
Bundled Payment for Care Improvement Initiative (BPCI)
10
7/8/2017 1 Bundled Payment for Care Improvement (BPCI) Overview Shawn Matheson MBA, LNHA, FACHCA Market Manager Idaho Health Care Association Annual Convention Boise, ID July 13, 2017 Retrospective Bundles Retrospective Reconciliation Surgeon Hospital SNF Home Health FFS Billing as Usual 3 PAC OPPORTUNITY & RISK FROM HOSPITAL EYES Inpatient Rehab Facility, Long-term Acute Care, Skilled Nursing Facility Home Health Surgeon, Hospital
Transcript of Bundled Payment for Care Improvement Initiative (BPCI)

7/8/2017
1
Bundled Payment for Care Improvement (BPCI)
Overview
Shawn Matheson
MBA, LNHA, FACHCA
Market Manager
Idaho Health Care Association
Annual Convention
Boise, ID
July 13, 2017
Retrospective Bundles
Retrospective
Reconciliation
SurgeonHospitalSNFHome Health
FFS Billing
as Usual
3
PAC OPPORTUNITY & RISK FROM HOSPITAL EYES
Inpatient Rehab Facility, Long-term Acute Care, Skilled Nursing Facility
Home Health
Surgeon,Hospital

7/8/2017
2
4
PAC OPPORTUNITY & RISK FROM HOSPITAL EYES
HospitalDischarge
90-DayBundle
Risk
Inpatient Rehab Facility, Long-term Acute Care, Skilled Nursing Facility
Home Health
Surgeon,Hospital
Hospitals are Increasingly Responsible for the
Financial & Quality Outcomes for a Patient’s Entire
Episode of Care
5
• Creates accountability for positiveoutcomes and efficiency
• Engages clinicians and drives a shift to coordinated, multidisciplinary care over the full Episode
• Promotes competition in an increasingly uncompetitive market
• Patients can choose the Provider that best fits their specific needs
• Providers with the greatest efficiency & best outcomes will grow, improving overall average outcomes and reducing average costs
• Providers with poor performance will need to either improve, or exit focus on areas where they can deliver clear value
Why Bundled Payments Work
OPPORTUNITY OVERVIEW | REMEDY OVERVIEW | 04.28.16
6
Remedy has created a comprehensive episode of care company with the largest footprint and broadest range of bundled payment capabilities: enabling Payers and Providers to succeed with bundled payments
Remedy
Partners
Hospitalists
ACH
SNFs
PGPs
Other
Convener Share By Competitor Remedy’s Bundled Payment Spend By Partner ($6.7B)
Remedy Partners Overview
66%
$6.7B$44 M
1%
$4,505M
67%
$1,515M
23%
$359M
5%
$263M
4%
OPPORTUNITY OVERVIEW | REMEDY OVERVIEW | 04.28.16

7/8/2017
3
7
-
10,000
20,000
30,000
40,000
50,000
60,000
70,000
2015Q1 2015Q2 2015Q3 2015Q4 2016Q1 2016Q2
65k
-
1
2
3
4
5
6
7
8
2015Q1 2015Q2 2015Q3 2015Q4 2016Q1 2016Q2
Remedy Spend Under Management
2015 Q1 – 2016 Q2
Remedy Episodes Under Management
2015 Q1 – 2016 Q2
Remedy Partners Overview
Episodes$ Billions
Spend & Episodes
OPPORTUNITY OVERVIEW | REMEDY OVERVIEW | 04.28.16
$6.7b
8
• Remedy’s role is to manage the bundled payment program for its Payer Partners including the development, organization, operationalization and ongoing management of the program
• Remedy supports its Partners with the technology, analytics, expertise, and process implementation to operationalize the program, along with technology and care protocols to efficiently manage the complex program
Remedy’s Role in Program Success
Program Design
& Administration
• Care coordination programs
• Contracts and protocols
• Compliance, Quality and Reconciliations
Software Tools
• Episode Connect
• Patient attribution, patient tracking
• Assessment, patient stratification and decision support
• Portals
Analytics
• Risk mitigation and actuarial support
• Predictive analytics
• Comprehensive reporting
Network Management,
Call Center
• SNF and HHA Performance Networks
• Post Acute Physician Network
• Care Innovation Center
BPO for Bundled Payments
OPPORTUNITY OVERVIEW | REMEDY OVERVIEW | 04.28.16
9
Full Bundle Administration
• Acute myocardial infarction
• Amputation
• Atherosclerosis
• Automatic implantable
cardiac defibrillator
• Back and neck except spinal fusion
• Cardiac arrhythmia
• Cardiac defibrillator
• Cardiac valve
• Cellulitis
• Cervical spinal fusion
• Chest pain
• Chronic obstructive
pulmonary disease
• Combined anterior posterior
spinal fusion
• Complex non-Cervical spinal fusion
• Congestive heart failure
• Coronary artery bypass graft surgery
• Diabetes
• Esophagitis, gastroenteritis
other digestive disorders
• Double joint replacement/
lower extremity
• Fractures femur and hip/pelvis
• Gastrointestinal hemorrhage
• Gastrointestinal obstruction
• Hip and femur procedures
except major joint
• Lower extremity and humerus
except hip, foot, femur
• Major bowel
• Major cardiovascular procedure
• Major joint replacement
of the lower extremity
• Major joint replacement
of upper extremity
• Medical non-infectious orthopedic
• Medical peripheral vascular disorders
• Nutritional and metabolic disorders
• Other knee procedures
• Other respiratory
• Other vascular surgery
• Pacemaker
• Pacemaker Device replacement
or revision
• Percutaneous coronary intervention
• Red blood cell disorders
• Removal of orthopedic devices
• Renal failure
• Revision of the hip or knee
• Sepsis
• Simple pneumonia and
respiratory infections
• Spinal fusion (non-Cervical)
• Stroke
• Syncope and collapse
• Transient ischemia
• Urinary tract infection
48 BPCI Bundles Representing 181 DRGs covering up to 50% of MLR
OPPORTUNITY OVERVIEW | REMEDY OVERVIEW | 04.28.16
7/8/2017
4
10
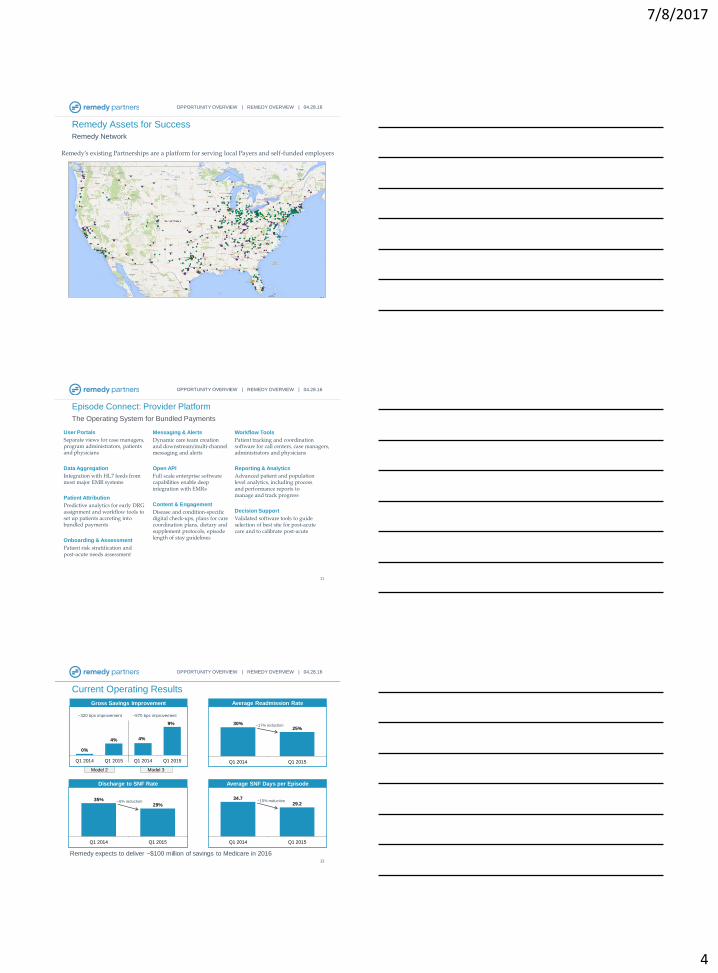
Remedy’s existing Partnerships are a platform for serving local Payers and self-funded employers
Remedy Assets for Success
Remedy Network
OPPORTUNITY OVERVIEW | REMEDY OVERVIEW | 04.28.16
11
Episode Connect: Provider Platform
The Operating System for Bundled Payments
User Portals
Separate views for case managers, program administrators, patients and physicians
Data Aggregation
Integration with HL7 feeds from most major EMR systems
Patient Attribution
Predictive analytics for early DRG assignment and workflow tools to set up patients accreting into bundled payments
Onboarding & Assessment
Patient risk stratification and post-acute needs assessment
Messaging & Alerts
Dynamic care team creationand downstream/multi-channel messaging and alerts
Open API
Full scale enterprise software capabilities enable deep integration with EMRs
Content & Engagement
Disease and condition-specific digital check-ups, plans for care coordination plans, dietary and supplement protocols, episode length of stay guidelines
Workflow Tools
Patient tracking and coordination software for call centers, case managers, administrators and physicians
Reporting & Analytics
Advanced patient and population level analytics, including process and performance reports to manage and track progress
Decision Support
Validated software tools to guide selection of best site for post-acute care and to calibrate post-acute
OPPORTUNITY OVERVIEW | REMEDY OVERVIEW | 04.28.16
12
Remedy expects to deliver ~$100 million of savings to Medicare in 2016
Current Operating Results
Gross Savings Improvement Average Readmission Rate
Discharge to SNF Rate Average SNF Days per Episode
35%29%
Q1 2014 Q1 2015
~6% reduction34.7
29.2
Q1 2014 Q1 2015
~15% reduction
30%25%
Q1 2014 Q1 2015
~17% reduction
~320 bps improvement ~570 bps improvement
0%
4% 4%
9%
Q1 2014 Q1 2015 Q1 2014 Q1 2015
Model 2 Model 3
OPPORTUNITY OVERVIEW | REMEDY OVERVIEW | 04.28.16
7/8/2017
5
13
Model 3 Opportunities for SNFs
1. Only 6% of SNFs in the country have put their revenue at risk
2. Model 3 SNFs have a strong incentive to achieve high-quality, low-
cost outcomes
3. Remedy’s partnership with 435 Model 3SNFs represents over 60%
of the entire BPCI Model 3 Program.
4. Helps with Model 2 Providers to see Model 3 Partner Commitment
5. Can retain savings compared to Adjusted Historical Rates
6. Advanced BPCI Forthcoming, narrow window to enroll
[email protected] | 801-856-8155
Shawn Matheson
Bundled Payment for Care Improvement Initiative (BPCI)
15
1
SAHS Director: Becky Swenson, MSN, MHA, RN, NEA-BC
7/8/2017
6
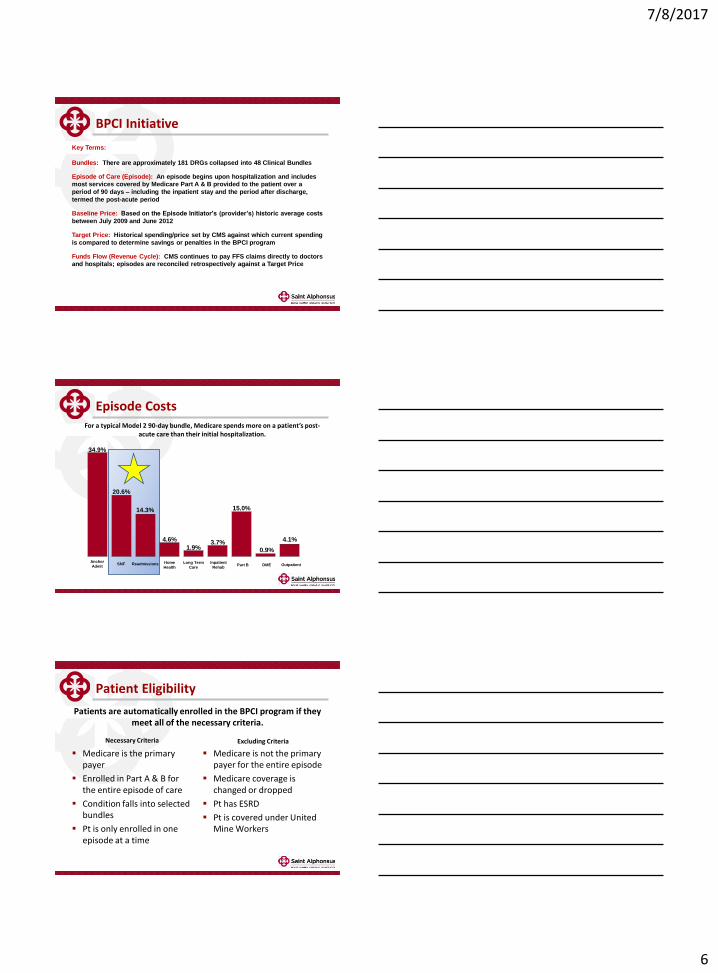
BPCI Initiative
Key Terms:
Bundles: There are approximately 181 DRGs collapsed into 48 Clinical Bundles
Episode of Care (Episode): An episode begins upon hospitalization and includes
most services covered by Medicare Part A & B provided to the patient over a
period of 90 days – including the inpatient stay and the period after discharge,
termed the post-acute period
Baseline Price: Based on the Episode Initiator's (provider’s) historic average costs
between July 2009 and June 2012
Target Price: Historical spending/price set by CMS against which current spending
is compared to determine savings or penalties in the BPCI program
Funds Flow (Revenue Cycle): CMS continues to pay FFS claims directly to doctors
and hospitals; episodes are reconciled retrospectively against a Target Price
Episode CostsFor a typical Model 2 90-day bundle, Medicare spends more on a patient’s post-
acute care than their initial hospitalization.
34.9%
20.6%
14.3%
Anchor
AdmitSNF Readmissions Home
Health
Long Term
Care
Inpatient
RehabPart B DME Outpatient
4.6%
1.9%3.7%
15.0%
0.9%
4.1%
Patient Eligibility
Patients are automatically enrolled in the BPCI program if they meet all of the necessary criteria.
Medicare is the primary payer
Enrolled in Part A & B for the entire episode of care
Condition falls into selected bundles
Pt is only enrolled in one episode at a time
Medicare is not the primary payer for the entire episode
Medicare coverage is changed or dropped
Pt has ESRD
Pt is covered under United Mine Workers
Necessary Criteria Excluding Criteria
7/8/2017
7
Key Levers of Success
Strong Patient Navigators
Appropriate Next Site of Care Decisions
Optimal Lengths of Stay at Next Site of Care
Strong Preferred Provider Networks
Early Intervention
Minimal Readmissions
What We Ask of Our Partners
Manage Length of Stay (Meet/Exceed ELOS)
Weekly Care Conferences Involving Pt Navigators
Implement Tools to Prevent Readmissions
Questions?

7/8/2017
8
Medicare Shared Savings Program (MSSP)
Accountable Care Organization (ACO) – Track
3
Elizabeth Barber, MSN, RN, CCM
Manager, Alliance Clinical Team (ACT)
2017
CMS Shared Savings Program -
MSSP ACO Track 3
• Established by section 3022 of the Affordable
Care Act
• ACOs partner with CMS in Advance Payment
Models Contracts (APMs)
• ACOs are groups of doctors and other healthcare
providers who voluntarily work with CMS to
provide high quality, cost effective care to
Medicare Fee for Service Beneficiaries
• Saint Alphonsus was an independent Track 1
(Pioneer Model) for 2 years (2015-16)
• Now a Track 3 Chapter participant (1 of 5) under
Trinity Health Integrated Care (THIC, LLC)
• Track 3 offers shared savings AND is a risk
model – if we don’t perform, we write a check
back to CMS
• Track 3 has several different benefits/structures
from Track 1 – of note, the 3 day SNF waiver
MSSP ACO T3 Patient Eligibility
• Traditional FFS Medicare is the
primary payer (A&B)
• Patients may be dual eligible
(Medicare/Medicaid)
• Patient cannot “opt out” of ACO
• Must be assigned by CMS to the
ACO and on the current year master
beneficiary list
• Patients retrospectively assigned
from CMS using their methodology –
largely claims based – can attribute
to PCP or Specialist
• Most participating attributed
providers are SAMG – one
independent provider group
7/8/2017
9
Proving “High Quality Care”
Some have higher implications for care
management than others:
• Cost savings (must meet a minimum threshold
to account for natural variance)
- Reduce unnecessary utilization (ED/1000,
IP/1000, readmit/1000)
- Right level of care/right time (reduce SNF
LOS, utilize 3 day SNF waiver)
- Care Coordination/Care
Management/Transitions
• Quality: meet report and/or performance
thresholds for 34 quality measures
• Mandatory Reporting Requirements
• EHR utilization (at least 50%)
• Patient satisfaction (CAHPS) Survey for ACOs
3 Day SNF Waiver Patient Eligibility
• Assigned to the ACO in year
admitted to eligible SNF
• Does not currently reside in SNF or
other LTC setting
• Medically stable – does not require
(further) inpatient
evaluation/treatment
• Has a confirmed diagnoses
• Has identified skilled nursing or
rehab need that cannot be met
outpatient
• Evaluated and approved for
admission by an ACO physician
3 Day SNF Waiver SNF Eligibility
• Must be enrolled in Medicare
• Existing written SNF Affiliation
Agreement with ACO
• SNF must have and maintain
an overall 3 star Quality Rating
(this is verified monthly by the
ACO and affiliate will be
removed immediately if they fall
below)
• Other quality/reporting
components as determined by
ACO, such as…

7/8/2017
10
Preferred Post-Acute Providers (PAP)
• Quality data reported to ACO at
regular intervals (SNF LOS,
readmit rates, etc.)
• Collaborative Care Coordination –
RN care managers attend
meetings, works with PAP to follow
and update Care Plan
• Engagement in collaborative post-
acute initiatives (clinical care
guidelines, patient education)
• 24/7 liaisons available for SNF
waiver
• Still a work in progress…
Questions?


















