
C. Noel Bairey Merz, MD Eileen M. Handberg, Chrisandra L. Shufelt, Puja K. Mehta, Margo B....
16
C. Noel Bairey Merz, MD Eileen M. Handberg, Chrisandra L. Shufelt, Puja K. Mehta, Margo B. Minissian, Janet Wei, Louise E. J. Thomson, Daniel S. Berman, Leslee J. Shaw, John W. Petersen, Garrett H. Brown, R. David Anderson, Jonathan J. Shuster, Galen Cook-Wiens, RWISE A Randomized, Placebo Controlled Trial of Late Na Current Inhibition (ranolazine) in Coronary Microvascular Dysfunction: Impact on Angina and Myocardial Perfusion Reserve
-
Upload
emma-french -
Category
Documents
-
view
220 -
download
0
Transcript of C. Noel Bairey Merz, MD Eileen M. Handberg, Chrisandra L. Shufelt, Puja K. Mehta, Margo B....
C. Noel Bairey Merz, MDEileen M. Handberg, Chrisandra L. Shufelt, Puja K. Mehta,
Margo B. Minissian, Janet Wei, Louise E. J. Thomson, Daniel S. Berman, Leslee J. Shaw, John W. Petersen,
Garrett H. Brown, R. David Anderson, Jonathan J. Shuster, Galen Cook-Wiens, André Rogatko, Carl J. Pepine
For the WISE and RWISE Investigators
RWISEA Randomized, Placebo Controlled Trial of Late Na Current
Inhibition (ranolazine) in Coronary Microvascular Dysfunction: Impact on Angina
and Myocardial Perfusion Reserve
Online November 11, 2015 http.//dx10.1093/eurheartj/ehv647
European Heart Journal
RWISEA Randomized, Placebo Controlled Trial of Late Na Current
Inhibition (ranolazine) in Coronary Microvascular Dysfunction: Impact on Angina
and Myocardial Perfusion Reserve
C. Noel Bairey Merz, MD, Eileen M. Handberg, Chrisandra L. Shufelt, Puja K. Mehta, Margo B. Minissian, Janet Wei, Louise E. J. Thomson,
Daniel S. Berman, Leslee J. Shaw, John W. Petersen, Garrett H. Brown, R. David Anderson, Jonathan J. Shuster, Galen Cook-
Wiens, André Rogatko, Carl J. PepineFor the WISE and RWISE Investigators
RWISE Trial Organization
Principal InvestigatorC. Noel Bairey Merz, MDCedars-Sinai Heart InstituteCedars-Sinai Medical Center
Executive CommitteeCarl J. Pepine MD, Eileen Handberg PhD, Leslee Shaw PhD, Puja Mehta MD, Chrisandra Shufelt MD, MS, Janet Wei MD
Data Management and BiostatisticsGalen Cook-Wiens MS, Jonathan Shuster PhD, Andre Rogatko PhD
Data Safety Monitoring BoardBernard J. Gersh, MD (Chair), Robert Bonow MD, Erika Brittain PhD
CMRI Core LabLouise Thomson MBBS, Daniel S. Berman MD
Coronary Angiographic /Physiology Core LabDavid Anderson MD, John Petersen MD
The study was investigator-initiated as an ancillary trial to the NHLBI-sponsored WISE, funded in part by Gilead Sciences. Statistical analysis was performed by the investigators independent of NHLBI and Gilead. The decision to submit for publication was made by the Principle Investigators who had access to all data
after the last subject completed the study.

WISE Background -1Coronary microvascular dysfunction (CMD) is highly prevalent in 20-54% of subjects with symptoms and signs of ischemia with and without obstructive CAD1-3
CMD is associated with elevated IHD morbidity, mortality, and healthcare costs4-8
Mechanistic pathways for CMD and no obstructive CAD are not well-defined, large outcome trials are lacking and treatment guidelines absent9
WISE = Women’s Ischemia Syndrome Evaluation1. Reis AHJ 2001 doi:10.1067/mhj.2001.114198 ; 2. Buchthal NEJM 200 DOI: 10.1056/NEJM2000032334212010; 3. Murthy Circ 2014 doi: 10.1161/CIRCULATIONAHA.113.008507; 4. Johnson Circ 2004 doi: 10.1161/01.CIR.0000130642.79868.B2 ; 5. von Mering Circ 2004 doi: 10.1161/01.CIR.0000115525.92645.16 ; 6. Pepine JACC 2010 doi:10.1016/j.jacc.2010.01.054; 8. Shaw Circ 2006 doi:10.1016/j.jacc.2004.11.075 ; 9. Fihn JACC 2012 doi:10.1016/j.jacc.2012.07.013
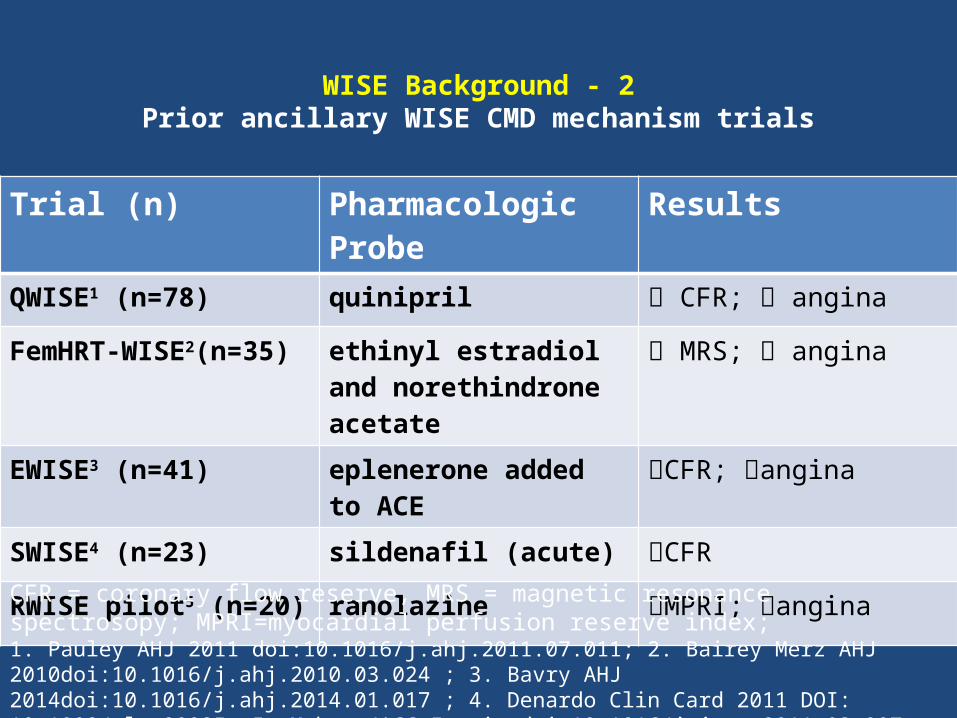
WISE Background - 2Prior ancillary WISE CMD mechanism trials
Trial (n) Pharmacologic Probe Results
QWISE1 (n=78) quinipril CFR; angina
FemHRT-WISE2(n=35) ethinyl estradiol and norethindrone acetate
MRS; angina
EWISE3 (n=41) eplenerone added to ACE CFR; angina
SWISE4 (n=23) sildenafil (acute) CFR
RWISE pilot5 (n=20) ranolazine MPRI; angina
CFR = coronary flow reserve, MRS = magnetic resonance spectrosopy; MPRI=myocardial perfusion reserve index; 1. Pauley AHJ 2011 doi:10.1016/j.ahj.2011.07.011; 2. Bairey Merz AHJ 2010doi:10.1016/j.ahj.2010.03.024 ; 3. Bavry AHJ 2014doi:10.1016/j.ahj.2014.01.017 ; 4. Denardo Clin Card 2011 DOI: 10.1002/clc.20935; 5. Mehta JACC Imagingdoi:10.1016/j.jcmg.2011.03.007

RWISE Study Design
R A N D
A
B
B
A
WASH-OUT
Randomized, double-blind, placebo-controlled, cross-over, short-term, mechanism trial
ClinicalTrials.gov NCT01342029
2 weeks 2 weeks 2 weeks
Baseline SAQ Angina/NTGDASI, QoL, Blood
CMRISAQ Angina/NTGDASI, QoL, Blood
CMRISAQ Angina/NTGDASI, QoL, Blood
RADOM IZED
CMRI conducted followingwithdrawal of vasoactive and anti-anginal medication
Primary: To mechanistically test short-term late Na current inhibition (ranolazine) in subjects with symptoms, no obstructive CAD but evidence of CMD, on SAQ angina, myocardial perfusion reserve and diastolic filling
Secondary: To investigate if symptoms are related to ischemia in such subjects

RWISE Efficacy Endpoints and Statistical Analyses
Co-primary Outcomes:Angina measured by the Seattle Angina Questionnaire (SAQ):
- Angina stability, Angina frequency, SAQ-7Secondary Outcome:
- Angina measured by diaryOther Outcomes:
- Cardiac magnetic resonance imaging (CMRI) gadolinium (Gd) perfusion and diastolic function- Quality of Life (SF-36, MOS-116, HIS-GWB, DASI)
Statistical Analyses:- Within-subjects comparison (paired) of the difference between baseline-treatments (SAQ, QoL) or treatment period (CMRI)- Linear regression models for treatment difference outcome
All subjects receiving both ranolazine and placebo in the appropriate treatment periods were included in the primary analysis

RWISE Enrollment and Randomization
22 Excluded 9 not treated 3 scientific misconduct
5 Excluded (no PCI) 10 Excluded (no PCI)
251 Randomized

RWISE Baseline Characteristics Variable (n=128) Mean ± SD, or absolute frequency (%)
Age (yrs) 55.2 ± 9.8Female 123 (96%) Typical Angina 40 (31.3%) Shortness of Breath 88 (68.8%) Palpitations 53 (41.4%) Nausea 40 (31.3%)Angina frequency (baseline SAQ angina frequency domain) 59.6 ± 26.9
Angina episodes (diary) 4.9±7.8 (wk)NTG usage (diary) 2.6±11.2 (wk)Qualifying CMRI MPRI<2 (n=67)* 1.6 ± 0.3Qualifying CFR<2.5 (n=35)* 2.2 ± 0.2Qualifying Ach response<0% (n=36)* -1.6± 15.6*subjects could have CMRI and CFR and ACH qualifiers
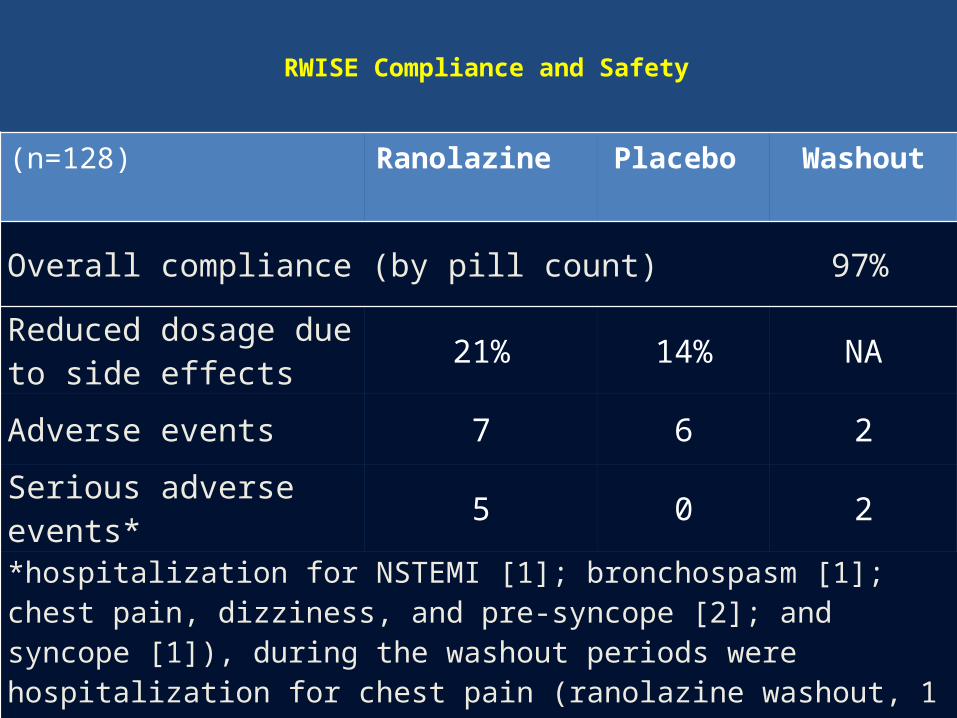
RWISE Compliance and Safety
(n=128) Ranolazine Placebo Washout
Overall compliance (by pill count) 97%
Reduced dosage due to side effects 21% 14% NA
Adverse events 7 6 2
Serious adverse events* 5 0 2
*hospitalization for NSTEMI [1]; bronchospasm [1]; chest pain, dizziness, and pre-syncope [2]; and syncope [1]), during the washout periods were hospitalization for chest pain (ranolazine washout, 1 patient) and bradycardia (placebo washout, 1 patient), and 0 during the placebo.

RWISE Primary, Secondary and QoL OutcomesRanolazine
(N=128) Placebo (N=128)
Treatment Change*
P-value
SAQ angina stability 58.40±26.11 51.17±27.68 5.12 0.24
SAQ angina frequency 63.91±26.09 62.73±25.96 0.08 0.97
SAQ-7 63.43±21.09 61.60±22.32 1.31 0.87
Angina episodes – diary (per week) 4.78±8.20 4.88±7.75 -0.10 0.81
DASI 6.35±4.85 6.20±5.05 0.31 0.49
HIS-GWB Depressed 4.39±0.74 4.27±0.87 0.20 0.009
*The SAQ, QoL, and DASI were measured pre- and post-treatment for both periods; treatment change is the difference ranolazine-placebo in post-pre periods. SAQ=Seattle Angina Questionnaire, DASI=Duke Activity Status Inventory, HIS-GWB=Health Insurance Study-General Well-Being

RWISE Pharm Stress and CMRI OutcomesRanolazine
(N=128) Placebo (N=128)
Treatment Change
P-value
Stress HR 95.17±13.50 98.73±14.15 -3.55 <0.0001
Stress RPP 12082±2707 12611±2796 -523 0.01
Stress MPRI 1.98±0.46 1.96±0.42 0.01 0.88
Stress MPRI-mid subendocardial 1.83±0.48 1.77±0.38 0.06 0.23
PFR 333.3±105.9 328.8±97.1 4.3 0.52
tPFR 163.9±45.3 157.4±37.7 6.6 0.09
Pharm stress and CMRI were measured only post-treatment; treatment change ranolazine vs placeob. HR=heart rate, RPP=rate pressure product, MPRI=myocardial perfusion reserve index, PFR=peak filling rate, tPFR=time PFR

RWISE Angina and Myocardial Perfusion
As the model MPRI-midventricular change increased, SAQ QoL change increased, adjusted for BMI, prior MI and site(top). Similar results were observed with MPRI-mid subendocardial (bottom).
All of the angina variables were tried in the model. Two SAQ variables could enter into the models singly, but not at the same time: SAQ QoL and SAQ-7. Each of these had similar associations with the MPRI variables, but QoL has slightly better model fit statistics.
A higher MPRI number indicates better myocardial perfusion index

RWISE Subgroup Analyses Among subjects with qualifying CRT available CFR and both period MPRI (n=78), lower CFR had significantly greater mid-ventricular MPRI change on ranolazine vs placebo
A higher MPRI number indicates better myocardial perfusion index
MPRI change according to qualifying CFR in subjects with invasive CRT

RWISE Limitations Short-term ranolazine exposureGd MPRI is not a direct measure of CFRSAQ may not measure “angina-equivalents”Invasive CFR determined only in a subset
RWISE Summary and Conclusions Short-term late Na current blockade (ranolazine) effective for effort angina in patients with obstructive CAD, did not significantly improve SAQ angina or myocardial perfusion index in subjects with no obstructive CAD but evidence of CMD
Changes in the SAQ and myocardial perfusion index were directly related, indicating that symptoms are related to myocardial perfusion index in this population
Angina and perfusion index improved in ranolazine-treated subjects with lower baseline CFR, suggesting these subjects should be included in future trials testing traditional and novel strategies


















