Transformational Practice and Partnerships Annual Report 2016
Upload
william-buddy-gillespie-itil-certifiedCategory
view
354download
0
Can HIEs Really Achieve Financial Sustainability: A Case Study and Discussion on Transformational
Approaches and Unique Partnerships
© 2012 PAeHI 1
Making Magic with Medicine, Technology, and Innovation Conference
New Jersey and Delaware Valley HIMSS ChaptersAtlantic City, NJ
October 4-5, 2012

Presented by
Dr. Chris Cavanaugh, Executive Director, Pennsylvania eHealth Initiative (PAeHI)
William “Buddy” Gillespie, PAeHI Chair HIE Committee, Director of HealthCare Solutions for Distributed Systems
Services (DSS)
Camilla Hull Brown, MBA, Principal & Founder, Strategies for Tomorrow Inc
© 2012 PAeHI
www.dsscorp.com
www.paehi.org

AgendaLearning Objectives
1• Discuss the Pennsylvania eHealth Initiative
2
• Explore trends and models from across the state and from a national perspective
3
• Examine critical lessons learned based on a case study of key stakeholder from the Commonwealth of Pennsylvania
4
• Highlight some best practices and care transformational approaches
HealthCare Transformation Track October 4, 2012
Overview
The Pennsylvania eHealth Initiative (PAeHI) was created in 2005 as a voluntary, public, private,
non-profit coalition to bring together Pennsylvania’s healthcare and business
stakeholders to develop a vision and a plan for the future of health information technology and
the secure exchange of health information in Pennsylvania.
Governed by a representative board of directors, PAeHI offers a neutral forum for the
health IT community to work together for a common mission—to improve patient care
through the effective use of health information technology.
Mission
To enable the use of information technology to improve healthcare quality and efficiency and ensure patient safety for all Pennsylvanians.
To ensure secure, confidential access to health information to enable individuals and
communities to make the best possible health decisions.
Purpose
Working collaboratively under the direction of a Board of Directors, PAeHI
endeavors to achieve greater HIT adoption throughout the Commonwealth.
Helping healthcare providers achieve meaningful use for HIT ultimately benefits
the patient; through our efforts, we hope to assist providers in improving quality,
improving patient safety and lowering costs.
The Pennsylvania eHealth Initiative

Key Foundational Roles
5
Identify opportunities for Pennsylvanians to use HIT
and HIE to improve healthcare.
Educate the public providers and policy makers regarding the
benefits and challenges of HIT and HIE.
Coordinate the efforts of all Pennsylvania HIT and
stakeholders.
Identify opportunities to coordinate with and benefit from federal
initiatives.
Develop statewide consensus on established and emerging standards
(e.g., data, communication and reporting).
Work with providers, payers, policy makers to define business cases for
HIT and HIE.

PAeHI Research Studies and White Papers
Establishing widespread adoption of
electronic health records and electronic
prescribing in Pennsylvania
(2008)
Ensuring privacy and security of
Health Information Exchange in
Pennsylvania (2009)
Building a Sustainable Model
for Health Information Exchange in
Pennsylvania (2009)
Financing Research and Framework
Development for a Health Information
Exchange (2010)
6
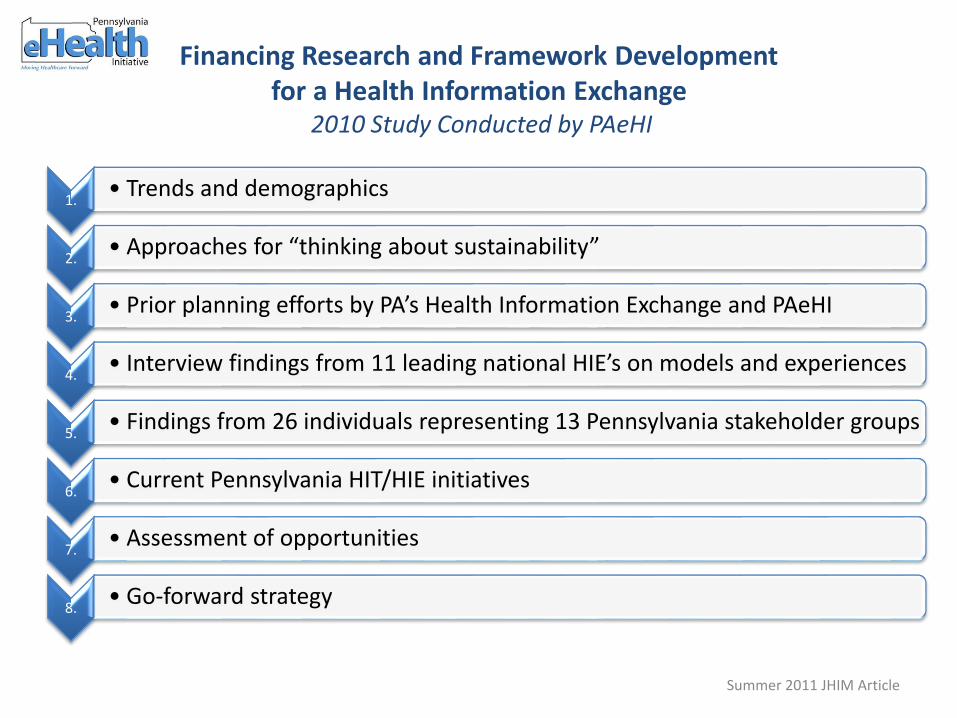
Financing Research and Framework Developmentfor a Health Information Exchange
2010 Study Conducted by PAeHI
1. • Trends and demographics
2. • Approaches for “thinking about sustainability”
3. • Prior planning efforts by PA’s Health Information Exchange and PAeHI
4. • Interview findings from 11 leading national HIE’s on models and experiences
5. • Findings from 26 individuals representing 13 Pennsylvania stakeholder groups
6. • Current Pennsylvania HIT/HIE initiatives
7. • Assessment of opportunities
8. • Go-forward strategy
Summer 2011 JHIM Article
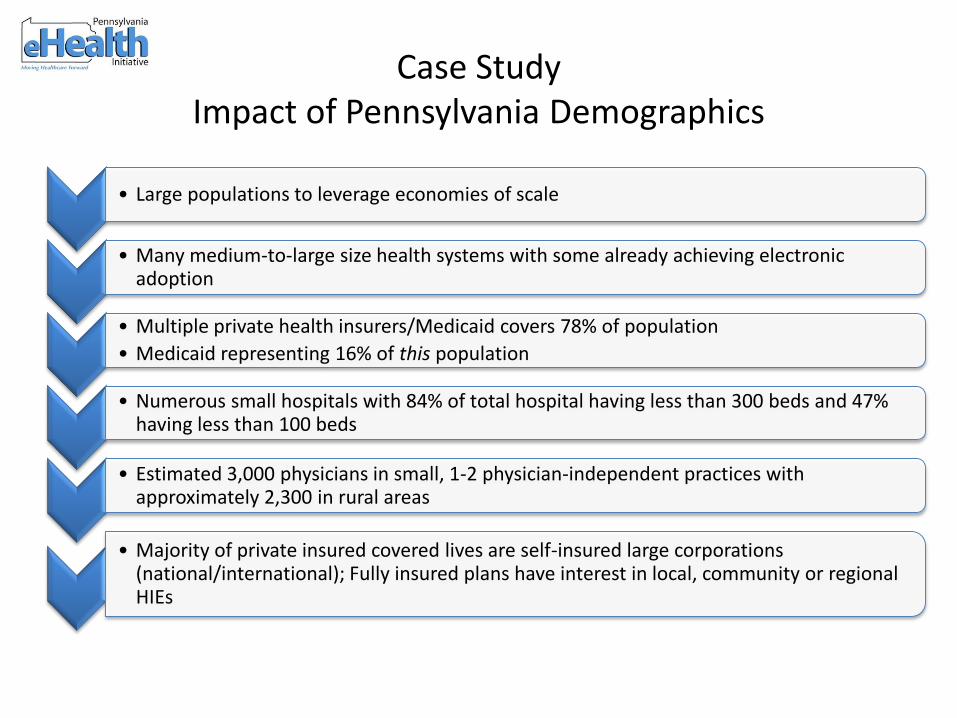
Case StudyImpact of Pennsylvania Demographics
• Large populations to leverage economies of scale
• Many medium-to-large size health systems with some already achieving electronic adoption
• Multiple private health insurers/Medicaid covers 78% of population
• Medicaid representing 16% of this population
• Numerous small hospitals with 84% of total hospital having less than 300 beds and 47% having less than 100 beds
• Estimated 3,000 physicians in small, 1-2 physician-independent practices with approximately 2,300 in rural areas
• Majority of private insured covered lives are self-insured large corporations (national/international); Fully insured plans have interest in local, community or regional HIEs

Case StudyHistorical Pennsylvania HIE Activities
• Comprehensive Roadmap -- Prescription for Pennsylvania (2007)
• ONC has provided $17.1M in funds for a state-level HIE
• HIE initiatives across Pennsylvania
• 12 Hospital based, community, regional HIE’s in operation/planning stages
• Public Health Initiatives
• 9 current or emerging
• Medicaid is developing plans to engage the state health care providers and patients
• Broadband deployment goals by 2015
• 6 initiatives totaling $130.2M in grants to expand broadband and telemedicine
• Includes $99.7M to establish 1,700-mile fiber network to provide affordable services across the Commonwealth
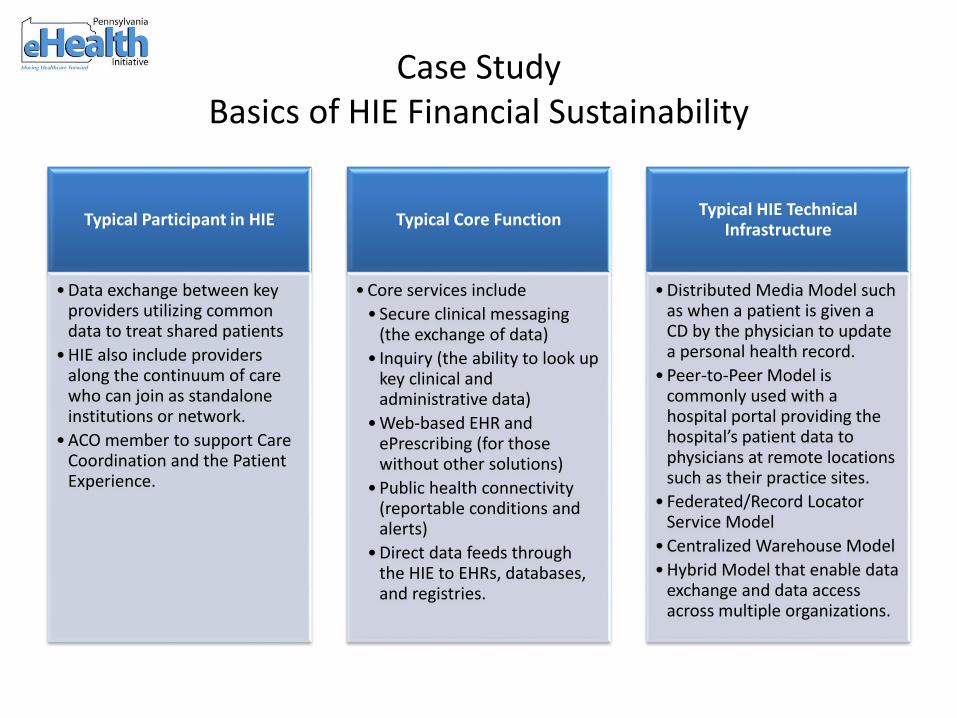
Case Study Basics of HIE Financial Sustainability
Typical Participant in HIE
• Data exchange between key providers utilizing common data to treat shared patients
• HIE also include providers along the continuum of care who can join as standalone institutions or network.
• ACO member to support Care Coordination and the Patient Experience.
Typical Core Function
• Core services include
• Secure clinical messaging (the exchange of data)
• Inquiry (the ability to look up key clinical and administrative data)
• Web-based EHR and ePrescribing (for those without other solutions)
• Public health connectivity (reportable conditions and alerts)
• Direct data feeds through the HIE to EHRs, databases, and registries.
Typical HIE Technical Infrastructure
• Distributed Media Model such as when a patient is given a CD by the physician to update a personal health record.
• Peer-to-Peer Model is commonly used with a hospital portal providing the hospital’s patient data to physicians at remote locations such as their practice sites.
• Federated/Record Locator Service Model
• Centralized Warehouse Model
• Hybrid Model that enable data exchange and data access across multiple organizations.

Case StudySimple Framework
Comparing HIEs & Impact on Financial Sustainability
Integrated delivery networks (IDNs)
•Organized by one Institution
•Hospital to connect its physicians & provider partners & ensures that hospitals and physicians can participate in Meaningful Use Incentive
•Costs are absorbed by Institution & Hospital vendors set up networks
•Examples: Pinnacle Health System and Doylestown Hospital
Community/Regional HIE
•Organized around one or more medical referral regions with a multi-stakeholder governing body
•Fees are paid by the stakeholders based on benefits received & startup funding coming from key stakeholders or outside funding sources (grants)
•Examples: Geisinger’s KeyHIE and UPMC’s HIE are blended IDN/Regional HIEs.
State-level HIE
• State geographic boundaries
• Responsible for addressing barriers to HIE adoption around privacy and security, standards, and legal issues with bordering states
• Funded by federal government to include state agencies such as Medicaid and Public Health
• Example: Designation of a state-level HIE in Pennsylvania

Case StudyPAeHI “Go Forward” Strategy
HIE Sustainability
Model for Three Levels
of HIE
1. Articulate a high-level model that shows how IDNs,
community/regional-level HIEs, and a state-level HIE
can flourish across the state. Consider the unique issues
in each medical referral region and statewide.
2. Collect market research by medical referral region and
statewide in areas that need more exploration.
3. Engage stakeholders in a discussion about the model.
4. Come to general consensus on an HIE
Sustainability Model for the state and next steps.
© 2012 PAeHI 12

Case Study– Pennsylvania's Next Steps
Phase 1- ONC 2012 (Push)
• Leverage DIRECT specifications
• PA eHealth Collaborative
• HISPs
• Allied HIE
• Geisinger Clinic (KeyHIE)
• MaxMD
• Secured Exchange Solutions (SES)
• RFP for Community Shared Services
• DIRECT Grants
• Establishing Authority (SB8)
Phase 2 – ONC 2013 (Push & Pull)
• PA eHealth Partnership Authority Board
• Sustainability
• Aligning HIPPA with PA
• Expand capabilities as defined by the stakeholder community
• MU Stage 1 & 2
Environmental Scan (Internal )
• Listing of all PA HIE Stakeholders
• Current
• Newly formed
• Planning phase
• Identify potential stakeholders not active and/or in under-served areas (urban, rural, CAH)
• Develop DB and map of HIE Stakeholders
Environmental Scan (External)
• PA shares borders with 5 states
• What are current cross-border data exchange use cases?
• Where do border HIEs currently exist?
• Can they be leveraged by PA stakeholders or visa versa?
• Identify issues and complexities of cross-border data exchange
Models
•Questions on Models
•Sustainability Whitepaper identifies three models; are there others?
•How do we categorize hybrid approaches?
•How do we categorize Direct Project participants?
•What are the models identified by other leading HIE authorities (e.g. ONC, eHI)?
•How do we make it easier for stakeholders to identify a model which is right for them?
•How do ACO’s fit into these models?
© 2012 PAeHI 13
National Perspective
Key Points
• Federal funding and prominence for HIE
• 250 HIE’s nationally with 18 financially self-sustaining
• Initiatives to drive Meaningful Use of EHRs and HIEs
• Health Reform Legislations 2010 is pushing coordinated care through ACO’s and patient centered medical home

Health Information ExchangeServices Provided
Majority Provide
• Clinical messaging and Inquiry (CCD)
• PH Dept. reportable conditions or Immunization Registry
Most Provide
• Had or planning eRX, orders, physician workflow tools
• Six of 11 had or planning low-cost, Web-based certified EHRS that meets Meaningful Use
Unique Services
• INHS (WA) offers shared IT services to 38 hospitals plus majority of physicians; others use Virtual Private Network
• MiHIN Resource Services plans to implement 7 sub-state HIEs over 18 months.

Seven Success Strategies
1 • Innovative stakeholder negotiations
2 • Building the right relations hospitals & payers
3 • Physician adoption as driver of sustainability
4 • Innovation to bring payers/providers together
5 • Innovative sources for fee income
6 • State leaders drive healthcare transformation
7 • Longer-term HIEs look to the future
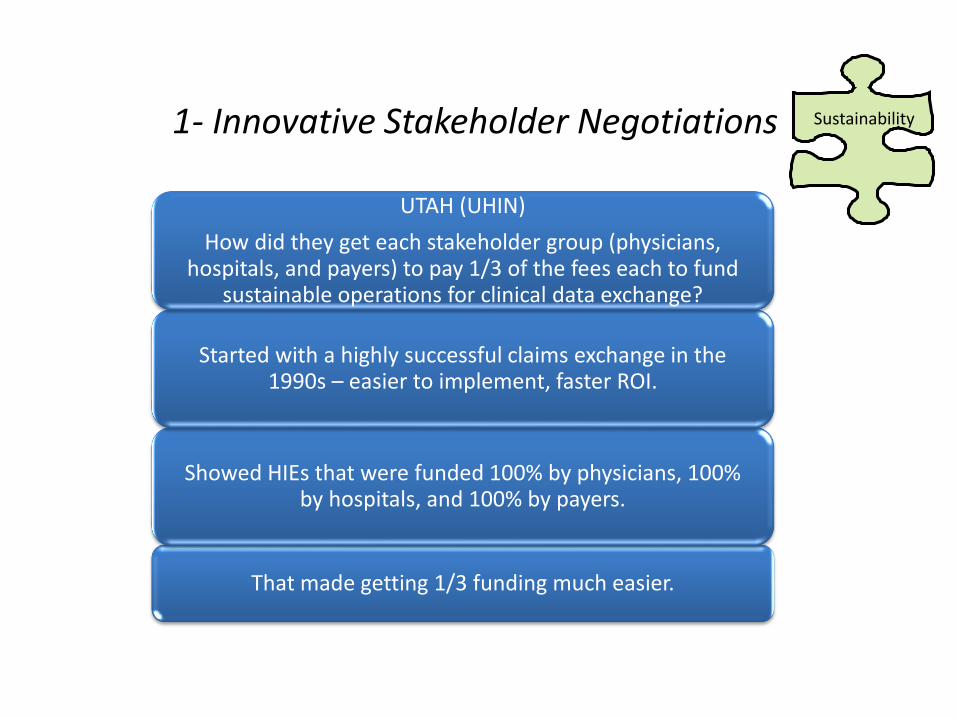
1- Innovative Stakeholder Negotiations
That made getting 1/3 funding much easier.
Showed HIEs that were funded 100% by physicians, 100% by hospitals, and 100% by payers.
Started with a highly successful claims exchange in the 1990s – easier to implement, faster ROI.
UTAH (UHIN)
How did they get each stakeholder group (physicians, hospitals, and payers) to pay 1/3 of the fees each to fund
sustainable operations for clinical data exchange?
Sustainability

2 - Establishing the Right Relations
New York (Rochester RHIO)
Budget is covered 2/3 by payers and 1/3 by hospitals.
Instead of being charged a RHIO fee, payers are assessed
a hospital fee at patient discharge to cover RHIO costs. The hospital then uses these
funds to pay fees to the RHIO.
PayersHospitals

3- Driver of Sustainability is Physician Adoption!
Secret to Sustainability? Common clear voice –
Inland Northwest, MedVirginia, HealthBridge,
Franciscan HIE
Priority on giving the leadership physicians the
services they want
Low cost of entry – no charge for clinical messaging & inquiry (CCD); charge for
add-ons
Physicians are primary outreach arm
Physicians will pay for value
(Inland Northwest)
Physicians

4 - Bringing Payers & Providers Together
Indiana (IHIE)
• Quality Health First – uses HIE’s access to both clinical and claims data for performance reporting
• 5 payers, 1400 physicians
Minnesota (MN HIE)
• 6 institutions are able to populate patient data for 84% of the residents in the state
• Joint sponsorship for 3-year start up
• 3 hospitals, 2 health plans and state government
• Why? Avoid the mistakes of the claims system
Providers
Payers

5 - Innovative Sources of Fees
Michigan (Capital Area RHIO with help from state-level MiHIN)
• Medicaid
• Michigan Office of State Employees
• Michigan Office of State Retirees
• Board membership
• Public health surveillance & alerts
• University research
Minnesota (MI HIE)
• Clinics
• Long-term care
• Public health
• School districts
Demographics
Other Resources
Govt.
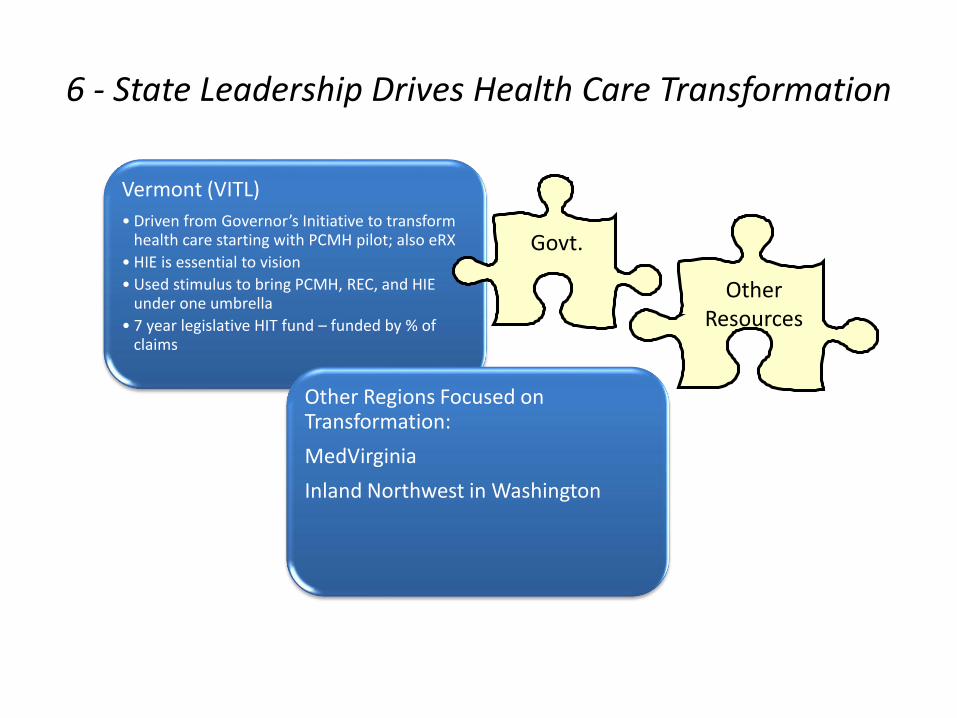
6 - State Leadership Drives Health Care Transformation
Vermont (VITL)
• Driven from Governor’s Initiative to transform health care starting with PCMH pilot; also eRX
• HIE is essential to vision
• Used stimulus to bring PCMH, REC, and HIE under one umbrella
• 7 year legislative HIT fund – funded by % of claims
Other Regions Focused on Transformation:
MedVirginia
Inland Northwest in Washington
Govt.
Other Resources
7 - Longer-term HIEs Look to the Future
Have a vision and strategy for
transformation
• HIEs as component of integrated care
Large data bases• Legacy system “took years
to develop”
• Can support ACOs, PCMH, care coordination programs,
transitions of care, work redesign, population-level outcome measures, etc.
Federal funding to finance growth
• Beacon, REC, SSA, VA, DoD, CMS, CDC, NHIN, etc.
Putting it all together!
• Government
• Hospitals
• Payers
• Physicians
• Sustainability
• Demographics
• Other Resources

What does the future holds?
Aging Demographics Chronic Disease Rising Costs
Provider Shortage
•Baby Boomer Retirements
•Lack of Primary Care Physicians
Patient/Consumer Demands
• Increased Physician-Patient Communications
Legislative Demands
•Meaningful Use
•ACO
•Privacy & Security
25
Taking HIE to the Next Level:Transforming Care Delivery
26
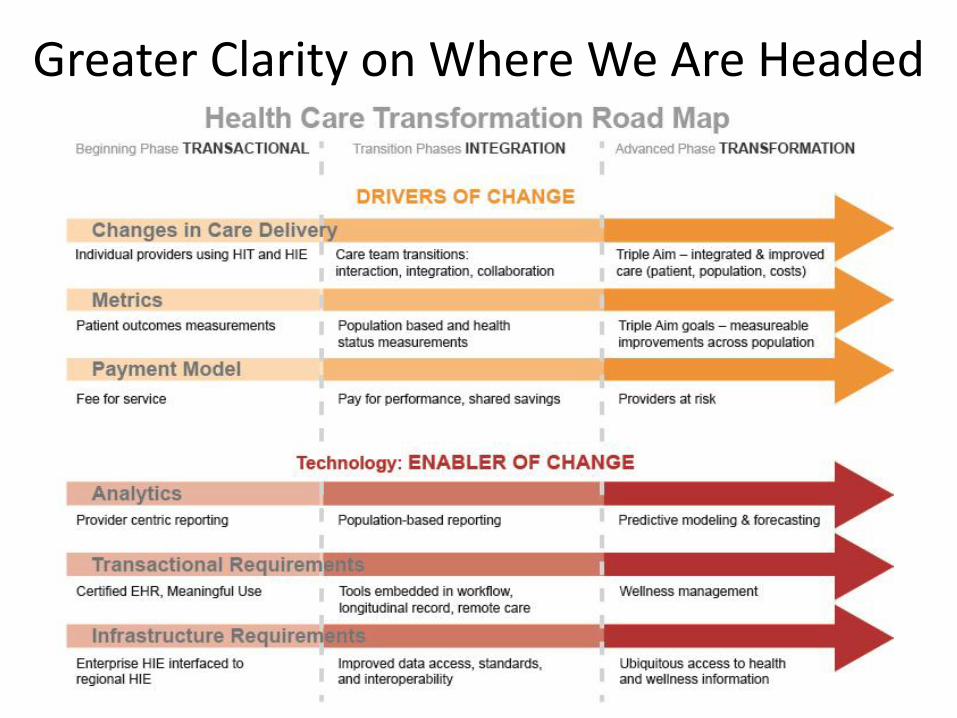
Greater Clarity on Where We Are Headed
8/16/201527
• How did HC Transformation Road Map influence outreach strategy?– April 25, 2012 HealthBridge announces HIE to expand
quality improvement analytics
– First customer, Quality Health Network (W. Colorado)
– Key tools• Infrastructure enhancement to support expanded data
exchange & large data sets – secure & accurate integration
• Analytics engines – ID gaps in care
• Business intelligence -- manage resources, risk, quality, utilization
• Reporting tools – slice & dice data, multiple reporting req.
8/16/201528
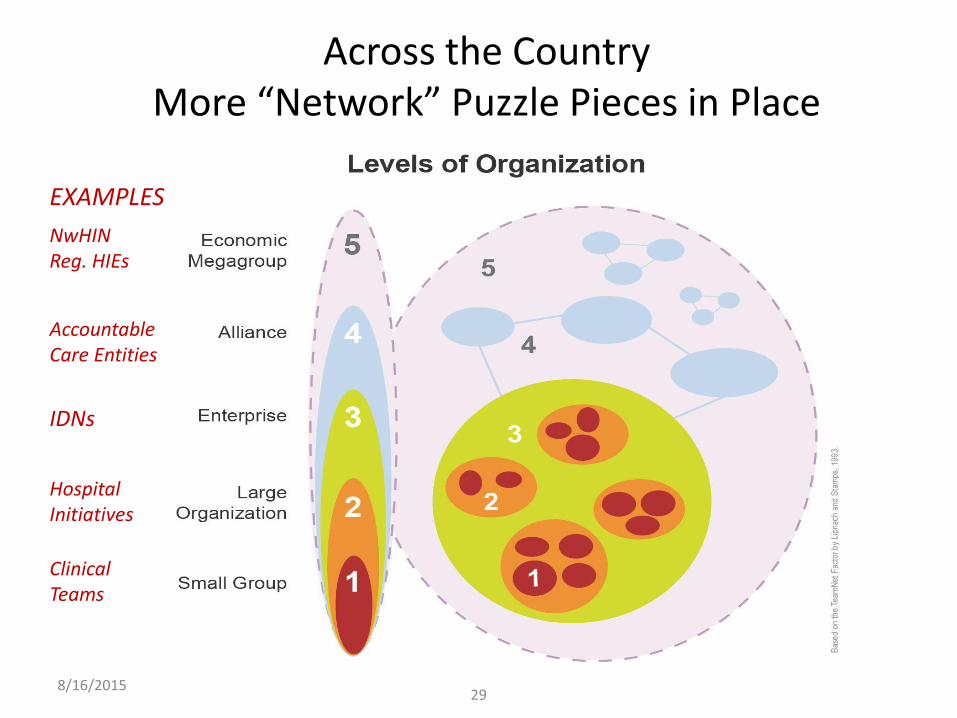
Across the CountryMore “Network” Puzzle Pieces in Place
8/16/201529
EXAMPLES
Accountable Care Entities
IDNs
HospitalInitiatives
Clinical Teams
NwHINReg. HIEs

Network Relationships – Key Points
• Change happens at multiple levels
• All levels are interconnected
• This has accelerated
• More puzzle pieces being filled in – remaining gaps become obvious
• More people see opportunity and resources are mobilized
• Greater competition; “arrow in the back”
8/16/201530
WHIO – Health Analytics Exchange
Transformation opportunities and risks for Wisconsin given WHIO, HITECH and HC reform?
• State-wide claims exchange – includes nearly all payers, Med Society, Hospital Association, and 5 health systems
• Participants can compare quality outcomes across all other participants using de-identified data
• Processes and policies in place to agree to– Measures– Access to data– Consensus-based decision making process
8/16/201531

Transformation opportunities and risks?
• Common management for QIO, REC, and HIE • QIO highly respected by hospitals, other stakeholders• REC very successful working with docs• HIE – key players with live data in short time frame; others in queue• Three long-standing ACO look-alikes – hospital, 2 practices• Major payer has majority of private market, wants transformation• Consortium of self-insureds also major player (e.g. casinos)• Many practices very high-level of IT adoption• Yet, high level of paper-based practices of 1-2 docs, hard to reach• State ranks near bottom of health outcomes nationally
8/16/201532

HealthLINC, Bloomington, INWhat Are Opportunities & Risks?
– Small innovative HIE serving South Central Indiana
– Surrounded by 5 sustainability HIEs
– High-level MD adoption, MU
– Starting care coord. model with self-insured employer
– Planning ED alerts for behavioral health
– Parent health system working on system-wide ACO
– Will have access to data and analytics of nation’s two largest HIEs
8/16/201533

Physicians in Michigan: Should We Join Health System Networks? As Employees?
Opportunities and Risks?
– BCBS Systems of Care Program with P4P – around 36 groups, 5,000 physicians
– Other health plans also
– 42,000 licensed physicians
– MiHIN Shared Services will link 6+ HIEs
– University Medical Center tells physicians: “You will use HIE”
– Health systems actively recruiting employed physicians
8/16/201534
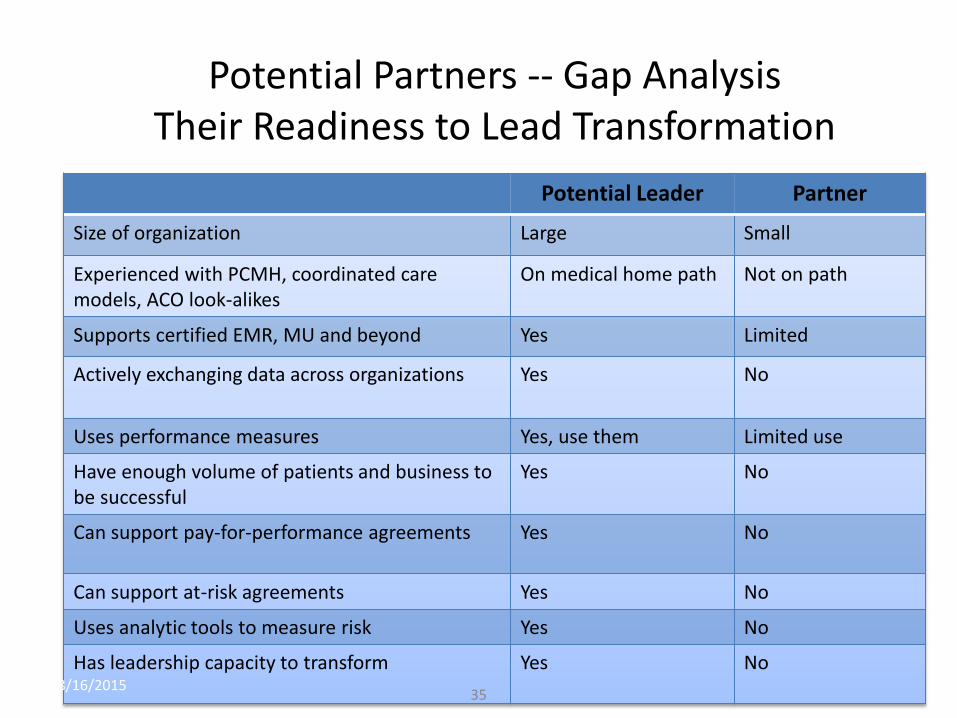
Potential Partners -- Gap AnalysisTheir Readiness to Lead Transformation
Potential Leader Partner
Size of organization Large Small
Experienced with PCMH, coordinated care models, ACO look-alikes
On medical home path Not on path
Supports certified EMR, MU and beyond Yes Limited
Actively exchanging data across organizations Yes No
Uses performance measures Yes, use them Limited use
Have enough volume of patients and business to be successful
Yes No
Can support pay-for-performance agreements Yes No
Can support at-risk agreements Yes No
Uses analytic tools to measure risk Yes No
Has leadership capacity to transform Yes No8/16/2015
35
Regional Network Puzzle PiecesNew Jersey, Delaware Valley, & Delaware
What are Opportunities and Risks?– HIEs – Foundation Being Built
• DHIN – one of original in US -- 90% Adoption-Immunization Sharing• Pennsylvania eHealth Collaborative-Authority Approved-130+ Stakeholders• NJ Health Information Network
– Regional Extension Centers -- achieving goals in all three regions• New Jersey –6157 members, 4120 live on EHR, 1128 Meaningful Users • PA REACH East – 3351 members, 2466 live on HER, 1164 Meaningful Users• Quality Insights of DE – 1375 members, 1239 live on EHR 1239, 349 Meaningful Users
– ACOs – Building Transformation Models• Renaissance Health Network (SE Pennsylvania)• Barnabas Health ACO-North (New Jersey)• 140+ Formed across USA
– Other Successes• ACO look-alikes• IDN, Private and Community HIEs• PCMH and other patient-centric models• Quality initiatives-Chronic Disease-Immunization • Consumer, payer, other stakeholder engagement• Mobile devices, broad band, telemedicine and more• Direct/HISPs-PA providing funding• Other?
36
Thank You!
PAeHI Team
Chris Cavanaugh, EdD, Executive Director
William (Buddy) Gillespie, Chair BCX Committee
Sharon Dorogy, Chair, PAeHI
Ken Coburn, MD, Co-Chair HIE Committee
Steven Fox, JD, Chair Policy Committee
Robert Torres, State HIT Coordinator
www.paehi.org
New Heights Consulting and Strategies for Tomorrow
Camilla Hull Brown, MBA, Principal & Founder, Strategies for Tomorrow, Inc.
Denise Reeser, MBA, Managing Principal, New Heights Consulting, LLC
Presentation for
Making Magic with Medicine, Technology, and Innovation Conference
New Jersey and Delaware Valley HIMSS Chapters
October 4-5, 2012
© 2012 PAeHI 37