C SPINE
47
C SPINE Y A Mamoojee
description
C SPINE. Y A Mamoojee. Importance of Prompt Diagnosis. Neck pain > quadriplegia > death Delayed recognition can lead to irreversible s.c injury and permanent neurologic damage. INDICATIONS. Who needs XR. NEXUS. NO - Alcohol intoxication Focal neuro deficit Midline tenderness - PowerPoint PPT Presentation
Transcript of C SPINE

C SPINE
Y A Mamoojee

Importance of Prompt Diagnosis
• Neck pain– > quadriplegia– > death
• Delayed recognition can lead to irreversible s.c injury and permanent neurologic damage.

INDICATIONS
• Who needs XR

NEXUS
NO - • Alcohol intoxication• Focal neuro deficit• Midline tenderness• GCS 15• Painful distracting injuries

CANADIAN C SPINE RULES

CASE DISCUSSION
• A person arrives by ambulance to ED on a backboard and a cervical collar after an MVA.
• Speed of 50km/hr• No LOC, no other injuries, no midline
tenderness, BAL 0.20.• Does he need imaging?

WHAT VIEWS?

• LATERAL• AP • ODONTOID
• SWIMMERS• FLEXION/EXTENSION?

ANATOMY OF NECK
• LIGAMENTS• BONES • MUSCLES• JOINTS

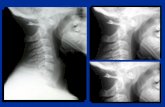
• Most important view• Can see 80-90% of injuries• Interpretation:• A - adequacy• A - alignment• B - bone• C - cartilage• D - disc• S – soft tissue
• A - Must have a view of C7 – T1• A - Use 3 lines• 1. anterior vertebral line• 2. posterior vertebral line• 3. spino laminar line (base of spinous
processes)• 4th line can be used ie. Tips of spinous
processes

• Check :• B - individual vertebrae• C - cartilage• D - disc• S - soft tissue - • <7mm at C3• <21mm at C7• no more than vertebral body
width at C7• Predental space – • 5mm child• 3mm adult• Fanning of spinous processes

• Open mouth view• Adequate if entire
Odontoid and lateral borders of C1 and C2 visible
• Check : • lateral masses of C1
must align with Odontoid• bilateral symmetry• Important also for
Odontoid fractures

SWIMMER’S AP

MECHANISM OF INJURY
• 1. Flexion• 2. flexion rotation• 3. extension• 4. axial compression• 5. Other


WEDGE FRACTURE
• STABLE• Compression fracture resulting from flexion• Features – – Buckled anterior cortex– Loss of height of anterior part of body– Anterosuperior fracture of vertebral body


FLEXION TEARDROP FRACTURE• UNSTABLE• Posterior ligament disruption
and anterior compression fracture of the vertebral body
• Prevertebral swelling• Tear drop fragment• Posterior vertebral body
subluxation into the spinal canal
• Spinal cord compression• Fracture of spinous process

• Mechanism – Hyperflexion and Compression – Excessive flexion of the neck in the sagittal plane, disrupts posterior ligament.
• Example – diving into shallow pool


ANTERIOR SUBLUXATION• Disruption of the posterior ligament complex.
Anterior subluxation of C4 on C5 is characterized by widening of the interspinous space (arrowhead), subluxation of the C4-C5 interfacetal joints (arrows), and anterior rotation of the C4 vertebra relative to C5.

• Stable but potentially unstable during flexion• Mechanism : hyperflexion• Disruption of posterior ligament complex,
anterior intact
• Stable – • loss of normal cervical lordosis• anterior displacement of body• fanning of interspinous distance
• Unstable – • anterior subluxation >4mm• assoc. compression fracture >25% of
affected body• increase or decrease in normal disc space• fanning of interspinous distance


BILATERAL FACET JOINT DISLOCATION
• Complete anterior dislocation of the vertebral body• Mechanism – extreme hyperflexion of head and neck
without axial compression• Unstable – very high risk of cord damage• Features –– complete anterior dislocation >50% of vertebral body
diameter– Disruption of the posterior ligament complex and anterior
longitudinal ligament– “Bow tie” appearance of the locked facets.


CLAY SHOVELLER’S FRACTURE
• Fracture of spinous process C6-T1• Mechanism – powerful hyperflexion, usually
combined with contraction of paraspinous muscles pulling on spinous processes
(e.g. shovelling).Features –
spinous process fracture on lateral viewGhost sign on AP – double spinous process of C6/C7 due to displaced fractured spinous process


UNILATERAL FACET JOINT DISLOCATION
• Stable• Mechanism –
simultaneous flexion and rotation
• Facet joint dislocation and rupture of the apophyseal joint ligaments
• FEATURES :• Anterior dislocation of
vertebral body by <50% of the diameter
• Discordant rotation above and below involved level
• Facet within intervertebral foramen on oblique view
• “Bow tie” appearance of the overriding locked facets

EXTENSION INJURIES
• Excessive extension of the neck in the sagittal plane.
• E.g. hitting the dash board in MVA


HANGMAN’S FRACTURE• Fractures through pars interaticularis
of the axis • Unstable if occurs with facet
dislocation• Mechanism – hyperextension• Features –
– Prevertebral soft tissue swelling– Avulsion of anterior inferior
corner of C2 assoc. with rupture of the ant. Longitudinal ligament
– Anterior dislocation of C2 body– Bilateral C2 pedicle fractures.


C1 POSTERIOR ARCH FRACTURE
• Hyperextended head• C1 arch is compressed by occiput and C2
spinous process• Odontoid process is normal• Stable• Distinguish from Jefferson fracture (unstable)

AXIAL COMPRESSION INJURIES


BURST FRACTURE
• Fracture of C3-C7 that results from axial compression
• Spinal cord injury secondary to displacement of posterior fragments is common.
• Mechanism – Axial compression• >25% loss of height of vertebral body• Stable• Needs CT or MRI



JEFFERSON FRACTURE
• Burst type fracture of C1• Lateral displacement of C1 masses• Fracture of anterior and posterior arches on
both sides – quadruple fracture• Unstable – transverse ligament rupture• Soft tissue swelling is marked on Xray




ATLANTO AXIAL SUBLUXATION
• Flexion and rotation causes the transverse ligament to rupture
• Predental space >3.5mm in adults and >5mm in children
• Unstable



ODONTOID FRACTURES
• 3 Types :– I Avulsion of tip at alar ligament (stable)– II Base of dens (unstable) – common, non union is
a complication– III Involves body of C2 (unstable)