By: Rose Fontana BSN, RRNA and Courtney Henderson BSN, RRNA.
32
The Effect of Intravenous Acetaminophen on Opioid Medication Requirements Following Cesarean Delivery By: Rose Fontana BSN, RRNA and Courtney Henderson BSN, RRNA
-
Upload
angel-walton -
Category
Documents
-
view
226 -
download
2
Transcript of By: Rose Fontana BSN, RRNA and Courtney Henderson BSN, RRNA.
The Effect of Intravenous Acetaminophen on Opioid Medication Requirements Following Cesarean Delivery
By: Rose Fontana BSN, RRNA and Courtney Henderson BSN, RRNA
Acknowledgements
• Webster University• Committee Members:
o Michael Burns MS, CRNAo Christopher Black MS, CRNAo Jill Stulce PhD(c), CRNA
• Phelps County Regional Medical Center
Cesarean Delivery (Martin et. al, 2013)
• Most common surgical procedure performed in U.S.o 2012: 1,296,531
• Major abdominal surgery• High postoperative pain• Pain delays ambulation,
mother-infant bonding, and decreases patient satisfaction
Postoperative Pain Opioids: first line of treatment Many adverse effects
Harmful to mom and possibly to baby
Delays bonding and ambulation
A multimodal analgesic regimen decreases the need for rescue opioids
Acetaminophen (Mehta & Shah, 2010)
• First synthesized in 1878 by Morse
• First used in clinical practice in 1887
by Von Mering
• N-acetyl-p-aminophenol
• Non-salicylate antipyretic
• Non-opioid analgesic
Acetaminophen(Mehta & Shah, 2010)
● Mechanisms of Action- not fully understood
○ Inhibits prostaglandin synthesis○ Serotonergic pathway activation○ Cannabinoid receptor stimulation○ N-methyl-D-aspartate receptor inhibition
Problem Statement
• Even after spinal anesthesia and TAP blocks, patients continue to experience breakthrough pain in the early post cesarean delivery period. A multimodal analgesic regimen can decrease the amount of rescue opioid medications necessary for adequate pain control with less unwanted opioid side effects.
Purpose of the Study
• The purpose of this study was to determine if the administration of intravenous acetaminophen following cesarean delivery leads to a decrease in postoperative opioid requirements
Hypotheses• Null Hypothesis: The use of intravenous
acetaminophen in combination with a multimodal pain management regimen will not decrease postoperative opioid requirements after cesarean delivery
• Alternative Hypothesis: The use of intravenous acetaminophen in combination with a multimodal pain management regimen will decrease postoperative opioid requirements after cesarean delivery
Phelps County Pain Management Protocol
• Each cesarean delivery patient will receive:o Subarachnoid block with 0.75% bupivacaine in
8.25% dextroseo Intrathecal morphine 0.1mgo Intrathecal fentanyl 10-15 mcgo TAP block with 20-30 mL 0.5% ropivacaineo Ketorolac 30 mg every 6 hours for the first 24
hours postoperatively
Research Question
Does intravenous acetaminophen decrease postoperative opioid requirements following cesarean delivery?
Research Design• Retrospective analysis of 329 patient charts
o 145 cases during January 1, 2012-November 2012 Control Group= No Acetaminophen
o 182 cases during November 2012- December 31, 2013 Experimental Group= 1 gram of IV Acetaminophen every
six hours for 24 hours
• The opioid medication consumption for each patient was totaled and converted to IV morphine equivalents using an opioid analgesic converter from GlobalRPH
Inclusion Criteria• Patients included in this study:
o Females undergoing elective cesarean delivery
o Each received entire pain management protocol: Subarachnoid block with 0.75% bupivacaine in 8.25%
dextrose Intrathecal morphine 0.1mg Intrathecal fentanyl 10-15 mcg TAP block with 20-30 mL 0.5% ropivacaine Ketorolac 30 mg every 6 hours for the first 24 hours
postoperatively
o Acetaminophen group also received 1 g of IV acetaminophen every 6 hours for the first 24 hours postoperatively
Exclusion Criteria• Exclusion criteria for this study
included:o Failure to receive the entire pain
management protocolo General anesthetico ICU admission or another surgery within 24
hourso Contraindication to regional anesthesiao Additional gynecological surgerieso Emergency cesarean delivery
Non-Acetaminophen Group• 145 charts were reviewed
o 40 charts were excluded due to an incomplete pain management protocol
o 27 charts were excluded due to additional gynecological procedures
o 13 charts were excluded due to conversion to general anesthesia, intensive care unit admission or additional surgery within 24 hours of cesarean delivery, or a multitude of factors
• Total of 65 patients in the non-acetaminophen group
Acetaminophen Group• 184 charts were reviewed
o 55 charts were excluded due to an incomplete pain management protocol
o 26 charts were excluded due to additional gynecological procedures
o 21 charts were excluded due to conversion to general anesthesia, intensive care unit admission or additional surgery within 24 hours of CD, or a multitude of factors
• Total of 82 patients in the acetaminophen group
Statistical Analysis
• Data was recorded in Microsoft Excel and converted for analysis using GraphPad Prism 5.0
• A significance level of p<0.05 was used in all analyses
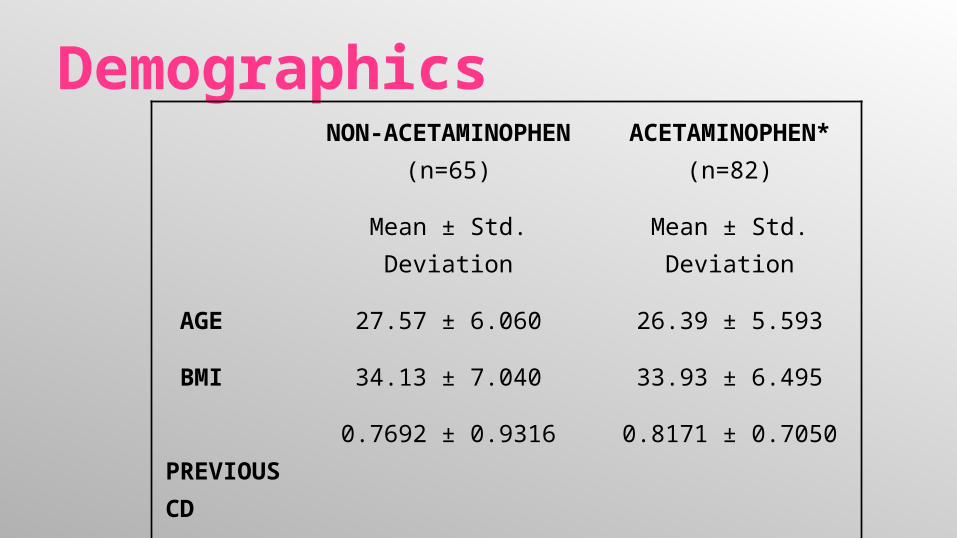
Demographics NON-
ACETAMINOPHEN (n=65)
ACETAMINOPHEN* (n=82)
Mean ± Std. Deviation Mean ± Std. Deviation
AGE 27.57 ± 6.060 26.39 ± 5.593
BMI 34.13 ± 7.040 33.93 ± 6.495
PREVIOUS CD
0.7692 ± 0.9316 0.8171 ± 0.7050
ASA 1/2/3
2/60/3 4/74/4
*Experimental group received 4g IV acetaminophen in the first 24 hours postoperatively in addition to the pain management protocol
Demographics
• Age: No significant difference (p=0.2237)• BMI: No significant difference
(p=0.8600)• Previous Cesarean Delivery: No
significant difference (p=0.7319)• ASA I/II/III
• Non-Acetaminophen Group- 2/60/3• Acetaminophen Group- 4/74/4
Assumptions
• Assumptions relative to this study includeo All anesthetic procedures were
performed and documented correctlyo Opioid medications and intravenous
acetaminophen were administered and documented accurately

Primary Findings: Mean Opioid Usage• Non-Acetaminophen: 3.33 mg of
morphine • Acetaminophen: 3.07 mg of morphine
Results
• Mean Morphine Consumption:
o One-tailed t-test showed: No significant decrease (p=0.3456)
Results
• No statistically significant decrease in postoperative morphine consumption with the addition of IV acetaminophen to a multimodal pain management regimen following cesarean delivery• The results are not conclusive for a
benefit of the addition of the IV acetaminophen• We accept the null hypothesis
Incidental Findings• Multimodal pain management protocol without
acetaminophen •mean opioid consumption was 3.33mg
• A study by Girgin, Gurbet, Turker, Aksu, and Gulhan
•Intrathecal morphine 0.1-0.4mg + 0.5% bupivacaine
•mean opioid consumption was 23.5mg• Supports use of this multimodal pain
management protocol
Incidental Findings:• A total of 28 patients from both the non-
acetaminophen and acetaminophen groups were excluded for no ketorolac administration
• These patients’ morphine consumption was calculated and found to be greater than those that received the entire pain management protocol
Incidental Findings• n=147 all those included in the study
o mean opioid consumption: 3.187 mg
• n=28 no ketorolac o mean opioid consumption: 7.429 mg
• A Welch’s correction was applied to a t-test to analyze significanceo There was a significance found with p= 0.0043• Although corrections were made for the variance in
sample size, it makes the significance of the p value unreliable
• cannot be considered dependable results• warrants further study
Incidental Findings• of the 28 that did not receive ketorolac
o n=11 non-acetaminophen group mean morphine consumption was: 6.955 mg
o n=17 acetaminophen group mean morphine consumption was: 7.735 mg
o p=0.7814
• No significance that intravenous acetaminophen lowers postoperative opioid requirements in the absence of ketorolac
Future Recommendations
• Perform a prospective randomized double-blind study evaluating the effect of ketorolac as part of a multimodal analgesic regimen post cesarean deliveryo Incidental findings of this study suggest
investigation of ketorolac efficacy would be advantageous
Limitations• Limitations for this study include
o Only measured opioid consumption for 24 hourso Did not evaluate
pain scores time to first ambulation sedation scores patient satisfaction
o Retrospective: no influence on multimodal pain management regimen, already in place dependent on staff to give appropriate postoperative
doseso Intrathecal morphine shortage
Future Recommendations
• Perform this study as a prospective randomized double-blind study with better controlled variableso Same surgeon and anesthesia provider placing the
spinal and TAP blocko The same postoperative opioid medicationso Identical anesthetic and analgesic dosages
?? Questions ??
References• Martin, J., Hamilton, B., Ventura S., Osterman M., Curtin, S.,
& Mathews, T. J., (2013). Births: Final data for 2012. National Vital Statistics Reports; National Center for Health Statistics, 62(9), 1-87.
● Mehta, V., & Shah, S. (2010). Paracetamol: the forgotten drug. British Journal Of Hospital Medicine (London, England: 2005), 71(11), 606-607.
● Girgin, N., Gurbet, A., Turker, G., Aksu, H., & Gulhan, N. (2008). Intrathecal morphine in anesthesia for cesarean delivery: dose-response relationship for combinations of low-dose intrathecal morphine and spinal bupivacaine. Journal of Clinical Anesthesia, 20(3), 180-185.