
Brian Arndt, MD Assistant Professor Department of Family Medicine
29
Estimating the Prevalence of Diabetes in Wisconsin Through an Innovative Data Exchange Between a Department of Family Medicine and Public Health Brian Arndt, MD Assistant Professor Department of Family Medicine UW School of Medicine & Public Health WREN Conference September 15, 2011
-
Upload
freya-franklin -
Category
Documents
-
view
38 -
download
2
description
Estimating the Prevalence of Diabetes in Wisconsin Through an Innovative Data Exchange Between a Department of Family Medicine and Public Health. Brian Arndt, MD Assistant Professor Department of Family Medicine UW School of Medicine & Public Health WREN Conference September 15, 2011. - PowerPoint PPT Presentation
Transcript of Brian Arndt, MD Assistant Professor Department of Family Medicine

Estimating the Prevalence of Diabetes in Wisconsin Through an Innovative Data Exchange
Between a Department of Family Medicine and Public Health
Brian Arndt, MD Assistant Professor
Department of Family MedicineUW School of Medicine & Public Health
WREN ConferenceSeptember 15, 2011

Background• Diabetes is a prevalent chronic disease
affecting over 475,000 adults in Wisconsin• Wisconsin Behavioral Risk Factor Surveillance
System (WI BRFSS) data provide annual statewide diabetes prevalence estimates – Data not useful for estimating prevalence at
smaller geographic areas– Unable to track quality performance
indicators (e.g. A1c levels)

Alternative Surveillance Data
• Electronic Health Record (EHR) data from UW Department of Family Medicine (DFM) Clinics to identify a population with diabetes at a census block level– Geographic analyses and maps may lead to the
identification and surveillance of Wisconsin patients with diabetes at the neighborhood level
• Contains parameters for quality evaluation (A1c, BP, Cholesterol, Kidney health, etc.)

Project Goals
• Can EHR data improve diabetes prevalence estimates over telephone survey data?
• How do diabetes prevalence estimates based on DFM clinic data and BRFSS compare?
• Evaluate Risk, Control, & Co-morbidities
• Link EHR data to community indicators (Median Income, Economic Hardship Index)

BRFSS Diabetes Definition
• Have you ever been told by a doctor that you have diabetes? – Gestational diabetes and pre-diabetes excluded
• Does not distinguish between Type 1 and Type 2

UW MED-PHINEXType 2 Diabetes Definition
• Problem list AND Encounter diagnosis
• Problem list OR Encounter Dx, AND– Fasting glucose ≥ 126 mg/dL– 2 hour GTT glucose ≥ 200 mg/dL– Random glucose ≥ 200 mg/dL– A1c ≥ 6.5%
or– Anti-diabetic medication Rx ≥ 1
> 2
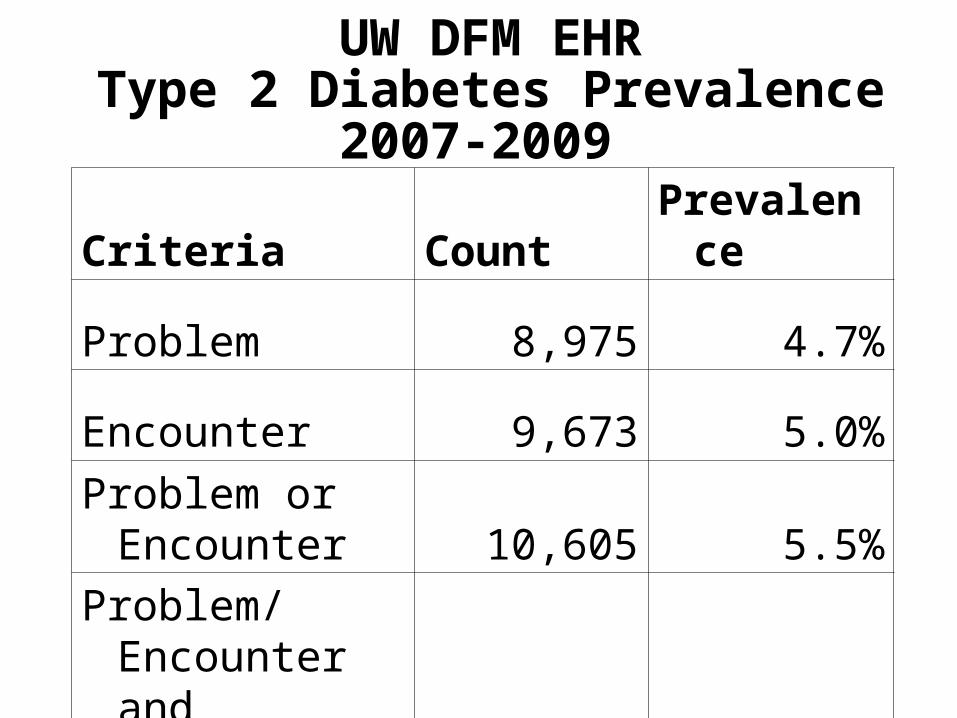
UW DFM EHRType 2 Diabetes Prevalence
2007-2009
Criteria Count Prevalence
Problem 8,975 4.7%
Encounter 9,673 5.0%
Problem or Encounter 10,605 5.5%
Problem/ Encounter and Labs/Meds 9,034 4.7%

2007-2009 Adult Type 2 Diabetes
WI BRFSS Data UW DFM Clinic Data
*NPrevalence
(95% CI) NPrevalence
(95% CI)
Overall 2,007 7.2(6.8-7.7) 9,023 6.0(5.9-6.1)
Sex
Female 1109 7.0 (6.4-7.7) 4,329 5.2 (5.1-5.4)
Male 898 7.5 (6.8-8.2) 4,694 6.9 (6.7-7.1)
Age Group
18-34 34 1.2(0.5-1.8) 366 0.7 (0.6-0.8)
35-64 959 7.0 (6.4-7.7) 5,589 6.8 (6.6-7.0)
65+ 991 18.3 (16.7-19.8) 3,068 17.4 (16.8-18.0)

2007-2009 Adult Type 2 Diabetes
WI BRFSS Data UW DFM Clinic Data
*NPrevalence
(95% CI) NPrevalence
(95% CI)
Race/Ethnicity
White (Non-Hispanic) 1,617 6.9 (6.4-7.4) 7,676 5.9 (5.8-6.0)
Black (Non-Hispanic) 210 11.7 (8.5- 14.9) 514 11.1 (10.2-12.0)
Other (Non-Hispanic) 124 10.5 (6.6-14.3) 281 6.2 (5.5-6.9)
Hispanic 31 5.5 (2.8-8.1) 352 7.0 (6.3-7.8)

2007-2009 Adult Type 2 Diabetes
WI BRFSS Data UW DFM Clinic Data
*NPrevalence
(95% CI) NPrevalence
(95% CI)
BMI
Normal or Underweight (<25.0) 249 2.7 (2.2-3.2) 513 1.6 (1.5-1.8)
Overweight (25.0 - <30.0) 613 6.3 (5.5-7.1) 1,458 4.4 (4.2-4.7)
Obese (30.0 - <40.0) 775 12.6 (11.4-13.9) 3,178 11.2 (10.9-11.6)
Morbidly Obese (≥40.0) 233 26.7 (21.5-31.9) 1,440 22.3 (21.3-23.3)

2007-2009 Adult Type 2 Diabetes
WI BRFSS Data UW DFM Clinic Data
*NPrevalence
(95% CI) NPrevalence
(95% CI)
Smoking
Never 865 5.9 (5.2-6.5) 3,619 5.1 (5.0-5.3)
Former 845 11.2 (10.1-12.3) 3,377 10.2 (9.8-10.5)
Current 294 5.8 (4.7-6.8) 1,326 5.2 (5.0-5.5)
Passive NA - 105 6.7 (5.4-7.9)

Multivariate Logistic Regression of Type 2 Diabetes Risk in Adults
• Good agreement with BRFSS• Each factor is a significant predictor in
direction expected:– Age, Gender, Race / Ethnicity, Smoking, BMI,
Median Income
• Insurance Status & Economic Hardship also predict risk
• DFM data volume 4x greater (or more) compared to BRFSS – provides greater precision and resolution

Economic Hardship Index
• Census data from the Census Block Group level
• Index from 1 to 100 (No → Very Hard)• Variables include:
– Crowded housing– Federal poverty level– Unemployment– Less than high school – Dependency (% under 18 or over 64)– Median income per capita

Wisconsin Economic Hardship Index

Madison Economic Hardship Index

MilwaukeeEconomic Hardship Index

Diabetes Co-MorbiditiesOdds Ratio = P(Disease | Diabetes)
P(Disease | No Diabetes)
Co-Morbidity Prevalence OR 95% CI
Depression 25.1% 1.7 1.7-1.8
Asthma 11.0% 1.5 1.4-1.6
COPD 8.4% 4.2 3.8-4.5
CKD 26.1% 9.6 9.1-10.2
Among 9,023 Adult Patients with Type 2 Diabetes

Diabetes Co-MorbiditiesOdds Ratio = P(Disease | Diabetes)
P(Disease | No Diabetes)
Co-Morbidity Prevalence OR 95% CI
IVD- Cardiac 16.2% 7.9 7.4-8.4
IVD – Cerebral 4.4% 5.7 5.0-6.4
CHF 9.1% 9.2 8.4-10.1
Among 9,023 Adult Patients with Type 2 Diabetes

Diabetes Co-MorbiditiesOdds Ratio = P(Disease | Diabetes)
P(Disease | No Diabetes)
Co-Morbidity Prevalence OR 95% CI
MI 2.1% 6.4 5.4-7.7
PTCA 1.8% 6.9 5.8-8.4
Dementia 3.2% 3.7 3.3-4.3
Among 9,023 Adult Patients with Type 2 Diabetes

Diabetes Co-morbiditiesConclusions
• Each risk is significant • Higher complexity likely leads to higher
utilization & cost• Next Steps – data mining
– What predicts co-morbidity?– Which co-morbidities group together?– What predicts clusters ?

Predictors of HbA1c Control in Patients with Type 2 Diabetes
Kristin Gallagher
University of Wisconsin
Department of Population Health Sciences
M.S. Thesis
June 2011

Methods
• Adult Type 2 Diabetes Definition
• Current A1c Value / Binary at 7%
• Logistic Regression
• Predictors of Poor A1c Control (>7%)– Age, Gender, Race / Ethnicity, Economic
Hardship Index, BMI, Depression

Regression Results Poor A1c Control
Characteristic OR 95% CI P-value
Age Group 0.0033
18-240.92 [0.52 - 1.60]
25-341.26 [0.98 - 1.62]
35-44 1.26 [1.08 - 1.46]
45-54 1.23 [1.09 -1.39]
55-64 1.00
Race/Ethnicity <.0001
White (Non-Hispanic)1.00
Black (Non-Hispanic)1.48 [1.20 - 1.83]
Other (Non-Hispanic)1.45 [1.09 - 1.93]
Hispanic/Latino 2.08 [1.60 - 2.71]

Regression Results Poor A1c Control
Characteristic OR 95% CI P-value
Sex 0.0031
Male1.00
Female0.85 [0.76 - 0.95]
Economic Hardship Index 0.0011
EHI <201.00
EHI 20 to <301.56 [1.18 - 2.05]
EHI >301.74 [1.28 - 2.37]
BMI <.0001
Normal or Underweight 1.00
Overweight 1.09 [0.83 - 1.44]
Obese 1.59 [1.23 - 2.06]
Morbidly Obese 1.76 [1.34 - 2.32]

Conclusions
• Socio-demographic factors:– Middle age groups, black, Hispanic, and other
race/ethnicities, obese, and morbidly obese BMI were all significantly associated with having higher odds of being in poor control
– Patients living in areas with increased economic hardship index (20-30; >30) have higher odds of being in poor control – this was significant
• Health factors:– Those without depression were found to have
significantly higher odds of being in poor control

Diabetes Next Steps
• Evaluate comorbidity predictors
• HEDIS performance definitions & analysis (PCP & clinic level; P4P)
• Measures of utilization in population x status
• Data mining & modeling community factors
• Expand variables exchanged

Diabetes Next Steps – GIS / Spatial Analysis

Diabetes Next Steps – GIS / Spatial Analysis

Collaborative Effort – Thank you!
• Brian Arndt-UW DFM• Amy Bittrich-DPH• Bill Buckingham-UW APL• Jenny Camponeschi-DPH• Michael Coen-UW Biostats• Tim Chang-UW Biostats• Dan Davenport-UW Health• Kristin Gallager-UW Pop
Health• Theresa Guilbert (PI)-UW
Peds
• Larry Hanrahan-DPH
• Lynn Hrabik-DPH• Angela Nimsgern-DPH• David Page-UW Biostats• Mary Beth Plane-UW DFM• David Simmons-UW DFM• Aman Tandias-SLH• Jon Temte-UW DFM• Kevin Thao-UW DFM• Carrie Tomasallo-DPH


















