Cannabis Youth Treatment Experiment: 12 and 30 Month Main Findings Michael Dennis, Ph.D. (On Behalf...
34
Cannabis Youth Treatment Experiment: 12 and 30 Month Main Findings Michael Dennis, Ph.D. (On Behalf of the CYT Steering Committee) Chestnut Health Systems Bloomington, IL Presentation at CSAT Pre-Session at the College of Problems on Drug Dependence, 65 th Annual Scientific Meeting, June 13, 2003, Bal Harbour, Florida. Available from author at www.chestnut.org/li/posters , [email protected] or 309- 827-6026.
-
Upload
marylou-garrett -
Category
Documents
-
view
216 -
download
2
Transcript of Cannabis Youth Treatment Experiment: 12 and 30 Month Main Findings Michael Dennis, Ph.D. (On Behalf...

Cannabis Youth Treatment Experiment: 12 and 30 Month Main Findings
Michael Dennis, Ph.D. (On Behalf of the CYT Steering Committee)Chestnut Health SystemsBloomington, IL
Presentation at CSAT Pre-Session at the College of Problems on Drug Dependence, 65th Annual Scientific Meeting, June 13, 2003, Bal Harbour, Florida. Available from author at www.chestnut.org/li/posters, [email protected] or 309-827-6026.

Acknowledgement
This presentation is based on the work, input and contributions from several other people including: Nancy Angelovich, Tom Babor, Laura (Bunch) Brantley, Joseph A. Burleson, George Dent, Guy Diamond, James Fraser, Michael French, Rod Funk, Mark Godley, Susan H. Godley, Nancy Hamilton, James Herrell, David Hodgkins, Ronald Kadden, Yifrah Kaminer, Tracy L. Karvinen, Pamela Kelberg, Jodi (Johnson) Leckrone, Howard Liddle, Barbara McDougal, Kerry Anne McGeary, Robert Meyers, Suzie Panichelli-Mindel, Lora Passetti, Nancy Petry, M. Christopher Roebuck, Susan Sampl, Meleny Scudder, Christy Scott, Melissa Siekmann, Jane Smith, Zeena Tawfik, Frank Tims, Janet Titus, Jane Ungemack, Joan Unsicker, Chuck Webb, James West, Bill White, Michelle White, Caroline Hunter Williams, the other CYT staff, and the families who participated in this study. This presentation was supported by funds and data from the Center for Substance Abuse Treatment (CSAT’s) Persistent Effects of Treatment Study (PETS, Contract No. 270-97-7011) and the Cannabis Youth Treatment (CYT) Cooperative Agreement (Grant Nos. TI11317, TI11320, TI11321, TI11323, and TI11324). The opinions are those of the author and steering committee and do not reflect official positions of the government .

CYT Cannabis Youth Treatment Randomized Field Experiment
Sponsored by: Center for Substance Abuse Treatment (CSAT), Substance Abuse and Mental Health Services Administration (SAMHSA), U.S. Department of Health and Human Services
Coordinating Center:Chestnut Health Systems, Bloomington, IL, and Chicago, ILUniversity of Miami, Miami, FLUniversity of Conn. Health Center, Farmington, CT
Sites:Univ. of Conn. Health Center, Farmington, CTOperation PAR, St. Petersburg, FLChestnut Health Systems, Madison County, ILChildren’s Hosp. of Philadelphia, Phil. ,PA

Marijuana
Use is starting at younger ages Is at an historically high level among adolescents Potency increased 3-fold from 1980 to 1997 Is three times more likely to lead to dependence
among adolescents than adults Is associated with many health, mental and
behavioral problems Is the leading substance mentioned in adolescent
emergency room admissions and autopsies

Treatment
Marijuana related admissions to adolescent substance abuse treatment increased by 115% from 1992 to 1998
Over 80% of adolescents entering treatment in 1998 had a marijuana problem
Over 80% are entering outpatient treatment Over 75% receive less than 90 days of treatment
(median of 6 weeks) Evaluations of existing adolescent outpatient treatment
suggest that last than 90 days of outpatient treatment is rarely effective for reducing marijuana use.

Purpose of CYT
To learn more about the characteristics and needs of adolescent marijuana users presenting for outpatient treatment.
To adapt evidence-based, manual-guided therapies for use in 1.5 to 3 month adolescent outpatient treatment programs in medical centers or community based settings.
To field test the relative effectiveness, cost and cost-effectiveness of five interventions targeted at marijuana use and associated problems in adolescents.
To provide validated models of these interventions to the treatment field in order to address the pressing demands for expanded and more effective services.

Design
Target Population: Adolescents with marijuana disorders who are appropriate for 1 to 3 months of outpatient treatment.
Inclusion Criteria: 12 to 18 year olds with symptoms of cannabis abuse or dependence, past 90 day use, and meeting criteria for outpatient treatment
Data Sources: self report, collateral reports, on-site and laboratory urine testing, therapist alliance and discharge reports, staff service logs, and cost analysis.
Random Assignment: to one of three treatments within site in two research arms and quarterly follow-up interview for 12 months
Long Term Follow-up: under a supplement from PETSA follow-up was extended to 30 months (42 for a subsample)

Randomly Assigns to:
MET/CBT5Motivational Enhancement Therapy/
Cognitive Behavioral Therapy (5 weeks)
MET/CBT12Motivational Enhancement Therapy/
Cognitive Behavioral Therapy (12 weeks)
FSN
Family Support Network
Plus MET/CBT12 (12 weeks)
ACRAAdolescent Community
Reinforcement Approach(12 weeks)
MDFTMultidimensional Family Therapy
Experiment 2Experiment 1Incremental Arm Alternative Arm
Two Experiments or Study Arms
Randomly Assigns to:
MET/CBT5Motivational Enhancement Therapy/
Cognitive Behavioral Therapy (5 weeks)
(12 weeks)
Source: Dennis et al, 2002

Contrast of the Treatment Structures
Individual Adolescent Sessions
CBT Group Sessions
Individual Parent Sessions
Family Sessions/Home Visits
Parent Education Sessions
Total Formal Sessions
Type of ServiceMET/CBT5
MET/CBT12 FSN ACRA MDFT
2
3
5
2
10
12
2
10
4
6
22
10
2
2
14
6
3
6
15
Case management/Other Contacts
As needed
As needed
As needed
Total Expected Contacts 5 12 22+ 14+ 15+
Total Expected Hours 5 12 22+ 14+ 15+
Total Expected Weeks 6-7 12-13 12-13 12-13 12-13
Source: Diamond et al, 2002

5
10
5
11
14
23
0
5
10
15
20
25
MET/CBT5
MET/CBT12
MET/CBT12 +
FSN
MET/CBT5
ACRA MDFT
Hou
rs
Day
s
CaseManagement
FamilyCounseling
Collateral only
Multi-Familygroup
Multi-ParticipantGroup
Participant only
Incremental Arm Alternative Arm
Actual Treatment Received by Condition
Source: Dennis et al, under review
MET/CBT12 adds 7 more sessions of
group
FSN adds multi family group,
family home visits and more case management
ACRA and MDFT both rely on
individual, family and case management instead of group
With ACRA using more individual therapy
And MDFT using more
family therapy

$1,559$1,413
$1,984
$3,322
$1,197$1,126
$-
$500
$1,000
$1,500
$2,000
$2,500
$3,000
$3,500
$4,000
MET/C
BT5 (6.8
wee
ks)
MET/C
BT12 (1
3.4 w
eeks
)
FSN (14.2
wee
ks w
/family
)
MET/C
BT5 (6.5
wee
ks)
ACRA (12.8
wee
ks)
MDFT(1
3.2 w
eeks
w/fa
mily)
$1,776
$3,495
NTIES E
st (6
.7 wee
ks)
NTIES E
st.(1
3.1 w
eeks
)
Ave
rage
Cos
t P
er C
lien
t-E
pis
ode
of C
are
|--------------------------------------------Economic Cost-------------------------------------------|-------- Director Estimate-----|
Average Episode Cost ($US) of Treatment
Source: French et al., 2002
Less than average
for 6 weeks
Less than average
for 12 weeks

Implementation of Evaluation
Over 85% of eligible families agreed to participate Quarterly follow-up of 94 to 98% of the adolescents from 3- to 12-
months (88% all five interviews) Long term follow-up completed on 90% at 30-months and 91% (of
116 subsample) at 42-months Collateral interviews were obtained at intake, 3- and 6-months on
over 92-100% of the adolescents interviewed Urine test data were obtained at intake, 3, 6, 30 and 42 months 90-
100% of the adolescents who were not incarcerated or interviewed by phone (85% or more of all adolescents).
Self report marijuana use largely in agreement with urine test at 30 months (13.8% false negative, kappa=.63)
5 Treatment manuals drafted, field tested, revised, send out for field review, and finalized (10-30,000 copies of each already printed and distributed)
Descriptive, outcome and economic analyses completed
Source: Dennis et al, 2002, under review

Adolescent Cannabis Users in CYT were as or More Severe Than Those in TEDS*
85%
46%
26%
78%
26%
47%
26%
71%
0%
20%
40%
60%
80%
100%
First usedunder age
15
Dependence Weekly ormore use at
intake
PriorTreatment
% o
f A
dm
issi
on
s
.
CYT Outpatient(n=600) TEDS Outpatient (n=16,480)* Adolescents with marijuana problems admitted to outpatient treatment
Source: Tims et al, 2002
Demographic Characteristics
62%
15%
55%50%
30%
83%
17%
0%
20%
40%
60%
80%
100%
Female Male AfricanAmerican
Caucasian Under 15 15 to 16 Singleparentfamily
Source: Tims et al, 2002

Institutional Involvement
25%
87%
47%
62%
0%
20%
40%
60%
80%
100%
In school Employed Current CJInvolvement
Coming fromControlled
Environment
Source: Tims et al, 2002

Patterns of Substance Use
9%17%
71%73%
0%
20%
40%
60%
80%
100%
Weekly Tobacco Use
WeeklyCannabis Use
Weekly AlcoholUse
Significant Timein ControlledEnvironment
Source: Tims et al, 2002

Multiple Problems are the NORM
86%
37%
12%
25%
61%
60%
66%
83%
83%
0% 20% 40% 60% 80% 100%
Any Marijuana Use Disorder
Any Alcohol Use Disorder
Other Substance Use Disorders
Any Internal Disorder
Any External Disorder
Lifetime History of Victimization
Acts of Physical Violence
Any (other) Illegal Activity
Three to Twelve Problems
Self-Reported in Past Year
Source: Dennis et al, under review
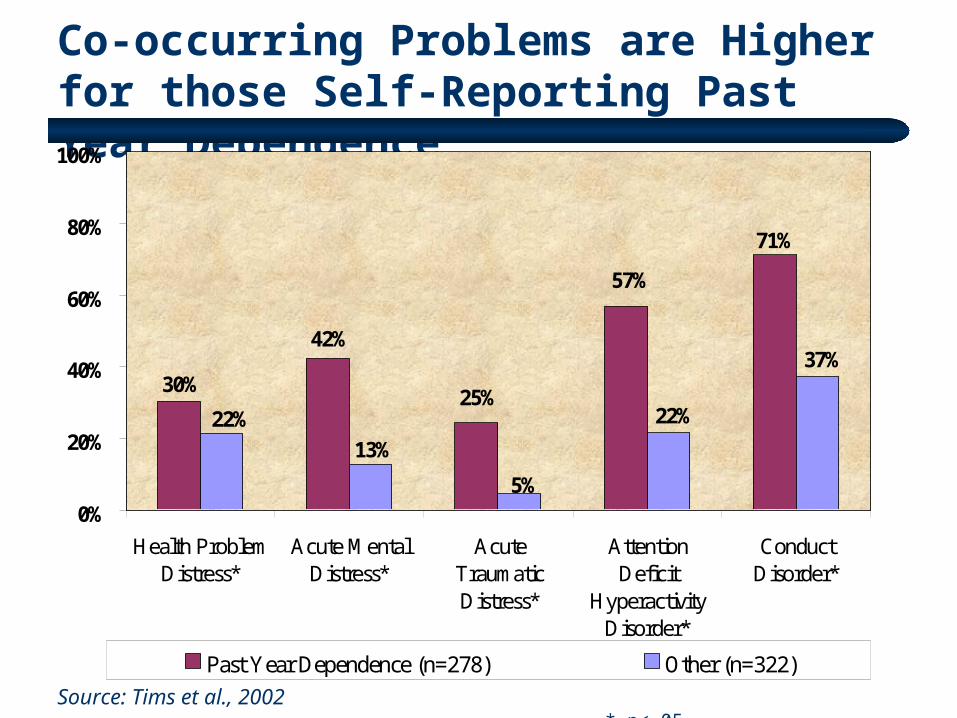
Co-occurring Problems are Higher for those Self-Reporting Past Year Dependence
71%
57%
25%
42%
30%37%
22%
5%
13%
22%
0%
20%
40%
60%
80%
100%
Health ProblemDistress*
Acute MentalDistress*
AcuteTraumaticDistress*
AttentionDeficit
HyperactivityDisorder*
ConductDisorder*
Past Year Dependence (n=278) Other (n=322)
Source: Tims et al., 2002 * p<.05
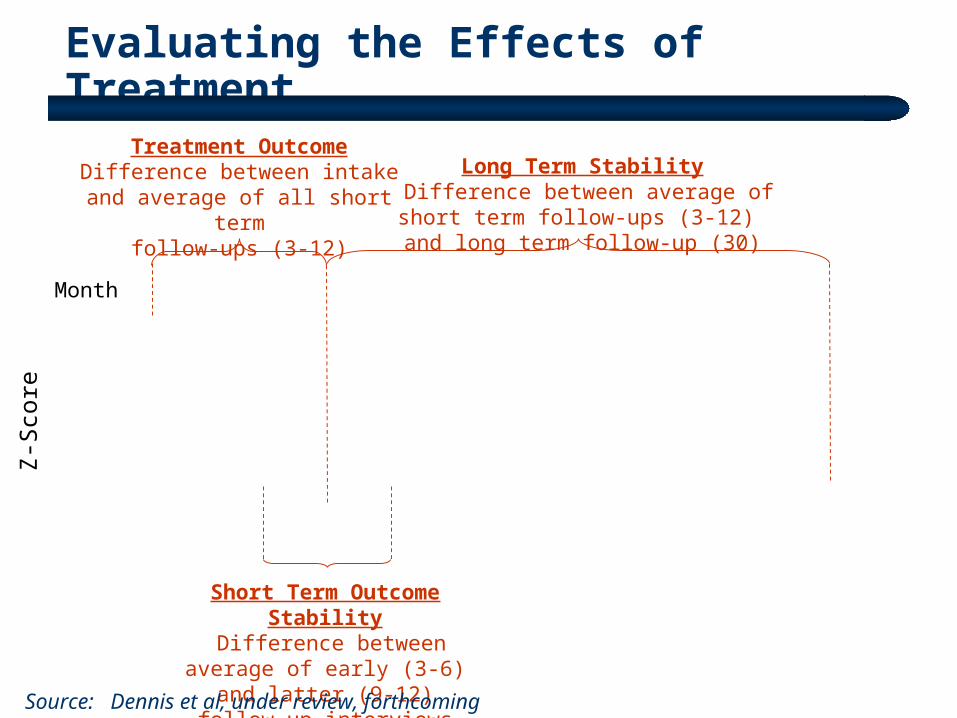
Evaluating the Effects of Treatment
Short Term Outcome Stability Difference between average of
early (3-6) and latter (9-12) follow-up interviews
Treatment OutcomeDifference between intake and average
of all short term follow-ups (3-12)
Long Term Stability Difference between average of short term
follow-ups (3-12) and long term follow-up (30)
Source: Dennis et al, under review, forthcoming
Month
Z-S
core
-0.60
-0.50
-0.40
-0.30
-0.20
-0.10
0.00
0 3 6 9 12
15
18
21
24
27
30
Freq. of Use
Sub. Prob.

Change in Substance Frequency Scale in CYT Experiment 1: Incremental Arm
Months from Intake
0.00
0.05
0.10
0.15
0.20
0.25
0 3 6 9 12 15 18 21 24 27 30
MET/CBT5
MET/CBT12
FSN
Source: Dennis et al, forthcoming
Treatment Outcome: -Use reduced (-34%)
- No Sig. Dif. by condition
Short Term Stability:- Outcomes stable (-1%) - No Sig. Dif. by condition
Long Term Stability:- Use increases (+64%)
- No Sig. Dif. by condition

Change in Number of Substance Problems in CYT Experiment 1: Incremental Arm
Months from Intake
0
1
2
3
4
5
0 3 6 9 12 15 18 21 24 27 30
MET/CBT5
MET/CBT12
FSN
Source: Dennis et al, forthcoming
Long Term Stability:-Problems increase (+17%)
-Sig. Dif. by condition (+37% vs +10% vs +7%)
Treatment Outcome: -Problems reduced (-46%)
- Sig. Dif. by condition(-50% vs. –33% vs. –51%)
Short Term Stability:-Further reductions (-25%)- No difference by condition

Change in Substance Frequency Scale inCYT Experiment 2: Alternative Arm
Months from Intake
0.00
0.05
0.10
0.15
0.20
0.25
0 3 6 9 12 15 18 21 24 27 30
MET/CBT5
ACRA
MDFT
Source: Dennis et al, forthcoming
Treatment Outcome: - Use reduced (-35%)
- No Sig. Dif. by condition
Short Term Stability:-Further reductions (-6%)
- Sig. Dif. by condition(+4% vs. –10% vs. –11%)
Long Term Stability:- Outcomes stable
(+20%)-No Sig. Dif. by condition

Change in Number of Substance Problems inCYT Experiment 2: Alternative Arm
Months from Intake
0
1
2
3
4
5
0 3 6 9 12 15 18 21 24 27 30
MET/CBT5
ACRA
MDFT
Source: Dennis et al, forthcoming
Long Term Stability:- Outcomes stable (+7%)-No Sig. Dif. by condition
Treatment Outcome: - Problems reduced (-43%)- No difference by condition
Short Term Stability:- Outcomes stable (-8%)
- No Sig. Dif. by condition
Percent in Past Month Recovery (no use or problems while living in the community)
14%17%
6%
14%11%
18%
0%
10%
20%
30%
40%
50%
0 3 6 9 12 30MET/ CBT5
0 3 6 9 12 30MET/ CBT12
0 3 6 9 12 30FSN
0 3 6 9 12 30MET/ CBT5
0 3 6 9 12 30ACRA
0 3 6 9 12 30MDFT
Source: Dennis et al, forthcoming

Cumulative Recovery Pattern at 30 months:(The Majority Vacillate in and out of Recovery)
Source: Dennis et al, forthcoming
37% Sustained Problems
5% Sustained Recovery
19% Intermittent, currently in
recovery
39% Intermittent, currently not in
recovery

Cost Per Person in Recovery at 12 and 30 Months After Intake by CYT Condition
Source: Dennis et al., under review; forthcoming
$0
$5,000
$10,000
$15,000
$20,000
$25,000
$30,000
CPPR at 30 months** $6,437 $10,405 $24,725 $27,109 $8,257 $14,222
CPPR at 12 months* $3,958 $7,377 $15,116 $6,611 $4,460 $11,775
MET/ CBT5 MET/ CBT12 FSNM MET/ CBT5 ACRA MDFT
Experiment 1 (n=299) Experiment 2 (n=297)
Cos
t P
er P
erso
n in
Rec
over
y (C
PP
R)
* P<.0001, Cohen’s f= 1.42 and 1.77 at 12 months** P<.0001, Cohen’s f= 0.76 and 0.94 at 30 months
Stability of MET/CBT-5
findings mixed at 30 months
Integrated family therapy (MDFT) was more cost effective than
adding it on top of treatment (FSN) at 30 months
MET/CBT-5, -12 and ACRA more cost effective at
12 months

Reduction in Average Cost to Society in CYT Experiment 1: Incremental Arm
$-
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
Intake 3 6 9 12 15 18 21 24 27 30
Months from Intake
MET/CBT5
MET/CBT12
FSNM
Source: French et al, in press; forthcoming
Includes the cost of CYT Treatment
Further Reductions
(-47%) occurred out to
30 months
Reductions (-23%) in Average
Cost to Society offset Treatment Costs within 12
months

Reduction in Average Cost to Society in CYT Experiment 2: Alternative Arm
$-
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
Intake 3 6 9 12 15 18 21 24 27 30
Months from Intake
MET/CBT5
ACRA
MDFT
Source: French et al, in press; forthcoming
Includes the cost of CYT Treatment
Average Cost to Society goes up then down and
does not offset Tx Costs within 12 months (+7%)
Further Reductions
occurred out to 30 months
(-40%)

Average Cost to Society Varied More by Site than Condition
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
0 3 6 9 12 15 18 21 24 27 30
Months from Intake
UCHC, Farmington, CT (-24%, -44%)
PAR, St. Petersburg, FL (-22%, -49%)
CHS, Madison Co., IL (-8%, -51%)
CHOP, Philadelphia, PA (+18%, -34%)
Source: French et al, in press; forthcoming

Reprise of Clinical Outcomes
Co-occurring problems were the norm and varied with substance use severity.
Most of the treatment effects came during active phase of treatment and were sustained or improved during the 12 months of initial follow-up; though longer term follow-up suggests that some ground was lost.
While there were some effects of treatment type, these were not easily explained by dosage or level of family therapy and produced only minor improvements.
While more effective than many earlier outpatient treatments, 2/3rds of the CYT adolescents were still having problems 12 months latter, 4/5ths were still having problems 30 months latter.

Reprise of Economic Outcomes
There were considerable differences in the cost of providing each of the interventions.
MET/CBT-5, -12 and ACRA were the most cost effective at 12 months, though the stability of the MET/Findings were mixed at 30 months.
Reductions in Average Quarterly Cost to Society offset the cost of treatment within 12 months in experiment 1 and with 30 months in experiment 2.
At 12 months the MET/CBT5 intervention clearly had the highest rate of return, though it was less likely to have “additional” benefits at 30 months
Results of clinical outcomes, cost-effectiveness, and benefit cost were different – suggesting the importance of multiple perspectives

Impact and Next Steps
Papers published on design, validation, characteristics, matching, clinical contrast, treatment manuals, therapist reactions, 6 month outcomes, cost, benefit cost
Papers with main findings at 12 months under review and 30 month findings being submitted this summer.
Interventions being replicated as part of over two dozen studies currently or about to go into the field
Over 10-30,000 copies of each of 5 manuals distributed to policy makers, providers, individual clinicians and training programs
Source: Dennis et al, 2002, under review

Implications
The CYT interventions provide replicable models of brief (1.5 to 3 month) treatments that can be used to help the field maintain quality while expanding capacity.
While a good start, the CYT interventions were still not an adequate dose of treatment for the majority of adolescents.
The majority of adolescents continued to vacillate in and out of recovery after discharge from CYT.
More work needs to be done on providing a continuum of care, longer term engagement and on going recovery management.

Contact Information
Michael L. Dennis, Ph.D., CYT Coordinating Center PILighthouse Institute, Chestnut Health Systems720 West Chestnut, Bloomington, IL 61701Phone: (309) 827-6026, Fax: (309) 829-4661E-Mail: [email protected]
Manuals and Additional Information are Available at: CYT: www.chestnut.org/li/cyt/findings or
www.chestnut.org/li/bookstore
NCADI: www.health.org/govpubs
PETSA: www.samhsa.gov/centers/csat/csat.html (then select PETS from program resources)