
By: Dr. Khalid R. Murshid
96
1 By: Dr. Khalid R. Murshid
Transcript of By: Dr. Khalid R. Murshid

1
By:
Dr. Khalid R. Murshid

2

Embryology
Branchial pouches:
3rd :
inferior parathyroid and thymus.
4th :
superior parathyroid and ultimobranchial bodies which form the parafollicular ( c ) cells of the thyroid.
3

Anatomy
Position Of The Parathyroids:
The superior parathyroid glands
The inferior parathyroid glands
4

5

6

1- HYPERPARATHYROIDISM
1ry
2ry
3ry
2- HYPERCALCEMIA
3- PARATHYROID CARCINOMA
7

Classification
Clinical Presentation
Lab Tests
Imaging Studies
Treatment
8

• 1ry:
hyperfunction of the glands.
oversecretion of PTH due to :
Adenoma
Hyperplasia
or rarely, Carcinoma of the parathyroid glands.
2ry: reaction of the glands to hypocalcemia caused by chronic renal
failure.
3ry: Result from hyperplasia of the glands and loss of response to
serum calcium levels.
most often seen in patients with chronic renal failure 9

Epidemiology / Frequency - Incidence of 1ry HPT = 1 in 2,500. - between the 5th and 7th decades . -2-4 X more common in women , rare in children. - -Approximately 100,000 new cases of HPT are reported in the United States annually.
10

Primary HPT
Asymptomatic or vague nonspecific symptoms
elevation of serum calcium levels
Hypercalcemia
- related signs and symptoms
- "stones, bones, abdominal groans and psychological overtones".
11

Is the most common cause of hypercalcemia
Etiology:
1. one (90 %) or, two (2 %) benign parathyroid adenoma(s)
2. Multiglandular hyperplasia (8 %)
3. Parathyroid carcinoma (<1 %)
12

PUD
Pancreatitis
HTN
MEN Syndrome
Familial HPT
Gout
Previous Radiation to neck
Band keratopathy 13

Renal (2ry) HPT - in patients with chronic renal disease and
intestinal malabsorption
- dramatic elevations of the PTH level
- normal or low serum calcium levels,
- marked bone demineralization related to renal osteodystrophy, soft tissue calcifications, and intense pruritus.
-
14

Labs: High PTH, low Ph and almost normal calcium
Treatment: - Non Surgical…Oral calcium and vitamin D
- Surgery if;
1. Uncontrolled bone pain
2. Fractures
3. Pruritis
4. Ectopic calcifications
15

3ry HPT - Presents similar to 2ry HPT.
- Patient had near-total parathyroidectomy or untreated 2ry HPT.
- - Progressive hyperphosphatemia of renal disease stimulates PTH, which causes hypercalcemia.
- High PTH, normal or high Ca.
- Corrected after renal transplant
16

General / Clinical Features: <1% of cases of HPT
equally in males and females, and rarely before age 30yrs
Usually functional, producing symptoms of HPT and hypercalcemia but more severe, with:
- serum calcium levels greater than 14 mg/dL
- Markedly elevated serum PTH levels. If Untreated, leads to severe symptoms of HPT.
palpable mass semifixed
LN and distant mets usually not present at Dx
17

18

PTH:
Increases serum Calcium through:-
1. Enhancing gastrointestinal absorption of calcium.
2. Stimulating the production of vitamin D3.
3. Inhibiting renal calcium excretion.
4. Increasing bone resorption .
19

Effects of elevated serum calcium are:
- Central nervous system - Mental alterations, impaired memory, emotional instability, depression, sleepiness, and coma
- Neuromuscular - Proximal muscle weakness, joint and muscle pain due to calcium deposition, pruritus, and abnormal leg movements during sleep
- Gastrointestinal - Peptic ulcer, pancreatitis, nausea, vomiting, reflux, and loss of appetite
- Renal - Kidney stones, polyuria, nocturia, and renal failure with uremia
- Cardiovascular - Hypertension, left ventricular hypertrophy unrelated to hypertension
- Eye – Conjunctivitis, band keratopathy
- Skin – Pruritus
20

Hypercalcemia
BONES;
arthralgia, path. #
STONES;
renal stones, renal failure, polyuria, polydipsia
ABDOMINAL GROANS;
PUD, pancreatitis, constipation
PSYCHIC MOANS; depression,
fatigue, weakness
21

Parathyroid 1ry HPT Nonparathyroid Endocrine Thyrotoxicosis Pheochromocytoma Acute adrenal
insufficiency Malignancy Solid tumors Lytic bone metastases Lymphoma and leukemia Infections Sarcoidosis Tuberculosis
Medications Calcium
supplementation Thiazide diuretics Vitamin A or D
intoxication Lithium Dietary Milk Alkali Syndrome Other Paget’s Disease Immobilization
22

Serum calcium or Ionised Ca2+: - In cases of 1ry or 3ry HPT heightened PTH leads to
increased serum calcium (hypercalcemia) due to:
- increased bone resorption
- reduced renal clearance of calcium
- increased intestinal calcium absorption
- Elevated ionized (Ca++) calcium may be a more reliable indicator of HPT.
- By contrast, in 2ry HPT effectiveness of PTH is reduced.
23

Serum Phosphate:-
- In 1ry HPT, serum phosphate levels are
abnormally low as a result of decreased renal tubular phosphate reabsorption.
- This contrasts with 2ry HPT, in which serum phosphate levels are generally elevated because of renal disease.
24

Laboratory Studies: Simultaneous calcium and PTH levels should be determined. Serum calcium and parathyroid hormone levels are usually elevated more markedly
than in benign 1ry HPT.
High Ca, Alk. Ph, PTH
25

The gold standard of diagnosis is an elevated PTH level. Once that has been confirmed, one is to determine whether the HPT is 1y or 2ry in origin by obtaining a serum calcium level:
3ry HPT has a high PTH and a high serum calcium. It is differentiated from 1ry HPT by a history of chronic renal failure and 2ry HPT.
26
PTH
serum calcium
Chronic renal failure
likely type of HPT
high
high
- ve 1ry HPT
high
low or normal
+ ve
2ry HPT
high
high
+ ve
3ry HPT

MEN I:
Parathyroid/Pancreas/Pituitary
MEN IIa:
Medullary/ Pheo/ Parathyroid
27

Imaging Studies: Radiographs:
Hand films - May show subperiosteal bone resorption of the distal
phalanges.
Skull films - Have a characteristic "ground glass" or "salt and
pepper" appearance.
In severe cases, plain films reveal the classic bone finding, osteitis fibrosa cystica. It consists of bone cysts with or without pathologic fractures. These cysts are also known as Brown tumors.
28

29

30

31

High-resolution ultrasonography:
- economic and informative.
- Shows enlarged glands and their relations and L.N.s.
-
- Can reveal multiple adenomas, hyperplasia of all 4 glands, and glands in ectopic cervical locations.
-
- Can not identify mediastinal adenomas. 32

33

34

CT scan:
- greater detail .
- Precise location of gland in relation to anatomy.
- Helpful in locating mediastinal adenomas
- helpful in staging and detecting metastatic disease.
35

Technetium-99m labeled Sestamibi Scan: - specific affinity for abnormal parathyroid tissue.
- Also taken up by thyroid, but diminishes and is retained in the parathyroid.
- Is useful in identifying single and multiple parathyroid adenomas and hyperplasia.
- reveals ectopic glands.
- Lesions < 2cm in size are often difficult to pick up.
36
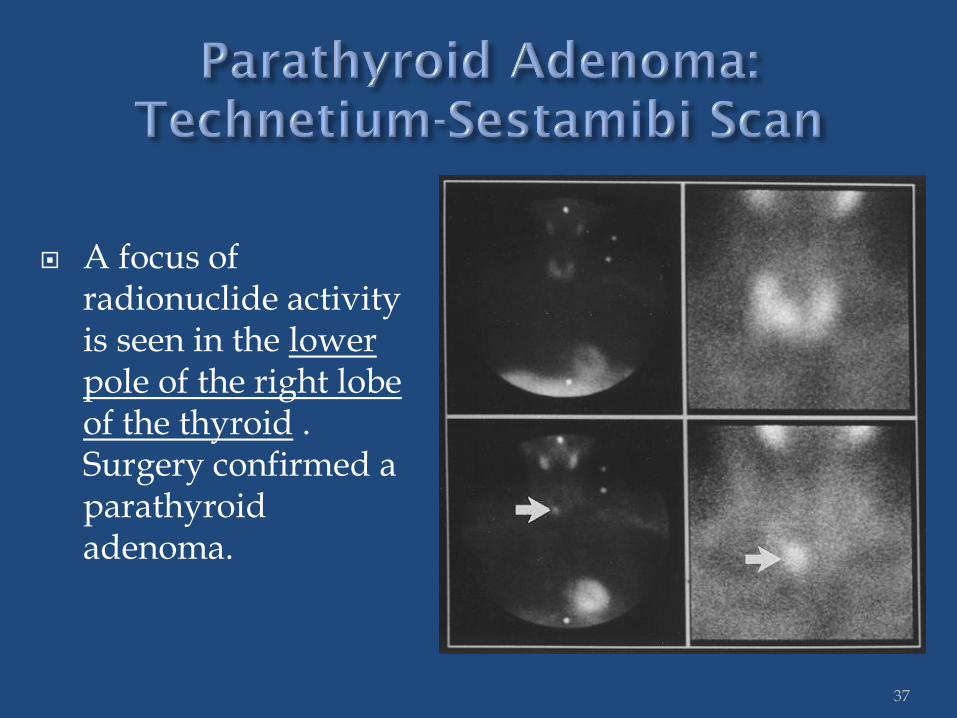
A focus of radionuclide activity is seen in the lower pole of the right lobe of the thyroid . Surgery confirmed a parathyroid adenoma.
37

THE INITIAL IMAGE (A)
shows the thyroid (th), submandibular glands (s), and a parathyroid adenoma (arrow).
A DELAYED 2-HOUR IMAGE (B) the radioactivity has faded in the thyroid and submandibular glands.
38

Technetium 99m Sestamibi Scan
39

MRI:
- Provides excellent contrast resolution.
- Images can be formatted in multiple planes (ie, axial, coronal, sagittal).
- Increased vascularity of the adenomas is ideal for identification with this modality.
- - May be useful in locating mediastinal adenomas.
40

MRI
41

Selective venography :-
42

- Combination of ultrasonography and sestamibi scan provides maximum information and is cost effective.
- CT scan or MRI for mediastinum adenomas may be required when an adenoma is suspected in the thorax.
43

- Endocrinologists should be consulted for HPT.
-
- Treatment for the three different types of HPT vary.
- Treatment is first directed at hypercalcemia.
- If HPT is caused by a tumor, it will almost always progress as the tumor grows, therefore Sx is a must.
- Testing for HPT should include:
PTH
Calcium level
Bone density
Vitamin D
Phosphorus
44

-Medical Treatment:-
-Medical management of HPT is generally reserved for patients with poor medical conditions and who are poor surgical candidates.
45

Indications for surgery Symptomatic patients fit for surgery Type of Sx:
Solitary parathyroidectomy for adenomas
3.5 parathyroidectomy for multiglandular hyperplasia OR
Total parathyroidectomy and reimplantation of 50 mg of gland in neck or forearm
46

Consultations: Medical endocrinologist - Experienced surgeon - Interventional radiologist - Percutaneous ablation or embolization
47

Medical Care:
No effective medical therapy is known.
Primarily geared toward management of the hypercalcemia
For rapid treatment of severe hypercalcemia: Volume loading and diuresis with a calcium-wasting
loop diuretic is the treatment of choice.
48

Operative management:
Resection of the parathyroid cancer is the only effective Rx.
The goal is to remove the tumor en bloc
with any adherent tissue, and any enlarged lymph nodes.
49

50

ACCORDING TO SITE CORTEX
ADENOMA FUNCTIONING NON-FUNCTIONING
CARCINOMA FUNCTIONING NON-FUNCTIONING
MEDULLA NEUROBLASTOMA PHEOCHROMOCYTOMA
BENIGN MALIGNANT
INCIDENTALOMAS FUNCTIONING
NON-FUNCTIONING
ADRENOCORTICAL CARCINOMAS 1RY
FUNCTIONING NON-FUNCTIONING
2RY
51

BENIGN: Medulla
Benign Pheochromocytoma
Cortex Z. Glomerulosa Z. Fasiculata Z. Reticularis
MALIGNANT: 1ry
Medulla Neuroblastoma Malignant Pheochromocytoma
Cortex Adreno-cortical Carcinoma
2ry
52

General:
- 1-10% of CT scans and MRIs detect adrenal incidentalomas (AIs) that are 5 mm or larger.
- Bilateral AMs should always raise the possibility of
hemorrhage. - 80% of AAs are nonfunctional and benign.
- 20%of AAs are either functional or malignant. - If Suspicion of Malignancy, FNA but R/O pheochromocytoma
first
53

Approach Considerations The 2 main concerns with regard to an adrenal incidentaloma (AI) are: - (1) whether it is hormonally active (functional) - (2) whether it is malignant.
- Pheochromocytomas should be considered in all adrenal adenoma (AA) cases because:
- relatively common
- often overlooked
- failure to recognize may lead to death.
54

SITE PHYSIOLOGY PATHOLOGY
MEDULLA
EPINEPHRINE NOREPINEPHRINE
NEUROBLASTOMA PHEOCHROMOCYTOMA
CORTEX Z. Glomerulosa
ALDOSTERONE
CONN’S DISEASE
Z. Fasiculata GLUCOCORTICOIDS
CUSHING’S SYNDROME
Z. Reticularis
SEX HORMONES
ADRENO-GENITAL SYNDROME
55

- The medulla is located at the center of the gland.
- It is composed of neuroendocrine (chromaffin) cells which produce and release epinephrine (adrenaline) into the bloodstream in response to activation of the sympathetic nervous system.
- Neuroblastoma and pheochromocytoma are the two most important tumors which arise from the adrenal medulla.
56

- aggressive cancer
- common pediatric cancer
- rapidly enlarging abdominal mass.
- highly curable when detected early
- Often produce elevated levels of catecholamine precursors, such as vanillylmandelic acid (VMA) and homovanillic acid, and may produce severe watery diarrhea through production of vasoactive intestinal peptide (VIP).
- Treatment of neuroblastoma includes surgery and radiation therapy for localized disease, and chemotherapy for metastatic disease.
57

Pheochromocytoma
General:
•Peak incidence is 40-50 years •10% tumor •(10% bilateral, 10% malignant, 10% extra-adrenal, 10% multiple, 10% children and 10% familial) •May be found extra-adrenally in abdominal paravertebral sympathetic chain or ganglia in UB, pelvic nerves 58

Clinical Presentation: Tense, anxious, and cold sweating Extreme Tachycardia, flushing Tumors are not palpable bimanually Sustained or episodic hypertension Triad of intermittent attacks of
palpitations, sweating and headache Anxiety, vertigo Abdominal, loin pain
59

Labs: Serum catecholamines 24-hour urine catecholamines, VMA Plasma free metanephrine…. sensitivity
99%
Imaging: USG, CT, MRI, MRA MIBG nuclear study
60

U/S image of pheochromocytoma
61

CT with contrast MRI
62
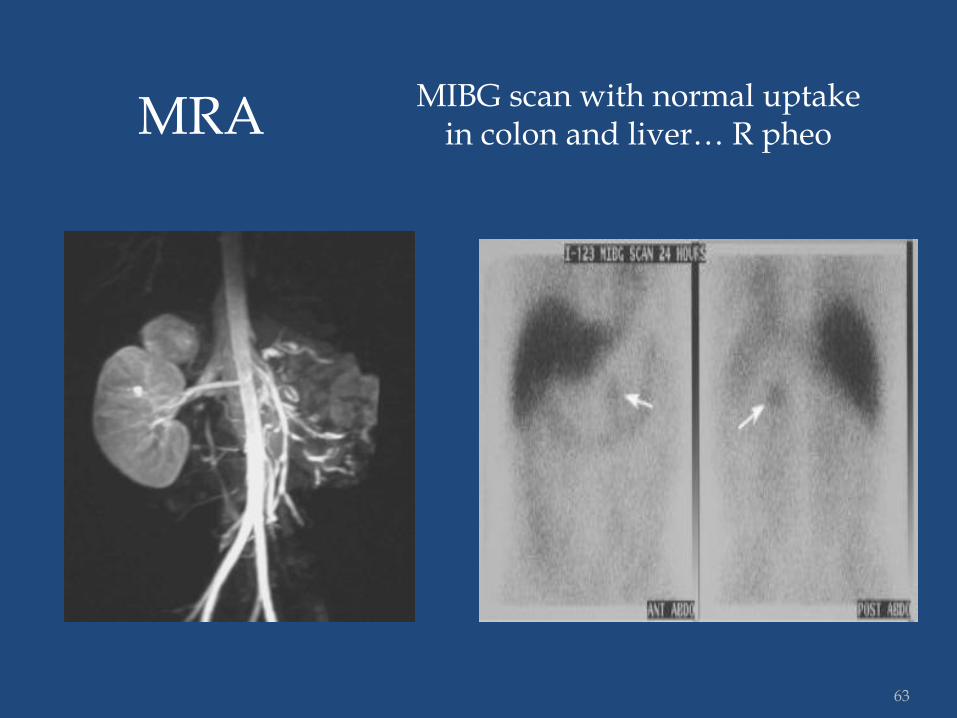
MRA MIBG scan with normal uptake
in colon and liver… R pheo
63

MIBG scan
Extra adrenal tumors Recurrent tumors Multiple tumors
64

TREATMENT: - PRE-OP:
α-adrenergic blockade, +/- propranolol
- INTRA-OP:
IV fluid, alpha or beta blockers
Minimal tumor manipulation
- POST-OP: fluid, dopamine, angiotensin, norepinephrine and Follow-up q6m
65

DIAGNOSIS :
Spread and Metastasis
TREATMENT :
Debulk
Medical Rx for hypertension
Chemo Rx
RRx for bony mets
PROGNOSIS :
5 yr survival – 50%
66

Adrenocortical Adenomas:
- Benign
- >30 years old.
- About 15% are "functional", producing Hormones resulting in endocrine disorders such as Cushing’s Syndrome, Conn’s Disease (hyperaldosteronism), virilization of females, or feminization of males.
67

SITE PHYSIOLOGY PATHOLOGY
MEDULLA
EPINEPHRINE NOREPINEPHRINE
PHEOCHROMOCYTOMA NEUROBLASTOMA
CORTEX Z. Glomerulosa
ALDOSTERONE
CONN’S DISEASE
Z. Fasiculata GLUCOCORTICOIDS
CUSHING’S SYNDROME
Z. Reticularis
SEX HORMONES
ADRENO-GENITAL SYNDROME
68

Mineralocorticoid
Secreted By Zona Glomerulosa
Action On Distal Tubules:-
Absorption Of :
Na+ and H2O
Excretion Of :
K+ , H+ and Mg 2+
69

CLINICAL PRESENTATION:- - Na+ reabsorption------
- HYPERTENSION – Headache
- K+ excretion------------
- HYPOKALEMIA- Weakness
- Polyuria
- polydipsia
- nocturia
- metabolic alkalosis
- tetany 70

PRIMARY:
From the Adrenal:
Adenoma (Conn’s Syndrome)
Hyperplasia
Carcinoma
SECONDARY:
Outside the Adrenal
71

General: - Incidence:- 0.5% of Hypertensives - Sex:- 2F : 1M - Age:- 30-50 yrs - Etiology:- Adenoma 70% Hyperplasia 30%
72

Labs:- - The test of choice is a plasma aldosterone–to–
renin ratio.
- A plasma aldosterone concentration–to–renin ratio greater than 30 and a plasma aldosterone concentration of greater than 0.5 nmol/L (18 ng/dL) are suggestive of primary aldosteronism.
73

Localization :- - CT Scan
- Iodocholesterol Scan
- Venous Assay
74

Treatment :- - Medical :-
diet, K+
Spironolactone, Amelioride, Nifedipine
- Surgical :-
pre-op:- restore K+ to normal
operative:- Open / Laparoscopic
post-op:- adequate salt in diet, Fluronef
75

Operative Complications Of Hypokalemia:
Arrhythmia
Tetany ( due to metabolic alk)
Digoxin Toxicity
Renal Failure
Respiratory Paralysis
76

Results of Surgery :-
Cure of Hypokalemia – 100%
Cure of Hypertension - 80%
77

Cushing’s Cushing's Syndrome: -Pharmacologic glucocorticoid use for the treatment of inflammatory disorders.
Cushing's Disease: Glucocorticoid excess caused by an ACTH-hypersecreting pituitary microadenoma
Primary Adrenal Cushing's Syndrome: Is caused by autonomous adrenal cortisol production by adenoma, associated with an undetectable ACTH level
78

79

Clinical features
Truncal Obesity – 90% Easy bruising -55% Striae – 70% Muscle weakness – 65% Osteoporosis – 55% Psychosis - 50% Plethora (a red facial appearance caused by thinning of the skin) Menstrual / sexual dysfunction – 75% Hirsutism /Acne – 70% Hypertension – 85% Hyperglycemia/ Glucosuria – 80% Edema / Hypo K+ - 40% Polyuria – 15% Delayed wound healing – 55% Pancreatitis 80

INVESTIGATIONS:
Labs: Serum and urinary cortisol levels
High or low ACTH levels
Imaging: MRI abdomen
MRI head…pituitary microadenoma
CT scan abdomen 81

TREATMENT Adrenelectomy …open or laparoscopy
82

83

84

85

Cushing’s disease :- mitotane, enz. Inhibitors, RRx(1ry and bony mets). Sx, bil. Adrenalectomy. Trans-sphenoidal Hypophesectomy
Adrenal Tumor :- Sx, mitotane for CA.
Ectopic ACTH :- Sx, bil. Adrenalectomy, palliative meds.
86

Rare but highly aggressive.
Any age.
May be:
Functional , producing steroid hormones and consequent endocrine dysfunction,
Non-Functional , presenting only after local or distant spread.
The most effective treatment is surgery, although not feasible for many patients. Chemotherapy, RRx, and hormonal therapy may also be employed.
The overall prognosis is poor 87

Classifying adrenal cancers:
I - Functional or nonfunctional
- More recent reports suggest that nonfunctional ACs may be more common than previously suggested.
- Virtually all feminizing adrenal tumors in men are malignant.
II - Primary and secondary metastatic adrenal tumors
88

Most common potential
primaries include the
following:
Lung
Breast
Melanoma
Renal cell carcinoma
Extra-adrenal
lymphoma
Leukemias
Pancreatic carcinoma
Colonic carcinoma
Ovarian carcinoma
Adrenomedullary Ts
Malignant pheo
Ganglioneuroblastoma
Neuroblastoma
Primary adrenal lymphoma -
Unilateral or bilateral
Stromal malignancies
Neurofibrosarcoma
Angiosarcoma
Liposarcoma
Fibrosarcoma
Leiomyosarcoma
Myxosarcoma
Malignant teratoma
Familial polyposis coli
Gardner syndrome
Turcot syndrome
MEN-1 89

Clinical Presentation: Relatively rare Present with advanced disease Nonfunctional variants: Approximately 40% of patients with AC. Present with fever, weight loss, abdominal pain and tenderness, back pain, abdominal fullness, or symptoms related to metastases. In other cases, the mass is found incidentally. - The hormonally active variants constitute 60% of cases.
90

Laboratory Studies for malignant tumors exclude excess hormone production.
CT scans and MRI The imaging studies of choice.
- Larger tumors ( > 4 cm) have a greater chance of being carcinomatous..
91

The major imaging features for a possible AC on
adrenal imaging:
- Unilateral.
- Large size (larger than 4 cm in diameter)
- Irregular margin sometimes with local invasion, lymphadenopathy and
metastases.
- Demonstrate a soft-tissue inhomogeneous density on CT scans, which
enhances with contrast (>20 HU).
- They have an intermediate increased intensity on T2-wtd MRIs.
- Hemorrhage shows characteristic images of blood.
- Intralesional calcification
92

Medical management Encompasses: (1) the treatment of endocrine excess syndromes; (2) the use of mitotane or several multi-agent chemotherapy regimens; (3) the treatment and prevention of potential complications; and (4) strategies for palliative and terminal care
issues, including symptom relief and management.
Radiation therapy
- Radiotherapy to the tumor bed may be considered in patients at high risk for local recurrence. - For palliative management of symptomatic metastases to bone or brain, or vena cava obstruction.
93

Surgical Care:
-Surgical resection - When feasible, total resection.
-
- Recurrent local and metastatic disease is
common In such settings, the only effective
treatment is attempted reoperation.
- Laparotomy vs laparoscopic resection.
94
Follow-Up
Even after curative surgery, life-long follow-up
is mandatory because documented cases exist
of AC recurrence more than 10 years after
presumed curative surgery.
95

Prognosis: Overall 5-year survival rate are approximately 20-35%.
Factors affecting Prognosis - Early detection of tumors .
- Total resection .
- Disease stage at diagnosis, Functional AC may have a better prognosis because they present earlier.
- Completeness of resection at surgery - Some suggest that children with AC have a better prognosis than adults.
96











![Al-Aqeedah al-Murshid [Urdu]](https://static.fdocuments.us/doc/165x107/577cb4161a28aba7118c4b69/al-aqeedah-al-murshid-urdu.jpg)





