Bronchiectasis, Past, Present and Future
53
Bronchiectasis, Past, Present and Future Professor Adam Hill Royal Infirmary and University of Edinburgh NHS Education for Scotland
Transcript of Bronchiectasis, Past, Present and Future

Bronchiectasis, Past, Present and FutureProfessor Adam Hill
Royal Infirmary and University of Edinburgh
NHS Education for Scotland

Plan of talk
• Diagnosis
• Aetiology
• Disease stratification
• Physiotherapy
• Long term treatments
• The future…

Bronchiectasis
1819, Laennec:
a chronic, debilitating disease
1932, Warner:
“copious foetid sputum...marked constitutional symptoms...a social outcast...”

PREVALENCE OF BRONCHIECTASIS IN THE UK FROM 2004 TO 2013
Prevalence >10 per 1,000 in the elderly
Eur Respir J 2016;47:186-193

Past
5

6

7

Score486 Patients
0 1 2 3
Bronchial dilatation
Absent Mild(lumen just > diameter of
adjacent vessel)
Moderate(lumen 2-3
times > diameter of
adjacent vessel)
Severe(lumen >3
times diameter of
adjacent vessel)
Number of bronchopulmonary segments with emphysema
Absent 1-5 >5
0
20
40
60
80
Emphysema No emphysema
Elas
tase
ng
/ml
Free Elastase
BRICS
1 MILD
2-3 MODERATE
4-5 SEVERE
Chest. 2018 153(5);1177-1186

Sputum purulence
ERJ 2009;34:361-4
N=141 MUCOID
MUCUPURULENT
PURULENT
M
I
L
D
S
E
V
E
R
E
Guides investigations, managementand clinicians to estimate prognosis

Bronchiectasis Severity Index ScoringScore range 0-26
Mild = 0-4
Moderate = 5-8
Severe = 9+
Variable Score
FEV1 % Predicted
50-80 1
30-49 2
<30 3
Hospital admission before study 5
Exacerbations before study >3 2
Dyspnoea MRC score
4 2
5 3
Pseudomonas colonization 3
Colonization with other organisms 1
Variable Score
Age
50-69 2
70-79 4
80+ 6
BMI <18.5 kg/m2 2
>3 lobes involved or cystic bronchiectasis
1
Am J Respir Crit Care Med. 2014;189:576-85
www.bronchiectasisseverity.com for online
calculation tool

0
10
20
30
40
50
60
70
80
SGRQ % Hospital admission % Mortality
Sco
re (
SGR
Q)
or
% o
f p
atie
nts
(h
osp
ital
ad
mis
sio
n a
nd
m
ort
alit
y)Mild: 0-4 Moderate: 5-8 Severe: 9+
n=191 n=224 n=193
Bronchiectasis Severity Index Scores Reflect Clinical Outcomes

12
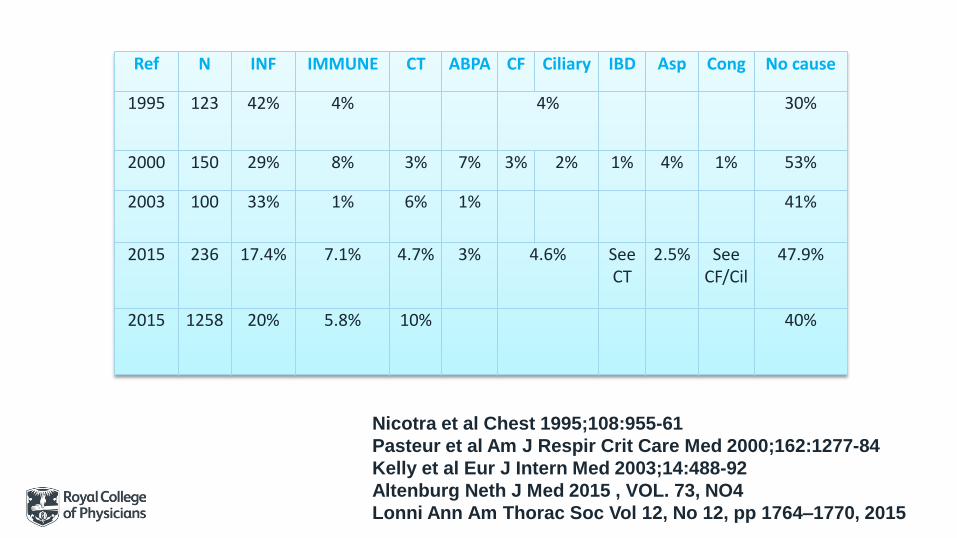
Ref N INF IMMUNE CT ABPA CF Ciliary IBD Asp Cong No cause
1995 123 42% 4% 4% 30%
2000 150 29% 8% 3% 7% 3% 2% 1% 4% 1% 53%
2003 100 33% 1% 6% 1% 41%
2015 236 17.4% 7.1% 4.7% 3% 4.6% See CT
2.5% See CF/Cil
47.9%
2015 1258 20% 5.8% 10% 40%
Nicotra et al Chest 1995;108:955-61
Pasteur et al Am J Respir Crit Care Med 2000;162:1277-84
Kelly et al Eur J Intern Med 2003;14:488-92
Altenburg Neth J Med 2015 , VOL. 73, NO4
Lonni Ann Am Thorac Soc Vol 12, No 12, pp 1764–1770, 2015

Aetiologies with specific treatments
Cystic Fibrosis e.g. DNAase
CVID e.g. Ig replacement
Active ABPA e.g. PN, Itraconazole
Hiatus Hernia e.g. PPI, prokinetics, Sx
NTM e.g. RECl/Cipro
IBD e.g. Corticosteroids

Primary care database
Study population 18, 793
Asthma 7988 (42.5)
Chronic obstructive pulmonary disease 6774 (36.1)
HIV 1300 (6.9)
Rheumatoid arthritis 1163 (6.2)
Other connective tissue diseases 969 (5.2)
Inflammatory bowel disease 527 (2.8)
Bone marrow transplant 20 (0.11)
Hypogammaglobulinaemia 172 (0.9)
Allergic bronchopulmonary aspergillosis 339 (1.8)
None of these comorbidities 6422 (34.2)
Eur Respir J 2016;47:186-193

Comorbidities- n=986
Lancet Respir Med 2016; 4(12):969–979
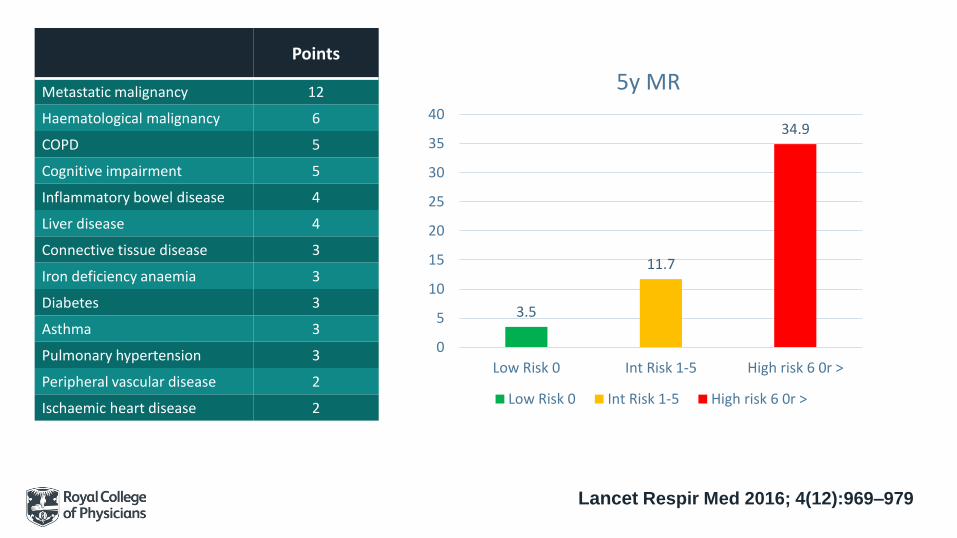
Points
Metastatic malignancy 12
Haematological malignancy 6
COPD 5
Cognitive impairment 5
Inflammatory bowel disease 4
Liver disease 4
Connective tissue disease 3
Iron deficiency anaemia 3
Diabetes 3
Asthma 3
Pulmonary hypertension 3
Peripheral vascular disease 2
Ischaemic heart disease 2
3.5
11.7
34.9
0
5
10
15
20
25
30
35
40
Low Risk 0 Int Risk 1-5 High risk 6 0r >
5y MR
Low Risk 0 Int Risk 1-5 High risk 6 0r >
Lancet Respir Med 2016; 4(12):969–979

COPD with Bx, inc. risk of exacerbations
PLoS One 2016; 11(3): e0150532.
Exacerbations Mortality

Vascular disease- primary care study in 3,895,710 adults (0.3% had Bx)
CORONARY HEART DISEASERISK OF FIRST EPISODE CHD
HR 1.44 (95% CI 1.27 to 1.63)
STROKERISK OF FIRST EPISODE STROKEHR 1.71 (95% CI 1.54 to 1.90)
Thorax 2017;72:161–166.

Secondary care study (n=400)
Chest 2017;151(2):383-388
0
2
4
6
8
10
12
14
16
IHD post PVD post CVD post AF post
%
v
a
s
c
u
l
a
r
e
v
e
n
t
BSI 0-4 BSI 5-8 BSI 9+
***
**
***

Multivariable analysisRisk of vascular disease
Independent Variable
Exp(B)
95% CI P value
Male 2.39 1.14-5.02 0.02
Hypertension 2.92 1.36-6.26 0.006
On maintenance statin therapy
7.78 3.16-14.55 <0.001
BSI Moderate 5-8 3.92 1.21-12.71 0.023
BSI Severe >9 8.12 2.44-27.0 0.001
• Population based GP study- n= 895
• There was an increased rate of first time cardiovascular events in the 91 day period after a respiratory tract infection
• IRR 1.56; 95% CI 1.20 to 2.02
• The rate of a first cardiovascular event was highest in the first three days following a respiratory tract infection
• IRR 2.73, 95% CI 1.41 to 5.27
Ann Am Thorac Soc 2018 Mar;15(3):315-321
GP STUDY

Does the isolation of a pathogen matter in Bx?

Conventional Microbiology Culturepathogenic microorganisms were isolated in 75% of patientsEnvironmental mycobacteria 2-30%; Metanalysis 9.2%
Am J Respir Crit Care Med. 2012;186(7):657-65
38.6
21
12.4
11.4
9.7
9.3Haemophilus influenzae
Pseudomonas aeruginosa
Staphylococcus aureus
Moraxella catarrhalis
Streptococcus pneumoniae
Others
Arch Med Sci 2014; 10: 661-8

Ps. aeruginosaAssociated more severe disease (CT)
More rapid decline in FEV1
Increased hospitalisation + worse HRQOL
Reduced survival
Martínez-García Chest. 2007;132(5):1565-72.
Evans Eur Respir J. 1996;9(8):1601-4.
Wilson Eur Respir J. 1997;10(8):1754-60.
Miszkiel Thorax 1997;53(3):260-4.
Ho PL Chest. 1998 Dec;114(6):1594-8.
Loebinger Eur Respir J. 2009 Oct;34(4):843-9.
0
5
10
15
20
25
30
2010 2011 2012
Pseudomonas aeruginosa
2010
2011
2012
Thorax. 2012 Oct;67(10):928-30.
Thorax. 2014 Mar;69(3):292-4.

Sputum purulence
ERJ 2009;34:361-4
N=141
MUCOID
MUCUPURULENT
PURULENT
M
I
L
D
S
E
V
E
R
E
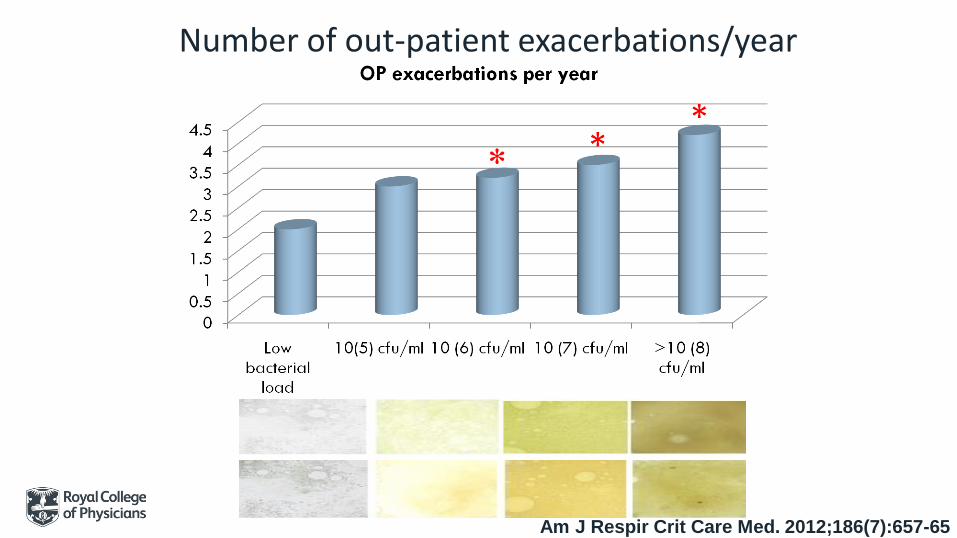
Number of out-patient exacerbations/year
*
Am J Respir Crit Care Med. 2012;186(7):657-65

27
J Clin Med. 2018 Nov; 7(11): 429.
42
21
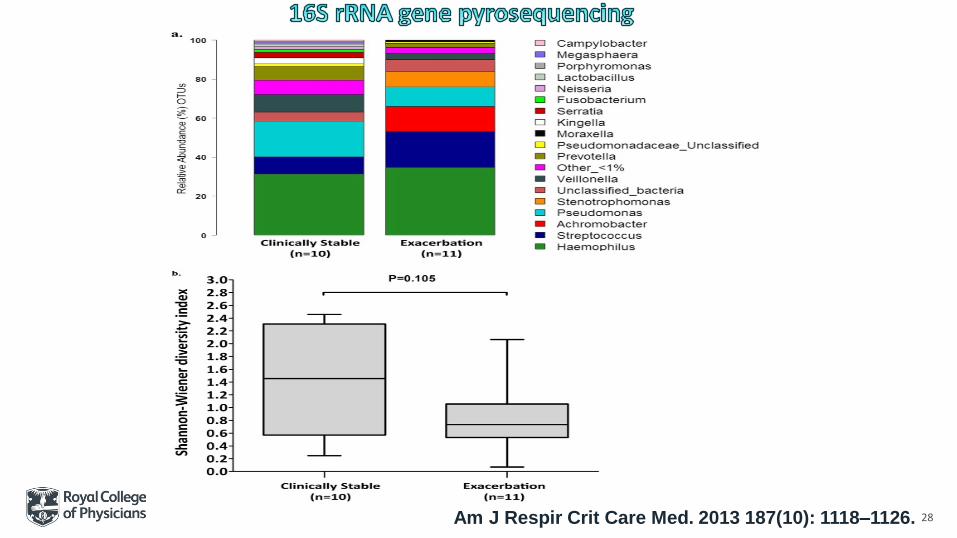
28Am J Respir Crit Care Med. 2013 187(10): 1118–1126.

Do genetic and environmental factors influence Bx?

Vit D and Bx- 402 patients<25nmol/L deficient25-74 nmol/L insufficient>75 nmol/L replete
0102030405060708090
DeficientInsufficientReplete
*
Thorax 2013;68:39-47
*
*
2.00E+07
6.00E+06
2.00E+05
Deficient Insufficient Replete
Bacterial Load
Bact Ld
*

MBL deficiency and Bx470 Bx Pts and 414 controls
Lancet Respir Med. 2013 May;1(3):224-32
12% vs. 10% Genotype
Genotype YO/YO;XA/YO
Low
55
High
280
P
FEV1(%P) 68.9% 74.3% 0.096
Chr. colonisation
85% 65% <0.0001
Ps. aeruginosa 35% 13% <0.0001
H. Influenzae 47% 28% 0.01
Bacterial load log10 cfu/ml
6.5(2.8) 5.0(3.3) 0.01
Exacerbations 2.7(1.8) 1.9(1.3) <0.0001
SQRQ 55.4(21.9) 44.3(21.9) 0.007
LCQ 12.7(4.9) 14.3(4.4) 0.03

What long term treatments influence Bx?

Muco-active treatmentsSaline/Carbocysteine
HTA Funded Study- Belfast
380 Patients; UK; 16+ Sites
6% Saline
BDCarbocisteine
6% Saline
BD
+
C
Standard Care
rhDNAse- 349 Pts
6m. Trial
Chest. 1998 May;113(5):1329-34.
Exacerbations rhDNAse Placebo
Per patient 0.95 0.71

Inhaled Mannitol- 461 patients- 1 year- 400mg BD Vs 50mg BD Placebo
34
Mean exacerbations- 1° endpoint
Mannitol 1.69 (95% CI 1.48 to 1.94)
Control 1.84 (95% CI 1.61 to 2.10)
RR 0.92 (95% CI 0.78 to 1.08), (p=0.31)
SGRQ (0-100; MCID 4U)
Mean difference −2.40 (−4.76 to −0.05), p= 0.0457
Side Effects
16.5% failed the challenge test
82% completed study
7.2% with S/E- Cough (3.1%), ↓FEV1 (2.2%), bronchospasm (0.5%), O2desaturation (0.7%) and wheeze (0.5%).
Thorax. 2014 Dec;69(12):1073-9.

STEP 1
Offer ACBT
Review within 3m
STEP 2
If ACBT not effective/poor adherence
Consider Oscillating PEP + FET
STEP 3
Nebulised saline
(isotonic or hypertonic)
Consider Gravity Assisted Positioning
Bronchodilator
MucoactiveTx
Airway clearance
Nebulisedantibiotic/ICS

Inhaled corticosteroids in Bx- no benefit in exacs.
36Cochrane Database Syst Rev 2018

Bacterial burden in airways
3 or more exacerbations per yr
Consider long term antibiotics
No. Adult
0 20.5%
1-2 35.2%
3 or more 25.7%
No Data 18.6%

Macrolides- anti-inflammatory or anti-infective
0
0.5
1
1.5
2
2.5
3
3.5
EMBRACE 6mEMBRACE 12m BAT BLESS BLESS Pa
Active Placebo
p<0.001
p<0.003
p<0.02
p<0.0001
p<0.001

Wu Respirology 2014 Gao PLOS ONE 2014
n 530 559
Exacerbations RR 0.7 (0.6-0.82)p<0.001
RR 0.42 (0.29-0.61)P<0.001
SQRQ -5.39 (-9.89 to -0.88)P=0.02
-6.56 (-11.99 to -1.12)P=0.02
Change FEV1 0.02 (0-0.04)P=0.01
0.31 (0.12-0.51)P=0.002
Eradication Pathogens
NS
Adverse Events NS NS
EmergentPathogens
NS
GI side effects RR 3.33 (1.8-6.15)P=0.0001
Diarrhoea
Abdo pain
RR 4.47 (1.83-6.89)P=0.0001NS
RR 4.33 (1.77-10.58)P=0.001RR 6.2 (1.43-26.83), P=0.01
Chron Respir Dis. 2019 Jan-
Dec;16:1479972318790269

-0.4 Amikacin
-1.4 Colistin
-2.6 Aztreonam
-3.4 Ciprofloxacin (inh)
-4.1 Ciprofloxacin (neb)
-4.6 Tobramycin
Overall-2.75↓
Summary- reduction in cfu at 4 weeks with inhaled antibiotics
Brodt ERJ 2014;44:383-393

Time to first exacerbation
Target organism
Duration CONT Placebo Active
GentamicinN-57
PPM 80mg bd 1y Continuous1 year
Y 61d 120d*
ColomycinN-144
PA 1MU bd Continuous6 months
Y 111s103d
165d168d*
RESPIRE 1N-278
PPM 32.5mg BD Inhaled Ciprofloxacin 1y 14/28d On and Off
N 186d186d
>336d***336
RESPIRE 2N-347
PPM 1y N NE NE
ORBIT 3N- 278
PA ARD-3150 (liposome encapsulated ciprofloxacin 135 mg and free ciprofloxacin 54 mg) once daily1y
N 136d 214d
ORBIT 4N- 304
PA 1y28d On and Off
N 158d 230d*
AztreonamN- 266N- 274
Mixed 75mg tds4m28d On and Off
N 120dNE
NENE


Future- 1- Aetiology
43
Adult
Immunodeficiency IgG, IgA and IgM 75.7%
Protein
electrophoresis
61.3%
Functional antibody
response
40.1%
ABPA IgE 69.6%
Aspergillus
fumigatus RAST or
skin prick
63.1%
CF Sweat test analysis 4.1%
CF Cytogenetics 5.8%
Aspiration 3.2%
PCD 2.1%?

Future- Associated conditions + Risks
44
Airways
disease
Adult-2017
4845 patients
105 Hospitals
Asthma 29.8%
COPD 23.7%
If co-existing airways disease- Mt may be different c.f.Bx without airways diseasee.g. ICS; inhaled antibiotics
Not forgetting to optimise airways disease- Airway pharmacotherapy- Pulmonary rehabilitation- LTOT/ NIV
In moderate and severe BX- Assess vascular risk factors (smoking, weight, DM, HTN, cholesterol)- Consider secondary prevention
Future- assessing treatments for patients
Phenotyping patients better
• Sputum purulence
• Severity score e.g. Bronchiectasis Severity Index
• CT Chest Scores e.g. BRICS for idiopathic Bx
• Need CT Chest scores for other aetiologies
45

Future- assessing treatment response• Patient perspective
LCQ, SQRQ, BrQOL, Bx health Questionnaire
• Exacerbations
Mean
Number
Time to first exacerbation
• Sputum microbiology
Qualitative vs. quantitative microbiology
16S
PCR based probes
46
• Airways calibre
FEV1, FVC
Mid expiratory Flows
Multiple Breath Washout (MBW) to measure Lung Clearance Index (LCI)
• CT scanning
Assessing treatment response e.g. mucus plugging, small airways disease, quantification of emphysema, bronchial dilatation
?other modalities MRI/PET
Eur Respir J. 2015 Dec;46(6):1645-53

Future- assessing treatments quantitative responseSputum colour
47
0
10
20
30
40
50
60
70
Saline
Gentamicin
0m
3m
6m
9m
12m
0
20
40
60
80
100
neb (27) oral (88) iv (30) All (145)
% p
atie
nts
Changes in ISWT (%)
Deterioration No change 1-4.99%
5-9.99% ≧10%
Chest. 2018 Dec;154(6):1321-1329.Am J Respir Crit Care Med. 2011 15;183(4):491-9.

PAST Present Future
BTS Gx 2019First line therapy
Active Cycle Breathing Technique+
Consider Gravity Assisted Positioning

Long term antibiotics
ORAL
Systemic treatment
INHALED
Targeted treatment
Evidence base strong
In reducing exacerbations
Evidence base weaker
In reducing exacerbations
Macrolides
Gentamicin
Colomycin
Ciprofloxacin
Aztreonam
GI s/e
Balance
Resistance
Oral S/E
Bronchospasm
?Resistance

Anti-inflammatory treatmentsTreatment Duration Exacerbations Ref
AZD9668 NE inhibitor 4 weeks No evidence Respiratory Med 2013; 107:524-33.
Atorvastatin 80mg bd mild/mod Bx
6 months ↓no. but no effect on mean
Lancet Respir Med 2014;2:455-463
Atorvastatin 80mg bd severe Bx 3 months No effect Chest. 2017 Aug;152(2):368-378.
CXCR2 AZD5069 antagonist 28d No evidence Eur Respir J. 2015 Oct;46(4):1021-32.
50

Anti-inflammatory or Antibiotics or Both
Continuous vs. 14d on/off and 28d on/off
Summer break
Long term impact on resistance