
CANINE PITUITARY DEPENDENT HYPERADRENOCORTICISM …€¦ · This article briefl y described the...
8
TODAY’S VETERINARY PRACTICE | January/February 2016 | tvpjournal.com CANINE PITUITARY DEPENDENT HYPERADRENOCORTICISM SERIES Peer Reviewed 36 Canine pituitary dependent hyperadrenocorticism (PDH), also known as Cushing’s disease, is a common endocrine disorder in older dogs. This disorder is caused by a pituitary adenoma (PA) that secretes inappropriate amounts of adrenocorticotropic hormone (ACTH), which results in bilateral adrenal hyperplasia and disorderly and excessive production of cortisol by the adrenal gland. Read Part 1 of this series—Comparative Epidemiology & Etiology in Dogs & Humans (November/December 2015)—at tvpjournal.com. This article briefly described the diagnosis of PDH, including clinical signs, common laboratory findings, and atypical presentations of canine PDH. BASELINE DIAGNOSTICS In all patients being screened for PDH, the following initial diagnostics should be performed prior to endocrine diagnostics: • Thorough history, including prior treatment with systemic or topical glucocorticoids • Physical examination (Table 1) • Complete routine database, including complete blood count, serum biochemical profile, urinalysis, urine culture, and blood pressure (Table 2). These diagnostics are important as the clinical signs of PDH are rarely pathognomonic, and patients are generally older and may have comorbidities that affect endocrine function tests (Table 3) and impact therapeutic options and prognosis. ENDOCRINE DIAGNOSTICS Specific endocrine tests and imaging modalities are available to both diagnose PDH (Table 3) and distinguish between the various causes of hyperadrenocorticism (HAC). No single test is perfect and, if the initial screening test is negative and high clinical suspicion of PDH exists, additional tests should be performed to determine a definitive diagnosis. CANINE PITUITARY DEPENDENT HYPERADRENOCORTICISM SERIES Part 2: Diagnostic Approach David Bruyette, DVM, Diplomate ACVIM VCA West Los Angeles Animal Hospital, Los Angeles, California, and Veterinary Diagnostic Investigation and Consultation, Woodland Hills, California TABLE 1. Common Clinical Signs & Sequelae of PDH in Dogs • Polyuria and polydipsia • Polyphagia • Abdominal distension • Bilaterally symmetric endocrine alopecia • Panting • Hypertension • Urinary tract infections • Additional dermatologic signs: » Thin skin » Pyoderma » Calcinosis cutis TABLE 2. Common Laboratory Findings in Dogs with PDH HEMATOLOGIC ABNORMALITIES • “Stress” leukogram: » Neutrophilic leukocytosis » Lymphopenia » Eosinopenia • Mild thrombocytosis • Mild erythrocytosis SERUM BIOCHEMICAL ABNORMALITIES • Increased serum alkaline phosphatase • Milder increase in alanine aminotransferase • Hypercholesterolemia • Hypertriglyceridemia • Hyperglycemia URINALYSIS ABNORMALITIES • Decreased urine specific gravity < 1.018 • Proteinuria • Urinary tract infection (even in absence of pyuria and bacteriuria) ACVIM Consensus Statement In 2012, the American College of Veterinary Internal Medicine (acvim.org) issued a consensus statement, Diagnosis of Spontaneous Canine Hyperadrenocorticism, that provides a thorough review of the diagnostic approach to patients with PDH and addresses many common clinical concerns. 1 Access this statement at onlinelibrary.wiley .com/doi/10.1111/ jvim.12192/epdf.
Transcript of CANINE PITUITARY DEPENDENT HYPERADRENOCORTICISM …€¦ · This article briefl y described the...

TODAY’S VETERINARY PRACTICE | January/February 2016 | tvpjournal.com
CANINE PITUITARY DEPENDENT HYPERADRENOCORTICISM SERIES Peer Reviewed
36
Canine pituitary dependent hyperadrenocorticism (PDH), also known as Cushing’s disease, is a common endocrine disorder in older dogs. This disorder is caused by a pituitary adenoma (PA) that secretes inappropriate amounts of adrenocorticotropic hormone (ACTH), which results in bilateral adrenal hyperplasia and disorderly and excessive production of cortisol by the adrenal gland.
Read Part 1 of this series—Comparative Epidemiology & Etiology in Dogs & Humans (November/December 2015)—at tvpjournal.com. This article briefl y described the diagnosis of PDH, including clinical signs, common laboratory fi ndings, and atypical presentations of canine PDH.
bASELINE DIAGNOSTICS In all patients being screened for PDH, the following initial diagnostics should be performed prior to endocrine diagnostics:• Thorough history, including prior treatment with
systemic or topical glucocorticoids• Physical examination (Table 1)• Complete routine database, including complete
blood count, serum biochemical profile,
urinalysis, urine culture, and blood pressure (Table 2). These diagnostics are important as the clinical
signs of PDH are rarely pathognomonic, and patients are generally older and may have comorbidities that affect endocrine function tests (Table 3) and impact therapeutic options and prognosis.
ENDOCRINE DIAGNOSTICSSpecifi c endocrine tests and imaging modalities are available to both diagnose PDH (Table 3) and distinguish between the various causes of hyperadrenocorticism (HAC). No single test is perfect and, if the initial screening test is negative and high clinical suspicion of PDH exists, additional tests should be performed to determine a defi nitive diagnosis.
CANINE PITUITARY DEPENDENT HYPERADRENOCORTICISM SERIES
Part 2: Diagnostic ApproachDavid Bruyette, DVM, Diplomate ACVIMVCA West Los Angeles Animal Hospital, Los Angeles, California, and Veterinary Diagnostic Investigation and Consultation, Woodland Hills, California
Table 1. Common Clinical Signs & Sequelae of PDH in Dogs• Polyuria and polydipsia• Polyphagia• Abdominal distension• Bilaterally symmetric endocrine alopecia• Panting • Hypertension• Urinary tract infections• Additional dermatologic signs:
» Thin skin » Pyoderma » Calcinosis cutis
Table 2. Common Laboratory Findings in Dogs with PDH HEMATOLOGIC ABNORMALITIES
• “Stress” leukogram: » Neutrophilic leukocytosis » Lymphopenia » Eosinopenia
• Mild thrombocytosis• Mild erythrocytosis
SERUM BIOCHEMICAL ABNORMALITIES
• Increased serum alkaline phosphatase• Milder increase in alanine aminotransferase• Hypercholesterolemia• Hypertriglyceridemia• Hyperglycemia
URINALYSIS ABNORMALITIES
• Decreased urine specifi c gravity < 1.018• Proteinuria• Urinary tract infection (even in absence of pyuria
and bacteriuria)
aCVIM Consensus StatementIn 2012, the American College of Veterinary Internal Medicine (acvim.org) issued a consensus statement, Diagnosis of Spontaneous Canine Hyperadrenocorticism, that provides a thorough review of the diagnostic approach to patients with PDH and addresses many common clinical concerns.1 Access this statement at onlinelibrary.wiley.com/doi/10.1111/jvim.12192/epdf.
tvpjournal.com | January/February 2016 | TODAY’S VETERINARY PRACTICE
CANINE PITUITARY DEPENDENT HYPERADRENOCORTICISM SERIES Peer Reviewed
37
Several endocrine screening tests are available to arrive at a diagnosis of HAC, including:• Low-dose dexamethasone suppression (LDDS)• ACTH stimulation• Urine cortisol to creatinine ratio (UCCR).
Additional tests may be required to differentiate PDH from other causes of hypercortisolemia, such as endogenous ACTH measurement and advanced imaging.
INITIAL ENDOCRINE SCREENINGLow-Dose Dexamethasone SuppressionLDDS demonstrates decreased pituitary sensitivity to negative feedback from glucocorticoids, via mechanisms discussed in the fi rst article in this series.
Indications. Most consider LDDS the screening test of choice for HAC unless the patient history suggests iatrogenic HAC, in which case ACTH stimulation is preferred.
Sensitivity/Specifi city. In veterinary medicine, the reported sensitivity and specifi city of the LDDS test range from 85% to 100% and from 44% to 73%, respectively.2-10
Test Results. Blood samples are obtained (1) before, (2) 4 hours after, and (3) 8 hours after dexamethasone administration (0.01 mg/kg IV). Diagnosis of HAC is based on lack of suppression of cortisol concentration 8 hours after dexamethasone administration.
ACTH StimulationACTH stimulation assesses adrenocortical reserve. Due to greater purity and quality control, use of synthetic ACTH is recommended. Use of compounded ACTH is discouraged, especially when monitoring patients on adrenolytic agents or adrenal enzyme blockers (see Synthetic Versus Compounded ACTH, page 38).
Indications. ACTH stimulation is the gold standard for diagnosis of iatrogenic HAC and spontaneous Addison’s disease (hypoadrenocorticism). Diagnosis of HAC is based on fi nding an elevated cortisol concentration (post ACTH administration) based on the reference range established by the laboratory.
Sensitivity/Specifi city. Sensitivity of ACTH stimulation for all forms of spontaneous canine HAC ranges from 57% to 95%. In dogs with PDH, sensitivity is 80% to 83%. Specifi city ranges from 59% to 93%.11-18
Due to its low sensitivity, it is inferior to LDDS as a screening test for spontaneous HAC. However, many clinicians still use ACTH stimulation because of its convenient study duration of 60 minutes and relative effectiveness in the clinical setting, especially when combined with abdominal ultrasound evaluation and interpreted in light of the history and physical examination.
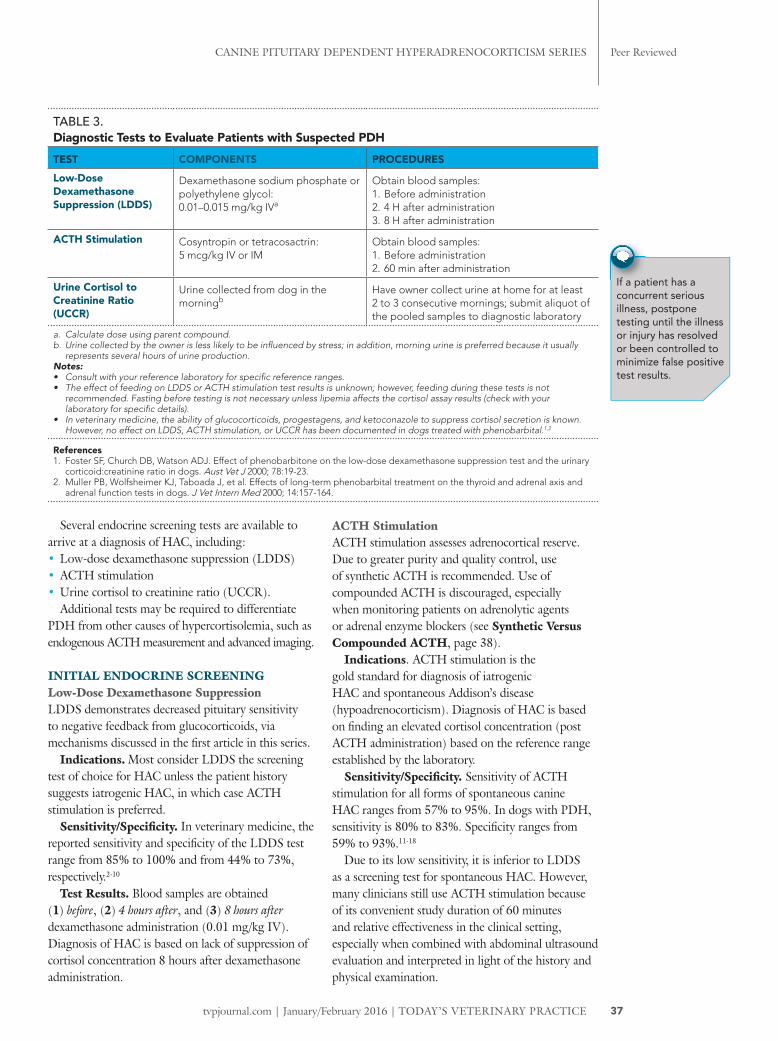
Table 3. Diagnostic Tests to Evaluate Patients with Suspected PDHTEST COMPONENTS PROCEDURESLow-Dose Dexamethasone Suppression (LDDS)
Dexamethasone sodium phosphate or polyethylene glycol: 0.01–0.015 mg/kg IVa
Obtain blood samples:1. Before administration2. 4 H after administration3. 8 H after administration
ACTH Stimulation Cosyntropin or tetracosactrin:5 mcg/kg IV or IM
Obtain blood samples: 1. Before administration2. 60 min after administration
Urine Cortisol to Creatinine Ratio (UCCR)
Urine collected from dog in the morningb
Have owner collect urine at home for at least 2 to 3 consecutive mornings; submit aliquot of the pooled samples to diagnostic laboratory
a. Calculate dose using parent compound.b. Urine collected by the owner is less likely to be infl uenced by stress; in addition, morning urine is preferred because it usually
represents several hours of urine production.Notes:• Consult with your reference laboratory for specifi c reference ranges.• The effect of feeding on LDDS or ACTH stimulation test results is unknown; however, feeding during these tests is not
recommended. Fasting before testing is not necessary unless lipemia affects the cortisol assay results (check with your laboratory for specifi c details).
• In veterinary medicine, the ability of glucocorticoids, progestagens, and ketoconazole to suppress cortisol secretion is known. However, no effect on LDDS, ACTH stimulation, or UCCR has been documented in dogs treated with phenobarbital.1,2
References1. Foster SF, Church DB, Watson ADJ. Effect of phenobarbitone on the low-dose dexamethasone suppression test and the urinary
corticoid:creatinine ratio in dogs. Aust Vet J 2000; 78:19-23.2. Muller PB, Wolfsheimer KJ, Taboada J, et al. Effects of long-term phenobarbital treatment on the thyroid and adrenal axis and
adrenal function tests in dogs. J Vet Intern Med 2000; 14:157-164.
If a patient has a concurrent serious illness, postpone testing until the illness or injury has resolved or been controlled to minimize false positive test results.

Today’s VeTerinary PracTice | January/February 2016 | tvpjournal.com
canine PiTuiTary dePendenT HyPeradrenocorTicism series Peer reviewed
38
Urine Cortisol to Creatinine RatioUCCR provides an integrated reflection of cortisol production, adjusting for fluctuations in blood concentrations. Determination of basal UCCRs can be performed alone or in tandem with other endocrine testing.
Indications. UCCR can be used as a screening test for hypercortisolemia, although a single positive result should not be overinterpreted. Adding oral dexamethasone suppression to UCCR testing has the advantage of potentially demonstrating both increased cortisol production and decreased sensitivity to glucocorticoid feedback.
Sensitivity/Specificity. When a single, random urine sample is collected in veterinary hospitals, reported sensitivity and specificity of UCCR for diagnosis of HAC ranges from 75% to 100% and 20% to 25%, respectively.20,21 In some dogs, there is considerable day-to-day variation in UCCR results.22
However, in dogs with physical and biochemical changes consistent with HAC, when 2 basal UCCRs were above the cut-off level:22
• Sensitivity was 99%; 95% confidence interval (94%–100%)
• Specificity was 77%; 95% confidence interval (64%–87%).
DIFFERENTIATING PDH FROM ADH: LAbORATORy ANALySISGiven that PDH and adrenal dependent hyperadrenocorticism (ADH) are the most common forms of HAC, and that their treatment options and prognoses differ, it is important to recommend additional testing to determine the exact etiology of HAC. Several diagnostic modalities are commonly used to differentiate between PDH and ADH (Table 4):• Endogenous ACTH• Dexamethasone suppression• Dexamethasone suppression with UCCR.
Endogenous ACTHCanine ACTH is secreted from the pituitary gland in an episodic, pulsatile fashion in both healthy dogs and those with PDH.1 A circadian rhythm has not been convincingly demonstrated, although one study reported higher plasma concentrations of canine ACTH (cACTH) in late afternoon than in the morning.23
Indications. Concentrations of cACTH do not differ between healthy dogs and those with PDH, and its measurement is not useful to screen for HAC. However, measurement of cACTH is the most accurate stand-alone biochemical test for differentiating PDH from an adrenocortical tumor (AT), but the sensitivity of the assay differs with methodology. Normal or elevated concentrations of cACTH are consistent with PDH, while suppressed values are consistent with ADH.
Sensitivity/Specificity. The most common problem with the cACTH assay is poor sensitivity. The largest study of cACTH in dogs with HAC used a 2-site solid-phase chemiluminescent immunometric assay (Immulite 2000 Immunoassay System for ACTH; healthcare.siemens.com) and showed excellent discrimination between PDH and AT.
The likelihood of falsely low ACTH values in dogs with PDH is increased by:• Intra-assay and interassay variability (increased at
lower cACTH concentrations)• Pulsatile ACTH secretion• Inappropriate sample handling allowing ACTH
degradation.23-28
Dexamethasone SuppressionDexamethasone administration in:• Normal dogs: Causes rapid and prolonged
suppression of cortisol secretion• Patients with an AT: At any dosage does not
suppress cortisol secretion• Dogs with PDH:2,29
Synthetic polypeptides, such as Cortrosyn (cosyntropin) or Synacthen (tetracosactrin), contain the biologically active first 24 amino acids of ACTH; however, their potencies have not been compared.
In several studies, after administration of cosyntropin (5 mcg/kg or 250 mcg/dog IV or IM), peak cortisol concentrations occurred at 60 to 90 minutes. After administration of 5 mcg/kg IV, no difference was detected between 60- and 90-minute cortisol concentrations.13-16
Cosyntropin can be reconstituted, divided into aliquots in plastic syringes, and frozen at -20°C for 6 months.19 Whether tetracosactrin can be frozen has not been investigated; according to the manufacturer, store it at temperatures from 2°C to 8°C.
Compounded ACTH products have been evaluated in healthy dogs. Sixty minutes after administration, cortisol concentrations were similar among 4 compounded products (2.2 U/kg IM) and cosyntropin (5 mcg/kg IV). However, at later times, cortisol concentrations varied considerably with the compounded products.13
Synthetic Versus Compounded ACTH

tvpjournal.com | January/February 2016 | Today’s VeTerinary PracTice
canine PiTuiTary dePendenT HyPeradrenocorTicism series Peer reviewed
39
» Does not appropriately suppress ACTH secretion (therefore does not suppress cortisol) when a low dose (0.01 mg/kg) is administered
» In 75% of dogs with PDH, ACTH and cortisol concentrations decrease when a high dose (0.1 mg/kg) is administered
» In 25% of dogs with PDH, suppression of ACTH and cortisol does not occur even after administration of higher dosages; in these patients, a large pituitary tumor or a tumor developing from the pars intermedia is more likely.
A description of how to perform dexamethasone suppression tests is outlined in Table 4. The largest study evaluating both suppression tests—LDDS and high-dose dexamethasone suppression (HDDS)—included dogs with PDH (n = 181) and ATs (n = 35).2 With LDDS, criteria for identifying dogs with PDH included: • 4-hour post LDDS cortisol concentrations below
laboratory cutoff or < 50% of basal cortisol concentration
• 8-hour post LDDS cortisol concentrations < 50% of the basal cortisol concentration and greater than the laboratory cutoff.With HDDS, criteria for cortisol suppression were
a 4- and/or 8-hour cortisol concentration below the laboratory cutoff or < 50% of the basal cortisol concentration.
Approximately 75% of dogs with PDH met at least one criterion for suppression on either LDDS (88%) or HDDS (12%).2
Dexamethasone resistance (ie, no criteria were met) occurred in all dogs with AT and the remainder (25%) of the dogs with PDH.2 In another study of 41 dogs with ATs, 28 LDDS and 30 HDDS tests were performed, with no suppression seen on any test.2,30
In dogs demonstrating lack of suppression with LDDS, use of endogenous ACTH rather than HDDS is recommended to differentiate PDH from ADH. Since suppression in response to dexamethasone supports a diagnosis of PDH, a dog with dexamethasone resistance can have either AT or PDH.
Table 4. Diagnostic Tests That Differentiate Between PDH and ADHTEST COMPONENTS PROCEDURES RESULTSLow-Dose Dexamethasone Suppressiona
Dexamethasone sodium phosphate or polyethylene glycol: 0.01–0.015 mg/kg IVb
Obtain blood samples:1. Before administration2. 4 H after administration3. 8 H after administration
• With LDDS, suppression to < 50% baseline in a dog with HAC confirms PDH.
• If no suppression with LDDS, cACTH measurement or abdominal ultrasound is recommended.
• With LDDS or HDDS, lack of suppression does not confirm AT (approximately 25% of dogs with PDH fail to suppress).
High-Dose Dexamethasone Suppressiona
Dexamethasone sodium phosphate: 0.1 mg/kg IVc
Endogenous ACTH cACTH 1. Collect blood into chilled, silicone-coated glass or plastic EDTA tubes.
2. Centrifuge within 15 min (ideally cooled centrifuge).
3. Transfer plasma to plastic tubes and freeze immediately; samples must stay frozen until analysis.d
Normal or elevated concentrations are consistent with PDH, while suppressed values are consistent with AT.
a. LDDS and HDDS results cannot be considered 100% absolute; when imaging and endocrine test results conflict, the latter should be given preference.b. Calculate dose using parent compound.c. For HDDS, avoid the free alcohol form.d. Addition of the protease inhibitor aprotinin prevents ACTH degradation by plasma proteases and greatly facilitates sample handling. Check with your laboratory
regarding suitability because, with some assays (ie, Immulite), aprotinin introduces an artifactual decrease in results.
Evaluation of the pituitary-adrenal axis is indicated in the following circumstances: ` Patients with clinical signs and laboratory findings consistent with PDH and in which nonadrenal illness has been ruled out or is well controlled.
` Patients in which an adrenal/pituitary mass or bilateral adrenal hyperplasia has been discovered in conjunction with compatible clinical signs.
` Patients with an incidentally discovered adrenal mass, with adrenalectomy being considered.
` Diabetic dogs with insulin resistance.
Evaluation of the Pituitary–Adrenal Axis

Today’s VeTerinary PracTice | January/February 2016 | tvpjournal.com
canine PiTuiTary dePendenT HyPeradrenocorTicism series Peer reviewed
40
Dexamethasone Suppression with UCCRDecreased blood cortisol concentration after dexamethasone administration is reflected in decreased UCCR.
After the patient’s owner/handler collects a morning urine sample on 2 consecutive days, 3 doses of dexamethasone (0.1 mg/kg PO) are administered at 6 to 8 hour intervals, with a third urine sample collected the next morning.
Decrease in the third UCCR to < 50% of the mean cortisol basal values is consistent with PDH. Lack of suppression does not confirm AT.
In 160 dogs with HAC (49 with ATs, 111 with PDH), the UCCR in 72% of dogs with PDH suppressed to < 50% of the basal UCCR, while the other 28% of those with PDH were dexamethasone-resistant. In dogs with ATs, maximum suppression was 44% of the baseline sample.31
DIFFERENTIATING PDH FROM ADH: IMAGINGWhile imaging can be very helpful in differentiating PDH from ADH, it cannot be used to establish a diagnosis of HAC. Moreover, finding normal adrenal glands on imaging studies does not rule out HAC.
RadiographyImaging results may include:• Abdominal distension • Good contrast due to abdominal fat deposition• Hepatomegaly• Bladder distension• Mineralization of bronchi and pulmonary
interstitium, and of dermal and subcutaneous tissues in areas predisposed to calcinosis cutis. A small liver makes HAC unlikely. An AT may
be visualized either due to mass effect or tumor calcification.32,33
Adrenal Gland ImagingAdrenal gland width is the most informative parameter identified on ultrasonography (Figure 1). However, the following may affect correct measurement:• Long axis of adrenal gland often is misaligned with
either the medial or dorsal plane of the body• Cross-sectional images may lead to oblique views
and miscalculation of glandular dimensions• Breed and body size differences• Macronodular hyperplasia (a rare form of PDH)
and some ATs can be difficult to differentiate. Test Results. In dogs with PDH, ultrasonography
reveals normal sized or enlarged adrenal glands that
are typically symmetrical; however, mild asymmetry may occur. In dogs with ATs, ultrasonography reveals moderate asymmetry, contralateral adrenocortical atrophy (adrenal width < 4–5 mm), destruction of normal tissue architecture, or some combination of these findings.34,35
Ultrasonography can also estimate AT size and possibly vascular or local soft tissue invasion. Although most ATs are unilateral, bilateral tumors may occur and in these patients, endogenous ACTH concentrations should be determined.
Metastasis. When an AT has been confirmed, certain thoracic and ultrasonographic findings suggest malignancy, including: • Adrenal gland width > 4 cm• Invasion into the vena cava or adjacent tissues.
However, computed tomography (CT) (Figure 2) and magnetic resonance imaging (MRI) are more sensitive techniques to identify vascular invasion and detect metastases.36
Adrenalectomy should not be performed without confirming the presence of an AT (and atrophy of contralateral adrenal gland) by abdominal ultrasonography (Figure 3), CT, MRI, or some
FIGURE 1. Ultrasound image of adrenal adenoma.
FIGURE 2. CT image of large right adrenal adenoma between the right kidney and caudal vena cava.

tvpjournal.com | January/February 2016 | Today’s VeTerinary PracTice
canine PiTuiTary dePendenT HyPeradrenocorTicism series Peer reviewed
41
combination of these. Metastasis can be confirmed by ultrasound-guided biopsy, but differentiating benign from malignant AT often is difficult, even with histopathologic examination.
Pituitary ImagingPituitary imaging provides valuable information regarding treatment options and prognosis.37 Pituitary lesions range from microscopic nests of hyperplastic cells to large tumors. Absence of neurologic abnormalities does not exclude pituitary macrotumors (ie, tumors that are > 1 cm in diameter, extend above the sella turcica, or have a pituitary:brain ratio of > 0.31).
Indications. Pituitary imaging should be considered for all dogs at time of PDH diagnosis, especially if hypophysectomy or radiation therapy is being considered. If clinical features suggest a pituitary macrotumor, confirmation requires imaging; clinical signs include:• Disorientation and aimless wandering• Severe polyuria/polydipsia• Lethargy• Hyporexia to anorexia• Visual impairment• Seizures (in some patients).
Test Results. Because pituitary lesions may be quite small, contrast-enhanced CT and MRI (Figure 4 and Figures 5–6, page 42) may identify normal sized pituitary glands in dogs with PDH. However, dynamic contrast-enhanced CT takes advantage of the pituitary gland’s blood supply: • The posterior pituitary gland’s blood supply is
direct (arterial)• The anterior pituitary gland’s blood supply is
mainly indirect via the pituitary portal system. In dogs with normal pituitary glands, after IV
administration of contrast medium, the posterior pituitary gland can be identified first—this phase is called the “pituitary flush.” Its absence indicates atrophy of the posterior pituitary gland due to compression by a pituitary tumor. Displacement or distortion of the flush can be used to identify and localize anterior pituitary microtumors.
Dorsal displacement and decreased signal intensity of the posterior lobe on T1-weighted MRI indicates the presence of a microtumor.38,39
IN SUMMARyDiagnosis of PDH requires incorporating information from the history, physical examination, and routine laboratory tests. Specific endocrine tests
FIGURE 3. Ultrasound (A) and surgical view (B) of adrenal adenoma.
A
BFIGURE 4. Axial (A) and sagittal (B) T1 post contrast MRI images from a dog with PDH and large pituitary macroadenoma.
B
A

TODAY’S VETERINARY PRACTICE | January/February 2016 | tvpjournal.com
CANINE PITUITARY DEPENDENT HYPERADRENOCORTICISM SERIES Peer Reviewed
42
and imaging modalities are available to diagnose HAC and distinguish between the various causes of hypercortisolism. No single test is perfect and, if the initial screening test is negative and high clinical suspicion of HAC exists, additional tests should be performed. Endocrine evaluation of patients with HAC and nonadrenal illness can be diffi cult, and it is important to eliminate or manage the concurrent illness before undertaking adrenal function tests.
ACTH = adrenocorticotropic hormone; ADH = adrenal dependent hyperadrenocorticism; AT = adrenocortical tumor; cACTH = canine ACTH; CT = computed tomography; HAC = hyperadrenocorticism; HDDS = high-dose dexamethasone suppression; LDDS = low-dose
dexamethasone suppression; MRI = magnetic resonance imaging; PA = pituitary adenoma; PDH = pituitary dependent hyperadrenocorticism; UCCR = urine cortisol to creatinine ratio
References1. Behrend EN, Kooistra HS, Nelson R, et al. Diagnosis of
spontaneous canine hyperadrenocorticism: 2012 ACVIM consensus statement (small animal). J Vet Intern Med 2013; 27:1292-1304.
2. Feldman EC, Feldman MS, Nelson RW. Use of low and high-dose dexamethasone tests for distinguishing pituitary dependent from adrenal tumor hyperadrenocorticism in dogs. JAVMA 1996; 9:772-775.
3. Feldman EC. Comparison of ACTH response and dexamethasone suppression as screening tests in canine hyperadrenocorticism. JAVMA 1981; 182:506-510.
4. Meijer JC, de Bruijne JJ, Rijnberk A, Croughs RJM. Biochemical characterization of pituitary-dependent hyperadrenocorticism in the dog. J Endocrinol 1978; 77:111-118.
5. Meijer JC, Lubberink AAME, Rijnberk A, Croughs JM. Adrenocortical function tests in dogs with hyperfunctioning adrenocortical tumors. J Endocrinol 1979; 80:315-319.
6. Mack RE, Feldman EC. Comparison of two low-dose dexamethasone suppression protocols as screening and discrimination tests in dogs with hyperadrenocorticism. JAVMA 1990; 197:1603-1606.
7. May ER, Frank LA, Hnilica KA, Lane IF. Effects of a mock ultrasonographic procedure on cortisol concentrations during low-dose dexamethasone suppression testing in clinically normal adult dogs. Am J Vet Res 2004; 65:267-270.
8. Rijnberk A, van Wees A, Mol JA. Assessment of two tests for the diagnosis of canine hyperadrenocorticism. Vet Rec 1988; 122:178-180.
9. van Liew CH, Greco DS, Salman MD. Comparison of results of adrenocorticotropic hormone stimulation and low-dose dexamethasone suppression test with necropsy fi ndings in dogs: 81 cases (1985-1995). JAVMA 1997; 211:322-325.
DAVID BRUYETTEDavid Bruyette, DVM, Diplomate ACVIM, is the medical director at VCA West Los Angeles Animal Hospital and President and CEO of Veterinary Diagnostic Investigation and Consultation. He was an assistant professor and head of internal medicine at Kansas State University and director of its Analytical Chemistry Laboratory. Dr. Bruyette received his DVM from University of Missouri and completed an internship at Purdue University and residency in internal medicine at University of California–Davis. He then became a staff internist at West Los Angeles Veterinary Medical Group and member of the Department of Comparative Medicine at Stanford University.
FIGURE 5. Axial (A) and sagittal (B) T1 post contrast MRI images from a dog with PDH prior to surgery. Note the pituitary (arrows).
A
B
FIGURE 6. Axial (A) and sagittal (B) T1 post contrast MRI images from dog in Figure 5 after surgery.
B
A

Today’s VeTerinary PracTice | January/February 2016 | tvpjournal.com
canine PiTuiTary dePendenT HyPeradrenocorTicism series Peer reviewed
44
10. Foster SF, Church DB, Watson ADJ. Effect of phenobarbitone on the low-dose dexamethasone suppression test and the urinary corticoid:creatinine ratio in dogs. Aust Vet J 2000; 78:19-23.
11. Monroe WE, Panciera DL, Zimmerman KL. Concentrations of noncortisol adrenal steroids in response to ACTH in dogs with adrenal-dependent hyperadrenocorticism, pituitary-dependent hyperadrenocorticism, and nonadrenal illness. J Vet Intern Med 2012; 26:945-952.
12. Cohen TA, Feldman EC. Comparison of IV and IM formulations of synthetic ACTH for ACTH stimulation tests in healthy dogs. J Vet Intern Med 2012; 26:412-414.
13. Kemppainen RJ, Behrend EN, Busch KA. Use of compounded adrenocorticotropic hormone (ACTH) for adrenal function testing in dogs. JAAHA 2005; 41:368-372.
14. Behrend EN, Kemppainen RJ, Bruyette DS. Intramuscular administration of a low dose of ACTH for ACTH stimulation testing in dogs. JAVMA 2006; 229:528-530.
15. Kerl ME, Peterson ME, Wallace MS, et al. Evaluation of a low-dose synthetic adrenocorticotropic hormone stimulation test in clinically normal dogs and dogs with naturally developing hyperadrenocorticism. JAVMA 1999; 214:1497-1501.
16. Frank LA, DeNovo RC, Kraje AC, Oliver J. Cortisol concentrations following stimulation of healthy and adrenopathic dogs with two doses of tetracosactrin. J Small Anim Pract 2000; 41:308-311.
17. Martin LG, Behrend EN, Mealey KL, et al. Effect of low doses of cosyntropin on serum cortisol concentrations in clinically normal dogs. Am J Vet Res 2007; 68:555-560.
18. Ginel PJ, Sileo PJ, Blanco B, et al. Evaluation of serum concentrations of cortisol and sex hormones of adrenal gland origin after stimulation with two synthetic ACTH preparations in clinically normal dogs. Am J Vet Res 2012; 73:237-241.
19. Frank LA, Oliver J. Comparison of serum cortisol concentrations in clinically normal dogs after administration of freshly reconsti-tuted versus reconstituted and stored frozen cosyntropin. JAVMA 1998; 212:1569-1571.
20. Stolp R, Rijnberk A, Meijer JC, Croughs JM. Urinary corticoids in the diagnosis of canine hyperadrenocorticism. Res Vet Sci 1983; 34:141-144.
21. Jensen AL, Iverson L, Koch J, et al. Evaluation of the urinary cortisol:creatinine ratio in the diagnosis of hyperadrenocorticism in dogs. J Small Anim Pract 1997; 38:99-102.
22. Rijnberk A, van Wees A, Mol JA. Assessment of two tests for the diagnosis of canine hyper-adrenocorticism. Vet Rec 1988; 122:178-180.
23. Castillo V, Blatter C, Gomez NV, et al. Diurnal ACTH and plasma cortisol variations in healthy dogs and in those with pituitary-de-pendent Cushing’s syndrome before and after treatment with retinoic acid. Res Vet Sci 2009; 86:223-229.
24. Hanson JM, Kooistra HS, Mol JA, et al. Plasma profiles of adenocorticotropic hormone, cortisol, alpha-melanocyte-stimulating hormone, and growth hormone in dogs with pituitary-dependent hyperadrenocorticism before and after hypophysectomy. J Endocrinol 2006; 190:601-609.
25. Kemppainen RJ, Clark TP, Peterson ME. Preservative effect of aprotinin on canine plasma immunoreactive adrenocorticotropin
concentrations. Domest Anim Endocrinol 1993; 11:355-362.
26. Rodriguez Pineiro MI, Benchekroun G, de Fornel-Thibaud P, et al. Accuracy of an adrenocorticotropic hormone (ACTH) immunoluminometric assay for differentiating ACTH-dependent from ACTH-independent hyperadrenocorticism in dogs. J Vet Intern Med 2009; 23:850-855.
27. Scott-Moncrieff JCR, Koshko M, Brown JA, et al. Validation of chemiluminescent enzyme immunometric assay for plasma adrenocorticotropic hormone in the dog. Vet Clin Pathol 2003; 32:180-187.
28. Zeugswetter F, Pagitz M, Hittmair K, Schwendenwein I. Diagnostic efficacy of plasma ACTH-measurement by a chemiluminometric assay in canine hyperadrenocorticism. Schweiz Arch Tierheilkd 2011; 153:111-116.
29. Bosje JT, Rijnberk A, Mol JA, et al. Plasma concentrations of ACTH precursors correlate with pituitary size and resistance to dexamethasone in dogs with pituitary-dependent hyperadrenocorticism. Domest Anim Endocrinol 2002; 22:201-210.
30. Reusch CE, Feldman EC. Canine hyperadrenocorticism due to adrenocortical neoplasia. Pretreatment evaluation of 41 dogs. J Vet Int Med 1995; 5:3-10.
31. Galac S, Buijtels JJCWM, Kooistra HS. Urinary corticoid:creatinine ratios in dogs with pituitary-dependent hypercortisolism during trilostane treatment. J Vet Intern Med 2009; 23:1214-1219.
32. Berry CR, Hawkins EC, Hurley KJ, Monce K. Frequency of pulmonary mineralization and hypoxemia in 21 dogs with pituitary-dependent hyperadrenocorticism. J Vet Intern Med 2000; 14:151-156.
33. Schwarz T, Stork CK, Mellor D, Sullivan M. Osteopenia and other radiographic signs in canine hyperadrenocorticism. J Small Anim Pract 2000; 41:491-495.
34. Rodriguez Pineiro MI, de Fornel-Thibaud P, Benchekroun G, et al. Use of computed tomography adrenal gland measurement for differentiating ACTH dependence from ACTH independence in 64 dogs with hyperadenocorticism. J Vet Intern Med 2011; 25:1066-1074.
35. Benchekroun G. Ultrasonography crite-ria for differentiating ACTH dependency from ACTH independency in 47 dogs with hyperadrenocorticism and equivocal adrenal asymmetry. J Vet Intern Med 2010; 24:1077-1085.
36. Schultz RM, Wisner ER, Johnson EG, MacLeod JS. Contrast-enhanced computed tomography as a preoperative indicator of vascular invasion from adrenal masses in dogs. Vet Radiol Ultrasound 2009; 50:625-629.
37. Auriemma E, Barthez PY, van der Vlugt-Meijer RH, et al. Computed tomography and low-magnetic resonance imaging of the pituitary gland in dogs with pituitary-dependent hyperadrenocorticism: 11 cases (2001-2003). JAVMA 2009; 235:409-414.
38. van der Vlugt-Meijer RH, Meij BP, van den Ingh TSGAM, et al. Dynamic computed tomography of the pituitary gland in dogs with pituitary-dependent hyperadrenocorticism. J Vet Intern Med 2003; 17:773-780.
39. Taoda T, Hara Y, Masuda H, et al. Magnetic resonance imaging assessment of pituitary posterior lobe displacement in dogs with pituitary-dependent hyperadrenocorticism. J Vet Med Sci 2011; 73:725-731.
TODAY’S VETERINARY PRACTICE | January/February 2016
CANINE PITUITARY DEPENDENT HYPERADRENOCORTICISM SERIES
44


















