Burnout in the senior medical workforce five years on
40
HEALTH DIALOGUE ISSUE 17 | APRIL 2021 “My employer is exhausting” Burnout in the senior medical workforce five years on
Transcript of Burnout in the senior medical workforce five years on

HEALTH DIALOGUEISSUE 17 | APRIL 2021
“My employer is exhausting”Burnout in the senior medical workforce five years on

Dr Charlotte Chambers, ASMS Director of Policy and Research
Queries about this research can be sent to [email protected]
WWW.ASMS.ORG.NZ HEALTH DIALOGUE i
ContentsForeword ii
Introduction 1
Definitions 2
Whyburnoutstillmatters 2
Methodology 4
Qualitativedataanalysis 5
Results 6
Demographicinformation 6
Burnout results 8
Burnoutanddemographicvariables 10
Genderandburnout2020 11
Dependants 13
Hoursofworkandburnout 15
Hoursofworkanddependants 17
Burnoutandplaceofwork 17
Specialtyandburnout 20
Qualitativedataanalysis 21
Qualitativeanalysisoftrends 24
Discussion 26
Timingofsurvey 26
Responderbias 26
Factorsassociatedwithburnout 27
Genderandburnout 27
Ageandburnout 28
Impactofdependants 28
Burnoutandmedicalspecialty 29
Conclusions 30
Whatneedstochange 31
Whatwearecallingfor 31
Appendix 1 32
References 32

ii HEALTH DIALOGUE APRIL2021
Foreword
Inourlatestsurvey,nearly50%ofrespondentsreportburnout.Thismeansinfiveyears,therehasbeennosubstantiveimprovementsinceourlastburnoutsurvey.
Thedoctorsanddentistswhosharedtheirexperiencesinthisresearchconveyedtheirpassionanddetermination,butalsospokeofthechallengingcircumstancesoftheirwork.
“The work is wonderful. I love caring for the patients but it is relentless and impossible to actually achieve within the current staffing climate.” – Radiation Oncologist
Thefactthatoneintwodoctorscontinuetosufferfromburnoutrepresentsaseriousfailurebythesystemtoaddresstherootcauseoftheproblem.Ourseniordoctorsanddentistscontinuetoshouldertheloadinourchronicallyunderstaffedandincreasinglybusyhospitals.Weknowtherearespecialiststaffingshortages(estimatedbyASMStobe24%),andwealsoknowthisrateofburnoutisunsustainable.Itseffectsarestartingtosnowballasacutedemandcontinuestooutstripworkforceresourceandsupply.
Burnoutisnotanindividualproblem;itisasystemfailure.Accordingly,wearecallingforformal
recognitionofemployers’responsibilitiestoprovidephysicallyandpsychologicallysafeworkplaces.Adequateresourcing,includingincreasedadministrativeandITsupport,mustalsoplayapart.
Wealsoneedacultureshiftinhospitalsandotherpublichealthcareemployers.Thenormalisationofexcessivelylongworkinghoursmuststop.
AstheGovernmentlaunchesitsresponsetotheHealthandDisabilitySystemReviewthereisnobettertimetotackletheburnoutproblem.
AsHealthMinisterAndrewLittleacknowledgedinhis24Marchspeechtosectorrepresentativesabouttheloomingchanges,thehealthworkforceisincreasinglystressed.
Ourmemberscanonlyworkwithgovernmenttoenactthesechangesiftheyhavethetime,space,andsupporttodoso.Thismeansinvestinginourpeoplefirst.
Wepresentthisburnoutstudywithspecificrecommendationsastowhatneedstochange.Wewelcomeconversationsabouthowthesechangescanbeimplemented.Ourhealthsystemandthoseworkingwithinitcannotwaitanylonger.Thetimeforactionisnow.
Sarah Dalton Executive Director Association of Salaried Medical Specialists
Burnout is now an entrenched feature of our specialist medical and dental workforce.
WWW.ASMS.ORG.NZ HEALTH DIALOGUE 1
IntroductionIn 2015 ASMS conducted the first nationwide survey of a senior medical workforce using the Copenhagen Burnout Inventory (CBI). The results were stark; one in two New Zealand medical and dental specialists were found to be suffering from high levels of fatigue and exhaustion. Many ascribed their symptoms to the conditions and experiences of their work. In August 2020, we repeated this study to see what, if anything, had changed in the intervening years. The 2020 survey findings are the focus of this report. This research extended observations made in the previous study regarding potential contributing factors to burnout, as well as improving aspects of the original methodology. This report focuses on differences in scores between the two surveys, and provides an updated commentary on the significance of burnout for the medical workforce. It concludes by presenting recommendations for change.

2 HEALTH DIALOGUE APRIL2021
DefinitionsPersonal burnout The degree of physical and psychological fatigue and
exhaustion experienced by the person overall, including work-related, patient-related burnout and non-work-related factors.
Work-related burnout The degree of physical and psychological fatigue and exhaustion that is perceived by the person as related to his/her work.
Patient-related burnout The degree of physical and psychological fatigue and exhaustion that is perceived by the person as related to his/her work with patients.
Why burnout still mattersThe2015reportintoburnoutprovidedacriticallensontheconsequencesofamedicalworkforceenduringlong-termstaffingshortages,growingpatientdemandandclinicalcreep.Atthetime,itwasthefirstnationwidestudyofburnoutinthecountry’spublichealthworkforceofseniordoctorsanddentistsusingtheCBI.Burnoutisnow established as a key indicator of the health andwellbeingoftheseniormedicalanddentalworkforceinNewZealandandemployershaveadutyofcareinthisregard.
In2019thedefinitionofburnoutwaschangedbytheWorldHealthOrganisation(WHO)torecogniseburnoutasanoccupationalsyndrome.TheInternationalClassificationofDiseasesdiagnosticmanualnowdefinesburnoutas“resultingfromchronicworkplacestressthathasnotbeensuccessfullymanaged”(WHO2019).Thischangeindefinitionsignalsanimportantshiftinunderstandingburnoutasbeingaconsequenceofwork.Burnoutisnotasignofanindividualweaknessorfailuretocope.Thissyndromeiscausedbystressorsintheworkplace.Thischangeinemphasisrequiresthedeploymentofnewstrategiestoaddressburnout.Whilemindfulnesstechniques,stressmanagement,andpersonal
resiliencehavetheirplace,fixingburnoutwillentailaddressingtheconditionsofworkwhichcreatestressandconsideringhowthesecanbemodified(MaslachandLeiter2017).
Burnout is not a sign of an individual weakness or failure to cope. This syndrome is caused by stressors in the workplace. This change in emphasis requires the deployment of new strategies to address burnout.
WhilescreeningtoolssuchastheCBIandtheMaslachburnoutinventory(MBI)arenotclinicaldiagnostictools(Bianchi,Boffyetal.2013,Lall,Gaetaetal.2019),surveysthatsignalahighprevalenceofburnoutinapopulationwarrantseriousconsiderationandattention.Asmyriadstudieshavedemonstrated,therearecloseassociationsbetweenburnoutandintentionstoleavework(Ran,Chenetal.2020),workingthroughillness(Pei,Linetal.2020),suicidalideation(Kane2019,Menon,Shanafeltetal.2020),andqualityofpatientcare(Hewitt,Ellisetal.2020).Burnouthassignificantassociationswithsleepdeprivationandisinturnrelatedtothelikelihoodofmakingclinicallysignificantmedicalerrors(Trockel,Menonetal.2020).Definedasacomplexanddynamic

WWW.ASMS.ORG.NZ HEALTH DIALOGUE 3
phenomenon,ratherthanafixedendpoint(Danhauer,Filesetal.2020),burnoutstudiessuchastheseundertakenbytheASMSprovideimportantinsightsintothehealthandwellbeingofcriticalworkforces.Thesestudiesarekeymarkerpoints,providingvaluableinformationanddataregardingburnout,hoursofwork,gender,andageaswellasperceptionsofkeystressorsthatindividualsviewaskeycontributingfactors.
Burnout is now established as a key indicator of the health and wellbeing of the senior medical and dental workforce in New Zealand and employers have a duty of care in this regard.
Oneofthekeyfindingsfromthe2015researchwasthehighlevelofburnoutexperiencedbydoctorsintheir30s,particularlywomen.Thesubsequentqualitativestudyintothelivedexperiencesofwomenworkinginmedicine(ASMS2019a)exploredwhetherburnoutcanresultfromchallengeswithwork-lifeintegration(Johnson,Irishetal.2020).Astheresearchdemonstrated,concernsforwork-lifeintegrationreflectedgenderschemaswhichframeresponsibilityfordomesticaffairsasthedutyofwomen(ChadwickandBaruah2020).Akeycontributionofthisstudy,moreover,wasthedemonstrationofthepervasivenature
ofgenderedassumptionsconcerningappropriatebehaviour,comportment,andindicatorsofsuccessanddedicationastheypertaintomedicine.Someoftheseindicatorssuchaslongworkinghours,negativeviewsconcerningpart-timework,andtheexpectationtoalwaysprioritiseworkwereshowntoresultinsignificantstressandillustratedconcerningaspectsofcurrentworkingpractices(ParedesandCochran2020).Theyalsoillustratedhowgender-baseddiscriminationcanaddsignificantpressuretothealreadydemandingnatureofmedicalwork(Wang,Taniousetal.2020).The2020studysoughttofurtherexplorethesetrendsbyincludingquestionspertainingtothenumberofdependantsaswellashoursofwork.
Atpresent,ASMSestimatesNewZealandhasanSMOstaffingshortageofapproximately24%basedontheviewsofclinicaldirectorsworkingaroundthecountry(ASMS2019b).Attendingtoconditionsofworkwhichmayimprovework-lifeintegration,andinturn,reduceburnoutpropensity,islikelytopaydividendsintheretentionofthishighlyqualifiedworkforce(Nuss,Tessieretal.2020).Aswithprevioussurveys,thisresearchsoughttoanalysequalitativecommentsleftbyresponderstohighlightissuesthatindividualsfeltweremostpressingintermsoftheirrespectivework-lifebalanceandsatisfactionatwork.

4 HEALTH DIALOGUE APRIL2021
MethodologyAtotalof4653membersoftheASMSwereaskedbyemailtotakepartinananonymousonlinesurveyinAugust2020.HostedbySurveyMonkey,itwasopenforonemonthandfourremindersweresenttoencouragesurveycompletion.Participationwasvoluntaryandnoincentivesforparticipationwereprovided.
Aswiththeoriginal2015burnoutsurvey,theresearchusedtheCBItoassessthedegreeofburnoutintheASMSmembership.TheCBIattemptstosimplifyandrefinetheconceptofburnouttoastateofemotionalandphysicalexhaustion.Inthisexaminationofburnout,personalburnoutisassessedonthedegreetowhichrespondentsfeeltired,wornout,orphysicallyandemotionallyexhausted,regardlessofperceivedcause.Itisconceptualizedasthedegreeofoverallburnoutexperiencedbyanindividual.Work-relatedburnoutisameasureofthe“degreeofphysicalandpsychologicalfatigueandexhaustionthatisperceivedbythepersonasrelatedtotheirwork”(Kristensen,Hannerzetal.2005p197).Clientorpatient-relatedburnoutis“thedegreeofphysicalandpsychologicalfatigueandexhaustionthatisperceivedbythepersonasrelatedtotheirworkwithclients”(Ibid).This‘client’or‘patient’relatedaspectisdeemedtobeasecondtierofwork-relatedissues,butonewhichhasafocusontheimpactof‘peoplework’.Onlythosewhoworkface-to-facewithclients,orinthemedicalcontext,patients,wererequiredtoanswerthissectionoftheinventory.
Degreeofburnoutwasmeasuredaccordingtoafive-itemLikertscaleusingresponsecategories‘Always’,‘Often’,‘Sometimes’,‘Seldom’,‘Never/almostnever’,and‘Toaveryhighdegree’,Toahighdegree’,‘Somewhat’,‘Toalowdegree’,and‘Toaverylowdegree’.Burnoutwasdefinedaccordingtoinstructionsintheinventorywherethosewhoscoreequaltoorabove50onaverageineachofthethreescalesareclassedasexperiencingahighlevelofburnout.Prevalencescoreswerecalculated
byassessingthepercentageofindividualswhoscoreas‘burnt-out’(i.e.withscores≥50)asapercentageoftheoverallrespondents.Meanburnoutscoreswerethencalculatedbyaveragingthescoresforeachlineofquestioningandtakinganoverallaverageofthescore(seeinstructionsontheCBIinKristensen,Hannerzetal.2005).
AdditionalquestionswerebasedontheAustralianMedicalAssociation’s(AMA)RiskAssessmentchecklistintohoursofwork,includingwhetherparticipantshadworkedmorethan24consecutivehours,andwhethertheyhaveaperiodofrestoflessthan10hours(AMA2005).Respondentswerealsoaskedtoestimatetotalhoursofworkfortheweekpriortocompletingthesurvey.Hoursofworkweredefinedasincludingstandardhoursworked,privatework,hourson-call(includingtimeon-callbutnotcalledin),andanytimespentdoingadministrativetasksathome,includingemail.Hoursofworkwerereportedintenhourincrements.
IndependantvariablesweretakenfromresponsestotheWorldHealthOrganisation’s(WHO)self-healthassessmenttool(asingleitemmeasureofhealth)anddemographicdataincludinggender,age(accordingtofivecategories),lengthoftimeworkedinNewZealand(accordingtofivecategories),primaryDHBandspecialty.Specialtiesweresummarisedaccordingtonumberofrespondentsandallspecialtieswithn>/=20wereincluded in the analysis. Others were included accordingtobroaderspecialtygroupings.Foralistofspecialties<20andtheirgroupingseeAppendix1.Additionaldemographicdatawassoughtonnumberofdependants.Dependantsweredefinedaschildrenforwhomanindividualwasparentorguardian,livinginthesamehousehold.Ethnicity data was not collected in this study. This isalimitationandfutureworkwillincludethisdemographicvariable.
TheCBIwassituatedalongsideabroadersuiteofquestionsexaminingindicatorsofworking

WWW.ASMS.ORG.NZ HEALTH DIALOGUE 5
conditions,staffingissuesandmembershipprioritiesfortheyearahead.Whererelevant,thesequestionswereusedincorrelationanalysis,butthisreportmainlyfocussesonthefindingsoftheburnoutquestionnaire.Associationsbetweenthemeanandprevalencescoresonthethreeburnoutscales,hoursofwork,responsestotheriskassessmentchecklistquestions,andtheindependantdemographicvariablesspecifiedaboveweretestedusingSpearman’srho,Chi-squareandone-wayANOVAasappropriateonSPSS(version23.0).Theseresultsaresummarisedusing95%confidenceintervals.
Qualitative data analysisDataanalysisofthecommentsleftineachsectionoftheburnoutsurveywasundertakenseparatelybyimportingthemintoNVivopro(version11),readingthemindetailandcodingthemesastheyemerged.Thosefromthe‘generalcomments’
sectionattheendofthesurveywerealsoexaminedbutthequalitativedataanalysiswasrestrictedinthisinstancetothecommentsleftintheburnoutsectionofthesurvey.
Patternsandtrendsemergingfromthequantitativedataanalysiswereexploredbycross-cuttingcommentsbygender,selectedspecialtieswithhighburnoutscoresandselectedDHBswithhighburnoutscores.Thiscross-cutqualitativematerialwasconsideredfurtherandwhererelevantcomparativeanalysiswasperformedbetweencategoriesofcommentstoexamineanydifferencesinhowthemeswereexpressedorthefrequencyofthematicexpression.
Commentsselectedforinclusioninthefinalreportwerethosethatbestexpressedthethemes.Theseweretranscribedverbatimandanyomittedwordsaresignalledbyellipses.Anywordsreplacedoralteredtopreserveanonymityorcorrectfortenseorsenseareplacedinsquarebrackets.

6 HEALTH DIALOGUE APRIL2021
Results
Demographic informationThedemographicpatternofrespondentsisbroadlyconsistentwithprevioussurveys.2020wasthefirsttimegender-diversewasincludedasanoption.Thelownumberofgender-diverserespondentsmeanttheiranswerswereexcludedfromthemainstatisticalanalysis.FulldemographiccharacteristicsofrespondentsaresummarizedinTable1.Mostrespondentsweremale(54%),agedbetween40-49(35%),andhadworkedinNewZealandforbetween15-30years(45%).48%hadtwoormoredependants.
HOW MANY YEARS HAVE YOU WORKED IN THE NEW ZEALAND PUBLIC HEALTH CARE SYSTEM? Lessthan5years 194 10%5-14years 644 33%15-30years 877 45%Morethan30years 225 12%IN GENERAL HOW WOULD YOU RATE YOUR HEALTH?Excellent 452 23%Verygood 855 44%Good 474 24%Fair 146 8%Poor 13 1%WHAT IS YOUR AGE GROUP?20-29 6 0.3%30-39 285 15%40-49 670 35%50-59 619 32%60orover 355 18%WHAT DO YOU PRIMARILY IDENTIFY AS? Male 1037 54%Female 837 43%Genderdiverse 5 0.3%Prefer not to answer 53 3%HOW MANY CHILDREN ARE YOU PARENT OR GUARDIAN FOR AND LIVE IN YOUR HOUSEHOLD?None 672 35%1 317 17%2 606 32%3 259 14%4 47 2%Morethan4 17 1%
TABLE 1: DEMOGRAPHIC INFORMATION OF RESPONDENTS
A total of 2102 of the 4653 potential respondents responded to the survey (45% response rate). Analysis was undertaken using the best available data. Where applicable, n values are specified for each question. Only 1.2% of the survey applied to non-DHB members. For ease of comparability, analysis of the burnout data is restricted to DHB members as this was the focus of the 2015 survey.

WWW.ASMS.ORG.NZ HEALTH DIALOGUE 7
WHAT IS YOUR PRIMARY SPECIALTY? Anaesthesia 289 16%Psychiatry 211 12%EmergencyMedicine 164 9%Medicine 146 8%Paediatrics 136 8%Diagnostic&InterventionalRadiology
94 5%
Obstetrics/Gynaecology 77 4%Geriatric Medicine 60 3%GeneralSurgery 55 3%IntensiveCareMedicine 51 3%Pathology 52 3%OrthopaedicSurgery 47 3%Dentistry 37 2%GeneralPractice 32 2%MedicalOncology 28 2%Otolaryngology 27 2%Public Health Medicine 26 2%RuralHospitalMedicine 22 1%Gastroenterology 21 1%Ophthalmology 21 1%RadiationOncology 20 1%RespiratoryMedicine 20 1%Internal Medicine 76 4%Surgery 58 3%WHICH DHB IS YOUR PRIMARY PLACE OF WORK? (% = PROPORTION OF POTENTIAL DHB RESPONDENTS)Auckland 302 37%Bay of Plenty 106 52%Canterbury 227 43%Capital&Coast 137 39%CountiesManukau 194 43%Hawke's Bay 59 44%HuttValley 59 47%Lakes 47 51%MidCentral 67 48%NelsonMarlborough 72 56%Northland 64 40%SouthCanterbury 20 48%Southern 101 63%Tairawhiti 17 40%Taranaki 38 37%Waikato 145 39%Wairarapa 9 47%Waitemata 178 39%WestCoast 12 46%Whanganui 15 35%
8 HEALTH DIALOGUE APRIL2021
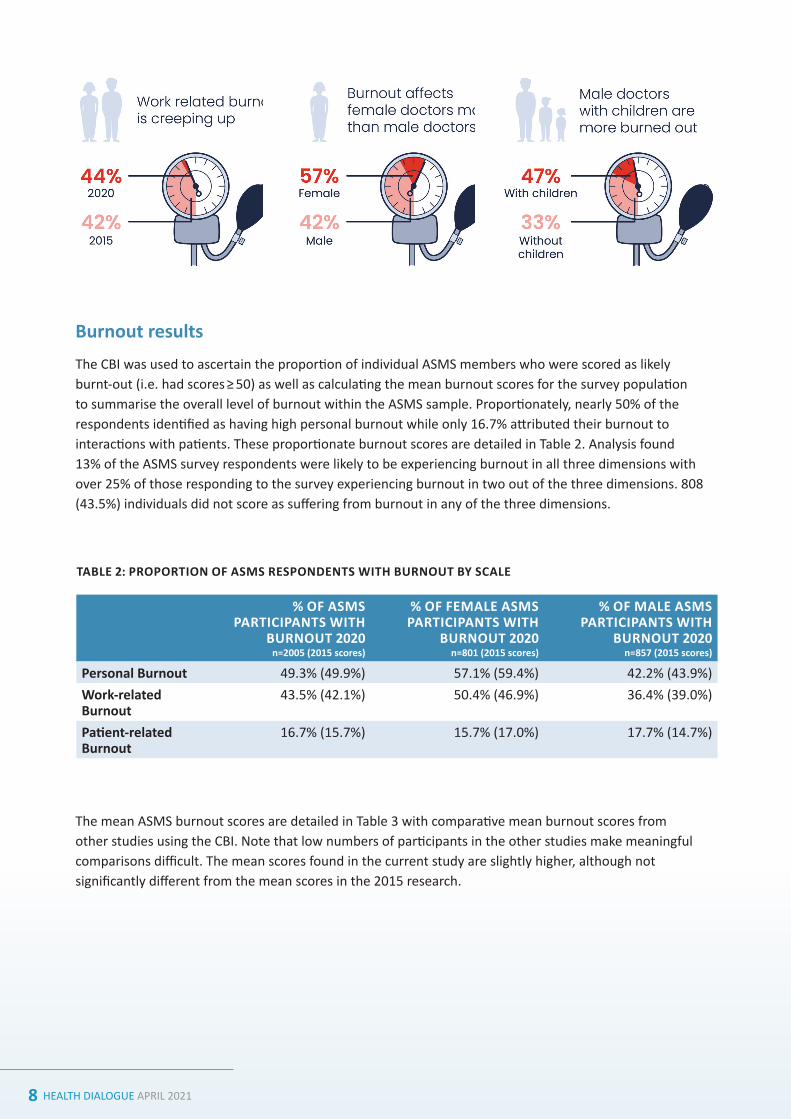
Burnout resultsTheCBIwasusedtoascertaintheproportionofindividualASMSmemberswhowerescoredaslikelyburnt-out(i.e.hadscores≥50)aswellascalculatingthemeanburnoutscoresforthesurveypopulationtosummarisetheoveralllevelofburnoutwithintheASMSsample.Proportionately,nearly50%oftherespondentsidentifiedashavinghighpersonalburnoutwhileonly16.7%attributedtheirburnouttointeractionswithpatients.TheseproportionateburnoutscoresaredetailedinTable2.Analysisfound13%oftheASMSsurveyrespondentswerelikelytobeexperiencingburnoutinallthreedimensionswithover25%ofthoserespondingtothesurveyexperiencingburnoutintwooutofthethreedimensions.808(43.5%)individualsdidnotscoreassufferingfromburnoutinanyofthethreedimensions.
TABLE 2: PROPORTION OF ASMS RESPONDENTS WITH BURNOUT BY SCALE
% OF ASMS PARTICIPANTS WITH
BURNOUT 2020 n=2005 (2015 scores)
% OF FEMALE ASMS PARTICIPANTS WITH
BURNOUT 2020 n=801 (2015 scores)
% OF MALE ASMS PARTICIPANTS WITH
BURNOUT 2020 n=857 (2015 scores)
Personal Burnout 49.3%(49.9%) 57.1%(59.4%) 42.2%(43.9%)
Work-related Burnout
43.5%(42.1%) 50.4%(46.9%) 36.4%(39.0%)
Patient-related Burnout
16.7%(15.7%) 15.7%(17.0%) 17.7%(14.7%)
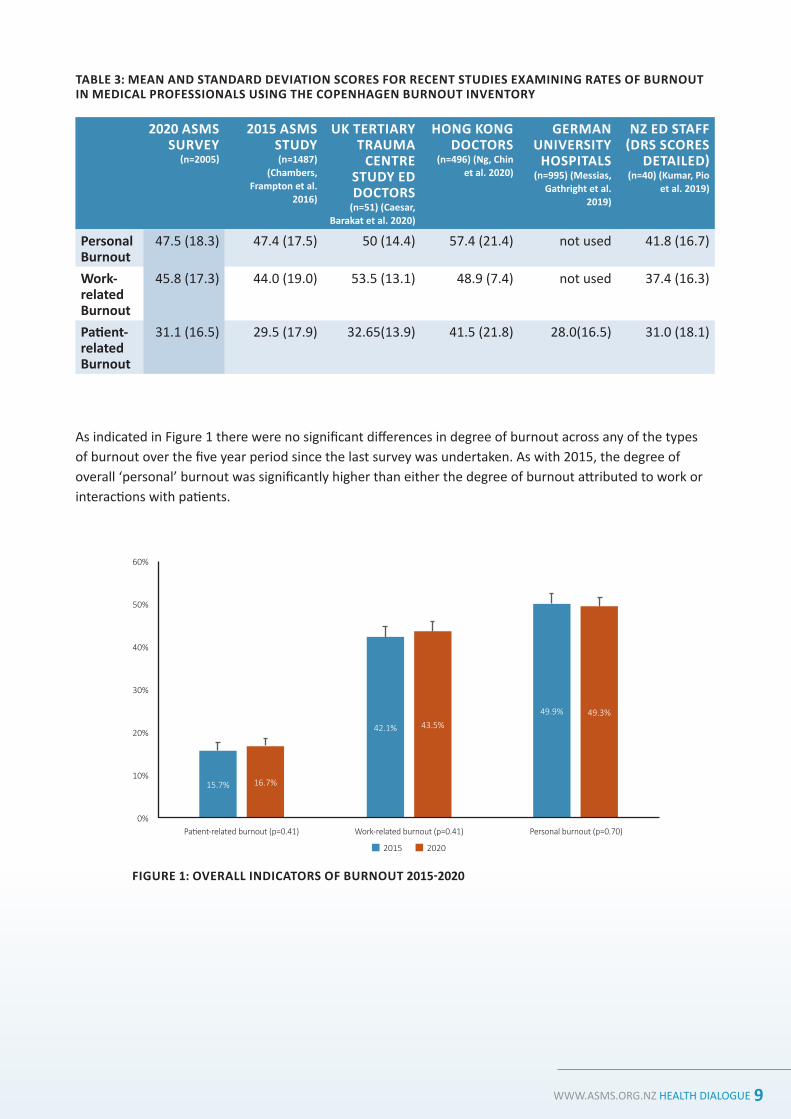
ThemeanASMSburnoutscoresaredetailedinTable3withcomparativemeanburnoutscoresfromotherstudiesusingtheCBI.Notethatlownumbersofparticipantsintheotherstudiesmakemeaningfulcomparisonsdifficult.Themeanscoresfoundinthecurrentstudyareslightlyhigher,althoughnotsignificantlydifferentfromthemeanscoresinthe2015research.
WWW.ASMS.ORG.NZ HEALTH DIALOGUE 9
TABLE 3: MEAN AND STANDARD DEVIATION SCORES FOR RECENT STUDIES EXAMINING RATES OF BURNOUT IN MEDICAL PROFESSIONALS USING THE COPENHAGEN BURNOUT INVENTORY
2020 ASMS SURVEY
(n=2005)
2015 ASMS STUDY (n=1487)
(Chambers, Frampton et al.
2016)
UK TERTIARY TRAUMA
CENTRE STUDY ED DOCTORS
(n=51) (Caesar, Barakat et al. 2020)
HONG KONG DOCTORS
(n=496) (Ng, Chin et al. 2020)
GERMAN UNIVERSITY
HOSPITALS (n=995) (Messias,
Gathright et al. 2019)
NZ ED STAFF (DRS SCORES
DETAILED) (n=40) (Kumar, Pio
et al. 2019)
Personal Burnout
47.5(18.3) 47.4(17.5) 50(14.4) 57.4(21.4) not used 41.8(16.7)
Work-related Burnout
45.8(17.3) 44.0(19.0) 53.5(13.1) 48.9(7.4) not used 37.4(16.3)
Patient-related Burnout
31.1(16.5) 29.5(17.9) 32.65(13.9) 41.5(21.8) 28.0(16.5) 31.0(18.1)
AsindicatedinFigure1therewerenosignificantdifferencesindegreeofburnoutacrossanyofthetypesofburnoutoverthefiveyearperiodsincethelastsurveywasundertaken.Aswith2015,thedegreeofoverall‘personal’burnoutwassignificantlyhigherthaneitherthedegreeofburnoutattributedtoworkorinteractionswithpatients.
FIGURE 1: OVERALL INDICATORS OF BURNOUT 2015-2020
60%
50%
0%
10%
20%
30%
40%
Patient-related burnout (p=0.41) Work-related burnout (p=0.41) Personal burnout (p=0.70)
20202015
49.9%
42.1%
15.7%
49.3%43.5%
16.7%

10 HEALTH DIALOGUE APRIL2021
Burnout and demographic variables Aswiththe2015surveyallformsofburnoutweresignificantlyassociatedwithworseninghealthstatus(Figure2).
Whenbrokendownbygender,maleandfemalerespondentshadaslightdecreaseinoverallburnoutbutthiswasnotsignificant(Figure3).Femalerespondentshadaslightincreaseintheproportionwithwork-relatedburnoutbutthiswasalsonotsignificant(Figure4).Nosignificantdifferenceswererecordedinthedegreeofburnoutrelatedtopatientinteractions(Figure5).
FIGURE 2: RELATIONSHIP BETWEEN BURNOUT AND SELF-RATED HEALTH STATUS (p=0.000)
% with personal burnout% with work-related burnout
90%
80%
70%
60%
50%
0%
10%
20%
30%
40%
Excellent Very good FairGood Poor
89
98108
250288
343392
113 128
FIGURE 3: PERSONAL BURNOUT BY GENDER 2015-2020
20202015
70%
60%
50%
0%
10%
20%
30%
40%
Female (p=0.38) Male (p=0.46)
59.4%
43.9%
57.1%
42.2%

WWW.ASMS.ORG.NZ HEALTH DIALOGUE 11
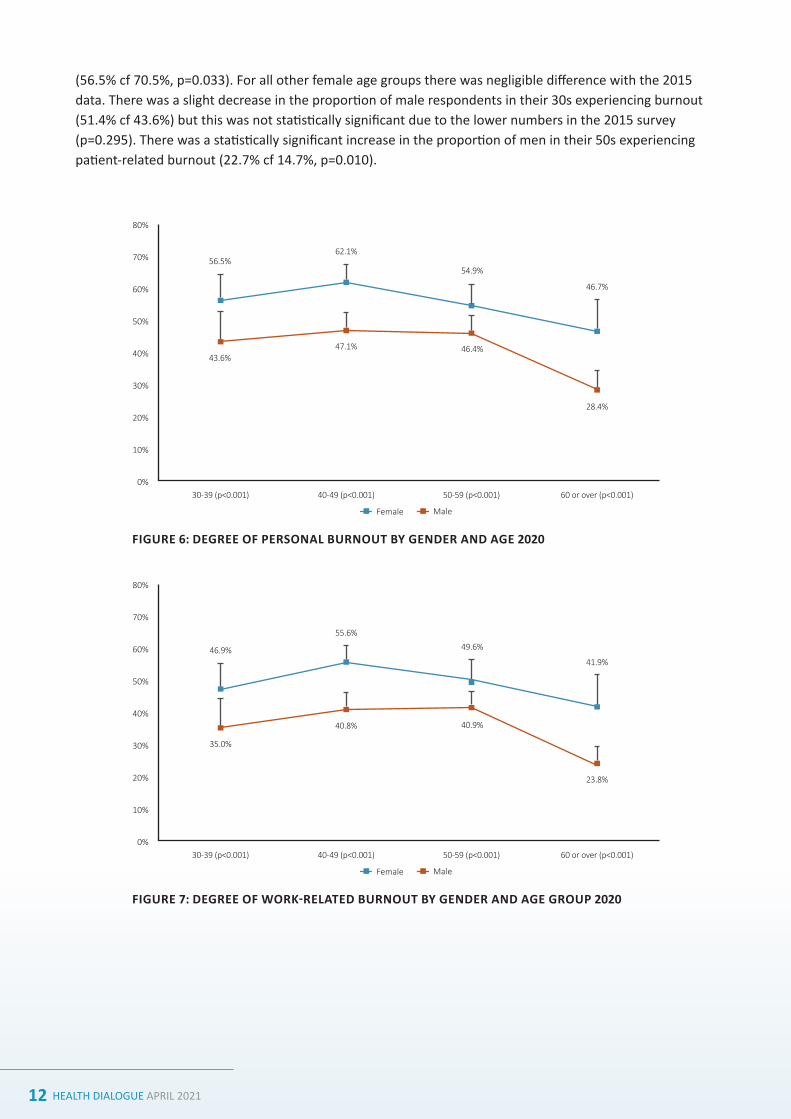
Gender and burnout 2020Figure6andFigure7displaytheproportionofrespondentsbyagegroupandgenderscoringaslikelytobeexperiencingpersonalandwork-relatedburnout.Therewasastatisticallysignificantdifferenceintheproportionofrespondentsexperiencingburnoutbygenderinallagegroupswithahigherproportionofwomenlikelytobeexperiencingburnoutthantheirmalecounterpartsoverall.Respondentsinyoungeragecohortsaremorelikelytoexperienceburnoutthanthoseintheolderagecohorts.Bothmenandwomenaremostlikelytoexperiencepersonalandwork-relatedburnoutintheir40s.Ofnotewasthedecreaseintheproportionofwomenintheir30slikelytobesufferingfromburnoutwhencomparedtothe2015data
FIGURE 4: WORK-RELATED BURNOUT BY GENDER 2015-2020
20202015
50.4%
60%
50%
0%
10%
20%
30%
40%
Female (p=0.20) Male (p=0.25)
46.9%
39.0%36.4%
FIGURE 5: PATIENT-RELATED BURNOUT BY GENDER 2015-2020
20202015
17.0%15.7%
17.7%
25%
20%
0%
5%
10%
15%
Female (p=0.53) Male (p=0.09)
14.7%
12 HEALTH DIALOGUE APRIL2021
(56.5%cf70.5%,p=0.033).Forallotherfemaleagegroupstherewasnegligibledifferencewiththe2015data.Therewasaslightdecreaseintheproportionofmalerespondentsintheir30sexperiencingburnout(51.4%cf43.6%)butthiswasnotstatisticallysignificantduetothelowernumbersinthe2015survey(p=0.295).Therewasastatisticallysignificantincreaseintheproportionofmenintheir50sexperiencingpatient-relatedburnout(22.7%cf14.7%,p=0.010).
FIGURE 6: DEGREE OF PERSONAL BURNOUT BY GENDER AND AGE 2020
MaleFemale
30-39 (p<0.001)
43.6%
56.5%
47.1%
62.1%
46.4%
54.9%
28.4%
46.7%
40-49 (p<0.001) 50-59 (p<0.001) 60 or over (p<0.001)
80%
70%
60%
50%
0%
10%
20%
30%
40%
FIGURE 7: DEGREE OF WORK-RELATED BURNOUT BY GENDER AND AGE GROUP 2020
MaleFemale
30-39 (p<0.001) 40-49 (p<0.001) 50-59 (p<0.001) 60 or over (p<0.001)
80%
70%
60%
50%
0%
10%
20%
30%
40%
35.0%
46.9%
40.8%
55.6%
40.9%
49.6%
23.8%
41.9%

WWW.ASMS.ORG.NZ HEALTH DIALOGUE 13
DependantsInthe2020surveywesoughttodeterminewhetherhavingdependants,specificallychildrenstilllivinginthehome,wasassociatedwithahigherdegreeofburnoutexperienced.Overall,wefoundthatthemeanscoreforpersonalburnoutincreasedslightlywithnumberofdependants(p=0.015).
Therewasnostatisticalrelationshipbetweenexperiencingeitherwork-relatedorpatient-relatedburnoutandwhetherrespondentshaddependants.
Whenthedatawassplitaccordingtogender,furtherpatternsemerged.Therewasnegligibledifferenceintheproportionoffemalerespondentsexperiencingeitherwork-relatedburnoutorpersonalburnoutandwhetherornottheyhaddependants.Formen,however,havingoneormorechildrenresultedinhigherratesofpersonalandwork-relatedburnout,aswellasaslightincreaseintheproportionexperiencingpatient-relatedburnout(Figure8,Figure9,Figure10).Thep-valuessignalthesignificantdifferenceindegreeofburnoutbygender.
FIGURE 8: PROPORTION OF RESPONDENTS EXPERIENCING PERSONAL BURNOUT BY DEPENDANT STATUS AND GENDER
MaleFemale
No children (p<0.001) One or more children (p<0.001)
70%
60%
50%
0%
10%
20%
30%
40%
54.9%
33.4%
58.3%
46.9%

14 HEALTH DIALOGUE APRIL2021
There was no statistical relationship between experiencing either work-related or patient-related burnout and whether respondents had dependants.
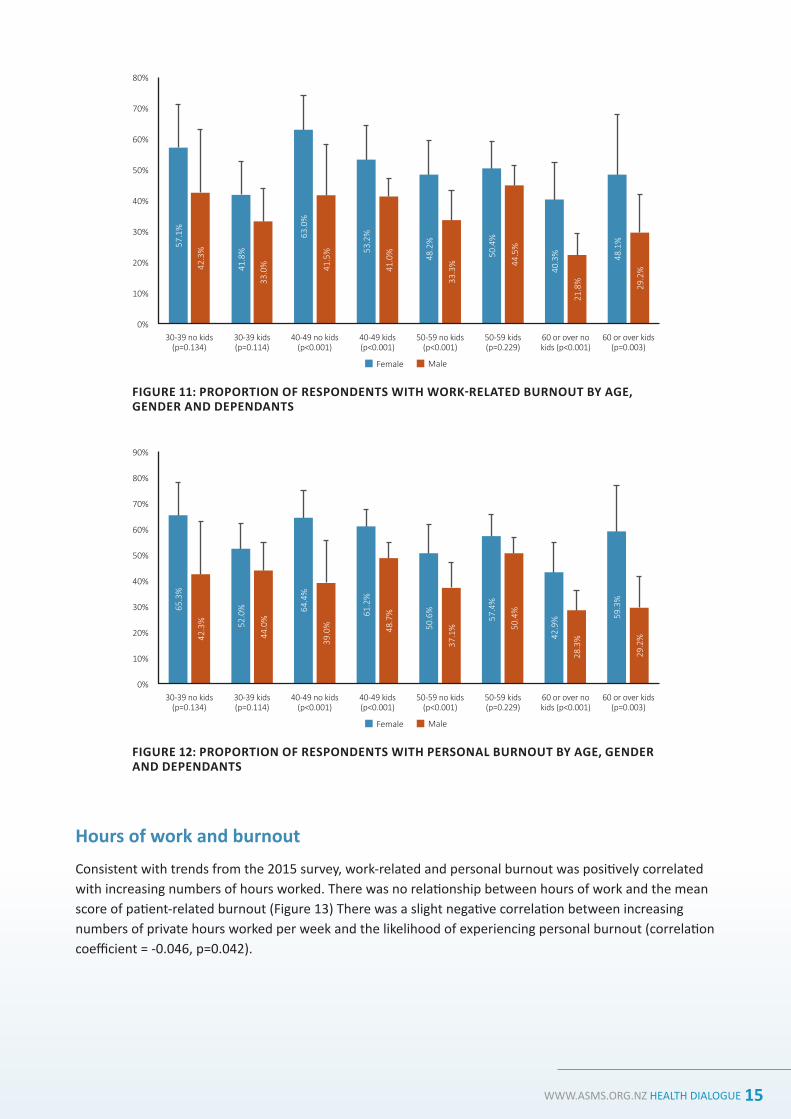
Furtheranalysiswasundertakentoexploretherelationshipbetweenage,dependants,andburnout.Thehighestproportionofwomenexperiencingpersonalburnoutwereintheir30sand40swithoutchildren(65.3%and64.4%respectively).Justover50%ofmenexperiencingpersonalburnoutwereintheir50swithchildren(50.4%).Similartrendsexistedforwork-relatedburnoutwiththehighestproportionexperiencingwork-relatedburnoutbeingwomenintheir30sand40swithoutchildren(57%and63%respectively).Furtheranalysisofthesetrendswasundertakenbyexaminingthenumberofhoursworkedbyage,gender,andnumberofdependants.
MaleFemale
FIGURE 9: PROPORTION OF RESPONDENTS EXPERIENCING WORK-RELATED BURNOUT BY DEPENDANT STATUS AND GENDER
No children (p<0.001) One or more (p<0.001)
70%
60%
50%
0%
10%
20%
30%
40%
51.4% 50.0%
40.1%
29.4%
FIGURE 10: PROPORTION OF RESPONDENTS EXPERIENCING PATIENT-RELATED BURNOUT BY DEPENDANT STATUS AND GENDER
MaleFemale
No children (p<0.001) One or more (p<0.001)
25%
20%
15%
0%
5%
10%
16.5%14.8%
18.5%16.6%
WWW.ASMS.ORG.NZ HEALTH DIALOGUE 15
Hours of work and burnout Consistentwithtrendsfromthe2015survey,work-relatedandpersonalburnoutwaspositivelycorrelatedwithincreasingnumbersofhoursworked.Therewasnorelationshipbetweenhoursofworkandthemeanscoreofpatient-relatedburnout(Figure13)Therewasaslightnegativecorrelationbetweenincreasingnumbersofprivatehoursworkedperweekandthelikelihoodofexperiencingpersonalburnout(correlationcoefficient=-0.046,p=0.042).
FIGURE 11: PROPORTION OF RESPONDENTS WITH WORK-RELATED BURNOUT BY AGE, GENDER AND DEPENDANTS
MaleFemale
30-39 no kids (p=0.134)
30-39 kids (p=0.114)
40-49 no kids (p<0.001)
40-49 kids (p<0.001)
50-59 no kids (p<0.001)
50-59 kids (p=0.229)
60 or over no kids (p<0.001)
60 or over kids (p=0.003)
80%
70%
60%
50%
0%
10%
20%
30%
40%
57.1
%
42.3
%
41.8
%
33.0
% 41.5
%
63.0
%
41.0
%53.2
%
33.3
%
48.2
%
44.5
%
50.4
%
21.8
%
40.3
%
29.2
%
48.1
%
MaleFemale
FIGURE 12: PROPORTION OF RESPONDENTS WITH PERSONAL BURNOUT BY AGE, GENDER AND DEPENDANTS
30-39 no kids (p=0.134)
30-39 kids (p=0.114)
40-49 no kids (p<0.001)
40-49 kids (p<0.001)
50-59 no kids (p<0.001)
50-59 kids (p=0.229)
60 or over no kids (p<0.001)
60 or over kids (p=0.003)
90%
80%
70%
60%
50%
0%
10%
20%
30%
40%
42.3
%
44.0
%
39.0
% 48.7
%
37.1
% 50.4
%
28.3
%
29.2
%
65.3
%
52.0
% 64.4
%
61.2
%
50.6
%
57.4
%
42.9
% 59.3
%

16 HEALTH DIALOGUE APRIL2021
CorrelationsbetweentheburnoutscoresandAMAsafeworkguidelinessuggestasignificantassociationbetweenrespondentsreportingworkingmorethan14consecutivehoursaswellasfailingtohavea24hourbreakfreeofanyscheduledworkandtheproportionscoringasburntoutforwork-relatedandpersonalburnout(Table4).
TABLE 4: BURNOUT AND RESPONSES TO THE AMA SAFE WORK GUIDELINES
PERSONAL BURNOUT WORK-RELATED BURNOUT PATIENT-RELATED BURNOUT
NOT BURNT-
OUT
BURNT-OUT
p VALUE NOT BURNT-
OUT
BURNT-OUT
p VALUE NOT BURNT-
OUT
BURNT-OUT
p VALUE
Have you worked more than 14 consecutive hours in any one period?
No 54.7% 45.3% 61.1% 38.9% 84.7% 15.3%
Yes 43.0% 57.0% <0.001 46.9% 53.1% <0.001 80.4% 19.6% 0.020
Did you have a period of rest between scheduled work
No 51.5% 48.5% 58.3% 41.7% 83.3% 16.7%
Yes 49.8% 50.2% 0.467 54.3% 45.7% 0.075 84.1% 15.9% 0.672
Did you have a 24-hour break free of any scheduled work
No 41.5% 58.5% 49.1% 50.9% 80.6% 19.4%
Yes 53.9% 46.1% <0.001 59.1% 40.9% <0.001 84.4% 15.6% 0.060
FIGURE 13: MEAN BURNOUT SCORE AND WEEKLY HOURS OF WORK
Work PersonalPatient
None <10 hours 10-20 hours
20-30 hours
30-40 hours
70-80 hours
40-50 hours
80-90 hours
50-60 hours
90-100 hours
60-70 hours
>100 hours
70
60
50
0
10
20
30
40
WWW.ASMS.ORG.NZ HEALTH DIALOGUE 17
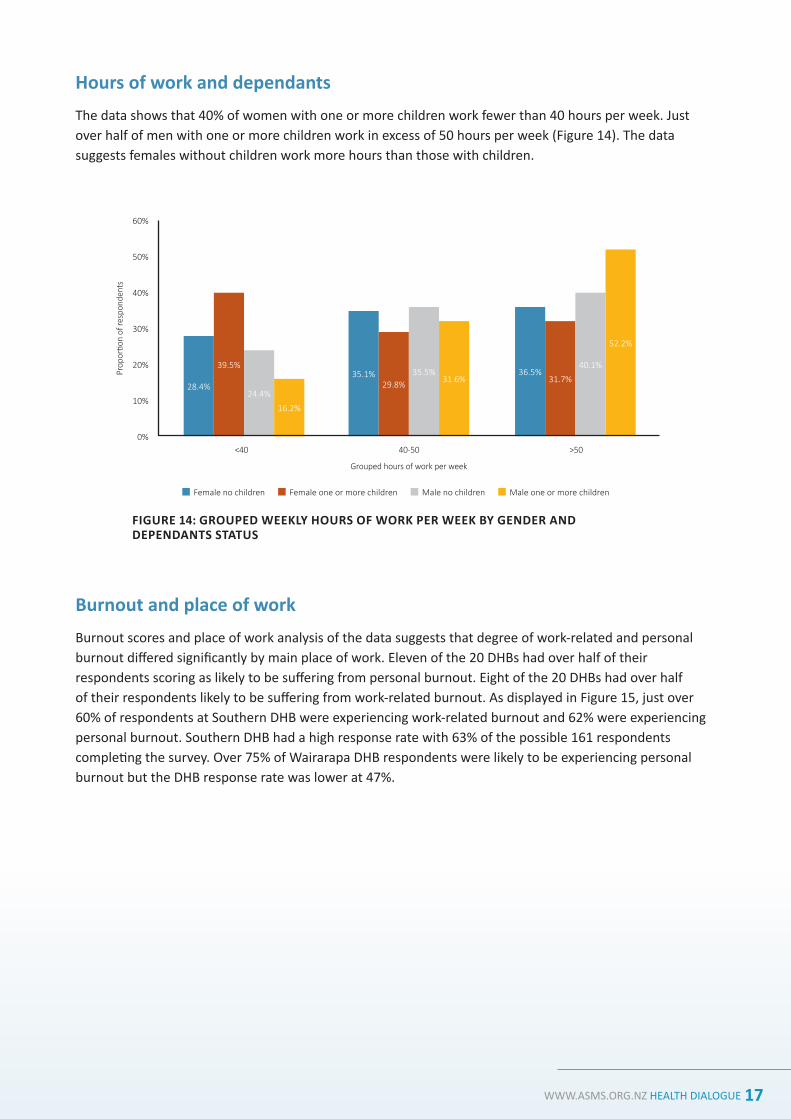
Hours of work and dependants Thedatashowsthat40%ofwomenwithoneormorechildrenworkfewerthan40hoursperweek.Justoverhalfofmenwithoneormorechildrenworkinexcessof50hoursperweek(Figure14).Thedatasuggestsfemaleswithoutchildrenworkmorehoursthanthosewithchildren.
Burnout and place of workBurnoutscoresandplaceofworkanalysisofthedatasuggeststhatdegreeofwork-relatedandpersonalburnoutdifferedsignificantlybymainplaceofwork.Elevenofthe20DHBshadoverhalfoftheirrespondentsscoringaslikelytobesufferingfrompersonalburnout.Eightofthe20DHBshadoverhalfoftheirrespondentslikelytobesufferingfromwork-relatedburnout.AsdisplayedinFigure15,justover60%ofrespondentsatSouthernDHBwereexperiencingwork-relatedburnoutand62%wereexperiencingpersonalburnout.SouthernDHBhadahighresponseratewith63%ofthepossible161respondentscompletingthesurvey.Over75%ofWairarapaDHBrespondentswerelikelytobeexperiencingpersonalburnoutbuttheDHBresponseratewaslowerat47%.
FIGURE 14: GROUPED WEEKLY HOURS OF WORK PER WEEK BY GENDER AND DEPENDANTS STATUS
Female one or more children Male no children Male one or more childrenFemale no children
<40 40-50 >50
Grouped hours of work per week
Prop
ortio
n of
resp
onde
nts
60%
50%
0%
10%
20%
30%
40%
28.4%35.1% 36.5%
39.5%
29.8%31.7%
24.4%
35.5%40.1%
16.2%
31.6%
52.2%

18 HEALTH DIALOGUE APRIL2021
FIGURE 15: WORK-RELATED AND PERSONAL BURNOUT BY DHB 2020
10% 20% 30% 40% 50% 60% 70% 80%
80%
70%
60%
50%
0%
10%
20%
30%
40%
Personal burnout
Wor
k-re
late
d bu
rnou
t
Wairarapa DHBTaranaki DHB
Nelson Marlborough DHBHawke’s Bay DHB
Canterbury DHB
Waikato DHB
Lakes DHB
Northland DHB
Whanganui DHB
Southern DHBMidCentral DHB
Bay of Plenty DHBWest Coast DHB
Tairawhiti DHB
Hutt Valley DHBWaitemata DHB
Counties Manukau DHBSouth Canterbury DHB
Capital & Coast DHB
Auckland DHB
Whencomparedwiththe2015data,12DHBshadincreasedtheirrateofpersonalandwork-relatedburnoutandsevenhaddecreased(Table5&Table6).OnlySouthernDHB’sincreasedburnoutscorewasstatisticallysignificantwhencomparedtothe2015survey(p=0.013).TheimprovementinpersonalburnoutforHuttValleyDHBwasalsostatisticallysignificant(p=0.033).SouthernDHBwasalsoastatisticallysignificantincreasedscoreforwork-relatedburnout(p=0.002).

WWW.ASMS.ORG.NZ HEALTH DIALOGUE 19
Greentextindicatesimprovementandredtextindicatesanincreaseintherateofburnout.Blueindicatesnochange. **indicatesstatisticalsignificance.
TABLE 5: PERSONAL BURNOUT AND DHB BY YEAR OF SURVEY
TABLE 6: WORK-RELATED BURNOUT AND DHB BY YEAR OF SURVEY
PERSONAL BURNOUT 2020 2015Auckland 48.7% 54.8%Bay of Plenty 50.0% 44.9%Canterbury 50.2% 46.8%CapitalandCoast 42.3% 46.5%CountiesManukau 36.6% 47.3%Hawke's Bay 50.8% 51.1%HuttValley 42.4% 63.6%Lakes 48.9% 44.8%MidCentral 56.7% 55.6%NelsonMarlborough 52.8% 59.6%Northland 48.4% 53.1%SouthCanterbury 35.0% 17.6%Southern 62.4% 44.6%Tairawhiti 47.1% 52.2%Taranaki 60.5% 58.3%Waikato 55.2% 48.7%Wairarapa 77.8% 42.9%Waitemata 50.0% 50.0%WestCoast 41.7% 40.0%Whanganui 53.3% 0.0%
WORK-RELATED BURNOUT 2020 2015Auckland 41.5% 48.3%Bay of Plenty 50.9% 38.8%Canterbury 44.1% 38.3%CapitalandCoast 34.3% 32.5%CountiesManukau 33.0% 32.8%Hawke's Bay 50.8% 40.4%HuttValley 42.4% 45.5%Lakes 40.4% 41.4%MidCentral 53.7% 57.8%NelsonMarlborough 51.4% 61.5%Northland 39.1% 48.4%SouthCanterbury 30.0% 29.4%Southern 60.4% 38.5%Tairawhiti 47.1% 47.8%Taranaki 52.6% 50.0%Waikato 39.3% 37.0%Wairarapa 55.6% 50.0%Waitemata 43.3% 39.4%WestCoast 50.0% 50.0%Whanganui 26.7% 0.0%
Greentextindicatesimprovementandredtextindicatesanincreaseintherateofburnout.Blueindicatesnochange. **indicatesstatisticalsignificance.
**
**
**

20 HEALTH DIALOGUE APRIL2021
Specialty and burnoutThelargernumberofrespondentsinthe2020surveymeantthatburnoutscorescouldbepresentedinamorefinelydelineatedmanner.AsdisplayedinFigure16,therewasagoodspreadofburnoutscoreswithRadiationOncologyandRespiratoryMedicinetoppingprevalenceforbothpersonalandwork-relatedburnout(totaln=20forboth).RespondentsinRuralHospitalMedicinehadthesecondhighestscoreforoverallpersonalburnout(totaln=21,64%personalburnout)andthoseinEmergencyMedicine(totaln=164)hadveryhighscoresforbothpersonalandwork-relatedburnout.
FIGURE 16: WORK-RELATED AND PERSONAL BURNOUT BY SPECIALTY 2020
30% 35% 40% 45% 50% 55% 60% 65% 70%
70%
65%
60%
55%
30%
35%
40%
45%
50%
Personal burnout
Wor
k-re
late
d bu
rnou
t
Radiation Oncology
Respiratory Medicine
Rural Hospital MedicineEmergency Medicine
Obstetrics/Gynaecology
PsychiatryDiagnostic & Interventional Radiology
Medical Oncology
Internal Medicine
Opthamology
Pathology
General Practice
Geriatric Medicine
General SurgeryPaediatrics
Surgery
Orthopaedic SurgeryPublic Health Medicine
Dentistry
Anaesthesia
Intensive Care MedicineOtolaryngology
Gastroenterology
General Medicine
Forpatient-relatedburnout,thoseworkinginGeneralPractice(n=39)hadthehighestprevalencescorefollowedbythoseinRuralHospitalMedicine(n=25).Specialtiesshadedingreyhadhigherthantheoverallpatient-relatedburnoutscore(16.7%).Comparisonswiththe2015groupeddatafoundthatonlyPsychiatryhadastatisticallysignificantchangeintheirpatient-relatedburnoutscores;30.1%in2015scoredwithpatient-relatedburnoutcomparedwith21%in2020(p=0.032).

WWW.ASMS.ORG.NZ HEALTH DIALOGUE 21
SPECIALITY n≥20 % PATIENT-RELATED BURNOUT TOTAL nGeneralPractice 35.9% 39
RuralHospitalMedicine 32.0% 25
MedicalOncology 28.6% 28
EmergencyMedicine 25.0% 160
RespiratoryMedicine 25.0% 20
Ophthalmology 23.8% 21
OrthopaedicSurgery 21.3% 47
Psychiatry 21.0% 210
Medicine 19.2% 146
Otolaryngology 17.9% 28
Other 17.1% 70
GeneralSurgery 16.4% 55
Obstetrics/Gynaecology 14.3% 77
Gastroenterology 13.6% 22
Geriatric Medicine 13.3% 60
Paediatrics 11.7% 137
Diagnostic&InterventionalRadiology 11.4% 79
Dentistry 10.8% 37
Anaesthesia 9.2% 292
IntensiveCareMedicine 8.0% 50
PalliativeMedicine 6.9% 29
Personal burnout n=202
Work-relatedburnout n=187
Patient-relatedburnout n=192
Overallcomments n=426
Qualitative data analysisInthisiterationoftheburnoutsurvey,therewerefewerqualitativecommentsleftbyrespondents.Analysiswasundertakenoncommentsbysectionoftheburnoutsurveyasfollows:
22 HEALTH DIALOGUE APRIL2021
Aswiththe2015survey,commentsreferencearangeofissuesincludingtheemotionallydrainingnatureofwork,theimpactofextradutiessuchasbeingaheadofdepartment,issuesoutsideofworksuchashavingyoungchildren,andthevariousstrategiesindividualshadimplementedtoavoidburnoutsuchasreducinghoursofwork.Consistentwiththe2015survey,themainthemesexpressedwereworkloadpressures,lackofstaffincludinglackofadministrativesupport,poorrelationshipswithmanagementandfrustrationswithresourcing,growingpatientload,lackofcontrolandautonomy.Consistentwithprevioustrends,mostrespondentsnotedthepleasuresassociatedwithpatientcontactandsignalledhowenergisingthiscomponentoftheirworkcouldbe.Notableinthisyear’ssurveywerecommentsexpressingtheimpactofCOVID-19withmanyreflectingonthesignificanttollCOVID-19hadtakenontheirworkandtheirpersonalstressandexhaustionlevels.
Onerespondentsummedupthecorethemesasfollowing:
“Lack of resources. Inefficiencies. Focus on targets rather on service provision. Low morale due to cultural factors. Lack of administrative support.”
Anothersummarisedtheirfeelingsas:
“I love my work, I love dealing with the patients, I wish I had more time to do my job properly. But I and my colleagues are frustrated by the unrealistic expectations of the management teams of our capability within the constraints of time and budgets.”
Aswithprevioussurveys,thecommentsprovidedimportantcontextualdetailtothestatisticaltrends,aswellasreflectinghowburnoutwasconceptualisedbytheparticipants,andwhatwassubjectivelyperceivedtobethemaincontributingfactors.ThemainthemesaregroupedintoTable7andsummarisedwithillustrativequotes.

WWW.ASMS.ORG.NZ HEALTH DIALOGUE 23
TABLE 7: MAIN THEMES FROM QUALITATIVE ANALYSIS
THEME ILLUSTRATIVE QUOTEWorkloadpressures Oftenfeelveryrushedandpressuredfortime,andfrequentlyinterrupted.I
usuallyneedtoworkduringmyhalfdayoff(likefillinginthissurvey)andworklateonenightperweek.Worryaboutclinicalsituationsornextday’sworkout-sideofwork.Thinkabouthowtofitmoreworkintheday....Verypoorsupportfor one role I do.
Personalstrategiestoavoidburnout
I’mverycarefulnowtosetasidedayswhereIdon’tlookatanythingtodowithwork,thisisduetopreviousburnout.Ihaveenergytospendonactivitieswhichregenerateme,butseldomcanmustertheenergytodedicatetothosethingsthatarenotwork,butthatIshoulddobutwhichdrainme.I’veusedallmyenergyforthatatwork.
Impactofpersonalsituation,family,health
Ihaveayoungchildathome.Shiftworkontopofthiscanmeanseveraldaysofverylittlesleep.Daysoffaredevotedtochildcareandnotthatrestorative.
Lackofrecognition/supportfrommanagement/frustrationswithmanagement
Inthelast2yearsorsotherehasbeenadramaticincreaseinworkload.Thishasnotbeenopenlyrecognizedbymanagementinanywayatall.Onthewholemanagementdeniesthatthereisaproblem.
Thelast3yearshavebeenparticularlybadwithincreasedin-patientworkload,alongwithconsistentveryhighout-patientworkload.Norecognitionofthisinanymeaningfulwaybythemanagerialgroup.Thelatterdonotengageastheyknowtheycannotsolvetheproblemsonexistingbudget.
Outofhourswork,callwork
Thisisduetoworkinglongconsecutivehoursontheweekendsandworkingwithinadequatesleeponweekendsandafterovernightoncall.
IfacemostdayswithananxiousfeelingbeforeI’veevenleftthedoor,andworseifIamoncall.TheburdenofcontinuitynowliesfirmlywiththeSMOanddemands/expectationsareincreasingyearbyyear,withmoretasks(includingclericalduties)fallingontoSMOs.
ImpactofCOVID DuringtheCOVID-19lockdownIworkedeverydayfor6weeks.Theongoingworkload(Iworkinpublichealth)isnotsustainable.
Stressful nature of work Workinginaverystressfulcombinationsofjobs,withverypoor/nopoorresourcinginatleastoneareaIworkin.Complexdynamicsinteamarestressful.Verylimitedadministrativesupport.Istillenjoyjobbutbattlingtogetadequatecareforpatientsandmakeafailingsystemworkisverytiring.
Thelonghoursofworkareacontributingfactorbutthemainexhaustingcomponentoftheworkisthedemands(unmetpatientneed)andstress(tryingtoaccommodatethisunmetneed)thatcomesfromthedemandsandunrealisticexpectationsfrommanagementthatthepressureofthisunmetneedwillbeaccommodatedbytheendprovider“thedoctors”.
Ifindpatienttimeusuallyquitesatisfyingbutendlesspaperworkisirritatingandcomplaintsinvolvehugestress,endlessunpaidhoursandmakemewishIwasn’tdoingmedicineinawayIneverfeltbefore.
Poorresourcing Itisexhaustingbecauseofchronicunder-resourcingandworkinginsubstandardconditions(physicalenvironmentandcrappyITsystemswhichcreateunnecessaryextrastress)-withnoendinsightorhopeofitimprovingbeforeIretire.
Thestraincomesfromalackofresources.Aconstantpressureregardingrequestsforradiologyandthelongwaitsassociatedisabigone-thefearofonceagainbeingpushedback.Difficultyingettingtheappropriatespecialistservicetoseethepatientinatimelywayisalsofrustrating.WhenIseewhatisavailableinprivate,it’sverydemoralisingforthoseofuscommittedtopublicpracticeandmeetingtheneedsofallofourpatientsnotjustthosewithmeans.

24 HEALTH DIALOGUE APRIL2021
THEME ILLUSTRATIVE QUOTEImpactofextraduties Mostofthefeelingofburnoutissecondarytohavingaclinicalworkloadontop
ofmanagerialwork(clinicaldirectorwork).Itisthemanagerial/DHBsideoftheworkthatisthemostfrustrating.
Lack of control Thereareveryspecificstressorswithworkwhichliearoundlackofcontroloverclinicsize,operatinglistsandtheconflictingpressuresofpatientcare,teachingjuniorsandmeetingDHBcompliancethresholds.IfIhadcontroloverthismystresscouldbemanagedbutIamforcedtohaveclinicsthataretoobigandpatientloadsthatprovidecompetingdemands.
Qualitative analysis of trendsFurtheranalysiswasundertakentoseeifthecommentscouldassistwithunderstandingsomeofthequantitativetrendswithburnout.Forexample,thequalitativedatawascutbyspecialtyandDHBtoseeiftherewereanyapparenttrends,especiallyforwork-relatedburnout.Thefollowingprovidesquotestakenfromrespondentsinthespecialtieswiththehighestcombinedwork-relatedandpersonalburnoutscores(seeFigure16)aswellasSouthernDHBwhichhadthehighestwork-relatedandpersonalburnoutscoresfortheplacesofworkanalysis.

WWW.ASMS.ORG.NZ HEALTH DIALOGUE 25
SPECIALTY QUALITATIVE COMMENTSRadiationOncologists
IncreasedfrustrationcausedbygapbetweencareIwouldliketoprovidetopatientsandthecareIamabletoprovideduetodepartmentalandDHBresourceconstraints.Insufficienttimetospendwithindividualpatients/whanauduetolackofFTEandhavingtoseetoomanypatientsperSMO.Newideaswhichcouldbehelpfularenotdevelopedbecauseofpossiblefundingramifications.
Weareunderstaffed.Thisdoesnotmeanpeopledonotgetleave,butitdoesplaceaburdenonthoseremaining.Iamsicktoday-insteadoftakingthedayoff,Iwillbeworkingthismorning,doingemailsattendingaclinicalmeetingviazoom,andmyclinicwillbeconvertedtophone.ProbablyasIhavehadleaveoverthelastwhileandupcoming,Ifeelless able to be sick.
MymainworkrelatedstressisthatIamtheoreticallyparttimeandworkmuchmorethanthehoursIampaidtowork.
Theworkiswonderful-Ilovecaringforthepatientsbutitisrelentlessandimpossibletoactuallyachievewithinthecurrentstaffingclimate,sowearealwaysgivingbeyondourselvestotryandmeettargetsetc.
EmergencyMedicine specialists
Admintimeneverends.Constantlybeingaskedtorespondtoemailsisabigpartoffatigue.
Workpressurehasincreased.Covid-19hashadaninsidiouseffectofgenerallyincreasingmanyworkplacestressors.Accessblockhasbecomeextremelydifficulttomanageinthefaceofpoorphysicalresourceandinadequatesystemwideplanning.
Southern Frustrationiswithmanagement.Growingdividebetweenmanagementandthoseatthecoal face.
Frustrationsareoftenaboutthesystem,e.g.operatinglistsinsufficientfortheservice,managersconstantlywantingtochangeprocessesthatareworking,inadequatephysicalspacetoworkin,lackofgoodequipment.ExpectationthatwewilldoextraworktocatchuponCOVID-19delayswithoutaclearideaofwhenwewillhaveachievedthetarget.Offeringoutsiderslocumratesbutnotwantingtobegeneroustocurrentstaffdoingextra.
MycolleaguesandIoftenworkwelloverthepaidnumberofhourstogetthejobdoneforourpatients.
TABLE 8: QUALITATIVE COMMENTS BY SPECIALTY AND DHB

26 HEALTH DIALOGUE APRIL2021
DiscussionThefindingsfromthisresearchprovideanupdatednationwideperspectiveonthedegreeofburnoutexperiencedbyseniordoctorsanddentistsworkingintheNewZealandhealthsystem.TheresearchsuggeststhatburnoutcontinuestobewidespreadamongsttheseniormedicalanddentalworkforceinNewZealandwithlittlechangeinthefiveyearssincethefirststudy.Thehighscoresforwork-relatedburnoutsuggestthattheimpactofwork,andparticularlythestressandexhaustionassociatedwithwork,continuetobeadrivingfactorforburnoutinthisprofessionalgroup.Therelativelylowincidenceofpatient-relatedburnoutsuggeststhatforthemajoritytheirfeelingsofexhaustionarenotdrivenbytheirinteractionswithpatients.Onthecontrarymanyreferencedtheircontactwithpatientsasbeingasourceofpleasureandfulfilment.
TheCBIcontinuestobeausefultoolforunderstandingwhichfactorsindividualsmostclearlyassociateasdrivingtheirfatigueandexhaustion.Inthisregard,thethemesnotedinthequalitativecommentsareparticularlyillustrativeforprovidingdetailastowhatindividualsperceiveasstressfulelementsoftheirlivesatthetimeofthesurvey.NotableinthesurveythisyearwerereferencestotheimpactofCOVID-19aswellasfindingsregardingtheimpactofdependantsanddegreeofburnout.Theseissuesarediscussedingreaterdetailbelow.
Thecorrelationanalyseswereconsistentwiththefindingsinthe2015survey;burnoutcontinuestobestronglyassociatedwithworseningself-ratedhealthstatus,youngerageandbeingfemale.Duetothecross-sectionalnatureofthesurvey,however,directionalcausalitycannotbeinferred.
Inthefollowingsections,matterswiththetimingandresponseratestothesurveyarediscussedasarepointspertainingtothe2015researchandcorefindingsregardinggender,age,anddependants.
The high scores for work-related burnout suggest that the impact of work, and particularly the stress and exhaustion associated with work, continue to be a driving factor for burnout in this professional group.
Timing of surveyThesurveywasdistributedintheAugustof2020,threemonthsafterthenationwidelockdownendedandNewZealandmovedtoAlertLevel2.Thetimingofthesurveywasdeliberateasitwasdecidednottodistributethesurveytoosoonafterthelockdownperiodended.Formanyspecialistslockdown had been an intensely stressful and uncertainperiod.Somequalitativecomments,however,referencedthattheirexperiencesofCOVID-19lockdownhadresultedinincreasedworkloadpressures,particularlyforthosewithworkthatwascancelledordelayedduringthatperiod.Forexample,onerespondentnoted:“It’sabitofatoughtimetoanswerthesequestions,theoverhangofCOVIDworkhastakenitstoll.IthinkI’mstillrecoveringfromthat!”.Anothernoted:“ThecurrentCOVID-19responsehasaccentuatedalotoftheissuesthathavebeenidentifiedinthissurvey”.ItispossibletheimpactofCOVID-19exacerbatedtheproblemofburnout.Again,itisnotpossibletointerrogatethisfullyduetothenatureofthesurveydesign.
Responder biasTheresponserateofthesurveywasreasonablegiventhemodeofdelivery(electronicdistribution)andwasconsistentwiththeresponseratesinprevioussurveysoftheASMSmembership.Therepresentativenessofthesurveyrespondentsisamootpoint.ResearchpublishedbySimonetti,Clintonetal.(2020)suggestthatdespitemanyburnoutsurveysofmedicalprofessionals

WWW.ASMS.ORG.NZ HEALTH DIALOGUE 27
experiencinglowresponserates,non-responderbiasmayslightlyfavourthoseexperiencingburnout.Intheirresearch,burnoutprevalencewasfoundtobe3-4%higherafteradjustingfornon-response(p3).Giventhathighworkloadsandlackoftimearekeycontributingfactorsforburnout,itispossiblethatnon-responderbiasmayresultinanunderestimationoftrueburnoutprevalence.Forexample,commentsonearlypresentationsofthesefindingsnotedthelowestimateofburnoutprevalenceforspecialistsworkinginpublichealthmedicine,particularlygiventheimpactofCOVID-19onthesemedicalspecialists.Itispossiblethatnon-responderbiasmayaffectthosewhowereexhaustedoroverworkedintheimmediateaftermathoftheCOVID-19outbreakwhomightnothavehadthecapacitytoanswerthesurveyrequest.Giventhecross-sectionalnatureofthedata,however,itisnotpossibletointerrogatethisfurther.Nevertheless,theclosecongruencebetweenthe2015and2020resultssuggeststhe50%burnoutprevalenceisareasonablyreliableestimate.
Factors associated with burnoutBurnoutscoresincreasedconcurrentlywithmorehoursworkedeachweek,atrendconsistentwiththe2015findings,aswellasotherrecentstudies(Ng,Chinetal.2020).Thequalitativecommentsfurthersuggestedthatissuessuchaslonghoursofwork,shiftworkandlackofrecoverytimeareperceivedassignificantfactorsforindividualrespondent’slevelsoffatigueandexhaustion.RecentresearchbyTrockel,Menonetal.(2020),foundacloseassociationbetweenburnoutandsleepdeprivation.Theirstudyfoundsleepdeprivationreducedcognitiveperformanceaswellasnegativelyaffectingmoodleadingtoagreaterpropensityforemotionalexhaustion.They.recommendcloserattentiontotheimpactofsleepdeprivationanditsrelationshiptoburnoutandsuggesttighterregulationonhoursofworkasasignificantfactorinreducingburnoutprevalence.Thecorrelationbetweenscoringasburnt-outandfailingtohavea24-hourbreakfreeofscheduledworkandworkingmorethan14consecutivehourssuggeststhatprotectingrestandrecovery
timeislikelytohaveasignificantpositiveeffectonburnoutpropensityintheNewZealandseniormedicalworkforce.
Totalhoursofprivateworkwerelowinthisstudy;overhalfofallrespondents(54%)hadworkednoprivatehours.Theslightnegativecorrelationbetweenhoursofprivateworkandburnoutwasconsistentwiththe2015studyandappearstosuggestworkinginprivatemaybeprotectiveagainstburnout.ThisfindingwasconsistentwithotherresearchincludingastudyintoNewZealandradiationoncologistsin2015(Leung,Riosecoetal.2015)andmorerecentresearchbyLiuandCheng(2018).
The qualitative comments further suggested that issues such as long hours of work, shift work and lack of recovery time are perceived as significant factors for individual respondent’s levels of fatigue and exhaustion.
Gender and burnoutVeryfewsurveyrespondentsidentifiedasgender-diverse(n=4);asaconsequenceoflownumberstheir burnout scores were not included in the analysis.Abriefassessmentfoundtheirscoreswereveryclosetotheoverallscoresforwomensurveyed.Ofnoteweretheproportionatelyhigherburnoutscoresexperiencedby52individualswhowishednottodisclosetheirgenderidentity.Thismaybeduetofearofidentification.Theburnoutscoresforthisgroupwereapproximately65%forwork-relatedburnoutand64%forpersonalburnout. These scores are of concern.
Consistentwiththe2015studyandotherresearch,thissurveyfoundwomencontinuetohavesignificantlyhigherburnoutscoresthantheirmalecounterparts(Obregon,Luoetal.2020).Gyorffy,Dweiketal.(2016),forexample,foundfemaledoctorshadsignificantlyworseindicatorsofmentalhealththanotherprofessionalwomen.Theirresearchalsofoundcorrelationsbetween

28 HEALTH DIALOGUE APRIL2021
workloadandfrequencyofwork-relatedstressfulsituationswithmanyexperiencingsleepdisordersandadecreasedsenseofpersonalaccomplishment(akeydimensionofburnout).Otherresearchfocusesonthewiderimpactofgender-baseddiscriminationonwomeninmedicineandsuggestsassociationswithburnout(Chesak,Cutshalletal.2020).ThesignificanceofgenderedexpectationsasanadditionalburdencarriedbywomeninmedicineisalsoemphasisedinresearchbyLinzerandHarwood(2018).Otherrecentresearchfoundexperienceofgender-baseddiscriminationtobeakeypredictorofwomenexperiencingburnout(Wang,Taniousetal.2020).Despitegrowingacknowledgementoftheexistenceandsignificanceofgenderdiscrimination,thepersistenceofhighburnoutscoresforwomeninthisstudysuggestfurtherattentionisrequired.Furtherdiscussionregardingtheinterfacebetweengender,dependantsandburnoutisbelow.
Age and burnoutIncontrasttothepriorresearchwhereburnoutscoresofrespondentspeakedintheir30s,thehighestprevalenceofburnoutinthiscurrentstudywasforbothmenandwomenintheir40s.Whileinitiallyitwasthoughtperhapstherewasacohorteffect(burnt-outrespondentsaging),therewasnegligibledifferenceinburnoutscoresforbothmaleandfemalerespondentsintheir40swhencomparingthe2015and2020studies.
Thischangeinburnoutscorebyagecohortisnotablebutgiventhelimitationsofthestudydesign,itisnotpossibletointerrogatefurther.Alongitudinalstudyexaminingthechangesinworkexperiencesandlevelsofburnoutofaconsistentcohortwouldbeausefulcontributiontothisresearchspace.Longitudinalresearchwouldhavetheadditionalbenefitofassessingtheimpactofsolutionsimplementedtoaddressburnout,aswellasenablingresearchtounderstandmorefullyhowexperiencesofburnoutchangeovertimeandwithwhatconsequences(West,Dyrbyeetal.2018).Thesignificantdecreaseofburnoutforwomenrespondentsintheir30sisalsoanotableand
pleasingimprovement;again,itisnotpossibletounderstandthefactorsthatmayhavecontributedtothisdecreaseinburnout,butitisapositivechange.
The significant decrease of burnout for women respondents in their 30s is also a notable and pleasing improvement; again, it is not possible to understand the factors that may have contributed to this decrease in burnout, but it is a positive change.
Impact of dependants Thissurveyimprovedupontheoriginal2015methodologybyexamininghowburnoutrelatedtonumbersofdependants.Forwomen,theirratesofburnoutwerearoundthesameirrespectiveofwhethertheyhaddependants.Formalerespondents,however,therewasasignificantassociationbetweenhavingdependantsandexperiencinghigherratesofburnout.Thistrendisnotconsistentwithotherstudies.ForexampledatapublishedbyElmore,Jeffeetal.(2016)suggestthatmenwhoareeitherpartneredorhavechildrenwillexperiencelowerratesofemotionalexhaustion(akeyfacetofburnoutaspertheMBI)thantheirfemalecounterpartsinthesamesituation.
Analysisofthequalitativedataforthoserespondentswithdependantsfoundanumberofcommentsleftbymalerespondentsnotingthattheirexhaustionwasaconsequenceofhavingsmallchildren.Forexample,“muchoftheexhaustionisduetohavingyourchildren”;“myanswersareaffectedbyhavingayoungfamily”;“Notsurethisiswork-related–Ihaveatoddlertoo”.Thiswasanunexpectedfindingintheresearchandmaysuggestthatmen’sexperiencesofwork-lifeconflictareasignificantcontributortotheirfeelingsofexhaustion.
Otherresearchpostulateswork-lifeconflictasbeingakeysourceofstressandexhaustionforwomeninmedicine,oftenbutnotalwaysduetothepressuresandexpectationsassociatedwithhavingchildren.Thenegligibledifferencesin
WWW.ASMS.ORG.NZ HEALTH DIALOGUE 29
burnoutratesforwomenwithdependantsversusthosewithoutinthisstudysuggeststhatfactorsotherthandependantsmaybecontributingtotheirlevelsofburnout(McMurray,Linzeretal.2000).AsexploredinASMS’HealthDialogue,‘Makingupforbeingfemale’(ASMS2019a)theconsistentlyhigherratesofburnoutexperiencedbywomenmayreflecttheimpactofgenderedbehaviouralexpectationsandthestressorsassociatedwithbeingawomaninmedicineratherthanwork-lifeconflictperse.
Burnout and medical specialtyThepatternofcertainmedicalspecialtieshavingconsistentlyhigherratesofburnoutisworryingandcauseforconcern.ThespikeinburnoutratesforthoserespondentsworkinginRadiationOncologyandRespiratoryMedicineisconcerning;duetothelowernumbersofrespondentsinthe2015surveyitisnotpossibletocheckwhetherthechangeisstatisticallysignificant.Itishoweverofconcern.TheconsistentlyhighratesofburnoutfordoctorsworkinginEmergencyMedicinesuggestslittlehasimprovedforthiscohortofdoctors.Thehighequalscoresforwork-relatedandpersonalburnoutfordoctorsinthesethreespecialtiessuggestthatworkingconditionsarethemainfactorstowhichrespondentsattributetheirfeelingsofexhaustionandfatigue.ThescoresforEmergencyMedicinespecialistsinthisstudyarehigherthanthosefoundinthestudybyKumar,Pioetal.(2019)whichfoundpersonalburnoutratesof42%(cf56%)andwork-relatedburnoutratesof37%(cf56%)fordoctorsworkinginasingleemergencydepartment(n=40cfn=167).
Knownfactorsthatleadtoburnoutincludelonghoursofwork,fatigue,andlackofcontrol.Thecommentsleftbydoctorsinemergencymedicinesettingsemphasisethewearingeffectsofpoorresourcing,growingadministrativeloadsandincreasingpatientnumbersandacuity.RecentUSresearchbyHarry,Sinskyetal.(2021)founddoctorsworkinginEmergencyMedicinehadthehighestscoresforphysiciantaskloads(ameasureofcognitivetaskloading)ofthedoctorssurveyed;theyfurtherfoundacloserelationship
betweenthedegreeofphysiciantaskloadandburnout.Theirresearchconcludesthatreducingthecognitivetaskloadingofdoctorsislikelytopaydividendsinreducingthepropensityfordoctorstoexperienceburnout,aswellasimprovingtheabilityofdoctorstoperformtheirjobwell.OtherstudiessummarizedbyZhang,Muetal.(2020)foundthatEmergencyMedicinedoctorswerelikelytobemoresusceptibletoburnoutlikelyduetotheparticularlystressfulnatureofEmergencyMedicine. These consistent trends for burnout inEmergencyMedicinespecialistshighlighttheimmediateneedtoattendtotheworkingconditionsofthisparticulargroupoftheASMSmembership.
The consistently high rates of burnout for doctors working in Emergency Medicine suggests little has improved for this cohort of doctors.

30 HEALTH DIALOGUE APRIL2021
Whiledoctorsaremorelikelytosufferfromburnoutthanotherprofessionalgroups(Shanafelt,Gorringeetal.2015),sufferingfromburnouthascriticalconsequencesandshouldnotbetakenasaninevitableconsequenceofchoosingtoworkinthemedicalprofession.Burnouthassignificantnegativeconsequencesforindividualdoctorsexperiencingthesyndrome(Menon,Shanafeltetal.2020),theircolleagues(Shanafelt,Makowskietal.2020),andthequalityofcaretheirpatientsreceive(Chung,Dillonetal.2020).Asnumerousstudiescontinuetosubstantiate,havingahighproportionofdoctorssufferingfromburnouthassignificantnegativeconsequencesforthequality,sustainability,andlongevityofamedicalworkforce(Willard-Grace,Knoxetal.2019,NiconchukandHyman2020).
ThefindingsfromthisresearchsuggestthatlittlehaschangedintermsoftheratesofburnoutexperiencedbyseniordoctorsanddentistsworkingintheNewZealandpublichealthsystem.ThenegligiblechangeinallthreespheresoftheCBIsuggestthatburnoutcontinuestobeasignificantandpressingproblem.
Consistentwiththechangeindefinitionofburnoutfromindividualisedfailingtoanoccupationalsyndrome,solutionsmustreflectthissignificantshiftinfocus.Fixingburnoutshouldnotbeseenastheresponsibilityofindividualsalone.Theproblemandfindingsolutionstomitigateburnoutinmedicineisasharedresponsibilitybetweenemployersandleadersaswellasindividualswhomaybeatrisk.Furthermore,failuretoenactorganisationallevelsolutionscanhavenegativeconsequences;researchhasfoundthatemphasisingindividualresponsibilityforburnoutcanunintentionallyincreasefeelingsofstresswhichcanleadtohigherratesofburnout(Eden,Jabbarpouretal.2020).
Thefindingsfromthisresearchcontinuetoemphasiseburnoutasarisingfromlongworkinghours,failuretohaveadequaterestbreaks,
medicalspecialtieswithgrowingpatientdemandandperpetualstaffingshortfalls.Thesethemesareechoedinthequalitativecommentswithclearemphasisonthesignificanceofhighworkloads,lackofadministrativesupport,lackofcontroland/orautonomyinworkplaces,poorworkplacecultureandissueswithleadershipormanagerialism(West,Dyrbyeetal.2018).
AssummarisedbyWest,Dyrbyeetal.(2018),ensuringfairlydistributedworkloads,roles,andhourscanassistwithmitigatingtheriskofburnoutascanincreasingnumbersofadministrativestafftorelievetheburdenplacedondoctors.Activelyrespectinghomeresponsibilitieswhenworkandmeetingsarescheduledcanpaydividendsinreducingwork-lifeconflictissues.Otherorganisationallevelstrategieslikelytohaveapositiveimpactonreducingratesofburnoutincludejobsizingallexpectedtaskstoexpectedhoursofwork(i.e.removingtheneedtotakeworkhome),supportingflexibleworkingschedulesincludingnormalisingpart-timeworkinmedicine,ensuringactiveengagementofdoctorsinallmanagerialdecision-makingprocessesthatimpactworkexpectationsandstructure,andhavingshareddecision-making(seep522forafulllist).
ASMSisoftheviewthatburnoutstrategiesneedtobebasedonformalrecognitionthatitistheemployer’sresponsibilitytoprovideaworkplacethatisbothphysicallyandpsychologicallysafe(Kendrick,Kendricketal.2020).Further,thosetaskedwithensuringthewellbeingandsustainabilityoftheseniormedicalanddentalworkforcemustlookatstrategiesandapproachestopreventburnoutbeforeitresultsinseriousconsequences,includingpotentialstaffattrition,doctorsuicide,patientcomplaints,andmedicalerror.Researchevidencesuggeststhatimplementingchangestoworkingpatternstoenableadequatesleep,restandrecoverytimewouldbeasensibleplacetostart(Ng,Chinetal.2020).Assummarisedinarecent
Conclusions
WWW.ASMS.ORG.NZ HEALTH DIALOGUE 31
Lancetarticle(Marchalik2019)thewellbeingofmedicalanddentalworkforcesmustbeseenasanorganisationalprioritywhere“likeoperatingbudgetsandexpansionplans,itmustbecomeastandingagendaitemattheleadershiptable”(p869).ParticularlyinlightoftherecentCOVID-19pandemic,thestressorsandpressuresthatmedicalprofessionalscontinuetofaceemphasisethepressingneedtoputwellbeingfirmlyontheagenda(RimmerandChatfield2020).
ASMS is of the view that burnout strategies need to be based on formal recognition that it is the employer’s responsibility to provide a workplace that is both physically and psychologically safe.
What needs to change: • Normalisationoflongworkinghoursthat
extendbeyondcontractedjob-sizing.
• Outdatedandinefficienttechnology,includingITsystemsandcumbersomeadministrativeprotocols.
• Lackofadministrativesupportandtheexpectationthatadminwillbecompletedoutsideofworkinghours.
• Poorconnectionsbetweenmanagementandclinicians,particularlyintermsofwork-placecultureandlackofunderstandingfrommanagementoftheday-to-dayrealitiesofthecoalface.
• Insufficientresourcestoenableclinicianstodothe work.
What we are calling for: • Formalrecognitionthatitistheemployer’s
responsibilitytoprovideaworkplacethatisbothphysicallyandpsychologicallysafe.
• Formalisedregularassessmentofburnoutratesusingconsistentandvalidatedtools.Inaddition,othermentalwellbeingsurveysshouldbeundertakenregularlyandreportedinanon-punitivemanner.
• Adequateresourcingofdepartmentsintermsofstaff,technology,andprovisionofappropriatelevelsofadministrativesupport.ThisshouldincludeworkwithunionsandCollegestoagreesafestaffinglevelsforeachserviceandrecognisingthatthesewillvarydependingonhospitalsize,location,andotherstaffing(Residentdoctors,allied,andnursing).
• Staffinglevelsandworkinghoursdatashouldbecollectedandreviewedtoestablishandmaintainsafesustainableworkforallclinicians.Thisdatashouldbepubliclyavailable.
• Regularstaff-focussedservicereviewsto accurately assess social factors and psychologicalstressorsaswellasphysicalworkplacefactorswhichpresentspecificstressfactorsfordoctorsandtheirteams.Placinganemphasisonthecreationofcongenialworkplacesandcivilbehaviourtominimisestaffexperiencesofstressatwork.
• Formalisedstrategiestopromoteprofessionalwellbeingincludingtheprovisionofconfidentialeasilyaccessibleprofessionalsupervisionandcounselling.Establishmentandnormalisationofano-blamecultureforreportingandhoursof(over)workandaspeakingoutcultureonmattersofstaffandpatientsafety,asperexistingMECAclauses.
• Ashiftinfocusawayfromfinancialprioritiestopeopleandattachingadollarvaluetowellbeing(decreaseinpresenteeism,decreaseinturnoverrates,bettermedicaloutcomes,bettercollegialityindepartmentsetc).
• AddingindicatorsofstaffwellbeingasstandingitemsinhospitalauditsandreportingtoBoardsandhavingMOHtargetsforDHBsonthesestaffwellbeingmeasures.
• NormalisingthepracticeofDHBleaders(Boardandexecutivestaff)speakingupaboutresourceconstraints,limitstocare,waitinglists.Thiswouldbedifferentfromthecurrentcultureofmakingdoandpretendingthereisenoughhealthresourceifwealljust“worksmarter”,whichisdamagingtostaffandcommunities.

32 HEALTH DIALOGUE APRIL2021
Appendix 1SPECIALTY GROUPINGPlastic&reconstructivesurgery Surgery
Urology Surgery
Paediatricsurgery Surgery
Neurosurgery Surgery
Vascularsurgery Surgery
Cardiothoracicsurgery Surgery
Oral&MaxillofacialSurgery Surgery
Haematology Internal Medicine
PalliativeMedicine Internal Medicine
InfectiousDiseasesMedicine Internal Medicine
Dermatology Internal Medicine
RehabilitationMedicine Internal Medicine
Sexual Health Medicine Internal Medicine
ClinicalGenetics Internal Medicine
Pain Medicine Internal Medicine
OccupationalMedicine Internal Medicine
Musculoskeletal Medicine Internal Medicine
FamilyPlanning&ReproductiveHealth GeneralPractice
Accident&MedicalPractice EmergencyMedicine
MedicalAdministration Miscellaneous
ReferencesAMA(2005).NationalCodeofPractice-HoursofWork,ShiftworkandRosteringforHospitalDoctors.Kingston,Australia,TheAustralianMedicalAssociation
ASMS(2019a).‘Makingupforbeingfemale’:Work-lifebalance,medicaltimeandgendernormsforwomenintheNewZealandseniormedicalworkforce.HealthDialogue.Wellington,NewZealand,AssociationofSalariedMedicalSpecialists.16.
ASMS(2019b).ForecastingNewZealand’sFutureMedicalSpecialistWorkforceNeeds.Research Brief. Wellington,AssociationofSalariedMedicalSpecialists.
Bianchi,R.,C.Boffy,C.Hingray,D.TruchotandE.Laurent(2013).“Comparativesymptomatologyofburnoutanddepression.”JHealthPsychol 18(6):782-787.
Caesar,B.,A.Barakat,C.BernardandD.Butler(2020).“EvaluationofphysicianburnoutatamajortraumacentreusingtheCopenhagenburnoutinventory:cross-sectionalobservationalstudy.”IrishJournalof MedicalScience(1971-) 189(4):1451-1456.

WWW.ASMS.ORG.NZ HEALTH DIALOGUE 33
Chadwick,A.J.andR.Baruah(2020).“Genderdisparityandimplicitgenderbiasamongstdoctorsinintensivecaremedicine:A‘disease’weneedtorecogniseandtreat.”JIntensiveCareSoc 21(1):12-17.
Chambers,C.N.,C.M.Frampton,M.BarclayandM.McKee(2016).“BurnoutprevalenceinNewZealand’spublichospitalseniormedicalworkforce:across-sectionalmixedmethodsstudy.”BMJOpen 6(11):e013947.
Chesak,S.S.,S.Cutshall,A.Anderson,B.Pulos,S.MoeschlerandA.Bhagra(2020).“BurnoutAmongWomenPhysicians:aCalltoAction.”CurrentCardiologyReports 22(7):45.
Chung,S.,E.C.Dillon,A.E.Meehan,R.NordgrenandD.L.Frosch(2020).“TheRelationshipBetweenPrimaryCarePhysicianBurnoutandPatient-ReportedCareExperiences:aCross-sectionalStudy.”Journalof General Internal Medicine 35(8):2357-2364.
Danhauer,S.C.,K.FilesandJ.A.Freischlag(2020).“BroadeningtheDiscussiononPhysicianBurnout.”JAMASurgery 155(11):1049-1049.
Eden,A.R.,Y.Jabbarpour,Z.J.Morgan,E.WilkinsonandL.E.Peterson(2020).“BurnoutAmongFamilyPhysiciansbyGenderandAge.”JAmBoardFamMed 33(3):355-356.
Elmore,L.C.,D.B.Jeffe,L.Jin,M.M.AwadandI.R.Turnbull(2016).“NationalSurveyofBurnoutamongUSGeneralSurgeryResidents.”JAmCollSurg 223(3):440-451.
Gyorffy,Z.,D.DweikandE.Girasek(2016).“Workload,mentalhealthandburnoutindicatorsamongfemalephysicians.”HumResourHealth 14:12.
Harry,E.,C.Sinsky,L.N.Dyrbye,M.S.Makowski,M.Trockel,M.Tutty,L.E.Carlasare,C.P.WestandT.D.Shanafelt(2021).“PhysicianTaskLoadandtheRiskofBurnoutAmongUSPhysiciansinaNationalSurvey.”TheJointCommissionJournalonQualityandPatientSafety 47(2):76-85.
Hewitt,D.B.,R.J.Ellis,Y.-Y.Hu,E.O.Cheung,J.T.Moskowitz,G.AgarwalandK.Y.Bilimoria(2020).“EvaluatingtheAssociationofMultipleBurnoutDefinitionsandThresholdsWithPrevalenceandOutcomes.”JAMASurgery 155(11):1043-1049.
Johnson,H.M.,W.Irish,P.D.Strassle,S.T.Mahoney,A.T.Schroen,A.P.Josef,J.A.Freischlag,J.E.TuttleandM.R.Brownstein(2020).“AssociationsBetweenCareerSatisfaction,PersonalLifeFactors,andWork-LifeIntegrationPracticesAmongUSSurgeonsbyGender.”JAMASurgery 155(8):742-750.
Kane,L.(2019).MedscapeNationalPhysicianBurnout,Depression&SuicideReport2019.M.B.o.Medicine.
Kendrick,M.,K.Kendrick,P.Morton,N.F.TaylorandS.G.Leggat(2020).“HospitalStaffReportItIsNotBurnout,butaNormalStressReactiontoanUncongenialWorkEnvironment:FindingsfromaQualitativeStudy.”IntJEnvironResPublicHealth 17(11).
Kristensen,T.S.,H.Hannerz,A.HoghandV.Borg(2005).“TheCopenhagenPsychosocialQuestionnaire--atoolfortheassessmentandimprovementofthepsychosocialworkenvironment.”ScandJWorkEnviron Health 31(6):438-449.
Kumar,R.,F.Pio,J.Brewer,C.FramptonandM.Nicholls(2019).“WorkplacewellbeinginanurbanemergencydepartmentinAotearoaNewZealand.”EmergencyMedicineAustralasia 31(4):619-625.

34 HEALTH DIALOGUE APRIL2021
Lall,M.D.,T.J.Gaeta,A.S.Chung,E.Dehon,W.Malcolm,A.Ross,D.P.Way,L.WeichenthalandN.T.Himelfarb(2019).“AssessmentofPhysicianWell-being,PartOne:BurnoutandOtherNegativeStates.” TheWesternJournalofEmergencyMedicine 20(2):278-290.
Leung,J.,P.RiosecoandP.Munro(2015).“Stress,satisfactionandburnoutamongstAustralianand NewZealandradiationoncologists.”JournalofMedicalImagingandRadiationOncology 59(1):115-124.
Linzer,M.andE.Harwood(2018).“GenderedExpectations:DoTheyContributetoHighBurnoutAmongFemalePhysicians?”JournalofGeneralInternalMedicine 33(6):963-965.
Liu,H.-C.andY.Cheng(2018).“PsychosocialWorkHazards,Self-RatedHealthandBurnout:AComparisonStudyofPublicandPrivateSectorEmployees.”JournalofOccupationalandEnvironmentalMedicine 60(4).
Marchalik,D.(2019).“Physicianburnoutinthemodernera.”The Lancet 393(10174):868-869.
Maslach,C.andM.P.Leiter(2017).“Newinsightsintoburnoutandhealthcare:Strategiesforimprovingcivilityandalleviatingburnout.”Med Teach 39(2):160-163.
McMurray,J.E.,M.Linzer,T.R.Konrad,J.Douglas,R.ShugermanandK.Nelson(2000).“Theworklivesofwomenphysiciansresultsfromthephysicianworklifestudy.TheSGIMCareerSatisfactionStudyGroup.” JGenInternMed 15(6):372-380.
Menon,N.K.,T.D.Shanafelt,C.A.Sinsky,M.Linzer,L.Carlasare,K.J.S.Brady,M.J.StillmanandM.T.Trockel(2020).“AssociationofPhysicianBurnoutWithSuicidalIdeationandMedicalErrors.”JAMAnetworkopen 3(12):e2028780.
Messias,E.,M.M.Gathright,E.S.Freeman,V.Flynn,T.Atkinson,C.R.Thrush,J.A.ClardyandP.Thapa(2019).“Differencesinburnoutprevalencebetweenclinicalprofessionalsandbiomedicalscientistsinanacademicmedicalcentre:across-sectionalsurvey.”BMJOpen 9(2):e023506.
Ng,A.P.P.,W.Y.Chin,E.Y.F.Wan,J.ChenandC.S.Lau(2020).“PrevalenceandseverityofburnoutinHongKongdoctorsupto20yearspost-graduation:Across-sectionalstudy.”BMJOpen 10(10).
Niconchuk,J.A.andS.A.Hyman(2020).“PhysicianBurnout:AchievingWellnessforProvidersandPatients.”CurrentAnesthesiologyReports 10(3):227-232.
Nuss,P.,C.Tessier,M.Masson,P.Fossati,R.Gaillard,N.LapidusandD.Gourion(2020).“FactorsAssociatedWithaHigherScoreofBurnoutinaPopulationof860FrenchPsychiatrists.”Front Psychiatry 11:371.
Obregon,M.,J.Luo,J.Shelton,T.BlevinsandM.MacDowell(2020).“AssessmentofburnoutinmedicalstudentsusingtheMaslachBurnoutInventory-StudentSurvey:across-sectionaldataanalysis.” BMCMedicalEducation 20(1):376.
Paredes,A.Z.andA.Cochran(2020).“CareerSatisfactionandBurnoutinSurgery—TheComplexInterplayofSelf-care,WorkLife,andHomeLife.”JAMASurgery 155(8):750-751.
Pei,P.,G.Lin,G.Li,Y.ZhuandX.Xi(2020).“Theassociationbetweendoctors’presenteeismandjobburnout:across-sectionalsurveystudyinChina.”BMCHealthServRes 20(1):715.
Ran,L.,X.Chen,S.Peng,F.Zheng,X.TanandR.Duan(2020).“JobburnoutandturnoverintentionamongChineseprimaryhealthcarestaff:themediatingeffectofsatisfaction.”BMJOpen 10(10):e036702.
Rimmer,A.andC.Chatfield(2020).“Whatorganisationsaroundtheworldaredoingtohelpimprovedoctors’wellbeing.”BMJ 369:m1541.

WWW.ASMS.ORG.NZ HEALTH DIALOGUE 35
Shanafelt,T.D.,G.Gorringe,R.Menaker,K.A.Storz,D.Reeves,S.J.Buskirk,J.A.SloanandS.J.Swensen(2015).“Impactoforganizationalleadershiponphysicianburnoutandsatisfaction.”MayoClinProc 90(4):432-440.
Shanafelt,T.D.,M.S.Makowski,H.Wang,B.Bohman,M.Leonard,R.A.Harrington,L.MinorandM.Trockel(2020).“AssociationofBurnout,ProfessionalFulfillment,andSelf-carePracticesofPhysicianLeadersWithTheirIndependantlyRatedLeadershipEffectiveness.”JAMANetworkOpen 3(6):e207961-e207961.
Simonetti,J.A.,W.L.Clinton,L.Taylor,A.Mori,S.D.Fihn,C.D.HelfrichandK.Nelson(2020).“Theimpactofsurveynonresponseonestimatesofhealthcareemployeeburnout.”Healthcare 8(3):100451.
Trockel,M.T.,N.K.Menon,S.G.Rowe,M.T.Stewart,R.Smith,M.Lu,P.K.Kim,M.A.Quinn,E.Lawrence,D.Marchalik,H.Farley,P.Normand,M.Felder,J.C.DudleyandT.D.Shanafelt(2020).“AssessmentofPhysicianSleepandWellness,Burnout,andClinicallySignificantMedicalErrors.”JAMANetworkOpen 3(12):e2028111-e2028111.
Wang,L.J.,A.Tanious,C.Go,D.M.Coleman,S.K.McKinley,M.J.Eagleton,W.D.ClouseandM.F.Conrad(2020).“Gender-baseddiscriminationisprevalentintheintegratedvasculartraineeexperienceandservesasapredictorofburnout.”JVascSurg 71(1):220-227.
West,C.P.,L.N.DyrbyeandT.D.Shanafelt(2018).“Physicianburnout:contributors,consequencesandsolutions.”JInternMed 283(6):516-529.
WHO(2019).Burn-outan“occupationalphenomenon”:InternationalClassificationofDiseases.
Willard-Grace,R.,M.Knox,B.Huang,H.Hammer,C.KivlahanandK.Grumbach(2019).“BurnoutandHealthCareWorkforceTurnover.”TheAnnalsofFamilyMedicine 17(1):36-41.
Zhang,Q.,M.C.Mu,Y.He,Z.L.CaiandZ.C.Li(2020).“Burnoutinemergencymedicinephysicians:Ameta-analysisandsystematicreview.”Medicine(Baltimore) 99(32):e21462.