
Business Affairs & Consumer Protection - City of Chicago · 04 Itemized receipt or invoice required...
23
Business Affairs & Consumer Protection Department of C I T Y O F C H I C A G O Fiscal TA Workshop - 2014 Delegate Agencies Vouchering Corporate Maria Lapacek, Commissioner January 29, 2014
Transcript of Business Affairs & Consumer Protection - City of Chicago · 04 Itemized receipt or invoice required...

Business Affairs & Consumer Protection
Department of
C I T Y O F C H I C A G O
Fiscal TA Workshop - 2014 Delegate Agencies Vouchering
Corporate
Maria Lapacek, Commissioner
January 29, 2014

2
• Opening Remarks – Jeffrey Lewelling
• Voucher and Fiscal Payment - Kenneth Jones
• Q & A
AGENDA

3
1. Finance & Program Teams
• For all finance and contract questions, call 312.744.6060
• Make sure to state your question regards “Delegate Agency finance and contracts” to ensure your call is directed appropriately.

4
2. Voucher and Fiscal Payment
• 2014 Vouchering Matters – Team
What is New – Operational Changes
Voucher Template & Instructions
Sample Voucher
Voucher Submission
Budget Revisions
Deletions Matters & Quick Tips

5
3. What is New – Operational Changes
• Maintain Appropriate Supporting Documentation
• Complete and Submit Budget (Voucher) Detail
• Personnel Transaction Support Payroll Register Cancelled Checks or Bank Statements Time and Attendance Sheets
• Non-Personnel Transaction Support Invoice Cancelled Checks Or Bank Statements

6
3b. What is New – Operational Changes (Cont.)
• Standard Voucher & Budget Detail Forms
• Must Track Monthly Expenditures Against Your
Budget
7
Standard Voucher Template &
Instructions
4. VOUCHER & BUDGET DETAIL FORMS OVERVIEW
Review of Budget Detail Form

8
SAMPLE CORPORATE
5. SAMPLE VOUCHER FORMS OVERVIEW

9
Voucher for Allowable Reimbursement
Expenditures are Submitted to:
6. VOUCHER SUBMISSIONS
Department of Business Affairs and Consumer Protection
Finance Division
City Hall Room 805
121 North LaSalle
Chicago, Illinois 60602
Only for BACP Programs:
NBDC SA

10
7. VOUCHER DELETIONS
Common Reasons03 Fringe benefits recalculated based on the approved salary amount
05 Additional or supporting documentation required
08 Expenditures billed to incorrect budget line. Resubmit under correct budget line
10 Expenditures have exceeded budget line
17 Inventory Control Card required
19 ADP Payroll Register and Payroll Summary needed.
20 Backup for proof of payment required
22 Fringe benefit breakdown needed on Invoice Detail Form
25 Mathematical error

11
7. VOUCHER DELETIONS (Cont’d) Other Reasons
01 Past due amount and late fee are not reimbursable
02 Receipt and/or invoice does not match requested amount
04 Itemized receipt or invoice required for unit/item cost at $5,000 or more
06 Recalculation based on percentage in the contract
07 Requested amount was previously paid
09 Time sheet needed for hourly wages
11 Petty cash: original invoice or receipt required
12 More descriptive budget narrative needed. Budget revision required.
13 Credit Card Statement, Bank Statement, Invoice/Receipt needed for Credit Card purchase
14 Payment Statement, Bank Statement, and/or Invoice/Receipt needed for online payment
15 Tax Payment Certificate required
16 Budget line does not exist. Budget revision required.
18 Positions not budgeted. Budget revision required.
21 Exceeds the maximum allowed per pay period
23 Item and/or amount not budgeted in the contract
24 Ineligible costs per contact budget. Do not resubmit.
26 Cost not incurred during contract period
27 Recoup of previous overpayment
28 Other: a specific reason should be addressed
12
8. VOUCHER HOLDS
• Expired Insurance
• Invalid Bank Information
• Invalid Address Information
• Unauthorized Signature on Voucher Form
• Audit and Other Non-Compliance Issues
• No Submission of Agency Performance Report
13
9. BUDGET REVISIONS OVERVIEW
• Budget Revision Required if:
Necessary Amount Changes Between Budgeted
Line Items
Staff Change with Different Salary Which Increases
or Decreases Personnel Account Line
Reduction or Increase in Lines
Change of Line Description

14
Inform Program Management of Important Program Changes
10. BUDGET REVISION OVERVIEW
• Cover Letter – Maria Lapacek
• Attention: BACP Finance
• Budget Revision Forms (4)
• Reason or Justification
• Overall Program Impact
• Approval Notification
15
11. CONTRACT COMPLIANCE MONITORING
• Independent Audit
• Internal Audit (Rena Lira, Director of Internal Audit) o A-122 Audits o A-133 Reviews
• Management Decision Letters

16
• Accounting Policies and Procedures • Cash Management/Bank Reconciliations • Disbursements and Supporting Documentation Payroll Cost Allocation Employee vs. Independent Subcontractor Proper Procurement of Goods and Services
• Financial Statements and Reporting • Program Documentation and Record Retention
12. FISCAL COMPLIANCE REQUIREMENTS

17
13. 2014 SPECIAL CLOSEOUT MANDATES
• Budget Revision Deadline
October 15, 2014
• Voucher Submission Deadline
January 15, 2015

18
CV Number:
Release # BFY Fund Dept Orgn Appr Rptg
29000 1 14 0100 070 2005 0135
Vendor Name: ABC Company Invoice Number: 1
Program Name: NBDC Invoice Period Covered: 01/01/14 to 01/31/14
Original Submission X Date Submitted 02/15/14
Federal Employer ID Number: 36-98765432 Resubmission Date Submitted
Line Account Approved Amount Additions Amount Adjmt
Cost Category # Code Budget Requested (Deletions) Approved Code
Personnel 220005 $4,615.00 $384.60
Fringe Benefits 220044 $500.00 $29.44
Operating/Technical 220100 $3,600.00 $250.00
Professional/Third Party Srvcs 220140 $1,500.00 $200.00
Travel 220200 $200.00
Material & Supplies 220300 $2,200.00
Equipment 220400 $385.00
Other 220999
Totals $13,000.00 $864.04
Amount Released: Vendor Number: SC000000 Date:
Preparer: Phone: 773-123-4567
Additions: Bank:
Bank Address:
Less Deletions: Account Number:
Approved For Payment:
Advance Liquidated:
Invoice Amount:
Audited By: Authorized Signature:
Date: Type or Print Name:
Approved By: Title: Date: 2/1/2014
DPD USE ONLY Date Recd: By:
Date Received VATS:
For Comptroller's Office Use Only
Comments
For Comptroller's Office Use Only Agency Certification
2/1/2014
99000888
First National Bank
I certify, as an officer of the agency, that this reimbursement claim represents expenditures incurred and disbursed during the reporting period, that said expenditures are part of the approved budget contained in the contract and that payment has not previously been requested or received. I further certify that original documents are on file and available for audit or review upon request.
Jane Smith
$
CHECK ONE:
PO Number
Executive Director
$
$
$
$
Site Address: 121 Anywhere Ave.
Comptr. Use Only
1313 Mockingbird Lane
$
Phone: 773-123-4567
John Doe
CITY OF CHICAGODEPARTMENT OF BUSINESS AFFAIRS AND CONSUMER PROTECTION
Monthly Delegate Agency Invoice Form 1 Cover Page
Resubmitted invoices: use original voucher number plus "R" (e.g "5-R")
CORPORATE SAMPLE VOUCHER

19
FORM 2
(A) Vendor Name: ABC Company
(B) Date Submitted: 02/15/14 (D) Invoice Period: 1/1/14 to 1/31/14
(C) PO Number: 29000 (E) Voucher Number: 1
(F) Check/DD
Date
(G) Check Number/ID
Number (H) Employee/Payee Name(I) Account
Code (J) Job Title/Fringe Description(K) Gross Salary/
Amount(L) % To Project
(M) Charged to Program
Comptr Use Addition & (Deletion)
1/15/14 000123 John Doe 220005 Exec Director $1,000.00 50.0% $192.30
ADP direct deposit US Treasury 220044 Social Security $200.00 $11.93
ADP direct deposit US Treasury 220044 Medicare $100.00 $2.79
1/31/14 000126 John Doe 220005 Exec Director $1,000.00 50.0% $192.30
ADP direct deposit US Treasury 220044 Social Security $11.93
ADP direct deposit US Treasury 220044 Medicare $2.79
$384.60
$29.44
$414.04
CITY OF CHICAGODEPARTMENT OF BUSINESS AFFAIRS AND CONSUMER PROTECTION
PERSONNEL-FRINGE COSTS DETAIL
TOTAL Vouchered (Category 220005 + 220044)
NOTE: Attach payroll documents (checks, direct deposit) and other comments as needed. Contractor comments:
City Comptroller Comments:
TOTAL for Cost Category 220005 (Insert total here)
TOTAL for Cost Category 220044 (Insert total here)
Total Adjustments
Amount Approved
For Comptroller's Office Use Only

20
FORM 3
(A) Vendor Name: ABC Company
(B) Date Submitted: 02/15/14 (D) Invoice Period: 01/01/14 to 01/31/14
(C) PO Number: 29000 (E) Voucher Number: 1
(F) Check Date (G) Check Number ( H ) Payee
(I) Account Code ( J ) Cost Category ( K ) Amount of Check
( L ) % To Project ( M ) Charge to Program
Comptr Use Additions & (Deletions)
01/13/13 0000124 XYZ Company - Rent 220100 Operating/Technical $500.00 50.0% $250.00
01/25/13 0000125 Mike Smith - Consulting 220140Professional/Third Party Srvc $200.00 100.0% $200.00
$450.00
CITY OF CHICAGODEPARTMENT OF BUSINESS AFFAIRS AND CONSUMER PROTECTION
NON-PERSONNEL COSTS DETAIL
Sort expenditures by Account Code
( y Code and transfer to the appropriate Account Codes in Form
1)Comptrollers Use Only
Comments:Total Adjustments
Amount Approved

21
Period Covered by the Certificate: Invoice Number: Fund Number:
From: 01/01/14 To: 01/31/14 1 0100
Purchase Order Number: Release Number:
29000 1
Federal Employer I. D. Number:
Authorized Signature
Printed Name
Title
Date
THIS TAX PAYMENT CERTIFICATE MUST ACCOMPANY ANY CLAIMS FOR PAYROLL PAYMENTSMADE ON A DELEGATE AGENCY INVOICE. COMP- TPC-01 REVISED 11/10/08
Site Address: 121 Anywhere Avenue
02/01/14
Executive Director
John Doe
I certify that all deposits of withheld Federal income taxes and employer-employee Social Security Taxes and Medicare Taxes required to be made with the Federal Tax Depository and all required reports have been made in a timely manner.
For the period covered, there are no delinquent liabilities for employer's payroll taxes due to the Federal and/or Illinois state governments.
I further certify that I have on file completed copies of Forms W-4 and IL-4 for each person who is now or has been paid wages by my organization.
CITY OF CHICAGO
DEPARTMENT OF BUSINESS AFFAIRS AND CONSUMER PROTECTION
DELEGATE AGENCY TAX PAYMENT CERTIFICATE
36-98765432
Program Name: NBDC
Vendor Name: ABC Company
22
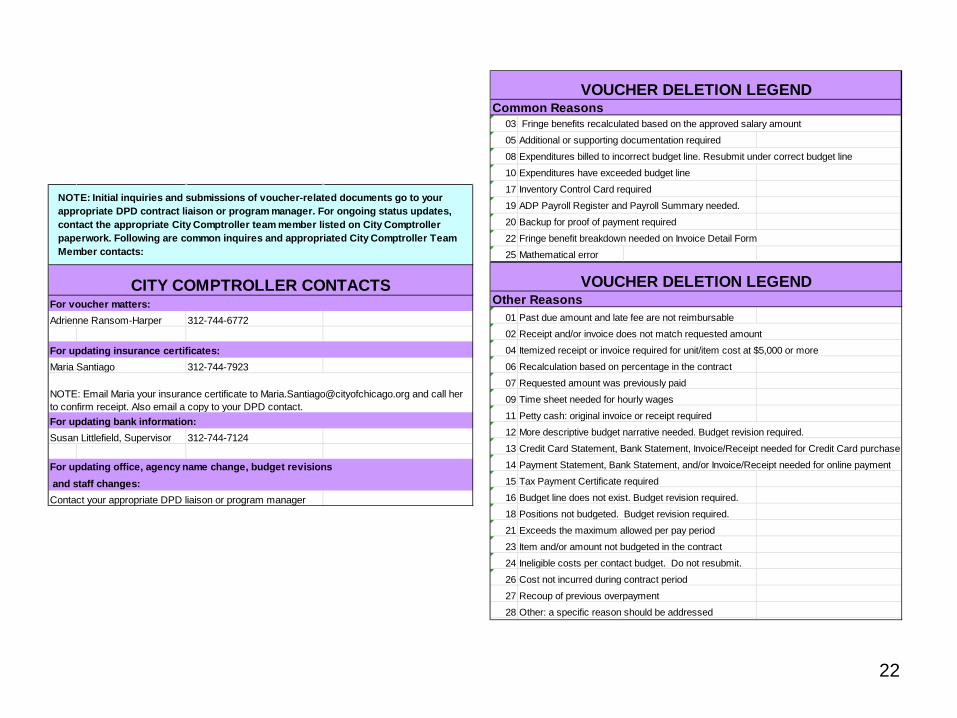
For voucher matters:Adrienne Ransom-Harper 312-744-6772
For updating insurance certificates:Maria Santiago 312-744-7923
For updating bank information:Susan Littlefield, Supervisor 312-744-7124
For updating office, agency name change, budget revisions and staff changes:Contact your appropriate DPD liaison or program manager
NOTE: Initial inquiries and submissions of voucher-related documents go to your appropriate DPD contract liaison or program manager. For ongoing status updates, contact the appropriate City Comptroller team member listed on City Comptroller paperwork. Following are common inquires and appropriated City Comptroller Team Member contacts:
CITY COMPTROLLER CONTACTS
NOTE: Email Maria your insurance certificate to [email protected] and call her to confirm receipt. Also email a copy to your DPD contact.
Common Reasons03 Fringe benefits recalculated based on the approved salary amount
05 Additional or supporting documentation required
08 Expenditures billed to incorrect budget line. Resubmit under correct budget line
10 Expenditures have exceeded budget line
17 Inventory Control Card required
19 ADP Payroll Register and Payroll Summary needed.
20 Backup for proof of payment required
22 Fringe benefit breakdown needed on Invoice Detail Form
25 Mathematical error
Other Reasons01 Past due amount and late fee are not reimbursable
02 Receipt and/or invoice does not match requested amount
04 Itemized receipt or invoice required for unit/item cost at $5,000 or more
06 Recalculation based on percentage in the contract
07 Requested amount was previously paid
09 Time sheet needed for hourly wages
11 Petty cash: original invoice or receipt required
12 More descriptive budget narrative needed. Budget revision required.
13 Credit Card Statement, Bank Statement, Invoice/Receipt needed for Credit Card purchase
14 Payment Statement, Bank Statement, and/or Invoice/Receipt needed for online payment
15 Tax Payment Certificate required
16 Budget line does not exist. Budget revision required.
18 Positions not budgeted. Budget revision required.
21 Exceeds the maximum allowed per pay period
23 Item and/or amount not budgeted in the contract
24 Ineligible costs per contact budget. Do not resubmit.
26 Cost not incurred during contract period
27 Recoup of previous overpayment
28 Other: a specific reason should be addressed
VOUCHER DELETION LEGEND
VOUCHER DELETION LEGEND

23
QUESTIONS & ANSWERS

















