Brief Reports Out_2001
39
Brief Reports LIGHTNING–INDUCED CATARACT AND NEURORETINOPATHY CHANGXIAN YI, MD, YUANGBO LIANG, MD, OU JIEXIONG, MD, HONG YAN, MD From the Zhongshan Ophthalmic Center, Sun Yat-sen University of Medical Science, Guangzhou, China. The mechanism of injury from lightning strike is not exactly understood, although heating, direct strike, blunt injuries, voltage, resistance, pathway, and dura- tion 1 have been considered the most important factors. Various mechanisms may lead to different types of damage. We report here a case with a special neuro- retinopathy that caused retinal edema around the pa- pilla and not prominently on the macula. The damage may also involve the optic nerve, which may explain the unfavorable visual recovery. Case Report A 32-year-old man was struck by lightning while working in a field. He lost consciousness and woke up a few hours later with no vision, which lasted for several days. Ten days later, he was transferred to our department with visual acuity of hand motions at 10 cm in the right eye and 20/200 in the left. Intraocular pressure was 17 mmHg in the right and 20 mmHg in the left eye. There was some slight opacity both in subanterior and subposterior capsule of lens in both eyes (Figure 1). The conjunctiva, cornea, and anterior chamber were unremarkable. The posterior vitreous seemed to have more cells and the right eye was particularly hazy. The right fundus was vague (Figure 2A), but it was still possible to observe the change of the retina. The boundary of the papilla was clear and peripapillary retina was clearly white, indicating retinal edema. The ratio of diameters of the arteriole and vein at the optic disk border was 2:3. No exudate or bleeding was observed. The left fundus was clearly better with no obvious edema (Figure 2B). Some mild retinal folds similar to the macular retinoschisis could be recognized. Peripheral retina and vessels were ophthalmoscop- ically normal in both eyes. Findings of scotopic and photopic electroretinography (ERG) were abnormal in both eyes (Figure 3). In the right eye, the scotopic blue flicker ERG was extinguished and the scotopic white 30-Hz flicker ERG was reduced in amplitude. In the left eye, both the photopic and scotopic ERG were reduced in amplitude. Pattern visual evoked response (PVER) was normal on the left side but of reduced amplitude on the right side (Figure 4). Examination with ERG, visual evoked potentials, and the unfavorable visual recovery indicated a combined injury of retina and optic nerve. There were no previous ocular diseases recorded and the patient believes that he had good vision until this happened. The systemic and laboratory examinations were unremarkable. After admission to the hospital, 50 mg of prednisone per day was given for 4 days. The adjunctive therapy included vitamins E and C; injection of vitamin B complex solution, which contains vita- mins B1, B6, and B12; adenosine triphosphate; and inosine, to- gether with some Chinese traditional medicine, such as panax notoginsang saponins, which was deemed to enhance the micro- circulation of optic nerve. Two days after treatment, vision was hand motions at 20 cm in the right eye and 20/100 in the left eye. Three days later, the right eye had a vision of 20/200 and the left 20/100, which remained unchanged until discharge from hospital 17 days later. Discussion Lightning injury has been associated with cataract, uveitis, punctate keratitis, cystic macular edema, and macular hole, 1 but to our knowledge retinal lesions centered in the optic nerve with an obvious discrep- ancy between the eyes has not been reported. Several points drew our attention. First, the cataract was formed in both eyes, whereas the lesion on the two fundi was very different, which may imply that the direction of the lightning strike could play an impor- tant role in fundus pathologic change. The retinal lesion was prominent on the right side but minimal on the left eye. Second, the lesion that showed retinal edema surrounding the optic disk was obvious; how- ever, the papilla had no swelling. It is difficult to evaluate ophthalmoscopically the damage to the optic nerve; however, according to the ERG, PVER, and the unfavorable visual recovery, we may conclude that the optic nerve was severely injured, in addition to the retinal damage. Third, with such heavy injury of the optic nerve and surrounding retina, the macula seem- ingly was spared. There have been several reports of macular lesions caused by lightning. 2,3 Because of the high content of melanin granules of retinal pigment The authors have no proprietary interest in the contents of this article. Reprint requests: Changxian Yi, MD, Zhongshan Ophthalmic Center, Sun Yat-sen University of Medical Science, 510060 Guangzhou, PR China; e-mail: [email protected] RETINA,™ The Journal of Retinal and Vitreous Diseases, encourages authors to submit Brief Reports describing unusual findings, new techniques, and new instruments. Material submitted for consideration in this section of the journal is done so with the assumption that the data provided do not duplicate previously published material and that the material has not been submitted for consideration elsewhere. Each author must sign a disclosure to this effect (see Instructions to Authors for complete wording of transfer letter). Brief Reports submitted for this section of the journal may be subjected to the standard review process that is applied to other material submitted to RETINA. Brief Reports should follow the requirements listed in the Instructions to Authors, with the following caveats: Brief Reports should not exceed 4 pages in length; no more than 5 references should be cited; and each Brief Report should include no more than 4 figures. 526
Transcript of Brief Reports Out_2001

Brief Reports
LIGHTNING–INDUCED CATARACT ANDNEURORETINOPATHY
CHANGXIAN YI, MD, YUANGBO LIANG, MD,OU JIEXIONG, MD, HONG YAN, MD
From the Zhongshan Ophthalmic Center, Sun Yat-senUniversity of Medical Science, Guangzhou, China.
The mechanism of injury from lightning strike is notexactly understood, although heating, direct strike,blunt injuries, voltage, resistance, pathway, and dura-tion1 have been considered the most important factors.Various mechanisms may lead to different types ofdamage. We report here a case with a special neuro-retinopathy that caused retinal edema around the pa-pilla and not prominently on the macula. The damagemay also involve the optic nerve, which may explainthe unfavorable visual recovery.
Case Report
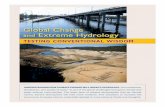
A 32-year-old man was struck by lightning while working in afield. He lost consciousness and woke up a few hours later with novision, which lasted for several days. Ten days later, he wastransferred to our department with visual acuity of hand motions at10 cm in the right eye and 20/200 in the left. Intraocular pressurewas 17 mmHg in the right and 20 mmHg in the left eye. There wassome slight opacity both in subanterior and subposterior capsule oflens in both eyes (Figure 1). The conjunctiva, cornea, and anteriorchamber were unremarkable. The posterior vitreous seemed tohave more cells and the right eye was particularly hazy.
The right fundus was vague (Figure 2A), but it was still possibleto observe the change of the retina. The boundary of the papilla wasclear and peripapillary retina was clearly white, indicating retinaledema. The ratio of diameters of the arteriole and vein at the opticdisk border was 2:3. No exudate or bleeding was observed. The leftfundus was clearly better with no obvious edema (Figure 2B).Some mild retinal folds similar to the macular retinoschisis couldbe recognized. Peripheral retina and vessels were ophthalmoscop-ically normal in both eyes.
Findings of scotopic and photopic electroretinography (ERG)were abnormal in both eyes (Figure 3). In the right eye, the
scotopic blue flicker ERG was extinguished and the scotopic white30-Hz flicker ERG was reduced in amplitude. In the left eye, boththe photopic and scotopic ERG were reduced in amplitude. Patternvisual evoked response (PVER) was normal on the left side but ofreduced amplitude on the right side (Figure 4). Examination withERG, visual evoked potentials, and the unfavorable visual recoveryindicated a combined injury of retina and optic nerve.
There were no previous ocular diseases recorded and the patientbelieves that he had good vision until this happened.
The systemic and laboratory examinations were unremarkable.After admission to the hospital, 50 mg of prednisone per day was
given for 4 days. The adjunctive therapy included vitamins E andC; injection of vitamin B complex solution, which contains vita-mins B1, B6, and B12; adenosine triphosphate; and inosine, to-gether with some Chinese traditional medicine, such as panaxnotoginsang saponins, which was deemed to enhance the micro-circulation of optic nerve.
Two days after treatment, vision was hand motions at 20 cm inthe right eye and 20/100 in the left eye. Three days later, the righteye had a vision of 20/200 and the left 20/100, which remainedunchanged until discharge from hospital 17 days later.
Discussion
Lightning injury has been associated with cataract,uveitis, punctate keratitis, cystic macular edema, andmacular hole,1 but to our knowledge retinal lesionscentered in the optic nerve with an obvious discrep-ancy between the eyes has not been reported. Severalpoints drew our attention. First, the cataract wasformed in both eyes, whereas the lesion on the twofundi was very different, which may imply that thedirection of the lightning strike could play an impor-tant role in fundus pathologic change. The retinallesion was prominent on the right side but minimal onthe left eye. Second, the lesion that showed retinaledema surrounding the optic disk was obvious; how-ever, the papilla had no swelling. It is difficult toevaluate ophthalmoscopically the damage to the opticnerve; however, according to the ERG, PVER, and theunfavorable visual recovery, we may conclude thatthe optic nerve was severely injured, in addition to theretinal damage. Third, with such heavy injury of theoptic nerve and surrounding retina, the macula seem-ingly was spared. There have been several reports ofmacular lesions caused by lightning.2,3 Because of thehigh content of melanin granules of retinal pigment
The authors have no proprietary interest in the contents of thisarticle.
Reprint requests: Changxian Yi, MD, Zhongshan OphthalmicCenter, Sun Yat-sen University of Medical Science, 510060Guangzhou, PR China; e-mail: [email protected]
RETINA,™ The Journal of Retinal and Vitreous Diseases,encourages authors to submitBrief Reports describing unusual findings, newtechniques, and new instruments. Material submitted for consideration in this section of the journal is done so with the assumption that thedata provided do not duplicate previously published material and that the material has not been submitted for consideration elsewhere. Eachauthor must sign a disclosure to this effect (see Instructions to Authors for complete wording of transfer letter). Brief Reports submitted forthis section of the journal may be subjected to the standard review process that is applied to other material submitted toRETINA . BriefReports should follow the requirements listed in the Instructions to Authors, with the following caveats: Brief Reports should not exceed 4pages in length; no more than 5 references should be cited; and each Brief Report should include no more than 4 figures.
526

epithelium, macula injury was much more frequentlyobserved. The changes include macular edema, mac-ular hole, and retinal pigment epithelium damage. Inthis patient, however, the retinal injury is not centeredin macula but optic nerve. Therefore the mechanismthat occurred in this patient might be different fromthe thermal damage as proposed in the previous re-ports.1–4The exact mechanism is unclear. There couldbe various explanations. There may have been retinalwhitening that extended around the macular regionand was absorbing 10 days later. There may have beenan occlusion of the vessels owing to acute swelling inthe optic head or for other reasons, such as transientvascular incompetence leading to the accumulation ofextracellular fluid in the macula or a kind of bluntinjury or blunt injury–associated mechanism such asshake wave. The retina surrounding the optic nerve is
Fig. 1. Color photograph of the lens, right eye.A, Mild opacity at subanterior capsule.B, Subposterior capsule opacity.
Fig. 2. Color photograph of the fundus.A, Vague appearance of the fundus owing to cataract and slightly hazy vitreous. Marked retinal edemasurrounds the optic disk. Macular foveal reflex was not visible; however, there was no obvious edema, hole, or other severe damage in the fovea.B,The left fundus was clearly visible. No edema was observed; however, mild macular fold was visible.
Fig. 3. Scotopic and photopic electroretinography (ERG) were abnor-mal in both eyes.A, The scotopic blue flicker ERG was extinguishedin the right eye.B, The scotopic white 30-Hz flicker ERG was reducedin amplitude in the right eye. The photopic (C) and scotopic (D) ERGwere reduced in amplitude in the left eye.
527BRIEF REPORTS

relatively thicker than other parts of the fundus, whichis more subject to contusion-like damage. However,there also may be combined strong voltage, whichinsulted the optic nerve; therefore, visual recoverywas uncertain. This case of lightning injury on fundusdemonstrates that lightning damage could predomi-nantly happen on the peripapillary retina. Besidesthermal injury, other mechanisms could lead to retinaldamage, which may be involved in this process. Thevisual prognosis may be poor in the form of retinalshock surrounding optic nerve even though the maculawas free from severe damage.
References1. Bullock J. Was Saint Paul struck blind and converted by
lightning? Surv Ophthalmol 1994;39:151–160.2. Lagreze WD, Bomer TG, Aiello LP. Lightning induced ocular
injury. Arch Ophthalmol 1995;113:1076–1077.3. Espaillat A, Janigian R, To K. Cataracts, bilateral macular
hole, and rhegmatogenous retinal detachment induced by light-ning. Am J Ophthalmol 1999;127:216–217.
4. Juffe GJ, Handa JT. Lightning maculopathy. Retina1994;14:169–172.
TRANSIENT AMAUROSIS ASSOCIATEDWITH INTRAOCULAR GAS DURINGASCENDING HIGH–SPEED TRAIN TRAVEL
KEVIN M. SHIRAMIZU, MD,ANNABELLE A. OKADA, MD,AKITO HIRAKATA, MD
From the Department of Ophthalmology, Kyorin Uni-versity School of Medicine, Tokyo, Japan.
Pain associated with elevated intraocular pressure(IOP) in patients with intraocular gas during air travel
is well documented,1–4 and has also been reportedwith car travel.5 Here we report on a patient withintraocular gas who experienced ocular pain and vi-sion loss while traveling via high-speed train in rapidascent.
Case Report
A 17-year-old man presented with a serous macula detachmentassociated with optic disk pit in the right eye. Vitrectomy with 14%perfluoropropane gas injection was performed in Tokyo, roughly atsea level. One week postoperatively, visual acuity (VA) was countfingers, IOP was 21 mmHg, and a 60% intraocular gas fill wasnoted. The patient returned that day via Shinkansen (high-speed“bullet train”) to his home in Nagano (elevation 575 m). Approx-imately 80 minutes into the trip, after passing through a tunnel nearKaruizawa (elevation 1025 m, roughly the highest point on thetrain route), the patient suddenly experienced sharp pain and black-out of vision in the operated eye, which resolved after 5–6 minutes.For his 2-week postoperative visit, the patient made an uneventfulreverse journey from Nagano to Tokyo by Shinkansen. Examina-tion revealed a VA of 20/100 and an IOP of 10 mmHg. The retinawas reattached with a 50% gas fill. The patient returned that day toNagano by Shinkansen and again experienced several minutes oftransient amaurosis and ocular pain near Karuizawa. The next fol-low-up examination in Tokyo, 3 weeks postoperatively, revealed a30% gas fill and a normal IOP. That day, returning home to Naganoby Shinkansen, the patient experienced a third and final episode oftransient amaurosis and ocular pain near Karuizawa. Four monthspostoperatively, the VA was 20/20 with a normal IOP.
Discussion
According to Boyle’s Law, the absolute IOP(AIOP 5 atmospheric pressure1 IOP) decreases withthe ambient atmospheric pressure, leading to an in-crease in intraocular gas volume. However, the drop inAIOP lags behind the drop in ambient atmosphericpressure, causing a relative increase in IOP.2 In ourpatient, pain consistently occurred when ascendingfrom sea level to 1025 m over 80 minutes. By Lin-coff’s analysis, the gas volume would have expandedby the AIOP ratio (7601 IOP)/(672.51 IOP).2 In thefirst episode, this would translate to a 13% expansion,changing a 60% gas fill (2.40 mL) to a 68% gas fill(2.70 mL), assuming a 4 mLvitreous cavity volume ina phakic eye. Theoretically, the sudden 0.30 mL in-crease in intraocular volume could not be compen-sated for by choroidal compression, scleral expansion,and/or aqueous outflow,2 and therefore increased IOPand pain resulted. Similar calculations for the secondand third episodes show that the intraocular volumeincreased 0.26 mL and 0.15 mL, respectively. Inter-estingly, the first time the reverse trip was taken,involving an asymptomatic ascent from 575 m to1025 m, the trip would have been associated with onlya 0.11 mL increase in intraocular volume.
In summary, symptomatic increases in IOP canoccur with high-speed train travel when ascending
Reprint requests: Akito Hirakata, MD, Department of Ophthal-mology, Kyorin University School of Medicine, 6-20-2 Shinkawa,Mitaka-shi, Tokyo 181-8611, Japan; e-mail: [email protected]
Fig. 4. A, Pattern visual evoked response shows reduced amplitudeon the right side.B, Pattern visual evoked response was normal on the left.
528 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

rapidly. With intraocular gas use, it is important to askpatients about travel plans that include a significantascent in elevation, whether by airplane, train, or car.
References1. Dieckert JP, O’Connor PS, Schacklett DE, et al. Air travel and
intraocular gas. Ophthalmology 1986;93:642–645.2. Lincoff H, Weinberger D, Reppucci V, Lincoff A. Air travel
with intraocular gas I. The mechanisms for compensation.Arch Ophthalmol 1989;107:902–906.
3. Lincoff H, Weinberger D, Stergiu P. Air travel with intraoculargas II. Clinical considerations. Arch Ophthalmol 1989;107:907–910.
4. Kokame GT, Ing MR. Intraocular gas and low-altitude airflight. Retina 1994;14:356–358.
5. Gandorfer A, Kampik A. [Expansion of intraocular gas due toreduced atmospheric pressure. Case report and review of theliterature.] Ophthalmologe 2000;97:367–370.
HUMIDIFIED AIR EFFECT ON PUPIL SIZEDURING FLUID–AIR EXCHANGE
OSMAN ÇEKIÇ, MD, MASAHITO OHJI, MD,ATSUSHI HAYASHI, MD, XIAO Y. FANG, MD,SHUNJI KUSAKA, MD, YASUO TANO, MD
From the Department of Ophthalmology, Osaka Uni-versity Medical School, Suita, Osaka, Japan.
Perioperative management of the pupil has long beena subject of considerable interest because adequatevisualization of the retina during vitrectomy is vitalfor a successful outcome.1 Various methods have beensuggested to manage small pupils that cannot be ad-equately dilated before surgery despite the best effortswith pharmacologic means or pupils that constrictduring surgery because of ocular hypotony or manip-ulation of the iris.2–4 Conversely, it is a commonobservation that initially well dilated pupils becomesmaller during fluid–air exchange although the sur-geon has avoided hypotony or direct trauma to the iris.We hereby report that the use of a humidifier andexposure time are possible factors that affect pupilsize in aphakic eyes during fluid–air exchange.
Materials and Methods
All Dutch pigmented rabbits used in the study weremaintained in accordance with the Statement for the
Use of Animals in Ophthalmic and Vision Researchby the Association for Research in Vision and Oph-thalmology. Fourteen pigmented rabbits underwenttwo-port pars plana lensectomy and vitrectomy afterintramuscular injection of ketamine hydrochloride (35mg/kg) (Ketalar, Parke-Davis, Tokyo, Japan) and xy-lazine hydrochloride (5 mg/kg) (Selektal, Bayer, To-kyo, Japan). One eye of each rabbit was randomlyassigned to be used in the study. Pupils were dilatedwith four drops of 0.5% tropicamide and 0.5% phen-ylephrine hydrochloride (Mydrin-P, Santen, Osaka,Japan). Pars plana lensectomy was performed with alens fragmentor. Removal of the lens cortex was ac-complished by means of the vitrector keeping theanterior capsule intact initially. After vitrectomy, theanterior capsule was removed just before the standardfluid–air exchange. Total operative time was approx-imately 15 minutes until fluid–air exchange.
Seven eyes (Group 1) were insufflated with dry airwith 50 mmHg air pump (Ten Thousand PosteriorSegment System, Alcon Surgical, Irvine, CA) pres-sure. Dry air was generated by passing the normalroom air through a silica gel contained closed system.Humidified air was used in the other seven eyes(Group 2) with 57 mmHg infusion pressure. Humidi-fied air was obtained by passing the room air throughclean, nonsterile water before it was instilled in theeye as described previously.6 The order of treatingrabbits with humidified versus desiccated air wasrandomized.
Because passing air through water causes a de-crease in air pressure proportional to the height ofwater in the bottle6 (75 mm in this study), we set apreliminary experiment and obtained air flow–infu-sion pressure curves for dry and humidified air. Basedon this preliminary experiment, whereas in Group 1,the air insufflator was set to 50 mmHg, air pumppressure was adjusted to 57 mmHg in Group 2 to getthe same air flow. Thus, air insufflated into the eye indry and humidified air groups was equalized also interms of actual infusion pressure. In both groups,infused air was allowed to flow out from the sclerot-omy site opposite the infusion cannula through thebackflush needle.
The surgeries were recorded with a videotape re-corder (model SLV-93 9; Sony, Tokyo, Japan) at onestandard illumination and a constant magnification ofthe operation microscope. Pupillary areas were com-puted in pixel units with a software program (NIHimage version 1.61) from the videotapes and ex-pressed as a percentage of the initial pupil area. Cal-culations were started immediately after taking out thefluid from the vitreous cavity and from the anterior
The authors have no proprietary interest in any instruments ordrugs used in the study.
Reprint requests: Masahito Ohji, MD, Department of Oph-thalmology, Osaka University Medical School, 2-2 Yamadaoka,E7 Suita, Osaka 565-0871, Japan; e-mail: [email protected]
529BRIEF REPORTS

chamber by using a backflush needle during fluid–airexchange.
Each animal was killed with an intracardiac injec-tion of 3 mL of pentobarbital sodium (Abbott Labo-ratories, North Chicago, IL) at the end of theoperation.
During the experiment, the humidity of the operat-ing room air was 30%; that of dry air after passingthrough silica gel was 19%; and that of humidified airafter passing through water was 73%. Mann-WhitneyU tests were used to compare the data.
Results
Collapse of the anterior chamber or globe was notobserved in any eye during surgery. Figure 1 shows
pupillary areas against time during fluid–air exchangein the groups. The pupils remained larger in the eyesexposed to humidified air compared with dry air(Group 2 versus Group 1) over the first 7 minutesduring fluid–air exchange (P 5 0.018). After thattime, pupil sizes did not show any statistical differ-ence throughout 20 minutes of fluid–air exchange(P 5 0.532). Figure 2 shows the pupil sizes in thegroups at the third minute during fluid–air exchange(P , 0.003).
Discussion
Recently, some adverse effects of normal room airused during fluid–air exchange have been reported.5–7
It is postulated that visual fielddefects after vitrec-tomy may result from desiccation of the retina by roomair during fluid–air exchange.5,6 Harlan et al7 haveshown that posterior lens desiccation during fluid–airexchange may be the initiating factor in the pathogenesisof posterior lens changes after vitrectomy.
Although we developed, in 1983, an automatic in-sufflation regulator that can generate humidified airbefore instilling to the eye, we stopped using it be-cause any adverse effect on visual outcome from usingroom air without humidification was not noted at thattime.8
Because we thought the desiccation of the iriswould also accelerate pupillary miosis during fluid–airexchange, we tested the effects of humidified and dryair on pupil size by setting all other conditions similarin this study. We used maximal dry and humidified airwe could obtain to simulate every possible room air
Fig. 1. Comparison of pupillary areas against time during fluid–airexchange in Group 1 (eyes exposed to dry air with 50 mmHg infusionpressure) and Group 2 (eyes exposed to humidified air with 57 mmHginfusion pressure).
Fig. 2. Pupil sizes at the third minute during fluid–air exchange. Dry air in an eye with 50 mmHg infusion pressure (left). Humidified air in an eyewith 57 mmHg infusion pressure (right).
530 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

condition. Additionally, because the infused air wouldrapidly become hydrated by residual fluid in the eye,9
we let the infused air flow through an open backflushneedle.
Pupils exposed to dry air started to constrict earlierthan did those exposed to the humidified air. Thedifference was significant during the first 7 minutes offluid–air exchange. In the humidifier system we used,water molecules are distributed to the airstream.10 Inthis way, humidified air probably creates more of aphysiologic environment for the iris structure in vit-rectomized eyes.
After 7 minutes, pupils of eyes receiving humidifiedair also began to constrict and the two groups did notshow any difference. It seems that allowing the in-fused air to leave from the sclerotomy site through abackflush needle could not maintain humidity of theiris any longer.
From Figure 1, one can also interpret that air expo-sure time is another factor affecting pupil size. Thedesiccated air and humidified air caused miosis astime elapsed, but the humidified air constricted pupilsto a size comparable to that of pupils exposed todesiccated air approximately 2 minutes more slowly,giving the surgeon approximately 2 extra minutes ofpupillary dilation.
Based on the data obtained from the current study,we can conclude that humidification of air infusionduring vitrectomy slows the rate of miosis in an apha-kic rabbit model.
References1. de Juan E. Management of pupil. In: Ryan SJ, Glaser BM,
eds. Retina. St Louis: CV Mosby, 1994:2243–2246.2. Stern WH. Argon laser photomydriasis during vitrectomy
surgery. Am J Ophthalmol 1985;99:366–367.3. Eckardt C. Pupillary stretching: a new procedure in vitreous
surgery. Retina 1985;5:235–238.4. de Juan E, Hickingbotham D. Flexible iris retractors. Am J
Ophthalmol 1991;111:776–777.5. Welch JC. Dehydration injury as a possible cause of visual
field defect after pars plana vitrectomy for macular hole.Am J Ophthalmol 1997;124:698–699.
6. Ohji M, Nao-i N, Saito Y, et al. Prevention of visual fielddefect after macular hole surgery by passing air used forfluid-air exchange through water. Am J Ophthalmol 1999;127:62–66.
7. Harlan JB, Lee ET, Jensen PS, et al. Effect of humidity onposterior lens opacification during fluid-air exchange. ArchOphthalmol 1999;117:802–804.
8. Tano Y, Ueno N, Nishikawa N, et al. Automatic insufflationregulator. Folia Ophthalmologica Japonica 1983;34:1880–1882.
9. Rubin JS, Thompson JT, Sjaarda RN, et al. Efficacy offluid-air exchange during pars plana vitrectomy. Retina 1995;15:291–295.
10. Peterson BD. Heated humidifiers: structure and function.Respir Care Clin N Am 1998;4:243–259.
HYPOPYON UVEITIS INIMMUNOCOMPETENT PATIENTSTREATED FOR MYCOBACTERIUM AVIUMCOMPLEX PULMONARY INFECTION WITHRIFABUTIN
MITCHELL S. FINEMAN, MD,*JAMES VANDER, MD,†CARL D. REGILLO, MD,†STEVEN W. FINEMAN, MD,‡GARY C. BROWN, MD†
From the *Retina Vitreous Consultants, Pittsburgh,Pennsylvania; †Retina Service, Wills Eye Hospital,Jefferson Medical College, Thomas Jefferson Univer-sity, Philadelphia, Pennsylvania; and ‡Beth IsraelDeaconess Medical Center, Harvard Medical School,Boston, Massachusetts.
Although human immunodeficiency virus (HIV)–neg-ative patients are increasingly being diagnosed withMycobacterium avium complex(MAC) pulmonary in-fection and treated with multidrug regimens that in-clude rifabutin and clarithromycin, there are few dataregarding the development and clinical manifestationsof iridocyclitis in these patients. We report the clinicalfindings in two HIV-negative patients who developedacute hypopyon uveitis while being treated with ri-fabutin for MAC pulmonary infection and review thecurrent literature.
Case Reports
Case 1
A 57-year-old woman weighing 57 kilograms with a 2-yearhistory of pulmonary infection with MAC was started on a multipledrug regimen including ethambutol 400 mg per oral twice daily,clarithromycin 500 mg per oral twice daily, and rifabutin 300 mgper oral daily 2 months before presentation. One week beforepresentation, the patient noted symptoms consistent with a diffusepolyarthralgia syndrome but did not seek medical evaluation. Oneday before presentation, she noted the acute onset of pain, redness,and decreased visual acuity (VA) in the right eye. Evaluation byher general ophthalmologist revealed a VA of 20/40. The anterior
Supported in part by the Vitreoretinal Research and EducationFoundation, Philadelphia, Pennsylvania.
None of the authors has a proprietary interest in any of theproducts mentioned in this article.
Reprint requests: Mitchell S. Fineman, MD, Retina VitreousConsultants, 3501 Forbes Avenue, Ste 500, Pittsburgh, PA 15213.
531BRIEF REPORTS

chamber revealed moderate fibrinoid inflammation. Fundus exam-ination was significant for moderate vitreous cell and no focal areasof retinitis. Treatment with topical prednisolone acetate 1% in theright eye hourly and a topical cycloplegic agent was initiated.
The following day, VA in the right eye had worsened to 20/60.Slit-lamp examination revealed marked conjunctival injection, sig-nificant fibrin, and a 2-mm hypopyon in the deep anterior chamber.No fundus details were discernible owing to the anterior segmentinflammation. The patient was referred for B-scan ultrasonography,and this revealed moderate vitreous debris without evidence ofretinal detachment. Liver function studies performed at this timewere normal.
Because the working clinical diagnosis at this time was possiblebacterial endogenous endophthalmitis, a diagnostic vitreous tapfollowed by intravitreal injection of vancomycin 1 mg/0.1 mL andamikacin 400 mcg/0.1 mL was performed. Treatment with topicalfortified vancomycin 50 mg/mL and tobramycin 15 mg/mL wasinitiated and topical steroids and cycloplegics were continued. Thefollowing day, VA was hand motions and the anterior chamberfibrinoid reaction had increased. The rifabutin was discontinued atthis time. Over the next several days, the hypopyon decreased andthe anterior segment and vitreous inflammation diminished. Fourweeks later, VA was 20/20, and the anterior chamber was deep andquiet. The amount of vitreous debris was minimal and the retinawas entirely normal appearing. Vitreous cultures failed to grow anybacteria. There remained no evidence of ocular inflammation orany systemic bacterial infection through 4 months of additionalfollow-up.
Case 2
A 72-year-old woman weighing 55 kilograms with chronic cul-ture-proven MAC pulmonary infection was started on a multidrugregimen that included clarithromycin 500 mg per oral twice dailyand rifabutin 300 mg per oral daily several weeks before presen-tation. Three days before presentation, she noted decreased visionand pain in the right eye. Her ocular history was negative. Onexamination, VA was 20/200 in the right eye and 20/30 in the lefteye. Slit-lamp examination of the right eye revealed 31 keraticprecipitates, 31 cell and flare in the anterior chamber, and a 10%hypopyon. Fundus examination of the right eye revealed traceanterior vitreous cells and was otherwise normal. Slit-lamp biomi-croscopy and fundus examination of the left eye had normalfindings.
Diagnostic evaluation including rapid plasma reagin and fluo-rescent treponemal antibody–antibody screen, ACE, Lyme titers,antinuclear antibodies, and complete blood count were negative ornormal. Liver function studies were not performed. Treatment wasinitiated with topical prednisolone acetate 1% hourly and scopol-amine 0.25% three times a day in the right eye. The rifabutin wascontinued because it was believed to be essential for treatment ofthe pulmonary infection. One week later, VA in the right eye hadimproved to 20/100, the hypopyon was no longer present, and theanterior chamber cells were present in trace amounts. One monthlater, VA in the right eye had improved to 20/50. The patientcontinued to use topical prednisolone acetate 1% four times dailywhile taking rifabutin. Eighteen months later, she was no longerusing any oral or topical medications and examination revealed aVA of 20/25 in the right eye without signs of ocular inflammation.
Discussion
Mycobacterium avium complex, a species of nontu-berculous mycobacteria, includes the two speciesM
aviumandM intracellulare. Infection in HIV-positivepatients primarily presents as disseminated disease inpatients with low CD41 lymphocyte counts and isassociated with an increased mortality. Infection inHIV-negative patients occurs less commonly and usu-ally manifests as one of three clinical presentations:elderly men with chronic obstructive pulmonary dis-ease who present with cough, weight loss, and cavi-tary lesions; patients with underlying bronchiectasis;nonsmoking women over 50 years old with an inter-stitial pattern on chest x-ray.1 The presence of MAC inthis last group was previously thought to representcolonization, but is now recognized as a true infection.The diagnosis of MAC infection is established byclinical and radiologic findings in conjunction withsputum cultures, smears, bronchial washings, or lungtissue biopsy.
Treatment of MAC infection in patients with andwithout HIV disease is similar and involves multipledrugs, increasing the risk of drug toxicity. Initial treat-ment in HIV-negative adults consists of a minimumthree-drug regimen that includes a macrolide antibi-otic (clarithromycin or azithromycin), ethambutol, anda rifamycin agent (rifabutin or rifampin).1 Treatmentis continued until the patient is culture-negative ontherapy for 1 year. Although treatment with clarithro-mycin alone is effective, the risk of emergence ofdrug-resistant bacteria precludes monotherapy.2 Ri-fabutin is the preferred rifamycin because it is moreactive in vitro against MAC than rifampin.3 This mul-tidrug treatment regimen is approximately 90% effec-tive in converting consecutive monthly sputum cul-tures to negative for at least 1 year.1
Most cases of uveitis associated with the use ofrifabutin have been reported in HIV-positive patients.4
Griffith and associates5 reported the first two cases ofuveitis in HIV-negative patients in a study involving26 patients treated for MAC pulmonary disease with amultidrug regimen that included rifabutin in combina-tion with ethambutol, streptomycin, and either clar-ithromycin or azithromycin. In this series, the mostsevere adverse effects were diffuse polyarthralgia syn-drome in 19% and anterior uveitis in 8% of patients.The uveitis was seen only in those patients random-ized to the regimen that included clarithromycin.However, no details regarding the clinical presenta-tion or treatment of the patients with uveitis werereported. Jewelewicz and associates6 reported an8-year-old boy who developed bilateral uveitis whileon a multidrug regimen including rifabutin and clar-ithromycin after bilateral lung transplantation. Al-though this patient was not HIV-positive, he wasimmunosuppressed. Previous studies involving HIV-positive patients treated for MAC infection reported a
532 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

40% incidence of anterior uveitis when doses of cla-rithromycin higher than 500 mg twice daily were usedin combination with doses of rifabutin higher than orequal to 600 mg per day.7 When the rifabutin dose wasreduced to 300 mg per day, the incidence of uveitisfell to 6%.8 Clarithromycin is thought to increaserifabutin levels and toxicity by inhibiting the metab-olism of rifabutin via the cytochromeP 2450 sys-tem.9 Based on these findings, it is recommended thatrifabutin doses should not exceed 300 mg/d in regi-mens that contain clarithromycin.1 Because azithro-mycin has not been shown to increase rifabutin levels,it may be a safer choice in patients at risk for rifabutintoxicity. Preliminary studies also suggest that azithromy-cin-containing multidrug regimens for MAC infectionmay be efficacious when administered intermittently.10
Both patients in our series presented with severeuveitis, and one patient’s clinical picture promptedtreatment for presumed endogenous bacterial endoph-thalmitis before the association with rifabutin treat-ment was realized. Most clinicians associate rifabutin-induced uveitis with the treatment of MAC infectionin HIV-positive patients; therefore, the clinical suspi-cion may not be as high when evaluating HIV-nega-tive patients. The patients described herein were beingtreated with the currently recommended multidrugregimens in recommended doses and still developedsevere uveitis. Both patients were women and hadrelatively low body mass, a possible predisposingfactor. Liver function was normal in the one patientwho was tested, suggesting that abnormal liver func-tion is not a prerequisite for this adverse event. Asbetter clinical recognition and increased culturing leadto higher prevalence rates of MAC infection in HIV-negative patients, more patients will be diagnosedwith this condition and treated with rifabutin-contain-ing drug regimens. Therefore, rifabutin-induced uve-itis should be considered in any patient who presentswith ocular inflammation and has a history of MACinfection, regardless of systemic immune status.
References1. Medical Section of the American Lung Association. Diagno-
sis and treatment of disease caused by nontuberculous my-cobacteria (official statement of the American Thoracic So-ciety). Am J Respir Crit Care Med 1997;156:S1–25.
2. Wallace RJ Jr, Brown BA, Griffith DE, et al. Initial clarithro-mycin monotherapy forMycobacterium avium–intracellularecomplex lung disease. Am J Respir Crit Care Med 1994;149:1335–1341.
3. Skinner MH, Blaschke TF. Clinical pharmacokinetics of ri-fabutin. Clin Pharmacokinet 1995;28:115–125.
4. Saran BR, Maguire AM, Nichols C, et al. Hypopyon uveitisin patients with acquired immunodeficiency syndrome treatedfor systemicMycobacterium avium complexinfection withrifabutin. Arch Ophthalmol 1994;112:1159–1165.
5. Griffith DE, Brown BA, Girard WM, et al. Adverse eventsassociated with high-dose rifabutin in macrolide-containingregimens for the treatment ofMycobacterium avium complexlung disease. Clin Infect Dis 1995;21:594–598.
6. Jewelewicz DA, Schiff WM, Brown S, et al. Rifabutin-associated uveitis in an immunosuppressed pediatric patientwithout acquired immunodeficiency syndrome. Am J Oph-thalmol 1998;125:872–873.
7. Shafran SD, Deschenes J, Miller M, et al. Uveitis andpseudojaundice during a regimen of clarithromycin, ri-fabutin, and ethambutol. MAC Study Group of the Cana-dian HIV Trials Network [letter]. N Engl J Med 1994;330:438 – 439.
8. Shafran SD, Singer J, Zarowny DP, et al. A comparison oftwo regimens for the treatment ofMycobacterium aviumcomplexbacteremia in AIDS: rifabutin, ethambutol, and cla-rithromycin versus rifampin, ethambutol, clofazimine, andciprofloxacin. Canadian HIV Trials Network Protocol 010Study Group. N Engl J Med 1996;335:377–383.
9. Hafner R, Bethel J, Power M, et al. Tolerance and pharma-cokinetic interactions of rifabutin and clarithromycin in hu-man immunodeficiency virus–infected volunteers. Antimi-crob Agents Chemother 1998;42:631–639.
10. Griffith DE, Brown BA, Murphy DT, et al. Initial (6-month)results of three-times-weekly azithromycin in treatment reg-imens for Mycobacterium avium complexlung disease inhuman immunodeficiency virus–negative patients. J InfectDis 1998;178:121–126.
BACTERIAL GROWTH INPERFLUOROCARBON LIQUIDS:An in vitro Study
CARLOS A. MOREIRA, JR, MD,AGOSTINHO BRYK, JR, MD,MARIA C. KOMATSU, MD,LECIANA C. VANZO, MD
From the Department of Ophthalmology, FederalUniversity of Paraná, Brazil.
The use of perfluorocarbon liquids (PFCL) in vitreo-retinal surgery was first reported by Chang et al in1987.1,2 Since then, it has increasingly been used byretinal surgeons for many purposes.3,4 These sub-stances have proven to be useful in vitreoretinal sur-gery because of their favorable physical and chemicalproperties, which provide good surgical performance,5
in that they are easily injected and removed. However,small amounts of PFCL (blisters or droplets) may
Presented at the XXII Club Jules Gonin Meeting, Taormina,Italy, September 2–6, 2000.
The authors do not have a proprietary interest in the study.Reprint requests: Carlos Moreira, Jr., MD, Rua Fernando Simas,
1010 Curitiba, Brazil 80430-190.
533BRIEF REPORTS

remain in the vitreous cavity or under the retina6 aftersurgery.
The vast use of PFCL in vitreoretinal surgery andthe possibility of droplets of this substance remainingin the vitreous cavity called to our attention the pos-sibility of bacterial contamination and risks to patientsand surgeons. Therefore, it is important to verify thepotential for contamination of PFCL. It has beenshown thatStaphylococcus aureusandPseudomonasaeruginosaare common pathogenic agents in intraoc-ular infections.7 The goal of this study was to deter-mine the growth ofS aureusand P aeruginosainperfluoro-octane, one of the most widely used PFCLin vitreoretinal sugery.5,8
Materials and Methods
Perfluoro-octane
Perfluorocarbon liquids are compounds belongingto a class of purified perfluoropropylene oxide oli-gomers with characteristic physicochemical proper-ties. These compounds are immiscible with water,transparent, colorless, chemically inert, odorless, non-flammable, of low viscosity, and insoluble in organicsolvents, with high specific gravity.5,8 They are opti-cally transparent and their refraction index is similarto that of the normal vitreous body (i.e., 1.29), afeature that permits their easy intraocular observationduring intraoperative maneuvers.2,8 The low viscosity(2–3 centistokes at 25°C) and insolubility in standardorganic solvents are other favorable properties.2,8
Procedure
Three culture media were used: perfluoro-octane(3 M, St. Paul, MN), tryptic soy and casein digestionbroth (TSB), and 0.9% saline solution.
Five milliliters of perfluoro-octane were dividedinto 1-mL flasks numbered 1 through 5. A full colonyof P aeruginosa(ATCC 27853) was inoculated intoFlasks 1 and 2, and a full colony ofS aureus(ATCC25932) was inoculated into Flasks 3 and 4. Flask 5served as a control with no contamination. Full bac-
terial colonies were used because perfluoro-octane isnot miscible with water.
To determine the bioavailability of such microor-ganisms, a colony of each bacteria was inoculated intoa flask containing 1 mL TSB, a culture medium rich innutrients favorable to bacterial proliferation. The sameprocedure was repeated to contaminate a 0.9% salinesolution to compare the results obtained with per-fluoro-octane with those obtained with another me-dium devoid of nutrients.
All solutions werehomogenized in a Vortex appa-ratus at 1,000 rotations per minute and later kept inan incubator at 37°C for 10 days. Replating was per-formed with a calibrated loop at 1:1000 and with amicropipette (0.05 mL) at time zero and 72 hours, 168hours, and 240 hours after contamination. The materialwas manipulated under a laminar flow hood through-out the procedure to prevent external contamination.Bacterial growth was determined by colony countingon blood agar plates 24 hours after each replating.
Results
In perfluoro-octane, we observed the growth of onecolony of P aeruginosain Flask 1 and of three colo-nies in Flask 2 at time zero. When a micropipette wasused for replating, Flask 1 yielded two colonies andthe other flask yielded six. At all other times, however,no growth of the bacteria was observed. In contrast, inTSB and 0.9% saline solution, growth was abundant atall time points (Table 1).
At time zero, one colony ofS aureuswas detectedin Flask 3 and 16 colonies were detected in Flask 4.When replating was performed with a micropipette,the results were four and two colonies, respectively.During the subsequent hours,S aureusgrowth was nolonger observed in perfluoro-octane. A reduction inSaureusgrowth occurred in TSB and saline over time,but even so, growth was abundant (Table 2). Nobacterial proliferation was observed at any time pointin the uncontaminated control flask (Flask 5).
Table 1. Quantification of Pseudomonas aeruginosa (ATCC 27853) Growth in Different Culture Media
Time, h
Perfluoro-octane Number of Colonies
Flask 1 Flask 2 Trypticase Soy Broth 0.9% Saline
0 1–2* 3–6* Abundant 1111/IV Abundant 1111/IV72 0–0* 0–0* Abundant 1111/IV Abundant 1111/IV168 0–0* 0–0* Abundant 1111/IV Abundant 111/IV240 0 0 Abundant 111/IV Abundant 111/IV
* Colony counting from micropipette inoculation on blood agar plates.
534 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

Discussion
As expected, the highest bacterial growth occurredin soy and casein digestion broth, which is a culturemedium favorable to bacterial growth. A calibratedloop and micropipette were used to get perfluoro-octane samples from Flasks 1 to 5, because of the highspecific gravity of perfluoro-octane. Replating with amicropipette was added to the procedure to make surethat samples obtained from flasks with perfluoro-oc-tane were of adequate amount.
AlthoughP aeruginosaare highly resistant bacteriacapable of developing even in extremely unfavorablemedia, they did not grow in any of the perfluoro-octane samples under study, except at time zero,which corresponds to the time of inoculation. Lack ofnutrients alone would not be sufficient to explain theabsence of growth of these bacteria in an adequatemanner because we showed that the bacteria grewabundantly even in 0.9% saline solution. There was noS aureusgrowth in perfluoro-octane except at timezero. The staphylococci grew abundantly in 0.9%saline, although growth was slightly reduced after 168hours (7 days). No bacterial proliferation occurred inthe perfluoro-octane sample used as an uncontami-nated control, showing that the perfluoro-octane beingused was a sterile product and that no external con-tamination had occurred during manipulation of thesubstance.
These in vitro results have shown that perfluoro-octane is not a favorable medium for bacterial growthand therefore is not prone to bacterial contaminationduring vitreoretinal surgery. The presence of smalldroplets of PFCL is relatively frequent after complexvitreoretinal procedures, and it appears that PFCLmay not represent a source of infection.
References1. Chang S, Zimmerman NJ, Iwamoto T, et al. Experimental
vitreous replacement with perfluorotributylamine. Am J Oph-thalmol 1987;103:29–37.
2. Chang S. Low viscosity liquid fluorochemicals in vitreoussurgery. Arch Ophthalmol 1987;103:38–43.
3. Coll GE, Chang S, Sun J, et al. Perfluorocarbon liquid in the
management of retinal detachment with proliferative vitreo-retinopathy. Ophthalmology 1989;102:630–639.
4. Moreira CA Jr, Uscocovich CE, Moreira AT. Experimentalstudies with perfluoro-octane for hemostasis during vitreoreti-nal surgery. Retina 1997;17:530–534.
5. Bourke RD, Cooling RJ, Simpson RN, et al. The stability ofperfluoro-N-octane during vitreoretinal procedures. Arch Oph-thalmol 1996;114:537–544.
6. Queiroz JM Jr, Özler SA, Moreira CA Jr, et al. Histopatho-logic evaluation of subretinal perfluorocarbon liquids. InvestOphthalmol Vis Sci 1991;32:881. Abstract.
7. Forster RK. Etiology and diagnosis of bacterial postoperativeendophthalmitis. Ophthalmology 1980;87:313–319.
8. Queiroz J Jr, Özler SA, Liggett P, et al. Experimental intra-operative use of perfluorotributylamine, perfluorodecaline, andperfluorooctane. Arq Bras Oftal 1992;55:112–116.
BILATERAL MULTIPLE RETINALHYPERFLUORESCENT DOTS IN APRESUMED RICKETTSIA CONORIIINFECTION
HALUK ESGIN, MD,* FILIZ AKATA, MD†
From the Departments of *Ophthalmology and †Clin-ical Microbiology and Infectious Disease, UniversityHospital Trakya, Edirne, Turkey.
In rickettsial diseases, various vascular lesions can beseen in the retina and optic disk. Optic nerve head andretinal edema, intraretinal hemorrhages, cotton-woolspots, retinal white infiltrates, retinal vasculitis, andvascular occlusions have been previously reported.1–3
We report a case with small retinal hyperfluorescentdots by angiography, which resemble multiple evanes-cent white dot syndrome (MEWDS), in aRickettsiaconorii infection.
This study has not been published or presented elsewhere. Theauthors have no proprietary interests related to this study.
Reprint requests: Haluk Esgin, MD, Trakya Üniversitesi TıpFakültesi, Göz hastalıkları, Anabilim dalı, 22030 Edirne, Turkey.
Table 2. Quantification of Staphylococcus aureus (ATCC 25923) Growth in Different Culture Media
Time, h
Perfluoro-octane Number of Colonies
Flask 3 Flask 4 Trypticase Soy Broth 0.9% Saline
0 1–4* 16–2* Abundant 1111/IV Abundant 1111/IV72 0–0* 0–0* Abundant 1111/IV Abundant 1111/IV168 0–0* 0–0* Abundant 1111/IV Abundant 111/IV240 0–0* 0–0* Abundant 1111/IV Abundant 11/IV
* Colony counting from micropipette inoculation on blood agar plates.
535BRIEF REPORTS

Case Report
A 51-year-old man developed shaking chills, shivering, fever,headache, and a sore throat 5 days after a tick bit him while he wasworking in his garden. Three days after the fever started, a macu-lopapular skin rash appeared over his body, including his palmsand soles. The patient was admitted to a local hospital for 2 daysand was treated only with antipyretics. Because of his increasingbody temperature (40.5°C) and generalized skin rash, he wastransferred to our hospital. The patient had a history of taking careof his neighbor’s dog in the same garden. On physical examination,a tick bite in his left buttock, 13 1 cm in size, and a black lesionassociated with eschar (tache noire) were identified. Although thepatient had no complaints regarding his eye, he was sent for aroutine ophthalmologic examination because of his Type II diabe-tes mellitus, controlled only by diet.
Visual acuity was 20/20 in both eyes. Findings from slit-lampexamination were normal. Fundus examination showed three cot-ton wool spots in the right eye (Figure 1) and two cotton-woolspots in the left eye. Signs of vasculitis were found in the supero-temporal quadrant of the right eye (Figure 2) and inferior quadrant
of the left eye periphery. No hemorrhages were seen in the retinaor choroid in either eye, and no inflammatory vitreous reaction oropacities were found. Fluorescein angiography of both eyesshowed leakage from the dilated peripapillary capillaries, fluores-cein blockage caused by the cotton-wool exudates, and vascularfluorescein leakage in the periphery caused by vasculitis. Also,punctuate hyperfluorescence in the posterior pole, which was moreprominent in the left eye (Figure 3), was seen. No signs of diabeticretinopathy were observed.
Results of the following laboratory tests were abnormal: eryth-rocyte sedimentation rate (67 mm in the first hour), hematocrit(35% consistent with anemia of chronic disease), platelet counts(146,000/mm3 on the first hospital day and 136,000/mm3 on thesecond hospital day), fasting blood glucose (257 mg/dL), alaninetransferase (ALT) (63 U/L), aspartate transferase (AST) (101 U/L),and lactic dehydrogenase (LDH) (1,043 U/L). C-reactive proteinwas not assessed. Abdominal ultrasonography showed an enlarged
Fig. 2. Midphase of fluorescein angiogram of the right eye showsperipheral vasculitis in the superotemporal quadrant of the retina.
Fig. 3. Midphase of fluorescein angiogram of the left eye showsdiscrete, punctuate focal areas of leakage in the deep retina at theposterior pole and leakage from the peripapillary capillaries.
Fig. 4. Fundus photograph of the right eye 2 months after the initialexamination.
Fig. 1. Fundus photograph of the right eye with cotton-wool spots inthe peripapillary region, 12 days after a tick bite.
536 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

spleen (141 mm). The most commonly used test for rickettsioses isthe Weil-Felix agglutination test, which is an old test with lowsensitivity and specificity. A definite increase of the Weil-Felixreaction from negative (OX19, OX2, and OXK) to 1/160 (OX19)and 1/320 (OX2) was observed within 10 days. Serology forBrucella, Salmonella, Treponema pallidum, hepatitis B and C,human immunodeficiency virus, Epstein-Barr virus, and toxoplas-mosis were all negative. The IgG antibodies for hepatitis A, rubellavirus, cytomegalovirus, and herpes simplex Type I were positive.
The patient was treated with 100 mg of doxycycline twice dailyfor 10 days. The fever decreased in the third day, and the skin rashdecreased by the seventh day after the onset of treatment. Plateletcount and AST, ALT, and LDH levels returned to normal after 10days. An oral hypoglycemic agent was prescribed for his diabetesmellitus and the blood glucose level was regulated. Two monthsafter the initial examination, all ophthalmic and angiographic signsof peripapillary leakage and punctuate hyperfluorescent areas re-solved with no chorioretinal scar (Figure 4).
Discussion
Based on the patient’s history, clinical signs, andserology, we concluded that the illness presented wasassociated with rickettsiae. Members of the genusRickettsia have been divided into three groups ofantigenically related species: typhus, scrub typhus,and spotted fever.4 The patient’s activity in taking careof the neighbor’s dog and tick bite history, the incu-bation time, and the marked titer increase of OX19and OX2 when assessed with epidemiologic findingsdirected us toward an infectious agent of the spottedfever group, most likelyR conorii, which occurs inthe Mediterranean area, Africa, parts of Europe, andIndia. As in other Mediterranean countries, in Turkey,Mediterranean spotted fever caused byR conorii isendemic. In ticks,R conorii is maintained transovari-ally and is transmitted to humans by the dog tickRhipicephalus sanguineus, and the main reservoir ofinfection is in domestic dogs, rabbits, and rodents. Acareful clinical examination may show a tache noire,which facilitates the clinical diagnosis.5
In rickettsioses, proliferation of organisms in theendothelium of small arteries, veins, and capillariesresults in vasculitis and microinfarcts.4,5 The cotton-wool exudates, peripapillary leakage from capillaries,peripheral vasculitis, and hyperfluorescent dots foundin our patient is supposedly based on microvesseldestruction and extravasation of blood into the retina.The differential diagnosis of the ocular findings in-cludes many diseases that were excluded by history,clinical course, and serology. Punctuate hyperfluores-cent lesions may mimic white dot syndromes. Themost important criterion in the differential diagnosis isthat the white dots are not apparent by ophthalmos-copy, as they were our patient. In addition, the com-plete disappearance of the lesions without any scarformation excluded chorioretinitis from other causes.
In acute posterior multifocal placoid pigment epithe-liopathy, fluorescence blockage occurs in the earlyphases of the angiogram. Conversely, the lesions inacute retinal pigment epitheliitis are hypofluorescentsurrounded with hyperfluorescence. With the lack ofthe vitreous reaction and the clinical course, weexcluded birdshot retinochoroidopathy. Multiple eva-nescent white dot syndrome cannot be excluded byfluorescein angiography findings, but with history andserology, we excluded it. In this report, we showedsmall retinal hyperfluorescent punctuate lesions byangiography inR conorii infection, which were simi-lar to the presentation of MEWDS.
References1. Lukas JR, Egger S, Parshalk B, et al. Bilateral small retinal
infiltrates during rickettsial infection. Br J Ophthalmol 1998;82:1217–1218.
2. Alio J, Roiz-Beltran R, Herrero-Herrero JI, et al. Retinalmanifestations of Mediterranean spotted fever. Ophthalmo-logica 1987;195:31–37.
3. Sulewski ME, Green WR. Ocular histopathologic features of apresumed case of Rocky Mountain spotted fever. Retina 1986;6:125–130.
4. McDade JE. Rickettsial diseases. In: Hausler WJ, Sussman M,eds. Topley & Wilson’s Microbiology and Microbial Infec-tions, 9th ed. London: Arnold, 1998;3:995–1011.
5. Walker DH, Raoult D.Rickettsia rickettsiiand other spottedfever group rickettsiae (Rocky Mountain spotted fever andother spotted fevers). In: Mandell GL, Bennett JE, Dolin R,eds. Mandell, Douglas and Bennett’s Principles and Practice ofInfectious Disease, 4th ed. New York: Churchill Livingstone,1995:1721–1727.
INDOCYANINE GREENVIDEOANGIOGRAPHY OF MULTIFOCALCRYPTOCOCCUS NEOFORMANSCHOROIDITIS IN A PATIENT WITHACQUIRED IMMUNODEFICIENCYSYNDROME
J. FERNANDO AREVALO, MD,*DARIO FUENMAYOR–RIVERA, MD,†AURA E. GIRAL, MD,† ENRIQUE MURCIA*†
From the *Retina and Vitreous Service, Clinica Of-talmologica Centro Caracas, and the†Instituto deOftalmologia, Caracas, Venezuela.
Cryptococcusneoformansis a fungus that causesopportunistic infection in patients with acquired
None of the authors has a proprietary or financial interest in anyof the products or techniques described in this article.
Reprintrequests: J. Fernando Arevalo, MD, Clinica OftalmologicaCentro Caracas, Centro Caracas PH-1, Av. Panteon, San Bernardino,Caracas 1010, Venezuela; e-mail: [email protected]
537BRIEF REPORTS

immunodeficiency syndrome (AIDS). Patientscommonly have meningitis and are referred to theophthalmologist with ophthalmoplegia, diplopia,nystagmus, sixth cranial nerve palsy, ptosis, opticatrophy, cryptococcal choroiditis, and papillede-ma.1 The clinical features of cryptococcal choroid-itis are cells in the vitreous with focal choroidallesions. The presence of the fungus in the choroidimplies hematogenous spread and, consequently, isassociated with poor prognosis.
Fluorescein angiography characteristics havebeen reported in some cases of cryptococcal cho-roiditis.1–2 To our knowledge, this report describesfor the first time the indocyanine green videoan-giography (ICG-V) characteristics of a patient withAIDS and cryptococcal choroidal disease.
Case Report
A 37-year-old man with AIDS was examined in March 1999because of a 5-day history of decreased visual acuity in both eyesand headaches and general lethargy. He had been human immu-nodeficiency virus (HIV)-positive since 1984, and his CD4 countwas 54 cells/mL. Highly active antiretroviral therapy had beenstarted 2 months before this visit. Ophthalmic examination showeda visual acuity of counting fingers in both eyes. The eyes werewhite, and slit-lamp examination was unremarkable with no ante-rior chamber or vitreous inflammation. Fundus examinationshowed a pattern of multiple deep, 300- to 400-mm, yellowishlesions that looked to be located beneath the retina at the level ofthe retinal pigment epithelium and choroid (Figure 1). The opticdisk and retinal vessels were healthy. A fluorescein angiogramconfirmed the presence of round lesions that were located under theneural retina. These lesions masked fluorescence early during thestudy, and there was no significant leakage in the late stages ofthe angiogram, although some late hyperfluorescence may be seenon the nasal aspect of the optic disk in both eyes. The retinalcomponent of the fluorescein angiogram was normal (Figure 2).Indocyanine green videoangiography confirmed the presence oflesions that were at the level of the choroid. These lesions maskedfluorescence throughout the study. Most of these hypofluorescentdark spots were already visible in the early phase of the videoan-giogram, became more sharply delineated in the intermediate an-giographic frames, and remained hypofluorescent in the late frames(Figure 3). They were more irregular in shape (some of themconfluent) and more numerous than those seen on fundusexamination.
The differential diagnosis included cryptococcal meningitis, tox-oplasma encephalitis, and cerebral lymphoma with posterior seg-ment involvement. Lumbar puncture performed 1 week latershowed cryptococcal meningitis. He was treated with intravenousamphotericin B but died of cryptococcal systemic complications 3weeks later. The family refused an autopsy.
Discussion
C neoformansis a yeastlike fungus widely found innature. An uncommon cause of human disease, it mayinfect healthy persons but has a special predilectionfor immunocompromised patients. This case report
describes a patient with visual symptoms and a funduspicture that, on fluorescein angiography and ICG-V,was consistent with disease of the retinal pigmentepithelium or choroid in a patient with AIDS. Adiagnosis of cryptococcal choroiditis was eventuallymade after lumbar puncture performed 1 week latershowed cryptococcal meningitis. The diagnosis ofcryptococcal choroiditis was presumed after extensiveworkup and numerous blood cultures showed that ourpatient had no other evidence of hematogenous op-portunistic infections. In addition, visual symptomsand the fundus lesions started to resolve on systemictreatment, but the patient died of cryptococcal sys-temic complications 3 weeks later.
The multifocal pattern and irregularly shaped hy-pofluorescent spots on ICG-V were also seen on flu-orescein angiography. This finding may be related toan active disease stage that may have involved thechoriocapillaris. More hypofluorescent spots on
Fig. 1. Fundus photographs of the right (A) and left (B) eyes showmultiple deep, 300- to 400-mm, yellowish lesions that seem to belocated beneath the retina at the level of the retinal pigment epitheliumand choroid.
538 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

ICG-V were detected than would correspond to theyellowish areas seen in color and red-free photo-graphs. Their distribution was most dense surroundingthe optic nerve and fovea. In addition, they had atendency to be confluent, and this characteristic wasbetter depicted with ICG-V (Figure 3) than with flu-orescein angiography.
Choroidal infiltration, which prevented normal cho-roidal indocyanine green impregnation, probably wasthe physiopathologic explanation for these persistenthypofluorescent dark spots. These ICG-V features de-scribed in our patient were nonspecific for the disease.Similar findings have been described in other inflam-matory conditions involving the choroid, such as bird-
shot chorioretinopathy, Vogt–Koyanagi–Harada dis-ease, sympathetic ophthalmia, posterior sarcoidosis,posterior tuberculosis, toxoplasmic retinochoroiditis,and acute posterior multifocal placoid pigmentepitheliopathy.3–7
To our knowledge, this is the first report of ICG-Vcharacteristics in a case of cryptococcal choroiditis.Our patient had a pigmented fundus, and the peculiarmultifocal pattern of choroiditis was subtle. In patientswith lightly pigmented fundi, choroidal lesions maynot appear on fundus photographs and ICG-V may behelpful in detecting and documenting the extent ofchoroidal involvement. Furthermore, ICG-V may pro-vide information on the pathophysiology of some oc-
Fig. 2. Fluorescein angiography confirmed the presence of round lesions that were located under the neural retina. These lesions masked fluorescenceearly during the study (top). There was no significant leakage in the late stages of the angiogram, although some late hyperfluorescence may be seenon the nasal aspect of the optic disk in both eyes (bottom).
539BRIEF REPORTS

ular inflammatory diseases and may be useful in mon-itoring the effect of therapeutic interventions.
The ophthalmologist plays a valuable role in thetreatment of patients with AIDS because an importantnumber of these patients have ocular diseases. Cyto-megalovirus retinitis is the most common ocular op-portunistic infection, although its incidence has de-creased in the last few years because of theintroduction of highly active antiretroviral therapy.The incidence of opportunistic infections that metas-tasize to the choroid is much lower and includesCneoformans, Mycobacterium avium, andPneumocys-tis carinii. The prognosis for these patients is poor bythis stage, and the diagnosis may elude the physician
until choroidal involvement develops. It is thereforeimportant for ophthalmologists to recognize the pat-tern of choroidal involvement produced by opportu-nistic infections in AIDS because prompt treatmentwill prolong life.
References1. Carney MD, Combs JL, Waschler W. Cryptococcal choroid-
itis. Retina 1990;10:27–32.2. Saran BR, Pomilla PV. Retinal vascular nonperfusion and
retinal neovascularization as a consequence of cytomegalovi-rus retinitis and cryptococcal choroiditis. Retina 1996;16:510–512.
3. Auer C, Herbort CP. Indocyanine green angiographic featuresin posterior scleritis. Am J Ophthalmol 1998;126:471–476.
Fig. 3. Indocyanine green videoangiography confirmed the presence of lesions, which were at the level of the choroid. These lesions maskedfluorescence throughout the study. Most of these hypofluorescent dark spots were already visible in the early phase of the videoangiogram, becamemore sharply delineated in the intermediate frames (top), and remained hypofluorescent in the late frames (bottom). The white circle in the bottomimages is an artifact.
540 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

4. Auer C, Bernasconi O, Herbort CP. Toxoplasmic retinocho-roiditis: new insights provided by indocyanine green angiog-raphy. Am J Ophthalmol 1997;123:131–133.
5. Oshima Y, Harino S, Hara Y, et al. Indocyanine green angio-graphic findings in Vogt–Koyanagi–Harada disease. Am JOphthalmol 1996;122:58–66.
6. Bernasconi O, Auer C, Zografos L, et al. Indocyanine greenangiographic findings in sympathetic ophthalmia. GraefesArch Clin Exp Ophthalmol 1998;236:635–638.
7. Wolfensberger TJ, Piguet B, Herbort CP. Indocyanine greenangiographic features in tuberculous chorioretinitis. Am JOphthalmol 1999;127:350–353.
SPONTANEOUS RESOLUTION OFCYTOMEGALOVIRUS RETINITIS IN ANINFANT WITH CONGENITALCYTOMEGALOVIRUS INFECTION
AMY S. NOFFKE, MD,MARILYN B. METS, MD
From the Division of Ophthalmology, Children’s Me-morial Hospital, Chicago; and the Department ofOphthalmology, Northwestern University MedicalSchool, Chicago, Illinois.
The treatment of active cytomegalovirus (CMV) reti-nitis in infants with congenital CMV is not well es-tablished. We report a case of bilateral CMV retinitisinvolving the posterior pole in a neonate with congen-ital CMV. The retinitis did not progress and resolvedspontaneously within 3 weeks without intravenoustherapy.
Case Report
A female infant was born at 37 weeks’ gestation with micro-cephaly, hepatosplenomegaly, and petechiae. She was diagnosedwith congenital CMV infection after isolation of virus from theurine. Ophthalmic examination at 1 week of age showed bilateralintraretinal hemorrhages without evidence of retinitis. Dilated fun-dus examination 5 weeks later showed multiple areas of retinitis ina perivascular distribution bilaterally (Figure 1). The retinitis wasconsidered immediately sight-threatening because it extended intothe posterior pole of each eye.
Consultation with the Pediatric Infectious Disease service re-garding systemic antiviral therapy was obtained. Because of theinfant’s otherwise stable condition and the potential toxicity ofganciclovir, the recommendation was for close follow-up, withinstitution of ganciclovir therapy if the retinitis progressed.
Frequent dilated fundus examinations were performed, and the
fundus appearance was documented using the RetCam 120 retinalimaging system (Massie Instruments, Los Angeles, CA). The ret-initis did not progress. At the end of the second week, earlypigmented scarring of the lesions was noted. The retinitis had fullyresolved within 3 weeks and remained inactive during the next 6months. Subsequently, the child’s family returned to Mexico, andshe was lost to follow-up.
Discussion
Ocular involvement in congenital CMV infectionmost commonly presents with inactive chorioretinalscars.1 There are only a few reports in the literature ofactive retinitis in neonates with congenital CMV in-fection. Coats et al2 found that only 1 of the 125infants with congenital CMV they examined had ac-tive retinitis, which progressed over several weeks butresolved rapidly with ganciclovir therapy. Baumal etal3 reported a case of bilateral retinitis of the posteriorpole in an infant with congenital CMV and encepha-litis that resolved with intravenous ganciclovir.
The treatment of CMV retinitis in neonates is notwell established.4 Retinitis in infants with congenitalCMV differs from that in immunocompromised pa-tients in that it is reported to rarely progress postna-
This work was supported by the Heed Ophthalmic Foundation,Cleveland, Ohio (Dr. Noffke), and by an unrestricted grant fromResearch to Prevent Blindness, Inc., New York, New York.
Reprint requests: Marilyn B. Mets, MD, Children’s MemorialHospital, Division of Ophthalmology, 2300 Children’s Plaza Box70, Chicago, IL 60614.
Fig. 1. Color fundus photographs show multiple perivascular foci ofretinitis in each eye.
541BRIEF REPORTS

tally and not to recur without immunocompromise.1
The use of ganciclovir is limited by its bone marrowtoxicity, and concerns exist regarding its potentialreproductive toxicity.
A Phase II multicenter clinical trial5 evaluatingganciclovir for the treatment of infants with symptom-atic congenital CMV infection and central nervoussystem involvement has established that ganciclovir at12 mg/kg/day in two divided doses can be adminis-tered without inordinate toxicity. A Phase III trial isongoing to evaluate the efficacy of ganciclovir inreducing visual, auditory, and neurologic impairmentin children with congenital CMV.
The case reported herein illustrates the dilemmathat clinicians may face regarding treatment of activeretinitis in an infant with congenital CMV. Our patienthad no concomitant life-threatening systemic illness,as did the infant with encephalitis described byBaumal et al,3 nor did the retinitis progress, as it hadin the child Coats et al2 described; instead, the retinitisresolved spontaneously while the patient was underclose observation. Although the authors of the PhaseII trial 5 caution against the routine use of ganciclovirfor symptomatic congenital CMV until efficacy hasbeen shown, other authors1,2 suggest that its use maybe cautiously considered in specific life- or sight-threatening situations.
References1. Demmler GJ. Congenital cytomegalovirus infection and dis-
ease. Adv Pediatr Infect Dis 1996;11:135–162.2. Coats DK, Demmler GJ, Paysse EA, et al. Ophthalmologic
findings in children with congenital cytomegalovirus infection.J AAPOS 2000;4:110–116.
3. Baumal CR, Levin AV, Read SE. Cytomegalovirus retinitisin immunosuppressed children. Am J Ophthalmol 1999;127:550–558.
4. Yoser SL, Forster DJ, Rao NA. Systemic viral infections andtheir retinal and choroidal manifestations. Surv Ophthalmol1993;37:313–352.
5. Whitley RJ, Cloud G, Gruber W, et al. Ganciclovir treatmentof symptomatic congenital cytomegalovirus infection: resultsof a phase II study. J Infect Dis 1997;175:1080–1086.
PURTSCHER RETINOPATHY FOLLOWINGDRUG-INDUCED PANCREATITIS IN ANHIV-POSITIVE PATIENT
STEVEN K. BUI, MD,*†JOAN M. O’BRIEN, MD,†EMMETT T. CUNNINGHAM, JR, MD, PHD, MPH*†
From the *Francis I. Proctor Foundation and the†Department of Ophthalmology, University of Cali-fornia at San Francisco Medical Center.
Human immunodeficiency virus (HIV) retinopathy af-fects as many as 50% of HIV-infected patients, typi-cally when CD41 T-lymphocyte counts are below 100cells/mL.1 Cotton-wool spots and intraretinal hemor-rhages, the hallmarks of HIV retinopathy, are usuallyasymptomatic, although a few patients experience vi-sion loss from macular ischemia.2,3 There are, how-ever, a number of additional causes of retinal micro-vasculopathy,4 and they also must be considered in allHIV-positive patients who have cotton-wool spots andintraretinal hemorrhages, particularly when the pre-sentation is atypical. We describe a patient with ac-quired immunodeficiency syndrome (AIDS) and reti-nal whitening and nonperfusion that was subsequentlyidentified as Purtscher retinopathy occurring in thesetting of drug-induced pancreatitis.
Case Report
A 32-year-old man with AIDS and a recent CD41 T-lymphocytecount of 82 cells/mL was seen by an ophthalmologist because ofdecreased vision that was worse in his left eye for 1 week. Thepatient’s ocular history was notable for toxoplasmic retinochoroid-itis in his left eye that was diagnosed 7 months before the onset ofhis current visual symptoms and that was treated with sulfadiazinefor 1 month with resolution. His medical history was notable foresophageal candidiasis, cutaneous herpes zoster infection, andhigh-grade non-Hodgkin lymphoma affecting his oral and rectalmucosa. Four months before the onset of the patient’s presentingvisual symptoms, his lymphoma recurred and he was administeredthe experimental antilymphoma drug, diethylhomospermine, withpartial improvement. The patient’s other medications included 1tablet of 160/800 trimethoprim/sulfamethoxazole 3 times a week,20 mg of omeprazole daily, 2 tablets of 5/500 hydrocodone/acetaminophen each night, and 10 mg of bisacodyl daily. He hadstopped taking all antiretroviral medications 2 months earlier be-cause of intolerance.
Ocular examination on referral revealed a best-corrected visualacuity of 20/25 in the right eye and counting fingers at 3 feet in theleft eye. An afferent pupillary defect was present on the left.External and slit-lamp examinations were unremarkable. Posteriorsegment examination showed areas of peripapillary and macularwhitening with scattered intraretinal hemorrhages in each eye(Figure 1, A and B) and two inactive retinochoroidal scars in thetemporal periphery of the left eye consistent with previous toxo-plasmic retinochoroiditis. Fluorescein angiography showed patchyretinal nonperfusion with late staining at the edge consistent withnerve fiber layer infarction (Figure 1, C and D). The cause of thenerve fiber layer infarcts was unknown, but because of the de-creased vision in the left eye and the history of ocular toxoplas-mosis, the patient was given 2 g of sulfadiazine daily, 75 mg ofpyrimethamine daily, 5 mg of leucovorin twice daily, and 600 mgof clindamycin four times daily.
During the next 2 weeks, the patient experienced progressive
Supported by a Career Development Award from Research toPrevent Blindness, Inc., New York, New York (Dr. Cunningham).
Reprint requests: Emmett T. Cunningham, Jr., MD, PhD, MPH,Pearl & Samuel J. Kimura Ocular Immunology Laboratory, FrancisI. Proctor Foundation, UCSF Medical Center, San Francisco, CA94143-0944; e-mail: [email protected]
542 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

abdominal pain, nausea, bloating, and loss of appetite for which hewas admitted to the hospital. During this time, his vision decreasedto hand motions in both eyes. Posterior segment examinationshowed massive, confluent peripapillary and macular whitening(Figure 2, A and B). A repeat fluorescein angiogram showedenlargement in the areas of nonperfusion, and late staining of theinvolved vessels.
The toxoplasmic retinochoroidal scars in the left eye remainedinactive. Laboratory testing at that time showed a serum amylaselevel of 2,400 U/L (normal range, 19–91 U/L), a serum lipase levelof 146 U/dL (normal range, 1–35 U/dL), and an anion gap acidosis.Retrospective review of the patient’s chemistry panel at the onsetof his visual symptoms showed a similar anion gap acidosis thathad gone unrecognized. The patient was diagnosed with acutepancreatitis with secondary Purtscher retinopathy. The toxoplas-mosis therapy, the antilymphoma medication (diethylhomosper-mine), and thePneumocystis cariniiprophylaxis (160/800 tri-methoprim/sulfamethoxazole) were discontinued. Four weeks afterpresentation, the patient’s visual acuity improved to 20/20 in theright eye and 20/80 in the left eye. He was subsequently lost tofollow-up.
Discussion
Although HIV retinopathy is the most commoncause of retinal whitening and nonperfusion in an
HIV-positive patient, the temporal correlation be-tween our patient’s ocular findings and the onset ofacute pancreatitis strongly suggests that our patienthad Purtscher retinopathy. Moreover, the partialresolution of our patient’s vision loss and fundusfindings after drug discontinuation strongly sug-gests that the pancreatitis and Purtscher retinopathywere drug-induced.
Purtscher retinopathy can occur after severe headtrauma, as first described by Purtscher himself in1910,5 or in association with other conditions, includ-ing thoracic trauma, childbirth, renal failure, pancre-atitis, barotrauma, retrobulbar anesthesia, and connec-tive tissue disorders.6 Although the pathogenesis ofPurtscher retinopathy is likely to be multifactorial, apossible shared mechanism may involve embolic ret-inal arteriolar obstruction. Various forms of embolihave been implicated, including air, fat, fibrin clots,and leukocyte aggregates.6 In acute pancreatitis, cur-rent evidence suggests that leukoemboli form whenpancreatic damage releases proteolytic enzymes intothe systemic circulation, thereby causing activation of
Fig. 1. Color (A, B) and fluorescein angiographic (C, D) images of the right and left posterior segments taken at presentation show peripapillaryand macular whitening with corresponding areas of nonperfusion.
543BRIEF REPORTS

the complement cascade and the formation of C5a-induced leukocyte, platelet, and fibrin aggregates.6
Our case of Purtscher retinopathy after drug-in-duced pancreatitis in an HIV-positive patient is, to ourknowledge, the first to be reported in the literature.The diagnosis of acute pancreatitis can be difficult, asit was in our patient, because pancreatitis is often mildor clinically silent in patients with AIDS. In fact,although autopsy studies indicate that as many as 90%of patients with AIDS have pancreatitis at the time oftheir death,7 fewer than 10% of HIV-positive patientswith pancreatitis seek medical attention.7 AIDS-spe-cific causes of pancreatitis include opportunistic in-fections, tumors, and most importantly, adverse drugreactions.7,8 HIV-positive patients are often prescribedcomplex drug regimens that include antiretroviralagents and a number of chemotherapeutic and prophy-lactic medications that can be individually or addi-tively toxic to the pancreas. The agents that have been
implicated most often in pancreatitis in HIV-positivepatients include pentamidine, dideoxyinosine, anddideoxycytidine, although trimethoprim–sulfamethox-azole, which was used by our patient, has also beenlinked to pancreatitis in this population.8
In summary, Purtscher retinopathy should be in-cluded in the differential diagnosis of HIV retinopa-thy, particularly because of the prevalence and life-threatening potential of unrecognized pancreatitis inthis population of patients. Clues to the diagnosis ofPurtscher retinopathy in our patient included extensiveand progressive retinal ischemia in the setting of se-vere abdominal pain. Serum amylase and lipase levelscan be used to confirm the diagnosis in patients sus-pected of having this disorder.
References1. Cunningham ET Jr, Margolis TP. Ocular manifestations of
HIV infection. N Engl J Med 1998;339:236–244.
Fig. 2. Color (A, B) and fluorescein angiographic (C, D) images of the right and left posterior segments taken 2 weeks after presentation showworsening of the peripapillary and macular whitening with corresponding enlargement in the areas of nonperfusion and late staining of the involvedvessels.
544 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

2. Akduman L, Feiner MA, Olk RJ, et al. Macular ischemia asa cause of decreased vision in a patient with acquired immu-nodeficiency syndrome. Am J Ophthalmol 1997;124:699–702.
3. Roth DB, McCabe CM, Davis JL. HIV-related occlusivevasculitis. Arch Ophthalmol 1999;117:696–698.
4. Brown GC, Brown MM, Hiller T, et al. Cotton-wool spots.Retina 1985;5:206–214.
5. Purtscher O. Noch unbekannte befunde nach schadeltrauma.Ber Dtsch Opththalmol Ges 1910;36:294–301.
6. Behrens-Baumann W, Scheurer G, Schroer H. Pathogenesisof Purtscher’s retinopathy: an experimental study. GraefesArch Clin Exp Ophthalmol 1992;1230:286–291.
7. Chehter EZ, Longo MA, Laudanna AA, et al. Involvement ofthe pancreas in AIDS: a prospective study of 109 post-mortems. AIDS 2000;14:1879–1886.
8. Dassopoulos T, Ehrenpreis ED. Acute pancreatitis in humanimmunodeficiency virus-infected patients: a review. Am JMed 1999;107:78–84.
RADIATION RETINOPATHY:The Role of Pentoxifylline
PRANAY GUPTA, MD,*BARRY MEISENBERG, MD,†PRADIP AMIN, MD,‡HOWARD D. POMERANZ, MD, PHD*
From the *Department of Ophthalmology, the†Uni-versity of Maryland Greenebaum Cancer Center, andthe‡Department of Radiation Oncology, University ofMaryland School of Medicine, Baltimore.
Radiation retinopathy is a potential vision-threateningconsequence of radiation treatment to the orbit or theadjacent structures in the brain. The primary damageoccurs in the retinal capillary endothelium. The vari-able extent of capillary nonperfusion based on radia-tion exposure of the endothelium leads to varyingdegrees of severity of retinopathy.1
Clinical reports have examined the useful effect ofpentoxifylline on the course of ocular diseases asso-ciated with capillary nonperfusion, such as centralretinal vein occlusion and diabetic retinopathy.2 Itsrheologic properties make it a potentially useful ther-apeutic agent in the treatment of radiation retinopathy.
We describe a patient with radiation-induced reti-nopathy. Treatment with oral pentoxifylline (400 mg 3times a day) was initiated. Within 8 months of treat-ment, a nearly full reversal of the effects of the radi-ation retinopathy was noted.
Case Report
A 28-year-old woman with a history of left temporal lobemedulloblastoma resection underwent whole brain and craniospi-nal radiotherapy of approximately 3,600 cGy in 20 fractions witha left temporal boost consisting of 1,980 cGy in 11 fractions.Approximately 10 months after the stereotactic radiosurgery, thepatient noticed a change in vision of her left eye. She described thechange as “a piece of gum stuck to the eyeball” that she “could seearound but not through.” The obscuration did not enlarge in sizebut underwent some variation in shape. She visited our clinic 2months after the onset of her visual symptoms.
Best-corrected visual acuity was 20/20 in the right eye and20/200 in the left eye. A left relative afferent pupillary defect waspresent. Slit-lamp examination findings, intraocular pressures, andocular motility were normal bilaterally. Goldmann visual fieldtesting showed a right homonymous superior quadrantanopsia,consistent with a left temporal lobe resection, and a paracentralscotoma approaching fixation inferotemporally in the left eye. Thedilated fundus examination showed normal-appearing optic nervesbilaterally. There were multiple small dot-and-blot and flame-shaped hemorrhages in the posterior pole of the left eye andcotton-wool spots just superior and nasal to the macula region(Figure 1). Fluorescein angiography showed areas of macularnonperfusion and capillary telangiectasias in the macular region(Figure 2).
A trial of oral pentoxifylline (400 mg 3 times a day) was begun.Eight months after initiation of pentoxifylline therapy, Snellenvisual acuity in the left eye had improved to 20/40. Results of heranterior segment and neuroophthalmologic examination remainedunchanged, but her dilated fundus examination showed a consid-erably decreased number of dot-and-blot hemorrhages and cotton-wool spots (Figure 3). A fluorescein angiogram showed normalperfusion of the previously nonperfused capillary beds (Figure 4)in comparison with the same region 8 months earlier (Figure 2),suggesting a significant improvement of the radiation-induced ret-inopathy in her left eye.
Discussion
First described in 1935, radiation-induced retinop-athy is a delayed effect of radiation to the retina andmay progress with time. The exact pathogenesis isuncertain, but selective destruction of the capillaryendothelial cells appears to be the principal mecha-nism. Vascular occlusion and atrophy of the capillar-ies may occur and result in retinal ischemia.3 Maculartelangiectatic vessels are a key feature, if not a hall-mark, of radiation damage.4
Many published studies discuss the pathogenesisand prevention of radiation retinopathy, but little in-formation has been published regarding treatment forthis condition. There is anecdotal evidence that lasertreatment has a therapeutic effect on radiation macularedema, particularly in less severe disease. Neovascu-larization appears to regress with panretinal photoco-agulation.4 To our knowledge, no therapeutic trial hasbeen reported for the treatment of ischemic changesinduced by radiation retinopathy.
Pentoxifylline is a synthetic xanthine derivative that
This study was supported in part by an unrestricted grant fromResearch to Prevent Blindness, Inc., New York, New York.
Reprint requests: Howard Pomeranz, MD, Department of Oph-thalmology, University of Minneapolis, Box 493, 420 Delaware St.SE, Minneapolis, MN 55455.
545BRIEF REPORTS

is used in treatment of peripheral vascular disorders.This drug has the ability to increase blood flow bydecreasing blood viscosity and improving the flexibil-ity of erythrocytes and leukocytes. In addition, it has adirect vasodilatory action.5 Pentoxifylline has beenshown to increase ocular blood flow in healthy pa-tients, in patients with nonproliferative diabetic reti-nopathy, and in patients with branch or central retinalvein occlusions.2–6
The patient described herein had nearly completereperfusion of the retinal capillary bed and resolutionof retinopathy in her left eye. A possible explanationfor this is the unique rheologic properties of pentoxi-fylline, which caused an increase in blood flow andoxygenation to the damaged retina. Improvement invision and reperfusion of retinal capillaries in patientswith untreated radiation retinopathy is not usual, but
Fig. 1. Red-free photograph of the left fundus at the initial examina-tion shows intraretinal hemorrhages and multiple cotton-wool spotssuperior and nasal to the macula.
Fig. 2. Early-phase fluorescein angiogram of the left eye at the initialexamination shows large areas of capillary nonfilling and telangiectasiain addition to blockage that corresponds to the areas of intraretinalhemorrhage.
Fig. 3. Red-free photograph of the left fundus at the 8-month exam-ination shows a significant reduction of the intraretinal hemorrhagesand cotton-wool spots.
Fig. 4. Early-phase fluorescein angiogram at the 8-month examinationshows reperfusion of the retinal capillary bed and resolution of thetelangiectatic vessels.
546 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

has been shown in some cases to occur. Therefore, theuse of pentoxifylline may have been coincidental tothe natural history of this condition. Because thispatient improved, however, we present this single caseto report our observation of the possible benefit ofpentoxifylline on the course of radiation retinopathy.A controlled, randomized prospective study would berequired to show a definitive effect of pentoxifylline inthe treatment of radiation retinopathy.
References1. Kinyoun JL, Lawrence BS, Barlow WE. Proliferative radiation
retinopathy. Arch Ophthalmol 1996;114:1097–1100.2. Jay WM, Aziz MZ, Chapman JM, et al. Effect of oral or
intravenous pentoxifylline on ocular and optic nerve bloodflow. Ophthalmic Res 1987;19:318–321.
3. Noble KG, Kupersmith MJ. Retinal vascular remodellingin radiation retinopathy. Br J Ophthalmol 1984;68:475–478.
4. Archer DB. Radiation retinopathy and papillopathy. In: YanoffM, Duker JS, eds. Ophthalmology, 1st ed. Philadelphia:Mosby, 1999:8.24.1–8.24.4.
5. Schmetterer L, Kemmler D, Breiteneder H, et al. A random-ized, placebo controlled, double-blind, crossover study of theeffect of pentoxifylline on ocular fundus pulsations. Am JOphthalmol 1996;121:169–176.
6. Kruger A, Matulla B, Wolzt M, et al. Short term oral pentoxi-fylline use increases choroidal blood flow in patients withage-related macular degeneration. Arch Ophthalmol 1998;116:27–30.
SELF–SEALING SCLEROTOMIES IN PARSPLANA VITRECTOMY
FREDERIK J. G. M. VAN KUIJK, MD, PHD,SAMI UWAYDAT, MD,BERNARD F. GODLEY, MD, PHD
From the Department of Ophthalmology and VisualSciences, University of Texas Medical Branch,Galveston, Texas.
Vitreoretinal surgery is usually performed throughsclerotomies that are placed in the anterior pars plana,3 to 4 mm posterior to the limbus, depending on the
phakic status of the eye. They are usually done with adisposable 20-gauge microvitreoretinal (MVR) bladedirected perpendicular to the sclera at the superotem-poral, inferotemporal, and superonasal quadrants. Vit-rectomy instruments are introduced through the twosuperior sclerotomy sites, and all three sclerotomiesmust be closed with a 7-0 coated Vicryl interruptedsuture at the end of surgery. Complications related tothe sclerotomy sites are vitreous incarceration, drag-ging of the retina, entry site breaks, injury to theciliary body, fibrovascular downgrowth, suture protru-sion, wound dehiscence, and difficulty in maintainingintraocular pressure during closure of the inferotem-poral sclerotomy after removal of the infusion cannu-la.1 To overcome these problems, several investigatorshave reported the use of self-sealing pars plana scle-rotomies.1–4 Initially, Chen et al1 reported the use ofscleral tunnels directed radially in the anterior to pos-terior direction. In a later study, they modified theirmethod by placing the tunnels in a circumferentialdirection parallel to the limbus, but the tunnels wereconstructed with the entrance away from the surgeon.3
In addition, the inferotemporal tunnel for the cannulawas constructedconventionally with an MVR blade.In this study, we created scleral tunnels parallel to thecorneoscleral limbus, with the entrance of the tunneltoward the surgeon, which is different from the previ-ous methods (Figure 1).1–4 In addition, the site for thecannula was created as a self-sealing sclerotomy. Fur-thermore, we performed the procedure on more patientsto establish whether this approach would be contraindi-cated in some patients.
Supported by an unrestricted grant from Research to PreventBlindness, Inc., New York, New York. Dr. Godley is an RPB SybilB. Harrington scholar.
None of the authors has proprietary interest in any of the prod-ucts mentioned in this article.
The material in this paper was presented in part at the annualARVO meeting, Ft. Lauderdale, Florida, April 30–May 4, 2000and at Club Vit, Sarasota, Florida, May 18–20, 2000.
Reprint requests: Bernard F. Godley, MD, PhD, 336 ClinicalScience Building, Department of Ophthalmology and Visual Sci-ences, The University of Texas Medical Branch, Galveston, TX77550-0787; e-mail: [email protected]
Fig. 1. View through the microscope of the right eye. The self-retaining cannula has been inserted inferotemporally through a self-sealing sclerotomy. The two superiorly located sclerotomies have theentry ports (straight lines) of the tunnels (dashed lines) directed towardthe surgeon.
547BRIEF REPORTS

Methods
We performed 120 self-sealing sclerotomies on 40consecutive patients, using a modification of themethod initially described by Chen et al1 and modifiedby Kwok et al.3 Chen et al1 constructed scleral tunnelsperpendicular to the limbus, and Kwok et al3 modifiedthe procedure by creating scleral tunnels parallel to thelimbus. We constructed scleral tunnels 3.0 mm poste-rior to the limbus, with the entry of the tunnels posi-tioned superiorly toward the surgeon, instead of awayfrom the surgeon, and the tunnel itself directed infe-riorly and parallel to the limbus (Figure 1). To stan-dardize the depth of the initial scleral incision, aguarded beaver blade (depth, 0.3 mm) was used. Sub-sequently a 1.5-mm scleral tunnel was made with a
crescent knife (width, 2.0 mm) (Alcon, Forth Worth,TX), and the tunnel was completed by using a blackMVR blade (Laseredge; Bausch & Lomb Surgical,Claremont, CA). The cannulas we used were a straight6.0-mm and a Weiss self-retaining 5.0-mm cannula(DORC, Kingston, NH).
Indications for vitrectomy included proliferative di-abetic retinopathy, retinal detachment, endophthalmi-tis, dropped nucleus, and central retinal vein occlu-sion. Additional intraoperative procedures performedincluded scleral buckle, endolaser, membrane peel,pars plana lensectomy, air–gas fluid exchange (SF6 orC3F8), and silicone oil injection. The same surgeon(B.F.G.) constructed all the scleral tunnels and waspresent during the entire procedure in each case. In
Table 1. Patients Who Underwent a Pars Plana Vitrectomy (PPV) With Sutureless Sclerotomies
Patient Age, yr/sex Diagnosis Procedure Intraoperative complications
IOP
POD 1 POD 30
1 61/F RRD PPV, EL, SF6 14 122 54/M RRD PPV, SB, C3F8 21 163 40/F PDR, VH, ERM OS PPV, EL, EMP Leak at 2; sutured 17 314 53/F Tractional macular edema OD PPV, EMP 7 135 46/F PDR, cataract, TRD PPV, EL, EMP, C3F8, phaco 27 106 36/M PDR, TRD OS PPV, EMP, EL, AFX 23 227 57/M Pseudophake RD OS PPV, SB, cryo, C3F8 21 138 45/M PDR, NVG OD PPV, EL 14 289 30/M PDR, VH OD PPV, EMP, EL Leak at 4, 11; sutured 11 12
10 15/M Traumatic VH, cataract OD PPV, PPL Leak at 2, 4, 11; sutured 40 1811 73/F PDR, VH OS PPV, EMP, EL Infusion extruded; choroidals 18 NA12 70/F Cataract, PDR, tractional macular detachment OS Phaco, PPV, EL, C3F8 Procedure was interrupted 21 NA13 62/M PDR, TRD, ERM OD PPV, EL, EMP, AFX 14 NA14 29/M PVR, chronic RD OD PPV, PPL, SB, C3F8 Leak at 11; sutured 19 1315 29/F PDR, TRD, RRD OD PPV, silicone oil, EL 16 1916 54/F PDR, VH OS PPV, EL, EMP, AFX 13 917 51/M RRD, macular hole OS PPV, SB, C3F8 23 2518 58/F Dropped nucleus OD PPV, PPL 11 2019 25/M PDR, TRD, ERM OD PPV, EMP, EL Leak at 11; sutured 12 920 84/M Pseudophake RRD OS PPV, SB, C3F8 31 2221 49/F PDR, VH, macular hole OD PPV, EMP, EL, C3F8 Infusion extruded 17 1122 38/M PDR, TRD OD PPV, EMP, EL, AFX 16 2123 53/F PDR, TRD OD PPV, EL, EMP 12 1224 60/F Endophthalmitis OD PPV, intravitreal vancomycin 17 1425 72/M PDR, TRD, VH OS PPV, EL, EMP, AFX 16 1726 46/F PDR, TRD, VH OS PPV, EMP 9 2627 64/F Dropped nucleus OS PPV, PPL Infusion extruded; choroidals 4 1228 56/F Pseudophake RRD OD PPV, SB, C3F8 17 1829 59/F VH, RRD OS PPV, C3F8 15 1030 70/M CRVO OS PPV, TPA Choroidals at 4 30 .4031 43/M VH, PDR OD PPV, EL Entry site break at 2 22 1332 45/F VH, PDR OD PPV 13 1433 54/M PDR, TRD, macular hole OD PPV, EMP Bleeding at 11 into vitrectomy 16 1434 41/M Cataract, vitreous membrane OS PPV, PPL Tunnel at 2 burned by phaco 34 5035 61/M Pseudophake RRD OD PPV, 240 SB, C3F8 26 1736 49/F PDR, VH OD PPV 13 1537 40/M PDR, TRD, ERM OD PPV, EMP 7 738 65/F Cataract, vitreous-macular traction OD Phaco IOL, PPV 7 639 38/M Dropped nucleus OS PPV, PPL Leak at 4; sutured 20 1640 58/M Pseudophake RRD, PVR OS PPV, SB, PFO, EMP, SO 22 18
IOP, intraocular pressure; POD, postoperative day; RRD, rhegmatogenous retinal detachment; EL, endolaser; SB, scleral buckle; PDR, proliferativediabetic retinopathy; VH, vitreous hemorrhage; ERM, epiretinal membrane; OS, left eye; EMP, ERM peel; OD, right eye; TRD, tractional retinal detachment;phaco, phacoemulsification; AFX, air–fluid exchange; cryo, cryocoagulation; NVG, neovascular glaucoma; NA, not applicable; PPL, pars plana lensectomy;CRVO, central retinal vein occulsion; TPA, tissue plasminogen activator; IOL, intraocular lens; PFO, perfluoro-octane.
548 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 57 ● NUMBER 5

nine cases, corneal topography or keratometry wasperformed before, 1 week after, and 1 month aftersurgery. Six patients were included in the series of 40patients, and three additional patients were treatedwith conventional sutured sclerotomy sites, as de-scribed in the introduction, to evaluate the effect ofsutureless sclerotomies on corneal refractive power.
Results
The indications and results in this series of 40patients are shown in Table 1. Nine sclerotomies re-quired a suture because of a leak. All occurred inpatients 40 years of age or younger. In two cases, theinfusion cannula extruded during the procedure. Thiswas related to indirect ophthalmoscopy with indenta-tion to examine the retina for entry site breaks. Wethen changed from a 6.0-mm straight cannula to acurved Weiss self-retaining 5.0-mm cannula (DORC),which can be secured by partial rotation. Subse-quently, one additional cannula extrusion occurred,and further recurrences were prevented by placing asingle retaining suture. One patient had an entry sitebreak with a localized retinal detachment. No cases ofhypotony or endophthalmitis developed. The patientwith the central retinal vein occlusion developed neo-vascular glaucoma with an intraocular pressure ofmore than 50 mmHg, but no leaks were noted at thesite of the self-sealing sclerotomies.
Effects on corneal curvature are shown in Table 2.Arciniegas and Amaya5 reported in rabbit eyes that asclerotomy parallel to the limbus leads to flattening inthe meridian where the surgery is performed and slightsteepening of the orthogonal meridian. We found no
significant difference in average keratometry valuesbefore and after surgery in sutured and suturelesssclerotomies.
Discussion
Self-sealing incisions were pioneered by cataractsurgeons and subsequently introduced into vitreoreti-nal surgery.1–4 The goal of this technique is to avoidthe use of sutures to close sclerotomy sites at the endof vitreoretinal surgery to maintain intraocular pres-sure. Intraoperatively, there is no need to use plugsbecause the sclerotomy will seal each time an instru-ment is removed. Both these factors will shorten theoperating time by as much as 20%, depending on thelength of the procedure. We found that even in longercases in which multiple instruments, including scis-sors and lighted forceps, were passed through thesclerotomy sites, no leaks were noted. The single mostimportant risk factor for leaks was patient age. All theleaks in this series occurred in patients younger than40 years of age. We attribute this to the fact that thesclera of younger patients is much less rigid,6 whichmakes it more difficult to construct self-sealing tun-nels at a depth of half thescleral thickness. Interest-ingly, Lam et al7 reported the successful use of theoriginal radially oriented scleral tunnel by Chen et al1
in eight eyes of children 8 to 48 months of age. Onepatient in our series developed shortness of breath be-cause of acute exacerbation of pulmonary edema, andwe interrupted the surgical procedure by removing ourinstruments and the cannula. Because of the self-seal-ing sclerotomies, the anesthesiologist was able to initi-
Table 2. Comparison of Changes in the Corneal Curvature With Sutureless and Sutured Sclerotomies
Patient Preop avK POD 7 avK DK7 POD 30 avK DK30
Sutureless sclerotomies1 43.05 42.9 20.15 42.83 20.222 42.25 41.75 20.5 42.05 20.23 45.7 46.26 0.56 44.21 21.494 43 42.8 20.2 42.88 20.125 41.9 40.83 21.07 43.28 1.386 43.86 45.6 1.74 45.21 1.35Mean 0.06 0.12
Sutured sclerotomies1 43.84 43.73 20.11 43.64 20.22 44.56 44.32 20.24 44.67 0.113 43.4 43.95 0.55 43.9 0.5Mean 0.07 0.14
Preop avK, averaged preoperative K reading taken 1–7 days before surgery; POD 7 avK, averaged K reading done on the 7thpostoperative day; DK7, change in the averaged corneal curvature on the 7th postoperative day; POD 30 avK, averaged K reading doneon the 30th postoperative day; DK30, change in the averaged corneal curvature on the 30th postoperative day.
549BRIEF REPORTS

ate resuscitation immediately, and the vitreoretinalsurgery was successfully completed at a later date.
Our technique differs from techniques previouslyused in that the entries of the tunnels are constructedtoward the surgeon. This facilitates the entry of in-struments and avoids interference with the nose orcannula. We also found that the guarded beaver bladeis useful because it standardizes the depth of the initialincision in the sclera. This modification allows foreach tunnel to be constructed at approximately half thescleral thickness, which minimizes anterior flap tearsor inadvertent entry into the posterior chamber, bothof which will result in the need of suture to seal thesclerotomy. Kwok et al3 used a 20-gauge hypodermicneedle to perforate the sclera at the end of the tunnelto avoid accidental scleral flap lacerations made by thesharp MVR blade. We also found that the black MVRblade used in this series (Laseredge; Bausch & LombSurgical) could be safely used. A green MVR blade(V-Lance knife; Alcon) used in two patients not partof this series caused scleral flap lacerations in fourtunnels, two of which leaked, requiring a suture.
Changing the direction of the scleral tunnel entrydid not reduce the success rate of this technique,which is 90% in eyes of patients older than 40 years.By comparison, Rahman et al8 reported a success rateof 76.6% with radially oriented tunnels. Previous re-ports did not include information on the age of thepatients, and we found that young age is an importantrisk factor for failure of this technique. In the 40 eyesreported in this study, none developed postoperativeendophthalmitis. It appears that sutureless scleroto-mies are safe in pars plana vitrectomy and do notinduce significant corneal astigmatism. In this study,sutureless sclerotomies in patients younger than 40years of age are associated with a higher rate of leaks(failure of the tunnel to self-seal) requiring sutures.The safety of this procedure and risk of complicationswill need to be established in more patients.
References1. Chen JC. Sutureless pars plana vitrectomy through self-sealing
sclerotomies. Arch Ophthalmol 1996;114:1273–1275.2. Milibak T, Suveges I. Complications of sutureless pars plana
vitrectomy through self-sealing sclerotomies. Arch Ophthal-mol 1998;116:119.
3. Kwok AKH, Tham CCY, Lam DSC, et al. Modified suturelesssclerotomies in pars plana vitrectomy. Am J Ophthalmol 1999;127:731–733.
4. Jackson T. Modified sutureless sclerotomies in pars planavitrectomy. Am J Ophthalmol 2000;129:116–117.
5. Arciniegas A, Amaya LE. Experimental modification of thecorneal curvature by means of scleral surgery. Ann Ophthal-mol 1984;16:1155–1166.
6. Michaels DD. Ocular disease in the elderly. In: Rosenbloom
AA Jr, Morgan MW, eds. Vision and Aging, 2nd ed. Boston:Butterworth-Heinemann, 1992;111–159.
7. Lam DSC, Chua JKH, Leung ATS, et al. Sutureless pars planaanterior vitrectomy through self-sealing sclerotomies in chil-dren. Arch Ophthalmol 2000;118:850–851.
8. Rahman R, Rosen PH, Riddell, C, et al. Self-sealing sclerot-omies for sutureless pars plana vitrectomy. Ophthalmic SurgLasers 2000;31:462–466.
DIFFUSE UVEAL MELANOMAPRESENTING AS AN AMELANOTICCYSTIC EPIBULBAR LESION
JERRY A. SHIELDS, MD,*RALPH C. EAGLE, JR, MD,†CAROL L. SHIELDS, MD,*ARUN D. SINGH, MD,* LOV K. SARIN, MD‡
From the *Oncology Service, the†Pathology De-partment, and the‡Retina Service, Wills Eye Hos-pital, Thomas Jefferson University, Philadelphia,Pennsylvania.
Uveal malignant melanoma can assume a variety ofgrowth patterns.1,2 Diffuse uveal melanoma is an ag-gressive variant that grows in a relatively flat pat-tern.3,4 As compared to the nodular uveal melanoma,it usually has a more malignant cell type, greatertendency toward extrascleral extension, and a highermortality. Extrascleral extension of a diffuse uvealmelanoma usually presents as a pigmented epibulbarmass in the ciliary body area.1,2 We report a largelyamelanotic diffuse uveal melanoma in which the ini-tial manifestation was a nonpigmented, pseudocystic,salmon-colored epibulbar mass that extended over thesuperior aspect of the cornea.
Case Report
In December 1998, a 76-year-old man noticed gradual onset ofpainless blurred vision in his left eye. Ocular examination by hislocal ophthalmologist revealed no abnormal findings. He returned3 months later complaining of worsening vision and a mass be-neath his left upper eyelid. Examination revealed an epibulbarmass and choroidal thickening. He was referred to the OncologyService for further evaluation.
Supported by the Eye Tumor Research Foundation, Philadel-phia, PA; the Award of Merit in Retina Research, Houston, Texas(Dr. J.A. Shields); the Macula Foundation, New York, New York(Dr. C.L. Shields); and the Noel and Sarah Simmonds Endowmentfor Ophthalmic Pathology, Wills Eye Hospital (Dr. Eagle).
Presented at the meeting of the Eastern Ophthalmic PathologySociety, Philadelphia, Pennsylvania, September 22, 2000.
Reprint requests: Jerry A. Shields, MD, Oncology Service, WillsEye Hospital, 900 Walnut Street, Philadelphia, PA 19107.
550 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

His medical history included systemic hypertension. He hadherpes zoster ophthalmicus on the right side in 1992 and bilateralcataract surgery in 1993. Ocular examination revealed pseudopha-kic visual acuities of 6/6 in his right eye and 6/60 in his left eye.Intraocular pressures were 19 mmHg in the right eye and 10 mmHgin the left. The right eye was otherwise normal. Examination of theleft eye showed a fleshy, salmon-colored mass deep to the con-junctival epithelium superonasally with an apparent semiopaquecyst that overhung the cornea and appeared to contain mucoid orpurulent material (Figure 1). The temporal part of the iris stromawas displaced anteriorly causing focal narrowing of the anteriorchamber angle, and there was diffuse iris neovascularization. Poorpupillary dilation and a hazy intraocular lens precluded a clearfundus view, but there was a diffuse amelanotic thickening of thesuperior half of the choroid and a retinal detachment. Ultrasonog-raphy confirmed choroidal thickening with high internal reflectivityand a maximum thickness of 4.7 mm (Figure 2). Blood count, liverenzymes, and a chest radiograph were normal.
Our differential diagnosis included lymphoma, metastasis, andintraocular extension of conjunctival mucoepidermoid carcinoma.Uveal melanoma was considered unlikely because a cystic lesionoverhanging the cornea would be an unlikely manifestation ofextraocular extension of a melanoma. An excisional biopsy wasperformed of the epibulbar mass. Histopathologic studies sug-gested melanoma and the eye was enucleated.
Pathologic Findings
Conjunctival Mass
The specimen measured 113 8 3 2.5 mm. Histopathologicexamination showed a diffuse cellular infiltrate involving the con-junctival stroma but sparing the epithelium. It was composed ofround, poorly differentiated, loosely cohesive, nonpigmented cellswith relatively small nuclei and prominent nucleoli (Figure 3).Numerous mitotic figures were present. The Fontana–Masson stainfor melanin was negative. Immunohistochemical stains showedintense cytoplasmic immunoreactivity for vimentin, minimal im-munoreactivity to melanoma specific antigen HMB-45, and noreactivity to leukocyte common antigen, cytokeratin marker CAM5.2, lysozyme, myoglobin, muscle specific actin, smooth muscleactin, and desmin. The diagnosis was poorly differentiated nonepi-thelial malignant neoplasm, most consistent with melanoma. Basedon these findings, the lesion was thought to represent extraocularextension of a uveal melanoma.
Fig. 1. The superior portion of the mass has a fleshy, salmon-coloredappearance, and the inferior portion has a cyst containing mucoid orpurulent material.
Fig. 2. B-scan ultrasonogram shows diffuse thickening of the choroidwith high internal reflectivity.
Fig. 3. The epibulbar mass is composed of loosely cohesive, round,malignant cells without cytoplasmic pigment (hematoxylin and eosin;original magnification3100).
Fig. 4. Gross appearance of sectioned globe, showing diffuse amela-notic tumor of the uveal tract.
551BRIEF REPORTS

Eyeball
On gross examination, the normal sized eye showed no transil-lumination abnormalities. The angle was partly occluded by pe-ripheral anterior synechiae, and a posterior chamber intraocularlens was present. The superior iris leaf was displaced forward bythe anterior part of a diffuse white mass that thickened the ciliarybody and choroid. It measured 18 mm in length and 4 mm inthickness and extended posteriorly to the optic nerve (Figure 4).
Microscopic examination revealed a fibrovascular membrane onthe anterior surface of the iris. The superior iris leaf was displacedanteriorly by a retroiridic mass that extended posteriorly to involvethe superior part of the ciliary body and choroid, reaching the opticnerve. In theanterior part of the choroid, these cells were looselycohesive and resembled the cells seen in the epibulbar surface(Figure 5). The more posterior part of the tumor was composedof large mitotically active epithelioid cells (Figure 6). Fifty-fivemitotic figures were counted in 40 high-power fields. Repeatimmunohistochemistry of the intraocular part of the tumor gavesimilar, inconclusive results; the tumor cells showed intenseimmunoreactivity for vimentin, but HMB 45 and S-100 proteinwere nonreactive. However, the additional deeper sections pre-pared for immunohistochemical analysis disclosed a small focus
of intensely pigmented cells (Figure 7) within the largely amela-notic tumor, which confirmed that the tumor was a melanoma.The sections disclosed no residual epibulbar tumor.
The final diagnosis was diffuse choroidal melanoma of theepithelioid cell type with extraocular extension. Within 6 months,metastatic melanoma to the liver and bone developed, and thepatient died shortly thereafter.
Discussion
Uveal melanoma usually presents as an elevatedpigmented mass with a characteristic dome or mush-room configuration. The diagnosis is readily madewith ophthalmoscopy by an experienced clinician.1,2
Diffuse uveal melanoma is a relatively uncommonvariant in which the tumor grows in a flat or slightlyelevated pattern.3–5 There is often a delay in diagnosisand misdirected therapy before a diffuse melanoma isfinally recognized. Many diffuse uveal melanomas arenonpigmented, making the diagnosis even morechallenging.
Extraocular extension is found in 8% to 14% ofeyes enucleated for ciliary body or choroidal melano-ma.5,6 Diffuse uveal melanomas are generally moreaggressive and show extrascleral extension more fre-quently. In the report of diffuse melanomas by Font etal,4 there was a 39% incidence of extraocular exten-sion. In the series by Shields et al,5 there was a 50%incidence of extraocular extension in eyes that wereenucleated. In cases of diffuse melanoma, the extra-scleral extension is usually in the ciliary body regionand is usually pigmented, findings that should suggestthe diagnosis clinically. When there is extraocularextension of an amelanotic melanoma, the extrascleralcomponent usually appears as a solid lesion withoutcysts.
The case reported here was highly unusual in thatthe diffuse uveal melanoma presented initially as a
Fig. 5. The anterior part of the tumor is composed of round, looselycohesive, nonpigmented malignant cells (hematoxylin and eosin; orig-inal magnification3250).
Fig. 6. The more posterior part of the tumor is composed of mitoti-cally active epithelioid cells with prominent mitoses (hematoxylin andeosin; original magnification3250).
Fig. 7. Focus of pigmented tumor within the deeper part of the tumor,consistent with malignant melanoma (hematoxylin and eosin; originalmagnification3100).
552 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

salmon-colored, epibulbar mass that was reminiscentof conjunctival lymphoma. However, a portion of theepibulbar mass overhung the cornea and resembled acyst filled with mucus or purulent material, makingthe diagnosis of lymphoma unlikely. The cystic ap-pearance was consistent with a mucoepidermoid car-cinoma of the conjunctiva, a tumor that has a tendencyto extend into the eye and develop a cystic compo-nent.7–10 Metastatic cancer was also a diagnostic con-sideration in our patient, because it can also present asa uveal thickening and an amelanotic epibulbarmass.11,12Although melanoma was considered, it wasthought to be unlikely based on the aforementionedclinical features.
The histopathologic diagnosis in our case was ini-tially challenging. The extraocular component of thetumor was composed predominantly ofround,loosely cohesive malignant cells that lacked cyto-plasmic pigment. Although intensely immunoreac-tive for vimentin, the cells showed only minimalimmunoreactivity for melanoma specific antigenHMB-45. However, the choroid contained a focusof heavily pigmented tumor cells in deeper his-topathologic sections, supporting the diagnosis ofmelanoma. In addition, the subsequent clinicalcourse with metastatic melanoma to the liver sup-ported the diagnosis.
In summary, we report a highly unusual, if notunique, presentation of a uveal melanoma. The firstmanifestation of the diffuse, amelanotic uveal tumorwas a fleshy, salmon-colored epibulbar lesion with apseudocyst that overhung the cornea. Cliniciansshould be cognizant of atypical manifestations ofuveal melanoma to make a correct diagnosis and toinstitute appropriate therapy.
References1. Shields JA, Shields CL. Posterior uveal melanoma: clinical
and pathologic features. In: Shields JA, Shields CL, eds.Intraocular Tumors. A Text and Atlas. Philadelphia: WBSaunders, 1996:117–136.
2. Shields JA, Shields CL. Clinical features of posterior uvealmelanoma. In: Shields JA, Shields CL, eds. Atlas of Intraoc-ular Tumors. Philadelphia: Lippincott Williams & Wilkins,1999:74–93.
3. Reese AB, Howard GM. Flat uveal melanomas. Am J Oph-thalmol 1967;64:1021–1028.
4. Font RL, Spaulding AG, Zimmerman LE. Diffuse malignantmelanoma of the uveal tract: a clinicopathologic report of 54cases. Trans Am Acad Ophthalmol Otolaryngol 1968;72:877–895.
5. Shields CL, Shields JA, DePotter P, et al. Diffuse choroidalmelanoma: clinical features predictive of metastasis. ArchOphthalmol 1996;114:956–963.
6. Collaborative Ocular Melanoma Study Group. Histopatho-logic characteristics of uveal melanomas in eyes enucleated
from the Collaborative Ocular Melanoma Study. COMS re-port no. 6. Am J Ophthalmol 1998;125:745–766.
7. Shields JA, Shields CL. Mucoepidermoid carcinoma of theconjunctiva with intraocular invasion. In: Shields JA, ShieldsCL, eds. Atlas of Eyelid and Conjunctival Tumors. Philadel-phia: Lippincott Williams & Wilkins, 1999;241.
8. Rao NA, Font RL. Mucoepidermoid carcinoma of the con-junctiva. Cancer 1976;38:1699–1709.
9. Brownstein S. Mucoepidermoid carcinoma of the conjunctivawith intraocular invasion. Ophthalmology 1981;88:1126–1130.
10. Gunduz K, Shields JA, Shields CL, et al. Intraocular neo-plastic cyst from mucoepidermoid carcinoma of the conjunc-tiva. Arch Ophthalmol 1998;116:1521–1523.
11. Shields JA, Shields CL, Eagle RC Jr, Gunduz K, Lin B.Diffuse ocular metastases as an initial sign of metastatic lungcancer. Ophthalmic Surg Lasers 1998;29:598–601.
12. Kiratli H, Shields CL, Shields JA, et al. Metastatic tumors tothe conjunctiva. Report of ten cases. Br J Ophthalmol1996;80:5–8.
VISUAL LOSS AFTER RENALTRANSPLANTATION
AMIR YAMANI, MD,*BRENDA A. MYERS–POWELL, MD, PHD,†SCOTT M. WHITCUP, MD,†STEVEN B. COHEN, MD,‡ERIC D. KANTER, MD,‡BRUCE KAPLAN, MD, PHD,§MARCO A. ZARBIN, MD, PHD*
From the *Department of Ophthalmology, Universityof Medicine and Dentistry of New Jersey, New JerseyMedical School, Newark;†The National Eye Institute,National Institutes of Health, Bethesda, Maryland;‡Saint Barnabas Medical Center, Livingston, NewJersey; and§The Division of Nephrology, MichiganUniversity Health System, Ann Arbor.
Visual loss is a rare but devastating complication oforgan transplantation. Previous reports have describedtransplant patients who developed retinal microvascu-lopathy and sudden visual loss while receiving cyclo-sporine A (CsA) plus conditioning therapy, includingcyclophosphamide (CY), busulfan, and/or total bodyirradiation (TBI).1–5
We report the case of a 52-year-old white man with
Dr. Whitcup is currently affiliated with Allergan, Irvine,California.
Supported in part by Research to Prevent Blindness, Inc., NewYork, New York; The Eye Institute of New Jersey; and the NewJersey Lions Eye Research Foundation, Newark.
Reprint requests: Marco A. Zarbin, MD, PhD, Doctors OfficeCenter, 6th Floor, 90 Bergen St, Newark, NJ 07103-2499; e-mail:[email protected]
553BRIEF REPORTS

Table 1. Test Results
Test Result Normal Interpretation
CMV IgG Ab 0.04 ISR ,0.90 ISRSeronegative—absence of
prior exposureCMV IgM Ab 0.29 ISR ,0.90 ISR Negative
Toxoplasmosis IgG Ab 1.66 ISR ,0.90 ISRSeropositive—indicates
prior exposureToxoplasmosis IgM Ab 0.25 ISR ,0.90 ISR NegativeAntinuclear antibodies Negative Negative NegativeTotal complement CH100 49.0 units/mL 48–153 units/mL NormalAnti-DNA Ab Negative Negative NegativeSerum angiotensin
converting enzyme 103.4 nmol/mL/min 0.60–52.0 nmol/mL/min ElevatedAnticardiolipin IgG 7 0–14 NormalAnticardiolipin IgM 13 0–9 Increasedc-ANCA ,7 ,7 Negativep-ANCA ,7 ,7 Negative
ESRPerformed twice—15 mm/h,
11 mm/h Male 0–15 mm/h, female 0–20 mm/h NormalCryoglobulins Absent Absent NormalC3 compliment QN 0.703 g/L 0.86–1.84 g/L DecreasedLyme Ab (ELISA) 0.28 ISR ,0.9 ISR SeronegativeC4 compliment QN 0.196 g/L 0.20–0.59 g/L Low normal
MRI/MRA of brain andthorax
Questionable narrowedintracranial arteriole,otherwise normal
Pelvic MRV NormalLower extremity
electromyogram NormalEchocardiogram NormalMUGA scan NormalVitreous PCR for
Toxoplasmosis gondiiDNA Negative Negative Negative
Vitreous PCR for herpessimplex virus DNA Negative Negative Negative
Vitreous PCR for herpeszoster virus DNA Negative Negative Negative
Mg 1.15 mmol/L 0.66–1.10 mmol/L ElevatedWBC 10.5 3 10*9/L 4.0 3 10*9–10.5 3 10*9/L NormalHgb 129 g/L 135–170 g/L DecreasedHct 39.70% 39.8–52.0% DecreasedPlt 141 3 10*9/L 140–450 3 10*9/L NormalPolys 82% 50–75% ElevatedLymphocytes 9% 20–40% DecreasedAtypical lymphocytes 3% ElevatedAlbumin 31 g/L 30–55 g/L NormalTotal protein 50 g/L 60–85 g/L DecreasedGlucose 6.22 mmol/L 3.89–6.38 mmol/L NormalBun 17.14 mmol/L 3.57–9.28 mmol/L ElevatedCreatinine 167.96 mmol/L 70.72–159.12 mmol/L ElevatedNa 138 mmol/L 136–145 mmol/L NormalK 3.9 mmol/L 3.5–5.0 mmol/L NormalCl 107 mmol/L 96–106 mmol/L ElevatedCa 2.68 mmol/L 2.13–2.63 mmol/L NormalTotal bilirubin 10.26 mmol/L 3.42–20.52 mmol/L NormalAlk phos 58 U/L 30–136 U/L NormalSGOT 15 U/L 7–58 U/L Normal
CMV, cytomegalovirus; Ig, immunoglobulin; Ab, antibodies; DNA, deoxyribonucleic acid; c-ANCA, antineutrophil cytoplasmic anti-body; ESR, erythrocyte sedimentation rate; QN, quantitative; ELISA, enzyme-linked immunosorbent assay; MRI, magnetic resonanceimaging; MRA, magnetic resonance angiography; MRV, magnetic resonance venogram; MUGA, multiple gated acquisition scan; PCR,polymerase chain reaction; WBC, white blood cells; Hgb, hemoglobin; Hct, hematocrit; Plt, platelets; Polys, polymorphonuclearleukocytes; Alk phos, alkaline phosphatase; SGOT, aspartate aminotransferase; PTT, partial thromboplastin time; PT, prothrombin time;INR, international normalized ratio; HDL, high-density lipoprotein; VLDL, very low density lipoprotein.
554 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

a history of polycystic kidney disease and hyperten-sion who developed progressive retinal vasculopathy5 months after successful renal transplantation whilereceiving CsA without conditioning therapy. Al-though a definite etiology has not been determined,CsA-induced drug toxicity may be the cause.
Case Report
A 52-year-old white man with a history of polycystic renaldisease was referred for evaluation of acute progressive retinopathyof unknown etiology 5 months after receiving a renal transplant (inMay 1998) from an unrelated living donor. The patient reportedsudden, bilateral, painless blurring of vision whilewatching televi-sion. The visual loss rendered him unable to carry out activities ofdaily living without assistance. This episode was preceded by approx-imately 1 week of “troubles” with his vision. His medications at thetime of the visual symptoms included prednisone 10 mg orally daily,acyclovir 800 mg orally twice daily, cyclosporine 150 mg orally twicedaily (4.25 mg/kg/d), mycophenolatemofetil 1,000 mg orally twicedaily, trimethoprim 160 mg/sulfamethoxazole 800 mg orally daily,clotrimazole 10 mg orally four times daily, Cernevit (multivitamin)5 cc injection intravenously daily, omeprazole 20 mgorally daily,tamsulosin hydrochloride 0.4 mg orally daily, furosemide 40 mgorally daily, amlodipine besylate 5 mg orally daily, aspirin81 mg orally daily, temazepam 15 mg orally every night, niacin200 mg orally twice daily, alendronatesodium 10 mg orallydaily, and digoxin 0.125 mg orally daily. Of note, the patient hadreceived two doses of basiliximab, a monoclonal chimeric antibodydirected against the interleukin-2 receptor, during the perirenaltransplant period and an intravenous injection of glucagon 12 hoursbefore the onset of symptoms.
In addition to polycystic renal disease and renal transplantation,the patient’s medical history was significant for hypertension (10-year duration), hepatitis C without active hepatitis, a frozen leftvocal cord (1996) with spontaneous resolution after 6 months, andsteroid-induced acne. Three weeks before the onset of ocularsymptoms, the patient had rapidly progressive, bilateral lowerextremity edema associated with a 5-pound per week weight gainand bilateral lower extremity proximal muscle pain attributed topravastatin, which was therefore stopped. Eventually the lowerextremity edema improved significantly, and the pain resolved. Adeep venous thrombosis was ruled out with a magnetic resonanceangiogram. The patient denied a history of trauma, cold extremi-
ties, fevers, paresthesias, hearing loss, extensive bruising, bleedingproblems, or rash. His ophthalmic history was unremarkable exceptas noted above. The diagnostic work-up was unrevealing (Table 1).The patient was examined immediately by a retinal specialist, whodiagnosed cytomegalovirus (CMV) retinitis and started the patienton intravenous ganciclovir; the oral acyclovir was discontinued.However, the patient’s visual acuity progressively deteriorated.
On our initial examination, 167 days after renal transplantation,the patient’s vital signs were normal (blood pressure 110/70). Hisweight was 72 kg. His visual acuity without correction was 20/200in the right eye and 20/400 in the left. With pinhole correction,acuity was 20/400 in the right eye and 20/50 in the left. Externalexamination, visual field (confrontation) testing, and extraocularmotility were normal bilaterally. Slit-lamp examination was nota-ble for trace nuclear sclerosis bilaterally and trace posterior sub-capsular changes in the left. The anterior chambers were quiet, andthe vitreous was syneretic without cell or definite posterior vitreousdetachment.
Fundus examination of the right eye showed clear media, a flatretina, and a myopic peripapillary temporal crescent. Retinal whit-ening was present in the macula but spared the foveola, giving acherry red spot appearance, and the perivascular retina (Figure 1A).A few intraretinal hemorrhages and a moderate number of cotton-wool spots were present. The left eye showed a similar funduspattern as well as a Weiss ring in the vitreous cavity (Figure 1B).The clinical appearance was consistent with occlusive diseaseinvolving second and third order retinal vessels. The initial differ-ential diagnosis included Purtscher-like retinopathy, noninfectiousvasculitis with secondary vascular occlusion, or viral retinitis suchas progressive outer retinal necrosis. Intravenous acyclovir (400mg intravenously twice daily) was added to the medical regimen,which also included ganciclovir. Cyclosporine was discontinued 5days after the onset of visual loss. Cyclophosphamide 50 mg orallydaily and tacrolimus 1 mg orally daily were prescribed, and theprednisone dose was increased to 30 mg orally twice daily.
The patient’s visual acuity progressively deteriorated to handmotion at 1 foot in the right eye and count fingers at 1 foot in theleft over the next 3 weeks. Additional funduscopic findings in-cluded sclerosis of the arterioles, perivasculitis, development ofintraretinal hemorrhages extending to the equator (Figure 2), ve-nous beading, impaired central artery perfusion with minimal ar-terial flow observed at the optic nerve head (as determined bydigital compression of the globe), and pale and edematous opticdisks. The vitreous was quiet at all times, and no neovasculariza-tion of the disk or peripheral retina was noted. By the eleventh day
Table 1. Continued
Test Result Normal Interpretation
Inorganic phosphorous 0.775 mmol/L 0.808–15.504 mmol/L DecreasedCO2 27 mmol/L 24–30 mmol/L NormalCsA 250,258,250,384 ng/mLAmylase 44 U/L 25–143 U/L NormalLipase 11 U/L 7–58 U/L NormalUrinalysis NormalPTT 27 seconds 21.5–34.5 seconds NormalPT 13.3 seconds 10.7–13.7 seconds NormalINR 1.2Blood cultures Negative Negative NegativeCholesterol 5.65 mmol/L 3.11–5.18 mmol/L ElevatedTriglyceride 7.67 mmol/L 0.113–2.15 mmol/L ElevatedHDL cholesterol 0.57 mmol/L 0.83–1.86 mmol/L DecreasedVLDL calculated 136 mg/dL 10–40 mg/dL Elevated
555BRIEF REPORTS

after presentation, the ganciclovir was discontinued because webelieved that the patient did not have a CMV infection. Acyclovirwas also temporarily discontinued in preparation for a diagnosticvitreous tap on the eleventh day of follow-up (Table 1). However,it was resumed by the renal transplant team after the vitreous tapper routine post renal transplant prophylaxis. Seven weeks after theonset of ocular symptoms, the Uveitis Service of the National EyeInstitute (NEI) evaluated the patient and suggested that the historyand examination seemed most consistent with 1) bilateral vascularocclusion at the central retinal artery distal to the branching of thelong posterior ciliary arteries and 2) bilateral central retinal veinocclusion or stasis.
Fluorescein angiography was done on day 1 of presentation and2 weeks after presentation (Figure 3). The findings were consistentwith bilateral central retinal artery occlusion and bilateral partialimpairment of choroidal vascular filling. At the NEI, a focalelectroretinogram was performed, which showed diminished butdetectable waveforms bilaterally (not shown).
The patient’s condition appeared to stabilize 6 weeks afterpresentation, and the cyclophosphamide was discontinued. Pred-
nisone was tapered to 10 mg to preserve renal graft function.Aspirin was increased to 325 mg orally daily, and pentoxifyllinewas started. Gradually, the intraretinal hemorrhages cleared.
Thirty-three weeks after presentation, the patient developed ru-beosis iridis and elevated intraocular pressure in the right eye andunderwent panretinal photocoagulation in the right eye. The rubeo-sis regressed and the intraocular pressure normalized. Sixty-twoweeks after presentation, the patient developed vitreous hemor-rhage in the right eye associated with posterior vitreous detach-ment. At last follow-up (May 15, 2000), the visual acuity wasstable at 1/200 in the right eye and 20/200 in the left. The intraoc-ular pressure was 12 mmHg in the right eye and 14 mmHg in theleft. Fundus examination was notable for persistent parafovealretinal whitening, mild macular intraretinal lipid deposition,marked pallor of the optic nerve head, and attenuation of retinalvessel caliber at the optic nerve head.
Discussion
Potential causes of this patient’s retinal vascularocclusive disease include Purtscher-like retinopathydue to leukoembolization, hypercoagulability, nonin-
Fig. 1. A, Color fundus photograph (October 2, 1998) of the right eye.Macular whitening is present with foveal sparing. A few retinal hem-orrhages are present in the area centralis. There is attenuation ofvascular caliber at the optic nerve head, and cotton wool spots arepresent.B, Color fundus photograph (October 2, 1998) of the left eye.A similar picture is present.
Fig. 2. Significant intraretinal hemorrhage developed during the in-terval between October 2, 1998 and October 13, 1998.A, Right eye,October 13, 1998.B, Left eye, October 13, 1998.
556 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

fectious vasculitis with secondary retinal vessel occlu-sion, hypertension during or due to the transplantsurgery, and infectious retinitis, such as a viral retini-tis. Prednisone was used not only to preserve renalfunction but also to reduce the possibility of furtherleukoembolization or inflammation. Acyclovir wasadded to the ganciclovir to cover the possibility ofprogressive outer retinal necrosis. However, thesemedications also have toxicities including leukopeniaand renal toxicity. The medication regimen was re-viewed with the renal transplant team to preserve graftfunction.
This patient used a number of medications withreported ocular side effects (Table 2). The pattern ofretinal whitening in this patient is most suggestive ofretinal arteriolar occlusion, and we believe this sug-
gests that CsA may have played a role in the devel-opment of his condition. We offer this suggestioncautiously in view of the widespread use of cyclospor-ine for many years in solid organ recipients receivingno irradiation with few proposed cases of clinicallyevident retinal microvascular changes. It is possiblethat the observed retinal vascular changes are due toan unrecognized side effect of one or more of themany other medications used by the patient (e.g.,Simulect [East Hanover, NJ], which is relatively new).For example, cyclosporine has been implicated in thedevelopment of optic nerve head edema, in somecases associated with pseudotumor cerebri.6–8 It is notclear whether the retinal vascular changes seen in ourpatient, if due to cyclosporine or cyclosporine plus anunidentified adjuvant, share pathogenetic features
Fig. 3. A, Intravenous fluorescein angiogram (October 1, 1998) of the right eye shows focal areas of retinal capillary dropout with a pathologicallyenlarged foveal avascular zone.B, Left eye (October 1, 1998).C, Intravenous fluorescein angiogram (October 13, 1998) of the right eye. Dye wasfirst noted in the central artery at 23.9 seconds (not shown). Choroidal filling was evident at this time. Filling of the retinal vessels is incomplete. Theoptic disks stain with minimal leakage in late frames.D, Left eye (October 13, 1998). Findings in the left eye are similar.
557BRIEF REPORTS

with the development of optic nerve head edema.Previous reports have documented ischemic retinalmicrovasculopathy and visual loss in patients treatedwith CsA conditioned with TBI, busulfan, and/or CYfollowing bone marrow transplantation.2–4 Typicalfindings include multiple cotton wool spots, retinalhemorrhages, lipid deposits, focal arteriolar narrow-ing, and optic disk edema.2–4 Our patient’s vascularocclusive disease may be related to his CsA use, ashas been reported previously.5 Cyclosporine can causeendothelial toxicity. Cyclosporine A–induced vasculardamage may be related to direct endothelial cell inju-ry.5 In previous studies, withdrawal or dose reductionof CsA led to complete resolution of the retinopathyand restoration of vision.2–4 Lopez-Jimenez et al1 de-scribed cortical blindness (diagnosed by electroretino-
gram, visual evoked response, and electromyography)in a patient with normal fundi who received the sameregimen of medications as in the previous studiesdescribed above, which was reversed with discontin-uation of the CsA. The range of CsA dosing in theprevious studies ranged from 4 to 12 mg/kg/d, and ourpatient was using 4.0–8.0 mg/kg/d.1–4
Thus far only patients receiving CsA conditionedwith TBI, busulfan, and/or CY have been reported tohave ischemic fundus lesions, and the lesions werereversible with reduction or discontinuation ofCsA.1–4 Previous investigators concluded that CsAand conditioning were additive in causing capillary/arteriolar damage and were both necessary for themicrovasculopathy previously described.2–4 We sug-gest that CsA alone may be responsible; however,
Table 2. Pertinent Medication Adverse Reactions*
Medication Relevant Adverse Reactions
Cyclosporine Glomerular capillary thrombosis with pathologic changes resembling hemolytic–uremic syndrome, thrombosis of the renal microvasculature with platelet–fibrinthrombi occluding glomerular capillaries and afferent arterioles,microangiopathic hemolytic anemia, thrombocytopenia, hypertension, viralinfections, hepatotoxicity, leukopenia, lymphoma, septicemia, systemic and/orlocal fungal infections, abscesses, peripheral ischemia, herpes zoster, herpessimplex, bacterial infections, moniliasis, hyperuricemia, diabetes mellitus,cataract, conjunctivitis, eye pain
Prednisone May enhance secondary ocular infections due to fungi or viruses, hypertension,ecchymosis, impaired wound healing, pseudotumor cerebri, cataract, increasedintraocular pressure, diabetes mellitus
Amlodipine besylate Vasodilation, conjunctivitis, diplopia, eye pain, abnormal visual accommodation,xerophthalmia
Pravastatin CNS vascular lesions characterized by perivascular hemorrhages and edema inanimal studies, a chemically similar drug in this class produced optic nervedegeneration, retinal ganglion cell chromatolysis in animal studies, progressionof cataracts, ophthalmoplegia
Trimethoprim/sulfamethoxazole Photosensitivity, conjunctival and scleral injection, pancreatitis
Mycophenolate mofetil Leukocytosis, increase in certain types of infection, ecchymosis, peripheralvascular disease, thrombosis, vasodilation, hypercholesterolemia, hemorrhage,conjunctivitis, cataract
Temazepam Horizontal nystagmus
Furosemide Systemic vasculitis, necrotizing angiitis (both of which are systemichypersensitivity reactions)
Digoxin Visual disturbances with blurred or yellow vision
Niacin Toxic amblyopia, cystoid macular edema
Tamsulosin hydrochloride Orthostatic hypotension
Alendronate sodium Rarely uveitis
Aspirin Bleeding
Simulect (basiliximab) Hypercholesterolemia, viral infection, sepsis, aggravated hypertension,hypotension, arrhythmia, atrial fibrillation, diabetes mellitus, hemorrhage,thrombocytopenia, thrombosis, polycythemia, herpes simplex, herpes zoster,vascular disorder, cataract, conjunctivitis, infection
Adapted from Physicians Desk Reference, 53rd edition. Montvale, NJ: Medical Economics Company, 1999.
558 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

CsA, if not solely responsible, may, in the setting ofanother unknown underlying acquired or inherent con-dition, have stimulated these changes. In previousstudies, estimates of the incidence of retinal microvas-culopathy were biased by ascertainment of only symp-tomatic cases.2 The true incidence may be higher. In aprospective study, Bernauer et al4 discovered that 46%of transplant patients with ischemic fundi wereasymptomatic. Therefore it may be beneficial to in-clude ophthalmologists in the management of patientstaking CsA, particularly those patients taking CsA toprevent transplant rejection. Because in previous stud-ies1–4,6,8 as well as in our case study the onset ofsymptoms after starting CsA therapy ranged from 31to 332 days, routine ophthalmologic evaluations ofpatients using CsA should be considered, especiallyduring the first year of therapy.
References1. Lopez-Jimenez J, Sanchez A, Fernandez CS, et al. Cyclospor-
ine-induced retinal toxic blindness. Bone Marrow Transplant1997;20:243–245.
2. O’Riordan JM, FitzSimon S, O’Connor M, McCann SR. Ret-inal microvascular changes following bone marrow transplan-tation: the role of cyclosporine. Bone Marrow Transplant1994;13:101–104.
3. Gloor B, Gratwohl A, Hahn H, et al. Multiple cotton-woolspots following bone marrow transplantation for treatment ofacute lymphatic leukaemia. Br J Ophthalmol 1985;69:320–325.
4. Bernauer W, Gratwohl A, Keller A, Daicker B. Microvascu-lopathy in the ocular fundus after bone marrow transplantation.Ann Intern Med 1991;115:925–930.
5. Zoja C, Furci L, Ghilardi F, et al. Cyclosporine-induced en-dothelial cell injury. Lab Invest 1986;55:455–462.
6. Avery R, Jabs DA, Wingard JR, et al. Optic disc edema afterbone marrow transplantation. Possible role of cyclosporinetoxicity. Ophthalmology 1991;98:1294–1301.
7. Katz B. Disk edema subsequent to renal transplantation. SurvOphthalmol 1997;41:315–320.
8. Cruz OA, Fogg SG, Roper-Hall G. Pseudotumor cerebri asso-ciated with cyclosporine use. Am J Ophthalmol 1996;122:436–437.
CENTRAL SEROUS CHORIORETINOPATHYIN A PATIENT USINGMETHYLENEDIOXYMETHAMPHETAMINE(MDMA) OR “ECSTASY”
LAMA HASSAN, MD,CYNTHIA CARVALHO, MD,LAWRENCE A. YANNUZZI, MD,TOMOHIRO IIDA, MD,SILVANO NEGRÃO, MD
From the LuEsther T. Mertz Retinal Research Center,Manhattan Eye, Ear, and Throat Hospital, New York,New York.
In recent years, converging lines of experimental andclinical evidence have clearly identified steroids as arisk factor for acute manifestations of central serouschorioretinopathy (CSC).1–7 The systemic use of ste-roids by virtually any route of administration2,3,6,7 orsystemic disorders associated with a state of hyper-corticalism, such as Cushing syndrome,4 have beenimplicated in the development of exudative maculardetachments in patients with CSC. Drugs that stimu-late an adrenergic effect or a catecholamine responseare also thought to be potential risk factors for CSC,but this association has not been clearly established.3,5
This report describes a patient who had primary, andsubsequently recurrent, acute exudative manifesta-tions of CSC after using the illicit drug methyl-enedioxymethamphetamine (MDMA), commonly re-ferred to as ecstasy, a popular party or club drug withpsychomimetic and adrenergic effects.8
Case Report
A 38-year-old man who was in perfect health and had noremarkable medical or ocular history experienced a visual distur-bance in his right eye 3 days after the use of MDMA. The exactformulation and dose of the drug were unknown. His examinationat that time showed a visual acuity of 20/40 in his right eye and20/20 in his left eye. He also had metamorphopsia and a relativecentral scotoma on Amsler grid testing. A large neurosensorymacular detachment was noted on slit-lamp examination with theGoldmann contact lens. No lipid or blood was seen. The macula inthe left eye was unremarkable, except for two minor, punctate,atrophic pigment epithelial changes. After several weeks, visualacuity returned to 20/20 in the right eye, and there was a corre-sponding complete resolution of the neurosensory retinal detach-ment. Approximately 10 months later, he used the same drug again,and he experienced a decrease in vision of his right eye similar towhat had been noted earlier. A recurrent neurosensory maculardetachment was seen in the same eye, but this time, the detachmentwas smaller. The visual acuity was reduced to 20/25. The detach-ment again spontaneously resolved. This patient had not usedMDMA at any other time except before the two episodes of acutemacular detachment.
Discussion
Central serous chorioretinopathy is a well-known,complex clinical disorder whose pathogenesis is stillpoorly understood.2,3,5,6 An array of risk factors, in-cluding refractive state, systemic blood pressure, gen-
Supported by The Macula Foundation, Inc.Reprint requests: Lawrence A. Yannuzzi, MD, Manhattan Eye, Ear,
and Throat Hospital, 210 East 64th Street, New York, NY 10021.
559CSC IN MDMA • HASSAN ET AL

der, age, and corticosteroids (exogenous or endoge-nous), have been identified in the past.2,3,5 Therelationship between the use of exogenous corticoste-roids and the pathogenesis of CSC have been re-viewed by Gass and Little.6 Although the precisemechanism for the relationship is unknown, a steroid-induced effect on the choroidal circulation is pre-sumed to be responsible for the exudative changes. Ina recent article by Carvalho and Yannuzzi,7 steroidswere implicated in the development of acute manifes-tations of CSC in more than 50% of patients in aprospective, consecutive series. The steroid use wasby several routes of systemic administration, includ-ing oral, intramuscular, intraarticular, and inhalation.In this report, the authors suggested that other drugsthat indirectly stimulate the adrenal cortex, inducing acatecholamine response, could also predispose pa-tients to acute manifestations of CSC.
Accordingly, stimulation of the adrenergic systemmay also be implicated in acute manifestations ofCSC, but evidence supporting this possible associa-tion, although attractive, is not conclusive. The possi-ble mechanisms by which increased corticosteroid andcatecholamine levels may contribute to the pathogen-esis of CSC have been reviewed recently byHaimovici et al.3 The basis of this concept involvesthe release of catecholamines and an increase in thesensitivity of adrenergic receptors by corticosteroids.The supporting evidence includes an experimentalmodel of CSC that was induced by intravenous injec-tions with epinephrine and norepinephrine in pri-mates.9 There is also a primate model for CSC usingintravenous epinephrine and intramuscular corticoste-roids.10 Also, urinary epinephrine and norepinephrinelevels are increased in patients with active CSC com-pared with control patients.11 Clinical evidence sup-porting a link between hypercorticalism and adrener-gic stimulation can be found in the known abnormalbehavioral pattern, specifically a Type A personality,seen in patients with CSC.5 These patients have anincreased secretion of cortisol and adrenergic agents,such as epinephrine and norepinephrine.5 Also, com-bined corticosteroids andb-adrenergic nasal inhalantshave been reported to be a risk factor for CSC.3
Furthermore, systemic hypertension is a known riskfactor for CSC.2 Increased catecholamine levels arecommon to systemic hypertension and to CSC.2,11,12
There is also an increased vasoconstrictive sensitivityto corticosteroids in systemic hypertension.13 Cortico-steroids increase catecholamine-mediated vasocon-striction in the peripheral vasculature and in the cho-roid.13,14 Although still unproven, vasoconstrictionand associated perfusion abnormalities in the choroidhave been hypothesized to be causative factors in the
pathogenesis of CSC.2,5 Corticosteroids are alsoknown to induce transcription ofa-adrenergic15 andb-adrenergic16 receptor genes, and they may potenti-ate the effects of adrenergic stimulation on certaintarget tissues, such as the retinal pigment epitheli-um.17,18 Accordingly, a potential synergistic state ex-ists between corticosteroids and catecholamine metab-olism as a potential causative factor for thedevelopment of acute manifestations of CSC. Essen-tially, corticosteroids may increase catecholamine re-lease and make critical tissues, such as the innerchoroid and the retinal pigment epithelium, more sus-ceptible to adrenergic effects.
Although an absolute causal relationship betweenthe use of MDMA and the development of CSC in ourpatient is uncertain, there is a pharmacologic basis forthe development of acute manifestations of CSC fromthe use of this agent. In MDMA, the pharmacologiccomponent theoretically predisposing to CSC is likelyto be methamphetamine, which is a combineda- andb-adrenergic agent.8 It is known to stimulate periph-eral and centrala- and b-adrenergic receptors. Acausal relationship is particularly possible because thepatient experienced symptoms only on the two occa-sions when he used the drug. Discontinuation of thedrug was also associated with spontaneous resolutionof the macular manifestations, further implicating theuse of the drug with the disorder.
The origin of this drug dates back to the early 1960swhen MDMA was first synthesized by the pharma-ceutical company, Merck, with no particular purposein mind. The drug remained dormant until the 1970s,when it was studied by psychotherapists who claimedthat it enhanced communication in therapy, essentiallyas a psychomimetic or psychedelic agent. By the1980s, however, MDMA emerged as an illicit, so-called party or club drug used in discotheques byyoung adults. In recent years, this drug has becomeincreasingly popular, and its users have extended intothe teenage population. As a drug that is not approvedfor any medical purpose, its formulation is not regu-lated or controlled, and its use and distribution con-tinue to be illegal. Research at the animal level to datehas established that MDMA shares the properties ofthe psychedelic drug lysergic acid diethylamide andthe adrenergic stimulant amphetamine. Structurally, itis similar to the hallucinogen mescaline and the ad-renergic agent methamphetamine. Typically, it is usedorally in a capsular, tablet form, and its effects last for3 to 6 hours, depending on the dose. Persistent cog-nitive abnormalities, such as confusion, depression,insomnia, anxiety, and paranoia, are known to be sideeffects of the drug, even several weeks after its use.What is most disturbing about MDMA is that it is
560 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

extremely dangerous with regard to cardiovascularand neurologic effects, with potentially long-lastingadverse complications affecting the brain to altermemory function and motor skills.
The adrenergic changes relate to the cardiovascularside effects. Because it is a stimulant, MDMA in-creases the heart rate, blood pressure, and body tem-perature, and it may have serious side effects, includ-ing dehydration, persistent hypertension, and heart orkidney failure. It is known to increase the release ofepinephrine,19 accounting for these systemic cardio-vascular changes. Plasma levels of steroids have alsobeen found to be higher in patients using MDMA.20
Thus, there is an adrenergic and a corticosteroid stim-ulation with MDMA that may be a factor in thedevelopment of CSC in our patient.
Neurologically, MDMA acts primarily as a seroto-nergic (5-HT) drug, a major neurotransmitter in thebrain, synthesized from tryptophan through the inter-mediate 5-hydroxetryptophan.8 MDMA actually af-fects 5-HT in the way that amphetamines affect do-pamine, by inhibiting the uptake and causing therelease of the molecule. This mechanism of action issimilar to the way that selective serotonin reuptakeinhibitors work. Serotonin effects are also thought tobe responsible for the psychologic and physiologiceffects of the drug, including mood, sleep, depression,and obsessive compulsions.8 Its neurotoxicity canhave permanent damage to neurons that release sero-tonin, impairing an individual’s memory and cogni-tive performance.
This case report suggests that MDMA may alsohave ocular effects that are most likely mediatedthrough its adrenergic and corticosteroid stimulation,which in turn may predispose patients to acute mani-festations of CSC. In patients with steroids as a con-tributing causative effect of their acute CSC manifes-tations, discontinuation of the drug is usuallyassociated with resolution of the neurosensory detach-ment.7 The same outcome seemed to be evident in thiscase. Although additional research is obviouslyneeded to confirm this singular observation, the rela-tionship between the use of MDMA and the acutemanifestations of CSC is rational, if not compelling.Accordingly, clinicians should be aware of this poten-tial association so that they can counsel their patients,particularly those who have other risk factors for CSCor who are actually known to have had the conditionitself. Therefore, patients who have acute manifesta-tions of CSC should be carefully asked about drug useso that they can be advised to discontinue any drug thatmight have a systemic, adrenergic stimulating effect be-fore any other form of treatment is considered.
References1. Wakakura M, Ishikawa S. Central serous chorioretinopathy
complicating systemic corticosteroid treatment. Br J Ophthal-mol 1984;68:329–331.
2. Tittl MK, Spaide RF, Wong D, et al. Systemic findingsassociated with central serous chorioretinopathy. Am J Oph-thalmol 1999;128:63–68.
3. Haimovici R, Gragoudas ES, Duker JS, et al. Central serouschorioretinopathy associated with inhaled or intranasal corti-costeroids. Ophthalmology 1997;104:1653–1660.
4. Garg SP, Dada T, Talwar D, et al. Endogenous cortisolprofile in patients with central serous chorioretinopathy. Br JOphthalmol 1997;81:962–964.
5. Yannuzzi LA. Type A behavior, central serous chorioreti-nopathy. Retina 1987;7:111–131.
6. Gass JD, Little H. Bilateral bullous exudative retinal detach-ment and complicating idiopathic central serous chorioreti-nopathy during systemic corticosteroid therapy. Ophthalmol-ogy 1995;102:737–747.
7. Carvalho C, Yannuzzi L, Coleman H, et al. Central serouschorioretinopathy and corticosteroids. Ophthalmology 2001(submitted for publication).
8. Rattray M. Ecstasy. Towards an understanding of the bio-chemical basis of actions of MDMA. Essays Biochem 1991;26:77–87.
9. Nagayoski K. Experimental study of chorioretinopathy byintravenous injection of adrenaline. Acta Soc Ophthalmol Jpn1971;75:1720–1727.
10. Yoshioka H, Katsume Y, Akune H. Experimental centralserous chorioretinopathy in monkey eyes: fluorescein angiog-raphy findings. Ophthalmologica 1982;185:168–178.
11. Wakakura M, Suzuki H. Central serous chorioretinopathy.Jpn J Clin Ophthalmol 1979;33:1237–1240.
12. Goldstein DS. Plasma catecholamine and essential hyperten-sion: an analytic review. Hypertension 1983;5:86–89.
13. Walker BR, Best R, Schackleton CH, et al. Increased vaso-constrictor sensitivity to glucocorticosteroids in essential hy-pertension. Hypertension 1996;27:190–196.
14. Koss MG, Gherezgheker T. Adrenoreceptor subtypes in-volved in neurally evoked sympathetic vasoconstriction inthe anterior choroid of cats. Exp Eye Res 1993;57:441–447.
15. Sakuve M, Hoffman B. Glucocorticosteroids induce tran-scription and expression of alpha adrenergic receptor gene inDDTI MR-2 smooth muscle cells. J Clin Invest 1991;88:385–389.
16. Hadcock JR, Malbon CC. Regulation of beta-adrenergic re-ceptors by permissive hormones: glucocorticoids increasesteady-state levels of receptors mRNA. Proc Natl Acad SciUSA 1988;85:8415–8419.
17. Koh SWM, Chader GJ. Retinal pigment epithelium in culturedemonstrates a distinct beta adrenergic receptor. Exp Eye Res1984;38:7–13.
18. Frambach DA, Fain GL, Farber DB, Bok D. Beta adrenergicreceptors on cultured human retinal pigment epithelium. In-vest Ophthalmol Vis Sci 1990;31:1767–1772.
19. Mas M, Favee M, de la Torre R, et al. Cardiovascular andneuroendocrine effects and pharmacokinetics of 3,4 methyl-enedioxymethamphetamine in humans. J Pharmacol ExpTher 1999;290:135–145.
20. Rothman RB, Baumann MH, Duesch CM, et al. Amphet-amine-type central nervous system stimulants release norepi-nephrine more potently than they release dopamine and se-rotonin. Synapse 2001;39:32–41.
561CSC IN MDMA • HASSAN ET AL

Correspondence
Reversed Self–Sealing Pars Plana Sclerotomies
Dear Editor:We read with interest the article by Assi et al1
describing a technique of reversed self-sealing scle-rotomies. It is a modification to the methods describedby Chen2 and Kwok et al.3 Chen constructed a radialscleral tunnel with opening 2 mm posterior to theintended pars plana entry; Kwok et al modified it byrotating the tunnel through 90 degrees, so that thetunnel was circumferential. The technique of Assi et alwas similar to that of Chen,2 except the opening of thetunnel was anterior to the intended pars plana entry.The common advantages of various self-sealing scle-rotomy techniques were echoed in his study, includingsutureless closure of the sclerotomy sites, reducedintraocular pressure fluctuation, and reduced likeli-hood of vitreous incarceration and leakage of fluid orgas.
Whereas the approach proposed by Assi et al mayhave some advantages, the infusion tubing is likely toenter the surgical field and cause obstruction of viewduring surgery when the opening of the scleral pocketis anterior and radial. The risk of the tip of the radialinfusion cannula touching the peripheral retina mayalso be higher, especially when a longer infusioncannula is used. Additionally, as the anterior openingof the scleral pocket is only 2 mm posterior to thelimbus, the conventional sutured ring system maymake insertion of instruments difficult. For example,the width of the sutured ring in the Lander’s system isalready 1.5 mm. Moreover, the instruments are to beinserted in a medial–lateral direction before enteringthe eyeball and this may hit the contact lens in thesutured ring. This problem is even more prevailingwith the use of panoramic viewing system, be it con-tact or noncontact type, as the wide-field lenses aremuch larger and hence easily interfere with the inser-tion of instruments. The above potential problems arenot present in our reported modified circumferentialsutureless technique.3 It appears to be immature at this
stage to recommend the authors’ reversed method asthe standard for sutureless pars plana sclerotomies.
Alvin K. H. Kwok, FRCSEl Neoh, FRCS
Dennis S. C. Lam, FRCS, FRCOPHTH
Department of Ophthalmology & Visual SciencesThe Chinese University of Hong Kong
Hong Kong Eye HospitalHong Kong
Reply
Dear Editor:We thank Drs. Kwok, Neoh, and Lam for their
interest in our article describing reversed self-sealingpars plana sclerotomies. We clearly stated that weused a traditional stab incision sclerotomy port for thetemporal infusion line and that we studied reversedself-sealing sclerotomies for the instruments in thesuperotemporal and superonasal quadrants. Kwok etal’s assumptions about potential problems with theinfusion line tubing and tip in the self-sealing sclerot-omy are therefore inappropriate and invalid. Regard-ing the insertion of instruments, we did not encounterany problems with the hand-held Machemer contactlenses nor with the noncontact wide angle system(Biom) that we currently use. As previously stated, thereversed self-sealing sclerotomies offer smoother andbetter access to the posterior segment and easier ex-change and manipulation of instruments owing to themore logical anteroposterior direction of the tunnel.We therefore reiterate the recommendation of ourtechnique as a standard for self-sealing sclerotomies.
Alexandre C. Assi, FRCOPHTH
Robert A. H. Scott, FRCOPHTH
David G. Charteris, MD, FRCS, FRCOPHTH
Moorfields Eye HospitalLondon, United Kingdom
References1. Assi AC, Scott RAH, Charteris DG. Reversed self-sealing pars
plana sclerotomies. Retina 2000;20:689–692.2. Chen JC. Sutureless pars plana vitrectomy through self-sealing
sclerotomies. Arch Ophthalmol 1996;114:1273–1275.3. Kwok AKH, Tham CCY, Lam DSC, Li M, Chen JC. Modified
sutureless sclerotomies in pars plana vitrectomy. Am J Oph-thalmol 1999;127:731–733.
RETINA,™ The Journal of Retinal and Vitreous Dis-eases,encourages readers to submitCorrespondencere-lated to recent articles or other material published in thejournal. Correspondence should be typed double-spaced on81⁄2 3 110 bond paper with 11⁄20 margins on all four sides.
562 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5

ICGA–Guided Laser Photocoagulation of FeederVessels of Choroidal Neovascular Membranes in
Age–Related Macular Degeneration
Dear Editor:I would like to congratulate Desatnik and cowork-
ers1 for attempting to further refine laser photocoagu-lation of feeder vessels (FV) of choroidal neovascu-larization (CNV). A number of other recent reportshave shown encouraging results after laser treatmentof FV.2,3 Although no definitive answers on the indi-cations and efficacy of this procedure can be drawn,some evidence derived from this and previous studiesmay contribute in identifying the subjects who maybenefit from the treatment.
It is clearly evident that the possibility to identifyand treat FV in choroidal neovascular nets dependsnot only on the different systems applied—i.e., indo-cyanine green angiography (ICGA) vs fluorescein an-giography (FA), scanning laser ophthalmoscopes vsdigital fundus cameras, confocal aperture—but alsoon the experience, skill, and knowledge of the singlephysician. In different case series FV have been de-tected in 22%,2 75%,4 and 86%3 of cases. Anatomicsuccess, defined as occlusion of FV and CNV, hasbeen obtained in 40–80% of treated eyes.1–3 Theapplication of new systems that permit visualization ofchoroidal blood flow by high-speed ICGA and simul-taneous delivery of laser photocoagulation to the FVmight improve the ability to identify and treat thetarget.5
Not all the FV respond positively to laser photoco-agulation. Staurenghi and coworkers3 found that FVthat “insert” into the CNV after a variable course(“racquet-like pattern”) might have a better outcomethan FV that seem to originate from the choroidalvascular bed beneath the CNV (“umbrella-like pat-tern”). This is the case of Patient 3 reported by De-satnik and coworkers.1 At the latest follow-up visit FAand ICGA showed progressive retinal pigment epithe-lium (RPE) atrophy adjacent to the laser scar, possiblydue to excessive laser irradiation in the attempt toclose the “umbrella-like” neovascular net. The lengthof the FV might positively influence the outcome oflaser treatment. There is evidence that the longer thecourse of the treatable vessels, the better the occlusiveeffect.3 Similar results are reported by Desatnik andcoworkers1 in Cases 1, 2, and 4. The caliber of the FVmight be another factor involved in the success rate. InCase 5 the width of the FV was large and repeatedlaser treatments caused an RPE rip and recurrence ofthe CNV. Staurenghi et al.3 reported that the successrate of FV laser photocoagulation increased from 40–75% when FV were selected for treatment on the basis
of a width of less than 85mm. The role of other factorsprognostic of good outcome after treatment, such asthe presence of a small CNV and the closest distanceof laser burns to the center of the foveal avascularzone, have been underlined by Shiraga et al.2 and needfurther studies.
The precise mechanisms by which laser photocoag-ulation is able to close choroidal new vessels havebeen debated for years and little is known regardingthe action by which laser stimulates FV closure. Pre-liminary experiences with ICGA-guided FV laser pho-tocoagulation have used different wavelengths andtechniques. Shiraga et al.2 placed confluent intenseburns covering the FV and an area of 300-mm beyondit on either side and around its origin with a dye laser(576 nm yellow and 630 nm red). An argon greenlaser was used by Staurenghi et al.3 The treatment wasadministered in two consecutive steps: the first with a100-mm spot size of moderate intensity on both sidesof the FV; the second with a 100- or 200-mm beamover the FV. Delivery of 810-nm wavelength diodelaser pulsed photocoagulation has been effectivelyapplied by Glaser et al.4 Hundreds of nonophthalmo-scopically visible or barely visible burns were placedover the FV. Desatnik and coworkers1 used intenseconfluent burns along the FV with a 200-mm spot sizeand an argon green laser. Although the authors statethat an argon green is preferable for treatment of FV,no definitive conclusions on the optimal wavelengthand technique for FV laser photocoagulation can bedrawn.
Only adequate randomized clinical trials will helpto define the efficacy and role of FV photocoagulationand the recommended technique and wavelength.
Paolo Lanzetta, MDDepartment of Ophthalmology
University of UdineUdine, Italy
Reply
Dear Editor:We would like to thank Dr. Lanzetta for his interest
in our article on laser treatment to feeder vessels ofCNV in age-related macular degeneration.
In our experience this technique can be useful topreserve or even improve vision in select cases ofsubfoveal CNV when a FV can be detected. There aremany unanswered questions regarding this mode oftreatment, including the difficulty in identifying theFV, the best wavelength and its effectiveness, and
563CORRESPONDENCE

visual outcome compared to other current treatmentsfor subfoveal CNV: photodynamic therapy, submacu-lar surgery and subfoveal removal, limited maculartranslocation, and others.
Only randomized multicenter clinical trials willhelp us to place the effectiveness of this treatmentmodality in its proper perspective. In the meantime, inthe absence of such data, we need to use our clinicaljudgment and experience to decide on an individualpatient basis when FV treatment will give better re-sults than other treatment options.
Howard Desatnik, MDJoseph Moisseiev, MD
Retina ServiceGoldschleger Eye Institute
Sheba Medical CenterTel-Hashomer, Israel
References
1. Desatnik H, Treister G, Alhalel A, Krupsky S, Moisseiev J.ICGA-guided laser photocoagulation of feeder vessels of cho-roidal neovascular membranes in age-related macular degen-eration. Retina 2000;20:143–150.
2. Shiraga F, Ojima Y, Matsuo T, Takasu I, Matsuo N. Feedervessel photocoagulation of subfoveal choroidal neovascular-ization secondary to age-related macular degeneration. Oph-thalmology 1998;105:662–669.
3. Staurenghi G, Orzalesi N, La Capria A, Aschero M. Lasertreatment of feeder vessels in subfoveal choroidal neovascularmembranes. A revisitation using dynamic indocyanine greenangiography. Ophthalmology 1998;105:2297–2305.
4. Glaser BM, Murphy RP, Lakhanpal RR, Lin SB, Baudo TA.Identification and treatment of modulating choroidal vesselsassociated with occult choroidal neovascularization [abstract1687]. Invest Ophthalmol Vis Sci 2000;41:S320.
5. Flower RW. Experimental studies of indocyanine green dye-enhanced photocoagulation of choroidal neovascularizationfeeder vessels. Am J Ophthalmol 2000;129:501–512.
564 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2001 ● VOLUME 21 ● NUMBER 5


















