in practice and reductions in harm and cost have occurred. The quality and safety markers concentrate on specific areas of harm: falls, healthcare associated infections and safe surgery. Below are our performance results as at 30 June 2018.
Marker Definition NZ GoalQ1 2017
July - SeptQ2 2017Oct - Dec
Q3 2018Jan - March
Q4 2018April - June
NZ AverageJuly – Sept 18
Falls:% if patients aged >75 (Māori and Pacific Islanders >55) that are given a falls risk assessment
90% 91% 93% 89% 85% 92%
Falls:% of patients assessed as being at risk who have an individualized care plan which addresses their falls risk
90% 92% 95% 95% 94% 95%
Falls:% of patients receiving falls risk assessment
88.8% 85.8% 91%
Safe Surgery:% of audits where all components of checklist were reviewed
Sign In
100%
100% - 98% 98%
Time Out 100% - 99% 100%
Sign Out 100% - 100% 100%
Safe Surgery:% of audits with engagement scores of 5 or higher
Sign In
95%
94% - 80% 80%
Time Out 99% - 90% 89%Sign Out 98% - 95% 88%
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
118

PUBLIC
9
Hand Hygiene:% of opportunities for hand hygiene for health professionals
80% 84% ** 82% 80% 84%
Surgical Site Infections - Dosing:% of primary procedures where antibiotics were administered in the right time
89.5% 100% 100% 98%
Surgical Site Infections - Timing:% of hip and knee arthroplasty primary procedures that were given an antibiotic at the right time
100% 100% 99% 100% 100% 98%
Surgical Site Infections - Dosing:% of hip and knee arthroplasty primary procedures that were given an antibiotic in the right dose
95% 98% 99% 99% 100% 97%
Cardiac Surgery - Timing:% of audited patients where an antibiotic is given 0-60 minutes before knife to skin
100% 100 100% + + 97%
Cardiac Surgery - Dosing:% of audited patients given correct antibiotic dose
95% 99% 100% + + 97%
Cardiac Surgery – Skin prep:100% of audited patients given appropriate skin antisepsis in surgery
100% 99% 100% + + 100%
Patient Deterioration% of audited patients that triggered an escalation of care and received the appropriate response to that escalation
* * 98% 84% 65%
Patient Deterioration * * 96% 91% 93%
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
119
PUBLIC
10
Number of patients where Early Warning Score was calculated correctly for the most recent set of vitals
Patient DeteriorationNumber of eligible wards using early warning score
* * 79% 100%
- Fewer than 50 observations* Deteriorating patients is a new safety marker which did not start until January 2018, there are currently no goals or NZ average on the HQSC site.** reported 3 times a year, therefore no data point is shown for Q4+ reported 6 months after the other QSMs
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
120

PUBLIC
11
Appendix 2 - Summary of CCDHB measures from HQSC Dashboard – updated 31 August 2018
Full interactive summary can be found at: https://public.tableau.com/profile/hqi2803#!/vizhome/Dashboard2_0Aug2018/Home
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
121

PUBLIC
12
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
122

PUBLIC
13
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
123

PUBLIC
14
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
124

PUBLIC
15
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
125

PUBLIC
16
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
126

PUBLIC
17
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
127

PUBLIC
18
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
128
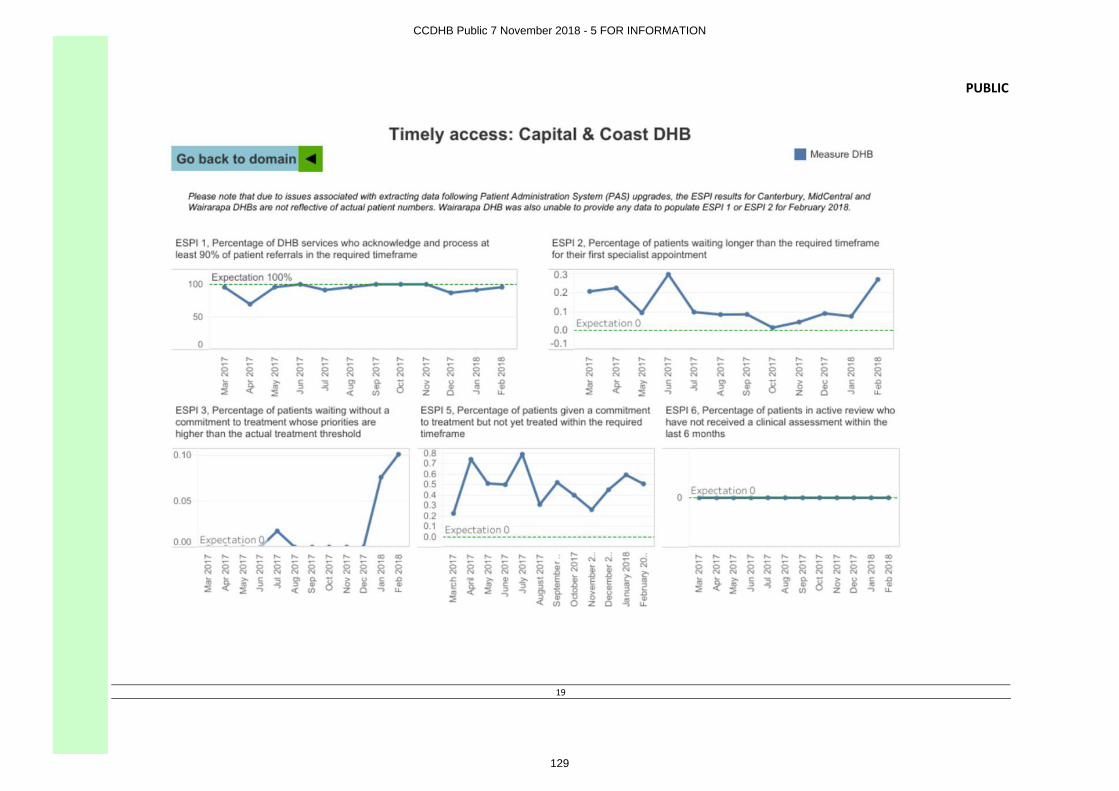
PUBLIC
19
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
129

PUBLIC
20
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
130

PUBLIC
21
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
131

PUBLIC
22
Appendix 3: Poster winner — HQSC Scientific Symposium
CCDHB Public 7 November 2018 - 5 FOR INFORMATION
132

PUBLIC
Capital & Coast District Health Board Page 1 Oct 2018
BOARD DISCUSSION
Date: 30 October 2018
Author James Crawford, Project Director
Endorsed by Thomas Davis, General Manager Corporate Services
Subject NEW CHILDREN’S HOSPITAL PROGRAMME OF WORKS STATUS REPORT
RECOMMENDATIONS
It is recommended that the Board:
Health & Safety Report
(a) Notes that there has been no incidents since the last report.
New Children’s Hospital Programme of Works
(a) Notes that Ministers of Health and Finance have approved the business case for the design and build of the new Children’s Hospital.
(b) Notes that the Concept design works for reconfiguration of the Oncology Dept is continuing whilst the Oncology Department undertake a review of the Oncology Services.
(c) Notes that the CCDHB teams completed reviews of the 50% Detailed Design documents that were issued to the CCDHB on the 17 September 2018 and discussed our comments with the architect but did not submit formal comments due to the incomplete status of the 50% design drop.
(d) Note that discussions with the Māori Partnership Board identified a location for laying of the Mauri stones, with this ceremony is expected to take place 07 November 2018.
(e) Notes an event is planned on 07 Novemeber 2018 to mark the commencement of the new Children’s Hospital works on the site, which will involve a wide range of stakeholders such as; CCDHB staff, the Crown, CCDHB Board, the Benefactor and his team, Consumer Groups, CCDHB Partnerships, and other as will be identified.
1. INTRODUCTION
1.1 Purpose
The purpose of the paper is to inform the CCDHB Board regarding progress with the new Children’s Hospital Programme of Works. The CCDHB new Children’s Hospital Programme of Works (projects) includes:
∑ New Children’s Hospital, including a new drive up drop off and pick up ramp and associated roadways
∑ Civil Diversion works∑ Demolition works∑ Car parking (temporary) works∑ New Link Bridge works∑ Internal reconfiguration works within the Regional Hospital∑ Building (Engineering) Services works∑ Landscaping (Hard & Soft) works∑ New Car parking deck works
CCDHB Public 7 November 2018 - Item 5.2 Children's Hospital Project Update
133
PUBLIC
Capital & Coast District Health Board Page 2 Oct 2018
2. UPDATE
2.1 Health & Safety
There has been no incidents in the last calendar month.
SiteSafe has been engaged to audit the new Children’s Hospital and Riddiford sites each month until each project achieves Practical Completion. SiteSafe will undertake monthly onsite audits for the active projects with the reports being provided to the Executive PCG and the Portfolio Board.
2.2 Business Case
Approval from Ministers of Health and Finance has been received for the design and build of the new Children’s Hospital. The approval is subject to a number of conditions which management will ensure are met.
2.3 Resourcing the new Children’s Hospital Programme
Currently the Programme is resourced via a combination of internal and external resources. Given the progress of the Programme to date and taking into consideration the resourcing required for the work ahead, management are considering the need for suitable resources to plan and manage the works ahead.
An FF&E manager will be recruited on a fixed term basis to manage the specification, procurement, logistics, storage, installation and commissioning of FF&E. This will include working with the Foundation to identify FF&E that can be sourced from in kind donations, supporters and existing suppliers of CCDHB.
2.4 Design
2.4.1 New Children’s Hospital project.The CCDHB teams have completed their reviews of the 50% Detailed Design.
∑ Further to that review, the Benefactors Architect will be ready with their 100% Detail Design for CCDHB review from the 9th Nov.
∑ Early indications from the Architect in regard to the CCDHB’s earlier Develop Design reviews, is that 99% of the feedback had been incorporated in the full 100% detail Design package due for release on 9th Nov.
∑ The remaining 1% was not related to clinical/Technical outcomes. The 1% is deemed as relating to items/areas that the Architect did include and changed claiming their design had improved outcomes over CCDHB suggestions.
2.4.2 Internal reconfiguration works within the Regional Hospital project.Concept design works for reconfiguration of the Oncology Dept L3 (Regional Hospital) continues with the End Users and the designers meeting to work through the design considerations.
Key Milestone dates include:Nov 2018 Identify & Approve the additional office spaceDec 2018 Concept Design completedDec 2108 Budget ApprovedFeb 2019 Develop Design interior corridor, Oncology & replacement offesMar 2019 Building Concept approvedJune 2019 Successful open tender appointedAug 2019 Phase 0 works complete (new office area, complete)Dec 2019 Phase 1 works complete (New Chair & assoc spaces)Mar 2020 Phase 2 works complete (new consult & office space)May 2020 Phase 3 works complete (corridor, records, office & services )May 2020 Phase 3b works complete (Link – corridor & ready for NCH services)
CCDHB Public 7 November 2018 - Item 5.2 Children's Hospital Project Update
134

PUBLIC
Capital & Coast District Health Board Page 3 Oct 2018
2.5 Stakeholders
Māori Partnership Board and the new Children’s Hospital project team continue to meet regularly and provide updates on progress. Recent discussions identified a location for laying of the Mauri stones, with this ceremony expected to take place 07 November 2018.
CCDHB plans to provide an update in regard to the new Children’s Hospital design process to the Consumers Group in early November.
2.6 Communication
Communication with the staff and neighbours continues and is being well received.
The CCDHB are planning an event on 07 Novemeber 2018 to mark the commencement of the new Children’s Hospital works on the site, which will involve a wide range of stakeholders such as; CCDHB staff, the Crown, CCDHB Board, the Benefactor and his team, Consumer Groups, CCDHB Partnerships, and other as will be identified.
2.7 Timeline programme
The Civil Diversion Works Project is now completed.
High level New Chlidren’s Hospoital Programme of Works timelines noted below:
TaskTarget
Completion Date
% Complete on site (as at Sept
2018)Comment
Civil Diversion Works Project
20/8/18 100% All inspections complete and expect CCC to be issued soon.
Demolition Works Project 26/04/19 65% Updated Programme identifiescompletion as late March 2019.
Internal Reconfiguration works within Regional Hospital
1/12/19 0% See milestone timesline included in report (Item 2.7.2)
Building Services Works Project (WRH)
20/5/19 0% Engineering scope of work yet to be determined in conjunction with the findings of Aurecon & WCC flood Planning
McKee Fehl Main Children’s Hospital Construction
4/12/20 0% MKF submitted detailed Construction Programme. Practical Completion -29.10.2020. Hand over -20.11.2020
New Children’s Hospital Project
Apr 2021 0% Time allocation allowance for the CCDHB to complete the final fitout / installation of FF&E
CCDHB Public 7 November 2018 - Item 5.2 Children's Hospital Project Update
135

PUBLIC
Capital & Coast District Health Board Page 4 Oct 2018
The New Children’s Hospital Project – Milestones Programme as at 12 Oct 2018 below:
CCDHB Wellington Children Hospital Project - Milestones Programme as at 12 Oct 2018
Construction & Associated Activities Start Complete Current Status
Design - Stages 25/05/2018 29/05/2019 Commenced
Approval of Budget and Development Deed Signed 20/08/2018 20/08/2018 Completed
Resource Consent 28/05/2018 25/07/2018 Completed
Building Consents (5 stages) 27/08/2018 22/05/2019 Commenced
Building Consent #1 - Foundations 3/10/2018 8/11/2018 Nearing Completion
Building Consent #2 - Superstructure (Building) 29/10/2018 7/01/2019Nearing Commencement
Building Consent #3 - Balance of works (Envelope, Services, Fitout) 7/11/2018 16/01/2019 Design Stage
Building Consent #4 - Link Structure & Associated Works 22/01/2019 23/03/2019 Design Stage
Building Consent #5 - Eastern carpark 23/01/2019 22/03/2019 Design Stage
Construction 15/10/2018 2/09/2020Nearing Commencement
Foundation 15/10/2018 26/03/2019 Commenced
Superstructure 5/03/2019 2/09/2019 Design Stage
Envelope 1/07/2019 11/11/2019 Design Stage
Roof 14/10/2019 26/11/2019 Design Stage
Main Building Services 4/07/2019 13/01/2020 Not due
Internal works & FFE 17/07/2019 2/09/2020 Design Stage
Link - Oncology to WCH 28/06/2019 10/03/2020 Design Stage
External & Associated works 29/04/2019 10/03/2020 Design Stage
Project Completion (processes) 20/08/2020 5/11/2020 Not due
CCC/CPU 22/10/2020 29/10/2020 Not due
Project Practical Completion 29/10/2020 29/10/2020 Not due
Handover 30/10/2020 5/11/2020 Not due
Client Defect notification - Architectural 6/11/2020 12/02/2021 Not due
Client Defect notification - Engineering Services 6/11/2020 5/11/2021 Not due
CCDHB Public 7 November 2018 - Item 5.2 Children's Hospital Project Update
136
PUBLIC
Capital & Coast District Health Board Page 1 November 2018
BOARD INFORMATION
Date: 29 October 2018
Author Valentino Luna Hernandez, Sustainability Manager
Endorsed by Gina Lomax Executive Director, Clinical and Support Services
Subject UPDATE ON SUSTAINABILITY ACTIVITIES AT CCDHB
RECOMMENDATION
It is recommended that the Board:
(a) Notes the results from sustainability activities and the progress with projects underway.
APPENDIX
1. Environmental Sustainability News and Articles.
1. INTRODUCTION
1.1 Purpose
This is the first quarterly report for sustainability-related activities. Reports will be produced quarterly in November, February, May and August.
1.2 Previous Board Discussions/Decisions
“Update on Sustainability Activities at CCDHB” was provided for the June 2018 Board meeting and it was requested that activity is reported quarterly.
The work in sustainability includes monthly metric/KPIs as well as qualitative (initiatives, projects, awards) elements. This update is then split into two parts, a table with metrics and a narrative update of new projects/initiatives.
2. ACTIVITY REPORT
All reporting is done following the high level targets of the Environmental Sustainability Policy:∑ Material and waste flows∑ Sustainable energy management∑ Sustainable Journeys
Apr-Jun 2018
Jul-Sep 2018
Oct-Dec 2018
Jan-Mar 2019
Apr-Jun 2019
PVC IV bags recycling actual (cumulative Kgs diverted from landfill) 3,600 4700Community sharps (actual Kgs collected) 1987 1938Furniture recycling (estimated $ savings) 90,000 110,000Electricity carbon emissions (CO2e)(tonnes) 865 971Gas carbon emissions (CO2e)(tonnes) 1,249 2,134Fleet carbon emissions (CO2e)(tonnes) 150 153
CCDHB Public 7 November 2018 - Item 5.3 Sustainability Update Report
137

PUBLIC
Capital & Coast District Health Board Page 2 November 2018
∑ Design for sustainability∑ Sustainable water management∑ Carbon management and reduction
Impact area Project description Outcomes (Environment, Budget, Risks)
Material and waste flows
Food waste diversion – Trial of ORCA food waste digester in Wellington Hospital main kitchen. Microorganisms process for waste to liquid form which goes through trade waste
7,000 KG of food waste diverted from landfill in the first 6 weeks of operation.First of its kind in Wellington region. Visited by regional trade waste officers.
Material and waste flows
Pallet waste is a problem waste due to the size and difficult manoeuvrability. CCDHB works with charities, Marae and NGOs to reuse and recycle 90% of the pallet waste
About 120 pallets/week are diverted from landfillThe saving is skip bin hire is over $1,000/week
Material and waste flows
Kenepuru A&E and Wellington ED departments arerecycling single use stainless steel instruments. If the trials are successful they will be replicated in other clinical areas.
30 kg of steel has been diverted from landfill, sterilised and put back into products
Material and waste flows
A second container load of (electricity powered) beds was donated through the ‘Take my Hands’ charity.Volunteers from CCDHB helped load the beds into containers.
This work prevented disposal of equipment that is still usableThe receiving organisations have access to equipment that otherwise they would not be able to affordThe Charity that CCDHB is working with has been nominated for a Sustainable Business Network award for their work with CCDHB
Sustainable Journeys Bike parking facilities were installed at the front of the Wellington Regional Hospital. The 12-rack-rainbow-coloured facility is used by staff, patients and visitors
Incentive for staff to bike to workPositive feedback from stakeholders
Sustainable Journeys Supporting cycling awareness by offering ‘have a go’ trials of electric bikes to staff during SUFS and Wellness Week
Tens of staff tried electric bikes for the first time A small increase in usage of the fleet electric bike after trials
Sustainable Journeys Advocacy to extend #18E route to cater for staff working shifts. The region-wide issues with the new bus network can be a deterrent to staff and patients adopting public transport as their mode to access to CCDHB hospitals
Awaiting reply from Chief Executive GWRC.
Sustainable Energy Management
Theatre LED lighting project finished. This project saw the installation of LED lights and specialist (cyanosis) LED tubes in all theatres in the Wellington Regional Hospital. The new lights are more energy efficient.
Estimated $2,000 savings year to date (from 1 July)Positive coverage in the NZ Herald and Stuff WebsiteReported in Health Matters
CCDHB Public 7 November 2018 - Item 5.3 Sustainability Update Report
138

PUBLIC
Capital & Coast District Health Board Page 3 November 2018
3. THEMES FOR THE NEXT QUARTER
3.1 Sustainability in tenders for café outlets and general services
In order to achieve greater environmental outcomes, it has been agreed to have more explicit sustainability requirements in the recent Request for Tenders for coffee outlets and the large General Services contract.The sustainability-related information received will inform scoring. Examples include: - Reduction in plastic food containers and cutlery- Increase in recycling infrastructure- Information about the source of goods brought into patient meals
3.2 Energy planning
As outlined in last month’s update regarding electric vehicles, a group of functional managers including Sustainability and Facilities Management will start to develop the framework for the future of energy consumption within CCDHB.
This plan must support future service and campus development as well as the site master planning process.
3.3 Reporting to Ministry of Health
Another stocktake of sustainability initiatives will be reported to the Ministry of Health in January 2019. This is a requirement from the Ministry and will be completed in conjunction with Strategy Innovation and Performance. A copy of the report will be provided in the February update.
CCDHB Public 7 November 2018 - Item 5.3 Sustainability Update Report
139
PUBLIC
Capital & Coast District Health Board Page 4 November 2018
APPENDIX 1 – Environmental Sustainability news and articles
Energy efficient lighting offers more than just a reduced power bill. New Zealand companies that have made the switch from traditional fluorescent and HID lighting technology to LEDs are reaping the benefits in improved working conditions, health and safety and, in some circumstances, saving lives.
An LED lighting conversion had never been done at a New Zealand port before and the project faced a harsh salt, wind and corrosion environment, huge safety requirements and the challenges of generating working light at ground level from lights on poles 30m high.
Ports of Auckland accessed Energy Efficiency and Conservation Authority Technology Demonstration Funding to switch floodlights on their city-side wharves to energy efficient LEDs.
Matt Ball, head of communications for the port, says port engineers had been studying alternatives for a few years, so jumped at the chance to work with EECA to test new technology on one half of the wharves.
"EECA funding support gave us the opportunity to report, measure and monitor for other ports around the country," says Ball. "It was really helpful to have support for a more rigorous approach to monitoring, to prove LEDs' effectiveness. We've measured a 50 per cent drop in lighting costs, the equivalent of 147 households' use."
The Ports of Auckland conversion aimed to demonstrate that LEDs are now a viable alternative in many HID lighting applications. The port changed floodlights on 46 light towers to a new type of LED, Philips Clear Flood. Twenty percent fewer light fittings were required, the challenges of the maritime environment were all met and the port plans to roll out the technology to a further 23 towers.
EECA Technology and Innovation Manager, Dinesh Chand, says "The funding contributes to the cost of demonstrating proven technology or an innovative process improvement opportunity that has yet to be widely adopted in New Zealand. It could apply to almost anything that would see new-to-New Zealand technology saving energy and/or reducing carbon emissions in business."
For New Zealand's district health boards, money saved on energy is money that can be spent on patient health. When Capital & Coast District Health Board (CCDHB) started their energy management journey in 2013, they understood that energy savings of potentially up to 10 per cent each year were possible.
CCDHB Public 7 November 2018 - Item 5.3 Sustainability Update Report
140

PUBLIC
Capital & Coast District Health Board Page 5 November 2018
LOUISE GOOSENS
New NATA certified cyanosis LED tubes have been installed in 15 operating theatres in Wellington Hospital
thanks in part to EECA’s Technology Demonstration Funding,
As part of CCDHB's efforts to reduce energy, some of the identified changes were surprisingly simple such as installing LED lighting, saving approximately $37,000 per year. Since work began on upgrading heating, ventilation and air conditioning as well as lighting, CCDHB has reduced its carbon footprint by over 980 tonnes per year.
Their most recent energy efficiency project involves the installation of new NATA certified cyanosis LED tubes in 15 operating theatres in Wellington Hospital. For this they were able to access EECA's Technology Demonstration Funding, as the lights had not been put to work in New Zealand before.
Cyanosis refers to a medical condition whereby skin can turn a bluish colour, indicating that the tissue is low on oxygen and therefore potentially a result of cardiac or respiratory problems. It is a symptom that medical professionals are trained to look for and that is easier to spot under special lighting.
Valentino Luna Hernandez, Sustainability Manager for CCDHB, says "Wellington Hospital is expected to save 40,000 kilowatt hours each year across all theatres, with additional cost savings on maintenance as the lights are longer lasting than the old fluorescent tubes – which also means reduced disruption to life-saving theatres to replace bulbs."
One of the requirements of EECA's Technology Demonstration Funding is replicability. The CCDHB theatre lighting project easily met this ask, as there are an estimated 150 operating theatres across other New Zealand DHBs, as well as in private hospitals.
For public sector organisation, Crown Loans are another funding stream that can help with efficient lighting and other projects that will save money for public funded organisation and reduce their energy use or emissions.
Shelley Park School in Auckland contracted Direct Energy Solutions to convert all their exterior and interior lightsto modern LEDs through EECA's Crown Loan funding. Crown Loans are a low cost, interest free way to fund energy efficiency and renewable energy projects for publicly funded organisations such as schools, local councils, universities and polytechnics, government departments and hospitals.
CCDHB Public 7 November 2018 - Item 5.3 Sustainability Update Report
141

PUBLIC
Capital & Coast District Health Board Page 6 November 2018
EECA PORTS OF AUCKLAND
Ports of Auckland save 66 per cent on annual lighting costs by switching to LED floodlights
The monthly energy savings from reduced power bills at Shelley Park go towards paying back the loan and, as the savings continue, the money can be invested in education facilities at the school. In the meantime, teachers and students are benefiting from an improved quality of light in classrooms.
"I strongly recommend other schools participate and take up this [Crown Loan] offer," says Brian Rolfe, Principal of Shelley Park School. "It is absolutely worthwhile to take the opportunity to save money for the school – I don't imagine there are too many schools who are happy to pay more than they have to for electricity," he said.
For more information about EECA funding, visit EECABusiness.govt.nz
CCDHB Public 7 November 2018 - Item 5.3 Sustainability Update Report
142

PUBLIC
Capital & Coast District Health Board Page 7 November 2018
CCDHB Public 7 November 2018 - Item 5.3 Sustainability Update Report
143

PUBLIC
Capital & Coast District Health Board Page 1 November 2018
BOARD INFORMATION
Date: 31 October 2018
Author Roger Palairet, Chief Legal Counsel
Endorsed by Julie Patterson, Interim Chief Executive
Subject BOARD GOVERNANCE MANUAL - REVIEW
RECOMMENDATIONS
It is recommended that the Board:
(a) Notes that the 2017 version of the Board Governance Manual is largely up to date;
(b) Notes that the references to the previous Hospital Advisory Committee (HAC) and Community and Public Health Advisory Committee (CPHAC) and the Terms of Reference of those committees are out of date given the establishment of the Health System Committee;
(c) Notes that the Terms of Reference of the Finance Audit and Risk Committee (FRAC) and the Memorandum of Understanding with the Maori Partnership Board are being reviewed and may change;
(d) Agrees that the Board Governance Manual should be amended (and resubmitted to the Board for approval) to take into account the Health System Committee arrangements.
1. PURPOSE
This report comments on the status of the Board Governance Manual and identifies areas that should be updated.
2. BOARD GOVERNANCE MANUAL
The Board considered the current version of the Board Governance Manual in September 2017, and it was finalised in October 2017. This version largely remains up to date. There have been no law changes since 2017 that require the manual to be updated.
2.1 Statutory Committees
There is a mismatch between what the Board Governance Manual says about the Board statutory committees and the current practice of CCDHB. The Health System Committee (HSC) has been formed as a combination of the previous Hospital Advisory Committee (HAC) and Community and Public Health Advisory Committee (CPHAC). This Board Governance Manual does not reflect this change because the manual still refers to HAC and CPHAC and includes their Terms of Reference in the schedules.
HSC has its own Terms of Reference, which are based on the Terms of Reference of HAC and CPHAC. The Board Governance Manual should be amended to replace the Terms of Reference in the schedules. The new Terms of Reference are careful to say HSC comprises HAC and CPHAC, and it is important that the manual also makes this distinction because HAC and CPHAC are statutory committees of the Board, that are required to be established under sections 34 and 26 of the New Zealand Public Health and Disability Act 2000 (NZPHDA).
The Disability Support Advisory Committee (DSAC) is the third statutory committee that is required to be established under section 35 of the NZPHDA, and there has been no change in its status as a joint CCDHB and HVDHB committee.
Finance Risk and Audit Committee
CCDHB Public 7 November 2018 - Item 5.4 Board Governance Manual - Review
144

PUBLIC
Capital & Coast District Health Board Page 2 November 2018
The Finance Risk and Audit Committee (FRAC) is an important Board subcommittee, but it is a committee established under Schedule 3 of the NZPHDA rather than being a named statutory committee like HAC, CPHAC and DSAC. The Board Governance Manual includes the Terms of Reference of FRAC, but FRAC has resolved to review these Terms of Reference.
If the FRAC Terms of Reference are amended, the revised version will need to be added to the Board Governance Manual.
2.2 Maori Partnership Board
The Board Governance Manual includes a copy of the Memorandum of Understanding with the Maori Partnership Board. I am aware that the Maori Partnership Board has proposed a new MOU, but the issues that arose have not been resolved. When a new MOU is agreed, it will need to be incorporated in the Board Governance Manual to ensure it remains up to date.
CCDHB Public 7 November 2018 - Item 5.4 Board Governance Manual - Review
145
PUBLIC
Capital & Coast District Health Board Page 1 October 2018
BOARD INFORMATION
Date: 30 October 2018
Authors Anne Stewart, Acting Executive Director Operations, Quality Improvement & Patient Safety
Sarah Jackson, Acting Executive Director Clinical, Quality Improvement & Patient Safety
Endorsed by Julie Patterson, Interim Chief Executive
Subject CLINICAL GOVERNANCE REVIEW UPDATE
RECOMMENDATIONS
It is recommended that the Board:
(a) Notes the progress on the implementation of the Clinical Governance recommendations;
(b) Notes the development of a Clinical Governance Framework for the CCDHB Provider Directorates.
APPENDIX
1. Clinical governance framework.
1. INTRODUCTION
The purpose of this paper is to update the Board on the progress of implementing the recommendations from the Clinical Governance review. The paper follows up on an earlier paper at the Board meeting on 12 September which outlined our response to the Clinical Governance Review undertaken by Dr Mary Seddon in April 2018 and a proposal for implementation of the recommendations.
Good progress is being made on implementing the recommendations. This includes development of a clinical governance framework and progress with the improvements to the sub-committees.
2. UPDATE
2.1 Clinical Governance Sub-Committees
∑ The Credentialing Committee is due to meet for the first time on 20th November with a view to undertaking the first service credentialing in April.
∑ The Family Violence Committee has its first meeting on 29 October and the Point of Care Testing Committee has also recently met.
∑ The Patient Quality Safety Indicators meeting has been dis-established and is re-forming as the Patient Safety Committee.
∑ A new Chair for the Death Review Committee (to change name to Morbidity and Mortality Committee) has been identified as the current Chair plans to retire next year. The current and proposed chair are leading discussions with the Departmental Leads for M&M about improving the processes around M&M meetings (becoming multi-disciplinary, standardised format and reporting) and it is planned to have a meeting early next year to formalise these changes.
CCDHB Public 7 November 2018 - Item 5.5 Clinical Governance Review Update
146

PUBLIC
Capital & Coast District Health Board Page 2 October 2018
∑ The terms of reference for the clinical governance sub-committees are being reviewed and standardised to give greater clarity and purpose to their function and responsibility.
∑ Discussions have been had with the chairs of a number of other committees and there is a plan underway to get all the chairs together in early December for a combined session about clinical governance, their roles as chairs of clinical governance committees as well as what support they need.
An area of concern is ensuring we have the appropriate resource to support these committees.
2.2 Clinical Governance Framework
A Clinical Governance Framework has been developed in consultation with the Professional Leads and, Clinical Executive Directors and chairs of the existing clinical governance sub-committees. It describes the systems, responsibilities and accountabilities for Clinical Governance for CCDHB Provider Directorates.
The attached Clinical Governance Framework Document includes the Overall framework description, Committee structure, Terms of Reference for the Clinical Governance Board, Clinical Governance systems, processes and committees.
CCDHB Public 7 November 2018 - Item 5.5 Clinical Governance Review Update
147

CCDHB Clinical Governance Framework Introduction
Clinical governance is the system by which the governing body, managers, clinicians and staff share responsibility and accountability for the quality of care, continuously improving, minimising risks, and fostering an environment of excellence in care for consumers/patients/residents.1 It requires a shared commitment from all clinical and non‐clinical staff to provide high quality and safe care, and organisational support from board to the ward. It is more than a structure, although this is required to support clinical governance (and should be reviewed every three years). It should permeate every aspect of care in a DHB and all staff (clinical and non‐clinical) should feel able to contribute to patient safety and quality improvement. This document provides a framework of how clinical governance is organised at CCDHB.
Vision
CCDHB strives to provide a culture of patient safety with quality, patient centred care by making patient safety and quality improvement of patient care everybody’s business. This is achieved by having all staff (clinical and non‐clinical) working together, putting patient/whānau at the centre of our focus and always striving to improve the quality of care provided. CCDHB also strives to provide a just, restorative environment for staff to work in.
Approach
An effective clinical governance framework has four components2. These are:
consumer engagement and participation
clinical effectiveness
quality improvement and patient safety
engaged effective workforce
They provide a structure to implement strategies to improve and enhance the quality of care. The clinical governance framework for CCDHB is attached in Appendix 1 and is divided into these four domains. This structure aims to bring individual elements together to strengthen and sustain ongoing improvement around the six dimensions of quality; safe, timely, equitable, effective, efficient and people centred (STEEEP).
Structure
CCDHB considers that everyone involved with the organisation, whether it is as board member, manager, clinician or support staff, has a responsibility to positively contribute to clinical governance. Below are the key structural components with their responsibilities and accountabilities.
CCDHB Public 7 November 2018 - Item 5.5 Clinical Governance Review Update
148

Board of governors
The board of governors has responsibility for creating the expectation of safe and quality patient services and has responsibility for holding the chief executive accountable for meeting this expectation.
Chief executive, executive management team and other management staff
The chief executive, executive management team (ELT) and other managers are accountable for ensuring that a culture of patient safety permeates the organisation and that, within their respective divisions or areas of responsibility, there are appropriate standards in place and resources available to enable staff to deliver to the expected standard, and that systems are in place and operational to ensure monitoring, measurement and risk management.
Provider Directorate Clinical Governance Board
Overseeing clinical governance is the Provider Directorate Clinical Governance Board (CGB) which reports to the chief executive. It has authority and influence on all matters related to patient safety and quality of care. Its key responsibility is to maintain standards, lead improvements in patient care and promote a culture of safety, quality and accountability. The terms of reference are attached in appendix two.
Committees and professional reference groups
All committees of the clinical board and directorate clinical governance groups report to the CGB. This structure enables all staff to raise concerns and make suggestions for improving safety and quality, clinical governance being everybody’s business. Clinical committees have a clinical chair and report to the CGB using a standardised format. The terms of reference for the subcommittees include a set of responsibilities, accountabilities and key performance indicators and are signed by the chair of the CGB. With the support of the clinical governance board and defined terms of reference, the committees have the authority to establish working groups with a direct reporting line to that committee or professional or service group. Other service/directorate committees (clinical or non‐clinical) can raise identified clinical risks for patients, staff and organisation to the CGB and will have the opportunity to address the board in the reporting plan.
Quality improvement and patient safety
The Quality Improvement and Patient Safety Directorate (QIPS) acts as the operational arm of the clinical governance board. It has responsibility for coordinating quality and risk activities and providing the CGB, clinical leaders and management with the formal linkages required to ensure the organisation takes a coordinated approach to quality improvement and patient safety.
Policies, procedures and guidelines
The clinical governance board ensures there are clinical processes in place and that policies and procedures are current and evidence‐based. Policies arising from the committees are signed off by the CGB chair.
CCDHB Public 7 November 2018 - Item 5.5 Clinical Governance Review Update
149

Commitment
The chief executive and professional heads support the vision and aims outlined in this document. However, the vision and aims can only become a reality if every member of staff makes patient safety and quality of care improvement their business. References
1. National Model Clinical Governance Framework. Australian Commission on Safety and Quality in
Healthcare. Nov 2017 2. Clinical Governance Guidance for Health and Disability Providers. Health Quality and Safety
Commission. Feb 2017
Appendices
1. Clinical board structure 2. Terms of reference
CCDHB Public 7 November 2018 - Item 5.5 Clinical Governance Review Update
150

CCDHB Board
CEO
Provider Directorates Clinical Governance Board
Clinical Council
Integrated Care Collaborative
Surgery Women’s & Children’s and Medicine Cancer & Community Directorate Clinical Governance
Committees
Surgery Women’s & Children’s and Medicine Cancer & Community
Directorate Service Improvement Group meetings
MHAIDS Quality Patient Safety Group
Primary & Secondary Clinical Governance
Clinical Ethics Advisory Group
Research & Audit Committee*
Credentialing Committee*
Morbidity & Mortality Committee *
The Voice Consumer Group
Infection Prevention & Control Committee*
Medicines Review Committee*
Point of Care Testing Committee*
Vascular Access & Treatment Committee
Restraint Advisory Group*
Transfusion Committee
Clinical Recognition & Response Committee
Quality Improvement Committee
Adverse Event Committee*
Family Violence Committee*
Patient Safety Committee*
Clinical Practice Committee
Proposed
Key
Exisiting
Change in function
Clinical Governance Committees are supported by Quality Improvement & Patient Safety, Information Communication & Technology, Strategy Innovation & Performance, Communications, People & Capability and Executive Leadership Team.
3DHB Clinical Governance Board
Capital & Coast District Health Board Clinical Governance Structure
Serious Event Review Committee*
Policy & Procedure Group
Mortality & Morbidity Committee*
Research & Audit Committee*
Medicines Advisory Group*
Primary Care Organisations Clinical
Governance Committees
Key:* Links with committee in MHAIDs
Choosing wisely
CCDHB Public 7 November 2018 - Item 5.5 Clinical Governance Review Update
151
Insert file path here Template capDocs ID 1.101816 Issued May 2017 Review May 2020
Month l Year
Purpose: The Provider Directorate Clinical Governance Board’s (CGB) key purpose and responsibility is to oversee clinical governance activities throughout the DHB. These include activities in all four domains of clinical governance; quality improvement and patient safety, consumer engagement, clinical effectiveness and engaged, effective workforce.
Objectives: The Clinical Governance Board should lead clinical governance at CCDHB by;
Promoting consumer engagement and co‐design
Prioritising quality improvement and patient safety
Measuring clinical processes and outcomes
Effectively managing clinical risks
Promoting a transparent, open learning culture
Ensuring effective multi‐disciplinary teamwork
Ensuring health services are provided in an equitable manner
The agenda will be structured to reflect these objectives
Function:
Lead the expectation to continually improve and raise the standard of patient care and patient experience
Provide clinical input and advice to support all clinical governance sub‐committees and service improvement committees
Monitor progress against HQSC quality markers and Atlas of Variation
Review external and internal reports on DHB performance
Review clinical risks and ensure these risks are minimised
Agree an annual patient safety, quality and risk programme
Agree an annual consumer engagement programme
Oversee the processes for assessing the organisation’s internal compliance, including certification and accreditation
Monitor clinical systems and standards to ensure that the care delivered is safe and evidenced‐based
Have oversight of processes of managing the recommendations from clinical incident analysis, Health and Disability Commissioner (HDC) and coronial investigations
Set the culture for clinical research, audit and innovation
Accountability:
The CGB will receive reports from all clinical governance sub‐committees and QIPS every quarter.
The CGB will receive reports from the Primary Secondary Clinical Governance and Quality Patient Safety Group every quarter
The CGB will provide verbal monthly reports and written quarterly reports to the Chief Executive
Provider Directorate Clinical Governance Board
CCDHB terms of reference
CCDHB Public 7 November 2018 - Item 5.5 Clinical Governance Review Update
152

Insert file path here Template capDocs ID 1.101816 Issued May 2017 Review May 2020
Chairperson and Membership: The chair shall be the General Manager of Clinical Governance and will be supported by the Executive Directors (Clinical and Operational) from QIPS. Standing members;
Consumers
Maori representative
Pacific representative
Executive Directors (Clinical), one representative from MCC, SWC and MHAIDs
Executive Director (operational) one representative from SWC/MCC/MHAIDs
Professional Heads (Chief Medical Officer, Director of Nursing and Midwifery and Director of Allied Health) Appointed members (term of two years, deputy to attend when member absent)
Medical representative or deputy (nominated by Medical Reference Group)
Nursing representative or deputy (nominated by DONM)
Allied Health representative or deputy (nominated by Director of Allied Health) The designated members of the committee are expected to attend all meetings. Attendance will be monitored annually.
Decision making process: A quorum shall consist of half the formal membership Decision making is by consensus, any matter not decided by this will result in the matter being decided by
the Chief Executive
Agenda: Agendas will be circulated no less than 3 working days prior to the meeting. All items will be submitted to
the Chair and no items can be submitted without their approval.
Minutes:
Minutes of meetings will be circulated no later than 10 working days after the meeting
Procedure: The CGB may call staff to report, present, explain and/or review any matter coming within the scope of their
activities and will do so with the authority of the Chief Executive
The requirements of the CGB will be conveyed to the relevant Executive Director, Director or Professional Head through its minutes in the first instance
The CGB may request that the relevant Executive Director, Director or Professional Head act directly to address issues of concern to the Clinical Governance Board, where it has been unable to bring about the attainment of basic levels of quality performance or risk mitigation
The CGB may highlight for the relevant sub‐committee any issues of significant concern which have not been addressed to its satisfaction within a timeframe commensurate with the risk involved. Any reporting of this nature will be discussed with the Chief Executive well prior to being included in any Committee agenda
The Board will review its performance against the requirements of the Terms of Reference annually
CCDHB Public 7 November 2018 - Item 5.5 Clinical Governance Review Update
153

Clinical Governance Systems, Processes and Committees
Consumer Engagement & Participation Clinical Effectiveness
Committees:
Consumer Council
The Voice
Consumer representatives on Committees
Working Groups:
Co‐design projects
Committees:
Clinical Recognition and Response Committee
Clinical Ethics Advisory Group
Point of Care Testing Committee
Morbidity and Mortality committees
Research and Audit Committees
Directorate/Service:
Service Morbidity and Mortality meetings
Service Audit groups
Service Research Groups
Service audits
Service Credentialing
Other:
Feedback/complaints processes
Patient experience surveys
Advance Care Planning
Open Communication (disclosure)
Consumer engagement policies, protocols and guidelines
Consumers employed
Other:
Health Roundtable data
Quality Safety Markers
Clinical Indicators
Maternal Quality Safety Programme
Policies, Protocols, Guidelines
Perinatal and Maternal Mortality Reviews
Child Youth Mortality Reviews
Engaged effective workforce Quality Improvement/ Patient Safety
Committees:
Credentialing committee
Directorate/Service:
Orientation
Peer review
Reflective Practice
Performance appraisal
Staff development
Sabbatical
Org wide:
Infection Prevention and Control Committee
Vascular Access and Treatment Committee
Medicines Review Committee
Quality Improvement Committee
Patient Safety Committee
Family Violence Steering Group
Adverse Event Review Committee
Transfusion
Restraint Advisory Group
Directorate/Service:
Service Improvement Groups
MHAID Quality Patient Safety Group
Primary Secondary Clinical Governance
SWC Governance Meeting
MCC Governance Meeting
Other:
Training and professional development
Speaking up for safety programme
Restorative Practice
Improvement Movement Training
RMO Improvement Residency
Other:
Certification
Learning from Excellence
HQSC Patient Safety Programmes
Risk Management Processes
SQUARE – adverse event reporting
Serious event review processes
Cold Chain monitoring
Legislative compliance
CCDHB Public 7 November 2018 - Item 5.5 Clinical Governance Review Update
154

PUBLIC
Capital & Coast District Health Board October 2018
BOARD DECISION
Date: 17 October 2018
Author Andrew Blair, Capital & Coast District Health Board Chair
Subject RESOLUTION TO EXCLUDE THE PUBLIC
RECOMMENDATION
It is recommended that the Board:
(a) Agrees that as provided by Clause 32(a), of Schedule 3 of the New Zealand Public Health and Disability Act 2000, the public are excluded from the meeting for the following reasons:
SUBJECT REASON REFERENCE
Public Excluded Minutes For the reasons set out in the respective public excluded papers.
Public Excluded Matters Arising from previous Public Excluded meeting
For the reasons set out in respective public excluded papers.
Chair’s report
CEO’s report
FRAC Recommendations
Risk Report
New Children’s Hospital Programme of Works Status Report
Allied Laundry
Workforce and Employment Relations Update
Investment Plan Update
Papers contain information and advice that is likely to prejudice or disadvantage commercial activities and/or disadvantage negotiations
9(2)(b)(i)(j)
* Official Information Act 1982.
CCDHB Public 7 November 2018 - 6 OTHER
155

Health
Keeping people safe - orderlies take charge
C a p i ta l & C o a s t D H B s ta f f n e w s
iSSUE 42 • OCTOBER 2018
MENTAL HEALTH AWARENESS WEEK
Mental wellbeing for health professionals
IMPROVEMENT MOVEMENT
Ward 5 south getting
patients up and dressed
CCDM UPDATE fOCUS
Additional nurses and
midwives to be employed
Matters
3DHB Allied Health, Scientific and Technical Award winners
CCDHB Public 7 November 2018 - APPENDIX
156

Dental – Kenepuru Community Hospital
My son had a dental operation and received general anaesthetic. I just wanted to offer a big thank you to all staff involved. The nurses, anaesthetist and dental surgeon were of professional but personable manners – it made myself and my son at ease. No judgements were given, just calm staff who guided us through the process and they made my son laugh. The anaesthetist especially had created a story of heading into space for him and he was in giggles by the time the gas mask was on. The experience made it so much better for me. Full credit to you all. You all do a wonderful job.
urology – Wellington regional Hospital
I wish to congratulate and thank all those involved in my treatment today. Helpful, clear, friendly and caring staff. The care could not have been more pleasant. I believe you strive to deliver an excellent level of service and from my perspective you achieved that fully.
Capital supportThank you for understanding our situation and directing us to the respite care programme which has been a long waiting concern to be resolved for our family. Thank you for all the information given to us and the kind support you and the capital support team offer.
KinD staff member – Wellington regional Hospital
A gentleman phoned in with the following compliment. He had an appointment at the Eye Clinic at 7.30am on Friday 28 September. When he got to the parking ticket machine his eftpos card wouldn’t work. A DHB employee noticed, and paid for the parking with his own credit card. When the gentleman asked for his name so he could repay him, he wouldn’t give it, and said make a donation to a church instead – which he has now done. Thank you whoever you are, it was very much appreciated.
Compliments
Cover photo: Chantalle Corbett, service manager, Wellington Community ORA; Catherine Epps, execetive director, allied health, scientific and technical; and Kate Marshall, team leader, Kenepuru Community ORA at the 3DHB Allied Health, Scientific and Technical Awards night earlier this month.
from the interim CE
Just wanted to say i am thoroughly impressed with the care, kindness and treatment I am receiving in your ED today. Wonderful, friendly staff and very prompt. Thank you!
The principles of restorative practices are incorporated into schools, many workplaces and community life. Nine years living and working in whanganui opened my eyes to the the benefits of such a people-focused approach.
Whanganui’s goal to become New Zealand’s first “restorative city” was built on the belief that individuals
and communities thrive in an environment of positive relationships.
While I was in Whanganui I saw firsthand that when a relationship is harmed, a restorative approach can help those involved to understand what went wrong and how to move on in a safe and respectful way. When I arrived at CCDHB, I was excited to learn that there was real interest in adopting restorative practices within our organisation.
With a goal of maintaining and improving relationships there’s a lot healthcare organisations can gain from this approach, not only in terms of workplace culture and safety but also with patients, family and whānau. I hope you’ll join Victoria University’s Professor Chris Marshall, an internationally recognised restorative practices expert, at our November 8 Grand Round (page 14) where he will share his insights and analysis.
A patient story shared with our Board recently, (page 11) powerfully illustrates the importance of thinking about the effect behaviour can have on those around us. The patient, who has a lung condition, was understandably upset because while she was grateful to have an outside view, she was disheartened to see people (including staff) smoking in a blatant breach of our policy. Please think about this and what you can do to help as we play our part in helping New Zealand become smokefree by 2025.
Walking in the shoes of others is at the heart of patient-centred care. And it’s fabulous to see more great examples in this month’s edition - from the work of the Improvement Movement (page 7) to the recipients of this month’s Allied Health Scientific and Technical awards (page 4). A hearty congratulations to all our finalists and winners – thank you for all the work you do caring for our community.
Enjoy this month's edition of Health Matters.
Ngā mihi,
Julie Patterson Interim chief executive
2 l CCDHB Health Matters October 2018
CCDHB Public 7 November 2018 - APPENDIX
157

The security orderly team have been working on a new approach to keep people safe in
our hospitals.
The security orderly team has been
working on a new approach to keep
people safe in our hospitals.Last month the team dealt with around 50 security emergencies, including assisting with aggressive patients and visitors.
“Hospitals can be stressful and frustrating places so we take an empathetic approach. Most people follow the rules when they’re here but there’s a few that don’t. Our goal is to manage that one percent better,” says orderlies service manager Karemoana Matamua.
There’s no textbook or best practice on hospital security. In the past, orderlies turned up and responded how they thought best. Responses varied depending on who turned up.
For the past two years the team has been focused on upskilling orderlies, supporting ward staff and formalising processes so responses are consistent and coordinated.
All 75 orderlies across Wellington Regional and Kenepuru Community Hospitals have completed an NZQA qualification in customer service and managing challenging incidents. Two trainer positions have been created to support orderlies and provide education to ward staff.
“When we step into a conflict situation, our presence can feel threatening. One of the first things we do now is introduce ourselves and explain why we are there. Our behaviour influences how someone responds and being respectful is one way to help de-escalate a situation,” says training assessor Dale Luke.
The team is also taking a more proactive approach when a potentially troublesome patient comes into the hospital. This could be a patient with a history of violence, situations where babies are being uplifted or a patient with threatening visitors.
“We work with the services looking after the patient and come up with a patient safety management plan. We see ourselves as part of the patient journey,” says training assessor Jason Tamaki.
This new approach has seen a drop in the number of people needing physical intervention.
“I’m really proud of the team and how much they have achieved. It’s been a massive turnaround but we want to do more,” says Karemona.
Keeping people safe
Orderly staff keeping an eye on hospital activities
Security call outS 777 Code Black security emergencies are top priority and responded to immediately.
Where orderlies are located at the time of the call will dictate how quickly they can respond – rest assured they are on their way.
A senior orderly is on duty at all times. They assess the jobs coming in and prioritise them.
If there are multiple security emergencies happening, the one of greatest risk will be first priority.
You can see the progress of your job on the Smartpage system.
The more information you provide about the security emergency, the more likely the right person and equipment will be sent.
CCDHB Health Matters October 2018 l 3
CCDHB Public 7 November 2018 - APPENDIX
158

Congratulations to all the finalists and
winners of the fourth biannual sub-regional Allied Health Scientific and
Technical Awards. Seventy five nominations were received from across the three DHBs. Around a quarter of the Allied Health Scientific and Technical staff were included in a nomination. There were eight award categories. The finalists and winners are listed below.
Allied Health Scientific and Technical covers over 40 professional groups. Staff work in the community, outpatient settings, and hospitals. They work with all ages, and across all the different areas of health and disability services.
To add to the festivities of the night, a talented crew of home grown Allied Health, Scientific and Technical musicians provided entertainment.
Thank you to all the nominees and allied health staff who came out to support the awards evening.
AWARD WINNERSChampion for Collaboration & IntegrationThis award recognises individuals, teams and services that have worked collaboratively with peers from different services, DHBs or organisations leading to tangible benefits for the patient.
Winner: 3DHB Nutrition and Dietetic Services, Wairarapa, Hutt Valley and Capital & Coast DHBs
The Nutrition and Dietetic Services work collaboratively across the three DHBs to ensure there is a consistent approach to professional development, supervision and the development of resources. This includes setting up a shared monthly dietetic education
session and developing a consistent process to follow for nutrition information sheets – of which there are over 250!
Excellence in Clinical PracticeThis award recognises an individual who has improved clinical care, patient safety, patient experience and/or health outcomes.
Winner: Liz Hunt - charge sonographer, HVDHB
Liz Hunt is the charge sonographer in the Hutt Hospital Radiology Department. She is continually improving practice, aware of recent research and challenging colleagues to ensure the best standards of care. Liz is generous with her expertise and leads teaching sessions for clinical staff. She has also been involved in the national sonographer recruitment campaign.
Delivering the DHB VisionThis award recognises individuals or teams who have “Delivered the DHB Vision” by achieving goals and/or priorities of their organisation. The recipient(s) will have achieved exactly what was needed to improve the way their organisation could deliver its services.
Winner: Chris Little - pharmacist, CCDHB
Chris has been the infectious diseases pharmacist at CCDHB since July 2016 and in that, time has worked hard to develop the role to a high standard of clinical and organisational care. He has embraced the DHB’s aims, and on a daily basis provides care that demonstrates shorter, safer patient journeys, growing our people and best value for money.
Allied Health, Scientific & Technical Awards
4 l CCDHB Health Matters October 2018
CCDHB Public 7 November 2018 - APPENDIX
159

Outstanding Contribution by a New GraduateThis award recognises an individual who is within their first two years of practice and who demonstrates exemplary contribution to patient care and/or team workings.
Winner: natasha lewthwaite - physiotherapist, CCDHB
Natasha joined the physiotherapy team at CCDHB as a rotational new graduate in 2017. During this short time, not only has she consolidated her physiotherapy skills but she has also further extended her clinical, communication and leadership skills beyond the expectations of a new graduate. She is already demonstrating strong leadership qualities.
Outstanding AssistantThis award recognises individuals who provide exceptional support and assistance for their Allied Health, Technical or Scientific colleagues in the provision of clinical care and/or support in diagnostic or technical processes.
Winner: Jane Duncan - allied health assistant, CCDHB
Jane works in the ORA Wellington Community team delivering rehabilitation in the community. She has excellent skills in working with patients to maximise their independence and works closely with occupational therapists to come up with solutions for patients. Jane also takes a lead in managing the equipment flow and a number of safety audits.
Inspirational Leadership awardThis award recognises individuals who have empowered others to fulfil their potential. They are individuals that are not exclusively titled ‘managers’, but have the dedication and charismatic inspiration to lead others and inspire others to act.
Winner: Alicia Graham - team leader, Te Haika, MHAIDS
Alicia is the Team Leader for the Te Haika telephone contact centre for MHAIDS. Her skills in helping people problem solve complex issues while under pressure over
the phone are impressive. The quality and consistency of telephone triaging for the service has greatly improved since she became the team leader and there is now a high level of confidence in the service.
Supporting the Growth of OthersThis award recognises individuals who act as preceptors, supervisors, mentors or educators to make a real difference in the growth and development of others. This will be evidenced through providing support, mentoring, coaching, training and guidance. They will motivate and foster enhanced learning in those they support.
Winner: Max Goodall - dietitian and AH health informatics lead, Wairarapa DHB
Max has been essential in supporting the wairarapa allied health team with the transition to the regional web pas referral management system. His willingness to work alongside the allied health staff and ICT has been the glue that has bought this project together. His efforts resulted in staff being aware, engaged and willing with this work.
Team of the YearThis award recognises a team who exhibits and demonstrates excellence in patient/client outcomes, inter-personal working and a high level of competency, to deliver an outstanding service.
Winner: MRI team, HVDHB
this team has pulled together when under pressure and shown resilience, patient focus and a fantastic team culture. They have proactively supported the plan to improve MRI wait times, and had excellent communication with referrers and their patients. There has been a marked improvement in service delivery and quality outcomes for patients.
CCDHB Health Matters October 2018 l 5
CCDHB Public 7 November 2018 - APPENDIX
160

CCDM upDATe
Additional nurses and midwives allocated to clinical areasMore nurses and midwives are being employed
to provide immediate relief to clinical areas with staffing pressures as part of a one-off $38 million nationwide Government package.
An extra 34 nursing and midwifery FTE will be employed, with recruitment already underway.
The Care Capacity Demand Management (CCDM) Council, which includes DHB and union representatives, analysed data from payroll, SQUARE and, where available, the DHB’s acuity tool TrendCare, to determine the areas in greatest need. They also used criteria from the Safe Staffing Healthy Workplace unit.
CCDM Council Chair and executive director of nursing and midwifery Andrea McCance says a lot of thought and work has gone into deciding where the additional staff go.
“It was a robust process done in partnership with the unions. “This allocation is the start of alleviating workload pressures experienced by our members. NZNO representatives on the CCDM council ensured the funding allocation was used in a way that best benefits nurses and midwives and to do this as soon as possible. There is more work to be done towards ensuring safe staffing and healthy workplaces is achieved at CCDHB.” says NZNO professional nursing advisor Suzanne Rolls.
“The inclusive approach has been appreciated and the additional funding for the maternity areas will be welcomed by midwives,” said MERAS co-leader (midwifery) Caroline Conroy.
“PSA appreciates the thoughtful approach the Council has taken. This makes sure workers and patients get the greatest possible benefit from this funding, including in mental health nursing and midwifery,” says PSA organiser Alex Ward.
The extra staff are part of a one-off Government package included in the 2018 DHB NZNO multi-employer collective agreement (MECA). Capital & Coast DHB’s proportion of this package was nearly $2.6 million.
The Government package also included resources to support the implementation of CCDM. The CCDM Council has agreed to use for a permanent Trendcare coordinator role across mental health (MHAIDs), and three CCDM project support coordinators for a three year period.
the CCDM programme is run partnership between the DHB and three health unions (NZNO, PSA and MERAS). Once fully operational, CCDM will help us better match the capacity to care with patient demand and workload using data from across our patient areas and wards.
Ward FTe Workforce capacityOutpatients - ophthalmology
1.2 1 additional 0.8 FTE RN 1 additional 0.4 FTE RN
Outpatients - Orthopaedics
0.8 1 additional 0.8 FTE RN
Ward 1 - Paediatrics 3.4 1 additional RN on nights 1 additional RN on PM
Ward 2 - Paediatrics 0.8 1 additional RN on AM Mon-Fri
4 north - Maternity 1.7 1 additional RM or RN on AM
Delivery suite 1.7 1 additional RM or RN on PM
niCU 0.5 1 additional RN on Sat-Sun
5 north 3.4 1 additional RN on AM 1 additional RN on night
5 south 1.7 1 additional RN on AM shifts (shared with 6 East)
6 North 1.7 1 additional RN on nights
Ward FTe Workforce capacity
6 South 2.21 additional RN on AM shifts 1 additional RN on PM shifts Thu-Fri
7 North 1.7 1 additional RN on nightsEmergency Department
1.7 1 additional RN on swing shift
MapU 1.7 1 additional RNPaediatric Diabetes 1 1 additional RN on AM Mon-FriCommunity nursing Service - Wellington
1 1 additional RN on AM Mon-Fri
Community nursing Service - Keneperu
1 1 additional RN on AM Mon-Fri
Ra Uta MHOP Psychogeriatric Inpatient Unit
3.4 1 additional RN on AM shift
Hikitea ID Youth Inpatient Unit
3.4 1 additional RN on AM shift 1 additional RN on PM shift
Additional FTE allocated through Government funding package
6 l CCDHB Health Matters October 2018
CCDHB Public 7 November 2018 - APPENDIX
161

CCDHB Health Matters October 2018 l 7
Ward 5 North are trying different
ways to get their patients up,
dressed and moving to prevent deconditioning. the ward was averaging eight referrals a month for deconditioned patients. Deconditioning is when a patient becomes weaker and their mobility or independence reduces while they are in hospital. Patients who experience deconditioning end up staying in hospital longer.
“People were playing the role of patient, just lying in bed,” says associate charge nurse manager Connie Rodrigues.
As part of the Improvement Movement, Connie and physiotherapist Shana Hall got together to look at ways to get patients active on the ward.
The first step was understanding why. They took a team approach to map out how their patients became deconditioned and what signs staff would see. This included surveying patients and staff as well as doing spot audits to see how many patients were in bed, dressed or sitting in a chair.
They decided to focus on patient and staff education
as well as making sure they had the right equipment to support people getting active. The pair have run three well attended staff education sessions and put up prompt signs including one asking patients if they have been for a walk today.
They also designed a walking map with short and long walk options after feedback from patients that the hospital corridors look the same and they get lost.
Getting active could be as simple as moving from the bed to a chair to eat a meal, but patients weren’t using the chairs because the chairs didn’t have arms.
“Patients told us they need chairs with arms so they can get in and out easier and feel more supported. We’ve got more high backed armchairs and are trialling them in one pod for the spot audit to see if it makes a difference ” says Shana.
While it’s still early days, they are already seeing positive results. Last week, only a third of patients where in a bed at midday, and last month there were only two referrals for deconditioned patients.
The ‘Active Ward’ project won them the Improvement Movement people’s choice award and a Health Quality and Safety Commission award.
Last month’s winner of the Embassy theatre tickets is – Nik Mounter, staff nurse, NICUCongratulations
Improvement Movement
Connie and Shana helping patients
get up and about on the ward
CCDHB Public 7 November 2018 - APPENDIX
162

What’s your role here?I'm a rotational physiotherapist
currently based at Wellington Regional Hospital. My role involves assessing
and rehabilitating patients after surgery or illnesses and assisting them to
reach their potential. To do this, I use techniques to help improve patients’ respiratory, neurological, and overall
function.
Who’s in your team?There are roughly 20 physiotherapists
based in the Wellington inpatient team alone, with more based at Keneperu, in
the community and in outpatients. Some are rotational staff like myself while
others are in senior or specialised roles.
What’s the best part of your job?
I love the nature of a rotational position, and moving between wards regularly.
I get to meet and work with new patients, nurses, doctors and allied health staff across the DHB, and I’m
constantly learning and expanding my knowledge base.
Tell us something most staff wouldn’t know
about youI’ve played the flute since I was 12, and
am currently in an amateur concert band. I enjoy playing as a de-stressor and
way to meet new people.
Staff Profile
Natasha Lewthwaitephysiotherapist
ThanksSpecial thanks and recognition
to the following staff
5 YearsNathan Fayen, community mental health nurseGladis Jose, registered nurseChristine Quimbo, registered nurseJacqualene McGivern, clinical nurse managerSarah Barton, oncologistShinae Bailey, hand therapistPuka Apineru, mental health support workerBelinda Christie, registered nurseHaide Hille, theatre store personMary Crewdson, registered nurse (casual)Katherine Baguley, ENT surgeon Aelred Refendor, registered nurseShini Paul, registered nurseShiny John, registered nurseNicola Walker, registered nurseRakesh Patel, pharmacy assistantKesiya Mithun Abraham, pharmacy technicianTessa Petelo, registered nurseCarol Reid, dietitian
10 YearsJacqueline Highgate, health care assistantMaree Brown, health service assistantSusan Bastion, community nurseSteven Robinson, service operations manager - Kenepuru & transportGrethel Navales, registered nurse
Walter Theurl, mental health support workerPeter Dunn, registered nurse (casual)Helen Costello, associate director of nursingMartin Adams, security orderlyHe Jiang, registered nurseHelen Harrison, associate charge nurseRobert Lenihan, 3DHB manager - infrastructure ICTLiezyl Tacderas, delivery suite assistantAkemi Teahan, registered nurse
15 YearsSohila Tayabi, registered nurseNicole Minskip, district nurseTukitama Tutaki, health care associate (casual)Susan Allan, administratorRichard Steele, respiratory physician Mary-Clare McCarthy, registered nurse (casual)
20 YearsTimothy Blackmore, infectious diseases physician
25 YearsDeborah Forsyth, specialist, anaesthesiaGraham Titchener, clinical leader
30 YearsMatelagi Mita, sterile services technicianSanh To Tri, security orderly
8 l CCDHB Health Matters October 2018
CCDHB Public 7 November 2018 - APPENDIX
163

Echocardiograms; an ultrasound that looks at the size, shape and performance of the heart, are
in hot demand, with the number of scans quadrupling in the past decade. We have a team of
seven cardiac sonographers who are the experts at doing these scans.
Cardiac sonographersAlex Sasse, cardiologist, says while doctors are trained to and can do an echo, it makes much more sense to have a specialist workforce to do them.
“They are able to do them at a much higher quality and more efficiently.”
One scan can take anywhere from 20 minutes to over an hour with around 90 images and video clips captured. Electrodes are put on a patient’s chest and an ultrasound probe is placed on different places on the chest to look at the heart. Once all the images, video clips and measurements are taken, the sonographer records their findings and writes a report. A cardiologist will then re-assess the images and write a further report.
The job is physical which can take its toll in sore muscles and aches and strains. To help with this, an average day is split into two. A morning may be spent doing a clinic load of outpatients and the afternoon doing scans on the wards or in more specialised scanning such as stress echoes, transoesophogeal echoes, or in theatre to help guide a procedure.
Catherine Googin, section head echocardiography, says the team go above and beyond to get urgent work done on time. They work to capacity and urgent short notice requests can be tricky, so a bit of extra notice for non-acute work would really help them.
“Patients are booked weeks and sometimes months in advance for surgery or other elective procedures but we often get told the patient needs an echo just before the planned procedure. We then have to do a frantic rejig to get it done. A bit more notice when possible would mean we could schedule it in.”
Some medical staff in places such as ICU, ED, NICU and anaesthetics have been trained to carry out ‘point of care ultrasounds’. This is very useful to quickly guide diagnosis and treatment, and if they require further information a formal echo is requested of the cardiology team.
Training to be an cardiac sonographer isn’t straightforward. You start off as a cardiac physiologist which in itself requires five years education and training, and then spend six months or so in a laboratory as a rookie to make sure you’re up to the task. If you are, you may enroll for training at one of two places in Australia while employed as a trainee sonographer in New Zealand for the two year post-graduate diploma.
Because there is no local training, many of the cardiac sonographers working in New Zealand are recruited internationally. Over half of the team here are from overseas.
CCDHB Health Matters October 2018 l 9
IN THE LIFEDAY
CCDHB Public 7 November 2018 - APPENDIX
164

10 l CCDHB Health Matters October 2018
we’ve marked two major milestones this month – the decision to appoint a single a chief executive
across Hutt Valley and Capital & Coast DHBs, and signing the development deed for the new Children’s Hospital.
Both of these are exciting developments which will help us better serve our communities. The decision to appoint a single chief executive was a collective one by both Boards after a thorough process which included several combined workshops.
The Boards’ view is that having a united vision and approach across the entire greater Wellington region will be essential to ensuring we are best placed to meet demand, improve the wellbeing of our communities, and to continue our strong relationship with neighbouring DHBs.
I want to thank interim CE Julie Patterson, who along with Dale Oliff at Hutt Valley DHB, is focused on preparing for the new model including strong leadership at both DHBs and collaborative processes.
We can’t put an exact timeframe on the recruitment process. The main goal is ensuring we get the right person for the job. A search and recruitment is about to get underway and I will keep you updated.
Deed paves way for Children’s Hospital construction to begin The signing of the new children’s hospital development deed with benefactor and developer Mark Dunajtschik this month was an important milestone and comes as construction gets set to begin on the site.
Mr Dunajtschik is contributing most of the cost of the building and is taking responsibility for the construction of the new building. The development deed sets out the details of how the project will proceed.
view from the board
Children’s Hospital benefactor Mark Dunajtschik (left) and Board Chair Andrew Blair (middle) sign the development deed in front of the Health Minister Hon. Dr David Clark.
childrens hospital update
Construction company McKee Fehl are now on site following the demolition of the old renal office and the sports complex, and the completion of the diversion and stormwater works.
McKee Fehl’s site offices have been set up,
and the crane has been delivered to site
and will be erected by mid-November.
A Mauri stone laying ceremony will be held on Wednesday 7 November to mark the beginning of construction work on the site.
Foundation work is expected to get
underway in late November.
The Riddiford building demolition is progressing to timeframe and external plaster removal is still being undertaken at the north end of the Riddiford Building. Demolition of the building is expected to be completed by late March 2019.
CCDHB Public 7 November 2018 - APPENDIX
165

The importance of the DHB’s non-
smoking policy has been highlighted in
a powerful story told by a patient who
witnessed staff and visitors smoking
on our premises. The Board heard last month how a patient with a lung condition, who regularly spends time in Wellington Regional Hospital, had seen people smoking on hospital grounds, including our carparks.
"On a recent stay, I had a view outside to the [area nearby the] emergency department. It is always nice to be part of the outside world, with something to look at, but I was very perturbed to see smokers outside my window.
Interim chief executive Julie Patterson says the patient is very courageous in bringing the issue to the attention of the board. She was also concerned about the challenges it raised in terms of reaching New Zealand’s goal of being smokefree by 2025.
“Many of our patients will have had similar experiences and likely find the presence of smoking
equally distressing. We all have a part to play in
helping
staff and visitors adhere to our smokefree policy, which is here to keep us all healthy and well,” Julie says.
CCDHB’s smokefree policy is focused on encouraging and providing support for patients, visitors and staff to make healthy decisions.
All staff are encouraged to constructively and politely bring the policy requirements to the attention of anyone who is smoking on our premises.
“I appreciate how difficult this is – as a health organisation let’s lead the way” Julie says.
What does CCDHB’s smokefree policy say?
� Smoking is prohibited on CCDHB premises and grounds
� Pre-employment screening of staff and assistance to quit is to be offered to those who smoke
� Expectation that staff will not smoke during work hours
� Assistance is offered to patients who normally smoke through the ABC Pathway and referrals to stop smoking services
� CCDHB provides staff training in smokefree ABC and NRT training, as well as a specific smokefree mental health and addiction services learning programme
� Associated risk to those patients who are under observation, surrounding patients, or staff that has been identified to outweigh the risk associated with smoking, the patient may be accompanied outside the hospital grounds to smoke under supervision.
Patient’s experience highlights impact of staff and visitors smoking
WANT HELP To qUIT SMokING? � ABC smoking cessation guide and
e-learning: www.smokefreenurses.org.nz/ABCQUIT+CARDS.html.
� CCDHB offers nicotine replacement therapy (NRT) training and elearning so that our health practitioners can administer NRT and offer quit support to patients.
For more information on quit cards and NRT training, contact Hori Waaka, smoking facilitator at ora Toa ([email protected]).
CCDHB Public 7 November 2018 - APPENDIX
166

Speaking up for SafeTY STarTing To effeCT Change
12 l CCDHB Health Matters October 2018
Speaking Up for Safety
it doesn’t just apply to our staffone of our staff spoke up about the behaviour of a police officer and they’ve
changed their training to avoid it happening again.
A nurse spoke up about the behaviour of a police officer following the death of a young Pacifika man in hospital. They didn’t feel the police officer's behaviour helped the family or staff deal with the trauma of the unexpected death.
The incident was formally followed up and the response from Police was positive. There was a meeting with the police officer involved to discuss the impact of his response on the family. The scenario is now part of the police values training package for all new staff.
Speaking up for Safety gave the nurse a framework to address the unprofessional behaviour with confidence and support.
one email stopped a medication errorClinical typists have spoken up about the quality of dictation and as a result of
speaking up, stopped a patient taking a double dose of their medication.
When a dictation is unclear it can be misinterpreted and end up causing harm to a patient. It can be unclear for a number of reasons including loud background noise, the speaker multi-tasking during dictation or lack of clarity for complex medical terminology.
One typist mentioned that when she had a hunch a doctor, for whom she had typed many letters over the years, had prescribed double the usual dose, she emailed him to check. Her hunch turned out to be correct; the wrong dose of medication had been prescribed, and she was profusely thanked by the doctor.
She said it felt good to avert patient harm and have enough confidence to raise a concern, even if she was wrong. She felt empowered, respected and valued by the doctor.
As a result of this situation, clinical leaders and service leaders have been asked to tell medical staff about the effect of noise during dictation. Planning is underway with capability development to incorporate this feedback into orientation of new medical staff.
CCDHB Public 7 November 2018 - APPENDIX
167

Mental Health Awareness Week
13 l CCDHB Health Matters October 2018
Last month we celebrated Mental
Health Awareness Week across the
three DHBs, in a joint approach to
raise awareness of the importance
of our mental wellbeing as health professionals.This year’s theme was ‘let nature in - Mā te taiao, kia whakapakari tōu oranga - which focused on boosting our wellbeing by inviting the elements of the outdoors into our lives.
Mental Health, Addictions and Intellectual Disability Service (MHAIDS) and the three DHBs held activities and provided tools across the week centred on the Mental Health Foundation’s ‘five ways to wellbeing’.
Activities included mindful movement sessions, staff
massage, resilience testing, TED talks, tree planting ceremonies, mindful money workshops, running and walking groups, art displays and a client concert at the Ratonga Rua o Porirua campus.
It’s an important time for us as health professionals to take stock of our own wellbeing, and take a moment for ourselves. The themes of the week highlight the importance of creating a culture of support - we want all our people to feel safe to ask for help and lead from the front.
This fits in well with the next part of our supporting safety culture programme, where we will be holding forums for Capital & Coast and MHAIDS staff to share and discuss results of the Safe and Supportive Workplace Survey.
Please keep an eye out for further information and forum dates on the intranet.
The awards ceremony is being held on Wednesday 21 November at Foxglove Bar from 5.30pm. See the intranet for
info and to buy tickets.
Celebrating our success awards
2018
CCDHB Public 7 November 2018 - APPENDIX
168

14 l CCDHB Health Matters October 2018
granD rounD
priVaCY & SeCuriTY
WHat is restorative justiCe anD HoW migHt it Help us builD a strong safety Culture?
proteCting ourselves anD our patients online
Come and find out at Grand Round, where we’ll hear form Professor Chris Marshall, the inaugural Chair
in Restorative Justice at the School of Government at Victoria University.
Chris is an international expert on restorative justice. He has a strong interest in conflict resolution and peacemaking and will talk about the need for restorative principles in healthcare.
Restorative principles are used in workplaces to underpin communication and help create a just and restorative culture. The approach can help workplaces build and maintain positive relationships among staff and transform conflict when it occurs.
New Zealand has well-established restorative justice processes in courts, particularly the Family Group Conference system. However its philosophy has also been introduced more widely with Whanganui becoming the country's first "restorative city”.
The approach is based on the concept that individuals and communities thrive in an environment of positive relationships. When a relationship is harmed, a restorative approach is used to help those involved to understand what went wrong and how to move on in a safe and respectful way.
Join us, as we explore the role of restorative practice in ‘Supporting Safety Culture at our place’.
Grand Round: How might restorative justice help us build a strong safety culture?When: 12-1pm on Thursday 8 November Where: Nordmeyer Lecture Theatre, School of Medicine and Health SciencesGrand Rounds are video linked to the Kenepuru Community Hospital education centre.
as a health care organisation we are at high risk of cyber-attacks. In fact, every day we experience
cyber-attacks on our IT systems, which could result in the release of private information or lock down of our systems.
The Cyber Smart Week campaign took place this month. This year’s theme – protecting your online self – provided a great opportunity for staff to become more aware of the simple measures they can take to protect themselves and our patients online.
“Health information is valuable to hackers. As we increasingly move towards electronic forms of communication, protecting online information becomes even more important,” says John Lambert from the 3DHB ICT team.
The DHB communicates with a range of different internal and external health providers such as GPs, rest homes, palliative care facilities, private hospitals and NGOs.
The campaign focused on the simple actions staff can take to help protect the patient information we share with other providers.
“One of the ways we can do this is using encryption. Encryption allows us to encode a message or information in such a way that only authorised parties can access it,” John says.
He says the new ‘encrypt’ button in our Outlook tools allow users to automatically encrypt emails by simply clicking on the button.
John also recommends password protecting files containing sensitive information.
for more information about encryption and password protecting documents, visit our Cyber Smart intranet page, under 'Staff Stuff'.
CCDHB Public 7 November 2018 - APPENDIX
169

CCDHB Health Matters October 2018 l 15
Health Care Home helping people across greater Wellington
CoMpaSS heaLTh wellington hospitals
New equipment for ED We’ve purchased a videolaryngoscope for Wellington Hospital’s ED. The videolaryngoscope enables practitioners to see down a patient’s throat.
“It’s a fantastic piece of equipment. Not only does it make intubation so much easier, safer and faster in emergency situations, it’s also wonderful for teaching,” says Dr Andre Cromhout, Director of Emergency Medicine.
Walk through the Heart of the City to support our Heart & Lung unit Join us on Saturday 17 november from 2pm to help raise funds to upgrade the Wellington Hospital’s Heart & Lung Unit’s patient lounge.
Participants walk from Waitangi Park to Wellington Hospital, finishing with a healthy BBQ. Tickets are $20 per person or $30 for the whole family (includes BBQ). Tickets can be purchased at the Wellington Hospital Gift Shop or from the foundation website.
Patient uses his birthday to give back! Tuhiwai has been a patient at Wellington Children’s Hospital three times in his life so far. Following his most recent stay a few weeks ago, Tuhiwai asked for donations to the hospital instead of presents for his 5th birthday. He and his mum wrote a poem and sent it to family and friends. He raised over $600.
foundation update
CCDHB Health Matters October 2018 l 15
independent research has found that people enrolled in a Health Care Home (HCH) practice are less likely to need
emergency department or hospital care.
The research – from the University of Auckland for the Productivity Commission – coincided with the release of the HCH ‘achievements & reflections’ report. The report provides a broad overview of the HCH’s second year in the Wellington region.
“HCH has represented a significant change in the delivery of primary care, and was achieved through successful collaboration between the DHB and local PHOs – Ora Toa, Cosine and Tū Ora Compass Health,” said CCDHB interim chief executive Julie Patterson.
“It puts patients and families’ needs at the heart of local healthcare delivery. It’s an investment in helping to ensure people can access services closer to home and stay well in the community.”
The research findings align with our own tracking of 42,000 patients over two years – which also found that HCH patients use technology more to manage their primary health care needs, and benefit from triage or telephone assessment and treatment.
Some practices even report that 35 percent of patients are being successfully managed over the phone, freeing up time to see people with more urgent needs.
I'm pleased that more and more practices are joining the HCH quality programme,” said Tū Ora Compass Health chief executive Martin Hefford.
“Their early achievements in providing more patient-centred care are encouraging, and we are delighted to be rolling out the model out to the Wairarapa, based on the success of our practices in CCDHB.”
Key FACTs � 42 practices across greater
wellington have adopted the HCH model.
� 240,000+ people are enrolled in a HCH practice across greater Wellington.
� 35 percent of HCH patients on average are being successfully managed by phone, avoiding the need for a face-to-face appointment.
� 4.8 percent decrease in HCH patients needing medical or surgical admissions to hospital.
� 3.4 percent decrease in HCH patients needing emergency department care.
Raumati Road Surgery team members receive Health Care Home certification
CCDHB Public 7 November 2018 - APPENDIX
170

Ministry staff structure changeDirector-General of Health, Dr Ashley Bloomfield has reviewed the way the Ministry business units are organised and, following a three week consultation period with staff, he has made some changes to the structure.
The new structure and operating model will help to ensure that the Ministry’s work programme is well led and governed.
For more information, visit the Ministry of Health website.
Pregnancy warning labels on alcoholPregnancy warning labels will now be required on alcohol, reminding people how dangerous drinking during pregnancy is.
The decision was made by the Australian and New Zealand Forum on Food Regulation. They agreed that, based on the evidence, a mandatory labelling standard for pregnancy warning labels on packaged alcoholic beverages should be developed and include a pictogram and relevant warning statement.
NeWSinBrieF
Staff christmas feast datesevery year a Christmas meal is put on for CCDHB staff at the four main campuses as a thank you for your hard work druing the year. There are five events held over two weeks in early December.
Friday 7 December: 7-8.30am (breakfast) & 12-2pm (lunch) - Wellington Regional Hospital
Monday 10 December: 12-2pm (lunch) - Ratonga Rua o Porirua
Tuesday 11 December: 12-2pm (lunch) - Kenepuru Community Hospital and 2.30-4pm (afternoon tea) - Kapiti Healh Centre.
Webinar and video conferencingStaff can now participate in webinars and video conferences hosted by external parties.
Webex, GotoMeeting and Skype Meetings are available on DHB computers with Windows 10. They don’t work in Citrix, or on kiosk or clinical terminals. Use Zoom to host your own video conference.
If you have any questions, call the 3DHB ICT Service Desk on #6146.
anaesthesia Day 2018This month we marked World Anaesthesia Day, commemorating the first successful demonstration of ether anaesthesia in October 1846.
The theme was ‘Anaesthesia isn’t sleep. It’s so much deeper’, and the anaesthesia Department had a display in Wellington Regional Hospital’s atrium. Among those to visit was CCDHB interim chief executive Julie Patterson, who took the opportunity to try her hand at intubating a patient.
allied health, scientific and technical staff videosWe recently published short videos of some of our allied health, scientific and technical staff talking about what it’s like to work at CCDHB and what they love about living here.
the videos will be used to help recruitment and will be featured on the CCDHB Facebook page over the coming weeks. You can watch them at www.ccdhb.org.nz under Careers.
16 l CCDHB Health Matters October 2018
CCDHB Public 7 November 2018 - APPENDIX
171

69 Tory Street, Wellington 6011, PO Box 23 075, Wellington 6140, New Zealand | Phone: +64 4 801 2430, Fax: +64 4 801 6230 Email: [email protected] Website: www.tas.health.nz
19 October 2018
SSHW Council c/- Andrea McCance Executive Director of Nursing Capital and Coast DHB (Sent by Email)
Dear Andrea,
APPROVAL FOR ADDITIONAL MOH FUNDING TO ADDRESS WORKFORCE CAPACITY ISSUE AND SUPPORT CCDM IMPLIMENTATON
As you are aware the Director General delegated responsibility for reviewing DHBs plans to the Safe
Staffing Healthy Workplaces (SSHW) Governance Group (Ministry of Health Guidance and information
for DHBs on the additional funding to address workforce capacity issues and support CCDM
implementation dated 29 August 2018)
On Friday 19 October the Governance group considered and approved your DHBs plans for addressing
workforce capacity issues and supporting CCDM implementation.
The Governance group has informed the Chief Nursing Officer at the Ministry of Health who will
facilitate the release of funding.
The Governance Group looks forward to maintaining an overview of your implementation progress
through your submission of two monthly reporting. Your first report is due on 31 December 2018
Yours Sincerely
Julie Robinson Hilary Graham-Smith Co-Chairs of the SSWH Governance Group
CCDHB Public 7 November 2018 - APPENDIX
172


















