Bronchiolitis: Management Strategies and Controversies Moyez B. Ladhani.
75
Bronchiolitis: Management Strategies and Controversies Moyez B. Ladhani
-
Upload
daniel-poole -
Category
Documents
-
view
213 -
download
1
Transcript of Bronchiolitis: Management Strategies and Controversies Moyez B. Ladhani.

Bronchiolitis: Management Strategies and Controversies
Moyez B. Ladhani

Disclosures: None

Objectives:
• Review RSV• Review Pathophysiology, • Presentation • Management

Introduction:
• Viral bronchiolitis is the commonest lower respiratory tract infection in children less than 12 months of age and is the most frequent cause of hospitalization in infants under 6 months of age.
• It is caused by viral infections of the lower respiratory tract, principally by respiratory syncytial virus (RSV).

Introduction:
• Outbreaks occur worldwide during the late fall, winter, and early spring.
• In North America, the season generally begins in early November and continues through April.

RSV Season in the US

Introduction:
• Fifty percent of all children develop RSV infection by 12 months of age; by 2 years of age, virtually all children have had RSV infection.

Introduction:
• Reinfections with RSV occur throughout life. Reinfection rates among preschool children can range from 40% to 70%.

Introduction:
• The annual risk of reinfection among school-age children, adolescents, and adults is approximately 20%.
• Reinfection illnesses are generally mild, with most children having only one infection associated with disease of the lower respiratory tract.

Pathophysiology:
• The average incubation period of RSV-induced respiratory disease is 5 days.
• Inoculation of upper respiratory tract epithelial cells occurs via the eye and nose, with subsequent cell-to-cell transfer of the virus to the lower respiratory tract.

Pathophysiology:
• Histopathologic descriptions from infant autopsy specimens document infection of the bronchiolar epithelium, with subsequent epithelial cell necrosis.
• In addition, there is peribronchiolar mononuclear infiltration and submucosal edema.

Pathophysiology:
• As a result of these changes, plugs of mucus laden with cellular debris are formed, leading to areas of partial or complete airway obstruction.


Pathophysiology:
• Hyperinflation occurs following trapping of air peripheral to the sites of partial occlusion. Subsequently, with complete obstruction, multiple areas of atelectasis develop.

Pathophysiology:
• Often infants who have lower respiratory tract disease from RSV exhibit pathologic evidence of both pneumonia and bronchiolitis.
• In cases of pneumonia, there is an interstitial infiltration of mononuclear cells, sometimes accompanied by edema and necrotic areas that lead to alveolar filling.


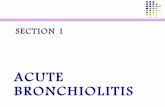
Copyright ©1998 American Academy of Pediatrics
Darville, T. et al. Pediatrics in Review 1998;19:55-61
Chest film findings in this infant include hyperexpanded lung fields, bilateral interstitial

Diagnosis:
• Bronchiolitis is a clinical diagnosis. Typically, infants present with breathing difficulty associated with coryza
• Less commonly, young infants, especially those born prematurely, may present with apnoea before developing the characteristic cough, tachypnoea and use of the accessory muscles of respiration.

Clinical Features:
• Nasal obstruction ± rhinorrhoea and an irritating cough are noticed first.
• After 1–3 days there follows increasing tachypnoea and respiratory distress. The chest is often overexpanded.
• Auscultatory signs are very variable: fine inspiratory crackles are often heard early, becoming coarser during recovery; expiratory wheeze is often present, initially high-pitched, with prolonged expiration.

Diagnosis:
• Respiratory distress may be mild, moderate or severe.
• Fever of 38.5°C or greater is seen in about 50% of infants with bronchiolitis.
• Apnoea may be the presenting feature, especially in very young, premature or low-birthweight infants. It often disappears, to be replaced by severe respiratory distress


Factors increasing the likelihood of hospital admission
• History of significant apnoea before assessment
• Known structural cardiac anomaly, especially large left-to-right shunt (eg, ventricular septal defect)
• Known pre-existing lung disease (eg, cystic fibrosis)
• Chronological age less than 6 weeks

Factors increasing the likelihood of hospital admission
• Significant prematurity (< 32 weeks) and/or chronic neonatal lung disease
• Severe degree of respiratory distress or apnoea
• Significant dehydration• Hypoxaemia (Spo2 < 93%)• Re-presentation to the emergency
department within 24

Treatment:
• Prevention of Cross Infection• Oxygen• Chest Physiotherapy• Bronchodilators• Epinephrine• Corticosteroids• Hypertonic Saline• Antibiotics

Prevention of Cross Infection:
• There is no direct evidence from RCTs that cohort segregation, handwashing, and use of gowns, masks, gloves and goggles, in combination or individually, reduces the nosocomial transmission of bronchiolitis in hospitalized infants.
• Three observational studies have found a lower incidence of RSV transmission in hospital after the introduction separately of cohort segregation, handwashing, gowns and masks, and goggles

Prevention of Cross Infection:
• Combinations of these strategies in one RCT found no advantage of gowns and masks over handwashing with gowns and masks,
• Consequently, the most important point to emphasize to parents and staff is that frequent adequate hand washing by nursing and medical staff, other staff and parents will minimize the risk of cross-infection

Oxygen
• The use of supplemental oxygen therapy has not been subjected to randomized controlled clinical trials, but its use is considered appropriate to overcome hypoxaemia .
• In general, maintain an Spo2 ≥ 93% saturation during the acute phase and during recovery, and accept 90% to 92% if the child is not distressed and is feeding well as sufficient for cessation of oxygen therapy and discharge.

Chest Physiotherapy:
• The Cochrane Library:
• Chest physiotherapy is thought to assist infants in the clearance of secretions and decrease ventilatory effort.

Chest Physiotherapy:
• chest physiotherapy using vibration and percussion techniques did not reduce length of hospital stay, oxygen requirements, or improve the severity clinical score in infants with acute bronchiolitis that are not under mechanical ventilation, and who do not have any other co-morbidity
• None of the trials included in this review reported adverse events

Chest Physiotherapy:
• Many Consensus statements do recommend the use of physiotherapy

Bronchodilators:
• In viral bronchiolitis, bronchodilators do not improve oxygen saturation, or affect rate or duration of hospitalizations
• Bronchodilators are commonly used in the management of bronchiolitis in North America but not in the United Kingdom

Bronchodilators:
• Cochrane Library:• Randomized controlled trials
(RCTs) comparing bronchodilators (other than epinephrine) with placebo in the treatment of bronchiolitis.
• Twenty-two clinical trials with 1428 infants with bronchiolitis were included in this review

Bronchodilators:
• There was no improvement in clinical score for 43% of those treated with bronchodilators compared to 57% of those treated with placebo

Bronchodilators:
• There was modest short-term improvement in clinical scores with the use of bronchodilators in the management of mild to moderately severe bronchiolitis
• there was no statistically significant improvement in oxygenation overall

Bronchodilators:
• Bronchodilator recipients showed no improvement in the rate of hospital admission after treatment as outpatients
• or duration of hospitalization for inpatients

Bronchodilators:
• Conclusion: Bronchodilators produce small short-term improvements in clinical scores
• Current practice parameter is to use a trail of bronchodilator, if there is a clinical improvement, continue its use else there is no benefit to continue.

Epinephrine:
• Cochrane Library:
• To compare epinephrine versus placebo and other bronchodilators in infants less than 2 years of age with bronchiolitis

Epinephrine:
• Studies were included if they: – 1) were RCTs comparing
epinephrine with placebo or other bronchodilator;
– 2) involved children less than two years with bronchiolitis;

Epinephrine:
• There is insufficient evidence to support the use of epinephrine for the treatment of bronchiolitis among inpatients.
• There is some evidence to suggest that epinephrine may be favourable to salbutamol and placebo among outpatients

Corticosteroids:
• Cochrane Library:
• To systematically review the evidence on the effectiveness of systemic glucocorticoids for the treatment of infants and young children with acute viral bronchiolitis.
• The primary outcome of interest was length of hospital stay (LOS). Secondary outcomes were: respiratory rate, haemoglobin oxygen saturation, and hospital admission and revisit rates

Corticosteroids:
• In the pooled analysis of eight trials, the day three clinical score indicated no difference between treatment groups

Corticosteroids:
• Hospital admission rates were examined in three trials and no difference was seen between treatment groups
• Readmission rates were reported in six studies; with no significant differences between treatment groups

Corticosteroids:
• The respiratory rate and haemoglobin oxygen saturation were reported descriptively in six RCTs; no differences were found between groups

Corticosteroids:
• No benefits were found in either LOS or clinical score in infants and young children treated with systemic glucocorticoids as compared to placebo. There were no differences in these outcomes between treatment groups; either in the pooled analysis or in any of the sub analyses.

Corticosteroids:
• Available evidence suggests that corticosteroid therapy is not of benefit in this patient group

Antibiotics:
• Cochrane Library:• To evaluate the effect of using antibiotics,
either routinely or in selected patients, in infants aged younger than 24 months old, diagnosed with acute bronchiolitis compared to placebo to reduce both the severity and duration of illness.
• This review found no evidence to support the use of antibiotics for bronchiolitis.

Antibiotics:
• Antibiotics are commonly prescribed in bronchiolitis, although they have no action against viruses.
• One small RCT failed to demonstrate any benefit in hospitalised infants with bronchiolitis.

Antibiotics:
• The only role for antibiotics is in complicated bronchiolitis where a secondary bacterial infection, such as with streptococcus or staphylococcus, is suspected.
• This is rare, but not easily excluded in a sick infant with fever, toxicity and significant opacities on the chest radiograph

Antibiotics:
• Unfortunately, antibiotics are most frequently prescribed in children with mild bronchiolitis with minimal chest radiographic changes, such as partial right upper lobe collapse, which are common place in uncomplicated RSV bronchiolitis.


What is on the horizon?

Nebulized Hypertonic Saline
• Breaks bonds in mucous• Induces osmotic flow of water into
mucous layer from submucosal cells• Reduction of edema • Stimulates ciliary beats by releasing
prostaglandin E2

3% Hypertonic Saline
• Given nebulized with a bronchodialator
• Given 3X/day throughout admission
• Decreases length of stay by 25%.
• NO side effects or adverse events

3% Hypertonic Saline in ERKuzik et al
• Can it prevent admission to hospital?• 3 doses neb HS in ER after arrival• Decrease admission rate by 9% but
study underpowered to reach stat sig.

3% Hypertonic saline….in progress
“Nebulized Hypertonic saline for Bronchiolitis”
• LA Children’s Hospital and Childrens Hospital at Oakland
• 3% Hypertonic Saline vs Normal saline• Up to 3 doses in ER, then Q8h if admitted• Admission Rate, Length of stay, clinical score• Feb 2008 – March 2010, n=600

Epinephrine and Steroids!!

“…combined therapy with dexamethasone and epinephrine may significantly reduce hospital admissions.”

Suggested Practice
• 4mls 3% HS + 1.5 mg epinephrineq8h until discharge
• Other meds at physicians discretion• Exclude
– Infants >18 months– Previous wheeze– Cardiac or Chronic lung diseases– Critically ill

Summary of Therapies
• Treatment is usually symptomatic• Isolation• Humidified oxygen is usually indicated• Ensure patients are well hydrated• Chest physio is of no proven benefit• Saline nose drops may be of value

Summary of Therapies
• Trial of bronchodilators may improve wheezing
• Epinephrine has shown some benefits• Corticosteroids are not indicated• Antibiotics are not useful• 3% Normal Saline of value• Ventilatory assistance should be
considered for those with increasing respiratory distress

Which of the following conditions puts an infant at higher risk for more severe disease?
a) Prematurityb) Congenital Heart Diseasec) Down Syndromed) All of the above

Which of the following are considered “Routine” orders for an infant being admitted with bronchiolitis?a) Chest Xrayb) Amoxilc) Oxygen and fluids as neededd) Ventolin q4h

Which of the following treatments may improve outcomes for bronchiolitis patients?
a) Ventolinb) Hypertonic saline (3%)c) Amoxild) Combination of Epinephrine and
Dexamethasone.

When is it Asthma?

When is it Asthma?


Virology:
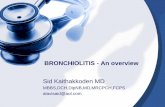
• RSV is an enveloped, single-stranded RNA virus. Two glycosylated surface proteins, the attachment (G) and fusion (F) proteins, are essential for RSV to infect cells

Virology:
• This electron micrograph of respiratory syncytial virus (RSV) illustrates five virions budding from an infected cell

SPREAD OF INFECTION
• RSV spreads easily from person to person through respiratory secretions. Spread within families is very high.
• RSV is a major nosocomial threat on pediatric wards, causing appreciable morbidity.
• The two primary modes of transmission for RSV include direct contact with large droplets of secretions and self-inoculation by touching contaminated objects.

SPREAD OF INFECTION
• Transmission by small-particle aerosol is not significant; thus, the risk of acquiring infection decreases with increasing distance from the patient.
• RSV-infected nasal secretions remain infectious on countertops for more than 6 hours.

SPREAD OF INFECTION
• RSV can be recovered from rubber gloves for 1 hour and 30 minutes, from gowns for 30 minutes, and from hands for 25 minutes.
• Thus, RSV can survive for extended periods in the hospital environment, increasing the risk for infectious transfer from fomites to hands and then to the eyes and nose of a susceptible individual. The eyes and nose appear to be the primary entry sites for RSV; the mouth is an insensitive route of inoculation.

SPREAD OF INFECTION
• RSV frequently is shed for prolonged periods, which increases its contagious nature.
• In a study of infants hospitalized
for RSV infection, the mean duration of shedding was 6.7 days, with a range of 1 to 21 days.

SPREAD OF INFECTION
• Viral shedding from asymptomatic patients does occur.
• In the immunocompromised host, viral shedding can extend beyond 6 weeks.

SPREAD OF INFECTION
• Because immunity to this virus is short-lived, there is always a large number of susceptible individuals.
• Hospital nursery units, child care centers, and other institutions are at high risk for RSV outbreaks.

SPREAD OF INFECTION
• Transmission among infants may not be as important as transmission between infants and staff.
• Visitors are another potential source of spread.