

Cadth 2015 d4 masuccietalp codr cadth_10april2015_final
15
Pharmacoeconomics Research Unit RESEARCH. DECISION SUPPORT. KNOWLEDGE TRANSLATION. CAPACITY BUILDING. Assessment of the pan-Canadian Oncology Drug Review Economic Evaluations Lisa Masucci 1 , Jaclyn Beca 1,2 , Mona Sabharwal 3 , Jeffrey Hoch 1,2,4 St. Michael’s Hospital 1 , Cancer Care Ontario 2 , pan-Canadian Oncology Drug Review 3 , University of Toronto 4 CADTH Symposium April 14 th , 2015
-
Upload
cadth-symposium -
Category
Health & Medicine
-
view
43 -
download
2
Transcript of Cadth 2015 d4 masuccietalp codr cadth_10april2015_final

Pharmacoeconomics Research UnitRESEARCH. DECISION SUPPORT. KNOWLEDGE TRANSLATION. CAPACITY BUILDING.
Assessment of the pan-Canadian Oncology
Drug Review Economic Evaluations
Lisa Masucci1, Jaclyn Beca1,2, Mona Sabharwal3, Jeffrey Hoch1,2,4
St. Michael’s Hospital1, Cancer Care Ontario2, pan-Canadian Oncology Drug Review3, University of Toronto4
CADTH Symposium
April 14th, 2015

Background I
• Expenditures on oncology drugs account for a large proportion of
health care spending and this trend is expected to increase.
• As health care budgets are limited, decision makers are faced with
difficult decisions of what drugs to fund over others.
• Canada has created a separate reimbursement review process.
Background II
• The pan-Canadian Oncology Review (pCODR) was established in
2011 to assess cancer drugs and make recommendations to provinces
and territories (except Quebec) to guide their funding decisions.
• pCODR uses a deliberative framework and takes into consideration
the drug’s overall clinical benefit, cost-effectiveness, alignment with
patient values, and feasibility of adoption into health systems.
• The submitter provides an economic evaluation of the drug and
economic reviewers review the submitted model. As part of their
guidance to the committee, they may make modifications to the
submitters’ estimates.
Objectives
• To identify and examine the main methodological issues frequently
reported in pCODR economic guidance reports.
• To explore relationships between reported methodological issues and
funding recommendations.

Methods I
• Publicly available Economic Guidance Reports were searched:
• Published between July 2011 (inception) and June 2014
• Had a final funding recommendation (34 reviews, 39 indications)
• Independently examined by two study authors
• Both study authors abstracted the major issues found within the
reports and together grouped them into types.
• Each issue was also categorized based on the economic reviewer’s
actions.

Methods II
• We collected final funding recommendations.
• We assessed relationships between each main issue and the funding
recommendations by exploring the data visually and with Fisher’s
exact tests.
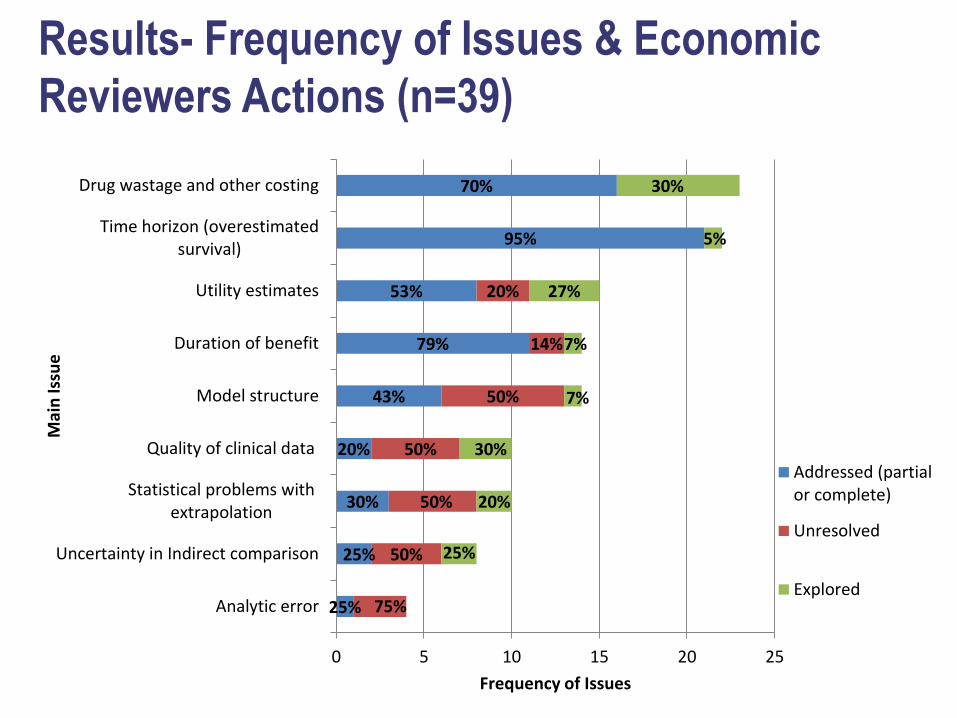
Results- Frequency of Issues & Economic
Reviewers Actions (n=39)
25%
25%
30%
20%
43%
79%
53%
95%
70%
50%
50%
50%
50%
14%
20%
75%
25%
20%
30%
7%
7%
27%
5%
30%
0 5 10 15 20 25
Analytic error
Uncertainty in Indirect comparison
Statistical problems withextrapolation
Quality of clinical data
Model structure
Duration of benefit
Utility estimates
Time horizon (overestimatedsurvival)
Drug wastage and other costing
Frequency of Issues
Mai
n Is
sue
Addressed (partialor complete)
Unresolved
Explored

Results- Funding Recommendation Type (n=39)

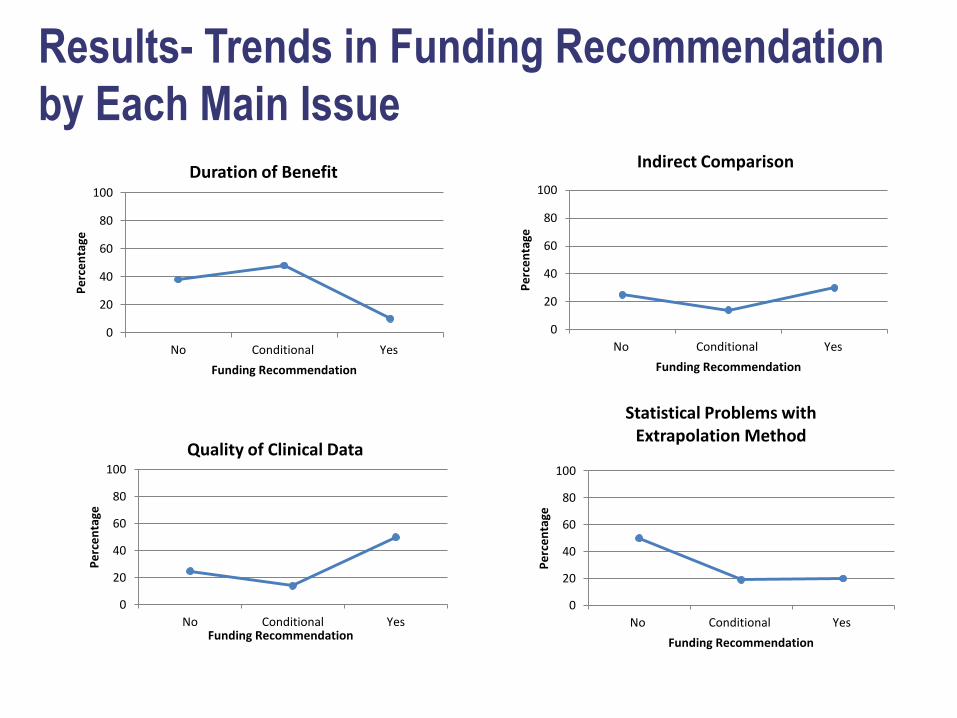
Results- Trends in Funding Recommendation
by Each Main Issue
*Interpretation example: among the reviews that were not recommended, 87% mentioned an issue with time horizon (i.e., overestimated survival) in the economic guidance report
0
20
40
60
80
100
No Conditional Yes
Pe
rce
nta
ge
Funding Recommendation
Time Horizon(overestimated survival)
0
20
40
60
80
100
No Conditional Yes
Pe
rce
nta
ge
Funding Recommendation
Model Structure

Results- Trends in Funding Recommendation
by Each Main Issue
0
20
40
60
80
100
No Conditional Yes
Pe
rce
nta
ge
Funding Recommendation
Drug Wastage & Other Costing
0
20
40
60
80
100
No Conditional Yes
Pe
rce
nta
ge
Funding Recommendation
Utility Estimates

Interpreting graphs
• Does this mean time horizon influences the recommendation while
drug wastage does not? No!
• Why not? We are not considering whether the reviewer could
modify/explore/improve the estimates. Not accounting for the ICER.
Not accounting for other factors in the deliberative framework.
These are just observational correlations.
Results- Trends in Funding Recommendation
by Each Main Issue
0
20
40
60
80
100
No Conditional Yes
Pe
rce
nta
ge
Funding Recommendation
Indirect Comparison
0
20
40
60
80
100
No Conditional Yes
Pe
rce
nta
ge
Funding Recommendation
Quality of Clinical Data
0
20
40
60
80
100
No Conditional Yes
Pe
rce
nta
ge
Funding Recommendation
Statistical Problems with Extrapolation Method
0
20
40
60
80
100
No Conditional Yes
Pe
rce
nta
ge
Funding Recommendation
Duration of Benefit

Limitations
• Small sample size (n=39)
• We only examined publicly available documents and we did not
gather additional information from the manufacturers, economic
reviewers or the committee to clarify interpretations or assess the
importance of each issue to the review.
• There are other major factors that are considered in forming each
recommendation - clinical benefit, alignment with patient values, and
adoption feasibility into the health care system.

Conclusion
• Many of the submissions had issues reported by reviewers related to
time horizon, drug wastage & other costing, and utility estimates;
however, the majority of time these issues could be addressed
(partially or completely).
• Issues that were frequently reported but could often not be resolved
by the economic reviewer were model structure and extrapolation
issues, as well as the quality of clinical and comparative data
informing the analysis.
• For future research similar work could be conducted in other disease
areas besides cancer.


















