Capita Selecta in Endocrinology and Metabolism-2007

of 14
-
Upload
andirio7486 -
Category
Documents
-
view
222 -
download
0
Transcript of Capita Selecta in Endocrinology and Metabolism-2007
-
8/10/2019 Capita Selecta in Endocrinology and Metabolism-2007
1/14
1BAGIAN-S MF PENYAKIT DALAM FK. UNAIR R SU D r. S OETOMO S URABAYA
Capita Selecta in Endocrinology and Metabolism - 2007
(GLOBESITY, Formula G/O : P-39.5-120, ADMA, CMR, Anakinra)
Capita Selecta in Endocrinology and Metabolism - 2007(GLOBESITY, Formula G/O : P-39.5-120, ADMA, CMR, Anakinra)
Askandar T jok roprawi ro
SUMMARY
The th eme o f the 22nd Continuing Medical Education (CME) of Internal Medicine
(PKB-22) of the Department of Internal medicine, Airlangga University School of Medicine
Dr. So etom o Tea ch ing Hos pita l Su ra ba ya is , Upd a te in Interna l Med ic ine fromBasic to Clinical Relevancies. Based on the department, targets, this CME may present
ap proximately 50% clinica l experienc es, 25% biom olec ula r as pects, an d 25% rece ntad vanc es in internal medicine.
In this plenary lecture (Capita Selecta in Endocrinology 2007), 5 selected topicswill be presented such as:
I. G LOBES ITY : Time-B omb Diseas e in the Future?
1. Sta ging of Lifestyle Re lated Disea se (Sta ge 0-4): Obesity Rela ted Disea se2. Obesity and Its Serious Cons equences
3. ADMA in Obe sity an d in Diab etes Mellitus
4. G loba l Ca rdiometabolic Risk (CMR)
II. Five S ATAN-CYCLES in Diabetic Nephropa ty
III. Dia g nos is of C la s sica l Thy roid Sto rm with FO RMULA G /O: P-39.5-120
IV. Onc e-Wee kly EXENATIDE-LAR fo r T2DM?
V. ANAKINRA: the p romising drug for T2DM
In a dd itio n, S tan da rds of Medica l C a re in Diabete s (ADA-2007) on the targe ts o fglycemic control, blood pressure, and lipid profile will be also included in one of
TAB LES o f th is p a pe r.
On the basis of clinical experiences, thyroid storm (thyroid crisis) can be categorized
into 2 classe s: C la ssica l Thyroid Storm which can b e diag no sed by a uthor with FormulaG /O: P-39.5-120, a nd Non -C la ss ic a l Thyro id S torm with Burc h-Wa rto fsky S co re.
Abbreviations: ADMA = a s ym m e tr ic d im e thy la rg in ine ; AOPP = Adva nc e d Oxida t ion P ro te in P roduc t ; CMR =ca rdiom etabolic ris k; CVD = c a rd iova s c u la r d is e a s e ; DDAH= dimethylarginine dim enthylaminohyd rolas e; ESRD = e nd -
s tage rena l diseas e ; FDA= food an d drug adm inis tra t ion; GLP-1 = glucagons - l ike peptide-1; LAR= long- ac ting re leas e ;LRD= lifes tyle re la ted diseas e ; MetS = m e t a b o lic s y n d ro m e ; NOS = n it ric o x ide s yn tha s e ; PRMTs = prote ina rgininemethyltransfe rases ; RONS = reac tive oxida tive nitrogen s pec ies ; TC= thy ro id c r is is ; TS = t hy r o id s t o rm
-
8/10/2019 Capita Selecta in Endocrinology and Metabolism-2007
2/14
2 PENDIDIKAN KEDOKTERAN BERKELANJUTAN ILMU PENYAKIT DALAM XXII-2007
Askandar Tjokroprawiro
I . Glo besity : Time-Bom b Disease in the future?
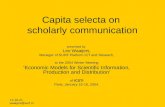
The epidemic of obesity as release by WHO in 1998 now has become pandemic,defined as an epidemic occurring over a wide geographic area and affecting anextreme high proportion of the population. Roth et al (2004) reported that it seemsnow even happen in developing countries (including Indonesia?). First noted in adults,but now it has spread to adolescents and children (FIGURE-2). Studies in the US(Mokda d e t al 1999) have further shown the rapid spread and worsening of the pandemicthat has globally or it can be termed globesity.
Hence, globesity and also diabesity (FIGURE-1) will be most likely starting nowin year 2007. If no immediate programmed intervention in obesity (esp. in Indonesia),the Time-Bomb Diseases (obesity related diseases) will be emerging in the future(2020?).
HealthcareEconomic
Burden
RespiratoryProblem
StrokeOsteo-
arthritis
LiverDi se a se
CellB l a dde rDi se a se
HeartDi se a se
P s i c o -soc i a l
CertainCa nce r
G o u t
Repro-ductionProblem
Typ e 2Diabetes
GLOBESITYGLOBESITYTime Bomb Disea se Time Bomb Dise ase
1 2
3
4
5
678
9
10
11
12
Provided: 2007Provided: 2007Related Dise as esRelated Dise as es
FIGUREFIGURE--1 GLOBESITY and Its Related Diseases1 GLOBESITY and Its Related Diseases
I .1. Staging o f l i festyle related d isease (stage-4)
Based on clinical experiences (FIGURE-2), the evolution of lifestyle relateddisease (LRD) can be staged as follows: Stage-0 (healthy lifestyle), Stage-1(unhealthy lifestyle), Stage-2 (abdominal obesity), Stage-3 (the MetS, prediabetes,adolescent obesity), and Stage-4 (ASCVD, T2DM, Stroke, Etc).
The MetS, which affects about 40% of the population over 50 in the US andnearly 30% in Europe, is a significant public health issue worldwide and one of the
-
8/10/2019 Capita Selecta in Endocrinology and Metabolism-2007
3/14
3BAGIAN-S MF PENYAKIT DALAM FK. UNAIR R SU D r. S OETOMO S URABAYA
Capita Selecta in Endocrinology and Metabolism - 2007
(GLOBESITY, Formula G/O : P-39.5-120, ADMA, CMR, Anakinra)
ma jor c a us es o f AS C VD. The prevalenc e of the MetS (ATP III criteria ) in ind ividua ls(over 40) who underwent medica l check up in Suraba ya wa s 32%, w hereas it wa s
reported 43.3% in trea ted T2DM a nd 59.0% in n a ve T2DM a s ob se rved in the private
clin ic; h ow ever, the p reva lenc e of the MetS (ATP III crite ria) in o b ese pa tien ts w ith
T 2 D M w a s 8 1 . 7 % (Tjokroprawiro 2005).
The MetS is a c ons tellation of interrela ted risk fac tors of me tab olic o rig in-meta bolic
risk factors that appear to directly promote the development of ASCVD, and
pa tients w ith the MetS a lso a re a t increase d ris k for developing T2DM.
The MetS (IDF 2005) :WC (INA) : > 90 cm () or > 80 cm ()Plus Any 2 of the Following 4 Factors
Waist Circumference = WC
> 90 cm > 80 cm
3 Blood Pressure
> 130/85 mmHg
4 Fasting Glucose
> 100 mg/dl
1 Triglyceride
> 150 mg/dl
2 HDL-Chol
< 40 mg/dl < 50 mg/dl
Healthy LifestylePreclinical Syndrome Clinical Dis eas esObesi ty
Unhealthy Lifestyle (Abdo minal Obes ity) ASCVD, T2DM, Stroke, etcPre DM, MetS,Adol. PreDM
STAGE 1 STAGE 2 STAGE 3 STAGE 4STAGE 0
Figure -2 Staging of Lifesty le Related Disease(Clinical Experiences : Tjokroprawi ro 2005-2007)
Figure -2 Staging of Lifesty le Related Disease(Clinical Experiences : Tjokroprawi ro 2005-2007)
IDF : International Diabetes Federation
WC : Waist Circumference
MetS : Metabolic SyndromeINA : Indonesia
I.2. Obesity and itS serious consequences
Obesity, a new pandemic, is a preclinical sign (Stage-2) of l i festyle related
disease and is associated with an increased cardiometabolic risk (CMR) factors dueto ab domina l obesi ty that a ppear to d irect ly (via the metab olic syndrome = the
MetS?) promote the development of cardiovascular disease (CVD).
Globally, there are more than 1 billion overweight adults, at least 300 million of
them o bes e (a B MI over 30 kg/m2; Ind one sian C riteria for ob ese is > 25 kg/m2). Such
fac ts po se a ma jor ris k for ch ron ic d isea se a s ma nifested in S ta ge -4, inc luding T2DM,CVD, hyper tens ion an d s t roke , a nd ce rta in form o f ca ncer (the Time-B omb
Disea se ). The ma in caus es o f such LRDs are increa sed c onsum ption o f energy-dens e
-
8/10/2019 Capita Selecta in Endocrinology and Metabolism-2007
4/14
-
8/10/2019 Capita Selecta in Endocrinology and Metabolism-2007
5/14
5BAGIAN- SM F PENYAKIT DALA M FK. UNAIR RSU Dr. SOETOMO SURAB AYA
Capita Selecta in Endocrinology and Metabolism - 2007
(GLOBESITY, Formula G/O : P-39.5-120, ADMA, CMR, Anakinra)
I.3. ADMA in obesity and in diabetes mellitus
Oxidative stress as occurs in severe obesi ty and uncontrol led DM (Eid et al 2004)
may increase the product ion of asymmetr ic d imethylarginine (ADMA), an endogenous
nitr ic ox ide synth ase (NO S) inhibi tor . Several l ines of eviden ce sug gest th at ADM A,be ing an endogenous NOS inh ib i to r , may not on ly be a marker o f severa l d isease
(end-stage renal disease = ESRD, liver failure, CVDs, hy pertension, diabetes, preeclamp sia)
but a lso as a n ac t ive p layer in the pro gression of atheroscleros is. ADMA is select ively
degraded by d imethy larg in ine d im enthy lam inohydro lase (DDAH) , and in hum ans there
are two major fo rms o f DDAH (DDAH-1 and DDAH-2) , w i th par t ly over lapp ing t issued i s t r i b u t i o n s i n k i d n e y , l i v e r a n d s m a l l i n t e s t i n e (Maas 2005) . Ox ida t i v e s t r es s
act ivates proteinarginine methyl transferases (PRMTs), and th is enzyme proteolyses
pro te in -1-arg in ine and leads to l ibera t ion o f ADMA. In k idney , ADMA is f i l t ra ted by
glomerul i whereas secret ion and re-uptake wi l l a lso happen in tubular cel ls .
Several studies reported that there is s trong relat ion ship foun d b etween BM I and
plasma levels o f ADMA and the Larg / A DM A rat io; th is indicates a l ink to end oth el ia l
dys func t ion in obese sub jec ts , and we ight loss may reduce c i rcu la t ing ADMA leve ls
in mor b id l y obes e women (Krzyanowska et al 2004) .
I.4. Global cardiometabo lic risk (CMR)
Car d iome tabo l i c r i s k i s bas ed on the c onc ep t o f r i s k c on t i nuum. G loba l CMR
represents the overa l l r i sk o f deve lop ing T2DM and / o r CVD ( inc lud ing myocard ia l
infarct ion an d strok e) , wh ich is due to a c luster of mo dif iable r isk factors / m arkers.
These factors / markers inc lude 9 com pon ents as seen in FIGURE-4.
1 . C lassica l r isk fac tors such as smo k ing, h igh LDL, hyper ten s ion , and e levatedb l o o d g l u c o s e
2 . E m e r g i n g r is k f a c t o rs s u c h a s ab d o m i n al o b e s i ty ( e sp . i n tr a- ab d o m i n a l
ad ipos i ty ) , insu l in res is tance, low HDL, h igh t r ig lycer ides , and in f lammatorymarkers
-
8/10/2019 Capita Selecta in Endocrinology and Metabolism-2007
6/14
6 PENDIDIKANKEDOKTERAN BERKELANJUTANILMUP ENYAKIT DALAMXXII- 2007
Askandar Tjokroprawiro
(Provided : 2007)
FIGURE-4 Global Cardiometabolic Risk (CMR)
CVDCVDType 2Type 2
DiabetesDiabetes LowLowHDLHDL--CC
IntraIntra--
abdominalabdominalAdiposityAdiposity
HighHigh
BloodBlood
PressurePressureHHighigh
LDLLDL--CC
InsulinInsulin
ResistanceResistance
ElevatedElevated
BloodBlood
GlucoseGlucose
InflammatoryInflammatory
MarkersMarkers
HighHigh TTGG
SmokingSmoking
II. Five Satan-Cycles in Diabetic Nephropaty
On slide presentation the five Satan Cycles will be much more easily understood.
On the basis of clinical experiences, 5 (five) Satan Vicious Cycles are summarized.
Thes e Vicious C yc les a re importantly well recog nized to unde rstand the p a thoge nes is,
and to perform rationa le trea tment of patients w ith diab etic neph ropa thy. Eac h S ata n
Cy cle is des c ribed b elo w. Recog nition of these S a tan Cy cles a re very importa nt tochose the appropriate drug for diabetic nephropathy.
The 1st Satan Cycle (especially in glomerular and tubular cells): from hypertension
proteinuria glomerular injury hy pertens ion). This C ycle s tarts from hypertension a nd
then be hypertension which is consecutively followed by proteinuria glomerular injury and back to hypertension again. Hence, hypertension and proteinuria are targets
of treatme nt. Ra tion ale tre a tment: AC E-1s, ARB s , Ins ulin a nd /or OAD.
The 2nd Sa tan Cy cle (from G LUT-1 a nd the n b e ba c k ag ain to G LUT-1). ThisCy cle occ urs esp ecially in the me sa ng ial c ells, a nd s tarts from G LUT-1 tha t permits
g lucose to en ter the ce l l , and subsequent ly to increase DAG produc t ion to
increa se a c t iva ted PKC increase s TG Fb tha t inh ib it s NOS , s t imula tes ECM
pro duction, a nd a lso a ctivates G LUT-1. The inc rea se d produ ction o f ECM ma y promote
-
8/10/2019 Capita Selecta in Endocrinology and Metabolism-2007
7/14
7BAGIAN- SM F PENYAKIT DALA M FK. UNAIR RSU Dr. SOETOMO SURAB AYA
Capita Selecta in Endocrinology and Metabolism - 2007
(GLOBESITY, Formula G/O : P-39.5-120, ADMA, CMR, Anakinra)
the progression of diabetic nephropathy. Rationale treatment: excellent glycemiccontrol, ACE-1s, and/or ARBs, TGFb inhibitors.
The 3rd Satan Cycle (in mesangial cells): from A-II and back to A-II. This Satan
Cycle starts from A-II (increased production is due to hyperglycemia) stimulatesTGF-formation stimulates PAI-1 and then back to stimulate A-II formation. PAI-1 also
decreases the activity of plasmin (which causes decreased matrix degradation, and
diabetic nephropathy may pursue). Rationale treatment; excellent glycemic control,
ARBs, TGF-b inhibitors, PAI-1 inhibitors.
The 4thSatan Cycle (in mesangial cells): from A-II PKC A-I and then back to
A-II. This Satan Cycle starts from A-II (due to hyperglycemia) which activates PKC
and this PKC may stimulate A-I and back to increase A-II production. Rationale
treatment: excellent glycemic control, ACE-1s, ARBs, and PKC-antagonists.The 5th Satan Cycle (from cytokines: IL-1, IL-8, TNF, PAF, VCAM-1, and MCP-1
increased ROS, and then back to these cytokines again). This Deadly Satan Cycle
most frequently occurs on hemodialyzed patients with diabetic nephropathy. The
cytokines of this Satan Cycle are generated by the 3 components (dialysate, mem-brane of the coil, and uremia or AOPP (Advanced Oxidation Protein Product) in which
all of them all present in hemodialyzed patients. These cytokines activate NADPH
oxidase, p47, p67, p21, rec stimulate ROS and RONS (reactive oxidative nitrogen
species) which then to increase the production of MMP9 (which may cause acute
thrombosis and vascular sudden death) and activated MAPK, NFkB/AP-1, and all ofthese may stimulate the production of the previous cytokines of this Cycle. Rationale
treatment: excellent glycemic control, low protein diet to suppress the increased
AOPP, or strong antioxidants, etc.
III. DIAGNOSIS OF Classical Thyroid Storm WITH Formula G/O: P-39.5-120
Based on clinical experiences and for practical point of view, thyroid storm(thyroid crisis) can be classified into 2 classes. 1. Classical Thyroid Storm and 2.
Non-Classical Thyroid Storm.
List of precipitant (TABLE-1) should be known before collecting the clinical score
of thyroid storm for diagnosis.
-
8/10/2019 Capita Selecta in Endocrinology and Metabolism-2007
8/14
8 PEN DIDIKAN KEDOKTE RAN BER KELANJUTAN ILMU PENYAKIT DAL AM XXII-2007
Askandar T j okro p ra wir o
Burch et al 1993, Tietgenset al 1995, Hall et al 1999,Turner et al 2003, Greenspan et al 2004(Summarized : Tjokroprawiro 2002 - 2007)
TABLE 1 24 Known Precipitants of Thyroid Storm
No 1No 1 -- 13 are Known Precipitants presented by Burch and Wartofsky13 are Known Precipitants presented by Burch and Wartofsky--19931993
1 Infection
2 Thyroid Surgery
3 Non-Thyroid Surgery
4 Iodinated Contrast Dyes
5
6 Radioiodine Therapy
7 Diabetic Ketoacidosis
8
9
10 Pulmonary Embolism
11 Cerebral Vascular Accident
12 Trauma : Fracture, etc.
13
Withdrawal of Antithyroid Drug Therapy
Severe Emotional Stress
Vigorous Thyroid Palpation
Parturition
14 Hypoglycemia
15
16 "Healthy Food" Preparation Containing
Sea weed or Kelp
17 Congestive Heart Failure18
19 Bowel Infarction
20 Tooth Extraction
21 TH Ingestion
22 Burn Injury
23 Sepsis
24 Childbirth
Sympathomimetic Drugs :
Toxemia of Pregnancy
Pseudoephedrine , Amiodarone , etc
1. Classical Thyroid StormCharac ter is t ics o f th is c lass are : the presence o f go i te r (G) and /o r o rb i ta l (O)
s i g n s , o n e o r m o r e p r e c i p i t a n t ( P ) , b o d y t e m p e r a t u r e> 39 .5 C, and pu lse ra te >
120 per minute. Hence, formula G/O: P-39.5-120 can be used for diagnosis of classicalthyroid storm. I f the case meets the character is t ics of th is formula, the total number of
Burch-Wartofsky Score (BW-Score) wi l l be > 50, wi th the calculat ion as fo l lows: P =
10, tempera ture > 39 .5 = 25 , pu l s e r ate ( tac hy c a r d ia ) > 1 2 0 = 1 5 , a n d t h e to t a l
score = 50. List o f p rec ip itan t can be fo und in TABLE-2.
-
8/10/2019 Capita Selecta in Endocrinology and Metabolism-2007
9/14
9BAGIAN-SMF PENYAKIT DALAM FK. UNAIR RSU Dr. SOETOMO SURABAYA
Capita Selecta inEndocrinology andMetabolism- 2007
(GLOBESITY, Formula G/O : P-39.5-120, ADMA, CMR, Anakinra)
(Clinical Experiences: Tjokroprawiro 2005-2007)
TABLE-2 Dx with ASK-SCORE >50 for Classical Thyroid Storm
Should this Tetralogy (TTS) is Met, the SCORE will be > 50
1 T w o o f th e F oll ow in g :
2
3
4
a Goiter, b Orbital Signs, c And /Or : TSHs, FT3, FT4
Tempera tu re > 39 .5 0C : S co re > 2 5
T a ch yc a rd ia > 1 2 0/m i n : S co re > 1 5
Precipi tant (+) : Score 10 , or CNS E ffects (+) : Score 10-30
FORMULA G/O : P 39.5 120
Diagnosis of CLASSICAL TS with FORMULA G/O : P 39.5 - 120
G /O = G o i t er , O r b i t al S i g n s : P 3 9.5 1 20
2. Non-Classical thyroid Storm
If the temperature of patients is less than 39.5 and tachycardia is less than 120,the calculation with the table of BW-Score should be used for diagnosis of Non-
Classical Thyroid Storm. TABLE-1, TABLE-2 and TABLE -3 can be used for score
calculation of BW-Score.
-
8/10/2019 Capita Selecta in Endocrinology and Metabolism-2007
10/14
10 PENDIDIKAN KEDOKTERAN BERKELANJUTAN ILMU PENYAKIT DALAM XXII-2 007
Askandar Tjokroprawiro
A score of 45 or greater is highly suggestive of thyroid crisis
A score of 25-44 is suggestive of impending thyroid crisis
A score below 25 is unlikely to represent thyroid crisis
IV. Once-Week ly EXENATIDE-LAR for the treatment of T2DM?
Incretins are hormones produced from the gastrointestinal track that act to
enhance the normal release of insulin after the oral ingestion of carbohydrates. Theirp l e i o t r o p i c e f f e c t s a r e (Gautier et al 2005, DeFronzo et al 2005):
1. to decrease gastric emptying
2. to promote a feeling of satiety that can lead to weight loss in overweightpatients (an increased sense of satiety)
3. to reduce post prandial glucagons levels
4. to increase islet cell mass (?)
-
8/10/2019 Capita Selecta in Endocrinology and Metabolism-2007
11/14
11BAGIAN- SM F PENYAKIT DALA M FK. UNAIR RSU Dr. SOETOMO SURAB AYA
Capita Selecta in Endocrinology and Metabolism - 2007
(GLOBESITY, Formula G/O : P-39.5-120, ADMA, CMR, Anakinra)
The most well-characterized incretin is GLP-1.Extenatide is the currently available incretin mimetic. On April 28, 2005, the Food
and Drug Administration (FDA) approved twice daily extenatide sc injection under
the trade name Byetta. This drug is the first in a new class of drugs for the treatment
of T2DM called incretin mimetic and exhibits many of the same effects as the human
incretin hormone glucagons-like peptide-1 (GLP-1). GLP-1, secreted in response tofood intake, has multiple effects on the intestine, liver, pancreas and brain that work
in concert to improve blood sugar.
Indications of Byetta injection (Buse et al 2004, Kendal l et al 2005 ):
1. Patients with T2DM who are unsuccessful at controlling their blood sugar levels
despite using commonly prescribed oral medications metformin, a sulfonylurea,
or both.2. Patients with T1DM who are undergoing islet cell transplantation; exenatide haspotential effects to help with islet function.
Amylin Parm., Inc., Eli Lilly and company and Alkermes, Inc. announced in 2006
the results from the ongoing Phase-2 multi-dose study of a long-acting release (LAR)formulation of Once-Weekly Extenatide-LAR clinical study in patients with T2DM (http:/
/ww w.diabetesincontrol.co m/results_print.php?storyarticle= 3060).
Results of Once-Weekly Extenatide-LAR (2.0 mg subcutaneous injection weekly),
after 15 weeks with Phase-2, randomized, placebo-controlled, double-blind studyincluding 45 patients with T2DM are:
1. AIC, improved approximately 2 (two) %
2. Fasting blood glucose dropped 50 mg/dl
3. Average weight loss was 9 poundsHowever, the most common adverse event was mild nausea which occurred in
approximately 20% of subjects in the high dose (2.0 mg) group compared to
approximately 7% in the placebo group.
These studies assessed the potential for exenatide to help improve beta-cell
survival in patients receiving islet cell transplants. In animal studies, this drug is
suggested can help increase islet cell mass. There are very small studies, but they
are encouraging, both for patients who are undergoing islet cell transplants and for
the potential of exenatide to help restore the abnormal beta-cell function in patientswith type 2 diabetes mellitus.
Excenatide_LAR has not been approved by the FDA for marketing in the United
States.
V. ANAKINRA: the promising drug for the treatment of T2DM
Anakinra is a recombinant version of the naturally occurring human interleukin-1
receptor antagon ist that blocks the effects of interleukin-1 and (Perr ier e t a l
2 0 0 6 ). Interleukin-1 , a proinflammatory cytokines, impiclated as an effector
molecule of inflammatory beta-cell destruction leading to T1DM, inhibits the functionand promotes the apoptosis of beta-cells (Dinare l lo 1996, Mandrup-Poulsen 1996,
Bend t zen e t a l 1986 ). Beta-cell producing interleukin-1 have been observed in
pancreatic sections obtained from patients with T2DM, leading to impaired insulin
-
8/10/2019 Capita Selecta in Endocrinology and Metabolism-2007
12/14
12 PENDIDIKAN KEDOKTERAN BERKELANJUTAN ILMU PENYAKIT DALAM XXII-2 007
Askandar Tjokroprawiro
secretion, decreased cell proliferation, and apoptosis (Maed le r 2002 , La rsen e t a l2007). The expression of interleukin-1 receptor antagonist is reduced in pancreatic
islet of patients with T2DM, and high glucose levels induce the production of
interleukin-1(Larsen et al 2007).
Anakinra (a recombinant of human interleukin-1 receptor antagonist), a naturally
occurring competitive inhibitor of interleukin-1 binding to the type 1 receptor, protects
human beta-cells from glucose-induced functional impairment and apoptosis (Dinarello
1996, 2000; Maed ler 2002).
Hypothetically, intervention in the islet balance between interleukin-1 receptor
antagonist and interleukin-1 might improve beta-cell function and glycemic control
in patients with T2DM.
Most recently, Larsen et al (2007) in double-blind, parallel-group trial involving70 patients with T2DM, randomly assigned 34 patients to receive 100mg of anakinra
subcutaneously, once daily for 13 weeks and 36 patients to receive placebo
concluded: that blockade of interleukin-1 with anakinra improve glycemia and beta-cell
secretory function and reduce markers of inflammation (C-reactive protein, interleukin-6).
In conclusion, ankinra is most likely to be promising therapeutic potential in the
treatment of patients with T2DM. However, further investigation is needed to evaluate
its long-term use and adverse reaction, and its detailed potential effects in preventing
beta-cell destruction and promoting beta-cell regeneration in T2DM.
As a supplement of this paper, Standard of Medical Care in Diabetes recommended
by ADA-2007 can be seen in TABLE-4.
-
8/10/2019 Capita Selecta in Endocrinology and Metabolism-2007
13/14
13BAGIAN-SMF PENYAKIT DALAM FK. UNAIR RSU Dr. SOETOMO SURABAYA
Capita Selecta inEndocrinology andMetabolism- 2007
(GLOBESITY, Formula G/O : P-39.5-120, ADMA, CMR, Anakinra)
TABLE-4 Standards of Medical Care in Diabetes of ADA : 2007
(Summ a rized : Tjokrop rawiro 2007)
Glycemic Control (D) :
AIC (Primary Target for Glycemic Control)
Pre Prandial Capillary Plasma Glucose
Peak Prandial Capillary Plasma Glucose
Blood Pressure (H) :
Lipids (L) :
LDL
TG*)
HDL
Target :
< 7%
90-130 mg/dl
< 180 mg/dl
< 130/80 mmHg
Target :
< 100 mg/dl
< 150 mg/dl
> 40 mg/dl **)
A normal AIC , < 6 % ; P ost P ra ndial G lucose ma y be ta rgete d if A IC G oals
Non-HDL = Total Chol. minus HDL Chol.
**) For W omen : I t has been suggested that HDL goal be increased by 10 mg/dl
are not met (despite normal prepra ndial glucose go als)*)CURRENT NCEP/ATPIII: If TG >200 mg/dl, Non-HDL Chol. should be < 130 mg/dl
REFERENCES
1. American Diabetes Association = ADA (2007). Standards of Medical Care in Diabetes 2006.
Diabetes Care 30,S4
2. Bendtzen K, Mandrup-Poulsen T, Nerup J et al (1986). Cytotoxicity of human pI 7 interleukin-1 for
pancreatic islets of Langerhans. Science 232,1545
3. Burch and Wartofsky, 1993, Burch HB, Wartofsky L (1993). Life-threatening thyrotoxicosis:
Thyroid Storm. Endocrinol Metab Clin North Amer 22,263
4. Buse JB, Henry RR Han J et al (2004). Effectsof exenatide on glycemic control over 30 weeks in
sulfonylurea-treated patients with type 2 diabetes. Diabetes Care 27,2628
5. DeFronzo RA, Ratner RE, Han J et al (2005). Effects of exenatide on glycemic control and weight
over 30 weeks in metformin-treated patients with type 2 diabetes. Diabetes Care 28,1092
6. Dinarello CA (1996). Biologic basis for interleukin-1 in disease. Blood 87,2095
7. Eid HM, Arnesen H, Hjerkinn EM, et al (2004). Relationship between obesity, smoking, and the
endogenous nitric oxide synthase inhibitor, asymmetric dimethylarginine. Metabolism 53(12),1574
8. Gautier JF, Fetita S, Sobngwi E, Salaun-Martin C (2005). Biological actions of the incretins GIPand GLP-1 and therapeutic perspectives in patients with type 2 diabetes. Diabetes Metab 31,233
-
8/10/2019 Capita Selecta in Endocrinology and Metabolism-2007
14/14
14 PENDIDIKAN KEDOKTERAN BERKELANJUTAN ILMU PENYAKIT DALAM XXII-2 007
Askandar Tjokroprawiro
9. Gr eenspan FS , Gardner DG (2004). Endocrine Emergencies. Basic & Clinical Endocrinology 7,867
10. Hall JB, S chmidt GA, Wood LDH (1999). Thyroid Di sease. P r inciples of Critical Care 2,715
11. http://w ww.diabetesincontrol.com/results_print.php?storyart icle= 3060 O ne Weekly Byetta
(Exenatide LAR) Drops A1C 2 Present with 9 lbs Wt Loss. News & information for MedicalP rofessionals Exenatide LAR (2007)
12. Kendall DM , Riddle MC, Rosentock J et al (2005). Effects of exenatide on glycemic contr ol in
patients with type 2 diabetes treated with metformin and a sulfonylurea. Diabetes Care 28,1083
13. Kr zyanowska K, M ittermayer, Kopp HP, et al (2004). Weight loss r educes cir culating asym-
metrical dimethylarginine concentrations in morbidly obese women. The Journal of Clinical
Endocrinology & Metabolism 89,6277
14. Larsen CM, Faulenbach M, Vaag A, et al (2007). Interleukin-1 Receptor Anatagonist in Type 2
Diabetes Mellitus. N Engl J Med 356,1517
15. Maas R (2005). P harmacotherapies and their influence on asymmetric dimethylar ginine(AD MA).
Vascular Medicine 10,S 49
16. Maedler K, S er geev P, Ri s F, et al (2002). Glucose-induced beta- cell production of IL-ibeta
contribute to glucotaoxicity in human pancreatic islets. J Clin Invest 110,851
17. Mandrup-P oulsen T (1996). Therole of interleukin-1 in thepathogenesis of IDDM. Diabetologia 39,1005
18. Mokdad AH, SerdulaMK, D ietz WHet al (1999). Thespread of the obesity epidemic in theUnited
S tates, 1991 1998. JAMA 282,1519
19. Roth J, Qiang X, M arban S L et al (2004). The Obesity P andemic: Wher e We Been and Wher e Are
We Going? Obesity Research 12,88S
20. Tietgens S , Leinung MC (1995). Thyroid S torm. Med Clin of N Amer 99,169
21. Tjokroprawir o A (1995). Di abetes Mellitus: Rekapitulasi 1995. KONAS -III P ER S ADI. Surabaya,
14-16 Oktober
22. Tjokroprawiro A (2003). Metabolic S yndrome: Obesity is the Central P roblem (Focus on the
Roles of S ibutr amine). National S ymposium on Metabolic S yndrome. Makassar, 17-18 May
23. Tjokroprawir o A (2004). Metabolic S yndromevs Insulin Resistance Syndrome. A Cluster of Compo-nents and S trategies for Treatment. P lenar y Lecture Nutri Indonesia-2004. Jakar ta, 14-15 Febr uar y
24. Tjokr oprawiro A (2005). The MetS : One of the Major Threat to Human Health. P lenary Lecture.S urabaya M etabolic Syndrome Update-1. S urabaya, 19-20 February
25. Tjokroprawiro A (2006). Diabetic Nephropathy: from Basic to Clinics (The Importance of FiveS atan Cir cles for Pathogenesis and Treatment). Malang, 26-27 August
26. Tjokroprawiro A (2007). Thyroid S torm : Diagnosis and Management (P r actical G uidelines with
Formula TS -41668.24.6 and CS -7.3.7) P ost Congress Course and Workshop of E NT Head and
Neck. S urabaya, 15 July
27. Turner HE, Wass JAH(2003). Thyroid S torm. Oxford Handbook of Endocrinology and Diabetes 1,35
-oOo-