

Building a Data-Driven Culture of Continuous Improvement 11/Chris DeRienzo Track... · Robinson) to...
38
Building a Data-Driven Culture of Continuous Improvement Chris DeRienzo, MD, MPP Chief Quality Officer, Mission Health
Transcript of Building a Data-Driven Culture of Continuous Improvement 11/Chris DeRienzo Track... · Robinson) to...

Building a Data-Driven Culture of Continuous Improvement
Chris DeRienzo, MD, MPPChief Quality Officer, Mission Health
Conflict of Interest
I have no real or apparent conflicts of interest to report

Agenda
• Why Analytics?
• What’s the Secret Recipe?
• Three Case Studies
Panalytics ∝ (T * CIP)Human

Learning Objectives
• Identify the key ingredients needed to create a true culture of continuous improvement grounded in analytics
• Describe actual workflows used to engrain a data-driven culture of continuous improvement including clinical and operational outcomes
• Describe how pairing clinicians with in-house data scientists can drive improvement “at the edge” of care using predictive analytics

About Mission Health
• Tracing its roots back over 130 years and based in Asheville, Mission Health is
western North Carolina’s only not-for-profit, independent community healthcare
system. We are guided by our BIG(GER) AIM — To get every person to their
desired outcome, first without harm, also without waste and always with an
exceptional experience for each person, family and team member.
• Employing nearly 11,000 dedicated professionals, the system includes seven
hospitals with 1,100+ licensed beds, 800+ employed / PSA providers across 140+
practices, and an Accountable Care Organization that includes hundreds of
community physicians and has 90,000+ lives under management.
• For more information, please visit www.mission-health.org

MAP OF MISSION HEALTH SYSTEM
Western North Carolina 18-County AreaPopulation (2016): 882,581
Percent over 65: 22%
Mission’s BIG(GER) AIM — To get every person to
their desired outcome, first without harm, also without
waste and always with an exceptional experience
for each person, family and team member.

Why healthcare is different…
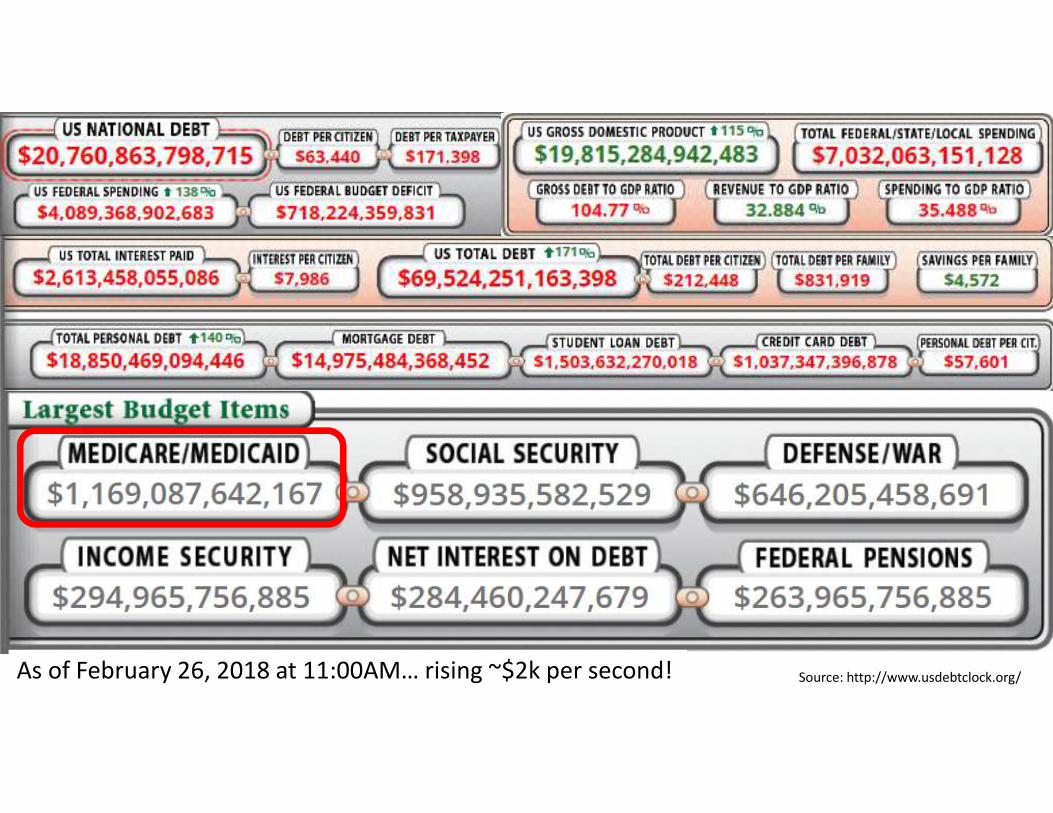
As of February 26, 2018 at 11:00AM… rising ~$2k per second! Source: http://www.usdebtclock.org/


http://www.commonwealthfund.org/publications/issue-briefs/2015/oct/us-health-care-from-a-global-perspective
Are We Delivering?

#analyticsx
C o p yr ig h t © 2 0 1 6 , S A S In s t i t u te In c . A l l r ig h ts reserved .


It’s feeling a bit stormy…
Healthcare’s MAJOR Challenge
• How do we accomplish ALL THREE of these things?
≠

Back to Asheville…
Our BIG(GER) AIM
To get every person to their
desired outcome, first without
harm, also without waste and
always with an exceptional
experience for each person,
family and team member.
Our Business Reality
We are dead in the water without a culture of continuous improvement grounded in analytics permeating everything we do and all that we are.
The Need at Mission Health
• Provide broad access to systemwide analytics, supporting both metrics at the individual unit, patient, and physician level for management to drive outcomes and “30,000” foot data with trends to drive board-level strategy and governance
• Drive the flywheel of continuous improvement by outfitting key clinical / operational roles with skills, tools, and a sense of ownership for improving their own processes
• Create the capability to leverage both operational and clinical predictive analytics
Core Recipe – The Ingredients
• A reliable Enterprise Data Warehouse and analytics environment
• Clinical Program Leadership• Must have strong physician, nurse, and administrative partnership
• A cadre of Lean Engineers / trusted advisors • Early wins always lead to more difficult and complex follow-up projects... build on
“low hanging fruit” to get to deep process transformation

Core Recipe - What To Do with The Ingredients
A Data-Driven
Culture of
Continuous
Improvement
= fDesire (and expectation) to
drive improvement as a
core part of our work
Access to the right tools
Ability to use the tools to
drive improvement
Leadership to provide
ongoing support and a
sense of accountability and
ownership

When it Works: Care Process Models (CPMs)
• Multidisciplinary team committed to a Quadruple Aim victory
• Engaged physician/provider leaders who…• Have the respect (“clinical gravitas”) of their partners
• Practice in the specialty that will use the work
• Are 100% “aligned” and committed to success
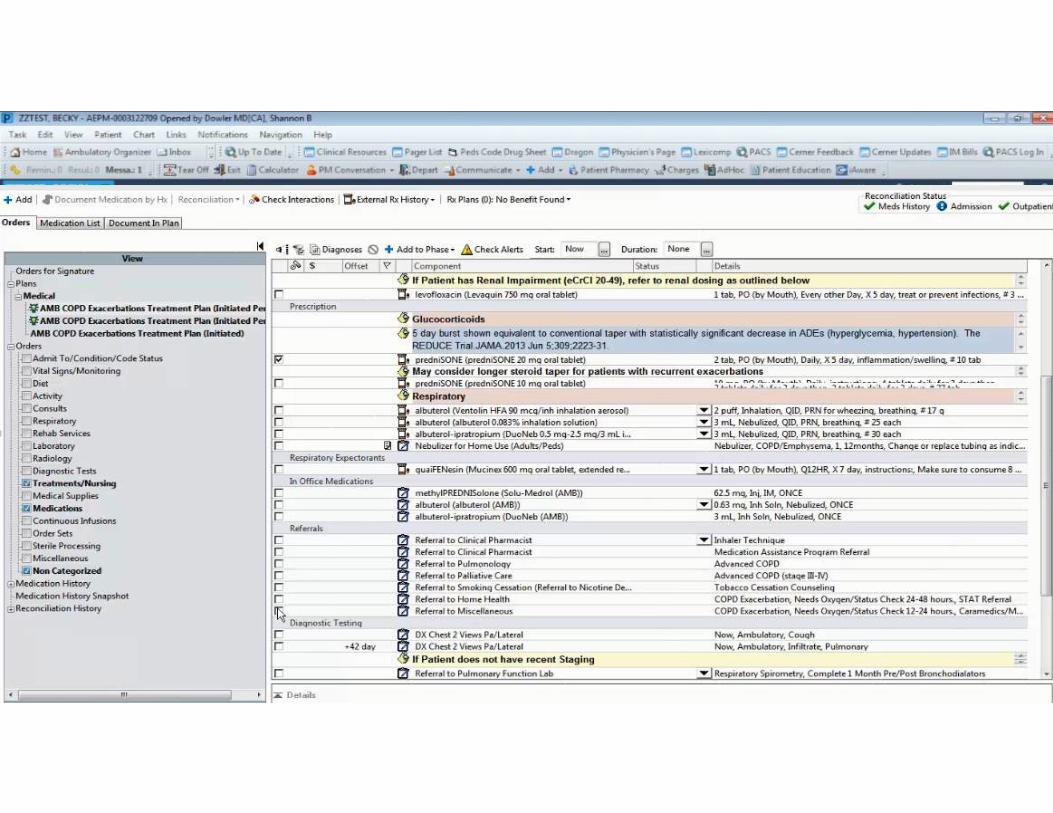
• An integrated / intuitive electronic workflow to implement protocol(s)
• “Unimpeachable” real-time data served within a reliable analytics platform that reaches the MD/patient level with use and outcomes

Members of the 24 CPM Teams Landed in just the first 9 months of FY2017 1. COPD Exacerbation: Liz Lafitte (Performance Improvement), Brian Pritchett (Performance Improvement), Dr. Shannon Dowler, Dr. Gregory Campbell, Tracy Phillips (Nursing), Andrea Beaudry (Informatics), Jonna Munroe (Pharmacy), John
Phillips (Pharmacy)
2. Splenic Injury: Scotta Orr (Performance Improvement), Dr. Anne Conquest, Terrie Smith (Nursing), Morgan Hembree (Informatics), Julie Bednarski (Pharmacy)
3. Breast Cancer Screening: Lisa Stephenson (Performance Improvement), Dr. Rachael Raab, Dr. Helen Sandven, Andrea Beaudry (Informatics)
4. Chronic Obstructive Sleep Apnea: Scotta Orr (Performance Improvement), Dr. Will Corcoran, Lynn Malloy (Nursing), Kathy Anders (Informatics)
5. Cellulitis: Lisa Stephenson (Performance Improvement), Dr. David McClain, Jeanie Bollinger (Nursing), Andie Slivinski (Nursing), Bearnidette Doyle (Informatics), John Phillips (Pharmacy), Beth Becker (Pharmacy)
6. Spine Fusion (Lumbar): Jackie Gosnell (Performance Improvement), Dr. Peter Steenland, Dr. Hubert Gooch, Kelly Phillips (Nursing), Kristy Smith (Nursing), Morgan Hembree (Informatics), Chris Brown (Pharmacy)
7. Induction: Theo Veil (Performance Improvement), Dr. Zack Bowman, Dr. Jack Bryant, Mary Leonidas (CRNA), CJ Smart (Nursing), Deanna McCraw (Informatics), Stephanie Lanning (Pharmacy)
8. Chronic Pain: Lisa Stephenson (Performance Improvement), Dr. Rebecca Bernstein, Tracy Phillips (Nursing), Karen Moseman (Informatics), Sam Olsen (Pharmacy)
9. Depression: John Wood (Performance Improvement), Dr. Kate Rasche, Andrea Beaudry (Informatics), Kristen Wohlford (MMA), Meghan Christian (MMA)
10. Hypertension: Brian Pritchett (Performance Improvement), Dr. Shannon Dowler, Dr. Rebecca Bernstein, Andrea Beaudry (Informatics), Jerod Braschler (Pharmacy)
11. Pulmonary Embolism: Lisa Stephenson (Performance Improvement), Dr. Andy Brown, Dr. Jan Pattanayak, Jeanie Bollinger (Nursing), Bearnidette Doyle (Informatics), Clay Otto (Pharmacy)
12. OB Hemorrhage: Theo Veil (Performance Improvement), Dr. Bre Bolivar, Deanna McCraw (Informatics), Mary Cascio (Nursing), Christine Conrad (Nursing), Stephanie Lanning (Pharmacy)
13. Perinatal Substance Abuse Screening: Theo Veil (Performance Improvement), Dr. Kellett Letson, Dr. Arthur Ollendorf, CJ Smart (Nursing), Deanna McCraw (Informatics)
14. Prenatal Substance Abuse: Theo Veil (Performance Improvement), Dr. Ansley Miller, CJ Smart (Nursing), Christine Conrad (Nursing), Tammy Cody (Care Management), Deanna McCraw (Informatics), Stephanie Lanning (Pharmacy)
15. Non-traumatic SAH: Jackie Gosnell (Performance Improvement), Dr. Robbie Hendry, Robin Jones (Nursing), Morgan Hembree (Informatics), Stephanie Holmes (Pharmacy)
16. Total Knee Arthroplasty: Jackie Gosnell (Performance Improvement), Dr. Skip Smith, Martha Hoskyns (Nursing), Bearnidette Doyle (Informatics)
17. Outpatient Wellness Screening: Brian Pritchett (Performance Improvement), Dr. Jennifer Dukowicz, Meghan Christian, Andrea Beaudry (Informatics), Megan Diffenbaugh (Pharmacy)
18. Hip Fracture: Jackie Gosnell (Performance Improvement), Dr.Adam Kaufman, Martha Hoskyns (Nursing), Bearnidette Doyle (Informatics), Megan Fales (Pharmacy), Krista Luck (Pharmacy)
19. Alcohol Withdrawal: Kyle Carter (Performance Improvement), Liz Lafitte (Performance Improvement), Dr. Samantha Read-Smith, Dr. Kate Mastriani, Jeanie Bollinger (Nursing), Karen Moseman (Informatics), Austin Ginn (Pharmacy), Tiffany
Gardella (Pharmacy, Barbara Kostic (Pharmacy)
20. Well-Child: Theo Veil (Performance Improvement), Dr. Patrick Brown, Deanna McCraw (Informatics)
21. Anticoagulation Reversal: Scotta Orr (Performance Improvement), Dr. Bill Shillinglaw, Terrie Smith (Nursing), Morgan Hembree (Informatics), Krista Luck (Pharmacy)
22. Suicide Assessment: John Wood (Performance Improvement), Dr. Stacia Moore, Sasha Bourne (Nursing), Michele Rowland (Informatics)
23. Chest Pain: Liz Lafitte (Performance Improvement), Kyle Carter (Performance Improvement), Dr. Jason Hunt, Dr. Bill Maddox, Dr. John McClelland, Andie Slivinski (Nursing), Angie Solesbee (Nursing), Bryant Barber (Informatics)
24. Total Hip Replacement: Jackie Gosnell (Performance Improvement), Dr, Ted Barnett, Martha Hoskyns (Nursing), Bearnidette Doyle (Informatics), Megan Fales (Pharmacy), Krista Luck (Pharmacy)
This list doesn’t include the work on all tracking dashboards from members of the Mission Analytics team (Knowledge Engineering, Data Architecture, Business Intelligence, Data
Science, QA/Training), the 50+ non-lead physicians who helped shaped each clinical algorithm, leadership from the Nursing Education Team (primarily Laurie Zone Smith and Rhonda
Robinson) to link CPM work to the nursing clinical ladder, and input / approval from multiple Committees (e.g., Clinical Plan Committee and Protocols Committee, Physician Leadership
Council, Medical Executive Committee, Nursing Leadership committees, and Pharmacy & Therapeutics).
Investment in CPMs
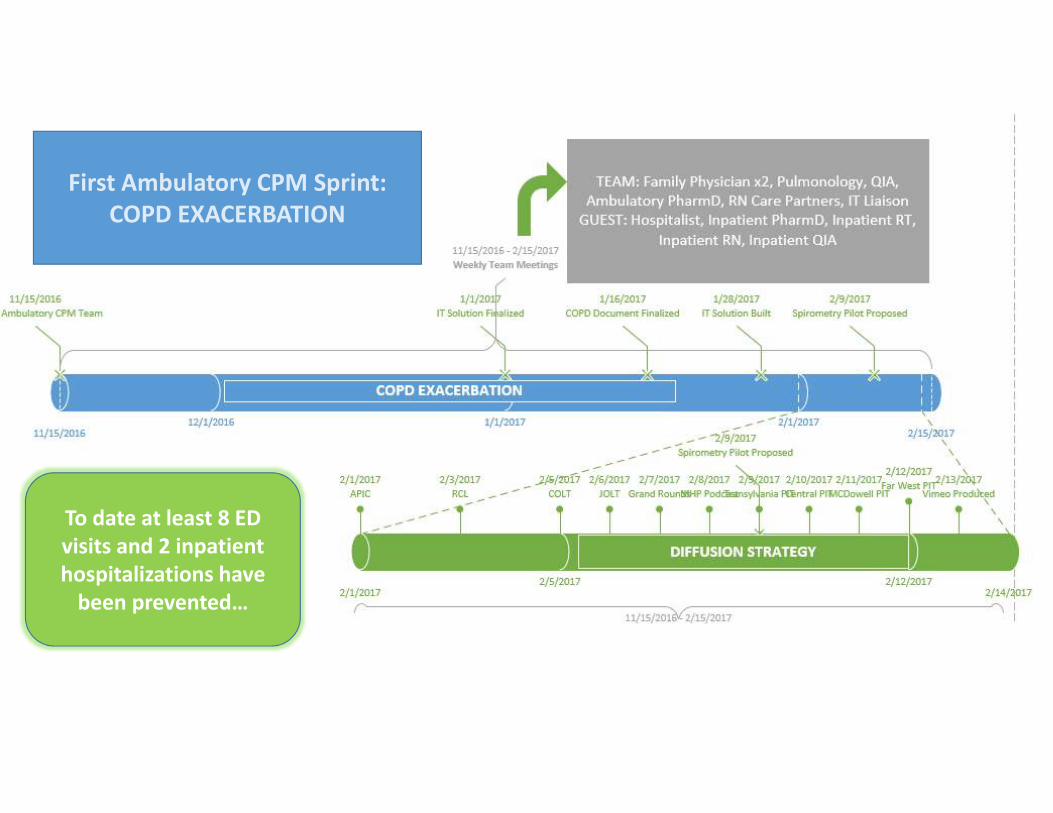
First Ambulatory CPM Sprint:
COPD EXACERBATION
To date at least 8 ED
visits and 2 inpatient
hospitalizations have
been prevented…



Real Outcomes
• 20% increase in full sepsis bundle AND 32% reduction in mortality
• 12 lung cancer deaths avoided with 37% increase in screening
• 9 fewer rib fracture deaths AND ~$350,000 in reduced direct costs
• 42% reduction in in-hospital stroke mortality
• 1,100 more women screened for breast cancer, 6,000 more people screened for colorectal cancer, and 7-fold increase in depression screening
• Compared to 2016, 8 more women avoided a post-hysterectomy SSI and 4 more micropreemies avoided grade III/IV intraventricular hemorrhage
• Reduced both length of stay AND cost per case for bowel surgery patients
• 5 hour reduction in time from door to OR for hip fracture
• Strong achievement across government/commercial pay-for-value programs

When it works… ED Throughput
July 2016
• Left without being seen (LWBS): 3.34% (9 patients / day)
• LOS for patient admitted: 401 minutes
Goals
• “Front 120” = All Patients 120 Minutes Door to Disposition
• “Back 120” = Admitted Patients 120 Minutes Disposition to Bed

Phase 1: Create Milestones –> Design to Future State

Phase II: Real Time Data To Track Specific Milestones

Phase III: Drive to Patient/Provider
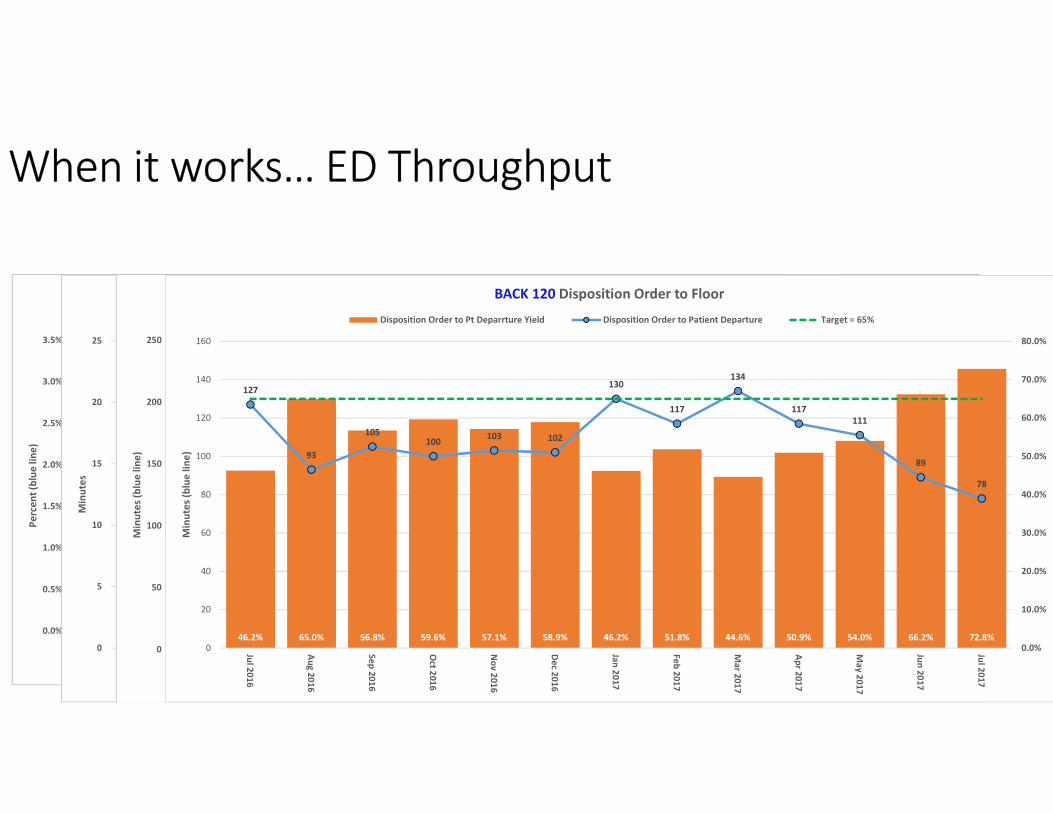
When it works… ED Throughput
287 111 57 48 3721
1253 25
3450 41 30
3.3%
1.3%
0.7%0.6%
0.5%
0.3%0.1%
0.6%
0.3%0.4%
0.6%0.5%
0.3%
0
50
100
150
200
250
300
350
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
Jul 2
01
6
Au
g 2
01
6
Se
p 2
01
6
Oct 2
01
6
No
v 2
01
6
De
c 20
16
Jan
20
17
Fe
b 2
01
7
Ma
r 20
17
Ap
r 20
17
Ma
y 2
01
7
Jun
20
17
Jul 2
01
7
Pa
tie
nts
LW
BS
(o
ran
ge
ba
rs)
Pe
rce
nt
(blu
e lin
e)
Left Without Being Seen
LWBS Count LWBS Target = 1.00%
20
18 18 18
17
13 13
15
13
14 14
13
12
0
5
10
15
20
25
Jul 2
01
6
Au
g 2
01
6
Se
p 2
01
6
Oct 2
01
6
No
v 2
01
6
De
c 20
16
Jan
20
17
Fe
b 2
01
7
Ma
r 20
17
Ap
r 20
17
Ma
y 2
01
7
Jun
20
17
Jul 2
01
7
Min
ute
s
Arrival to Provider (median)
Arrival to Provider Target = 20 mins
17.1% 20.0% 19.9% 22.2% 21.5% 22.6% 21.7% 19.6% 25.8% 26.0% 23.7% 24.9% 21.6%
229
203208
193 192186
194 192
174170
180 181 182
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
0
50
100
150
200
250
Jul 2
01
6
Au
g 2
01
6
Se
p 2
01
6
Oct 2
01
6
No
v 2
01
6
De
c 20
16
Jan
20
17
Fe
b 2
01
7
Ma
r 20
17
Ap
r 20
17
Ma
y 2
01
7
Jun
20
17
Jul 2
01
7M
inu
tes
(blu
e lin
e)
FRONT 120 - Arrival to Disposition Order (Admit Pts, Excl BH Pts)
Arrival to Disposition Order Yield Arrival to Disposition Order Target = 35%
46.2% 65.0% 56.8% 59.6% 57.1% 58.9% 46.2% 51.8% 44.6% 50.9% 54.0% 66.2% 72.8%
127
93
105100
103 102
130
117
134
117
111
89
78
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
0
20
40
60
80
100
120
140
160
Jul 2
01
6
Au
g 2
01
6
Se
p 2
01
6
Oct 2
01
6
No
v 2
01
6
De
c 20
16
Jan
20
17
Fe
b 2
01
7
Ma
r 20
17
Ap
r 20
17
Ma
y 2
01
7
Jun
20
17
Jul 2
01
7
Min
ute
s (b
lue
lin
e)
BACK 120 Disposition Order to Floor
Disposition Order to Pt Deparrture Yield Disposition Order to Patient Departure Target = 65%

When it Works… Readmission Prediction v1
Initial tool: LACE
Goal: to construct and automate the calculation of a risk model for 30-day, all-cause inpatient readmission
Requirements:
• Performance must beat LACE in our (Mission
Hospital’s) patient population
• Be available before 8am day after discharge
• First version must use fields currently in EDW

The Plan…

Real Life…

Perseverance Does Pay Off…

Implementation
Lessons Learned
• Panalytics ∝ (T * CIP)Human
• Start with principles core to the organization’s purpose, mission and vision
• Clear ownership of processes will minimize ambiguity and “spin”
• Tools without purpose will not be adopted – don’t miss an ingredient!
• Achieving both cultural AND resource alignment is crucial to success
• Scaling can be challenging… ask if a “quick sauce” could work just as well
• And most of all… remember that process and technology exist
to help HUMANS to do more of what only humans can do…



















