Brief History of the Disease
17
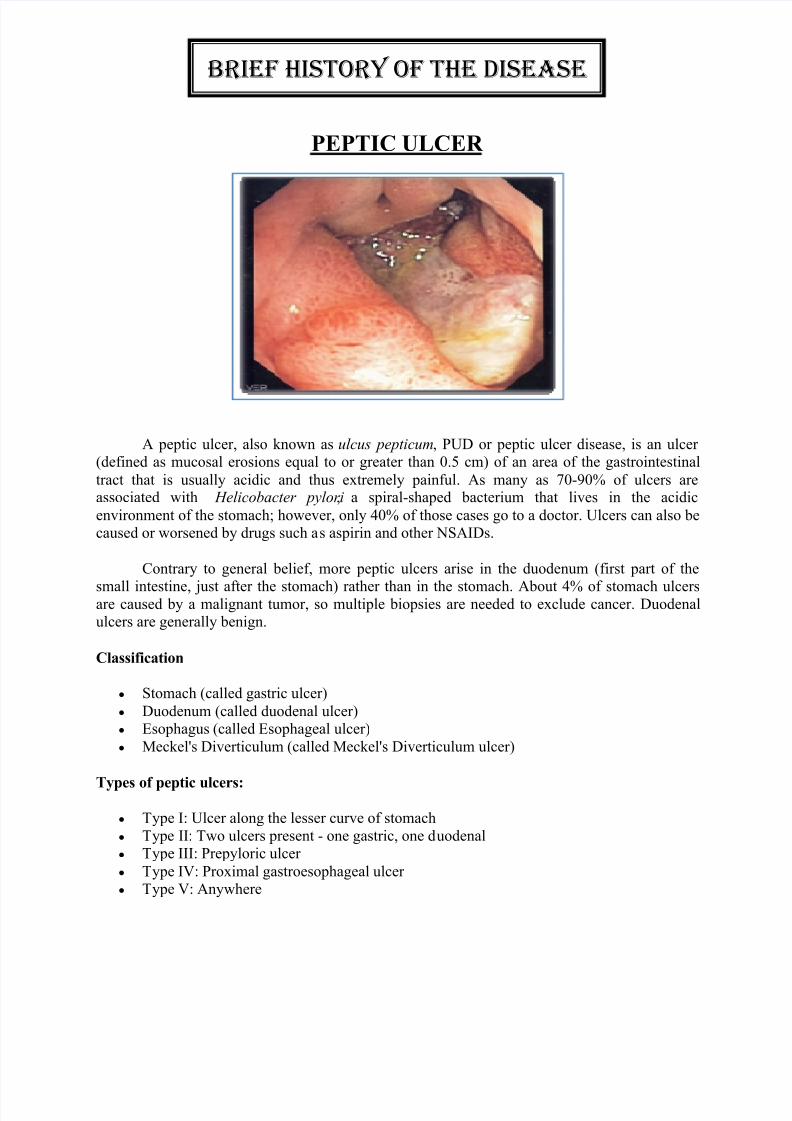
PEPTIC ULCER A peptic ulcer, also known as ulcus pepticum, PUD or peptic ulcer disease, is an ulcer (defined as mucosal erosions equal to or greater than 0.5 cm) of an area of the gastrointestinal tract that is usually acidic and thus extremely painful. As many as 70-90% of ulcers are associated with Helicobacter pylori , a spiral-shaped bacterium that lives in the acidic environment of the stomach; however, only 40% of those cases go to a doctor. Ulcers can also be caused or worsened by drugs such a s aspirin and other NSAIDs. Contrary to general belief, more peptic ulcers arise in the duodenum (first part of the small intestine, just after the stomach) rather than in the stomach. About 4% of stomach ulcers are caused by a malignant tumor, so multiple biopsies are needed to exclude cancer. Duodenal ulcers are generally benign. Classification y Stomach (called gastric ulcer) y Duodenum (called duodenal ulcer) y Esophagus (called Esophageal ulcer) y Meckel's Diverticulum (called Meckel's Diverticulum ulcer) Types of peptic ulcers: y Type I: Ulcer along the lesser curve of stomach y Type II: Two ulcers present - one gastric, one d uodenal y Type III: Prepyloric ulcer y Type IV: Proximal gastroesophageal ulcer y Type V: Anywhere BRIEF HISTORY OF THE DISEASE
-
Upload
jon-corpuz-aggasid -
Category
Documents
-
view
218 -
download
0
Transcript of Brief History of the Disease
8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 1/17
PEPTIC ULCER
A peptic ulcer, also known as ulcus pepticum, PUD or peptic ulcer disease, is an ulcer (defined as mucosal erosions equal to or greater than 0.5 cm) of an area of the gastrointestinal
tract that is usually acidic and thus extremely painful. As many as 70-90% of ulcers areassociated with Helicobacter pylori, a spiral-shaped bacterium that lives in the acidic
environment of the stomach; however, only 40% of those cases go to a doctor. Ulcers can also becaused or worsened by drugs such as aspirin and other NSAIDs.
Contrary to general belief, more peptic ulcers arise in the duodenum (first part of the
small intestine, just after the stomach) rather than in the stomach. About 4% of stomach ulcersare caused by a malignant tumor, so multiple biopsies are needed to exclude cancer. Duodenalulcers are generally benign.
Classification
y Stomach (called gastric ulcer)
y Duodenum (called duodenal ulcer)y Esophagus (called Esophageal ulcer)
y Meckel's Diverticulum (called Meckel's Diverticulum ulcer)
Types of peptic ulcers:
y Type I: Ulcer along the lesser curve of stomach
y Type II: Two ulcers present - one gastric, one duodenaly Type III: Prepyloric ulcer
y Type IV: Proximal gastroesophageal ulcer y Type V: Anywhere
BRIEF HISTORY OF THE DISEASE

8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 2/17
Signs and symptoms
Symptoms of a peptic ulcer can be:
y abdominal pain, classically epigastric with severity relating to mealtimes, after around 3
hours of taking a meal (duodenal ulcers are classically relieved by food, while gastriculcers are exacerbated by it);y bloating and abdominal fullness;
y waterbrash (rush of saliva after an episode of regurgitation to dilute the acid inesophagus);
y nausea, and copious vomiting;y loss of appetite and weight loss;
y hematemesis (vomiting of blood); this can occur due to bleeding directly from a gastriculcer, or from damage to the esophagus from severe/continuing vomiting.
y melena (tarry, foul-smelling feces due to oxidized iron from hemoglobin);y rarely, an ulcer can lead to a gastric or duodenal perforation, which leads to acute
peritonitis.T
his is extremely painful and requires immediate surgery.
A history of heartburn, gastroesophageal reflux disease (GER D) and use of certain forms of
medication can raise the suspicion for peptic ulcer. Medicines associated with peptic ulcer include NSAID (non-steroid anti-inflammatory drugs) that inhibit cyclooxygenase, and most
glucocorticoids (e.g. dexamethasone and prednisolone).
In patients over 45 with more than two weeks of the above symptoms, the odds for pepticulceration are high enough to warrant rapid investigation by EGD (see below).
The timing of the symptoms in relation to the meal may differentiate between g astric and
duodenal ulcers: A gastric ulcer would give epigastric pain durin g the meal, as gastric acid issecreted, or after the meal, as the alkaline duodenal contents reflux into the stomach. Symptoms
of duodenal ulcers would manifest mostly before the meal²when acid (production stimulated byhunger) is passed into the duodenum. However, this is not a reliable sign in clinical practice.
Also, the symptoms of peptic ulcers may vary with the location of the ulcer and the patient'sage. Furthermore, typical ulcers tend to heal and recur and as a result the pain may occur for few
days and weeks and then wane or disappear. Usually, children and the elderly do not develop anysymptoms unless complications have arisen.
Burning or gnawing feeling in the stomach area lasting between 30 minutes and 3 hours
commonly accompanies ulcers. This pain can be misinterpreted as hunger, indigestion or heartburn. Pain is usually caused by the ulcer but it may be aggravated by the stomach acid when
it comes into contact with the ulcerated area. The pain caused by peptic ulcers can be feltanywhere from the navel up to the breastbone, it may last from few minutes to several hours and
it may be worse when the stomach is empty. Also, sometimes the pain may flare at night and itcan commonly be temporarily relived by eating foods that buffer stomach acid or by taking anti-
acid medication. However, peptic ulcer disease symptoms may be different for every sufferer.

8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 3/17
Complications
y Gastrointestinal bleeding is the most common complication. Sudden large bleeding can be life-threatening. It occurs when the ulcer erodes one of the blood vessels.
y Perforation (a hole in the wall) often leads to catastrophic consequences. Erosion of the
gastro-intestinal wall by the ulcer leads to spillage of stomach or intestinal content intothe abdominal cavity. Perforation at the anterior surface of the stomach leads to acute peritonitis, initially chemical and later bacterial peritonitis. The first sign is often sudden
intense abdominal pain. Posterior wall perforation leads to pancreatitis; pain in thissituation often radiates to the back.
y Penetration is when the ulcer continues into adjacent organs such as the liver and pancreas.
y Scarring and swelling due to ulcers causes narrowing in the duodenum and gastric outletobstruction. Patient often presents with severe vomiting.
y Cancer is included in the differential diagnosis (elucidated by biopsy), Helicobacter pylori as the etiological factor making it 3 to 6 times more likely to develop stomach
cancer from the ulcer.
Cause
A major causative factor (60% of gastric and up to 90% of duodenal ulcers) is chronic
inflammation due to Helicobacter pylori that colonizes the antral mucosa. The immune system isunable to clear the infection, despite the appearance of antibodies. Thus, the bacterium can cause
a chronic active gastritis (type B gastritis), resulting in a defect in the regulation of gastrin production by that part of the stomach, and gastrin secretion can either be decreased (most cases)
resulting in hypo- or achlorhydria or increased. Gastrin stimulates the production of gastric acid by parietal cells and, in H. pylori colonization responses that increase gastrin, the increase in acid
can contribute to the erosion of the mucosa and therefore ulcer formation.
Another major cause is the use of NSAIDs (see above). The gastric mucosa protects itself from gastric acid with a layer of mucus, the secretion of which is stimulated by certain
prostaglandins. NSAIDs block the function of cyclooxygenase 1 (cox-1), which is essential for the production of these prostaglandins. COX-2 selective anti-inflammatories (such as celecoxib
or the since withdrawn rofecoxib) preferentially inhibit cox-2, which is less essential in thegastric mucosa, and roughly halve the risk of NSAID-related gastric ulceration. As the
prevalence of H. pylori-caused ulceration declines in the Western world due to increased medicaltreatment, a greater proportion of ulcers will be due to increasing NSAID use among individuals
with pain syndromes as well as the growth of aging populations that develop arthritis.
The incidence of duodenal ulcers has dropped significantly during the last 30 years, whilethe incidence of gastric ulcers has shown a small increase, mainly caused by the widespread useof NSAIDs. The drop in incidence is considered to be a cohort-phenomenon independent of the
progress in treatment of the disease. The cohort-phenomenon is probably explained by improvedstandards of living which has lowered the incidence of H. pylori infections.
8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 4/17
Although some studies have found correlations between smoking and ulcer formation,others have been more specific in exploring the risks involved and have found that smoking by
itself may not be much of a risk factor unless associated with H. pylori infection Somesuggested risk factors such as diet, spice, consumption and blood type, were hypothesized as
ulcerogens (helping cause ulcers) until late in the 20th century, but have been shown to be of
relatively minor importance in the development of peptic ulcers. Similarly, while studies havefound that alcohol consumption increases risk when associated with H. pylori infection, it doesnot seem to independently increase risk, and even when coupled with H. pylori infection, the
increase is modest in comparison to the primary risk factor.
Gastrinomas (Zollinger Ellison syndrome), rare gastrin-secreting tumors, also causemultiple and difficult to heal ulcers.
Stress
R esearchers also continue to look at stress as a possible cause, or at least complication, in
the development of ulcers.T
here is debate as to whether psychological stress can influence thedevelopment of peptic ulcers. Burns and head trauma, however, can lead to physiologic stressulcers, which are reported in many patients who are on mechanical ventilation.
An expert panel convened by the Academy of Behavioral Medicine R esearch concluded
that ulcers are not purely an infectious disease and that psychological factors do play asignificant role.
[1] R esearchers are examining how stress might promote H. pylori infection. For
example, Helicobacter pylori thrives in an acidic environment, and stress has been demonstratedto cause the production of excess stomach acid. This was supported by a study on mice showing
that both long-term water-immersion-restraint stress and H. pylori infection were independentlyassociated with the development of peptic ulcers.
A study of peptic ulcer patients in a Thai hospital showed that chronic stress was strongly
associated with an increased risk of peptic ulcer, and a combination of chronic stress andirregular mealtimes was a significant risk factor.
Diagnosis
The diagnosis is mainly established based on the characteristic symptoms. The stomach pain is usually the first to signal a peptic ulcer. In some cases, doctors may treat ulcers without
diagnosing them with specific tests and observe if the symptoms resolve, meaning their primarydiagnosis was accurate.
Confirming the diagnosis is made with the help of tests such as endoscopies or barium
contrast x-rays. The tests are typically ordered if the symptoms do not resolve after a few weeksof treatment, or when they first appear in a person who is over age 45 or who has other
symptoms such as weight loss, because stomach cancer can cause similar symptoms. Also, whensevere ulcers resist treatment, particularly if a person has several ulcers or the ulcers are inunusual places, a doctor may suspect an underlying condition that causes the stomach to
overproduce acid.
8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 5/17
An esophagogastroduodenoscopy (EGD), a form of endoscopy, also known as agastroscopy, is carried out on patients in whom a peptic ulcer is suspected. By direct visual
identification, the location and severity of an ulcer can be described. Moreover, if no ulcer is present, EGD can often provide an alternative diagnosis.
One of the reasons why blood tests are not reliable on establishing an accurate pepticulcer diagnosis on their own is their inability to differentiate between past exposure to the bacteria and current infection. Additionally, a false-negative is possible with a blood test if the
patient has recently been taking certain drugs, such as antibiotics or proton pump inhibitors.
The diagnosis of Helicobacter pylori can be made by:
y Urea breath test (noninvasive and does not require EGD);
y Direct culture from an EGD biopsy specimen; this is difficult to do, and can beexpensive. Most labs are not set up to perform H. pylori cultures;
y Direct detection of urease activity in a biopsy specimen by rapid urease test;y M
easurement of antibody levels in blood (does not requireE
GD). It is still somewhatcontroversial whether a positive antibody without EGD is enough to warrant eradicationtherapy;
y Stool antigen test;y Histological examination and staining of an EGD biopsy.
The breath test uses radioactive carbon atom to detect H. pylori. To perform this exam the
patient will be asked to drink a tasteless liquid which contains the carbon as part of the substancethat the bacteria breaks down. After an hour, the patient will be asked to blow into a bag that is
sealed. If the patient is infected with H. pylori, the breath sample will contain carbon dioxide.This test provides the advantage of being able to monitor the response to treatment used to kill
the bacteria.
The possibility of other causes of ulcers, notably malignancy (gastric cancer) needs to bekept in mind. This is especially true in ulcers of the g reater (lar g e) curvature of the stomach;
most are also a consequence of chronic H. pylori infection.
If a peptic ulcer perforates, air will leak from the inside of the gastrointestinal tract (which
always contains some air) to the peritoneal cavity (which normally never contains air). This leadsto "free gas" within the peritoneal cavity. If the patient stands erect, as when having a chest X-
ray, the gas will float to a position underneath the diaphragm. Therefore, gas in the peritonealcavity, shown on an erect chest X-ray or supine lateral abdominal X-ray, is an omen of
perforated peptic ulcer disease.
Treatment
Younger patients with ulcer-like symptoms are often treated with antacids or H2antagonists before EGD is undertaken. Bismuth compounds may actually reduce or even clear organisms, though the warning labels of some bismuth subsalicylate products indicate that the
product should not be used by someone with an ulcer.
8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 6/17
Patients who are taking nonsteroidal anti-inflammatories (NSAIDs) may also be prescribed a prostaglandin analogue (Misoprostol) in order to help prevent peptic ulcers, which
may be a side-effect of the NSAIDs.
When H. pylori infection is present, the most effective treatments are combinations of 2
antibiotics (e.g. Clarithromycin, Amoxicillin,T
etracycline,M
etronidazole) and 1 proton pumpinhibitor (PPI), sometimes together with a bismuth compound. In complicated, treatment-resistant cases, 3 antibiotics (e.g. amoxicillin + clarithromycin + metronidazole) may be used
together with a PPI and sometimes with bismuth compound. An effective first-line therapy for uncomplicated cases would be Amoxicillin + Metronidazole + Pantoprazole (a PPI). In the
absence of H. pylori, long-term higher dose PPIs are often used.
Treatment of H. pylori usually leads to clearing of infection, relief of symptoms andeventual healing of ulcers. R ecurrence of infection can occur and retreatment may be required, if
necessary with other antibiotics. Since the widespread use of PPI's in the 1990s, surgical procedures (like "highly selective vagotomy") for uncomplicated peptic ulcers became obsolete.
Perforated peptic ulcer is a surgical emergency and requires surgical repair of the perforation. Most bleeding ulcers require endoscopy urgently to stop bleeding with cautery,
injection, or clipping.

8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 7/17
A N E M I A
Anemia (pronounced /nimi/, also spelled anemia and anæmia; from Ancient
Greek anaimia, meaning lack of blood ) is a decrease in normal number of red blood
cells (R BCs) or less than the normal quantity of hemoglobin in the blood. However, it can
include decreased oxygen-binding ability of each hemoglobin molecule due to deformity or lack in numerical development as in some other types of hemoglobin deficiency.
Because hemoglobin (found inside R BCs) normally carries oxygen from the lungs to thetissues, anemia leads to hypoxia (lack of oxygen) in organs. Because all human cells depend on
oxygen for survival, varying degrees of anemia can have a wide range of clinical consequences.
Anemia is the most common disorder of the blood. There are several kinds of anemia, produced by a variety of underlying causes. Anemia can be classified in a variety of ways, based
on the morphology of R BCs, underlying etiologic mechanisms, and discernible clinical spectra,to mention a few. The three main classes of anemia include excessive blood loss (acutely such as
a hemorrhage or chronically through low-volume loss), excessive blood cell destruction(hemolysis) or deficient red blood cell production (ineffective hematopoiesis).
There are two major approaches: the "kinetic" approach which involves evaluating production, destruction and loss, and the "morphologic" approach which groups anemia by red
blood cell size. The morphologic approach uses a quickly available and cheap lab test as itsstarting point (the MCV). On the other hand, focusing early on the question of production may
allow the clinician to more rapidly expose cases where multiple causes of anemia coexist.
Signs and symptoms
Main symptoms that may appear in anemia

8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 8/17
Anemia goes undetermined in many people, and symptoms can be minor or vague. Thesigns and symptoms can be related to the anemia itself, or the underlying cause.
Most commonly, people with anemia report non-specific symptoms of a feeling of
weakness, or fatigue, general malaise and sometimes poor concentration. They may also report
dyspnea (shortness of breath) on exertion. In very severe anemia, the body may compensate for the lack of oxygen carrying capability of the blood by increasing cardiac output. The patient mayhave symptoms related to this, such as palpitations, angina (if preexisting heart disease is
present), intermittent claudication of the legs, and symptoms of heart failure.
On examination, the signs exhibited may include pallor (pale skin, mucosal linings andnail beds) but this is not a reliable sign. There may be signs of specific causes of anemia, e.g.,
koilonychia (in iron deficiency), jaundice (when anemia results from abnormal break down of red blood cells ² in hemolytic anemia), bone deformities (found in thalassaemia major) or leg
ulcers (seen in sickle cell disease).
In severe anemia, there may be signs of a hyperdynamic circulation: a fast heart rate(tachycardia), flow murmurs, and cardiac enlargement. There may be signs of heart failure.
Pica, the consumption of non-food based items such as dirt, paper, wax, grass, ice, andhair, may be a symptom of iron deficiency, although it occurs often in those who have normal
levels of hemoglobin.
Chronic anemia may result in behavioral disturbances in children as a direct result of impaired neurological development in infants, and reduced scholastic performance in children of
school age.
R
estless legs syndrome is more common in those with iron deficiency anemia.
Less common symptoms may include swelling of the legs or arms, chronic heartburn,
vague bruises, vomiting, increased sweating, and blood in stool.
Diagnosis
Peripheral blood smear microscopy of a patient with iron-deficiency anemia.

8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 9/17
Generally, clinicians request complete blood counts in the first batch of blood tests in thediagnosis of an anemia. Apart from reporting the number of red blood cells and the hemoglobin
level, the automatic counters also measure the size of the red blood cells by flow cytometry,which is an important tool in distinguishing between the causes of anemia. Examination of a
stained blood smear using a microscope can also be helpful, and is sometimes a necessity in
regions of the world where automated analysis is less accessible.
In modern counters, four parameters (R BC count, hemoglobin concentration, MCV and
R DW) are measured, allowing others (hematocrit, MCH and MCHC) to be calculated, andcompared to values adjusted for age and sex. Some counters estimate hematocrit from direct
measurements.
WHO's Hemoglobin thresholds used to define anemia ( 1 g/dL = 0.6206 mmol/L)
Age or gender group Hb threshold (g/dl) Hb threshold (mmol/l)
Children (0.5±5.0 yrs) 11.0 6.8
Children (5±12 yrs) 11.5 7.1
Teens (12±15 yrs) 12.0 7.4
Women, non-pregnant (>15yrs) 12.0 7.4
Women, pregnant 11.0 6.8
Men (>15yrs) 13.0 8.1
R eticulocyte counts, and the "kinetic" approach to anemia, have become more common
than in the past in the large medical centers of the United States and some other wealthy nations,in part because some automatic counters now have the capacity to include reticulocyte counts. A
reticulocyte count is a quantitative measure of the bone marrow's production of new red bloodcells. The reticulocyte production index is a calculation of the ratio between the level of anemia
and the extent to which the reticulocyte count has risen in response. If the degree of anemia issignificant, even a "normal" reticulocyte count actually may reflect an inadequate response.
If an automated count is not available, a reticulocyte count can be done manuallyfollowing special staining of the blood film. In manual examination, activity of the bone marrow
can also be gauged qualitatively by subtle changes in the numbers and the morphology of youngR BCs by examination under a microscope. Newly formed R BCs are usually slightly larger than
older R BCs and show polychromasia. Even where the source of blood loss is obvious, evaluationof erythropoiesis can help assess whether the bone marrow will be able to compensate for the
loss, and at what rate.
When the cause is not obvious, clinicians use other tests: ESR , ferritin, serum iron,transferrin, R BC folate level, serum vitamin B12, hemoglobin electrophoresis, renal function tests
(e.g. serum creatinine).
When the diagnosis remains difficult, a bone marrow examination allows directexamination of the precursors to red cells.
8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 10/17
Classification
Production vs. destruction or loss
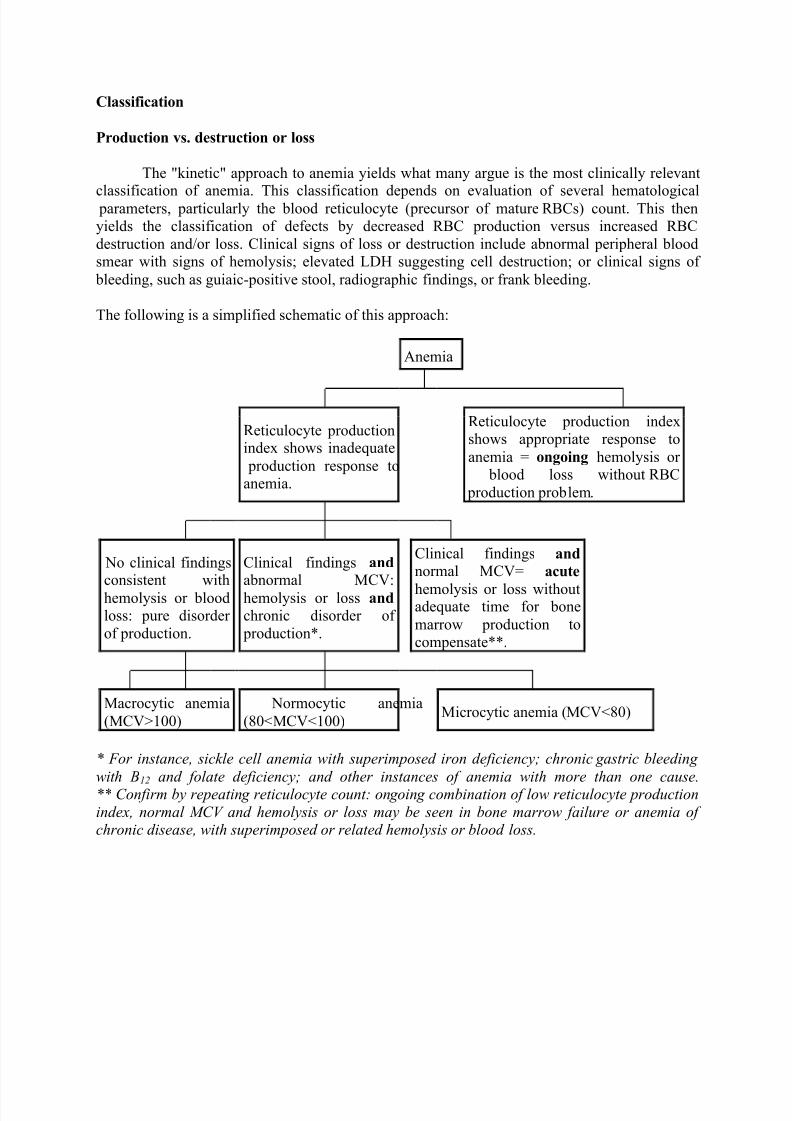
The "kinetic" approach to anemia yields what many argue is the most clinically relevant
classification of anemia.T
his classification depends on evaluation of several hematological parameters, particularly the blood reticulocyte (precursor of mature R BCs) count. This thenyields the classification of defects by decreased R BC production versus increased R BC
destruction and/or loss. Clinical signs of loss or destruction include abnormal peripheral bloodsmear with signs of hemolysis; elevated LDH suggesting cell destruction; or clinical signs of
bleeding, such as guiaic-positive stool, radiographic findings, or frank bleeding.
The following is a simplified schematic of this approach:
Anemia
R eticulocyte productionindex shows inadequate
production response toanemia.
R eticulocyte production indexshows appropriate response to
anemia = ongoing hemolysis or blood loss without R BC
production problem.
No clinical findingsconsistent with
hemolysis or bloodloss: pure disorder
of production.
Clinical findings and abnormal MCV:
hemolysis or loss and chronic disorder of
production*.
Clinical findings and normal MCV= acute
hemolysis or loss withoutadequate time for bone
marrow production tocompensate**.
Macrocytic anemia
(MCV>100)
Normocytic anemia
(80<MCV<100)Microcytic anemia (MCV<80)
* F or instance, sickle cell anemia with superimposed iron deficiency; chronic g astric bleedin g
with B12 and folate deficiency; and other instances of anemia with more than one cause. ** C onfirm by repeatin g reticulocyte count: on g oin g combination of low reticulocyte production
index, normal M CV and hemolysis or loss may be seen in bone marrow failure or anemia of chronic disease, with superimposed or related hemolysis or blood loss.

8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 11/17
Red blood cell size
In the morphological approach, anemia is classified by the size of red blood cells; this iseither done automatically or on microscopic examination of a peripheral blood smear. The size is
reflected in the mean corpuscular volume (MCV). If the cells are smaller than normal (under 80
fl), the anemia is said to be microcytic; if they are normal size (80±100 fl), normocytic; and if they are larger than normal (over 100 fl), the anemia is classified as macrocytic. This schemequickly exposes some of the most common causes of anemia; for instance, a microcytic anemia
is often the result of iron deficiency. In clinical workup, the MCV will be one of the first piecesof information available; so even among clinicians who consider the "kinetic" approach more
useful philosophically, morphology will remain an important element of classification anddiagnosis.
Here is a schematic representation of how to consider anemia with MCV as the starting point:
Anemia
Macrocytic
anemia(MCV>100)
Normocytic
anemia (MCV 80± 100)
Microcytic
anemia(MCV<80)
Highreticulocyte
count
Lowreticulocyte
count
Other characteristics visible on the peripheral smear may provide valuable clues about a more
specific diagnosis; for example, abnormal white blood cells may point to a cause in the bonemarrow.
Microcytic anemia
Microcytic anemia is primarily a result of hemoglobin synthesis failure/insufficiency, whichcould be caused by several etiologies:
y Heme synthesis defecto Iron deficiency anemiao Anemia of chronic disease (more commonly presenting as normocytic anemia)
y Globin synthesis defecto alpha-, and beta-thalassemia
o HbE syndromeo HbC syndrome
o and various other unstable hemoglobin diseases
8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 12/17
y Sideroblastic defecto Hereditary sideroblastic anemia
o Acquired sideroblastic anemia, including lead toxicityo R eversible sideroblastic anemia
Iron deficiency anemia is the most common type of anemia overall and it has many causes.R BCs often appear hypochromic (paler than usual) and microcytic (smaller than usual) whenviewed with a microscope.
y Iron deficiency anemia is caused by insufficient dietary intake or absorption of iron to
replace losses from menstruation or losses due to diseases. Iron is an essential part of hemoglobin, and low iron levels result in decreased incorporation of hemoglobin into red
blood cells. In the United States, 20% of all women of childbearing age have irondeficiency anemia, compared with only 2% of adult men. The principal cause of iron
deficiency anemia in premenopausal women is blood lost during menses. Studies have
shown that iron deficiency without anemia causes poor school performance and lower IQ
in teenage girls. Iron deficiency is the most prevalent deficiency state on a worldwide basis. Iron deficiency is sometimes the cause of abnormal fissuring of the angular
(corner) sections of the lips (angular stomatitis).y Iron deficiency anemia can also be due to bleeding lesions of the gastrointestinal tract.
Faecal occult blood testing, upper endoscopy and lower endoscopy should be performedto identify bleeding lesions. In men and post-menopausal women the chances are higher
that bleeding from the gastrointestinal tract could be due to colon polyp or colorectalcancer.
y Worldwide, the most common cause of iron deficiency anemia is parasitic infestation(hookworm, amebiasis, schistosomiasis and whipworm).
Macrocytic anemia
y Megaloblastic anemia, the most common cause of macrocytic anemia, is due to adeficiency of either vitamin B12, folic acid (or both). Deficiency in folate and/or vitamin
B12 can be due either to inadequate intake or insufficient absorption. Folate deficiencynormally does not produce neurological symptoms, while B12 deficiency does.
o Pernicious anemia is caused by a lack of intrinsic factor. Intrinsic factor isrequired to absorb vitamin B12 from food. A lack of intrinsic factor may arise
from an autoimmune condition targeting the parietal cells (atrophic gastritis) that produce intrinsic factor or against intrinsic factor itself. These lead to poor
absorption of vitamin B12.o Macrocytic anemia can also be caused by removal of the functional portion of the
stomach, such as during gastric bypass surgery, leading to reduced vitaminB12/folate absorption. Therefore one must always be aware of anemia following
this procedure.y Hypothyroidism
y Alcoholism commonly causes a macrocytosis, although not specifically anemia. Other types of Liver Disease can also cause macrocytosis.
y Methotrexate, zidovudine, and other drugs that inhibit DNA replication.

8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 13/17
Macrocytic anemia can be further divided into "megaloblastic anemia" or "non-megaloblasticmacrocytic anemia". The cause of megaloblastic anemia is primarily a failure of DNA synthesis
with preserved R NA synthesis, which result in restricted cell division of the progenitor cells. Themegaloblastic anemias often present with neutrophil hypersegmentation (6±10 lobes). The non-
megaloblastic macrocytic anemias have different etiologies (i.e. there is unimpaired DNA globin
synthesis,) which occur, for example in alcoholism.
In addition to the non-specific symptoms of anemia, specific features of vitamin B 12
deficiency include peripheral neuropathy and subacute combined degeneration of the cord withresulting balance difficulties from posterior column spinal cord pathology. Other features may
include a smooth, red tongue and glossitis.
The treatment for vitamin B12-deficient anemia was first devised by William Murphy who bled dogs to make them anemic and then fed them various substances to see what (if anything)
would make them healthy again. He discovered that ingesting large amounts of liver seemed tocure the disease. George Minot and George Whipple then set about to chemically isolate the
curative substance and ultimately were able to isolate the vitamin B12 from the liver. All threeshared the 1934 Nobel Prize in Medicine.
Normocytic anemia
Normocytic anemia occurs when the overall hemoglobin levels are always decreased, but the red blood cell size (Mean corpuscular volume) remains normal. Causes include:
y Acute blood loss
y Anemia of chronic diseasey Aplastic anemia (bone marrow failure)
y Hemolytic anemia
Dimorphic anemia
When two causes of anemia act simultaneously, e.g., macrocytic hypochromic, due to
hookworm infestation leading to deficiency of both iron and vitamin B12 or folic acid or following a blood transfusion more than one abnormality of red cell indices may be seen.
Evidence for multiple causes appears with an elevated R BC distribution width (R DW), whichsuggests a wider-than-normal range of red cell sizes.
Heinz body anemia
Heinz bodies form in the cytoplasm of R BCs and appear like small dark dots under themicroscope. There are many causes of Heinz body anemia, and some forms can be drug induced.
It is triggered in cats by eating onions
or acetaminophen (paracetamol). It can be triggered indogs by ingesting onions or zinc, and in horses by ingesting dry red maple leaves.
Causes
8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 14/17
Broadly, causes of anemia may be classified as impaired red blood cell (R BC) production, increased R BC destruction (hemolytic anemias), blood loss and fluid overload
(hypervolemia). Several of these may interplay to eventually cause anemia. Indeed, the mostcommon cause of anemia is blood loss, but this usually doesn't cause any lasting symptoms
unless a relatively impaired R BC production develops because of iron deficiency.
Impaired RBC production
y Disturbance of proliferation and differentiation of stem cells.o Pure red cell aplasia
o Aplastic anemia, affecting all kinds of blood cells. Fanconi anemia is a hereditarydisorder or defect featuring aplastic anemia and various other abnormalities.
o Anemia of renal failure, by insufficient erythropoietin productiono Anemia of endocrine disorders
y Disturbance of proliferation and maturation of erythroblastso
Pernicious anemia is a form of megaloblastic anemia due to vitamin B12 deficiency dependent on impaired absorption of vitamin B12.o Anemia of folic acid deficiency. As with vitamin B12, it causes megaloblastic
anemiao Anemia of prematurity, by diminished erythropoietin response to declining
hematocrit levels, combined with blood loss from laboratory testing. It generallyoccurs in premature infants at 2 to 6 weeks of age.
o iron deficiency, resulting in deficient heme synthesiso thalassemias, causing deficient globin synthesis
o Anemia of renal failure (also causing stem cell dysfunction)
y Other mechanisms of impaired
R
BC productiono Myelophthisic anemia
or Myelophthisis is a severe type of anemia resulting from
the replacement of bone marrow by other materials, such as malignant tumors or granulomas.
o Myelodysplastic syndromeo anemia of chronic inflammation
Increased RBC destruction
Anemias of increased red blood cell destruction are generally classified as hemolyticanemias. These are generally featuring jaundice and elevated LDH levels.
y Intrinsic (intracorpuscular) abnormalities, where there the red blood cells have defects
that cause premature destruction. All of these, except paroxysmal nocturnalhemoglobinuria, are hereditary genetic disorders.
o Hereditary spherocytosis is a hereditary defect that results in defects in the R BCcell membrane, causing the erythrocytes to be sequestered and destroyed by the
spleen.o Hereditary elliptocytosis,
another defect in membrane skeleton proteins

8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 15/17
o Abetalipoproteinemia, causing defects in membrane lipidso Enzyme deficiencies
Pyruvate kinase and hexokinase deficiencies, causing defect glycolysis Glucose-6-phosphate dehydrogenase deficiency and glutathione
synthetase deficiency, causing increased oxidative stress
o Hemoglobinopathies
Sickle cell anemia Hemoglobinopathies causing unstable hemoglobins
o paroxysmal nocturnal hemoglobinuria
y Extrinsic (extracorpuscular) abnormalitieso Antibody-mediated
Warm autoimmune hemolytic anemia is an anemia caused by autoimmuneattack against red blood cells, primarily by IgG. It is the most common of
the autoimmune hemolytic diseases. It can be idiopathic, that is, without
any known cause, drug-associated or secondary to another disease such as
systemic lupus erythematosus, or a malignancy, such as chroniclymphocytic leukemia (CLL)
Cold agglutinin hemolytic anemia is primarily mediated by IgM. It can beidiopathic or result from an underlying condition.
R h disease, one of the causes of hemolytic disease of the newborno Transfusion reaction to blood transfusions
Mechanical trauma to red cells
Microangiopathic hemolytic anemias, including thromboticthrombocytopenic purpura and disseminated intravascular coagulation
[13]
Infections, including malaria heart surgery
Blood loss
y Anemia of prematurity from frequent blood sampling for laboratory testing, combinedwith insufficient R BC production.
y Trauma or surgery, causing acute blood loss
y Gastrointestinal tract lesions, causing a rather chronic blood loss
y Gynecologic disturbances, also generally causing chronic blood loss
Fluid overload
Fluid overload (hypervolemia) causes decreased hemoglobin concentration and apparent anemia:
y General causes of hypervolemia include excessive sodium or fluid intake, sodium or
water retention and fluid shift into the intravascular space.y Anemia of pregnancy is anemia that is induced by blood volume expansion experienced
in pregnancy.
Treatments
8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 16/17
There are many different treatments for anemia and they depend on severity and cause.
Iron deficiency from nutritional causes is rare in non-menstruating adults (men and post-menopausal women). The diagnosis of iron deficiency mandates a search for potential sources of
loss such as gastrointestinal bleeding from ulcers or colon cancer. Mild to moderate iron
deficiency anemia is treated by oral iron supplementation with ferrous sulfate, ferrous fumarate,or ferrous gluconate. When taking iron supplements, it is very common to experience stomachupset and/or darkening of the feces. The stomach upset can be alleviated by taking the iron with
food; however, this decreases the amount of iron absorbed. Vitamin C aids in the body's abilityto absorb iron, so taking oral iron supplements with orange juice is of benefit.
Vitamin supplements given orally (folic acid) or subcutaneously (vitamin B-12) will
replace specific deficiencies.
In anemia of chronic disease, anemia associated with chemotherapy, or anemia associated
with renal disease, some clinicians prescribe recombinant erythropoietin, epoetin alfa, to
stimulate red cell production.
In severe cases of anemia, or with ongoing blood loss, a blood transfusion may be
necessary.
Blood transfusions
Doctors attempt to avoid blood transfusion in general, since multiple lines of evidence
point to increased adverse patient clinical outcomes with more intensive transfusion strategies.The physiological principle that reduction of oxygen delivery associated with anemia leads to
adverse clinical outcomes is balanced by the finding that transfusion does not necessarily
mitigate these adverse clinical outcomes.
In severe, acute bleeding, transfusions of donated blood are often lifesaving.
Improvements in battlefield casualty survival is attributable, at least in part, to the recentimprovements in blood banking and transfusion techniques.
Transfusion of the stable but anemic hospitalized patient has been the subject of
numerous clinical trials.
Four randomized controlled clinical trials have been conducted to evaluate aggressive
versus conservative transfusion strategies in critically-ill patients. All four of these studies failed
to find a benefit with more aggressive transfusion strategies.
In addition, at least two retrospective studies have shown increases in adverse clinical
outcomes in critically ill patients that underwent more aggressive transfusion strategies.
Hyperbaric oxygen
8/8/2019 Brief History of the Disease
http://slidepdf.com/reader/full/brief-history-of-the-disease 17/17
Treatment of exceptional blood loss (anemia) is recognized as an indication for hyperbaric oxygen (HBO) by the Undersea and Hyperbaric Medical Society.The use of HBO is
indicated when oxygen delivery to tissue is not sufficient in patients who cannot be transfusedfor medical or religious reasons. HBO may be used for medical reasons when threat of blood
product incompatibility or concern for transmissible disease are factors.The beliefs of some
religions (ex: Jehovah's Witnesses) may prohibit the receipt of transfused blood products.
In 2002, Van Meter reviewed the publications surrounding the use of HBO in severe
anemia and found that all publications report a positive result.
















![HANSEN’S DISEASE - MAPHN.orgs[1].pdf• To discuss brief history of Hansen’s disease ... cause claw hand deformity • Lower extremities – examine for loss of sensation, muscle](https://static.fdocuments.us/doc/165x107/5e8135b5e5915b01c87dd49e/hansenas-disease-maphnorg-s1pdf-a-to-discuss-brief-history-of-hansenas.jpg)