
Cancer Care Outreach Program on Education (CCOPE) … Ne… · UBC CPD | EDUCATIONAL MODULE Cancer...
40
Transcript of Cancer Care Outreach Program on Education (CCOPE) … Ne… · UBC CPD | EDUCATIONAL MODULE Cancer...

UBC CPD | EDUCATIONAL MODULE
Cancer Care Outreach Program on Education (CCOPE) Advanced Cancers Workshop Authorship Acknowledgements Workshop syllabus was authored by (in alphabetical order): Tanuja Barker, MSc, BSc Senior Research Assistant, UBC Division of Continuing Professional Development (UBC CPD) Jennie Barrows, BSc (Hons) Project Manager, UBC Division of Continuing Professional Development (UBC CPD) Pippa Hawley, B. Med FRACP, MRCP, FRCPC Palliative Care Physician, Internist, BCCA Neil Hilliard, MD Family Physician, Chilliwack Lilli Kerby, MD, CCFP Family Physician, Rossland Brenna Lynn, PhD, MSc, BHK Executive Director, UBC Division of Continuing Professional Development (UBC CPD) Douglas McGregor, MB ChB, FRCP (UK), MRCGP, BA, CCFP Medical Director, Victoria Hospice Philip White, MB, BS, CCFP Medical Director, FPON & GPAC representative
UBC CPD | EDUCATIONAL MODULE
Faculty / Author Disclosure Statements In accordance with Accreditation Council of Continuing Medical Education (ACCME) Standards for Commercial Support, all faculty participating in these programs are expected to disclose to the program audiences any real or apparent conflict of interest related to the content in their preparation.
Name Affiliations, financial or otherwise, with a commercial organization that may have a direct or indirect connection
to the content of this syllabus
Ms. Tanuja Barker Nothing to disclose Ms. Jennie Barrows Nothing to disclose Dr. Pippa Hawley Nothing to disclose Dr. Neil Hilliard Received a grant in aid from Hospira for an investigator
initiated pilot RCT Dr. Lilli Kerby Nothing to disclose Dr. Douglas McGregor Nothing to disclose Dr. Brenna Lynn Nothing to disclose Dr. Philip White Member of the Eliquis and Cialis advisory boards for
Pfizer. Received an honorarium from Pfizer for advisory board participation. Participated in Acasti pharma clinical trial on hypertriglyceridemia.
Important intellectual contributions were provided by other members of the CCOPE Steering Committee and the following individuals: Dr. Bob Bluman, Medical Director, Special Projects, UBC CPD (CCOPE Physician Lead) Dr. Charmaine Kim-Sing, Radiation Oncologist, BCCA Ms. Allison Macbeth, Research Assistant, UBC CPD Funding Acknowledgements We gratefully acknowledge funding provided by the BC Cancer Agency (BCCA). Use of Material This material is provided for individual use by workshop participants only. Contact [email protected] to request permission to copy or reproduce. Syllabus Updated: October 2015

UBC CPD | EDUCATIONAL MODULE
CCOPE Advanced Cancers Workshop: Participant Syllabus
Table of Contents
I Overview of Cancer Care Program on Education (CCOPE)………………………….......................... i II BC Cancer Resources………………………………………………………………………………………………………. ii III Workshop Learning Objectives…………………………………………………………………........................... iv V Case 2: Breast Cancer (Pt: Ms. Jenny Dalewood)…………………………………................................. 7 VI Supplemental Resources……………………………………………………………………………………………….
1. Pre-filled Lab Requisition Form……………………………………………………………………………………… 27 2. Coping with Anxiety Fact Sheet………………………………..………………………………………………….. 28 3. Screening for Measuring Distress Tool.………………………………………………………………………… 29 4. BC Cancer Agency Patient Referral Form……………………………………………………………………… 30 5. Relevant Cancer Centres Contact Information…………………..……………….………………………… 31 6. SPIKES Protocol for Breaking Bad News………………………………………………………………….……. 32 7. BC Government Advance Care Planning ……….……………………………………………………………... 33 7.1. BC Government Advance Care Planning…………………………………………………………………….. 34 8. Endoscopic Biliary Stenting………………………………………………………………………………………….. 35 9. BC College of Physicians and Surgeons Contact Information………………………………………… 36 10. Employee & Family Assistance Program (EFAP)…………………………………………………………. 37 11. BC Cancer Agency Counselling for Coping with Cancer………….……………………………………. 38 12. Palliative Performance Scale (PPS)……………………………………………………………………………… 39 13. BC Ministry of Health Palliative Care Benefits Program - Physician Guide…….……………… 40 14. GPAC Guidelines - Pain Management…..…………………………………………………………………….. 41 15. GPAC Guidelines - Cancer Pain Management Algorithm….……………………………….………… 42 16. GP Services Committee Palliative Care Incentives…...…………………………………………………. 43 17. GPAC Guidelines - Grief & Bereavement….…………………………………………………………………. 44 18. World Health Organization’s Cancer Pain Ladder for Adults….……………………………………. 45 19. Ohio Health Celiac Plexus Block…..……………………………………………………………………………... 46 20. Victoria Hospice Book “Medical Care of the Dying” Flyer….……………………………………….. 47 21. BC Government Employment Insurance Compassionate Care Benefits…..…………………… 48 22. GPAC Guidelines - Bereavement Assessment and Support….…………………………………….. 49 23. GPAC Grief and Bereavement Guideline Resource Links for Patient Handout….………….. 50 24. BC Ministry of Health Oncologist Follow-up Plan…..…………………………………………………… 51 25. Fraser Health Symptom Assessment Acronym “OPQRSTUV”…..………………………………… 52 26. Medications Used in Pain Management….………………………………………………………………….. 53 27. Edmonton Symptom Assessment System (ESAS) Numerical Scale…………………………….. 54 28. BC Ministry of Health Pharmacare Covered Drugs……………………………………………………… 55 29. BC Cancer Agency Outpatient Bowel Protocol Summary……………………………………………. 56 30. Constipation Management Algorithm………………………………………………………………………… 57

UBC CPD | EDUCATIONAL MODULE
31. BC Cancer Agency Lung Cancer Symptoms………………………………………………………………… 58 32. BC Government Smoking Cessation Program……………………………………………………………… 59 33. The Lung Association Quit Now Smart Steps……………………………………………………………… 60 34. Canadian Cancer Society Lodges……………………………………………………………………………….. 61 35. BC Cancer Agency Bowel Protocol……………………………………………………………………………… 62 36. The Bow Tie Model of 21st Century Palliative Care by P. Hawley…………………………………. 63 37. BC Ministry of Health Palliative Care Benefits Program………………………………………………. 64 38. Early Palliative Care for Patients with Metastatic Non-Small-Cell Lung Cancer…………… 65 39. BC Cancer Agency Advance Care Planning: Making Decisions for Your Future…………… 66 40. BC Government My Voice Advanced Care Planning Guide Quick Tips……………………….. 67 41. BC Cancer Agency Advanced Cancer Patient Links…………………………………………………….. 68
42. The Canadian Medical Protective Association Medico-legal Handbook for Physicians in Canada………………………………………………………………………………………………………………………… 69
43. BC Palliative Care Benefits Program Application………………………………………………………… 70 VII Cases Q&A……………………………………………………….………………………………………………………..…… 71 X Participant Feedback Survey……………………………………………………….………………… 96
UBC CPD | EDUCATIONAL MODULE | i
I. Overview of the Cancer Care Outreach Program on Education (CCOPE) What is CCOPE? The Cancer Care Outreach Program on Education (CCOPE), provided by the UBC Division of Continuing Professional Development (UBC CPD) in partnership with the BCCA Screening Groups and Family Practice Oncology Network (FPON), is an important educational initiative to provide BC family physicians with a better understanding of their roles and best practices across the cancer care continuum. How do the CCOPE Workshops work? These interactive workshops are designed for family physicians, and are also relevant to others working in family practice settings. Each workshop will be led by a facilitator who is well-versed in providing advanced cancer care to patients. The workshops will be delivered to a small group of family physicians in an informal environment (over dinner) in order to allow for dialogue surrounding case management. A follow-up session will take place two months after the workshop. This will be an opportunity for participants to share how they applied what they learned in practice and to address outstanding questions. A specialist will call in to the session to provide their perspective. With the help of our Steering Committee and Advanced Cancers Care Working Group, we have developed a workshop designed to help participants familiarize themselves with best practices for the management of advanced cancers care. The syllabus contains three cases and address:
• Role of primary care physicians along the advanced cancer care continuum and recognition of this relationship with other healthcare providers;
• Appropriate diagnostic and prognosis procedures; • Main treatment options and their potential side-effects; and • Palliative approaches to care with consideration of prognosis and patient perspective

UBC CPD | EDUCATIONAL MODULE | ii
II. BC Cancer Resources The BC Cancer Agency (BCCA) offers several facilities and networks across the province to support cancer care. These include 6 regional centres (see the table below).
BC Cancer Agency Facilities
Location Main Contact Number
Toll Free Number
Abbotsford Centre 32900 Marshall Rd, Abbotsford, BC V2S 0C2 604-851-4710 1-877-547-3777
Sindi Ahluwalia Hawkins Centre for the Southern Interior
399 Royal Avenue, Kelowna, BC V1Y 5L3 250-712-3900 1-888-563-7773
Fraser Valley Centre 13750 96th Avenue, Surrey, BC V3V1Z2 604-930-2098 1-800-523-2885
Vancouver Centre 600 West 10th Avenue, Vancouver, BC V5Z 4E6 604-877-6000 1-800-663-3333
Vancouver Island Centre 2410 Lee Avenue, Victoria, BC V8R 6V5 250-519-5500 1-800-670-3322
Centre for the North 1215 Lethbridge Street, Prince George, BC V2M 7E9 250-645-7300 1-855-775-7300
There are also 19 community-based Community Cancer Centres located across the province. For more information about these centres and other community services, please visit the BC Cancer Agency website at: http://www.bccancer.bc.ca/RS/default.htm Family Practice Oncology Network (FPON) The Family Practice Oncology Network (FPON) offers support to family physicians in British Columbia who provide cancer care by offering access to various resources and tools. For example, they publish a bi-annual journal, are involved with the development of cancer care guidelines and offer CME opportunities, such as partnering to deliver these series of workshops and hosting monthly Oncology CME Webcasts. The General Practitioners in Oncology (GPO) training program allows family physicians the opportunity to strengthen their oncology skills and build valuable contacts and confidence. In turn, the GPOs offer access to their knowledge base to family physicians within their communities. For a list of GPOs per community, please see the table on the following page. For further information about the Family Practice Oncology Network, please visit their website at: http://www.bccancer.bc.ca/HPI/FPON/default.htm or contact Jennifer Wolfe at 604 219 9579.

UBC CPD | EDUCATIONAL MODULE | iii
General Practitioners in Oncology by Community Updated April 2015 Source: BCCA (2014). GPOs by Community At present, 70 GPOs from 35 different communities have completed the GPO Training Program and are actively practising in BC. Ten (*) are in the process of completing the program and 15 have been practising since before the program began in 2004. In total, there are 95 GPOs practising in BC at present.
Community Name Abbotsford Dr. Al Chafe* Dr. Eric Gable Dr. Raziya Mia Dr. Sian Shuel Campbell River Dr. Anne Morrison Dr. Willem Prinsloo Dr. Jim Proctor Comox Dr. Tanya Austin Dr. Amitabh Bakshi Dr. Wai Ling Dan Cranbrook Dr. Shawna Dawe* Dr. Keith Lowden Dawson Creek Dr. Cornelia Popa* Dr. Servaas Verster Duncan Dr. Valorie Cunningham Fort St. John Dr. Mike Wright Dr. Becky Temple Gibsons Dr. Monica Marton Golden Dr. Trina Larsen Soles Grand Forks Dr. Jeanne Borstlap Dr. Geoffrey Coleshill Hope Dr. Ertha Nanton Kamloops Dr. Suzi Tevendale Dr. Johan Van Heerdan Kelowna Dr. Henry Docherty Dr. Carolyne McLelland Dr. Gerald Patridge Dr. Mary Wall Kitimat Dr. Sabina Kay Dr. Andries Van Schalkwyk* Dr. Marius Wahl Ladysmith Dr. Emanuel Fritsch Dr. Michael McGuire Masset Dr. Michele Leslie Nainamo Dr. Michael Dunne Dr. Elizabeth Kenward Dr. Randy Marback Osoyoos Dr. Karin Kilpatrick Penticton Dr. Donella Anderson Dr. Sandra Pansegrouw Dr. Wendy Ross Dr. Marianne Willis Port Alberni Dr. Wendy Johnsen Powell River Dr. Stephen Burns Prince George Dr. Meredith Hunter Dr. Sandra Lamb Dr. John Mah Dr. Linda Wilson Prince Rupert Dr. Luke Tse Queen Charlotte City Dr. Jamie Chrones Dr. Tracy Morton Dr. Caroline Shooner
Community Name Salmon Arm Dr. James Levins Sechelt Dr. Robert Newman Smithers Dr. Elizabeth Bastian Dr. Daphne Hart Dr. Mary Knight Dr. Roderick Leighton* Surrey Dr. Melodie Herbert Dr. Karen Hossack Dr. Amrish Joshi Dr. Andrea Pollock Terrace Dr. Jaco Fourie Dr. Paul Warbeck* Vancouver Dr. Sherry Chan* Dr. Andrea Cheung Dr. Donald Cooper Dr. Rose-marie Coschizza Dr. Val Geddes Dr. Mary Georgilas Dr. Mike Mamacos Dr. Maryam Nazary Dr. Leah Norgrove Dr. Peter Pavlovich Dr. Judith Rodrigo Dr. Lori Saretsky Dr. Ismet Tejpar Dr. Angela Thermann Dr. Sherry Zheng Vanderhoof Dr. Suzanna Campbell Dr. Davy Dhillon Dr. Shannon Douglas Vernon Dr. Christine Blyth Dr. Chris Cunningham Dr. Allison Rankin Victoria Dr. Jody Anderson Dr. Stephen Ashwell Dr. Elisabeth Crisci* Dr. Taryl Felhaber Dr. Dean Kolodziejczyk Dr. Ryan Liebscher Dr. David Peterson* Dr. Dagmar Smatanova Dr. Margaret Smith Whitehorse Dr. Robin Jamieson Dr. Danusia Kanachowski Dr. Sally McDonald Dr. Lucille Stuart Williams Lake/100 Mile House
Dr. Gord Hutchinson
Dr. Emil LaBossière **Nigeria Dr. Kelechi Eguzo

UBC CPD | EDUCATIONAL MODULE | iv
III. Workshop Learning Objectives As a result of completing these workshop cases, participants will: 1. Describe the role of the primary care physician along the advanced cancer care continuum
and recognize how this relates to the roles of other healthcare providers, including specialists
2. Describe common treatment options and their expected side effects
3. Access available resources for palliative care
4. Specify a plan for integrating what is learned at the workshop into practice
UBC CPD | EDUCATIONAL MODULE
Breast Cancer
Patient: Ms. Jenny Dalewood
UBC CPD | EDUCATIONAL MODULE Case | 2
Case: Breast Cancer Learning Objectives:
As a result of completing this workshop case, participants will be able to:
1. Describe the role of the primary care physician along the advanced cancer care continuum and recognize how this relates to the roles of other healthcare providers, including specialists
2. Describe common treatment options for advanced breast cancer and their expected side effects
3. Access available resources for palliative care.
Case Scenario:
Jenny is a 35 year old woman who presented to your office because she had found a lump in her right breast. Lumpectomy and sentinel lymph node biopsy revealed a Stage IIa right breast invasive ductal carcinoma with a 3cm grade 3 primary tumour, estrogen receptor (ER) negative, progesterone receptor (PR) negative, HER-2/neu negative with clear surgical margins and 0/6 sentinel nodes involvement. Staging investigations including a CT of the chest, abdomen and pelvis were negative for metastatic disease.
Due to having high grade disease and being triple receptor negative, Jenny is told by her oncologist that she has a 43% chance of recurrence in the next 10 years which could be reduced to 19% by adjuvant chemotherapy. She receives adjuvant chemotherapy with the FEC-D protocol* followed by adjuvant radiotherapy to the right breast with a boost to the tumour bed.
Your patient is otherwise healthy with no allergies. She and her husband, Rick, have no children as her husband is infertile.
*FEC-D chemotherapy protocol: 5-fluorouracil-epirubicin-cylophosphamide followed by docetaxel 1. Jenny has been discharged following treatment. She is anxious about her cancer coming back
and asks you what she should be looking for and how often she should come in for follow-up.
Notes:
UBC CPD | EDUCATIONAL MODULE Case | 3
Case Progression:
Two and a half years later Jenny develops minor neck pain on the right side. She comes in to see you about what she thought was a muscle strain, but on examination you find a lump in the right supraclavicular fossa that feels firm and is tender to palpation.
2. What are your next steps? What do you tell your patient?
Notes:
Case Progression:
You sent her to your local surgeon who excises the lump. Pathology shows metastatic adenocarcinoma compatible with breast adenocarcinoma. Jenny has made a follow-up appointment to see you. She tells you that she does not have an appointment with the surgeon for 3 weeks because her surgeon is away on holiday. Jenny continues to have pain in the right supraclavicular region which now radiates down the right arm. She has been taking some Tylenol #3 that she had left over after some dental work. Jenny is hoping that you have the pathology results.
3. What do you share with Jenny?
Notes:
UBC CPD | EDUCATIONAL MODULE Case | 4
4. Does she need just localized treatment with palliative radiotherapy or are there more widespread metastases requiring palliative chemotherapy for treatment?
Notes:
Case Progression:
The CT scan shows a conglomerate mass of nodes measuring 1.5 x 2.5 cm at level IV in her right neck, as well as several smaller abnormal looking nodes. The remainder of the CT scan and bone scan is negative for metastatic disease.
Jenny arrives for her follow-up appointment with her husband, Rick. You have set aside extra time to give the bad news and asked your secretary that you not be disturbed during the appointment. Following the SPIKES protocol, you inform them of the diagnosis and suggested approach. It is good that the recurrence is localized. For that reason you will arrange an appointment with a radiation oncologist. He recommends that Jenny undergoes a course of radiation; but that this is unlikely to completely eradicate all of her disease in her neck and that she retains a high risk of developing additional recurrence in the future.
5. What should you discuss at your next appointment with Jenny?
Notes:
UBC CPD | EDUCATIONAL MODULE Case | 5
Case Progression:
Jenny agrees that he would be her alternate decision maker, but she appears anxious, and wonders why you are asking. She says she wants everything done: “I want to live.” In response, you say it is your responsibility to ask about what your patient’s wishes would be if they were suddenly in an accident or dying. You reassure her that she is not dying now, but if she was in the future and unable to make her own decisions, has she discussed what her wishes would be with her husband? Jenny says she doesn’t like to talk about these things and that you are making her nervous. You provide her and her husband with a copy of the “My Voice” booklet and tell her that when she is ready, the first half of the book is to help with the discussion.
Case Progression:
A course of palliative radiotherapy 50Gy in 20 fractions to the right cervical and supraclavicular nodes was administered over 5 weeks. There was some shrinkage of palpable nodes in her neck and some improvement of neuropathic pain in her right arm.
Two months later you see Jenny with complaints of pain in her right upper back and shoulder area radiating into her neck. It is again radiating down her right arm. The pain is achy and everything feels tight, rated 4-7/10. Applying pressure on several areas helps, as does the use of heat or ice. Tylenol #3 gives minimal relief for up to an hour. Jenny has been unable to work for the last week.
6. What are your next steps?
Notes:
Case Progression:
One week later Jenny’s pain is better controlled but her lymphedema is becoming worse. Currently she is taking MS-IR 10 mg 5 times a day and breakthrough doses of 5mg twice a day along with gabapentin 300 mg tid. Pain is still radiating into her right arm, but not as severe. She is having nausea, abdominal cramps and has not had a bowel movement for 4 days.
UBC CPD | EDUCATIONAL MODULE Case | 6
7. What are your next steps?
Notes:
Case Progression:
One week later you see Jenny. Her pain and nausea are less, but she again has not had a bowel movement for 4 days. She says she can’t tolerate the sennosides because of severe cramping. You remember that she has a history of irritable bowel syndrome.
8. What do you recommend now?
Notes:
Case Progression:
One and a half months later Jenny comes to the ER in pain crisis. The ER doctor notes marked swelling of her right arm. She has difficulty lifting the arm due to swelling and pain. She is tearful and cannot sleep because of the pain. For pain the ER Doctor doubles her M-Eslon 60 mg bid and MS-IR 5 mg every hour (fifteen times in the last 24 hours). She has noticed that she is a bit twitchy. A CT scan has been booked by her oncologist in another month to assess for response to palliative capecitabine.
*Note: In some communities, the ER doctor may be the family physician.
UBC CPD | EDUCATIONAL MODULE Case | 7
9. What would you do now?
Notes:
Case Progression:
While in hospital, pain and swelling are still not well controlled. She is depressed and anxious. You ask that the medical oncologist see her in follow-up. In addition you start her on nortriptyline 10 mg qhs and over the next few days increase it to 30 mg qhs to see if this will help with her sleep and neuropathic pain. When she was admitted, she stated that she wanted full resuscitation and everything done. You ask if she has had a chance to discuss her wishes with her husband. She again says, “I want to live.” You write a progress note that the patient wishes full treatment and resuscitation.
While in hospital, your patient is started on palliative cisplatin and gemcitabine. Her pain and swelling in her right arm start to improve. She is sleeping better and less anxious and depressed. You are now managing her pain with hydromorphone SR 30 mg bid and Hydromorphone IR 6 mg q1h prn along with gabapentin 600 mg tid and nortriptyline 30 mg qhs.
On follow-up in the office 3 months later, you are amazed that your patient is now again able to use her right arm and the lymphedema has now almost totally resolved. She has been tolerating the cisplatin and gemcitabine well. She no longer needs to take any breakthrough hydromorphone. However she is quite drowsy and her husband is concerned that she is sleeping most of the day. He also asks whether it is still necessary to continue the dalteparin injections every day. Although she has 80% coverage through extended benefits, it still costs her and her husband $300 per month.
UBC CPD | EDUCATIONAL MODULE Case | 8
10. What do you think is the problem? What are your next steps?
Notes:
Case Progression:
Over the next 6 months, your patient continues on cisplatin and gemcitabine and continues to do well. She was able to take a holiday by the lake in the Okanagan with her husband. However, now she comes in complaining of numbness and burning pain in her feet that is keeping her awake at night. Her oncologist has dose reduced her cisplatin by 20% at her last visit.
11. What do you think is the cause and what do you recommend?
Notes:
Case Progression:
The oncologist stops the cisplatin and carries on with single agent gemcitabine for another several months. Unfortunately, pain and swelling are again increasing in the right arm. The pain in the right arm is burning and feels like sharp needles and jabs. Despite increasing her hydromorphone back up to 30 mg bid, your patient is again requiring 5 or 6 breakthrough per day. Increasing the gabapentin further just made her drowsier.

UBC CPD | EDUCATIONAL MODULE Case | 9
12. What do you recommend now?
Notes:
Case Progression:
Her oncologist has switched your patient from single agent gemcitabine to single agent vinorelbine. Three months later she comes in to see you, again with increased pain in her right shoulder and arm, but now also with right sided headache. For her right shoulder and arm pain, her pain specialist has increased her methadone to 12.5 mg q8h. Breakthrough hydromorphone does not seem to help. Ibuprofen 800 mg helped her headache. On exam there was noted to be palpable spasm of her right para-cervical muscles and trapezius. Full right lateral flexion of the neck was accompanied by pain radiating into the right arm. There was good range of motion of the right shoulder. She asks you about acupuncture.
13. What would you do now?
Notes:
Case Progression:
Your patient returns in several days with migraine headaches with nausea and vomiting. She experienced some photophobia. Also she noticed more difficulty walking, but did not have any falls. The CT scan is booked for next week.

UBC CPD | EDUCATIONAL MODULE Case | 10
14. What would you do now?
Notes:
Case Progression:
The CT scan shows a 2-3 cm mass in the right cerebellar hemisphere with a moderate amount of edema and displacement of the 4th ventricle. As well there are smaller lesions in the left cerebellar hemisphere, right occipital lobe and both frontal lobes.
15. What are the next steps?
Notes:

UBC CPD | EDUCATIONAL MODULE Case | 11
Case Progression:
Right cerebellar tumour was resected and pathology was consistent with metastatic breast cancer ER negative, PR negative and HER-2/neu negative. She received 10 fractions of palliative whole brain radiotherap. She decided not to resume Vinorelbine. Dalteparin had been held while in hospital, but restarted postoperatively. She is now on a tapering dose of dexamethasone at 4 mg bid, methadone 15 mg q8h, hydromorphone 8 mg q1h prn for breakthrough, gabapentin 300 mg tid, venlafaxine XR 75 mg daily, rabeprazole 20 mg daily.
For several months your patient did well but she now presents to the emergency department with severe neck pain and new weakness and numbness in her right arm. She is admitted to the hospital’s palliative care unit where her pain is managed with an increased dose of methadone and dexamethasone. An MRI of the spine shows abnormal changes within the central cervical and thoracic spinal cord between C4 and C7 and T2 to T5. Nodular changes affecting the distal spinal cord are suspicious for leptomeningeal metastases. While you are visiting her, she tells you that she has been offered more palliative radiotherapy. She and her husband ask you how much time you think she has left and whether or not you recommend radiation therapy?
16. What would you tell them?
Notes: Case Progression:
After your discussion with your patient and her husband, they decide not to go ahead with palliative radiotherapy and opt for just comfort measures.
UBC CPD | EDUCATIONAL MODULE Case | 12
17. Is there anything else you should discuss?
Notes:
Case Progression:
Unfortunately, Jenny goes on to develop complete paralysis of both lower extremities and required a Foley catheter for urinary incontinence. She no longer wishes hospital care, including intravenous fluids and medication, and is transferred to hospice where she gradually declined. For the last few days she was non-responsive and died peacefully, 4 1/2 years after her initial diagnosis.
You send a card expressing your condolences to her husband.
You take some time to reflect on what a journey that Jenny and her husband have had over the past 5 years. Initially there was surgery, then chemotherapy and radiotherapy, more radiotherapy, palliative chemotherapy, neurosurgery and more radiotherapy.
The husband Rick, who is also your patient, comes in two weeks later having trouble sleeping.
18. What do you do?
Notes:
Case Progression:
Rick agrees to be contacted by a hospice volunteer. He thanks you for all that you have done for his wife over the last 5 years and that he could not have done it otherwise.

UBC CPD | EDUCATIONAL MODULE
Supplemental Resources
1. Pre-filled Lab Requisition Form…………………………………………………………………………………………………………. 27 2. Coping with Anxiety Fact Sheet………………………………..…………………………………………….……..…………………. 28 3. Screening for Measuring Distress Tool.……………………………………………………………………………………………. 29 4. BC Cancer Agency Patient Referral Form…………………………………………………………………………………………. 30 5. Relevant Cancer Centres Contact Information…………………..……………….…………………….………………………. 31 6. SPIKES Protocol for Breaking Bad News………………………………………………………………….….….…………………. 32 7. BC Government Advance Care Planning ……….…………………………………………………………………………………. 33 7.1. BC Government Advance Care Planning………………………………………………………………………………...………. 34 8. Endoscopic Biliary Stenting………………………………………………………………………………………………………………. 35 9. BC College of Physicians and Surgeons Contact Information………………………………………….…………………. 36 10. Employee & Family Assistance Program (EFAP)…………………………………………………………..…………………. 37 11. BC Cancer Agency Counselling for Coping with Cancer………….……………………………………..…………………. 38 12. Palliative Performance Scale (PPS)…………………………………………………………………………………………………. 39 13. BC Ministry of Health Palliative Care Benefits Program – Physician Guide…….…………………………………. 40 14. GPAC Guidelines – Pain Management…..……………………………………………………………………..…………………. 41 15. GPAC Guidelines – Cancer Pain Management Algorithm….……………………………….….…………………..……. 42 16. GP Services Committee Palliative Care Incentives……………………………………………….……….…………………. 43 17. GPAC Guidelines – Grief & Bereavement….………………………………………………………….……….……...…………. 44 18. World Health Organization’s Cancer Pain Ladder for Adults….…………………………………….…………………. 45 19. Ohio Health Celiac Plexus Block…..…………………………………………………………………………………………………. 46 20. Victoria Hospice Book “Medical Care of the Dying” Flyer….………………………………….……..…………………. 47 21. BC Government Employment Insurance Compassionate Care Benefits…..…………….…………………………. 48 22. GPAC Guidelines – Bereavement Assessment and Support….……………………………………..…………………. 49 23. GPAC Grief and Bereavement Guideline Resource Links for Patient Handout….….………..…………………. 50 24. BC Ministry of Health Oncologist Follow-up Plan…..………………………………………….……………………………. 51 25. Fraser Health Symptom Assessment Acronym “OPQRSTUV”…..……………………………………………………. 52 26. Medications Used in Pain Management….…………………………………………………………………..…………………. 53 27. Edmonton Symptom Assessment System (ESAS) Numerical Scale…………………….………..…………………. 54
UBC CPD | EDUCATIONAL MODULE Case | 14
28. BC Ministry of Health Pharmacare Covered Drugs…………………………………………………………………………. 55 29. BC Cancer Agency Outpatient Bowel Protocol Summary………………………………….………….…………………. 56 30. Constipation Management Algorithm……………………………………………………………………………………………. 57 31. BC Cancer Agency Lung Cancer Symptoms……………………………………………………….……………………………. 58 32. BC Government Smoking Cessation Program…………………………………………………………………………………. 59 33. The Lung Association Quit Now Smart Steps………………………………………………….………………………………. 60 34. Canadian Cancer Society Lodges………………………………………………………………….……………..…………………. 61 35. BC Cancer Agency Bowel Protocol……………………………………………………………………………….…………..……. 62 36. The Bow Tie Model of 21st Century Palliative Care by P. Hawley…………………………………..…………………. 63 37. BC Ministry of Health Palliative Care Benefits Program………………………………………………..…………………. 64 38. Early Palliative Care for Patients with Metastatic Non-Small-Cell Lung Cancer…………….…………………. 65 39. BC Cancer Agency Advance Care Planning: Making Decisions for Your Future…………….…………………. 66 40. BC Government My Voice Advanced Care Planning Guide Quick Tips…………………………………………… 67 41. BC Cancer Agency Advanced Cancer Patient Links…………………………………………………………………………. 68 42. The Canadian Medical Protective Association Medico-legal Handbook for Physicians in Canada……………………………………………………………………………………………………………………………………………...... 69 43. BC Palliative Care Benefits Program Application……………………………………………………………………………. 70

UBC CPD | EDUCATIONAL MODULE Cases Q&A | 1
Case Q&A

UBC CPD | EDUCATIONAL MODULE Cases Q&A | 2
Case: Breast Cancer
1. Jenny has been discharged following treatment. She is anxious about her cancer coming back and asks you what she should be looking for and how often she should come in for follow-up
Key point Notes Resources Refer to oncologist advice
Oncologist has provided you with a plan for follow-up: - see her every 6 months for 5 years then annually - mammogram at 6 months, and then annual
mammogram
BC Ministry of Health Oncologist Follow-up Plan
Involve patient in management
If she notices a new lump, swelling of the right arm, specific recurring pain, shortness of breath or loss of appetite she should make an appointment to see you
2. What are your next steps? What do you tell your patient?
Key point Notes Resources History and physical
Check for: - other areas of possible recurrent disease or - other reasons for an enlarged cervical lymph node - if not already ascertained a full history should be
taken, particularly regarding smoking, alcohol, use of street drugs, family Hx of substance abuse
Biopsy Arrange a biopsy of the lymph node Order / referral form
Employ effective communication techniques
Tell the patient that it could just be a reactive lymph node but that we need to rule out recurrent disease
Pain management
At this time it is unknown whether this is cancer or non-cancer pain. First treat as non-cancer pain with WHO ladder step one medications, Acetaminophen or Ibuprofen
WHO Pain Ladder
3. What do you share with Jenny?
Key point Notes Resources Employ effective techniques for disclosing an advanced cancer diagnosis
- Normally give her the option of bringing her husband to the appointment
- Ask how she would like the test results, all the information now, or to sketch out the results and spend more time on the treatment plan? She agrees to the latter. You tell her that you are concerned about the results, but that you need more information.
Treatment plan

UBC CPD | EDUCATIONAL MODULE Cases Q&A | 3
Key point Notes Resources Pain management - Give her something for the pain. Step 2
medications Step 2 medications on the WHO pain ladder, if step 1 medications are not sufficient.
- Record pain type, location, and scale. To be thorough, it is important to ask about timing of the pain, what makes it worse or better, whether the pain remains localized or radiates, and whether there are other pains.
Record pain type, location & scale - WHO pain ladder,
if step 1 medications are not sufficient
- Symptom Assessment Acronym (OPQRSTUV)
4. Does she need just localized treatment with palliative radiotherapy or are there more widespread metastases requiring palliative chemotherapy for treatment?
Key point Notes Resources Restaging studies
Arrange restaging studies including: - CT of the neck, chest and abdomen - bone scan If the patient has been discharged from care, this would be considered to be a new referral. To avoid long delays in obtaining imaging, best care would be to arrange the restaging tests ASAP and results available for the oncologist appointment. Knowing the results will also help direct referral to the most appropriate oncologist – radiation oncologist or medical oncologist.
Order / referral form
- Navigating the bureaucratic system
Timely access to imaging may be a big problem and this may depend on where the patient lives (rural or urban). In this case, to expedite restaging tests it is essential that the reason for the imaging study is recorded on the requisition (ie; patient has recurrent breast cancer, need restaging info ASAP to direct referral and treatment). It will likely also be necessary to phone the radiologist to discuss and expedite the imaging studies. Note: Jenny could keep her appointment with the local surgeon, but it would not be necessary if you have arranged restaging and appropriate referrals. If these have not been done, the surgeon may be able to expedite.
Employ effective techniques for disclosing an advanced cancer diagnosis
- Ask her to arrange a follow-up appointment for the results
Suggest bringing her husband or a friend along
Bring a note book or recording device
UBC CPD | EDUCATIONAL MODULE Cases Q&A | 4
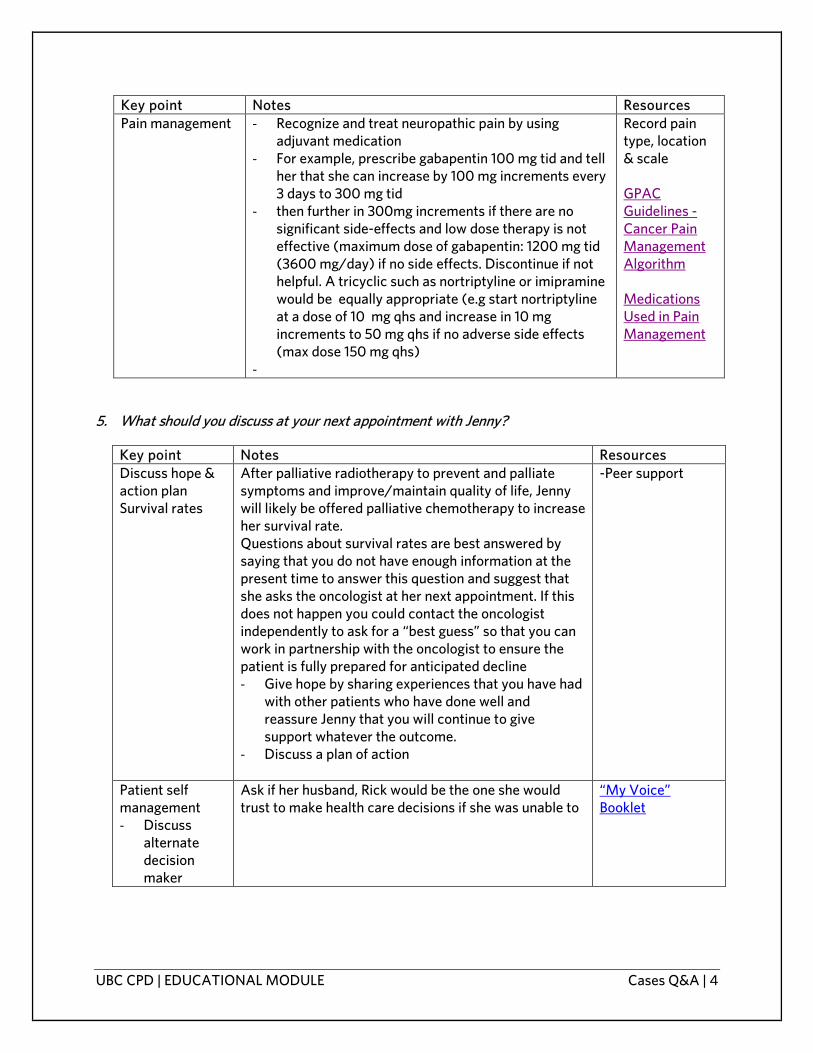
Key point Notes Resources Pain management - Recognize and treat neuropathic pain by using
adjuvant medication - For example, prescribe gabapentin 100 mg tid and tell
her that she can increase by 100 mg increments every 3 days to 300 mg tid
- then further in 300mg increments if there are no significant side-effects and low dose therapy is not effective (maximum dose of gabapentin: 1200 mg tid (3600 mg/day) if no side effects. Discontinue if not helpful. A tricyclic such as nortriptyline or imipramine would be equally appropriate (e.g start nortriptyline at a dose of 10 mg qhs and increase in 10 mg increments to 50 mg qhs if no adverse side effects (max dose 150 mg qhs)
-
Record pain type, location & scale GPAC Guidelines - Cancer Pain Management Algorithm Medications Used in Pain Management
5. What should you discuss at your next appointment with Jenny?
Key point Notes Resources Discuss hope & action plan Survival rates
After palliative radiotherapy to prevent and palliate symptoms and improve/maintain quality of life, Jenny will likely be offered palliative chemotherapy to increase her survival rate. Questions about survival rates are best answered by saying that you do not have enough information at the present time to answer this question and suggest that she asks the oncologist at her next appointment. If this does not happen you could contact the oncologist independently to ask for a “best guess” so that you can work in partnership with the oncologist to ensure the patient is fully prepared for anticipated decline - Give hope by sharing experiences that you have had
with other patients who have done well and reassure Jenny that you will continue to give support whatever the outcome.
- Discuss a plan of action
-Peer support
Patient self management - Discuss
alternate decision maker
Ask if her husband, Rick would be the one she would trust to make health care decisions if she was unable to
“My Voice” Booklet

UBC CPD | EDUCATIONAL MODULE Cases Q&A | 5
6. What are your next steps?
Key point Notes Resources Physical exam You examine her and note a great deal of thickening on the
right side of her neck where she previously has had radiation. There is tenderness to palpation. There is normal strength and sensation in her right arm, but you note mild lymphedema
Medical Oncologist
Arrange appointment with her medical oncologist, if the radiation oncologist has not already done so
Referral Form
Employment insurance
Check if Jenny is entitled to employment insurance medical disability benefits. If she is, ask her to visit the employment insurance office and advise Jenny to complete the medical disability form and drop it off for you to sign
Medical disability form
Medication review
- Conduct a medication review - always a good idea, especially regarding benzodiazepines when starting opioids.
- It is also worthwhile to ask about, smoking, alcohol, use of street drugs, family Hx of substance abuse as 10% of population (including cancer patients) have substance abuse problems and/or are chemical copers
- It is also helpful to ask about herbals and naturopathic remedies
Pain management
- Continuous pain requires continuous analgesia; prescribe regular dose versus prn
- Start with regular short-acting opioids and titrate to effective dose over a few days before switching to slow release opioids. For example, start her on MS-IR 5-10 mg q4h with 2.5 to 5 mg q1h prn (additional morphine as needed, if initial dose every 4 hours is not adequate)
- For the neuropathic component of her pain you restart gabapentin 100 mg tid and ask her to up-titrate every 3 days to 300 mg tid, then review for further dose titration if needed
- To avoid future financial shock for the patient, if there are no extended medical benefits and because the patient does not yet qualify for palliative drug benefits, choose an opioid that fair Pharmacare will cover in its slow release formulation (ie: morphine)
Record pain type, location & ESAS scale BC Ministry of Health Pharmacare Covered Drugs
Follow-up appointment
Ask her to schedule a follow-up appointment in one week

UBC CPD | EDUCATIONAL MODULE Cases Q&A | 6
7. What are your next steps?
Key point* Notes Resources Pain management
- Start her on M-Eslon 30 mg bid with MS-IR 5 mg q1h prn
o Once analgesic requirements have been determined by titrating MS-IR q4h doses, switch to slow release morphine
o Total daily dose (TDD) of morphine = (MS-IR 10 mg x 5 = 50 mg) + (BT 5 mg x 2 = 10 mg) = 60 mg.; therefore M-Eslon 30 mg bid (BT = breakthrough)
o The breakthrough dose is 10% of the total daily dose = 60 mg x 0.1 = 6 mg; therefore MS-IR 5 mg prescribed q1h prn
Additional Note: Suggest introduce process first, such as the following, then get into the numbers: “Calculate oral morphine equivalent of current medication. 1 T3# is equivalent to 5mg oral morphine in 80-90% of the population, but some people can be slow metabolizers and get little benefit from codeine, whereas others are fast metabolizers and you may need to be more conservative than that when switching. “
GPAC Guidelines - Pain Management
Anticipate opioid induced nausea
- Within one week of starting regular opioid medication, tolerance to opioid induced nausea develops
- Metoclopramide can be prescribed 10 mg qid prn
Anticipate opioid induced constipation
- Prescribe sennosides - Provide BCCA bowel protocol handout
BCCA Outpatient Bowel Protocol Summary
Lymphedema in right arm
Arrange for lymphedema massage if locally available. - Lymphedema massage is performed by a
physiotherapist with special training in this treatment modality.
- Usually physiotherapy is private pay, unless the patient has extended medical benefits, and this depends on the plan.
- Some hospital physiotherapy departments (Surrey, Burnaby) will provide this service without user payment
Ask MOA to call the local hospital physio department and the private physiotherapy clinics to see who has the training to deliver this treatment modality
Key point Notes Resources Pain management
- Recognize and treat neuropathic pain by using adjuvant medication
- For example, prescribe gabapentin 100 mg tid and tell her that she can increase by 100 mg increments every 3 days to 300 mg tid
Record pain type, location & scale GPAC Guidelines - Cancer Pain

UBC CPD | EDUCATIONAL MODULE Cases Q&A | 7
- then further in 300mg increments if there are no significant side-effects and low dose therapy is not effective (maximum dose of gabapentin: 1200 mg tid (3600 mg/day) if no side effects. Discontinue if not helpful. A tricyclic such as nortriptyline or imipramine would be equally appropriate (e.g start nortriptyline at a dose of 10 mg qhs and increase in 10 mg increments to 50 mg qhs if no adverse side effects (max dose 150 mg qhs)
-
Management Algorithm Medications Used in Pain Management
Treat underlying disease
- Worsening pain and lymphedema suggest disease progression.
- She has just been started on capecitabine 1500 mg bid by her medical oncologist
Update other health professionals involved in Jenny’s care
- Ask MOA to fax your progress notes and updated med list from your EMR / paper based chart to the oncologist. This information is then scanned into CAIS (BCCA Computer Assisted Information System) where it becomes part of the Cancer Agency Clinical Record for all to see.
- The consulting oncologist also receives this information in his/her action list for review
-
For oncologists working out a BCCA cancer center, this would be to the fax number of the secretary for medical oncology
*Note: Morphine was chosen as it is considered the standard opioid for treatment. It is inexpensive and covered by Fair Pharmacare in its extended release form, whereas hydromorphone and oxycodone are not. Fentanyl patches are also expensive and would not be used for initial drug titration. However, if renal function were compromised, hydromorphone or oxycodone would be preferred. If the patient had problems taking pills, problems with GI absorption because of rapid bowel transit time (ileostomy), or problems with nausea and vomiting, the fentanyl patch would be better choice for a slow release opioid.
8. What do you recommend now?
Key point Notes Resources Constipation - Perform a rectal exam to rule out impaction if you are
treating vs. prescribing to prevent constipation - Recommend PEG solution (Lax-a-day, Restorolax) 17 gm
mixed in juice, water or tea daily. Now that nausea is improved metoclopramide could be given 10 mg qid prn.
Constipation Management Algorithm
9. What would you do now?

UBC CPD | EDUCATIONAL MODULE Cases Q&A | 8
Key point Notes Resources CT scan Move the scheduled CT scan forward on a need to know
basis. The oncologist should be copied on the requisition so that if there is disease progression noted that the palliative chemotherapy regime can be changed now rather than waiting for another month. Shows localized progression of lymphadenopathy in her neck
Doppler ultrasound
Shows a DVT in her right arm
Pain management
- Rotate her opioid to hydromorphone and resume q4h dosing so that you may more rapidly titrate to the effective dose
- Start at hydromorphone 6 mg PO or 3 mg SC q4h and 3 mg PO q1h prn or 1.5 mg SC q30 min prn
- Increase her gabapentin to 600 mg tid
Opioid Switching (“rotation”) GPAC Guidelines – Pain Management
DVT Start Dalteparin 18,000 U SC daily
10. What do you think is the problem? What are your next steps?
Key point Notes Resources Palliative chemotherapy
Effective in managing her pain and swelling - If the patient’s pain is reduced by treatment of the
underlying disease by palliative chemotherapy or radiotherapy, expect that opioid requirements will become less
Medications Side effects are causing the drowsiness: - reduce her gabapentin from 600 mg tid to 300 mg tid - reduce her hydromorphone SR to 24 mg q12 h with a
corresponding reduction in hydromorphone IR to 4 mg q1h prn
- Over the next weeks you are able to gradually taper your patient off gabapentin, discontinue her nortriptyline and drop her hydromorphone dosage down to 12 mg PO bid before she again was requiring some breakthrough hydromorphone at a dose of 2 mg q1h prn
- advise her and her husband that best evidence supports her to continue on dalteparin injections, but the dosage is reduced to 12,500 U daily according to her present weight
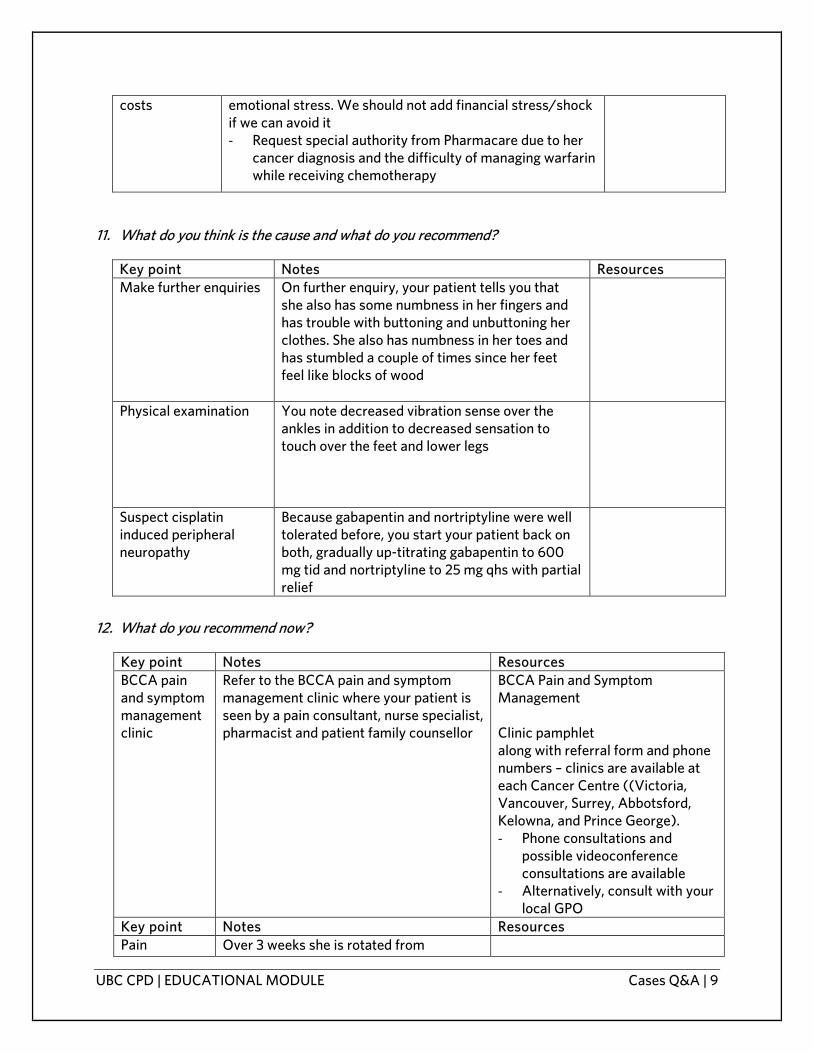
Key point Notes Resources Medication Patient and family are already under a lot of physical and
UBC CPD | EDUCATIONAL MODULE Cases Q&A | 9
costs emotional stress. We should not add financial stress/shock if we can avoid it - Request special authority from Pharmacare due to her
cancer diagnosis and the difficulty of managing warfarin while receiving chemotherapy
11. What do you think is the cause and what do you recommend?
Key point Notes Resources Make further enquiries On further enquiry, your patient tells you that
she also has some numbness in her fingers and has trouble with buttoning and unbuttoning her clothes. She also has numbness in her toes and has stumbled a couple of times since her feet feel like blocks of wood
Physical examination You note decreased vibration sense over the ankles in addition to decreased sensation to touch over the feet and lower legs
Suspect cisplatin induced peripheral neuropathy
Because gabapentin and nortriptyline were well tolerated before, you start your patient back on both, gradually up-titrating gabapentin to 600 mg tid and nortriptyline to 25 mg qhs with partial relief
12. What do you recommend now?
Key point Notes Resources BCCA pain and symptom management clinic
Refer to the BCCA pain and symptom management clinic where your patient is seen by a pain consultant, nurse specialist, pharmacist and patient family counsellor
BCCA Pain and Symptom Management Clinic pamphlet along with referral form and phone numbers – clinics are available at each Cancer Centre ((Victoria, Vancouver, Surrey, Abbotsford, Kelowna, and Prince George). - Phone consultations and
possible videoconference consultations are available
- Alternatively, consult with your local GPO
Key point Notes Resources Pain Over 3 weeks she is rotated from

UBC CPD | EDUCATIONAL MODULE Cases Q&A | 10
management hydromorphone to methadone at a dose of 10 mg q8h with hydromorphone 4 mg PO qid prn for breakthrough, requiring 0 to 2 breakthrough doses per day. Gabapentin was reduced to 300 mg tid and Nortriptyline was able to be discontinued. Both the neuropathic pain in her right arm and her peripheral neuropathy pain are improved. She is less drowsy and able to sleep well. She is able to go shopping for up to 5 hours and to enjoy going out for dinner with friends and with her husband. - If pain or sleep is still an issue, medical
cannabis could be discussed
Compression stocking
Arranged for her right arm Canvas local supply shops
13. What would you do now?
Key point Notes Resources Acupuncture Advise against acupuncture as long as she is on
chemotherapy because of the risk of infection introduced by puncturing the skin* *Note that this remains a controversial area and others may advocate for the use of acupuncture if sterile needles and adequate skin preparation are provided by a qualified practitioner
Pain management
- Remind the patient not to take Tylenol, ibuprofen or NSAIDS post chemotherapy when it might prevent fever and diagnosis of febrile neutropenia
- Usually pain for patients on cytotoxic chemotherapy can be controlled without acetaminophen or NSAIDS
- Recommend massage or acupressure for the muscle spasm as well as the application of local warmth or cold
- If pain is not well controlled without NSAIDS, I would discuss with the oncologist if ok to prescribe and also for the oncologist to know that the patient is on NSAIDS. Some chemotherapy can adversely affect renal function (ie: cisplatin) and may be more likely to do so if renal function already borderline and especially if patient is also on NSAIDs
Key point Notes Resources CT of head and To rule out metastatic disease

UBC CPD | EDUCATIONAL MODULE Cases Q&A | 11
neck 14. What would you do now?
Key point Notes Resources Physical / coordination exam
You note that she has difficulty with tandem gait and some difficulty with finger nose testing and rapid alternating movements on the right. Plantar responses were equivocal
Gastric cyto-protection Start her on dexamethasone 20 mg qam and rabeprazole 20 mg qam for gastric cyto-protection while on steroids
15. What are the next steps?
Key point Notes Resources Discuss care goals With patient and her husband
Contact the neurosurgeon on call
After reviewing her films, he agrees to take your patient for urgent craniotomy to remove the large cerebellar lesion
Palliative whole brain radiotherapy
Following recovery, she will need palliative whole brain radiotherapy for her remaining brain lesions
Palliative drug benefits You arrange for palliative drug benefits
Home nursing Refer to home nursing in preparation for when she returns home
16. What would you tell them?
Key point Notes Resources Confirm understanding - Ask them what they have been told, what
they understand, and how fast they have noticed things changing. They tell you that things now seem to be changing weekly rather than monthly
Key point Notes Resources Time - Kindly agree with their observation of weeks

UBC CPD | EDUCATIONAL MODULE Cases Q&A | 12
and inform them that once the cancer spreads to the spine that is an ominous sign
- Inform them that radiation therapy takes several weeks to work
Chemotherapy Mention that chemotherapy is not effective
when there are leptomeningeal metastases unless given into the spinal fluid, and even then it is not very effective
17. Is there anything else you should discuss?
Key point Notes Resources Resuscitation - Ask if your patient has spoken to her
husband about her wishes for when she is dying and she says no
- Ask when it is your time for dying would you like it to be peaceful and natural, or are you still wanting to fight at the end? She says she would rather it be peaceful
- Write a progress note in the chart that the patient has decided on no resuscitation
- Write a DNR order
18. What do you do?
Key point Notes Resources Ask what is troubling him
- Rather than just writing a prescription for zopiclone, you take time to find out that he has been wondering if he and his wife made the right decision not to have radiotherapy to the spine
- Rick tells you he is feeling really lonely, especially at night
Offer reassurance - Rick is reassured when you tell him that you have heard of a similar case where it was decided to proceed with radiation therapy where the patient still became paraplegic and died several weeks later
- Reassure him that grieving is normal
Offer support services Ask if Rick would like to be contacted by a hospice volunteer

UBC CPD | EDUCATIONAL MODULE
Participant Feedback Survey
UBC CPD | EDUCATIONAL MODULE
CANCER CARE OUTREACH PROGRAM ON EDUCATION (CCOPE) PROJECT Advanced Cancer Workshop Evaluation Survey
Thank you for taking the time to evaluate this workshop. Your feedback is important in our ongoing efforts to offer these workshops across the province. Once you have completed this survey, please place it in the envelope provided by the facilitator. By filling out this survey, you are providing consent to collect your responses as research data. Please note that all data will be kept strictly confidential.
UBC CPD | EDUCATIONAL MODULE Feedback Survey
DATE: LOCATION: 1. Which cases did you cover?: Case 1 – Larry Goodman Case 2 – Jenny Dalewood Case
3 – Walter Olsen
2. Following today’s workshop, please rate your level of confidence and the level of relevance you believe it has to your practice.
Topic
Level of confidence 1=very low; 5=very high
Level of relevance
1=very low; 5=very high
Role of primary care practitioners along the advanced care continuum
The referral process for advanced cancer
Employ effective techniques for disclosing an advanced cancer diagnosis and discussing the prognosis with patients and their families
Common treatment options for advanced cancers and their expected side effects
Palliative approach to care based on the four pillars of palliative care, with consideration of prognosis and patient perspective
Palliative care resources to support patient care
3. Following today’s workshop please rate your level of agreement with these statements:
1=Strongly Disagree 5=Strongly
a) Role Clarity: I have a clear understanding of my role across the advanced cancer care continuum
1 2 3 4 5
b) Confidence: I am confident that I can provide patients with care and information regarding advanced cancers based on provincial guidelines/recommendations and best practice approaches
1 2 3 4 5
c) Resource Awareness: I am aware of available resources for advanced cancers and palliative care (such as GPOs in the community, GPAC guidelines, BC Cancer Agency, patient resources)
1 2 3 4 5
4. Please indicate your knowledge about the following billing code
(1=no understanding of code; 3 =some understanding; 5=understanding of code)
GPSC Billing code Don’t
understand code
Understand code

UBC CPD | EDUCATIONAL MODULE Feedback Survey
14063 – palliative care planning fee 1 2 3 4 5
Do you intend to use the palliative care planning fee for future advanced cancer cases? If so, how?
5. Please rate your perceptions of the workshop:
Poor Average Excellent a) Content: Relevance to my practice 1 2 3 4 5 c) Interactivity: Opportunities for interaction 1 2 3 4 5 d) Facilitators/presenters: Organized and respectful 1 2 3 4 5 e) Pre-reading and supplementary materials 1 2 3 4 5 f) Session format 1 2 3 4 5 g) Overall rating of the workshop 1 2 3 4 5
5. What was the most effective part of this workshop? Why? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
6. How could this workshop be improved? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
7. Is there anything related to advanced cancer that was not covered in the workshop that would be
useful to your practice? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
8. Do you feel that there was any industry bias in this workshop? Yes No ____________________________________________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________

UBC CPD | EDUCATIONAL MODULE Feedback Survey
9. Additional comments or suggestions: ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ 10. In which town / community do you primarily practice? ___________________________________
11. I am a: Family physician / General Practitioner Specialist Resident / Student Nurse / Nurse Practitioner Allied Health Professional Other health care provider (please specify) ___________________________________
12. How many years have you been in practice? Less than 1 1 to 5 6 to 10 11 to 15 16 to 20 21 to 25 26 to 30 30+ N/A
13. What type of practice do you work in? Solo Group


















