Cancer pain. Anatomy, physiology, and pharmacology
9
Cancer Pain Anatomy, Physiology, and Pharmacology RICHARD PAYNE, MD Cancer pain can be divided into three classes: somatic, visceral, and deafferentation. Somatic and visceral pain result from activation of nociceptors by tumor infiltration of tissues and from secondary inflammatory changes with release of algesic chemicals that act to sensitize nociceptors. Pain may be experienced locally (somatic and visceral) or referred to remote cutaneous sites (visceral). Deafferentation pain results from injury to the nervous system due to tumor infiltration or cancer therapy and may persist even after the cause of the injury has been removed. Somatic, visceral, and deafferentation pain may be complicated by sympathetically maintained pain, in which efferent sympathetic activity promotes persistent pain, hyper- pathia, and vasomotor and sudomotor changes after tissue injury from cancer or its therapy. The neuro- biology of cancer pain is complex and incompletely understood. This article summarizes current knowledge in this area and briefly discusses approaches to cancer pain management that are based on this knowledge. Cancer 63:2266-2274, 1989. AIN is perhaps best defined as “an unpleasant sensory P and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.”‘ Advances in neuroanatomy, neurophysiology, and neuropharmacology made in the last decade have given us a greater understanding of the peripheral and central nervous system mechanisms of nociception.24 The perception of pain and the behaviors that characterize the psychologic concomitants of pain are complex phenom- ena related to synaptic activity in the nervous system in ways that are not yet understood. Nevertheless, the study of the physiology and pharmacology of nociceptive and antinociceptive systems has been helpful in providing the scientific rationale for new approaches to the management of acute and chronic pain, including pain related to cancer and to cancer therapy. Pain associated with cancer may result from tumor in- filtration of pain-sensitive structures; injury to nerves, bone, and soft tissue resulting from chemotherapy, radio- therapy, or surgery; or vascular occlusion by tumor. Less commonly, it is unrelated to cancer or cancer treatment.5 The pathophysiology of pain is complex, but studies in animal models have provided clearer insight into its mechanism^.^,^ The cancer patient with pain has served as a clinical model for the study of acute and chronic pain From the Department of Neurology, University of Cincinnati Medical Center, Cincinnati, Ohio. Address for reprints: Richard Payne, MD, Department of Neurology, University of Cincinnati Medical Center, 23 1 Bethesda Avenue, Cincin- nati, OH 45267. The author thanks Diane Longest for assistance in the preparation of this manuscript. Accepted for publication March 3, 1989. in man, and three basic categories of pain have been dis- tinguished: somatic, visceral, and deafferentation (Table 1). In this article I review the anatomy, physiology, and pharmacology of cancer pain and nociception in the cen- tral and peripheral nervous systems. I also briefly discuss current concepts that relate advances in our understanding of the neurobiology of pain to approaches to the man- agement of patients with cancer pain. Somatic and Visceral Pain Sensory receptors that are preferentially sensitive to noxious (tissue-damaging) or potentially noxious stimuli are prevalent in skin, muscle, connective tissues, and tho- racic and abdominal viscera (Fig. 1).6 These nociceptors have been most extensively studied in skin, but nocicep- tive units of viscera and muscle share many of the phys- iologic properties. of cutaneous nociceptors.’ Activation of these units by tumor infiltration of tissue is a major cause of somatic and visceral pain. Cutaneous nociceptors have been defined morphologically by light and electron microscopy and physiologically by their patterns of re- sponse to mechanical, thermal, and chemical stimuli. Ten percent of all myelinated fibers of human cutaneous nerves carry nociceptive information; at least 90% of all unmyelinated fibers are noci~eptive.’,~ Myelinated nociceptors respond to noxious mechanical stimuli almost exclusively, and their afferent fibers con- duct impulses with a velocity of 5 to 50 m/sec (in the A- delta and, rarely, A-beta ranges).8 The threshold for ac- tivation of these nociceptors is five to 100 times higher than that for activation of nonnociceptive mechanore- ~eptors.~.~ Unmyelinated nociceptors are typically poly- 2266
-
Upload
richard-payne -
Category
Documents
-
view
218 -
download
1
Transcript of Cancer pain. Anatomy, physiology, and pharmacology

Cancer Pain
Anatomy, Physiology, and Pharmacology
RICHARD PAYNE, MD
Cancer pain can be divided into three classes: somatic, visceral, and deafferentation. Somatic and visceral pain result from activation of nociceptors by tumor infiltration of tissues and from secondary inflammatory changes with release of algesic chemicals that act to sensitize nociceptors. Pain may be experienced locally (somatic and visceral) or referred to remote cutaneous sites (visceral). Deafferentation pain results from injury to the nervous system due to tumor infiltration or cancer therapy and may persist even after the cause of the injury has been removed. Somatic, visceral, and deafferentation pain may be complicated by sympathetically maintained pain, in which efferent sympathetic activity promotes persistent pain, hyper- pathia, and vasomotor and sudomotor changes after tissue injury from cancer or its therapy. The neuro- biology of cancer pain is complex and incompletely understood. This article summarizes current knowledge in this area and briefly discusses approaches to cancer pain management that are based on this knowledge.
Cancer 63:2266-2274, 1989.
AIN is perhaps best defined as “an unpleasant sensory P and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.”‘ Advances in neuroanatomy, neurophysiology, and neuropharmacology made in the last decade have given us a greater understanding of the peripheral and central nervous system mechanisms of nociception.24 The perception of pain and the behaviors that characterize the psychologic concomitants of pain are complex phenom- ena related to synaptic activity in the nervous system in ways that are not yet understood. Nevertheless, the study of the physiology and pharmacology of nociceptive and antinociceptive systems has been helpful in providing the scientific rationale for new approaches to the management of acute and chronic pain, including pain related to cancer and to cancer therapy.
Pain associated with cancer may result from tumor in- filtration of pain-sensitive structures; injury to nerves, bone, and soft tissue resulting from chemotherapy, radio- therapy, or surgery; or vascular occlusion by tumor. Less commonly, it is unrelated to cancer or cancer treatment.5 The pathophysiology of pain is complex, but studies in animal models have provided clearer insight into its mechanism^.^,^ The cancer patient with pain has served as a clinical model for the study of acute and chronic pain
From the Department of Neurology, University of Cincinnati Medical Center, Cincinnati, Ohio.
Address for reprints: Richard Payne, MD, Department of Neurology, University of Cincinnati Medical Center, 23 1 Bethesda Avenue, Cincin- nati, OH 45267.
The author thanks Diane Longest for assistance in the preparation of this manuscript.
Accepted for publication March 3, 1989.
in man, and three basic categories of pain have been dis- tinguished: somatic, visceral, and deafferentation (Table 1). In this article I review the anatomy, physiology, and pharmacology of cancer pain and nociception in the cen- tral and peripheral nervous systems. I also briefly discuss current concepts that relate advances in our understanding of the neurobiology of pain to approaches to the man- agement of patients with cancer pain.
Somatic and Visceral Pain
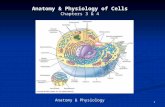
Sensory receptors that are preferentially sensitive to noxious (tissue-damaging) or potentially noxious stimuli are prevalent in skin, muscle, connective tissues, and tho- racic and abdominal viscera (Fig. 1).6 These nociceptors have been most extensively studied in skin, but nocicep- tive units of viscera and muscle share many of the phys- iologic properties. of cutaneous nociceptors.’ Activation of these units by tumor infiltration of tissue is a major cause of somatic and visceral pain. Cutaneous nociceptors have been defined morphologically by light and electron microscopy and physiologically by their patterns of re- sponse to mechanical, thermal, and chemical stimuli. Ten percent of all myelinated fibers of human cutaneous nerves carry nociceptive information; at least 90% of all unmyelinated fibers are noci~eptive.’,~
Myelinated nociceptors respond to noxious mechanical stimuli almost exclusively, and their afferent fibers con- duct impulses with a velocity of 5 to 50 m/sec (in the A- delta and, rarely, A-beta ranges).8 The threshold for ac- tivation of these nociceptors is five to 100 times higher than that for activation of nonnociceptive mechanore- ~ e p t o r s . ~ . ~ Unmyelinated nociceptors are typically poly-
2266

No. 11 ANATOMY, PHYSIOLOGY, AND PHARMACOLOGY OF CANCER PAIN * PUyne 2267
TABLE 1. Categories of Cancer-Related Pain
Somatic Visceral DealTerentation
Characteristics of pain Constant, aching, gnawing, well Constant, aching, poorly Paroxysmal shooting or electrical
cutaneous sites burning, constricting sensations
discharges in the peripheral and central nervous systems
Loss of central inhibitory modulation Sympathetic-somatic afferent
localized localized; often referred to shock-like pain on background of
Putative mechanisms Activation of nociceptors Activation of nociceptors Spontaneous and paraoxysmal
nociceptor interaction
Examples
Management
Bone metastasis Pancreatic cancer, liver/lung metastases with shoulder pain
Metastatic brachial and lumbosacral plexopathies; postherpetic neuralgia
Treatment of tumor: analgesics; nerve blocks, somatic and sympathetic?; cordotomy; sympathetic?; cordotomy blocks, somatic and sympathetic?; TENS cordotomy; invasive (brain and
Treatment of tumor: analgesics; nerve blocks, somatic and
Treatment of tumor: analgesics (especially adjuvants)*; TENS; nerve
spinal cord) stimulation
TENS: transcutaneous electrical nerve stimulation. * Adjuvant analgesics such as tricyclic antidepressants (e.g., amitrip-
tyline) and anticonvulsants (e.g., carbamazepine) are often useful. t Somatic, visceral, and deafferentation pain may be complicated by
sympathetically maintained pain. This pain is severe, burning in quality,
modal, responding to mechanical, thermal, and chemical stimuli.8 The afferent fibers for unmyelinated nociceptors in man conduct impulses with a velocity of 0.6 to 2 m/ sec (in the C range).
As revealed by microneurographic studies in man, ac- tivation of a single myelinated nociceptor is sufficient to cause a sharp, stinging Activation of unmyelin- ated nociceptors is associated with a dull, burning, or ach- ing pain." These studies have also demonstrated that no- ciceptors are not spontaneously active but may show sen- sitization, particularly after thermal injury to the skin.' Sensitization is manifested as (1) a lower threshold of ac-
PRESSURE
FIG. 1. Polymodal nociceptor: Nociceptors are specialized sensory re- ceptors that respond preferentially to stimuli in the tissuedamaging range (ie., they are not normally spontaneously active and have a high threshold for activation). Once the threshold is reached, the polymodal nociceptor may respond to noxious thermal, chemical, or mechanical stimuli, with a linear increase in its firing rate that is directly proportional to increasing stimulus intensity. Polymodal nociceptors conduct their afferent impulses over unmyelinated (C) fibers (Reprinted with permission from Fields HL. Pain. New York McGraw-Hill, 1987; 27).
and associated with dyesthesias and hyperpathia. There are accompanying vasomotor and sudomotor changes such as brawny edema, subcutaneous atrophy, fibrosis, bony ankylosis, and osteoporosis. This pain can be significantly relieved by blockade of the appropriate sympathetic efferent innervation of the painful part.
tivation after injury, (2) greater intensity of response to a noxious injury, and (3) the emergence of spontaneous a~ t iv i ty .~ , '~
Sensitization of nociceptors may occur within minutes of an injury and may last for hours. It has been speculated that this is one of the physiologic correlates of hyperpathia (or allodynia), which occurs after thermal injury to kin,^,'^ and it may be a mechanism of chronic or acute recurrent pain in man after tissue injury. Sensitization of nociceptors may be mediated by algesic substances such as potassium ions, adenosine triphosphate, bradykinin, and prosta- glandins (especially prostaglandin E2) released as a result of tissue i n j ~ r y . ~ , ' ~
Once activated, nociceptors generate impulses that are conducted into the central nervous system via A-delta afferent fibers (mechanonociceptors) or C afferent fibers (polymodal nociceptors). These fibers enter the spinal cord laterally in the dorsal root and synapse in the superficial dorsal horn to activate ascending nociceptive systems (spinothalamic, spinocervical, and spinoreticular tracts) (Fig. 2).
Deep pain originating from skeletal muscle, bone, and thoracic, abdominal, and pelvic viscera is much more common than cutaneous pain.4 Metastatic tumor infil- tration of bone and gastrointestinal and genitourinary tu- mors that invade abdominal and pelvic viscera are very common causes of pain in the cancer ~ a t i e n t . ~ Although not nearly as well studied as their cutaneous counterparts, muscular and visceral nociceptors have been found in almost all organs studied, and they appear to have ana- tomic and physiologic properties similar to those of cu- taneous n o c i ~ e p t o r s . ~ , ' ~ ~ ~ ~

Vol. 63 2268 CANCER June 1 Supplement 1989
Muscular pain can be produced by injections of sodium chloride and potassium chloride into muscle, fascia, and tendons or by squeezing or exercising muscle, especially under ischemic c~nditions. '~, ' '~'~ These same stimuli ex- cite muscle nociceptors.2 The pain is typically felt deeply rather than superficially and is often described as aching.2
Metastatic bone disease causes the most common pain syndrome in patients with cancer.' Tumor metastasis to bone is associated with bone destruction and new bone formation, Myelinated and unmyelinated afferent fibers are present in bone, and their density is greatest in the periosteum. Prostaglandins are necessary for osteolytic and osteoclastic metastatic bone changes, and prostaglan- din E2 is known to sensitize nociceptors and produce hy- peralgesia.20 Drugs that inhibit prostaglandin synthesis decrease bone pain2' and may decrease tumor growth in bone.22,23 In addition, osteoclast-activating factor (which is not a prostaglandin) is also thought to be an algesic chemical that activates nociceptor~.~~
Visceral pain is mediated by nociceptors in the cardio- vascular, respiratory, gastrointestinal, and genitourinary systems and is usually described as deep, aching, and col- icky. Visceral pain typically is poorly localized and often is referred to cutaneous points, which may be tender.2 When normal human viscera are manipulated in con- scious patients, pain is usually not elicited, even when the viscera are cut,iburned, or cru~hed.~' Stimuli sufficient to cause visceral pain are (1) irritation of the mucosal and serosal surfaces, (2) torsion and traction of the mesentery, (3) distention or contraction of a hollow viscus, and (4) impaction.26 Similar stimuli are necessary to provoke pain in the bladder, ureter, or ~ r e t h r a . ~ ~ ? ~ '
Several hypothetical mechanisms for pain referral have been p r o p o ~ e d , ~ , ~ , ' ~ . ' ~ , ~ ~ including dual innervation of so- matic and visceral structures by common afferent fibers29 and release of algesic chemicals in the vicinity of somatic afferent fibers by antidromic activity in visceral afferent fibers.2 One hypothesis supported by some experimental data is that visceral nociceptor activity converges with input from somatic afferents into common pools of spi- nothalamic tract cells in the dorsal horn of the spinal ~ord! , '~ , '~ ,~~,~ ' According to this theory, pain is referred to remote cutaneous sites because the brain "misinter- prets" input as coming from a peripheral cutaneous source, which normally bombards the central nervous system with sensory stimuli2
Tumor infiltration, with associated inflammation and release of algesic chemical mediators in skin, bone, and viscera, activates and sensitizes nociceptors, which may promote ongoing activation of these units to produce pain, even with minimal additional mechanical pressure in the tissues as a result of tumor growth. In fact, mechanical deformation of tissues alone may not be adequate to pro- duce acute or chronic pain.32
In summary, somatic pain occurs as a result of acti-
FIG. 2. Dorsal horn circuitry: Nociceptive afferent fibers (A-delta and C) enter the spinal cord through the lateral portion of the dorsal root and synapse in lamina I (A-delta fibers) and lamina I1 (C fibers). Lamina I neurons receive indirect input from intemeurons ("stalk" cells) in lamina 11. A major projection cell from which the ascending spinothalamic tract originates is the lamina V neuron, which receives direct and indirect nociceptive afferent input from A-delta and C fibers (Reprinted with permission from Fields HL. Pain. New York: McGraw-Hill, 1987; 55).
vation of nociceptors in cutaneous and deep tissues (e.g., by tumor metastasis in bone) and is the most common type of pain in cancer patients. This pain is typically well localized, usually constant, and frequently described as aching or gnawing. Visceral pain also is common in the cancer patient and presumably results from stretching or distending or from the production of an inflammatory response and the release of algesic chemicals in the vicinity of nociceptors. Common examples are abdominal, back, and shoulder pain resulting from liver metastasis and pancreatic cancer. This type of pain is typically poorly localized, often is described as deep, squeezing, and pres- sure, and it may be associated with nausea, vomiting, and diaphoresis, particularly when acute. Visceral pain is often referred to cutaneous sites, which may be far from the lesion (e.g., shoulder pain resulting from diaphragmatic irritation), and associated with tenderness at the cutaneous site.
Deafferentation Pain
Deafferentation pain results from injury to the periph- eral and/or central nervous system as a result of tumor compression or infiltration of peripheral nerve or the spi- nal cord, or injury to peripheral nerve as a result of surgery, chemotherapy, or radiation therapy for cancer.' Examples of deafferentation pain are metastatic or radiation-induced brachial or lumbosacral plexopathies, epidural spinal cord and/or cauda equina compression, and postherpetic neu- ralgia.5 Pain resulting from neural injury is often severe.

No. 1 1 ANATOMY, PHYSIOLOGY, AND PHARMACOLOGY OF CANCER PAIN * PUyne 2269
120 WDR SaUEEZE
90
z YI
3 r? 60 n P
4- 4- + +
0 30 60 90 120 150
HT
SRUEEZE
TIME, S
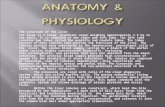
FIGS. 3A AND 3B. Wide-dynamic-range and high-threshold neurons: Spinothalamic tract neurons in the dorsal horn exhibit two types of re- sponse to sensory stimuli. Both are important for pain transmission in the central nervous system. (A, top) The wide-dynamic-range neuron responds in a graded fashion to innoxious (brush and press) as well as noxious (pinch and squeeze) stimuli applied to its receptive field, which is here depicted as the lower limb of the monkey (+). The negative signs indicate areas of the body that are inhibitory to the wide-dynamic-range neuron. This neuron is believed to be involved in the modulation of afferent nociceptive input and not just in the simple signaling of the presence or absence of potential or actual tissue-damaging stimuli. (B, bottom) A high-threshold or nociceptive-specific neuron responds only to a noxious squeeze stimulus applied to its receptive field in the foot. This neuron is believed to signal the presence or absence of a tissue- damaging stimulus (Reprinted with permission from Willis WD. The spinothalamic tract. In: Rosenberg RN, ed. The Clinical Neurosciences, vol. 5. New York Churchill-Livingstone, 1983; 335).
It is typically described as a constant, dull, squeezing, and aching sensation, with superimposed paroxysms of burn- ing and/or electric shock-like sensations. These paroxysms likely involve spontaneous and ectopic firing of damaged peripheral nerve structure^.^^ Peripheral nerve injury also induces “epileptiform” activity in the medial thalamus in the area of projection of the paleospinothalamic t r a ~ t . ~ ~ , ~ ~ In addition, stimulation of the medial thalamus (central lateralis, parafasicularis, and centrum median nuclei) produces burning pain in patients who have preexisting deafferentation pain but not in patients with- out pain.35,36
Sympathetic Nervous System and Cancer Pain
The sympathetic nervous system may be involved in cancer pain (particularly acute visceral and deafferentation pain), but its role is poorly under~tood.’~ Evidence for the involvement of the sympathetic nervous system in
pain includes the following observations: (1) pain is re- lieved in patients with reflex sympathetic dystrophy by sympathetic blockade with local anesthetics or by the ad- ministration of systemic adrenergic blocking drugs, such as pheno~ybenzamine~’; (2) sympathetic stimulation in- creases pain in some patients with reflex sympathetic dystrophy39; (3) in animal models of peripheral nerve in- jury, new alpha-adrenergic receptors develop, and regen- erating neuritis is pharmacologically sensitive to system- ically or locally applied cat echo la mine^^^; and (4) in other animal models, peripheral sensory receptors are activated by sympathetic ~timulation.~’
Dorsal Horn Circuitry and Ascending Neural Pathways Involved in Nociception
The dorsal horn consists of six laminae, with lamina I, the marginal zone, being the most dorsal. Lamina I1 is the substantia ge la t in~sa .~~ The dendrites in laminae IV and V make synaptic contact with primary afferents in the more dorsal laminae, and cell bodies in laminae I and V are important contributors to spinothalamic tract as- cending projections. Dorsal horn and thalamic cells re- ceiving input from primary afferent fibers can have two types of response: wide dynamic range and nociceptive specific (Figs. 3A and 3B).2,4,43 The wide-dynamic-range neuron responds to multiple low-threshold and high- threshold inputs and increases its firing pattern in pro- portion to the intensity of the stimulus. In contrast, the nociceptive-specific neuron has a high activation thresh- old, responding only to stimuli that are intense enough to damage tissue.
Afferent fibers from nociceptors enter the spinal cord laterally in the dorsal root and ascend or descend one to two segments in Lissauer’s tract. Thinly myelinated no- ciceptive (A-delta) fibers synapse in lamina I and the ven- tral portions of laminae I1 and I11 of the dorsal horn.223,44,45 A-delta afferents also synapse in lamina V. Unmyelinated (C) fibers terminate predominately in lamina I1 (Fig. 2).45 The apical dendrites of neurons in laminae IV and V project into laminae I and I1 and make synaptic contact with primary nociceptive afferent fiber^.^^,^' Thus, cells in laminae I and V respond maximally to noxious stimuli, and axons from laminae I (not shown) and V neurons decussate in the central gray matter of the spinal cord and become the ascending projections of the neospinothalamic and paleospinothalamic
Melzack and Wall49 have postulated that the balance of activity in myelinated (large-fiber) and unmyelinated (small-fiber) afferents is important to the perceived inten- sity of pain. According to this theory, known as the gate- control theory, myelinated and unmyelinated primary af- ferent fibers have direct excitatory effects on dorsal horn transmission neurons (so-called T-cells) and indirect in- hibitory (unmyelinated fiber) and excitatory (myelinated

2270 CANCER June 1 Supplement 1989 Vol. 63
fiber) effects on interneural cells of the substantia gelati- nosa in lamina I1 (Fig. 4). Since the net effect of cells of the substantia gelatinosa on T-cells is inhibitory, activation of myelinated afferent fibers would have a dual positive and negative influence, and there would be no net increase in T-cell firing. In contrast, activity in unmyelinated (Le., nociceptive) afferent fibers produces a large increase in T- cell firing by direct and indirect effect^.^ Since most stimuli activate both classes of afferent, the effect on T-cells is intermediate.
The gate-control theory predicts that relatively selective stimulation of large fibers, which can be produced by transcutaneous electrical nerve stimulation (which acti- vates large-fiber mechanoreceptors in the skin), may pro- vide pain relief by dampening the excitatory effects of small-fiber nociceptive input on T-cells. In some patients with painful peripheral nerve injury, transcutaneous elec- trical nerve stimulation may provide pain relief,50,5’ and it has been used successfully in the treatment of postop- erative pain syndromes affecting peripheral nerve (e.g., incisional intercostal neuralgia complicating thoracotomy) and painful vincristine-induced neuropathy. In fact, Lee et al. 52 have demonstrated that transcutaneous electrical nerve stimulation can effectively inhibit C fiber-evoked responses in spinothalamic tract neurons in a primate model and that, because this response is not reversed by naloxone, it is not opioid mediated.
The neospinothalamic tract ascends in the anterolateral quadrant of the spinal cord and has a heavy input from A-delta nociceptive fibers (Fig. 5). This system projects monosynaptically to the ventrobasilar thalamic complex (primarily the ventroposterolateral nucleus). From there, axons project to the somatosensory cortex (SI and SII) in the parietal lobe. The paleospinothalamic tract has a pre- dominant C fiber input. It ascends in continuity with the neospinothalamic tract in the anterolateral quadrant of the spinal cord and sends diffuse projections to the retic- ular formation in the brain stem and to the posterior thal- amic nucleus and the central-lateral nuclei of the intra- laminar nuclear complex.* From the posterior thalamic nuclear complex, projections extend to the retroinsular cortex. The central-lateral nuclear complex projects to the striaturn and sends profuse projections to the cerebral cortex.
The neospinothalamic tract subserves the sensory-dis- criminative aspects of pain perception (stimulus localiza- tion and recognition of pain intensity). The phylogenet- ically older paleospinothalamic tract appears to subserve the arousal, emotional, and affective/suffering compo- nents of pain.48 In addition to receiving input from the paleospinothalamic tract, the intralaminar nuclear com- plex also receives afferents from the cerebellum and pro- jects efferent fibers to the striatum. This suggests that this system may also be important for the motor responses that accompany pain.2 Nociceptive ventral posterolateral
M
U
Alfluenl I Cell T Cell T-cell Output Input Elfect Elfect (T-1) M + + 0 U + ++
M + U 0 + +
FIG. 4. Gate-control theory: The revised gate-control hypothesis sug- gests that interactions between myelinated nonnociceptive afferents (A- beta fibers) (M) and unmyelinated nociceptive afferents (C fibers) (U) act on pain transmission cells (“T” cells) through direct and indirect connections via interneurons (“I” cells). An increase in T-cell activity ordinarily provides nociceptive information to be transmitted to rostral levels of the central nervous system. The I cell is inhibitory to the T-cell. Activity in M fibers excites both the I and T-cells, with the effect that there is no net increase in T-cell firing. Activity in U fibers inhibits I cells but excites T-cells, with the net effect of a large increase in T-cell firing. A mixture of activity in these cells produces an intermediate effect. This hypothesis has been used to explain a variety of phenomena, in- cluding the analgesic effects of transcutaneous electrical nerve stimulation and the soothing effects of counterstimulation ofan acutely injured body part (Reprinted with permission from Fields HL. Pain. New York: McGraw-Hill, 1987; 139).
-
neurons have restricted receptive fields, are contralateral to the applied stimulus, and are somatotypically organ- ized. Thalamic projections from the ventral posterolateral nucleus are organized into cortical columns.2 Many spi- nothalamic tract cells in the ventral posterolateral nucleus and medial thalamus receive convergent input from skin, muscle, and viscera, or all three. These cells may also contribute to referred pain.
In the primate, at least three other ascending spinal tracts, the spinoreticular tract, the spinocervicothalamic tract, and postsynaptic dorsal column fibers, convey no- ciceptive information, although their role in pain trans- mission is not as clear as that of the spinothalamic tract. The spinoreticular tract decussates and ascends in the contralateral anterolateral quadrant, intermingled with fibers from the spinothalamic tract. In general, cells of origin of the spinothalamic tract are in laminae VII and VIII (and perhaps V and VI), and fibers project to the bulbopontine and mesencephalic levels of the reticular formation of the brain stem3 The spinocervicothalamic tract has neurons of origin in lamina IV, ascends in the ipsilateral dorsolateral quadrant, and projects to the lateral cervical nucleus, eventually joining spinothalamic tract fibers in the medial lemniscus. This tract carries mostly information from mechanoreceptors in hair follicles, but some neurons carry nociceptive inf~rmation.~ The post- synaptic dorsal column fibers have cells of origin in lam- inae I1 and IV (in the monkey), and carry noxious and

No. 11 ANATOMY, PHYSIOLOGY, AND PHARMACOLOGY OF CANCER PAIN * Payne 227 1
MEDIAL THALAMIC NUCLEI
0
@ iIVDUCTAL
C NUCLEUS CUNEIFORMIS
GIGANTOCELLULARIS NUCLT& SPINOTHALAMIC
TRACT
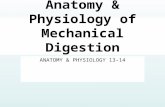
FIG. 5 . Ascending spinothalamic tracts: The spinothalamic pathway ascends in the anterolateral quadrant of the spinal cord, contralateral to its cells of origin in the dorsal horn. The pathway is somatotopically organized, with sacral fibers represented most dorsolaterally, and cervical fibers most ventrally at spinal and brain stem levels. This pathway projects to the ventral posterolateral thalamic nucleus; second-order fibers project to the somatosensory cortex. Ablation of fibers in this pathway at spinal cord levels (cordotomy) may provide contralateral analgesia. Other as- cending fiber systems (especially the spinoreticular, spinocervicothalamic, and polysynaptic dorsal column tracts) end in the reticular formation of the brain stem, the nucleus gigantocellularis, and the nucleus cunei- formis. These systems are phylogenetically older than the neospinothal- amic tract and are thought to be important in mediating arousal and affective responses associated with pain. They project to medial thalamic nuclei. In addition, these paleospinoreticulothalamic systems may be responsible, in part, for the failure of cordotomy to provide permanent analgesia by providing alterative routes for transmission of nociceptive information to higher levels of the nervous system after interruption of the spinothalamic tracts (Reprinted with permission from Maciewicz R, Sandrew BB. Physiology of pain. In: Aronoff G , ed. Evaluation and Treatment of Chronic Pain. Baltimore: Urban and Schwarzenberg, 1985; 25).
innoxious information; they ascend in the ipsilateral dor- sal column to the medial lemni~cus.~
It should be noted that dorsal column stimulation may relieve cancer pain in certain situation^.^^ Such stimula- tion is thought to produce analgesia by causing collaterals of large-fiber primary afferents to exert inhibitory effects on nociceptive neurons in the spinal cord.3
The tngeminal subnucleus caudalis (spinal tngeminal nucleus) and the adjacent reticular formation are directly continuous with the dorsal horn of the cervical spinal cord, and this nucleus is essentially the equivalent of the spinal dorsal horn.54,55 Descending fibers in the spinal tri- geminal tract convey pain and thermal and tactile infor- mation from the ipsilateral face, forehead, and mucous membranes of the nose and mouth. The subnucleus cau- dalis appears to be the only part of the trigeminal complex uniquely concerned with pain and thermal sensation, and neurons within laminae I and V, and the adjacent reticular formation, encode nociceptive information in the same manner as spinal dorsal horn neurons. Second-order neu- rons cross to the other side of the brain stem, ascend in the contralateral medial lemniscus, and terminate in the ventroposteromedial thalamic nucleus. Chronic head and neck pain caused by tumors such as squamous cell car- cinomas of the larynx, floor of the mouth, posterior phar- ynx, and eustachian tube is conveyed by afferent dis- charges in the glossopharyngeal nerve, which synapse in the spinal nucleus of the trigeminal nerve in the medulla and upper cervical cord.56
Cerebral Cortex and Pain
The exact role of the cortex in pain is still un- ~ l e a r . ~ ~ - ~ ’ Some ~ t u d i e s ~ ~ ? ~ ’ suggest that pain is not altered by large lesions of the cerebral hemispheres, including the somatosensory cortex. In contrast, Marshall5* reported that small lesions of the cortex are associated with 10s crf pain perception. Primary and metastatic brain tumors usually do not produce pain but may produce headache when associated with increased intracranial pressure. The following observations suggest that, in man, the cortex does play a part in pain: (1 ) the somatosensory cortex (SI) contains nociceptive-specific neurons that contain pro- jections from the ventral posterolateral nucleus of the thalamus (these neurons can have large or small receptive fields, and may be activated by bilateral or contralateral stimuli)6’; (2) stimulation of exposed cortex sometimes produces paid9; (3) pain is sometimes experienced in epi- leptic auras62; and (4) lesions of the cortex can produce a syndrome mimicking “thalamic” pain.2
Pain-Suppression Pathways
As demonstrated by Bausbaum and field^,^^,^^ neural pathways that arise in the brain stem and descend to the spinal cord are important modulators of nociceptive in- formation (Fig. 6).4,64 A major pathway begins in the peri- aqueductal gray matter of the midbrain and descends to the nucleus raphe magnus in the medulla. From the nu- cleus raphe magnus, a projection extends to the dorsal horn of the spinal cord via the dorsal longitudinal fascic- ulus and terminates in laminae I, 11, and IV. A second, more lateral descending pathway that starts in the nucleus

2272 CANCER June 1 Supplement 1989 Vol. 63
reticularis paragigantocellularis in the pons also projects to the dorsal horn via the dorsal longitudinal fasciculus.
About 15% of the cells in the nucleus raphe magnus contain serotonin, and the projection from the nucleus raphe magnus is the major projection to the spinal cord.64 However, the nucleus raphe magnus also contains sub- stance P, enkephalin, and thyrotropin-releasing hormone, all putative neurotransmitters that have, as yet, poorly characterized roles in this pathway. In the projection from the nucleus reticularis paragigantocellularis, norepineph- rine and serotonin are among the major neurotransmit- t e r ~ . ~ , ~ ~ A third projection to the spinal cord from the brain stem, the dorsal raphe nucleus, contains serotonin and enkephah6* Thus, serotonergic and catecholamin- ergic terminals that have been found on the dendrites of dorsal horn neurons originate from these descending pro- jections of the brain stem.64
Electrical stimulation of the periaqueductal gray matter or nucleus raphe magnus , or microinjection of morphine at these sites, produces total-body analgesia without con- comitant motor, sensory, or autonomic b l ~ c k a d e . ~ , ~ ~ This analgesia is blocked by prior section of the dorsal longi- tudinal fasciculus and, in animals, by pretreatment with parachlorophenylamine (which blocks serotonin synthe- sis). This, as well as other evidence, demonstrates the im- portance of the spinal serotonergic pathway in the pro- duction of analge~ia.~
Opioid analgesics appear to act by binding to opioid receptors in the descending pathway, thereby mimicking the action of endogenous opioids. Although the physio- logic effects of systemically administered opioids are complex and incompletely e l~c ida ted ,~~ recent studies have demonstrated some of the neuronal mechanisms of morphine’s action.4s66 Fields and Heinricher66 observed that the systemic administration of morphine, or its direct injection into the periaqueductal gray matter of the rat, had specific effects on neurons in the rostral-ventral me- dulla. This system is part of the endogenous descending control pathway from the brain stem to the spinal cord. These authors demonstrated an excitatory effect of mor- phine on “of’ cells in the rostral-ventral medulla; the effect of this excitation is to produce continuous firing in this cell, thereby inhibiting pain transmission at spinal levels. This phenomenon is reversible by the administra- tion of n a l ~ x o n e . ~ , ~ ~
Tricyclic antidepressant compounds, such as amitrip- tyline, block presynaptic uptake of serotonin and nor- epinephrine, thus augmenting their postsynaptic effects. Tricyclic antidepressants are useful analgesic agents in a variety of pain syndromes, including cancer pain,4,5967 and augmentation of serotonergic effects (and possibly nor- adrenergic effects as well) in this descending system may be an important mechanism of the action of these d r ~ g s . ~ , ~ ~ , ~ ’ Evidence for this is the observation that the analgesic activity of tricyclic antidepressants appears to
FIG. 6. Endogenous pain-control pathway: Descending neuronal pro- jections from the cortex and brain stem (especially the periaqueductal gray matter [PAG] and the nucleus raphe magnus [NRM]) connect to the nociceptive dorsal horn cells via the dorsal longitudinal fasciculus [DLF]. Electrical stimulation or microinjection of opioids into the peri- aqueductal gray or the nucleus raphe magnus may produce analgesia in the absence of motor, sensory, or autonomic blockade. Morphine appears to excite “off’ cells in the rostral-ventral medulla (near the nucleus raphe magnus) that project to the spinal dorsal horn and has the net effect of inhibiting spinal reflexes activated by noxious heat. Serotonin (5-hy- droxytryptophan [5HT]), enkephalin [ENK], and norepinephrine [NE] appear to be important neurotransmitters in this system. Augmentation or inhibition of the synaptic activity of these chemicals may affect no- ciceptive transmission in animals, and potentiation of serotonergic activity has been proposed as a possible mechanism for the analgesic actions of tricyclic antidepressant compounds. PGL nucleus reticularis giganto- cellularis (Reprinted with permission from Bausbaum A. The generation and control of pain. In: Rosenberg RN, ed. The Clinical Neurosciences, vol. 5 . New York Churchill-Livingstone, 1983; 301).
be independent of their antidepressant a ~ t i v i t y . ~ , ~ ~ - ~ ~ In addition, they appear to potentiate morphine analgesia in the experimental animal, presumably by potentiation of serotonergic synaptic mechanisms in the descending endogenous pain-control Finally, the in- trathecal administration of alpha-2 adrenergic agonists (clonidine, for example) appears to produce analgesia in animals and man,72,73 and destruction of norepinephrine-

No. 11 ANATOMY, PHYSIOLOGY, AND PHARMACOLOGY OF CANCER PAIN * PUyne 2273
containing pathways attenuates response to serotonin ag- oni~ts.’~ These observations indicate that serotonin and norepinephrine together play an important role in the analgesic effects of tricyclic compounds.
The descending pathway system can be activated by many physiologic and pathologic stimuli, including stress. It has been suggested that activation of this control system may account for placebo-induced analgesia and the ap- parent analgesic effects of acupuncture and hypno~is.~ However, the reversibility of these phenomena by nal- oxone and the role of endogenous opioid systems in their production are still in doubt.
Management of Cancer Pain
Somatic and visceral pain involve direct activation of nociceptors and are often complications of tumor infil- tration of tissues or of tissue-damaging effects of cancer therapy. These types of pain usually are managed by treating the tumor (when possible) and using appropriate nonopioid, opioid, and adjuvant analgesic drugs. Neu- roablative therapies may be helpful in specific circum- stances. Cordotomy, that is, sectioning of the spinothal- amic tracts contralateral to the site of pain, may be helpful for unilateral somatic and visceral pain below the waist. This procedure may also be helpful in early deafferentation pain (e.g., lumbosacral plexopathy), in which peripheral nerves are compressed but not infiltrated or destroyed by metastatic growth.
Deafferentation pain is most often a complication of tumor infiltration of large peripheral nerve trunks (e.g., metastatic brachial plexopathy in breast and lung cancer) but may also be a complication of cancer therapy (such as vincristine-induced peripheral neuropathy or radiation- induced myelopathy or plexopathy). This type of pain is often poorly tolerated and difficult to control, particularly if not treated early and aggressively. As discussed above, the pathophysiology of deafferentation pain is different from that of somatic or visceral pain, and treatment strat- egies may be different. Management of deafferentation pain usually is mainly palliative, because pain of this type is often severe and treatment of its cause may not be ef- fective if the nervous system has been irreversibly injured. In addition, many deafferentation pain syndromes occur as a complication of cancer the rap^.^ Opioid analgesics are widely used in the management of deafferentation pain, although their overall efficacy in this use does not appear to be as great as it is in the treatment of somatic or visceral pain. Adjuvant analgesic drugs, such as tricyclic antidepressants, anticonvulsants, and steroids, may be helpful in individual cases, and when deafferentation pain is complicated by sympathetic dystrophy, early sympa- thetic blockade is indicated. Neurostimulation, either transcutaneous or invasive (spinal dorsal column, thal- amic, and periventricular gray stimulation), has also been
advocated, but its ultimate role in the management of deafferentation pain remains to be ~ l a r i f i e d . ~ ~ . ~ ~
REFERENCES
1. Lindblom U, Merskey H, Mumford JM, Nathan PW, Noordenbos W, Sunderland S. Pain terms: A current list with definitions and notes on usage. Pain 1986; (Suppl) 3:S215-S221.
2. Willis WD Jr. The Pain System: The Neural Basis of Nociceptive Transmission in the Mammalian Nervous System. (Pain and Headache, vol. 8.) Basel: Karger, 1985; 1-346.
3. Besson JM, Chaouch A. Peripheral and spinal mechanisms of no- ciception. Physiol Rev 1987; 67:67-186.
4. Fields HL. Pain: Mechanisms and Management. New York McGraw-Hill, 1987; 1-416.
5. Foley KM. The treatment of cancer pain. N Engl J Med 1985;
6. Light A, Perl ER. Peripheral sensory systems. In: Dyck PJ, Thomas PK, Lambert EH, Bunge R, eds. Peripheral Neuropathy, vol. 2, ed. 2. Philadelphia: WB Saunders, 1984; 2 10-230.
7. Hagbarth K-E, Torebjork HE, Wallen BG. Microelectrode record- ings from human skin and muscle nerves. In: Dyck PJ, Thomas PK, Lambert EH, Bunge R, eds. Peripheral Neuropathy, vol. 2, ed. 2. Phil- adelphia: WB Saunders, 1984; 1016-1029.
8. Perl ER. Characterization of nociceptors and their activation of neurons in the superficial dorsal horn: First steps for the sensation of pain. In: Kruger L, Liebeskind JC, eds. Neural Mechanisms of Pain: Advances in Pain Research and Therapy, vol. 6. New York Raven Press,
9. Meyer RA, Campbell JN. Myelinated nociceptive afferents account for the hyperalgesia that follows a bum to the hand. Science 198 1 ; 2 13:
10. Hagbarth K-E. Exteroceptive, proprioceptive, and sympathetic activity recorded with microelectrodes from human peripheral nerves. Mayo Clin Proc 1979; 54:353-365.
1 1. Torebjork HE. Activity in C nociceptors and sensation. In: Ken- shalo DR, ed. Sensory Function of the Skin of Humans. New York: Plenum Press, 1979; 3 13-325.
12. Torebjork HE, Hallin RG. Microneurographic studies of peripheral pain mechanisms in man. In: Bonica JJ, Liebeskind JC, Albe-Fessard DG, eds. Proceedings of the 2nd World Congress on Pain; Advances in Pain Research and Therapy, vol. 3. New York: Raven Press, 1979; 121- 131.
13. Vallbo AB, Hagbarth K-E, Torebjork HE, Wallin BG. Somato- sensory, proprioceptive, and sympathetic activity in human peripheral nerves. Physiol Rev 1979; 59:919-957.
14. Wall PD, McMahon SB. Microneurography and its relation to perceived sensation: A critical review. Pain 1985; 21:209-229.
15. Campbell JN, Myer RA. Primary afferents and hyperalgesia. In: Yaksh TL, ed. Spinal Afferent Processing. New York Plenum Press,
16. Foreman RO. Spinal substrates in visceral pain. In: Yaksh TL, ed. Spinal Afferent Processing. New York: Plenum Press, 1986; 207- 221.
17. Cervero F, Momson JFB, eds. Progress in Brain Research, vol. 67. Visceral Sensation. Amsterdam: Elsevier, 1986; 1-336.
18. Mense S, Schmidt RF. Muscle pain: Which receptors are respon- sible for transmission of noxious stimuli? In: Rose FC, ed. Physiological Aspects of Clinical Neurology. Oxford: Blackwell, 1977; 265-277.
19. Mense S, Stahnke M. Responses in muscle afferent fibers of slow conduction velocity to contractions and ischaemia in the cat. J Physiol (Lond) 1983; 342:383-397.
20. Ferreira SH, Nakamura M, Castro MSA. The hyperalgesic effects of prostacyclin and prostaglandin E2. Prostaglandins 1978; 16:3 1-37.
21. Brodie GN. Indomethacin and bone pain (letter). Lancet 1974; 1:1160.
22. Powels TJ, Clark SA, Easty DM, Easty GC, Neville AM. The inhibition by aspirin and indomethacin of osteolytic tumor deposits and hypercalcaemia in rats with Walker tumour and its possible application to human breast cancer. Br J Cancer 1973; 28:3 16-322.
23. Stoll BA. Indomethacin and breast cancer (letter). Lancet 1973; 2:384.
24. Horton JE, Raisz LG, Simmons HA, Oppenheim JJ, Mergenhagen
313~84-95.
1984; 23-52.
1527-1 529.
1986; 59-81.

2214 CANCER June 1 Supplement 1989 Vol. 63
SE. Bone resorbing activity on supernatant fluid from cultured human peripheral blood leukocytes. Science 1972; 177:793-795.
25. Newman PP. Visceral Afferent Functions ofthe Nervous System. London: Arnold, 1974; 1-273.
26. Leek BF. Abdominal visceral receptors. In: Neil E, ed. Handbook of Sensory Physiology, vol 3. Berlin: Springer-Verlag, 1972; 1 13- 160.
27. Learmouth JR. A contribution to the neurophysiology of the uri- nary bladder in man. Brain 1931; 54:147-176.
28. McLellan AM, Goddell H. Pain from the bladder, ureter, and kidney pelvis. Res Public Assoc Res Nerv Mental Dis 1943; 23:252-262.
29. Sinclair DC, Weddel G, Feindel WH. Referred pain associated phenomena. Brain 1948; 7 1 : 184-2 1 I .
30. Head H. On disturbances of sensation with especial reference to pain of visceral disease. Brain 1893; 16:l-132.
3 I . Milne RJ, Foreman RD, Giesler GJ, Willis WD. Convergence of cutaneous and pelvic visceral nociceptive inputs onto primate spinothal- amic neurons. Pain 1981; 11:163-183.
32. Wall PO. Cancer pain: Neurogenic mechanisms. In: Fields HL, Dubner R, Cervero F, eds. Proceedings of the Fourth World Congress on Pain: Advances in Pain Research and Therapy, vol. 9. New York Raven Press, 1985; 575-587.
33. Culp WJ, Ochoa J. Abnormal Nerves and Muscles as Impulse Generators. New York: Oxford University Press, 1982; 1-764.
34. Albe-Fessard D, Condks-Lara M, Sanderson P, Levante A. Ten- tative explanation of the special role played by the areas of paleospi- nothalamic projection in patients with deafferentation pain syndromes. In: Kruger L, Liebskind JC, eds. Neural Mechanisms of Pain: Advances in Pain Research and Therapy, vol. 6. New York Raven Press, 1984;
35. Tasker RR, Tsuda T, Hawrylyshyn P. Clinical neurophysiological investigation of deafferentation pain. In: Bonica JJ, Lindblom U, Iggo A, Jones LE, Benedetti C, eds. Proceedings of the Third World Congress on Pain: Advances in Pain Research and Therapy, vol. 5. New York Raven Press, 1983; 718-738.
36. Tasker R. Deafferentation. In: Wall PD, Melzack R, eds. Textbook of Pain. New York: Churchill Livingstone, 1984; 119-132.
37. Nathan PW. Pain and the sympathetic system. JAuton Nerv Syst
38. Ghostine SY, Comair YG, Turner DM, Kassell NF, Azar CG. Phenoxybenzamine in the treatment of causalgia: Report of 40 cases. J Neurosurg 1984; 60:1263-1268.
39. Walker AE, Nulson F. Electrical stimulation of the upper thoracic portion of the sympathetic chain in man. Arch Neurol Psychiatr 1948;
40. Devor M. Nerve pathophysiology and mechanisms of pain in causalgia. JAuton Nerv Syst 1983; 7:371-384.
41. Roberts WJ. A hypothesis on the physiological basis for causalgia and related pain. Pain 1986; 24:297-311.
42. Cervero F, Iggo A. The substantia gelatinosa of the spinal cord A critical review. Brain 1980; 103:717-772.
43. Price DD, Dubner R. Neurons that subserve the sensory-discrim- inative aspects of pain. Pain 1977; 3:307-338.
44. Yaksh TL, Hammond DL. Peripheral and central substrates in- volved in the rostrad transmission of nociceptive information. Pain 1982;
45. Light AR, Per1 ER. Differential termination of large-diameter and small-diameter primary afferent fibers in the spinal gray matter as in- dicated by labeling with horseradish peroxidase. Neurosci Lett 1977; 6:
46. Ralston HJ. Fine structure of laminae I, 11, and 111 ofthe macaque spinal cord. J Comp Neurol 1979; 184:619-642.
47. Ralston HJ. The fine structure of laminae IV, V, and VI of the macaque spinal cord. J Comp Neurol 1982; 212:425-443.
48. Mehler WR, Fefeman ME, Nanta WJ. Ascending axon degen- eration following antero-lateral cordotomy: An experimental study in the monkey. Brain 1960; 83:718-751.
49. Melzak R, Wall PD. Pain mechanism: A new theory. Science
167-182.
1983; 7:363-370.
5:559-560.
13~1-85.
59-63.
1965; 150:971-978.
50. Wall PD, Sweet WH. Temporary abolition of pain in man. Science
5 1. Meyer GA, Fields HL. Causalgia treated by selective large fibre stimulation of peripheral nerve. Brain 1972; 95: 163-168.
52. Lee KO, Chung JM, Willis MD. Inhibition of primate spinothal- amic tract cells by transcutaneous electrical nerve stimulation. J Neu- rosurg 1985; 62:276-287.
53. Krainick JV, Thoden V. Dorsal column stimulation. In: Wall PD, Melzack R, eds. Textbook of Pain. New York Churchill-Livingstone,
54. Dubner R, Bennett GJ. Spinal and trigeminal mechanisms of nociception. Annu Rev Neurosci 1983; 6:381-418.
55. Goebel S, Hockfield S, Ruda MA. Anatomic similarities between medullary and spinal dorsal horns. In: Kawamura Y, Dubner R, eds. Oral Facial Sensory and Motor Functions. Tokyo: Quintessence, 1981;
56. Macdonald DR, Strong E, Nielsen S, Posner JB. Syncope from head and neck cancer. J Neurooncol 1983; 1:257-267.
57. Head H, Holmes G. Sensory disturbances from cerebral lesions. Brain 1911; 34:102-125.
58. Marshall J. Sensory disturbances in cortical wounds with special reference to pain. J Neurol Neurosurg Psychiatry 195 I; 14: 187-204.
59. Penfield W, Boldrey E. Somatic motor and sensory representation in the cerebral cortex of man as studied by electrical stimulation. Brain
60. Casey KL. Clinical evidence for cortical independence of posterior lateral thalamic neurons mediating the sensory-discriminative component of pain in humans (Abstr). American Pain Society, Fifth General Meeting, 1985; 91.
6 1. Kenshalo DR, Isensee. 0. Responses of primate SI cortical neurons to noxious stimuli. J Neurophysiol 1983; 50: 1479-1496.
62. Young GB, Blume WT. Painful epileptic seizures. Brain 1983;
63. Bausbaum AI, Fields HF. Endogenous pain control mechanisms: Review and hypothesis. Ann Neurol 1978; 4:451-462.
64. Bausbaum AI. The generation and control of pain. In: Rosenberg RN, ed. The Clinical Neurosciences, vol. 5. New York: Churchill-Liv- ingstone, 1983; 301-324.
65. Duggan AW, North RA. Electrophysiology of opioids. Pharmacol
66. Fields HL, Heinricher MM. Anatomy and physiology of a noci- ceptive modulatory system. Philos Trans R Soc Lond [Biol] 1985; 308:
67. Getto CJ, Sorkness CA, Howell T. Antidepressants and chronic non-malignant pain: A review. JPain Sympt Manag 1987; 2:9-18.
68. Feinmann C. Pain relief by antidepressants: Possible mode of action. Pain 1985; 23:l-8.
69. Watson CP, Evans RJ, Reed K et al. Amitriptyline versus placebo in postherpetic neuralgia. Neurology 1982; 32:67 1-673.
70. Botney M, Fields HL. Amitriptyline potentiates morphine anal- gesia by a direct action on the central nervous system. Ann Neurol1983; 13: 160-164.
7 1. Spiegel K, Kalb R, Pasternak GW. Analgesic activity of tricyclic antidepressants. Ann Neurol 198 I; 54:45 1-467.
72. Yaksh TL, Reedy SVR. Studies in the primate on the analgetic effects associated with intrathecal actions of opiates, alpha-adrenergic agonists and baclofen. Anesthesiology 198 1; 54:45 1-467.
73. Coombs DW, Saunders RL, Lachance D et al. Intrathecal mor- phine tolerance: Use of intrathecal clonidine, DADLE, and intraven- tricular morphine. Anesthesiology 1985; 62:358-363.
74. Archer T, Arwestrom E, Jonsson G, Minor PE, Post C. Complete blockade and attenuation of 5-hydroxytryptamine induced analgesia fol- lowing Na depletion in rats and mice. Acta Pharmacol Toxicol 1985;
75. Levy RM, Lamb S, Adams JE. Treatment ofchronic pain by deep brain stimulation: Long-term follow-up and review of the literature. Neurosurgery 1987; 212385493.
1967; 155:108-109.
1984; 701-705.
21 1-233.
1937; 60:389-443.
106:537-554.
Rev 1983; 35:219-281.
36 1-374.
57:255-261.