
CANCER ADVOCACY COALITION OF CANADA REPORT … REPORT CARD O… · 2 REPORT CARD ON CANCER IN...
44
REPORT CARD REPORT CARD CANCER ADVOCACY COALITION OF CANADA ON CANCER IN CANADA TM 2010–2011 Fighting cancer is hard enough– your government should not make it worse.
-
Upload
phungthien -
Category
Documents
-
view
214 -
download
0
Transcript of CANCER ADVOCACY COALITION OF CANADA REPORT … REPORT CARD O… · 2 REPORT CARD ON CANCER IN...

REPORT CARD REPORT CARDCANCER ADVOCACY COALITION OF CANADA
ON CANCER IN CANADA TM
2 01 0 – 2 011
Fighting cancer is hard enough–your government should not make it worse.

2 REPORT CARD ON CANCER IN CANADA, 2010–11
CACC EDITORIAL ADVISORY COMMITTEEPierre Major, David Saltman, Sandi Yurichuk, Colleen Savage
STATEMENT OF NON-CONFLICT. Authors were not compensated for the articles in this publication; the work is entirely theirs and original.
DESIGN Bob Wilcox
SPECIAL THANKS to all the cancer patients and patient-centred cancer groups who offered their insight and support forthis publication. In particular: the Best Medicines Coalition, the Canadian Breast Cancer Network, the Canadian CancerSociety, the Canadian Testicular Cancer Association, the Canadian Cancer Action Network, the Canadian Lung Association,the CLL Patient Advocacy Group, CML Society of Canada, GIST Sarcoma LifeRaft Group Canada, the Global Lung CancerCoalition, Lung Cancer Canada, the London and District Multiple Myeloma Support Group, Ovarian Cancer Canada. Manyother organizataions and individuals generously share their experiences and ideas with us all year, including cancer agen-cies, policy and research institutes, think-tanks, elected officials and health professionals from coast to coast. We applaudthe renewed mandate of the Canadian Partnership Against Cancer to bring the cancer community together in constructivecollaboration.
A NOTE OF APPRECIATION to Cohn & Wolfe for a generous amount of pro bono public relations work on our behalf andfor their spirited commitment to the cause.
BOARD OF DIRECTORSDauna Crooks (Co-Chair) RN, DNSc, is currently the Dean of the Faculty of Nursing, University of Manitoba as well as an
Associate Professor at both the University of Toronto and McMaster University. Dauna is also a member of seven pro-fessional organizations and has numerous grants and publications.
Douglas Emerson has spent the last decade working in communications, public affairs and government relations. He losthis father to cancer in 2005.
James Gowing (Past Chair) BA, MB, BS, FRCPC, founded the community cancer clinic in Cambridge, ON and establishedthe National Conference on Community Cancer Clinics. He has been an advocate for community cancer care and can-cer control throughout his 40-year medical career.
Darwin Kealey (Past Chair) BA, MA, is a former executive public servant and international entrepreneur with extensiveadvocacy experience.
Kong Khoo (Vice Chair) MD, FRCPC, is a Medical Oncologist based in the Southern Interior of British Columbia in Kelowna. Pierre Major (Co-Chair) MD, has worked in Medical Oncology for 30 years and has a special interest in treating elderly
patients with cancer. He has over one hundred publications and is actively involved in developing novel treatments forcancer including using viruses to attack cancer cells.
Jackie Manthorne, BA, BEd, is CEO of the Canadian Breast Cancer Network (CBCN), a member of the Metastatic BreastCancer (MBC) Global Advocacy Advisory Board, the global Breast Cancer Dialogue Series, the Community CapacityBuilding Committee (CCBC) of the Canadian Breast Cancer Initiative (CBCI) and CCBC Ambassador-at-Large.
Robert Pearcey MA, MBBS, FRCR, FRCPC, is a practicing academic Radiation Oncologist and Professor of Oncology inEdmonton. He also has 14 years of previous administrative experience in Radiation Oncology and is the current chairof the specialty committee in Radiation Oncology for the Royal College of Physicians of Canada.
Joseph Ragaz MD, FRCPC, is a Senior Medical Oncologist and breast cancer researcher, Clinical Professor, Faculty ofMedicine and School of Population Health, University of British Columbia, Vancouver, B.C.
David Saltman MD, PhD, FRCP(C) is the Chair and Professor of the Discipline of Oncology, Faculty of Medicine, MemorialUniversity. His current interests include cancer advocacy, community oncology and telehealth.
Sandeep Sehdev MD, FRCPC, is a community focused Medical Oncologist at the William Osler Health Centre in Brampton,Ontario—one of Canada’s largest community hospitals—where he has worked since 1992. He is past chair (five years)of the Pharmacy and Therapeutics Committee.
Elizabeth (Liz) Whamond has a long and distinguished history in the Canadian cancer community. In 2001, Ms.Whamond was one of the founding members of the Canadian Cancer Action Network and currently serves as Chair aswell as the CCAN representative on the Cancer Journey Advisory Group of the Canadian Partnership Against Cancer.
Sandi Yurichuk (Vice Chair) BS, MBA, PhD candidate, is a cancer advocate and management consultant in the field of oncology.
BOARD SUPPORTDaniel Gillespie BSc, is a graduate of the University of Toronto. He has been a consultant and research assistant to the
Cancer Advocacy Coalition of Canada for the past five years.Colleen Savage is a public affairs and communications consultant serving as President & CEO for the CACC.
© 2011, CACC except where otherwise noted.All photos supplied by the individuals and used with their consent.
Cancer Advocacy Coalition of CanadaSuite 204 – 60 St. Clair Avenue East
Toronto, Ontario M4T 1N5E-mail [email protected] toll free 1-877-472-3436
DISCLAIMER: Cancer Advocacy Coalition of Canada (CACC) provides the Report Card for general information related tocurrent events and topics relevant to cancer in Canada. While CACC makes best efforts to ensure the accuracy and timeli-ness of the information contained in the Report Card the information is taken from various public and private sources sothat no responsibility can be assumed by CACC for the accuracy or timeliness of this information. The opinions expressedin the Report Card are those of the individual authors of individual articles and material. Their views do not necessarilyreflect the views of CACC.
WARNING: CACC’s Report Card should not be used for the purpose of self diagnosis, self treatment or as an alternative tomedical care. If you have any concerns arising out of the information contained in CACC’s Report Card, you should con-sult your own physician or medical advisor. If you suspect you have cancer, seek professional treatment immediately.
VOLUME 13, WINTER 2010–11
REPORT CARD REPORT CARDON CANCER IN CANADA
CANCER ADVOCACY COALITION OF CANADA
About the Cancer Advocacy Coalition of Canada
The CACC is a full-time,registered, non-profit cancergroup dedicated to advocacy,public education, policy analy-sis and evaluation of healthsystem performance. TheCACC is not a charity andoperates on unrestricted grantsfrom sponsors based on guide-lines that ensure the organiza-tion’s autonomy. The CACCpublishes Canada’s onlyindependent evaluation ofcancer system performance,the annual Report Card onCancer in Canada. The Boardof Directors is comprised ofunpaid volunteer oncologists,health sector executives andpatient advocates from acrossthe country.
Our Vision for theCancer SystemAn effective, comprehensive,evidence-based cancer systemthat offers Canadians the bestchances for preventing andtreating this disease, andaddresses the emotional,physical and financial needsof patients and survivors.
Our Goals: to benefitcancer survivors and all Canadians• Consistent adherence to bestpractices in cancer care andprevention, making best use offinancial and human resources • Accountability to patients,survivors and taxpayers• Transparency of decision-making, priority-setting andperformance measurement • Reduction of the emotional,physical and financial distressassociated with a cancerdiagnosis• Access to best practices indisease prevention and timely,effective treatment options • Increased awareness ofprevention choices
TM

TRIBUTEA Tribute to Linda Jalbertby Joseph Ragaz, MD, FRCPC
EDITORIALby Pierre Major, MD and Colleen Savage
The Cancer Patient’s Challenging Journey
ADVOCACYOpen Letter to Physiciansfrom Alberta Health Services
Walking the Tightrope: Physician Advocacy and Institutional Fidelityby David Saltman, MD, PhD
PREVENTIONCancer Prevention in Canada: The Sooner the Betterby Joseph Ragaz, MD, FRCPC
Prevention Update: SmokingRare Cancers Update: Orphan Drugs
LIVING WITH CANCERChronic Lymphocytic LeukemiaOvarian CancerTesticular Cancer
UPDATE ON LIVING WITH CANCERChronic Myelogenous LeukemiaMultiple MyelomaNeuroendocrine TumoursGIST
THE ORGANIZATION OF CANCER CARE Waiting Times by Pierre Major, MD
Should Clinical Trials be Considered Part of “Standard of Care”?by Susan F. Dent, BSc, MD, FRCPC and Sandi Yurichuk, BSc, MBA, Ph.D. candidate
The Role of the Nurse Practitioner and Clinical Pharmacistby Jonathan Edwards, BSc, Scott Edwards, PharmD, and David Saltman, MD, PhD
Bone Marrow Transplantation: Improving Outcomes for Canadian Patientsby Ronan Foley, MD, FRCPC
Personalized Medicine: What is Missing?by Jennifer Levin Carter, MD, MPH with Jillian Lokere
The 21-Gene Assay: Canada’s Uneven Responseby Joseph Ragaz, MD, FRCPC
Noteworthyby James D. Gowing, BA, MB, BS, FRCPC
4
5
6
8
9
10
15
16
18
21
23
30
33
38
41
44
IN THIS ISSUE
REPORT CARD ON CANCER IN CANADA, 2010–11 3
4 REPORT CARD ON CANCER IN CANADA, 2010–11
Style, grace and courage. Three little words that sumup how Linda Jalbert lived and faced life’s biggestchallenges. Ever the optimist, Linda’s vivacious per-sonality and sense of humour were inspirational andinfectious— she was loved by all who knew her.
Linda’s personality seemed perfectly suited to hercareer in the hospitality industry and over the yearsshe worked for some of Montreal’s best hotels—asDirector of Sales for the Ritz Carlton, the FourSeasons and the Loews Hotel Vogue. Her passion forher work radiated from her, and impressed col-leagues and clients alike with her professionalism,spirit and energy.
Her fervor for her career was matched by that ofher beloved husband, Renaud, himself a GeneralManager of luxury hotels. Their love, friendship andpartnership was evident to all who knew them, andRenaud was a constant source of support for Linda,always at her side through the ups and downs thatcame their way.
And challenges certainly came their way. At only49, Linda was diagnosed with high-risk breast cancer.But, as only she could, Linda faced this battle headon—never complaining, the epitome of courage andoptimism. While undergoing rounds of chemotherapyand radiation, she remained bubbly and witty, neverallowing friends, loved ones, hospital staff or evenother patients around her to feel down.
And thus, Linda’s new role as a cancer advocatewas born. In 2005, she was one of the first patientsin Canada to receive Herceptin, but was concernednot by her own condition, but about other womenwho may not get access to this drug. She took herstory to the Globe & Mail and through hard workand dedication was able to help thousands of otherpatients across the country gain access to a valuabletreatment.
Inspired to continue helping other cancerpatients, accepting a seat on the Board of the CACCwas a natural next move and her energy, enthusi-asm, solid counsel and efficiency were appreciatedby all of us who had chance to work alongside her.
With her breast cancer undetectable, she seemedto have beaten the odds. And none of us were sur-prised that a woman with her determination and
optimism could overcome such an aggressive disease.But, cancer dealt Linda another cruel blow. Diagnosedwith lung cancer in 2008, she again remained true toform, battling courageously while retaining her spiritand zest for life, right until the end.
We all know too well the devastation and griefthat cancer leaves in its wake. While we can neverfill the hole that Linda has left in our hearts, we cankeep her memory alive by continuing her work withthe same spirit, energy and passion that she sharedwith so many.
by Joseph Ragaz, MD, FRCPC
A Tribute to Linda Jalbert

As Canadians go the polls this year, federally and in fiveprovinces and at least one of the territories, we repeatedlytell pollsters that our number one priority is health. In allthese jurisdictions we will hear the candidates conclude:first, that health already consumes too much of the budget;second, that they agree we should do more; and third, thattheir solutions are the best choices, given all the competingdemands.
We all know it will not be enough. This edition of theReport Card is meant to help every political candidate in thecountry understand what it means to carry the physical,emotional and financial burdens of cancer. For the cancerpatient, Winston Churchill said it best, “if you are goingthrough hell, keep going.”
During the cancer patient’s challenging journey, the cur-rent health system can seem self-absorbed, tilted towardoverhead and paper processes rather than direct patient serv-ices. The weight of administration comes as a direct result ofgovernments’ belief that rigid guidelines, forms and applica-tions will provide a speed bump for utilization and a veil forservice denial. A clever strategy, until it is over-used. Today’shealth system often appears locked up, with creativity aimedsolely at finding new ways to say no.
Front-line health care professionals are not responsible forthe design and funding of Canada’s multiple health systems.Our governments are. In fact, the health professionals in thiscountry work against discouraging odds to adjust to increas-ing constraints, shifting priorities, growing caseloads and alack of capital and human resources. They save our lives.What does your government do for you?
The people we elect this year will become responsible fornegotiating a new federal/provincial/territorial healthaccord. The new health accord will establish priorities, tar-gets, timelines and a new funding base for the delivery ofhealth services in Canada. How will cancer fare?
Cancer prevention. The science for cancer preventioncontinues to improve, consistently linking cancer withlifestyle choices, harmful products or environments, as wellas genetic markers. Funding for cancer prevention lagsbehind this knowledge, leaving 50 per cent of all avoidablecancer diagnoses looming in the future, for lack of actiontoday. In many of these situations legislative protections areneeded, in other cases, active medical intervention is best,including counselling to improve lifestyle choices, or drugtherapy.
Waiting times. The last accord defined five priorityareas, with targets and new funding to address the increasingproblem of waiting times for health services. For cancer, thatlist included only radiation oncology. Indeed, as the illustra-tion on the following page shows, the waits at every point ofactivity quickly accumulate to become a substantial delay,with overwhelming fear and anxiety for the patient.
Provinces agreed to address the five priorities over fiveyears and report annually to their citizens on progress. For
this, the provinces received $5.5 billion as part of the $41 bil-lion health accord deal. The definitions of a waiting time forcancer care, other than radiology, remain impossibly differ-ent across the country, other than a general preference tostart counting at “ready to treat” (meaning post-surgery); notthe first suspicious test result, not even the diagnosis, butsomewhere farther down the path. Added to these manoeu-vres is the unanswered practical question: if the waiting timefor one type of surgery in your province has dropped signif-icantly in the past few years, what happened to the waits forother surgical procedures?
Catastrophic drug coverage. Some perspective, please.Creating a new pharmacare plan, with expanded eligibilityso more citizens have coverage for a limited list of drugs, isnot the same as protection from financial ruin caused byextraordinary prescription drug costs. The provinces thatclaim to offer a catastrophic drug plan do no such thing.Federal and provincial officials duck responsibility, pointingat each other, invoking amnesia of past promises, while can-cer patients are dealt another crushing blow. A Canadianwho has to choose between the treatment recommended bythe oncologist or the financial solvency of the family has nohappy ending. True catastrophic drug coverage would meanCanadians are not confronted with that decision. One payercannot handle such a plan. The health accord is an idealinstrument to formulate a multi-payer plan.
Accountability. As taxpayers, we object to the layers ofgovernment fighting over our wallets. We expect clear, hon-est answers for the “difficult funding decisions” that impedetimely access to cancer care. How does one priority supersedeanother?
Provinces insist their constitutional authority for thedelivery of healthcare relegates the federal government tothe role of ATM. This ATM needs better rules: more flexibili-ty to deliver our money back to us for services we want; anda higher degree of surveillance over the provincial spendingof that money. More importantly, the federal role for estab-lishing and ensuring national standards in healthcare is theonly mechanism that will alleviate the persistent inter-provincial disparities in access to care. If a new health accordis to offer financial incentives to the provinces for meetinghealthcare targets, an equivalent range of penalties are need-ed for failure.
By the end of 2011, our newly elected governments acrossthe country will be deeply engaged in negotiations for a newhealth accord. In the last two years, approximately 345,000Canadians were diagnosed with cancer—and this year willbring more. Eighty-two per cent of Canadians report cancerhas touched their lives either through their own illness orthat of a close friend or family member. It would appear tobe a substantial group of voters. This is the year to be heard.
by Pierre Major, MD, Co-Chair of the Board of Directors, andColleen Savage, President & CEO
E D I T O R I A L
REPORT CARD ON CANCER IN CANADA, 2010–11 5

The Cancer Patient’s Challenging Journey
Routinevisit toDoctor
1
Follow-up4Later5
Fiveyearslater
6
Firstsuspicioustest result
Tests to rule outsimple explanatons
no referral
DEAD END
DEAD END
DEATH
GOOD NEWS
GOOD NEWS
CONGRATULATIONS!
RECOVERYand more
tests
Tests
Pathology
Imaging
WA
IT
WA
IT
GP Disbelief/ Misdiagnosis
TREATMENTNOT
SUFFICIENT
More testsTOUGHDECISIONS• risks• side effects• quality of
life• financial
impact
Rapid assessment,go to DIAGNOSIS
Go back to step 3
Distraction–find“miracle”cure onlineMore
chemo
Moreradiation
Moreclinicaltrials
Moresurgery
What drugs?
Supportive/palliative care
RECURRENCE
How much more?
YOU’RE ALIVE.
REFERRAL
6 REPORT CARD ON CANCER IN CANADA, 2010–11
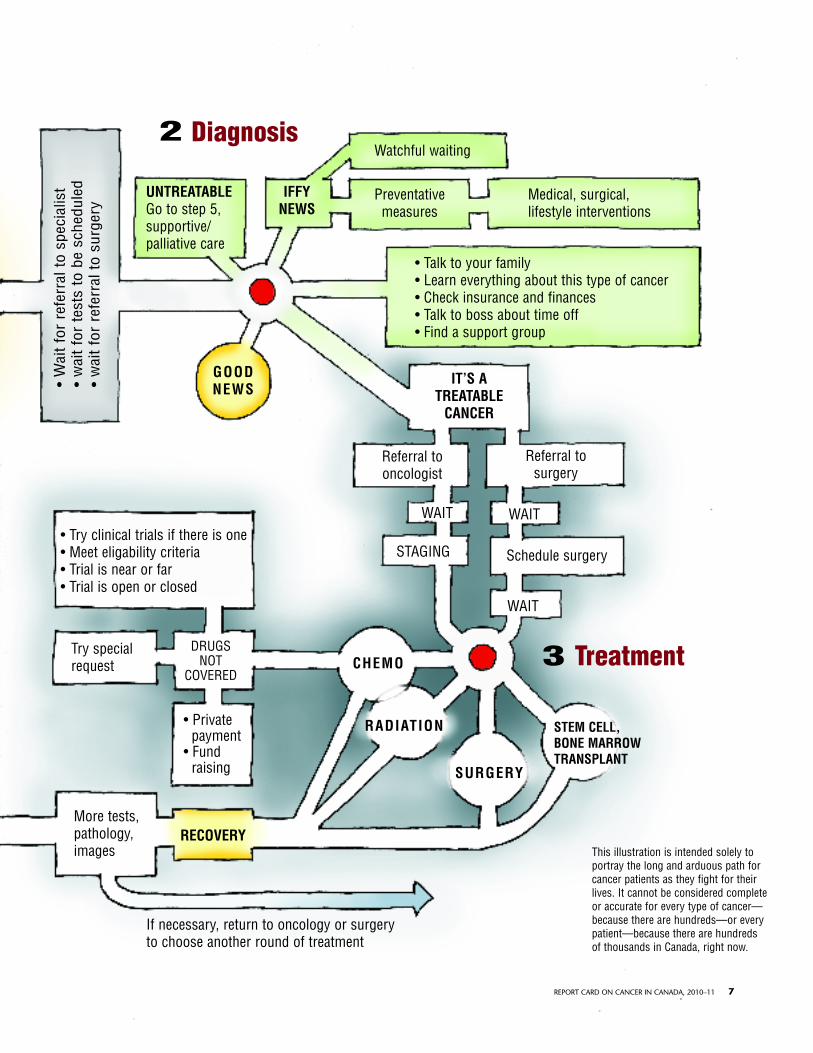
Diagnosis2
Treatment3
• W
ait
for
refe
rral
to
spec
ialis
t•
wai
t fo
r te
sts
to b
e sc
hedu
led
• w
ait
for
refe
rral
to
surg
ery
UNTREATABLEGo to step 5,supportive/palliative care
GOOD NEWS
CHEMO
RADIATION
RECOVERY
SURGERY
STEM CELL,BONE MARROWTRANSPLANT
IFFYNEWS
IT’S ATREATABLE
CANCER
Watchful waiting
Preventativemeasures
Referral tooncologist
Referral tosurgery
Schedule surgery
WAIT
STAGING
WAIT
WAIT
Medical, surgical,lifestyle interventions
• Talk to your family• Learn everything about this type of cancer• Check insurance and finances• Talk to boss about time off• Find a support group
• Try clinical trials if there is one• Meet eligability criteria• Trial is near or far• Trial is open or closed
If necessary, return to oncology or surgery to choose another round of treatment
Try specialrequest
• Privatepayment
• Fundraising
More tests, pathology,images
DRUGSNOT
COVERED
This illustration is intended solely toportray the long and arduous path forcancer patients as they fight for theirlives. It cannot be considered completeor accurate for every type of cancer—because there are hundreds—or everypatient—because there are hundredsof thousands in Canada, right now.
REPORT CARD ON CANCER IN CANADA, 2010–11 7

8 REPORT CARD ON CANCER IN CANADA, 2010–11
ADVOCACYADVOCACY
Open Letter to PhysiciansFrom the Alberta Health Services Website: www.albertahealthservices.ca/4052.aspMarch 16, 2011
It is our responsibility as clinical leaders, as it is the collective responsibility of all physicians and health carepractitioners, to unequivocally address public concerns that our colleagues are restricted in any way fromadvocating on behalf of their patients.
This is not a political issue up for debate. It is not opinion or commentary.As physicians and practitioners, it is our duty to our patients, our colleagues and our profession to represent
and articulate the needs and best interests of our patients, and the health system as a whole. It is a standard setcenturies ago within the Hippocratic Oath and it remains the touchstone for our profession to this day. As such,it is an expectation of the College of Physicians and Surgeons of Alberta Code of Conduct, and of the CanadianMedical Association Code of Ethics.
This, an open letter to all Alberta physicians, is our personal commitment to do all in our power to enableevery physician in Alberta to meet this standard. As medical leaders, we must intervene, even at the risk ofbeing drawn into the current debate, because we have a higher and greater obligation to our patients. Wewant to make it clear to our patients and the public that caregivers can and must advocate without hesitation.
Today, we are stating for the record, as per the Alberta Health Services Medical Staff Bylaws & Rules,developed by physicians and practitioners for physicians and practitioners, that medical staff and AHS share jointresponsibility and accountability for the provision of health services to Albertans. Furthermore, the AHS MedicalStaff Bylaws & Rules describe the behaviour and professionalism expected of individual medical staff membersand AHS leaders. Included is an explicit statement confirming the right and responsibility of medical staffmembers to advocate for their patients.
The Bylaws & Rules also ensure a system of protection that affords due process and procedural safeguardsfor physicians with respect to their actions and interactions with AHS. In addition, the Bylaws & Rules providemultiple avenues and mechanisms for physicians, and medical staff, to discuss and report patient care issues,and to participate proactively with AHS in improving the health care system.
These words represent more than bylaws in and of themselves. They are founded on a set of principles, andAlberta Health Services will not allow these principles to be undermined. These principles as defined in the AHSCode of Conduct are intended to guide all actions and interactions, and underpin all AHS bylaws, policies,procedures, standards, guidelines, regulations and directives that must be followed by AHS and those whoprovide services on behalf of AHS. We must work in the best interests of patients and clients, we must exerciseour best judgement, we must raise our hands if we see something we think is not best for our patients or ourorganization, and we must have the courage to stand up for what is right.
The AHS Code of Conduct does not restrict a physician or other practitioner to speak out, quite the opposite.In essence, we are required to bring our concerns forward; we are not merely given permission to do so. TheCode sets out a number of options for raising issues including speaking to a manager or a physician leader,speaking to the Ethics and Compliance Officer or by contacting the External Confidential Reporting andDisclosure Service.
Today, we are speaking personally as physicians, and making a commitment as leaders, that we supportour physician colleagues in upholding their duty and responsibility to advocate for their patients. This is acommitment that goes beyond any policy and to the heart of the oath made by all of us.
Now, and as we move forward in the weeks and months ahead, we have an opportunity to define the futureand to develop a partnership that ultimately benefits our individual patients, and the health system as a whole.
Sincerely,
Dr. Chris Eagle, Acting CEO & President, Alberta Health ServicesDr. David Megran, EVP and Acting Executive Lead for Quality and Service ImprovementDr. Francois Belanger, Acting EVP and Chief Medical Officer
Alberta HealthServices

REPORT CARD ON CANCER IN CANADA, 2010–11 9
By DAVID SALTMAN, MD, PhD
The American Medical Association defines physician advoca-cy as action by a physician to promote those social, econom-ic, educational, and political changes that ameliorate the suf-fering and threats to human health and well-being that he orshe identifies through his or her professional work andexpertise.1 The spectrum of opportunities for physicianadvocacy in our society is very broad. It ranges from advocat-ing on behalf of a single patient, to advocating for a commu-nity or for society as a whole.
Despite the public endorsement of advocacy by medicaleducators, national accreditation bodies and professionalmedical associations, evidence suggests that physicians infre-quently get engaged in advocacy activities at a local ornational level. There are some notable exceptions. Probablythe most famous is Dr. Helen Caldicott, the Australian pedi-atrician and antinuclear activist. Dr. Fernand Turcotte fromthe University of Laval has been a strong advocate for ban-ning tobacco products and the mining and sale of asbestos.
Physician advocacy groups include the InternationalPhysicians for the Prevention of Nuclear War, an organiza-tion that was awarded the Nobel Peace Prize in 1983. TheOntario College of Family Physicians and many individualdoctors advocated successfully for banning cosmetic pesti-cides in Ontario. The Canadian Association for theProtection of the Environment (CAPE) has more than 5,000members and advocates for a number of environmentalissues that affect Canadians. Physicians in Northern Albertahave spoken publicly about the concerns of possibleincreased rates of cancer in communities near or down-stream from oil sands projects and uranium mines, despiteopposition from within the medical profession, HealthCanada, industry and governments.
There have been many ideas put forward as to why morephysicians don’t engage in advocacy activities. Perceived bar-riers include a lack of advocacy training, physicians’ busylives and concerns about the negative effect public advocacymay have on career advancement.2 We are more likely toendorse and celebrate physicians who are involved in directpatient care, basic sciences, drug development and education
but less likely to acknowledge the efforts of physician advo-cating for changes in public policy or protection of the envi-ronment. These views may often be in conflict with the val-ues we try to instill in medical students and residents.
The vast majority of oncologists in Canada are salariedemployees of healthcare institutions. Many have clinical orfull-time university appointments. Those who do advocateinternally or externally may find that their cause or agendacould be at odds with their employer and academic institu-tion. Many of these institutions have either formal or infor-mal fidelity agreements, which severely limit an advocate’sability to speak publicly about a number of issues, even thosethat do not involve confidentiality issues. Advocacy activi-ties may result in physicians being in conflict with govern-ment healthcare priorities and agendas. In an era when hos-pitals and cancer centres are run as big business, corporateloyalty and other values may sometimes override the bestinterests of society and the environment.
The recent endorsement of community and societal advo-cacy as a requirement for successful completion of under-graduate medical training in this country by the MedicalCouncil of Canada and by some residency programs, willhopefully lead to more physician advocates. Healthcareadministrators and Deans of our Medical Schools need toencourage and facilitate advocacy activities. Public discourseabout how cancer drugs are funded in Canada, concernsabout secondhand smoke, the use of cosmetic and agricul-tural pesticides and other relevant issues should be wel-comed by our hospitals and universities and not seen as anattempt to undermine those institutions or the politicalprocess.
David Saltman, MD, PhD is the Chair and Professor of theDiscipline of Oncology, Faculty of Medicine, Memorial University.
References1 American Medical Association. Declaration of Professional Responsi-
bility: Medicine’s Social Contract with Humanity. Available at: http://www.ama-assn.org/ama/upload/mm/369/decofprofessional.pdf.Accessed February 9, 2011.
2 Earnest Ma, Wong SL, Federico SG. Physician advocacy: What is itand how do we do it? Academic medicine 2010; 85:63-7.
WALKING THE TIGHTROPE
Physician Advocacy and Institutional Fidelity

by JOSEPH RAGAZ, MD, FRCPC
The objective of this report is to show that prevention is thesingle most cost-effective initiative Canada could successful-ly escalate quickly in the fight against breast (and other) can-cers. The report will provide an updated review of theresearch on breast cancer prevention and reveal its currentpotential impact for breast cancer risk reduction. The scien-tific community has already been made aware of these datathrough the normal scientific channels, albeit not all clini-cians are aware. So now it is imperative that the informationbe presented to all the medical community and the otherstakeholders - the Canadian public and administrative andmedical policy decision makers.
The research shows that if individual lifestyle factors andthe identified preventive medical interventions were appliedconsistently to high risk women, then hormone receptorpositive breast cancer could be prevented in 20-50 per centof cases. The result would be several thousand fewer breastcancers each year in Canada. This report will summarize thedata and identify some of the challenges that delay imple-menting these interventions.
BackgroundBreast Cancer mortality has decreased by approximately 25-30 per cent in most parts of the western world over the lasttwo decades, with variations across Canada depending onlocal services.1,2
The main factors known to impact breast cancer mortalityinclude:1 Widespread public education about breast cancer leading
to earlier diagnosis particularly by using screening mam-mography.
2 Evidence-based therapy i.e., effective surgery, adjuvantchemotherapy, hormonal therapy, radiotherapy and post-recurrence therapy.
Breast cancer incidence rates have stabilized since the mid1990s and slowly decreased since the late 1990s. This hasbeen attributed, according to some reports, to the reduced
use of hormonal replacement therapy (HRT) based on theU.S. Women’s Health Initiative group (WHI) publication ofadverse HRT effects.3 However, breast cancer incidence rateshad already stabilized in the mid-1990s, and thus other rea-sons ought to be considered.
Some aspects of breast cancer prevention, common to car-diovascular and breast cancer pathogenesis and related tolifestyle, have been increasingly practised by small cohorts ofmostly urban-located western populations – such as weightreduction and diet focused on vegetables, fruit and exercise.In addition, across the western world there has beenincreased use of anti-cholesterol and anti-inflammatoryinterventions,4 which may also beneficially affect breast can-cer risk rates.
Despite the decreasing mortality rates for breast cancerover the last decade, more than 22,000 women are still diag-nosed each year in Canada and of these, close to 20 per centwill die, with absolute numbers of breast cancer deathsincreasing annually (from 4,335 in 1986 to 5,066 in 2007).5
The ongoing breast cancer morbidity and the anguish ofthose affected remain one of the largest public health con-cerns of the female population.
Practical Aspects of Cancer PreventionOf all breast cancer cases diagnosed in Canada annually, lessthan five per cent are associated with the expression of iden-tified mutations in the two known genes: the BRCA-1/BRCA-2. Carriers of these genes have a 60–80 per cent life-long chance of developing breast cancer and a 40–60 percent lifelong risk for ovarian cancer, particularly those withthe BRCA-2 mutations.6,7
These patients and their families are now part of thegenetic counselling programs in most cancer institutionsacross the country, involving professional counsellors, withemphasis on two important steps. 1 Preventive surgery in the form of bilateral mastectomy
and/or bilateral oophorectomy. 2 Medical interventions with tamoxifen and raloxifene.
However, the remaining breast cancers, although still likelyhaving some genetic component other than BRCA-1/BRCA-2,
10 REPORT CARD ON CANCER IN CANADA, 2010–11
CANCER PREVENTION IN CANADA
The Sooner the Better
PREVENTIONPREVENTION

cannot be identified by a single genetic test before diagnosisand thus are not sought out by organized initiatives aimed atprevention. There is evidence that a large sector of this pop-ulation of women would benefit from the lifestyle and med-ical interventions described in this review.
To implement population-based breast cancer preventionas part of the accepted clinical guideline programs acrossCanada will, however, require infrastructure changes and ini-tiatives, including the formation and funding of dedicatedbreast cancer prevention clinics, ideally associated with, orunder the auspices of existing cancer facilities. Currently,only a few U.S. based cancer centres provide preventioncounselling by oncologists to non BRCA-1/BRCA-2 women,and there are currently no dedicated breast cancer coun-selling centres in Canada for the purpose of breast cancerprevention. Due to expected population health gains andrelated long-term societal cost savings as described below,this should be a high priority.
At least three steps are required:1 identify which breast cancer risk reduction interventions
are evidence-based and most cost-effective; 2 identify women at higher risk using quantitative predic-
tion tools8 and preferentially counsel this group; 3 finalize the cancer prevention logistics: identify who
should do the counselling, who should fund it and con-sciously expand the focus from diagnosis and treatmentof established disease to include prevention.
Risk Factors and Risk-reducing Interventions Risk measure, named as relative risk (RR) or hazardrates (HR), is a statistical term that compares eventswith or without a given risk factor or intervention.If risk is unaltered, RR=1.0; if risk increases, forexample by 20 per cent, it is expressed as RR=1.2;if risk is reduced by 20 per cent, RR=0.8.
Current literature indicates that the impact of some of therisk-reducing interventions could be profound, with rangesof 20–50 per cent fewer new hormone receptor positivebreast cancers annually, (i.e., RR=0.5–0.8) depending on theindividual intervention. These data permit estimates that ifrisk-reduction interventions are practiced with a higher levelof compliance, several thousand new breast cancer cases inCanada could be avoided annually. What are these individ-ual risk factors and possible interventions?
1. Excess weight and obesityThe current western diet (based on high carbohydrates, ani-mal fat with high cholesterol and too few vegetables andfruits), associated with obesity and higher body mass index(BMI), has a well-established link to higher breast cancerrates, particularly if associated with a sedentary lifestyle.1-3
High breast densities on mammogram and or higher serumestrogen hormonal levels are probably markers of thesemetabolic phenomena. Obesity, with adipose tissue as a
source of carcinogenic molecular growth factors, has beendescribed as increasingly relevant in the recent literature.9
The impact of long-term dietary and weight-reducinginterventions on breast cancer risk is not precisely known, asno long-term validated intervention studies have been donefor breast cancer. The proposed prevention clinics aimed athigh risk populations will have potential to study the impactof these interventions. In addition, new data are accumulat-ing on the adverse effects of obesity after a breast cancerdiagnosis,10 showing potential for improving survival ratesthrough life style initiatives, in women already diagnosedwith breast cancer.
What about interventions leading to obesity reduction,with dieting and exercise and or more targeted interven-tions? Old literature did not support a substantial influenceof dietary manipulation on either breast cancer rates orbreast cancer outcomes after the diagnosis. However, morerecent studies come to a different conclusion. George et al.11
showed, in 670 women with breast cancer, that patients con-suming better-quality diets (as defined by higher HealthyEating Index-2005 scores) had a 60 per cent reduced risk ofdeath from any cause when compared to ordinary diet,(HR=0.40, 95 per cent CI: 0.17, 0.94) and an 88 per centreduced risk of death from breast cancer (HR=0.12, 95 percent CI: 0.02, 0.99)
2. ExerciseRecent evidence associates regular aerobic exercise withreduced breast cancer incidence rates and improved survivalin women with diagnosed breast cancer.12-14 In 2008, Irwinet al.15 reported that when compared with inactive women,the multivariate hazard ratios (HRs) showed a 31 per centreduction of total deaths for women who are physicallyactive in the year before diagnosis – meaning approximatelytwo to three hours per week of brisk walking. (HR=0.69, 95
REPORT CARD ON CANCER IN CANADA, 2010–11 11
The results are in…An ounce of prevention equals thousands of pounds of cure

per cent CI 0.45 to 1.06; P=.045.) In patients who exercisedtwo years after diagnosis, even larger benefits were seen, witha 67 per cent reduction of deaths (HR=0.33, 95 per cent CI,0.15 to 0.73; P=.046).
The estimates for risk reduction depend on the quality ofthe study, the duration of follow-up and the intensity ofexercise, but fall in the range of 20-30 per cent (RR=0.7-0.8)or more with prolonged exercise. On the basis of 20-30 percent risk reduction, comparing 1,000 women who do notexercise with 1,000 women who do, the sedentary groupwould produce 100 cases of breast cancer while the exercis-ing group would produce 80 or less. Thus, a large number ofthe annual 22,000+ new breast cancers in Canada could beavoided through lifestyle changes that incorporate regularexercise, simultaneously reducing cardiovascular risk.
3. Alcohol There is rising evidence for an association of increased breastcancer risk with alcohol intake,16,17,18 with some data indi-cating dose dependence: the more alcohol, the higher breastcancer incidence. More than six drinks per week wouldincrease the risk by 30-90 per cent compared to less than oneto two drinks per week (RR=1.3–1.9). The mechanism is like-ly related to metabolic changes leading to increased breasttissue estrogen effect, which is considered carcinogenic.17
4. Medical interventions with breast cancer preventionagents
i. Tamoxifen. At least four randomized trials have doc-umented a 40–50 per cent risk reduction of estrogen positiveinvasive and in situ breast cancer rates by tamoxifen(RR=0.5-0.6) given to women at high risk of breast cancerHigh risk was determined by the Gail model, based on firstdegree family history at a young age, or abnormal pathology(atypia lobular carcinoma in situ, etc.).19 Prolonged adversepublicity associating tamoxifen with uterine cancer andincreased thromboembolism (clotting), cited in the earlyyears when they were identified but not rated accurately, hasnegatively affected its use in prevention. More recentupdates of tamoxifen net-effect in patients with establishedbreast cancer clarify the picture.
• Incidence rather than mortality from uterine cancer isincreased (i.e., more uterine cancers are diagnosed ontamoxifen, but because of early diagnosis most arecured), with reduced breast cancer mortality leading toa much larger net gain: reduction of overall mortality.20
• Thromboembolism rates are similar to those on birthcontrol pills and or hormone replacement therapy, sothe rates are not disproportionately increased withtamoxifen.
• Updated data from the original NSABP P-1 preventiontrial show minimal risk of uterine cancer or throm-boembolism among younger women, under age 55,while the benefit of breast cancer risk reduction of40–50 per cent is significant.21
• Most recently, Noah-Vanhoucke et al.22 provided oneof the most comprehensive cost-benefit analysis oftamoxifen. Their meta-analysis of four randomized tri-als indicated that tamoxifen chemoprophylaxis, forpostmenopausal women under age 55, is cost-effective
in reducing breast cancer incidence and improving lifeexpectancy.
Thus, tamoxifen for breast cancer prevention in youngwomen, under age 55, at high risk of developing futurebreast cancer, is generally much safer than many other med-ical interventions and is currently substantially underuti-lized.20
ii. Raloxifene (Evista). In a recently completed ran-domized trial of tamoxifen against raloxifene in a high riskpopulation of postmenopausal women (the STAR trial),raloxifene produced similar risk reduction to that of tamox-ifen, while being associated with significantly lower uterinecancer and thromboembolism.21,23
Therefore, the 2010-2011 St. Gallen’s-based consensusconference on breast cancer prevention24 recommendstamoxifen for premenopausal women and raloxifene forpostmenopausal women at high risk, indicating that“Because of its proven effectiveness and well understoodside-effect profile, tamoxifen is presently deemed to be thepreventive agent of choice in most high-risk women, espe-cially in premenopausal women or those with atypicalhyperplasia or lobular carcinoma in situ.”
iii. Lasofoxifene. The newest agent, lasofoxifene is amodified SERM, with more cholesterol-reduction and lessuterine cancer rates than tamoxifen.25,26 Furthermore, laso-foxifene was associated with significantly reduced risk ofbone fractures, a very significant (more than 80 per cent)reduction in ER-positive invasive breast cancers and morethan 30 per cent reduction in coronary heart disease andstrokes. In addition, there was a reduction of more than 30per cent in coronary heart disease and strokes. Thus, in post-menopausal women with osteoporosis, lasofoxifene presentsa favourable prevention profile. Longer follow-up is requiredto confirm these promising results. The agent is not yet avail-able in Canada for clinical use.
iv. Bisphosphonates are a class of medicationsapproved in North America and Europe for prevention ofbone loss. These drugs have been recently shown to preventbone fractures not only in cases with advanced metastaticbreast cancer (where their use in Canada has been approved),but also to reduce rates of metastases in hormone sensitivebreast cancer cases treated with hormonal therapies in theadjuvant setting, just after the primary surgery, to preventrecurrences.27
Recent analysis of one of the largest breast cancer epi-demiology studies has shown a strong association of oral bis-phosphonates taken by women without breast cancer, with asignificant reduction of primary breast cancer in the range of32 per cent (RR=0.68; 95 per cent CI, 0.52 to 0.88; P < .01).28
v. COX 2 inhibitors such as aspirin,29-31 celecoxib(Celebrex)31-35 and many non-steroidal anti-inflammatoryagents, have been known to reduce carcinogenesis in animalstudies. Recent human studies in colon cancer and morerecently breast cancer confirm almost a 40–50 per centreduction of new cancers in subjects with regular use ofaspirin—a strong anti-inflammatory and a Cox2 inhibitor—compared to non-aspirin users.29-31,36,39 There is promisingpotential of celecoxib or ibuprofen as examples of a morepowerful Cox2 inhibitor. Confirmation of their cost-benefitimpact is needed in future studies.36-39
12 REPORT CARD ON CANCER IN CANADA, 2010–11
PREVENTION

Interpretation of Prevention StudiesThese estimates are relevant to the prevention issues underdiscussion: if all prevention initiatives were put into practicetoday, with high adherence by high risk Canadian women,several thousand breast cancers could be prevented inCanada annually.
Conversely, if prevention is not practiced, and the presentstatus quo is perpetuated, Canadians will be confronted withseveral thousand additional breast cancers each year.
Thus, delays in incorporating appropriate interventionsinto guidelines result in higher rates of death in our popula-tion, compared to the decreasing rates if optimum preven-tion interventions were adopted today.
Low Profile of Breast Cancer Prevention in North AmericaThere are several reasons why prevention of breast cancer isnot systematically practiced.
First, no medical specialty in Canada has a mandate forpractising prevention at the present time simply becausenone is claiming this practice as their main domain.Oncologists within cancer institutions accept cases only afterbiopsy-confirmation of cancer.
Surgeons, even those specialized in breast cancer, do notdeal with cancer cases unless a surgical procedure is contem-plated. Even then, most lack the knowledge base and thetime required to counsel high risk women. Family physiciansalso lack the specialized background required. They refercancer patients to oncology centres only when a cancer diag-nosis is imminent and or biopsy-proven.
Second, no provincial funding is available for the sus-tained operation of cancer prevention counselling services.Such a clinical infrastructure would require dedicated oncol-ogists, non-specialty physicians, nurses, social workers, phys-iotherapists, and nutritionists.
Additional skills would be required in risk assessment andselection of cases for the counselling clinics. Educationalresources are required to introduce, reinforce, and monitorrecommendations for lifestyle change. Dedicated activitywould involve prescription of the appropriate preventiveagents and monitoring of their use. These activities are anal-ogous to those involved in operating well-established andfunded cancer clinics.
One of the most important steps in planning a targetedprevention practice is to narrow down as much as possiblethe at-risk population, so that costly preventive initiativeswill be focused on those who need them most.
The risk of getting breast cancer can be assessed by arefined new generation of risk assessment tools—most ofthem expanding on the original Gail risk model,44,45 takinginto consideration, besides the family history and pathology,also weight, body mass index, exercise and alcohol intake.Attempts are underway to integrate these established risk fac-tors prospectively with screening mammography criteriasuch as high breast density.
These risk models define a quantitative risk prediction ofan individual woman to develop breast cancer and if the riskexceeds a certain level, the woman would be a candidate fora prevention trial or ideally, for prevention initiatives onceincorporated into guidelines.
SummaryData increasingly indicate that breast cancer prevention ini-tiatives should be at the forefront of action. Today, however,despite these data, obesity rates are on the rise, particularlyamong young teenage girls and generally among womenwith low socio-economic or aboriginal background. This inturn is related to higher rates of sedentary lifestyle associat-ed with lower exercise in the western population as a whole.
The data forecast a very promising impact of obesityreduction on breast cancer rates, through a combination ofdiet and exercise. A similar effect is apparent on generalhealth outcomes, including profound cardiovascular andstress-relief benefits, with an associated high cost-benefit tothe health system. Professional counselling to promote exer-cise and sensible diet, in a dedicated prevention clinic,deserves priority attention from health planners and admin-istrators.
Both tamoxifen and raloxifene are substantially underuti-lized for breast cancer prevention, mostly due to the biasedperception of their side effects, despite randomized trialsshowing Level 1 evidence for their large scale benefit inbreast cancer. The tamoxifen/raloxifene underutilization ismade worse by these drugs not being approved and fundedfor prevention in Canada, where only Quebec funds their usefor breast cancer prevention. In contrast, in the U.S., insur-ance companies fund these agents for prevention if indicat-ed by an oncologist.
In Canada, in general, we lack dedicated prevention facil-ities and systematically organized cancer prevention pro-grams. One of the first such programs in Canada, proposedby the University of British Columbia, is the Breast CancerPrevention Clinic to open in Vancouver in the late Spring of2011.
ConclusionThe main objective of this report is to alert Canadians to theissues of cancer prevention using breast cancer as an exam-ple and to document the huge potential for avoiding a largenumber of breast cancers if all evidence-based preventioninitiatives were systematically applied to high risk women.While prevention interventions with medication are clearlyindicated due to their documented impact and cost-benefit,the advantages of aggressive weight and diet control, withescalating exercise, are undeniable for both breast cancer andcardiovascular disease. Furthermore, large societal cost sav-ing for Canadian taxpayers will follow, as in the long-termmillions more would be spent to cure a developed breast can-cer than to prevent it today.
It is the intention of this report to provide compellingsupport for the development of dedicated breast cancerprevention clinics supervised by trained oncologists,staffed with the related counselling team of nurses, dieti-tians, physiotherapists and social workers. Truly, an ounceof prevention is worth many pounds of cure. The soonerthe better.
Joseph Ragaz, MD, FRCPC, is a Director of the CACC and aSenior Medical Oncologist, Breast Cancer Researcher, ClinicalProfessor, Faculty of Medicine and School of PopulationHealth, University of British Columbia, Vancouver, B.C.
REPORT CARD ON CANCER IN CANADA, 2010–11 13

References1. Coleman MP. Trends in Breast Cancer Incidence, Survival, and Mortality.
Lancet. 2000 Aug 12;356(9229):590-591. 2. Ragaz J, Wong H, Qian H. Comparative Analysis of Breast Cancer Mortality
Reduction Among Regions of Canada Between 1950-2004: Impact ofSystemic and Diagnostic Guidelines After 1977. Cancer Research.2009;69(24):613s.
3. Ravdin PM, Cronin KA, Howlader N, Berg CD, Chlebowski RT, Feuer EJ, etal. The Decrease in Breast Cancer Incidence in 2003 in the United States.N Engl J Med 2007 Apr 19;356(16):1670-1674.
4. Taylor F, Ward K, Moore TH, Burke M, Davey Smith G, Casas J, et al. Statinsfor the Primary Prevention of Cardiovascular Disease. Cochrane DatabaseSyst Rev. 2011;1:CD004816.
5. Canadian Cancer Statistics, 1950-2007. Canadian Cancer Society,National Cancer Institute of Canada, Public Health Agency of Canada (orHealth Canada) and Statistics Canada.
6. Skolnick MH, Frank T, Shattuck-Eidens D, Tavtigian S. GeneticSusceptibility to Breast and Ovarian Cancer. Pathol Biol 1997Mar;45(3):245-249.
7. Cannon-Albright LA, Skolnick MH. The Genetics of Familial Breast Cancer.Semin Oncol 1996 Feb;23(1 Suppl 2):1-5.
8. Ward EM, Smith RA. Integrating Tools for Breast Cancer Risk Assessment,Risk Reduction, and Early Detection. Cancer Epidemiol Biomarkers Prev2010 Oct;19(10):2428-2429.
9. Hursting SD. Inflammatory Talk: Linking Obesity, NF-kB, and Aromatase.Cancer Prev Res 2011;4:285-287. Published online March 2, 2011.
10. Sparano J, Wang M, Martino S et al. Obesity at Diagnosis is AssociatedWith Inferior Outcome in Hormone Receptor Positive Breast Cancer.Cancer Research. 2010;70:78s.
11. George SM, Irwin ML, Smith AW et al. Postdiagnosis Diet Quality, theCombination of Diet Quality and Recreational Physical Activity, andPrognosis After Early-Stage Breast Cancer. Cancer Causes Control. 20112(4):589-98. Epub 2011 Feb 22.
12. Lynch BM, Neilson HK, Friedenreich CM. Physical Activity and BreastCancer Prevention. Recent Results Cancer Res 2011;186:13-42.
13. Friedenreich CM. Physical Activity and Breast Cancer: Review of theEpidemiologic Evidence and Biologic Mechanisms. Recent Results CancerRes 2011;188:125-139.
14. Eliassen AH, Hankinson SE, Rosner B, Holmes MD, Willett WC. PhysicalActivity and Risk of Breast Cancer Among Postmenopausal Women. ArchIntern Med 2010 Oct 25;170(19):1758-1764.
15. Irwin ML, Smith AW, McTiernan A, Ballard-Barbash R, Cronin K, GillilandFD, Baumgartner RN, Baumgartner KB, Bernstein L. Influence of Pre- andPost Diagnosis Physical Activity on Mortality in Breast Cancer Survivors:the Health, Eating, Activity, and Lifestyle Study. Clin Oncol.2008 Aug20;26(24):3958-64.
16. Kwan ML, Kushi LH, Weltzien E, Tam EK, Castillo A, Sweeney C, et al.Alcohol Consumption and Breast Cancer Recurrence and Survival AmongWomen With Early-Stage Breast Cancer: The Life After CancerEpidemiology Study. J Clin Oncol 2010 Oct 10;28(29):4410-4416.
17. Holmes MD. Challenge Of Balancing Alcohol Intake. J Clin Oncol 2010Oct 10;28(29):4403-4404.
18. Smith-Warner SA, Spiegelman D, Yaun SS, van den Brandt PA, Folsom AR,Goldbohm RA, et al. Alcohol and Breast Cancer in Women: A PooledAnalysis of Cohort Studies. JAMA. 1998 Feb 18;279(7):535-540.
19. Cuzick J, Powles T, Veronesi U, Forbes J, Edwards R, Ashley S, et al.Overview of the Main Outcomes in Breast-Cancer Prevention Trials.Lancet. 2003 Jan 25;361(9354):296-300.
20. Ragaz J, Coldman A. Survival Impact of Adjuvant Tamoxifen onCompeting Causes of Mortality in Breast Cancer Survivors, With Analysisof Mortality From Contralateral Breast Cancer, Cardiovascular Events,Endometrial Cancer, and Thromboembolic Episodes. J Clin Oncol 1998Jun;16(6):2018-2024.
21. Wickerham DL, Costantino JP, Vogel VG, Cronin WM, Cecchini RS, FordLG, et al. The Use of Tamoxifen and Raloxifene for the Prevention of BreastCancer. Recent Results Cancer Res. 2009;181:113-119.
22. Noah-Vanhoucke J, Green LE, Dinh TA, Alperin P, Smith RA: Cost-effective-ness of Chemoprevention of Breast Cancer Using Tamoxifen in aPostmenopausal US Population. Cancer. 2011 Mar 14. doi:10.1002/cncr.25926. [Epub ahead of print]
23. Vogel VG, Costantino JP, Wickerham DL, Cronin WM, Cecchini RS, AtkinsJN, et al. Effects of Tamoxifen vs Raloxifene on the Risk of DevelopingInvasive Breast Cancer and Other Disease Outcomes: the NSABP Study ofTamoxifen and Raloxifene (STAR) P-2 trial. JAMA. 2006 Jun
21;295(23):2727-2741.24. Cuzick J, Decensi A, Arun B, Brown PH, Castiglione M, Dunn B, Forbes JF,
Glaus A, Howell A, von Minckwitz G, Vogel V, Zwierzina H.: Preventivetherapy for breast cancer: a consensus statement.
25. LaCroix AZ, Powles T, Osborne CK, Wolter K, Thompson JR, ThompsonDD, et al. Breast Cancer Incidence in the Randomized PEARL Trial ofLasofoxifene in Postmenopausal Osteoporotic Women. J Nat. Cancer Inst2010 Nov 17;102(22):1706-1715.
26. Swan VJD, Hamilton CJ, Jamal SA. Lasofoxifene in Osteoporosis and ItsPlace in Therapy. Adv Ther 2010 Dec;27(12):917-932.
27. Gnant M, Mlineritsch B, Schippinger W, Luschin-Ebengreuth G,Pöstlberger S, Menzel C, et al. Endocrine Therapy Plus Zoledronic Acid inPremenopausal Breast Cancer. N Engl J Med 2009 Feb 12;360(7):679-691.
28. Chlebowski RT, Chen Z, Cauley JA, Anderson G, Rodabough RJ, McTiernanA, et al. Oral Bisphosphonate Use and Breast Cancer Incidence inPostmenopausal Women. J. Clin Oncol 2010 Aug 1;28(22):3582-3590.
29. Ararat E, Sahin I, Altundag K. Aspirin Intake May Prevent Metastasis inPatients With Triple-Negative Breast Cancer. Med Oncol [Internet]. 2010Jul 29 [cited 2011 Jan 25];Available from: http://www.ncbi.nlm.nih.gov/pubmed/20668965
30. Bardia A, Olson JE, Vachon CM, Lazovich D, Vierkant RA, Wang AH, et al.Effect of Aspirin and Other NSAIDS on Postmenopausal Breast CancerIncidence by Hormone Receptor Status: Results From a Prospective CohortStudy. Breast Cancer Res Treat 2011 Feb;126(1):149-155.
31. Holmes MD, Chen WY, Li L, Hertzmark E, Spiegelman D, Hankinson SE.Aspirin Intake and Survival After Breast Cancer. J Clin Oncol 2010 Mar20;28(9):1467-1472.
32. Ashok V, Dash C, Rohan TE, Sprafka JM, Terry PD. SelectiveCyclooxygenase-2 (COX-2) Inhibitors and Breast Cancer Risk. Breast[Internet]. 2010 Aug 17 [cited 2011 Jan 25];Available from:http://www.ncbi.nlm.nih.gov/pubmed/20724158
33. Bocca C, Bozzo F, Bassignana A, Miglietta A. Antiproliferative Effects ofCOX-2 Inhibitor Celecoxib on Human Breast Cancer Cell Lines. Mol. Cell.Biochem [Internet]. 2010 Dec 8 [cited 2011 Jan 25];Available from:http://www.ncbi.nlm.nih.gov/pubmed/21140284
34. Pierga J, Delaloge S, Espié M, Brain E, Sigal-Zafrani B, Mathieu M, et al. AMulticenter Randomized Phase II Study of SequentialEpirubicin/Cyclophosphamide Followed by Docetaxel With or WithoutCelecoxib or Trastuzumab According to HER2 Status, as PrimaryChemotherapy for Localized Invasive Breast Cancer Patients. BreastCancer Res Treat 2010 Jul;122(2):429-437.
35. Singh B, Irving LR, Tai K, Lucci A. Overexpression of COX-2 in Celecoxib-Resistant Breast Cancer Cell Lines. J Surg Res 2010 Oct;163(2):235-243.
36. Din FVN, Theodoratou E, Farrington SM, Tenesa A, Barnetson RA,Cetnarskyj R, et al. Effect of Aspirin and NSAIDs on Risk and Survival FromColorectal Cancer. Gut. 2010 Dec;59(12):1670-1679.
37. Greenspan EJ, Madigan JP, Boardman LA, Rosenberg DW. IbuprofenInhibits Activation of Nuclear {beta}-Catenin in Human Colon Adenomasand Induces the Phosphorylation of GSK-3{beta}. Cancer Prev Res (Phila).2011 Jan; 4(1):161-171.
38. Moreira L, Castells A. Cyclooxygenase as a Target for Colorectal CancerChemoprevention. Curr Drug Targets [Internet]. 2010 Dec 15 [cited 2011Jan 25]; Available from: http://www.ncbi.nlm.nih.gov/pubmed/21158711
39. Rothwell PM, Wilson M, Elwin C, Norrving B, Algra A, Warlow CP, et al.Long-Term Effect of Aspirin on Colorectal Cancer Incidence and Mortality:20-Year Follow-Up of Five Randomised Trials. Lancet. 2010 Nov20;376(9754):1741-1750.
40. Hochberg MC. What Have We Learned From the Large Outcomes Trials OfCOX-2 Selective Inhibitors? The Rheumatologist’s Perspective. Clin ExpRheumatol 2001 Dec;19(6 Suppl 25):S15-22.
41. Ross JS, Madigan D, Konstam MA, Egilman DS, Krumholz HM. Persistenceof Cardiovascular Risk After Rofecoxib Discontinuation. Arch Intern Med2010 Dec 13;170(22):2035-2036.
42. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects ofChemotherapy and Hormonal Therapy for Early Breast Cancer onRecurrence and 15-Year Survival: An Overview of the Randomized Trials.Lancet 2005; 365:1687–1717.
44. Gail MH. The Estimation and Use of Absolute Risk for Weighing the Risksand Benefits of Selective Estrogen Receptor Modulators for PreventingBreast Cancer. Ann NY Acad Sci 2001 Dec;949:286-291.
45. Gail MH, Costantino JP, Bryant J, Croyle R, Freedman L, Helzlsouer K, et al.Weighing the Risks and Benefits of Tamoxifen Treatment for PreventingBreast Cancer. J Nat Cancer Inst 1999 Nov 3;91(21):1829-1846.
14 REPORT CARD ON CANCER IN CANADA, 2010–11
PREVENTION

REPORT CARD ON CANCER IN CANADA, 2010–11 15
PREVENTION UPDATE
Smoking
Smoking is the most preventable cause of lung cancer andharms anyone in the near environment. In 2009, 20 percent of adult Canadians were smoking, with provincialrates varying from a low of 16 per cent in BritishColumbia, up to 22 and 23 per cent from Quebec all theway to Newfoundland and Labrador. The territories areterrifying, with smoking rates of 36 per cent in the Yukonand NWT, but a jaw-dropping 61 per cent in Nunavut. Insubsets, males are smokers more often than women ineach province or territory. Excluding the territories for amoment, merely because the numbers betray a phenome-non more diverse than tobacco alone, males in Alberta,Nova Scotia and Newfoundland and Labrador are smok-ing more than anyone in the country, at rates of 26 and27 per cent.
Smoking rates have dropped, slowly, for decades. All ittook was decades of aggressive anti-tobacco campaigns,massive amounts of public education and health promo-tion, numerous controls on the marketing of tobacco prod-ucts, frequent price increases for tobacco products, smok-ing bans extending out from restaurants and bars to allpublic buildings, transit systems, parks, entire communi-ties. The vigilance and creativity of the anti-tobacco move-ment is impressive, as is the commitment by most govern-ments to deny a safe haven to a lit cigarette. Alberta andQuebec are the only provinces that have not introducedlegislation for smokeless cars when children are present.Newfoundland and Labrador will implement the ban inMay, 2011.
With all this activity, so clearly focused on one goal,why is one out of every five Canadians still smoking? Whyis the smoking rate for teenage girls increasing and theoverall rate for all adults apparently levelling off?
There may be answers in the unique resistance of somesmokers to standard quit techniques. Perhaps a more for-malized program of counselling and medical interventionis needed, but are physicians ready for this role? Perhaps amore stringent regulatory environment is appropriate, ormore targeted health promotion messages, perhaps a moretailored form of government spending to reach the resis-tive smoker. This year the CACC will pursue the subject inthe search for evidence-based solutions that are relevant tothe dilemma.
RARE CANCERS UPDATE
Orphan Drugs
Ontario and Alberta each have an established frameworkfor dealing with rare diseases but no other Canadian juris-diction has taken that step. In a standard drug review,where each province tries to decide whether a new drug isimportant, effective and affordable, there are fairly rigidrules about the extent and quality of evidence that must bedelivered before a drug can be considered a worthwhileexpenditure.
However, rare diseases are exactly that and there are aninsufficient number of patients to run the full-scale clini-cal trials that are common to research on other diseases.With incidence rates in the single digits per 100,000 oreven 200,000 people a rare cancer is hard to diagnose, hardto put in front of the rare clinician who knows it well, andhard to explain. The trials are small and often deemedunconvincing. Furthermore, the discovery of a treatmentfor any of the rare diseases is likely a breakthrough, whichcan cause the trial to be suspended for ethical reasons – itis improper to withhold an effective drug from the controlarm of the trial.
In short, the usual standards and processes stack againsta new, orphan drug. It is for this reason that two provincesdeveloped a special policy to consider more relevant crite-ria for these drugs reviews. Otherwise the new orphandrugs fail the reviewers’ analysis and are rejected.
The pan-Canadian Oncology Drug Review (pCODR) is anew review process initiated by the provinces and territo-ries to conduct expert reviews and provide recommenda-tions on the clinical merits and cost-effectiveness of anew cancer drug. The provinces then have common,expert advice on which to base their funding decisions. IfpCODR had a rare cancers policy, the entire nation wouldreap the benefits of an insightful analysis of these orphandrugs. But that is not the case. As it stands, only twoprovinces will be able to sensibly evaluate the merits ofsuch products.
For a disease like cutaneous T-cell lymphoma, thatstrikes approximately one person out of 150,000 theinability to count on a drug review process that knowsyour disease can be unnerving. Cutaneous T-cell lym-phoma is a general term for many lymphomas of the skin.There are no proven causes, but the usual arsenal of cancerweapons is applied, including radiation and chemotherapyalong with ultraviolet light and topical treatments. A newtreatment option is, to say the least, welcome.
It is encouraging to hear that Ontario will spur the otherprovinces into a common rare diseases policy, allowing alljurisdictions to benefit from the analyses already conductedand the expert recommendations for a new set of best prac-tices in these special reviews. The test will be whetherorphan drugs survive or fail the new pCODR process.

16 REPORT CARD ON CANCER IN CANADA, 2010–11
LIVING WITH CANCERLIVING WITH CANCER
ChronicLymphocytic LeukemiaB-cell Chronic Lymphocytic Leukemia(CLL) and Small LymphocyticLymphoma (SLL) are cancers of thewhite blood cells that are characterizedby a proliferation of B cell lympho-cytes. According to Statistics Canada(2006), about 1900 new patients arediagnosed every year. SLL primarilyinvolves the lymph nodes while CLLaffects the blood, bone marrow andlymph nodes. CLL and SLL are nowconsidered to be different manifesta-tions of the same disease. Resultinganemia, low platelets and frequentinfections because of low immunityare common.
Most cases of CLL are diagnosed inpeople over age 50 and its incidenceincreases with age. CLL tends to beindolent in the early stages and isoften diagnosed as a result of routineblood tests. In many cases, a watchfulwaiting period begins as there are littlebenefits to early treatment. This periodoften lasts several years during whichpatients often complain of various lev-els of fatigue and anxiety. Proper diag-nosis is critical as a subset of patientshave an aggressive form of CLL andneed to make the best therapy choicesquickly.
CLL symptoms leading to treat-ment include fever and/or chills,severe weight loss, soaking nightsweats and overwhelming fatigue.Chemotherapy agents such as fludara-bine (Fludara) and cyclophosphamide(Procytox, Cytoxan) are typically usedin combination with monoclonal anti-bodies such as rituximab (Rituxan) inorder to reduce these symptoms. Thiscombination, known as FCR hasbecome the gold standard for treat-ment. However it tends to be quitetoxic and typically leaves patients in amore immune-compromised state.Younger or high-risk patients may beoffered an allogeneic stem cell trans-plant. Clinical trials are one waypatients can receive emerging drugcombinations while waiting forprovinces to fund drugs officiallyapproved by Health Canada. These tri-als tend to be restricted to patientswho meet stringent criteria and who
have access to a cancer centre offeringthe trial. Many patients are frustratedthat there is no standard of practicefor CLL in Canada as treatmentdepends on which province you livein.
CLL is due to DNA genetic damageduring cell division, as part of the B-cell regenerative process. Defective B-cells accumulate and can eventuallylead to bone marrow failure, if leftuntreated. Genetic biomarker testingsuch as FISH (Fluorescent In SituHybridization) and the more recentintroduction of ChromosomalMicroarray Analysis known as arrayComparative Genomic Hybridization(aCGH) are expanding the field ofgenetic markers in CLL. FISH testing isdone for patients in clinical trials butthey are generally not given theresults. The aCGH is currently notavailable to Canadian patients unlessthey make their own arrangements tohave it completed out of the country.Advances in treatment, a better under-standing of how the cancer functionsand mapping of the chromosomedamage that causes CLL has led togreatly increased response rates anddurations of response. Treatments canbe repeated but they typically result inshorter remissions. Not much advancehas been made in extending overallsurvival, however.
Canada does not have a Centre ofExcellence for CLL. We are fortunateto have a dedicated group of cliniciansand researchers who form theCanadian CLL group and meet inManitoba every year. CLLPAG is anational volunteer organization ofpatients committed to advocacy,awareness, education and equal accessto care on behalf of Canadians affect-ed by CLL and SLL. The Leukemia andLymphoma Society of Canada,Lymphoma Foundation of Canada andJuravinski Cancer Centre in Hamilton,ON support CLLPAG in organizing anInternational Conference on CLL everyfew years. This unique event, organ-ized by CLL patients for CLL patientsand practitioners, provides a world-class forum to learn about the latestdevelopments on the treatment of thiscomplex, heterogeneous disease.
As we learn more about the geneticvariations in CLL/SLL, there will be agrowing need for individualized treat-ment and advanced biomarker testing.
These will require further treatmentapprovals based on new criteria, newways of thinking about the disease,new technologies and a greateremphasis on targeted therapies thatclosely match the needs of the patient.
Personalized medicine will savemoney by reducing ineffective orunnecessary treatments. Canadiansshould be able to receive optimalhealth care no matter where they live.It is imperative that the cancer careagencies of Canada and provincial andfederal health ministries supportresearch into new treatments andtechnologies as well as fast-trackapproval of selective inhibitors whichare newer, innovative, less toxic treat-ments. A great deal of progress hasbeen achieved with the approval ofFCR as the therapy of choice for mostuntreated CLL patients. Approval ofFCR or FR for repeat therapy and selectalternatives, such as bendamustine(Treanda), for older patients is para-mount.
Submitted by members of the CLL PatientAdvocacy Group www.cllpag.ca© 2011 CLLPAG. Used with the kind permissionof the authors.
Ovarian CancerWhile considered rare compared tosome cancers, Canadian women havea 1 in 70 lifetime risk of developingovarian cancer. Approximately 2,600women are diagnosed and there are1,750 deaths from the disease eachyear. Seventy per cent of women withovarian cancer do not survive fiveyears—making the disease Canada’smost fatal gynecologic cancer.Although ovarian cancer is most com-mon among women over the age of50, it also affects younger women.About 10 per cent of ovarian cancersare hereditary—usually due to a muta-tion to the BRCA1 or BRCA2 (Breast
GROUPE DE DÉFENSE DES DROITSDES PATIENTS ATTEINTS DE LLC
CLLPATIENT ADVOCACY
GROUP

REPORT CARD ON CANCER IN CANADA, 2010–11 17
Cancer 1 or 2) gene. One in 50Ashkenazi Jews carries one of thesegene mutations that increases their riskfor breast, ovarian and related cancers.Segments of the French Canadian pop-
ulation may also be at increased risk.As the country’s sole charity dedicatedto overcoming ovarian cancer, OvarianCancer Canada has a continuous dia-logue with women and families livingwith the disease, other families whohave lost loved ones, health profes-sionals who deliver care andresearchers who study ovarian cancer.Our stakeholders speak with one voicewhen they say that their biggest frus-tration is the absence of a screeningtest for the early detection of ovariancancer. The need for increasedresources to support Canada’s mostpromising research in this area cannotbe overstated. When detected andtreated at an early stage, five-year sur-vival of ovarian cancer can be as highas 90 per cent. Unfortunately, the lackof a screening test and the fact thatsymptoms can be vague and attributedto other causes means ovarian canceris usually diagnosed in later stages,when the disease has already spread toother parts of the body.
The signs and symptoms of ovariancancer—including swelling or bloatingof the abdomen, pelvic discomfort orheaviness, difficulty eating or feelingfull quickly and emptying the bladderfrequently—are not well knownamong Canadian women and manyprimary health care providers. Thislack of awareness and the absence of ascreening test for early detection canresult in a longer wait for a correctdiagnosis compared to other cancers.Until an early detection test is avail-able, knowledge and awareness of the
cancer by: • supporting women and families
living with the disease • educating the public and health
professionals about ovarian cancer• and raising funds for research
into early detection and, ulti-mately, a cure.
We believe that success can best beachieved through a collaborativenational cancer strategy that bringsgreater focus and improved researchopportunities for diseases that are aslethal as ovarian cancer. We alsobelieve that a coordinated nationalapproach can best address the humanand financial resource issues, andensure equal access to the best evi-dence-based care and support for allCanadian women and their familiesliving with ovarian cancer.
Elisabeth Ross is Chief Executive Officer ofOvarian Cancer Canada.www.ovariancanada.org She also co-chairs the NationalSurvivorship Working Group of theCanadian Partnership Against Cancer.
© 2011 Elizabeth Ross. Used with the kindpermission of the author.
TesticularCancerTesticular cancer starts in the cells of atesticle. The testicles are part of aman’s reproductive system. They arethe two egg-shaped organs found inthe sac of loose skin (scrotum) at thebase of the penis. The testicles are heldin the scrotum by the spermatic cord.The spermatic cord contains the duc-tus deferens, some lymph nodes, veinsand nerves.
Testicles make the male sex hor-mone testosterone and sperm. Spermbegins to form in “germ” cells insidethe testicles. Most testicular cancersstart in the germ cells and are calledgerm cell tumours.
There are two main types of germcell tumours: seminomas and non-seminomas. Each type grows different-ly and is treated differently. Both typescan be treated successfully.
Testicular cancer, although a rarecancer in the spectrum of cancersoverall, is still the most common can-cer for males from 15–29 years of age.On average, one out of every 273males in Canada will be diagnosed
signs and symptoms are the bestdefence against this disease. A womanwho experiences one or more symp-toms that persist for three weeksshould see her doctor for a fullinvestigation.
If ovarian cancer is suspected, thefamily doctor or gynecologist shouldrefer the patient to a gynecologiconcologist, a specialist with five yearsof postgraduate training in obstetricsand gynecology plus an additional twoyears of cancer training. The gyneco-logic oncologist will manage treat-ment—usually surgery and chemother-apy. Studies have shown that there arebetter outcomes for ovarian cancerwhen surgery is performed by a gyne-cologic oncologist. Canada has 82 ofthese specialists and more are neededto meet the growing demand for care.
Women with ovarian cancer tell usthat the wait to see a gynecologiconcologist, and the wait for surgeryand other treatment to begin, can bevery stressful. A shortage of specialistsplus other challenges, such as limitedaccess to operating rooms and incon-sistencies in available therapies acrossthe country—intraperitonealchemotherapy, for example—are otherfrustrations they experience.
It is estimated that the incidence ofgynecologic cancers in Canada willrise by 47 per cent between 2001 and2014. The Society of GynecologicOncology of Canada (GOC), in part-nership with Ovarian Cancer Canada,is now conducting a study of waittimes and treatment protocols forgynecologic cancers across the countrywith an aim to improve care forwomen requiring treatment.
Women across Canada also tell usthat they experience high stress in theperiod immediately following comple-tion of their treatment. By this pointin their ovarian cancer journey, theyhave educated themselves about thedisease and know that they have tolive with the possibility of recurrence.Issues ranging from survivorship torecurrence, palliative care and end-of-life care mean women with ovariancancer and their families need supportservices close to home.
Since our organization was founded13 years ago, Ovarian Cancer Canadahas worked diligently with survivors,volunteers and the cancer communitytoward the goal of overcoming ovarian
Elisabeth Ross

18 REPORT CARD ON CANCER IN CANADA, 2010–11
with testicular cancer in their lifetime. The highest overall incidence of
testicular cancer occurs in Alberta,then Nova Scotia and Saskatchewan.However, it is the age-specific inci-dence rates that reveal the poignanttruth about the impact of this disease.
The highest rate of testicular cancerin one age group occurs in NovaScotia, for men 25–29 years of age.Across the country, the highest inci-dence occurs in young men betweenthe age of 25 and 34, with onlyManitoba having a higher rate in the35–39 age group. The incidence oftesticular cancer increases from age15 and decreases after age 40.1
While this cancer has the highestcurability rate for all men’s cancers at97 per cent, the aftershock followingdiagnosis causes deeper problems andcomplications for survivors.
The stigma of an orchiectomy(semi or full surgical castration), cre-ates typically unaddressed issues for thesurvivor and his sense of masculinity.Akin to breast cancer mastectomy andreconstruction, testicular cancer sur-vivors who opt for a testicular implantdo have a quick recovery time and gen-erally are sent home to recover, eitherwith a surety of having been cured orgetting a finite chemotherapy scheduleas the next, final step to being cured.What is left untreated is the how thepatient feels as a man.
The psychological impact of testic-ular cancer is as relevant as any othercancer, regardless of the curability fac-tor. The emotional effect following anorchiectomy is parallel to a mastecto-my for a woman. Only in momentsof intimacy or examination wouldsomeone know the man in front ofthem has had testicular cancer.
The typical responses by TCsurvivors are either, “sweep it underthe carpet”—living in denial that itever happened—or a gradual accept-ance of the new reality, dependingon the survivor’s personal sense ofsecurity and whether a social supportsystem is in place.
Cancer is a catalyst for con-fronting one’s mortality. It offers aperspective like no other, bringingissues to the forefront. What onceseemed important and/or tolerablebecomes insignificant and/or intoler-able, leaving you with your worldupside down, asking “where do I gofrom here?”
In men, this experience is difficultto adjust to, as we do not oftenexpress feelings liberally and honest-ly. When combined with the agegroup involved—often as young as15— the impact on personal, emo-tional development can be severe.
TCTCA offers a peer support systemfor survivors to network via email,telephone, or in person. As the onlyregistered non-profit charity forCanadian testicular cancer awareness,if every TC survivor were to approachour group at once, we would be over-whelmed accommodating an entirecountry of males in need.
Testicular cancer is one face to theyoung adult cancer issue in Canada,where we are effectively “a lost gen-eration.” With so much effortfocused on paediatric/geriatric cancercare and support programs, hospitalsand cancer treatment centres do nothave as many young adult survivoroutreach programs in place yet. Thisis mostly due to the lack of a youngadult approach within the cancersystem, stemming from the insecuri-ty and fear of patients who retreatfrom drawing attention.
Encouraging an open forum for tes-ticular cancer patients at the time ofdiagnosis is just as important as thediagnosis itself. Hopefully this leads toeasier adjustment in developing self-identity through any/all treatments,approaching friends and/or family foremotional support and security asmen following cancer’s touch.
Peter Laneas is a two-time testicularcancer survivor and the nationalspokesperson for The CanadianTesticular Cancer Association. Formore information on testicular
UPDATEChronicMyelogenousLeukemiaKey issues last year were disease resist-ance and patient intolerance to cur-rent front line therapy, imatinib(Gleevec). Newer second-generationdrugs are now available to treat theseissues. In August 2010, Health Canadaapproved nilotinib (Tasigna), whichjoined dasatinib (Sprycel) as secondline therapies. The approval of nilo-tinib is good news, but because eachprovince must approve the drug for
reimbursement on their provincial for-mularies, it has been very difficult forsome Canadian patients to access thisdrug. In BC, Alberta, Saskatchewanand Quebec, nilotinib has beenapproved on provincial formularies asa second line treatment. However, inOntario, nilotinib funding is onlyavailable for third line treatment, set-ting up a potential disaster for somepatients. Some patients linger longeron the first line treatment while theirhealth deteriorates to the point thatwhen they may be able to access sec-
LIVING WITH CANCER
Cheryl-Anne Simoneau
Peter Laneas
cancer, www.tctca.org.(c) 2011 Peter Laneas. Used with the kind per-mission of the author.
References1 Sources: Surveillance and Risk Assessment
Division, CCDPC, Health Canada; StatisticsCanada and the Canadian Council of CancerRegistries

REPORT CARD ON CANCER IN CANADA, 2010–11 19
ond and third line therapies, neitherof them offers any improvement. Wemust be able to trust our doctors toprotect our health.
The next issue we addressed waspurchasing our oral cancer therapythrough private employer insurance,with some assistance from provincialdrug plans. For some patients, the gapleaves them paying $1,500 that is notreimbursable. Why are we subjectingthese patients to something thatsounds like a “cancer tax”?Additionally, colleagues frown uponco-workers with diseases on “designer”priced drugs, as premiums areincreased or benefits are scaled back tomeet the costs. BC and Alberta contin-ue to be the only provinces that pro-vide oral cancer drugs through theircancer and rare disease drug pro-grams.
Our third issue was asking the gov-ernment to step in and get involved insupporting drug combination trials orstopping drug trials for CML. This ishappening in Europe. The data fromEurope indicate that 10 per cent ofCML patients on the current front linetherapy, imatinib, may be candidatesto safely stop taking drugs. This figurecould be as high as 40 per cent if wefactor in the superior responses thatpatients achieve on the second linedrugs such as dasatinib and nilotinib.We hear rumours that industry is step-ping up to the plate, but where is ourgovernment?
We would like the governments tosupport a personalized medicineapproach with regards to CML. If wecould allow our physicians to conductappropriate diagnostic tests up frontfor CML patients, such as immuno-phenotying, mutation detection com-bined with cytogenetics, PCR, FISHand standard blood tests, as well asother tests that may be deemed appro-priate, we may be able to ensure thatthe right patient gets matched withthe right drug, at the right dose, at theright time.
Next year we hope to report thatthese critical issues are resolved, withimprovements in patients’ quality oflife and return to good health.
Cheryl-Anne Simoneau is President of theCML Society of Canada.
© 2011 Cheryl-Anne Simoneau. Used with kindpermission of the author.
MultipleMyelomaHave there been improvements in ouraccess to drug treatments? This year’sanswer—maybe yes, maybe no.
There are two parts of the equation.First there is the funding approval andthen, the challenge of physically get-ting the drug.
The Pan Canadian Oncology DrugReview is to be a more transparent,accountable system of cancer drugreview. pCODR is a step forward asmore public inclusion has been desiredand requested—including patient sub-
missions. It is a modest step, but wewelcome it and look forward to furtheropenness and understanding.
Then each province and territorywill make their own funding decisionsbased on the pCODR evaluation ofeffectiveness and cost-benefit. Evenassuming, with great optimism, thatthe provinces and territories all accepta positive recommendation frompCODR and decide to fund a new can-cer drug, there are always conditionsand restrictions.
The second part of this equation isreceiving the needed drug therapy.
The actual receipt of a needed drugmay be either a simple or an oneroustask—most stressful and unfair whenone’s life is hanging in the balance.Ontario’s Expanded Access Programputs restrictions on access with theintent of protecting the patient. A per-fect example is lenalidomide(Revlimid). Processes must be andhave been put in place because of thehistorical birth defect issue. So this isgood. However, the organization oradministration of this program is a
convoluted nightmare. An application to receive a drug
under the EAP is supposed to receive adecision within two weeks. Approvalshave been taking up to two months.This system has forced some physi-cians to spend extraordinary amountsof time on paperwork rather than pro-viding patient care. Hospitals alreadyhire “reimbursement navigators” tohelp patients and doctors find a wayto obtain the many treatments notcovered by the provincial drug plan.
Would you, as a patient with anadvancing cancer, want to wait twomonths simply because of paperworkto find out if your EAP application isapproved? Whether or not the healthministry feels any sense of urgency,the cancer patients certainly do.
Physicians who work with this sys-tem 24/7 are strong proponents forpositive change. But patients also can,and must, have a voice. It is theresponsibility of the patient popula-tion to become more informed, moreinvolved and more outspoken.
Carolyn Henry is a myeloma patient andco-group leader, London and DistrictMyeloma Support Group, London, ON. www.myelomacanada.ca
© 2011 Carolyn Henry. Used with the kind per-mission of the author.
NeuroendocrineTumoursNeuroendocrine tumours, now knownmore commonly as NET cancers, is theumbrella term for a group of unusual,often slow-growing cancers, whichdevelop from cells in the diffuseendocrine system. They are foundmost commonly in the lung or gas-trointestinal system, but they can alsooriginate in other parts of the bodysuch as the pancreas, ovary, and testes,among other sites.
Increased awareness of NET cancerhas developed as a result of media cov-erage of Apple founder Steve Jobs’pancreatic NET cancer. We are nowrecognized as the fastest growing can-cer community worldwide (BBC,Belfast, September, 2010).
Despite increased media exposure,NET cancer still remains, for the mostpart, a no-name cancer. Although the
Carolyn Henry

20 REPORT CARD ON CANCER IN CANADA, 2010–11
Canadian Cancer Encyclopedia nowboasts a Neuroendocrine Cancer chap-ter, it is filed under the category of“other endocrine.” Usually NETCancers are enmeshed inside the gas-trointestinal category. We NET Cancerpatients would dearly love to see ourown category emerge on officialcancer sites.
The problem seems to be that NETcancers do not originate from a specif-ic site. This seems to confound provin-cial health ministries and cancer agen-cies when it comes to identifying usproperly.
An important NET cancer diagnos-tic scan, the octreoscan, still has nobillable code, which means hospitalshave to individually foot the bill forour scans, making us an expensive andunattractive patient group for hospi-tals worried about their bottom line.
For most of last year, the only cen-tre in Canada accepting patients fromall over the country were theNeuroendocrine Cancer Centres inCalgary and Edmonton. The CrossCancer Centre in Edmonton was actu-ally the first location in Canada tobegin to treat patients with the not-yet-approved rare nuclear isotopeLutetium 177, which targets all NETcancer cells and is regarded as a signif-icant treatment option for a substan-tial segment of our community.
The London Regional CancerCentre, which in the past had accept-ed patients from all over Canada, hadbeen closed to patients outside theLocal Health Integrated Network,(LHIN) for 2009 and much of 2010,but in the second half of 2010 Ontariobowed to patient pressure and theLondon HSC opened its doors again.
Currently Cancer Care Ontario has
an Expert Panel and SteeringCommittee looking at the delivery ofradioisotope treatment for qualifyingpatients in Ontario. CNETS Canada isacting in a consultative capacity.
Our Vancouver InternationalConference in May 2010, with 35 fac-ulty from six countries, focused on thebest and most innovative practicesworldwide and our DVDs are availablefor distribution across Canada to med-ical and patient libraries everywhere.
On June 2, 2010, CNETS Canadaspoke of the need for radioisotopetreatment at the Health Committee ofthe House of Commons. On October10, 2010 the Canadian NET Cancerscommunity took part in the firstWorld NET Cancer Awareness Day byhosting information tables in key hos-pitals and making sure our newly pub-lished information leaflets were in thestacks. We will host more hospitalinformation tables and put leafletsinto many more hands in 2011.
Maureen Coleman is the President ofCNETS Canada. www.cnetscanada.org © 2011 Maureen Coleman. Used with the kindpermission of the author.
GISTIn last year’s Report Card on Cancer inCanada, Life Raft Group Canada notedthe many difficulties faced by patientsliving with GIST (gastrointestinal stro-mal tumour), a rare sarcoma of thegastrointestinal tract.
Drug access is a particular problemfor patients with rare cancers. Imatinib(Gleevec) was the first approved target-ed chemotherapy for GIST.Subsequently, several other drugs,including sunitinib (Sutent), nilotinib(Tasigna), and dasatinib (Sprycel), haveeither been approved or are in trial forGIST. All of these drugs cost thousandsof dollars per month, and provincialdrug plans have been slow to providecoverage.
There are unacceptable differencesin drug coverage between provinces: a“patchwork quilt” or “postal code lot-tery.” A particular problem right nowis access to “adjuvant” Gleevec, that is,treatment intended to delay or preventrecurrence of GIST, following surgery.This treatment is known to be highly
effective, based on results of severalpublished clinical trials, but remainsunavailable to many Canadian GISTpatients, because of financial barriers.Novartis Pharma-ceuticals had provid-ed access, through its compassionate-use program, but this program wasshut down to all new patients, as ofFeb. 1, 2011.
So, we monitor the provincial fund-ing decisions and we press the case forimproved access. • In B.C., funding approval for adju-
vant Gleevec was given, with somerestrictions, in 2009.
• In Quebec, funding can be provid-ed through the Exceptional PatientProgram.
• In N.S., funding was approved inDec. 2010.
• One month later, in N.B., fundingwas denied.
• In Ontario and Alberta, decisionshave not yet been made. Ontario isa key province, and its pendingdecision could make a huge differ-ence. For now, many patientsneeding adjuvant Gleevec haveno options, and can only waitand hope that their cancer doesnot return.
These capricious and arbitrarydifferences in drug funding acrossCanada must end. The provinces mustharmonize their coverage at the BestPractices/highest standard of care thatcan be achieved. Our patients cannotbe left without access to needed drugs!
David Josephy is the President, GISTSarcoma Life Raft Group Canada.www.liferaftgroup.ca
© 2011 David Josephy. Used with the kind permission of the author.
LIVING WITH CANCER
David Josephy
Maureen Coleman

REPORT CARD ON CANCER IN CANADA, 2010–11 21
THE ORGANIZATION OF CANCER CARETHE ORGANIZATION OF CANCER CARE
WAITING TIMES
Waiting for Personalized Cancer Care
BY PIERRE MAJOR, MD
The word cancer is frightful. When there is a suspicion of cancer, access to timelydiagnostic tests and care is important to allay fears and offer the patient some senseof action, control and movement that is away from danger and toward solutions.
This year the CACC team set out to document what patients encounter whenfaced with a potential diagnosis of cancer. We could not find any reliable informationon wait times from the initial referral by family physicians to specialists and definitivediagnostics procedures and treatment. We searched provincial health ministry websites and government e-publications.
The ministry of health of Ontario has a web site with wait times for several surgi-cal procedures but no comprehensive database is currently available on wait timesfor cancer diagnostic procedures. Ontario’s cancer agency has brought much greatertransparency to access times for medical and radiation oncology services. This is animportant first step in identifying bottle necks and improving access to diagnosticand surgical services.
All provinces need to bring greater transparency to their cancer care resources.What consistently contrasts the perceptions of physicians and patients on the frontline about wait times is the lack of a sense of urgency from health care authorities.This leaves a very unsatisfactory perception that the concerns of the individualpatients are lost in the far-removed discussions of administrators.
Information on wait times is important for health care managers/planners. Forthe individual patient this is less useful. The patient first brings symptoms of con-cern to their family physician who then has to arrange medical specialist referralsfor definitive diagnostic tests and then to a surgeon for treatment. Primary carephysicians develop patterns of referral with a limited number of specialists in theirgeographic areas.
Wait time information throughout a province, as is available in Ontario, does notfrequently influence the referral pattern of the family physician. It is only when asurgeon declines a referral because his operating room time constraints wouldjeopardize timely care that the patient and primary care physician will look foralternatives. This brings uncertainty to the patient; there is also a growing body ofinformation that shows that delays in initiating treatment not only caused patientanxiety but may adversely affect the outcome of treatment for certain cancers.
There is no information on the effect of delays in access to cancer care andoutcomes. What we have is information from Europe. When the U.K. decided toinvestigate the cause of having the worst outcomes from cancer compared to westernEuropean countries, delays in accessing cancer care appeared to be the only variablecapable of explaining this large disparity. In response, the U.K. has channeledincreased resources to cancer care.

22 REPORT CARD ON CANCER IN CANADA, 2010–11
THE ORGANIZATION OF CANCER CARE
Similarly, delayed access to drug therapy in Canada is often caused by the multiplelayers of review, from the initial federal review for safety and efficacy, to price reviewsthat establish an acceptable market price, to the inter-provincial clinical and cost-benefitreview and then to the individual provinces for a funding decision. A new drug that israpidly adopted in the U.S. does not become an insured treatment in Canada until yearsof this regulatory consideration are completed. And then, as with all aspects of ourhealth system, the patient access will vary from province to province.
The international disparities in access to new medicines for cancer treatment werereported last year by the U.K.’s own Sir Michael Richards, National Cancer Director.The U.K. placed 12th on a list of 14 countries surveyed; Canada placed 13th. Theuproar in the U.K. caused an immediate influx of funding for new cancer drugs anddismissal of the drug review committee responsible for rejecting these treatmentoptions.
Canada has relatively fewer hospital beds per population than most Europeancountries and Ontario has the fewest hospital beds for its patients than any otherprovince. This situation is chronic; better productivity of the Canadian hospital systemthat could explain our lower need for acute care beds is an undocumented assumptionthat needs to be challenged. Navigating the hospital network is daunting for primarycare physicians and detrimental to patient care.
The discourse on the need for patience while hospital administrators look forsolutions is of little solace to the patient who needs care now.
The first five priority areas for improved wait times are considered to have beensuccessful. Reporting on the results for 2010, the Canadian Institute for HealthInformation states that eight out of 10 patients received their priority procedureswithin the recommended time frames.
ELECTIONS 2011Federal Election May 2, 2011
Newfoundland and Labrador October 11, 2011
Prince Edward Island October 3, 2011
Ontario October 6, 2011
Manitoba October 4, 2011
Saskatchewan November 7, 2011
Northwest Territories October 3, 2011
Yukon Election possible in 2011
It is time for the next step—selecting the next priorities and negotiatingthe terms of a federal/provincial/territorial agreement on wait times. Our readers are invited to vote on their own priorities.
Vote on our website, www.canceradvocacy.ca or email to [email protected]
with your thoughts on priorities for wait time improvement.

REPORT CARD ON CANCER IN CANADA, 2010–11 23
THE ORGANIZATION OF CANCER CARETHE ORGANIZATION OF CANCER CARE
by SUSAN F. DENT, BSc, MD, FRCPC, and SANDI YURICHUK, BSc, MBA, PhD CANDIDATE
In 2010, an estimated 173,800 new cases of cancer (exclud-ing about 75,500 non-melanoma skin cancers) occurred inCanada.1 While major inroads have been made in cancertreatment with earlier diagnosis and treatment intervention,40 per cent of women and 45 per cent of men (based on 2009incidence rates) will develop cancer during their lifetime.One out of every four Canadians is still expected to die fromthis disease. Only continued clinical research focused on bet-ter methods of cancer treatment and prevention willimprove these statistics.
In view of this, should clinical trials be offered as part ofstandard treatment for Canadians diagnosed with cancer? Inorder to answer this question we need to address severalimportant issues.
1. How important is clinical cancer research? 2. What is Canada’s contribution to clinical cancer
research? 3. What are the barriers to conducting clinical research?
and, 4. What are the proposed solutions?
How Important is Clinical Cancer Research?There is general agreement that in the last four decades theincremental steady improvements in cancer outcomes havelargely resulted from carefully planned and executed clinicaltrials testing new treatments. The last two decades have seenmajor advances in knowledge of cancer cell biology. Put sim-ply, we now have a better understanding of what turns a“normal” cell into a “cancer” cell and what allows these can-cer cells to grow wildly, avoiding all the normal body checksand balances.
In the last decade, based on this knowledge, we have seenthe emergence of a new generation of “targeted” cancer ther-apies. Targeted therapies are generally better tolerated thantraditional cytotoxics and have expanded the concept ofindividually tailored cancer treatment as some of these drugsmay be effective in patients whose cancers have a specificmolecular target, but may not be effective in the absence ofsuch a target. Clinical trials are important vehicles for evalu-ating these and other novel therapies that emerge fromtranslational research activities. Moreover, institutions with
high participation rates in academic clinical trials have bet-ter patient outcomes than institutions with low participationrates.2
What is Canada’s Contribution to Cancer Clinical Research?So, where does Canada stand in terms of participation inclinical cancer research? Accurate data are difficult to deter-mine on the number of cancer patients enrolled in clinicaltrials and the types of trials in which they are enrolled. Awidely quoted estimate is that three per cent of adult cancerpatients are enrolled in clinical trials.3 In 2009, the percent-age of patients enrolled in therapeutic clinical trials acrossCanada ranged from two per cent in the Atlantic Provincesto 11 per cent in Alberta, with a national average of seven percent (Figure 1).4 With so few adult patients involved in can-cer trials, progress in clinical research is slow. Additionally,
FOR CANCER PATIENTS IN CANADA
Should Clinical Trials be ConsideredPart of “Standard of Care”?
FIGURE 1
ADULT CLINICAL TRIAL PARTICIPATION RATIO—CASESSEEN BY PROVINCIAL CANCER CENTRES IN 2009 4
AB ON AVERAGE BC MB NB NS PE SK NL
Pro
port
ion
0.14
0.12
0.10
0.08
0.06
0.04
0.02
0.00
Value = 0.107 0.081 0.069 0.051 0.045 0.024 0.023 0.022 0.021 0.018
N = 9,790 52,754 97,580 16,409 5,204 3,486 2,568 647 5,235 1,487
Data Source: Provincial cancer agencies
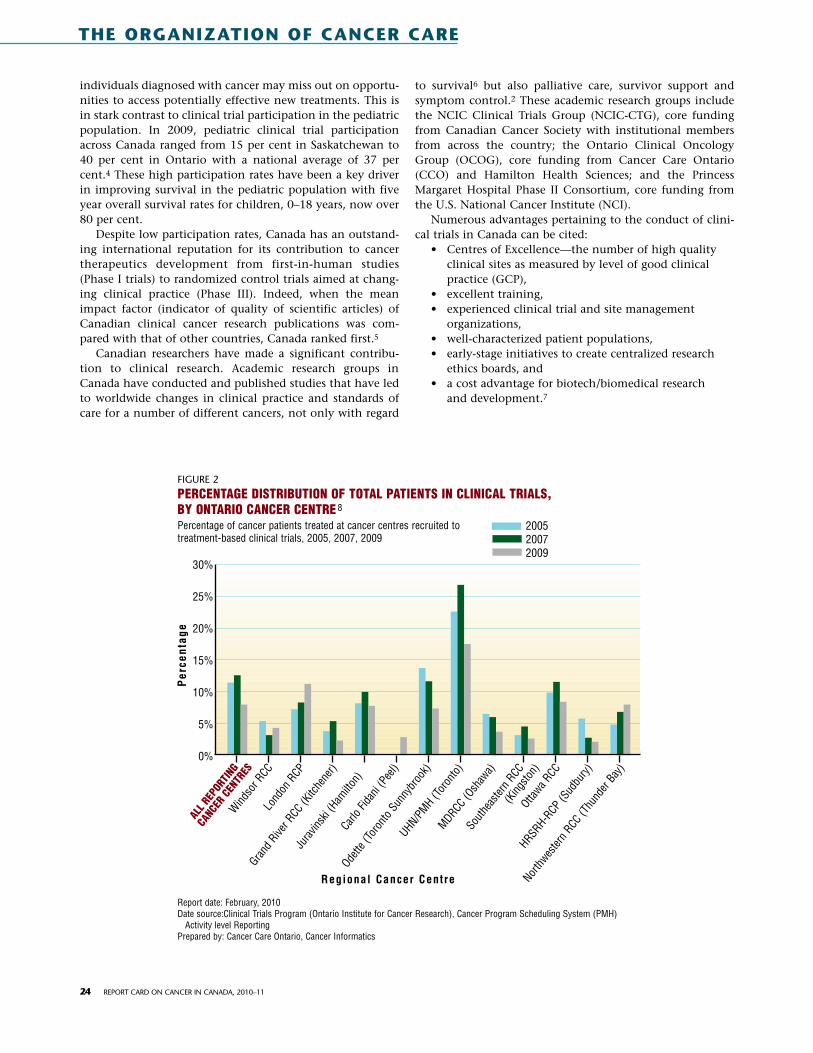
individuals diagnosed with cancer may miss out on opportu-nities to access potentially effective new treatments. This isin stark contrast to clinical trial participation in the pediatricpopulation. In 2009, pediatric clinical trial participationacross Canada ranged from 15 per cent in Saskatchewan to40 per cent in Ontario with a national average of 37 percent.4 These high participation rates have been a key driverin improving survival in the pediatric population with fiveyear overall survival rates for children, 0–18 years, now over80 per cent.
Despite low participation rates, Canada has an outstand-ing international reputation for its contribution to cancertherapeutics development from first-in-human studies(Phase I trials) to randomized control trials aimed at chang-ing clinical practice (Phase III). Indeed, when the meanimpact factor (indicator of quality of scientific articles) ofCanadian clinical cancer research publications was com-pared with that of other countries, Canada ranked first.5
Canadian researchers have made a significant contribu-tion to clinical research. Academic research groups inCanada have conducted and published studies that have ledto worldwide changes in clinical practice and standards ofcare for a number of different cancers, not only with regard
to survival6 but also palliative care, survivor support andsymptom control.2 These academic research groups includethe NCIC Clinical Trials Group (NCIC-CTG), core fundingfrom Canadian Cancer Society with institutional membersfrom across the country; the Ontario Clinical OncologyGroup (OCOG), core funding from Cancer Care Ontario(CCO) and Hamilton Health Sciences; and the PrincessMargaret Hospital Phase II Consortium, core funding fromthe U.S. National Cancer Institute (NCI).
Numerous advantages pertaining to the conduct of clini-cal trials in Canada can be cited:
• Centres of Excellence—the number of high qualityclinical sites as measured by level of good clinicalpractice (GCP),
• excellent training,• experienced clinical trial and site management
organizations,• well-characterized patient populations,• early-stage initiatives to create centralized research
ethics boards, and• a cost advantage for biotech/biomedical research
and development.7
24 REPORT CARD ON CANCER IN CANADA, 2010–11
THE ORGANIZATION OF CANCER CARE
FIGURE 2
PERCENTAGE DISTRIBUTION OF TOTAL PATIENTS IN CLINICAL TRIALS, BY ONTARIO CANCER CENTRE 8
Percentage of cancer patients treated at cancer centres recruited to treatment-based clinical trials, 2005, 2007, 2009
30%
25%
20%
15%
10%
5%
0%
Per
cent
age
ALL R
EPOR
TING
CANC
ER C
ENTR
ESW
indso
r RCC
Lond
on R
CP
Grand R
iver R
CC (K
itche
ner)
Jurav
inski
(Ham
ilton)
Carlo
Fida
ni (P
eel)
Odette
(Tor
onto
Sunn
ybro
ok)
UHN/PMH (T
oron
to)MDRCC
(Osh
awa)
South
easte
rn R
CC(K
ingsto
n)Otta
wa RCC
HRSRH-R
CP (S
udbu
ry)
Northw
ester
n RCC
(Thu
nder
Bay)
Regional Cancer Centre
Report date: February, 2010Date source:Clinical Trials Program (Ontario Institute for Cancer Research), Cancer Program Scheduling System (PMH)
Activity level ReportingPrepared by: Cancer Care Ontario, Cancer Informatics
200520072009

Yet the clinical trial landscape in Canada is chang-ing—for the worse. In 2009, market research con-ducted by the Canadian Cancer Research Alliancerevealed that cancer clinical trials in Canada wereunder growing threat.2 This was particularly thecase for trials based on ideas developed by the aca-demic sector (i.e., those from cooperative groups).In 2010, CCO reported that cancer patient partic-ipation in clinical trials in Ontario from 2007 to2009 had decreased 28 per cent, (from 5,469patients enrolled in 2007 to 4,287 patients in2009) citing a changing environment for support-ing clinical trials (Figure 2).8
The NCIC-CTG shares similar concerns, accord-ing to Dr. Ralph Meyer, Director of the NCIC-CTG.While total patient enrollment in NCIC basedclinical trials has remained relatively stable overthe past five years, the costs (financial andhuman) of conducting clinical trials have escalat-ed and there is greater complexity in activatingclinical trials.
The Canadian Institute for Health Research(CIHR) has acknowledged that Canada is rapidlyfalling behind other industrial countries interms of capacity to undertake patient-orientedresearch.9 Failing new action, Canada will rapidlylose its competitive advantage in developing noveltherapies and evaluating them in patients.
What are the Barriers to Conducting Clinical Trials in Canada?
The barriers to conducting clinical trials inCanada appear to be multi-factorial and include:
• a relative lack of agency funding,• a declining ability of hospitals/ cancer
centres to support core clinical trialinfrastructure,
• complex regulatory and administrativeenvironments,
• increasingly complex studies, and • emerging international competition
The lack of agency funding for clinician cancerresearch is perhaps the most serious barrier. TheCanadian Institute for Health Research invest-ment in patient oriented research represents onlysix per cent ($60 million) of their annual budgetwhich is markedly lower than comparative invest-ments made by the U.S. NIH, the U.K. NationalInstitute of Health Research and Australia’sNational Health and Medical Research Council.9
In 2007, $398.5 million was spent on peer-reviewed cancer research, from 37 funding agen-cies in Canada. These statistics reflect a 5.4 percentincrease in cancer research funding from federalgovernment programs over a two year period(2005–2007) however, the proportion of fundsdedicated to “clinical” cancer research is uncertain(Figure 4).2 Approximately 45 per cent of researchfunding was allocated to biology, 11 per cent to
REPORT CARD ON CANCER IN CANADA, 2010–11 25
What are Clinical Trials?
Clinical trials are research studies done to
evaluate whether a drug or treatment is both
safe and effective for people. Each study tries
to answer scientific questions and to find bet-
ter ways to prevent, diagnose and treat cancer.
Participating in a clinical trial can provide
researchers with valuable information on new
treatments; in some cases, it may also offer
the chance for a cure or improvement in a
patient’s quality of life that is not provided by
standard therapy. Clinical trials can range from
testing new drugs for the first time in humans
(Phase I) to testing the effectiveness of the
drug in a certain tumour type, e.g., breast
cancer (Phase II), to testing a new therapy
compared to the standard of care (Phase III).
FIGURE 3
DISTRIBUTION OF 2007 CANCER RESEARCH INVESTMENT BYFUNDING SOURCE FOR EACH PROVINCE ($398.5M) 10
Funding source refers to source of dollars for each project and not to the funder sector of the funding organization.
AB
BC
MB
NB
NL
NS
ON
PEI
QC
SK
0% 20% 40% 60% 80% 100%
Federal government Provincial government
Voluntary organization Industry Other
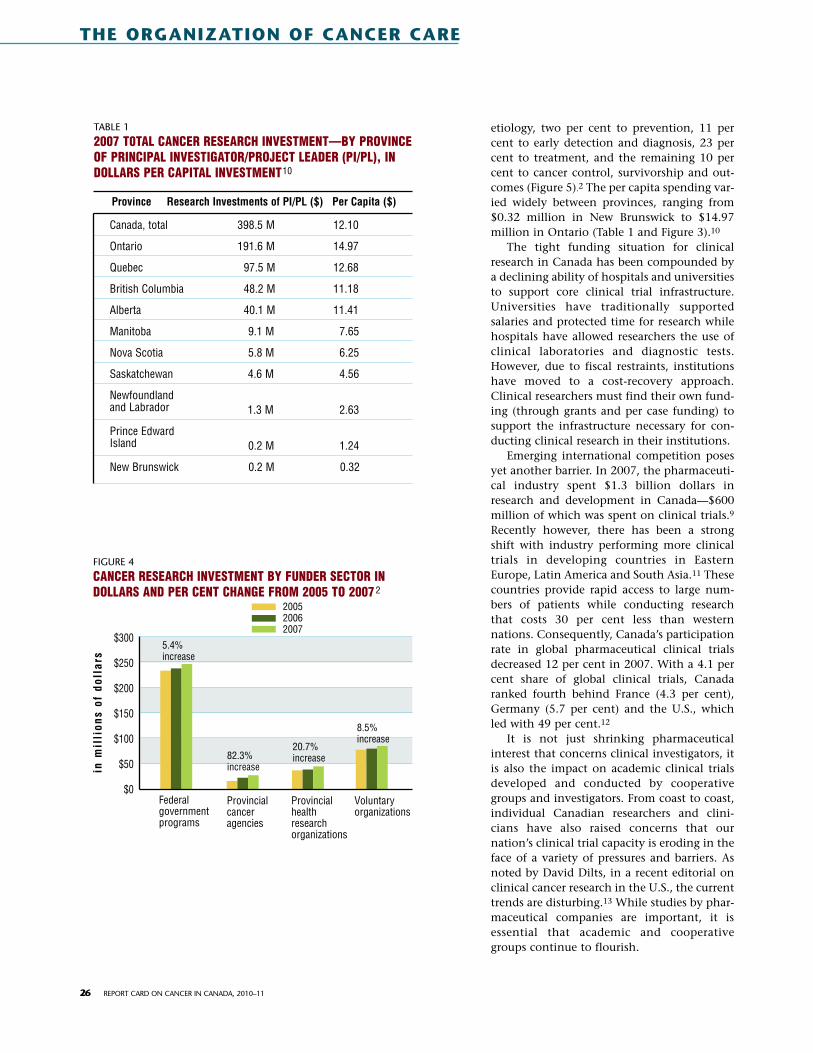
etiology, two per cent to prevention, 11 percent to early detection and diagnosis, 23 percent to treatment, and the remaining 10 percent to cancer control, survivorship and out-comes (Figure 5).2 The per capita spending var-ied widely between provinces, ranging from$0.32 million in New Brunswick to $14.97million in Ontario (Table 1 and Figure 3).10
The tight funding situation for clinicalresearch in Canada has been compounded bya declining ability of hospitals and universitiesto support core clinical trial infrastructure.Universities have traditionally supportedsalaries and protected time for research whilehospitals have allowed researchers the use ofclinical laboratories and diagnostic tests.However, due to fiscal restraints, institutionshave moved to a cost-recovery approach.Clinical researchers must find their own fund-ing (through grants and per case funding) tosupport the infrastructure necessary for con-ducting clinical research in their institutions.
Emerging international competition posesyet another barrier. In 2007, the pharmaceuti-cal industry spent $1.3 billion dollars inresearch and development in Canada—$600million of which was spent on clinical trials.9
Recently however, there has been a strongshift with industry performing more clinicaltrials in developing countries in EasternEurope, Latin America and South Asia.11 Thesecountries provide rapid access to large num-bers of patients while conducting researchthat costs 30 per cent less than westernnations. Consequently, Canada’s participationrate in global pharmaceutical clinical trialsdecreased 12 per cent in 2007. With a 4.1 percent share of global clinical trials, Canadaranked fourth behind France (4.3 per cent),Germany (5.7 per cent) and the U.S., whichled with 49 per cent.12
It is not just shrinking pharmaceuticalinterest that concerns clinical investigators, itis also the impact on academic clinical trialsdeveloped and conducted by cooperativegroups and investigators. From coast to coast,individual Canadian researchers and clini-cians have also raised concerns that ournation’s clinical trial capacity is eroding in theface of a variety of pressures and barriers. Asnoted by David Dilts, in a recent editorial onclinical cancer research in the U.S., the currenttrends are disturbing.13 While studies by phar-maceutical companies are important, it isessential that academic and cooperativegroups continue to flourish.
26 REPORT CARD ON CANCER IN CANADA, 2010–11
THE ORGANIZATION OF CANCER CARE
TABLE 1
2007 T0TAL CANCER RESEARCH INVESTMENT—BY PROVINCEOF PRINCIPAL INVESTIGATOR/PROJECT LEADER (PI/PL), INDOLLARS PER CAPITAL INVESTMENT10
Canada, total 398.5 M 12.10
Ontario 191.6 M 14.97
Quebec 97.5 M 12.68
British Columbia 48.2 M 11.18
Alberta 40.1 M 11.41
Manitoba 9.1 M 7.65
Nova Scotia 5.8 M 6.25
Saskatchewan 4.6 M 4.56
Newfoundland and Labrador 1.3 M 2.63
Prince Edward Island 0.2 M 1.24
New Brunswick 0.2 M 0.32
Province Research Investments of PI/PL ($) Per Capita ($)
FIGURE 4
CANCER RESEARCH INVESTMENT BY FUNDER SECTOR INDOLLARS AND PER CENT CHANGE FROM 2005 TO 2007 2
in m
illi
ons
of d
olla
rs
$300
$250
$200
$150
$100
$50
$0Federal governmentprograms
Provincialcanceragencies
Provincialhealthresearchorganizations
Voluntaryorganizations
200520062007
5.4%increase
82.3%increase
20.7%increase
8.5%increase

Losing the competitive edge has far-reaching implicationsin our ability to lead the work of translating new discoveriesinto clinical applications.3 Clinical trials developed and con-ducted by Canadian academic investigators could answer theclinical and translational questions that are based on themost promising discoveries from Canadian laboratoryresearchers. Such trials could address the greatest concernsfor the health and well-being of Canadians, in a mannermost relevant to the Canadian healthcare system. Thus, thethreat to cancer trials, at a time of great opportunity for thetranslation of research discoveries to clinical testing, is a crit-ical national issue.
The increasing complexity of clinical trials has also had asignificant impact on clinical cancer research centres acrossthe county. The NCIC-CTG has seen a two-to-three foldincrease in staffing demands necessitated in part by theincrease in ethics and regulatory compliance required forconducting clinical studies. The timeline for conducting atrial – the time from activation of the trial to the first patient
enrolled in the trial – has also increased significantly.So what can we do to ensure the future “health” of clini-
cal cancer research in Canada?
What are the Proposed Solutions?A number of initiatives aimed at promoting the “health” ofour research community and preventing further erosion ofresources have recently been launched in Canada.
In February 2010, the Canadian Institute of HealthResearch (CIHR) proposed a 10-year plan to change healthcare including a strategy for patient-oriented research (SPOR)in Canada.9 It was proposed that Canada increase its invest-ments and better coordinate its efforts in patient-orientedresearch to improve the quality, accessibility and cost-effectiveness of health care. The success of such a plan wouldrequire support not only from the federal, provincial and ter-ritorial governments but also from major stakeholdersincluding research institutions (universities, hospitals, com-munity centres), and clinician scientists as well as private
REPORT CARD ON CANCER IN CANADA, 2010–11 27
FIGURE 5
DISTRIBUTION OF 2007 CANCER RESEARCH INVESTMENT BYCSO CATEGORY ($402.4M) 2
50%
40%
30%
20%
10%
0%
10%
20%
30%
40%
50%Biology Etiology
(causes of cancer)
Prevention(interven-tions)
Early detection,diagnosis &prognosis
Treatment Cancer control, survivor-ship & outcomes
Scientificmodel outcomes
44.5% 10.6% 1.8% 10.8% 22.4% 9.1% 0.8%
“Any improvements in cancer care come from clinical trials.”—Ezekiel J. Emanuel, MD, PhD, Chair, Department of Clinical Bioethics, U.S. National Institutes of Health3

and charitable sectors. This strategy would consist of fourmajor components:
1. Improvements to the research environment andinfrastructure,
2. up of mechanisms to better train and mentor healthprofessionals and non-clinicians,
3. strengthening organizational, regulatory and financialsupport for multi-site studies, and
4. supporting best practices in health care.
Members of the Association of Canadian Academic Health-care Organizations (ACAHO) strongly supported the patient-oriented clinical research initiative.15 To advance the initia-tive, the Association proposed that the federal governmentincrementally invest $10 million that would allow for theimplementation of a series of pilot projects that if successful,would move to a broader series of projects across the coun-try. But would this be enough? Comparatively, the NationalCancer Research Network funding for cancer research alonein the U.K. is close to four times this amount per year.The U.K. investment in clinical research infrastructure for alldiseases (NIH) is hundreds of millions per year.9 An invest-ment of 10 million dollars in Canada for all diseases isunlikely to have any real impact.
In May 2010, with support from the CanadianPartnership Against Cancer, the Canadian Cancer ResearchAlliance launched the Pan-Canadian Cancer ResearchStrategy (PCCRS).3 This strategy provides a vision forCanadian cancer research achievements over the next fiveyears. Priorities for enhanced funding and collaborationinclude cancer prevention, basic discovery research (i.e.,genomics, cancer initiating cells, new agent discovery, bio-markers), clinical trials, health services/economics andtumour-specific partnered initiatives (e.g., collaboration withCanadian Breast Cancer Research Alliance).
These priorities have resulted in the identification of 24key action items to be implemented between 2010 and 2012.The plan for clinical trials is to clearly outline the issues fac-ing trials in Canada and make recommendations on howthese issues can be resolved. The report will examine jurisdic-tions with healthy and growing cancer trial enterprises, con-sider how to engage the pharmaceutical industry and identi-fy ways to maximize patient-oriented clinical research. Inaddition, the Pan-Canadian Cancer Research Strategy willaim to create an optimal cancer research system - one inwhich there is a balance of research funding across the threemain categories: project grants, infrastructure and researchpersonnel.
Regional initiatives have also been launched to enhancepatient enrollment in cancer clinical trials in Canada. In2004, the Ontario Institute of Cancer Research (OICR) set agoal to double Ontario patient recruitment into cancer clin-ical trials, within three years, in 28 participating cancer cen-tres throughout the province. With a three year budget of$12.9 million clinical trials recruitment increased from 8.9per cent in 2004 to 12.4 per cent in 2007 (Figure 2).8 The suc-
cess of this program however was based on a business modelpredicated on self-sustaining fiscal resources from enhancedpatient recruitment to pharmaceutical trials. Increasing reg-ulatory requirements and lack of ongoing infrastructure sup-port resulted in a drop in clinical trial enrollment to 8.5 per-cent in 2009, a lower figure than before the program wentinto effect.
In contrast, the National Cancer Research Network(NCRN) was established in the U.K. by the Department ofHealth in 2001 to provide the National Health Service withthe infrastructure to support prospective trials of cancertreatments and support research undertaken by cancer char-ities. The initial goal was to double the trial enrollment ofcancer patients by 2004. With an annual investment of ?20million per year, overall accrual to clinical trials rose from abaseline of less than four per cent of new cases to 14 per centby 2006. By 2010, recruitment of cancer patients to CancerNetwork studies had quadrupled since 2001—from one in 26patients to around one in six.16,17 Unlike the OICR infra-structure program, the Department of Health funding con-tinued beyond the initial three year commitment.18
In 2001, stakeholder consultations with researchers, studysponsors, clinical trials sites and regional ethics boards iden-tified inefficiencies in the research ethics review process as amajor barrier to the establishment of multi-centre cancerclinical trials in Ontario. In 2003, the Ontario CancerResearch Network responded by establishing the OntarioCancer Research Ethics Board (OCREB).19 The board now has22 member-centres, representing the majority of theprovince’s hospitals that conduct cancer trials in Ontario.This overarching ethics board markedly reduces the duplica-tion and workload for researchers, sponsors and local ethicboards throughout Ontario. Similar specialized multi-institu-tional research ethics boards operate in Alberta and BritishColumbia.
Recommendations If we believe, as a society, that finding a cure for cancer isimportant then federal and provincial governments, healthcare organizations, hospitals, universities and foundationsmust acknowledge and support clinical cancer research.The success of programs such as the Pan Canadian CancerResearch Strategy, and the CIHR Strategy for Patient-Oriented Research, along with other clinical cancer
28 REPORT CARD ON CANCER IN CANADA, 2010–11
THE ORGANIZATION OF CANCER CARE
“If Canada is not successful in rewarding innovation, innovation will be developed elsewhere.”14
—Russell Williams, President of Rx&D Canada

REPORT CARD ON CANCER IN CANADA, 2010–11 29
initiatives, will depend on the following commitments.1 A long term financial commitment by government(s)
and healthcare organizations to provide stable fund-ing and a system of support for clinical cancerresearchers. Funding support could be modeled afterthe U.K.’s National Cancer Research Network programthat has successfully supported clinical cancerresearchers and consistently increased patient partici-pation in clinical trials throughout the U.K. over thepast ten years.
2 Adequate infrastructure support within cancer basedhealthcare organizations that facilitate patient partici-pation in clinical trials. This would require sustainableresources for patient recruitment, clinical researchassociates, data managers and oncology nurses.
3 Measurable indicators that include real time assess-ment and implementation of what is working welland elimination of what is not.
4 Improved efficiencies in the activation and conduct ofclinical trials in order to remain competitive in inter-national markets, to ensure that Canadians have con-tinued access to novel cancer drugs and treatments.This would require the development of a seamlessnational approach to contract negotiations, researchethics approval, regulatory monitoring and budgetnegotiations.
All of this could be made possible if each Canadian affectedby cancer were offered a clinical trial as a “standard” treat-ment option. We, the general public, can do our part byaccepting the importance of cancer clinical research andendorsing this change in medical practice. No longer wouldindividuals who participate in clinical trials have to feel like“guinea pigs”. Rather, by understanding that participationin clinical cancer trials assures consistent standards and reli-able quality of care, concerns about participating in researchwould evaporate. Participation in a study may lead not onlyto better outcomes for the patient but may also make a signif-icant contribution to the discovery of new and better cancertreatments. Importantly, cancer control would be immeasur-ably accelerated.
Susan F. Dent, BSc, MD, FRCPC, is a Medical Oncologist atThe Ottawa Hospital Cancer Centre; Associate Professor ofMedicine, University of Ottawa. She is a member of theNCIC-CTG Breast Disease Site Group, Cancer Care OntarioBreast Disease Site Guideline Committee and the OntarioCancer Research Ethics Board.
Sandi Yurichuk, BSc, MBA, PhD candidate, is on the Boardof Directors of the CACC. Sandi has her own consultingcompany based in California and specializes in oncologydrug development. She is currently enrolled in a PhD pro-gram at the International School of Management in Paris,France.
© 2011 Susan Dent and Sandi Yurichuk. Used with the kind permis-sion of the authors.
References 1 Canadian Cancer Society (2010). General Cancer Statistics for 2010.
Retrieved January 26, 2011, from www.cancer.ca/Canadawide/About%20cancer/Cancer%20statistics/Stats%20at%20a%20glance/General%20can-cer%20stats.aspx?sc_lang=en
2 Canadian Cancer Research Alliance (2010). Pan-Canadian Cancer ResearchStrategy: A plan for Collaborative Action by Canada’s Cancer Research Funders.Toronto: CCRA. Retrieved March 16, 2011 from http://www.ccra-acrc.ca
3 Barriers to Clinical Trial Enrollment - National Cancer Institute 11 Apr 2001... “Any improvements in cancer care come from clinical trials,” said EzekielJ. Emanuel, M.D., Ph.D., chair of the Department of Clinical. RetrievedMarch 12, 2011 from www.cancer.gov/clzzinicaltrials/conducting/.../doctors-barriers0401
4 2010 Systemic Performance Report. The Canadian Partnership AgainstCancer, November 2010 Retrieved March 27, 2011 from www.can-cerview.ca/idc/groups/public/documents/webcontent/system_perform-ance_2010.pdf
5 Grossi F, Belvedere O, Rosso R. Geography of Clinical Cancer ResearchPublications from 1995 to 1999, Eur J Cancer, 39: 106-111, 2003.
6 Winer E, Gralow J, Diller L, et al (2008). Clinical Cancer Advances 2008:Major Research Advances in Cancer Treatment, Prevention, and Screening: AReport from the American Society of Clinical Oncology. J Clin Oncol 27:812-826.
7 Clinical Trials in Canada: Quality with Cost Advantage. Government ofCanada 2003. Retrieved March 30, 2011 from http://investincanada.gc.ca/eng/default.aspx
8 Cancer Care Ontario – Cancer Quality Council of Ontario Report: CancerPatient Participation in Clinical Trials. Retrieved March 16, 2010 fromhttp://csqi.cancercare.on.ca/cms/one.aspx?objectId=67928&contextId=63405 and http://csqi.cancercare.on.ca/search/default.aspx?q=clinical%20trial%20participation&type=0,6-76,6-40484|-1,63405-78
9 Canadian Institute for Health Research (2010); Strategy for Patient-OrientedResearch: A Discussion Paper for a 10-Year Plan to Change Health Care Usingthe Levers of Research. Retrieved January 13, 2011 from www.cihr-irsc.gc.ca/e/41232.html
10 Canadian Cancer Research Alliance (2009). Cancer Research Investment inCanada, 2007: The Canadian Cancer Research Alliance’s Survey ofGovernment and Voluntary Sector Investment in Cancer Research in 2007.Toronto: CCRA.
11 Getz KA (2005). A Swift Predominance of Ex-U.S. Sites. Applied ClinicalTrials. Retrieved January 27, 2011, from http://appliedclinicaltrialsonline.findpharma.com/appliedclinicaltrials/article/articleDetail.jsp?id=261633
12 Thiers FA, Sinskey AJ, Berndt ER (2008). Trends in the Globalization of ClinicalTrials. Nature Reviews Drug Discovery 7, 13–14 doi:10.1038/ nrd2441News Analysis.
13 Dilts DM (2010). Early Warning: An Ailing Canary in the Mine. Journal ofClinical Oncology 28(24): 3799-3800.
14 Williams Russell. President of Canada’s Research based PharmaceuticalCompanies (R&D statement – PMPRB Report 2005 Canada Newswire 23June 2006.
15 Association of Canadian Academic Healthcare Organizations (ACAHO)(2010) Leveraging Health Research, Innovation & Commercialization InSupport Of Health System Renewal And Economic Prosperity; A Submission tothe House of Commons Standing Committee on Finance; August 13, 2010.Retrieved March 16, 2011 from http://www.acaho.org/?document&id=205.
16 National Cancer Research Institute Press Release; Sunday 7 November2010. Number of cancer patients taking part in clinical studies quadruplesin a decade. Retrieved March 17, 2011 fromhttp://info.cancerresearchuk.org/news/archive/pressrelease/2010–11-07-NCRN-clinical-trials]
17 Cameron D, Cooper M, Haward B, et al. Four-fold increase in recruitmentof cancer patients to NCRN portfolio studies between 2001 and 2010: atale of investment bringing returns. National Cancer Research Institute(NCRI) 2010. Retrieved March 30, 2011 from: www.ncri.org.uk/ncriconfer-ence/2010abstracts/abstracts/PP39.htm
18 National Institute for Health Research (NHS) 2010 Press Release. RetrievedMarch 15, 2011 from http://www.nihr.ac.uk/Pages/default.aspx
19 Sanginur R, Dent SF, Schwartz L. et al. Ontario Cancer Research Ethics Board:Lessons Learned From Developing a Multicenter Regional Institutional ReviewBoard JCO Mar 20, 2008:1479-1482; DOI:10.1200/JCO.2007. 12.6441.

IntroductionIt is anticipated that because of our aging population theincidence and prevalence of cancer in Canada will continueto increase. The rise in the volume of patients will need to bemet with an expansion of oncology services. This shouldinclude an increase in the number of healthcare profession-als involved in the initial patient assessment, the safe deliv-ery of chemotherapy and supportive care medications, sur-veillance and palliative care. The current and anticipatedshortage in qualified medical oncologists in Canada is beingmitigated in many cancer centres by utilizing clinical prac-tice associates or general practice oncologists. Expanding therole of non-physician healthcare professionals, such as nursepractitioners (NPs) and pharmacists, may be another solu-tion to concerns regarding the oncology workforce.
Pharmacists are ideally suited to work in a systemic ther-apy collaborative practice because of their knowledge ofpharmacology, drug toxicities, drug interactions, order entrysystems and funding mechanisms in those jurisdictions thatdo not have a fully funded public drug coverage system.Nurse practitioners also work effectively within cancer careprograms as part of a multidisciplinary team. In addition totheir ability to prescribe supportive care medications andchemotherapy, they can offer psychosocial care, perform cer-tain procedures and participate in patient education. Nursepractitioners also have formal training in patient assessmentand physical examination.
Over the last decade a growing number of nurse practi-tioners and clinical pharmacists are providing direct patientcare as part of a collaborative agreement with oncologists,particularly in the United States.1 Collaborative agreementsmay be informal or, more appropriately, a written agreementdescribing a cooperative practice relationship between a NPor pharmacist and a physician, with legal authority to pre-scribe medications.2,3 In North Carolina, pharmacists canprescribe medications under a collaborative agreement witha supervising physician.4 The State Board of Pharmacy andMedical Board must first approve this collaborative agree-ment. Once this process has been completed, the pharmacistis licensed as a clinical pharmacist practitioner (CPP). Thescope of practice varies between institutions but may include
the ability to assess patients, order supportive care medica-tions (antiemetics, growth factors, anticoagulants, bisphos-phonates, blood products, antibiotics, smoking cessationproducts), order intravenous chemotherapy, depot hormonetherapies and order laboratory and imaging investigations.
Similar collaborative agreements exist in cancer centres inCalifornia and other states, where CPPs may also prescribetake home oral cancer drugs such as capecitabine and tyro-sine kinase inhibitors. Pharmacists and nurse practitionerscan also prescribe narcotics but require a special license fromthe United States Drug Enforcement Agency (DEA).5 Surveysof state pharmacy organizations and state pharmacy boardsin the United States have demonstrated that collaborativepractices in the oncology and non-oncology settings have apositive effect on pharmacist-physician relationships.6
Although some Canadian provinces now have legislationthat allows pharmacists to have limited prescribing privilegesin the retail setting, many jurisdictions still don’t have lawswhich allow hospital or cancer centre pharmacists to pre-scribe.7 Nurse practitioners are legislated in several provincesto prescribe. They also directly assess patients and perform anumber of other functions historically done by physicians,depending on the scope of their practices as defined by theirhealthcare authority.
We surveyed comprehensive cancer centres from eachprovince to determine the current status of the nurse practi-tioner and pharmacist in the setting of a collaborative prac-tice and to see whether they were prescribing supportive caremedications and chemotherapy.
MethodsPharmacists and nurse practitioners working in comprehen-sive cancer centres in 10 Canadian provinces were surveyedeither by telephone or by e-mail. A structured questionnairewas used to determine their scope of practice, involvementin direct patient care and prescribing. A senior pharmacy stu-dent or pharmacist conducted the survey. The survey wasstarted on November 1, 2010 and completed on January 18,2011.
ResultsThere was one response from each of the 10 provinces (Table1). In four provinces (AB, ON, NS and NB), both NPs andpharmacists have prescribing privileges in their institutions
The Role of the Nurse Practitioner and Clinical Pharmacist
IN COLLABORATIVE PATIENT CARE AND DRUG THERAPY MANAGEMENT IN CANADIAN CANCER CENTRES
by JONATHAN EDWARDS, BSc, SCOTT EDWARDS, PharmD, and DAVID SALTMAN, MD, PhD
THE ORGANIZATION OF CANCER CARETHE ORGANIZATION OF CANCER CARE
30 REPORT CARD ON CANCER IN CANADA, 2010–11

REPORT CARD ON CANCER IN CANADA, 2010–11 31
as part of a collaborative agreement. However, the pharma-cist does not prescribe in any of the centres surveyed. Thereare six centres with NPs who prescribe one or more types ofoncology medications (Table 2). Two centres (NS and AB)indicated that NPs were involved in prescribing intravenouschemotherapy, oral chemotherapy, hormone therapies andsupportive care medications. Three centres (NS, ON and AB)follow patients in their clinics who are no longer on activetreatment.
In Manitoba, NPs supervise chemotherapy but do not pre-scribe the drugs. They do prescribe supportive care medica-tions except narcotics. In the cancer centres in NS and NBthat were surveyed, NPs use preprinted orders forchemotherapy, while centres surveyed in Ontario andAlberta used electronic ordering systems. In three of the cen-tres where NPs are prescribing chemotherapy, they treatpatients in both the adjuvant and metastatic settings.Centres indicated in the survey that NPs prescribechemotherapy after the oncologist initiates cycle 1 (Table 2).In those centres where chemotherapy patients were underthe supervision of NPs, they are referred back to their oncol-ogists when there are serious adverse events, significant doseadjustments required, after assessment of disease status andat the end of a prescribed number of chemotherapy cycles.
Newfoundland and Labrador does not have legislationthat allows institution-based pharmacists to enter into a col-laborative agreement with a physician or prescribe.Pharmacists in NL do supervise the administration of oralchemotherapy (capecitabine and temozolomide) for patientsreceiving combined modality concomitant chemotherapyand radiation but they must have a physician order investi-gations and sign chemotherapy orders. There is one NPworking within a cancer centre in the department of radia-tion oncology who has authority to prescribe hormone ther-apies and supportive care medications. There were only twocentres where NPs prescribe take home cancer drugs. Cancercentres in Saskatchewan and Quebec that were surveyedindicated they do not have any oncology nurse practitioners.Pharmacists do not have the authority to prescribe in thosecentres.
The cancer centres with NPs supervising and prescribingdrug therapy indicated an improvement in job satisfactionand thought there was a decrease in wait-times for patientsto start chemotherapy.
DiscussionOur survey results suggest that the role of both nurse practi-tioners and pharmacists in Canadian cancer centres isexpanding to include more direct patient assessment anddrug therapy management. Although several provincialnursing, pharmacy and medical boards allow NPs and phar-macists to enter into collaborative agreements with physi-cians, only NPs are prescribing cancer therapies at the timethis survey was conducted.
The reasons why there aren’t more NPs with prescribingauthority in collaborative practice working in Canadiancancer centres is not clear. A 2008 survey of British specialistnurses working in cancer and palliative care looked at thebenefits and barriers to uptake of nurse prescribing training.8
The main reason for obtaining prescribing privileges was the
prospect of improving care. The main reasons why nursespecialists did not pursue prescribing training were: resourceissues, lack of medical support and mentorship, and con-cerns about the relevance of prescribing as a nursing role.
There are a number of factors that may be limiting pharma-cists from expanding their roles in oncology. The separationof prescribing and dispensing is thought to be an importantsafety or quality control issue. However, within a cancer centreor program, it is likely that a limited number of clinical phar-macists will enter into a collaborative agreement to pre-scribe, thereby separating the functions and maintainingquality assurance. Healthcare administrators and govern-ments may not support the transition of pharmacists fromtheir traditional roles to those where they would have the
TABLE 1
SURVEYED CANCER CENTRES AND THE CHEMOTHERAPYPRESCRIBING STATUS FOR NURSE PRACTITIONERS (NPs)AND PHARMACISTS
NL 1 Yes* Yes No NoNS 1 Yes Yes Yes No PE 1 No No No NoNB 1 Yes Yes Yes NoQC 1 No No No NoON 1 Yes Yes Yes NoMB 1 Yes Yes No NoSK 1 No No No NoAB 1 Yes Yes Yes NoBC 1 No No No No
*Radiation oncology nurse practitioner
Province Numberof cancercentressurveyed
NPs incollabora-tive practice
NPs pre-scribing
Pharmacistsin collabo-rative practice
Pharmacistsprescribing
TABLE 2SCOPE OF PRACTICE FOR NPs PRESCRIBING ONCOLOGY MEDICATIONS
NL Computer No No Yes YesNS Preprinted Yes* Yes* Yes Yes
ordersNB Preprinted Yes* No No Yes
ordersON Computer Yes* No No NoMB Computer No No No YesAB Computer Yes* Yes* Yes Yes
* Ordered by NP after cycle 1.** Except narcotics
Province Order entrysystem
Intravenouschemo-therapy*
Oralchemo-therapy
Hormonetherapy
Supportive care drugs**

authority to directly assess cancer patients and prescribemedications. We did not interview oncologists as part of thisstudy to determine their attitudes towards NPs and pharma-cists expanding their roles in direct patient care and prescrib-ing. However, the support is likely high because theincreased participation of the NPs and pharmacists should intheory free up more time for oncologists to see new patients,formulate treatment plans, participate in research and fulfilltheir administrative commitments. Many cancer centrepharmacies are short staffed making it difficult for pharma-cists to expand their clinical roles. This issue will need to beaddressed for pharmacists to increase the scope of their prac-tices.
Unlike nurse practitioners, many pharmacists may lackthe clinical assessment and diagnostic skills needed to partic-ipate more fully in collaborative practices. These skills couldbe easily acquired through formal education programs orthrough supplemental training within cancer centres.
Concerns have also been raised about the attitudes ofpatients regarding the expanded role for pharmacists in areaslike clinical assessment. Our experience with pharmacist-ledoral chemotherapy clinics suggests that the patient satisfac-tion is high. Clients and their families are always instructedthat pharmacists are part of a multidisciplinary team, whichallows us to better monitor safety and reduce clinic waitingtimes. Internal audits of our pharmacy-/general practiceoncology-led rectal cancer neoadjuvant capecitabine clinicshave demonstrated a reduction in serious adverse events.
LimitationsThis survey was conducted at a limited number of compre-hensive cancer centres throughout the country. For thesmaller provinces, data from a single centre may be reflectiveof current practices in the entire province. However, for larg-er provinces like Ontario with multiple cancer centres andclinics, there may be differences in practice for both NPs andpharmacists that are not reflected in this study. We did notconduct the survey in any of the Territories.
ConclusionsThe disciplines of nursing and pharmacy are evolving rapid-ly, thus allowing practitioners to diversify and deliver directpatient care as part of a collaborative practice. Our surveysuggests that only nurse practitioners are prescribingchemotherapy in Canadian cancer centres and that moreneeds to be done to encourage and assist qualified pharma-cists who wish to obtain the right to prescribe within theirscope of practice. For pharmacists, the decision to enter intoa collaborative practice with the authority to prescribeshould be based on competency and not necessarily on edu-cational attainment. Pharmacist may be required to com-plete a multi-step process to demonstrate they have therequired competencies, similar to the process used by theAlberta College of Pharmacists.7 Outcomes from the expand-ing role of NPs and pharmacists in oncology should be meas-ured to assess their impact. Oncology healthcare profession-als, health authority administrators and provincial and terri-torial medical and pharmacy boards should work together torapidly facilitate the development of collaborative practiceguidelines and regulations.
Recommendations• Implement changes to the Pharmacy Act for those
provinces that currently do not incorporate practice stan-dards for pharmacist prescribing in their regulatory guide-lines.
• Develop formal collaborative practice agreements.Collaboration with other health providers is an importantand integral component to pharmacist prescribing. Thepharmacist should develop a collaborative practicemodel, which includes ongoing two-way communicationand documentation regarding drug therapy decisionswith other health care professionals.
• Develop educational and competency requirements. Thepharmacist should participate in continuing educationprograms, annually complete a professional developmentlog for review, use a self-assessment tool to identifystrengths and opportunities for further development, andparticipate in assessments of practice.
• Develop a process for notification of other health careprofessionals. Actions related to prescribing and medica-tion management need to be communicated verbally, inwriting or through electronic media, when appropriate, toother health professionals. All actions should be support-ed by documentation.
• Include the ability to order laboratory tests into the phar-macist’s collaborative agreement. Pharmacists shouldhave the authority to order laboratory tests for the pur-pose of monitoring drug therapy outcomes.
• Provide for quality assurance. The pharmacist in a collab-orative practice should develop, maintain and coordinatea comprehensive quality assurance program to assure thequality of their prescribing.
Jonathan Edwards, BSc, Senior Pharmacy Student, School ofPharmacy, Memorial University
Scott Edwards, PharmD, Clinical Oncology Pharmacy Specialist,Dr. H. Bliss Murphy Cancer Centre, and Assistant ClinicalProfessor, School of Pharmacy, Memorial University
David Saltman, MD, PhD, is the Chair and Professor of theDiscipline of Oncology, Faculty of Medicine, Memorial University.
References1 Status of collaborative drug therapy management in the United
States, March 2004. Am J Health Syst Pharm 2004; 61: 1609-10.2 Emmerton L, Marriott J, Bessell T, Nissen l, Dean L. Pharmacists and
prescribing rights: Review of international developments. J PharmPharmaceut Sci 2005; 8(2): 217-25.
3 Pearson GJ, Yuskel N, Card D, et al. Task force on pharmacist prescrib-ing. An information paper on pharmacist prescribing within a healthcare facility. Can J Hosp Pharm 2002; 55: 56-62.
4 Sessions JK, Valgus J, Yowell Barbour S, Iacovelli L. Roe of oncologyclinical pharmacists in light of oncology workforce study. J OncolPract 2010; 6: 270-71.
5 Dole EJ, Murawski MM, Adolphe AB, Aragon FD, Hochstadt B.Provision of pain management by a pharmacist with prescribingauthority. Am J Health Systm Pharm 2007; 64(1): 85-9.
6 Punekar Y, Lin SW., Thomas J3rd. Progress of pharmacist collaborativepractice: status of state laws and regulations and perceived impact ofcollaborative practice. J Am Pharm Assoc 2003; 43(4): 503-10.
7 Pearson JG. Evolution in the practice of pharmacy-not a revolution.CMAJ. April 24, 2007; 176 (90. Doi:10.1503/cmaj.070041.
8 Ryan-Woolley B, McHugh G, Luker K. Exploring the views of nurseprescribing among Macmillan nurses. Br J Community Nurs 2008;13(4): 174-7.
32 REPORT CARD ON CANCER IN CANADA, 2010–11
THE ORGANIZATION OF CANCER CARE

REPORT CARD ON CANCER IN CANADA, 2010–11 33
By RONAN FOLEY, MD, FRCPC
Clinical BackgroundAllogeneic bone marrow transplantation (BMT) offers thehope of cure to patients with otherwise fatal blood andhematological malignancies. In its simplest form the processinvolves replacement of a diseased bone marrow with mar-row from an otherwise healthy donor. Although complex, itis now known that a balanced engraftment of both donorhematopoietic blood forming stem or progenitor cells as wellas donor immune white blood cell effectors (T-lymphocytes)is required for sustained hematopoiesis and long term eradi-cation of disease. Thus, it is not just the transplant condi-tioning that destroys host cancer cells but the downstreamimmunological consequences of a persistent attack from adonor immune system (also known as graft-versus-tumoureffect).
Immune function of donor T-lymphocytes contributes toboth therapeutic efficacy as well as unwanted post transplantside effects, including at times severe graft versus host disease(GVHD). Shifting the balance of therapeutic efficacy fromstem cell replacement to maintenance of a transplantedimmune system has led to less intense preparative regimensthat focus on stable chimeric donor white blood cellimmune survival. These less intense, reduced intensity con-ditioning (RIC) or “mini” allogeneic transplants are now rou-tinely recommended for older patients with underlyingincurable myeloid and lymphoid malignancies. BMT as anoption for older patients has increased transplant activity intransplant centres across the country. In addition to RIC,other breakthroughs (i.e., use of cord blood in adult patients)in the field of stem cell transplant are transforming this pro-cedure from a few, to many. During this growth phase weneed to confirm that proper infrastructure, regulation andsupports are in place to ensure success in this “high stakes”life saving procedure.
Allogeneic Transplants are Saving LivesOnce associated with a mortality of more than 60 per cent,the outcome of allogeneic BMT has dramatically improvedthrough a blend of incremental breakthroughs. Theseinclude antimicrobials with greater specificity for bacterialand fungal infections that result from prolonged neutrope-nia. Preventive treatment strategies to mitigate severe sys-temic viral infections, rational use of growth factors and
advances in general supportive care have also contributed toimproved survival.
The process of safely performing allogeneic BMT is com-plex and requires the experience of a comprehensive multi-disciplinary team comprised of oncologists/hematologists,nurse practitioners, primary care nursing staff, pharmacy,social work, dietitians as well as consultation from a widerange of sub-specialities: gastroenterology, dermatology,infectious disease and respirology. Laboratory expertise in
stem cell manipulation, enumeration and cryopreservation,utilization of blood products as well as DNA specific HLA-typing are also highly essential components of a successfultransplant unit. Despite diverse backgrounds and an exten-sive list of steps, each specialty must properly perform andcoordinate specific roles and responsibilities in an effort toensure the optimal outcome for any individual patient. Asmentioned, the hospital laboratory plays a unique and cen-tral role in the management of BMT patients which startswith ensuring that the stem cell product, either blood ormarrow derived has been properly managed, modified (ifrequested), labelled, preserved and characterized. Given thata clinical outcome depends on the predicted performance ofa specific product there is little room for error.
Bone Marrow TransplantationIMPROVING OUTCOMES FOR CANADIAN PATIENTS
THE ORGANIZATION OF CANCER CARETHE ORGANIZATION OF CANCER CARE
Ronan Foley

Stakes are High: Need for Regulation and Standardization Bone marrow transplants are performed in 23 centres acrossCanada and there is a need to standardize transplant policiesand procedures. Therapeutic cell products are regulated bio-logicals and evaluation and accreditation of each transplantcentre is obtained through inspections from Health Canada(mandatory) and in a growing number of centres by theFoundation of Cellular Therapy (FACT). Both organizationsrequire a comprehensive set of validated Standard OperatingProcedures (SOPs) and specific policies that ensure absolutepatient/product safety. Evidence of well-developed, highlydetailed and validated SOPs ensure that a program functionsin an integrated manner under thorough scrutiny. Givenmany single points of failure, it is this absolute level of detailwith a “no stone left unturned” mentality that results in con-sistent patient outcomes. Seeking and obtaining FACTapproval remains important to Canadian transplant centresbut does require appropriate support (infrastructure and staff)to establish and properly maintain. These ongoing fundingrequirements remain a significant current challenge inCanada; however given the direct link to patient safety thereis a need to ensure that ongoing developments in transplantaccreditation are maintained without compromise.
Despite important advances in the safety and outcome ofallogeneic BMT patients there remains room for improve-ment in prevention and treatment of severe acute and chron-ic GVHD as well as relapse of the original disease. Whileresearch continues into the biological mechanisms of relapse,efforts to identify the best possible marrow donors in Canadaalso have the potential to dramatically improve transplantoutcomes. In this regard increasing the collective pool ofCanadian donors will also increase the likelihood of findingthe “best match” thus yielding the best clinical results.
Bone Marrow DonorsEfforts to improve outcomes of patients undergoing BMT areconstantly being refined and improved. Perhaps not surpris-ingly it is now known that the outcome of BMT largelyrelates to the individual that is providing the bone marrowgraft. Obtaining stem cells from a donor can occur in one ofthree transplant situations.
Stem cells may be collected from a patient to be adminis-tered back into that patient. This is referred to as an autolo-gous stem cell transplant and is used to treat patients up tothe age of around 70 with multiple myeloma, relapsed non-Hodgkin’s lymphoma and Hodgkin’s lymphoma. Relapse ofprimary disease remains a predominant issue in this type oftransplant.
An allogeneic transplant involves the use of a stem cellgraft (containing CD34+ progenitor cells) that is provided bya healthy donor to a patient. In this setting a brother or sis-ter, or twin may be called upon to donate blood/marrowstem cells. This is known as a matched-related alloBMT.Family members will be asked to undergo typing to deter-mine if a sibling is a match (25 per cent chance). In Canadaa sibling donor may have an option of providing bone mar-row (approximately 1 litre – adult) collected from the pelviswhile under anesthesia or mobilized peripheral blood pro-
genitors (collected by leukopheresis – CBMTG Canadianphase III study). If a patient does not have a suitable avail-able sibling an unrelated donor search will be initiated.
When an HLA matched unrelated donor is sought manyadditional issues emerge. These otherwise healthy donors areengaging in an altruistic act with the potential to save a life.At the same time it is important to ensure that the productscollected from these donors remain confidential and havethe best chance of optimal clinical performance. Whereasthe availability of matched related sibling donor transplantsmay diminish over time due to smaller families, unrelateddonors are clearly a future focus for growth and develop-ment. With the importance of maintaining a strong younghealthy pool of Canadian donors this article will focus ontwo issues that will influence the state of allogeneic BMT inCanada. One relates to science and technology and the otherto public or social awareness in our younger generations.
Sources of Marrow Stem CellsSources of stem cells have expanded over the past decade.While stem cells were traditionally obtained from the poste-rior pelvis of a donor under general anesthesia, stem cellscan now be obtained from peripheral blood as well as fromumbilical cord blood. Each source of stem cells, blood vs.marrow vs. cord, exhibits different biological properties. Ifone compares a bone marrow graft (approximately 1,000ml)to mobilized blood stem cells collected by leukopheresis dis-tinct differences can be seen in graft composition.Interestingly, a mobilized peripheral blood product usuallycontains a greater number of CD34+ progenitor stem cellsbut also a greater number of CD3+ T lymphocytes and poten-tially a greater risk of chronic GVHD.
The Canadian Bone Marrow Transplant Group (CBMTG)is nearing completion of a large phase III study which willaddress the issue of optimal graft source by comparingfilgrastim-mobilized blood to filgrastim-mobilized marrow inmatched related alloBMT. This Canadian-led study will indi-
Optimal clinical out-comes are seen whenyoung and healthydonors are engaged.
34 REPORT CARD ON CANCER IN CANADA, 2010–11
THE ORGANIZATION OF CANCER CARE

cate the optimal source of stem cells based on a compositeendpoint of relapse/mortality and GVHD, and will also eval-uate what is the preferred approach based on the donor’soverall experience. Understanding these properties, includ-ing the recent use of cord blood derived stem cell productsfor children and more recently for adults, enables the abilityto tailor which graft source should perform best for a givenindividual clinical situation.
As previously mentioned, a donor may be asked to donatestem cells for a sibling (brother or sister) or other familymember (matched related donor) or to join a large nationalregistry (matched unrelated donor). A national marrowdonor program will HLA-type potential donors and maintaininformation in a registry that can be searched for a range oftransplant eligible patients in need of a suitable marrowdonor. All donors should be in good general health andundergo rigorous donor screening.1,2 As the transplant eligi-ble age increases so does the potential donor pool of relatedsiblings. Co-morbidities such as COPD, diabetes, heart dis-ease need to be taken into consideration.
Any potential donor should be in satisfactory health so asto tolerate either anaesthesia-marrow harvest or administra-tion of filgrastim and large volume apheresis. In addition togeneral health bone marrow donors must be screened foractive malignancies (excluding “benign” basal cell skin can-cer), transmissible viral disease (HIV, hepatitis B/C, HTLV-1,West Nile virus, syphilis), haematological diseases (sicklecell) as well as bleeding disorders. A combination of compre-hensive questionnaires, complete history and physical exam-ination ensure a donor is suitable.
Once screened and considered eligible the most relevantdonor factor that predicts success across several clinical end-points is age.3 Bone marrow recipients from younger donors(i.e., less than 30 years of age) demonstrate improved five-year overall and disease-free survival. A modest decrease insevere GVHD has been noted with younger donors. Otherfactors4,5 include CMV serological status and blood type .Finally there may be a higher rate of chronic GVHD in recip-ients of stem cells from a female donor with a history of mul-tiple births.
Finding the Best MatchAs in other transplant situations, matches are based on thehuman leukocyte antigen (HLA) system. HLA is comprised ofa series of genes on chromosome6 that encode cell-surfaceantigen presenting proteins intrinsically linked to ourimmune system. The major histocompatibility complex(MHC) is made up of two basic classes involved in antigenpresentation and subsequent immune activation. MHCclass I is typically involved in presentation of small peptidesthat result from intracellular digestion. MHC class II presentsthose extra-cellular antigens to host T lymphocytes. MHCclass I includes HLA-A, HLA-B and HLA-C, whereas MHCclass II includes HLA-DR, HLA-DQ, and HLA-DP. Proteinsencoded by HLA define our unique self and directly instructthe immune system to recognize self versus non-self. In anyindividual one set (haplotype) of HLA genes comes directlyfrom the mother and the other set from the father, leavingonly a 25 per cent chance that any given sibling will matcha brother or sister.
Previously, HLA typing was performed using serologicaltesting to identify HLA serotypes. This provides a low-resolu-tion map of an individual’s HLA type. Although useful in therelated setting, there have been concerns regarding its use inunrelated donors where higher resolution of HLA geneticmapping will lead to a better match. If HLA typing lackedsufficient accuracy this would undoubtedly influence therate of GVHD. HLA laboratories now perform high resolutionmolecular or DNA typing to ensure a potential unrelateddonor/recipient pair are as highly matched (HLA A,B,C, DR)as possible.6,7 Studies suggest that employing a molecularapproach can reduce the incidence of severe GVHD andimprove survival by as much as 50 per cent.8
Careful donor selection and molecular typing haveimproved the overall quality of unrelated transplants to thepoint where they are considered nearly as safe as when arelated donor is used. However there are downsides, the firstbeing that employing a highly specific molecular analysiswill effectively reduce the number of available donors.Moreover the process may increase the time required to iden-tify a potential donor worldwide. On average three to sixmonths may be required and given the nature and stability ofprimary diseases requiring transplant (i.e., relapsed myeloidleukemia) this may not be feasible. Various algorithms nowexist that combine a serological search with latter confirma-tory molecular analysis. These steps may improve the timeand expense of finding a suitable marrow donor.
Issues such as the number of simultaneous potentialdonors to be typed by high-resolution include whether arecipient has a rare allele or haplotype as well as the clinicalurgency for allogeneic BMT are important. It should also benoted that a single allele mismatch (9/10) when typing forHLA-A, -B, -C, DRB1 and DQB1 (i.e., 10/10) may be consid-ered by some centres. In this regard a single mismatch at Bor C may be less of a concern than mismatches at A or DR.Potential Canadian donors are currently represented byOneMatch Stem Cell and Marrow Network. This group isactively developing algorithms to effectively and efficientlyscreen for possible Canadian donors in the least time possi-ble using the results of a blend of intermediate and high res-olution typing techniques.
Despite these challenges the OneMatch national registryhas seen a marked improvement in the number of availabledonors and utilization of Canadian stem cell products(Figures 1 and 2) and continues to provide highly matchedbone marrow donors to Canadian patients in need of atransplant.
Donor Registry—The ChallengesSigning up to be a marrow donor is a voluntary act. Thestrength of any national registry, including our ownCanadian registry is the number of potential donors avail-able as well as the time and cost to search the registry in astep-wise efficient manner. In terms of creating a robustnational registry Canada faces two challenges.
First, our overall population is relatively small and spreadout. Our second major challenge relates to Canada as a highlydiverse ethnic population.
As can be seen in Figure 3, the ethnic composition of thecurrent OneMatch database demonstrates a non-representa-
REPORT CARD ON CANCER IN CANADA, 2010–11 35
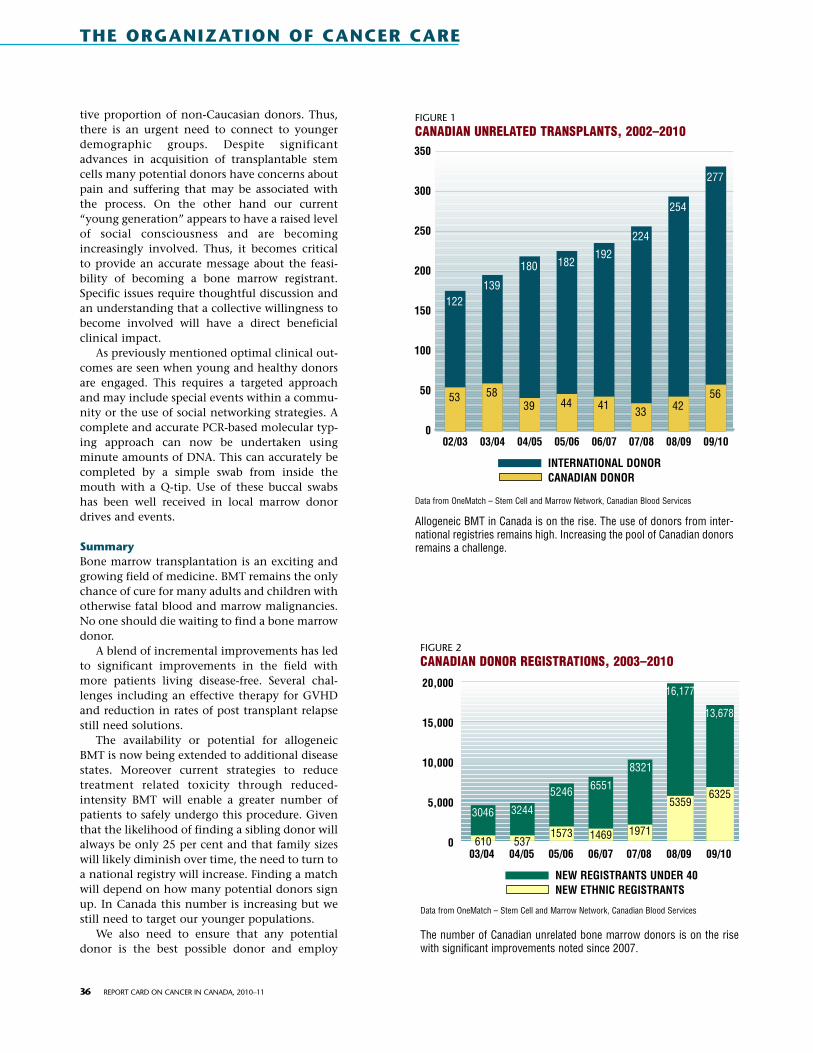
tive proportion of non-Caucasian donors. Thus,there is an urgent need to connect to youngerdemographic groups. Despite significantadvances in acquisition of transplantable stemcells many potential donors have concerns aboutpain and suffering that may be associated withthe process. On the other hand our current“young generation” appears to have a raised levelof social consciousness and are becomingincreasingly involved. Thus, it becomes criticalto provide an accurate message about the feasi-bility of becoming a bone marrow registrant.Specific issues require thoughtful discussion andan understanding that a collective willingness tobecome involved will have a direct beneficialclinical impact.
As previously mentioned optimal clinical out-comes are seen when young and healthy donorsare engaged. This requires a targeted approachand may include special events within a commu-nity or the use of social networking strategies. Acomplete and accurate PCR-based molecular typ-ing approach can now be undertaken usingminute amounts of DNA. This can accurately becompleted by a simple swab from inside themouth with a Q-tip. Use of these buccal swabshas been well received in local marrow donordrives and events.
SummaryBone marrow transplantation is an exciting andgrowing field of medicine. BMT remains the onlychance of cure for many adults and children withotherwise fatal blood and marrow malignancies.No one should die waiting to find a bone marrowdonor.
A blend of incremental improvements has ledto significant improvements in the field withmore patients living disease-free. Several chal-lenges including an effective therapy for GVHDand reduction in rates of post transplant relapsestill need solutions.
The availability or potential for allogeneicBMT is now being extended to additional diseasestates. Moreover current strategies to reducetreatment related toxicity through reduced-intensity BMT will enable a greater number ofpatients to safely undergo this procedure. Giventhat the likelihood of finding a sibling donor willalways be only 25 per cent and that family sizeswill likely diminish over time, the need to turn toa national registry will increase. Finding a matchwill depend on how many potential donors signup. In Canada this number is increasing but westill need to target our younger populations.
We also need to ensure that any potentialdonor is the best possible donor and employ
36 REPORT CARD ON CANCER IN CANADA, 2010–11
FIGURE 1CANADIAN UNRELATED TRANSPLANTS, 2002–2010
Data from OneMatch – Stem Cell and Marrow Network, Canadian Blood Services
Allogeneic BMT in Canada is on the rise. The use of donors from inter-national registries remains high. Increasing the pool of Canadian donorsremains a challenge.
350
300
250
200
150
100
50
0
122
53
02/03
139
58
03/04
180
39
04/05
182
44
05/06
192
41
06/07
224
33
07/08
254
42
08/09
277
56
09/10
INTERNATIONAL DONORCANADIAN DONOR
FIGURE 2CANADIAN DONOR REGISTRATIONS, 2003–2010
Data from OneMatch – Stem Cell and Marrow Network, Canadian Blood Services
The number of Canadian unrelated bone marrow donors is on the risewith significant improvements noted since 2007.
20,000
15,000
10,000
5,000
0
3046
61003/04
3244
53704/05
5246
1573
05/06
6551
1469
06/07
8321
1971
07/08
16,177
5359
08/09
13,678
6325
09/10
NEW REGISTRANTS UNDER 40NEW ETHNIC REGISTRANTS
THE ORGANIZATION OF CANCER CARE

high resolution HLA-typing to our matching strategy.Ultimately our goal is to ensure that all transplant eligiblepatients find a donor (either Canadian or from another reg-istry) in a timely manner and enable all patients the chanceof being cured.
Positive clinical outcomes will continue to improve withthe implementation of comprehensive accreditation organi-zations and suitable funding required to maintain the cur-rent excellence of BMT transplant units across our country.
Ronan Foley, MD, FRCPC, is a clinical hematologist with an activepractice in malignant hematology at the Juravinski CancerCentre in Hamilton, ON. He is Director of the Stem CellLaboratory and Cell Diagnostic Units. Dr. Foley is an AssociateProfessor of Pathology and Molecular Medicine at McMasterUniversity, President of CBMTG, a Director of the Clinical TrialsNetwork and a member of the NIH Consensus Panel for theDiagnosis and Classification of Chronic Graft vs. Host Diseasealong with several other affiliations. Other activities includeboard membership on OCREB and panel chair for the CIHR CBTpanel. Dr. Foley’s current research focus is the development oftherapeutic cell-based autologous vaccines. He currently hasactive grants with CANVAC, OICR, and NCIC.
© 2011 Ronan Foley. Used with the kind permission of the author.
References1 Rowley SD, Donaldson G, Lilleby K, et al. Experiences of donors
enrolled in a randomized study of allogeneic bone marrow orperipheral blood stem cell transplantation. Blood 2001; 97:2541.
2 Sacchi N, Costeas P, Hartwell L, et al. Hematopoietic stem celldonor registries: World Marrow Donor Association recommenda-tions for evaluation of donor health. Bone Marrow Transplant2008; 42:9.
3 Kollman C, Howe CW, Anasetti C, et al. Donor characteristics asrisk factors in recipients after transplantation of bone marrowfrom unrelated donors: the effect of donor age. Blood 2001;98:2043.
4 Gross TG, Steinbuch M, DeFor T, et al. B cell lymphoproliferativedisorders following hematopoietic stem cell transplantation: riskfactors, treatment and outcome. Bone Marrow Transplant 1999;23:251.
5 Schultz KR, Green GJ, Wensley D, et al. Obstructive lung diseasein children after allogeneic bone marrow transplantation. Blood1994; 84:3212.
6 Sasazuki Juji T, Morishima Y, et al. Effect of matching class I HLAalleles on clinical outcome after transplantation of hematopoiet-ic stem cells from an unrelated donor. N Engl J Med 1998;339:1177.
7 Petersdorf EW, Lonton GM, Anasetti C, et al. Association of HLA-C disparity with graft failure after marrow transplantation fromunrelated donors. Blood 1997; 89:1818.
8 Lee SJ, Klein J, Haagenson M, et al. High-resolution donor-recip-ient HLA matching contributes to the success of unrelated donormarrow transplantation. Blood 2007; 110:4576.
Data from OneMatch – Stem Cell and Marrow Network, Canadian Blood Services
The current ethnic composition of Canadian unrelatedmarrow donors. Efforts to increase donors in end-specificpopulations will increase the likelihood of finding a matchfor any given patient.
FIGURE 3ETHNICITY OF CANADIAN DONOR REGISTRANTS, 2010
Black, 0.6Asian,3.3Hispanic, 0.5Aboriginal, 0.9Other, 3.1
Unknown, 4.8
East Indian, 1.9Chinese, 2.0
South Asian, 0.4Multi-ethnic, 0.3
South-east Asian, 0.2
Caucasian, 81.9 per cent
REPORT CARD ON CANCER IN CANADA, 2010–11 37

by JENNIFER LEVIN CARTER, MD, MPH with JILLIAN LOKERE
Cancer treatment has changed dramatically over the last fewyears. It is now not only possible, but also often important togo beyond classifying tumours based on where they occur inthe body. In fact, two patients with cancer of the same organof origin may well have two very different cancers that canrequire different treatment strategies. Decades of painstakingresearch have demonstrated that each tumour has a uniqueset of genetic aberrations and molecular changes. Some ofthese genetic and molecular characteristics have been termedbiomarkers since they can mark how well a tumour willrespond to certain treatments or how quickly the disease willprogress.
The goal of biomarker research in oncology is to person-alize cancer treatment based on individual tumour character-istics. In the ideal scenario, each tumour is tested to identifyits unique biomarker profile and that information helps toinform decisions about prognosis and treatment. In some cir-cumstances, treatments may be selected more effectivelybased on the biomarker profile of a patient’s tumour. Drugsthat are not likely to work or are not necessary can be avoid-ed, thus saving the significant costs, both financial and per-sonal, of needless therapy.
This is the future of cancer care, but we are not there yet.What is missing? To answer this question, it is instructive toreview the progress that has been made. The journey from thegeneral (all breast cancers are the same) to the specific (breastcancers are of several types) to the near-personalized (yourbreast tumour has biomarkers that indicate it will respond wellto a particular treatment strategy) began in the 1970s with thediscovery of the first biomarker: the estrogen receptor (ER).
The Biomarker RevolutionIn 1971, Elwood V. Jensen at the University of Chicagoshowed that breast tumours rich in ERs were more likelythan ER-poor tumours to respond to treatment that wouldreduce the amount of circulating estrogen in the body.1
When the anti-estrogen compound tamoxifen2,3 was discov-ered as part of a fertility control program, its potential for thetreatment of breast cancer became the subject of muchresearch. By 1973, tamoxifen was known to interfere withestrogen’s ability to stimulate the growth of breast cancercells and was recognized as an effective treatment approachfor breast cancer rich in ERs (“ER-positive” cancer).4
The real breakthrough in biomarker discovery, however,came a few years later. Before the mid-1970s, researchersknew that certain genes, termed “oncogenes”, seemed to be
responsible for the unchecked growth and division charac-teristic of cancer cells. At the time, it was widely believedthat oncogenes were viral in origin, not human, and that thecause of all cancer was infection of human cells by virusescontaining these viral oncogenes. In 1976, J. Michael Bishopand Harold E. Varmus of the University of California, SanFrancisco demonstrated that oncogenes are human in originand can be found in normal human cells. For this revolu-tionary discovery, Bishop and Varmus were awarded theNobel Prize in Physiology or Medicine in 1989.5 Armed witha completely new model for understanding cancer,researchers started to study how normal human genes couldchange to become cancer-causing oncogenes. The race touncover new oncogenes was on.
One of those newly discovered oncogenes was HER2/neu.Studies by Genentech scientists in the early 1980s demon-strated that, in normal human cells, the HER2/neu gene pro-duces a protein that regulates cell growth. In 1987, DennisSlamon at the University of California, Los Angeles and col-leagues from the University of Texas studied breast tumoursamples and found that cancer cells from 25 per cent of thepatients contained many more copies of the gene than didnormal breast tissue cells. This resulted in abnormally highlevels of the HER2/neu protein (“HER2/neu overexpression”).
PERSONALIZED MEDICINE
What is Missing?
THE ORGANIZATION OF CANCER CARETHE ORGANIZATION OF CANCER CARE
38 REPORT CARD ON CANCER IN CANADA, 2010–11
Jennifer Levin Carter

REPORT CARD ON CANCER IN CANADA, 2010–11 39
Most importantly, they found that patients whose tumourshad higher levels of HER2/neu protein had a shorter time torelapse and a shorter overall survival time. In sum, the workshowed that a high level of HER2/neu in a patient’s tumourwas a reliable biomarker for aggressive tumour growth and aworse prognosis.6
In response to this discovery, researchers from Genentechdeveloped a drug to bind to excessive HER2/neu on breasttumour cells, slowing their growth and triggering thepatient’s immune system to destroy them. By May 1998, theresulting molecularly targeted agent, Herceptin (trastuzum-ab), had been shown to increase response rates by about 50per cent and improve time to disease progression by about 60per cent when used with chemotherapy for women withmetastatic breast cancer.7 Herceptin was approved by theUnited States Food and Drug Administration (FDA) later thatyear, followed by approval by Health Canada in 1999.
During the same time period that HER2/neu was discov-ered and targeted through the development of Herceptin,another well-known cancer biomarker was exploited forrational drug design: the Philadelphia chromosome. Thisgenetic mutation results from a translocation, or break-and-swap, that results in part of human chromosome 22 beingjoined to chromosome 9.8 Termed BCR-ABL, this new geneproduces a protein that causes uncontrolled white blood cellgrowth and division in Chronic Myelogenous Leukemia(CML). Researchers at Novartis (then Ciba-Geigy) developedan inhibitor of the BCR-ABL protein, imatinib (Gleevec). By1999, early clinical trials of Gleevec demonstrated remark-able response rates of greater than 90 per cent.9 In 2001,Gleevec was approved in the United States and Canada forPhiladelphia (Ph) chromosome-positive CML.
The success of Herceptin and Gleevec paved the way foradditional important advances in the field of molecularlytargeted therapy. Since 2001, the number of known biomark-ers and targeted therapeutics has grown exponentially. Wenow know that a single biomarker is not always confined toone type of cancer. The Epidermal Growth Factor Receptor(EGFR) is one example. EGFR is a protein that can be overex-pressed or abnormally active in the tumour cells from sever-al cancer types, including lung, colon, head and neck, pan-creatic, and brain. EGFR is the target of more than one drug:gefitinib (Iressa), erlotinib (Tarceva), cetuximab (Erbitux),Vectibix (panitumumab), and lapatinib (Tykerb).10 Suchmedications are typically tested in and approved for use in asingle type of cancer first, then further trials are conductedin other types of cancer that express the appropriate bio-marker. This is the case for Herceptin, a drug originally test-ed and approved for metastatic breast cancer expressing thebiomarker Her2/neu. In late 2010, Herceptin was approvedby the FDA and Health Canada for use in HER2/neu-positivemetastatic stomach cancer.11
Advances in oncology research have demonstrated thatbiomarkers are not limited to a paradigm of “one biomark-er—one targeted agent.” In fact, the biomarkers present orabsent on a patient’s tumour make up a unique molecularprofile that can, in some cases, help physicians predict thepatient’s response to chemotherapy, targeted therapy, orboth. One good example are the multi-gene assays, whichare laboratory tests that check a tumour sample for multiple
biomarkers at the same time. Such multi-targeted assays arean important area of research. Some examples includeMammostrat and MammaPrint for breast cancer, andOncotype Dx for breast and colon cancers. Clinical studieshave shown that these panels can, for certain cancers, dividepatients into groups according to their risk of recurrence.Those in the high-risk group have been shown to benefitfrom an aggressive course of chemotherapy after surgery,while patients in the low-risk group do not appear to bene-fit.12,13 Another example is the biomarker KRAS. A 2009study found that patients with metastatic colorectal cancerwhose tumours had a normal KRAS gene were more likely torespond to a combination of chemotherapy and Erbituxthan those whose tumours had a specific mutated version ofthe KRAS gene.14
The strategic use of tumour biomarker profiling can helpspare patients from the lost time and potential side effectsthat come from trying a medication that is unlikely to beeffective. Further, tumour biomarker profiling can producesignificant savings on a national scale. In the case of KRAStesting, a U.S. pharmacoeconomic study found that upfrontKRAS testing of tumours from patients with colorectal cancerwould cost $13 million annually but would result in a netsavings of $740 million, a savings realized through theavoidance of Erbitux treatment in those patients very unlike-ly to respond.15 Clearly, moving toward large-scale biomark-er testing makes financial sense for large-scale payers; how-ever, it is important to keep in mind that the benefits—topatients and to payers—cannot be realized unless a testingprogram is under strict quality control and produces consis-tently accurate results. These issues cannot be taken forgranted, as made clear by a 2009 study from the Universityof California, San Francisco that found approximately 20 percent of HER2 tests conducted today are inaccurate.16 TheCommission of Inquiry on Hormone Receptor Testing inNewfoundland, released in 2009, revealed that 383 breastcancer patients of 1,013 tested between 1997 and 2005 hadinaccurate ER/PR results, which in many cases led to theomission of appropriate hormone therapy.17 This stronglyhighlights the need for strict quality control when nationalprograms for biomarker testing are undertaken.
From Targeted Therapeutics to Personalized MedicineWith all of the advances in molecular medicine, it is frustrat-ing to realize that the goal of personalized treatment has stillnot been attained. The average five-year survival rate for can-cer patients in Canada is still just 62 per cent, and about aquarter of cancer types have five-year survival rates under 25per cent.18 This is the reality even though there are morethan a hundred approved cancer drugs in Canada, including24 molecularly targeted agents. Is the problem that the avail-able drugs are not effective? Certainly continued develop-ment of efficacious drugs is needed. Tumours can developresistance to both standard chemotherapy and targetedagents over time. Yet, a major part of the problem in mostcountries is the unacceptably long lag time between theattainment of knowledge by the research community andthe integration of that knowledge into the standard of care.On average, it takes 17 years for new treatment strategies tobecome part of published guidelines.19

The reasons for the lag between the research and bedsideare complex. Cancer treatment is one of the fastest movingfields in medicine. The explosion of research is overwhelm-ing, and it is challenging even for those who craft the guide-lines to keep current. In addition, key opinion leaders do notalways agree about whether or not a new medication or treat-ment strategy has enough data to support its incorporationinto the guidelines. Once new research appears in the guide-lines, there is a further lag as clinicians incorporate theupdated guidelines into practice. A recently published U.S.National Cancer Institute (NCI) Office of Education andSpecial Initiatives survey of 2,864 oncology practitioners inall types of practice settings found that only 33 per cent indi-cated that they had adequate time to access best-practiceinformation.20 Regardless of the reasons, the current modelfor cancer care remains, in some ways, stuck in the past.
For example, the Tumor-Node-Metastasis (TNM) stagingsystem was devised in the 1940s.21 Under this system, alltumours of the same stage and organ of origin are given asimilar prognosis and are approached with a similar treat-ment strategy. Yet, one tumour may respond well to a partic-ular chemotherapy or targeted agent, while another “simi-lar” tumour will continue to grow and progress. Biomarkertools, where they have been developed, may offer a betterassessment of risk than does the TNM system. For example,many patients in the clinical trials of multi-gene assays werelabeled as high risk by the TNM system but low risk by theassay. These patients would have almost certainly receivedchemotherapy that followed the standard of care, yet themulti-gene assay revealed that they did not require such anaggressive course of treatment.22 Although these data havebeen published for four years, multi-gene assays are still notroutinely used in the management of breast cancer inCanada, and their cost is rarely covered by the provincialhealth care plans. In practice, this means that Canadianbreast cancer patients will receive unnecessary chemothera-py.23,24 Clearly, something must be done about the lagbetween the advancement of knowledge and its implemen-tation in the clinic.
As the pace of research and development in oncologytreatment continues to accelerate, bridging strategies willbecome increasingly necessary to make personalized cancertreatment a reality. Busy clinicians will need to find time-sparing and cost-effective ways to bring individualized treat-ment strategies to their patients. Patients will want a way toplay an active role in their disease management in a mannerthat goes beyond internet searching and recommendationsfrom friends or family. Payers and drug developers have astake in ensuring that health-care dollars are spent on thera-pies that have the highest likelihood of producing a diseaseresponse. These goals are attainable—if knowledge fromresearch can be quickly moved into the mainstream cancercommunity. The age of personalized medicine is, indeed,upon us, and it is up to us to seize that opportunity.
Jennifer Levin Carter, MD, MPH, is the Founder, President andChief Medical Officer of N-of-One Therapeutics, Inc. (www.n-of-one.com). Dr. Carter is a physician, entrepreneur, and formerhealthcare analyst in bio- and medical technology. She graduat-ed with distinction in Molecular Biophysics and Biochemistryfrom Yale University. She received an MD from Harvard Medical
School and a Masters of Public Health from The Harvard Schoolof Public Health.
Jillian Lokere is a freelance science and medical writer.
© 2011 N-of-One Therapeutics, Inc. Used with the kind permissionof the authors.
References1 Jensen EV, Block GE, Smith, S, et al. Estrogen receptors and breast can-
cer response to adrenalectomy. J. Natl. Cancer Inst. Monogr. 1971:34:55–70.
2 Harper, M. J., and Walpole, A. L. Contrasting endocrine activities of cisand trans isomers in a series of substituted triphenylethylenes. Nature(Lond.). 1966;212: 87.
3 Bedford, G., and Richardson, D. N. Preparation and identification of cisand trans isomers of a substituted triphenylethylene. Nature (Lond.).1966;212: 733–4.
4 Ward, HW. Anti-oestrogen therapy for breast cancer: a trial oftamoxifenat two dose levels. Br. Med. J. 1973; 1: 13–14.
5 Marx JL. Cancer gene research wins medicine Nobel. Science.1989;246:326-7.
6 Slamon DJ, Clark GM, Wong SG, et al. Human breast cancer: correlationof relapse and survival with amplification of the HER-2/neu oncogene.Science. 1987;235:177-82.
7 Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus amonoclonal antibody against HER2 for metastatic breast cancer thatoverexpresses HER2. N Engl J Med. 2001; 344:783-792.
8 Rowley D. A new consistent chromosomal abnormality in chronic myel-ogenous leukaemia identified by quinacrine fluorescence and Giemsastaining. Nature. 1973;243:290-293.
9 Druker BJ, Talpaz M, Resta DJ, et al. Efficacy and safety of a specificinhibitor of the BCR-ABL tyrosine kinase in chronic myeloid leukemia. NEngl J Med. 2001;344:1031-7.
10 Palazzo A, Iacovelli R, Cortesi E. Past, present and future of targetedtherapy in solid tumours. Curr Cancer Drug Targets. 2010;10:433-61.
11 Herceptin (trastuzumab) prescribing information. Genentech, Inc.Revised October 2010.
12 Oakman C, Santarpia L, Di Leo A. Breast cancer assessment tools andoptimizing adjuvant therapy. Nat Rev Clin Oncol. 2010 Oct 26 Epub.
13 Ross JS, Torres-Mora J, Wagle N, et al. Biomarker-based prediction ofresponse to therapy for colorectal cancer: current perspective. Am J ClinPathol. 2010;134:478-90.
14 Bokemeyer C, Bondarenko I, Makhson A, et al. Fluorouracil, leucovorin,and oxaliplatin with and without cetuximab in the first-line treatment ofmetastatic colorectal cancer. J Clin Oncol. 2009;27:663-71.
15 Shankaran V, Bentrem DJ, Mulcahy MF, et al. Economic implications ofKras testing in metastatic colorectal cancer (mCRC). ASCO 2009Gastrointestinal Cancers Symposium. Abstract 298.
16 Phillips KA, Marshall DA, Haas JS, et al. Clinical practice patterns and costeffectiveness of human epidermal growth receptor 2 testing strategiesin breast cancer patients. Cancer. 2009;115:5166-74.
17 The Government of Newfoundland and Labrador. Commission ofInquiry on Hormone Receptor Testing. 2009. Available athttp://www.releases.gov.nl.ca/releases/2009/health/Volume1_Investigation_and_Findings.pdf
18 Ellison L and Wilkins K. An update on cancer survival. Component ofStatistics Canada Catalogue no. 82-003-X. September 2010. Availableat http://www.statcan.gc.ca/pub/82-003-x/2010003/article/11334-eng.pdf.
19 Balas EA, Boren SA (2000) Managing clinical knowledge for health careimprovement. In: Van Bemmel JH, McCray AT (eds) Yearbook of medicalinformatics 2000: patient-centered systems. Schattauer, Stuttgart, pp65–70.
20 Ousley AL, Swarz JA, Milliken EL, Ellis S. Cancer education and effectivedissemination: information access is not enough. J Cancer Educ.2010;25:196-205.
21 Denoix PF. Enquete permanent dans les centres anticancereux. Bull InstNat Hyg 1946;1:70
22 Paik S, Tang G, Shak S, et al. Gene expression and benefit of chemother-apy in women with node-negative, estrogen receptor-positive breastcancer. J Clin Oncol. 2006;24:3726-34.
23 Ragaz J. The 21-Gene Assay: Impact on breast cancer in Canada. ReportCard on Cancer in Canada. 2009-2010;12:10-13.
24 Ragaz J. The 21-Gene Assay, Part 2, Canada’s Uneven Response. ReportCard on Cancer in Canada. 2010-2011;13;41–43
40 REPORT CARD ON CANCER IN CANADA, 2010–11
THE ORGANIZATION OF CANCER CARE

REPORT CARD ON CANCER IN CANADA, 2010–11 41
By JOSEPH RAGAZ, MD, FRCPC
In 2010, the first part of this series1 reported that the 21-geneassay recurrence score (RS), when used at the point of diag-nosis of breast cancer, can predict the effectiveness of adju-vant chemotherapy in reducing cancer recurrence moreaccurately than any known biomarker.
Adjuvant chemotherapy is one of the key factors respon-sible for decreasing breast cancer mortality in the westernworld. The Oxford-based Early Breast Cancer Trialists’Collaborative Group conducted a review of all randomizedtrials over the last 20 years, documenting the benefit of adju-vant chemotherapy in reducing recurrences and mortality by25-30 per cent2 according to subsets.
However, the benefits of adjuvant therapy are not guaran-teed. The molecular classification of the tumour specimenbased on the 21-gene assay RS is a vital tool to distinguishthose who will have considerable benefits from those whomay derive less, or no benefit, from standard chemotherapy.
On a scale of one to100, a score less than 19 predicts lit-tle or no benefit, while a score of 30 or more indicates a veryhigh impact of adjuvant chemotherapy, reducing recur-rences by 50–70 per cent. Scores between 19–30 are less clear-ly predictive, but answers are expected shortly from therecently completed TAILORx trial, which compared theimpact of chemotherapy or no chemotherapy in this inter-mediate group.
The RS score creates an opportunity for physicians tospare cancer patients from any unnecessary toxicity and sideeffects of chemotherapy. Anyone, especially cancer patients,would wonder why that step is not automatically in place,pursued with enthusiasm. Perhaps the learning curve inCanada is not what it should be.
Since 2007, the American Society of Clinical Oncology(ASCO) and the U.S. National Comprehensive CancerNetwork (NCCN) guidelines have recommended that the 21-gene assay (Oncotype Dx) be part of the routine manage-ment for early stage breast cancer patients with hormonereceptor positive tumours.
However, until 2009, this test was virtually unavailable inCanada outside clinical trials. If the test were more widelyused in Canada it could facilitate the avoidance of thousandsof rounds of unnecessary, toxic chemotherapy in the sizablepatient subset with low RS.
Since our report last year, two Canadian studies haveshown the rising value of molecular classification with the21-gene assay,3,4 with one of them concluding, “The 21-geneassay appears cost-effective from a Canadian health care per-spective.”4
With data mounting on the benefit of using the 21-geneassay, Canadian provinces have responded as follows:• British Columbia began a registration study for the 21-
gene assay in 2010. However, it is restricted to nodenegative cases and until recently was active only in theVancouver clinic.
• Ontario started funding the21-gene assay more consis-tently, using an OHIP provi-sion for out-of-country healthservices, which requires anapplication by the oncologistand prior approval from thehealth ministry.
• In the last few months,Quebec’s RAMQ has startedfunding an increasing num-ber of 21-gene assay tests.
Table 1 shows the trend ofincreased use of the 21-geneassay in Canada since 2007. A significant increase occurredin the number of tests ordered between 2009 and 2010, from464 to 962. Also, more recently, the medical advisory secre-tariat to Ontario’s Ministry of Health and Long-Term Caredrafted an in-depth analysis and recommendations regard-ing the 21-gene assay test, basically approving the use of thetest for newly diagnosed node negative breast cancer patientswith estrogen receptor (ER) positive tumours.5
While these are positive trends, there is still massiveunder-utilization of this predictive tool in Canada. Researchdata show that of all ER positive tumours more than half willhave low RS, whether node negative or node positive. Thus,the test could be used for all node negative and the low risknode positive cases if they are ER positive (70 per cent of alldiagnosed) and candidates for chemotherapy (65 per cent ofthose). Thus, out of the 22,000+ newly diagnosed with newbreast cancer each year in Canada, at least 10,000 women
PART 2
The 21-Gene AssayCANADA’S UNEVEN RESPONSE
TABLE 1NUMBER OF 21-GENE ASSAYS PER YEAR IN CANADA 2007–2010
2007 150
2008 348
2009 464
2010 962
Source: Feb 2011 updates, Genomic Health Database
Year Breast cancer patients tested
THE ORGANIZATION OF CANCER CARETHE ORGANIZATION OF CANCER CARE

TABLE 2RECURRENCE SCORES OF CANADIAN PATIENTS 2007–2010
Low 1,029 55.03% 29 55.77% 1,058 55.05%(< 19)Intermediate 654 34.97% 18 34.62% 672 34.96%(19–30)High 187 10.00% 5 9.62% 192 9.99%(>30)
Totals 1,870 100% 52 100% 1,922 100%
Source: Feb 2011 updates, Genomic Health Database
Score Numberof
Patients
Per Cent
Numberof
Patients
Per Cent
Numberof
Patients
Per Cent
Node Negative Cases Node Positive Cases Total Cases
TABLE 3ESTIMATED COST-BENEFIT OF THE 21-GENERECURRENCE SCOREBased on one year, 10,000 newly diagnosed ER positive cases (i.e., those who are candidates for the 21 gene assay) and variable rates of avoiding chemotherapy.$ in millions
Cost of chemotherapy $150 $112.5 $97.5 $75.0
Cost of 21-gene assay $0 $40 $40 $40
Health system cost $150 $152.5 $137.5 $115.0
Costs Added (+) or Saved (-) /10,000 cases $0 + $2.5 – $12.50 – $35.0
These estimates are based on $4,000 for the test and a conservative estimate of $15,000 per course of adjuvant chemotherapy, potentiallyavoided in 2,500, 3,500 or 5,000 patients.
Cost Factors 0 (no test) 25% 35% 50%
Rate of Chemotherapy Avoidance
42 REPORT CARD ON CANCER IN CANADA, 2010–11
THE ORGANIZATION OF CANCER CARE
would be eligible for the 21 gene assay test. Instead, in2010, only 962 were done, representing approximately10 per cent of eligible women.
The significance of not doing the molecular test atdiagnosis on those who are eligible is considerable. Ofthe 10,000 cases eligible for the test each year, morethan half (5,000/year) would be in the low RS category(Table 2).
Based on the available statistics from the most recentresearch,3,4 chemotherapy in these patients will haveonly minimal or no effect on the recurrence rates.However, without the test, all 5,000 would be consid-ered candidates for chemotherapy under present guide-lines. If given the choice, this course of action shouldlikely be avoided as the well known toxicity ofchemotherapy can only be justified when the treatmentbenefits are documented more clearly.
Added to this are the cost benefits of adjuvant policybased on molecule classification, rather than the presentempirical approach, using the 21 gene test to identify5,000 women, of whom most, if not all, could avoidchemotherapy. The estimates of dollars spent versus dol-lars saved are based on the present practice, which stillrepresents less than optimum use of the 21-gene assay.At one end of the spectrum, perhaps the ideal way, is thepossibility that none of the low RS cases should havechemotherapy as very few, or none will benefit.
As the low RS occurred in more than 50 per cent ofCanadians already tested, this represents a 50 per centavoidance of chemotherapy costs (see Table 3).However, many, if not most oncologists confronted witha low RS would still prescribe the chemotherapy forwhat is considered in the conventional staging a highrisk situation, such as large tumour, vessel invasion,nodes involved, etc. This would diminish the rate ofavoidance to less than 50 per cent of all tested, e.g., 35per cent or even 25 per cent.
If 50 per cent avoidance were achieved, representinga full compliance in withholding chemotherapy to alllow RS cases, a substantial societal saving becomes pos-sible, estimated to be $35 million saved for every 10,000tested. A smaller rate of avoidance of chemotherapy willlead to smaller savings, or even an extra cost.
These estimates are based on $4,000. for the test anda conservative estimate of $15,000. per course of adju-vant chemotherapy, potentially avoided in 2,500, 3,500or 5,000 patients.
DISCUSSIONThe data indicate that for node negative cases and like-ly also for the low risk node positive cases, the 21-geneassay could be used for all breast cancer patients withwell differentiated, ER positive tumours, whenever adju-vant chemotherapy is potentially indicated, regardlessof tumour size or vessel invasion. Once a low RS is doc-

REPORT CARD ON CANCER IN CANADA, 2010–11 43
umented, chemotherapy should not be given as incurringtoxicity for minimum benefits is clearly unacceptable. If theRS is high, chemotherapy ought to be considered even if notoriginally planned; for intermediate RS cases, individualizeddecisions need to be made. This approach should become aguideline policy for treatment across Canada.
Node positive cases. Preparations are underway in theU.S. for a randomized trial of chemotherapy vs. nochemotherapy in node positive breast cancer cases where RSis low. Canadian participation is expected. This study will berequired due to the present international policy of usingchemotherapy in all node positive cases. This is still the casedespite the study of Albain et.al.6 showing little benefit fromchemotherapy in low RS cases among node positive breastcancer patients, regardless of the number of nodes involved,exactly as was the case for node negative cases.7 The chanceof chemotherapy having a meaningful effect among low RScases in the new study of node positive cases is understand-ably extremely low, posing a dilemma for prescribingchemotherapy to this cohort of patients, at least to some ofthe lower risk subsets (e.g., less than four nodes, those withfocal nodal involvement only, etc.).
In addition, a related challenge to the present guidelinesemerges for patients not participating in the above study: inall situations with low RS, chemotherapy may have tobecome the “experimental” option.
In summary, several key questions need consideration.• Is it feasible to obtain, within a reasonable time, much
higher levels of evidence in order to bring molecular clas-sification with the 21-gene assay into guidelines?Reviewing the data, this approach seems unlikely, at leastnot for node negative and low risk node positive cases.
• Which is worse, over-treating large numbers of breast can-cer patients with chemotherapy that we already know willbe pointless yet toxic and immunosuppressive, or nottreating a few who could receive a slight benefit?
• Can the medical establishment be more pragmatic aboutaccepting the present data into practice guidelines moreswiftly and yet continue research into unanswered ques-tions?
• Should patients be informed about these issues and havetheir own input into pursuing the 21-gene assay and act-ing on the RS score, i.e., declining or acceptingchemotherapy?
ConclusionAt this point the 21-gene assay is the only validated testbased on molecular classification to guide decisions for oragainst chemotherapy. Without it, the status quo of empiri-cal approaches towards chemotherapy selection leads toconsiderable over-treatment with chemotherapy in a largenumber of low RS cases routinely planned for adjuvantchemotherapy, or in some cases under-treatment in caseswith high RS not planned for adjuvant chemotherapy.
Unquestionably, more research is required to refine themolecular classifications for patients with cancer, especiallythe cost and comparability with surrogate markers. However,the data reviewed in this report document very low expecta-tions of a meaningful benefit from adjuvant chemotherapyfor breast cancer patients with low RS scores. If the 21-geneassay became a requirement in Canada, as part of routinepolicy for all eligible patients, we would see less cost, lesstoxicity and far less suffering on the part of most patients—and no less effective treatment. We have a choice to make.
Joseph Ragaz, MD, FRCPC, is a Director of the CACC and asenior Medical Oncologist, Breast Cancer Researcher, ClinicalProfessor, Faculty of Medicine and School of PopulationHealth, University of British Columbia, Vancouver, B.C.
References1 Ragaz J. The 21-Gene Assay: Impact on breast cancer in Canada: Ethically
and Economically When Do We Act? Report Card on Cancer in Canada2009-2010;10-13-.
2 Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects ofChemotherapy and Hormonal Therapy For Early Breast Cancer OnRecurrence and 15-Year Survival: An Overview of the Randomized Trials.Lancet 2005; 365:1687–1717.
3 Tsoi DT, Inoue M, Kelly CM, Verma S, Pritchard KI: Cost-EffectivenessAnalysis of Recurrence Score-Guided Treatment Using a 21-Gene Assay inEarly Breast Cancer. The Oncologist 2010;15:457-65.
4 Kelly CM, Warner E, Tsoi DT, Verma S, Pritchard KI: Review of the ClinicalStudies Using the 21-Gene Assay. The Oncologist 2010;15:447-56.
5 Ontario Health Technology Assessment Series 2010; Vol. 10, No. TBA6 Albain, K KS, Barlow, WE, Shak S, Hortobagyi GN, et.al. Prognostic and
Predictive Value of the 21-Gene Recurrence Score Assay inPostmenopausal Women With Node-Positive, Estrogen-Receptor-PositiveBreast Cancer On Chemotherapy: A Retrospective Analysis of aRandomized Trial, for The Breast Cancer Intergroup of North America.Lancet Oncology December 10, 2009; DOI:10.1016/S1470.
7 Paik S, Tang G, Shak S, et al. Gene Expression and Benefit ofChemotherapy In Women With Node-Negative, Estrogen Receptor-Positive Breast Cancer. J Clin Oncol. 2006;24: 3726–3734.
There is still massiveunder-utilization ofthis predictive tool in Canada.

by JAMES D. GOWING, BA, MB, BS, FRCPC
PATIENT-CENTERED CARE AND PERSONALIZED PATIENT TREATMENT Over the last decade the buzz words used by many medical institutions has been “Patient-
Centered Care”, but what does this mean? The Royal College of Physicians and Surgeons of
Canada has debated the meaning of professionalism and their conclusions include altruism as
the hallmark of professionalism and appear to coincide with Francis Peabody’s statement in
1927 that “The secret of the care of the patient is in caring for the patient”.
Today’s medical institutions are using this term when in effect the care of hospitalized
patients is based more on process and funding than on caring for the particular needs of the
individual patient with their ethnic, cultural, religious and gender differences. We need to
change our approach to patients based on caring rather than process.
For many years we treated all cancer patients based on clinical trials that included at best
three per cent of the target population and applied it to all. Many of our guidelines are still based
on this concept. However, clinicians and patients knew that not all breast cancers behaved
the same and with increased research into the differences and our understanding of DNA
mutations and intracellular pathways we are now more able to tailor treatments that are
targeted to the patient’s cancer. Our knowledge of the cellular changes of all cancers continues
to expand and with new tumour markers that truly reflect individual tumours, future treatments
will be truly reflective of the needs of individual patients with their individual cancers. Only then
will we be delivering personalized patient treatments.
CACC believes in advocacy and is committed to speaking openly about cancer issues,to highlight the concerns of patients and families, and to press governments for amore effective response to the enormity of the cancer problem in Canada. We foregocharitable status to retain this freedom. Through the generosity of sponsors anddonors, we use unrestricted grants to collect information, consult with cancer expertsand families, and lobby governments for improvements. Sponsorship guidelines canbe found on our web site.
If you are one of the millions of Canadians concerned about the state of cancer care,tell your federal MP and your provincial MPP/MLA. Make sure the people you electedto govern know that cancer is a priority to you and should be for them.
CANCER ADVOCACY COALITION OF CANADA60 St. Clair Ave. East, Suite 204, Toronto, Ontario M4T 1N5
Tel: (416) 538-4874 Toll Free: [email protected] www.canceradvocacy.ca
´Noteworthy
44 REPORT CARD ON CANCER IN CANADA, 2010–11


















