CADASIL vs HYPERTENSIVE MICROANGIOPATHY
28
Case discussions Dr Subhash Kumar MD, DM Associate Consultant ‐Neuroradiology
-
Upload
subhash-kumar -
Category
Documents
-
view
81 -
download
1
description
A case of dementia with multiple microbleeds in the brain, skin biopsy was negative for CADASIL
Transcript of CADASIL vs HYPERTENSIVE MICROANGIOPATHY

Case discussions
Dr Subhash Kumar MD, DM Associate Consultant ‐Neuroradiology

65 years old male HTN Seizures Dementia, abnormal behavior Left hemiparesis P/C: RT sided seizures




Hypertensive microangiopathy CADASIL

Waxing –waning neurological deficits Cortical involvement Hemorrhage Infarcts of various ages, various locations


Defined radiologically as small,rounded, homogeneous, hypointense lesions on T2*
Not seen on routine CT or MRI Due to tiny bleeds adjacent to abnormal small vessels, being mainly affected by hypertensive angiopathy (arteriolosclerosis – usually lipohyaline degeneration related to hypertension) or cerebral amyloid angiopathy (CAA)







Andreas Charidimou, Qiang Gang, David J Werring. Sporadic cerebral amyloid angiopathy revisited: recent insights into pathophysiology and clinical spectrum. J Neurol Neurosurg Psychiatry 2012;83:124e137. doi:10.1136/jnnp‐2011‐301308

Recurrent ischemic episodes Cognitive deficits Migraine mostly with aura Psychiatric disorders Seizures

mutations in the Notch3 gene unique type of nonarteriosclerotic, amyloid‐negative angiopathy involving small arteries and capillaries primarily in the brain but also in other organs
Characteristic granular osmiophilic material within the vascular basal lamina, which is often seen in close association with vascular smooth muscle cells
Vascular smooth muscle cells have been shown to degenerate and eventually disappear

Diffuse white matter hyperintensities on T2 and FLAIR weighted images Subcortical white matter Basal ganglia
Changes on MRI may be evident in persons who are in their 20s Penetrance complete by age 35 and all will have MRI findings
The syndrome may not be suspected until affected individuals are in their 50s or older
Lesion volume is inversely correlated with cognitive function

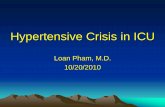
Axial FLAIR images 59 yr old woman Multiple confluent hyperintensities in deep and periventricular white matter


Van Der Boom et al. http://www.ajnr.org/cgi/content‐nw/full/27/2/359/F1

most petechial hemorrhages occur independently from ischemic lesions in CADASIL
clinical implications of MBs in CADASIL are unknown; from large patient series, there is no evidence of an increased frequency of hemorrhagic stroke

Charles André. Arq Neuropsiquiatr 2010;68(2):287‐299

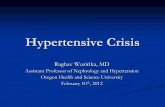
MRI shows microbleeds in a patient with CADASIL.
et al. Neurology 2001;57:941-942
©2001 by Lippincott Williams & Wilkins

Antiplatelet therapy Investigate for other causes of stroke (cardiac, afib, hypercoag state, etc.)
Cholinesterase inhibitors Work in vascular dementia
Screen for mood disorders, cognitive decline, seizure
Life expectancy may be shortened by 6 years

Control vascular disease risk factors ▪ BP ▪ Increased SBP independent risk factor for progression of CADASIL
▪ Cholesterol ▪ DM ▪ Smoking ▪ Obesity ▪ Avoid OCP, HRT

Jacqueline A. Pettersen et al. Arch Neurol. 2008;65(6):790‐795