InstallationDirective N45 MNA M10 N67 MNA M15 P3D64N003E May06

Reviews in Clinical Gerontology 2007 17; 293–310C! 2008 Cambridge University Press Printed in the United Kingdom doi:10.1017/S095925980800258X
The Mini Nutritional Assessment (MNA) after20 years of research and clinical practiceMarion Secher,1 Maria E Soto,1 Helene Villars,1 Gabor Abellan van Kan1 and Bruno Vellas1,2
1Gerontopole Department of Geriatric Medicine, Toulouse University Hospital, France and 2Inserm, U558,University Toulouse III, F-31073, Toulouse, France
Introduction
Nutritional assessment in older people to detectmalnutrition or risk of malnutrition is essentialto avoid adverse nutrition-related outcomes. Poornutritional status appears to be a major contrib-uting factor for poor prognosis in malnourishedindividuals. Nowadays, nutritional assessment isconsidered to be one of the domains which shouldbe evaluated in comprehensive geriatric assessment(CGA). CGA is a comprehensive assessment toolwith the capacity of detecting impairments in olderpeople and, at the same time, suggest interventions.Although many assessment tools are proposed,those used in CGA are not widely agreed. After20 years of clinical practice and research, theMini Nutritional Assessment (MNA) seems to bethe tool most widely accepted by health carersand patients for the assessment of nutritionalimpairment in CGA.
MNA classifies, with well-established thresh-olds, the nutritional status of older people withthe added advantage of proposing and guidinginterventions. Even more, the MNA is correlated tonutritional interventions when these are successful,with improved scores showing response to theintervention.
Several studies have shown that older peopleat risk of or suffering malnutrition have aworse prognosis in terms of different adverseclinical outcomes. In community-dwelling elderlypeople, malnutrition is associated with diminishedcognitive and functional performance, diminishedself-care ability,1,2 worse oral health, poor eyesightand several difficulties with mealtimes such asproblems in using a fork or a knife.3 In hospitalizedpatients, depression scores (using the Geriatric
Address for correspondence: Gabor Abellan vanKan, Gerontopole Department of Geriatric Medicine,University Hospital Toulouse, 170 avenue de Casselardit,31059 Toulouse cedex 9, France.
Depression Score) were higher in malnourishedpatients than in those who were at risk.4 Manystudies have shown that low MNA scores arepredictive of adverse outcomes, including longerlengths of hospital stay, more frequent dischargesto a nursing home and a nearly threefold increasein mortality.4–8 Weight loss and malnutrition aremajor complications of Alzheimer’s disease (AD).9
After a one-year follow-up of community-dwellingelderly patients suffering from Alzheimer’s di-sease, lower nutritional status, measured by theMNA, was found to be associated with risk of insti-tutionalization, and lower MNA scores were foundin emergency hospital admissions.10,11
The aim of the present paper was toperform an exhaustive review on the MNA byrevising the relevant literature on the topic aftermore than 20 years of research and clinicalpractice.
Historical background
The development of the MNA began during the1989 International Association of Geriatrics andGerontology (IAGG) meeting in Acapulco with adiscussion between Bruno Vellas (Department ofGeriatric Medicine, Toulouse University Hospital,France) and Yves Guigoz (Researcher at the NestleResearch Centre, Switzerland). This meeting high-lighted that even if there was proven evidence ofthe high prevalence of malnutrition in institutional-ized, frail and hospitalized older people, nutritionalassessment was not currently performed in clinicalpractice due to the complexity of nutritionalevaluation. The aim of the discussion was to designan assessment tool for nutritional status in olderpeople, analogous to the Mini-Mental State Ex-amination (MMSE) for the assessment of cognitivefunction,12 reliable, cheap and quick to perform.
The MNA was initially validated in a cohort ofmore than 150 healthy, frail and acutely ill elderly

294 M Secher et al.
patients in Toulouse, France, between 1990 and1991.13 Subsequently, the MNA was validated inthe New-Mexico Aging Process Study (NMAPS), alongitudinal survey on nutrition and aging and in2001 by the Nestle Research Centre in Lausanne(Switzerland). Thus the MNA was validated,in three studies assessing more than 600 olderpersons, using two principal validation criteria: (1)Clinical status, which consisted of a nutritionalassessment conducted independently by two phys-icians trained in nutrition, on the basis of the sub-ject’s clinical record without the knowledge of theMNA result; and (2) a comprehensive nutritionalassessment which included a complete assessmentof anthropometrics, biochemical markers such asvitamins, trace minerals and proteins status, and acomplete three-day dietary intake record.
The first article, that included the MNA forthe assessment of nutritional status, was publishedin 1994.14 In 2001, a short form of the MNA(MNA-SF) was developed in collaboration withL.Z Rubenstein.15 The MNA-SF is a validatedshortened version of the MNA, allowing a two-step screening process in low-risk populationsthat retains the validity and accuracy of the fullMNA. Since 1994, the MNA has been translatedinto almost 20 languages and has been usedfor nutritional evaluation in nearly 200 scientificpublications in PubMed/Medline. Many articleshave evaluated the sensitivity, specificity andreliability of the MNA in different settings andcountries. In both medical practice and clinicalresearch, the MNA is by far the most widely usedtool for nutritional screening and assessment inolder people.
The MNA: description of the tool
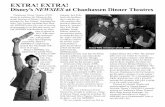
The MNA is able to classify older peopleas well nourished, at risk for malnutrition ormalnourished. The MNA consists of 18 self-reported questions derived from four parametersof assessment: anthropometric assessment, generalassessment, dietary assessment and self- assessment(see Figure 1) administered in two steps. TheMNA-SF is a screening tool composed of thefirst six items (of the 18 questions) that permitsdetection of a decline in ingestion over thepast three months (loss of appetite, decline offood intake, digestive problems, chewing or swal-lowing difficulties), weight loss in the past
three months, current mobility impairment, anacute illness or major stress in the past threemonths, a neuropsychological problem (dementiaor depression) and a decrease in body mass index(BMI). If indicated after Step 1 (MNA-SF), the riskof malnutrition should be assessed using the fullMNA. The MNA evaluates living arrangements,the presence of polypharmacy or pressure ulcers,the number of full meals eaten daily, the amountand frequency of specific foods and fluids, and themode of feeding. The patient reports nutritionaland health status, and the practitioner determinesweight and height (to calculate BMI), and mid-armand mid-calf circumferences.
As stated earlier, nutritional status using theMNA should be evaluated using a two-stepprocess. The first step, the MNA-SF, takes only fewminutes to complete. The maximum score for thispart is 14; a score of 12 points or greater indicatethat the patient has an acceptable nutritional statusand that it is not necessary to complete the fullMNA. However, a score of 11 points or below isan indication to proceed with the complete versionof the MNA. The full MNA can be performed in 10to 15 minutes. The maximum score for the secondpart is 16. Scores from the two parts must be addedto obtain the malnutrition indicator score. Eachanswer in the two parts has a numerical valueand contributes to the final score, which has amaximum of 30. Assessment of the cognitive statusof the patient should be obtained by the caregiver,or by the medical or nursing staff. If a cognitivedecline is present, answers should be checked byproxies (caregiver, or medical or nursing staff). Ifthe patient suffers from severe cognitive decline,the caregiver or nursing staff can complete theMNA instead. In fact, the physician, dietician, ornurse in charge of an institutionalized patient caneasily complete the MNA with a minimal risk ofbias.
The MNA-SF: a nutritional screening tool
Given the adverse consequences of potential riskof malnutrition or malnutrition, it is clinicallyimportant to detect patients with this condition asearly as possible. In hospitalized older patients, lowMNA scores predict adverse outcomes.16 Thus,earlier identification of hospitalized patients at riskof malnutrition using the MNA-SF could facilitatetimely initiation of nutritional support. Moreover,

Mini Nutritional Assessment after 20 years 295
Figure 1 The Mini Nutritional Assessment (MNA).
MNA-SF can be used as a first step for screeningpreoperative patients,17 and can be used as anefficient screening tool for community-dwellingolder people undergoing CGA.
The MNA-SF maximum score is 14. When thescore of the MNA-SF is greater than 12, thepatient has a satisfactory nutritional status. At this
stage, it is important to give nutritional adviceeven if no signs of malnutrition are present, tofollow the patient’s weight regularly at routinevisits (usually every month) and to complete theMNA-SF at regular intervals (each three or sixmonths), independently of the setting. Nutritionalassessment and eventual intervention should be

296 M Secher et al.
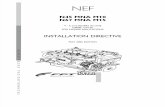
Figure 2 The Mini Nutritional Assessment, MNA, as a diagnostic tool for malnutrition and a guide for nutritionalintervention.
proposed if weight loss is documented. If the scoreis less than 12, the second part of the MNAshould be completed to establish the presence ofmalnutrition and obtain the malnutrition indicatorscore to be used for proposing and afterwardsguiding nutritional interventions.
The MNA: a diagnostic tool
The MNA is a reliable nutritional assessment toolin older people with clearly defined thresholds (seeFigure 2):
1) A score of 23.5 or higher classifies an individualas well-nourished. As mentioned above, andsimilarly, when a score greater of 12 inthe MNA-SF is found, no specific follow-up is needed except to measure the person’sweight regularly at routine visits, complete theMNA at regular intervals and provide generalnutritional counselling. Detailed nutritionalevaluation and, if needed, nutritional interven-tion should be given if significant weight lossis documented or if the MNA score decreasesduring follow-up. In all cases, nutritional adviceshould be based upon the basic rules ofa balanced diet (recalling the recommendedintake frequencies of daily fruits and vegetables,starchy foods, dairy products, meats, fish,products of the sea and eggs, with therecommendation of not over-using fat contentsand sweetened products), to perform regular
daily physical activity and maintain goodhydration.
2) Scores between 17 and 23.5 indicate that anindividual is at risk of malnutrition. Nutritionalintervention is always indicated for an MNA<23.5 and should start as soon as possiblebefore the associated disorders (like functionalimpairment) become irreversible. Based uponCGA, cognitive, functional, nutritional andsocial status of the patient at risk of malnutri-tion should be obtained. A detailed nutritionalevaluation should include the analysis ofa three-day food-intake record, revision ofthe medical history, evaluating previous andcurrent diseases and treatments, checkingoral hygiene and the presence of swallowingimpairment. A specific nutritional interventionprogram should be implemented, based on theimpairments found after assessment by CGAand the MNA (items presenting loss of points).The key benefit of the MNA is that it hasthe capacity to detect older people at riskof malnutrition even before severe changesin weight or in albumin levels occur.18,19
The use of oral supplementation (OS) shouldbe evaluated and could be implementedwhen the risk of malnutrition is present.Concentrated formulas increasing total intakeof calories, proteins or micronutrients, can beused to improve nutritional status. Nutritionalcounselling, as in the previous stage, shouldalways be provided.

Mini Nutritional Assessment after 20 years 297
3) Scores of less than 17 usually indicate thatindividuals have a protein-caloric malnutrition.At this stage, it is important to quantifythe severity of the malnutrition by measuringbiochemical parameters (such as plasma levelalbumin or transthyretin), evaluating a three-day record of food intake and measuringanthropometric features (such as weight, mid-arm and calf-circumference and skinfolds).Nutritional intervention is clearly indicatedand should be based on achievable objectivesestablished after a detailed CGA. No nutritionalintervention should be started without settingspecific and reasonable goals in advance. Itwill be necessary to use the oral route as longas possible by improving the total intake ofcalories and prescribing OS with proteins andmicronutrients when needed.
The MNA: guiding nutritional intervention
The MNA is not only a tool for detecting malnu-trition but it also guides nutritional interventions.Interventional studies with increased food choicesor with nutritional supplements demonstrate thattimely intervention stops weight loss in olderpeople who are at risk of malnutrition orundernourished. Identifying the major contributingcauses of malnutrition and critically reviewingdiet should allow for targeted corrective measures.It is necessary to look carefully at where thepatient loses points on the MNA, and proposeguided interventions in order to correct them.Additionally, the proposed intervention also de-pends on the setting of the patient. In community-dwelling older people, if the person only takestwo meals daily or fewer prepared completemeals, simple corrective measures can be taken,such as providing a nutrition programme, helpingwith shopping and cooking, providing meals-on-wheels, or providing adaptive cooking tools.20–22
Nutritional guidance will be given if patients do notconsume some foodgroups or if they do not drinkenough water. In hospitalized patients, dependingon current disease, those with malnutrition or atrisk of malnutrition can benefit from temporaryOS during the length of the hospitalization. Atdischarge, long-term OS needs specific follow-up and regular reassessment at the outpatientconsultation, taking into account the nutritionalgoals established during hospitalization. In insti-
tutionalized patients, nutritional interventions likesupplements or buffet dining may be effective.23
Implementation of a dietary programme consistingof an increased protein and energy content ofmeals, adapting meals to oral health, additionalhelp during meals, and dietary supplementsbetween meals, may result in improved orstabilized nutritional status and weight gain.24
In institutionalized older people, environmentalchanges, for example using tables that allow thesupervision of more than one resident at a time,can help increase the input of health-care workersat mealtimes.25 A favourable atmosphere, family-style meals and a homelike environment haveproved effective, not only for increasing energyintake and decreasing the risk of malnutrition butalso for maintaining the quality of life, physicalperformance and body weight of nursing-homeresidents, and consequently increasing the MNAscore during the nutritional intervention follow-upif it is proven to be effective.26–28 If patients presentwith pressure ulcers or skin breaks, an increasedintake of calories, proteins and micronutrients withOS will be needed and nutritional interventionguided by the MNA should be implemented.29
Impaired cognitive function makes the need forassistance imperative in all activities of everydaylife, particularly assistance during mealtimes. Incommunity-dwelling older people suffering fromAlzheimer’s disease (AD), home-support services,when needed, should be implemented as soonas possible, even starting at the mild stages ofthe disease, in order to prevent further functionaldecline and prevent institutionalization. As shownby Riviere et al. home-based programmes ofnutritional education for caregivers of AD patientsmay have positive effects on weight and cognitivefunction.30 In institutionalized patients sufferingfrom dementia, behavioural and psychologicalsymptoms, such as exhausting wandering orfood and eating behavioural disorders, should beevaluated as possible causes of malnutrition.31
Nutritional interventions in AD patients have beenshown to reduce morbidity and mortality.32,33
Polypharmacy identified by MNA might be oneof the causes of anorexia and malnutrition.Interventions should be directed to reduce thispolypharmacy if possible. If the patient presentswith anorexia, it will be necessary to search forany possible somatic cause.
The aim of nutritional intervention is to providesufficient nutrients to cover daily needs, using OS

298 M Secher et al.
Table 1. Prevalence of malnutrition in different settings
Clinical Setting % MNA < 17 (malnutrition) % MNA < 23.5 (at risk of malnutrition)
Community-dwelling 1% (range 0–3%)" 29% (range 15–44%)"
2% (range 0–8%)"" 24% (range 8–76%)""
Home Care provided 4% (range 0–13%)" 33% (range 8–63%)"
Outpatients 9% (range 0–30%)"" 45% (range 8–65%)""
Hospitalized 20% (range 7–32%)" 49% (range 25–60%)"
23% (range 1–74%)"" 46% (range 8–63%)""
Institutionalized 37% (range 5–71%)" 44 (range 26–67%)"
21% (range 5–71%)"" 51% (range 27–70)""
"Source: Guigoz et al.20
""Source: Guigoz et al.16
if necessary. As shown by Vellas et al., nutritionalintervention is indicated for an MNA of 23.5or lower and should start as soon as possiblebefore the associated functional decline becomesirreversible.33 In a study performed with a cohortof 573 AD-affected older people, an MNA ofless than 23.5 was associated with an increasedrisk of mortality after two years of follow-up,presenting a relative risk of 2.74 (95%CI 1.58–4.75) and an increased risk of institutionalizationof 1.92 (95%CI 1.24–2.93).33 Many studies haveshown that OS improves biochemical parametersand anthropometric measures in the majorityof malnourished or at risk of malnutritionpatients.34–37 Additionally, in these studies, olderpeople improved or maintained their MNA scoresafter nutritional intervention, suggesting that theMNA can be used for evaluation if nutritional-intervention strategies are successful during thefollow-up period. Thus, the patient’s weight shouldbe assessed monthly and the MNA completedregularly every three months. Moreover, theMNA-guided nutritional intervention has alsodemonstrated to be cost-effective.38,39
The MNA in different clinical settings
Numerous studies have evaluated the prevalenceof malnutrition using the MNA in different clinicalsettings, showing the excellent acceptability andvalidity of the tool in all these settings. Asshown in Table 1, Guigoz et al. evaluated theprevalence of malnutrition and risk of malnutritionin different settings with two systematic revisionsof the literature. The main finding was a ‘setting-related’ prevalence of malnutrition and risk of
malnutrition with huge differences in betweenthe settings.16,20 The large variability resultedmainly from the difference in levels of dependenceand health status among the older people livingin retirement homes, nursing homes, or long-term care facilities. In community-dwelling elderlyindividuals the prevalence of malnutrition (21evaluated studies, n = 14149) was 2% (range 0–8%) and risk of malnutrition was 24% (range8–76%); in outpatient and home-care patients(25 evaluated studies, n = 3119) the prevalence ofmalnutrition was 9% (range 0–30%) and risk ofmalnutrition 45% (range 8–65%); in hospitalizedelderly patients (35 evaluated studies, n = 8596),the prevalence of malnutrition was 23% (range 1–74%) and risk of malnutrition was 46% (range8–63%); in institutionalized elderly patients (32evaluated studies, n = 6821) the prevalence ofmalnutrition was 21% (range 5–71%) and risk ofmalnutrition was 51% (range 27–70%).
Finally, in cognitively impaired older people (11evaluated studies, n = 2051), who were screenedusing the MNA, the prevalence of malnutritionwas 15% (range 0–62%), risk of malnutritionwas 44% (range 19–87%) and well-nourished was41% (range 0–80%).
The MNA as part of Comprehensive GeriatricAssessment
CGA was created to detect disabilities and deficien-cies in older people in order to prevent furtherdecline by implementing interventions that targetedthese deficiencies. It is proven that CGA improvesdiagnostic accuracy and long-term prognosis forelderly patients.40–41 CGA has been used in a

Mini Nutritional Assessment after 20 years 299
variety of settings to detect medical, psychological,social and environmental problems of elderlypeople to identify unmet needs and to preventor treat disability by implementing specificinterventions.42 Initially, nutritional assessmentwas not part of the usual CGA, which includedprimarily assessment of cognitive functions (mostlyby MMSE), assessment of physical performanceby evaluating the activities of daily living (ADL),43
the instrumental activities of daily living (IADL),44
gait and balance impairments using the Tinettiscale,45 and mood was normally assessed usingthe Geriatric Depression Scale (GDS).46 Thecomplexity of nutritional assessment was one of themajor drawbacks for the inclusion of the domainin CGA, even if the presence of malnutrition inthe evaluated geriatric population was important.Since its inception, the MNA has helped to includenutritional assessment in current CGA, due toits applicability and wide acceptance.47,48 At thepresent time, nutritional evaluation, generally as-sessed using the MNA, is an essential part of CGA.
The MNA in clinical research
The MNA has been used in hundred of studiesin a wide range of different settings and in manycountries. Many literature reviews concerningnutritional assessment tools in elderly people, andin particular the MNA, have been published.Guigoz et al. in 2006 published a systematicreview on observational and interventional studiesconcerning nutritional assessments of over 30 000elderly persons.16 It showed that the prevalenceof malnutrition and risk of malnutrition wasrelated to the study setting and was modifiedby the presence of cognitive impairment, butalso that the MNA had excellent acceptance indifferent settings. With the more general use ofthe MNA as a nutritional assessment tool, specificconcerns related to the use of the MNA havebeen evaluated by many studies. Clinical researchinvolving the MNA has proved to be useful forbetter understanding of the physiopathology ofmalnutrition in older people, and much clinicalprogress has been made. Several studies havedemonstrated that the MNA can identify those atrisk for malnutrition before biochemical or weightchanges appear, and also that timely interventioncan stop weight loss in elderly people at riskof malnutrition or already malnourished.18,19
Intervention studies have shown associations withimprovements in MNA scores. The MNA andMNA-SF were found to be sensitive, specific,and accurate in identifying nutritional risk.16
Sieber et al. demonstrated that, 15 years after itsintroduction, the MNA is the gold standard fornutritional assessment in ambulatory community-living elderly people and those in long-termcare facilities. Sieber compared the MNA to theNutrition Risk Screening (NRS).49 Vellas et al.highlighted the usefulness of the MNA, as a simplenutritional assessment tool, in clinical practice tomeasure nutritional status in older people and innutritional intervention follow-up for evaluatingthe success of the intervention.50 Many studiesfound that the MNA was correlated with clinicalnutritional assessment18,20,50 and to objectiveparameters of nutritional status such as serumalbumin,15,51 BMI triceps skinfold,55 caloric intakeand vitamin status.51 Pepersack et al. used theMNA to establish a biochemical threshold for mal-nutrition by evaluating prealbumine (transthyretin)in relation to the MNA score. In the same study,evidence was found that malnutrition detected bythe MNA appeared before an alteration in thebiochemical parameters was present.56 Hudgenset al. evaluated immunity in older people and founda direct relationship between the MNA score andimmunity impairment and also showed that wholeblood lymphocyte proliferation was significantlylower in malnourished older people identified bythe MNA.57 Low MNA scores have also shownto predict a greater incidence of adverse clinicaloutcomes during hospitalization and mortality.8,51
The MNA has been used successfully in manyinterventional studies in patients who are ill orfrail.58,59 The MNA is not only a tool for detectingmalnutrition or risk of malnutrition but it also hasbeen used as guide for nutritional interventions.Finally, many studies have demonstrated thatcognitive functions were associated with lowerMNA or MNA-SF scores and that in patientssuffering from dementia, even in moderate orsevere stages, nutritional education was effective.The MNA appeared to be a valid and acceptedassessment tool for clinical studies involvingdemented patients.33,60 A recent literature reviewconcerning 42 studies with institutionalized olderpeople, performed by Harris et al., compareddifferent nutritional assessment tools.61 BMI wasthe most frequently used parameter for nutritionalassessment (22 studies), followed by the MNA,

300 M Secher et al.
Table 2. Sensitivity and specificity of the MiniNutritional Assessment, MNA, and the MNA short form,MNA-SF, in different clinical settings
MNA SENSITIVITY SPECIFICITY
Harris et al., 200862 89% 90%Ferreira et al., 200863 89% 82%Elkan et al, 200764 84% 36%Kuzuya et al., 200565 81% 86%Delacorte et al., 200466 100% 74,3%Visvanathan et al.,
20046789.5% 87.5%
Guigoz et al., 199568 96% 98%
MNA-SF SENSITIVITY SPECIFICITY
Wikby et al., 200869 89% 90%Charlton et al., 200770 100% 94.6%Kuzuya et al., 200565 85.9% 84%Visvanathan et al.,
20046792.5% 37.8%
Cohendy et al., 200117 85.6% 88.8%Rubenstein et al., 200115 97.9% 100%
MNA = Mini Nutritional Assessment and MNA-SF =Short Form of the MNA.
which was used for nutritional assessment in 12studies. The other assessment tools used were:comparison of the body weight against standardor ideal body weight, weight loss, biochemicalparameters (albumin, prealbumin, transferrin andretinol-binding protein), anthropometric values(mid-arm and calf-circumference, skinfold), andthe Subjective Global Assessment (SGA) tool.According to the MNA, malnutrition was observedin 2%–38% and a risk of malnutrition in 37%–62%. One of the main issues in clinical research isto evaluate whether a nutritional assessment toolhas the capacity to identify malnourished olderpeople as malnourished and normal older people asnormal; in other words evaluate the sensitivity andspecificity of a tool. A high sensitivity is necessaryfor screening tests (MNA-SF) and a high specificityis necessary in order to confirm the diagnosis.Table 2 gives a summary of the sensitivity andspecificity obtained using the MNA and the MNA-SF.15,17,62–70
Tables 3 and 4 summarize recent publicationsof studies performed in community and clinicalsettings and in older persons with specific disease.(Table 3: 62–90; Table 4: 91–102) The studiesusing the MNA provided comparative and compre-hensive data on the prevalence of malnutrition and
risk of malnutrition in clinical settings, includinghospitals and nursing homes, and in communitysettings around the world, and show a very similartrend. The observational studies show the highprevalence of malnutrition and risk of malnutritionin elderly persons especially in hospitalized andinstitutionalized patients.
New challenges for the MNA
MNA offers opportunities in clinical research.As demonstrated in more than 200 publications,the MNA is a very useful tool for clinicalresearch. The International Association of Geron-tology/International Academy of Nutrition andAging (IAGG-IANA) Task Force on MinimumData Set recommended the MNA for nutritionalstudies in elderly patients.103 A recent consensusconcerning research in older people has proposeda tool to harmonize future clinical trials in the fieldof geriatric medicine. This tool, named the GMDS-25, has been created in order to become a referenceminimum data set to be included in all clinicalstudies involving older subjects. It consists of differ-ent parameters of assessment: general parameters,cardiovascular risk factors, functional status,cognitive and psychological status, nutritionalstatus, biological parameters and social status. Thenutritional assessment is based on the MNA-SFfollowed by MNA if at risk, BMI, and weight loss(4% in one year or 5 kg in six months).104
One of the future challenges is to integratethe MNA in research protocols not only as anutritional assessment tool. The MNA as aninclusion or exclusion criterion could be usefulfor the homogenization of samples or useful as anoutcome criterion in order to permit meta-analyses.
Another challenge is to evaluate other types ofdisorders or syndromes using the MNA. It has beenproposed that the MNA could eventually measureAD severity, frailty or the indication for tube-feeding by changes the thresholds and the studypopulations to which it is directed. Future researchwill need to demonstrate all these hypothesis.
Conclusion
The MNA provides a number of unique opportuni-ties useful for practice. It is important to sensitizehealth professionals to the problem of malnutrition

Mini Nutritional Assessment after 20 years 301
Table 3. Prevalence of malnutrition in elderly determined by the MNA
Author, Year Reference Type of study Results
Harris DG, 200862 Observational study, N = 100Mean age = 79Living in sheltered housing
Sensitivity = 80%; Specificity = 90%;PPV = 0,47; NPV = 0,98
Wikby K, 200869 Cross-sectional study, N = 127Mean age = 85Residential homes
Agreement level between the 2 assessmentmethods (MNA by authors and MNA bynurses) was 62%
Comparison between MNA-SF and full MNA:agreement of 87% between the MNA-SF andthe full MNA to classify older people asmalnourished; sensitivity of 89%; specificity of82%; PPV was 92%
Hengstermann S, 200871 Cross-sectional study, N = 808Mean age = 78Geriatric hospital
The score of the MNA and MNA-SF correlatedwith r = 0.910
Correlation between MNA and MNA-SF groupclassification = 83%
Gil-Montoya JA, 200872 Cross-sectional study, N = 2860Mean age = 74Representative sample of
Spaniards
Mean MNA score = 243.5% were malnourished; 31.5% were at risk of
malnutrition; 65% were well-nourished
Formiga F, 200873 Observational study, N = 140Age > 89Living in urban community
Investigation into the rate of fallsNo statistically significant association was found
between the fallers and the non-fallersaccording to the MNA-SF
Cuyac Lantigua M, 200774 Observational study, N = 197Ages between 60–75 yearsGeriatrics service
MNA < 24 = 68%; MNA < 17 = 19.3%MNA scores <24 were concentrated in
neurological disorders (80%), Neoplasms andlymphoproliferative processes (77.8%), heartand blood vessels diseases (74.2%),gastrointestinal disorders (70.6%).
Patients with the lowest scores associated tolowest values of anthropometric andbiochemical markers
MNA scoring was 80% coincident with thenutritional diagnostic
Tsai AC, 200775 Observational studyInstitutionalized elderly Taiwanese
The MNA was effective in predicting 12-monthfollow-up mortality in cognition-normalelderly and in predicting 6-month follow-upmortality in cognition-impaired elderly
Tsai AC, 200776 Observational study, N = 1583 M;1307 W
Age # 65In home
Substitution of population-specificanthropometric cut-points (BMI, mid-armcircumference and calf circumference) forrespective values resulted of loweredprevalence of malnutrition
Feldblum I, 200777 Observational study, N = 259Age # 65Internal medicine departments
Mean MNA score = 19.518.5% were malnourished; 81.5% were at risk
of malnutritionThe patients who were malnourished were less
educated, had higher depression, lowercognitive and physical functioning, had higherchewing problems, higher nausea andvomiting

302 M Secher et al.
Table 3. (Continued)
Author, Year Reference Type of study Results
Suominen MH, 200799 Cross-sectional study, N = 1043Mean age = 81Long-term care hospitals
According to the nurses: 15% were malnourishedAccording to the MNA: 56.7% were
malnourished patients considered to havenormal nutrition by the nurses: 50.2% weremalnourished and 46.7% were at risk ofmalnutrition
Norman K, 200779 Observational study, N = 112Mean age = 85Nursing homes
19.6% were well-nourishedHandgrip strength, knee-extension strength,
Barthel’s index and phase angle decreased withdecreasing MNA
Charlton KE, 200770 Cross-sectional study, N = 283Mean age = 72Institutionalized (15%);
community-dwelling (85%)
Mean MNA = 235% were malnourished; 50–4% were at risk of
malnutrition; 44.4% were well-nourishedThe MNA was positively and significantly
associated with anthropometric values,cognitive function
MNA-SF vs full MNA: Sensitivity = 100%;Specificity = 94.6%
MNA-SF was strongly correlated with the fullMNA (r = 0.811; p < 0,0001)
MNA-SF was associated with cognitive functionscore (r =$0.31; p < 0,0001)
Kostka T, 200780 Observational study, N = 300Age = 66–79Community-dwelling persons
Mean MNA = 24MNA was associated with physical activity:Mobility (W: 0.86; p < 0,01-M:0.83; p < 0.05)Usual activity (W: 0.81; p < 0.001-M: 0.70;
p < 0.001)
Espaulella J, 200781 Prospective longitudinal cohortstudy, N = 165
Mean age = 83Hospitals
Mean MNA = 16Six-month mortality = 29.1%MNA was associated with mortality
Venzin RM, 200782 Prospective study, N = 430Mean age = 63Hospitals
The agreement between the clinical judgment andthe MNA was significant (r = 0.73; p < 0.001)
Bauer JM, 200783 Cross-sectional study, N = 121Mean age = 80Geriatric hospital
MNA identified 70% with malnutrition or at-riskNo correlation between MNA and basal ghrelin
level was found
Formiga F, 200784 Cohort study, N = 186Mean age = 93At home (74%); Institutionalized
(26%)
Rate of mortality = 19.3%MNA-SF was associated with mortality in
multivariate analysis
Ghisla MK, 200785 Observational study, N = 2650Age # 60Geriatric rehabilitation
In patients with MMSE # 18, better nutritionalstatus according to the MNA-SF emerged as afactor associated with functional improvement
Nijs KA, 200686 Randomized controlled trial,N = 178
Mean age = 77Nursing homes
The percentage of residents in the interventiongroup classified by the MNA as malnourisheddecreased from 17% to 14%, whereas thispercentage increased from 11% to 23% in thecontrol group
Wojszel ZB, 200687 Observational study, N = 100Age # 65Nursing homes
Malnutrition was associated with: chewingproblems; ADL dependence; limited mobility;dementia; cerebral stroke; nursing homes;depression

Mini Nutritional Assessment after 20 years 303
Table 3. (Continued)
Author, Year Reference Type of study Results
Kabir ZN, 200688 Observational study, N = 457Mean age = 69Home (population in rural
Bangladesh)
26% were malnourished; 62% were at risk ofmalnutrition
Wikby K, 200689 Cohort study, N = 127Age # 65 community
residential homes
Cohort 2: people who were newly admitted tothese community residential homes
Cohort 1: previous study performed in the samemunicipality 4 years earlier
32% were malnourished in Cohort 2; 38% weremalnourished Cohort 1
Soini H, 200690 Observational study, N = 178Elderly patientsAt home
50% were at risk of malnutrition; 3% weremalnourished
MNA: Mini Nutritional Assessment; MNA-SF: Mini Nutritional Assessment Short Form; W: Women; M: Men; PPV:Positive Predictive Value; NPV: Negative Predictive Value; BMI: Body Mass Index; HR: Hazard Ratio; CI: ConfidenceInterval; MMSE: Mini Mental State Examination.
Table 4. Prevalence of malnutrition associated with other diseases
Authors, YearReference Type of study Disease Results
Zekry D, 200891 Prospective study, N = 349Mean age = 85Rehabilitation and Geriatric
hospital
Dementia (46.1%cognitively normal;10.6% MCI; 43.3%dementia)
MNA-SF decreased with cognitivestatus (p = 0,001)
No association was found betweenMNA-SF and type of dementia
Hengsterman S,200792
Prospective study, N = 484Mean age = 80Hospitals
Pressure ulcer (PU)Prevalence = 16.7%
PU patients: 2,.% were well-nourished; 39.5% weremalnourished
Non-PU patients: 23.6% werewell -nourished; 16.6% weremalnourished
Riccio D, 200793 Prospective study, N = 47Mean age = 84Institutionalized
Dementia MMSE low score was correlatedwith a worse MNA (HR = 19.5;p = 0.003)
Schiffman SS, 200794 Cohort study, N = 107Elderly patients
Cancer with chemotherapy Intervention group receivedflavour enhancement,chemosensory education andnutritional information
After 8-month follow-upinterventional group had betterscores on the MNA, had betterself-reported taste and smellperception than the controlgroup
Hosia-Randell H,200795
Cross-sectional study,N = 1987
Mean age = 84Nursing homes
Constipation 55.3% of allresidents receivedlaxatives regularly
Poor MNA score was associatedwith regular laxative use inunivariate analysis (OR = 1.51;95%CI = 1.19–1.93)

304 M Secher et al.
Table 4. (Continued)
Authors, YearReference Type of study Disease Results
Olofsson B, 200796 Randomized controlledtrial, N = 157
Age # 70Hospitals
Femoral neck fracture Intervention group received anutritional assessment to detectnutrition deficiencies,protein-enriched meals andprotein drinks
Mean MNA: Intervention group:23; Control group: 22
Risk of malnutrition ormalnutrition on admission:
Intervention group: 58%; Controlgroup: 64%
Postoperative complications:Fewer patients in the intervention
group developed delirium (46 vs54 in the control group;p = 0.022) and the number ofdays with delirium wassignificantly lower (2,3 days vs 8in the control group;p < 0.001)
Half as many in the interventiongroup developed pressure ulcers(p = 0.054)
The length of stay for theintervention group was shorter(27 days vs 40; p = 0.019)
Cabrera MA, 200797 Cross-sectional study,N = 267
Age = 60–74At home
Depression (identified asregular use ofantidepressives or/andscores higher than 5points on the GDS)
21.7% were at risk of malnutritionor malnourished
Depression was identified in24.3%
Nutritional deficit (MNA < 24)was associated significantly withdepression even after adjustment(OR = 4,38; 95%CI = 2.23–8.64; p < 0,001)
Hassen TA, 200798 Prospective study, N = 68Mean age = 71Hospitals
Vascular surgeryOpen AAA (n = 35)EVAR (n = 16)Lower limb
revascularization(n = 17)
MNA:Open AAA: 24 were
well-nourished; 6 were at risk ofmalnutrition
EVAR: 15 were well-nourished; 1was at risk of malnutrition
Lower limb revascularization: 9were well-nourished; 8 were atrisk of malnutrition
Using the MNA neither SIRSseverity nor sepsis occurrencediffered significantly betweenwell-nourished patients andthose at risk

Mini Nutritional Assessment after 20 years 305
Table 4. (Continued)
Authors, YearReference Type of study Disease Results
Suominen MH,200799
Randomized controlledtrial, N = 40
Mean age = 85Nursing homes
Dementia (moderate orsevere dementia)
Group 1: assessment of energy andnutrient intake before and afternutritional education
Group 2: assessment of nutritionalstatus with MNA before andafter nutritional education
Group 1: Before intervention theenergy intake was on average1230 kcal/d
After intervention the energyintake was 1487 kcal/d(p % 0,001)
Mean energy intake increased 21%Group 2: Before intervention: none
was well-nourished; 89% wereat risk of malnutrition; 11%were malnourished
After intervention: 16%well-nourished; 63% were atrisk of malnutrition; 21% weremalnourished
Formiga F, 2006100 Prospective study, N = 88Mean age = 79Hospitalized
New diagnosis of heartfailure (HF)
Mean MNA-SF = 1127% died during the first year of
follow-upMNA-SF was not associated with
HF related mortality orreadmission
Soini H, 200690 Cross-sectional study,N = 3480
Elderly patientsNursing homes (n = 2036)Long-term care wards
(n = 1444)
Dental problems Patients living in nursing homes:11% well-nourished; 60% were at
risk of malnutrition; 29% weremalnourished
Patients living in long term carewards:
3% well-nourished; 40% were atrisk of malnutrition; 57% weremalnourished
Salminen H, 2006102 Cross-sectional study,N = 351
Mean age = 73+/$2,3Free-living
Osteoporosis Median MNA = 27; 7,4% were atrisk of malnutrition
Osteoporosis of the femoral neckwas observed by 22%
Fracture after the age of 50reported by 31%
Low score of MNA increased riskof having osteoporosis in thefemoral neck and/or total hip(for MNA < 27: OR = 2.09;95%CI = 1.14–3.83)
MNA: Mini Nutritional Assessment; MNA-SF: Mini Nutritional Assessment Short Form; W: Women; M: Men;CI: Confidence Interval; MMSE: Mini Mental State Examination; AD: Alzheimer’s disease; OR: Odds Ratio; GDS:Geriatric Depression Scale; AAA: Aortic Abdominal Aneurysm; EVAR: Endovascular Abdominal Aortic Aneurysm;SIRS: Systemic Inflammatory Response Syndrome.

306 M Secher et al.
in older people, especially the frail and ill. Up todate, the MNA is the most validated and acceptedscreening tool for geriatric patients, no matter thesetting, with clearly defined thresholds. It is themost efficient, simple and appropriate nutritionalassessment tool for older people: BMI cannotdifferentiate thin with good nutritional status orobese with malnutrition; albumin plasma-level isnot useful in the presence of dehydration or aninflammation; previous weight (which is oftendifficult to determine) is not necessary; the MNAcan detect malnutrition or risk of malnutritionbefore severe weight or albumin loss is present; theMNA allows nutritional intervention and follow-up; it can be completed easily by a physician,a dietician, a nurse or generalist assessor in fewminutes; and it is acceptable to patients. TheMNA not only detects malnutrition but alsofavours early nutritional intervention in orderto improve nutritional parameters and especiallyimprove quality of life.
References
1 Eriksson BG, Dey DK, Hessler RM, Steen G, SteenB. Relationship between MNA and SF-36 in afree-living elderly population aged 70 to 75.J Nutr Health Aging 2005; 9:212–20.
2 Pearson JM, Schlettwein-Gsell D, Brzozowska A,van Staveren WA, Bjornsbo K. Lifestylecharacteristics associated with nutritional risk inelderly subjects aged 80–85 years. J Nutr HealthAging 2001; 5:278–83.
3 Saletti A, Johansson L, Yifter-Lindgren E, WissingU, Osterberg K, Cederholm T. Nutritional statusand a 3-year follow-up in elderly receiving supportat home. Gerontology 2005; 51:192–98.
4 Thomas DR, Zdrowski CD, Wilson MM et al.Malnutrition in subacute care. Am J Clin Nutr2002; 75:308–13.
5 Gazzotti C, Albert A, Pepinster A, Petermans J.Clinical usefulness of the Mininutritionalassessment (MNA) scale in geriatric medicine.J Nutr Health Aging 2000; 4:176–81.
6 Kagansky N, Berner Y, Koren-Morag N, PerelmanL, Knobler H, Levy S. Poor nutritional habits arepredictors of poor outcome in very oldhospitalized patients. Am J Clin Nutr 2005;82:784–91.
7 Van Nes MC, Herrmann FR, Gold G, Michel JP,Rizzoli R. Does the mini nutritional assessmentpredict hospitalization outcomes in older people?Age Ageing 2001; 30:221–26.
8 Donini LM, Savina C, Rosano A. MNA predictivevalue in the follow-up of geriatric patients. J NutrHealth Aging 2003; 7:282–93.
9 Guerin O, Andrieu S, Schneider SM et al. Differentmodes of weight loss in Alzheimer disease: aprospective study of 395 patients. Am J Clin Nutr2005; 82:435–41.
10 Andrieu S, Reynish W, Nourhashemi F et al.Nutritional risk factors for institutional placementin Alzheimer’s disease after one-year follow-up.J Nutr Health Aging 2001; 5:113–17.
11 Nourhashemi F, Andrieu S, Sastres N et al.Descriptive analysis of emergency hospitaladmissions of patients with Alzheimer disease.Alzheimer Dis Assoc Disord 2001; 15:21–25.
12 Folstein MF, Folstein SE, Mc Hugh PR.Mini-mental state: a practical method for gradingthe cognitive state of patients for the clinician.J Psychiatr Res 1975; 12:189–98.
13 Vellas B, Guigoz Y, Baumgartner M, Garry PJ,Lauque S, Albarede JL. Relationships betweennutritional markers and the mini-nutritionalassessment in 155 older persons. J Am Geriatr Soc2000; 48:1300–09.
14 Guigoz Y, Vellas B, Garry PJ. Mini NutritionalAssessment: a practical assessment tool forgrading the nutritional state of elderly patients.Facts Res Gerontol 1994: 12–13.
15 Rubenstein LZ, Harker JO, Salva A, Guigoz Y,Vellas B. Screening for undernutrition in geriatricpractice: developing the short-formmini-nutritional assessment (MNA-SF). J GerontolA Biol Sci Med Sci 2001; 56:366–72.
16 Guigoz Y. The Mini Nutritional Assessment(MNA) review of the literature.What does it tellus? J Nutr Health Aging 2006; 10:466–85.
17 Cohendy R, Rubenstein LZ, Eledjam JJ. The MiniNutritional Assessment-Short Form forpreoperative nutritional evaluation of elderlypatients. Aging (Milano). 2001; 13:293–97.
18 Vellas B, Guigoz Y, Garry PJ et al. The MiniNutritional Assessment (MNA) and its use ingrading the nutritional state of elderly patients.Nutrition 1999; 116–22.
19 Deplas A, Debiais F, Alcalay M, Bontoux D,Thomas P. Bone density, parathyroid hormone,calcium and vitamin D nutritional status ofinstitutionalized elderly subjects. J Nutr HealthAging 2004; 8:400–04.
20 Guigoz Y, Lauque S, Vellas B. Identifying theelderly at risk for malnutrition. The MiniNutritional Assessment. Clin Geriatr Med 2002;18:737–57.
21 Kelsheimer HL, Hawkins ST. Older adult womenfind food preparation easier with specializedkitchen tools. J Am Diet Assoc 2000; 100:950–52.

Mini Nutritional Assessment after 20 years 307
22 Kretser AJ, Voss T, Kerr WW, Cavadini C,Friedmann J. Effects of two models of nutritionalintervention on homebound older adults atnutritional risk. J Am Diet Assoc 2003;103:329–36.
23 Remsburg RE, Luking A, Baran P et al. Impact ofa buffet-style dining program on weight andbiochemical indicators of nutritional status innursing-home residents: a pilot study. J Am DietAssoc 2001; 101:1460–63.
24 Menecier-Ossia L, Menecier P, Debatty D, PirothL, Bonnet N, Lenoir C. Suivi nutritionnel enhebergement medicalise pour personnes agees[Nutritional report in nursing homes]. Rev Geriatr2000; 25:65–70.
25 Desai J, Winter A, Young KW, Greenwood CE.Changes in type of food service and dining-roomenvironment preferentially benefit institutionalizedseniors with low body mass indexes. J Am DietAssoc 2007; 107:808–14.
26 Nijs KA, de GC, Siebelink E et al. Effect offamily-style meals on energy intake and risk ofmalnutrition in Dutch nursing home residents: arandomized controlled trial. J Gerontol A Biol SciMed Sci 2006; 61:935–42.
27 Nijs KA, de GC, Kok FJ, van Staveren WA. Effectof family style mealtimes on quality of life,physical performance, and body weight of nursinghome residents: a cluster randomised controlledtrial. BMJ 2006; 332(7551):1180–84.
28 Mathey MF, Vanneste VG, de GC, de Groot LC,van Staveren WA. Health effect of improved mealambiance in a Dutch nursing home: a 1-yearintervention study. Prev Med 2001; 32:416–23.
29 Donini LM, De Felice MR, Tagliaccica A, DeBernardini L, Cannella C. Nutritional status andevolution of pressure sores in geriatric patients. JNutr Health Aging 2005; 9:446–45.
30 Riviere S, Gillette-Guyonnet S, Voisin T et al. Anutritional education program could preventweight loss and slow cognitive decline inAlzheimer’s disease. J Nutr Health Aging 2001;5:295–99.
31 Cicconetti P, Fionda A, Bauco C, Migliori M,Marigliano V. Nutritional deficiency andAlzheimer’s disease: how to identify and prevent.Recenti Prog Med 2000; 91:135–40.
32 Gil GP, Ramirez Diaz SP, Ribera Casado JM.Dementia and nutrition. Intervention Study ininstitutionalised patients with Alzheimer disease.J Nutr Health Aging 2003; 7:304–08.
33 Vellas B, Lauque S, Gillette-Guyonnet S et al.Impact of nutritional status on the evolution ofAlzheimer’s disease and on response toacetylcholinesterase inhibitor treatment. REAL FRGroup. J Nutr Health Aging 2005; 9:75–80.
34 de Jong N, Chin A, Paw M et al. Appraisal of 4months’ consumption of nutrient-dense foodswithin the daily feeding pattern of frail elderly.J Aging Health 2001; 13:200–16.
35 Fiatarone MA, Marks EC, Ryan ND, MeredithCN, Lipsitz LA, Ewans WJ. High-intensitystrength training in nonagenarians. Effects onskeletal muscle. JAMA 1990; 263:3029–34.
36 Odlund Olin A, Armyr I, Soop M. Energy-densemeals improve energy intake in elderly residents ina nursing home. Clin Nutr 2003; 22:125–31.
37 Delmi M, Raphin CH, Bengoa JM, Delmas PD,Vasey H, Bonjour JD. Dietary supplementation inelderly patients with fractured neck of the femur.Lancet 1990; 335:1013–16.
38 Rypkema G, Adang E, Dicke H et al. Cost-effectiveness of an interdisciplinary intervention ingeriatric inpatients to prevent malnutrition. J NutrHealth Aging 2003; 8:122–27.
39 Arnaud-Battandier F, Malvy D et al. Use of oralsupplements in malnourished elderly patientsliving in the community: a pharmaco-economicstudy. Clin Nutr 2004; 23:1096–103.
40 Rubenstein LZ, Stuck AE, Siu AL, Wieland D.Impacts of geriatric evaluation and managementprograms on defined outcomes: overview of theevidence. J Am Geriatr Soc. 1991; 39:8S–16S.
41 Stuck AE, Siu AL, Wieland GD, Adams J,Rubenstein LZ. Comprehensive geriatricassessment: a meta-analysis of controlled trials.Lancet 1993; 342(8878):1032–36.
42 Bula CJ, Berod AC, Stuck AE et al. Effectivenessof preventive in-home geriatric assessment inwell-functioning community-dwelling olderpeople: secondary analysis of a randomized trial.J Am Geriatr Soc 1999; 47:389–95.
43 Katz S. Assessing self-maintenance: activities ofdaily living, mobility, and instrumental activitiesof daily living. J Am Geriatr Soc 1983; 31:721–27.
44 Lawton MP, Brody EM. Assessment of olderpeople: self-maintaining and instrumental activitiesof daily living. Gerontologist 1969; 9:179–86.
45 Tinetti M. Performance-oriented assessment ofmobility problems in the elderly patients. J AmGeriatr Soc 1986; 34:119–26.
46 Sheikh JI, Yesavage JA. Geriatric Depression Scale(GDS): recent evidence and development of ashorter version. In: BrinkTL ed. Clinicalgerontology. A guide to assessment andintervention. NewYork, NY: Haworth Press,1986: 12–13.
47 Vellas B, Guigoz Y. Nutritional assessment as partof the geriatric evaluation. In Rubestein LZ,Bernabei R, Wieland D eds. Geriatric assessmenttechnology: state of the art. Milano, Italy: KurtizPublishing Company, 1995: 179–515.

308 M Secher et al.
48 Morley JE. A brief history of geriatrics. J GerontolA Biol Sci Med Sci 2004; 59:1132–52.
49 Sieber CC. Nutritional screening tools–how doesthe MNA compare? Proceedings of the sessionheld in Chicago May 2–3, 2006 (15 Years of theMini Nutritional Assessment). J Nutr HealthAging 2006; 10:488–92.
50 Vellas B, Villars H, Abellan G et al. Overview ofthe MNA– its history and challenges. J NutrHealth Aging 2006; 10:456–63.
51 Guigoz Y, Vellas B. Malnutrition in the elderly:the Mini Nutritional Assessment (MNA) TherUmsh. 1997; 54:345–60.
52 Guigoz Y, Vellas B, Garry PJ. Mini NutritionalAsessment: a practical assessment tool for gradingthe nutritional state of elderly patients. Facts ResGerontol 1994; 15–59.
53 Bleda MJ, Bolibar I, Pares R, Salva A. Reliabilityof the Mini Nutritional Assessment (MNA) ininstitutionalized elderly people. J Nutr HealthAging 2002; 6:134–37.
54 Saletti A, Lindgren EY, Johansson L, CederholmT. Nutritional status according to MiniNutritional Assessment in an institutionalizedelderly population in Sweden. Gerontology. 2000;46:139–45.
55 Siebens H, Trupe E, Oster G. Correlates andconsequences of eating dependency ininstitutionalized elderly. J Am Geriatr Soc 1986;34:192–98.
56 Pepersack T, Rotsaert P, Benoit F et al. Prevalenceof zinc deficiency and its clinical relevance amonghospitalised elderly. Arch Gerontol Geriatr 2001;33:243–53.
57 Hudgens J, Langkamp-Henken B, Stechmiller JKet al. Immune function is impaired with a MiniNutritional Assessment score indicative ofmalnutrition in nursing-home elders with pressureulcers. J Parenter Enteral Nutr 2004; 28:416–22.
58 Soini H, Routasalo P, Lagstrom H. Nutritionalstatus in cognitively intact older people receivinghome-care services a pilot study. J Nutr HealthAging 2005; 9:249–53.
59 Cairella G, Baglio G, Censi L et al. MiniNutritional Assessment (MNA) and nutritionalrisk in elderly. A proposal of a nutritionalsurveillance system for the Department of PublicHealth. Ann Ig 2005; 17:35–46.
60 Guerin O, Soto ME, Brocker P, Robert PH, BenoitM, Vellas B. Nutritional status assessment duringAlzheimer’s disease: results after one year (theREAL French Study Group); REAL FR Group.J Nutr Health Aging 2005; 9:81–84.
61 Pauly L, Stehle P, Volkert D. Nutritional situationof elderly nursing home residents. Z GerontolGeriatr 2007; 40:3–12.
62 Harris DG, Davies C, Ward H, Haboubi NY. Anobservational study of screening for malnutritionin elderly people living in shelteredaccommodation. J Hum Nutr Diet 2008; 21:3–9.
63 Ferreira LS, Nascimento LF, Marucci MF. Use ofthe mini nutritional assessment tool in elderlypeople from long-term institutions of southeast ofBrazil. J Nutr Health Aging 2008; 12:213–17.
64 Elkan AC, Engvall IL, Tengstrand B, CederholmT, Hafstrom I. Malnutrition in women withrheumatoid arthritis is not revealed by clinicalanthropometrical measurements or nutritionalevaluation tools. Eur J Clin Nutr 2007 Jul 18.doi:10.1038/sj.ejcn.1602848
65 Kuzuya M, Kanda S, Koike T, Suzuki Y, Satake S,Iguchi A. Evaluation of Mini-NutritionalAssessment for Japanese frail elderly. Nutrition2005; 21:498–503.
66 Delacorte RR, Moriguti JC, Matos FD, Pfrimer K,Marchinil JS, Ferriolli E. Mininutritionalassessment score and the risk for undernutrition infree-living older persons. J Nutr Health Aging2004; 8:531–34.
67 Visvanathan R, Penhall R, Chapman I. Nutritionalscreening of older people in a subacute care facilityin Australia and its relation to dischargeoutcomes. Age Ageing 2004; 33:260–65.
68 Guigoz Y, Vellas B. Test d’evaluation de l’etatnutritionnel de la personne agee: le MiniNutritional Assessment (MNA) [Test to assess thenutritional status of the elderly: The MiniNutritional Assessment (MNA]. Med Hyg 1995;53:1965–69.
69 Wikby K, Ek AC, Christensson L. The two-stepMini Nutritional Assessment procedure incommunity resident homes. J Clin Nurs 2008;17:1211–1218.
70 Charlton KE, Kolbe-Alexander TL, Nel JH. TheMNA, but not the DETERMINE, screening tool isa valid indicator of nutritional status in elderlyAfricans. Nutrition 2007; 23:533–42.
71 Hengstermann S, Nieczaj R, Steinhagen ThiessenE, Schulz RJ. Which are the most efficient items ofMini Nutritional Assessment in multimorbidpatients? J Nutr Health Aging 2008; 12:117–22.
72 Gil-Montoya JA, Subira C, Ramon JM,Gonzalez-Moles MA. Oral health-related qualityof life and nutritional status. J Public Health Dent2008 Jan 29.
73 Formiga F, Ferrer A, Duaso E, Olmedo C, Pujol R.Falls in nonagenarians after 1-year of follow-up:the NonaSantfeliu study. Arch Gerontol Geriatr2008; 46:15–23.
74 Cuyac Lantigua M, Santana Porben S. The MiniNutritional Assessment of the elderly in thepractice of a hospital geriatrics service: inception,

Mini Nutritional Assessment after 20 years 309
validation and operational characteristics. ArchLatinoam Nutr 2007; 57:255–65.
75 Tsai AC, Ku PY. Population-specific MiniNutritional Assessment effectively predicts thenutritional state and follow-up mortality ofinstitutionalized elderly Taiwanese regardless ofcognitive status. Br J Nutr 2007; 152–58.
76 Tsai AC, Ho CS, Chang MC. Population-specificanthropometric cut-points improve thefunctionality of the Mini Nutritional Assessment(MNA) in elderly Taiwanese. Asia Pac J Clin Nutr2007; 16:656–62.
77 Feldblum I, German L, Castel H et al.Characteristics of undernourished older medicalpatients and the identification of predictors forundernutrition status. Nutr J 2007; 6: 37.
78 Suominen MH, Sandelin E, Soini H, Pitkala KH.How well do nurses recognize malnutrition inelderly patients? Eur J Clin Nutr 2007: Sep 19;doi:10.1038/sj.ejcn.1602948.
79 Norman K, Smoliner C, Valentini L, Lochs H,Pirlich M. Is bioelectrical impedance vectoranalysis of value in the elderly with malnutritionand impaired functionality? Nutrition 2007;23:564–69.
80 Kostka T, Bogus K. Independent contribution ofoverweight/obesity and physical inactivity to lowerhealth-related quality of life incommunity-dwelling older subjects. Z GerontolGeriatr 2007; 40:43–51.
81 Espaulella J, Arnau A, Cubı D, Amblas J, YanezA. Time-dependent prognostic factors of 6-monthmortality in frail elderly patients admitted topost-acute care. Age Ageing. 2007; 36:407–13.
82 Venzin RM, Kamber N, Keller WC, Suter PM,Reinhart WH. How important is malnutrition? Aprospective study in internal medicine. Eur J ClinNutr 2007 Nov 7.
83 Bauer JM, Wirth R, Troegner J et al.Anthropometry and nutritional assessment ingeriatric hospital patients. Z Gerontol Geriatr2007; 40:31–36.
84 Formiga F, Ferrer A, Mascaro J, Ruiz D, OlmedoC, Pujol R. Predictive items of one-year mortalityin nonagenarians. The NonaSantfeliu Study. AgingClin Exp Res 2007; 19:265–68.
85 Ghisla MK, Cossi S, Timpini A, Baroni F, FacchiE, Marengoni A. Predictors of successfulrehabilitation in geriatric patients: subgroupanalysis of patients with cognitive impairment.Aging Clin Exp Res 2007; 19:417–23.
86 Nijs KA, de Graaf C, Siebelink E et al. Effect offamily-style meals on energy intake and risk ofmalnutrition in Dutch nursing home residents: arandomized controlled trial. J Gerontol A Biol SciMed Sci 2006; 61:935–42.
87 Wojszel ZB. Determinants of nutritional status ofolder people in long-term care settings on theexample of the nursing home in Bialystok. AdvMed Sci 2006; 51:168–73.
88 Kabir ZN, Ferdous T, Cederholm T, KhanamMA, Streatfied K, Wahlin A. Mini NutritionalAssessment of rural elderly people in Bangladesh:the impact of demographic, socio-economic andhealth factors. Public Health Nutr 2006;9:968–74.
89 Wikby K, Ek AC, Christensson L. Nutritionalstatus in elderly people admitted to communityresidential homes: comparisons between twocohorts. J Nutr Health Aging 2006; 10:232–38.
90 Soini H, Routasalo P, Lauri S. Nutrition inpatients receiving home care in Finland: tacklingthe multifactorial problem. J Gerontol Nurs 2006;32:12–17.
91 Zekry D, Herrmann FR, Grandjean R et al.Demented versus non-demented very oldinpatients: the same co-morbidities but poorerfunctional and nutritional status. Age Aging 2008;37:83–89.
92 Hengstermann S, Fischer A, Steinhagen-ThiessenE, Schulz RJ. Nutrition status and pressure ulcer:what we need for nutrition screening. J ParenterEnteral Nutr 2007; 31:288–94.
93 Riccio D, Solinas A, Astara G, Mantovani G.Comprehensive geriatric assessment in femaleelderly patients with Alzheimer disease and othertypes of dementia. Arch Gerontol Geriatr 2007;44 (suppl 1):343–53.
94 Schiffman SS, Sattely-Miller EA, Taylor EL et al.Combination of flavor enhancement andchemosensory education improves nutritionalstatus in older cancer patients. J Nutr HealthAging. 2007; 11:439–54.
95 Hosia-Randell H, Suominen M, Muurinen S,Pitkala KH. Use of laxatives among older nursinghome residents in Helsinki, Finland. Drugs Aging2007; 24:147–54.
96 Olofsson B, Stenvall M, Lundstrom M, SvenssonO, Gustafson Y. Malnutrition in hip fracturepatients: an intervention study. J Clin Nurs 2007;16:2007–38.
97 Cabrera MA, Mesas AE, Garcia AR, de AndradeSM. Malnutrition and depression amongcommunity-dwelling elderly people. J Am Med DirAssoc 2007; 8:582–84.
98 Hassen TA, Pearson S, Cowled PA, Fitridge RA.Preoperative nutritional status predicts the severityof the systemic inflammatory response syndrome(SIRS) following major vascular surgery. Eur JVasc Endovasc Surg 2007; 33:696–702.
99 Suominen MH, Kivisto SM, Pitkala KH. Theeffects of nutrition education on professionals’practice and on the nutrition of aged residents in

310 M Secher et al.
dementia wards. Eur J Clin Nutr 2007;61:1226–32.
100 Formiga F, Chivite D, Sole A, Manito N, RamonJM, Pujol R. Functional outcomes of elderlypatients after the first hospital admission fordecompensated heart failure (HF). A prospectivestudy. Arch Gerontol Geriatr 2006; 43:175–85.
101 Soini H, Muurinen S, Routasalo P. Oral andnutritional status–is the MNA a useful tool fordental clinics. J Nutr Health Aging 2006;10:495–99.
102 Salminen H, Saaf M, Johansson SE, Ringertz H,Strender LE. Nutritional status, as determined by
the Mini-Nutritional Assessment, andosteoporosis: a cross-sectional study of an elderlyfemale population. Eur J Clin Nutr 2006;60:486–93.
103 Salva A, Corman B, Andrieu S et al. IAG/IANATask Force. Minimum data set for nutritionalintervention studies in the elderly IAG/IANA taskforce consensus. J Nutr Health Aging 2004;8:202–06.
104 Abellan Van Kan G, Sinclair A, Andrieu S, OldeRikkert M, Gambassi G, Vellas B. The GeriatricMinimum Data Set for Clinical Trials (GMDS).J Nutr Health Aging 2008; 12:197–200.