Bronchial Asthma · Bronchial Asthma Definition Bronchial asthma is a clinical syndrome...
54
Bronchial Asthma Nathir M Obeidat
Transcript of Bronchial Asthma · Bronchial Asthma Definition Bronchial asthma is a clinical syndrome...
Bronchial Asthma
Nathir M Obeidat
Bronchial Asthma Definition
Bronchial asthma is a clinical syndrome characterised by recurrent episodes of airway obstruction, which resolve spontaneously or as a result of treatment.
The reversibility of the airway obstruction in asthma is the feature that distinguishes it from other forms of obstructive lung diseases.
Definition of Bronchial Asthma
• A chronic inflammatory disease of the airways in which
many cells play a role, in particular, mast cells, eosinophils
and T lymphocytes.
• In susceptible individuals this inflammation causes
recurrent episodes of wheezing, breathlessness, chest
tightness and cough, particularly at night and or early
morning.
•These symptoms are associated with airflow limitation that
is at least partially reversible either spontaneously or with
treatment.
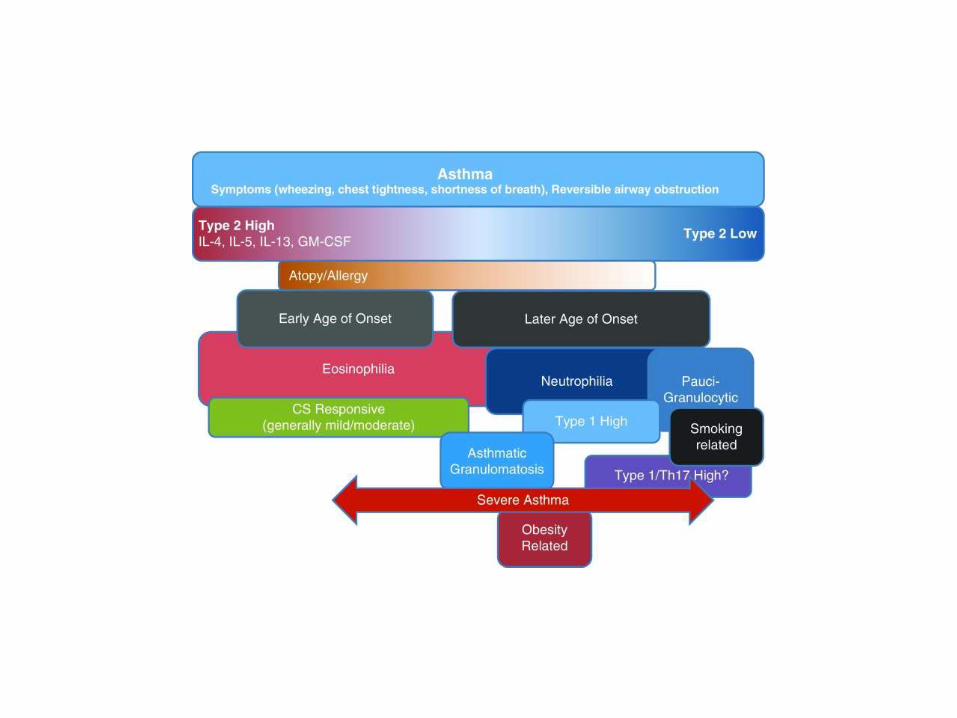
Asthma Phenotypes
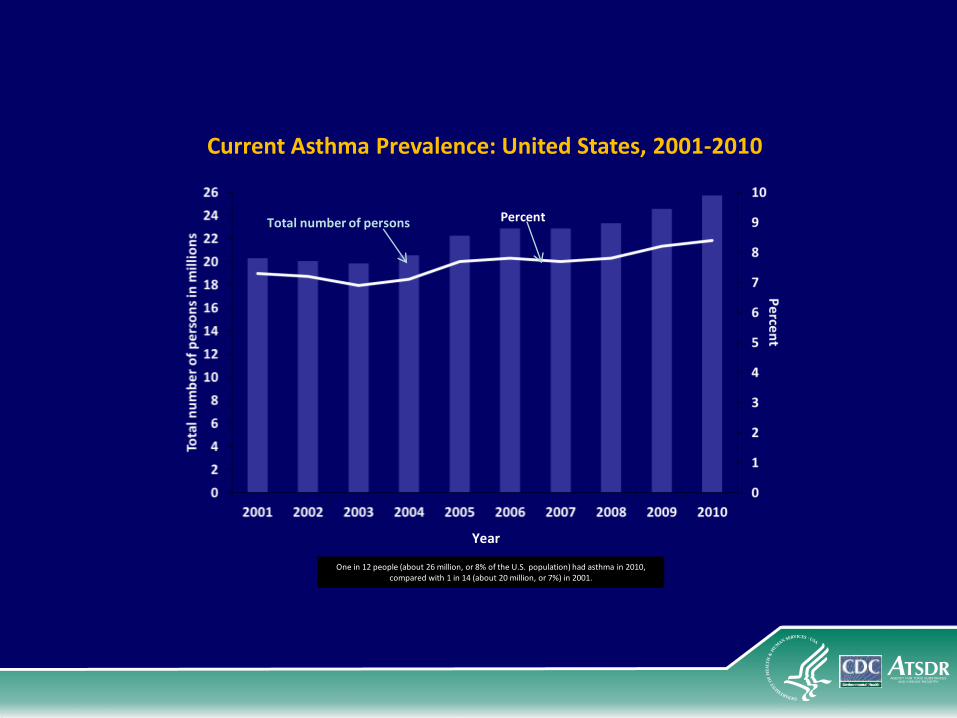
Total number of persons Percent
Current Asthma Prevalence: United States, 2001-2010
One in 12 people (about 26 million, or 8% of the U.S. population) had asthma in 2010, compared with 1 in 14 (about 20 million, or 7%) in 2001.
Year
Risk Factors for Developing Asthma
Genetic characteristics
Occupational exposures
Environmental exposures
Risk Factors for Developing Asthma:
Genetic Characteristics
Atopy
The body’s predisposition to develop an antibody
called immunoglobulin E (IgE) in response to
exposure to environmental allergens
Can be measured in the blood
Includes allergic rhinitis, asthma, hay fever, and
eczema
Pathophysiology of Bronchial Asthma
• It is a Complex interaction of cells and mediators, which lead to:
1- Inflammation
2- Bronchial hyperresponsiveness
3- Airflow limitation
4- Variability.
5- Reversibility
Inflammation 1
• It is a result of interaction of Cellular changes which includes:
1- Cells such as epithelial cells, mucous glands , endothelial cells and myofibroblasts.
2- Resident cells such as bone marrow-derived mast cells and macrophages.
3- Infiltrating cells such as eosinophils, CD4 , neutrophils , basophils and platelets.
Inflammation 2
- The above cells will lead to generation of mediators that can induce bronchoconstriction.
- These mediators includes histamine ,platelet activating factor, and some derivatives of arachidonic cascade such as PGD2 ,C4 ,D4, E4 (LTC4,LTD4 ,LE4).
- Infiltration of airways by mast cells, eosinophils, activated T lymphocytes and neutrophils
Inflammation 3
- Mast cells as aresult of IgE – Mediated stimulation also release mediators
- Cytokines most of which are product of lymphocytes and macrophages
- Edema of the airway mucosa is due to inflammation and increased capillary permeability.
Inflammation 4
• Death from severe asthma usually occurs from blockage of airways by mucous plugging.
• The presence of mucous plug is associated with hyperplasia and metaplasia of goblet cells

Airway Hyper responsiveness
- It is an exaggerated bronchoconstrictive response by the airways to a variety of stimuli such as histamine , methacholine ,cold air ,and environmental irritants.
- It is not known whether bronchial hyperreacyivity ( BHR) is acquired or is present at birth.
- it is thought that inflammation is the stimulus for BHR
- The degree of BHR usually correlates with the clinical severity of asthma
AIRWAY OBSTRUCTIONCauses
- Acute bronchoconstriction
- Mucous plugging of airways
- Bronchial wall edema
- Inflammatory cell infiltration
- Airway wall remodeling
- Smooth muscle hypertrophy
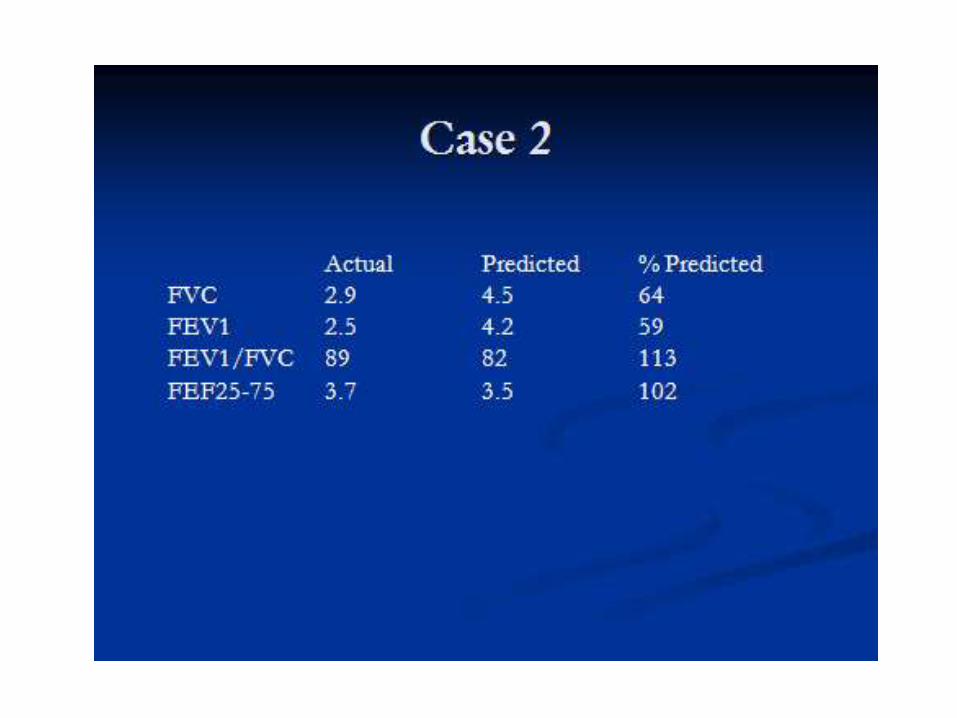
Airflow limitation
• Defined as FEV1/FVC <75%.
• During remission this can be normal.
• Age Dependent.
• Needs spirometry for assement of severity of the disease.
ATOPY• Defined as genetic susceptibility for developing
immunoglobilin IgE directed to epitopes expressed on common environmental allergens such as dust mites , animal proteins, pollens, and fungi.
• Atopic asthma has seasonal variation and avoidance of the offending antigens may result in dramatic improvement.
• Atopy manifests as allergic asthma, allergic rhinitis , allergic sinusitis with eosinophilia and high serum IgE level
Variability• Defined as a diurnal variation of PEEFR of 20%.
• This is diagnostic for asthma.
• The degree of variability is proportional to the severity of asthma.
• A high degree of variability signals unstable asthma that demands increased medications
Direct Medical Care
Hospital stay
Intensive care
Emergency department
Primary care
Medications
Indirect Costs
Social security
Loss of work output
Loss of school days
Impact on individual / family / society
Cost of asthma
GINA Guidelines 2010

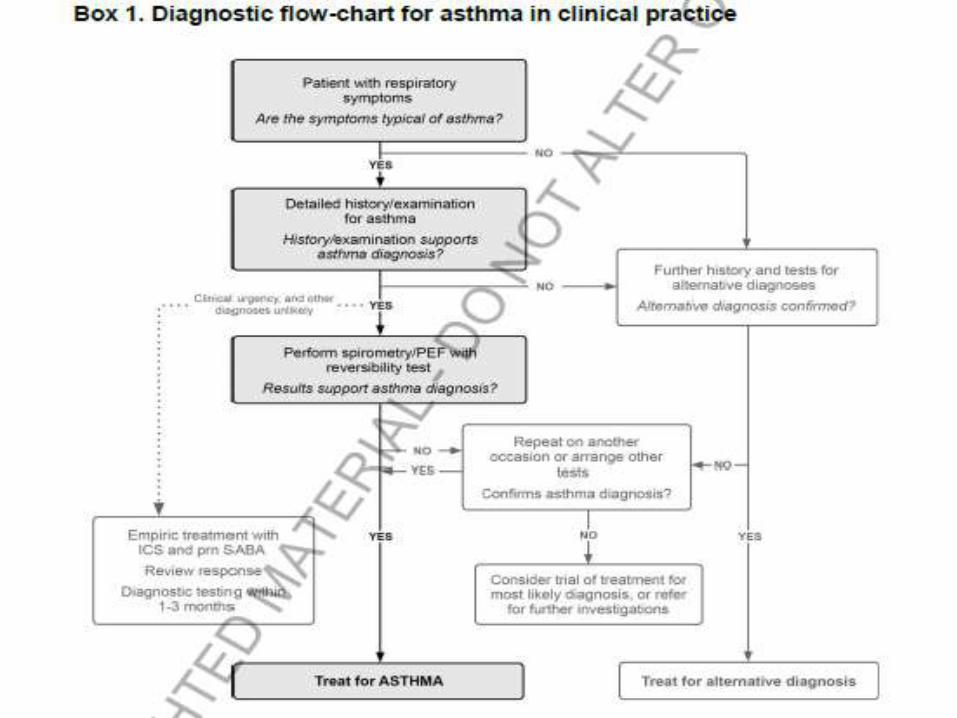
Diagnosis• History
• Physical Examination
• PFT
- Vitalogram
- Spirometry
- FVL
- Lung Volumes
- DLCO
- PFM
- ABG
Diagnosis
• CXR
• IgE Level and Eosinophills
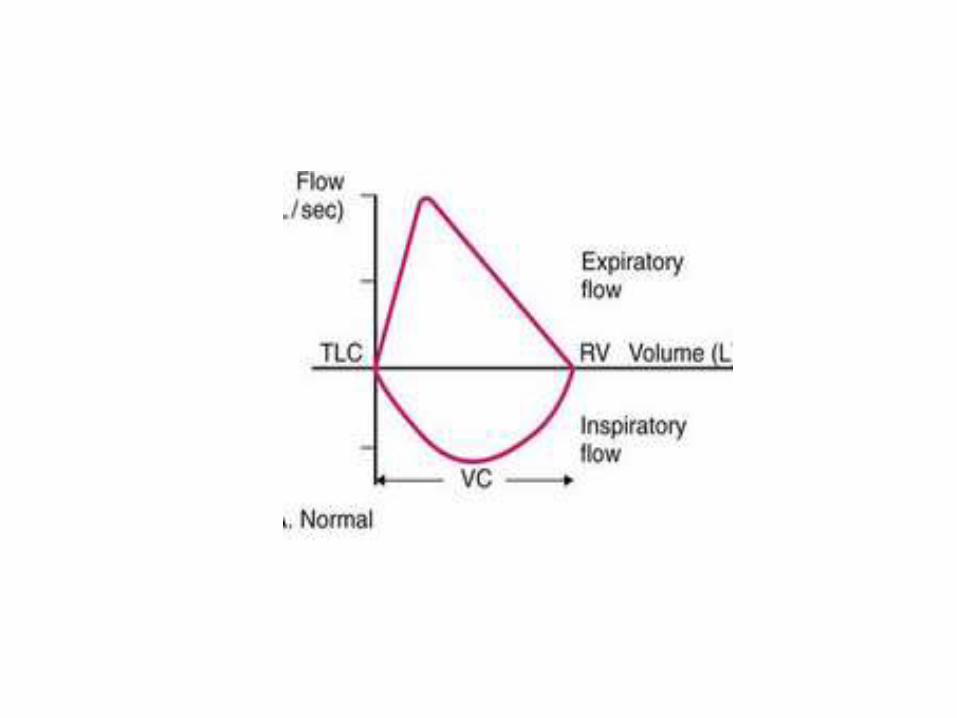
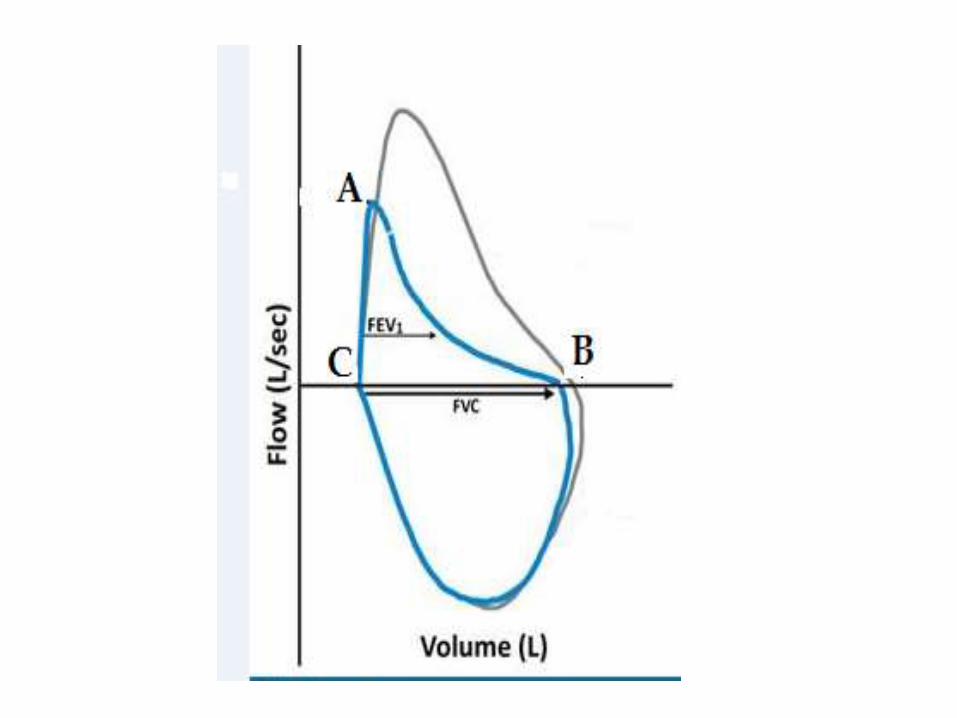
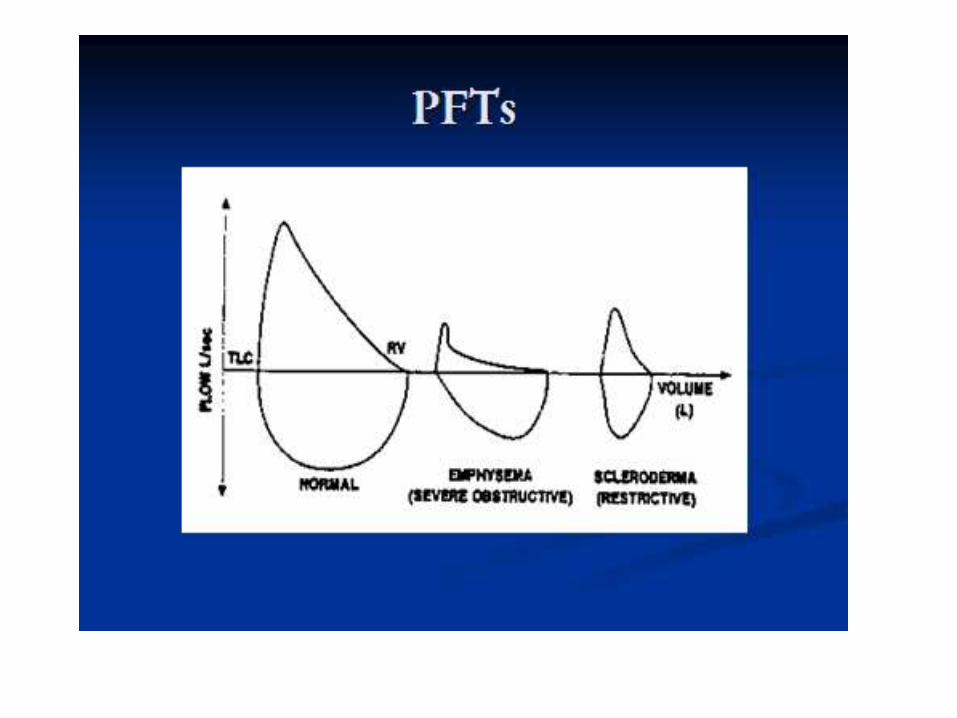
FVL
• Location of the changes :
- Above the line (Expiratory Arm)
Or
- Below the line (Inspiratory arm)
• Shape of the Loop
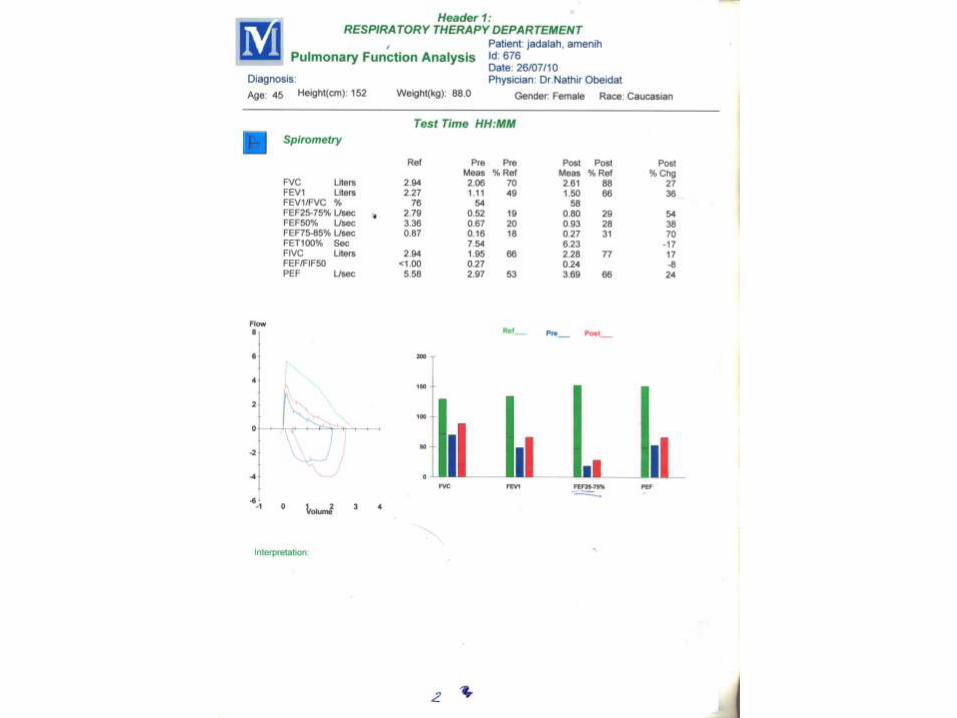
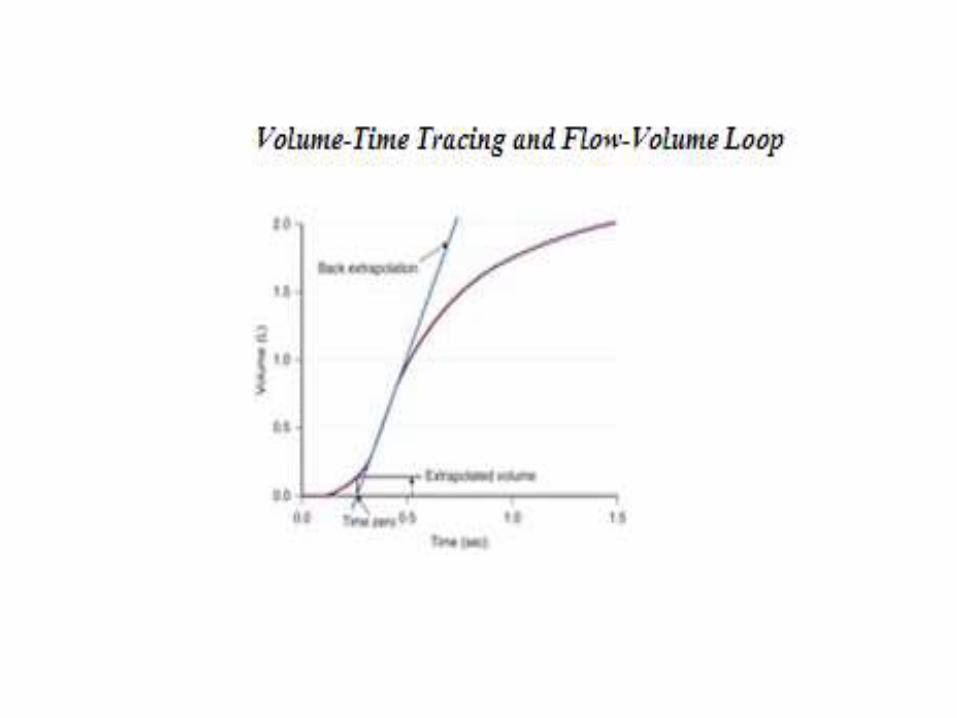
SPIROMETRY
• Volume-time tracing.
• Flow-volume tracing.
Asthma:
Treatment options & guidelines
Goals of Treatment of Asthma
• In spite of Immunotherapy, No real hope for cure of Bronchial Asthma.
But
• Treatment can achieve Asthma control and decrease exacerbations.
• No asthma attacks
• No emergency visits
• Minimal need for quick relief (as needed) ß2-agonist
• Maintain normal physical activity including exercNo chronic
symptoms ise
• Maintain lung function as close to normal as possible
• Minimal (or no) adverse effects from medicine
GINA Guidelines 2010
Treatment objectives
Domains of Asthma Control
Impairment of Function :
1- Subjective Impairment:
- Frequency and intensity of symptoms.
- Limitations of daily activities.
2- Objective Impairment:- Variations and Severity of Impairment of lung function.
Future risk:- Likelihood of exacerbations.
- Progressive loss of lung function.
- Adverse effects from medications.
Control of airway inflammation
BMJ. 2006 Apr 1; 332(7544): 767–771
fumarate
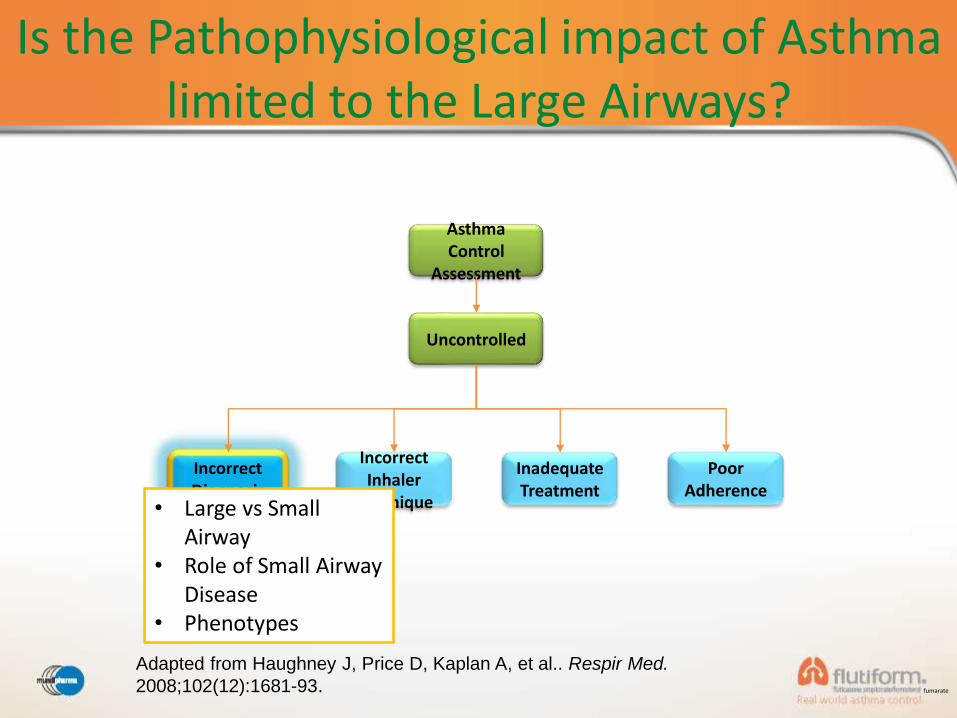
Is the Pathophysiological impact of Asthma limited to the Large Airways?
Adapted from Haughney J, Price D, Kaplan A, et al.. Respir Med.
2008;102(12):1681-93.
Asthma Control
Assessment
Uncontrolled
Incorrect Diagnosis
Incorrect Inhaler
Technique
Inadequate Treatment
Poor Adherence
• Large vs Small Airway
• Role of Small Airway Disease
• Phenotypes
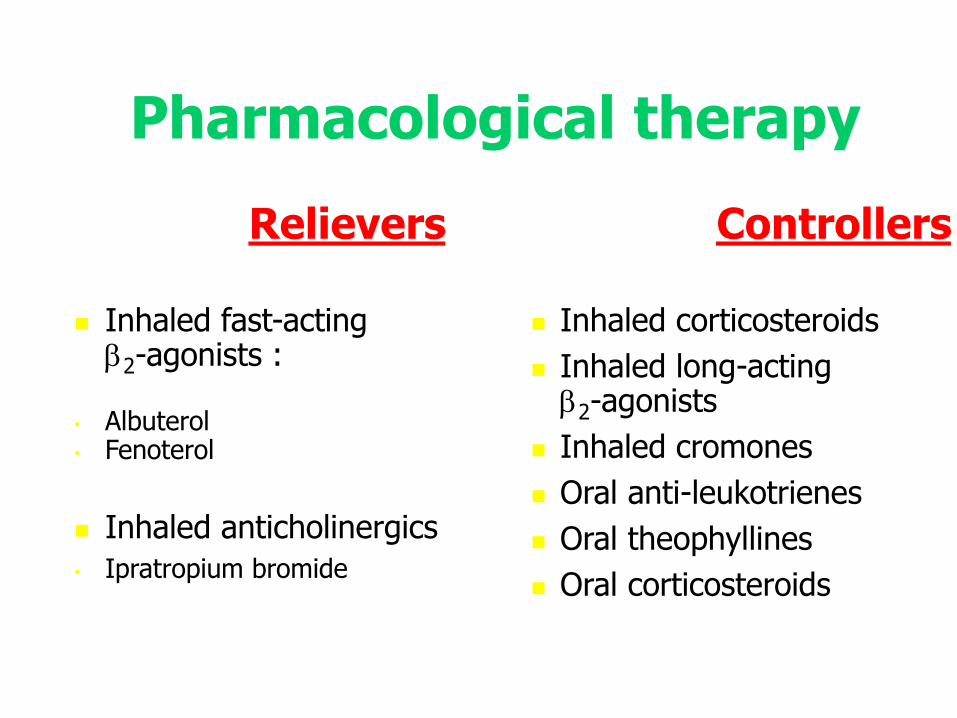
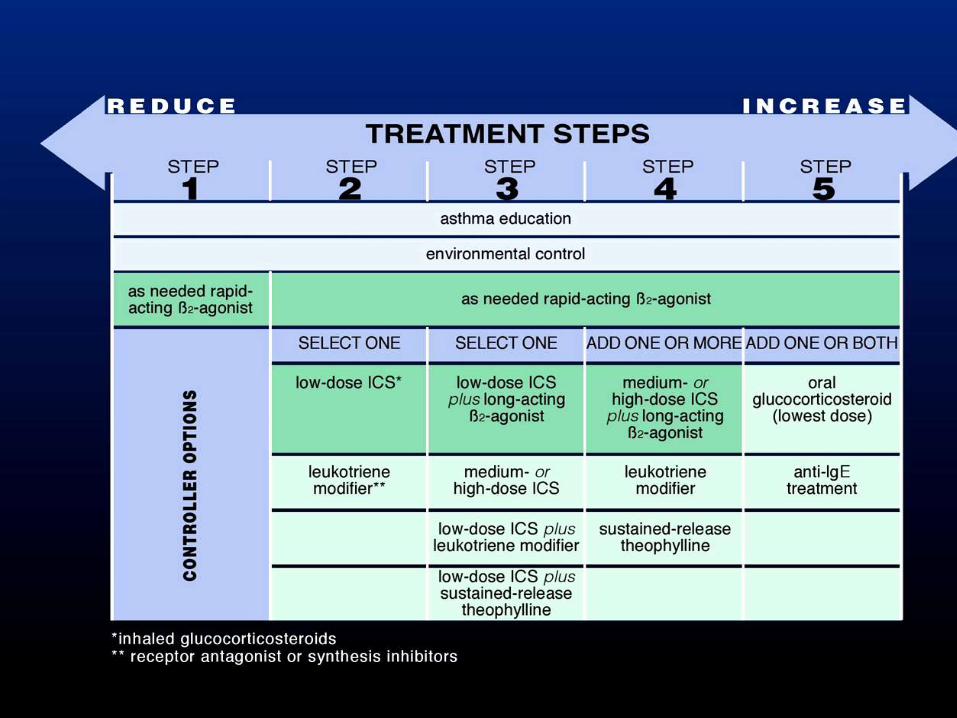
Pharmacological therapy
Controllers
Inhaled corticosteroids
Inhaled long-acting 2-agonists
Inhaled cromones
Oral anti-leukotrienes
Oral theophyllines
Oral corticosteroids
Relievers
Inhaled fast-acting 2-agonists :
• Albuterol• Fenoterol
Inhaled anticholinergics
• Ipratropium bromide
The choice of treatment should be guided by:
Level of asthma control
Current treatment
Pharmacological properties and availability of the various
forms of asthma treatment
Economic considerations
Cultural preferences and differing health care systems need to be considered
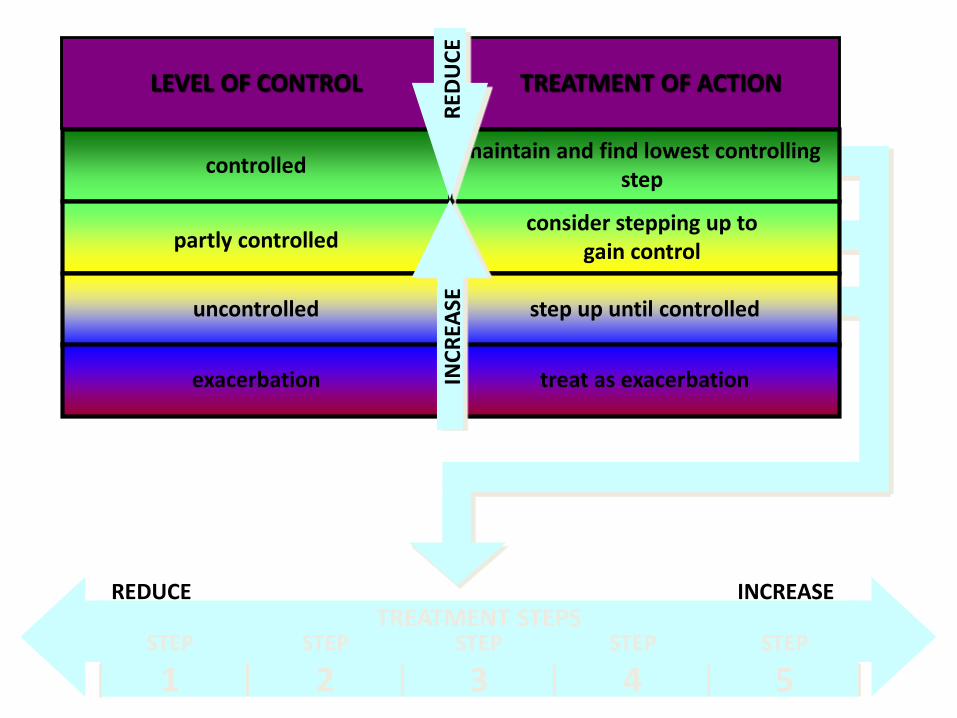
controlled
partly controlled
uncontrolled
exacerbation
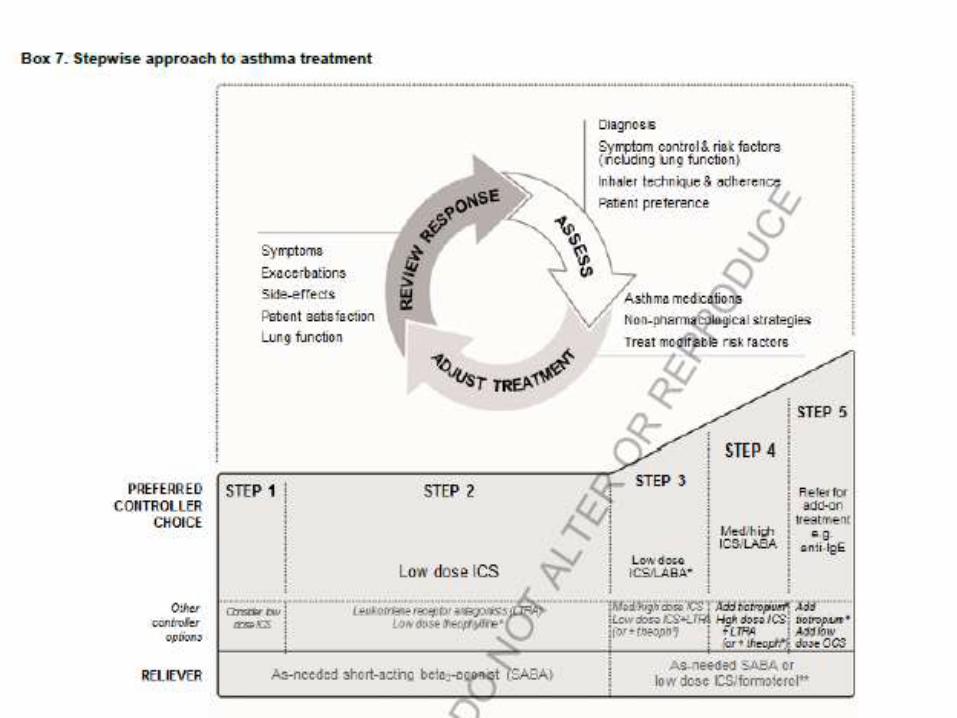
LEVEL OF CONTROL
maintain and find lowest controlling step
consider stepping up to gain control
step up until controlled
treat as exacerbation
TREATMENT OF ACTION
TREATMENT STEPSREDUCE INCREASE
STEP
1STEP
2STEP
3STEP
4STEP
5
RED
UC
EIN
CR
EASE
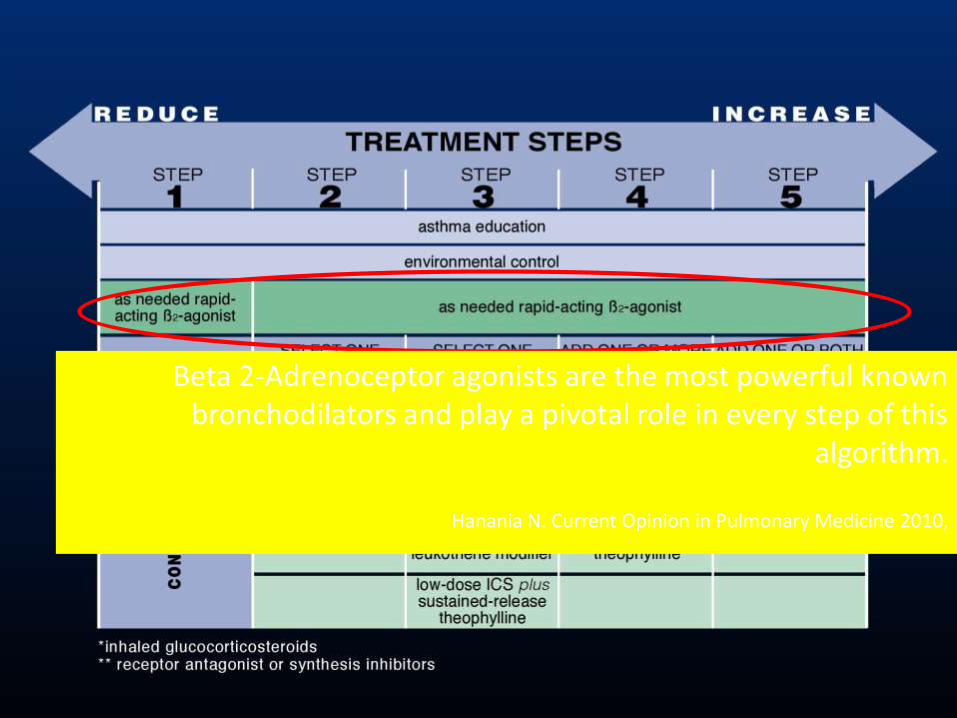
Beta 2-Adrenoceptor agonists are the most powerful known bronchodilators and play a pivotal role in every step of this
algorithm.
Hanania N. Current Opinion in Pulmonary Medicine 2010,
Review Response and Adjusting the Dose
• 2-4 weeks after starting controller therapy.
• 1-3 months regular visit.
• 4-6 weeks regular visit in Pregnancy.
• within 1 week after exacerbation.
The frequency of visits depends on:
1. Initial levelof control
2. previous response to treatment.
3. His ability and willingness to be engaged in self – management plan.
Stepping Up Treatment
• Sustained step up every 2-3 months
If symptoms persists or exacerbation in spite of 2-3 months controller therapy.
• Before stepping up consider:
1. Incorrect Inhaler Technique
2. Adherence
3. Modified risk ( Smoking)
4. Symptoms of comorbid condition(AR,GERD)
Day to Day Adjustment
• By The Patient’s himself.
• Smart Symbicort.
Stepping Down Approach
• When Asthma is controlled Well.
• Asthma controlled achieved for 3 months.
• You aim to find the lowest dose of treatment that maintain:
1. symptoms free
2. no exacerbation
3. minimize side effects.

Step down Technique
• Appropriate Timing ( no infection ,no travell no Pregnancy).
• Document the baseline , symptoms and PFT.
• Reduce ICS dose by 20-50% EVRY 2-3 months
Treating Modifiable Risk Factoers• Decrease Exacerbation Risk by
optimizing medications.
• Self monitoring of symptoms and by using PEF.
• Avoid Tobacco smoke Exposure.
• Confirmed Food Allergy: Avoidance and availability of Epinephrine.
• For Severe Asthma : Refer to especial centre.
Asthma Exacerbation
• Exacerbations of asthma are episodes of progressive increase in shortness of breath, cough, wheezing, or chest tightness
• Exacerbations are characterized by decreases in expiratory airflow that can be quantified and monitored by measurement of lung function (FEV1 or PEF)
• Severe exacerbations are potentially life-threatening and treatment requires close supervision
Asthma Exacerbations Management
Primary therapies for exacerbations:
• Repetitive administration of rapid-acting inhaled β2-
agonist
• Early introduction of systemic glucocorticosteroids.
• Oxygen supplementation
Closely monitor response to treatment with serialmeasures of lung function
GINA Guidelines 2010
Non Pharmacological Strategies and interventions• Smoking Cessation Advice.
• Regular Physical Activities.
• Avoid NSAIDs and Aspirin.
• Occupational Asthma.

Treatment in special Population’s contexts
• Pregnancy
• Elderly
• Allergic Rhinitis and Sinusitis
• Obesity
• GERD
• Anxiety
• Aspirin induced Respiratory distress.
Identifying patients at high risk of Asthma related death
• Asthma needed Intubation and Ventilations.
• Asthma Hospitalization or ICU care for Asthma in the last 12 months.
• Currently not on ICS or poor inhaler adhirence.
• currently using or recently stopping OCS.
• Over use of SABA more than canister/month
• Lack of written Asthma action plan.
• confirmed food aleergy.