CALL ME PORC BUTT · dentist s name _____ phone # _____ dentist s address _____
1
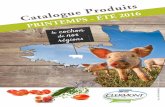
DENTIST’S NAME ________________________________________________________________________ PHONE # _______________________________________________________________________________ DENTIST’S ADDRESS _____________________________________________________________________ CITY, STATE, ZIP _________________________________________________________________________ PATIENT’S NAME ______________________________ SEX M F AGE _______________________________ RX DATE _____________________________________ DUE DATE PORCELAIN TO METAL o Porcelain to Noble o Porcelain to High Noble (white alloy) o Porcelain to High Noble (yellow alloy) o Captek METAL FREE o FYZ • Full Zirconia o E-max - Monolithic o Press to Zirconia o Empress HD (Layered) o E-max HD (Layered) o Procera Allceram o Porcelain to Zirconia COMPOSITES o Premise Indirect FULL METAL CROWNS o Elite 80 type II HN o Premium 50 III N o Elite 60 type III HN o Econo-Gold 20 IV N Instructions: A copy of this form must be retained in the dental laboratory office and the dentists’ office for a period of 2 years. B C E H J K N Visible Design Chart _______________________________________________________ _______________________________________________________ DOCTOR’S SIGNATURE DDS/DMD LICENSE # ORIGINAL SHADE A G M L DAY BEFORE PATIENTS’ S APPOINTMENT o PORC BUTT - MARGIN o CALL ME 1 2 3 4 5 6 7 16 8 9 10 11 12 13 14 15 MAXILLARY 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 MANDIBULAR OCC STAIN o None o Light o Med o Dark o Decalcification PONTIC DESIGN (CIRCLE) MODIFIED RIDGE LAP HYGIENIC CONICAL 16280 westwoods business park • ellisville, mo 63021 (636) 227-0186 • (888) 868-3724 o Images To Be Emailed To [email protected] NEW NEW
Transcript of CALL ME PORC BUTT · dentist s name _____ phone # _____ dentist s address _____

Dentist’s name ________________________________________________________________________
Phone # _______________________________________________________________________________
Dentist’s aDDress _____________________________________________________________________
City, state, ziP _________________________________________________________________________
Patient’s name ______________________________
sex m F age _______________________________
rx Date _____________________________________
due date
Porcelain to metalo Porcelain to Nobleo Porcelain to High Noble (white alloy)o Porcelain to High Noble (yellow alloy)o Captek
metal freeoFYZ • Full Zirconiao E-max - Monolithic o Press to Zirconiao Empress HD (Layered) o E-max HD (Layered)o Procera Allceram oPorcelain to Zirconia
comPositeso Premise Indirect
full metal crownso Elite 80 type II HN o Premium 50 III No Elite 60 type III HN o Econo-Gold 20 IV N
Instructions:
A copy of this form must be retained in the dental laboratory office and the dentists’ office for a period of 2 years.
B C e
H J K
N
Visible Design Chart
_______________________________________________________ _______________________________________________________
DoCtor’s sIGNAturE DDs/DMD LICENsE #orIGINAL
sHADE
a
G
ML
Day Before Patients’s aPPointment
o Porc Butt - MArGIN
o call me
1
2
3
45
67
16
8 9 1011
12
13
14
15
MaxILLarY
17
18
19
20
2122
2324252627
2829
30
31
32
MaNDIBULar
oCC stAINo None
o Light
o Med
o Dark
o Decalcification
PoNtIC DEsIGN (CIrCLE)
MODIFIeDrIDGe LaP
HYGIeNICCONICaL
16280 westwoods business park • ellisville, mo 63021(636) 227-0186 • (888) 868-3724
oImages To Be Emailed To [email protected]
NeW
NeW
Dentist’s name ________________________________________________________________________
Phone # _______________________________________________________________________________
Dentist’s aDDress _____________________________________________________________________
City, state, ziP _________________________________________________________________________
Patient’s name ______________________________
sex m F age _______________________________
rx Date _____________________________________
due date
Porcelain to metalo Porcelain to Nobleo Porcelain to High Noble (white alloy)o Porcelain to High Noble (yellow alloy)o Captek
metal freeoFYZ • Full Zirconiao E-max - Monolithic o Press to Zirconiao Empress HD (Layered) o E-max HD (Layered)o Procera Allceram oPorcelain to Zirconia
comPositeso Premise Indirect
full metal crownso Elite 80 type II HN o Premium 50 III No Elite 60 type III HN o Econo-Gold 20 IV N
Instructions:
A copy of this form must be retained in the dental laboratory office and the dentists’ office for a period of 2 years.
B C e
H J K
N
Visible Design Chart
_______________________________________________________ _______________________________________________________
DoCtor’s sIGNAturE DDs/DMD LICENsE #orIGINAL
sHADE
a
G
ML
Day Before Patients’s aPPointment
o Porc Butt - MArGIN
o call me
1
2
3
45
67
16
8 9 1011
12
13
14
15
MaxILLarY
17
18
19
20
2122
2324252627
2829
30
31
32
MaNDIBULar
oCC stAINo None
o Light
o Med
o Dark
o Decalcification
PoNtIC DEsIGN (CIrCLE)
MODIFIeDrIDGe LaP
HYGIeNICCONICaL
16280 westwoods business park • ellisville, mo 63021(636) 227-0186 • (888) 868-3724
oImages To Be Emailed To [email protected]
NeW
NeW
Dentist’s name ________________________________________________________________________
Phone # _______________________________________________________________________________
Dentist’s aDDress _____________________________________________________________________
City, state, ziP _________________________________________________________________________
Patient’s name ______________________________
sex m F age _______________________________
rx Date _____________________________________
due date
Porcelain to metalo Porcelain to Nobleo Porcelain to High Noble (white alloy)o Porcelain to High Noble (yellow alloy)o Captek
metal freeoFYZ • Full Zirconiao E-max - Monolithic o Press to Zirconiao Empress HD (Layered) o E-max HD (Layered)o Procera Allceram oPorcelain to Zirconia
comPositeso Premise Indirect
full metal crownso Elite 80 type II HN o Premium 50 III No Elite 60 type III HN o Econo-Gold 20 IV N
Instructions:
A copy of this form must be retained in the dental laboratory office and the dentists’ office for a period of 2 years.
B C e
H J K
N
Visible Design Chart
_______________________________________________________ _______________________________________________________
DoCtor’s sIGNAturE DDs/DMD LICENsE #orIGINAL
sHADE
a
G
ML
Day Before Patients’s aPPointment
o Porc Butt - MArGIN
o call me
1
2
3
45
67
16
8 9 1011
12
13
14
15
MaxILLarY
17
18
19
20
2122
2324252627
2829
30
31
32
MaNDIBULar
oCC stAINo None
o Light
o Med
o Dark
o Decalcification
PoNtIC DEsIGN (CIrCLE)
MODIFIeDrIDGe LaP
HYGIeNICCONICaL
16280 westwoods business park • ellisville, mo 63021(636) 227-0186 • (888) 868-3724
oImages To Be Emailed To [email protected]
NeW
NeW
Dentist’s name ________________________________________________________________________
Phone # _______________________________________________________________________________
Dentist’s aDDress _____________________________________________________________________
City, state, ziP _________________________________________________________________________
Patient’s name ______________________________
sex m F age _______________________________
rx Date _____________________________________
due date
Porcelain to metalo Porcelain to Nobleo Porcelain to High Noble (white alloy)o Porcelain to High Noble (yellow alloy)o Captek
metal freeoFYZ • Full Zirconiao E-max - Monolithic o Press to Zirconiao Empress HD (Layered) o E-max HD (Layered)o Procera Allceram oPorcelain to Zirconia
comPositeso Premise Indirect
full metal crownso Elite 80 type II HN o Premium 50 III No Elite 60 type III HN o Econo-Gold 20 IV N
Instructions:
A copy of this form must be retained in the dental laboratory office and the dentists’ office for a period of 2 years.
B C e
H J K
N
Visible Design Chart
_______________________________________________________ _______________________________________________________
DoCtor’s sIGNAturE DDs/DMD LICENsE #orIGINAL
sHADE
a
G
ML
Day Before Patients’s aPPointment
o Porc Butt - MArGIN
o call me
1
2
3
45
67
16
8 9 1011
12
13
14
15
MaxILLarY
17
18
19
20
2122
2324252627
2829
30
31
32
MaNDIBULar
oCC stAINo None
o Light
o Med
o Dark
o Decalcification
PoNtIC DEsIGN (CIrCLE)
MODIFIeDrIDGe LaP
HYGIeNICCONICaL
16280 westwoods business park • ellisville, mo 63021(636) 227-0186 • (888) 868-3724
oImages To Be Emailed To [email protected]
NeW
NeW