Canadian Institute Conference - Arvind Mani's Presentation - Final - April 1 2015
48
pdci.ca ©2015 PDCI Market Access Global Trends: Drug Pricing, Reimbursement and Market Access Arvind Mani Director, Market Access and Policy Research E-mail: [email protected] 1 ©2015 PDCI Market Access
-
Upload
arvind-mani -
Category
Documents
-
view
280 -
download
3
Transcript of Canadian Institute Conference - Arvind Mani's Presentation - Final - April 1 2015
pdci.ca
©2015 PDCI Market Access
Global Trends: Drug Pricing, Reimbursement and Market Access
Arvind ManiDirector, Market Access and Policy Research
E-mail: [email protected]
1©2015 PDCI Market Access
2
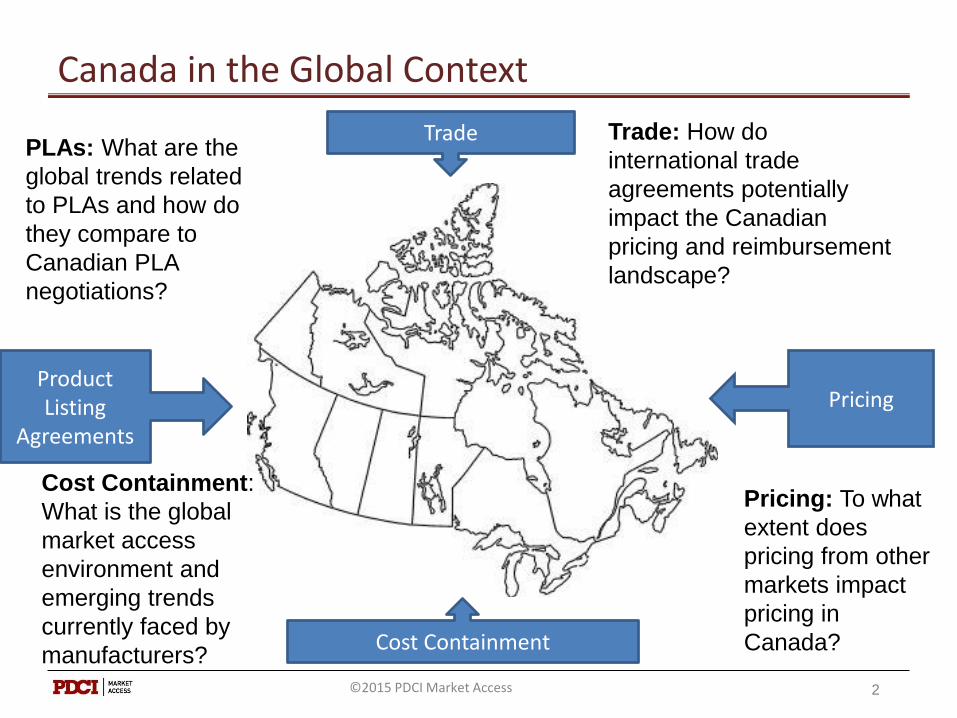
Canada in the Global Context
Product Listing
Agreements
Pricing
Cost Containment
Trade Trade: How do
international trade
agreements potentially
impact the Canadian
pricing and reimbursement
landscape?
Pricing: To what
extent does
pricing from other
markets impact
pricing in
Canada?
Cost Containment:
What is the global
market access
environment and
emerging trends
currently faced by
manufacturers?
PLAs: What are the
global trends related
to PLAs and how do
they compare to
Canadian PLA
negotiations?
©2015 PDCI Market Access
Context
3©2015 PDCI Market Access
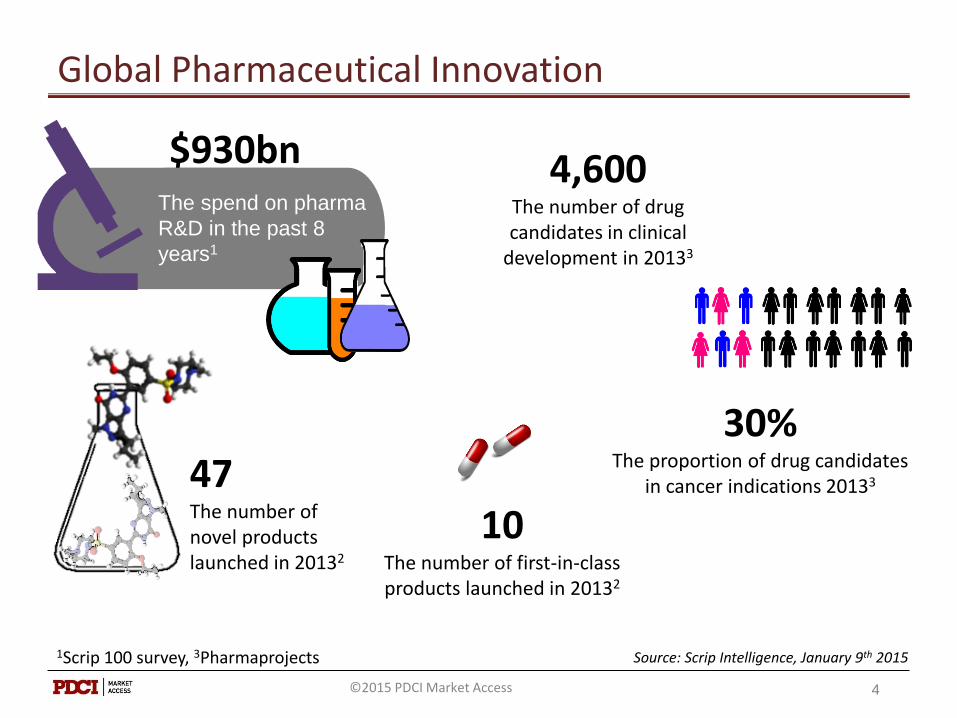
4,600The number of drug candidates in clinical
development in 20133
$930bnThe spend on pharma
R&D in the past 8
years1
30%The proportion of drug candidates
in cancer indications 20133
1Scrip 100 survey, 3Pharmaprojects Source: Scrip Intelligence, January 9th 2015
4
47The number of novel products launched in 20132
Global Pharmaceutical Innovation
10The number of first-in-class products launched in 20132
©2015 PDCI Market Access
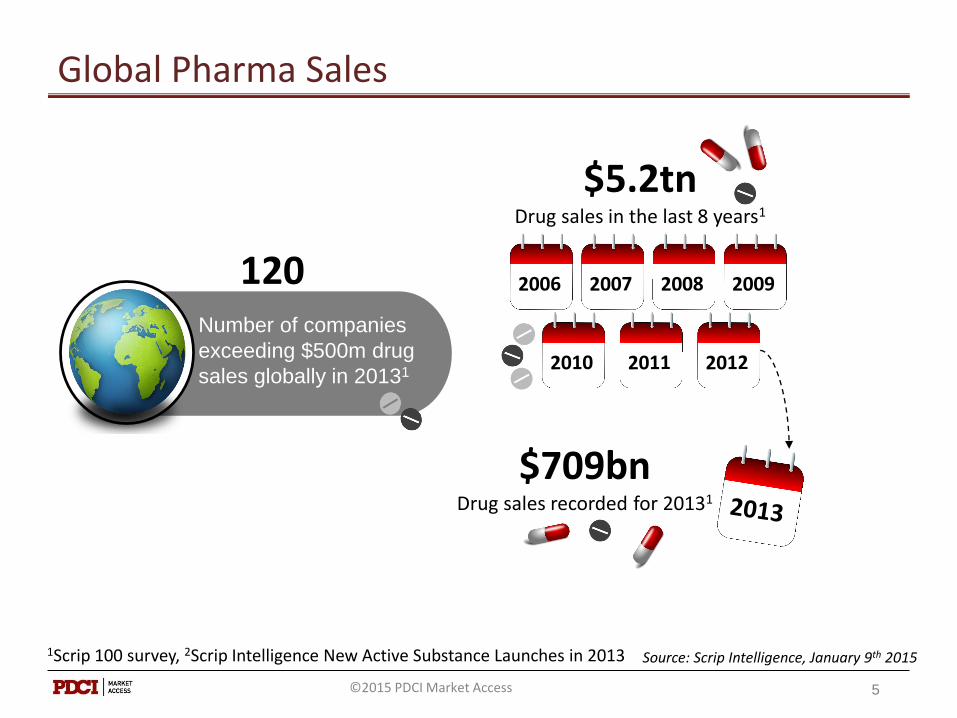
120Number of companies
exceeding $500m drug
sales globally in 20131
$5.2tnDrug sales in the last 8 years1
$709bnDrug sales recorded for 20131
1Scrip 100 survey, 2Scrip Intelligence New Active Substance Launches in 2013 Source: Scrip Intelligence, January 9th 2015
5
Global Pharma Sales
©2015 PDCI Market Access
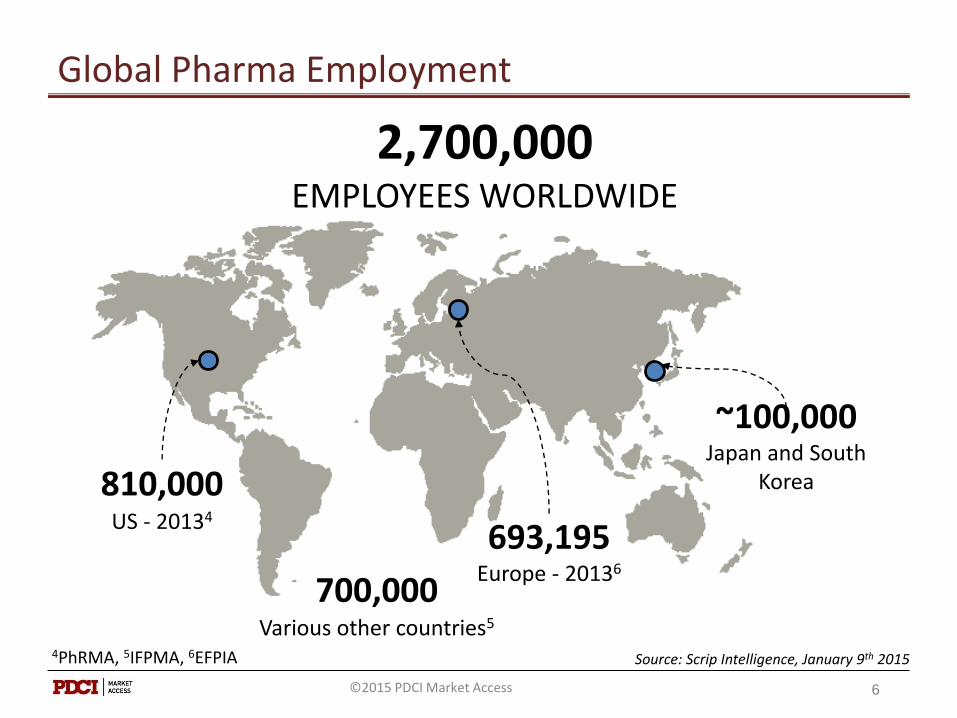
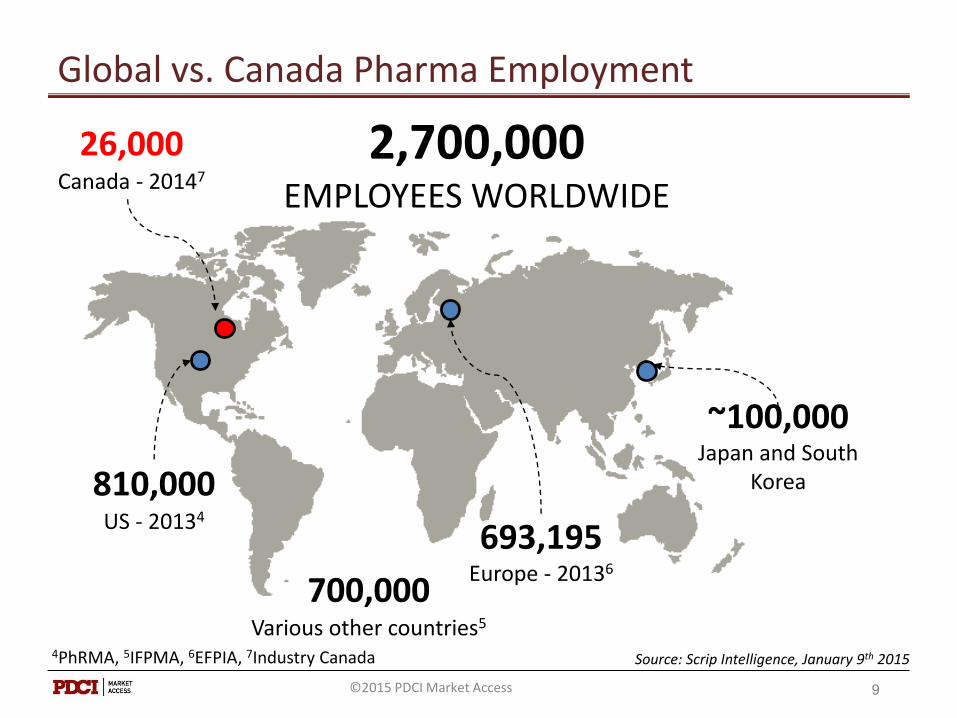
2,700,000EMPLOYEES WORLDWIDE
810,000US - 20134
700,000Various other countries5
693,195Europe - 20136
~100,000Japan and South
Korea
4PhRMA, 5IFPMA, 6EFPIA Source: Scrip Intelligence, January 9th 2015
Global Pharma Employment
6©2015 PDCI Market Access
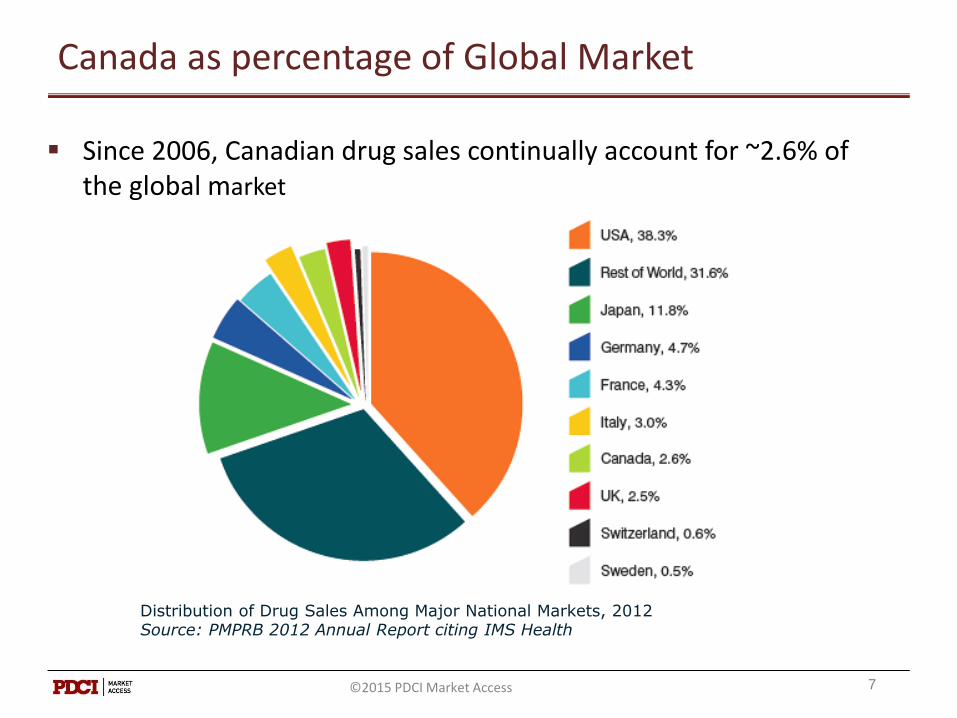
Canada as percentage of Global Market
Since 2006, Canadian drug sales continually account for ~2.6% of the global market
7
Distribution of Drug Sales Among Major National Markets, 2012Source: PMPRB 2012 Annual Report citing IMS Health
©2015 PDCI Market Access
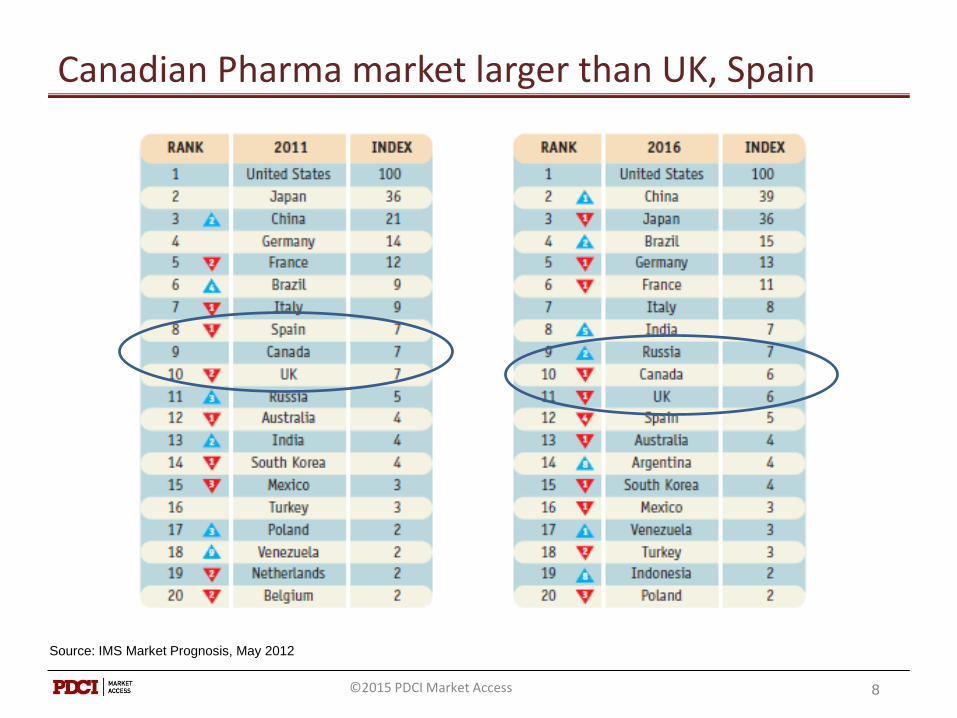
Canadian Pharma market larger than UK, Spain
8
Source: IMS Market Prognosis, May 2012
©2015 PDCI Market Access
2,700,000EMPLOYEES WORLDWIDE
810,000US - 20134
700,000Various other countries5
693,195Europe - 20136
~100,000Japan and South
Korea
4PhRMA, 5IFPMA, 6EFPIA, 7Industry Canada Source: Scrip Intelligence, January 9th 2015
Global vs. Canada Pharma Employment
9
26,000Canada - 20147
©2015 PDCI Market Access
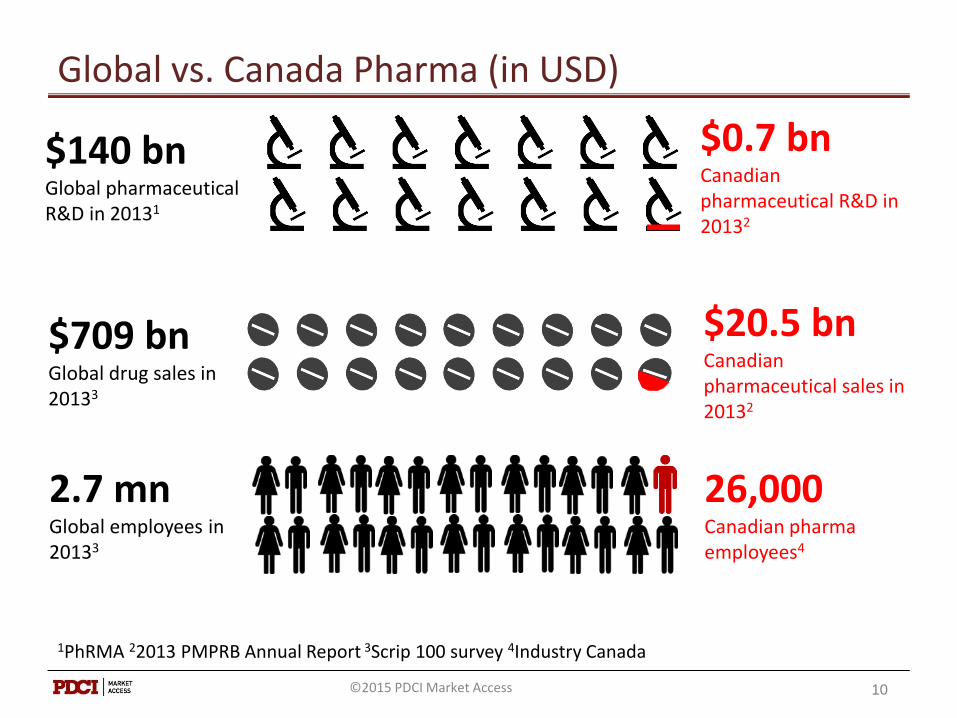
Global vs. Canada Pharma (in USD)
1PhRMA 22013 PMPRB Annual Report 3Scrip 100 survey 4Industry Canada
10
$140 bnGlobal pharmaceutical R&D in 20131
$0.7 bnCanadian pharmaceutical R&D in 20132
$709 bnGlobal drug sales in 20133
$20.5 bnCanadian pharmaceutical sales in 20132
26,000Canadian pharma employees4
2.7 mnGlobal employees in 20133
©2015 PDCI Market Access

Trade
11
Product Listing
Agreements
Pricing
Cost Containment
Trade
©2015 PDCI Market Access

Canada - EU Trade Agreement - CETA
Comprehensive Economic and Trade Agreement (CETA):Pharma IP Provisions: (Details still to be announced)
• Patent Term Restoration
Extended Data Protection
• Innovator Right of Appeal
12©2015 PDCI Market Access
CETA and Patent Act
13
Innovative Pharmaceutical
lndustry
Generic Pharmaceutical
lndustry
Private Drug Plans & Insurers
PMPRB and Staff
Patient Advocacy
Organizations
Health Canada
Public Drug Plans Labour
organizations
©2015 PDCI Market Access
Potential Amendments & Implications
1. PMPRB Jurisdiction & Definitions
2. Excessive Price Factors
3. Research & Development
4. Resolution, Hearings and Arbitration
5. Practical Amendments
6. Reference Countries
14©2015 PDCI Market Access
Pricing
15
Product Listing
Agreements
Pricing
Cost Containment
Trade
©2015 PDCI Market Access
Factors in setting pharmaceutical prices
Domestic Factors
• Return on investment
• Competition / Market forces
• Prices of alternatives
• Price regulation / HTA / reimbursement policies
International /Global Factors
• External price referencing
• Currency fluctuations
• Health Reform
16©2015 PDCI Market Access
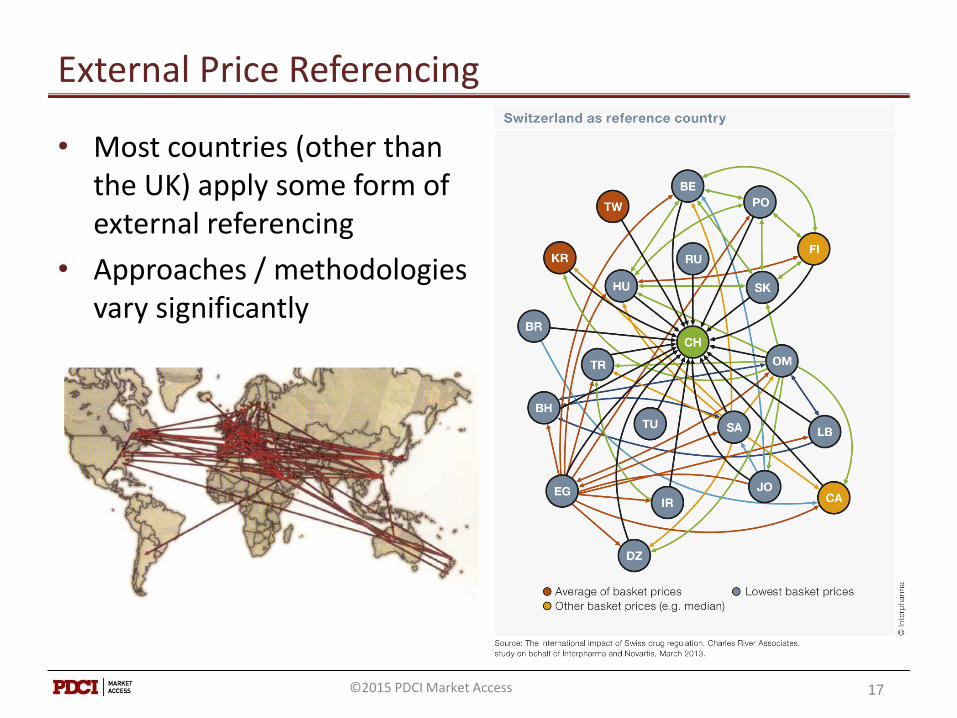
External Price Referencing
• Most countries (other than the UK) apply some form of external referencing
• Approaches / methodologies vary significantly
17©2015 PDCI Market Access
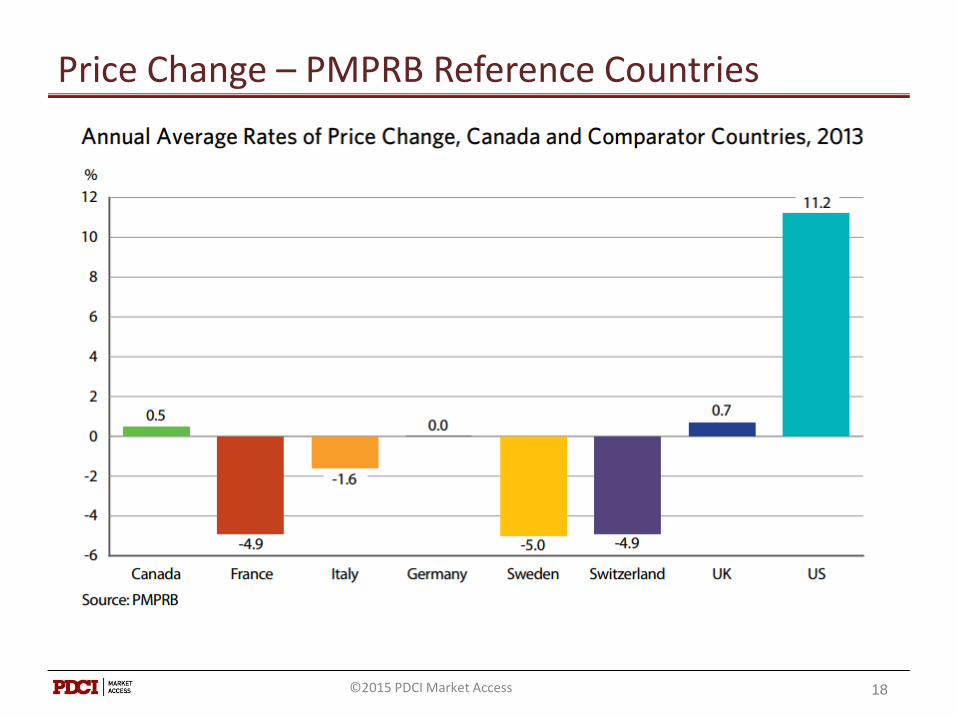
Price Change – PMPRB Reference Countries
18©2015 PDCI Market Access
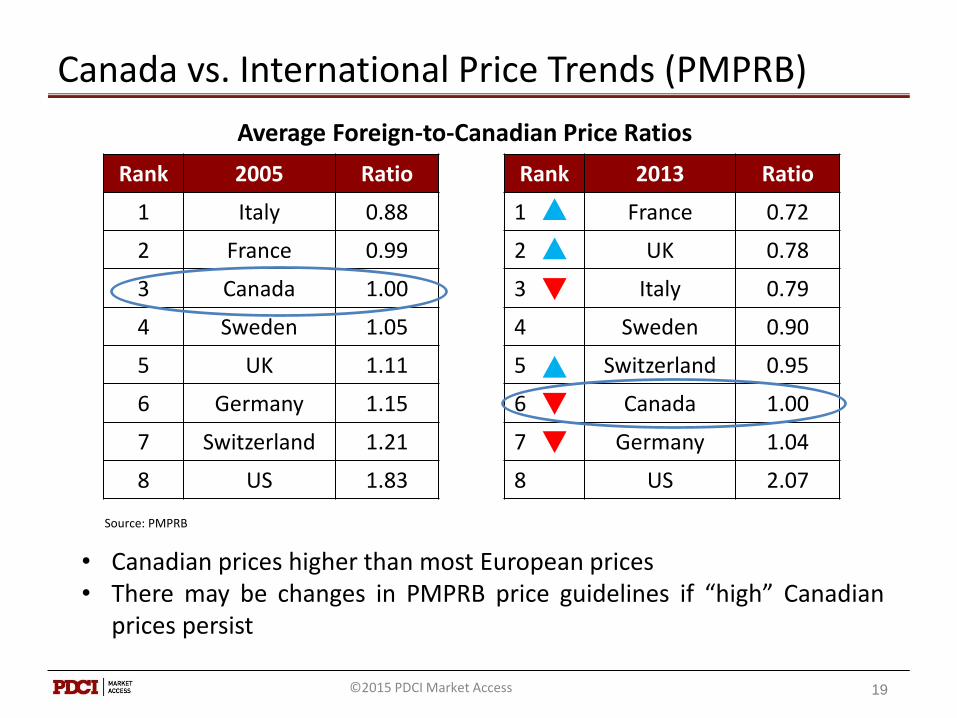
Canada vs. International Price Trends (PMPRB)
Rank 2005 Ratio
1 Italy 0.88
2 France 0.99
3 Canada 1.00
4 Sweden 1.05
5 UK 1.11
6 Germany 1.15
7 Switzerland 1.21
8 US 1.83
19
Rank 2013 Ratio
1 France 0.72
2 UK 0.78
3 Italy 0.79
4 Sweden 0.90
5 Switzerland 0.95
6 Canada 1.00
7 Germany 1.04
8 US 2.07
• Canadian prices higher than most European prices• There may be changes in PMPRB price guidelines if “high” Canadian
prices persist
Average Foreign-to-Canadian Price Ratios
Source: PMPRB
©2015 PDCI Market Access
Pricing & International Price Referencing
• Price increases are possible in the US, and to a limited extent in Canada but rarely in Europe and Japan
• Currency exchange fluctuations are beyond the control of manufacturer
• Price cuts are common in many European markets
• Reimbursement status is reviewed periodically in some markets which can lead to new price negotiations
• New health reform policies (e.g., Germany)
20©2015 PDCI Market Access
Cost Containment
21
Product Listing
Agreements
Pricing
Cost Containment
Trade
©2015 PDCI Market Access
Emerging Developments Related to Cost Containment
1. Delisting of Oncology Treatments
2. Off-Label Prescribing
3. Downgrading Coverage
4. Uptake of Biosimilars
5. Private Payer Exclusivity Arrangements
22©2015 PDCI Market Access
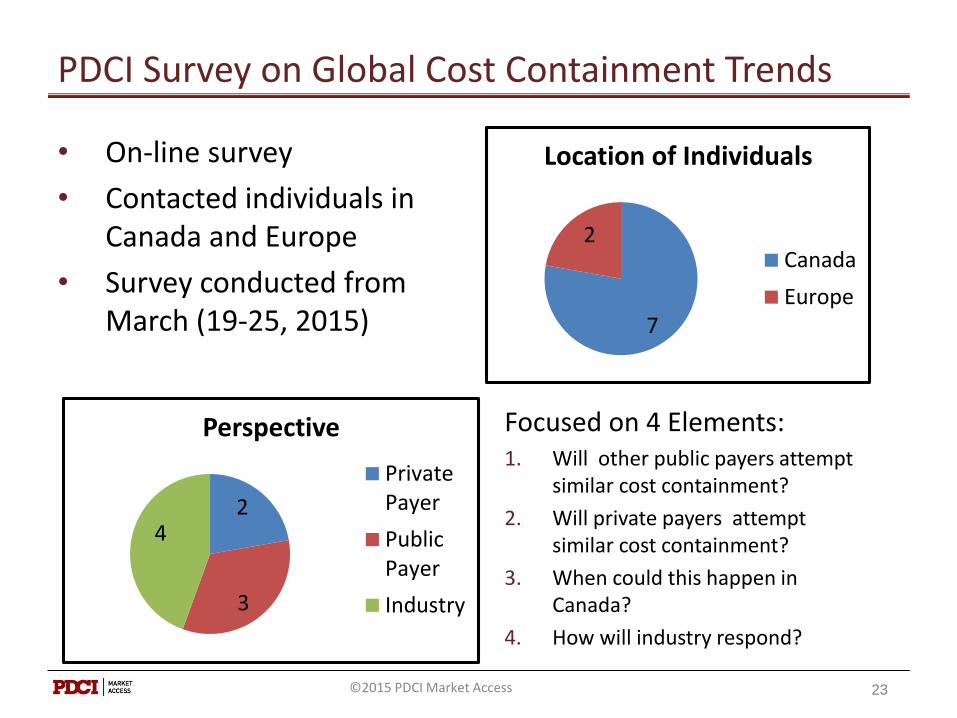
PDCI Survey on Global Cost Containment Trends
7
2
Location of Individuals
Canada
Europe
23
2
3
4
Perspective
PrivatePayer
PublicPayer
Industry
• On-line survey
• Contacted individuals in Canada and Europe
• Survey conducted from March (19-25, 2015)
Focused on 4 Elements:1. Will other public payers attempt
similar cost containment?
2. Will private payers attempt similar cost containment?
3. When could this happen in Canada?
4. How will industry respond?
©2015 PDCI Market Access
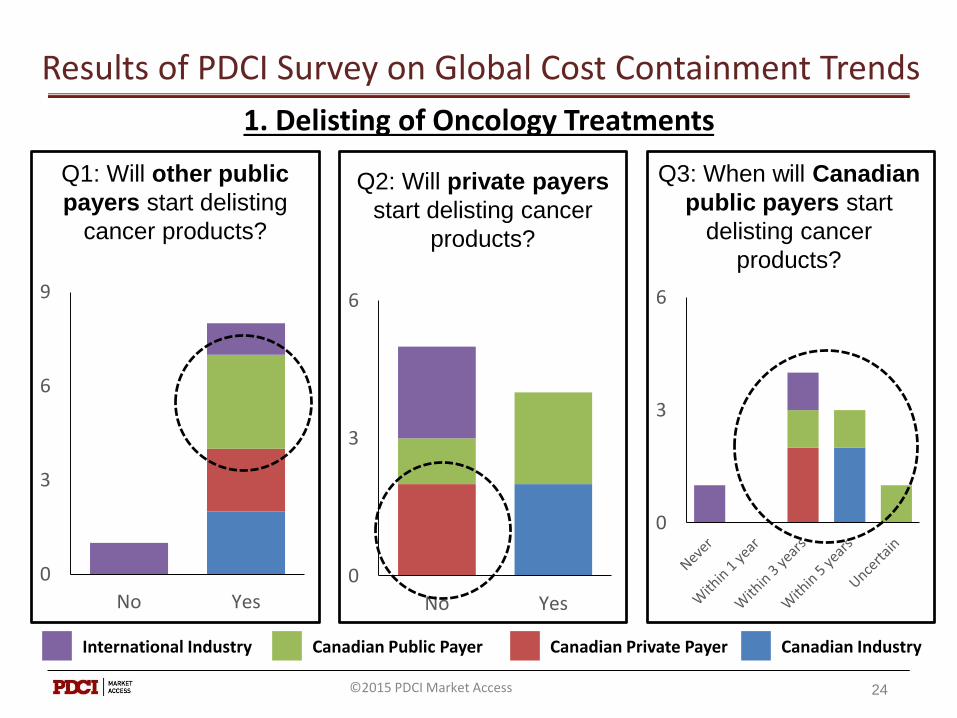
Results of PDCI Survey on Global Cost Containment Trends
24
1. Delisting of Oncology Treatments
International Industry Canadian Public Payer Canadian Private Payer Canadian Industry
Q1: Will other public
payers start delisting
cancer products?
0
3
6
9
No Yes
Q2: Will private payers
start delisting cancer
products?
0
3
6
No Yes
Q3: When will Canadian
public payers start
delisting cancer
products?
0
3
6
©2015 PDCI Market Access
Results of PDCI Survey on Global Cost Containment Trends
25
Public Payer: “It is unlikely a price decrease willovercome a lack of clinical evidence soproposals for PLAs may focus more on evidencegathering and/or risk-sharing.”
Private Payer: “I hope pharma reconsiderstheir pricing models. Assuming quality andefficacy are comparable, then public payersare absolutely right to insist on price reductionor other added value as a condition of listing.Governments are stewards of taxpayer moneyfor which there is no shortage of alternativeuses.”
Q: How do you think industry will respond to the delisting of their products?
©2015 PDCI Market Access
Results of PDCI Survey on Global Cost Containment Trends
26
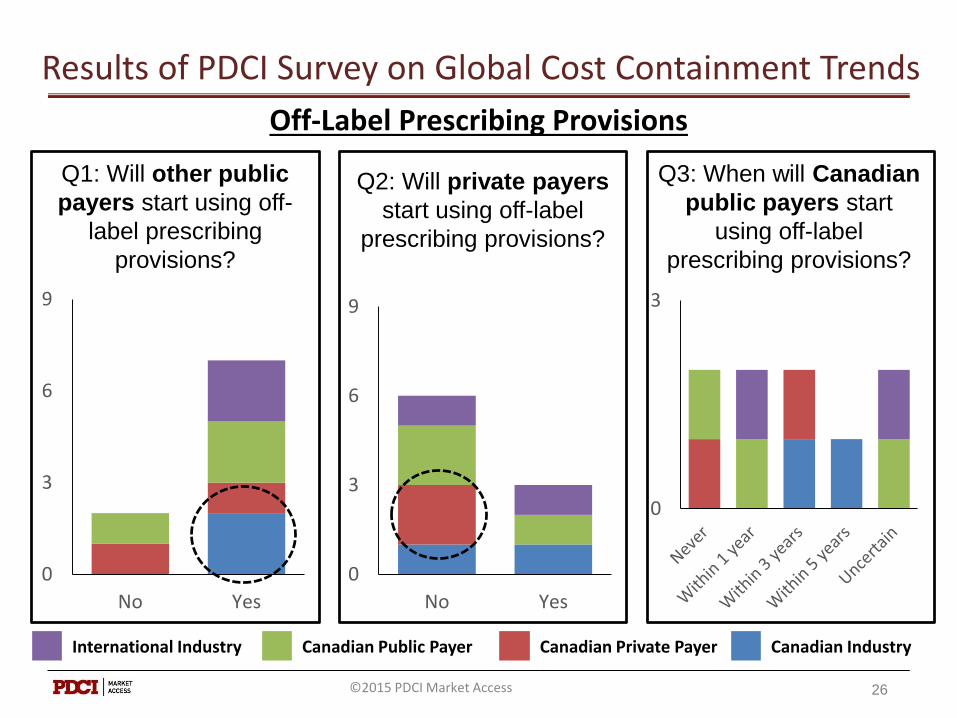
Off-Label Prescribing Provisions
International Industry Canadian Public Payer Canadian Private Payer Canadian Industry
Q1: Will other public
payers start using off-
label prescribing
provisions?
0
3
6
9
No Yes
Q2: Will private payers
start using off-label
prescribing provisions?
0
3
6
9
No Yes
Q3: When will Canadian
public payers start
using off-label
prescribing provisions?
0
3
©2015 PDCI Market Access
Results of PDCI Survey on Global Cost Containment Trends
Q: How do you think industry will respond to the introduction of provisions for off-label prescribing?
27
Public Payer: “They [industry] will notappreciate the increased competitionit [off-label prescribing] creates. In theCanadian market they may respond bylowering confidential public prices tomaintain the private market.”
International Industry: “They [industry] will encourage that evidence based medicine with appropriate labels should be used.”
©2015 PDCI Market Access
Results of PDCI Survey on Global Cost Containment Trends
28
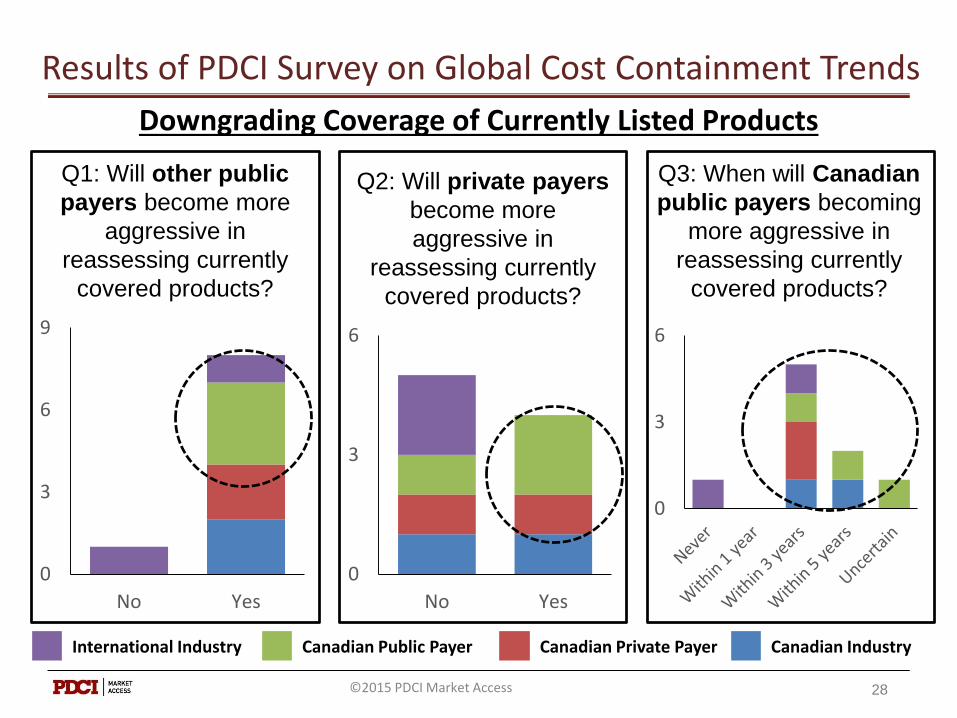
Downgrading Coverage of Currently Listed Products
International Industry Canadian Public Payer Canadian Private Payer Canadian Industry
Q1: Will other public
payers become more
aggressive in
reassessing currently
covered products?
0
3
6
9
No Yes
Q2: Will private payers
become more
aggressive in
reassessing currently
covered products?
0
3
6
No Yes
Q3: When will Canadian
public payers becoming
more aggressive in
reassessing currently
covered products?
0
3
6
©2015 PDCI Market Access
Results of PDCI Survey on Global Cost Containment Trends
Q: How do you think industry will respond to aggressive reassessments of their products?
29
Private Payer: “Concede on originalpricing to re-establish the relative value oftheir products relative to competitors.”
Public Payer: “More aggressive marketingto physicians.”
©2015 PDCI Market Access
Results of PDCI Survey on Global Cost Containment Trends
30
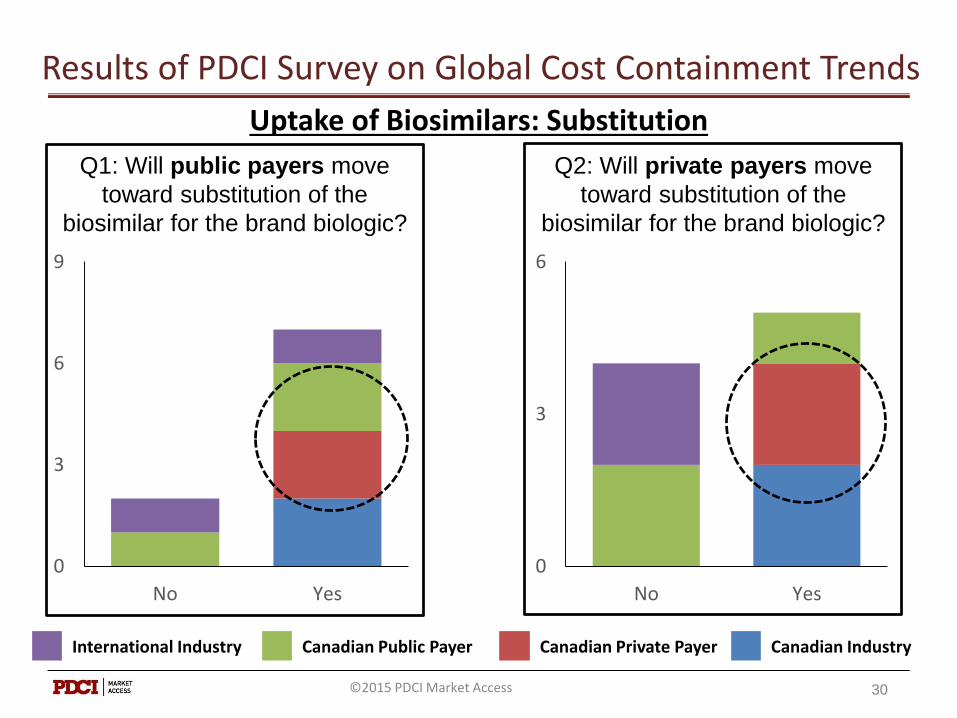
Uptake of Biosimilars: Substitution
International Industry Canadian Public Payer Canadian Private Payer Canadian Industry
Q1: Will public payers move
toward substitution of the
biosimilar for the brand biologic?
0
3
6
9
No Yes
Q2: Will private payers move
toward substitution of the
biosimilar for the brand biologic?
0
3
6
No Yes
©2015 PDCI Market Access

Results of PDCI Survey on Global Cost Containment Trends
31
Uptake of Biosimilars: Therapeutic Priorities
Rank the following biosimilar classes in terms of which will have the most
impact in driving payer adoption of biosimilar. 3 points = most impact; 2 points = medium impact; 1 point = least impact; 0 points = no impact
0
3
6
9
12
15
18
21
24
Rheumatoid Arthritis Diabetes Oncology
International Industry Canadian Public Payer Canadian Private Payer Canadian Industry
©2015 PDCI Market Access
Results of PDCI Survey on Global Cost Containment Trends
32
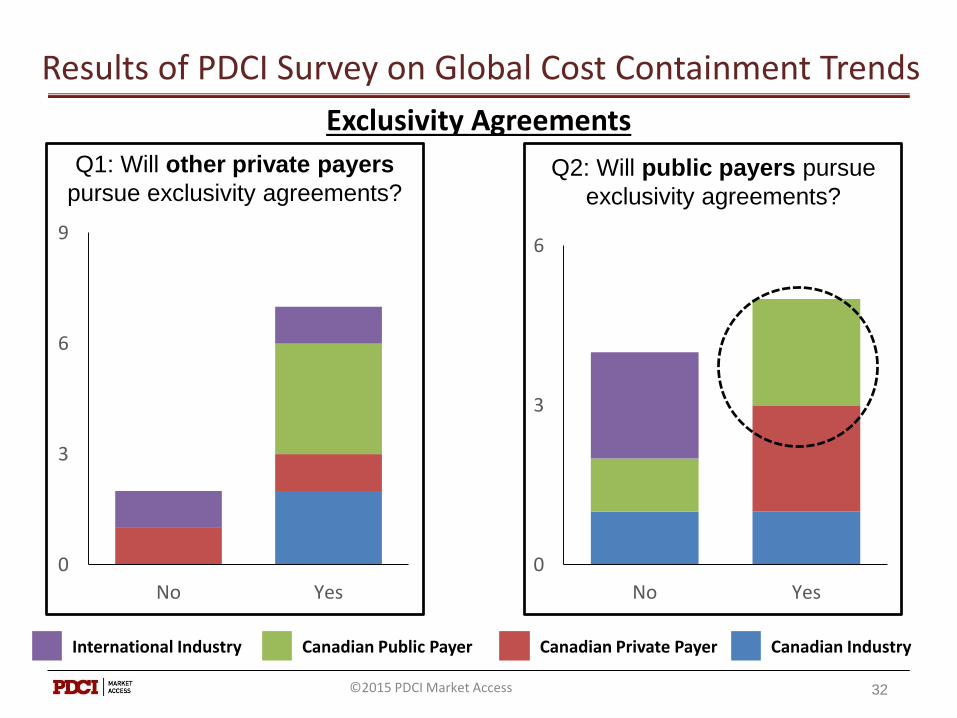
Exclusivity Agreements
Q2: Will public payers pursue
exclusivity agreements?
International Industry Canadian Public Payer Canadian Private Payer Canadian Industry
Q1: Will other private payers
pursue exclusivity agreements?
0
3
6
9
No Yes
0
3
6
No Yes
©2015 PDCI Market Access

Results of PDCI Survey on Global Cost Containment Trends
Q: How do you think industry will respond if private payers start to pursue more exclusivity agreements?
33
Public Payer: “Much the same way as they did to public payers -PLAs, risk-shares and evidence-gathering.”
Private Payer: “More aggressive marketing push direct to members via patient assistance programs, financial assistance”
Public Payer: “The market will become more of an all or nothing for manufacturers. For the aggressive manufacturers there is a chance to get a greater market share. But overall manufacturers will not like this because it ultimately will drive down their profit margin per unit.”
Canadian Industry: “More aggressive PLAs. As we saw years back with PPIs, there will always be a company that is willing to push negotiations for exclusivity”
©2015 PDCI Market Access
Product Listing Agreements
34
Product Listing
Agreements
Pricing
Cost Containment
Trade
©2015 PDCI Market Access

Product Listing Agreements
35
The Performance Based Risk Sharing (PBRS) web-enabled database was developed by the Pharmaceutical Outcomes Research & Policy Program at the University of Washington https://depts.washington.edu/pbrs/index.php
©2015 PDCI Market Access

PBRSA - Defined
“Performance-based risk-sharing arrangements (PBRSAs)—involve a plan by which the performance
of the product is tracked in a defined patient population over a specified period of time and the amount or level of reimbursement is based on the
health and cost outcomes achieved.”
36
Source: Risk-Sharing/Performance-Based Arrangements for Drugs and Other Medical Products, June, 1, 2014,
Garrison, Towse and Carlson.
©2015 PDCI Market Access
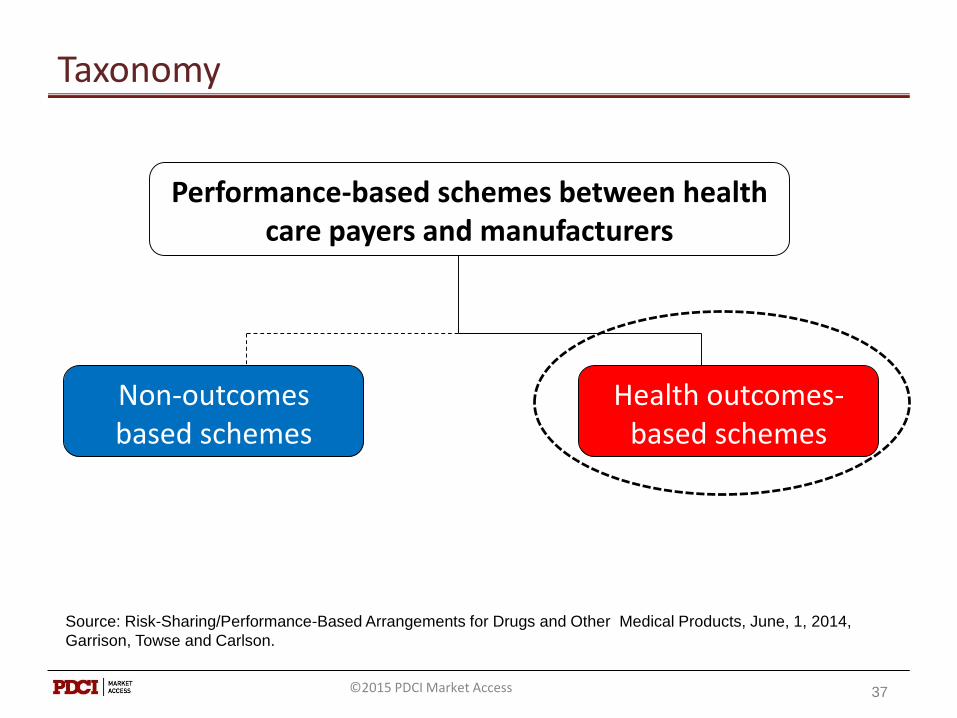
Taxonomy
37
Health outcomes-based schemes
Non-outcomes based schemes
Performance-based schemes between health care payers and manufacturers
Source: Risk-Sharing/Performance-Based Arrangements for Drugs and Other Medical Products, June, 1, 2014,
Garrison, Towse and Carlson.
©2015 PDCI Market Access
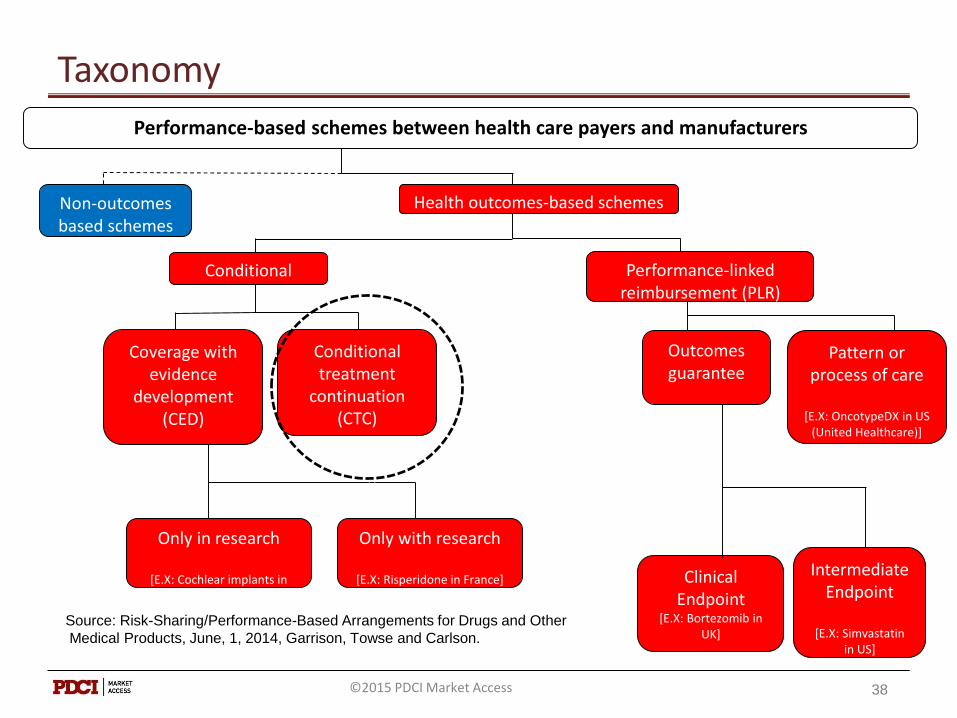
Taxonomy
Outcomes guarantee
Clinical Endpoint
[E.X: Bortezomib in UK]
Intermediate Endpoint
[E.X: Simvastatinin US]
Performance-based schemes between health care payers and manufacturers
Health outcomes-based schemesNon-outcomes based schemes
Performance-linked reimbursement (PLR)
Pattern or process of care
[E.X: OncotypeDX in US (United Healthcare)]
Only in research
[E.X: Cochlear implants in US(CMS)]
Only with research
[E.X: Risperidone in France]
Coverage with evidence
development (CED)
Conditional coverage
Conditional treatment
continuation (CTC)
[E.X: Alzheimer’s drugs in Italy]
38
Source: Risk-Sharing/Performance-Based Arrangements for Drugs and Other
Medical Products, June, 1, 2014, Garrison, Towse and Carlson.
©2015 PDCI Market Access
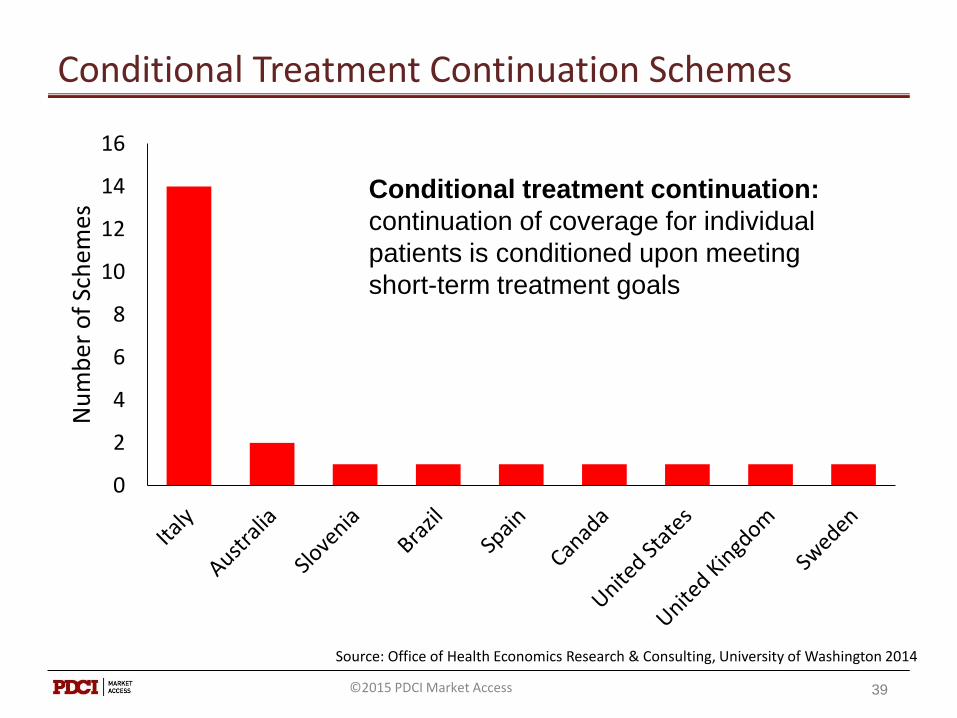
Conditional Treatment Continuation Schemes
0
2
4
6
8
10
12
14
16
Nu
mb
er o
f Sc
hem
es
39
Source: Office of Health Economics Research & Consulting, University of Washington 2014
Conditional treatment continuation:
continuation of coverage for individual
patients is conditioned upon meeting
short-term treatment goals
©2015 PDCI Market Access
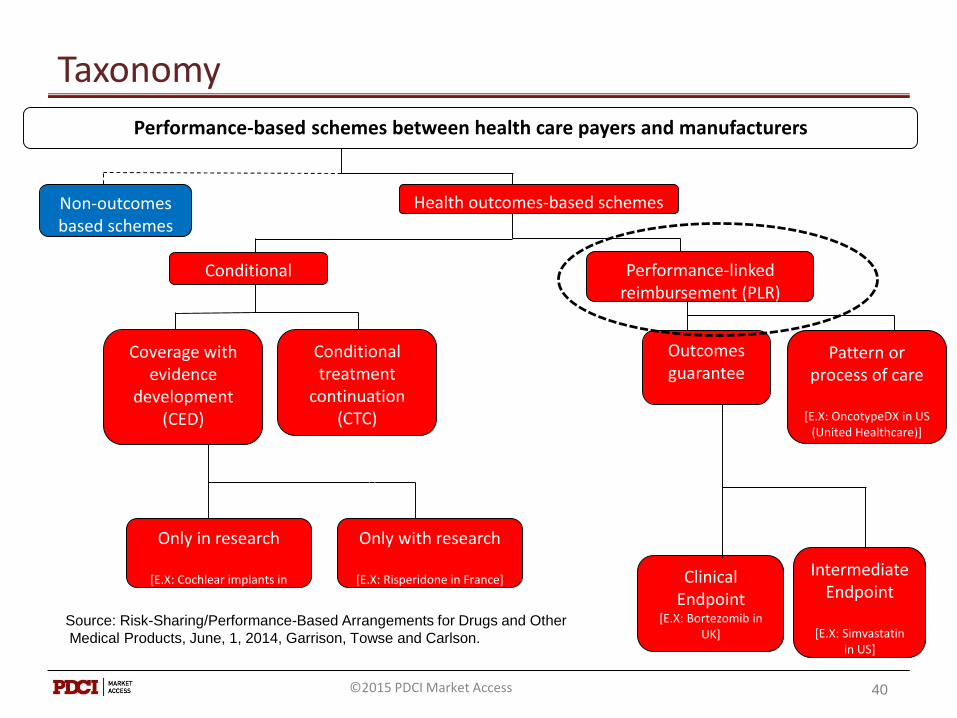
Taxonomy
Outcomes guarantee
Clinical Endpoint
[E.X: Bortezomib in UK]
Intermediate Endpoint
[E.X: Simvastatinin US]
Performance-based schemes between health care payers and manufacturers
Health outcomes-based schemesNon-outcomes based schemes
Performance-linked reimbursement (PLR)
Pattern or process of care
[E.X: OncotypeDX in US (United Healthcare)]
Only in research
[E.X: Cochlear implants in US(CMS)]
Only with research
[E.X: Risperidone in France]
Coverage with evidence
development (CED)
Conditional coverage
Conditional treatment
continuation (CTC)
[E.X: Alzheimer’s drugs in Italy]
40
Source: Risk-Sharing/Performance-Based Arrangements for Drugs and Other
Medical Products, June, 1, 2014, Garrison, Towse and Carlson.
©2015 PDCI Market Access

Performance-Linked Reimbursement Schemes
0
5
10
15
20
25
30
Nu
mb
er o
f Sc
hem
es
41
Source: Office of Health Economics Research & Consulting, University of Washington 2014
Performance-linked reimbursement:
reimbursement level for covered
products is tied, by formula, to the
measure of clinical outcomes in the
“real world”
©2015 PDCI Market Access

Taxonomy
42
Health outcomes-based schemes
Non-outcomes based schemes
Performance-based schemes between health care payers and manufacturers
Source: Risk-Sharing/Performance-Based Arrangements for Drugs and Other Medical Products, June, 1, 2014,
Garrison, Towse and Carlson.
©2015 PDCI Market Access
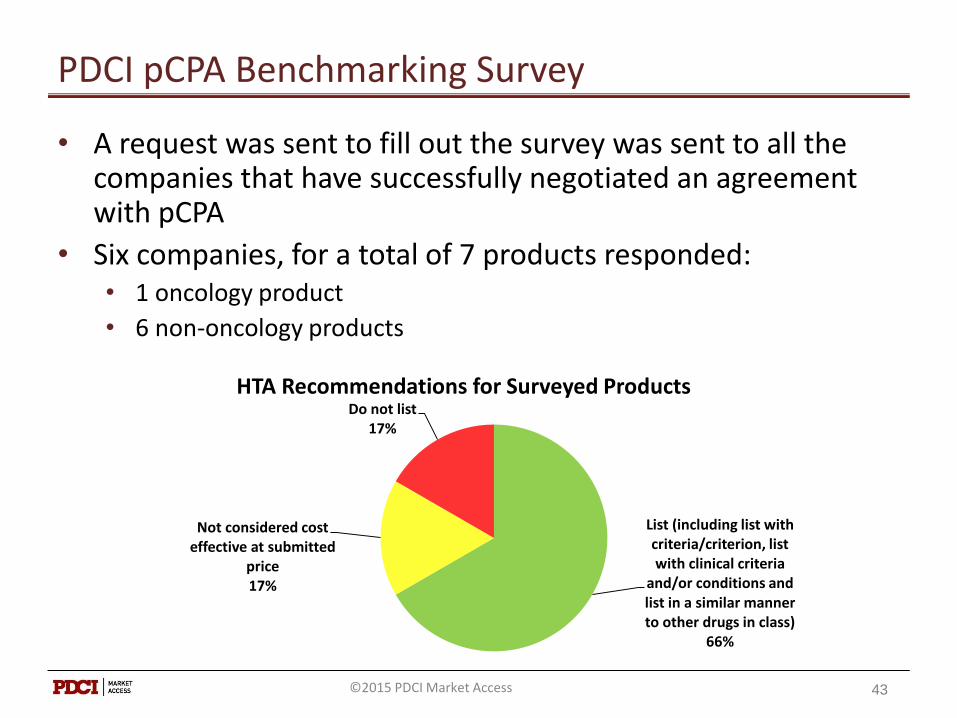
PDCI pCPA Benchmarking Survey
• A request was sent to fill out the survey was sent to all the companies that have successfully negotiated an agreement with pCPA
• Six companies, for a total of 7 products responded: • 1 oncology product
• 6 non-oncology products
List (including list with criteria/criterion, list with clinical criteria
and/or conditions and list in a similar manner to other drugs in class)
66%
Not considered cost effective at submitted
price17%
Do not list17%
HTA Recommendations for Surveyed Products
43©2015 PDCI Market Access
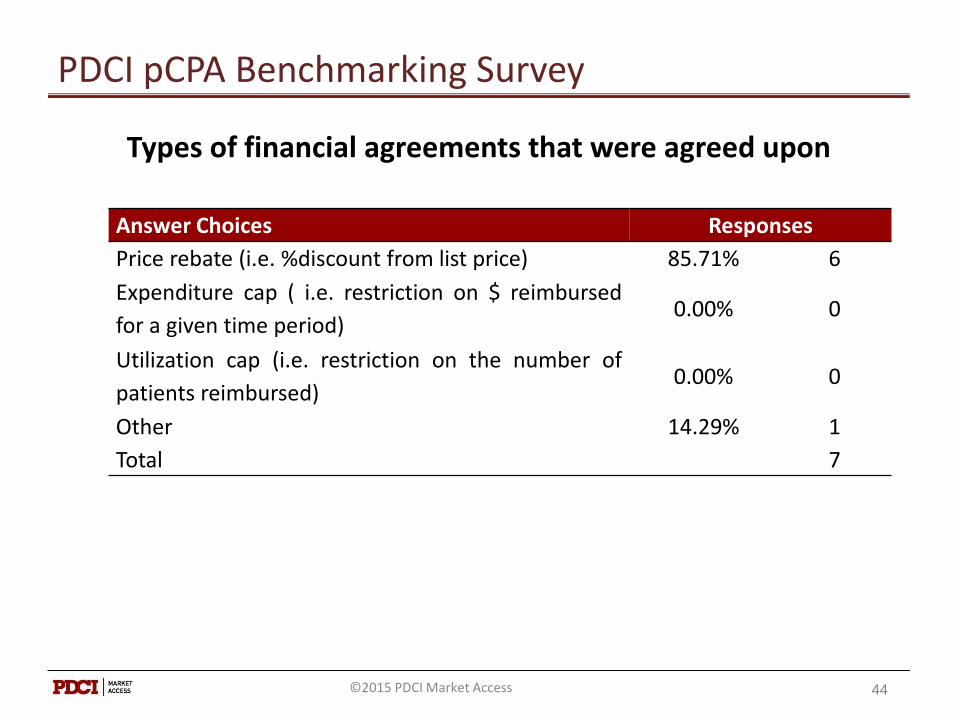
PDCI pCPA Benchmarking Survey
Types of financial agreements that were agreed upon
Answer Choices Responses
Price rebate (i.e. %discount from list price) 85.71% 6
Expenditure cap ( i.e. restriction on $ reimbursed
for a given time period)0.00% 0
Utilization cap (i.e. restriction on the number of
patients reimbursed)0.00% 0
Other 14.29% 1
Total 7
44©2015 PDCI Market Access
45
Outlook
©2015 PDCI Market Access
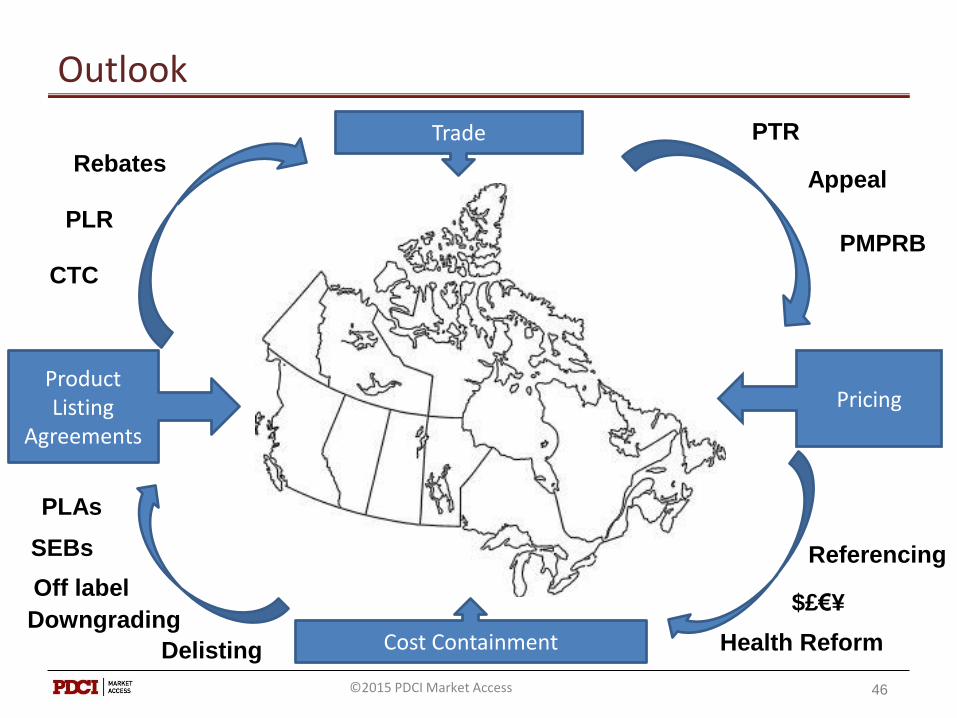
46
Outlook
Product Listing
Agreements
Pricing
Cost Containment
Trade PTR
Appeal
PMPRB
$£€¥
Referencing
Health ReformDelisting
Downgrading
Off label
PLAs
SEBs
Rebates
CTC
PLR
©2015 PDCI Market Access
47©2015 PDCI Market Access

Biography
Arvind ManiDirector, Market Access and Policy Research
PDCI Market Access Inc
www.pdci.ca
Arvind Mani is the Director of Market Access and Policy Research at PDCI. Arvind leads a team of consultants onpharmaceutical reimbursement (budget impact analyses), policy, and patent litigation projects. Arvind has morethan 15 years of experience working in industry, associations and consulting. He provides expert knowledge tocompanies, governments on pharmaceutical pricing, regulatory, market access, and patent issues and is alsoresponsible for contributing to pricing and reimbursement policy and analysis projects. Before joining PDCI,Arvind spent several years as the Director of Corporate Affairs at the National Association of Pharmacy RegulatoryAuthorities (NAPRA) in Ottawa. Prior to NAPRA, he worked for 8 years at Canada’s Research-BasedPharmaceutical Companies (Rx&D), an association that represents the interests of innovative pharmaceuticalcompanies in Canada. Arvind held various positions at Rx&D, including Research Analyst, Director of RegulatoryAffairs, and Director of Policy Development. Prior to joining Rx&D, Arvind was a Market Analyst with Ciba Geigy(now Novartis Pharmaceuticals Canada Inc.).
PDCI Market Access (PDCI) is a leading pharmaceutical pricing and reimbursement (P&R) consultancy based inOttawa and Toronto. Established in 1996, the firm features a senior team of multi-lingual market accessprofessionals with extensive experience assisting clients navigate the complex P&R challenges facing Canadianpharmaceutical manufacturers. PDCI develops successful P&R strategies and prepares comprehensivesubmissions to CDR, pCODR, public & private payers and the PMPRB. The firm’s senior consultants facilitatemeetings with CDR/payers/PMPRB, negotiate product listing agreements (PLAs) and resolve pricing complianceissues with the PMPRB. PDCI maintains databases of international pharmaceutical prices and provincial drugclaims and costs.
48©2015 PDCI Market Access