Budd chiari syndrome
29
BUDD CHIARI SYNDROME BY DR.JINO JUSTIN
-
Upload
jino-justin -
Category
Health & Medicine
-
view
364 -
download
3
Transcript of Budd chiari syndrome

BUDD CHIARI SYNDROME
BY DR.JINO JUSTIN
Budd–Chiari syndrome is a condition caused
by occlusion of the hepatic veins that drains the
liver.
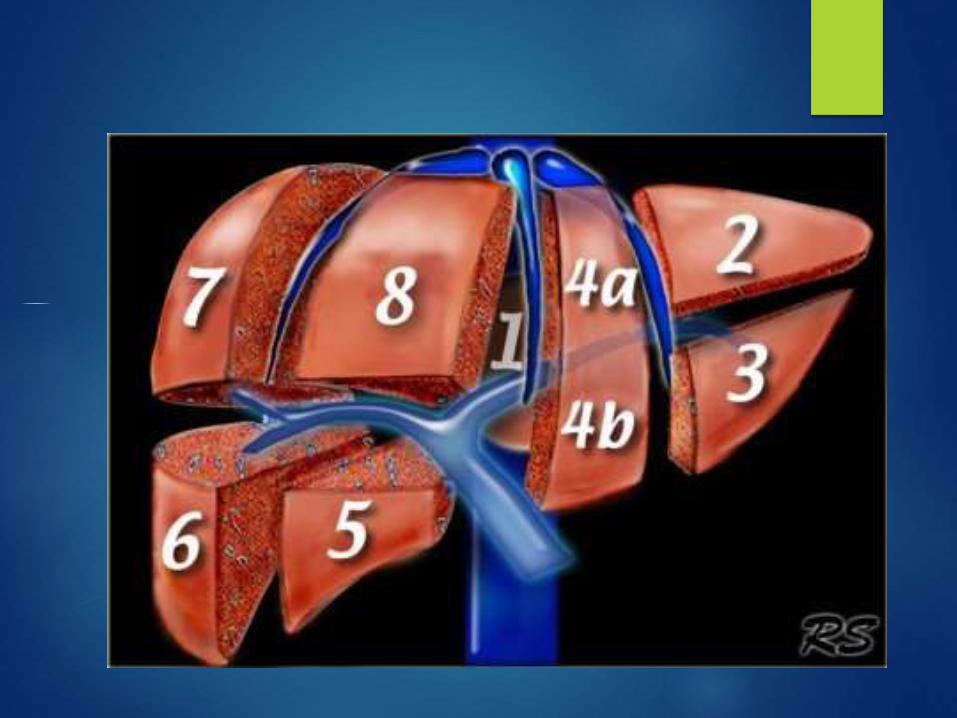
Couinaud classification of
liver anatomy
Divides the liver into eight functionally indepedent
segments.
Each segment has its own vascular inflow, outflow and biliary drainage.
centre of each segment there is a branch of the
portal vein, hepatic artery and bile duct.
periphery of each segment there is vascular
outflow through the hepatic veins.
epidemology
m:f 1:2
3rd and 4th decade
Median age – 35
Location
Hepatic vein 62%
IVC 7%
Both IVC & hepatic veins 31%
Associated portal vein thrombus 14%
Pathogenesis
HEPATIC VEIN THROMBOSIS
Sinusoidal pressure
Sinusoidal flow
Sinusoidal dilatation+Interstitial fluid filtration
Fluid passes through hepatic capsule(Ascitis)

portal vein pressure & perfusion of liver via portal vein
Hypoxia of hepatocyte
inflammatory centrilobular cell necrosis
Release of free oxygen radicals
Atrophy
chronic
weeks of obstruction
fibrosis of centrilobar area
nodular regeneration in periportal area
cirrhosis portovenous
. collateral
cirrhosis
Etiology:
majority of patients have an underlying hematologic
abnormality.
Tumor
Hepatocellular carcinoma
Carcinoma of pancreas
Carcinoma of kidneys
Metastatic disease
Normal biopsy findings do not exclude this entity
Role of imaging:
Evaluation of occlusion of the hepatic veins and inferior vena
cava
Caudate lobe enlargement
Inhomogeneous liver enhancement and
Intrahepatic collateral vessels and hypervascular nodules.
Budd-Chiari syndrome Presents with - acute or
chronic form.
acute - results from an acute thrombosis of the hepatic veins or the IVC
Chronic form is related to fibrosis of the
intrahepatic veins.

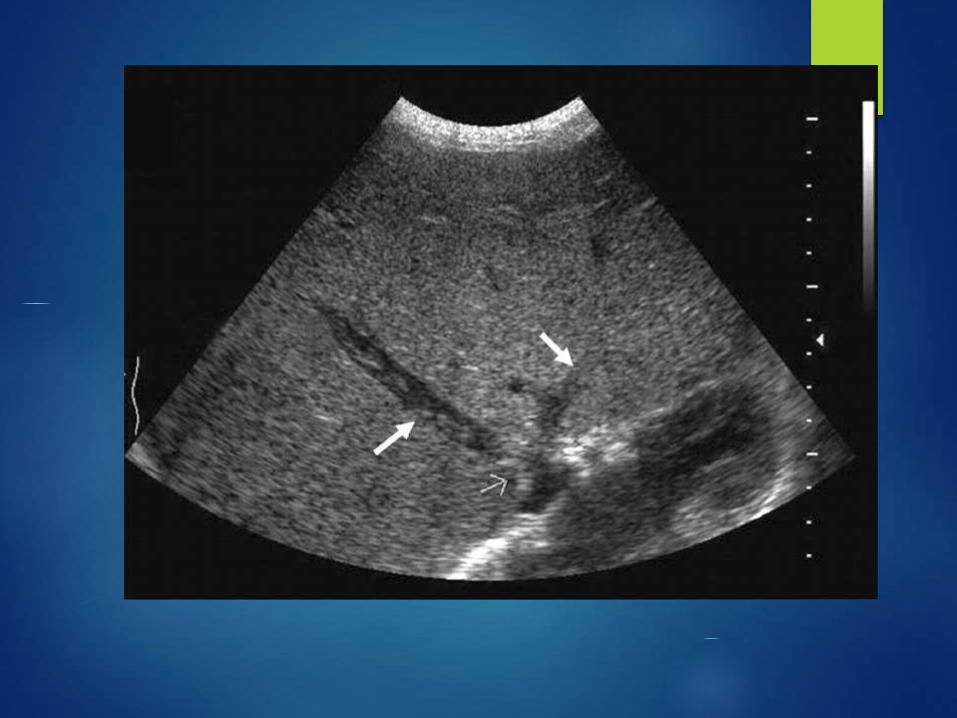
Ultrasound findings
Enlargement of the caudate lobe.
Ascitis
Partial or complete inability to see the hepatic
veins ; stenosis with proximal dilatation, and
thrombosis
Narrowing of IVC due to compression by the
enlarged caudate lobe.
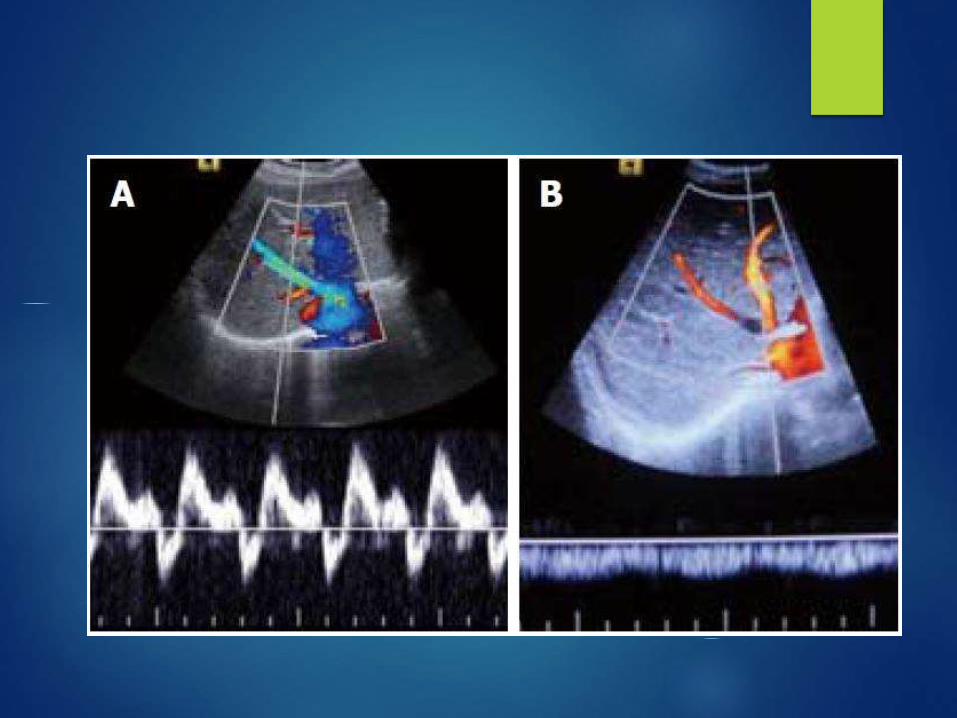
Color Doppler studies shows absent or flat or
reversed flow in the hepatic veins,IVC, or both
increased resistive index within the hepatic artery
- >0.75 is seen


Classification of BCS According to
the Level of Obstruction
Type I Obstruction of IVC with or without
secondary hepatic vein occlusion
Type II Obstruction of major hepatic veins
Type III Obstruction of the small centrilobular
venules.
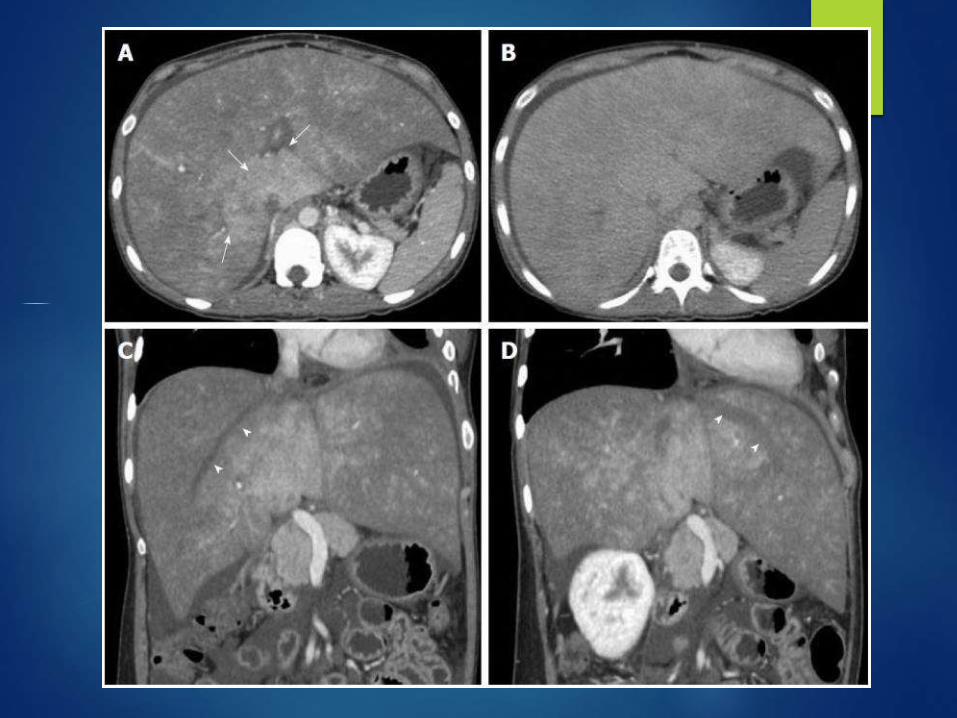
CT:Acute BCS
The liver appears enlarged and swollen with presence of ascites.
decreased peripheral enhancement.
stronger enhancement of the central portion of the liver parenchyma
Thrombosed hepatic veins and IVC appears hypoattenunated.
inferior vena cava is compressed by the enlarged caudate lobe.
liver may have a heterogeneous appearance secondary to hemorrhage and infarction.
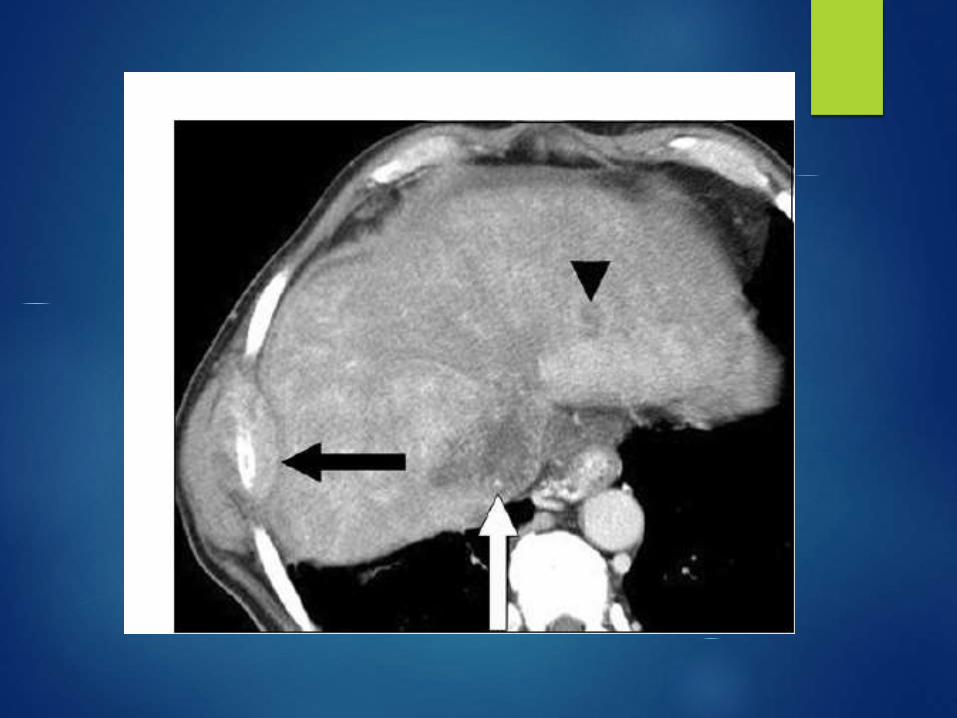
CT chronic BCS
Multiple regenerative nodules (diameter of 0.5–4.0 cm)
regenerative nodules are homogeneously hyperattenuating
on arterial phase and remain slightly hyperattenuating on
portal venous phase.
multiple tortuous intrahepatic collaterals may be seen.
CECT
Arterial phase:
--strongly enhancing nodular lesions or may show patchy enhancing areas due to arterio-portal shunting and opacification of portal vein.
The portal phase:
--patchy and mottled type of heterogeneous strong enhancement in the central part of the liver.
--poor or no enhancement in the periphery.
Delayed phase:
--enhancement pattern becomes more homogeneous
HV remain unopacified in all the phases

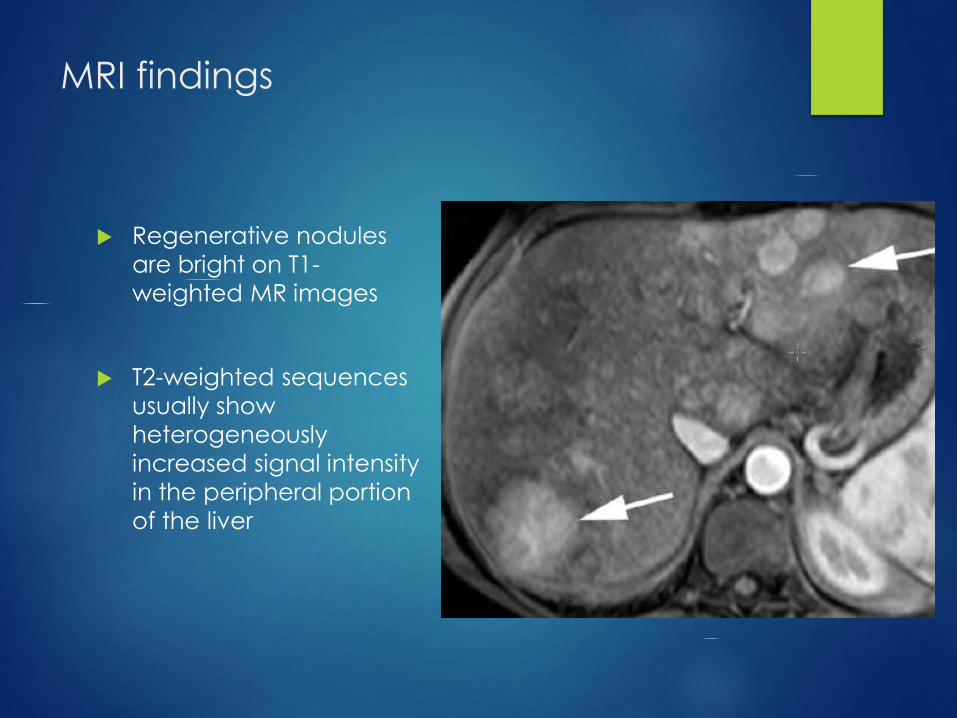
MRI findings
Regenerative nodules
are bright on T1-
weighted MR images
T2-weighted sequences
usually show
heterogeneously
increased signal intensity
in the peripheral portion
of the liver

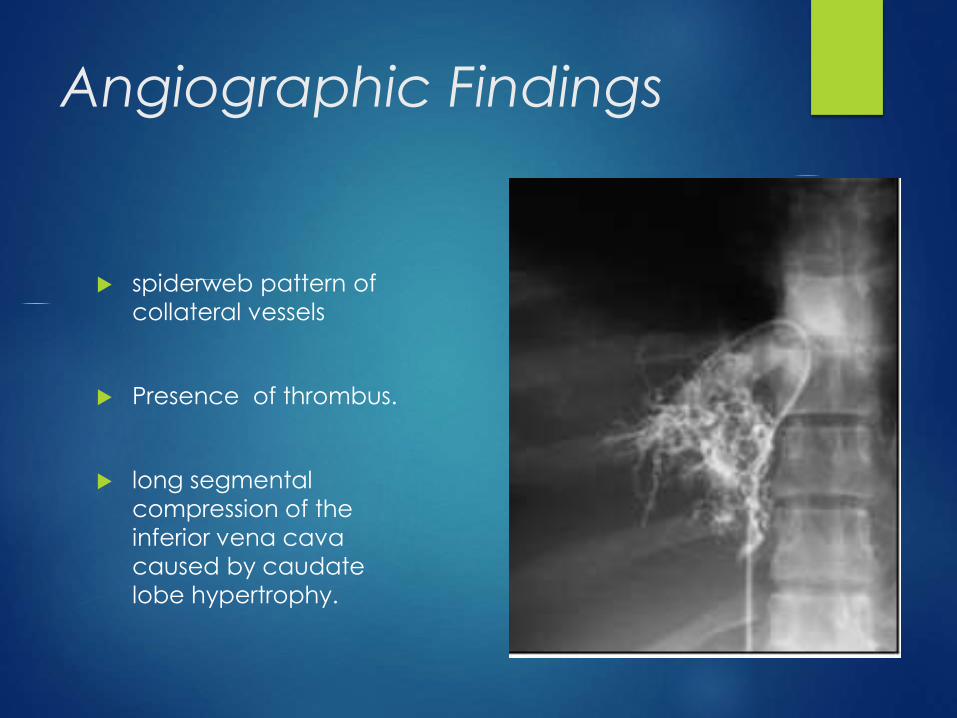
Angiographic Findings
spiderweb pattern of
collateral vessels
Presence of thrombus.
long segmental
compression of the
inferior vena cava
caused by caudate
lobe hypertrophy.

Differential Diagnosis
Hepatic Cirrhosis:
Regenerative nodules smaller than BCS
Increased iron content
Patent HV & IVC
Primary sclerosing cholangitis
Chronic cholestatic disease of unknown cause
Mostly associated with ulcerative colitis.
THANK YOU