British Journal of Oral and Maxillofacial Surgery 45-1-83 84 Buccal Corticotomy for Removal of...
2
British Journal of Oral and Maxillofacial Surgery 45 (2007) 83–84 Technical note Buccal corticotomy for removal of deeply impacted mandibular molars Andrew B.G. Tay ∗ Department of Oral & Maxillofacial Surgery, National Dental Centre, 5 Second Hospital Avenue, Singapore 168938, Singapore Accepted 23 December 2005 Available online 3 February 2006 Keywords: Mandibular buccal corticotomy; Sagittal split ramus osteotomy (SSRO); Deeply impacted molar; Inferior alveolar nerve (IAN) Sagittal split ramus osteotomy has been used to remove deeply impacted mandibular third molars. 1–3 The main dis- advantages of conventional operations for such teeth are the extent of bone removed, limited visibility, 1 high risk of injury to the inferior alveolar nerve, and fracture of the mandible. 2 In comparison, sagittal split ramus osteotomy gives good access, conserves bone that would otherwise have been removed, and allows the nerve to be seen and avoided. 1–3 However, the osteotomy puts the occlusion at risk (although this is rare) and there is a risk of an unfavourable split in either the proxi- mal or distal segment (2%). 4 This is about twice as high if the third molar is impacted. 4 The published incidence of distur- bance of the inferior alveolar nerve is high: as much as 58% at 6 months, and 35% at 1 year postoperatively. An alternative approach that offers access to deeply impacted mandibular teeth is by buccal corticotomy. 5 A trapezoidal mucoperiosteal flap is raised in the mandibular molar region, and a rectangular window is made over the deeply impacted tooth using a narrow fissure bur, with the mesial and distal cuts almost reaching the inferior border of the mandible (Fig. 1). The buccal corticotomy window is removed with an osteotome, and the deeply impacted molar is exposed, divided with a bur, and removed. The alveolar nerve bundle is often in close proximity and may be seen after the tooth has been removed. The bony fragment removed at buc- cal corticotomy is replaced and secured with wires or plates and screws at the mesial and distal edges, and the wound is sutured. We did this operation under general anaesthesia in two patients: a 17-year-old girl with a deeply impacted left lower ∗ Tel.: +65 6324 8817; fax: +65 6324 8899. E-mail address: [email protected]. Fig. 1. Fig. 2. 0266-4356/$ – see front matter © 2006 The British Association of Oral and Maxillofacial Surgeons. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.bjoms.2005.12.009
-
Upload
gonzalo-barrientos -
Category
Documents
-
view
70 -
download
0
Transcript of British Journal of Oral and Maxillofacial Surgery 45-1-83 84 Buccal Corticotomy for Removal of...

T
BmA
D
AA
K
daetccaoamtba
itmdmorebtcas
p
0
British Journal of Oral and Maxillofacial Surgery 45 (2007) 83–84
echnical note
uccal corticotomy for removal of deeply impactedandibular molars
ndrew B.G. Tay ∗
epartment of Oral & Maxillofacial Surgery, National Dental Centre, 5 Second Hospital Avenue, Singapore 168938, Singapore
ccepted 23 December 2005vailable online 3 February 2006
(SSRO); Deeply impacted molar; Inferior alveolar nerve (IAN)
Fig. 1.
eywords: Mandibular buccal corticotomy; Sagittal split ramus osteotomy
Sagittal split ramus osteotomy has been used to removeeeply impacted mandibular third molars.1–3 The main dis-dvantages of conventional operations for such teeth are thextent of bone removed, limited visibility,1 high risk of injuryo the inferior alveolar nerve, and fracture of the mandible.2 Inomparison, sagittal split ramus osteotomy gives good access,onserves bone that would otherwise have been removed, andllows the nerve to be seen and avoided.1–3 However, thesteotomy puts the occlusion at risk (although this is rare)nd there is a risk of an unfavourable split in either the proxi-al or distal segment (2%).4 This is about twice as high if the
hird molar is impacted.4 The published incidence of distur-ance of the inferior alveolar nerve is high: as much as 58%t 6 months, and 35% at 1 year postoperatively.
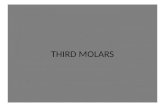
An alternative approach that offers access to deeplympacted mandibular teeth is by buccal corticotomy.5 Arapezoidal mucoperiosteal flap is raised in the mandibular
olar region, and a rectangular window is made over theeeply impacted tooth using a narrow fissure bur, with theesial and distal cuts almost reaching the inferior border
f the mandible (Fig. 1). The buccal corticotomy window isemoved with an osteotome, and the deeply impacted molar isxposed, divided with a bur, and removed. The alveolar nerveundle is often in close proximity and may be seen after theooth has been removed. The bony fragment removed at buc-al corticotomy is replaced and secured with wires or platesnd screws at the mesial and distal edges, and the wound is
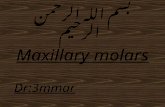
utured.We did this operation under general anaesthesia in twoatients: a 17-year-old girl with a deeply impacted left lower
∗ Tel.: +65 6324 8817; fax: +65 6324 8899.E-mail address: [email protected]. Fig. 2.
266-4356/$ – see front matter © 2006 The British Association of Oral and Maxillofacial Surgeons. Published by Elsevier Ltd. All rights reserved.doi:10.1016/j.bjoms.2005.12.009

84 A.B.G. Tay / British Journal of Oral and Ma
Fig. 3.
sdtcccspopa
R
1
2
3
4. Mehra P, Castro V, Freitas RZ, Wolford LM. Complications of themandibular sagittal split ramus osteotomy associated with the presenceor absence of third molars. J Oral Maxillofac Surg 2001;59:854–8.
5. Miloro M. Surgical access for inferior alveolar nerve repair. J Oral Max-illofac Surg 1995;53:1224–5.
xillofacial Surgery 45 (2007) 83–84
econd molar (Figs. 2 and 3), and a 12-year-old boy with aeeply impacted left lower first molar and a complex odon-ome in place of the left lower second molar. In both casesomputed tomograms showed the location of the mandibularanal in relation to the deeply impacted teeth and the buc-al cortex. The deeply impacted teeth (and odontome in theecond case) were completely removed piecemeal and bothatients recovered well and showed evidence of bony healingn radiography 6 months later. The second patient had mildaraesthesia of his left lower lip and chin, which resolvedfter a month.
eferences
. Jones TA, Garg T, Monaghan A. Removal of a deeply impacted mandibu-lar third molar through a sagittal split ramus osteotomy approach. Br JOral Maxillofac Surg 2004;42:365–8.
. Amin M, Haria S, Bounds G. Surgical access to an impacted lower thirdmolar by sagittal splitting of the mandible: a case report. Dent Update1995;22:206–8.
. Toffanin A, Zupi A, Cicognini A. Sagittal split osteotomy in removal ofimpacted third molar. J Oral Maxillofac Surg 2003;61:638–40.