
CAN-IMPLEMENT © for Guideline Adaptation and Implementation Part 2: The Methodology (August 2011)
52
CAN-IMPLEMENT© for Guideline Adaptation and Implementation Part 2: The Methodology (August 2011)
-
Upload
byron-barber -
Category
Documents
-
view
236 -
download
0
Transcript of CAN-IMPLEMENT © for Guideline Adaptation and Implementation Part 2: The Methodology (August 2011)
CAN-IMPLEMENT© for Guideline Adaptation and
Implementation
Part 2: The Methodology(August 2011)
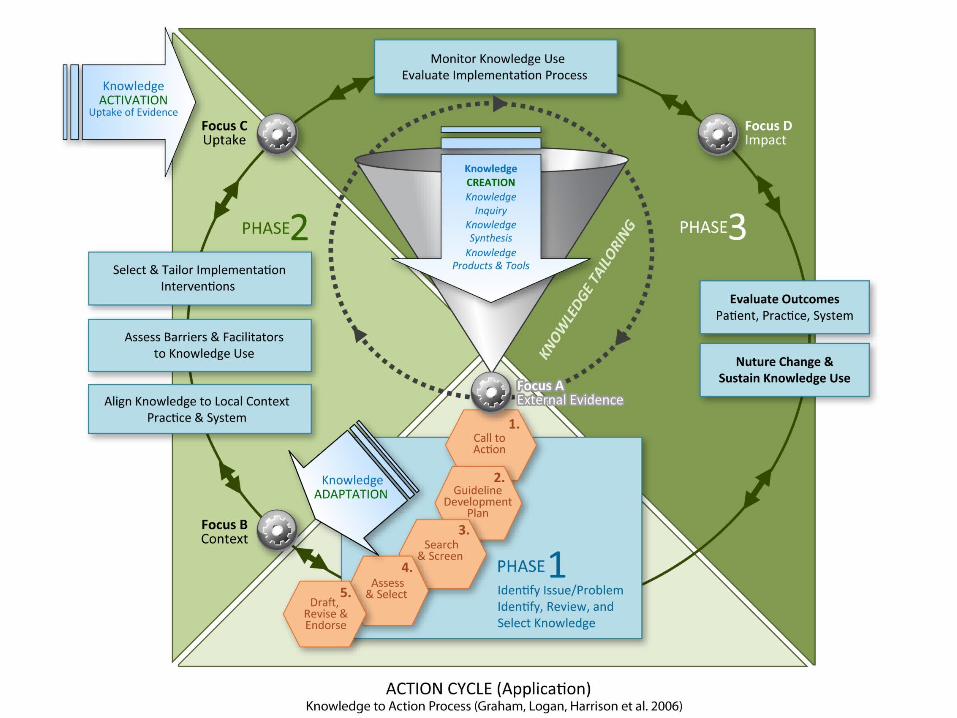

3 Phase Methodology
PHASE 1Identification and
Clarification of Issue/Problem
PHASE 2Solution Building
PHASE 3Implementation, Evaluation and Sustainability

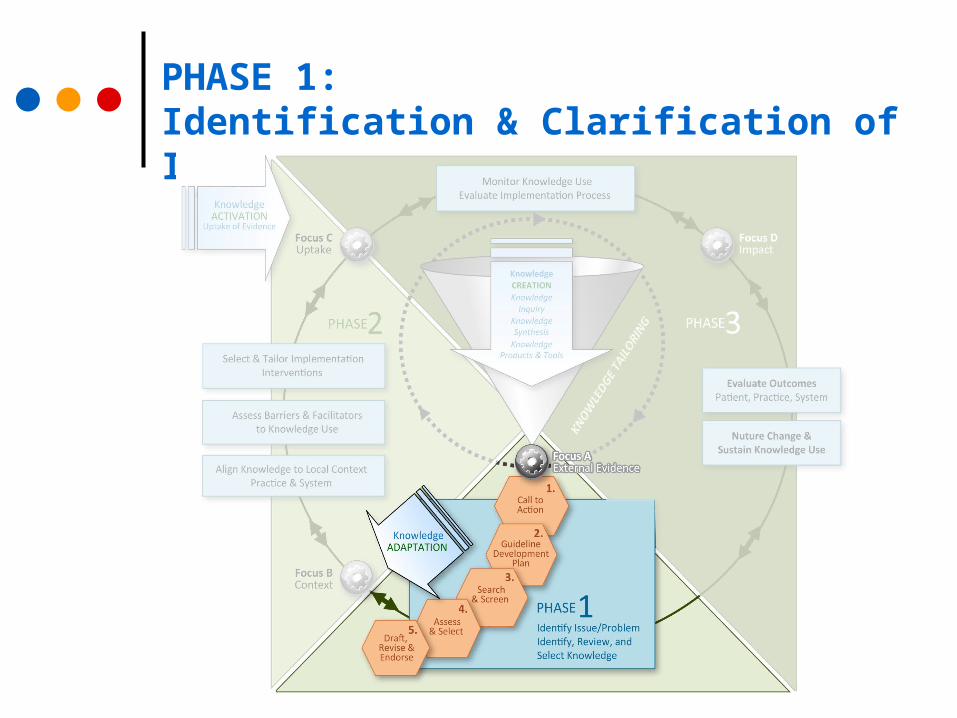
PHASE 1: Identification & Clarification of Issue/Problem
PHASE 1, Step 1: Call-to-Action
1.1 Clarify the motivation, purpose and scope of the proposed initiative. Consider:
What is the agency/ institutional mandate and infrastructure
supporting evidence-informed practice? Is this a response to a specific practice challenge? Is a guideline the most appropriate solution to the challenge? Who (person/group) will lead, implement and maintain these
recommendations? What is the intended practice jurisdiction (local, regional,
national??
PHASE 1, Step 1: Call-to-Action
A critical, strategic element requiring strong facilitation and
leadership skills; establishes legitimate guideline development
mandate and infrastructure; especially important for new groups
Plan an orientation session for participants Discuss: What is a “guideline”?

Tools PHASE 1: Evidence-informed practice Training Resources

PHASE 1, Step 2: Plan
2.1 Establish scope of guideline and articulate Health Question(s).
2.2 Determine feasibility of adaptation.
2.3 Form steering committee and working panel(s) and determine key stakeholders and necessary resources
2.4 Determine consensus process.
2.5 Write the Adaptation Work Plan.

PHASE 1, Step 2: Plan
Use the PIPOH instrument to develop health questions Determine required expertise and resources;
(using the Skills Assessment Checklist) Understand Facilitation and the role of the Coordinator Draft Adaptation Work Plan – an essential document
outlining: Scope of topic and health questions Terms of reference (steering committee and working panel(s) Funding and resource commitments Consensus process Conflicts of interest Projected timeline Meeting arrangements
Tools PHASE 1: PIPOH Checklist
► Patient population: average risk women► Intervention: screening► Professionals: family physicians/ GPs/nurses► Outcomes: screening interval/modality► Healthcare setting: family practice
Example Question: What is appropriate cervical cancer screening (CCS)for average risk women seen in family practice?

Tools PHASE 1: Search Sources

Tools PHASE 1: Skills Assessment Checklist

Tools PHASE 1: Sample Declaration of Conflict of Interest CONFLICT OF INTEREST DISCLOSURE DECLARATION

Tools PHASE 1: Sample Adaptation Work Plan
PHASE 1, Step 3: Search and Screen
3.1 Search existing guidelines, systematic reviews, and new or emerging areas of evidence; confirm if guideline is de novo, adaptation or mixed initiative.
3.2 Screen search results to develop short list for full appraisal; document selection.

PHASE 1, Step 3: Search and Screen
Designing and executing the search - engaging services of a health science librarian or information specialist
Managing citations: Developing a screening protocol and documenting selection decisions
Library Science Supplement and Toolkit resources

Designing the search:Choosing inclusion/exclusion criteria
Selecting only evidence-based guidelines (guideline must include a report on systematic literature searches and explicit links between individual recommendations and their supporting evidence
Selecting only national and/or international guidelines; selecting guidelines written in a particular language Fr/Eng?)
Specifying a range of dates for publication; selecting only those published since an important review was published
Selecting peer reviewed publications only; excluding guidelines written by a single author not on behalf of an organization – ideally has multidisciplinary input
Excluding guidelines published without references – panel must have access to the evidence

Potential papers found(n=599)
Potential papers found(n=599)
Rejected – not CPGs(n=537)
Rejected – not CPGs(n=537)
Remaining more Carefully reviewed
(n=62)
Remaining more Carefully reviewed
(n=62)
Rejected – not population screening
(n=10)
Rejected – not population screening
(n=10)
Duplicates searched for in remaining
(n=52)
Duplicates searched for in remaining
(n=52)
Duplicates(n=32)
Duplicates(n=32)
Updates searchedfor in remaining
(n=20)
Updates searchedfor in remaining
(n=20)
Updated(n=2)
Updated(n=2)
Cervical cancer population
screening CPGs(n=18)
Cervical cancer population
screening CPGs(n=18)
8 from Medline9 from Web
1 from CCOHTA
8 from Medline9 from Web
1 from CCOHTA
Evidence/ Literature
Search and Screen

PHASE 1, Step 4: Assess and Select
4.1 Assess shortlisted guidelines (recommendations and supporting evidence) in detail for: quality (e.g. AGREE), currency, content, coherence between evidence and recommendations, and applicability and acceptability to local context. 4.2 Decision and Selection: review all assessments and achieve consensus with respect to Selecting, Rejecting or Modifying specific

PHASE 1, Step 4: Assess and Select
Assessing Quality of guidelines Using the AGREE II Instrument Summarizing and displaying AGREE scores Assessing Quality of Systematic Reviews
Assessing guideline Currency
Assessing guideline Content Preparing the ‘Recommendations Matrix’ The evidence: type and level; classification systems Critical appraisal (interpretation and Consistency of evidence)
Assessing Acceptability and Applicability
Making Decision to Accept, Reject or Modify Achieving and documenting consensus
www.agreetrust.org

Tools PHASE 1: AGREEII Instrument
23 items
7 point Scale
Overall Assessment
User Guide & Manual
1. Scope & purpose (3)
2. Stakeholder involvement (3)
3. Rigour of development (8)
4. Clarity of presentation (3)
5. Applicability (4)
6. Editorial independence (2)
SIX Domains

CURRENCY Assessment
Is there any new evidence relevant to guideline?
Does new evidence invalidate any of the recommendations?
Are there any plans to update the guideline in the near future?
When was the guideline last updated?

CONSISTENCY Assessment
Quality of source guideline search strategy and study selection ( ADAPTE Tool 13) Was the search for evidence comprehensive? Is there any bias in the selection of articles?
Consistency between evidence and interpretations; between interpretations and recommendations ( ADAPTE Tool 14) Is the evidence valid, overall? Are the recommendations based on data and
interpretations?

Tools PHASE 1: Evaluation: Search and Selection of Evidence

Tools PHASE 1: Evaluation Sheet: Scientific Validity of GuidelinesConsistency between evidence, its interpretation and recommendations)

Tools PHASE 1: Recommendations Matrix (template)
APPLICABILITY Assessment
Review of each of the recommendations with respect to 2 main questions (ADAPTE Tool 15)
Can the recommendation be put into practice? Consider patient similarity, interventions, outcomes, patient preferences, availability of equipment, availability of expertise, any constraints?
Is the benefit from this recommendation worth implementing?

Tools PHASE 1: Evaluation Sheet: Acceptability/Applicability
Decision and Selection; you might …
Use process of elimination based on overall AGREE scores
Eliminate any outdated CPGs
Look at recommendations of top 3 CPGs and decide which you could adopt in entirety; which you cannot reach agreement upon; which individual recommendations you can agree to adopt …
Decision and Selection Options
1. ACCEPT a whole guideline and all of its recommendations After reviewing all of the assessments, the panel accepts the guideline as is.
2. REJECT a whole guideline and all of its recommendations After reviewing all of the assessments, the panel decides to reject the complete
guideline. The decision will be based on how the panel weighs the assessments (e.g., poor AGREE scores, guideline is out-of-date, the recommendations do not apply to the panel’s context).
3. ACCEPT the evidence summary of the guideline After reviewing all of the assessments, the panel decides to accept the description of
the evidence (or parts) but to reject the interpretation and the recommendations.
4. ACCEPT a single recommendation After reviewing the recommendations from the guideline or guidelines, the panel
decides which to accept and which to reject which may be from one or more guidelines.
5. MODIFY single recommendations After reviewing all of the recommendations from the guideline(s), the panel decides
which are acceptable but need to be modified.

PHASE 1, Step 5: Draft, Review, and Endorse Recommendations
5.1 Draft Customized Guideline
5.2 Conduct internal review and make revisions
5.3 Conduct external review and obtain endorsement
5.4 Prepare final documents, including any practitioner and patient information, records or application tools, and appropriate source acknowledgments
5.5 Establish a Renewal Plan

PHASE 1, Step 5: Draft, Review, and Endorse Recommendations
Customizing recommendations: Using a template for structure and content Authors, acknowledgements, permissions and copyright
issues from source developers Using brief, unambiguous, actionable language Including application tools, algorithms, patient information Including a short preface summarizing recommendations,
and methodology; appendices and possible web links to documents
Important aspect: Transparency of all decision making (e.g., consensus process is described, how decisions were arrived at and resolved; if recommendations were modified, how and why they were modified);

External Review
External review with those affected by uptake, e.g., experts (practitioners, patients) and users (policy makers, managers)
Consultation with endorsement bodies Inclusion of representative on panel throughout process?
Consultation with source guideline developers
Acknowledgement of source documents

Tools PHASE 1: Sample External Review Survey

Sustainability/Planning for renewal
Guideline maintenance specifying in the guideline when, how and by whom the
recommendations will be updated

PHASE 2: Solution Building
PHASE 2, Step 1: Align Knowledge to Local Context (Practice and System)
Conduct a gap analysis
To focus an implementation action plan, it is necessary to first understand the difference between current practices and the new recommendations.
The objective of the gap analysis is to clarify exactly what and how much will need to change in the prevailing practice and
system.

Gathering information
Information about the local population, organization, and providers can be obtained from many sources using a variety of formal and informal methods, including:
Guideline documentation from PHASE 1 Steps 1-5, e.g. previous environmental scans or other baseline measurements, and meeting notes from discussions on re: acceptability and feasibility of recommendations
Clinical/Chart Audit
Interviews, focus groups, town hall sessions, surveys and questionnaires

PHASE 2, Step 2: Assess the Innovation, Adopters and Practice Environment for “Barriers and Supports”
Innovation (examples):
Attributes of the evidence-informed recommendations
The rigour/credibility of the guideline development process
Perceived compatibility of recommendations with existing routines (e.g. complexity, convenience, relative advantages or costs

PHASE 2, Step 2: Assess the Innovation, Adopters and Practice Environment for “Barriers and Supports”
Adopters (examples):
Awareness Knowledge and Skills Attitudes, expectations, motivation Current behaviours or routines Concerns, preferences
NOTE: Adopters include allied health practitioners (the care “providers”), administrative and organizational staff and leaders – and patients and their families!
PHASE 2, Step 2: Assess the Innovation, Adopters and Practice Environment for “Barriers and Supports”
Practice Environment/Organizational Context (examples):
Organizational culture and “readiness” for evidence-based practice Infrastructure; levels of authority and decision-making processes Resources; economic constraints Leadership; availability of Champions Work Load; levels of job stress Quality Improvement mechanisms

(Tools) RNAO “Environmental Readiness Assessment”

PHASE 2, Step 3: Select and Tailor Implementation Interventions
Best practice Implementation strategies should address barriers related to the individual practitioner, social context and organizational and environmental context - and should be tailored to different groups of stakeholders (i.e. nursing staff, project leaders and administrators.”) Ploeg, 2007

Implementation Strategies/Tactics
Educational Outreach Reminders: manual or computerized Introduction of computers in practice; computerized decision support Multi-faceted interventions Interactive small group meetings Multi-professional collaboration Mass media campaigns Financial interventions (fund-holding/budgets) Use of opinion leaders/champions Audit and feedback Conferences and courses Educational materials Patient-mediated interventions Dissemination of printed educational material Didactic educational sessions (lectures) Total quality improvement/continuous quality improvement

Usability Testing
Barrier management and knowledge transfer are iterative processes.
Consider the value of testing new procedures, decision making algorithms, training information and other support tools with both patients and providers before proceeding with a full scale implementation.

Tools PHASE 2: Implementation Action Planning (template)

PHASE 3: Implementation, Evaluation & Sustainability
Evaluation Planning:Monitoring Uptake and Assessing Outcomes
In PHASE 3, groups evaluate both the level of evidence uptake and the impact of the new recommendations for care on the intended:
patient population health care providers organization

Evaluation Planning:Monitoring Uptake and Assessing Outcomes
Key Concepts:
Evaluating use of recommendations: Defining the evaluation period - from date of “knowledge
activation” to “targeted threshold” of guideline uptake
Evaluating implementation process Monitoring, revisiting and augmenting or modifying implementation “interventions” to enhance uptake
Evaluating impact: Defining specific ‘indicators’ Establishing tracking measures (data collection/resources) Assessing Patient, Practice (provider) and System outcomes

Using the CAN-IMPLEMENT© ResourceNavigation
Field Notes Tips Checklists Thinking about Implementation Progress Checks - Direction - Outputs - Documents - Tools


















