By: Cecilia Galan- Fernandez, DPPS, DPSHBT, DPSPO Place: 5 th floor ASMPH Date : January 11,2011
88
By: Cecilia By: Cecilia Galan- Fernandez, DPPS, DPSHBT, Galan- Fernandez, DPPS, DPSHBT, DPSPO DPSPO Place: 5 Place: 5 th th floor ASMPH floor ASMPH Date : January 11,2011 Date : January 11,2011 CANCER IN CHILDREN CANCER IN CHILDREN
description
SOLID. By: Cecilia Galan- Fernandez, DPPS, DPSHBT, DPSPO Place: 5 th floor ASMPH Date : January 11,2011. CANCER IN CHILDREN. Cancer Pathogenesis. All kinds of cancer, including childhood cancer, have a common disease process cells grow out of control, develop abnormal sizes and - PowerPoint PPT Presentation
Transcript of By: Cecilia Galan- Fernandez, DPPS, DPSHBT, DPSPO Place: 5 th floor ASMPH Date : January 11,2011

By: CeciliaBy: Cecilia Galan- Fernandez, DPPS, DPSHBT, DPSPOGalan- Fernandez, DPPS, DPSHBT, DPSPO
Place: 5Place: 5thth floor ASMPH floor ASMPHDate : January 11,2011Date : January 11,2011
CANCER IN CHILDRENCANCER IN CHILDREN

All kinds of cancer, including All kinds of cancer, including childhood cancer, have a childhood cancer, have a common disease process common disease process
• cells grow out of control,cells grow out of control,•develop abnormal sizes and develop abnormal sizes and
shapesshapes•ignore their typical boundaries ignore their typical boundaries
inside the bodyinside the body• destroy their neighbor cellsdestroy their neighbor cells•spread (or metastasize) to other spread (or metastasize) to other
organs & tissues organs & tissues • As cancer cells grow, they As cancer cells grow, they demand demand
more nutrition from the bodymore nutrition from the body
Normally, your body forms new cells as you need them, replacing old cells that die
Cell cycle

•Incidence 14/100,000Incidence 14/100,000
•Among all age groups, the most Among all age groups, the most common childhood cancers are common childhood cancers are
leukemia, , lymphoma, and , and brain cancerbrain cancer..
• As children enter their teen years, there is an As children enter their teen years, there is an increase increase in the in the incidence of incidence of osteosarcoma (bone (bone cancer).cancer).
•The sites of cancer are different for each typeThe sites of cancer are different for each type

Pediatric vs. Adult CancersPediatric vs. Adult Cancers
Lifestyle factors that contribute to the Lifestyle factors that contribute to the development of cancer in adults:development of cancer in adults:
smokingsmoking dietdiet obesityobesity occupation occupation prolonged exposure to carcinogenic prolonged exposure to carcinogenic
agentsagents

For the 0-14 yrs oldFor the 0-14 yrs old
Acute leukemias (ALL-most common)Acute leukemias (ALL-most common)Central nervous system tumorsCentral nervous system tumorsNeuroblastomaNeuroblastomaWilms’ tumorWilms’ tumorNon Hodgkin’s LymphomaNon Hodgkin’s LymphomaRhabdomyosarcoma, soft tissue tumors,germ Rhabdomyosarcoma, soft tissue tumors,germ cell tumors, retinoblastoma and bone tumorscell tumors, retinoblastoma and bone tumors
For 15 – 19 yrs oldFor 15 – 19 yrs oldHodgkin’s diseaseHodgkin’s diseaseGerm cell tumorsGerm cell tumorsOsteosarcoma, Ewing’s sarcomaOsteosarcoma, Ewing’s sarcoma

Pediatric vs. Adult CancersPediatric vs. Adult Cancers
Lifestyle factors are not associated Lifestyle factors are not associated with cancer in childrenwith cancer in children
Genetic condition- anomaliesGenetic condition- anomaliesFamily historyFamily historyEnvironmental- ionizing radiation, Environmental- ionizing radiation, chemicalschemicalsInfections – EBV Infections – EBV ChemotherapyChemotherapy
Precise cause – unknownPrecise cause – unknown

Signs of Childhood CancerSigns of Childhood Cancer
CContinued, unexplained weight lossontinued, unexplained weight lossHHeadaches, often with early morning vomitingeadaches, often with early morning vomitingIIncreased swelling or persistent pain in bones, joints, back, or ncreased swelling or persistent pain in bones, joints, back, or legslegsLLump or mass, esp. in the abdomen, neck, chest, pelvis, or ump or mass, esp. in the abdomen, neck, chest, pelvis, or
armpitsarmpitsDDevelopment of excessive bruising, bleeding, or rashevelopment of excessive bruising, bleeding, or rash
CConstant/recurrent infectionsonstant/recurrent infectionsAA whitish color behind the pupil whitish color behind the pupilNNausea which persists or vomiting with or w/o seizureausea which persists or vomiting with or w/o seizure
CConstant tiredness or noticeable palenessonstant tiredness or noticeable palenessEEye or vision changes which occur suddenly and persistsye or vision changes which occur suddenly and persistsRRecurrent or persistent fevers of unknown originecurrent or persistent fevers of unknown origin

WHY DIFFICULT TO WHY DIFFICULT TO DIAGNOSE CHILDHOOD DIAGNOSE CHILDHOOD CANCER?CANCER?
Vague manifestationsVague manifestations
Childhood malignancies are rareChildhood malignancies are rare
Doctor’s reluctance to consider Doctor’s reluctance to consider cancer diagnosiscancer diagnosis

Important Factors to Important Factors to CureCure
EARLY DETECTIONEARLY DETECTION
PROPER TREATMENTPROPER TREATMENT
GOOD SUPPORTIVE CAREGOOD SUPPORTIVE CARE

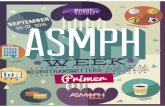
RETINOBLASTOMARETINOBLASTOMA

RETINOBLASTOMARETINOBLASTOMA
Most common intraocular malignancy of Most common intraocular malignancy of childhood childhood
2nd most freq solid malignancy2nd most freq solid malignancy 80% are diagnosed before 3-4 years old80% are diagnosed before 3-4 years old Median age at diagnosis: 2 years oldMedian age at diagnosis: 2 years old Beyond 6 years old is rare!!!Beyond 6 years old is rare!!! Incidence:Incidence:
1. 60% --non-heriditary & unilateral1. 60% --non-heriditary & unilateral2. 25% --hereditary & bilateral2. 25% --hereditary & bilateral3. 15% --hereditary & unilateral3. 15% --hereditary & unilateral

CLASSIFICATIONCLASSIFICATION
1.Laterality ---unilateral or bilateral1.Laterality ---unilateral or bilateral
2.Focality ---Unifocal or multifocal2.Focality ---Unifocal or multifocal
3.Genetics --- hereditary or3.Genetics --- hereditary or nonheriditarynonheriditary

LATERALITYLATERALITY
UNILATERALUNILATERAL
-Knudson’s two hit -Knudson’s two hit phenomenonphenomenon
-15% carry -15% carry constitutional constitutional mutationmutation
BILATERALBILATERAL
-asstd. with -asstd. with advanced parental advanced parental ageage
-present earlier than -present earlier than unilateralunilateral
-hereditary form-hereditary form
-worse prognosis-worse prognosis
-autosomal dominant-autosomal dominant

RetinoblastomaRetinoblastoma
RB gene on Chromosome 13, “two-hit theory”RB gene on Chromosome 13, “two-hit theory”
Round blue cell tumor arising in any of the Round blue cell tumor arising in any of the nucleated layers of the retinanucleated layers of the retina
Hematogenous, lymphatic spread, direct Hematogenous, lymphatic spread, direct extension thru the optic nerveextension thru the optic nerve
Only 10% detected by Only 10% detected by ophthalmologic ophthalmologic screeningscreening

COMMON SIGNS & COMMON SIGNS & SYMPTOMSSYMPTOMS1.1. Leukokoria --most commonLeukokoria --most common2.2. Strabismus --2Strabismus --2ndnd most common most common3.3. Decreased visual acuityDecreased visual acuity4.4. Inflammatory changesInflammatory changes5.5. GlaucomaGlaucoma6.6. Vitreous hemorrhage resulting in black Vitreous hemorrhage resulting in black
pupilpupil7.7. Rubeosis iridis –(neovascularization of Rubeosis iridis –(neovascularization of
surface surface of iris) of iris) *in 50% with advanced dsespontaneous *in 50% with advanced dsespontaneous
bleed---hyphemableed---hyphema


Investigations for Diagnosis of Retinoblastoma
1.Examinations-done under anesthesia by pedia ophtha-done by pedia oncologist-Audiology evaluation if chemo with carbplatin
2. Imaging studies-CT scan of brain and orbits
3. Laboratory evaluations-CBC,Bld chem,electrolytes-Creatinine clearance if chemo with carboplatin

Investigations for Diagnosis of Retinoblastoma
4. Diagnostic Studies4. Diagnostic Studies
-Lumbar puncture ---only if with radiographic or -Lumbar puncture ---only if with radiographic or clinical suspicion of CNS diseaseclinical suspicion of CNS disease
-Bone scan --- only if with bone pain or other extra--Bone scan --- only if with bone pain or other extra-
ocular diseaseocular disease
-Bone marrow biopsy –only with abnormal -Bone marrow biopsy –only with abnormal CBC(without alternative explanation) or other CBC(without alternative explanation) or other extraocular diseaseextraocular disease
5.Pathologic evaluation---if enucleation is 5.Pathologic evaluation---if enucleation is performedperformed

HistologyHistology: The only human tumor : The only human tumor that is radically treated without that is radically treated without tissue biopsy confirmationtissue biopsy confirmation
Flexner-Wintersteiner rosettes: lined by tall cuboidal cells that circumbscribe and an apical lumen

Patterns of SpreadPatterns of SpreadIntraocular:Intraocular:
1. With endophytic growth, there is a white 1. With endophytic growth, there is a white hazy mass.hazy mass.
2. With exophytic growth, there is retinal 2. With exophytic growth, there is retinal detachment.detachment.
3. Most tumors have combined growth.3. Most tumors have combined growth.
4. Retinal cells frequently break off from the 4. Retinal cells frequently break off from the main mass and seed the vitreous or new main mass and seed the vitreous or new locations on the retina.locations on the retina.

Extraocular:Extraocular:
1.1. Retinoblastoma spreads first to surrounding Retinoblastoma spreads first to surrounding structures and then by hematogenous or structures and then by hematogenous or lymphatic extension.lymphatic extension.
2.2. Retinoblastoma invades the optic nerve. From Retinoblastoma invades the optic nerve. From there it can spread directly along the axons to the there it can spread directly along the axons to the brain or may cross into the subarachnoid space brain or may cross into the subarachnoid space and spread via the CSF to the brain.and spread via the CSF to the brain.
3.3. Hematogenous spread leads to metastatic disease, Hematogenous spread leads to metastatic disease, most commonly to brain, bone marrow, or bone.most commonly to brain, bone marrow, or bone.
4.4. Lymphatic spread is rare because there is minimal Lymphatic spread is rare because there is minimal lymphatic drainage of the orbit. Occasionally, lymphatic drainage of the orbit. Occasionally, retinoblastoma spreads lymphatically to the retinoblastoma spreads lymphatically to the preauricular and submandibular nodes.preauricular and submandibular nodes.

PARTS OF THE EYEPARTS OF THE EYE


retinoblastomaretinoblastoma


SITES OF METASTASISSITES OF METASTASIS
1.1. BRAINBRAIN
2.2. BONEBONE
3.3. BONE MARROWBONE MARROW
4.4. LUNGSLUNGS

RISKS FOR METASTATIC RISKS FOR METASTATIC SPREADSPREAD
11. If optic nerve stump is <5mm—bad . If optic nerve stump is <5mm—bad
>5mm---better>5mm---better
2. Tumor invasion into the anterior chamber2. Tumor invasion into the anterior chamber
3. Large tumor with vitreous seeding3. Large tumor with vitreous seeding
4. Rubeosis iridis4. Rubeosis iridis
5. Glaucoma5. Glaucoma

RetinoblastomaRetinoblastoma
GOAL OF TREATMENT:GOAL OF TREATMENT:
Primary Goal: Cure!!!!Primary Goal: Cure!!!!
Secondary Goal: Preservation of visionSecondary Goal: Preservation of vision

TREATMENTTREATMENT
I.I. SurgerySurgeryEnucleation—if no hope for salvage of useful Enucleation—if no hope for salvage of useful visionvision
II. II. RadiotherapyRadiotherapy
III. III. ChemotherapyChemotherapy

NeuroblastomaNeuroblastoma
Most common Most common extracranial solid tumor extracranial solid tumor in infancyin infancy
8-10% of all childhood 8-10% of all childhood malignanciesmalignancies
Affects infants & Affects infants & preschool preschool – 50% younger than 2 50% younger than 2
year oldyear old– 30% younger than 1 30% younger than 1
year oldyear old

NEONATAL NEUROBLASTOMANEONATAL NEUROBLASTOMA
Subcutaneous nodulesSubcutaneous nodules. If massaged, a zone of pallor . If massaged, a zone of pallor develops around the nodule due to catecholamine dischargedevelops around the nodule due to catecholamine discharge
Extensive metastasis to the liverExtensive metastasis to the liver Bone marrow involvementBone marrow involvement Massive adrenal hemorrhage into tumorMassive adrenal hemorrhage into tumor Hydrops fetalis and/or signs of erythroblastosis fetalisHydrops fetalis and/or signs of erythroblastosis fetalis Stage 4S Stage 4S
Diagnosis:Diagnosis: prenatal ULTZ prenatal ULTZ In many cases, a mass is not palpableIn many cases, a mass is not palpable Only 50% have elevated urinary catecholaminesOnly 50% have elevated urinary catecholamines Prognosis:Prognosis: favorable course (if with + favorable factors) favorable course (if with + favorable factors) Treatment:Treatment: Curative by surgery Curative by surgery Course:Course: Others regress Others regress

NEUROBLASTOMANEUROBLASTOMA
Originates from primordial neural crest cells Originates from primordial neural crest cells that normally give rise to adrenal & that normally give rise to adrenal & sympathetic gangliasympathetic ganglia
Are tumors of the sympathetic nerve tissueAre tumors of the sympathetic nerve tissue
Can occur anywhere along the sympathetic Can occur anywhere along the sympathetic neural pathwayneural pathway

Neuroblastoma – Clinical Neuroblastoma – Clinical FeaturesFeatures
Arise from the sympathetic outflowArise from the sympathetic outflow Primary sitesPrimary sites
– 70% 70% abdominalabdominal primary primary(50% adrenal medulla, 50% extra-adrenal tissue)(50% adrenal medulla, 50% extra-adrenal tissue)
– Thoracic tumours, Thoracic tumours, posterior mediastinumposterior mediastinum (20%) (20%)– Head & neck tumours (10%)Head & neck tumours (10%)– Epidural (dumbbell or hourglass shaped) tumors – Epidural (dumbbell or hourglass shaped) tumors –
cord compression/paraplegiacord compression/paraplegia– BoneBone– Lymph nodes are enlargedLymph nodes are enlarged– Lungs—rarely involved(0.7%), involvement should be Lungs—rarely involved(0.7%), involvement should be
proven by bxproven by bx– Pelvis---constipation,urinary retention,presacral Pelvis---constipation,urinary retention,presacral

MANIFESTIONSMANIFESTIONS
1.1. Excessive catecholamine Excessive catecholamine (VMA/HVA)(VMA/HVA)
intermittent attacks of sweating,pallorintermittent attacks of sweating,pallor Headaches,palpitationHeadaches,palpitation Hypertension—renin induced due to Hypertension—renin induced due to
renovascular compromise & seen in 1-5%renovascular compromise & seen in 1-5%

MANIFESTATIONSMANIFESTATIONS
2. 2. Signs & symptoms of Vasoactive Signs & symptoms of Vasoactive Intestinal Peptide (VIP)Intestinal Peptide (VIP)
Intractable watery diarrhea resulting to Intractable watery diarrhea resulting to failure to thrivefailure to thrive
Abdominal distentionAbdominal distention hypokalemiahypokalemia

MANIFESTATIONSMANIFESTATIONS
3. Acute myoclonic encephalopathy3. Acute myoclonic encephalopathy Bursts of rapid involuntary random eye movements in Bursts of rapid involuntary random eye movements in
all directions of gaze (OPSOCLONUS)all directions of gaze (OPSOCLONUS) Motor incoordination due to frequent,irregular jerking Motor incoordination due to frequent,irregular jerking
of muscles of the limbs and trunk (MYOCLONIC of muscles of the limbs and trunk (MYOCLONIC JERKING)JERKING)
Note:Note:
1.May or may not resolve after the tumor is removed or 1.May or may not resolve after the tumor is removed or symptoms may resolve only after several months. symptoms may resolve only after several months. Some , Some , it may be permanentit may be permanent
2. 2. Prognosis is goodPrognosis is good

PATHOPHYSIOLOGY OF OMPATHOPHYSIOLOGY OF OM
NOT DUE due to direct involvement of the CNS by NOT DUE due to direct involvement of the CNS by tumor or due to the production of catecholaminestumor or due to the production of catecholamines
It is associated by well-defined IgG & IgM It is associated by well-defined IgG & IgM autoantibodies that bind to the cytoplasm of cerebellar autoantibodies that bind to the cytoplasm of cerebellar Purkinje cells & to some axons in the white matterPurkinje cells & to some axons in the white matter
Diffuse & extensive lymphocytic infiltration with Diffuse & extensive lymphocytic infiltration with lymphoid follicles is a characteristic histologic feature lymphoid follicles is a characteristic histologic feature of OMof OM
This suggests an This suggests an IMMUNE-MEDIATED MECHANISM OF IMMUNE-MEDIATED MECHANISM OF THISTHIS RARE SYNDROMERARE SYNDROME

Recommended Criteria at INSS Conference for a Diagnosisof Neuroblastoma
Established if: (1) Unequivocal pathologic diagnosisa is made from tumor
tissue by light microscopy(with or without immunohistology, electron microscopy), and/or increased urine or
serum catecholamines or metabolites.b
OR (2) Bone marrow aspirate or trephine biopsy contains
unequivocal tumor cellsa (e.g.,syncytia or immunocytologically positive clumps of cells) and increased urine or
serum catecholamines or metabolites
Source: Manual of Pediatric Hematology & Oncology (4th ed) p534

Recommended Studies for Assessment of Extent of Disease
Tumor site Recommended testsPrimary site CT and/or MRI scana with 3-D measurements; MIBG scan.bMetastatic sites
Bone marrow Bilateral posterior iliac crest marrow aspirates and trephine core bone marrow biopsies
required to exclude marrow involvement. A single positive site documents marrow involvement. Core biopsies must contain at least 1 cm of marrow (excluding cartilage) to be considered adequate.
Bone MIBG scan; 99Tc scan required if MIBG scan negative or unavailable. Plain radiographs of positive lesions.
Lymph nodes Clinical examination (palpable nodes confirmedhistologically.
CT scan for nonpalpable nodes (3-D measurements).
Abdomen/liver CT and/or MRI scana with 3-D measurements.
Chest AP and lateral chest radiographs. CT/MRI necessary if chest
radiograph positive, or if abdominal mass/nodes extend into chest

NB – NB – ClinicalClinical features features MetastasesMetastases
– Bone marrow- Bone marrow- anaemiaanaemia
– Bone (Pain)Bone (Pain)
– Orbit (Peri-orbitalOrbit (Peri-orbital
– Skin (blue-berry Skin (blue-berry muffin)muffin)

NB – TherapyNB – Therapy
SurgerySurgery –laminectomy to –laminectomy to decompressiondecompression
ChemotherapyChemotherapy-responsive in -responsive in 80-85%;advantageous in 80-85%;advantageous in making surgery safer by making surgery safer by reduction of tumor sizereduction of tumor size
TransplantTransplant (Stage 4, Nmyc (Stage 4, Nmyc amplification amplification – HD Chemo with Autologous HD Chemo with Autologous
Bone Marrow TransplantBone Marrow Transplant

Evaluation of a Lymph NodeEvaluation of a Lymph Node
A diagnosis of lymphoma or any malignancy must A diagnosis of lymphoma or any malignancy must always be considered when evaluating a child always be considered when evaluating a child with an enlarged peripheral lymph nodewith an enlarged peripheral lymph node
It must be emphasized that not all palpable It must be emphasized that not all palpable nodes are pathologically enlarged and that most nodes are pathologically enlarged and that most pathologically enlarged nodes are benign.pathologically enlarged nodes are benign.
Points to consider in evaluating a lymph node:Points to consider in evaluating a lymph node:
I. LOCATION OF THE NODEI. LOCATION OF THE NODE a. Nodes of the axilla, neck and groin are often a. Nodes of the axilla, neck and groin are often
palpable palpable in normal children in normal children
b. Palpable supraclavicular nodes -- always b. Palpable supraclavicular nodes -- always considered considered abnormal abnormal
* if with left-sided (Virchow’s) – metastases * if with left-sided (Virchow’s) – metastases from from intra-abdominal CA intra-abdominal CA
* if with right-sided nodes --- intrathoracic * if with right-sided nodes --- intrathoracic diseasedisease

IIII When size mattersWhen size matters
a.Cervical and axillary nodes --- > 1 cma.Cervical and axillary nodes --- > 1 cm
b. Inguinal node ------ >1.5 cmb. Inguinal node ------ >1.5 cm
c. Epitrochlear node ----> 0.5 cmc. Epitrochlear node ----> 0.5 cm

IV.INDICATIONSIV.INDICATIONS
III. GENERALIZED OR LOCALIZED?III. GENERALIZED OR LOCALIZED?
a. Generalized --- involvement of more than two a. Generalized --- involvement of more than two (2) (2) noncontiguous noncontiguous areas areas
caused by many different caused by many different disease disease process process
b. Localized ---- enlarged lymph nodes within b. Localized ---- enlarged lymph nodes within contiguous anatomic regions and contiguous anatomic regions and usually due to one of two ( infection or usually due to one of two ( infection or malignancy) malignancy)
III. CHARACTERIII. CHARACTER
Malignant nodes ---- non-tender, firm, rubbery and Malignant nodes ---- non-tender, firm, rubbery and rapidly enlarging rapidly enlarging becoming becoming cnonfluent cnonfluent and located in the and located in the supraclavicular regionsupraclavicular region

INDICATIONS FOR LYMPH NODE BIOPSYINDICATIONS FOR LYMPH NODE BIOPSY
Chronic,persistent,progressive adenopathyChronic,persistent,progressive adenopathy If an infectious etiology has not been If an infectious etiology has not been
uncovered, a dominant node that persists for uncovered, a dominant node that persists for 6 weeks should be biopsied6 weeks should be biopsied
. . Node > 2.5 cm in diameter in the absence of Node > 2.5 cm in diameter in the absence of
signs of infection that warrant a trial of signs of infection that warrant a trial of antibioticantibiotic
Supraclavicular adenopathySupraclavicular adenopathy
Sytemic symptomsSytemic symptoms

Non-Hodgkin LymphomaNon-Hodgkin Lymphoma
– 5-7% malignant disease of childhood5-7% malignant disease of childhood– 3rd most common childhood malignancy3rd most common childhood malignancy– 60% of childhood lymphomas60% of childhood lymphomas– M>FM>F– Peak age:Peak age: 5-15 years old 5-15 years old– EtiologyEtiology: unknown: unknown– Risk factors:Risk factors:
Genetic-- SCID, WASGenetic-- SCID, WAS Posttransplantation immunosuppressionPosttransplantation immunosuppression Drugs ex. Drugs ex. PhenytoinPhenytoin (cause pseudolymphoma that (cause pseudolymphoma that
regress with cessation of treatment)regress with cessation of treatment) Radiation – treatment with radiotherapy (4-5% Radiation – treatment with radiotherapy (4-5%
develop NHL within 10 yearsdevelop NHL within 10 years Virus---EBV and HIVVirus---EBV and HIV

APPROACH TO THE DIAGNOSIS OF NON APPROACH TO THE DIAGNOSIS OF NON HODGKIN’S LYMPHOMAHODGKIN’S LYMPHOMA
I.I. History and PEHistory and PE
childhood lymphoma more often extranodal rapid childhood lymphoma more often extranodal rapid tumor growthtumor growth
frequently involved site: Intra-abdominal ( B-cell)frequently involved site: Intra-abdominal ( B-cell) Intrathoracic (precursor Intrathoracic (precursor
T-cell) T-cell)Sites:Sites:
Abdomen --- Abdomen --- primary site (35%)primary site (35%)
Head and neck ---- 13%Head and neck ---- 13%Mediastinum ---- 26%Mediastinum ---- 26% CNS and BM --- CNS involvement and epidural CNS and BM --- CNS involvement and epidural
tumor tumor uncommon at uncommon at presentation but more presentation but more common in common in the presence of BM the presence of BM involvement.involvement.
--- 2/3 with BM disease have --- 2/3 with BM disease have simultaneous simultaneous CNS involvement CNS involvement
--- Intracranial tumor more likely --- Intracranial tumor more likely epidural epidural although it can occur although it can occur within brain within brain parencyma parencyma

B SYMPTOMS OF HODGKIN B SYMPTOMS OF HODGKIN LYMPHOMALYMPHOMA
1. Unexplained 1. Unexplained feverfever with temp above with temp above 38.038.0ْْ C orallyC orally
2. Drenching night 2. Drenching night sweatssweats
3. Unexplained 3. Unexplained weight lossweight loss of 10% of 10% within 6 months preceding diagnosiswithin 6 months preceding diagnosis
Source: Principles & Practice of Pediatric Oncology 5Source: Principles & Practice of Pediatric Oncology 5thth ed p.701 ed p.701

IMPORTANT INVESTIGATIONSIMPORTANT INVESTIGATIONS FOR NHLFOR NHL
Histologic analysis- Primary mode of Histologic analysis- Primary mode of definitive diagnosisdefinitive diagnosis
CBC and APCCBC and APC Chemistries and Serum electrolytesChemistries and Serum electrolytes
– Liver and renal function testsLiver and renal function tests– SLDH- measures tumor volumeSLDH- measures tumor volume– Uric acid Uric acid
Imaging studiesImaging studies– Chest X-rayChest X-ray– Chest CTChest CT– Abdominal CT/ UltrasoundAbdominal CT/ Ultrasound
BMA with biopsy ( bilateral)BMA with biopsy ( bilateral) CSF examination -- essentialCSF examination -- essential

ST. JUDE CHILDREN’S STAGING ST. JUDE CHILDREN’S STAGING SYSTEMSYSTEM
STAGE ISTAGE I A single tumor (extranodal) or single anatomic area (nodal) with the A single tumor (extranodal) or single anatomic area (nodal) with the
exclusion of mediastinum or abdomenexclusion of mediastinum or abdomen
STAGE IISTAGE II
A single tumorA single tumor (extranodal) with regional node involvement (extranodal) with regional node involvement Two or more nodal areas Two or more nodal areas on the same side of the diaphragmon the same side of the diaphragm Two single (extranodal) tumors with or without regional node involvement Two single (extranodal) tumors with or without regional node involvement
on the same side of the diaghragmon the same side of the diaghragm A primary gastrointestinal tract tumorA primary gastrointestinal tract tumor, usually in the ileocecalarea, with or , usually in the ileocecalarea, with or
without involvement of associated mesenteric nodes onlywithout involvement of associated mesenteric nodes only
STAGESTAGE III III
Two single tumorsTwo single tumors (extranodal) on (extranodal) on opposite sidesopposite sides of the diaphragm of the diaphragm Two or more nodal areas Two or more nodal areas above and below the diaphragmabove and below the diaphragm All the primary intrathoracic tumors (mediastinal, pleural and thymic)All the primary intrathoracic tumors (mediastinal, pleural and thymic) All extensive primary intraabdominal diseaseAll extensive primary intraabdominal disease All paraspinal or epidural tumors, regardless of other tumor site(s)All paraspinal or epidural tumors, regardless of other tumor site(s)
STAGE IVSTAGE IV Any of the above with initial CNS and/or bone marrow involvementAny of the above with initial CNS and/or bone marrow involvement

Lymphomas – Lymphomas – 33rdrd most common most common
Hodgkin LymphomaHodgkin Lymphoma Childhood form Childhood form << 14yo, 14yo,
young adult form 15-34yo, young adult form 15-34yo, older adult form 55-74yoolder adult form 55-74yo
EBV implicatedEBV implicated, <10 yrs, , <10 yrs, male, with preexisting male, with preexisting immunodeficiencyimmunodeficiency
Reed-Sternberg cellReed-Sternberg cell hallmark hallmark of diseaseof disease
PainlessPainless lymphadenopathy, lymphadenopathy, anterior mediastinal mass anterior mediastinal mass and and systemic symptomssystemic symptoms like like fever, night sweats and fever, night sweats and weight lossweight loss
Ann Arbor Staging SystemAnn Arbor Staging System Same + neck CT, ESR, serum Same + neck CT, ESR, serum
copper and ferritincopper and ferritin
Non- Hodgkin LymphomaNon- Hodgkin Lymphoma Classified as B or non-B Classified as B or non-B
types (previously classified types (previously classified as lymphoblastic, SNCCL, as lymphoblastic, SNCCL, LCL)LCL)
Intrathoracic, abdominal Intrathoracic, abdominal skin , bone, soft tissues, skin , bone, soft tissues, CNSCNS
St Jude Staging systemSt Jude Staging system
CBC, electrolytes, uric acid, CBC, electrolytes, uric acid, sldh, creatinine, sgpt,chest sldh, creatinine, sgpt,chest Xray or scan, abdominal Xray or scan, abdominal scan or MRI, bone scan, scan or MRI, bone scan, BMA or biopsy, CSF cytologyBMA or biopsy, CSF cytology

WILMS’ TUMORWILMS’ TUMOR
Most common primary malignant Most common primary malignant tumor of childhoodtumor of childhood
EPIDEMIOLOGY:EPIDEMIOLOGY:1975-1995 – 7.6 1975-1995 – 7.6 CasesCases per million per million
children children younger than 15 y/oyounger than 15 y/o
6% of childhood cancer6% of childhood cancerhigher for blacks, low in Asianshigher for blacks, low in AsiansF>MF>M

A CHILD WITH ANIRIDIAA CHILD WITH ANIRIDIA
Wilms’ tumor associated syndrome (WAGR)
1. Wilms’ tumor
1.Aniridia
2.Hemihypertrophy
3.Genitourinary abnormalities
4. Mental retardation

Wilm’s Tumor Wilm’s Tumor (Nephroblastoma)(Nephroblastoma) Clinical Features:Clinical Features:
1.Abdominal mass 1.Abdominal mass
-Synchronous (4.4-7%)-Synchronous (4.4-7%)
-Metachronous(1-1.9%)-Metachronous(1-1.9%)
2.Abdominal pain2.Abdominal pain
3. Hematuria (10%)3. Hematuria (10%)
4.Hypertension (254.Hypertension (25%)%)

PHYSICAL PHYSICAL EXAMINATIONEXAMINATION LocationLocation Size of the massSize of the mass
Note:Note:
WT WT is usually a large flank mass is usually a large flank mass that does not particularly move with that does not particularly move with respiration.respiration.

WORKUPWORKUP
CBCCBC Liver testsLiver tests Renal function tests (urinalysis,creatinine)Renal function tests (urinalysis,creatinine) Serum calcium (elev.in rhabdoid or cmn)Serum calcium (elev.in rhabdoid or cmn) Coagulation assaysCoagulation assays Imaging studies:Imaging studies:
CT (abdomen)CT (abdomen)Doppler ULTZ –to assess the IVCDoppler ULTZ –to assess the IVCCXR/ CT (chest)CXR/ CT (chest)Bone scan or skeletal surveyBone scan or skeletal surveyBrain imaging (MRI)Brain imaging (MRI)

STAGING (NWTS-5)STAGING (NWTS-5)
Stage IStage I ---confined to the kidney & ---confined to the kidney & completelyresected. completelyresected.
no renal capsule penetration no renal capsule penetration or involvement of renal sinus vesselor involvement of renal sinus vessel
Stage IIStage II --- tumor extends beyond the kidney but --- tumor extends beyond the kidney but completely resected (neg.margins & LN) completely resected (neg.margins & LN)
At least 1 of the ff:At least 1 of the ff:a. Penetration of the renal capsulea. Penetration of the renal capsuleb. Invasion of renal sinus vesselsb. Invasion of renal sinus vesselsc. biopsy of tumor prior to removalc. biopsy of tumor prior to removal

STAGING (STAGING (NWHTS-5NWHTS-5))
STAGE IIISTAGE III --- Gross or microscopic residual tumor --- Gross or microscopic residual tumor remains postop,including remains postop,including
inoperable tumor inoperable tumor
spillage of tumor preop or intraop spillage of tumor preop or intraop regional LN metastasis or regional LN metastasis or transected tumor thrombus transected tumor thrombus
STAGE IVSTAGE IV ---- Hematogenous or LN mets ---- Hematogenous or LN mets
outside the abdomenoutside the abdomen
(lung,liver,bone,brain)(lung,liver,bone,brain)
STAGE VSTAGE V ----- Bilateral Wilms’ tumor ----- Bilateral Wilms’ tumor

Predictive factorsPredictive factors (recurrence/progressio(recurrence/progressionn
1.size1.size2.age of patient2.age of patient3.histology 3.histology
a .blastemal– hi a .blastemal– hi stage/invasivestage/invasive
b. stromalb. stromalc. epithelial –low stage/ less c. epithelial –low stage/ less
invasive and invasive and resistant to resistant to chemotx chemotx

PROGNOSISPROGNOSIS
4. LN metastasis4. LN metastasis 5. local features of tumor – capsular or 5. local features of tumor – capsular or
vascular invasionvascular invasion
IMPORTANT: The histologic finding of ANAPLASIA is the most important determinant prognosis

BILATERAL WILMS’ BILATERAL WILMS’ TUMORTUMOR HistologyHistology: favorable: favorable Prognostic factorsPrognostic factors::
11. Age. Agediagnosis at early age (<2 y/o) –betterdiagnosis at early age (<2 y/o) –bettersurvival rate:survival rate:
<2 y/o ---70-75%<2 y/o ---70-75%>2 y/o --- 20-45%>2 y/o --- 20-45%
2.2. StageStage survival rate:survival rate:
Stage 1 & II ---85%Stage 1 & II ---85% Stage III & IV --- 0%Stage III & IV --- 0%

POSITIVE PROGNOSTIC POSITIVE PROGNOSTIC FACTORSFACTORS
1.1. Stage I an IIStage I an II
2. Neg. Para-oartic nodes2. Neg. Para-oartic nodes
3. Absence of anaplasia/sarcomatous 3. Absence of anaplasia/sarcomatous
4. Absence of tumor rupture4. Absence of tumor rupture
5. Time of relapse (later better than early)5. Time of relapse (later better than early)
(> 15 months from diagnosis)(> 15 months from diagnosis)
6. Site of metastases at relapse6. Site of metastases at relapse
(Lung better than liver(Lung better than liver))

NEPHROGENIC RESTS

TREATMENTTREATMENT
OBJECTIVE:OBJECTIVE:
1. Maximum preservation of 1. Maximum preservation of renal tissuerenal tissue
2. Tumor removal by partial 2. Tumor removal by partial nephrectomynephrectomy

TREATMENTTREATMENT1.1. Laparotomy and bx of both kidneys (stage Laparotomy and bx of both kidneys (stage
and histology)and histology)LN should be bx & each side is staged LN should be bx & each side is staged separately.separately.
Excision of the tumor(s) is performed at Excision of the tumor(s) is performed at the initial operation only if all of the the initial operation only if all of the tumor can be removed with tumor can be removed with preservation of sufficient renal preservation of sufficient renal parenchyma for normal renal function parenchyma for normal renal function on at least one sideon at least one side
2.2. ChemotherapyChemotherapyBabies < 12 mo.– half the doseBabies < 12 mo.– half the doseBabies > 12 mo.– full doseBabies > 12 mo.– full dose

CHEMOTHERAPYCHEMOTHERAPY
DOSE:DOSE:– A- Dactinomycin (45ug/kg,IV)A- Dactinomycin (45ug/kg,IV)– D* Doxorubicin (1.0mg/kg, IV)D* Doxorubicin (1.0mg/kg, IV)– D # Doxorubicin (1.5mg/kg,IV)D # Doxorubicin (1.5mg/kg,IV)– V – Vincristine(0.05mg/kg,IV)V – Vincristine(0.05mg/kg,IV)– V* Vincristine(0.67mg/kg,IV)V* Vincristine(0.67mg/kg,IV)– XRT – Radiation therapyXRT – Radiation therapy
** ** for StageIII and IV, FH or StageII-for StageIII and IV, FH or StageII-IV,UHIV,UH

TREATMENTTREATMENT Evaluation and Abdominal CTEvaluation and Abdominal CT – at week 5 – at week 5
at wk 6at wk 6 – if the imaging showed persistent – if the imaging showed persistent
but resectable tumor or tumor but resectable tumor or tumor responded completelyresponded completely
do second look surgery and biopsydo second look surgery and biopsy• at 2at 2ndnd look surgery look surgery ---complete ---complete
excision of the tumor frm.the least excision of the tumor frm.the least involved kidney shld. be carried out. involved kidney shld. be carried out.
• If the procedure leaves a viable & If the procedure leaves a viable & functioning kidney on 1 side & the functioning kidney on 1 side & the other kidney, if extensively involved other kidney, if extensively involved with tumor, should be removed.with tumor, should be removed.

TREATMENTTREATMENT
Postoperative chemo shld. be adapted Postoperative chemo shld. be adapted to renal function abnormalitiesto renal function abnormalities::
a.If 2a.If 2ndnd look surgery showed no gross or look surgery showed no gross or pathologic evidence of persistent tumor, pathologic evidence of persistent tumor, chemo be given accordinglychemo be given accordingly
b. If 2b. If 2ndnd look surgery showed gross or look surgery showed gross or pathologic evidence of persistence that pathologic evidence of persistence that can’t be resected, do radiotx and change can’t be resected, do radiotx and change chemochemo
(ICE)(ICE)

Abdominal TumorsAbdominal TumorsNeuroblastomaNeuroblastoma
Peripheral sympathetic Peripheral sympathetic nervous system malignancynervous system malignancy
<5 yrs old, median 2 years <5 yrs old, median 2 years old, male predominanceold, male predominance
Most common abdominal Most common abdominal malignancymalignancy
Shimada classification, MYC Shimada classification, MYC genegene
Retroperitoneal, palpable Retroperitoneal, palpable causing abdominal causing abdominal discomfort, opsomyoclonus, discomfort, opsomyoclonus, diarrheadiarrhea
(+) calcification and(+) calcification and hemorrhage on CThemorrhage on CT
Bone, marrow liver, nodes Bone, marrow liver, nodes skin metsskin mets
Wilms’ tumorWilms’ tumor – 2 – 2ndnd Nephroblastoma or mixed Nephroblastoma or mixed
embryonal neoplasm of the embryonal neoplasm of the kidney with three elements: kidney with three elements: blastema, epithelia and blastema, epithelia and stromastroma
2-5 years of age2-5 years of age WT1 gene (11p13) Denys-WT1 gene (11p13) Denys-
Drash syndrome, WT2 gene Drash syndrome, WT2 gene Beckwith-Wiedenman Beckwith-Wiedenman syndrome, GUT abnsyndrome, GUT abn
Smooth and firm, pain, Smooth and firm, pain, vomiting and hematuria, vomiting and hematuria, hypertensionhypertension
(-) calcification(-) calcification Pulmonary metastasis, nodesPulmonary metastasis, nodes

Abdominal TumorsAbdominal Tumors
NeuroblastomaNeuroblastoma CT or MRI, BMA, bone CT or MRI, BMA, bone
scan, urine VMA and scan, urine VMA and HVA (95% +)HVA (95% +)
Prognostic factors:Prognostic factors: age age at diagnosis, stage, at diagnosis, stage, MYCN MYCN status, Shimada status, Shimada histology and ploidy in histology and ploidy in infantsinfants
Stage IV-S:Stage IV-S: <1year old, <1year old, with dissemination to with dissemination to the skin, liver, bone the skin, liver, bone marrow without bone marrow without bone involvement plus a involvement plus a primary tumorprimary tumor
Wilms’ tumorWilms’ tumor – 2 – 2ndnd
CT or MRI and chest CT or MRI and chest XRayXRay
Prognosis Prognosis affected by affected by stage and type of stage and type of histology, histology, unfavoprable in the unfavoprable in the presence of large presence of large nuclei, nuclei, hyperchromatism, hyperchromatism, multiple mitotic multiple mitotic figuresfigures
Stage VStage V – bilateral – bilateral tumorstumors

HEPATOBLASTOMAHEPATOBLASTOMA

Liver TumoursLiver Tumours Hepatomegaly Hepatomegaly ± jaundice± jaundice Raised AFP Raised AFP (age-specific (age-specific
normogram)normogram) 2 types:2 types:
– HepatoblastomaHepatoblastoma most commonmost common infants & young childreninfants & young children
– Hepatocellular Hepatocellular carcinomacarcinoma Rare, olderRare, older HBV, HCVHBV, HCV

RhabdomyosarcomaRhabdomyosarcoma
Most common soft tissue sarcomaMost common soft tissue sarcoma Found in any anatomic site: head/neck (40%), GUT Found in any anatomic site: head/neck (40%), GUT
(20%), trunk (10%)(20%), trunk (10%) Associated with Li Fraumeni syndrome and Associated with Li Fraumeni syndrome and
NeurofibromatosisNeurofibromatosis Arise from the same embryonic mesenchyme as Arise from the same embryonic mesenchyme as
striated musclestriated muscle
Types: embryonal (60%) intermediate prognosisTypes: embryonal (60%) intermediate prognosis
boytryoid, alveolar, pleomorphic, boytryoid, alveolar, pleomorphic, undifferentiated undifferentiated

ClinicalClinical
Non-tender mass with no unusual hue to the Non-tender mass with no unusual hue to the overlying skin or subcutaneous tissueoverlying skin or subcutaneous tissue
Growth of a nontender mass esp. without a Growth of a nontender mass esp. without a clearcut history of trauma, should always alert clearcut history of trauma, should always alert the MD to consider biopsy, esp. if expansion is the MD to consider biopsy, esp. if expansion is confirmed by repeated observations over 1-2 confirmed by repeated observations over 1-2 weeksweeks
Mass within a body cavity producing Mass within a body cavity producing obstruction or discharge,mandates a biopsyobstruction or discharge,mandates a biopsy

RhabdomyosarcomaRhabdomyosarcoma
Diagnosis: disseminates earlyDiagnosis: disseminates early
CT/MRI, BMA, bone scans, lymph node biopsyCT/MRI, BMA, bone scans, lymph node biopsy
The most essential element of the work-up is The most essential element of the work-up is examination of the tumor tissue w/c include examination of the tumor tissue w/c include the use of special stains(desmin, muscle the use of special stains(desmin, muscle specific actin, MyoD).specific actin, MyoD).
Completely excised tumors have the best Completely excised tumors have the best prognosis. Favorable site: orbitprognosis. Favorable site: orbit
older children and disseminated diseases older children and disseminated diseases have poorer prognosishave poorer prognosis

RhabdomyosarcomaRhabdomyosarcoma SitesSites
– Head & neckHead & neck Orbit, nasopharyngeal & Orbit, nasopharyngeal &
middle ear tumoursmiddle ear tumours– Genitourinary tractGenitourinary tract
Bladder & prostate, Bladder & prostate, vaginal & uterinevaginal & uterine
– Extremity Extremity PrognosisPrognosis
– Orbit - excellentOrbit - excellent– GU tract - goodGU tract - good– Extremity, retroperitoneal, Extremity, retroperitoneal,
metastatic - poormetastatic - poor

Bone TumoursBone Tumours

Malignant Bone TumorsMalignant Bone Tumors
OsteosarcomaOsteosarcoma Most common primary Most common primary
malignant bone tumors in malignant bone tumors in childrenchildren
Second decade of life, growth Second decade of life, growth spurt, long bones, metaphysisspurt, long bones, metaphysis
Pleomorphic, spindle shaped Pleomorphic, spindle shaped cells with malignant osteoidcells with malignant osteoid
Bone pain and swellingBone pain and swelling ““Sunburst pattern” xraySunburst pattern” xray Primary site: FEMUR Primary site: FEMUR
(metaphyseal portion)(metaphyseal portion) Long bonesLong bones
Ewing’s SarcomaEwing’s Sarcoma More common in the first More common in the first
10 years of life10 years of life Small round Small round
undifferentiated tumors of undifferentiated tumors of neural crest origin, flat neural crest origin, flat bones, diaphysisbones, diaphysis
Askin tumorAskin tumor –if tumors –if tumors arise in the chest wallarise in the chest wall
S100 and NSE (+)S100 and NSE (+) Pain and swelling, (+) Pain and swelling, (+)
fever and weight lossfever and weight loss ““onion-skinning”onion-skinning” patternpattern
xray xray (flat & diaphyses)(flat & diaphyses) Primary: pelvic,LE,bones of Primary: pelvic,LE,bones of
chest wall chest wall

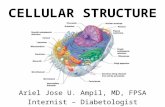
Radiological differenceRadiological difference
Sunburst of Osteosarcoma
Onion skin of Ewings sarcoma

Malignant Bone tumorsMalignant Bone tumors Diagnosis:Diagnosis: MRI or CT of tumor MRI or CT of tumor
SLDHSLDH
bone scanbone scan
Alkaline phosphataseAlkaline phosphatase
chest ct scanchest ct scan
bone biopsy/BMA in Ewing’s Sarcomabone biopsy/BMA in Ewing’s Sarcoma
Both with 75% cure rate if non-metastatic on Both with 75% cure rate if non-metastatic on presentation.presentation.
Treatment:Treatment: Multi-agent chemotherapy and surgery. Multi-agent chemotherapy and surgery.
Radiotherapy also needed in Ewing’s Radiotherapy also needed in Ewing’s SarcomaSarcoma

Brain TumoursBrain Tumours Special problemsSpecial problems
– Blood-brain barrier limits Blood-brain barrier limits chemotherapychemotherapy
– Developing brain is vulnerable to Developing brain is vulnerable to toxicity of therapytoxicity of therapy
– Proximity of tumours to vital structures Proximity of tumours to vital structures precludes extensive surgeryprecludes extensive surgery
– Tendency to spread within neuraxisTendency to spread within neuraxis

Brain Tumours - Brain Tumours - ClassificationClassification
Location2/3 above & 1/3 below tentorium

Site and symptomsSite and symptoms Posterior fossaPosterior fossa – limited space, disrupt – limited space, disrupt
CSF flowCSF flow– Vomiting, Increased ICPVomiting, Increased ICP– Motor tract involvement – cranial n, long Motor tract involvement – cranial n, long
tractstracts SupratentorialSupratentorial
– Seizures – focal seizuresSeizures – focal seizures– Deterioration in school performanceDeterioration in school performance– Hormonal defects – central precocity, Hormonal defects – central precocity,
diabetes insipidus diabetes insipidus

(L) parieto-occipital low grade astrocytoma

Brain Tumours - Brain Tumours - TherapyTherapy SurgerySurgery
– ResectabilityResectability RadiotherapyRadiotherapy
– ToxicityToxicity IQ dropIQ drop EndocrinopathyEndocrinopathy Growth failureGrowth failure
ChemotherapyChemotherapy– Prolong survivalProlong survival– Increase cure ratesIncrease cure rates
Prognosis depends on
Resectability
Age
Metastases
Chemosensitivity
Prognosis depends on:
•Resectability
•Age
•Metastases
•Chemosensitivity

Oncologic emergenciesOncologic emergencies
Tumour lysis syndromeTumour lysis syndrome

Tumour lysis syndromeTumour lysis syndrome Metabolic derangement resulting from rapid death of Metabolic derangement resulting from rapid death of
malignant cellsmalignant cells
Must have 2 important factors :Must have 2 important factors :– high tumour burden, high tumour burden, – highly sensitive tumour – ALL, AML, NHLhighly sensitive tumour – ALL, AML, NHL
Hyperkalaemia - hydration, no K supplements, K Hyperkalaemia - hydration, no K supplements, K bindersbinders
Hyperuricaemia – hydration, alkalinisation, Hyperuricaemia – hydration, alkalinisation, allopurinol, allopurinol, uricozyme to convert to uricozyme to convert to allantoinallantoin
Hyperphosphataemia – Phosphate bindersHyperphosphataemia – Phosphate binders
Hypocalcaemia – if symptomatic, partial correctionHypocalcaemia – if symptomatic, partial correction

Thank You!!!Thank You!!!