Cancer Program Statistical Report, 2006 - Cleveland Clinic
6
Cleveland Clinic, located in Weston and West Palm Beach, Florida, is a not-for-profit, multi-specialty, academic medical center that integrates clinical and hospital care with research and education. Cleveland Clinic has approximately 150 physicians with expertise in 35 specialties. The medical campus is fully integrated and includes diagnostic centers, outpatient surgery, and a 24- hour emergency department located in the state-of-the-art hospital, which was named one of the nation’s 100 Top Hospitals® in cardiovascular care by Thomson Healthcare in 2007. Cleveland Clinic was 1 out of only 4 hospitals in the nation to be recognized by the American Heart Association for the highest level of performance in all three categories of the Get with the Guidelines program: Coronary Artery Disease, Heart Failure & Stroke. Cleveland Clinic in Florida is an integral part of Cleveland Clinic in Ohio, where providing outstanding patient care is based upon the principles of cooperation, compassion and innovation. Physicians at Cleveland Clinic are experts in the treatment of complex conditions that are difficult to diagnose. For more information about Cleveland Clinic in Florida, please call 954-659-5000 or visit clevelandclinicflorida.org 06/08 About Cleveland Clinic in Florida 2950 Cleveland Clinic Blvd. Weston, Florida 33331 Our Mission is to provide better care of the sick, investigation of their problems, and further education of those who serve. Cancer Program Statistical Report
Transcript of Cancer Program Statistical Report, 2006 - Cleveland Clinic

Cleveland C
linic, located in Weston and W
est Palm B
each,Florida,
is a
not-for-profit, m
ulti-specialty, academ
icm
edical center that integrates clinical and hospital carew
ith research
and education.
Cleveland
Clinic
hasapproxim
ately 1
50
physicians
with
expertise in
35
specialties. The medical cam
pus is fully integrated andincludes diagnostic centers, outpatient surgery, and a 2
4-
hour emergency departm
ent located in the state-of-the-arthospital, w
hich was nam
ed one of the nation’s 10
0 Top
Hospitals®
in cardiovascular care by Thomson H
ealthcarein 2
00
7. C
leveland Clinic w
as 1 out of only 4
hospitals inthe
nation to
be recognized
by the
Am
erican H
eartA
ssociation for the highest level of performance in all three
categories of
the G
et w
ith the
Guidelines
program:
Coronary A
rtery Disease, H
eart Failure & Stroke. C
levelandC
linic in Florida is an integral part of Cleveland C
linic inO
hio, where providing outstanding patient care is based
upon the
principles of
cooperation, com
passion and
innovation. Physicians at C
leveland Clinic are experts in
the treatment of com
plex conditions that are difficult todiagnose.
For m
ore inform
ation about
Cleveland Clinic
in Florida,
please call 954-659-5000 or visit clevelandclinicflorida.org
06/0
8
About C
leveland Clinic in Florida
2950 C
leveland Clinic B
lvd.W
eston, Florida 33331
Our Mission is to provide better care of the sick, investigation of their problems, and further education of those who serve.
Cancer ProgramStatistical Report

I’m proud to present the third annual Cancer Program StatisticalReport reflecting 2006 data and activities at Cleveland Clinic inFlorida. The Program has grown since our first report: 449 cancerpatients were treated in our inaugural year, 497 in 2005 and 571in 2006. We continue to add physicians and surgeons to ourprofessional staff, who specialize in oncology and bring new andcurrent expertise to the care of our patients. Our Cancer Program continues its commitment to providecomprehensive, quality, multidisciplinary, and patient orientedcare to patients diagnosed with cancer. The Program providesclinical services adept in the prevention, early diagnosis,pretreatment evaluation, staging, optimal treatment,rehabilitation, and surveillance for recurrent disease, support
services, and end-of-life care for our patients. Patients referred toCleveland Clinic for diagnosis, staging, and treatment of their cancers receive the advantagesof inpatient areas dedicated only for the care of cancer patients, an outpatient chemotherapyinfusion unit, and a Cancer Prevention Clinic that offers genetic testing, family phenotyping,and counseling.
This report will update you on the activity of our cancer services, weekly cancer conferences,quality improvement program, cancer registry and database, community outreach programs,patient education and support groups, and clinical trials.
The Cancer Committee has chosen to review rectal cancer in this year’s Report. In 2006, rectalcancer was the second most common cancer treated at our institution. It is also an exampleof a cancer whose management is optimized by multi-modality therapy: chemotherapy,radiation therapy, and surgery all play a major role in determining the extent of the initialoperation, local control, and patient survival. In 2006, only 36% of patients with rectal cancertreated at our institution had surgery alone to treat their tumor, the remainder receivedadjuvant or neo-adjuvant treatment. Subsequently, 76% of the operations performed by thesurgeons in our Colorectal Surgery Department for rectal cancer spared the anal sphinctersand preserved fecal continence.
Once again, it is my pleasure to present this Report for your review of the 2006 activities of ourCancer Program. The Cancer committee is proud of the strides that we have made for ourpatients ensuring that they continue to receive the best and most personalized care possible.
Mark E. Sesto, MD, FACSCancer Committee Chairman
2
Cancer Committee Chairman’s Report
Colorectal cancer arises from gene mutations typically caused by dietary factors and aging. Approximately 10% ofcolorectal cancers are inherited from a specific gene mutation. Inherited colorectal cancer is suspected whenmultiple generations of a family are affected. The manifestations become clinically evident at a younger age, andtumors and cancers may also occur in other organs. Through investigation of the family tree, inherited colorectalcancer can be documented. The inherited colorectal cancer syndromes include Hereditary Non-polyposis ColorectalCancer (HNPCC) and Familial Adenomatous Polyposis (FAP). A significant breakthrough in the diagnosis of HNPCCand FAP was made with the discovery of the genes responsible for these cancers and a laboratory assay developed totest for them. Colaris is a genetic test for HNPCC and the genes tested for are the MLH1 and MSH2 genes. Colaris APis a genetic test for adenomatous polyposis syndromes. Patients with the mutation are at high risk for developingcolon cancer as well as other cancers of the gastrointestinal tract (stomach, small intestine, pancreas), urinarysystem (kidney, ureter), and female reproductive organs (uterus). APC is the gene tested for FAP. All patients with FAPwill develop colorectal cancer usually by the age of 40. The Hereditary Cancer Prevention Clinic was created atCleveland Clinic in 2004 to evaluate, counsel, and treat all patients deemed high risk for developing cancer and theirfamilies. Genetic testing is completed when warranted and helps to make an early diagnosis before the diseaseoccurs. This enables our physicians to recommend appropriate chemoprevention, surveillance, and treatmentstrategies including prophylactic surgery. All of these measures translate into substantial risk reduction. In 2006, 13patients evaluated in the Hereditary Cancer Prevention Clinic underwent genetic testing for inherited colorectalcancer, the majority of which were for HPNCC. One was positive for the mutation, 9 were negative, and 3 wereinconclusive or incomplete for various reasons. Detailed family histories were obtained and the test resultssignificantly altered treatment selection. The patient with the positive result chose a restorative proctocolectomy bywhich the entire organ at risk (colon and rectum) was removed and not just the segment containing the tumor.Patient outcomes are then followed longitudinally.
Mark E. Sesto, MD, FACSCancer Committee Chairman
10
Rectal Cancer 2006 Data Continued
References:
1. National Cancer Institute: http://www.cancer.gov/
2. The Standards Practice Task Force, The American Society of Colon and Rectal Surgeons. Practice parameters for thesurveillance and follow up of patients with colon and rectal cancer. Dis Colon Rectum 2004 Jun; 47 (6):807-17.
3. Stewart DB, Dietz DW. Total Mesorectal Excision: What are we doing? Clin Colon Rectal Surg 2007; 20: 190-202.
4. Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl JMed 2004; 351: 1731-1740.
5. Cleveland Clinic: http://www.clevelandclinic.org/registries/inherited/
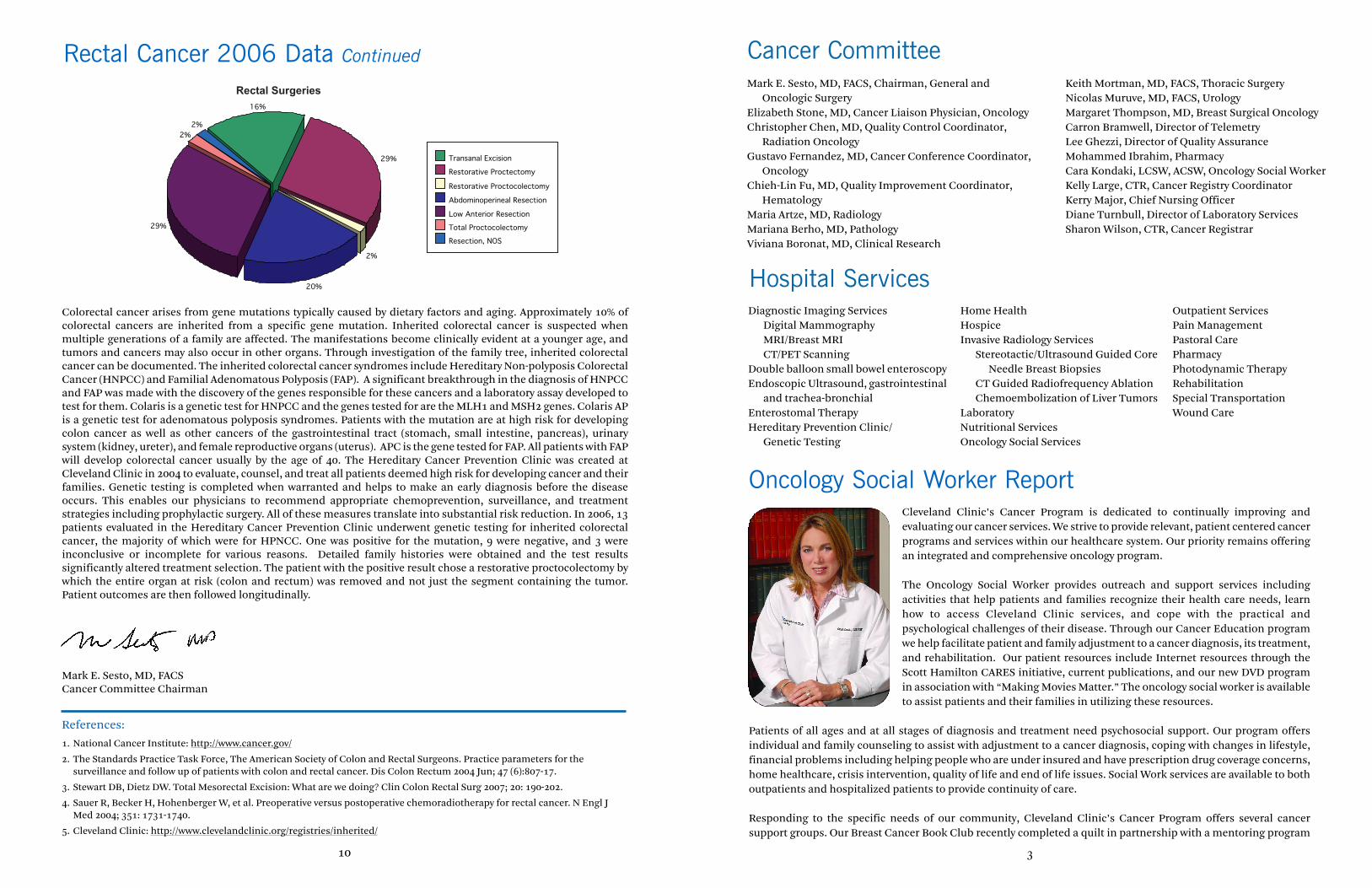
Rectal Surgeries
Transanal Excision
Restorative Proctectomy
Restorative Proctocolectomy
Abdominoperineal Resection
Low Anterior Resection
Total Proctocolectomy
Resection, NOS
29%
16%
2%2%
29%
20%
2%
Mark E. Sesto, MD, FACS, Chairman, General and Oncologic Surgery
Elizabeth Stone, MD, Cancer Liaison Physician, OncologyChristopher Chen, MD, Quality Control Coordinator,
Radiation OncologyGustavo Fernandez, MD, Cancer Conference Coordinator,
OncologyChieh-Lin Fu, MD, Quality Improvement Coordinator,
HematologyMaria Artze, MD, Radiology Mariana Berho, MD, PathologyViviana Boronat, MD, Clinical Research
Keith Mortman, MD, FACS, Thoracic SurgeryNicolas Muruve, MD, FACS, UrologyMargaret Thompson, MD, Breast Surgical OncologyCarron Bramwell, Director of TelemetryLee Ghezzi, Director of Quality AssuranceMohammed Ibrahim, PharmacyCara Kondaki, LCSW, ACSW, Oncology Social Worker Kelly Large, CTR, Cancer Registry CoordinatorKerry Major, Chief Nursing OfficerDiane Turnbull, Director of Laboratory ServicesSharon Wilson, CTR, Cancer Registrar
3
Cancer Committee
Cleveland Clinic’s Cancer Program is dedicated to continually improving andevaluating our cancer services. We strive to provide relevant, patient centered cancerprograms and services within our healthcare system. Our priority remains offeringan integrated and comprehensive oncology program.
The Oncology Social Worker provides outreach and support services includingactivities that help patients and families recognize their health care needs, learnhow to access Cleveland Clinic services, and cope with the practical andpsychological challenges of their disease. Through our Cancer Education programwe help facilitate patient and family adjustment to a cancer diagnosis, its treatment,and rehabilitation. Our patient resources include Internet resources through theScott Hamilton CARES initiative, current publications, and our new DVD programin association with “Making Movies Matter.” The oncology social worker is availableto assist patients and their families in utilizing these resources.
Patients of all ages and at all stages of diagnosis and treatment need psychosocial support. Our program offersindividual and family counseling to assist with adjustment to a cancer diagnosis, coping with changes in lifestyle,financial problems including helping people who are under insured and have prescription drug coverage concerns,home healthcare, crisis intervention, quality of life and end of life issues. Social Work services are available to bothoutpatients and hospitalized patients to provide continuity of care.
Responding to the specific needs of our community, Cleveland Clinic’s Cancer Program offers several cancersupport groups. Our Breast Cancer Book Club recently completed a quilt in partnership with a mentoring program
Oncology Social Worker Report
Diagnostic Imaging ServicesDigital MammographyMRI/Breast MRICT/PET Scanning
Double balloon small bowel enteroscopyEndoscopic Ultrasound, gastrointestinal
and trachea-bronchialEnterostomal TherapyHereditary Prevention Clinic/
Genetic Testing
Home HealthHospiceInvasive Radiology Services
Stereotactic/Ultrasound Guided Core Needle Breast Biopsies
CT Guided Radiofrequency AblationChemoembolization of Liver Tumors
LaboratoryNutritional ServicesOncology Social Services
Outpatient ServicesPain ManagementPastoral CarePharmacyPhotodynamic Therapy RehabilitationSpecial TransportationWound Care
Hospital Services

Particularly because of the typical advanced stage at diagnosis, rectal cancer is best managed in a multidisciplinary,integrated, and patient-centered format. Recurrence rates, survival, functional results, and patient satisfaction areoptimized. At Cleveland Clinic in Florida, treatment is personalized and the patient’s age, co-morbid illnesses,clinical stage of disease, and personal expectations are considered. Treatment includes surgery, chemotherapy,radiotherapy, or multi-modality therapy. The use of multi-modality therapy has demonstrated improved outcomesin the management of patients with stage 2 or greater rectal cancers. Chemotherapy, radiotherapy, or both whenused with surgery have been demonstrated to improve resectability, (“down-stage” the tumor), local recurrence rate,and survival. The treatment can be given before surgery (neo-adjuvant), after surgery (adjuvant), or both. Theadvantage of neo-adjuvant therapy is the potential to improve resectability, permit a lesser, more functional surgicalresection, and treat the “whole patient” without delay. Subsequent surgery in the irradiated pelvis has not beendemonstrated to increase complications.
Once again, because of the advanced stage at diagnosis, the majority of our patients with rectal cancer receivedmulti-modality therapy. Fifty-six percent of patients received neo-adjuvant treatment, adjuvant treatment, or both.Forty-three percent of those patients received only neo-adjuvant treatment, and 48% of those received both. Onlythirty-six percent of patients received surgery only. Survival after treatment for Stage 1 rectal cancer is 90-95 %. Withmulti-modality therapy, five-year survival for Stage 2 and 3 rectal cancers is 75%.
9
Rectal Cancer 2006 Data Continued
Rectal Cancer Treatment Combinations
Surgery only
Neoadjuvant Chemo/RT only
Both neoadjuvant and adjuvant Chemo withneoadjuvant RTNo surgery
Adjuvant Chemo/RT only
Both neoadjuvant and adjuvant Chemo/RT
Adjuvant Chemo only
24%
24%
36%
3%3%
5%5%
Rectal Cancer 2006 by Stage
0I
II
III
IV
Unknown
I30%
02%
Unknown17%
II23%
III20%
IV8%
There are three major objectives of the surgical treatment of rectal cancer: Perform an adequate resection of thetumor including its lymphadenic drainage basin. This is called a total meso-rectal excision. When possible, performa sphincter mechanism sparing resection, permitting preservation of fecal continence. And, when possible,perform the least invasive procedure utilizing laparoscopic techniques. Seventy-six percent of the surgicalprocedures performed spared the sphincter mechanism and maintained fecal continence, (transanal excision,restorative proctectomy, restorative proctocolectomy, low anterior resection). In only 22%, this could not beaccomplished, and a permanent stoma had to be constructed (abdominoperineal resection, total proctocolectomy).Excluding local, transanal excisions, 20% (10/49) of the surgeries were performed laparoscopically.
2006 marked my 3rd year as the Cancer Liaison Physician at Cleveland Clinic inFlorida. Our Community Outreach programs continue to grow in number andmaturity. Cara Kondaki, our Licensed Clinical Oncology Social Worker has reviewedmany of these programs in her report. I would like to highlight a few others that wewere very proud to offer to our cancer patients and their families.
Our Annual Community Health Fair in January included PSA screenings.Participants were informed of normal results and given appointments in theDepartment of Urology for elevated values. In March, we held another earlydetection and prevention program performing colorectal cancer risk assessmentson participants. Participants with elevated risk assessments were givenappointments in the Department of Gastroenterology. In addition, our staff hosteda variety of lectures on assorted cancers including breast and colon. Once again, ourhospital participated in the Relay for Life and I again had the honor of sashing
cancer survivors.
In May, we initiated our well-attended Breast Cancer Book Club. We also started offering yoga classes to our cancerpatients as an adjunct to our services. Cara has been instrumental in creating and organizing these groups and hasformally shared her ideas with other social workers.
In October, Breast Cancer Prevention Month, our hospital participated in Making Strides against Breast CancerWalk and the Department of Hematology and Oncology hosted a breast cancer early detection table that focused oneducation on self-breast exams and breast cancer screening.
Elizabeth Stone, MDCancer Liaison Physician
4
Cancer Liaison Physician Report
Oncology Social Worker Report Continued
through Girl Scouts of America and participated in the annual “Making Strides against Breast Cancer” walk. TheMultiple Myeloma Support Group continues to partner with the International Myeloma Foundation for educationand disease management. We recently added the “Man to Man prostate Cancer Support Group” in affiliation withthe American Cancer Society. We are also pleased to offer a Patient Mentor Program through the 4th Angel MentorProgram available through the Scott Hamilton Cares initiative. Our support groups continue to strive to offereducation about cancer, treatment options, and networking opportunities in the community.
The Oncology social worker can serve as a link between you and the healthcare system, and the community. Our goalis to provide a variety of services to aide in the long-term adjustment to a cancer diagnosis.
Cara S. Kondaki, LCSW, ACSWLicensed Clinical Social Worker-Oncology

Colorectal cancer is the third most common malignancy and the third most common cause of cancer related deathsin the United States. In 2007, there will be approximately 40,000 new cases of rectal cancer diagnosed and 50,000deaths caused by colorectal cancer. In 2006, 111 cases of colorectal cancer were treated at the Cleveland Clinic inFlorida. There were 59 cases of rectal cancer representing 53% of all colorectal cancer cases. The high percentage isresult of the referral pattern to our Department of Colorectal Surgery whose four surgeons have over 60 years ofclinical experience in managing complex diseases related to their specialty. Colorectal cancers (111 cases) and rectalcancer (59 cases) both represent the second most common cancers treated at the Cleveland Clinic in Florida in 2006.
8
Lym
ph N
odes
Thyr
oid
Gla
nd
Kid
ney
Hem
atop
oiet
ic
Bla
dder
Bro
nchu
s &
Lun
g
Col
on
Bre
ast
Rec
tum
Pro
stat
e G
land
Top 10 Sites 2006
160
140
120
100
80
60
40
20
0
12 17 1824
30
34
52 54 59
151
Rectal Cancer 2006 Data
Early diagnosis and treatment is essential for successful outcomes and improved survival. Colorectal cancer is anexcellent example of a screen-worthy disease: the incidence is substantial. The disease is serious but not uniformlyfatal. Diagnosis at an earlier stage confers improved probability of survival. Finally, screening tests are widelyavailable. The current recommendations for colorectal cancer screening are digital rectal exam and colonoscopyevery 5-10 years beginning at age 50. For those who are at higher risk, such as family history of colorectal cancer,screening should commence at age 40 or 10 years before the age when diagnosed of the youngest afflicted familymember. All polyps or suspicious lesions are biopsied and evaluated histologically.
Once diagnosed, the clinical stage of the rectal cancer must be accurately determined. Clinical stage is the mostimportant prognostic indicator of survival and directs therapeutic options. CT scan, PET scan, MRI and endo-rectalultrasound are commonly used and are available at our institution. In spite of screening recommendations andprocedures, only 32% of our rectal cancer patients presented at an early stage (stage 0 or 1). Fifty-one percent of thepatients presented at an advanced stage (stage 2, 3, and 4) and 17% the stage was unknown. These representedpatients diagnosed at our institution then subsequently staged and treated elsewhere, or patients operated on at ourinstitution after having neoadjuvant treatment elsewhere and the stage at diagnosis is not known.
5
BREAST Adjuvant Hormonal NSABP B42 8863 Stage I-IIIA ER/PR+completed 5yrs of hormonal therapy:
Letrozole/placebo x 5yrs
Other, Bone Loss CALGB 79809 8693 Breast cancer stages I-III actively menstruating or last menstruation Prevention within 6 months: 2 schedules of Zometa/ Calcium and Vitamin D
(Closed to Enrollment)
Oncotype Dx Assay PACCT-1 8881 Trial assessing individual options for breast cancer treatment
GI Gastric/GE Junction CALGB 8676 Resected, adjuvant chemoRT: 5-FU/LV with RT vs.
80101 E/C/5-FU with RT
Colorectal. Metastatic CALGB 8902 First line, FOLFOX or FOLFIRI plus Cetuximab or80405 Bevacizumab or both every 2 weeks.
Colon. Adjuvant E 5202 8944 High risk (5-FU, Leucovorin and Oxaliplatin +/- bevacizumab) Low risk (observation)
GUProstate, Stage D2 CALGB 9594 8663 Intermittent vs continuous combined androgen deprivation
Renal Cell, adjuvant CTSU E-2805 8869 May be registered pre or post-surgery. T1b -T4, N0-2: Sunitinib vs. sorafenib vs placebo
Companion CTSU E-1Y031 8868 Pharmacogenetic and Genomic study
LUNGE 1505 8937 Stage IB-IIIA NSCLC chemo +/- bevacizumab
ONCOLOGY AND HEMATOLOGY CLINICAL RESEARCH PROTOCOLS
LEUKEMIAMDS CALGB 10105 8677 Primary or secondary MDS: Oral VEGF TKI (PTK787/ZK222584)
Companion CALGB 9665 8699 The CALGB Leukemia Tissue Bank
Companion CALGB 8461 8710 Cytogenetic Studies In Acute Leukemia
Companion CALGB 20203 8700 Molecular markers
LYMPHOMANHL, untreated CALGB 50303 8883 Stage II/III/IV diffuse large B-cell: R-CHOP vs. dose adjusted EPOCH-R
MYELOMACleveland Clinic NIH 8738 Biologic and Clinical Role of COX-2 Inhibitor (celecoxib) in the Foundation Management of MGUS and Smoldering Myeloma
PHARM SPONSOREDAML Gemzyme 8768 Clorfarabine +/- Ara C adult AML
MDS Alexion 8810 Examination of PNH, by Level of CD59 on Red and white blood cells, in bone marrow failure syndromes (EXPLORE)
Paroxysmal Alexion 8726 PNH RegistryNocturnal Hemoglobinuria
ITP Amgen 8817 Single patient use AMG 531 in patients with ITP
NSCL Eli Lilly 8893 Non-small Cell Lung Cancer: The impact of Ethnic Origin on Patients being Treated Second Line with Pemetrexed
Blood-based Assay BioTheme 8895 A Blood-based Diagnostic Assay for Human Cancers
HEMATOLOGY STUDIES

7
Rectal Cancer Radiation Therapy Options
Radiation therapy is typically used in several scenarios in patients diagnosed withrectal cancer. Sometimes, at the time of surgery, it is found that the tumorpenetrated into the mesorectum (stage II) or that the lymph nodes are involved withdisease (stage III). In these patients, chemotherapy and radiation therapy are usuallyrecommended to improve both local and distant control.
If the initial evaluation shows a person to have stage II or III rectal cancer, thenneoadjuvant chemotherapy and radiation therapy should be considered beforesurgery. Neoadjuvant therapy has been shown to increase the likelihood ofsphincter preservation and overall local control. It also aids in the resectability ofthe tumor. In approximately 1/3 of patients, this treatment protocol results in acomplete pathological response, which also predicts for improved overall survival. Ifthe rectal cancer is metastatic, radiation therapy is usually only performed ifpersistent bleeding or pain from the rectal mass exist.
A new radiation technique for rectal cancer includes Intensity Modulated Radiation Therapy (IMRT), which utilizesa highly precise radiation system to deliver carefully calculated beams of intense radiation directly into a cancer.Patients with rectal cancer can benefit from a higher radiation dose to the cancer along with a lower dose to thebladder and small bowel. Successful IMRT depends both on specialized equipment and on a highly trained team ofphysicians, physicists, and technologists.
IMRT is delivered by specially equipped linear accelerators guided by a revolutionary computer system. After acomprehensive series of tests and evaluations, each patient’s unique and complex data are programmed into theIMRT computer to create the ideal treatment plan. Computer-generated imaging of the exact location of the tumorwithin the patient allows the oncology team to calibrate the radiation beam therapy with an accuracy that has neverbefore been available. The beam itself is shaped by the linear accelerators 120 computer-controlled “fingers” andcan be directed on a 360-degree axis. The painless procedure is repeated in a series of outpatient visits, enablingpatients to return to the privacy of their own homes after each treatment.
IMRT can be delivered in conjunction with the TrilogyTM. The Trilogy Stereotactic Machine from Varian MedicalSystems is the most advanced, sophisticated machine of its type. As the leading image-guided radiotherapy (IGRT)system, Trilogy marks the beginning of a new generation of cancer care. This equipment includes on-boardadvanced imaging capabilities built into the system which allows therapists to position patients with unprecedentedaccuracy.
Another new radiation technique includes the use of high dose rate (HDR) brachytherapy. HDR brachytherapy hasbeen increasingly used to deliver focused radiation therapy directly into the tumor prior to surgery to aid inresectability as well as in the patients who have locally advanced unresectable disease. This technique providesadditional local control while maximally sparing the surrounding normal tissues of radiation.
Chris Chen, MDRadiation Oncologist
The Cancer Registry at Cleveland Clinic in Florida is an information system designedto manage the collection, analysis and reporting of cancer-related data to meet stateand national cancer reporting requirements as well as statistical and research needsof clinicians, administrators and the public. The Cancer Registry maintains data onall cancer patients seen since January 1, 2004. Certified tumor registrars prepare anabstract for each patient using information from their medical record. Data includesdemographic information, diagnostic findings, histology, stage of disease, type oftreatment and survival information. The Registry also monitors follow-up of ourpatients through a lifetime tracking record.
In 2006, 726 tumors were reported to the Florida Cancer Data System (FCDS),Florida’s central cancer registry. Of these, 559 were analytic cases meaning thesereceived diagnosis and/or first course of treatment at our facility. The top fiveanalytic sites include prostate, rectum, breast, colon, and lung and bronchus. The
following figure compares the percentage of cases at Cleveland Clinic in Florida to therest of Florida, as well as the United States.
Weekly Cancer Conferences at Cleveland Clinic are integral to improving the care of cancer patients and providingeducation to physicians and other allied health professionals. Various types of malignancies are selected forpresentation on the basis of complexity, unusual manifestation of the disease or special interest. The Conferenceformat includes a complete presentation of medical history, physical findings, clinical course, radiographic studiesand pathological interpretation. Cancer Conferences are approved for one hour of Category 1 Continuing MedicalEducation credit.
During 2006, thirty Cancer Conferences were held in a facility-wide format with multi-disciplinary attendance. Atotal of sixty-one cases were presented. The number of cases presented represents 11% of the 2006 analytic caseload.
Kelly Large, CTRCancer Program Coordinator
Cancer Registry Report 2006
6
27.0%
9.7%
20.0%
6.1%
18.3%
13.5%
10.1%
13.4%
16.7%
15.3%
10.6%
12.5%
Prostate
Breast
Colon & Rectum
Bronchus & Lung
CCF
Florida
USA
These figures were obtainedfrom the 2006 Cancer Facts andFigures, published by theAmerican Cancer Society andmay represent estimates.