
Cancer du sein et sujet âgé - Longue Vie et Autonomie · 1 Cancer du sein et sujet âgé Docteur...
43
1 Cancer du sein et sujet âgé Docteur Etienne Brain Oncologie Médicale Hôpital René Huguenin / Institut Curie Saint-Cloud, France [email protected] • 2006: Mrs BON… IR… 84 yo – Previous history: HBP; high blood sugar? – Fully independent, no depression, feels ”better” than most her friends – Husband: 86 yo w/ severe advanced Parkinson, 2 children – Breast self exam T1c N0 M0 left breast – 54 kg (stable)/167 cm, no anorexia, – Treatment: metoprolol, lisinopril, hydrochlorothiazide, atorvastatine • Conservative surgery + axillary lymph node dissection – Invasive ductal carcinoma, 17 mm, SBR II, 8 N- – ER- PgR-, Ki 67 40%, HER2- • Adjuvant strategy – Chemotherapy with anthracylines (GERICO 06)? + XRT • Scoring – Oncologist: PS 0 “Easy! Go for it“ – Geriatrician • Functional status, cognition, nutrition, GDS OK • However! 3 falls < 1 year A frailty revealed…
Transcript of Cancer du sein et sujet âgé - Longue Vie et Autonomie · 1 Cancer du sein et sujet âgé Docteur...

1
Cancer du sein et sujet âgé
Docteur Etienne BrainOncologie Médicale
Hôpital René Huguenin / Institut CurieSaint-Cloud, France
• 2006: Mrs BON… IR… 84 yo– Previous history: HBP; high blood sugar?– Fully independent, no depression, feels ”better” than most her
friends– Husband: 86 yo w/ severe advanced Parkinson, 2 children– Breast self exam � T1c N0 M0 left breast– 54 kg (stable)/167 cm, no anorexia, – Treatment: metoprolol, lisinopril, hydrochlorothiazide,
atorvastatine• Conservative surgery + axillary lymph node dissection
– Invasive ductal carcinoma, 17 mm, SBR II, 8 N-– ER- PgR-, Ki 67 40%, HER2-
• Adjuvant strategy– Chemotherapy with anthracylines (GERICO 06)? + XRT
• Scoring– Oncologist: PS 0 � “Easy! Go for it“– Geriatrician
• Functional status, cognition, nutrition, GDS � OK• However! 3 falls < 1 year
A frailty revealed…

2
• LVEF by MUGA scan normal
• Not in GERICO 06 trial, but OK for the oncology staff!
• The lady “accepted”….
… treatment decision process
• LVEF by MUGA scan normal
• Not in GERICO 06 trial, but OK for the oncology staff!
• The lady “accepted”….
• Central venous access + 1 cycle of AC-like chemo � febrile neutropenia + severe stroke (cardiac arythmia?)
– Chemotherapy stopped– Husband placed in nursing home– Delayed XRT– Recovered with neurological sequelae– Seniors residence– No relapse so far (last visit early 2017 i.e. 95 yo)
… treatment decision process & respect

3
2009
2050
http://www.un.org/esa/population/publications/ageing/ageing2009chart.pdf
Projected number of cancer cases for 2000–2050 by a ge group (<45, 45–64, 65–84, 85+) based on projected census population estimates and delay-adj usted SEER-17 cancer incidence rates
Hayat The Oncologist 2007;12:20-37©2007 by AlphaMed Press
Incidence of cancer from 2010 to 2030 (Smith JCO 2009)• +11% < 65 yo• +67% > 65 yo

4
China has the largest elderly population (92 millio n)… but this is only 7% of the Chinese population!!!
www.worldmapper.org
Binder-Foucard INCa report 2013

5
De Angelis Lancet Oncol 2013
Relative survival accounts for mortality from causes other
than the relevant cancer, which can vary widely between
countries
Breast
Ovary
20071991 2002
2013 2015

6
• Most common shortcut in statistics
“1 in 8 women will develop BC in their lifetime”instead of
“If everyone lived beyond the age of 70, 1 in 8 of those women would get or have had BC”
• Since BC risk increases w/ age, lifetime risk changes depending on age
– Age 20-29 1 in 2,000– Age 30-39 1 in 229– Age 40-49 1 in 68– Age 50-59 1 in 37– Age 60-69 1 in 26– Ever 1 in 8
Worldwidebreastcancer.com
Current dilemna and extreme positions
1. Therapeutic nihilism– Elderly patients do not receive any treatment
2. The intermediate position?– Elderly patients may benefit from treatments
3. Blind therapeutic enthusiasm– Elderly patients receive futile/non beneficial
treatments
� Place and role of geriatrician and oncologistPelike from Attica 480–470 BC
Musée du Louvre

7
Phénotype
Plus de formes hormonosensibles (RH+)Moins de formes agressives (triple négatif, HER2+++)
BC biology according to age
de Kruijf Mol Oncol 2014, Jenskins Oncologist 2014

8
Dépistage
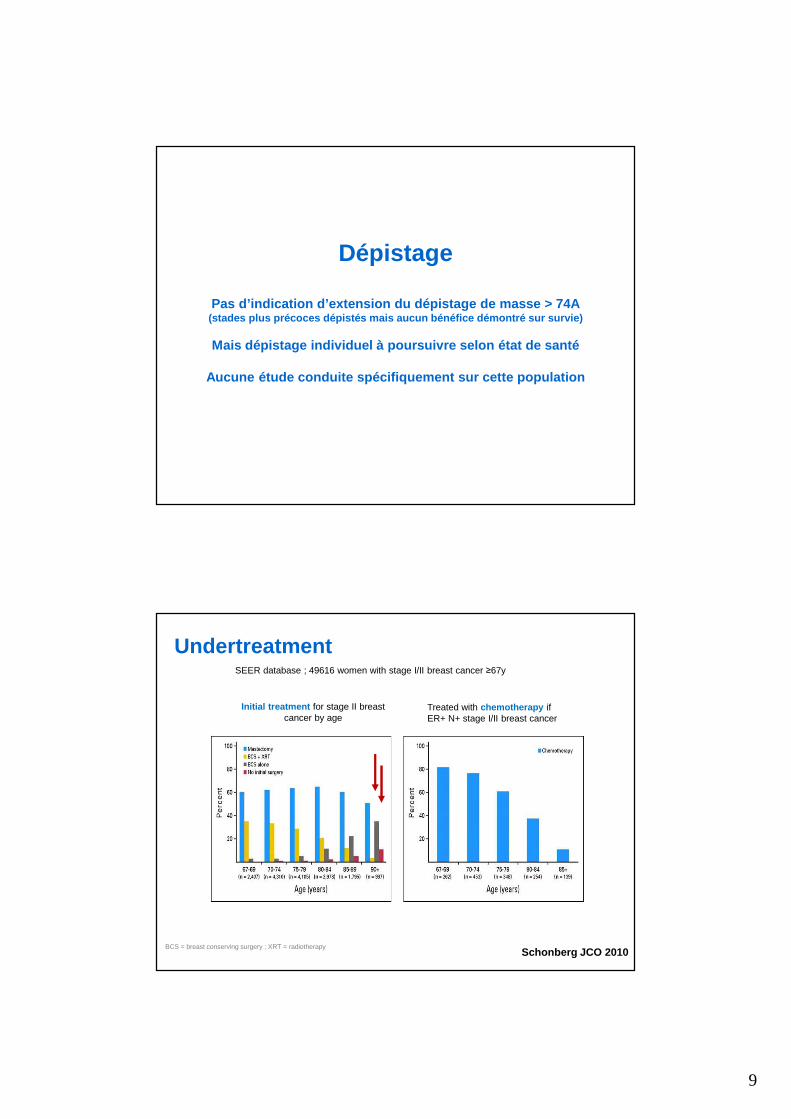
Pas d’indication d’extension du dépistage de masse > 7 4A(stades plus précoces dépistés mais aucun bénéfice démont ré sur survie)
Mais dépistage individuel à poursuivre selon état de sant é
Aucune étude conduite spécifiquement sur cette population
Breast-cancer screening > 70?
16
Warner NEJM 2011; Royce JAMA 2014; Gross JAMA 2014
Age(yr)
Nb of trial(s) Relative riskof death (95%CI)
60-69 Malmö &Ostergöland
0.68 (0.54-0.87)
70-79 Ostergöland 1.12 (0.73- 1.72)
75+: YES YOU CAN, but– No mass screening– Depends on life expectancy
9
Dépistage
Pas d’indication d’extension du dépistage de masse > 7 4A(stades plus précoces dépistés mais aucun bénéfice démont ré sur survie)
Mais dépistage individuel à poursuivre selon état de sant é
Aucune étude conduite spécifiquement sur cette population
Treated with chemotherapy ifER+ N+ stage I/II breast cancer
Initial treatment for stage II breastcancer by age
SEER database ; 49616 women with stage I/II breast cancer ≥67y
BCS = breast conserving surgery ; XRT = radiotherapy
Undertreatment
Schonberg JCO 2010

10
Breast cancer mortality
Other cause mortality
• Univariate HR 1.66 (95% CI 1.34-2.06), p<0.001
• Multivariable HR 1.63(95% CI 1.23-2.16), p<0.001
Cau
sesp
ecifi
cde
ath
Substudy from TEAM trial (adjuvant exemestane)
Age <65y Age ±75yAge 65 – 74y
Schonberg JCO 2010, Van de Water JAMA 2012
Under & overtreatment
Kendal Cancer 2008
Competing causes for mortality
11
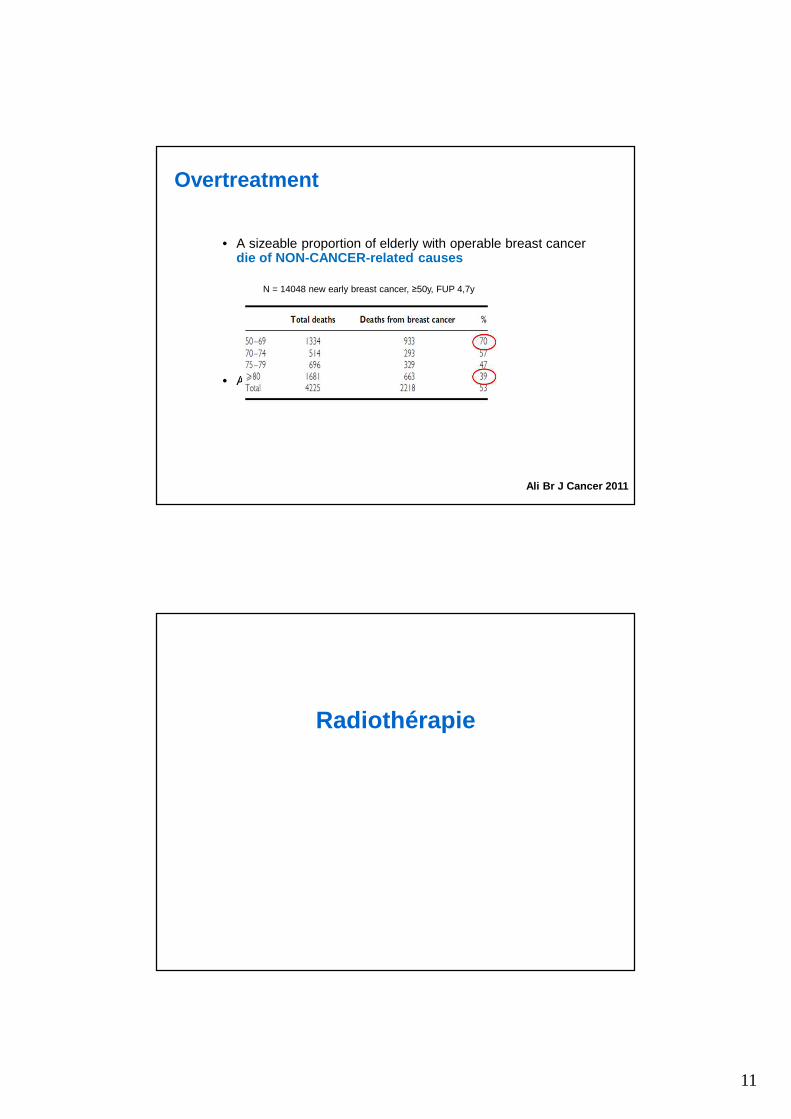
• A sizeable proportion of elderly with operable breast cancer die of NON-CANCER-related causes
• Absolute benefit of treatments is lower
N = 14048 new early breast cancer, ≥50y, FUP 4,7y
Overtreatment
Ali Br J Cancer 2011
Radiothérapie

12
Hughes J Clin Oncol 2013
After BCS: TAM vs XRT + TAM (CALGB 9343)
334/636 deaths(21 i.e 6.3% due to BC)
Radiotherapy
• Omission if pT1 ER+? (NCCN)– According to life expectancy– > 80 yo, multi-morbidities, good compliance to endocrine treatment?
• Low risk patients– Once-per-week fraction schedule (Whelan regimen)
– Accelerated partial breast irradiation (APBI)• Larger radiation doses given to the localized tumour bed (instead of to the
entire breast)
� Spare extensive and burdensome transportations
But don’t neglect the psychological burden of recurrenc e!
Khan Semin Radiat Oncol 2012
13
Les traitements
Le cancer du sein de la femme âgée se prête volontiers à
l’hormonothérapie car il est plus souvent RH+
Mais entre anti-aromatase (letrozole/FEMARA, anastro zole/ARIMIDEX, exemestane/AROMASINE et anti-oestrogène (tamoxifène) ,
la question de l’observance est majeure (et donc l’aju stement à la tolérance)
En contexte adjuvant/précoce, l’hormonothérapie se do nne 5 ans en général (discussion sur les extensions au delà)
En contexte métastatique, l’hormonothérapie est le tra itementgénéralement de première intention (phénotype RH+ fré quent)

14
• TAM / 0
15105
60 %
50 %
40 %
30 %
20 %
10 %
rech
ute
26,5
38,3
45,0
24,7
15,1
33,2
contrôle
TAM 5A
• IA / TAM
Réduction du risque de rechute
Bénéfice absolu à 10
ans
RO+ 41 % 13,6 %
Réduction du risque de rechute
Bénéfice absolu à 10
ans
RO+ Post-MP
20 % 5 %
AI 5A
COMPLIANCEis the issue!!!
TAM AINeurocognition
Sexuality
Hot flushes
Thrombosis & embolism
Uterus cancer
Gynecological tractus
Vaginal discharge
Cataract
Arthralgias & myalgias
Osteoporosis
Fractures
Dryness
Cardiovascular
Lipid profile
?

15
Copyright © American Society of Clinical Oncology
Morales, L. et al. J Clin Oncol; 26:3147-3152 2008
Getting a grip on aromatase inhibitor–associated arthr algiasDawn L. Hershman
724 patients � 265 (40%) 65+ � 164 (23%) 70+
Baselga. N Engl J Med 2012Pritchard. Clin Breast Cancer 2013
70+ vs <70Similar efficacy & incidences of AEs
More on-treatment deathsBut
Prior chemo x 2 if <70

16
• European phase IIIb• Expanded-access multicenter trial• 2133 patients, 26% 70+• Key AEs: stomatitis, fatigue, anemia, NIP
Jerusalem. Ann Oncol 2016
<70 70+
AE-related treatment discontinuations (%) 13 24
Median duration of exposure (months) 5 4
Dose reduction/interruption (%) 27/54 38/61
Stomatitis any grade/3-4 (%) 52/8 56/12
Asthenia any grade/grade 3-4 (%) 21/3 29/6
Decreased appetite (%) 14 22
Hyperglycemia grade 3-4 (%) 2 5
NIP (%) 9 11
La chimiothérapie, c’est plus compliqué…
Car index thérapeutique plus étroit que l’hormonothéra pie
Des doses généralement ajustées (inférieures)

17
Physiological variations x PK & PD
Mechanism Consequences
Absorption
Gastric dumping and secretions �
Absorption of proteins, vitamins and drugs �
Metabolism
Hepatocytes, blood flow, CYP P450 activity �
Interactions (CYP P450)
Protein synthesis, (de-) activation of drugs and carcinogens �
Distribution H2O, albumin, Hb �
Vd hydrosolubles drugs �
Vd liposolubles drugs �
ExcretionGFR, tubular filtration �Biliary excretion �
Renal elimination of drugsexcreted by kidney �
Biliary elimination �
Balducci. Oncologist 2000; Wildiers. Clin Pharmacoki net 2003; http://www.ema.europa.eu
Les grands médicaments
• Anthracyclines (adriamycine, épirubicine, schémas FEC 100 ou AC)– Myélotoxicité– Cardiotoxicité
• Alkylants (cyclophosphamide/Endoxan®, schéma FEC 100 ou AC)– Myélotoxicité– Attention à la fonction rénale
• Taxanes (docetaxel/Taxotère®, paclitaxel/Taxol®)– Myélotoxicité– Neuropathie– Onycholyse– Rétention hydrique
• Antimétabolites (5-flurorouracile, forme orale = capecitabine/Xeloda®)– Syndrome mains pieds– Diarrhée
34

18
• Myelosuppression : greater in older patients– Lower threshold (<20%) for primary prophylaxis of febrile neutropenia w/ G-CSF
• Cardiomyopathy : more common in older patients– Certainly if underlying cardiac disease
• Mucositis, delayed nausea and vomiting• Peripheral or central neurotoxicity
– Debilitating and interfering w/ functionality and independence– !Concomitant problems that affect mobility and function (e.g. arthritis)
• Renal function : declines with age! ~ 1 mL/min/year – Creatinineserum = insufficient! Cockcroft-Gault CLcreatinine = better but not as
accurate as in younger patients � MDRD/CDK-EPI = best in elderly?
Benefit/risk balance of chemotherapy is narrower than other treatments, especially in elderly
• CPA & renal function
• Capecitabine– 750-1000 mg/m² x 2/d 2 wk/3
Gelman. J Clin Oncol 1984; Crivellari. J Clin Oncol 2 000; Bajetta. J Clin Oncol 2005
CMF
Chemotherapy � Specific doses!!!
19
0
0.2
0.4
Cumulative proportion with event
0.6
0.8
1.0Hazard ratio (>65:£65) = 2.2595% CI of (>65: £65) = (1.04–4.86)Log rank p-value = 0.029Wilcoxon p-value = 0.78
0 200 300 400 700 800 900 1000Cumulative dose of doxorubicin (mg/m 2)
600500100
468172
345110
29692
10328
61
41
203
5912
431151
£65*>65*
*Patients at risk
£65
>65
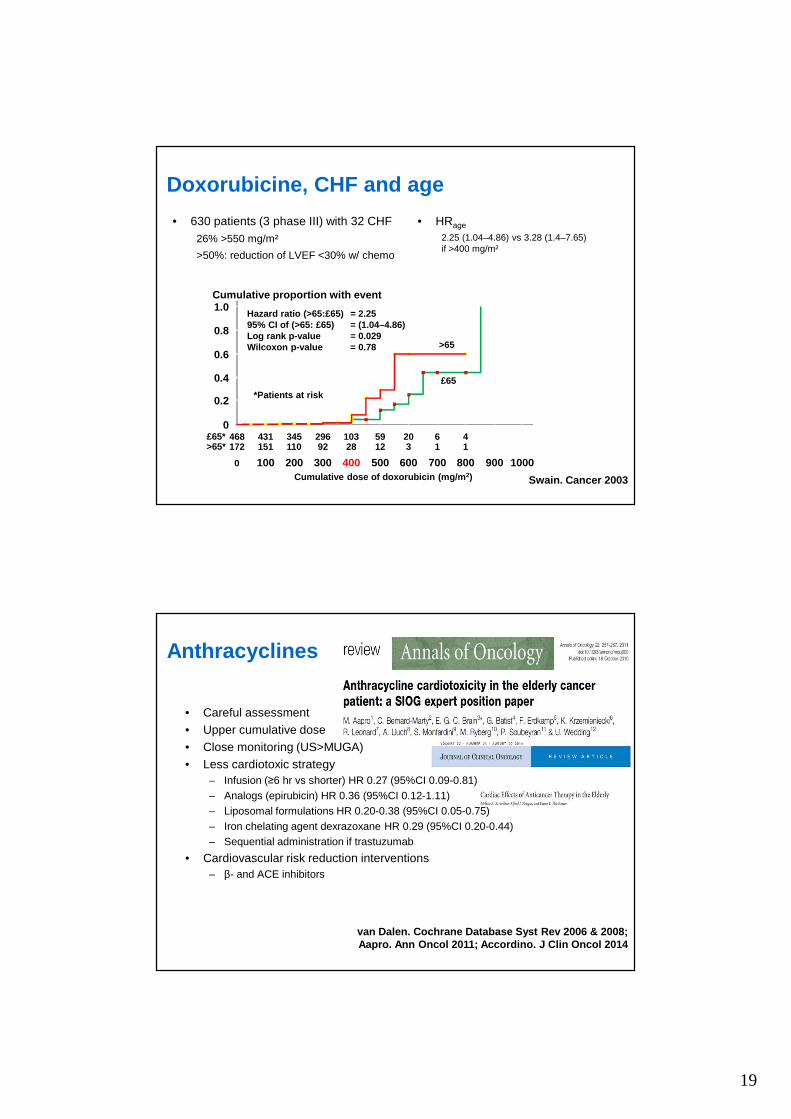
• 630 patients (3 phase III) with 32 CHF26% >550 mg/m²
>50%: reduction of LVEF <30% w/ chemo
Doxorubicine, CHF and age
• HRage
2.25 (1.04–4.86) vs 3.28 (1.4–7.65) if >400 mg/m²
Swain. Cancer 2003
van Dalen. Cochrane Database Syst Rev 2006 & 2008;Aapro. Ann Oncol 2011; Accordino. J Clin Oncol 2014
• Careful assessment• Upper cumulative dose• Close monitoring (US>MUGA)• Less cardiotoxic strategy
– Infusion (≥6 hr vs shorter) HR 0.27 (95%CI 0.09-0.81)– Analogs (epirubicin) HR 0.36 (95%CI 0.12-1.11)– Liposomal formulations HR 0.20-0.38 (95%CI 0.05-0.75)– Iron chelating agent dexrazoxane HR 0.29 (95%CI 0.20-0.44)– Sequential administration if trastuzumab
• Cardiovascular risk reduction interventions– β- and ACE inhibitors
Anthracyclines

20
• 2 cornerstones– Paclitaxel <80 mg/m²qw– Docetaxel q3w but not standard @ 100 mg/m²!
• Same pharmacokinetics , but increased risk of neutropenia ± febrile if 65+– q3w 75 mg/m² grade 3-4 ANC/FN: 63%/16% vs 30%/0%– qw 35 mg/m² > 50% grade ≥ 3 � RD: 26 mg/m²– q2w 50 mg/m² GERICO-04
– Grade 3-4 neurosensory/motor toxicity 28%/14% (vs <18%/<8% if <65)
• Nab-paclitaxel– Efficacy comparable with solvent-based taxanes
– No need for steroid premedication
Taxanes
Del Mastro. Ann Oncol 2005;ten Tije. J Clin Oncol 2005; Girre. Ann Oncol 2008; Biganzoli. Cancer Treat Rev 2016
Oral chemotherapy
PROS CONS
ConvenienceLess need to visit clinic
Reduced complianceFailure to start therapy;
missed doses; overdosage
Greater feeling of control Patient persists takingdrug despite AEs
No difficulty w/ IVadministration
No AE w/ central line
Less cost to health caresystem and/or patient
Patients are lesstied to hospital
Less support frommeeting fellow patients
Rousseau. CROH 2010; Biganzoli. Eur J Cancer 2015

21
La chimiothérapie adjuvante « marche » si on est attentif aux
effets secondaires…
DFS
OS
• CALGB (1975-1999)
• 4 randomized trials
• 6487 pts> 65 yo 542 (8%)> 70 yo 159 (2%)
• Results– Benefit identical– Toxicity careful!!
• Toxic deaths 1.5%
Adjuvant chemo for breast cancerAll
All
≤50
≤50
≥65
≥6551-64
51-64
Muss JAMA 2005

22
Doxorubicin, CHF and age
• SEER 1992-2002: 43,338 women 66-80 years, no CHF history– stage I to III BC, chemotherapy vs no– AC: younger, fewer comorbidities, advanced (p=.001)– CHF10 years (%)
Pinder J Clin Oncol 2007
ACN =
4,712
OtherchemoN = 3,921
No chemo
N = 34,705
38.4 32.5 29• 66-70 years HR 1.26 (95% CI, 1.12-1.42) if AC• 71-80 years no impact of CT type
Baseline HR (95%CI)
Age (decade)
1.79
(1.66-1.93)
Black 1.40
(1.30-1.50)
Trastuzumab
1.46
(1.21-1.77)
Hypertension
1.45
(1.39-1.52)
Giordano* Elkin
No. total
No. w/CT
I-III, ∀ ER , 65+41,390
4,500
I-III, ER-, 66+5,081
1,711
pN ER HR (95% IC) HR (95% IC)pN0 ∀ 1.05 (0.85-1.31) NA
pN+ + 1.05 (0.85-1.31) NA
both - NA 0.85 (0.77-0.95)
pN+ - 0.72 (0.54-0.96) 0.76 (0.65-0.88)
pN+ > 70 yo - 0.74 (0.56-0.97)
Adjuvant chemotherapy and mortality
Adjuvant chemo is useful FIRST
in ER-, pN0 or pN+, even > 70 yo
*: BC specific mortality
Giordano & Elkin J Clin Oncol 2006

23
All
ER-
ER+
DFS OSCALGB/CTSU 49907(AC or CMF vs X)
Muss NEJM 2009
GERICO 06 (EUDRACT N° 2005-000069-20, PHRC national 2005)
MC MC MC MC XRT
ADLTolerance
CGAADL + MNA +MMS + GDS +
CIRSG
QLQ-C30Willingness
CGAADL + MNA +MMS + GDS +
CIRSG
QLQ-C30WillingnessTolerance
CGAADL + MNA +MMS + GDS +
CIRSG
QLQ-C30WillingnessTolerance
1 & 2 yearDFS & OS
ADLTolerance
ADLTolerance
± trastuzumab
if HER2+++
trastuzumabif HER2+
q3w q3w q3w
4 cycles of “AC-like” chemoIn MC, M stands for liposomal non pegylated doxorub icin

24
1. Febrile neutropenia 15%2. Risk of denutrition 15% vs 38%3. Impact on QoL (social & role functioning)4. Cardiac tolerance of trastuzumab5. No palmar plantar erythrodysesthesia6. DFS3A 85%
Copyright © American Society of Clinical Oncology
Jones, S. et al. J Clin Oncol; 27:1177-1183 2009
Fig 1. Disease-free survival (DFS) and overall surv ival (OS) (A) DFS by treatment; (B) DFS by treatmen t and age; (C) OS by treatment: 1 day; (D) OS by trea tment and age

25
Targeted treatments
Lack of specific data!But clinical evidence for benefit
Tyrosinekinase
domain
Ligand-bindingdomain
Erb-B1EGFRHER1
Erb-B2HER2/neu
Erb-B3HER3
Erb-B4HER4
Trans-membrane
TGF-αEGFEpiregulinBetacellulinHB-EGFAmphiregulin
Heregulin(neuregulin-1)
Heregulin(neuregulin-1)EpiregulinHB-EGFNeuregulins-2,3,4
Domaine de liaison
ATP
Domaine C Terminal(sites de phosphorylation) Transduction
du signal
Région trans-membranaire
Domaine extra-cellulaire
Domaine intra-cellulaire
Substrats deTyrosine Kinase
phosphorylés
Noyau
Membranecellulaire
LigandDomaineTyrosineKinase
Structure et fonction de l’EGF-R

26
The incidence of CHF from the Finnish Herceptin Stud y (FINHER), Herceptin Adjuvant trial (HERA), Breast Cancer International Collaborative Group trial 006 (006) with TCH and AC-TH analyzed separately, the No rth
Central Cancer Treatment Group trial 9831 (N9831), and NSABP B-31 (B-31).
Bird B R H , Swain S M Clin Cancer Res 2008;14:14-24
©2008 by American Association for Cancer Research
• NSABP B31– Age
– 2% < 50 yo vs 5.4% > 60 yo– LVEF > 4 AC
– 12% if LVEF < 55%– Concomitant > sequential– Hypertension comedications
• B31/N9831– 6.7% pts who had completed AC had a lower LVEF or
developed cardiac symptoms preventing the initiation of TZT
– 1/3 pts who started TZT discontinued it: 4.7% with symptomatic CHF, 14.2% with confirmed asymptomatic decline in LVEF, and the rest for noncardiac reasons
• SEER database• 2,028 patients ≥ 66, stage I-III, 2005-2009, trastuzumab
– 71.2% < 76
– 66.8% w/o comorbidities (Charlson)
– 85.2% w/ chemotherapy
– 81.7% w/ complete trastuzumab treatment (> 9 months)
– Factors correlated w/ incomplete treatment• Age 80+ vs 66-70 OR 0.40 (0.30-0.55)• Comorbidities 2 vs 0 OR 0.65 (0.49-0.88)
Vaz-Luiz. J Clin Oncol 2014

27
- 2 gr 3 LVSD (0.5%) (95% CI, 0.1%-1.8%)- 13 significant asymptomatic LVEF decline (3.2%) (95% CI, 1.9%-5.4%)
Tolaney NEJM 2015
- Adjuvant! Online not accurate in older patients- Predict quite accurate for OS prediction
Standard decision tools
de Glas Lancet Oncol 2014 & Br J Cancer 2016

28
General recommendations for adjuvant chemo & tratsuzumab in elderly
• Focus on ER-
• Regimen– Validated 4 AC, 6 CMF– Option 4 TC– Capecitabine no– Docetaxel qw no– Sequential regimen no data– Liposomal doxorubicin ?
• Primary prophylaxis of febrile neutropenia w/ G-CSF
• No restriction on trastuzumab if chemo indicated– 4 TC + trastuzumab– Paclitaxel qw x 12 + trastuzumab– TCH x 6??? (carboplatin AUC 6!)
Miles Breast Cancer Res Treat 2013
Pertuzumab

29
Verma N Engl J Med 2013Dieras J Clin Oncol 2014
Barrios ASCO 2015
T-DM1
Kamilla 194 pts 65-69, 78 pts 70-74, 120 pts 75+
%< 70
N = 2,018
70+
N = 233*
HBP gade ≥ 3 4.2 6.9
Proteinuria grade ≥ 3 1.5 4.0
ATE (A or V) 3.3 2.9
Stop for toxicity
ATE
CHF
15
1.8
0.3
23
2.9
0.6
HTN 1.8 2.9
Biganzoli. Annals Oncol 2011
ATHENA: CT w/o anthracyclines + beva
*175 (7.8%) 70+, 51 (2.3%) 75+, 7 (0.3%) 80+
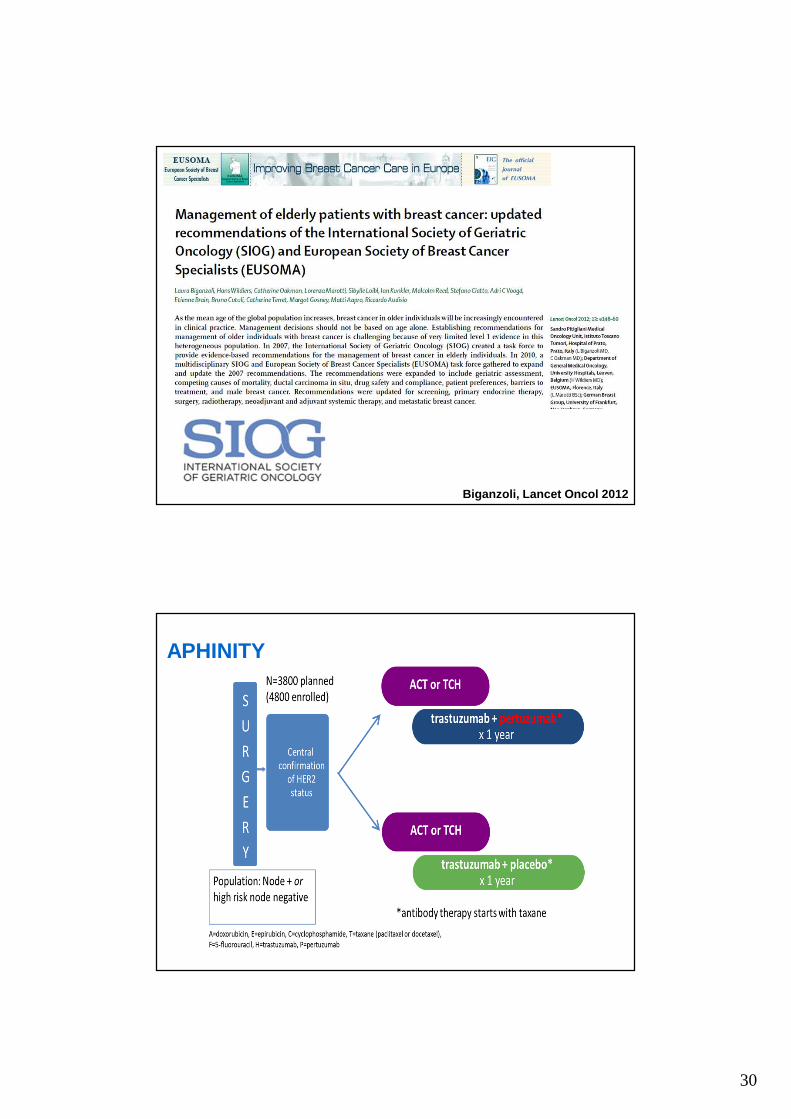
30
Biganzoli, Lancet Oncol 2012
APHINITY

31
80 pts HER2+ MBC≥ 70 Years
(≥65/≥60y with co-morbidity)
Pertuzumab +
Trastuzumab
Pertuzumab + Trastuzumab +metronomic CT
® 1:1 T-DM1
Primary endpointPFS at 6 months of PH or PHM
Pertuzumab 840 mg loading dose, further 420 mg q3w ivTrastuzumab 8 mg/kg loading dose, further 6 mg/kg q3w ivChemotherapy Metronomic chemotherapy: cyclophosphamide 50 mg/d p o continuouslyOn progression Option to have T-DM1 (3.6 mg/kg iv q3w) till progression
PD
Stratification: ER/PgR, previous HER2 treatment, G8Secondary endpointsOS, BCSS, toxicity, RR (RECIST v1.1), HRQoL, evolution of GA during treatment
EORTC 75111-10114(Co-PI Hans Wildiers & Etienne Brain)
32
Problèmedémographique
Rechercheclinique
peureprésentée
Mortalitéspécifique
et effetssecondairessignificatifs
Phénomène hétérogène
Espérance de vie ou
pronostic « hors cancer »
?
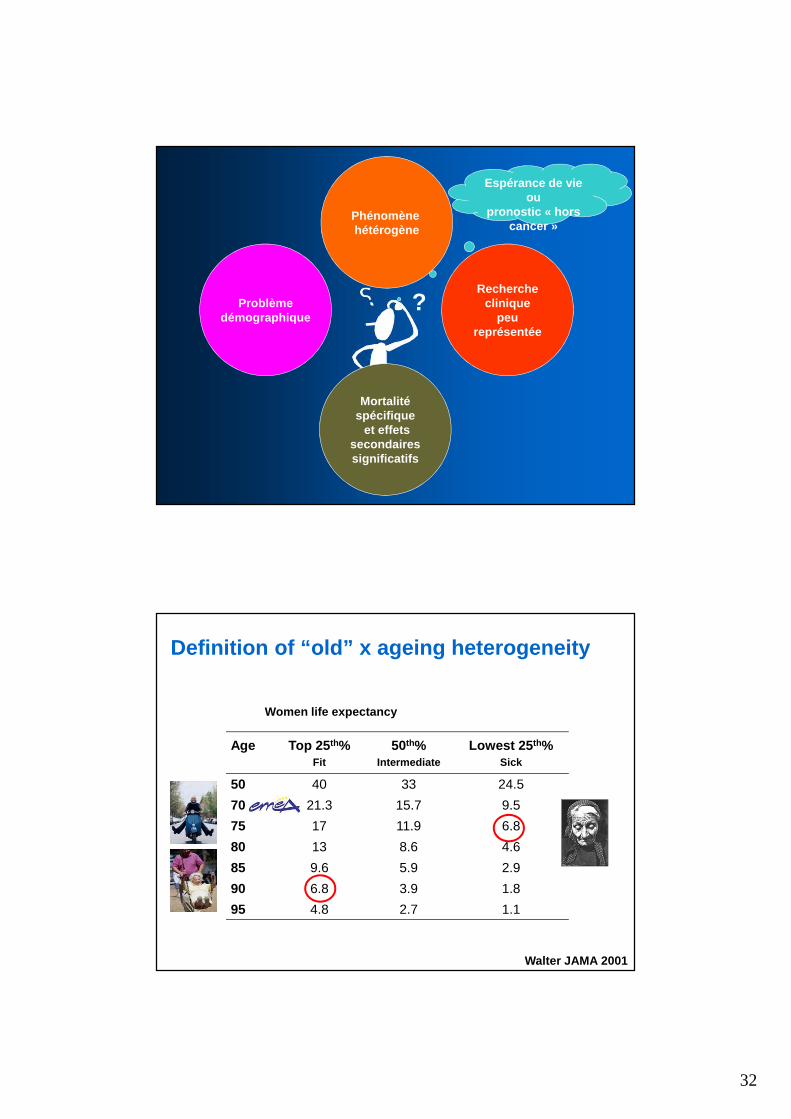
Definition of “old” x ageing heterogeneity
Age Top 25 th%Fit
50th%Intermediate
Lowest 25 th%Sick
50 40 33 24.5
70 21.3 15.7 9.5
75 17 11.9 6.8
80 13 8.6 4.6
85 9.6 5.9 2.9
90 6.8 3.9 1.8
95 4.8 2.7 1.1
Women life expectancy
Walter JAMA 2001

33
Multimorbidities across age
Piccirillo, Critical Rev Oncol Haematol 2008
dementia CHF
solid tumour AIDS
diabetes HBP
Kendal Cancer 2008
Competing causes for mortality

34
Do we have tools?
Comprehensive Geriatric Assessment
Assessment Instrument Administration Prognosis
Dependency, functionalstatus
PS, Activity of Daily Living (ADL), Instrumental ADL
Self administered +
ComorbidityCharlson Comorbidity Index (CCI), Cumulative Illness rating Scale-Geriatric (CIRS-G)
Self- or interviewer-administered or chart-based
+
Economic / social support
Life conditions, relatives, care-givers ?
CognitionFolstein Mini-mental State Examination (MMSE)
Interviewer-administered
+functional status
Depression Geriatric Depression Scale (GDS) Self administered +
Polypharmacy List ?
NutritionMini Nutritional Assessment (MNA), BMI
Interviewer-administered
+
Geriatricsyndromes
Dementia, delirium, falls+
functional status
Mobility/falls Timed-up-and-go-test, Tinetti Performance-tests ?

35
≥ 75 yo1st visit
New cancer or relapse
G8Physician± nurse
≤ 14/17> 14/17
Primary focus on*: systemic treatment?
Decision 1
YESNO
Standard health caresvigilance and geriatrician
sought according to needs
GA
* But not exclusively
Adjusted health cares± MDTB 2 and decision 2Geriatric interventions
1. Streamlining geriatrician time2. Involvement of oncologists3. Impact- Decisions 1 and 2- Geriatric interventions- Day hospital in geriatric oncology
MDTB 1 + geriatrician
Adapted recommendations for patient’s referral for GA at Instit ut Curie
MDTB: multi disciplinary tumor board
• 2006: Mrs BON… IR… 84 yo– Previous history: HBP; high blood sugar?– Fully independent, no depression, feels ”better” than most her
friends– Husband: 86 yo w/ severe advanced Parkinson, 2 children– Breast self exam � T1c N0 M0 left breast– 54 kg (stable)/167 cm, no anorexia, – Treatment: metoprolol, lisinopril, hydrochlorothiazide,
atorvastatine• Conservative surgery + axillary lymph node dissection
– Invasive ductal carcinoma, 17 mm, SBR II, 8 N-– ER- PgR-, Ki 67 40%, HER2-
• Adjuvant strategy– Chemotherapy with anthracylines (GERICO 06)? + XRT
• Scoring– Oncologist: PS 0 � “Easy! Go for it“– Geriatrician
• Functional status, cognition, nutrition, GDS � OK• However! 3 falls < 1 year
A frailty revealed…

36
• 2006: Mrs BON… IR… 84 yo– Previous history: HBP; high blood sugar?– Fully independent, no depression, feels ”better” than most her
friends– Husband: 86 yo w/ severe advanced Parkinson, 2 children– Breast self exam � T1c N0 M0 left breast– 54 kg (stable)/167 cm, no anorexia, BMI 19.4 (<25, 18.5-21)– Treatment: metoprolol, lisinopril, hydrochlorothiazide,
atorvastatine• Conservative surgery + axillary lymph node dissection
– Invasive ductal carcinoma, 17 mm, SBR II, 8 N-– ER- PgR-, Ki 67 40%, HER2-
• Adjuvant strategy– Chemotherapy with anthracylines (GERICO 06)? + XRT
• Scoring– Oncologist: PS 0 � “Easy! Go for it“ !!!– Geriatrician
• Functional status, cognition, nutrition, GDS � OK• However! 3 falls < 1 year
A frailty revealed… and assessed+5
+1+1 +2+2+2
+3+2+1
+1
+0
� Lee 7 ~ 50%� G8 = 13
6 key messages forelderly cancer patients
1. Age and standard approach upfront influence treatment decision in
40% cases but not always in the right direction!
2. Under and over-treament are frequent
3. Access to innovation is unbalanced
4. Geriatric problems are far more frequent than usually believed
– 2/3 impaired G8, > 50% functional dependence, >10% cognitive
dysfunctions, 20% depression, > 40% significant comorbidities, > 50%
risk of malnutrition, polypharmacy, etc.
5. � Comprehensive Geriatric Assessment CGA
– Brings to clinicians new information in > 2/3 cases
– Modifies clinical decision in 20-25% cases (function & nutrition)
6. Competing risks for mortality � call for a certain degree of assessment
of life expectancy to balance treatment decision
� need for specific researchCaillet J Clin Oncol 2011; Kenis Ann Oncol 2013; Bode EBCC9 2014, abstract 414

37
8842 studies found for :Open Studies | Interventional Studies | cancer | Adult, Senior | Phase 1, 2, 3
www.clinicaltrials.gov
298 studies found for:older OR elderly | Open Studies | Interventional Studies | cancer | Senior | Phase 1, 2, 3
www.clinicaltrials.gov
3.4%!!!

38
Agent Name Approval N Age ≥ 65 N Age ≥ 75
Palbociclib 2/201537 44% 8 10%86 25% --
Everolimus 7/2012 290 40% 109 15%Pertuzumab 6/2012 60 15% 5 1%Eribulin mesylate 11/2010 121 15% 17 2%
Lapatinib 1/201034 17% 2 1%
282 44% 77 12%
Ixabepilone 10/200745 10% 3 <1%32 13% 6 2.5%
Package Insert, “Geriatric Usage” section
Few older adults included in registration studies!Breast cancer as an example
Courtesy to Arti Hurria (adapted)
GERICO ≥ 2,000 patients2002 Creation (F Pein & AC Braud) Age Phase Primary endpoint N Ancillary Publication
2002 G-01: X+VNR PO breast, lung, prostate 70+ II ADL 80 PK CROH 2010
G-02: CT XELOX CCR M+ 70+ II ADL 60 PK JGO 2011
2004 G-03: per op brachyXRT breast < 3 cm pN0 70+ IIFaisabilité
Qualité40 Cost Brachy 2013
2005 G-04: CT TxT q2w breast M+ 70+ II IADL 27/60 NA Poster
G-05: CT TxT q2w NSCLC M+ 70+ II IADL 5/60 NA Poster
2006 G-06: CT adjuvant anthra (MC) breast ER- 70+ II ADL 40 Will CROH 2010
2008 G-07: validation CRASH 70+ Cohorte Composite NA NA NA
Sarcoma Aegide + G-CSF 70+ II R Composite NA NA NA
2009 G-09: breast M+ HER2+++ X + lapatinib 70+ II Composite 4/52 NA Poster
Retrospective L1 CT M+ breast (Bergonié) 75+ Cohorte Description 500 NA CROH 2001
DOGMES L1 DXR lipos (GINECO) 70+ II RR 60 NA EJC 2012
2010 G-10/GETUG P-03: CT TxT prostate + PK 75+ II R Composite 66/60 :144 PK Poster
PRODIGE 20 (G-08): CT ± beva CCR M+ 75+ IIR/III Composite 102 CTC/RX Pending
2011 ASTER 70s/G-11/PACS 10 : CT adj breastRH+ HER2- GGI
70+ IIIOS
(competing risks)897/1,080
1,671/2,000BiomarkersCost, Will
Poster, oral
2012 ELAN (PAIR ORL, GORTEC/GERICO) 70+ Multiple OS 380 NA Poster
SHS (cognition, acceptability, etc.) 70+ SHS Qualitative res NA Poster
2013 Frail lung (GFPC/GERICO), poly vs mono 70+ III OS + QoL 252 NA NA
2014UCGI-30 (G-12) XRT/CTneo vs XRT rectumOSAGE (Besançon)
75+IIII/II
R0 + IADLMTD, RR EOT
42054
2014 Pain (intergroupe soins support AFSOS) 70+ Cohorte Description > 1,000
2015 ASTER 2/3 + EORTC/BIG 70+ III Outcome + QoL 1,200/2,500

39
Protocol ASTER 70sGERICO 11 / PACS10
Adjuvant systemic treatment for oestrogen-receptor ( ER)-positive HER2-negative breast carcinoma in women ov er 70
according to Genomic Grade (GG): chemotherapy + end ocrine treatment versus endocrine treatment. A French UNIC ANCER
Geriatric Oncology Group (GERICO) and Breast Group (UCBG) multicentre phase III trial
MicroarrayqRT-PCR
CGA
EUDRACT N° 2011-004744-22, PHRC national 2011, NCT01564056
R**
1:1
All patientsLee ScoreG8, CCI
Polymedications
Genomic Grade(GG)
evaluation
CCIPolymedications
Events
Group IILow GG
NO CHEMOTHERAPY IS RECOMMENDED - Follow up
Cy1+ GCSF
Cy2+ GCSF
Cy3+ GCSF
Cy4+ GCSF
q3w q3w q3w
HT 5 yr
Group I **High GG
Arm B = CT + HT
Arm A = HT HT 5 yrXRT
XRT
baseline 16 weeks 1, 2, 3 & 4 year
1, 2, 3 & 4 year
MMSE, IADLQLQ C30 & ELD15LVEFSocioeconomicStandard Lab
1 blood + serum
PolymedicationsMMSE, IADLQLQ C30 & ELD15LVEFSocioeconomicWillingnessStandard Lab1 blood + serum
G8, CCIPolymedicationsMMSE, IADLQLQ C30 & ELD15LVEFSocioeconomicWillingness
Standard Lab every year
1 blood + serum (M12 & M48)
Events
Chemo toleranceStandard Lab
Completecurativesurgery
Screening
** Group I include both high and equivocal GG cases
*Randomization stratified on pN, G8 and centre
time
GERICO 11 (EUDRACT N° 2011-004744-22, PHRC national 2011, NCT0 1564056)
2,000
1,100
900
Hypothesis B > A ∆+7.5% (A 80% vs B 87.5%) HR 0.60 α 5% β 10%

40
Inclusions on May 19 th, 2016(FR + BE) (48 months)
1,989
1,089

41
• Young patient
– Social and family obligations
(children)
– Quantity of life +++
• Elderly patient
– QoL+++
– Independence
– Staying at home
• Oncology
– Therapies and innovation
– Toxicity, response, survival
• RECIST
• NCI CTC v4.0
• Survival (DFS, PFS, DDFS,
OS)
– Fast-moving world
– "Molecular portrait" of
tumour & GEP
• Geriatrics
– Symptoms, diagnosis
– Quality of survival, i.e. amount of life with good QoL
• Cognition
• Functional status
• QoL
• Nutrition, etc.
– Requiring time
– "Global portrait" of patient & CGA
CGA
versus
or
+
?
Two worlds confronting
one another?
Genomic
defect
targeted
therapy
CGA
defect
targeted
geriatric
intervention
FEC, AACR, FAC, ASCO, anti-PDL1,
anti-PD1, CMF, SABCS, PD-1, PDL1,
DXR, PK/PD, CEX, 5FU CDDP, Calvert
AUC, ESMO, Chatelut AUC, CTC, TILs,
population PK, EORTC, FOLFIRI,
ctDNA, FOLFOX 7, CPA, DFS, CALGB,
DDFS, OS, TTP, NCI, CYP P450, JCO,
JNCI, HER2, PI3K, mTOR, Phase 0,
ECCO, ib and ab, Unicancer, EORTC,
SWOG, CALGB, etc.
Charlson, CIRSG, CGA, AD, MCI,
MNA, GDS, MMS, ADL, IADL,
GFI, CMR2, JAGS, EUGMS, G8,
CARG, Oncodage, VES-13, TRFs,
JGO, NIA, SoFOG, Walter’s score,
Lee’s score, CRASH, etc.

42
FEC, FAC, SoFOG, ADL, IADL, CMF,
SABCS, DXR, PK/PD, CEX, G8, EORTC,
5FU CDDP, MCI, Calvert and Chatelut
AUC, CARG, GDS, population PK, AD,
FOLFIRI, MMS, FOLFOX, CPA, CRASH,
SWOG, DFS, OS, TTP, NCI, GERICO,
TILs, CARG, anti-PDL1, anti-PD1,
EORTC TFE, JCO, JNCI, Charlson, JGO,
CIRSG, PD-1, PDL-1, ctDNA, EGS, EGA,
MNA, GFI, Unicancer, Lee’s score,
JAGS, etc.
To be practice changing,
let us be practice sharing!
Join our unique CME accredited training programme lead by international experts in the field ofgeriatrics AND oncology designed to provide specific skills in assessment, care pathways andtherapeutic choices about the elderly patients with cancer in order to provide the basis of theassessment and the multi-dimensional approach that should be applied to elderly cancerpatients.
Admission process opens on January 9, 2017
Find out more at www.siog.org
This course is an ESO recommended activity and is held with the support of
Pending auspices and endorsements:
Course director: Silvio Monfardini (IT) Course co-director: Etienne Brain (FR) Course coordinator: Giuseppe Colloca (IT)

43
www.siog.org


















