Brock Syndrome

of 18
-
Upload
srishti-jain -
Category
Documents
-
view
216 -
download
0
Transcript of Brock Syndrome
-
8/7/2019 Brock Syndrome
1/18
introduction
Background
Right middle lobe syndrome (RMLS) generally refers to atelectasis in the right middle lobe of the
lung. It is caused by various etiologies and has no consistent clinical definition. Right middle lobe
syndrome is characterized by a wedge-shaped density that extends anteriorly and inferiorly
from the hilum of the lung, which is best visualized using lateral chest radiography.
Lateral view chest radiograph of Media file 1 showing a wedge-shaped density extending from the
hilum anteriorly and inferiorly.
This condition is most common in children with a history of asthma or atopy. Although the
mechanism by which asthma leads to lobar atelectasis is unknown, associated inflammation,
bronchospasm, and secretions that cause mucus plugging are likely major contributors.
-
8/7/2019 Brock Syndrome
2/18
Management is determined by etiology, and most patients respond to medical therapy alone.
P athophysiology
Certain anatomical characteristics make the right middle lobe susceptible to transient obstruction as
a result of inflammation or edema. The narrow diameter of the lobar bronchus and acute take-
off angle create poor conditions for drainage. Relative anatomical isolation of the middle lobe
and poor collateral ventilation decrease the chance of reinflation once atelectasis occurs.
Bronchial obstruction can result from extrinsic compression as in hilar lymphadenopathy or
tumor of neoplastic origin; however, atelectasis in children usually results from a process such
as asthma-associated edema and inflammation. Foreign body aspiration into the right middle
lobe orifice can also predispose to collapse of the lobe.
FrequencyUnited States
The precise incidence in children is unknown. Right middle lobe syndrome is widely underdiagnosed
and frequently unrecognized.
Mortality/Morbidity
Severity in children ranges from mild atelectasis and scarring of no consequence to severe
bronchiectasis requiring surgical resection.
Sex
Right middle lobe syndrome has been said to occur twice as often in girls than in boys; however,
large epidemiologic studies are lacking.
Age
Symptoms begin in early childhood, usually in children aged 1-2 years. Symptom frequency
decreases in later childhood, but the interval between onset of symptoms and diagnosis widely
varies.
Clinical
History
y The most common symptoms in right middle lobe syndrome (RMLS) include the following:
o P ersistent or recurrent cough
o Intermittent wheezing
o Dyspnea
-
8/7/2019 Brock Syndrome
3/18
o H istory of recurrent or chronic pneumonia (May often be a misinterpretation of the
radiographic findings)
y In many cases, these respiratory symptoms are refractory to normal treatment.
y At least half of the patients report a history of asthma or atopy, and one third report a family
history of atopy.
y Less frequently reported symptoms, which may be indicative of chronic disease with
suppurative complications, include the following:
o Hemoptysis
o Low-grade fever
o Fatigue
o W eight loss
o Chest pain
P hysical
y Right middle lobe syndrome is essentially a radiographic diagnosis, and physical findings widely
vary.
y Auscultation of the lungs may reveal a fine wheeze, rales, or diffuse rhonchi, ranging from
decreased aeration and dullness to percussion in the region of the right middle lobe. The right
middle lobe is anterior, best heard at the nipple. The medial segment is located medial to the
nipple; the lateral segment is lateral to the nipple. Failure to listen to this area results in failure
to hear the right middle lobe.
y Clubbing is rarely found in patients with advanced disease.
Causes
y Intra-airway origin
o In children, right middle lobe syndrome is usually secondary to primary ventilation
disorders. Chronic inflammation of the airways, which contributes to atelectasis of the
right middle lobe, is present. A paucity of collateral ventilation is observed in children
and serves to prevent reinflation.
o P rimary disorders of ventilation include the following:
Asthma
Bronchopulmonary dysplasia
Chronic pneumonia or bronchitis
Cystic fibrosis
-
8/7/2019 Brock Syndrome
4/18
O ther chronic lung diseases caused by aspiration or gastroesophageal reflux
P rimary ciliary dyskinesia (immotile cilia syndrome)
o Airway foreign body aspiration
o Endobronchial tumors
o Mucous plugging, as from any of the above
o G ranulation tissue
y Extra-airway origin
o Extraluminal compression is caused by the following:
Cardiovascular anomalies
Congenital malformations such as situs inversus and other anatomical defects
such as anomalous branching or abnormal diameter, length, or structure of the
bronchi Lymphadenopathy of peribronchial nodes
Tumors
Traction diverticula of the esophagus
y Infectious etiologies
o W hether the infection is a cause of the collapse or a result of airway stasis and poor
clearance may not be clear.
o P rimary infectious etiology is more frequent in adults; however, one pediatric study
found that 50% of children with collapsed right middle lobe had an underlying bacterial
infection. [1 ]
o Infectious causes also increase in frequency among immunocompromised patients.
o Common bacterial causes in children include Streptococcus
pneumoniae and Haemophilus influenzae .
o Fungal causes include histoplasmosis, blastomycosis, and aspergillosis, which manifest
as allergic bronchopulmonary aspergillosis (A P BA).
o Mycobacteria, including My cobacterium tuberculosis , My cobacterium avium-
intracellulare , and My cobacterium fortuitum have also been identified as causal agents.
o O ccurrence is mainly caused by extrinsic compression by hilar lymph nodes, which are
commonly observed in these infections as well as in fungal infections.
D ifferential D iagnoses
P neumonia
-
8/7/2019 Brock Syndrome
5/18
O ther P roblems to Be Considered
Diagnosis of right middle lobe syndrome (RMLS) is mainly based on the presence of atelectasis of
the right middle lobe of long duration. Rule out acute right middle lobe pneumonia with repeat
chest radiography within 3-4 weeks of initial onset.
Workup
Laboratory Studies
The following studies may be indicated in right middle lobe syndrome (RMLS):
y P urified protein derivative (tuberculin) skin test
y CBC count and differential
y W estergren sedimentation rate
y Fungal serology by complement fixation and immune diffusion
y Q uantitative immunoglobulins panel
Imaging Studies
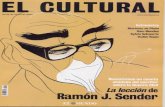
y Chest radiography with anteroposterior (A P ) and lateral views
o The classic finding of right middle lobe syndrome is a blurred right heart border and a
loss of volume in the right middle lobe (see Media file 1).
P osteroanterior chest radiograph demonstrating right middle lobe collapse and infiltrate. Note
blurred right heart border.
-
8/7/2019 Brock Syndrome
6/18
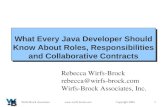
o A wedge-shaped density extending from the hilum anteriorly and inferiorly is best
visualized on a lateral view (see Media file 2).
Lateral view chest radiograph of Media file 1 showing a wedge-shaped density extending from the
hilum anteriorly and inferiorly.
o Consolidation and infiltration are less commonly observed.
o Acute pneumonia should clear radiologically in 6-8 weeks.
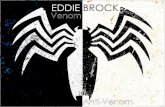
y CT scanning
o If bronchiectasis is suspected, confirm diagnosis by performing high-resolution chest CT
scanning (see Media file 3), which carries less risk to younger patients or patients with
asthma than the seldom-used traditional bronchography.
-
8/7/2019 Brock Syndrome
7/18
Chest CT scan showing extensive bronchiectasis of both medial and lateral segments of the right
middle lobe.
o H igh-resolution chest CT imaging is also helpful for follow-up medical therapy.
O ther Tests
y P ulmonary function tests ( P FTs) can be used to establish a previously unidentified asthmatic
component.
y Although findings on a baseline forced expiratory volume in one second (F EV1) may be normal, a
prebronchodilator and postbronchodilator study with 10-15% changes in F EV1 is diagnostic for
asthma.
P rocedures
y The value of bronchoscopy is 2-fold, as follows:
o It is immediately therapeutic in removing mucus and clearing the airway and can be
curative in some cases.
o It allows visualization of the airway and the ability to determine patency of the rightmiddle lobe bronchus and to discern whether endobronchial obstruction is the cause.
y Bronchoalveolar lavage can be concurrently performed to determine cellular elements in the
right middle lobe. It can also be used to assess the presence of infections by culturing and
staining for bacterial, fungal, viral, and mycobacterial pathogens.
Treatment
-
8/7/2019 Brock Syndrome
8/18
Medical Care
y Long-term follow-up of children with right middle lobe syndrome (RMLS) shows that most
patients do not experience recurrent or persisting symptoms. This indicates that the first line of
treatment in all cases is conservative medical management, except in cases involving neoplastic
origin and those with bronchiectasis.
y Chest physical therapy and postural drainage are the hallmarks of therapy.
o Treat the asthmatic child with aggressive anti-inflammatory therapy such as inhaled
steroids. Consider systemic steroids. Guidelines for the diagnosis and management of
asthma have been established. [2 ]
o P rovide the patient with chest physical therapy and postural drainage. In unresponsive
patients or patients who have a predisposition to airway colonization, an appropriate
antibiotic, as determined by a bronchoalveolar lavage (BAL) culture, should be added totheir regimen.
y P atients with fungal infections (eg, histoplasmosis) or tuberculous infections who have hilar
adenopathy and complete blockage of their right middle lobe should be treated aggressively.
The addition of systemic corticosteroids may be necessary.
Surgical Care
y Lobectomy
o Lobectomy is indicated in cases of malignancy and bronchiectasis that are unresponsive
to medical therapy.
o O nly perform lobectomy when right middle lobe syndrome is associated with systemic
symptoms such as failure to thrive, persistent cough, and recurrent fever or when
chronic infection threatens the remainder of the lung.
y Bronchography: Avoid bronchography because of potential risks to the patient unless surgery is
seriously considered; therefore, always explore high-resolution CT imaging as an alternative.
Medication
The role of antibiotic therapy in the treatment of right middle lobe syndrome (RMLS) is not well
studied. Antibiotics are usually administered during acute exacerbations and when
bronchiectasis is well established. In this latter instance, long-term rotation of antibiotics (ie, 3
weeks on and 1 week off, then change antibiotic) is advocated. Base the choice of antibiotic on
culture and sensitivity results of either sputum or bronchoaveolar lavage (BAL) fluid. W hen this
is not available, select a broad-spectrum antibiotic to cover S pneumoniae, other streptococci, H
-
8/7/2019 Brock Syndrome
9/18
influenzae, and M oraxella catarrhalis. Antibiotics can be orally or intravenously administered.
The use of nebulized antibiotics has not been studied in right middle lobe syndrome. Also see
Asthma for relevant treatment information.
Antibiotics
Empiric antimicrobial therapy must be comprehensive and should cover all likely pathogens in the
context of the clinical setting.
Cefuroxime (Ceftin, Zinacef)
Second-generation cephalosporin maintains gram-positive activity that first-generation
cephalosporins have; adds activity against P roteus mirabilis, H influenzae, Escherichia coli,
Klebsiella pneumoniae, and M catarrhalis. D osing
Adult
500 mg PO bid
750 mg to 2 g I V q8h
P ediatric
30 mg/kg/d PO divided q12h
75-150 mg/kg/d I V divided q8h; not to exceed 6 g/d
Interactions
Disulfiramlike reactions may occur when alcohol is consumed within 72 h after taking cefuroxime;
may increase hypoprothrombinemic effects of anticoagulants; may increase nephrotoxicity in
patients receiving potent diuretics such as loop diuretics; coadministration with aminoglycosides
increase nephrotoxic potential
Contraindications
Documented hypersensitivity
P recautions
P regnancy
B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
P recautions
Administer half dose if creatinine clearance is 10-30 mL/min and one-quarter dose if less than 10
mL/min; fungal and microorganism overgrowth may occur with prolonged therapy
-
8/7/2019 Brock Syndrome
10/18
Cefpodoxime proxetil (Vantin)
Inhibits bacterial cell wall synthesis by binding to one or more of the penicillin-binding proteins;
bacteria eventually lyse because of ongoing activity of cell wall autolytic enzymes while cell wall
assembly is arrested.
D osing
Adult
100-400 mg PO q12h
P ediatric
10 mg/kg/d PO divided q12h; not to exceed 400 mg/d
Interactions
P robenecid increases effect; coadministration with furosemide and aminoglycosides increases
nephrotoxic effects
Contraindications
Documented hypersensitivity
P recautions
P regnancy
B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
P recautions
Caution with documented hypersensitivity to penicillins
Cefprozil (Cefzil)
Binds to one or more of the penicillin-binding proteins, which, in turn, inhibits cell wall synthesis and
results in bactericidal activity.
D osing
Adult
250-500 mg PO divided q12h
P ediatric
7.5-15 mg/kg/dose PO q12h
Interactions
-
8/7/2019 Brock Syndrome
11/18
P robenecid increases effect; coadministration with furosemide and aminoglycosides increases
nephrotoxic effects
Contraindications
Documented hypersensitivity
P recautions
P regnancy
B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
P recautions
Adjust dosage in renal impairment
Erythromycin and sulfisoxazole (P
ediazole)Erythromycin is a macrolide antibiotic with a large spectrum of activity. Erythromycin binds to the
50S ribosomal subunit of the bacteria, which inhibits protein synthesis.
Sulfisoxazole expands erythromycin's coverage to include gram-negative bacteria. Sulfisoxazole
inhibits bacterial synthesis of dihydrofolic acid by competing with para-aminobenzoic acid.
D osing
Adult
400 mg erythromycin and 1200 mg sulfisoxazole PO q6h
P ediatric
40-50 mg/kg/d (erythromycin component) PO divided q6-8h; not to exceed 2 g/d of erythromycin or
6 g/d of sulfisoxazole
Interactions
Decreases clearance of terfenadine (recalled from US market) , cisapride and astemizole (recalled
from US market) , which may result in serious cardiac arrhythmias; decreases clearance of
cyclosporin, midazolam, phenytoin, triazolam, and theophylline; increases the toxicity of
warfarin and ergotamine
Contraindications
Documented hypersensitivity; hepatic impairment; concomitant administration of terfenadine,
cisapride, and astemizole; G -6-PD deficiency; infants
-
8/7/2019 Brock Syndrome
12/18
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if
benefits outweigh risk to fetus
P recautions
Caution in liver disease; G I adverse effects are common (administer doses pc); discontinue use if
nausea, vomiting, malaise, abdominal colic, or fever occur
Azithromycin (Zithromax)
Inhibits bacterial growth, possibly by blocking dissociation of peptidyl tRNA from ribosomes, causing
RNA-dependent protein synthesis to arrest.
D osing
AdultDay 1: 500 mg/d PO
Days 2-5: 250 mg/d PO
P ediatric
Day 1: 10 mg/kg PO once; not to exceed 500 mg/d
Days 2-5: 5 mg/kg PO qd; not to exceed 250 mg/d
Interactions
May increase toxicity of theophylline, warfarin, and digoxin; effects are reduced with
coadministration of aluminum and/or magnesium antacids; nephrotoxicity and neurotoxicity
may occur when coadministered with cyclosporine
Contraindications
Documented hypersensitivity; hepatic impairment; administration with pimozide
P recautions
P regnancy
B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
P recautions
Site reactions can occur with I V route; bacterial or fungal overgrowth may result with prolonged
antibiotic use; may increase hepatic enzymes and cholestatic jaundice; caution in patients with
impaired hepatic function, prolonged Q T intervals, or pneumonia
-
8/7/2019 Brock Syndrome
13/18
Clarithromycin (Biaxin)
Inhibits bacterial growth, possibly by blocking dissociation of peptidyl tRNA from ribosomes, causing
RNA-dependent protein synthesis to arrest.
D osing
Adult
250-500 mg PO q12h
P ediatric
15 mg/kg/d PO divided bid
Interactions
Toxicity increases with coadministration of fluconazole, astemizole (recalled from US market) ,
terfenadine (recalled from US market) , and pimozide; clarithromycin effects decrease and G I
adverse effects may increase with coadministration of rifabutin or rifampin; may increasetoxicity of anticoagulants, cyclosporine, tacrolimus, digoxin, omeprazole, carbamazepine, ergot
alkaloids, triazolam, and HMG CoA-reductase inhibitors; serious cardiac arrhythmias may occur
with coadministration of cisapride; plasma levels of certain benzodiazepines may increase,
prolonging CNS depression; arrhythmias and increase in Q Tc intervals occur with disopyramide;
coadministration with omeprazole may increase plasma levels of both agents
Contraindications
Documented hypersensitivity; coadministration of pimozide, astemizole, cisapride, and terfenadine
P recautions
P regnancy
C - Fetal risk revealed in studies in animals but not established or not studied in humans; may use if
benefits outweigh risk to fetus
P recautions
Coadministration with ranitidine or bismuth citrate is not recommended with CrCl
-
8/7/2019 Brock Syndrome
14/18
Drug combination treats bacteria resistant to beta-lactam antibiotics. For children >3 months, base
dosing protocol on amoxicillin content. Due to different amoxicillin/clavulanic acid ratios in 250-
mg tab (250/125) vs 250 mg chewable-tab (250/62.5), do not use 250-mg tab until child weighs
>40 kg.
D osing
Adult
250-500 mg PO q8h
P ediatric
3 months: if using 200 mg/5 mL or 400 mg/5 mL susp, 45 mg/kg/d PO divided q12h; if using
125 mg/5 mL or 250 mg/5 mL suspension, 40 mg/kg/dPO
divided bid for 7-10 d>40 kg: Administer as in adults
Interactions
Coadministration with warfarin or heparin increases risk of bleeding
Contraindications
Documented hypersensitivity
P recautions
P regnancy
B - Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
P recautions
Adjust dose in renal impairment
Sulfamethoxazole and trimethoprim (Bactrim, Septra, Cotrim)
Inhibits bacterial growth by inhibiting synthesis of dihydrofolic acid.
D osing
Adult
160 mg (trimethoprim component)/800 mg (sulfamethoxazole component) PO q12h (ie, 1 double-
strength tab q12h)
P ediatric
-
8/7/2019 Brock Syndrome
15/18
2 months: 15-20 mg/kg/d (based on trimethoprim) PO divided q12h
Interactions
May increase P T when used with warfarin (perform coagulation tests and adjust dose accordingly);
coadministration with dapsone may increase blood levels of both drugs; coadministration of
diuretics increases incidence of thrombocytopenia purpura in elderly patients; phenytoin levels
may increase with coadministration; may potentiate effects of methotrexate in bone marrow
depression; hypoglycemic response to sulfonylureas may increase with coadministration; may
increase levels of zidovudine
Contraindications
Documented hypersensitivity; megaloblastic anemia due to folate deficiency; age
-
8/7/2019 Brock Syndrome
16/18
asthma who have atelectasis of the right middle lobe during an acute asthma exacerbation and
in children with acute pneumonia of the right middle lobe to document resolution.
y Recently, a more aggressive approach in a cohort of 55 symptomatic children with right middle
lobe syndrome followed for a median duration of 2 years yielded good outcome. [3 ]All these
children underwent flexible bronchoscopy at presentation, and specific antibiotic therapy was
given based on bronchial alveolar lavage fluid. Bronchiectasis was documented in 27% of
patients, and the duration of symptoms correlated with the development of this unfavorable
complication.
Complications
y Long-term complications range from none to minimal pulmonary scarring of no discernible
physiological consequence to severe bronchiectasis requiring surgical intervention.
y In children with asthma, right middle lobe syndrome may produce a vicious cycle of infection,inflammation, and asthma exacerbation.
P rognosis
y Right middle lobe syndrome resolves in approximately 33% of children after bronchoscopy.
Approximately 33% recover eventually with medical management, 22% require lobectomy, and
11% have decreased severity of symptoms but should be monitored for the possibility of
requiring lobectomy later.
y About one third of patients with right middle lobe syndrome in early childhood continue to have
symptoms in later childhood. These patients usually experience asthma symptoms or another
chronic lung condition such as cystic fibrosis. A recent study examined the efficacy of early
postnatal corticosteroids for preventing chronic lung disease in preterm infants. [4 ]
y The remaining two thirds of children with right middle lobe syndrome do not have persistent
symptoms later in adulthood.
P atient Education
y Because chest physical therapy and postural drainage are of paramount importance in the
management of RMLS, instruct the caretaker with appropriate techniques and position for right
middle lobe physiotherapy. This is often performed by a registered respiratory or physical
therapist. Regardless, the therapist should be somebody who frequently deals with children.
y Flutter valve and high-frequency oscillation (known as the vest) have not been studied in this
setting, but they may be alternative modalities of delivering chest physical therapy.
Miscellaneous
-
8/7/2019 Brock Syndrome
17/18
Medicolegal P itfalls
y The vague nature of right middle lobe syndrome (RMLS) symptoms may lead to a delay in
diagnosis. Approximately 10% of children admitted for acute asthma have atelectasis of one or
more lobes; the right middle lobe is most commonly affected. Because of the high incidence in
children with asthma, if chest radiography suggests right middle lobe atelectasis, another chest
radiograph should be obtained 3-4 weeks later to document total resolution. Early detection
and aggressive initial management may alter the course of this disease.
y Too often, right middle lobe syndrome is mistaken for an acute pneumonia and is simply treated
with antibiotics, without a follow-up radiograph. This underdiagnosis with resultant
undertreatment can be harmful to the underlying lung.
Multimedia
Media file 1: P osteroanterior chest radiograph demonstrating right middle lobe collapse and
infiltrate. Note blurred right heart border.
-
8/7/2019 Brock Syndrome
18/18
Media file 2: Lateral view chest radiograph of Media file 1 showing a wedge-shaped density
extending from the hilum anteriorly and inferiorly.
Media file 3: Chest CT scan showing extensive bronchiectasis of both medial and lateral segmentsof the right middle lobe.