By Prof. Dr. Abdel Fatah Ali Ismael Head of Vascular Surgery Department Al Azhar University F.R.C.S...
33
-
Upload
samir-laughter -
Category
Documents
-
view
216 -
download
2
Transcript of By Prof. Dr. Abdel Fatah Ali Ismael Head of Vascular Surgery Department Al Azhar University F.R.C.S...



ByBy
Prof. Dr. Abdel Fatah Ali IsmaelProf. Dr. Abdel Fatah Ali IsmaelHead of Vascular Surgery DepartmentHead of Vascular Surgery Department
Al Azhar UniversityAl Azhar University
F.R.C.S Lon.F.R.C.S Lon.
F.R.C.S Ed.F.R.C.S Ed.

IntroductionIntroduction

Ultrafiltration of fluid from the leg of the capillaries must be removed from interstitial compartment and if not it will lead to edema, If ISF compartment is doubled edema will be clinically detectable this usually occur when lymphatics are unable to clear the ISF compartment. Particles enter the initial lymphatics through inter endothelial openings and pores, large particles are actively phagocytosed by macrophages and transported through the lymphatic system intracellularly.

2-4 liter of lymph are transported to the venous system every day.
Lymph pulsation include active, passive motion, squeezes lymph from ISF space through lymphatics aided by arterial pulsation, respiration, massage and contraction of lymphangioms.
Valves prevent back flow of lymph.

LYMPHEDEMADefinition: Abnormal collection of interstitial lymph
fluid due to congenital maldevelopment of lymphatics or due to 2nd lymphatic obstruction.
It affect 2% of population causing limb swelling.

Scope of the clinical problem:
It causes severe emotional, psychological distress particularly in late cases and on occurrence of complication.
If early diagnosed simple measures can be highly effective at this stage and can prevent the development of disabling, late disease which is often very difficult to treat.

Etiology: Lymphedema may be 1ry or 2ry
(A) 1ry lymphedema: It is due to “developmental error” in the
lymphatics. According to the severity of this error, the lymphedema may appear:
a) At birth (<1 year) Lymphedema congenita (if familial, it is called Milroy’s disease).
b) Between 1-35 years of age Lymphedema praecox.
c) Later (> 35 years) lymphedema tarda.

This congenital variety may be hereditary or familial (Milroy’s disease) which is very rare.
The edema may involve one or both lower limbs. It continues throughout life & does not of itself
produce any constitutional disturbance.
According to Lymphography: Abnormality may assume one of 4 patterns:
1. Aplasia (15%): The main SC lymph trunks can not be demonstrated, while the dermal lymphatic plexus is dilated.
2. Hypoplasia (55%): The main SC lymphatics are few & under-developed i.e. in number & diameter (only one minute lymph vessel can be visualized at the ankle).
3. Hyperplasia (35%): Lymph trunks are dilated & varicosed ( in number & length & become tortuous) + incompetent valves. It may be associated with cong. A-V fistula or with dermal backflow.
4. Dermal backflow (Chylous reflux): The retrograde flow causes abnormal filling of the dermal plexus.

Predisposing factors: These factors may cause the “developmental
error” to be evident:1. Any inflammatory process ends by resolution or
“fibrosis” which will strangle the remaining lymphatics & will end by the appearance of lymphedema.
2. Trauma: it may be mild (a blow), or severe (fracture).
3. Pregnancy.
4. Puerperal sepsis.
5. However, most cases of 1ry lymphedema appear spontaneously without any precipitating factor.

Secondary lymphoedema:Causes:
Trauma (operative – accidental).
Inflammation.
Filariasis.
Post-phlebitic leg.
Irradiation.
Malignancy.
Allergy.

Filariasis: This is the most common cause of lymphedema
more prevalent in Africa, India, South America (5-10%).
Caused by Wuchreria bancrofti, spread by mosquito.
It causes proximal lymphatic obstruction by adult parasites and associated lymphatic inflammation due to immune response of the host.

In lead to: Fever. Headache. Malaise. Lymphadenopathy. Lymphangitis. Cellulites. Abscess (in the acute stage) and lymphedema –
hydrocele and abdominal lymphatic varices in the chronic stage.
Diagnosed by night blood film and complement fixation test.
Treated by diethyl carbamazine.

Clinical classification of lymphedema:
Subclinical
(latent)
There is excess interstitial fluid and histological
abnormalities in lymphatics and lymph nodes, but
no clinically apparent lymphedema
IEdema pits on pressure and swelling largely, or
completely disappears on elevation and bed rest.
IIEdema does not pit and does not significantly
reduce upon elevation
IIIEdema is associated with irreversible skin changes,
i.e. fibrosis, popillae

Symptoms frequently experienced by patients with lymphedema:
Constant dull ache, even severe pain. Burning and bursting sensations. General tiredness and debility. Sensitivity to heat. Pins and needles. Cramps. Skin problems, including dehydration, flakiness,
weeping, excoriation and breakdown. Immobility, leading to obesity and muscle wasting. Backache and joint problems. Athelet’s foot. Acute infective episodes.

Signs of lymphedema:High molecular weight substances will lead to the
development of hyperplasic fibrotic dermal thickening, hyperkeratosis, chronic eczema, fissuring, verrucae, papillae (warts), it also will lead to fungal injection of the skin and nails.
Investigation of lymphedema: Routine tests: Lymphangiography. Isotope lymphosintigraphy. Computerized tomography. (CT). Magnetic resonance imaging (MRI). Ultrasound. Pathological examination.

Causes of a “Swollen Limb”
Central Peripheral
Medical causes Bilateral edema
Surgical causes Unilateral edema
Cardiac: CHF- constrictive pericarditis.
Renal: acute nephritis-nephrotic syndrome.
Hepatic: cirrhosis, end-stage liver disease (ESLD) or liver failure (LF).
Nutritional: protein-losing enteropathy, thiamine deficiency.
Endocrinal: cushing syndrome-myxedema.
Allergic.
Venous disease: DVT. Aterio-venous disease: A-V fistula. Lymphatic disease: Lymphedema
(1st-2nd). Miscellaneous:
1. Lipidema (lipodystrophy/lipomatosis).
2. Neurofibromatosis.3. Erythrocyanosis frigida.4. Injuries: fractures-muscle
contusion.5. Tight bandage or plaster.6. Infection: cellulitis.7. Tumors: deep cavernous
heamangioma!

Complications:
Local infection.
Systemic infection.
Lymphangiosarcoma, kaposi’s, sarcoma
basal cell carcinoma and lymphoma.

Treatment of lymphedema:Early treatment is highly effective, late disease is
very difficult to treat.Patient cooperation in the treatment is essential
as the patient will take the most important part of the treatment by himself, every patient with lymphedema should receive the following:
An explanation as to why their limb is swollen and the underlying cause of lymphedema and he should be instructed to:

Use an electric razor to depilate. Never let the skin become macerated. Treat cuts and grazes promptly (wash, dry, application
of antiseptic and a plaster). Use insect repellent sprays and treat bites promptly
with antiseptics and antihistamines. Seek medical attention as soon as limb becomes hot,
painful or more swollen. Do not allow blood to be taken from, or injections to be
given into the affected arm (and avoid blood pressure measurement).
Protect the affected skin from sun (shade, high factor sun block).
Consider taking antibiotics if going on holiday.

Guidance on skin hygiene and care and, specifically, the avoidance of acute infective episodes.
Antifungal prophylactic therapy to prevent athelet’s foot.
Rapid access to antibiotic therapy and, if necessary, hospital admission for acute infective episodes.
Protect hands when washing up or gardening, wear a thimble when sewing.
Never walk barefoot and wear protective footwear outside.

Appropriate instructions regarding exercise
therapy.
Manual lymphatic drainage (MLD).
Multilayer lymphedema bandaging (MLLB).
Compression garments and, if appropriate,
specialized footwear.
Advice on diet.
Access to support services and networks.

I-Medical treatment including the following: Relief of pain by non opioid and opioid
analgesics. Reduce swelling by decongestive lymph-
therapy (DLT).a. Manual lymph therapy (MLT) manual
massage).b.Multilayer lymph bandage + exercise
(MLLB).c. Skin care

II- Surgical treatment:1. Bypass surgery (lymphovenous shunt).
2. Reducing surgery:
a) Sistrunk: wedge removal and skin closure.
b) Homans: subcutaneous tissue removed and skin closure.
c) Thompson: denuded skin sutured to deep fascia.
d) Charles: remove every thing cover raw area by skin graft.
III- Treatment of complication accordingly


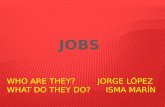
Before treatment Before treatment
The same limb after treatment The same limb
after treatment

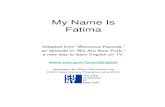
Before treatment Before treatment The same limb after treatment The same limb
after treatment

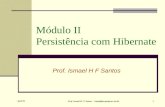
Before treatment Before treatment The same limb after treatment The same limb
after treatment

Before treatment Before treatment The same limb after treatmentThe same limb after treatment

Before treatment Before treatment The same limb after treatment The same limb
after treatment

Before treatment Before treatment The same limb after treatment The same limb
after treatment